
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 06 June 2024
Sec. Public Health Education and Promotion
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1393188
This article is part of the Research Topic Breaking Barriers in LGBT+ Health: Innovations and Insights View all 9 articles
 Ughetta Maria Favazzi1†
Ughetta Maria Favazzi1† Matteo Marconi2†
Matteo Marconi2† Pietro Carbone1
Pietro Carbone1 Debora Guerrera1
Debora Guerrera1 Angela Ruocco2
Angela Ruocco2 Martina Manoli2,3
Martina Manoli2,3 Francesca Molinaro1
Francesca Molinaro1 Federica Maria Regini1
Federica Maria Regini1 Andrea Vittozzi1
Andrea Vittozzi1 Alfonso Mazzaccara1
Alfonso Mazzaccara1 Marina Pierdominici2*
Marina Pierdominici2*Background: Transgender and gender diverse (TGD) individuals face significant healthcare barriers, with one of the most critical being the inadequate knowledge and skills of healthcare professionals (HCPs) in TGD health. To address this issue, we undertook a project to develop a distance learning course for all healthcare professions, encompassing a comprehensive range of topics related to TGD health issues.
Objectives: This study aimed to evaluate the impact of a course on gender-affirming healthcare competence, with a focus on knowledge acquisition and satisfaction levels. The hypothesis was that participating in the course would enhance the participants' knowledge on the covered topics.
Methods: A distance learning course, designed for all Continuing Medical Education professions, was conducted between March and September 2023. The course was structured according to the Problem-Based Learning methodology. We implemented a pre-test vs. post-test study design to evaluate the enhancement of knowledge, based on a set of Multiple Choice Questions (MCQs), and investigated users' satisfaction through the administration of a semi-structured questionnaire. We examined the pre- and post-course proportions of correct responses to questions, along with the mean score difference, categorized by learners' sex, age, and geographical area. Eventually, a Satisfaction Training Index was created.
Results: The maximum capacity was reached, with 29,998 out of 30,000 available spots filled. Of those enrolled, 18,282 HCPs successfully completed the training. Post-test results revealed an increase in correct answers across all MCQs, with overall mean score rising from 48.8 to 68.0 (p < 0.001). Stratified analysis indicated improvements across all participant categories. A higher average increase among female (19.87) compared to male enrollees (17.06) was detected (p < 0.001). Both “over 55” and “46–55” age groups showed the greatest score increases compared to “35–46” and “under 35” groups, despite no significant differences in pre-test scores. Course satisfaction was high, averaging 4.38 out of 5. Top-rated aspects included “learning new concepts” (4.49), “accessibility” (4.46), and “platform functionality” (4.46).
Conclusion: Our research hypothesis was confirmed by the significant increase in knowledge going from pre-test to post-test and by the high level of user satisfaction. The obtained results serve as a foundation for planning additional professional education in TGD health.
Transgender and gender diverse (TGD) people represent a broad spectrum of individuals whose gender identities differ from the assigned sex at birth (1). At the beginning of the twentieth century, TGD identities were often viewed through a pathological lens. However, the global medical community has since reclassified TGD identities as not being mental disorders. In the American Psychiatric Association's Diagnostic and Statistical Manual, Fifth Edition (DSM-5), published in 2013, the diagnosis of gender dysphoria pertains to the distress and discomfort associated with being TGD, rather than the gender identity itself (2). Subsequently, the World Health Organization's International Classification of Diseases, Eleventh Edition (ICD-11), released in 2019, includes gender incongruence in a chapter on sexual health, emphasizing the individual's experienced identity and the necessity for gender-affirming treatment arising from that identity (3).
Some TGD individuals—but not all—choose to modify their bodies to align more closely with their gender identity through a gender-affirming pathway that progresses in stages. This process may include hormonal treatment and/or surgical interventions (1, 4). It is crucial to highlight that the healthcare needs of the TGD population extend beyond the medical process of gender affirmation, which has been the primary focus of scientific literature to date. Indeed, there are general healthcare needs (e.g., participation in cancer screenings, etc.) that are similar to those of the cisgender population, although they require specific preparation. In line with what has been stated, international recommendations advocate for an inter- and multidisciplinary approach to TGD healthcare, involving professionals from various fields to support gender-affirming interventions as well as preventive care and chronic disease management (1). Unfortunately, TGD individuals still face significant healthcare challenges, resulting in health disparities compared to the cisgender population (4–8). These disparities, affecting both physical and mental wellbeing, arise from discrimination, systemic biases limiting healthcare access, and lack of knowledge and skills among healthcare professionals (HCPs) in delivering competent care to TGD individuals (4–6, 9). Indeed, across diverse disciplines, educational programs at all stages, spanning undergraduate, graduate, residency, and continuing education levels, have typically disregarded cultural or clinical training pertaining to TGD individuals (1, 10). Various international studies, mainly conducted in the US, Canada, and Europe, have reported instances of TGD individuals feeling estranged in healthcare settings due to a lack of knowledge among HCPs (8, 9, 11–15). Consequently, TGD individuals often avoid seeking healthcare, resulting in negative consequences like poor adherence to cancer screening, delayed disease diagnosis, and self-medication without proper supervision (6, 16, 17).
Underscoring the significance of training HCPs in TGD health is essential, as it is recognized as crucial not only by the TGD community but also by the HCPs themselves. Indeed, while previous studies reveal that only a minority of healthcare personnel have undergone training on TGD health (18–22), many of HCPs regard focused training as one of the most pressing measures necessary to enhance the wellbeing of this population (18, 23).
Although recommendations from international institutions and scientific organizations highlight the importance of HCPs' expertise in TGD issues (1, 24, 25), efforts to incorporate them into both undergraduate and graduate education are still nascent (1, 26). Furthermore, there is still limited evidence on the most effective way to deliver this training (27, 28); what we know is that all too often, this education is provided in a generic manner within courses dedicated to the health of the LGBT+ population, rather than being specifically targeted at addressing the health needs of the TGD population (26). To bridge this gap, and in alignment with the “Italian Plan for the Implementation and Dissemination of Gender Medicine” (29), the Reference Center for Gender Medicine and the Training Office, both located at the Istituto Superiore di Sanità (ISS)—National Institute of Health in Italy, in collaboration with the Ufficio Nazionale Antidiscriminazioni Razziali (UNAR)—National Office against Racial Discrimination, conducted a project aimed at developing a distance learning course targeting all healthcare professions, covering a comprehensive array of topics, such as gender identity, language, TGD health issues, best practices in serving TGD patients, and pertinent legislation. To the best of our knowledge, this was the first such institutional course in Italy and one of the few established at an international level. The objective of this study was to report the results regarding the effectiveness of the course in terms of knowledge improvement and the satisfaction levels of the participants.
With a commitment to developing a course characterized by a multidisciplinary approach that carefully addressed the needs of both HCPs and TGD individuals, a scientific board was established. Comprising recognized experts in TGD healthcare and legal domains, along with representatives from TGD organizations, the primary objective of this board was to identify thematic areas to be covered in the tailored training program for the target audience. Considering that the course represented the first institutional initiative of its kind in Italy, the scientific board deemed it appropriate to formulate a program targeting all healthcare professions, encompassing various aspects related to the care of TGD individuals, and taking into account diverse gender identities. In alignment with the aforementioned goal and considering the available scientific literature on the subject, the following topics were selected: components of sexual identity and its biological foundations, aspects pertinent to psychological support for individuals with gender incongruence in both developmental and adult stages (with a particular focus on communication between HCP and user), best practices for hormonal treatment in individuals with gender incongruence in both developmental and adult stages, fundamental aspects of the gender affirmation surgical pathway, and general principles of the right to gender identity in Italian law.
These themes were translated into the following specific Learning Objectives (LOs).
LO1. Describe the components of sexual identity and its biological bases;
LO2. Identify the aspects useful for providing psychological support to individuals experiencing gender incongruence, both in developmental stages and adulthood;
LO3. Identify best practices for gender affirming hormone therapy, spanning across developmental stages and adulthood;
LO4. Outline the fundamental aspects of gender affirmation surgery;
LO5. Understand the general principles of gender identity rights according to Italian law.
Additionally, a brochure focusing on Sexually Transmitted Infections was developed.
The distance course “Transgender Population: From Health to Rights” was accessible free of charge on the ISS e-learning platform (EDUISS, www.eduiss.it). The language utilized in the course was Italian. The course was structured according to Problem-Based Learning (PBL), a methodological approach based on andragogic principles, that stimulates participants to “learn to learn” solving real-world problems that reflect their work context (30). PBL was chosen due to its learning success (e.g., in critical thinking) and its increased usage as a teaching method, especially in medical and healthcare education (31). Over the years PBL has been adapted to the e-learning context and different learning models have been developed, depending on the level of interaction among participants and facilitators (32, 33).
In courses with high turnout, the participants follow the steps of the PBL on their own, without the presence of a facilitator. In this course, the entire PBL cycle (consisting in seven steps) was set up using Totara tools (forum, feedback, sharable content object reference model, file, book, folder, web pages, quiz, and certificate). The first steps of the PBL cycle, consisting of problem analysis and LOs identification, were provided through an interactive tool that allowed to track the results provided by participants.
The course, open to all healthcare professions, was delivered from March 27th, 2023, to September 22nd, 2023. The maximum number of subscribers was 30,000. Successful completion of the course included the release of 16 Continuing Medical Education (CME) credits. The estimated time required to complete all learning activities and the entire course was 16 h. Participants had access to the platform at any time of the day (24 h). According to the Italian regulation, ethics approval was not required for this study: by registering for the course on the online platform, the participants gave the consent to the use of their anonymous data.
The course was structured in four sections:
1. Introductive section: introduction to the course explaining its relevance, general aims and structure, general objectives of the course, guide for participants containing all the instructions to attend the course, Attitudes, Skills and Practices Questionnaire (ASPQ) at time T0, preliminary formative assessment test (pre-test) to set the initial knowledge with Multiple Choice Questions (MCQs). No minimum score was required to complete the pre-test.
2. PBL cycle with the following resources: a problem presentation, a Sharable Content Object Reference Model (SCORM) exercise for analyzing the problem and identifying specific LOs, research and study of materials (bibliographical references and a list of useful websites to be consulted, reading materials to deepen the topics of the course, and audio-video tutorials by experts), and the problem solution.
3. Conclusive section: ASPQ at time T1, formative assessment test (post-test) to set the acquired knowledge with the same MCQs set of the pre-test, final certification test, Satisfaction Questionnaire (SQ). The SQ, which was optionally fillable, could be accessed by users who had completed the learning unit. Passing the final certification test, consisting of 48 MCQs, was mandatory to complete the course and get the CME credits. The final certification test was passed with a score of at least 75% correct answers. Three passing attempts were allowed.
4. Follow-up: it includes ASPQ and formative assessment test at T2 (6 months after the end of the course, and ongoing at the time of writing).
It has been observed that MCQs may not be entirely suitable for evaluating the skills developed through PBL, as assessment ideally should gauge performance rather than simply correct responses (34). However, MCQ tests can be deemed appropriate for formative assessment, particularly when assessing a large volume of knowledge, as in the present case (35). The utilization of MCQ tests was also chosen since the evaluation targeted the levels of “understanding” and “remembering” (36). It was mandatory to answer all questions in each MCQ test.
When registering for the course on the e-learning platform, the following demographic and professional information about the participants was collected: sex, age, place of residence, CME profession and discipline, and professional status.
Before accessing the training resources two tools were administered:
- ASPQ. The Questionnaire consisted of batteries of items using Likert scale to detect attitudes, skills and practices;
- Pre-test. The test comprised 10 MCQs (two questions for each LO), aimed at acquiring insights into various areas of knowledge.
At the end of the course the following tools were administered:
- The same set of 10 MCQs was administered (post-test), prior to the CME certification exam;
- The same ASPQ was administered to assess changes over time;
- Participants who completed the learning unit were required to fill in the SQ, consisting of a battery of 18 items using a Likert scale from 1 (minimum level of agreement) to 5 (maximum level of agreement) and two open questions to collect the positive aspects and suggestions for improving the quality of the course.
All data were extracted from EDUISS platform. We performed a descriptive analysis (absolute numbers and percentages) to represent demographic, professional, and course completion status information. The pre-test and post-test results were reported as percentages of correct answers to each question and compared through the McNemar test. Data were stratified by sex, age categories and place of residence (Northwest Italy, Northeast Italy, Central Italy, South Italy, and Islands). A new variable denominated Score Increase (SI) was created using the difference between the post- and pre-test individual scores. To identify any differences in scores based on the variables under consideration, one-way analysis of variance (ANOVA) and post-hoc tests with Bonferroni method were carried out. We analyzed the satisfaction data taking into account all users who completed the SQ (n = 20,450), rather than only those who finished the course (n = 18,282), in order to mitigate the possibility of overestimating satisfaction. A Satisfaction Training Index (STI) was created using the average scores of the 18 items of the satisfaction scale. In particular, all satisfaction items were subjected to Pearson correlation that showed a large correlation (>0.6) (37). All items were also subjected to principal axis factorization analysis, which revealed a single factor that reproduces 69% of the total variability, thus the reliability of the unidimensional scale was assessed using Cronbach's alpha. The findings indicate excellent reliability of the instrument, with Cronbach's alpha value exceeding the index of 0.9 (38). To identify any differences in satisfaction based on participants' characteristics, ANOVA and post-hoc tests with Bonferroni method were carried out. Statistical analysis was performed using IBM SPSS Statistics 28.0. The results were considered statistically significant at p < 0.05.
The training was intended for all CME professions and disciplines and a maximum number of 30,000 members was expected. The maximum capacity has been reached, with a total of 29,998 participants enrolled. All participants were from Italy. The number of participants who completed the course (completers) was 18,282 (60.9%) out of the total enrolled users (Table 1); this proportion raised to 69.4% when excluding users who registered but never entered the course (3,667).
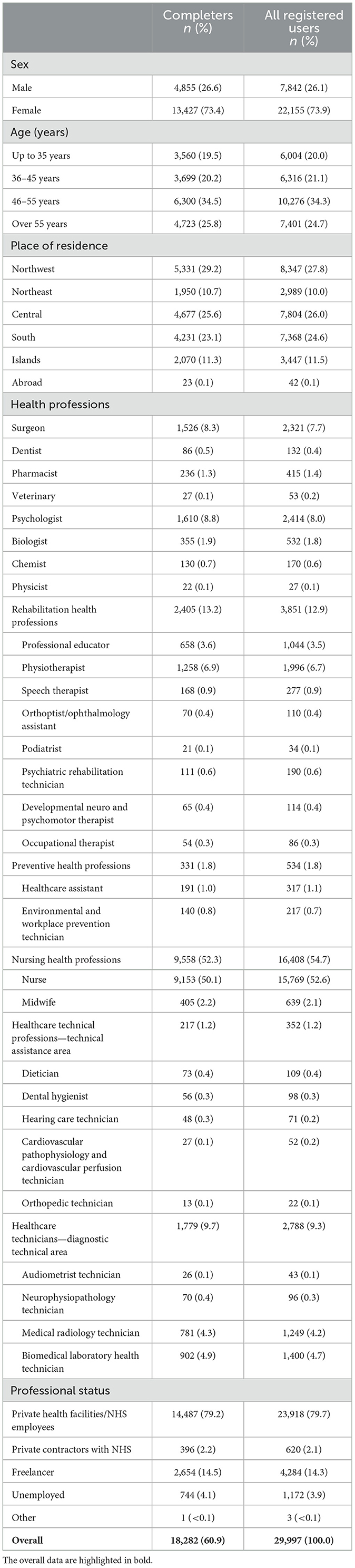
Table 1. Characteristics of participants.
Among the completers, 4,855 (26.6%) were males, and 13,427 (73.4%) were females. The mean age was 47.1 years, with the most represented age group being between 46 and 55 years (34.5%). Considering the place of residence, 29.2% of completers were from the Northwest of Italy, followed by the Central (25.6%), and the Southern (23.1%) areas. Around 11% of completers came from the Northeast and the Islands. In terms of professional status, most participants were NHS employees or employees of private health facilities (79.2%).
The results of the pre-test vs. post-test comparison are reported in Tables 2, 3. Table 2 displays the percentage of correct answers to test questions associated with each LO. We observed a significant improvement across all 10 questions (p < 0.001), as determined by the McNemar test. Particularly noteworthy are the questions linked to LO1 (i.e., the components of sexual identity and its biological bases), LO3 (i.e., best practices for gender affirming hormone therapy), and LO5 (i.e., general principles of gender identity rights), which exhibited a substantial increase in knowledge from pre- to post-test. Moreover, users initially demonstrated a stronger familiarity with topics related to LO2 (i.e., aspects useful for providing psychological support) and LO4 (i.e., fundamental aspects of gender affirmation surgery). Table 3 displays the results of the comparison between average pre-test and post-test scores according to participants' characteristics using t-test for paired data. The average overall pre-test and post-test scores were 48.8 and 67.9, respectively (p < 0.001), with a mean SI of 19.1. In stratified analysis, a significant improvement in average scores between pre- and post-test was recorded for all the categories considered. When considering SI, comparison by sex showed a higher average increase among females (19.8) compared to males (17.1), p < 0.001. Females also reported a higher average pre-test score than males (49.2 vs. 47.7, p < 0.001). ANOVA and post-hoc test by place of residence showed a higher score increase among completers in the Northwest (21.2) and Northeast (23.2), p < 0.001, compared to other geographical area. Post-hoc tests showed that users residing in northern areas obtained pre-test higher scores than users from other geographical areas.
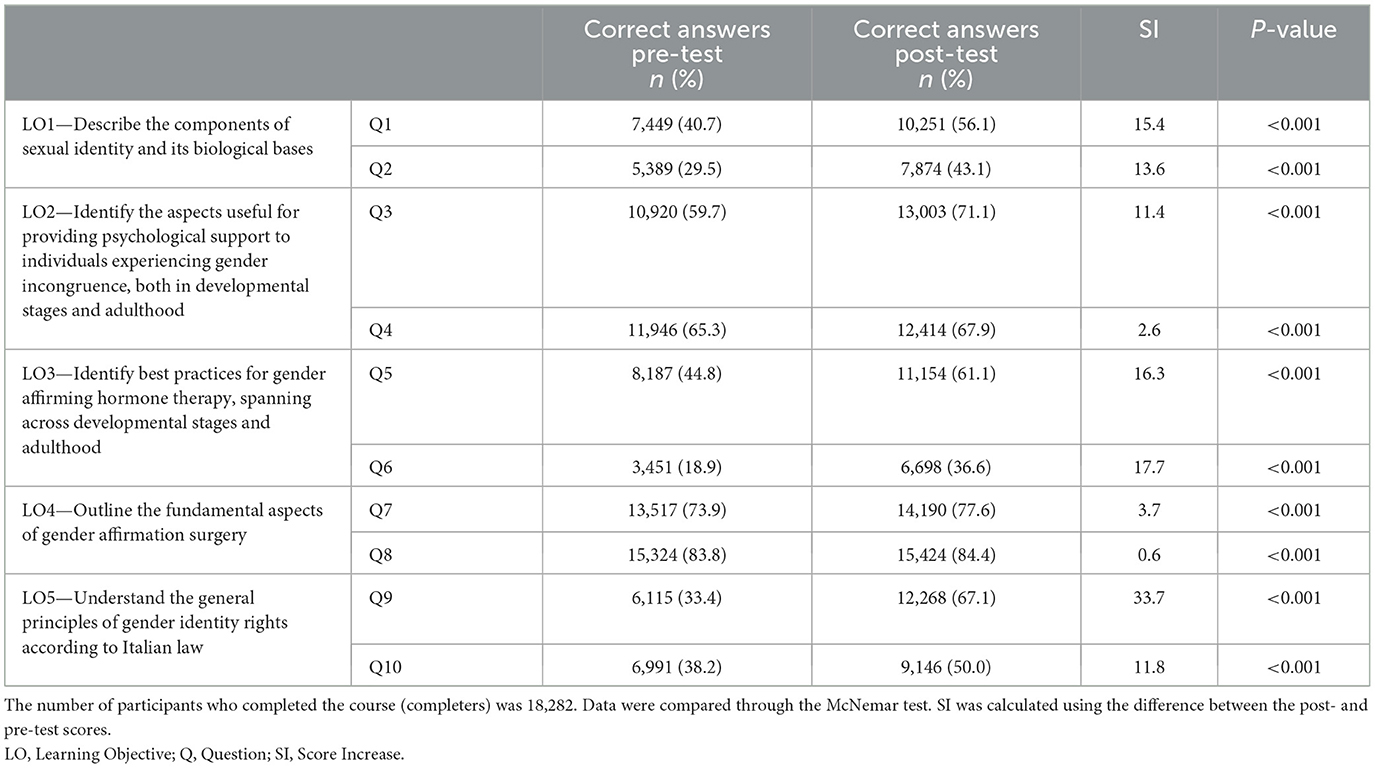
Table 2. Knowledge level of completers before and after the course.
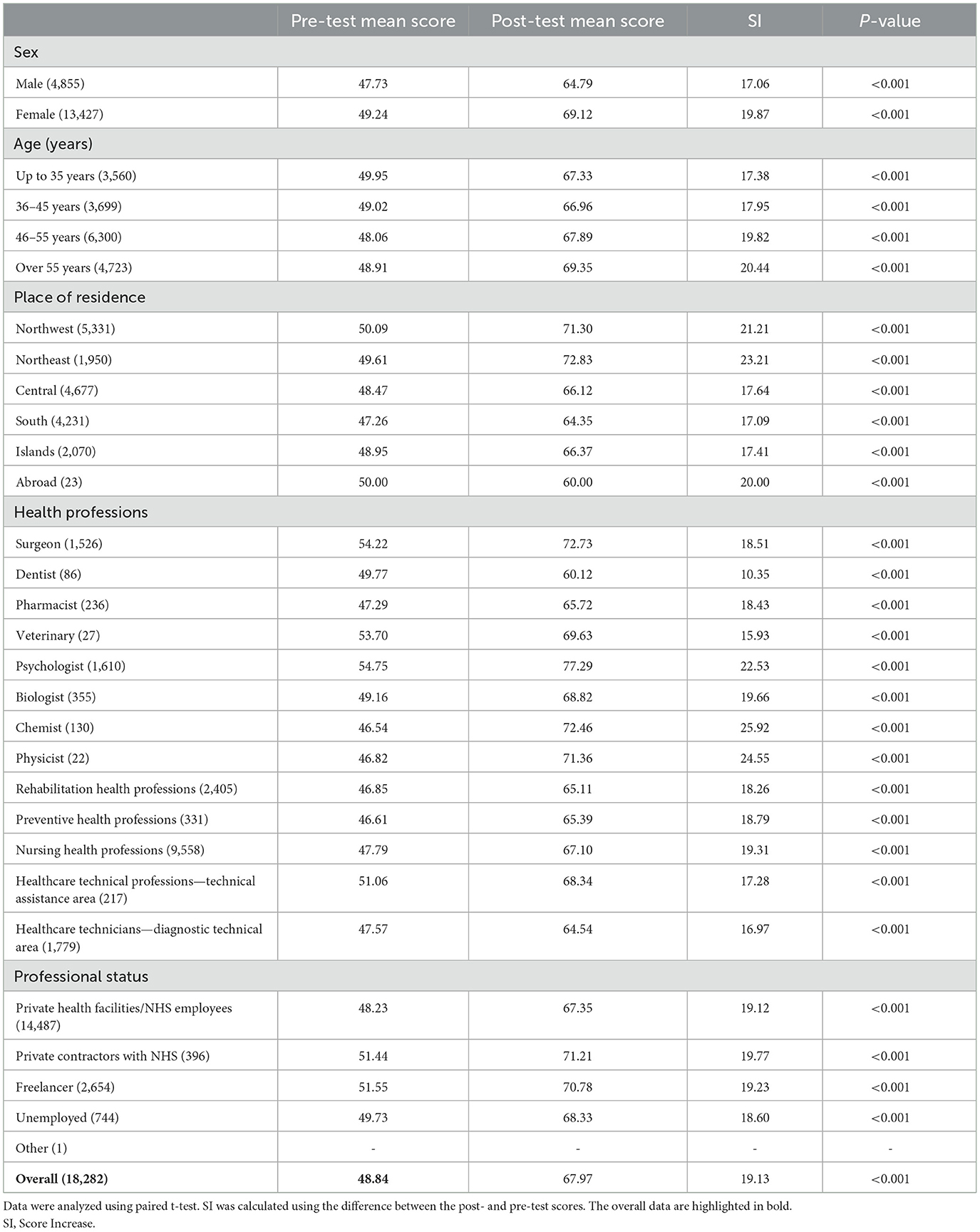
Table 3. Comparison of pre-test and post-test average scores among completers based on participants' characteristics.
Furthermore, “over 55” and “46–55” completers age groups showed the highest score increase compared to the “35–46” and “under 35” completers group, although there were no significant differences in the pre-test score between the age groups.
STI revealed an average satisfaction of 4.38 in all those who filled out the questionnaire. Consequently, a high overall approval of the course emerged, considering that the attributed scores were >4, with 5 representing the highest level of satisfaction (Figures 1–3).
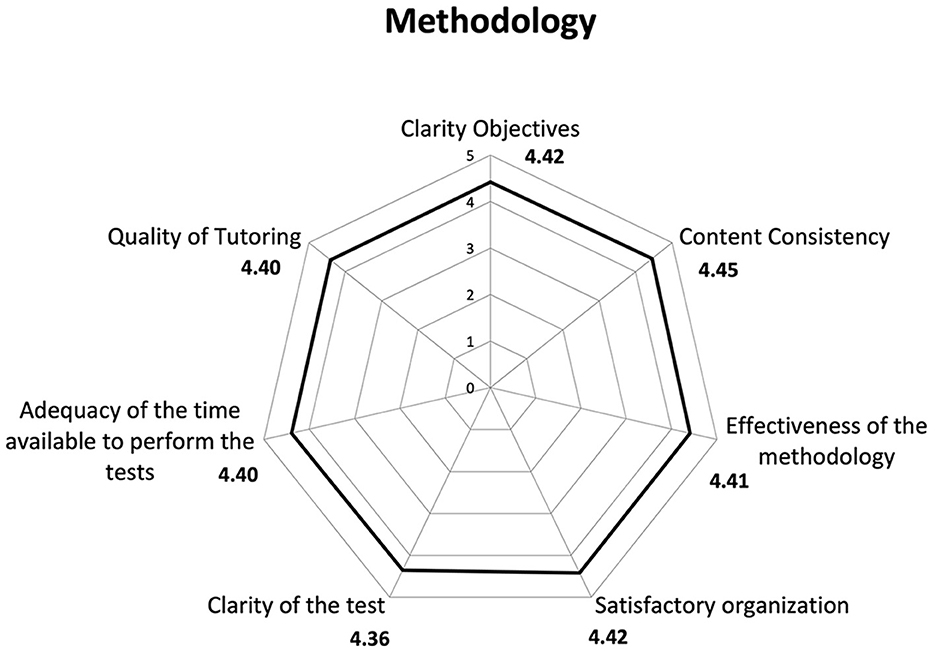
Figure 1. Results of Satisfaction Questionnaire on the learning methodology of the course. We analyzed the satisfaction data taking into account all users who completed the Satisfaction Questionnaire (n = 20,450).
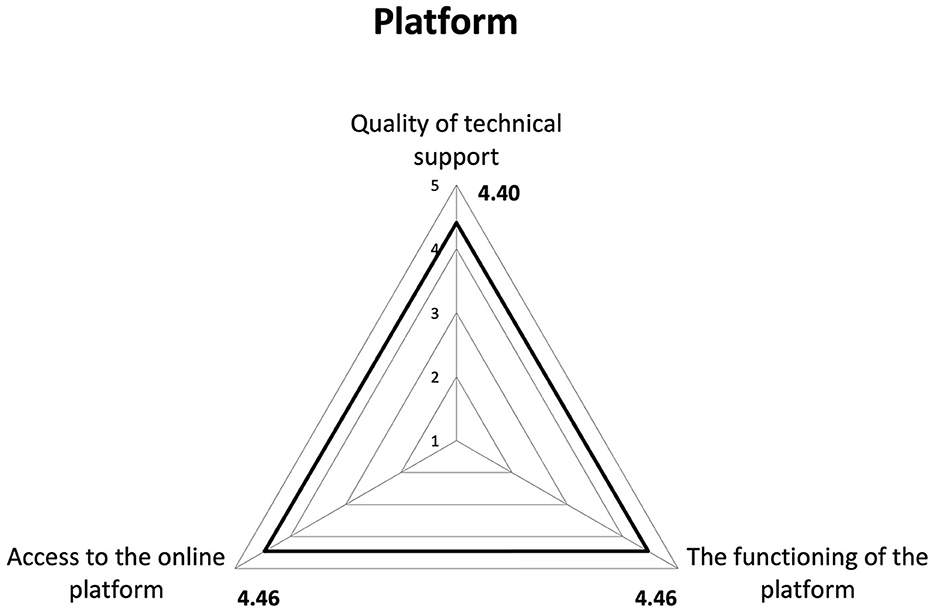
Figure 2. Results of Satisfaction Questionnaire on e-learning platform. We analyzed the satisfaction data taking into account all users who completed the Satisfaction Questionnaire (n = 20,450).
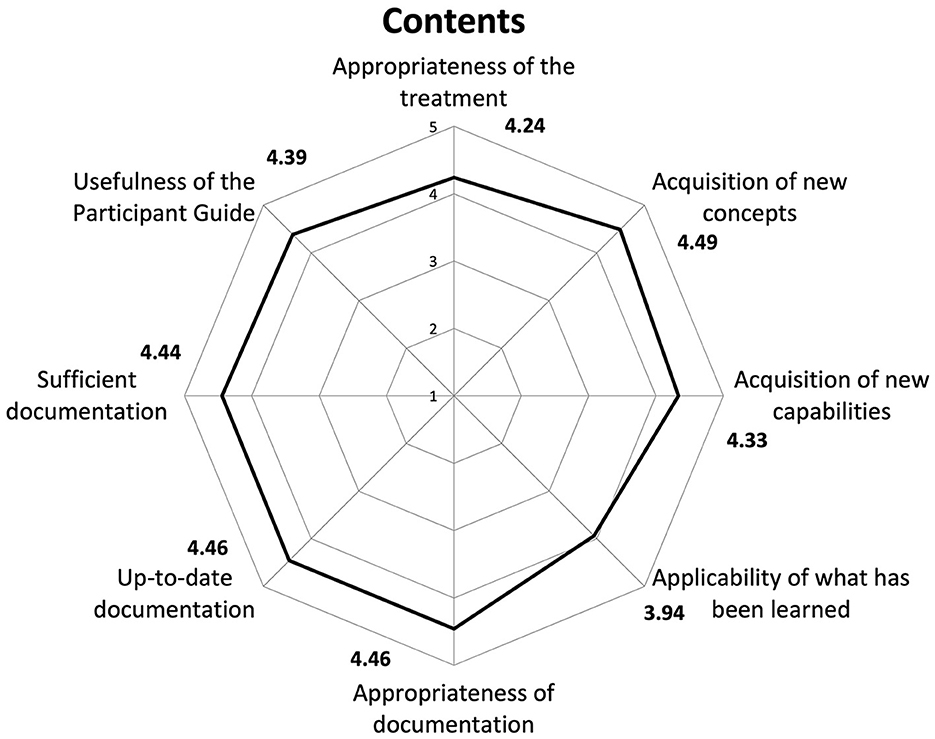
Figure 3. Results of Satisfaction Questionnaire on contents. We analyzed the satisfaction data taking into account all users who completed the Satisfaction Questionnaire (n = 20,450).
ANOVA by place of residence and Bonferroni post-hoc test showed that participants residing in the Islands reported a higher level of satisfaction (4.46), compared with participants from the Northwest (4.37), Central (4.38), and Southern Italy (4.37), p < 0.001. Lower satisfaction was observed among younger participants in comparison to other age groups, while no significant differences were found based on sex.
Regarding satisfaction with different aspects of the training, items that received scores closer to five included “learning new concepts” (4.49), “accessibility” (4.46), and the “functionality of the platform” (4.46). In contrast, a slightly lower score (3.94) was recorded for the item on participants' perception regarding the applicability of what they learned in the course to their professional context.
The course “Transgender Population: From Health to Rights” represents the first Italian institutional experience in training HCPs on TGD health. The primary innovative feature of this course lies in its teaching methodology, emphasizing active training. The PBL approach employed encourages participants to engage in “learning to learn” by tackling real-world problems that mirror their professional contexts (30, 39). According to Schmidt et al. (30), PBL leverages the presentation of a problem to stimulate participants' existing knowledge, facilitating more effective learning. In contrast to traditional methods, PBL requires participants to actively address and solve problems, taking charge of identifying their own LOs. Consequently, learners encounter cognitive conflicts and construct their understanding based on prior knowledge and experiences (40). Additional strengths of the course included its large participant base and its comprehensive approach to TGD health, which not only covered every aspect of the subject but also emphasized the importance of appropriate communication between healthcare professionals and the community, while simultaneously addressing the social and legal barriers that contribute to health inequalities.
The results of our course offer a foundation for understanding the effectiveness and reach of the training initiative. Overall, the high participation indicates a significant interest in the training across CME professions and disciplines. The significant concentration of participants aged 46–55 raises interesting questions about the training's appeal to mid-career professionals. Typically, individuals within the older demographic are noted to display heightened enthusiasm for online learning, attributed to their perceived higher self-efficacy and enhanced mental preparedness (41). Moreover, within our study, it is plausible that professionals in the 46–55 age bracket might have encountered fewer opportunities for exposure to or formal education on subjects like TGD health during their earlier training years. Conversely, in today's digital age, younger professionals often encounter diverse perspectives and emerging issues like TGD health more readily through their interactions on social media platforms and engagement with online communities. Understanding what attracts participants from different age groups can help tailor the course content, format, and outreach efforts to better meet the needs and interests of a diverse range of HCPs.
The outcomes derived from our course demonstrate a notable enhancement in the knowledge levels of participants, as evidenced by the comparison between pre-test and post-test results across all categories. This suggests that individuals with diverse backgrounds and characteristics derived substantial benefits from the course, affirming its effectiveness in reaching a broad audience. This emphasizes the importance of establishing a foundational knowledge on TGD health that is shared across various health professions. Sex-based analysis revealed a higher average increase among female participants compared to their male counterparts. The observation that females also reported a higher average pre-test score suggests a potential baseline difference in attitudes to transgender health topics (42, 43), further emphasizing the importance of tailoring educational interventions to address diverse starting points among participants.
In addition, the age-based analysis revealed that participants aged over 55 and those aged 46–55 demonstrated the highest score increase compared to younger age groups, despite no significant differences in the initial scores between age groups being detected. This finding is consistent with previous research indicating that older students tend to achieve higher grades than their younger counterparts (41, 44). Moreover, our study suggests that mid-career and older participants, who were more numerous as previously mentioned, may have been particularly motivated and engaged in the course. This heightened motivation and engagement could have contributed to the observed score improvements.
Analysis of the distribution of correct responses to pre-test and post-test questions highlighted some points of interest. Concerning aspects useful for providing psychological support (LO2) and the fundamental aspects of gender affirmation surgery (LO4), users showed a greater propensity to provide a correct answer during the pre-test. This result may reflect existing awareness or knowledge among participants regarding these important aspects of transgender health, although it's also plausible that the questions related to these topics were relatively less complex.
Conversely, concerning the description of components of sexual identity and its biological underpinnings (LO1), best practices for gender-affirming hormone therapy (LO3), and the general principles of gender identity rights (LO5), the initial assessment indicated a more pronounced educational gap. However, encouragingly, participants exhibited substantial improvement in their understanding of these topics by the conclusion of the course, as evidenced by the post-test results. These findings underscore the effectiveness of the course curriculum in addressing educational gaps and fostering knowledge acquisition among participants. Moreover, they provide valuable insights for enhancing question design in future iterations of the course. By identifying areas of strength and weakness in participant understanding, educators can refine course content and assessments to optimize learning outcomes and better meet the educational needs of the target audience.
In terms of participant satisfaction, our findings revealed a positive overall response. This high level of approval is noteworthy, signifying a strong endorsement of the course among the participants. It is worth noting that younger participants expressed lower satisfaction levels, suggesting a potential misalignment between course content and the expectations or requirements of this demographic. This highlights the importance of considering not only the knowledge level but also the satisfaction and engagement of participants when tailoring effective training programs. Collecting feedback from younger participants through surveys, focus groups, or individual interviews can provide invaluable insights into their specific needs, preferences, and areas for improvement.
Analyzing satisfaction with different aspects of the training, several key aspects stood out. Learning new concepts, access to the course, and the functioning of the platform received high scores, indicating that participants found these elements particularly beneficial and well-executed. Conversely, a slightly lower score was recorded for the item assessing participants' perception of their ability to apply what they learned in the course to their working context. This finding suggests an area for potential improvement, with implications for the design and implementation of future TGD health courses. Incorporating clinical competencies related to TGD individuals across the entire curriculum of HCPs, rather than in one or a few condensed lectures, is a priority to be addressed at the institutional level (1).
Our course represents the first institutional attempt to provide HCPs with the basic knowledge related to the health needs of the TGD population. Therefore, the course was designed to be accessible to all healthcare professions, as classified by the Agenzia Nazionale per i Servizi Sanitari Regionali (AGENAS)—National Agency for Regional Health Services. Extending access to all HCPs, including those not directly involved in healthcare assistance, appeared to be a strategic approach to foster a culture of inclusivity for TGD individuals on a wider scale. However, behind this aim lies one of the study's limitations, as the identified constraints reflect weaknesses in the course design. The distribution of enrolled participants mirrors the composition of HCPs accredited in EDUISS, where nurses constitute approximately one-third of the total accredited professionals (with 223,000 nurses out of 616,000 healthcare professionals). Due to this limitation, to ensure robust results when comparing pre-test and post-test scores, we opted to aggregate certain categories within the “profession” variable according to the classification proposed by AGENAS. Consequently, we abstained from providing average pre-test and post-test scores for individual professions. Another limitation of the study is the lack of consideration of follow-up data. As of the time of writing, the course's follow-up is in progress, involving the administration of the formative assessment test (T2) and the ASPQ 6 months after the course's conclusion. These data may be explored in a future study focused on tracking the progression of attitudes, skills, and practices.
In conclusion, the goal of this study, as well as the overall success of the training program, was evidenced by the high enrollment numbers, which hit the maximum capacity. The research hypothesis was validated by the notable improvement in knowledge from pre-test to post-test and the high degree of user satisfaction. Our results mark a crucial first step in refining and optimizing the delivery of educational programs in TGD health. They underscore the necessity of considering specific demographic factors in the formulation of forthcoming educational strategies in TGD health. Future literature addressing the assessment of learners in clinical settings and the impact on patient outcomes is urgently warranted. The implications of these findings extend beyond the immediate educational context, contributing to the broader discourse on promoting inclusivity and understanding in healthcare practices related to TGD health.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical approval was not required for the studies involving humans because, according to the Italian regulation, ethics approval was not required for this study: by registering for the course on the online platform, the participants gave the consent to the use of their anonymous data. The study was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
UF: Validation, Software, Methodology, Investigation, Formal analysis, Data curation, Conceptualization, Writing – review & editing, Writing – original draft. MMar: Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization, Writing – review & editing, Writing – original draft. PC: Software, Methodology, Formal analysis, Data curation, Writing – review & editing. DG: Software, Methodology, Formal analysis, Data curation, Writing – review & editing. AR: Methodology, Investigation, Writing – review & editing. MMan: Formal analysis, Data curation, Writing – review & editing. FM: Software, Methodology, Data curation, Writing – review & editing. FR: Software, Project administration, Methodology, Data curation, Writing – review & editing. AV: Software, Methodology, Data curation, Writing – review & editing. AM: Supervision, Methodology, Writing – review & editing. MP: Supervision, Resources, Project administration, Investigation, Funding acquisition, Formal analysis, Data curation, Conceptualization, Writing – review & editing, Writing – original draft.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The project was established with the co-funding of the European Union, National Operational Programme for Social Inclusion—European Social Fund 2014–2020.
We are deeply grateful to all experts in TGD healthcare and legal domains who played a role in the success of this project: Teresa Bini, Andrea D'Ambrosio, Marco Falcone, Ilaria Ferro, Alessandra D. Fisher, Cathy La Torre, Giulia Lo Russo, Francesca Mazzoli, Maria Cristina Meriggiola, Federica Peretti, Mirko Preto, Jiska Ristori, Alessia Romani, and Daniele Tesoro. We also express our gratitude to the study participants for generously sharing their experiences. Furthermore, we thank TGD organizations for their active contribution in the project (ALA Milano; Associazione Consultorio Transgenere, Associazione Libellula Italia APS; Associazione Maurice GLBT, Spo.T Sportello Trans; Associazione Transessuale Napoli, ATN; Azione Trans; Boramosa, Centro Salute Trans e Gender Variant, CEST; Gruppo Ascolto Giovani Arcobaleno, G.A.G.A; Gay Center; Gender X; Gruppo Trans APS; I Ken; Intersexioni; Movimento Identità Trans, MIT; Sat Pink APS; Sunderam; T Genus: Magna Grecia).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Coleman E, Radix AE, Bouman WP, Brown GR, de Vries ALC, Deutsch MB, et al. Standards of care for the health of transgender and gender diverse people, version 8. Int J Transgend Health. (2022) 23:1–259. doi: 10.1080/26895269.2022.2100644
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: American Psychiatric Association (2013).
3. World Health Organization. International Classification of Diseases, Eleventh Revision (ICD-11). (2022). Available online at: https://icd.who.int/ (accessed May 23, 2024).
4. Reisner SL, Poteat T, Keatley JA, Cabral M, Mothopeng T, Dunham E, et al. Global health burden and needs of transgender populations: a review. Lancet. (2016) 388:684. doi: 10.1016/S0140-6736(16)00684-X
5. Safer JD, Coleman E, Feldman J, Garofalo R, Hembree W, Radix A, et al. Barriers to healthcare for transgender individuals. Curr Opin Endocrinol Diabet Obes. (2016) 23:168–71. doi: 10.1097/MED.0000000000000227
6. Winter S, Diamond M, Green J, Karasic D, Reed T, Whittle S, et al. Transgender people: health at the margins of society. Lancet. (2016) 388:390–400. doi: 10.1016/S0140-6736(16)00683-8
7. Feldman JL, Luhur WE, Herman JL, Poteat T, Meyer IH. Health and health care access in the US transgender population health (TransPop) survey. Andrology. (2021) 9:1707–18. doi: 10.1111/andr.13052
8. Marconi M, Pagano MT, Ristori J, Bonadonna S, Pivonello R, Meriggiola MC, et al. Sociodemographic profile, health-related behaviours and experiences of healthcare access in Italian transgender and gender diverse adult population. J Endocrinol Invest. (2024) 24:2362. doi: 10.1007/s40618-024-02362-x
9. Tanenbaum GJ, Holden LR. A review of patient experiences and provider education to improve transgender health inequities in the USA. Int J Environ Res Public Health. (2023) 20:6949. doi: 10.3390/ijerph20206949
10. de Vries E, Kathard H, Müller A. Debate: why should gender-affirming health care be included in health science curricula? BMC Med Educ. (2020) 20:51. doi: 10.1186/s12909-020-1963-6
11. Transgender Europe. Overdiagnosed but Underserved (2017). Available online at: https://www.tgeu.org/files/uploads/2023/11/Overdiagnosed_Underserved-TransHealthSurvey.pdf (accessed May 29, 2024).
12. Giblon R, Bauer GR. Health care availability, quality, and unmet need: a comparison of transgender and cisgender residents of Ontario, Canada. BMC Health Serv Res. (2017) 17:283. doi: 10.1186/s12913-017-2226-z
13. Kattari SK, Call J, Holloway BT, Kattari L, Seelman KL. Exploring the experiences of transgender and gender diverse adults in accessing a trans knowledgeable primary care physician. Int J Environ Res Public Health. (2021) 18:13057. doi: 10.3390/ijerph182413057
14. Skuban-Eiseler T, Orzechowski M, Steger F. Why do transgender individuals experience discrimination in healthcare and thereby limited access to healthcare? An interview study exploring the perspective of German transgender individuals. Int J Equity Health. (2023) 22:211. doi: 10.1186/s12939-023-02023-0
15. Holland D, White LCJ, Pantelic M, Llewellyn C. The experiences of transgender and nonbinary adults in primary care: a systematic review. Eur J Gen Pract. (2024) 30:2296571. doi: 10.1080/13814788.2023.2296571
16. Leone AG, Trapani D, Schabath MB, Safer JD, Scout NFN, Lambertini M, et al. Cancer in transgender and gender-diverse persons. J Am Med Assoc Oncol. (2023) 9:556. doi: 10.1001/jamaoncol.2022.7173
17. de Blok CJ, Wiepjes CM, van Velzen DM, Staphorsius AS, Nota NM, Gooren LJ, et al. Mortality trends over five decades in adult transgender people receiving hormone treatment: a report from the Amsterdam cohort of gender dysphoria. Lancet Diabetes Endocrinol. (2021) 9:663–70. doi: 10.1016/S2213-8587(21)00185-6
18. Burgwal A, Gvianishvili N, Hård V, Kata J, Nieto IG, Orre C, et al. The impact of training in transgender care on healthcare providers competence and confidence: a cross-sectional survey. Healthcare. (2021) 9:967. doi: 10.3390/healthcare9080967
19. Johnston CD, Shearer LS. Internal medicine resident attitudes, prior education, comfort, and knowledge regarding delivering comprehensive primary care to transgender patients. Transgend Health. (2017) 2:91–5. doi: 10.1089/trgh.2017.0007
20. Honigberg MC, Eshel N, Luskin MR, Shaykevich S, Lipsitz SR, Katz JT. Curricular time, patient exposure, and comfort caring for lesbian, gay, bisexual, and transgender patients among recent medical graduates. LGBT Health. (2017) 4:237–9. doi: 10.1089/lgbt.2017.0029
21. Mikulak M, Ryan S, Ma R, Martin S, Stewart J, Davidson S, et al. Health professionals' identified barriers to trans-health care: a qualitative interview study. Br J Gen Pract. (2021) 71:e941–7. doi: 10.3399/BJGP.2021.0179
22. Burgart JM, Walters RW, Shanahan M. Transgender education experiences among obstetrics and gynecology residents: a national survey. Transgend Health. (2022) 7:30–5. doi: 10.1089/trgh.2020.0018
23. Davidge-Pitts CJ, Nippoldt TB, Natt N. Endocrinology fellows' perception of their confidence and skill level in providing transgender healthcare. Endocr Pract. (2018) 24:1038–42. doi: 10.4158/EP-2018-0307
24. European Commission. Union of Equality: LGBTIQ Equality Strategy 2020–2025 (2020). Available online at: https://commission.europa.eu/document/download/5100c375-87e8-40e3-85b5-1adc5f556d6d_en?filename=lgbtiq_strategy_2020-2025_en.pdf (accessed May 29, 2024).
25. Pregnall AM, Churchwell AL, Ehrenfeld JM. A call for LGBTQ content in graduate medical education program requirements. Acad Med. (2021) 96:828–35. doi: 10.1097/ACM.0000000000003581
26. Dubin SN, Nolan IT, Streed Jr CG, Greene RE, Radix AE, Morrison SD. Transgender health care: improving medical students and residents training and awareness. Adv Med Educ Pract. (2018) 9:377–91. doi: 10.2147/AMEP.S147183
27. Dubin S, Kutscher E, Nolan I, Levitt N, Cook TE, Greene RE. Assessment of medical education on transgender health: a scoping literature review. Eval Health Prof . (2023) 2023:1632787231214531. doi: 10.1177/01632787231214531
28. Nolan IT, Blasdel G, Dubin SN, Goetz TG, Greene RE, Morrison SD. Current state of transgender medical education in the United States and Canada: update to a scoping review. J Med Educ Curric Dev. (2020) 7:238212052093481. doi: 10.1177/2382120520934813
29. Italian Ministry of Health. Piano per l'applicazione e la diffusione della Medicina di Genere (Italian Plan for the Implementation and Dissemination of Gender Medicine) (2019). Available online at: https://www.salute.gov.it/imgs/C_17_pubblicazioni_2860_allegato.pdf (accessed May 29, 2024).
30. Schmidt HG, Rotgans JI, Yew EH. The process of problem-based learning: what works and why. Med Educ. (2011) 45:792–806. doi: 10.1111/j.1365-2923.2011.04035.x
31. Mansholt H, Götz NA, Babitsch B. Chances and Barriers of Online Problem-Based Learning (ePBL) for advanced training in the healthcare sector. Stud Health Technol Inform. (2021) 281:822–3. doi: 10.3233/SHTI210292
32. Calabrò GE, Tognetto A, Mazzaccara A, Barbina D, Carbone P, Guerrera D, et al. Capacity building of health professionals on genetics and genomics practice: evaluation of the effectiveness of a distance learning training course for Italian physicians. Front Genet. (2021) 12:626685. doi: 10.3389/fgene.2021.626685
33. Barbina D, Carbone P, Di Pucchio A, Guerrera D, Vittozzi A, Mazzaccara A. Formazione a distanza in tempo di pandemia da SARS-CoV-2: l'esperienza dell'Istituto Superiore di Sanità. Turin: Atti del MoodleMoot Italia 2021 (2021).
34. Azer SA. Assessment in a problem-based learning course: twelve tips for constructing multiple choice questions that test students' cognitive skills. Biochem Mol Biol Educ. (2003) 31:428–34. doi: 10.1002/bmb.2003.494031060288
36. Anderson LW, Krathwohl DR. Taxonomy for Learning, Teaching, and Assessing: A Revision of Bloom's Taxonomy of Educational Objectives. New York, NY: Longman (2001).
38. George D, Mallery P. SPSS for Windows Step by Step: A Simple Guide and Reference (11.0 Update). 4th ed. Boston, MA: Allyn & Bacon(2003).
39. Mazzaccara A, Barbina D, Guerrera D. Problem-based learning in distance training for health professionals: a high interactivity model. In: Proceedings of the Atti Conference Mediterranean MoodleMoot. Sousse(2013).
40. Masek A, Yamin S. A comparative study of the effect of problem based learning and traditional learning approaches on students' knowledge acquisition. Int J Eng Educ. (2012) 28:1161–7.
41. Morin D, Safaee Fard H, George Saadé R. Understanding online learning based on different age categories. Iss Inform Sci Inform Technol. (2019) 16:307–17. doi: 10.28945/4313
42. MorganH, Lamprinakou C, Fuller E, AlbakriM. Attitudes to Transgender People. Research Report. Equality and Human Rights Commission Research Report Series (2020). Available online at: https://www.equalityhumanrights.com/sites/default/files/attitudes_to_transgender_people.pdf (accessed May 29, 2024).
43. Arslantas I, Gokdemir O, Dagbagli G, Mustan K, Guldal D. Determining the attitudes of medicine faculty instructors toward LGBT individuals. J Contin Educ Health Prof. (2022) 42:e131–3. doi: 10.1097/CEH.0000000000000435
Keywords: transgender, healthcare, distance learning, healthcare professionals, training, knowledge, Problem-Based Learning
Citation: Favazzi UM, Marconi M, Carbone P, Guerrera D, Ruocco A, Manoli M, Molinaro F, Regini FM, Vittozzi A, Mazzaccara A and Pierdominici M (2024) Evaluating the impact of distance learning on gender-affirming healthcare competence: knowledge acquisition and satisfaction among healthcare professionals in Italy. Front. Public Health 12:1393188. doi: 10.3389/fpubh.2024.1393188
Received: 28 February 2024; Accepted: 24 May 2024;
Published: 06 June 2024.
Edited by:
Piotr Karniej, WSB Merito University in Wroclaw, PolandReviewed by:
Noelia Navas-Echazarreta, University of La Rioja, SpainCopyright © 2024 Favazzi, Marconi, Carbone, Guerrera, Ruocco, Manoli, Molinaro, Regini, Vittozzi, Mazzaccara and Pierdominici. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marina Pierdominici, bWFyaW5hLnBpZXJkb21pbmljaUBpc3MuaXQ=
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.