 Vicente Martín Moreno1*
Vicente Martín Moreno1* María Inmaculada Martínez Sanz2
María Inmaculada Martínez Sanz2 Miriam Fernández Gallardo2Amanda Martín Fernández3María Palma Benítez Calderón2Helena Alonso Samperiz2Elena Pérez Rico2Laura Calderón Jiménez2Sara Guerra Maroto2Elena Sánchez Rodríguez2Eva Sevillano Fuentes2Irene Sánchez González2Miguel Recuero Vázquez4Julia Herranz Hernando2Irene León Saiz2 on behalf of the GIDO Collaborative Group (Orcasitas Dependency Research Group)
Miriam Fernández Gallardo2Amanda Martín Fernández3María Palma Benítez Calderón2Helena Alonso Samperiz2Elena Pérez Rico2Laura Calderón Jiménez2Sara Guerra Maroto2Elena Sánchez Rodríguez2Eva Sevillano Fuentes2Irene Sánchez González2Miguel Recuero Vázquez4Julia Herranz Hernando2Irene León Saiz2 on behalf of the GIDO Collaborative Group (Orcasitas Dependency Research Group)- 1Orcasitas Health Care Center and i+12 Research Institute of the Doce de Octubre Hospital, Grupo de Investigación sobre Dependencia en Orcasitas (GIDO Collaborative Group), Madrid, Spain
- 2Orcasitas Health Care Center, Grupo de Investigación sobre Dependencia en Orcasitas (GIDO Collaborative Group), Madrid, Spain
- 3Polibea Concert, Grupo de Investigación sobre Dependencia en Orcasitas (GIDO Collaborative Group), Madrid, Spain
- 4Orcasitas Health Care Center, Grupo de Investigación sobre Dependencia en Orcasitas (GIDO Collaborative Group), Nursing Home Care Unit of the Center, Madrid, Spain
Background: Prolonged confinement can lead to personal deterioration at various levels. We studied this phenomenon during the nationwide COVID-19 lockdown in a functionally dependent population of the Orcasitas neighborhood of Madrid, Spain, by measuring their ability to perform basic activities of daily living and their mortality rate.
Methods: A total of 127 patients were included in the Orcasitas cohort. Of this cohort, 78.7% were female, 21.3% were male, and their mean age was 86 years. All participants had a Barthel index of ≤ 60. Changes from pre- to post-confinement and 3 years afterward were analyzed, and the effect of these changes on survival was assessed (2020–2023).
Results: The post-confinement functional assessment showed significant improvement in independence over pre-confinement for both the Barthel score (t = −5.823; p < 0.001) and the classification level (z = −2.988; p < 0.003). This improvement progressively disappeared in the following 3 years, and 40.9% of the patients in this cohort died during this period. These outcomes were associated with the Barthel index (z = −3.646; p < 0.001) and the level of dependence (hazard ratio 2.227; CI 1.514–3.276). Higher mortality was observed among men (HR 1.745; CI 1.045–2.915) and those with severe dependence (HR 2.169; CI 1.469–3.201). Setting the cutoff point of the Barthel index at 40 provided the best detection of the risk of death associated with dependence.
Conclusions: Home confinement and the risk of death due to the COVID-19 pandemic awakened a form of resilience in the face of adversity among the population of functionally dependent adults. The Barthel index is a good predictor of medium- and long-term mortality and is a useful method for detecting populations at risk in health planning. A cutoff score of 40 is useful for this purpose. To a certain extent, the non-institutionalized dependent population is an invisible population. Future studies should analyze the causes of the high mortality observed.
Introduction
The COVID-19 pandemic brought about changes in personal and social habits unprecedented in this century and altered the social and health balance of affected countries. In Spain, nationwide lockdown was decreed on March 15, 2020. This measure slowed the spread of the pandemic but had an impact on people, especially dependents (1).
Dependence is a vulnerability criterion that increases the risk of hospitalization and death (2). Although confinement affected all population groups, dependent people were among the most sensitive to this situation since their dependence is associated with greater age and comorbidities, which were risk factors for morbidity and mortality due to COVID-19 (3–5). Further, the risk of contagion is probably greater among dependent populations, especially those institutionalized, due to the need for interaction with others for care (6).
Apart from the COVID-19 pandemic, dependency is an emerging socio-health problem that requires multiple socio-health resources, with a progressively increasing cost, and with two models of care, depending on whether the dependent persons reside at home or are institutionalized in nursing homes. To maintain equity in the care of both groups, it is necessary to carry out adequate healthcare planning and evaluate the actions carried out (7). The 20th Report of the State Observatory on Dependency (8), February 2020, states that 3% of the Spanish population needs support to perform basic activities of daily living (ADL), most of this population being female. At the healthcare level, care for dependency falls on primary care nurses, the main clinical manager of this multidisciplinary problem (9).
However, dependency is not a standalone issue and requires a broader approach. Chronicity, complexity, and dependency form an increasingly prevalent interrelated triad in our society (10), contributing to the creation of vulnerable populations and social inequalities (11). Thus, in a pandemic, with the added factor of confinement, new conditions and rules of the game were created, which need to be analyzed to design strategies that will enable us to deal with these situations in the future.
The new rules of social and personal functioning and supervision, for which no one had an adaptation period, included the elimination of visits by relatives to those not strictly necessary, leaving food at the door, the loss of attention in day centers, and the suspension of home care performed by hired caregivers. These changes aggravated the loneliness of the dependent adults and forced them to perform functions and responsibilities that they had not before. All the above was added to the fear generated by the media bombardment, showing a high mortality rate among people like them. All the above factors impact the physical and mental health of people, which requires further analysis (12, 13).
Although previous studies have examined institutionalized dependent populations (14–16) or involved research before and after hospital discharge (17, 18), generally in association with patient interventions (19), there have been fewer longitudinal studies of non-institutionalized dependent populations in the context of the COVID-19 pandemic. A 2019 study addressed the complexity of these factors and their interrelationships (20). The current study aims to analyze whether the nationwide lockdown, which was declared under a state of alarm by the Government of Spain, conditioned short- and long-term changes in the functional dependence of the dependent population of the Orcasitas neighborhood of Madrid (Spain), and to quantify the relationships of these changes with sociodemographic variables and survival at 3 years.
Materials and methods
Design
A longitudinal descriptive study was conducted in the Orcasitas neighborhood of the city of Madrid (Spain) between June 2020 and August 2023 on the entire functionally dependent population assigned to the Orcasitas Healthcare Center that was registered in the e-SOAP application of the Community of Madrid. One hundred and fifty patients were included in the Orcasitas cohort. The nationwide lockdown began in Spain on March 15, 2020. Madrid moved to phase 1 of the de-escalation on May 18, 2020, and the state of alarm ended on June 21, 2020. In the de-escalation phase 1, people were allowed to leave for non-compulsory activities within time limits.
The Orcasitas Healthcare Center is a primary care center that serves the basic health area of Orcasitas, a neighborhood in Madrid (Spain) with a population of 22,452 people. It provides health services in person at the center, by telematic means, and at the patient's home, as required.
Participants
Inclusion criteria were: participants needed to be 65 years or older, have a diagnosis of functional dependence to perform basic activities of daily living (ADL), and have a previous Barthel score in the last year. The exclusion criteria were: 1: Not belonging to the basic health area. 2: Not being in the usual home during the study period (hospital or nursing home admission, older adults living in their children's homes). 3: Not having a previous Barthel score in the last year. 4: Not being able to respond autonomously or through a trained usual caregiver to the questionnaires used. 5: Having a diagnosis of a terminal illness. Five patients refused to participate in the study. And 18 were excluded: not located (n = 1), being in another home (n = 2), admission to a nursing home (n = 4), admission to hospital (n = 2), death before the start of the study (n = 4), not dependent due to error in previous Barthel score (n = 1), and not having a previous Barthel score (n = 4). Finally, 127 patients participated.
This study was approved by the Center Local Research Commission of the Primary Care Management of Madrid (reference number 16/20-C-Bis) on June 29, 2020. The Ethics Committee of the Hospital 12 de Octubre endorsed this approval as sufficient in resolution CEIm 23/501 dated September 26, 2023.
Data collection
Functional dependence in ADL was assessed using the Barthel index, according to the internationally recognized classification (21) used as a criterion in the Spanish National Health System Primary Care dependence protocol (22), with four levels of dependence: mild (Barthel 60), moderate (Barthel 40–55), severe (Barthel 20–35), and total (Barthel < 20). A second cutoff point was also established at Barthel 40, with two groups, severe dependents (Barthel < 40) and moderate dependents (Barthel 40–60) (23). The pre-pandemic baseline Barthel, Barthel in June 2020, and Barthel in 2023 were recorded.
The Barthel assessment was performed by a single blind, with the nursing staff unaware of the pre-confinement value. At the same visit, the variables that could be studied were obtained using a previously validated questionnaire that collected age, sex, marital status, and educational level. The questionnaire was validated through a pilot study in a population over 80 years of age, dependent and non-dependent, in the Orcasitas neighborhood. It consisted of 48 questions, mostly closed and generally dichotomous. To avoid errors in the way the questionnaire was administered, some questions included explanatory notes on the correct way to ask the question, with the double objective of avoiding bias associated with the interviewer, and the way the question was asked would condition a different response in the interviewee. No question required modifications in its wording to facilitate its comprehension in the pilot study.
Definitions of covariates
The clinical variables, body mass index (BMI), number of chronic diseases, and whether the patient was polymedicated (cutoff point five active components), were collected through the AP-Madrid application of the Health System. The Individual Health Card (IHC) application was used to obtain the number of persons aged 65 years or over registered at the Orcasitas Health Center by age group and the economic income data.
The IHC and AP-Madrid applications classified the population over 65 years according to their level of income in two groups: (1) income above 11,200 euros/year; and (2) income below 11,200 euros/year. This cutoff point was used in this study for the analyses associated with this variable. With respect to educational level and given the high illiteracy rates in the Orcasitas neighborhood, two categories were established: having education and not having education (illiterate, knowing how to read and write, but not having studied and not having completed primary education).
The housing situation of the dependent persons was classified into three groups: (1) they live independently, either alone or with a partner; (2) they live with their children; and (3) they live with other people who are neither children nor a partner.
Age was assessed in the statistical analyses as a quantitative variable, but functional dependents were also classified into three age groups: (1) age < 80; (2) age between 80 and 89; and (3) age equal to or more than 90 years.
The date of death of each functionally dependent person during the study period (June 2020 to June 2023) was recorded, obtaining the data from the Health System's IHC application.
Data analysis
The analysis of the collected variables was performed with the statistical package SPSS 18.0. First, a descriptive analysis of the sample was performed. Continuous variables were described as mean and standard error, and categorical variables as absolute numbers and/or proportions. The normality of the data distribution was tested using the Shapiro-Wilk test for each variable. When the outcome variable did not follow a normal distribution, ANOVA was performed with Levene's homogeneity test, applying Welch's correction as a robust test of equality of means when the sample size was <30. Differences between continuous variables were analyzed using the Student's t-test or the Mann–Whitney U-test, and differences between categorical variables were analyzed using the chi-square test. Before-after differences in the Barthel index were analyzed using the Wilcoxon signed-rank test. The probability of occurrence of an event was analyzed by the odds ratio (OR).
ADL dependence was analyzed according to the original Barthel index clusters and was also dichotomized into two categories: “moderate,” which included the categories mild (Barthel 60) and moderate (Barthel 40–55); and “severe,” which included the categories severe (Barthel 20–35) and total (Barthel < 20), in both univariate and multivariate analysis.
Mortality information was obtained for all patients during the 3 years of follow-up. Survival curves for levels on the Barthel index before and after the nationwide COVID-19 lockdown and for each Barthel index item were estimated using the Kaplan–Meier method. Comparisons of the curves were made using the log-rank test.
Univariate analysis was performed to identify the variables associated with the long-term survival of the people included in this cohort and the subgroup of dependent people who showed changes in the Barthel index score during the nationwide COVID-19 lockdown. Covariates that were significant in the bivariate analysis were introduced into the multivariate regression model. The resulting model was summarized by the estimated coefficients, p-values, and hazard ratios (HR) with their 95% confidence intervals. Crude and adjusted hazard ratios (HR) and confidence intervals (95% CI) were calculated using Cox proportional regression models.
Using Cox regression, adjusted for sex, educational level, and income level, survival in June 2021 and June 2023 was analyzed according to the level of functional dependence, disaggregated for each Barthel index level. Statistical significance was considered p < 0.05.
Results
Demographic characteristics
The mean age of the population of the Orcasitas cohort was 86.6 years, with 21.3% of the participants being male, generally married (55.6%; n = 15), and 78.7% female, mostly widowed (71%; n = 71). A large majority (87.4%) reported having insufficient education (illiterate, has no schooling but can read and write; or having incomplete primary education). The sociodemographic and health variables are presented in Table 1. According to the analysis of variance, no differences were observed between the sexes in terms of the score obtained on the Barthel index, BMI, educational level, or income level (Table 2).
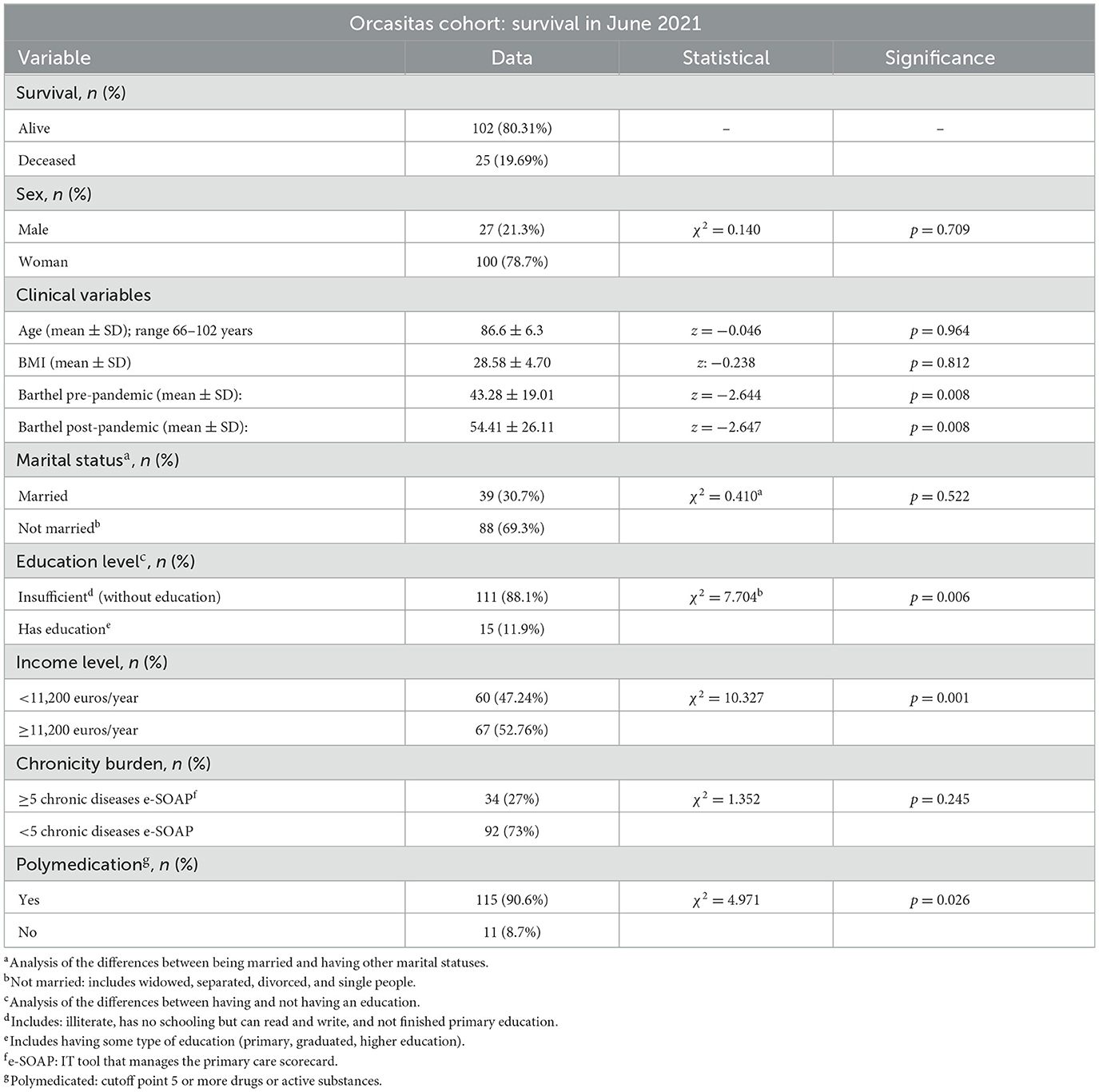
Table 1. Clinical and sociodemographic data of the Orcasitas cohort in June 2020 and analysis of their relationship with survival in June 2021.
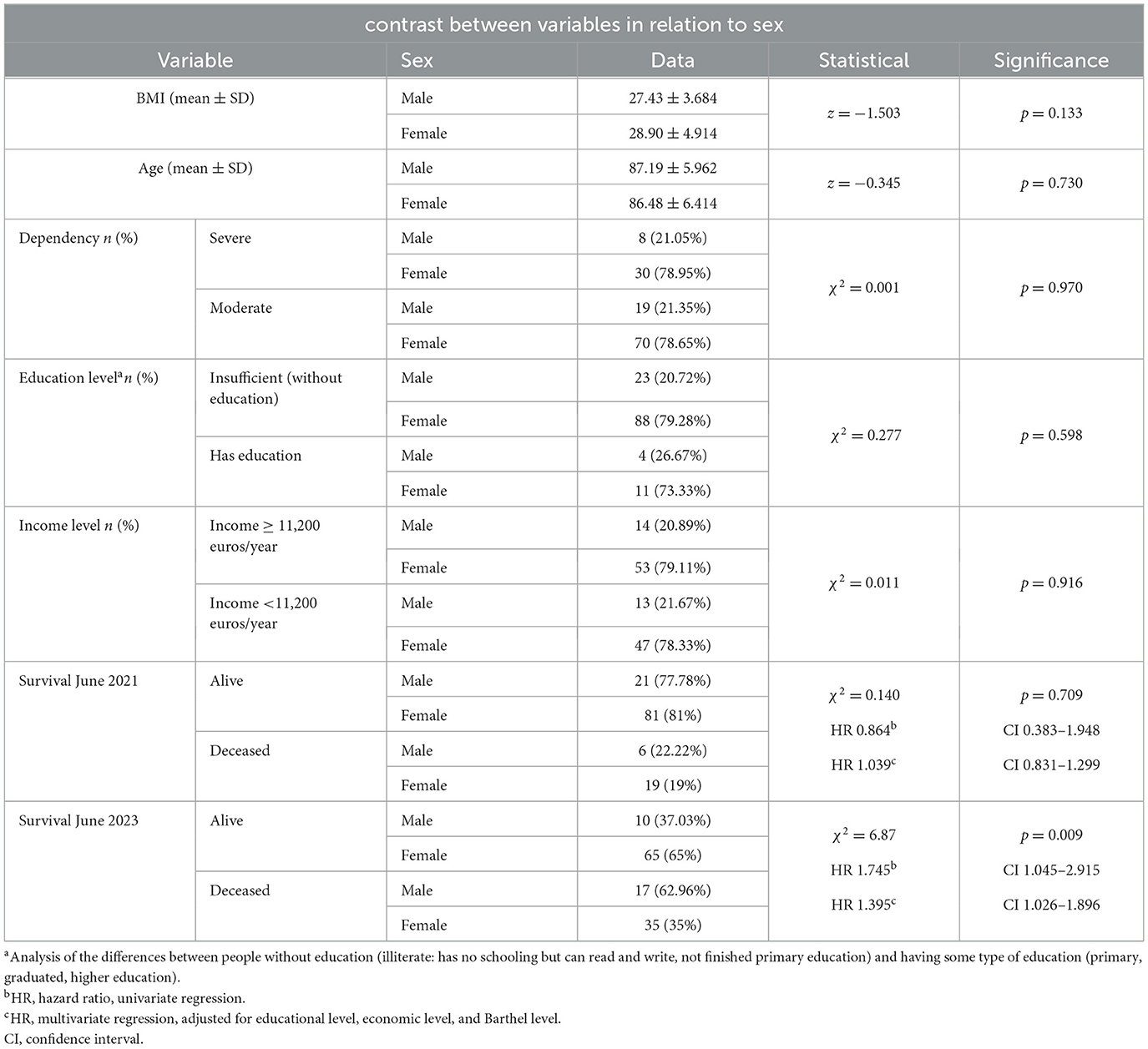
Table 2. Analysis of the differences between the socioeconomic and health variables based on sex and survival at 1 and 3 years.
About the population of the Orcasitas neighborhood (Madrid), and within the group of persons over 65 years of age, the IHC application of the Health System of the community of Madrid established three population groups: patients aged 65–74 years (1,808 persons); patients aged 75–79 years (703 persons); and patients aged 80 years or more (1,797 persons). In the dependent population, among the non-dependent population, the group of people over 80 years of age was highly represented. Out of a total population of 22,452 people in the Orcasitas neighborhood in June 2020, the group of people over 80 years of age represented 8%, and the group of people over 65 represented 19.2%. The group of people under 14 years of age (3,248 people) assigned to this health center represented 14.5% of the population of this neighborhood. The population with functional dependency in the Orcasitas neighborhood represented 7.1% of the population over 80 years of age and 3.1% of the population over 65 years of age. The aging index ([population over 65 years old/population under 14 years old] × 100) was 1.33.
Changes in the level of functional dependence due to nationwide COVID-19 lockdown
Before confinement, 15% (n = 19) of the persons in this cohort had total dependence (Barthel < 20), 15% (n = 19) severe dependence (Barthel 20–35), 36.2% (n = 46) moderate dependence (Barthel 40–55), and 33.9% mild dependence (Barthel 60). The mean Barthel index scores before confinement were 43.28 ± 19.017.
After confinement, 11% (n = 14) had total dependence, 15% (n = 19) had severe dependence, 21.3% (n = 27) had moderate dependence, and 9.4% (n = 12) had mild dependence. Approximately 43.3% (n = 55) of those who were dependent pre-confinement ceased to be dependent after confinement by improving their Barthel score and surpassing the cutoff point of 60. The mean Barthel index scores after confinement were 54.41 ± 26.115.
A significant improvement (t = −5.823; p < 0.001) in functional dependence to perform ADLs during national COVID-19 confinement was observed in 62.2% of patients in the Orcasitas cohort. Twenty-six percentage of the dependent persons worsened their baseline Barthel index score. The improvement in the Barthel index score was reflected in the level of dependency (χ2 = 28.710; p < 0.001), a result shown in Figure 1. This figure combines the two most widely used dependency classification models using the Barthel index. The decision to combine both models in the same figure allowed us to reflect the impact of home confinement due to the COVID-19 pandemic on the ability to perform basic activities of daily living for each level of dependency of the classic Barthel scale. It also helped to investigate the second classification model analyzed in this study with two levels, severe (Barthel < 20 and Barthel 20–35) and moderate (Barthel 40–55 and Barthel 60).
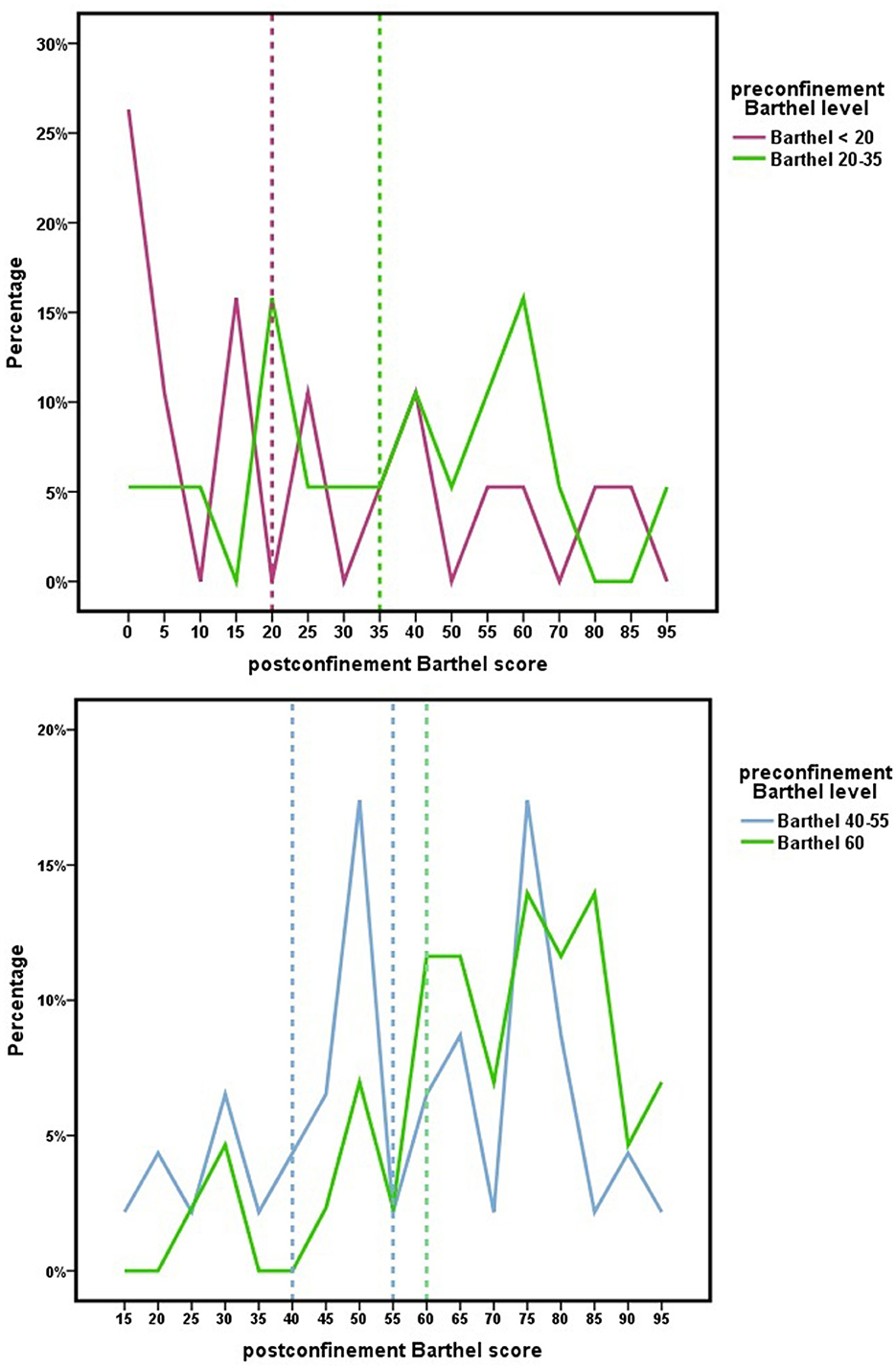
Figure 1. Changes in the score in the Barthel index because of the nationwide COVID-19 lockdown for each level in the Barthel index. Dependency is established for a Barthel index score of 60 or less. After confinement, the scores achieved are reflected, indicating a Barthel index score > 60 that the person no longer meets dependency criteria according to the National Health System protocol.
Figure 2 includes the age factor as the central axis on which to observe the changes in functional capacity during confinement, estimated by the Barthel scale score, and the effect of these changes, or their absence, in terms of survival at 1 and 3 years.
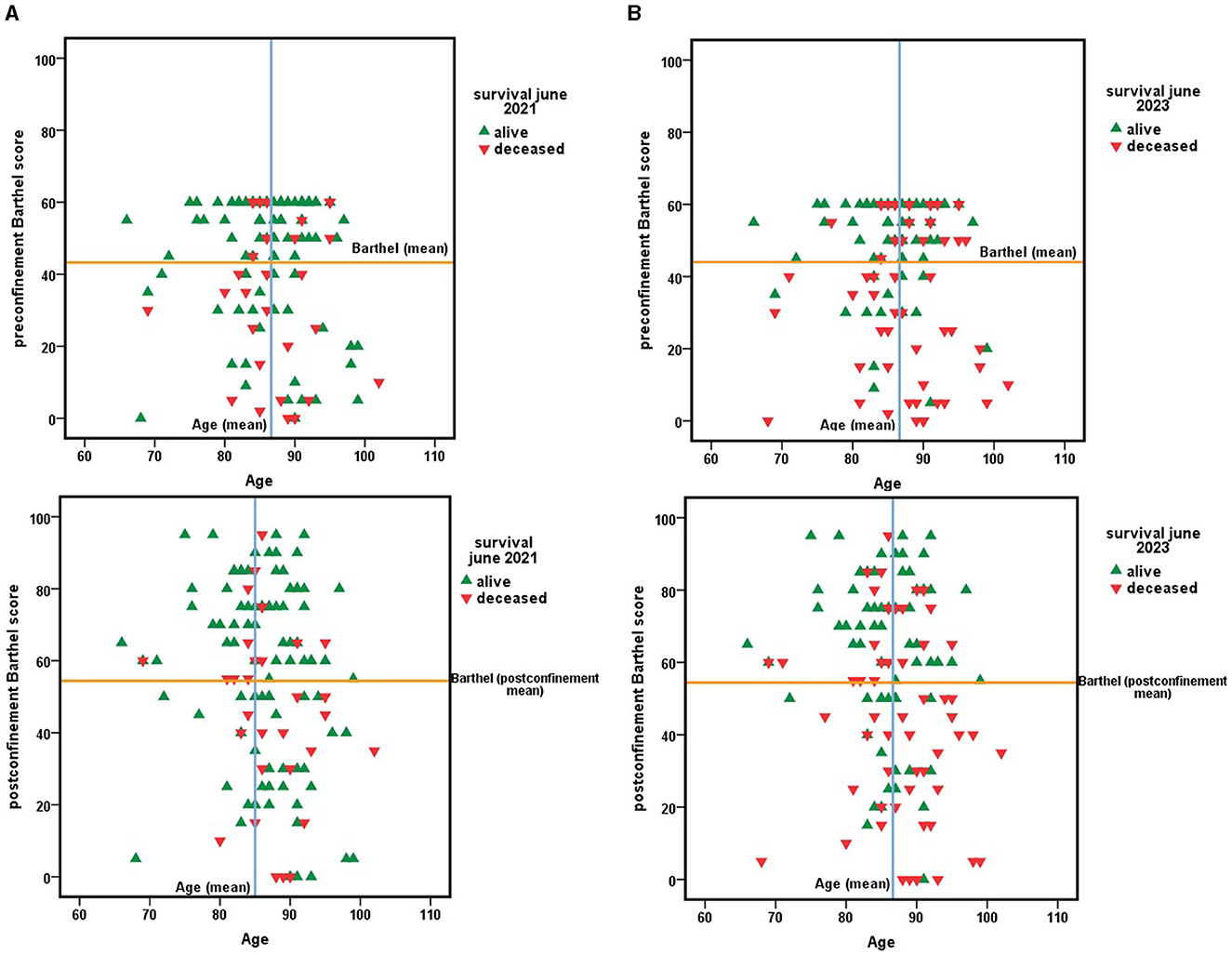
Figure 2. (A) Survival 1 year after the end of the nationwide COVID-19 lockdown depending on age and functional dependency, estimated by the Barthel index score at two time cutpoints, before March 2020, the start date of confinement, and in June 2020, the end date of confinement in Spain. (B) Survival 3 years after the end of the nationwide COVID-19 lockdown. A function of age and functional dependency, estimated by the Barthel index score at two time cutpoints, before March 2020, the start date of confinement, and June 2020, the end date of confinement in Spain.
A total of 43.3% (n = 55) of the dependent persons in this cohort ceased to meet the inclusion criteria of the dependency protocol after the nationwide COVID-19 lockdown by improving their Barthel score and exceeding the cutoff point of 60. Three years later (June 2023), 56.4% (n = 31) of these functionally dependent persons who ceased to be functionally dependent during nationwide COVID-19 lockdown remained non-dependent, while, regarding those who improved their functional abilities, 3 years later, 29.9% (n = 38) maintained such improvement.
These results, observed for any level of baseline dependence (Figure 1; Table 3), allowed 10.5% of people with total or severe dependence to improve their dependence to the point of no longer being dependent. This percentage was much higher among persons with moderate dependence (45.7%) or mild dependence (69.8%). For others, however, confinement led to a deterioration in their baseline state, with 11.8% increasing their level of dependence by one level and 3.1% by two levels.
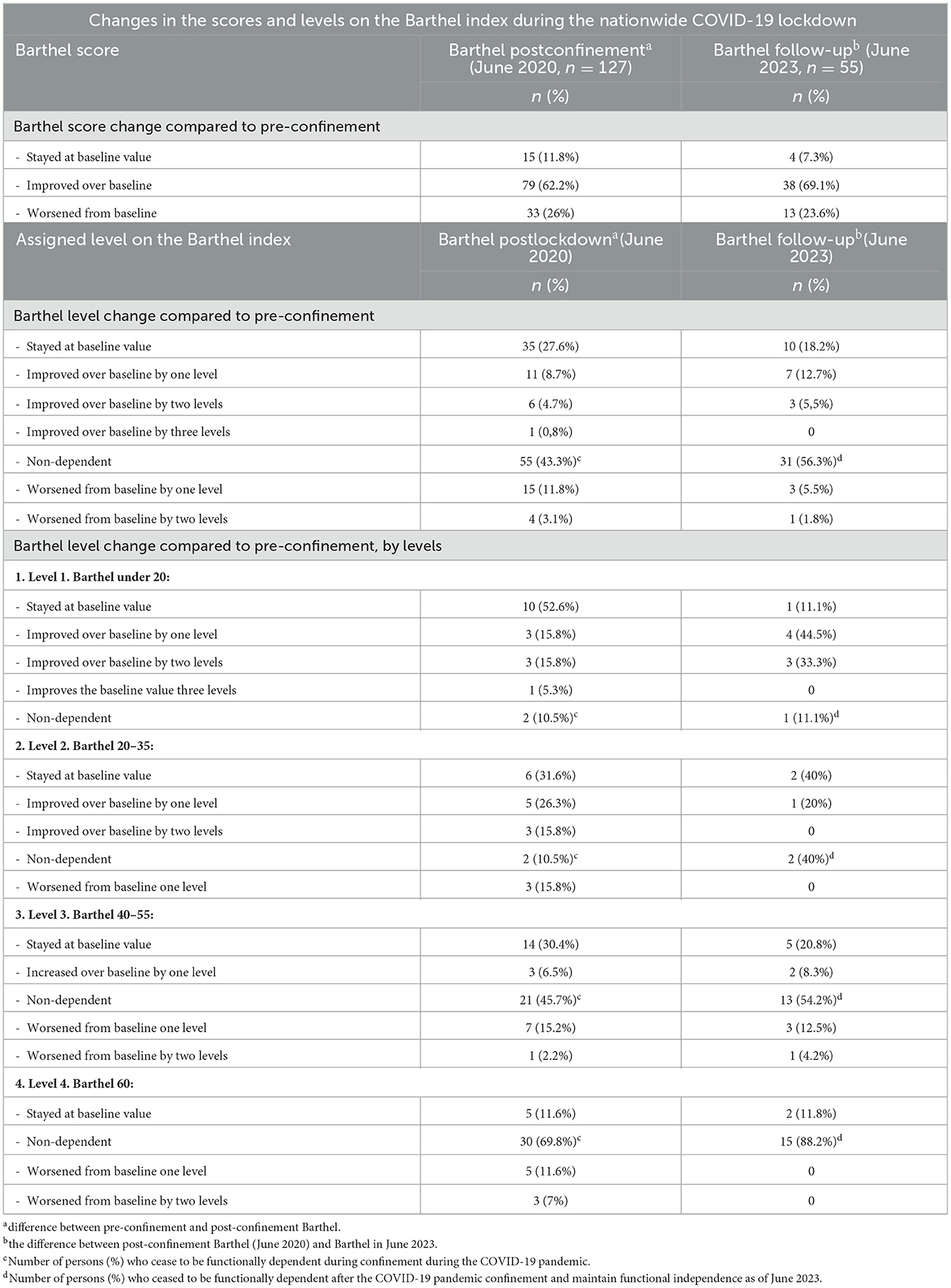
Table 3. Changes observed in June 2020 in the score and classification in the Barthel index because of the nationwide COVID-19 lockdown decreed by the Government of Spain (March-May 2020) and assessment of the changes observed after 3 years (June 2023).
We also observed that the percentage of dependent persons who improved their abilities was higher among persons who were previously less dependent (Barthel 60). And this result was observed both against people with total dependence (Barthel < 20; χ2 = 9.030; p < 0.01) and against people with moderate dependence (Barthel 40–55; χ2 = 4.810; p < 0.05) but not against people with severe dependence (Barthel 20–35; χ2 = 3.500; p = NS).
Improving or worsening the Barthel score did not imply changing the level on the scale, with 27.6% maintaining the same level and 72.4% modifying their level, including patients with total dependence (Table 3). Among the group that improved their functional capacity during confinement, 48.1% (38) maintained this improvement at 3 years, representing 69.1% of the cohort in 2023.
The changes in functional capacity during confinement reflected in the Barthel index score performed in June 2020 were not associated with greater or lesser comorbidity (z = −0.221; p = 0.825), nor with greater or lesser drug consumption in relation to that comorbidity (z = −0.386; p = 0.700). When the subgroups were analyzed, these results were maintained, and no association was observed between improving the Barthel index score during confinement with disease burden (z = −0.386; p = 0.699) or with being polymedicated (z = −1.329; p = 0.184). Among the persons whose functional capacity worsened during confinement, none was a polymedicated patient, and this worsening was not associated with disease burden (z = −0.204; p = 0.222).
These changes in the Barthel scale score due to the COVID-19 pandemic confinement were similar in both sexes, Figures 3, 4. No significant differences were observed between sexes with respect to Barthel index score before confinement (z = −0.217; p = 0.828), after confinement (z = −0.269; p = 0.788), or as a consequence of changes during confinement (z = −0.269; p = 0.788).
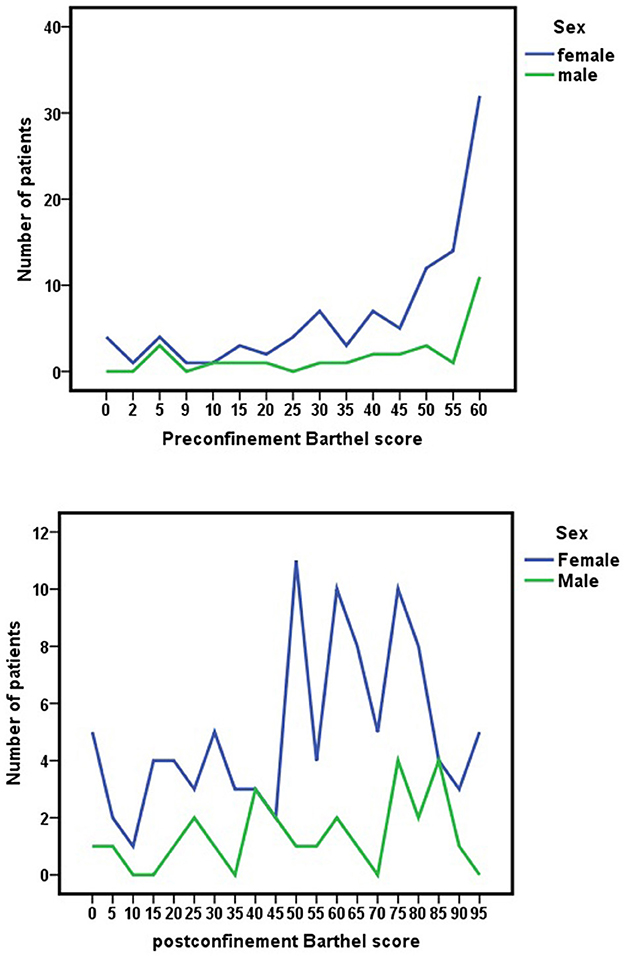
Figure 3. Pre-lockdown Barthel index scores (before March 15, 2020) and changes by the nationwide COVID-19 lockdown in Barthel scores (June 2020) for each sex.
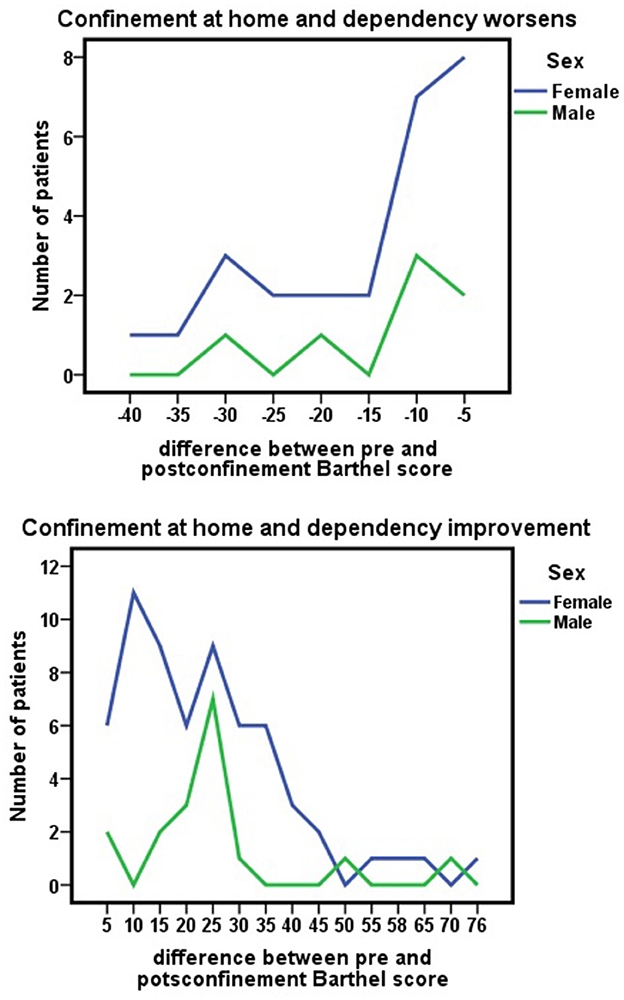
Figure 4. Improvement or worsening of Barthel scores due to nationwide COVID-19 lockdown (difference between pre-confinement Barthel score and post-confinement Barthel score) for each sex.
Pooling the data for the period 2020–2023, before confinement, the mean Barthel index score was 43.28 ± 19.017. During the COVID-19 pandemic, confinement functional capacity improved (t = −5.823; p < 0.001), with a mean Barthel index score of 54.41 ± 26.115 in June 2020. From this date until June 2023, a worsening in functional capacity was observed (t = 4.930; p < 0.001). Despite this worsening, the mean Barthel scale score in June 2023 (48.36 ± 21.711) remained higher than the pre-pandemic baseline score but without statistical significance (t = 0.555; p = 0.581), with a sawtooth observed in this period with peak improvement in June 2020.
Aging as a modulator of functional response during COVID-19 pandemic confinement
Improvement in functional abilities during confinement occurred in all age groups. By age group, 91.7% (n = 11) of those younger than 80 years (n = 12), 69.7% (n = 46) of those aged 80–89 years (n = 66), and 64.7% (n = 22) of those aged 90 years or older (n = 34) improved their ability to perform basic activities of daily living during the COVID-19 pandemic confinement. In contrast, 8.3% (n = 1) of those younger than 80 years, 30.3% (n = 20) of those aged 80–89 years, and 35.3% (n = 12) of those aged 90 years or older worsened their functional abilities during confinement. The remaining components of this cohort maintained their Barthel index scores. Although there was a tendency for improvement capacity to decrease with increasing age, the differences did not reach statistical significance (χ2 = 3.157; p = 0.206).
Analysis comparing age groups, establishing 80 and 90 years of age as cutoff points, did not show a greater improvement in functional capacity among persons under 80 years of age, with respect to those of that age or older (OR 5.254; CI 0.650–42.476). Nor was it observed among persons under 90 years of age for those who were that age or older (OR 1.481; CI 0.625–3.510).
The housing situation factor as a modulator of functional response during COVID-19 pandemic confinement
The effect of the housing situation of the dependent persons was analyzed as a modulator of the response to the functional capacity of the COVID-19 pandemic home confinement. This analysis showed that 83.7% (n = 36) of the dependent persons living independently (n = 43) improved their functional capacity; meanwhile, 64% (n = 32) of those living with their children improved their functional capacity, and 57.9% (n = 11) of those living with people other than their children or partner (n = 19) showed improvement in their functional capacity. In contrast, 16.3% (n = 7) of those living independently, 36% (n = 18) of those living with their children, and 42.1% (n = 8) of those living with others worsened in their functional capacity (χ2 = 6.086; p = 0.048). The remaining dependent persons of this cohort did not modify their Barthel index score.
Grouping housing situations between living independently or living with others, including adult children and dependent persons who, during the COVID-19 pandemic confinement, lived alone or with a partner, showed greater improvement in the ability to perform basic activities of daily living than those who lived with their children or with others (z = −2.054; p = 0.040). Dependent persons were more likely to respond to confinement by increasing functional capacity when living independently (OR 3.110; CI 1.209–7.999).
Survival of the functionally dependent population of the orcasitas cohort from 2020 to 2023
In the follow-up of this cohort after the end of the nationwide COVID-19 lockdown in June 2020, it was observed that in June 2021, survival was 80.3%, with 19.7% of members dying during this year; at the end of the 3-year follow-up period (June 2023), 40.9% of the members of the Orcasitas cohort had died. This outcome affected people with Barthel's < 20 to a greater extent [78.95% (n = 15)]. Three-year mortality was not associated with BMI, marital status, economic or educational level, or the burden of chronicity (Tables 1, 4).
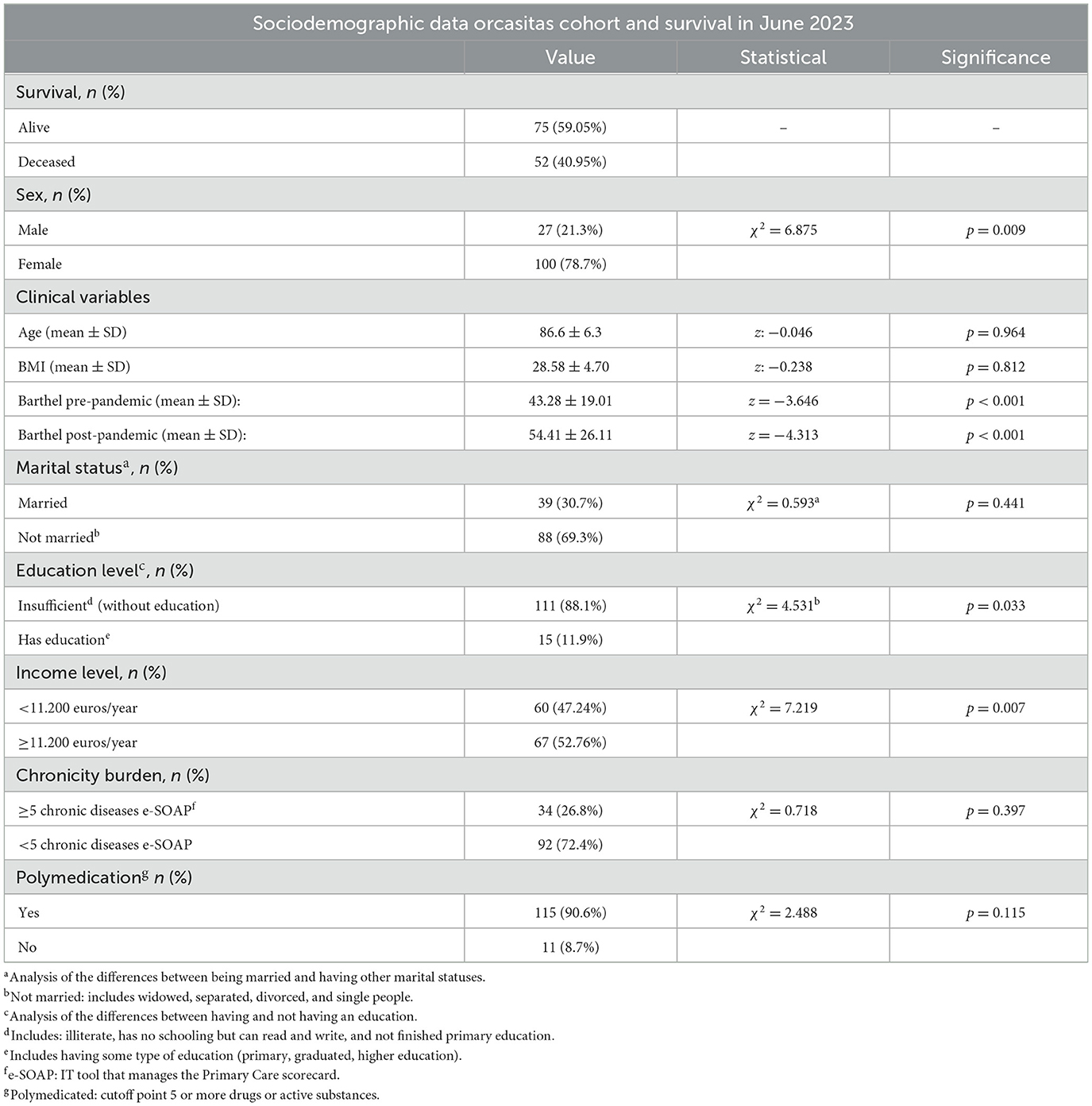
Table 4. Clinical and sociodemographic data of the Orcasitas cohort in June 2020 and analysis of their relationship with survival in June 2023.
This group was very old, and to avoid possible biases, only the group of people aged 80 years or older, representing 90.5% of this cohort, was included compared to the general non-dependent population. In relation to this age group, 36.7% (n = 33) of the dependent women (n = 90) and 60% (n = 15) of the men (n = 25) died in the period 2020–2023. Data from the Health System's IHC application shows 1,682 non-dependent persons in June 2020, 1,110 women and 572 men. In June 2023, 10.18% (113) of women and 9.6% (55) of non-dependent men were no longer registered in this application, with 997 (92.6%) women and 517 (92.8%) men remaining registered. Compared to the non-dependent population, the functionally dependent population aged 80 years or older in this cohort was more likely to drop out of the registries in the following 3 years (OR 5.767; CI 3.882–8.568), a situation that occurred in both sexes, women (OR 5.108; CI 3.190–8.179) and men (OR 11.750; CI 5.235–26.370).
When the data were analyzed using the classic classification of dependence into four levels, a method used in the Spanish National Health System, it was observed that the risk of mortality increased progressively as the level of dependence increased until it became significant between mild dependence and total dependence. The difference between mild dependence and moderate or severe dependence was not significant (Table 5). The difference between mild dependence and moderate- and severe-dependence groups was not significant (Table 5). One year after the end of the nationwide COVID-19 lockdown, the pre-pandemic level on the Barthel scale was not associated with survival, but the post-pandemic level was (Table 6). Three years after the end of confinement, both the pre-pandemic level and the post-pandemic level were associated with survival (Table 6), with higher mortality observed among people with severe and total functional dependence.
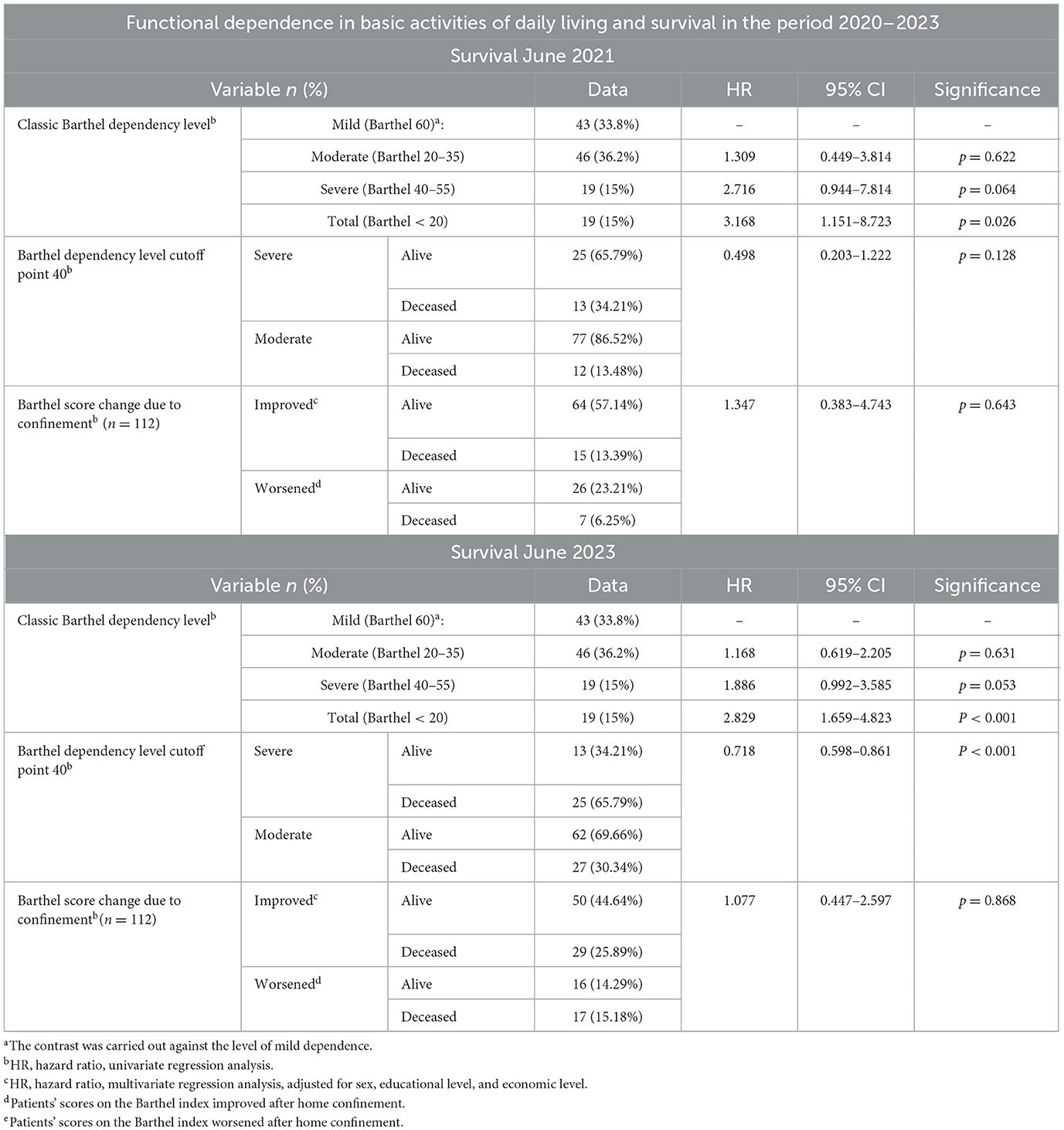
Table 5. Survival at 1 year and 3 years of follow-up among people with functional dependence in the Orcasitas cohort in relation to their level of dependence and the changes in the Barthel index during the nationwide COVID-19 lockdown decreed by the government of Spain.
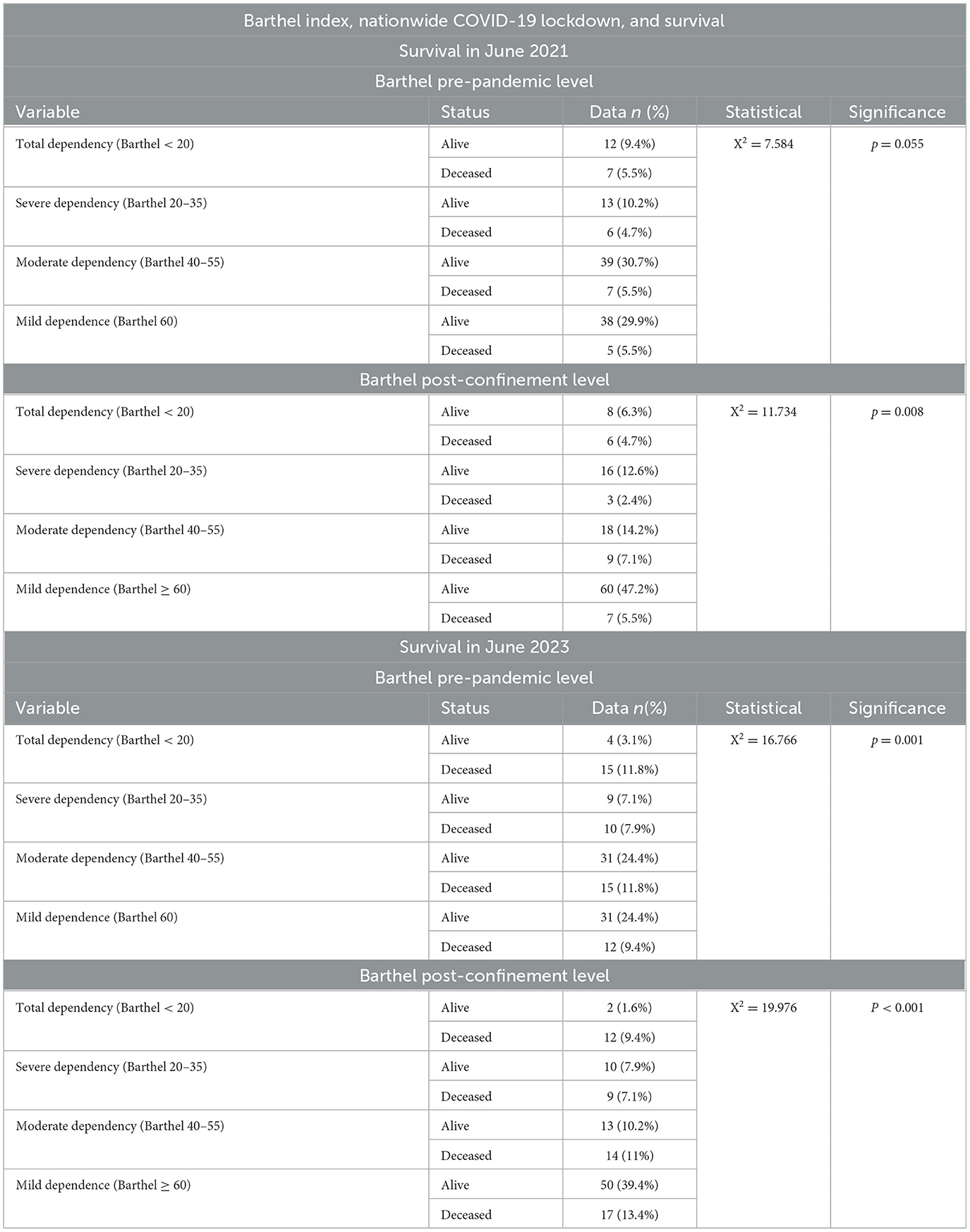
Table 6. Evolution of functional dependence during COVID-19 pandemic home confinement, estimated using the Barthel index, and its relationship with survival at 1 year (June 2021) and 3 years (June 2023).
Taking a cutoff point on the Barthel index of 40 as a reference, in June 2021, 34.21% of people with severe dependency died, a percentage that rose to 65.79% in June 2023. Among people with moderate dependence, these percentages were 13.48 and 30.34%, respectively.
A lower score on the Barthel index and a higher degree of dependence were associated with higher mortality (Tables 1, 4, 5). Patients with severe dependence had a greater probability of dying than patients with moderate dependence during this period, with an HR in June 2021 of 2,537 (CI 1.277–5.041) and 2.169 (CI 1.469–3.201) in June 2023. These results were maintained when the data were adjusted for age, sex, educational level, and income level, with an HR of 2.606 (CI 1.314–5.167) in June 2021 and an HR of 2.227 (CI 1.514–3.276) in June 2023, and by Cox regression. The results are represented graphically in Figure 5.
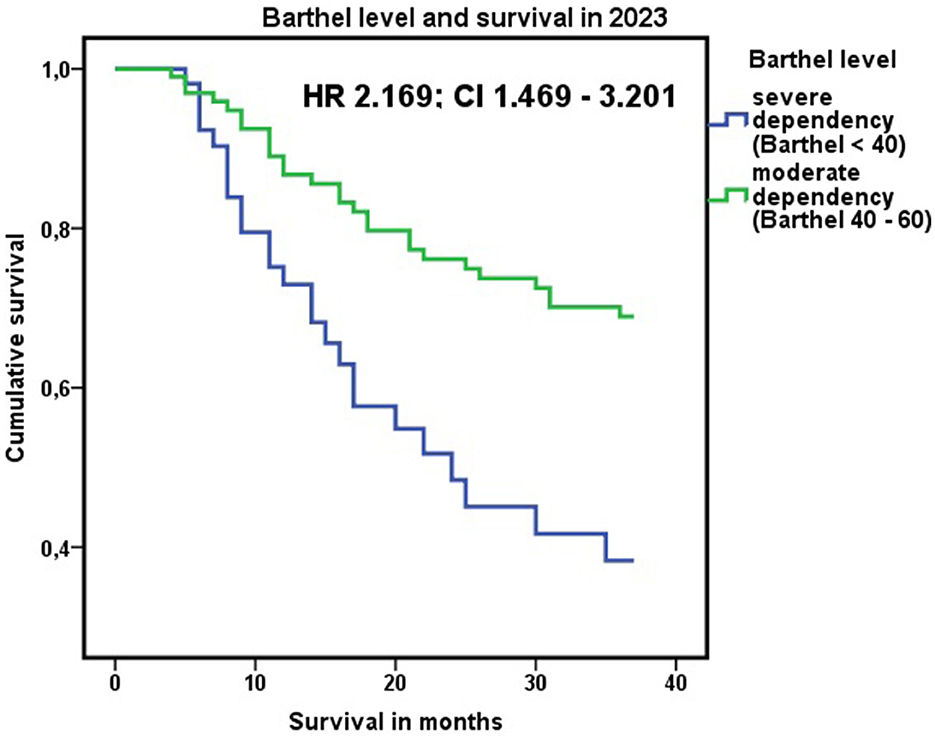
Figure 5. Association between the level of dependency (<40 or ≥40 on the Barthel index) and cumulative mortality through June 2023. HR 2.169; CI 1.469–3.201. Cox regression: survival in 2023 adjusted for age, sex, educational level, and income level of the dependent person.
After confinement for the COVID-19 pandemic, 43.3% (n = 55) of the individuals in this cohort were no longer dependent. Of these, 74.5% (n = 41) were still alive at the end of the 3-year follow-up period, with the remaining 25.5% (n = 14) dying. Among those who remained dependent, 47.2% (n = 34) were still alive at 3 years, and 52.8% (n = 38) died. During the COVID-19 pandemic confinement, those dependent persons who improved their functional abilities to the point of no longer being considered dependent had a higher probability of survival at 3 years (OR 0.306; CI 0.142–0.655).
A cutoff point of 40 on the Barthel index was a better indicator of the risk of mortality associated with dependency than the classic classification into four levels (Table 5). No influence on survival was observed in 2021 or 2023, with an improved or worsened Barthel score between pre- and post-confinement. When this relationship was analyzed according to level of dependence and sex, however, women with moderate dependence who improved their Barthel score during confinement had a higher probability of survival at 3 years (OR 3.700; CI 1.111–12.327).
However, in Figure 1, the quadrant delimited by an age higher than the mean age and a Barthel index score lower than the cohort mean presented the highest mortality in the period 2020–2023.
In 2023, the mean age was 85.89 ± 5.63 years, and the mean BMI was 29.25 ± 4.33. In the 2020–2023 period, there was greater mortality in men than in women; 63% of the men and 35% of the women in the Orcasitas cohort died, with an HR for the male sex of 1.745 (CI 1.045–2.915) (Table 2). In 2023, 24.4% (n = 31) of initially functional-dependent people still had a Barthel score >60, thus falling outside the Health System dependency protocol.
The Barthel index and the items that compose it as predictors of survival
Finally, when the ability of the Barthel index as a test to discriminate mortality associated with dependence was analyzed using ROC curves, both the score and the level on the Barthel index had confidence intervals above 0.5, indicating the existence of a discriminative capacity between persons with and without dependency. However, in both cases, the AUCs were between 0.5 and 0.7, indicating a low degree of discrimination (Figure 6). By Cox regression and adjusting for possible confounding factors, the Barthel index showed that at the cohort level, it could adequately discriminate population mortality risk (Figure 7).

Figure 6. Barthel index and survival data. Areas under the ROC curve for levels on the Barthel index before and after nationwide COVID-19 lockdown with respect to survival in 2021 and 2023.
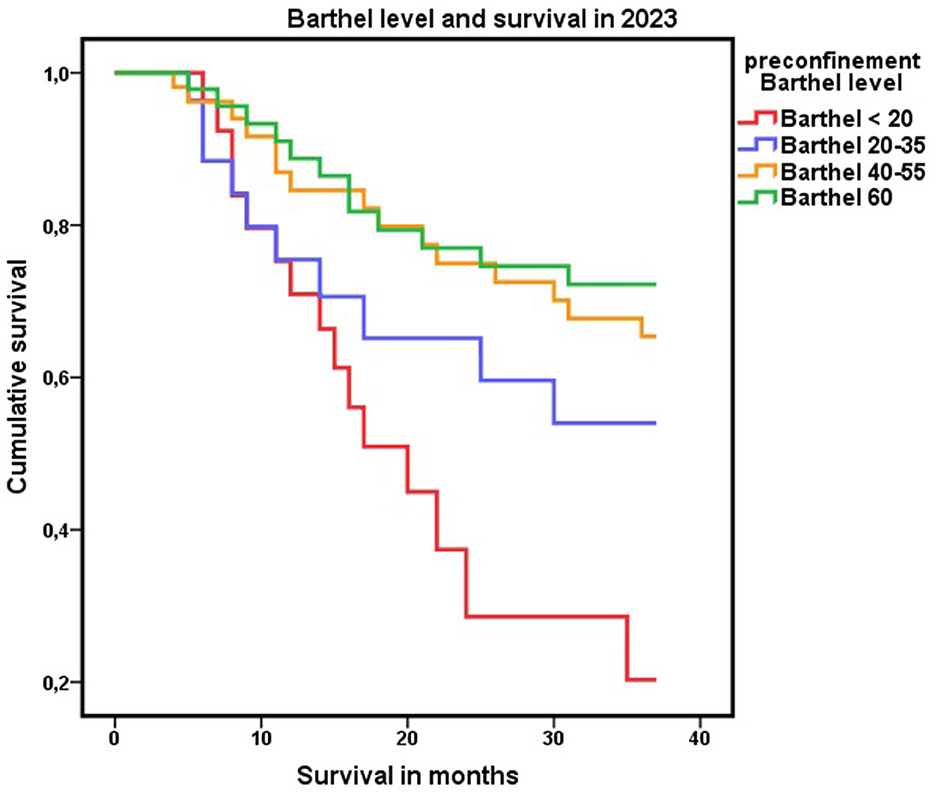
Figure 7. Level of dependence on the Barthel Index. Cox regression analysis of mortality at 3 years of follow-up according to the baseline level on the Barthel index.
Breaking down the Barthel index according to its items to analyze the influence of each one in relation to survival, at 1 year, the discriminative capacity as a test of most of the items was low. However, the discriminative capacity of some items increased over time. For example, during follow-up, the AUC of the Barthel item “chair–bed transfers” improved to the category “useful in some circumstances” in 2023 (Figure 8).
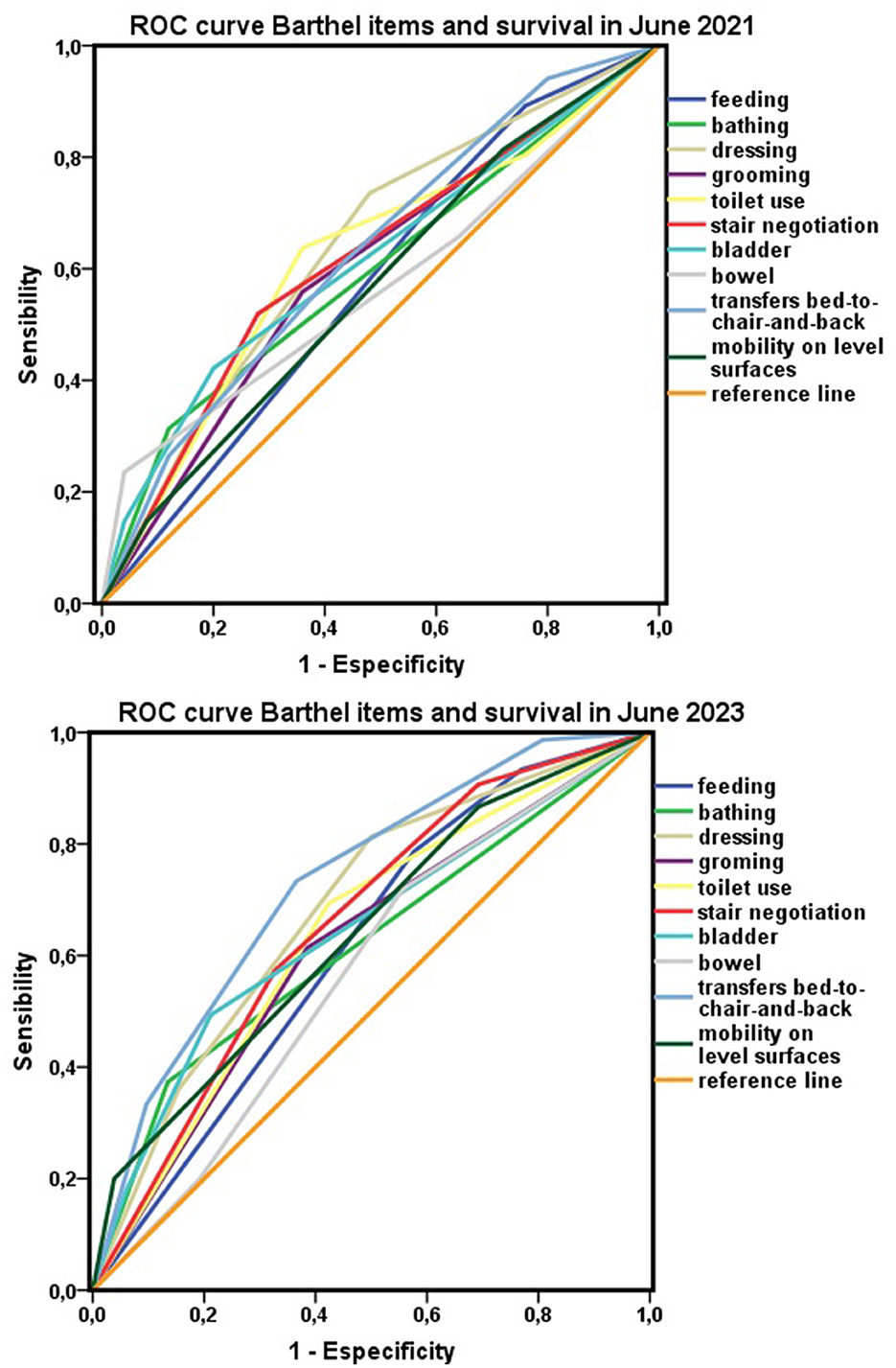
Figure 8. Items of the Barthel index and survival. Areas under the ROC curve for each item of the Barthel index with respect to survival in 2021 and 2023.
Discussion
The COVID-19 pandemic was the reason for carrying out this study, which made visible an already pre-existing situation, that of a population that was to a certain extent invisible, with a high mortality rate, and about which there was a great lack of knowledge. This lack of knowledge led to the prediction of results that reality showed to be radically different. The confinement and the risk of death due to the pandemic produced an awakening in the functionally dependent population of the Orcasitas cohort as a form of resilience in the face of adversity. This awakening, in response to the challenge posed to the functionally dependent population by being locked in their homes for months at a time, was observed across all ages and showed a non-significant tendency to become less frequent as the group analyzed got older.
The way in which older people lived in their environment influenced the level of functional improvement observed. A significant trend toward greater functional improvement was found among people living alone or with a partner, compared to those living with their children or others. Having fewer social support resources forced these people to respond to adversity in a way that people who did have these resources may not have needed since their cohabitants covered their basic subsistence needs.
In addition to making it possible to visualize a vulnerable group due to their frailty, this study provided relevant results on a diagnostic tool that is easy to use and inexpensive, the Barthel index. This tool showed its full potential as a predictor of short-term mortality during the COVID-19 pandemic (2, 18–20, 24–28). In this study, it was also a good predictor of medium- and long-term mortality (27–29). These results place the Barthel index at an advantage as a tool for detecting at-risk populations in health planning (20, 27–29) and in risk assessment in multiple clinical situations requiring discriminating the risk of adverse events.
In older persons, functional dependence is associated with greater mortality (24, 25), and this study showed that this risk was significantly higher in men than in women and that it was greater the higher the level of dependence (26, 27). These results are similar to those reported in other studies and show that age and sex influence the development and progression of functional disability (28). However, sex, age, and dependence are not isolated factors; rather, they evolve in a context that, as other studies have also reported, influences the observed results (29). The context described in this cohort is an unfavorable social environment, consisting of a suburb of the capital of Spain with an aging population, in which one in five people is 65 or older, and with a large group of people over 80 years. This environment was complemented by unfavorable economic and cultural indicators. The population with functional dependence in the Orcasitas cohort had a low socioeconomic level, which placed almost half of them in the vicinity of the poverty threshold; in 2020, the poverty threshold in Spain was 9,626 euros/year. In addition, they shared a low cultural level, with almost all the dependents in this cohort having an insufficient level of education.
It is in this social environment that the nationwide confinement by COVID-19 took place, with an unexpected effect observed in the population with functional dependence due to this confinement: improvement in functional capacity to perform basic activities of daily living. Although initially this response could be considered a temporary adaptive response to a stressful event that put survival at risk, longitudinal follow-up showed that it involved greater changes. Changes were observed not only in the persistence of improved functional dependence at 3 years but also in that many people ceased to be dependent after confinement and maintained and regained functional independence in the long term. Such changes were relevant in terms of survival.
The presence of a very old dependent population that potentially has few cultural and economic coping tools in an environment of home confinement was expected to worsen baseline conditions (30–32), which occurred during the pandemic in institutionalized patients (33–36). However, in the non-institutionalized dependent population of the Orcasitas cohort, nationwide COVID-19 lockdown triggered an “awakening” phenomenon, developing survival defense mechanisms that made it possible to improve their functional capacities, with a direct effect: half of the dependent persons in this cohort ceased to be dependent. This result was also observed in people with total dependence, in a more moderate form and in relation to their important limitations. This change left a visible imprint as a sawtooth in the functional assessment conducted with the Barthel index between 2020 and 2023. Research on the pandemic and home confinement has shown that dependency is a dynamic process that is susceptible to intervention (37), and that there is no age limit for this intervention.
In addition to the data described above on the social environment, the population of Orcasitas came from a socioeconomic immigration background to the outskirts of large cities in the middle of the last century and lived for many years in substandard housing or shantytowns. These individuals were the first marginal population group to design their own housing for rehousing in the 1970s and 1980s, forming a social group with a markedly vindictive nature that may have generated an important resilience in the face of adversity (37, 38), which could justify the improvement described. On the other hand, the loss of support resources, such as daycare centers or home-help assistants, forced them to carry out activities that they had not previously done, a situation that has been described as increasing resilience (39) and which did not happen in nursing homes (40).
The intervention of protective psychosocial factors acquired prior to exposure to the new stressor posed by the COVID-19 pandemic has already been described in other studies (41) and probably played a relevant role in the fact that the results observed in this study did not describe functional deterioration. This deterioration is usually the predictable outcome when people with frailty are subjected to prolonged stressors and was observed during COVID-19 pandemic confinement in institutionalized individuals or those requiring hospital admissions, including admissions for COVID-19 (2, 27, 32–35, 42, 43). These living situations (nursing home, hospital) generally entail an added dependence on third parties (nursing home staff, health professionals), which can affect the person's own self-concept (43) and the innate resilience or resilience developed over the course of life, making its protective effect less visible or non-existent (44).
The increase in life expectancy has led to the appearance of new factors, which may have influenced the results observed in this study. These factors, such as subjective age (the age the patient feels he or she is), subjective aging (how the individual perceives his or her own aging process), and, in age groups as advanced as this one, the role of the subjective proximity of death (45, 46) probably play a role in the life history observed.
However, the data obtained also show that not all the dependent population behaved in the same way in the face of the stressor event of the COVID-19 pandemic, and these differences could be based on Antonovsky's theory of salutogenesis (47, 48), with implications in relation to survival. Beyond the classic coping strategies, part of this population, due to their origins, their life history (poverty at birth, emigration, living in substandard housing, unemployment, low or no education, low income), and their constant struggle to get by, would have developed a chronic adaptive resilience—resilience that they applied daily to survive in permanent adverse living conditions. This vital evolution would have generated psychosocial resources and even biological and material resources not studied (subsistence economy), which would be included within the so-called General Resilience Resources of Antonovsky and would have ended up giving a Sense of Coherence to their lives even in adversity. These resources would remain active or latent, depending on the person's basal state and degree of dependence, and the COVID-19 pandemic brought them to light. Its effect would be reflected in the person's capacity to make the necessary changes to improve his or her functionality, trying to survive the pandemic, changes that were recorded in this study employing the Barthel index, and for which age was not a limiting factor. However, this response showed that these changes had a result not only in terms of functionality but also in terms of survival, so those who made the changes were more likely to stay alive in the long term. This situation was observed in this study not only among women with moderate dependency, who improved their functional capacity during confinement and significantly increased their survival, but also in the observation that those who had the capacity to make positive changes and did make them, had a higher representation among those who survived to 3 years.
Functional dependence is a progressive process clearly associated with high mortality. The COVID-19 pandemic was relevant enough to motivate these people to face it within the “sense of coherence” proposed by Antonovsky. These people, despite their dependence, had the capacity to rearrange themselves again to survive. This capacity for improvement was independent of age, previous disease burden, and the presence of polypharmacy and was observed at all levels of functional dependence. These changes not only had short-term but also long-term effects. For instance, it implied that people who were functionally dependent before the pandemic ceased to be so with the pandemic and maintained this change over time, some of them being functionally independent 3 years later. All of this was in a context with a mean age of 86 years.
This functional improvement at the cohort level allowed them to gain time as the group currently has slightly better functionality than in 2020, even though almost half of the cohort died in this triennium.
In this line, the mean age of this cohort was advanced, and a high abandonment rate was to be expected due to the mere fact of natural deaths due to age (at the end of the study, the mean age, if no one had died, would have been 89 years, well-above life expectancy in Spain). However, among the non-dependent population over 80 years of age, the same abandonment rate was not observed, so being over 80 years of age and being functionally dependent was probably a risk factor for mortality. This cannot be confirmed in this study because the abandonment rate in the non-dependent population includes both deaths and changes of residence outside the Orcasitas neighborhood.
Mortality was higher in men, and although at the general population level, men have a lower life expectancy than women (49), other causes cannot be ruled out for the different mortality by gender observed in the dependent population. As expected, mortality was also higher in persons with greater functional dependence.
For non-institutionalized dependent patients, being included as a total dependent is equivalent to being placed on the threshold of death. The final causes of this mortality, its evolutionary course, and the actions developed by the different agents involved in its follow-up have been the subject of few studies. Moreover, this high mortality rate is not usually made visible by society, which associates it with aging itself, favoring ageism that increases social inequalities (7).
Although the percentage of non-institutionalized older persons with functional dependence might not seem to be high compared to the general population of the same age, the high mortality rate observed in this group makes it advisable to implement changes in health planning to address this problem. This problem, although not strictly health-related, form part of the holistic care that Primary Health Care should provide citizens to maintain equity in care. Above all, an environment where the aging of the population is likely to increase in functional dependence, justifies these actions.
Suggested changes to the current model of care for older persons with functional dependence are supported by the evidence observed in this study that there is room for improvement, there is no age limit for improvement, and this improvement influences long-term survival. Other studies also observe positive changes in long-term functional dependence through proactive actions in these persons (50).
The Barthel index is a simple method of assessment and, as confirmed by this study, it allows easy discrimination of population risk (19, 26, 42), being a good predictor of medium- and long-term mortality (27, 51, 52) and justifying its use to discriminate at-risk populations in health planning (19, 26, 41). In this study, we used two methods for assessing the Barthel index: the classic method, which consists of four levels of dependence, and the method that establishes two levels of dependence, with a cutoff point at Barthel 40. The justification for this approach is 2-fold: on the one hand, to favor comparison of the results of this study with those of other studies, and, on the other hand, to allow health planning to benefit from this double criterion to establish the appropriate indicator in relation to survival.
This study unified the risk levels “total dependence” and “severe dependence” into a single level of severe dependence with a cutoff point of 40 on the Barthel index. This showed greater discrimination in terms of the risk of death. This result, supported by the guidelines of some health systems (23, 51, 53), allows us to recommend using this criterion in medium- and long-term health planning to obtain better health results. The discriminative power of the Barthel index as a test seems to increase as the cohort follow-up is prolonged, as in parallel, each of the items that make up the scale.
A limitation of this study is that the sample size and follow-up time did not allow us to reach greater statistical significance. This could perhaps be present in larger samples or over longer times. Another limitation of the study is that non-parametric estimates of the AUC tend to be underestimated when data from discrete rating scales are used, such as those included in the Barthel index (54).
Evaluating the Barthel index, the pre-confinement level prior to March 2020 was taken as a reference to avoid the biases of the pandemic, the loss of attendant care for domestic work, and the high variability of care of non-cohabitating children toward their parents in this phase. These factors caused a “storm” among dependents, and their effect on the items comprising the Barthel index was not predictable.
The time variable had its effect on this baseline state, “filtering” in terms of survival of those items that are most related to it and highlighting those on which health planning should have an impact to minimize its impact and improve the quality of life of these people. As the components of this population died, this filter effect on the time variable showed its potential, allowing us to detect new questions about the indisputable value of the Barthel index, such as the extent to which the loss of mobility is the factor that leads to this higher mortality among people with functional dependence.
The role of each item of the Barthel index in identifying the most vulnerable patients should be established. Furthermore, items that assess instrumental ADLs should be integrated to provide more individualized care to provide equivalent care for non-institutionalized people with dependency and those in institutionalized care (54).
In summary, unexpected confinement that was forced on this cohort did not have the same effect on functional deterioration as that produced by other sudden events, such as hospital admission (3, 18) or institutionalization (16). Nor was it associated with progressive deterioration associated with age and comorbidities (9, 10), social isolation (20, 27, 55), or the situation of loneliness that affects many of our older people (56). A stressful situation, such as a pandemic, triggers response mechanisms to ensure survival—mechanisms that are present in all individuals, regardless of their level of dependence (35). The results for the Orcasitas cohort, in line with what is proposed in Antonovsky's theory of salutogenesis (57, 58), indicate a resilient population that shows strength in an unforeseen situation and attempts to give the best of itself to be able to move forward (38). Longitudinal studies are needed to analyze the characteristics of the non-institutionalized functionally dependent population and establish policies to improve the quality of life of this population group (54, 59) and to move away from the stereotypical image of dependent persons who consume many resources without contributing anything, promoting their integration in the face of growing social discrimination based on ageism (60).
Conclusions
The functionally dependent population that is not institutionalized in nursing homes and remains in the community is a group that is, to some extent, invisible in epidemiological studies. Advanced age, and especially very advanced age, such as that of this cohort, predisposes us to assimilate that mortality is part of the normal evolutionary course. Similarly, we assimilate the loss of functional capacities as normal. However, accepting these premises should not imply doing nothing to improve the quality of life of these people. Perhaps the main result of this study has been to show that there is a capacity for improvement at any age. And that this capacity for improvement is maintained at all levels of functional dependence. Stereotypes and labels can be a source of inequalities. Against ageism, integration, the promotion of the maintenance of social roles, and the development of activities that encourage the maintenance or recovery of functional capacities may be the appropriate strategies to maintain equity in the care of our older people.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Center Local Research Commission of the Primary Care Management of Madrid (reference number 16/20-C-Bis) on June 29, 2020. The Ethics Committee of the Hospital provided approval by resolution CEIm 23/501 dated September 26, 2023. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
VM: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MF: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MB: Conceptualization, Data curation, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. HA: Conceptualization, Formal analysis, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. EP: Conceptualization, Data curation, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. LC: Conceptualization, Data curation, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. SG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. ESá: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. ESe: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. IS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MR: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. JH: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. IL: Conceptualization, Formal analysis, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
GIDO Collaborative Group (Orcasitas Dependency Research Group)
Vicente Martín Moreno, Orcasitas Health Care Center and i+12 Research Institute of the Doce de Octubre hospital; GIDO group co-director, Madrid, Spain; María Inmaculada Martínez Sanz, Orcasitas Health Care Center; GIDO group co-director, Madrid, Spain; Miriam Fernández Gallardo, María Palma Benítez Calderón, Helena Alonso Samperiz, Elena Pérez Rico, Laura Calderón Jiménez, Sara Guerra Maroto, Elena Sánchez Rodríguez, Eva Sevillano Fuentes, Irene Sánchez González, Julia Herranz Hernando, and Irene León Saiz, Orcasitas Health Care Center, Madrid, Spain; Amanda Martín Fernández, Polibea Concert, Madrid, Spain; Miguel Recuero Vázquez, Orcasitas Health Care Center and Nursing Home Care Unit of the Center Assistance Directorate, Madrid, Spain.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The authors declare that they have received financial support for the translation and publication of this article from the Fundación para la Investigación e Innovación Biosanitaria de Atención Primaria (FIIBAP), a public foundation dependent on the Madrid Health Service, Spain, IP: COVID 2020-06.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1385058/full#supplementary-material
References
1. Ramiro Fariñas D, Mazzoni S, Ruiz-Santacruz JS, Osorio Arjona J, Muñoz Díaz C. Impacto del COVID-19 en los Indicadores Demográficos de la Comunidad de Madrid y su estructura de edad. Dirección General de Economía. Consejería de Economía, Hacienda y Empleo. Madrid : Comunidad de Madrid (2022). Available online at: https://www.madrid.org/iestadis/fijas/estructu/demograficas/mnp/descarga/indecovidinfo21.pdf (accessed August 8, 2023).
2. Ocagli H, Cella N, Stivanello L, Degan M, Canova C. The Barthel index as an indicator of hospital outcomes: a retrospective cross-sectional study with healthcare data from older people. J Adv Nurs. (2021) 77:1751–61. doi: 10.1111/jan.14708
3. Dessie ZG, Zewotir T. Mortality-related risk factors of COVID-19: a systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect Dis. (2021) 21:855. doi: 10.1186/s12879-021-06536-3
4. Parohan M, Yaghoubi S, Seraji A, Javanbakht MH, Sarraf P, Djalali M. Risk factors for mortality in patients with Coronavirus disease 2019 (COVID-19) infection: a systematic review and meta-analysis of observational studies. Aging Male. (2020) 23:1416–24. doi: 10.1080/13685538.2020.1774748
5. Mas Romero M, Avendaño Céspedes A, Tabernero Sahuquillo MT, Cortés Zamora EB, Gómez Ballesteros C, Sánchez-Flor Alfaro V, et al. COVID-19 outbreak in long-term care facilities from Spain. Many lessons to learn. PLoS ONE. (2020) 15:e0241030. doi: 10.1371/journal.pone.0241030
6. Causa R, Almagro Nievas D, Bermúdez Tamayo C. COVID-19 y dependencia funcional: análisis de un brote en un centro sociosanitario de personas mayores. Rev Esp Salud Publica. (2021) 95:e202103045. Available online at: https://ojs.sanidad.gob.es/index.php/resp/article/view/573
7. Abdi S, Spann A, Borilovic J, de Witte L, Hawley M. Understanding the care and support needs of older people: a scoping review and categorisation using the WHO international classification of functioning, disability and health framework (ICF). BMC Geriatr. (2019) 19:195. doi: 10.1186/s12877-019-1189-9
8. XX Dictamen del Observatorio Estatal de la Dependencia. Asociación Estatal de directores y Gerentes en Servicios Sociales. Available online at: https://directoressociales.com/wp-content/uploads/2021/01/INFO-GLOBAL-XX-DICTAMEN-3-3-20_compressed.pdf (accessed June 16, 2020).
9. Molina-Mula J, Miguélez-Chamorro A, Taltavull-Aparicio JM, Miralles-Xamena J, Ortego-Mate MDC. Quality of life and dependence degree of chronic patients in a chronicity care model. Healthcare. (2020) 8:293. doi: 10.3390/healthcare8030293
10. Makovski TT, Le Coroller G, Putrik P, Choi YH, Zeegers MP, Stranges S, et al. Role of clinical, functional and social factors in the association between multimorbidity and quality of life: findings from the Survey of Health, Ageing and Retirement in Europe (SHARE). PLoS ONE. (2020) 15:e0240024. doi: 10.1371/journal.pone.0240024
11. Violan C, Foguet-Boreu Q, Flores-Mateo G, Salisbury C, Blom J, Freitag M, et al. Prevalence, determinants and patterns of multimorbidity in primary care: a systematic review of observational studies. PLoS ONE. (2014) 9:e102149. doi: 10.1371/journal.pone.0102149
12. Verlaan S, Ligthart-Melis GC, Wijers SLJ, Cederholm T, Maier AB, de van der Schueren MAE. High prevalence of physical frailty among community-dwelling malnourished older adults-a systematic review and meta-analysis. J Am Med Dir Assoc. (2017) 18:374–82. doi: 10.1016/j.jamda.2016.12.074
13. Wei K, Nyunt MS, Gao Q, Wee SL, Yap KB, Ng TP. Association of frailty and malnutrition with long-term functional and mortality outcomes among community-dwelling older adults: results from the Singapore Longitudinal Aging Study 1. JAMA Netw Open. (2018) 1:e180650. doi: 10.1001/jamanetworkopen.2018.0650
14. Alves VP, Casemiro FG, Araujo BG, Lima MAS, Oliveira RS, Fernandes FTS, et al. Factors associated with mortality among elderly people in the COVID-19 pandemic (SARS-CoV-2): a systematic review and meta-analysis. Int J Environ Res Public Health. (2021) 18:8008. doi: 10.3390/ijerph18158008
15. Cases L, Vela E, Santaeugènia Gonzàlez SJ, Contel JC, Carot-Sans G, Coca M, et al. Excess mortality among older adults institutionalized in long-term care facilities during the COVID-19 pandemic: a population-based analysis in Catalonia. Front Public Health. (2023) 11:1208184. doi: 10.3389/fpubh.2023.1208184
16. Oliva J, Peña Longobardo LM. Impacto de la COVID-19 en la atención sociosanitaria: el caso de las residencias. Informe SESPAS 2022. Gac Sanit. (2022) 36(Suppl. 1):S56–60. doi: 10.1016/j.gaceta.2022.02.003
17. Bickel H. Das letzte Lebensjahr: Eine Repräsentativstudie an Verstorbenen. Wohnsituation, Sterbeort und Nutzung von Versorgungsangeboten. Z Gerontol Geriatr. (1998) 31:193–204. doi: 10.1007/s003910050034
18. González Del Castillo J, Jacob J, García-Lamberechts EJ, Piñera Salmerón P, Alquézar-Arbé A, Llorens P, et al. Red de investigación SIESTA. Sociodemographic characteristics, comorbidity, and baseline functional status of older patients treated in emergency departments during the COVID-19 pandemic and associations with mortality: an analysis based on the EDENCOVID cohort. Emergencias. (2022) 34:428–36.
19. Wang E, Liu A, Wang Z, Shang X, Zhang L, Jin Y, et al. The prognostic value of the Barthel Index for mortality in patients with COVID-19: A cross-sectional study. Front Public Health. (2023) 10:978237. doi: 10.3389/fpubh.2022.978237
20. Wilk P, Ruiz-Castell M, Stranges S, Bohn T, Fagherazzi G, Nicholson K, et al. Relationship between multimorbidity, functional limitation, and quality of life among middle-aged and older adults: findings from the longitudinal analysis of the 2013-2020 Survey of Health, Ageing, and Retirement in Europe (SHARE). Qual Life Res. (2023) 33:169–81. doi: 10.1007/s11136-023-03508-9
21. Sistema Nacional de Salud. Ministerio de Sanidad y Política Social. Cartera de Servicios de Atención Primaria. Desarrollo, organización, usos y contenido. Madrid: Mayo (2010). Available online at: https://www.sanidad.gob.es/estadEstudios/estadisticas/docs/siap/Cartera_de_Servicios_de_Atencion_Primaria_2010.pdf (accessed June 16, 2020).
22. Mahoney FI, Barthel DW. Functional evaluation: The Barthel Index. Md State Med J. (1965) 14:61–5. doi: 10.1037/t02366-000
23. Dirección General de Coordinación Socio-Sanitaria. Consejería de Sanidad. Comunidad de Madrid. Plan de Atención a la fragilidad y promoción de la longevidad saludable en personas mayores de la comunidad de Madrid 2022-2025. Madrid (2022). Available online at: https://www.comunidad.madrid/transparencia/sites/default/files/plan/document/paifls_2022_2025._version_definitva.pdf (accessed October 9, 2023).
24. Millán-Calenti JC, Tubío J, Pita-Fernández S, González-Abraldes I, Lorenzo T, Fernández-Arruty T, et al. Prevalence of functional disability in activities of daily living (ADL), instrumental activities of daily living (IADL) and associated factors, as predictors of morbidity and mortality. Arch Gerontol Geriatr. (2010) 50:306–10. doi: 10.1016/j.archger.2009.04.017
25. Beltran B, Cuadrado C, Martin ML, Carbajal A, Moreiras O. Activities of daily living in the Spanish elderly. Association with mortality. J Nutr Health Aging. (2001) 5:259–60.
26. Ryg J, Engberg H, Mariadas P, Pedersen SGH, Jorgensen MG, Vinding KL, et al. Barthel Index at hospital admission is associated with mortality in geriatric patients: a Danish nationwide population-based cohort study. Clin Epidemiol. (2018) 10:1789–800. doi: 10.2147/CLEP.S176035
27. Fernández Alonso C, Fuentes Ferrer ME, García-Lamberechts EJ, Aguiló Mir S, Jiménez S, Jacob Rodriguez J, et al. Impact of functional dependency of elderly patients seen in Spanish emergency departments during the first wave of the COVID-19 pandemic on mortality at 30, 180 and 365 days depending on the diagnosis (COVID versus non-COVID). Rev Esp Salud Publica. (2023) 97:e202310085.
28. Okabe T, Suzuki M, Iso N, Tanaka K, Sagari A, Miyata H, et al. Long-term changes in older adults' independence levels for performing activities of daily living in care settings: a nine-year follow-up study. Int J Environ Res Public Health. (2021) 18:9641. doi: 10.3390/ijerph18189641
29. Redzovic S, Vereijken B, Bonsaksen T. Aging at home: factors associated with independence in activities of daily living among older adults in Norway-a HUNT study. Front Public Health. (2023) 11:1215417. doi: 10.3389/fpubh.2023.1215417
30. Atici E, Girgin N, Çevik Saldiran T. The effects of social isolation due to COVID-19 on the fear of movement, falling, and physical activity in older people. Australas J Ageing. (2022) 41:407–13. doi: 10.1111/ajag.13063
31. Fettes L, Bayly J, de Bruin LM, Patel M, Ashford S, Higginson IJ, et al. Relationships between prolonged physical and social isolation during the COVID-19 pandemic, reduced physical activity and disability in activities of daily living among people with advanced respiratory disease. Chron Respir Dis. (2021) 18:14799731211035822. doi: 10.1177/14799731211035822
32. Saraiva MD, Apolinario D, Avelino-Silva TJ, de Assis Moura Tavares C, Gattás-Vernaglia IF, Marques Fernandes C, et al. The impact of frailty on the relationship between life-space mobility and quality of life in older adults during the COVID-19 pandemic. J Nutr Health Aging. (2021) 25:440–7. doi: 10.1007/s12603-020-1532-z
33. Greco GI, Noale M, Trevisan C, Zatti G, Dalla Pozza M, Lazzarin M, et al. Increase in frailty in nursing home survivors of coronavirus disease 2019: comparison with noninfected residents. J Am Med Dir Assoc. (2021) 22:943–7.e3. doi: 10.1016/j.jamda.2021.02.019
34. Cortés Zamora EB, Mas Romero M, Tabernero Sahuquillo MT, Avendaño Céspedes A, Andrés-Petrel F, Gómez Ballesteros C, et al. Psychological and functional impact of COVID-19 in long-term care facilities: the COVID-A study. Am J Geriatr Psychiatry. (2022) 30:431–43. doi: 10.1016/j.jagp.2022.01.007
35. Thompson MQ, Jadczak AD, Tucker GR, Theou O, Visvanathan R. Frailty change based on minimally important difference in nursing home residents: FIRST cohort study findings. Age Ageing. (2022) 51:afac246. doi: 10.1093/ageing/afac246
36. Escribà-Salvans A, Vemorel C, Font-Jutglà C, Minobes-Molina E, Goutan-Roura E, Rosa-Oliveira V, et al. Efecto del confinamiento por COVID-19 sobre la incidencia y gravedad de las caídas en personas mayores institucionalizadas: estudio longitudinal. Rev Esp Geriatr Gerontol. (2023) 58:155–60. doi: 10.1016/j.regg.2023.02.005
37. Ungar R, Wu L, MacLeod S, Tkatch R, Huang J, Kraemer S, et al. The impact of COVID-19 on older adults: results from an annual survey. Geriatr Nurs. (2022) 44:131–6. doi: 10.1016/j.gerinurse.2022.01.010
38. de Uriarte Arciniega J. La resiliencia. Una nueva perspectiva en psicopatología del desarrollo. Rev Psicodidáctica. (2005) 10:61–80. Available online at: http://www.redalyc.org/articulo.oa?id=17510206
39. Carriedo A, Cecchini JA, Fernandez-Rio J, Méndez-Giménez A. COVID-19, Psychological well-being and physical activity levels in older adults during the nationwide lockdown in Spain. Am J Geriatr Psychiatry. (2020) 28:1146–55. doi: 10.1016/j.jagp.2020.08.007
40. Palacios-Ceña D, Fernández-Peña R, Ortega-López A, Fernández-Feito A, Bautista-Villaécija O, Rodrigo-Pedrosa O, et al. Long-term care facilities and nursing homes during the first wave of the COVID-19 pandemic: a scoping review of the perspectives of professionals, families and residents. Int J Environ Res Public Health. (2021) 18:10099. doi: 10.3390/ijerph181910099
41. Morse JL, Fischer IC, Na PJ, Afari N, Pietrzak RH. Functional decline during the COVID-19 pandemic among US military veterans: results from the National Health and Resilience in Veterans Study. Int J Geriatr Psychiatry. (2023) 38:e6040. doi: 10.1002/gps.6040
42. da Costa JC, Manso MC, Gregório S, Leite M, Pinto JM. Barthel's index: a better predictor for COVID-19 mortality than comorbidities. Tuberc Respir Dis. (2022) 85:349–57. doi: 10.4046/trd.2022.0006
43. Pérez-Rodríguez P, Díaz de Bustamante M, Aparicio Mollá S, Arenas MC, Jiménez-Armero S, Lacosta Esclapez P, et al. Functional, cognitive, and nutritional decline in 435 elderly nursing home residents after the first wave of the COVID-19 pandemic. Eur Geriatr Med. (2021) 12:1137–45. doi: 10.1007/s41999-021-00524-1
44. Caplan G. Loss, stress, and mental health. Community Ment Health J. (1990) 26:27–48. doi: 10.1007/BF00752675
45. Petashnick JR, Shrira A, Hoffman Y, Palgi Y, Kavé G, Shmotkin D. Subjective age and late-life functional status: mediating and moderating effects. J Gerontol B Psychol Sci Soc Sci. (2022) 77:61–70. doi: 10.1093/geronb/gbab181
46. Westerhof GJ, Nehrkorn-Bailey AM, Tseng HY, Brothers A, Siebert JS, Wurm S, et al. Longitudinal effects of subjective aging on health and longevity: an updated meta-analysis. Psychol Aging. (2023) 38:147–66. doi: 10.1037/pag0000737
47. Rivera de los Santos F, Ramos Valverde P, Moreno Rodríguez C, Hernán García M. Salutogenic model analysis in Spain: application in public health and implications for asset health model. Rev Esp Salud Publica. (2011) 85:129–39. Spanish. doi: 10.1590/S1135-57272011000200002
48. Seah B, Espnes GA, Hong WT, Wang W. Salutogenic Healthy Ageing Programme Embracement (SHAPE)- an upstream health resource intervention for older adults living alone and with their spouses only: complex intervention development and pilot randomized controlled trial. BMC Geriatr. (2022) 22:932. doi: 10.1186/s12877-022-03605-3
49. García González JM, Grande R. Cambios en las diferencias por sexo en la esperanza de vida en España (1980-2012): descomposición por edad y causa. Gac Sanit. (2018) 32:151–7. doi: 10.1016/j.gaceta.2017.03.004
50. Dong HJ, Peolsson A, Johansson MM. Effects of proactive healthcare on pain, physical and activities of daily living functioning in vulnerable older adults with chronic pain: a pragmatic clinical trial with one- and two-year follow-up. Eur Geriatr Med. (2024). doi: 10.1007/s41999-024-00952-9
51. Formiga F, Ferrer A, Montero A, Chivite D, Pujol R. Predictors of 3-year mortality in subjects over 95 years of age. The NonaSantfeliu study. J Nutr Health Aging. (2010) 14:63–5. doi: 10.1007/s12603-010-0011-3
52. Conde-Martel A, Hemmersbach-Miller M, Marchena-Gomez J, Saavedra-Santana P, Betancor-Leon P. Five-year survival and prognostic factors in a cohort of hospitalized nonagenarians. Eur J Intern Med. (2012) 23:513–8. doi: 10.1016/j.ejim.2012.02.007
53. Nahm FS. Receiver operating characteristic curve: overview and practical use for clinicians. Korean J Anesthesiol. (2022) 75:25–36. doi: 10.4097/kja.21209
54. Frutos ML, Cruzado DP, Lunsford D, Orza SG, Cantero-Téllez R. Impact of social isolation due to COVID-19 on daily life activities and independence of people over 65: a cross-sectional study. Int J Environ Res Public Health. (2023) 20:4177. doi: 10.3390/ijerph20054177
55. Estrategia de Atención a las Personas Mayores de la Comunidad de Madrid 2017-2021. Consejería de Políticas Sociales y Familia. Madrid: Comunidad de Madrid (2017). Available online at: https://www.comunidad.madrid/transparencia/sites/default/files/plan/document/372_767_estrategia_atencion_al_mayor_version_digital_0.pdf (accessed September 26, 2023).
56. Hajek A, Brettschneider C, Eisele M, Mallon T, Oey A, Wiese B, et al. Social support and functional decline in the oldest old. Gerontology. (2022) 68:200–8. doi: 10.1159/000516077
57. Schlomann A, Bünning M, Hipp L, Wahl HW. Aging during COVID-19 in Germany: a longitudinal analysis of psychosocial adaptation. Eur J Ageing. (2021) 19:1077–86. doi: 10.1007/s10433-021-00655-1
58. Tan JY, Tam WSW, Goh HS, Ow CC, Wu XV. Impact of sense of coherence, resilience and loneliness on quality of life amongst older adults in long-term care: a correlational study using the salutogenic model. J Adv Nurs. (2021) 77:4471–89. doi: 10.1111/jan.14940
59. Porcel-Gálvez AM, Badanta B, Barrientos-Trigo S, Lima-Serrano M. Personas mayores, dependencia y vulnerabilidad en la pandemia por coronavirus: emergencia de una integración social y sanitaria. Enferm Clin. (2021) 31:S18–23. Spanish. doi: 10.1016/j.enfcli.2020.05.004
Keywords: COVID-19, basic activities of daily living, Barthel, functional impairment, social inequalities, vulnerability, frailty, salutogenesis
Citation: Martín Moreno V, Martínez Sanz MI, Fernández Gallardo M, Martín Fernández A, Benítez Calderón MP, Alonso Samperiz H, Pérez Rico E, Calderón Jiménez L, Guerra Maroto S, Sánchez Rodríguez E, Sevillano Fuentes E, Sánchez González I, Recuero Vázquez M, Herranz Hernando J and León Saiz I (2024) The influence of nationwide COVID-19 lockdown on the functional impairment and long-term survival of dependent people for carrying out basic activities of daily living in a neighborhood of the city of Madrid, Spain: Orcasitas Cohort Longitudinal Study. Front. Public Health 12:1385058. doi: 10.3389/fpubh.2024.1385058
Received: 11 February 2024; Accepted: 14 June 2024;
Published: 09 July 2024.
Edited by:
Linda L. D. Zhong, Nanyang Technological University, SingaporeReviewed by:
John Dierx, Avans University of Applied Sciences, NetherlandsMiao Jiang, University of Italian Switzerland, Switzerland
Copyright © 2024 Martín Moreno, Martínez Sanz, Fernández Gallardo, Martín Fernández, Benítez Calderón, Alonso Samperiz, Pérez Rico, Calderón Jiménez, Guerra Maroto, Sánchez Rodríguez, Sevillano Fuentes, Sánchez González, Recuero Vázquez, Herranz Hernando and León Saiz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vicente Martín Moreno, YW1hbnZpY0Bob3RtYWlsLmNvbQ==