
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Public Health, 27 March 2024
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1376513
This article is part of the Research TopicWorld Antimicrobial Awareness WeekView all 25 articles
 Qi Li1,2
Qi Li1,2 Xiaoshi Zhou1,2
Xiaoshi Zhou1,2 Rou Yang1,2
Rou Yang1,2 Xiaoyan Shen2,3
Xiaoyan Shen2,3 Guolin Li1,4Changji Zhang1,4Pengfei Li2Shiran Li1,2Jingxian Xie1
Guolin Li1,4Changji Zhang1,4Pengfei Li2Shiran Li1,2Jingxian Xie1 Yong Yang1,2*
Yong Yang1,2*Intensive care units (ICUs) are specialized environments dedicated to the management of critically ill patients, who are particularly susceptible to drug-resistant bacteria. Among these, carbapenem-resistant Gram-negative bacteria (CR-GNB) pose a significant threat endangering the lives of ICU patients. Carbapenemase production is a key resistance mechanism in CR-GNB, with the transfer of resistance genes contributing to the extensive emergence of antimicrobial resistance (AMR). CR-GNB infections are widespread in ICUs, highlighting an urgent need for prevention and control measures to reduce mortality rates associated with CR-GNB transmission or infection. This review provides an overview of key aspects surrounding CR-GNB within ICUs. We examine the mechanisms of bacterial drug resistance, the resistance genes that frequently occur with CR-GNB infections in ICU, and the therapeutic options against carbapenemase genotypes. Additionally, we highlight crucial preventive measures to impede the transmission and spread of CR-GNB within ICUs, along with reviewing the advances made in the field of clinical predictive modeling research, which hold excellent potential for practical application.
Antibiotics play a vital role in controlling bacterial infections; however, the development of new antibiotics lags far behind the worldwide spread of antimicrobial resistance (AMR) (1, 2). It has been estimated that in 2019, drug-resistant bacterial pathogens were responsible for 1.27 million deaths (3). This number has nearly doubled from the 700,000 deaths reported in 2016 from AMR globally, in just a few years. According to experts, this number could reach 10 million by 2050 if resistance is not reduced or new antibiotics are not developed (4). Carbapenem-resistant Gram-negative bacteria (CR-GNB) possess a high resistance rate against a wide range of antibiotics, further limiting the antibiotic options available for patients. CRE (carbapenem-resistant Enterobacteriaceae), CRAB (carbapenem-resistant Acinetobacter baumannii), and CRPA (carbapenem-resistant Pseudomonas aeruginosa) are classified as pathogens posing a significant threat to human health (4).
Patients admitted to the intensive care unit (ICU) are typically immunocompromised, presenting with multiple comorbidities, overuse of broad-spectrum antibiotics, indwelling catheters, and undergoing multiple invasive procedures, which puts them at a relatively high risk of bacterial infections (5). According to Vincent et al. (6), the incidence of infection in ICU patients exceeds 50%. At present, the commonly employed microbiological methods for diagnosing bacterial infections suffer from a delayed nature, making it challenging to promptly target antibiotics based on drug sensitivity tests. The lack of rapid diagnostic methods to identify resistance genes in the clinical setting, as well as the scarcity of targeted antimicrobials, often results in the overuse of broad-spectrum antibiotics, which is a major contributor to AMR (7). Treatment options for infections caused by CR-GNB are limited and associated with high rates of clinical failure, morbidity, and mortality. Once a CR-GNB infection occurs and is left uncontrolled, it is highly likely to progress into a severe infection and lead to the mortality of patients in the ICU. Understanding the appropriate range of antibiotics for treatment is crucial for establishing an effective treatment strategy initially, alongside enhancing preventive and control measures within the ward to halt pathogen dissemination and deter drug resistance development. This paper offers a comprehensive examination of bacterial resistance mechanisms, CR-GNB resistance genes, and therapeutic options for respective infections. It concludes by outlining strategies for preventing CR-GNB colonization and infections in the ICU, including advancements in infection prediction models for critically ill populations. The application of prediction models in the ICU to promptly identify high-risk groups for CR-GNB infection can provide valuable insights for controlling the spread of CR-GNB in the ICU and improving the prognosis of ICU patients.
The AMR is a complex as well as multifactorial phenomenon. In terms of its mechanism, AMR is associated with both selective pressure on bacteria and horizontal gene transfer between bacteria (8, 9). Figure 1 illustrates complex resistance mechanisms in bacteria: (i) Restriction of antibiotic entry. Many antibiotic targets are within bacteria, reducing the uptake of antimicrobials and thereby preventing their binding to the target site. (ii) Enhancement of efflux pumps. A large amount of antibiotic is released out of the cell, reducing the concentration of antibiotics within the bacteria. (iii) Regulation and defense of antibiotic target sites. Preventing the antibiotic from reaching its binding site and modifying the target site so that the affinity of the antibiotic molecule is reduced. (iv) Production of hydrolytic enzymes. Inactivation of the drug by adding specific chemical parts to the compound or destruction of the molecule itself so that the antibiotic cannot interact with its target. In addition, bacteria can adapt to antibiotic attacks by acquiring key DNA through horizontal gene transfer. Plasmids and transposons play a crucial role in developing and spreading bacterial resistance in clinical infections (10). Many resistance genes are localized on plasmids, and these mobile genetic elements can quickly transfer resistance within or between different bacterial species. Transformation (incorporation of naked DNA), transduction (phage-mediated), and splicing (bacterial “sexing”) are the three main ways. The emergence of resistance in the hospital setting usually involves splicing, a very efficient gene transfer method involving cell-to-cell contact.
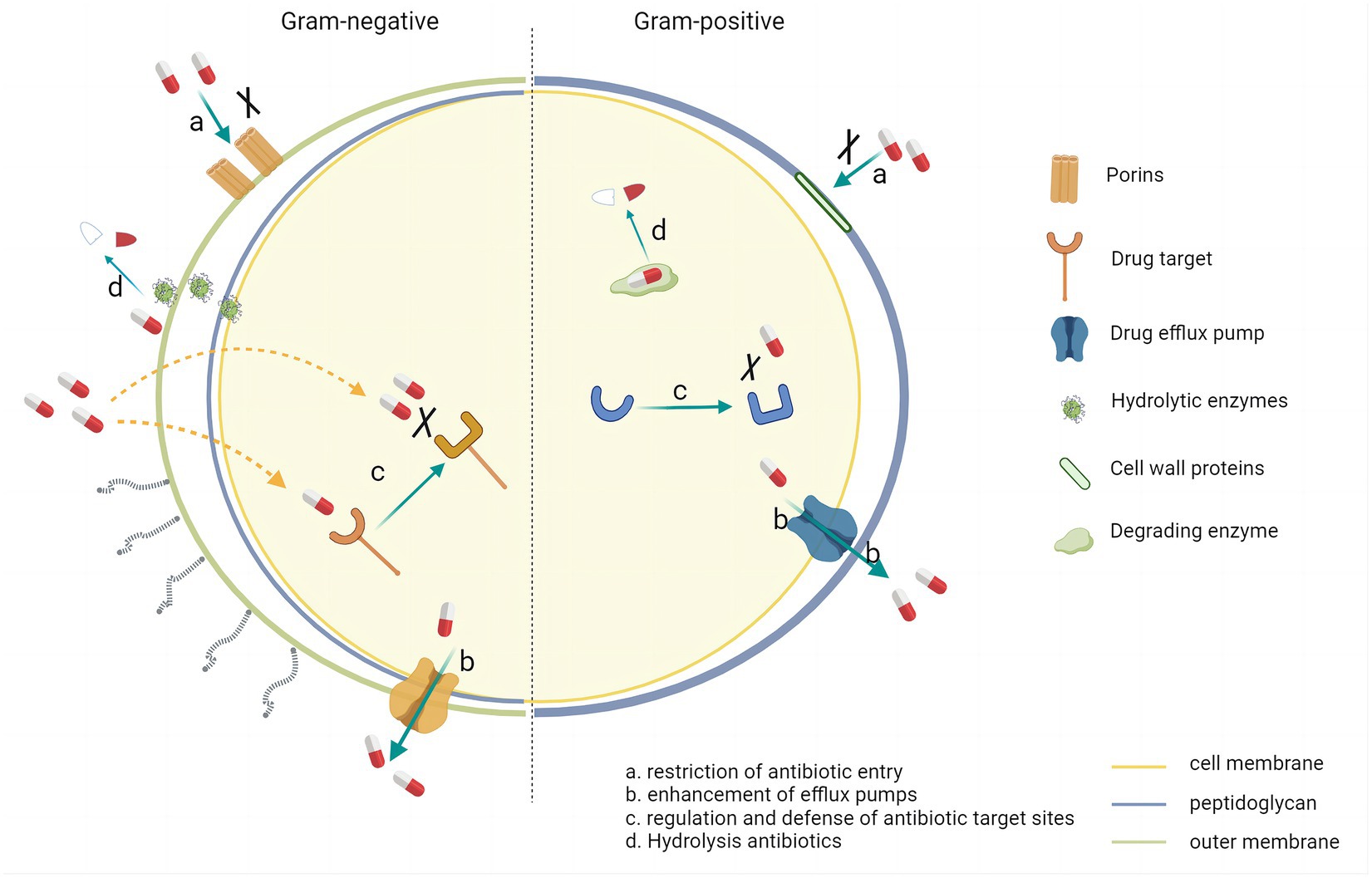
Figure 1. Resistance mechanisms in Gram-negative bacteria and Gram positive bacteria.
The production of β-lactamases is a crucial mechanism of drug resistance in Gram-negative bacteria. Ambler’s classification categorizes these bacteria into four groups: A to D. The enzymes in classes A, C, and D use serine residues in their active catalytic site to hydrolyze β-lactams, while class B enzymes are metallo β-lactamases (MBLs) that contain zinc in their active site (11). Among these, extended spectrum β-lactamases (ESBLs), which belong to Ambler class A, can hydrolyze various β-lactam antibiotics such as cefotaxime, ceftriaxone, and ceftazidime, but they cannot hydrolyze and are resistant to cephalosporins and carbapenems (12). Infections caused by ESBL-producing Enterobacteriaceae (EBLS-E), which are mainly Klebsiella pneumoniae (K. pneumoniae) and Escherichia coli, are increasing worldwide (13, 14). The primary resistant genotypes of ESBL include blaCTX-M, blaSHV, and blaTEM (15). CTX-M type ESBL is the most predominant type of Enterobacteriaceae cultured from blood and hydrolyzes cefotaxime and ceftriaxone more effectively than ceftazidime (16). Carbapenem antibiotics, which are atypical β-lactam antibiotics with the broadest antimicrobial spectrum and the strongest antibacterial activity, can prevent cell wall synthesis and lead to bacterial lysis by inhibiting penicillin binding proteins (17). The resistance mechanism of CR-GNB can be classified into enzymatic and non-enzymatic types. Production of carbapenemase is a critical mechanism of GNB resistance to carbapenem antibiotics. The carbapenemase type of CR-GNB is shown in Figure 2. The genes encoding for carbapenemases are highly transmissible and easily spread through plasmid-and transposon-mediated dissemination (18). Non-enzymatic CR is primarily mediated by the acquisition of resistance genes, including mutations in chromosomally encoded porin genes (e.g., OprD) and overexpression of genes encoding efflux pumps (including MexAB-OprM, Mexxy-OprM, and MexCD-OprJ) (19). The genes that lead to resistance to carbapenem antibiotics in different species of Gram-negative bacilli are thus somewhat different. In the following section, the common CR-GNB within the ICU are summarized along with the genes they have been found to cause resistance.
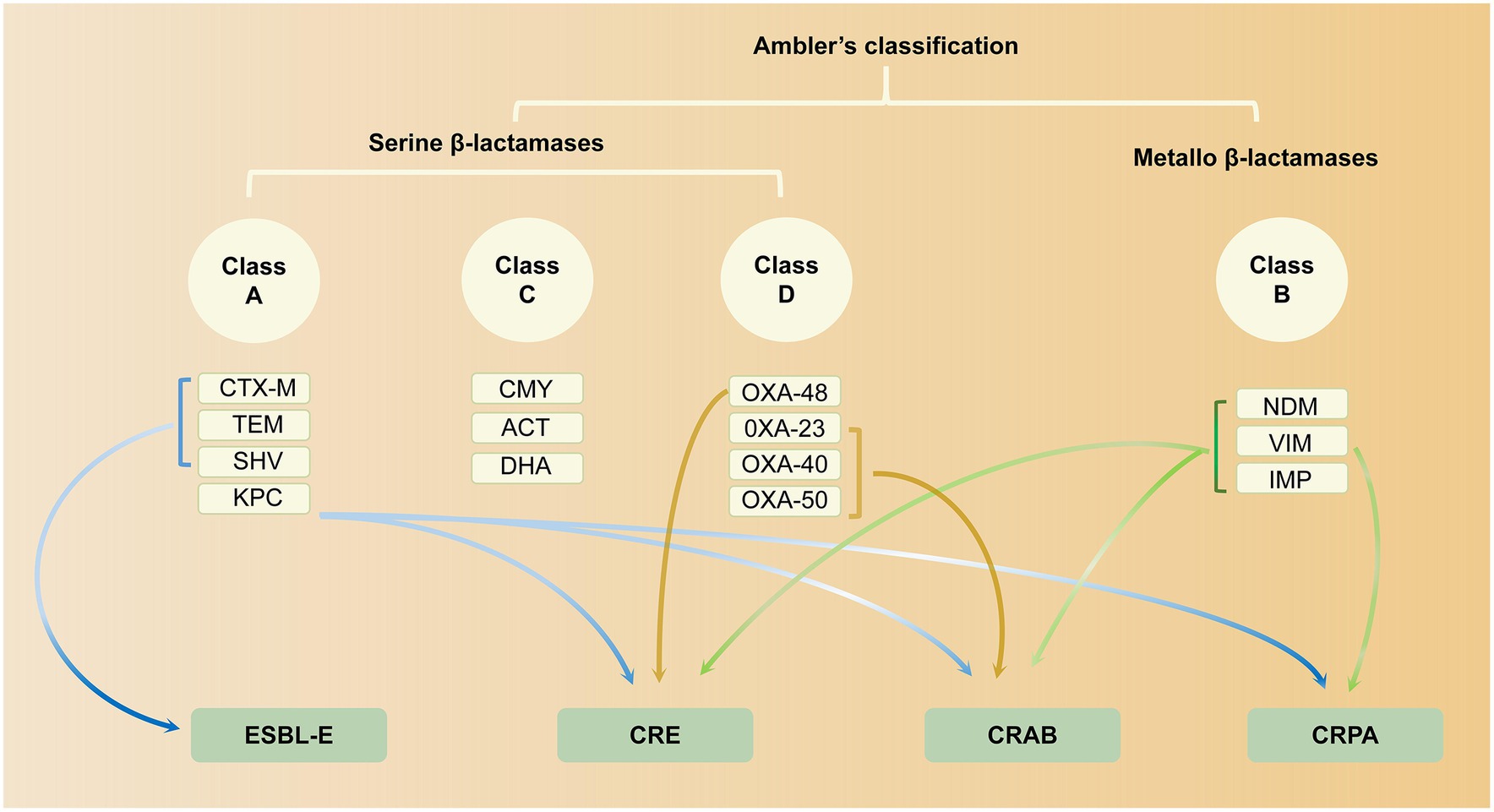
Figure 2. β-lactamases in MDR-GNB according to Ambler’s classification.
The Centers for Disease Control and Prevention (CDC) defines CRE as Enterobacteriaceae that are resistant to carbapenem antibiotics. In the United States, approximately 13,000 infections caused by CRE have been reported in hospitalized patients, resulting in an estimated 1,100 deaths (20). Patients who require medical devices such as ventilators, urinary catheters, or intravenous catheters, those who are on prolonged antibiotic treatment, and individuals with weakened immune systems are at a relatively high risk of contracting CRE infections (21). Hence, it is crucial to exercise caution in implementing therapeutic measures to avoid unnecessary invasive procedures for patients who usually have underlying medical conditions and those who require ICU-level interventions. Based on the resistance mechanism, CRE can be categorized into carbapenemase-producing enterobacteria (CPE) and non-carbapenemase-producing enterobacteria (non-CPE). CPE comprises carbapenemase-resistant enzymes such as K. pneumoniae carbapenemase (KPC) in class A, benzoxacillin carbapenemase/oxacillinase (OXA) in class D, and MBLs belonging to class B, including imipenemase metallo-β-lactamase (IMP), New Delhi metallo-β-lactamase (NDM), and Verona integrase-encoded metallo-β-lactamase (VIM) (11). The blaKPC gene is the most prevalent gene in Ambler class A, and its production plays a significant role in the carbapenem-resistant K. pneumoniae (CRKp). On the other hand, blaOXA-48 is a more common gene responsible for resistance to carbapenem antibiotics in Escherichia coli (22). Single CRE isolate can possess multiple carbapenemase-encoding genes. For instance, in Egypt, where NDM and OXA-48-like enzymes are widespread, polymerase chain reaction results demonstrated that about 90% of Enterobacteriaceae isolates harbored one or more carbapenemase-encoding genes, with blaNDM-1 being the most prevalent genotype, followed by blaOXA-48 (23).
Acinetobacter baumannii (A. baumannii) is the most frequently isolated pathogen in ICUs (24), leading to various infections such as pneumonia, skin and soft tissue infections, and bloodstream infections (BSIs) (25, 26). The emergence of CRAB poses a significant challenge for treatment and has intensified the prevalence of hospital-acquired infections, thus becoming a major threat to global public health (11). The mechanisms of carbapenem resistance in A. baumannii involve various factors such as increased efflux pumps, decreased expression or inactivation of pore proteins, modifications of penicillin-binding proteins, and production of several types of β-lactamases (27, 28). The most common mechanism observed in CRAB is the production of carbapenemases, and the genes encoding the acquired carbapenemases play a key role. Among carbapenemases, the OXA enzymes are the most frequently reported in A. baumannii, such as OXA-23, OXA-24, OXA-40, OXA-51, OXA-58, and OXA-143 (29, 30). Additionally, metastable MBLs, including VIM, IMP, and NDM enzymes, have also been linked with drug resistance phenotypes in A. baumannii (11). It is essential to note that although KPC enzymes have primarily been detected in K. pneumoniae, variants of blaKPC, such as blaKPC-2 and blaKPC-3, have been reported in A. baumannii in a Brazilian hospital (31). The acquisition of blaKPC might be associated with A. baumannii’s resistance to carbapenems.
Pseudomonas aeruginosa (P. aeruginosa) is a Gram-negative bacterium commonly found in moist environments, such as washing tanks, aerators, respirators, and other equipment, as well as solutions exposed in hospital environments (32). It is a significant cause of healthcare-related problems, leading to urinary, respiratory, and BSIs in long-stay hospitalized patients (11, 33). These infections can be fatal in critically ill and immunocompromised patients in ICUs, and they may be further exacerbated by AMR (34). Infections caused by CRPA result in longer hospitalization periods and higher mortality rates compared to infections caused by carbapenem antibiotic-sensitive strains (35, 36). The development of CRPA involves the interaction of several complex resistance mechanisms. Firstly, the upregulation of efflux pumps (e.g., MexAB-oprM) allows for increased drug efflux, leading to resistance against most β-lactams (37). Additionally, the loss of OprD outer membrane proteins, which normally prevent the entry of antibiotics, coupled with the overproduction of Ambler C-like enzymes, can result in the near-exhaustion of P. aeruginosa’s resistance to β-lactams (38). Resistance to carbapenem antibiotics through carbapenemase production is a less common mechanism (39). Out of 28 CRPA strains isolated in the ICU, only three strains produced KPC (40). However, carbapenemase production as a resistance mechanism appears to be increasingly common, with blaVIM in MBLs being the most commonly detected gene, typically encoded on plasmids that are highly capable of dissemination (38). In instances where CRPA lacks carbapenemases, resistance is typically due to the absence of OprD or the overexpression of efflux pumps.
Given the limited therapeutic options for extensively drug-resistant Gram-negative bacteria, it is crucial to adopt a rational approach in utilizing available antibiotics to mitigate the emergence and spread of AMR. To effectively manage infections caused by CR-GNB, it is recommended to carefully select appropriate therapeutic agents based on the genetic characteristics of the bacteria. Below, it provides a concise summary of the mechanisms and efficacy of therapeutic selection. The activity of the treatment options on CR-GNB is summarized in Table 1.
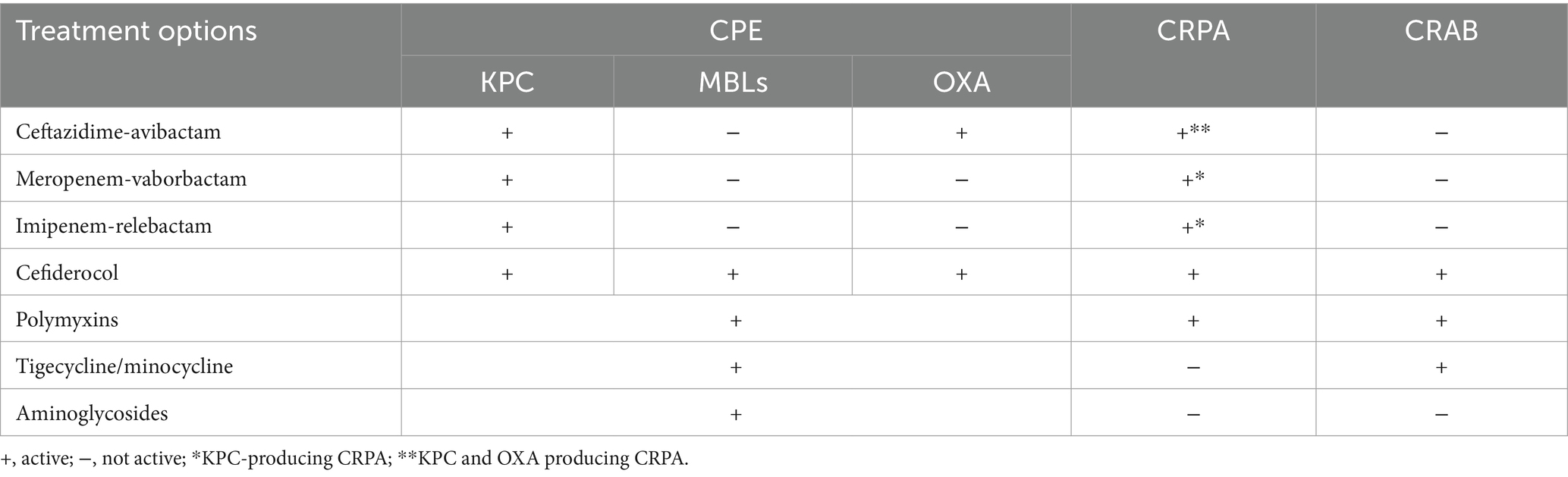
Table 1. List of treatment options against carbapenemase-producing Gram-negative organisms.
Avibactam binds reversibly to β-lactamases and exhibits activity against carbapenemases, thereby restoring the inhibitory activity of ceftazidime against the majority of CRE and CRPA. Ceftazidime/avibactam generally demonstrates high efficacy against organisms producing KPC, although resistance has been observed in isolates producing KPC-2 and KPC-3, which may be attributable to reduced porin expression (41). Combination therapy could reduce mortality in BSIs caused by KPC-producing K. pneumoniae (42). However, the use of ceftazidime/avibactam in combination with other antimicrobial agents for the treatment of CRE and CRPA infections did not exhibit significant advantages in terms of survival and cure rates (43, 44). Ceftazidime/avibactam alone demonstrates superior effectiveness in patients with OXA-48-producing CRE infections compared to treatment with colistin, tigecycline, and meropenem (45, 46). Therefore, prioritizing ceftazidime/avibactam for the treatment of KPC-producing or OXA-48-producing CRE, as well as CRPA, may improve survival rates among patients in the ICU and reduce the risk of renal injury, as opposed to selecting alternative drugs or multidrug combinations. Moreover, since avibactam does not inhibit MBLs (NDM, VIM, and IMP), combining it with aztreonam, a drug stable against metallo-β-lactamases, may be a potential therapeutic strategy for treating CR-GNB infections belonging to class B. The combination of ceftazidime/avibactam and aztreonam exhibits good in vitro activity against Enterobacteriaceae producing metallo-β-lactamases, with favorable in vitro effectiveness (47).
Vaborbactam is a β-lactamase inhibitor that primarily targets KPC carbapenemases but not MBLs, as well as class D β-lactamases (48). On the other hand, meropenem effectively treats Gram-negative bacilli, such as K. pneumoniae, Enterobacter spp., and P. aeruginosa. Together, meropenem/vaborbactam is a novel combination that exhibits strong and specific activity against KPC-producing CRE. While Vaborbactam also possesses the capacity to inhibit ESBLs and AmpC β-lactamases, its supplementary activity is not necessary, as meropenem alone effectively stabilizes these β-lactamases. Though multi-agent treatments may benefit high-risk patients, mono-therapy may be enough for other patients. For instance, meropenem/vaborbactam alone showed higher cure rates and lower patient mortality and nephrotoxicity in individuals with predominantly bacteremic CRE infections compared to other drug combinations (49). Therefore, along with considering the type of carbapenemase, a successful treatment of CR-GNB infections also necessitates consideration of different infection types, the severity of the infection, susceptibility of the causative organism, and the patient’s general health condition. Thus, meropenem/vaborbactam is another viable option for KPC-producing CRE infections.
Relebactam is a type of β-lactamase inhibitor, structurally similar to avibactam, that can inhibit common class A carbapenemases (e.g., KPC) and class C cephalosporinases (e.g., AmpC). In vitro, relebactam has been shown to reverse resistance to imipenem in KPC-producing P. aeruginosa but has no potentiation effect in isolates with class B or D carbapenemase activity (50). In an in vivo C. elegans model, imipenem/relebactam was found to be a significant treatment for KPC-producing K. pneumoniae infections (51). Furthermore, relebactam in combination with imipenem/cilastatin inhibited AmpC, thus restoring the susceptibility of P. aeruginosa to imipenem. The combination demonstrated better efficacy with lower mortality and nephrotoxicity for the treatment of patients infected with CR-GNB (52). It is worth noting that this study included high-risk patients with poor outcomes, and the combination of relebactam and IMI is a potential therapeutic option for ICU patients infected with CR-GNB. Against blaKPC-containing P. aeruginosa, Imipenem/relebactam was shown in vitro to have a higher inhibitory activity than meropenem/vaborbactam but lower than ceftazidime/avibactam (53). Therefore, rapid diagnosis of the carbapenemase genotype of CRE or CRPA is significant for β-lactam/β-lactamase inhibitor combinations (BL/BLI) selections in clinical settings.
The recently approved BL/BLIs expand the therapeutic options available for KPC-producing and OXA-48-producing Enterobacteriaceae. Cefiderocol, the first cephalosporin containing an iron-based carrier, has gained approval for the treatment of carbapenem-resistant non-fermenting bacteria, including P. aeruginosa and A. baumannii (54). Current studies have demonstrated significant in vitro activity and effectiveness of cefodilol against CR-GNB (55). Cefodilol exhibits inherent stability against a wide range of carbapenemases, including class A, B, and D, as well as class C cephalosporinase hydrolases. Patients infected with KPC, NDM, VIM, IMP, and OXA-48 harboring CRE experiencing BSI or urinary tract infections can potentially benefit from cefodilol therapy (56). However, it is important to acknowledge that resistance may arise when cefiderocol is employed in the treatment of CRE. Instances of cefiderocol resistance in these isolates can be attributed to factors such as the clinical environment, in vitro exposure to cefiderocol, or resistance to other β-lactam antibiotics (e.g., ceftazidime or cefepime) prior to treatment. The application of cefiderocol in these cases carries a risk of mutation resulting in the development of specific mutations, such as NDM-5 (57), KPC-41, KPC-50 (58), and OXA-427 (59).
A study by Falcone et al. (60) conducted in the ICU featured 10 patients with A. baumannii BSI and ventilator-acquired pneumonia. These individuals had previous treatment failures with antibiotics, including colistin, and had developed renal and hepatic injury. Clinical success and survival rates at 30 days were 70 and 90%, respectively, with cefiderocol treatment. Cefiderocol monotherapy for critically ill patients was revealed to result in a lower infection recurrence rate and higher clinical success compared to combination therapy using drugs like colistin (61). However, all-cause mortality was higher with cefiderocol monotherapy. This trend may be linked to the heightened risk of infection recurrence or death in critically ill patients, who commonly experience trauma-induced immune compromise, prolonged hospitalization, invasive procedures, and colonization of the skin by multidrug-resistant organisms. Consequently, in addition to the timely and accurate selection of appropriate drug therapy, implementing specific preventive and control measures against CR-GNB infections in the ICU setting is paramount.
The newly approved BL-BLIs have emerged as the primary treatment options for CRE and CRPA infections. However, the treatment landscape for CRAB infections is becoming increasingly limited. Although BL-BLI therapy is recommended for urinary tract infections due to the high concentration of polymyxins in the urinary tract, it is still considered an alternative therapy for CRAB infections (62). According to the 2023 guidelines by the Infectious Diseases Society of America (IDSA) for the management of resistant Gram-negative bacteria infections, high-dose ampicillin-sulbactam in combination with other agents, including Polymyxin B, is recommended for the treatment of moderate-to-severe CRAB infections (63). Polymyxin B is specifically indicated for the treatment of severe infections, such as BSIs. However, the efficacy and safety of Polymyxin B as a monotherapy are not well-established. Thus, it is generally advised to administer Polymyxin B in combination with at least one other antimicrobial agent from a different class. Colistin, another approved drug from the polymyxin class of antibiotics, is considered a last-resort treatment for A. baumannii infections (64).
However, the emergence of polymyxin-resistant strains has been well-documented, potentially due to colistin’s prodrug nature and the prolonged presence of its active form in the body, which can predispose to resistance (65). Typically, colistin is recommended in combination with other agents for the treatment of CRE with CRPA infections. However, a clinical observational study (66) found that the difference in outcomes between patients treated with colistin sulfate alone versus in combination with other antibiotics was not statistically significant. The use of low-dose polymyxins in the treatment of multidrug-resistant A. baumannii infections may elevate the risk of mortality (66). A trial in 2018 demonstrated that colistin combined with meropenem treatment did not yield improved outcomes for severe infections caused by CR-GNB (67). Additionally, colistin therapy, especially when employed as part of combination therapy for patients with CR-GNB infections, may result in unfavorable clinical outcomes and potentially increase the risk of kidney injury in patients (68, 69). Combination therapy could heighten the probability of adverse effects, escalate the cost of antimicrobial therapy, and contribute to the development of antimicrobial resistance. Further clinical trials are imperative to establish the efficacy and safety of colistin as a complementary or alternative treatment for severe CR-GNB infections, particularly in cases where BL-BLI treatment proves ineffective.
Tigecycline is a novel intravenous antibiotic with broad-spectrum activity and is derived from minocycline. It has traditionally been considered the preferred treatment for infections caused by CRE. However, the latest guidelines from the IDSA recommend β-lactams as the primary option for treating CRE infections, with tigecycline as an alternate option if necessary (63). Combining tigecycline with colistin, carbapenems, or aminoglycosides is the most commonly used regimen for treating CRE infections. Studies comparing these combinations found that tigecycline-colistin was most effective against Klebsiella, while imipenem-colistin was best against Escherichia coli (70). Tigecycline combined with amikacin and colistin, or minocycline with cefoperazone-sulbactam, showed synergistic inhibitory activity against CRAB (71, 72). OXA-24-producing strains are more sensitive to tigecycline-amikacin and OXA-23-producing strains are more sensitive to tigecycline-mucin use [1]. Minocycline and tigecycline have lower nephrotoxicity compared to mucins versus aminoglycosides and can be used in combination with other drugs as another treatment option for CRAB (72). Notably, tigecycline-based regimens with high-doses (200 mg loading and 100 mg maintenance) showed lower mortality rates in ICU patients than standard doses (100 mg loading and 50 mg maintenance), and combination therapy with tigecycline was more effective than monotherapy (73). Consequent to exposure to tigecycline, resistance was induced in CRKp but tigecycline-resistant strains exhibited greater susceptibility to other drugs, including aminoglycosides, carbapenems, and cephalosporins (74). Sequential combination therapy with tigecycline and aminoglycosides may be a more effective approach to treating CRE.
Aminoglycoside antibiotics possess strong bactericidal properties and remain effective in treating MDR-GNB. However, their application is somewhat limited due to the side effect of nephrotoxicity. Generally, aminoglycosides are not the primary treatment option for severe infections. However, they can still be considered as a therapeutic alternative for combating CR-GNB when other options are unavailable. This is usually done in combination with other drugs such as β-lactams (75). For instance, studies have shown that the combination of imipenem and amikacin has a synergistic effect on CR-GNB both in vivo and in vitro (76–78). Amikacin exhibits lower resistance than gentamicin in most CRE strains (79). Many studies have supported the use of aminoglycosides in the treatment of CRE infections in critically ill patients before the introduction of novel BL-BLIs (80). Furthermore, gentamicin has demonstrated the potential to reduce mortality in K. pneumoniae sepsis caused by class A β-lactamase-producing enzymes, including KPC-3, SHV-11, and TEM-1 (81). A recent case report highlighted successful treatment of a patient with a CRKp intracranial infection after craniotomy using intrathecal injection of gentamicin and intravenous injection of amikacin, which displayed gentamicin susceptibility (82).
Plazomicin, a next-generation aminoglycoside antibiotic, has demonstrated a lower minimum inhibitory concentration compared to other aminoglycosides, making it a potential treatment option for infections caused by carbapenemase-producing, NDM-producing CRE (83). In a multicenter, randomized, open-label phase III trial that compared plazomicin with colistin (both in combination with imipenem) for the treatment of severe infections in CRE, plazomicin proved to be effective with a relatively low mortality and complication rate (84). Due to the nephrotoxicity associated with aminoglycoside antibiotics, they are generally not used in combination with colistin. To ensure optimal efficacy and minimal toxicity, appropriate dosage, administration, and therapeutic drug monitoring of the patient are essential when using aminoglycosides.
Infection control measures can be broadly classified into two types: horizontal and vertical strategies (85). Horizontal strategies are not pathogen-specific and aim to reduce infections caused by all pathogens. These strategies include standard precautions, such as hand hygiene, universal decolonization, and antimicrobial stewardship programs. On the other hand, vertical strategies are designed to target specific pathogens, involving carrier screening and contact precautions. The debate continues as to which of these two approaches is more effective. Nevertheless, implementing both strategies in parallel in the ICU setting may optimize infection control. Although monitoring the transmission route of CR-GNB is challenging, identifying high-risk groups is relatively simple. Implementing targeted prophylaxis and control measures for patients at high risk seems to be a promising approach. Furthermore, predictive or early warning models for CR-GNB infection are currently being explored and hold potential for application in the ICU.
Hand hygiene: Multi-drug resistant organisms (MDROs) have exhibited the ability to persist in hospital environments, such as floors, walls, beds, doorknobs, bedside tables, and equipment (86). Barnes et al. (87) developed a patient–patient transmission model within the ICU and compared the effects of hand hygiene and environmental cleanliness on MDRO acquisition rates; findings suggest that universal decolonization methods could eliminate colonization of MDRO Gram-positive bacteria. For example, patients in the ICU receiving mupirocin nasal injection have lower rates of MRSA BSIs compared to those undergoing chlorhexidine bathing (88). Extensively resistant MDROs, such as CRE, have shown poor response to chlorhexidine treatment, and current clinical evidence does not support the removal of patient colonization (89, 90). A meta-analysis indicated that ICU bathing with chlorhexidine significantly reduces A. baumannii colonization (91). Compliance with hand hygiene is widely considered as the foundation for preventing MDRO spread in ICUs. However, in hospitals with low compliance rates, proactive detection of CR-GNB has substantial benefits for patients when implemented with increased environmental cleanliness. Nevertheless, in high hand hygiene compliance environments, contact precautions and screening for CR-GNB colonization contribute little to preventing MDRO spread, especially for CR-GNB.
Antimicrobial Stewardship: Antimicrobial Stewardship (AMS) is a significant measure of importance as defined by the IDSA. It entails implementing coordinated interventions aimed at enhancing and evaluating proper utilization of antimicrobials. This is accomplished through facilitating optimal selection of antimicrobial regimens, determining appropriate dosage, therapy duration, and administration route. For patients in the ICU, the potential negative consequences of antimicrobial overuse are considered less perilous compared to the inadequate employment of restraints. Reports indicate a substantial proportion of ICU patients receiving excessive antimicrobial therapy, which includes treatment involving antimicrobials for suspected infections, utilization of overly broad-spectrum antibiotics, delayed initiation of timely antibiotic de-escalation and optimization, and prolonged duration of therapy (92, 93). The implementation of Antibiotic Stewardship Programs (ASP) within the ICU setting can potentially reduce the misuse of antimicrobials, shorten hospital stays, minimize costs, and decrease the emergence of drug resistance (94). Also, the study conducted by Khdour et al. (95) highlights the importance of establishing a well-structured antimicrobial stewardship team in the context of AMS. They found that timely feedback and prospective audits from the antibiotic stewardship team, within 48–72 h of antibiotic administration for ICU patients, had a positive impact on patient outcomes. Calcitoninogen as a biomarker in the ICU has been shown to reduce the use of antibiotics and mortality rates to some extent (96). However, further investigation is needed to determine the efficacy of calcitonin as a treatment indicator, and the cost of frequent testing must be balanced with potential savings from shorter antibiotic therapy. To address the growing issue of carbapenem resistance, experts emphasize the importance of implementing clear strategies to guide the appropriate use of carbapenem antibiotics (97).
Rapid Diagnostic Tests: Standard microbial identification techniques typically take 48–72 h, while optimizing antibiotic therapy within the first 6–12 h of infection is critical for treating life-threatening infections. Rapid diagnostic tests (RDTs) provide assistance to ASP by contributing to timely and effective antimicrobial therapy, potentially reducing mortality, hospitalization, and costs, as well as improving antimicrobial use and clinical and economic outcomes. Recently developed RDTs are able to provide identification results within 3 h of collection and 2.5 h after Gram staining (98). The RDTs provide an opportunity to rapidly optimize antimicrobial therapy, but have been shown to be combined with ASP to maximize translation into improved patient outcomes (99). Studies have identified genotyping and phenotyping of Escherichia coli, Klebsiella, etc. based on RDTs to predict susceptibility to β-lactams (ceftazidime, piperacillin-tazobactam, imipenem, and meropenem). RDTs can support downgrading decisions for the treatment of GNB infections (99).
Screening and prophylactic isolation: Patients in the ICU are particularly vulnerable to colonization or infection with MDRO either upon admission or during their hospital stay due to various risk factors. To reduce the spread of MDRO, it is crucial to implement proactive screening or isolate patients with high-risk factors (100). Although proactive testing methods differ among hospitals in different regions, they usually involve obtaining fecal/rectal swabs from patients upon admission or at regular intervals (weekly or bi-weekly). This practice applies to all patients or those at high risk (e.g., ICU patients, those with a history of previous colonization/infection), with a focus on identifying CRE. Results of a study revealed a high incidence of CRKp colonization and a likelihood of eventual CRKp infection in patients who carried Klebsiella pneumoniae (including CRKp or carbapenem antibiotic-susceptible Klebsiella pneumoniae) upon ICU admission (101). Proactive screening in high-risk units for CRE colonization or infection has also shown that CRE-positive patients, both neonatal and non-neonatal, exhibit different genotypes of carbapenemases. Notably, over 90% of CRE-positive neonates carry NDM. Isolating and placing these patients appropriately may help reduce the risk of CRE infection (102).
Additionally, the implementation of proactive testing and isolation strategies has shown a decrease in infections caused by CRAB and CRPA at a broader scale (103). Hospitals with limited isolation facilities have commonly resorted to a contact precautions approach in confining ICU patients to their own beds, similar to horizontal measures. Notably, no transmission of resistant organisms, such as Klebsiella pneumoniae, was detected in these cases (89). Implementing universal contact precautions, regardless of the specific pathogen, may also impede the spread of CR-GNB within the ICU.
The emergence and spread of CR-GNB are influenced by various factors. Identifying high-risk factors to determine ideal target populations for proactive testing or prophylactic contact helps optimize the allocation of limited resources. Depending on the purpose of the prediction model, different target populations can be selected for retrospective or prospective studies. The CR-GNB infection prediction model and the early warning model in Table 2 were designed to identify patients infected with or carrying CR-GNB, respectively. In order to prevent the spread of CR-GNB before culture results are available, modeling techniques have been employed to assist in the pre-isolation of potential carriers of CR-GNB or patients who are at a high risk of infection upon admission. There is also a type of predictive modeling that predicts infection at a particular site. BSI is a severe infection characterized by positive blood cultures in patients displaying symptoms of systemic infection. BSI often leads to unfavorable outcomes for patients in the ICU, including longer hospital stays and higher mortality rates (109, 110). While blood cultures serve as the gold standard and primary tool for diagnosing pathogens causing BSI, they are susceptible to delays in initiating effective treatment due to the time required (111). In addition to performing timely blood cultures or rapid diagnostic tests when BSI is suspected, several studies have explored the use of predictive modeling to construct early warning models for BSI. Several studies, as depicted in Table 3, have developed early warning models to identify BSI in vulnerable populations, such as children, the older adults, and individuals with immunodeficiencies. These models rely on risk factors or biomarkers to target high-risk populations and implement prophylactic measures, thereby reducing the occurrence of BSI and the associated mortality risk. While most of these models have demonstrated reliable predictive performance, unfortunately, only a limited number of studies have conducted validation in diverse healthcare settings. Consequently, the geographical applicability of these models may be constrained due to this lack of validation across multiple centers.
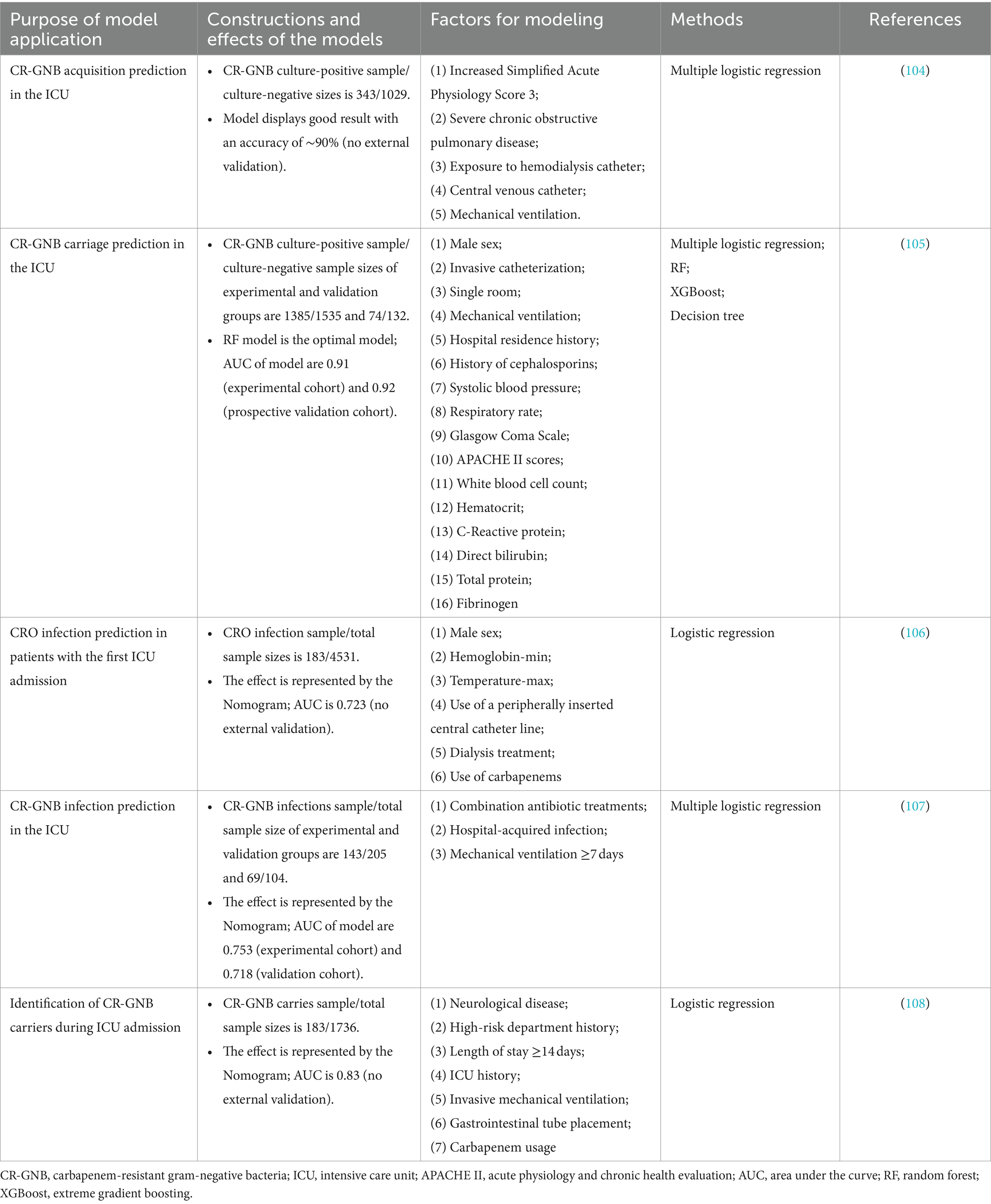
Table 2. CR-GNB carriage or infection prediction models in ICUs.
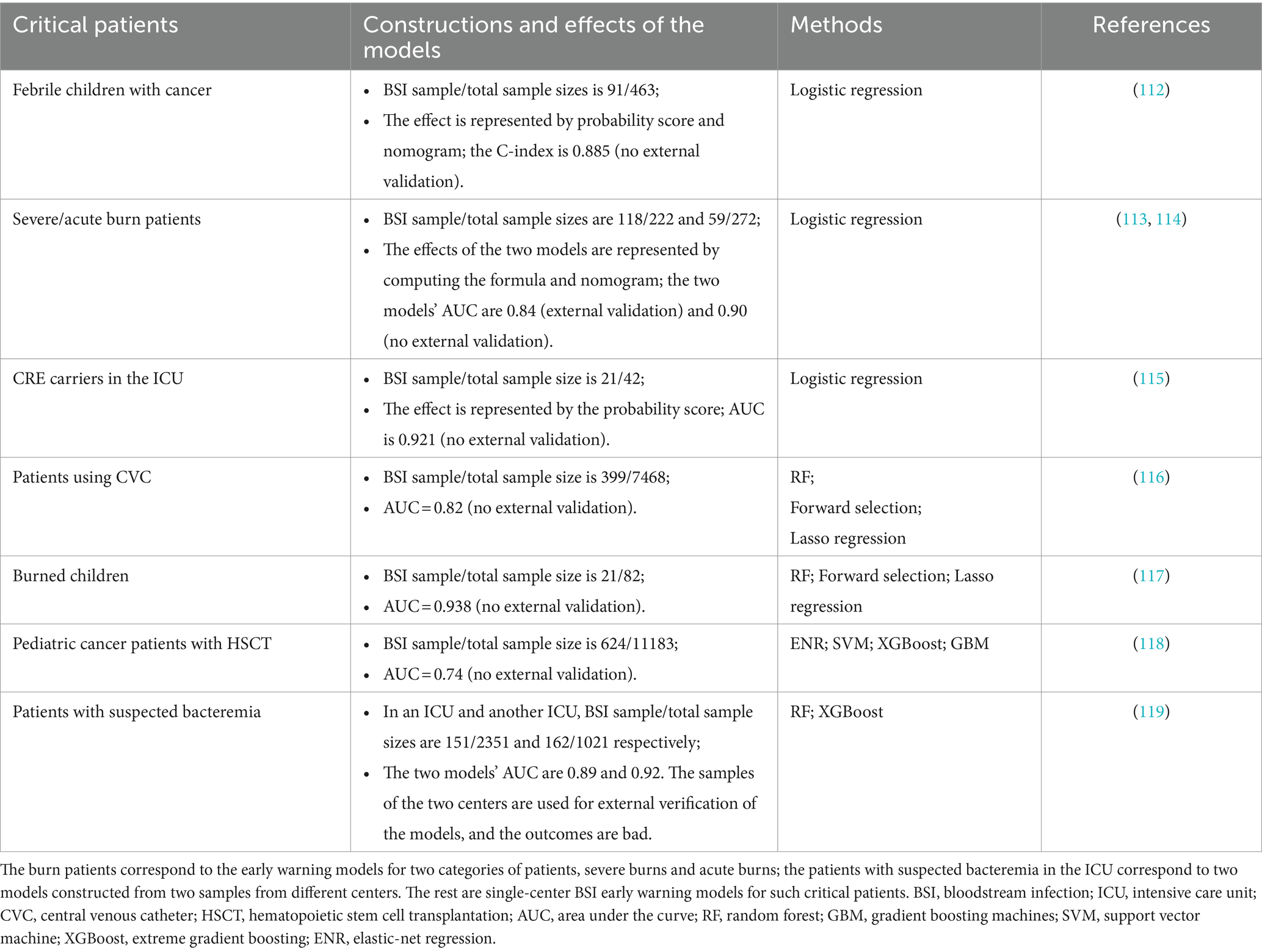
Table 3. BSI early warning models of critical patients.
The ICU is particularly susceptible to the emergence and spread of CR-GNB, necessitating the urgent strengthening and implementation of preventive measures within this high-risk setting. Currently, the range of antibiotics available for treating CR-GNB infections is limited. In the long term, it is crucial to prioritize the optimal utilization of existing antibiotics rather than relying solely on the development of new drugs. The presence of drug resistance genes in CR-GNB makes it difficult to promptly diagnose the pathogen and select suitable antibiotics. The high-density care provided in ICUs further increases the likelihood of cross-transmission of drug-resistant gene. This greatly affects the prognosis of ICU patients.
Having a thorough understanding of the common resistance genes found in CR-GNB and selecting appropriate antibiotics are crucial prerequisites for delaying the development of resistance. Pathogenic bacteria producing different genotypes of carbapenemases may have varying sensitivities to antibiotics. Selection of rational antibiotics based on enzyme genotypes not only controls the patient’s condition in time but also delays the development of drug resistance. Recent studies have highlighted the efficacy of newly approved BL-BLIs like ceftazidime/avibactam, meropenem/vaborbactam, and imipenem/relebactam as the first-line therapeutic options for most CRE and CRPA infections. However, these BL-BLIs have been found to be less effective in treating CRAB. For the treatment of CRAB and as an alternative when BL-BLIs are ineffective against KPC, NDM, VIM, IMP, and OXA-48 producing Escherichia coli, cefiderocol is recommended. While high-dose tigecycline has shown potential benefits in managing CR-GNB, conclusive evidence regarding its superiority over standard tigecycline dosing or the comparative effectiveness of combination therapy versus monotherapy remains elusive (120, 121). Monotherapy with cefiderocol has been shown to be more effective than combination therapy. Polymyxins, tigecycline, minocycline, and aminoglycosides are generally suggested as combination therapies or alternative treatments for CRE. Moreover, CR-GNB often exhibit a significant degree of co-resistance, limiting the range of effective therapeutic interventions. In cases where CR-GNB demonstrate resistance to key antibiotics such as fluoroquinolones, piperacillin, third-generation cephalosporins, and carbapenems, only colistin, aminoglycosides, tigecycline, fosfomycin, ceftazidime/avibactam, and ceftolozan/tazobactam are some of the few therapeutic options available (122).
The RDTs play a crucial role in ensuring that patients receive appropriate treatment in a timely manner, thereby decreasing the turnaround time for empirically prescribing broad-spectrum antibiotics. Additionally, RDTs aid in screening patients admitted to the ICU for carriage of CR-GNB, which is a vital preventive measure. The ICU requires strict infection control measures, such as hand hygiene, antimicrobial stewardship, proactive screening and prophylactic isolation, among other common practices. Another valuable tool for decision support is clinical predictive modeling, which can forecast the carriage and infection of drug-resistant bacteria. Currently, these models are typically built using multivariate logistic regression. However, the advancement of machine learning technology allows for the construction of infection-related models using large datasets and new algorithms, potentially improving their stability and effectiveness. The integration of machine learning algorithms with RDTs holds promise for enhancing the detection of predominant carbapenem resistance genes within clinical isolates of CR-GNB (123–125). This approach also enables the refinement of dosing regimens through the analysis of in vitro experimental data and pharmacodynamic considerations, thereby supporting the ASP of CR-GNB infections (126). It was discovered that most of the existing clinical prediction models based on machine learning for relevant infections lacked external validation, and those that were externally validated displayed poor performance. This aspect may also explain why prediction models for CR-GNB infection or carriage within the ICU are not widely implemented.
In order to improve patients’ prognosis and enhance their long-term quality of life, it is crucial to heighten vigilance against CR-GNB during ICU hospitalization. As well as administering antibiotics rationally based on the pathogen type and susceptibility, it is vital to swiftly identify the carbapenemase type in CR-GNB cases and take appropriate measures to prevent and control associated infections. We anticipate the emergence of more therapeutic strategies based on carbapenemase genotypes. We anticipate that future studies will delve further into treatment options based on genotypes of drug-resistant bacteria. Additionally, exploring CR-GNB-related models based on machine learning is expected to develop more effective infection control tools for ICU settings.
QL: Writing – original draft, Writing – review & editing, Conceptualization, Investigation, Software. XZ: Investigation, Writing – review & editing. RY: Conceptualization, Investigation, Writing – review & editing. XS: Conceptualization, Investigation, Writing – review & editing. GL: Investigation, Software, Writing – review & editing. CZ: Conceptualization, Investigation, Writing – review & editing. PL: Investigation, Writing – original draft. SL: Conceptualization, Software, Writing – review & editing. JX: Investigation, Software, Writing – review & editing. YY: Conceptualization, Software, Writing – original draft, Writing – review & editing, Supervision.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was supported by the Committee of Cadre Health, Sichuan Province, China (No.2023–220).
We acknowledge the support from Sichuan Academy of Medical Sciences & Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu Qingbaijiang District People’s Hospital, China Pharmaceutical University. And thank YY for his contribution to the paper.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Spellberg, B, Blaser, M, Guidos, RJ, Boucher, HW, Bradley, JS, Eisenstein, BI, et al. Combating antimicrobial resistance: policy recommendations to save lives. Clin Infect Dis. (2011) 52:S397–428. doi: 10.1093/cid/cir153
2. Tacconelli, E, Sifakis, F, Harbarth, S, Schrijver, R, van Mourik, M, Voss, A, et al. Surveillance for control of antimicrobial resistance. Lancet Infect Dis. (2018) 18:e99–e106. doi: 10.1016/s1473-3099(17)30485-1
3. Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. (2022) 399:629–55. doi: 10.1016/S0140-6736(21)02724-0
4. Willyard, C. The drug-resistant bacteria that pose the greatest health threats. Nature. (2017) 543:15. doi: 10.1038/nature.2017.21550
5. Vallés, J, and Ferrer, R. Bloodstream infection in the ICU. Infect Dis Clin N Am. (2009) 23:557–69. doi: 10.1016/j.idc.2009.04.005
6. Vincent, JL, Rello, J, Marshall, J, Silva, E, Anzueto, A, Martin, CD, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA. (2009) 302:2323–9. doi: 10.1001/jama.2009.1754
7. Akova, M. Epidemiology of antimicrobial resistance in bloodstream infections. Virulence. (2016) 7:252–66. doi: 10.1080/21505594.2016.1159366
8. Armand-Lefèvre, L, Angebault, C, Barbier, F, Hamelet, E, Defrance, G, Ruppé, E, et al. Emergence of imipenem-resistant gram-negative bacilli in intestinal flora of intensive care patients. Antimicrob Agents Chemother. (2013) 57:1488–95. doi: 10.1128/aac.01823-12
9. Woerther, PL, Lepeule, R, Burdet, C, Decousser, JW, Ruppé, É, and Barbier, F. Carbapenems and alternative β-lactams for the treatment of infections due to extended-spectrum β-lactamase-producing Enterobacteriaceae: what impact on intestinal colonisation resistance? Int J Antimicrob Agents. (2018) 52:762–70. doi: 10.1016/j.ijantimicag.2018.08.026
10. Munita, JM, and Arias, CA. Mechanisms of antibiotic resistance. Microbiol Spectr. (2016) 4. doi: 10.1128/microbiolspec.VMBF-0016-2015
11. Nordmann, P, and Poirel, L. Epidemiology and diagnostics of carbapenem Resistance in gram-negative bacteria. Clin Infect Dis. (2019) 69:S521–s528. doi: 10.1093/cid/ciz824
12. Bradford, PA. Extended-spectrum beta-lactamases in the 21st century: characterization, epidemiology, and detection of this important resistance threat. Clin Microbiol Rev. (2001) 14:933–51. doi: 10.1128/cmr.14.4.933-951.2001
13. Paterson, DL, and Bonomo, RA. Extended-spectrum beta-lactamases: a clinical update. Clin Microbiol Rev. (2005) 18:657–86. doi: 10.1128/cmr.18.4.657-686.2005
14. Pitout, JD, and Laupland, KB. Extended-spectrum beta-lactamase-producing Enterobacteriaceae: an emerging public-health concern. Lancet Infect Dis. (2008) 8:159–66. doi: 10.1016/s1473-3099(08)70041-0
15. Fernández, J, Piano, S, Bartoletti, M, and Wey, EQ. Management of bacterial and fungal infections in cirrhosis: the MDRO challenge. J Hepatol. (2021) 75:S101–s117. doi: 10.1016/j.jhep.2020.11.010
16. Rodríguez-Baño, J, Navarro, MD, Romero, L, Muniain, MA, de Cueto, M, Ríos, MJ, et al. Bacteremia due to extended-spectrum beta-lactamase-producing Escherichia coli in the CTX-M era: a new clinical challenge. Clin Infect Dis. (2006) 43:1407–14. doi: 10.1086/508877
17. Papp-Wallace, KM, Endimiani, A, Taracila, MA, and Bonomo, RA. Carbapenems: past, present, and future. Antimicrob Agents Chemother. (2011) 55:4943–60. doi: 10.1128/aac.00296-11
18. Nordmann, P, and Poirel, L. Strategies for identification of carbapenemase-producing Enterobacteriaceae. J Antimicrob Chemother. (2013) 68:487–9. doi: 10.1093/jac/dks426
19. Rodríguez-Martínez, JM, Poirel, L, and Nordmann, P. Molecular epidemiology and mechanisms of carbapenem resistance in Pseudomonas aeruginosa. Antimicrob Agents Chemother. (2009) 53:4783–8. doi: 10.1128/aac.00574-09
20. Kadri, SS. Key takeaways from the U.S. CDC's 2019 antibiotic Resistance threats report for frontline providers. Crit Care Med. (2020) 48:939–45. doi: 10.1097/ccm.0000000000004371
21. Prevention, U.S.C.F.D.C.A. (2021). Clinicians: Information about CRE [Online]. Available at: https://www.cdc.gov/hai/organisms/cre/cre-clinicians.html (Accessed February 25, 2021).
22. Grundmann, H, Glasner, C, Albiger, B, Aanensen, DM, Tomlinson, CT, Andrasević, AT, et al. Occurrence of carbapenemase-producing Klebsiella pneumoniae and Escherichia coli in the European survey of carbapenemase-producing Enterobacteriaceae (EuSCAPE): a prospective, multinational study. Lancet Infect Dis. (2017) 17:153–63. doi: 10.1016/s1473-3099(16)30257-2
23. Tawfick, MM, Alshareef, WA, Bendary, HA, Elmahalawy, H, and Abdulall, AK. The emergence of carbapenemase Bla(NDM) genotype among carbapenem-resistant Enterobacteriaceae isolates from Egyptian cancer patients. Eur J Clin Microbiol Infect Dis. (2020) 39:1251–9. doi: 10.1007/s10096-020-03839-2
24. Llaca-Díaz, JM, Mendoza-Olazarán, S, Camacho-Ortiz, A, Flores, S, and Garza-González, E. One-year surveillance of ESKAPE pathogens in an intensive care unit of Monterrey, Mexico. Chemotherapy. (2012) 58:475–81. doi: 10.1159/000346352
25. Garnacho-Montero, J, Amaya-Villar, R, Ferrándiz-Millón, C, Díaz-Martín, A, López-Sánchez, JM, and Gutiérrez-Pizarraya, A. Optimum treatment strategies for carbapenem-resistant Acinetobacter baumannii bacteremia. Expert Rev Anti-Infect Ther. (2015) 13:769–77. doi: 10.1586/14787210.2015.1032254
26. Zurawski, DV, Banerjee, J, Alamneh, YA, Shearer, JP, and Demons, ST. Skin and soft tissue models for Acinetobacter baumannii infection. Methods Mol Biol. (2019) 1946:271–87. doi: 10.1007/978-1-4939-9118-1_25
27. Rumbo, C, Gato, E, López, M, Ruiz de Alegría, C, Fernández-Cuenca, F, Martínez-Martínez, L, et al. Contribution of efflux pumps, porins, and β-lactamases to multidrug resistance in clinical isolates of Acinetobacter baumannii. Antimicrob Agents Chemother. (2013) 57:5247–57. doi: 10.1128/aac.00730-13
28. Vashist, J, Tiwari, V, Das, R, Kapil, A, and Rajeswari, MR. Analysis of penicillin-binding proteins (PBPs) in carbapenem resistant Acinetobacter baumannii. Indian J Med Res. (2011) 133:332–8.
29. Ramirez, MS, Bonomo, RA, and Tolmasky, ME. Carbapenemases: transforming Acinetobacter baumannii into a yet more dangerous menace. Biomol Ther. (2020) 10:720. doi: 10.3390/biom10050720
30. Rodríguez, CH, Nastro, M, and Famiglietti, A. Carbapenemases in Acinetobacter baumannii. Review of their dissemination in Latin America. Rev Argent Microbiol. (2018) 50:327–33. doi: 10.1016/j.ram.2017.10.006
31. Ribeiro, PC, Monteiro, AS, Marques, SG, Monteiro, SG, Monteiro-Neto, V, Coqueiro, MM, et al. Phenotypic and molecular detection of the Bla (KPC) gene in clinical isolates from inpatients at hospitals in São Luis, MA, Brazil. BMC Infect Dis. (2016) 16:737. doi: 10.1186/s12879-016-2072-3
32. Paterson, DL. The epidemiological profile of infections with multidrug-resistant Pseudomonas aeruginosa and Acinetobacter species. Clin Infect Dis. (2006) 43:S43–8. doi: 10.1086/504476
33. Bassetti, M, Vena, A, Croxatto, A, Righi, E, and Guery, B. How to manage Pseudomonas aeruginosa infections. Drugs Context. (2018) 7:212527:1–18. doi: 10.7573/dic.212527
34. Pachori, P, Gothalwal, R, and Gandhi, P. Emergence of antibiotic resistance Pseudomonas aeruginosa in intensive care unit; a critical review. Genes Dis. (2019) 6:109–19. doi: 10.1016/j.gendis.2019.04.001
35. Cai, B, Echols, R, Magee, G, Arjona Ferreira, JC, Morgan, G, Ariyasu, M, et al. Prevalence of carbapenem-resistant gram-negative infections in the United States predominated by Acinetobacter baumannii and Pseudomonas aeruginosa. Open Forum Infect Dis. (2017) 4:ofx176. doi: 10.1093/ofid/ofx176
36. Reyes, J, Komarow, L, Chen, L, Ge, L, Hanson, BM, Cober, E, et al. Global epidemiology and clinical outcomes of carbapenem-resistant Pseudomonas aeruginosa and associated carbapenemases (POP): a prospective cohort study. Lancet Microbe. (2023) 4:e159–70. doi: 10.1016/s2666-5247(22)00329-9
37. Livermore, DM. Multiple mechanisms of antimicrobial resistance in Pseudomonas aeruginosa: our worst nightmare? Clin Infect Dis. (2002) 34:634–40. doi: 10.1086/338782
38. Gill, CM, Aktaþ, E, Alfouzan, W, Bourassa, L, Brink, A, Burnham, CD, et al. The ERACE-PA global surveillance program: Ceftolozane/tazobactam and ceftazidime/avibactam in vitro activity against a global collection of carbapenem-resistant Pseudomonas aeruginosa. Eur J Clin Microbiol Infect Dis. (2021) 40:2533–41. doi: 10.1007/s10096-021-04308-0
39. Escandón-Vargas, K, Reyes, S, Gutiérrez, S, and Villegas, MV. The epidemiology of carbapenemases in Latin America and the Caribbean. Expert Rev Anti-Infect Ther. (2017) 15:277–97. doi: 10.1080/14787210.2017.1268918
40. Souza, GHA, Rossato, L, Brito, GT, Bet, G, and Simionatto, S. Carbapenem-resistant Pseudomonas aeruginosa strains: a worrying health problem in intensive care units. Rev Inst Med Trop São Paulo. (2021) 63:e71. doi: 10.1590/s1678-9946202163071
41. Tamma, PD, and Hsu, AJ. Defining the role of novel β-lactam agents that target carbapenem-resistant gram-negative organisms. J Pediatric Infect Dis Soc. (2019) 8:251–60. doi: 10.1093/jpids/piz002
42. Tumbarello, M, Trecarichi, EM, De Rosa, FG, Giannella, M, Giacobbe, DR, Bassetti, M, et al. Infections caused by KPC-producing Klebsiella pneumoniae: differences in therapy and mortality in a multicentre study. J Antimicrob Chemother. (2015) 70:2133–43. doi: 10.1093/jac/dkv086
43. Onorato, L, Di Caprio, G, Signoriello, S, and Coppola, N. Efficacy of ceftazidime/avibactam in monotherapy or combination therapy against carbapenem-resistant gram-negative bacteria: a meta-analysis. Int J Antimicrob Agents. (2019) 54:735–40. doi: 10.1016/j.ijantimicag.2019.08.025
44. Shields, RK, Nguyen, MH, Chen, L, Press, EG, Potoski, BA, Marini, RV, et al. Ceftazidime-avibactam is superior to other treatment regimens against carbapenem-resistant Klebsiella pneumoniae Bacteremia. Antimicrob Agents Chemother. (2017) 61:e00883-17. doi: 10.1128/aac.00883-17
45. Alraddadi, BM, Saeedi, M, Qutub, M, Alshukairi, A, Hassanien, A, and Wali, G. Efficacy of ceftazidime-avibactam in the treatment of infections due to carbapenem-resistant Enterobacteriaceae. BMC Infect Dis. (2019) 19:772. doi: 10.1186/s12879-019-4409-1
46. van Duin, D, Lok, JJ, Earley, M, Cober, E, Richter, SS, Perez, F, et al. Colistin versus ceftazidime-avibactam in the treatment of infections due to carbapenem-resistant Enterobacteriaceae. Clin Infect Dis. (2018) 66:163–71. doi: 10.1093/cid/cix783
47. Marshall, S, Hujer, AM, Rojas, LJ, Papp-Wallace, KM, Humphries, RM, Spellberg, B, et al. Can ceftazidime-avibactam and Aztreonam overcome β-lactam Resistance conferred by Metallo-β-lactamases in Enterobacteriaceae? Antimicrob Agents Chemother. (2017) 61:e02243-16. doi: 10.1128/aac.02243-16
48. Livermore, DM, and Mushtaq, S. Activity of biapenem (RPX2003) combined with the boronate β-lactamase inhibitor RPX7009 against carbapenem-resistant Enterobacteriaceae. J Antimicrob Chemother. (2013) 68:1825–31. doi: 10.1093/jac/dkt118
49. Wunderink, RG, Giamarellos-Bourboulis, EJ, Rahav, G, Mathers, AJ, Bassetti, M, Vazquez, J, et al. Effect and safety of Meropenem-Vaborbactam versus best-available therapy in patients with carbapenem-resistant Enterobacteriaceae infections: the TANGO II randomized clinical trial. Infect Dis Ther. (2018) 7:439–55. doi: 10.1007/s40121-018-0214-1
50. Mushtaq, S, Meunier, D, Vickers, A, Woodford, N, and Livermore, DM. Activity of imipenem/relebactam against Pseudomonas aeruginosa producing ESBLs and carbapenemases. J Antimicrob Chemother. (2021) 76:434–42. doi: 10.1093/jac/dkaa456
51. Yang, TY, Hsieh, YJ, Kao, LT, Liu, GH, Lian, SH, Wang, LC, et al. Activities of imipenem-relebactam combination against carbapenem-non-susceptible Enterobacteriaceae in Taiwan. J Microbiol Immunol Infect. (2022) 55:86–94. doi: 10.1016/j.jmii.2021.02.001
52. Motsch, J, Murta de Oliveira, C, Stus, V, Köksal, I, Lyulko, O, Boucher, HW, et al. RESTORE-IMI 1: a Multicenter, randomized, double-blind trial comparing efficacy and safety of imipenem/Relebactam vs colistin plus imipenem in patients with imipenem-non-susceptible bacterial infections. Clin Infect Dis. (2020) 70:1799–808. doi: 10.1093/cid/ciz530
53. Lee, SY, Gill, CM, and Nicolau, DP. Activity of novel β-lactam/β-lactamase inhibitor combinations against serine carbapenemase-producing carbapenem-resistant Pseudomonas aeruginosa. J Antimicrob Chemother. (2023) 78:2795–800. doi: 10.1093/jac/dkad225
54. Kollef, M, Dupont, H, Greenberg, DE, Viale, P, Echols, R, Yamano, Y, et al. Prospective role of cefiderocol in the management of carbapenem-resistant Acinetobacter baumannii infections: review of the evidence. Int J Antimicrob Agents. (2023) 62:106882. doi: 10.1016/j.ijantimicag.2023.106882
55. Oueslati, S, Bogaerts, P, Dortet, L, Bernabeu, S, Ben Lakhal, H, Longshaw, C, et al. In vitro activity of Cefiderocol and comparators against carbapenem-resistant gram-negative pathogens from France and Belgium. Antibiotics. (2022) 11:1352. doi: 10.3390/antibiotics11101352
56. Kaye, KS, Naas, T, Pogue, JM, and Rossolini, GM. Cefiderocol, a Siderophore cephalosporin, as a treatment option for infections caused by carbapenem-resistant Enterobacterales. Infect Dis Ther. (2023) 12:777–806. doi: 10.1007/s40121-023-00773-6
57. Simner, PJ, Mostafa, HH, Bergman, Y, Ante, M, Tekle, T, Adebayo, A, et al. Progressive development of Cefiderocol Resistance in Escherichia coli during therapy is associated with an increase in blaNDM-5 copy number and gene expression. Clin Infect Dis. (2022) 75:47–54. doi: 10.1093/cid/ciab888
58. Poirel, L, Sadek, M, Kusaksizoglu, A, and Nordmann, P. Co-resistance to ceftazidime-avibactam and cefiderocol in clinical isolates producing KPC variants. Eur J Clin Microbiol Infect Dis. (2022) 41:677–80. doi: 10.1007/s10096-021-04397-x
59. Jacob, AS, Chong, GL, Lagrou, K, Depypere, M, and Desmet, S. No in vitro activity of cefiderocol against OXA-427-producing Enterobacterales. J Antimicrob Chemother. (2021) 76:3317–8. doi: 10.1093/jac/dkab304
60. Falcone, M, Tiseo, G, Nicastro, M, Leonildi, A, Vecchione, A, Casella, C, et al. Cefiderocol as rescue therapy for Acinetobacter baumannii and other carbapenem-resistant gram-negative infections in intensive care unit patients. Clin Infect Dis. (2021) 72:2021–4. doi: 10.1093/cid/ciaa1410
61. Bassetti, M, Echols, R, Matsunaga, Y, Ariyasu, M, Doi, Y, Ferrer, R, et al. Efficacy and safety of cefiderocol or best available therapy for the treatment of serious infections caused by carbapenem-resistant gram-negative bacteria (CREDIBLE-CR): a randomised, open-label, multicentre, pathogen-focused, descriptive, phase 3 trial. Lancet Infect Dis. (2021) 21:226–40. doi: 10.1016/s1473-3099(20)30796-9
62. Nation, RL, Li, J, Cars, O, Couet, W, Dudley, MN, Kaye, KS, et al. Framework for optimisation of the clinical use of colistin and polymyxin B: the Prato polymyxin consensus. Lancet Infect Dis. (2015) 15:225–34. doi: 10.1016/s1473-3099(14)70850-3
63. Tamma, PD, Aitken, SL, Bonomo, RA, Mathers, AJ, van Duin, D, and Clancy, CJ. Infectious Diseases Society of America 2023 guidance on the treatment of Antimicrobial resistant gram-negative infections. Clin Infect Dis. (2023) 18:ciad428. doi: 10.1093/cid/ciad428
64. Cai, Y, Chai, D, Wang, R, Liang, B, and Bai, N. Colistin resistance of Acinetobacter baumannii: clinical reports, mechanisms and antimicrobial strategies. J Antimicrob Chemother. (2012) 67:1607–15. doi: 10.1093/jac/dks084
65. Tran, TB, Velkov, T, Nation, RL, Forrest, A, Tsuji, BT, Bergen, PJ, et al. Pharmacokinetics/pharmacodynamics of colistin and polymyxin B: are we there yet? Int J Antimicrob Agents. (2016) 48:592–7. doi: 10.1016/j.ijantimicag.2016.09.010
66. Hao, M, Yang, Y, Guo, Y, Wu, S, Hu, F, and Qin, X. Combination regimens with colistin Sulfate versus colistin Sulfate monotherapy in the treatment of infections caused by carbapenem-resistant gram-negative bacilli. Antibiotics. (2022) 11:1440. doi: 10.3390/antibiotics11101440
67. Paul, M, Daikos, GL, Durante-Mangoni, E, Yahav, D, Carmeli, Y, Benattar, YD, et al. Colistin alone versus colistin plus meropenem for treatment of severe infections caused by carbapenem-resistant gram-negative bacteria: an open-label, randomised controlled trial. Lancet Infect Dis. (2018) 18:391–400. doi: 10.1016/s1473-3099(18)30099-9
68. El Chakhtoura, NG, Saade, E, Iovleva, A, Yasmin, M, Wilson, B, Perez, F, et al. Therapies for multidrug resistant and extensively drug-resistant non-fermenting gram-negative bacteria causing nosocomial infections: a perilous journey toward 'molecularly targeted' therapy. Expert Rev Anti-Infect Ther. (2018) 16:89–110. doi: 10.1080/14787210.2018.1425139
69. Nelson, BC, Eiras, DP, Gomez-Simmonds, A, Loo, AS, Satlin, MJ, Jenkins, SG, et al. Clinical outcomes associated with polymyxin B dose in patients with bloodstream infections due to carbapenem-resistant gram-negative rods. Antimicrob Agents Chemother. (2015) 59:7000–6. doi: 10.1128/aac.00844-15
70. Dundar, D, Duymaz, Z, Genc, S, Er, DK, İrvem, A, and Kandemir, N. In-vitro activities of imipenem-colistin, imipenem-tigecycline, and tigecycline-colistin combinations against carbapenem-resistant Enterobacteriaceae. J Chemother. (2018) 30:342–7. doi: 10.1080/1120009x.2018.1516270
71. Pei, G, Mao, Y, and Sun, Y. In vitro activity of minocycline alone and in combination with cefoperazone-sulbactam against carbapenem-resistant Acinetobacter baumannii. Microb Drug Resist. (2012) 18:574–7. doi: 10.1089/mdr.2012.0076
72. Wu, H, Feng, H, He, L, Zhang, H, and Xu, P. In vitro activities of Tigecycline in combination with amikacin or colistin against carbapenem-resistant Acinetobacter baumannii. Appl Biochem Biotechnol. (2021) 193:3867–76. doi: 10.1007/s12010-021-03664-z
73. Ni, W, Han, Y, Liu, J, Wei, C, Zhao, J, Cui, J, et al. Tigecycline treatment for carbapenem-resistant Enterobacteriaceae infections: a systematic review and meta-analysis. Medicine. (2016) 95:e3126. doi: 10.1097/md.0000000000003126
74. Chen, HL, Jiang, Y, Li, MM, Sun, Y, Cao, JM, Zhou, C, et al. Acquisition of Tigecycline Resistance by carbapenem-resistant Klebsiella pneumoniae confers collateral hypersensitivity to aminoglycosides. Front Microbiol. (2021) 12:674502. doi: 10.3389/fmicb.2021.674502
75. Thy, M, Timsit, JF, and de Montmollin, E. Aminoglycosides for the treatment of severe infection due to resistant gram-negative pathogens. Antibiotics. (2023) 12:860. doi: 10.3390/antibiotics12050860
76. Hagihara, M, Kato, H, Yamashita, R, Soda, M, Watanabe, H, Sakanashi, D, et al. In vivo study assessed meropenem and amikacin combination therapy against carbapenem-resistant and carbapenemase-producing Enterobacteriaceae strains. J Infect Chemother. (2020) 26:1–7. doi: 10.1016/j.jiac.2019.10.014
77. Singkham-In, U, and Chatsuwan, T. In vitro activities of carbapenems in combination with amikacin, colistin, or fosfomycin against carbapenem-resistant Acinetobacter baumannii clinical isolates. Diagn Microbiol Infect Dis. (2018) 91:169–74. doi: 10.1016/j.diagmicrobio.2018.01.008
78. Wilhelm, CM, Nunes, LS, Martins, AF, and Barth, AL. In vitro antimicrobial activity of imipenem plus amikacin or polymyxin B against carbapenem-resistant Pseudomonas aeruginosa isolates. Diagn Microbiol Infect Dis. (2018) 92:152–4. doi: 10.1016/j.diagmicrobio.2018.05.004
79. Bremmer, DN, Clancy, CJ, Press, EG, Almaghrabi, R, Chen, L, Doi, Y, et al. KPC-producing Klebsiella pneumoniae strains that harbor AAC(6′)-Ib exhibit intermediate resistance to amikacin. Antimicrob Agents Chemother. (2014) 58:7597–600. doi: 10.1128/aac.03831-14
80. Zavascki, AP, Klee, BO, and Bulitta, JB. Aminoglycosides against carbapenem-resistant Enterobacteriaceae in the critically ill: the pitfalls of aminoglycoside susceptibility. Expert Rev Anti-Infect Ther. (2017) 15:519–26. doi: 10.1080/14787210.2017.1316193
81. Gonzalez-Padilla, M, Torre-Cisneros, J, Rivera-Espinar, F, Pontes-Moreno, A, López-Cerero, L, Pascual, A, et al. Gentamicin therapy for sepsis due to carbapenem-resistant and colistin-resistant Klebsiella pneumoniae. J Antimicrob Chemother. (2015) 70:905–13. doi: 10.1093/jac/dku432
82. Zhou, M, Liang, R, Liao, Q, Deng, P, Fan, W, and Li, C. Lumbar cistern drainage and gentamicin intrathecal injection in the treatment of carbapenem-resistant Klebsiella Pneumoniae intracranial infection after intracerebral Hemorrhage craniotomy: a case report. Infect Drug Resist. (2022) 15:6975–83. doi: 10.2147/idr.S378753
83. Martins, AF, Bail, L, Ito, CAS, da Silva Nogueira, K, Dalmolin, TV, Martins, AS, et al. Antimicrobial activity of plazomicin against Enterobacteriaceae-producing carbapenemases from 50 Brazilian medical centers. Diagn Microbiol Infect Dis. (2018) 90:228–32. doi: 10.1016/j.diagmicrobio.2017.11.004
84. Shaeer, KM, Zmarlicka, MT, Chahine, EB, Piccicacco, N, and Cho, JC. Plazomicin: a next-generation aminoglycoside. Pharmacotherapy. (2019) 39:77–93. doi: 10.1002/phar.2203
85. Landelle, C, Marimuthu, K, and Harbarth, S. Infection control measures to decrease the burden of antimicrobial resistance in the critical care setting. Curr Opin Crit Care. (2014) 20:499–506. doi: 10.1097/mcc.0000000000000126
86. Chaoui, L, Mhand, R, Mellouki, F, and Rhallabi, N. Contamination of the surfaces of a health care environment by multidrug-resistant (MDR) bacteria. Int J Microbiol. (2019) 2019:3236526–7. doi: 10.1155/2019/3236526
87. Barnes, SL, Morgan, DJ, Harris, AD, Carling, PC, and Thom, KA. Preventing the transmission of multidrug-resistant organisms: modeling the relative importance of hand hygiene and environmental cleaning interventions. Infect Control Hosp Epidemiol. (2014) 35:1156–62. doi: 10.1086/677632
88. Huang, SS, Septimus, E, Kleinman, K, Moody, J, Hickok, J, Avery, TR, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. (2013) 368:2255–65. doi: 10.1056/NEJMoa1207290
89. Gall, E, Long, A, and Hall, KK. Chlorhexidine bathing strategies for multidrug-resistant organisms: a summary of recent evidence. J Patient Saf. (2020) 16:S16–s22. doi: 10.1097/pts.0000000000000743
90. Ni, L, Zhang, Z, Shen, R, Liu, X, Li, X, Chen, B, et al. Disinfection strategies for carbapenem-resistant Klebsiella pneumoniae in a healthcare facility. Antibiotics. (2022) 11:736. doi: 10.3390/antibiotics11060736
91. Fan, CY, Lee, WT, Hsu, TC, Lee, CH, Wang, SP, Chen, WS, et al. Effect of chlorhexidine bathing on colonization or infection with Acinetobacter baumannii: a systematic review and meta-analysis. J Hosp Infect. (2019) 103:284–92. doi: 10.1016/j.jhin.2019.08.004
92. Barlam, TF, Cosgrove, SE, Abbo, LM, MacDougall, C, Schuetz, AN, Septimus, EJ, et al. Implementing an antibiotic stewardship program: guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. (2016) 62:e51–77. doi: 10.1093/cid/ciw118
93. Shappell, CN, Klompas, M, Ochoa, A, and Rhee, CCDC Prevention Epicenters Program. Likelihood of bacterial infection in patients treated with broad-Spectrum IV antibiotics in the emergency department. Crit Care Med. (2021) 49:e1144–50. doi: 10.1097/ccm.0000000000005090
94. Kernéis, S, and Lucet, JC. Controlling the diffusion of multidrug-resistant organisms in intensive care units. Semin Respir Crit Care Med. (2019) 40:558–68. doi: 10.1055/s-0039-1696980
95. Khdour, MR, Hallak, HO, Aldeyab, MA, Nasif, MA, Khalili, AM, Dallashi, AA, et al. Impact of antimicrobial stewardship programme on hospitalized patients at the intensive care unit: a prospective audit and feedback study. Br J Clin Pharmacol. (2018) 84:708–15. doi: 10.1111/bcp.13486
96. Campion, M, and Scully, G. Antibiotic use in the intensive care unit: optimization and de-escalation. J Intensive Care Med. (2018) 33:647–55. doi: 10.1177/0885066618762747
97. Bedos, JP, Daikos, G, Dodgson, AR, Pan, A, Petrosillo, N, Seifert, H, et al. Early identification and optimal management of carbapenem-resistant gram-negative infection. J Hosp Infect. (2021) 108:158–67. doi: 10.1016/j.jhin.2020.12.001
98. Pogue, JM, Heil, EL, Lephart, P, Johnson, JK, Mynatt, RP, Salimnia, H, et al. An antibiotic stewardship program blueprint for optimizing Verigene BC-GN within an institution: a tale of two cities. Antimicrob Agents Chemother. (2018) 62:e02538-17. doi: 10.1128/aac.02538-17
99. Beganovic, M, McCreary, EK, Mahoney, MV, Dionne, B, Green, DA, and Timbrook, TT. Interplay between rapid diagnostic tests and Antimicrobial stewardship programs among patients with bloodstream and other severe infections. J Appl Lab Med. (2019) 3:601–16. doi: 10.1373/jalm.2018.026450
100. Yoon, YK, Ryu, JM, Lee, MJ, Lee, SE, Yang, KS, Lee, CK, et al. Active surveillance at the time of hospital admission for multidrug-resistant microorganisms among patients who had recently been hospitalized at health care facilities. Am J Infect Control. (2019) 47:1188–93. doi: 10.1016/j.ajic.2019.04.008
101. Qin, X, Wu, S, Hao, M, Zhu, J, Ding, B, Yang, Y, et al. The colonization of carbapenem-resistant Klebsiella pneumoniae: epidemiology, Resistance mechanisms, and risk factors in patients admitted to intensive care units in China. J Infect Dis. (2020) 221:S206–s214. doi: 10.1093/infdis/jiz622
102. Yin, L, He, L, Miao, J, Yang, W, Wang, X, Ma, J, et al. Actively surveillance and appropriate patients placements' contact isolation dramatically decreased carbapenem-resistant Enterobacteriaceae infection and colonization in pediatric patients in China. J Hosp Infect. (2020) 105:486–94. doi: 10.1016/j.jhin.2020.03.031
103. Tomczyk, S, Zanichelli, V, Grayson, ML, Twyman, A, Abbas, M, Pires, D, et al. Control of carbapenem-resistant Enterobacteriaceae, Acinetobacter baumannii, and Pseudomonas aeruginosa in healthcare facilities: a systematic review and reanalysis of quasi-experimental studies. Clin Infect Dis. (2019) 68:873–84. doi: 10.1093/cid/ciy752
104. Dantas, LF, Dalmas, B, Andrade, RM, Hamacher, S, and Bozza, FA. Predicting acquisition of carbapenem-resistant gram-negative pathogens in intensive care units. J Hosp Infect. (2019) 103:121–7. doi: 10.1016/j.jhin.2019.04.013
105. Liang, Q, Zhao, Q, Xu, X, Zhou, Y, and Huang, M. Early prediction of carbapenem-resistant gram-negative bacterial carriage in intensive care units using machine learning. J Glob Antimicrob Resist. (2022) 29:225–31. doi: 10.1016/j.jgar.2022.03.019
106. Zhang, J, Liu, W, Shi, W, Cui, X, Liu, Y, Lu, Z, et al. A nomogram with six variables is useful to predict the risk of acquiring carbapenem-resistant microorganism infection in ICU patients. Front Cell Infect Microbiol. (2022) 12:852761. doi: 10.3389/fcimb.2022.852761
107. Liao, Q, Feng, Z, Lin, H, Zhou, Y, Lin, J, Zhuo, H, et al. Carbapenem-resistant gram-negative bacterial infection in intensive care unit patients: antibiotic resistance analysis and predictive model development. Front Cell Infect Microbiol. (2023) 13:1109418. doi: 10.3389/fcimb.2023.1109418
108. Dai, Y, Zhang, L, Pan, T, Shen, Z, Meng, T, Wu, J, et al. The ICU-CARB score: a novel clinical scoring system to predict carbapenem-resistant gram-negative bacteria carriage in critically ill patients upon ICU admission. Antimicrob Resist Infect Control. (2023) 12:118. doi: 10.1186/s13756-023-01326-9
109. Kollef, MH, Torres, A, Shorr, AF, Martin-Loeches, I, and Micek, ST. Nosocomial infection. Crit Care Med. (2021) 49:169–87. doi: 10.1097/ccm.0000000000004783
110. Timsit, JF, Ruppé, E, Barbier, F, Tabah, A, and Bassetti, M. Bloodstream infections in critically ill patients: an expert statement. Intensive Care Med. (2020) 46:266–84. doi: 10.1007/s00134-020-05950-6
111. Seymour, CW, Gesten, F, Prescott, HC, Friedrich, ME, Iwashyna, TJ, Phillips, GS, et al. Time to treatment and mortality during mandated emergency Care for Sepsis. N Engl J Med. (2017) 376:2235–44. doi: 10.1056/NEJMoa1703058
112. Esbenshade, AJ, Pentima, MC, Zhao, Z, Shintani, A, Esbenshade, JC, Simpson, ME, et al. Development and validation of a prediction model for diagnosing blood stream infections in febrile, non-neutropenic children with cancer. Pediatr Blood Cancer. (2015) 62:262–8. doi: 10.1002/pbc.25275
113. Walker, SAN, Cooper, A, Peragine, C, Elligsen, M, and Jeschke, MG. Development and validation of a screening tool for early identification of bloodstream infection in acute burn injury patients. Surgery. (2021) 170:525–31. doi: 10.1016/j.surg.2021.02.034
114. Wang, Y, Li, Q, Shu, Q, Liu, M, Li, N, Sui, W, et al. Clinical epidemiology and a novel predicting nomogram of central line associated bloodstream infection in burn patients. Epidemiol Infect. (2023) 151:e90. doi: 10.1017/s0950268823000766
115. Wang, Y, Lin, Q, Chen, Z, Hou, H, Shen, N, Wang, Z, et al. Construction of a risk prediction model for subsequent bloodstream infection in intestinal carriers of carbapenem-resistant Enterobacteriaceae: a retrospective study in Hematology department and intensive care unit. Infect Drug Resist. (2021) 14:815–24. doi: 10.2147/idr.S286401
116. Bonello, K, Emani, S, Sorensen, A, Shaw, L, Godsay, M, Delgado, M, et al. Prediction of impending central-line-associated bloodstream infections in hospitalized cardiac patients: development and testing of a machine-learning model. J Hosp Infect. (2022) 127:44–50. doi: 10.1016/j.jhin.2022.06.003
117. Tsurumi, A, Flaherty, PJ, Que, YA, Ryan, CM, Banerjee, A, Chakraborty, A, et al. A preventive tool for predicting bloodstream infections in children with burns. Shock. (2023) 59:393–9. doi: 10.1097/shk.0000000000002075
118. Sung, L, Corbin, C, Steinberg, E, Vettese, E, Campigotto, A, Lecce, L, et al. Development and utility assessment of a machine learning bloodstream infection classifier in pediatric patients receiving cancer treatments. BMC Cancer. (2020) 20:1103. doi: 10.1186/s12885-020-07618-2
119. Roimi, M, Neuberger, A, Shrot, A, Paul, M, Geffen, Y, and Bar-Lavie, Y. Early diagnosis of bloodstream infections in the intensive care unit using machine-learning algorithms. Intensive Care Med. (2020) 46:454–62. doi: 10.1007/s00134-019-05876-8
120. Chen, J, Lin, J, Weng, J, Ju, Y, and Li, Y. Clinical success of anti-infective combination therapy compare to monotherapy in patients with carbapenem-resistant Pseudomonas aeruginosa infection: a 10-years retrospective study. BMC Infect Dis. (2024) 24:248. doi: 10.1186/s12879-024-09060-2
121. Qu, J, Feng, C, Li, H, and Lv, X. Antibiotic strategies and clinical outcomes for patients with carbapenem-resistant gram-negative bacterial bloodstream infection. Int J Antimicrob Agents. (2021) 57:106284. doi: 10.1016/j.ijantimicag.2021.106284
122. Fritzenwanker, M, Imirzalioglu, C, Herold, S, Wagenlehner, FM, Zimmer, KP, and Chakraborty, T. Treatment options for carbapenem-resistant gram-negative infections. Dtsch Arztebl Int. (2018) 115:345–52. doi: 10.3238/arztebl.2018.0345
123. Miglietta, L, Moniri, A, Pennisi, I, Malpartida-Cardenas, K, Abbas, H, Hill-Cawthorne, K, et al. Coupling machine learning and high throughput multiplex digital PCR enables accurate detection of carbapenem-resistant genes in clinical isolates. Front Mol Biosci. (2021) 8:775299. doi: 10.3389/fmolb.2021.775299
124. Wang, J, Xia, C, Wu, Y, Tian, X, Zhang, K, and Wang, Z. Rapid detection of carbapenem-resistant Klebsiella pneumoniae using machine learning and MALDI-TOF MS platform. Infect Drug Resist. (2022) 15:3703–10. doi: 10.2147/idr.S367209
125. Yu, J, Lin, YT, Chen, WC, Tseng, KH, Lin, HH, Tien, N, et al. Direct prediction of carbapenem-resistant, carbapenemase-producing, and colistin-resistant Klebsiella pneumoniae isolates from routine MALDI-TOF mass spectra using machine learning and outcome evaluation. Int J Antimicrob Agents. (2023) 61:106799. doi: 10.1016/j.ijantimicag.2023.106799
126. Smith, NM, Lenhard, JR, Boissonneault, KR, Landersdorfer, CB, Bulitta, JB, Holden, PN, et al. Using machine learning to optimize antibiotic combinations: dosing strategies for meropenem and polymyxin B against carbapenem-resistant Acinetobacter baumannii. Clin Microbiol Infect. (2020) 26:1207–13. doi: 10.1016/j.cmi.2020.02.004
Keywords: ICU, CR-GNB, mechanism, genes, infection control strategies, predictive model
Citation: Li Q, Zhou X, Yang R, Shen X, Li G, Zhang C, Li P, Li S, Xie J and Yang Y (2024) Carbapenem-resistant Gram-negative bacteria (CR-GNB) in ICUs: resistance genes, therapeutics, and prevention – a comprehensive review. Front. Public Health. 12:1376513. doi: 10.3389/fpubh.2024.1376513
Edited by:
Marwan Osman, Yale University, United StatesReviewed by:
Eustachio Cuscianna, University of Bari Aldo Moro, ItalyCopyright © 2024 Li, Zhou, Yang, Shen, Li, Zhang, Li, Li, Xie and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yong Yang, eXl4cG93ZXJAMTYzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.