
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 10 June 2024
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1375773
This article is part of the Research Topic One Health and Preparedness for Disease X in the Tropics: Spillover Prevention, Surveillance, Vaccines and Drugs View all 10 articles
 Roméo Mèdéssè Togan1,2,3,4*†
Roméo Mèdéssè Togan1,2,3,4*† Amadou Ibra Diallo3Wendpouiré Ida Carine Zida-Compaoré1,2Mouhamadou Faly Ba3Arnold Junior Sadio1,2,4,5Rodion Yao Konu1,2,4,5Akila Wimima Bakoubayi1,2Martin Kouame Tchankoni1,2,4Gatibe Yendu-Suglpak Gnatou1,2Fifonsi Adjidossi Gbeasor-Komlanvi1,2,4Fatoumata Binetou Diongue3Jean Augustin Diégane Tine3
Amadou Ibra Diallo3Wendpouiré Ida Carine Zida-Compaoré1,2Mouhamadou Faly Ba3Arnold Junior Sadio1,2,4,5Rodion Yao Konu1,2,4,5Akila Wimima Bakoubayi1,2Martin Kouame Tchankoni1,2,4Gatibe Yendu-Suglpak Gnatou1,2Fifonsi Adjidossi Gbeasor-Komlanvi1,2,4Fatoumata Binetou Diongue3Jean Augustin Diégane Tine3 Adama Faye3Didier Koumavi Ekouévi1,2,4,5
Adama Faye3Didier Koumavi Ekouévi1,2,4,5Background: Health statistics on dengue are virtually non-existent, despite the fact that the virus is circulating in Togo. This study aimed to assess the knowledge, attitudes, and practices (KAP) of health professionals in the Kara health region.
Methods: A cross-sectional study was conducted from March to June 2022 among healthcare professionals who had worked in the Kara region of northern Togo were selected using an exhaustive recruitment method. Data were collected by trained resident doctors with a face-to-face interview using a standardized, pretested questionnaire based on the WHO 2009 dengue guide. Three multivariate regression models were utilized to investigate factors associated with knowledge, attitudes and, and practices.
Results: A total of 464 respondents (37.1% female), median age 35 years, interquartile range (29–43 years) were included. Only (3.0%) of the participants had received training on dengue fever diagnosis, treatment and prevention in the last 3 years, and 10.3% had dengue rapid diagnostic tests available at their hospital. Half of the respondents (49.1%) had good knowledge of dengue fever, compared with 30.0% who had positive attitudes. Of a total of 256 professionals who had encountered a case of dengue fever in their practice, only 24 (9.4%) had appropriate practices for diagnosing and treating dengue fever. In multivariate analysis, the healthcare professionals who had taken part in ongoing training on dengue fever were more likely to have adequate dengue diagnosis and treatment practice aOR = 8.1; CI 95% = [1.7–36.0].
Conclusion: Strengthening healthcare professionals' dengue-related skills through ongoing training and the provision of dengue diagnostic tests could help improve early detection practices and management of dengue fever in Togo.
Dengue fever, a viral infection transmitted by Aedes aegypti or Aedes Albopictus mosquito bites, is categorized among the notifiable neglected tropical diseases (1–3). It is part of the group of neglected tropical diseases that are notifiable (4, 5). Presently, it is endemic in numerous tropical and subtropical regions (6). Recent models estimate a significant rise in the global incidence of dengue fever, from 505,430 cases in 2000 to 5.2 million in 2019, with over half of the world's population being at risk in 2023 (7, 8). Currently, there is no specific treatment for dengue fever (9). Early diagnosis and treatment can reduce the mortality rate of DF patients from 20% to 1% or less (10). The role of healthcare professionals in implementing prevention, early detection, and early treatment strategies is crucial (11). Their knowledge, attitudes, and practices significantly impact the success of dengue prevention and control measures (12, 13). Studies have shown that enhancing healthcare professionals' understanding and practices of dengue is vital for early diagnosis and effective management, reducing complications, morbidity, and mortality (4, 14, 15). Most of these studies were conducted in Southeast Asian nations like Vietnam, Nepal, Thailand, and India (16–19).
In Togo, limited data exists on healthcare professionals' knowledge, attitudes, and practices (KAP) of healthcare professionals. A survey carried out in Lomé in 2020 revealed a low level of knowledge about dengue fever among healthcare professionals (20). Kara, Togo's second-largest cosmopolitan city, is near Burkina Faso, where dengue epidemics have occurred, raising concerns about disease spread (21–24). A 2022 study of 659 patients in 13 health facilities in the Kara region reported a dengue AgNS1 prevalence of 0.2% (95% CI: [0.1–0.3]). Similarly, the prevalence of IgM and IgG antibodies to dengue was 1.5% (IC95%: [0.8–2.8]) and 15.8% (IC95%: [13.2–18.8]) respectively (25). Dengue fever is therefore present in the Kara region. However, this potentially epidemic disease is under-reported and under-diagnosed throughout Togo because it is often confused with malaria.
In this context, it is vital to assess the CAPs for dengue among health professionals in the Kara region in order to identify gaps and contributing factors, an understanding of which would help in the development of strategies aimed at improving knowledge, changing attitudes and promoting appropriate practices. This study aimed to evaluate the knowledge, attitudes, and practices of healthcare professionals in the Kara health region, focusing on identifying associated factors.
The Kara region, a pivotal area in northern Togo, spans between latitudes 9°20′ and 10°05′ North and longitudes 0°55′ and 1°25′ East (Figure 1). It encompasses an area of 11,738 km2, accounting for nearly 21% of the country's total land area. The region's economy primarily revolves around agriculture, livestock breeding, and fishing, complemented by a robust informal sector. Two major rivers traverse the region, supporting a rich variety of vegetation. Furthermore, Kara is notable for its considerable trade and human interactions with neighboring countries, particularly Burkina Faso, which has recently confronted several dengue outbreaks (26). These factors collectively heighten the risk for the introduction and propagation of Aedes mosquito vectors in the Kara region.
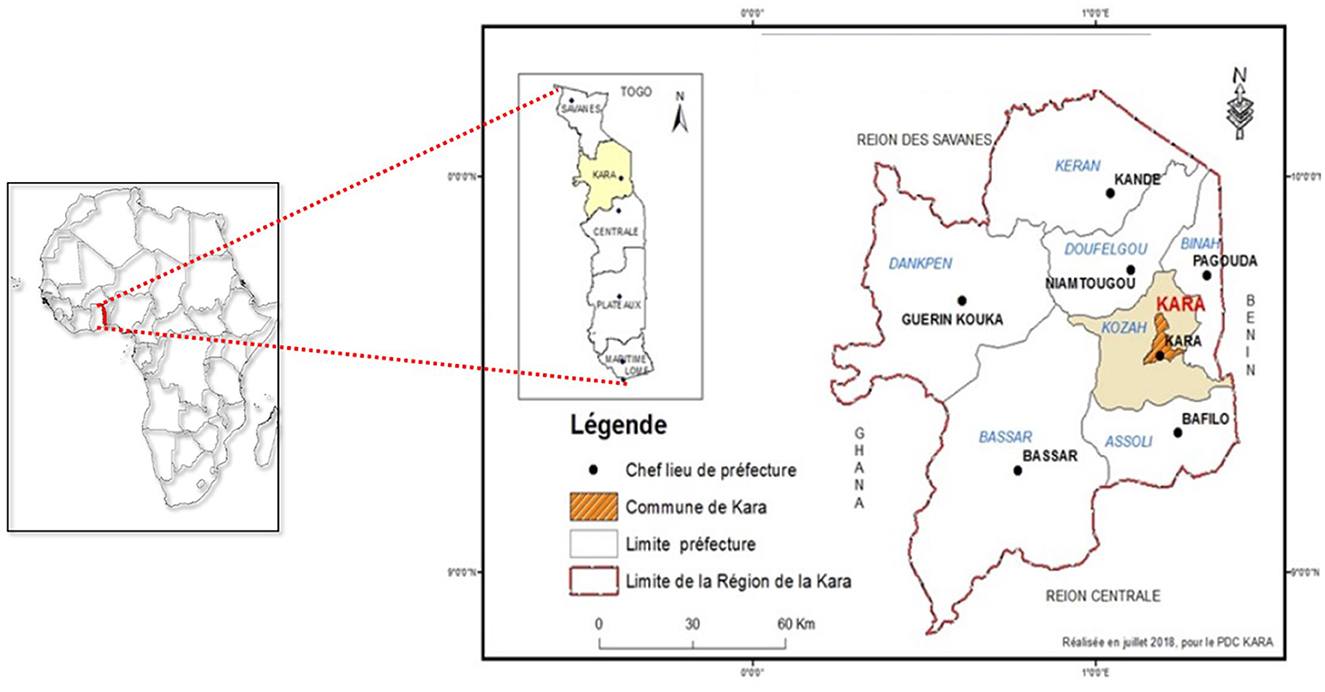
Figure 1. Map of the Kara health region (source Ministry of Health, Togo 2024).
From March to June 2022 a cross-sectional study was conducted to assess KAP and associated factors related to dengue fever among health professionals in the Kara region.
Care professionals were recruited in an exhaustive recruitment process. All healthcare professionals working in the health facilities of the Kara region involved in the diagnosis, treatment and management of cases of dengue fever, who had given their written consent and who were present during the data collection period were included. Healthcare professionals who were absent or on sick leave during the data collection period and those who refused to participate were excluded from the study. Based on the last study carried out in 2020 on the same subject which reported a proportion of good knowledge of 47.1% in Lomé of Togo, we assume a level of knowledge of 50 % on dengue, a margin of error of 5% and a confidence interval of 95%, the sample size was initially calculated as 384 (20).
Face-to-face interviews were conducted using a structured questionnaire including questions on professional socio-demographic characteristics and work environment, knowledge, attitudes, and diagnostic and treatment practices regarding dengue fever. The questionnaire, based on the 2009 WHO guidelines and a review of the literature on dengue fever, was pre-tested and validated before use (8, 19, 20, 27–30) (Supplementary File 1). All the researchers were residents training as public health specialists and medical students and had been trained by experts to ensure the quality of data. Each interview lasted between 10 and 15 min. Appointments were made with the heads of the health establishments. The interviewers made daily visits to the designated healthcare establishments to administer the questionnaire to available staff. Staff who were unavailable or absent during the first visit were rescheduled during the week. Those who missed three appointments were considered to have refused to take part in the study.
The information collected is as follows:
- Socio-demographic and professional characteristics
The collected data included details such as age, sex, marital status, occupation, years of professional experience, recent participation in dengue training (within the last 3 years), primary sources of dengue information, and the availability of rapid diagnostic tests for dengue.
- Knowledge of dengue
We assessed participants' knowledge of DF through 10 questions covering aspects such as the distribution of dengue in Togo, the causal agent, modes of transmission, factors favoring transmission, incubation period, clinical symptoms, differential diagnoses and prevention strategies. Each correct answer was worth 1 point. The knowledge score ranged from 0 to 10 points.
- Attitudes toward dengue fever
Four questions were asked to assess healthcare professionals' attitudes toward dengue fever, in particular their ability to recognize a suspected case, to prevent and diagnose dengue fever in the workplace, and to recognize people at risk of dengue infection. These questions offered three possible answers: “strongly agree” and “agree”, both scored 1, and “disagree”, scored 0. As a result, the total possible attitude score ranged from 0 to 4.
- Dengue diagnosis and treatment practices
The assessment of practices for diagnosing, treating and preventing dengue fever was limited to participants who had already experienced a case of dengue fever. Each correct answer was worth one point, giving a score from 0 to 3.
Participants who obtained a score ≥60% for knowledge, attitudes and practices were considered to have respectively good knowledge, positive attitudes and appropriate practices for treating dengue (25, 26).
The data analysis was performed using R© version 4.3.3 software. Quantitative variables were characterized using medians and interquartile ranges, while qualitative variables were described through absolute and relative frequencies. Univariable and multivariable logistic regressions were performed to assess the factors associated with knowledge, attitudes and practices regarding dengue fever among healthcare professionals. In the model building, characteristics that had a p < 0.25 in univariable analysis were considered for the full multivariable models, which were subsequently finalized using a stepwise backward elimination approach (p < 0.05). This procedure allowed the estimation of adjusted odds ratios (aORs) with 95% confidence intervals.
Initially, a total of 672 healthcare professionals were targeted for exhaustive recruitment. However, during the study period, 84 of them were absent at the time of our visits for reasons of leave, on-call duty or illness, 64 refused to give their consent to participate and 60 people were not available after three visits, leaving 464 healthcare professionals representing a participation rate of 69.0%. Figure 2 shows the flow chart of patients enrolled in the study.
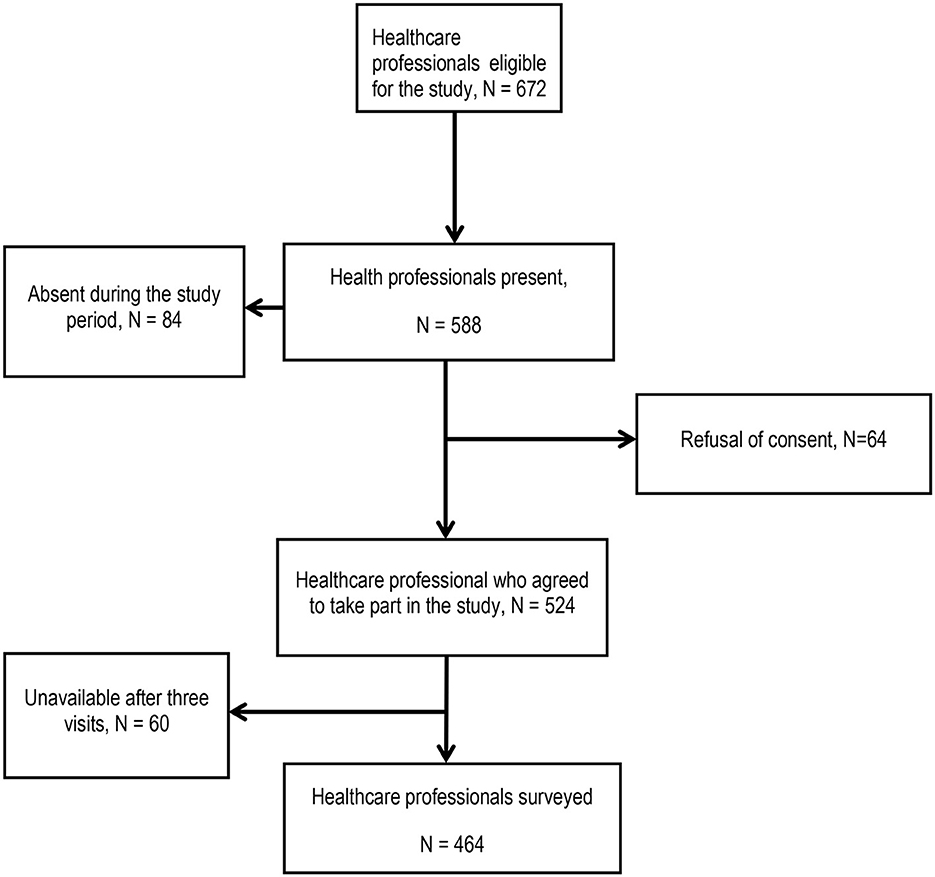
Figure 2. Participant flow chart.
A total of 464 healthcare professionals (HCPs) with a median age of 35 years (interquartile range (IQR) 29–43 years) were questioned, 37.1% of whom were women. The majority had attained a higher level of education (72.6%), resided in the Kozah district (53.4%) and were paramedics (65.5%). Median professional experience was 8 years (IIQ: 4–14 years). The main sources of information about dengue fever were initial training (34.5%) and workplace resources (23.5%). Only 3.0% (n = 14) had received dengue training in the last 3 years. In addition, 10.3% (n = 48) indicated that their health center had dengue diagnostic equipment (Table 1).
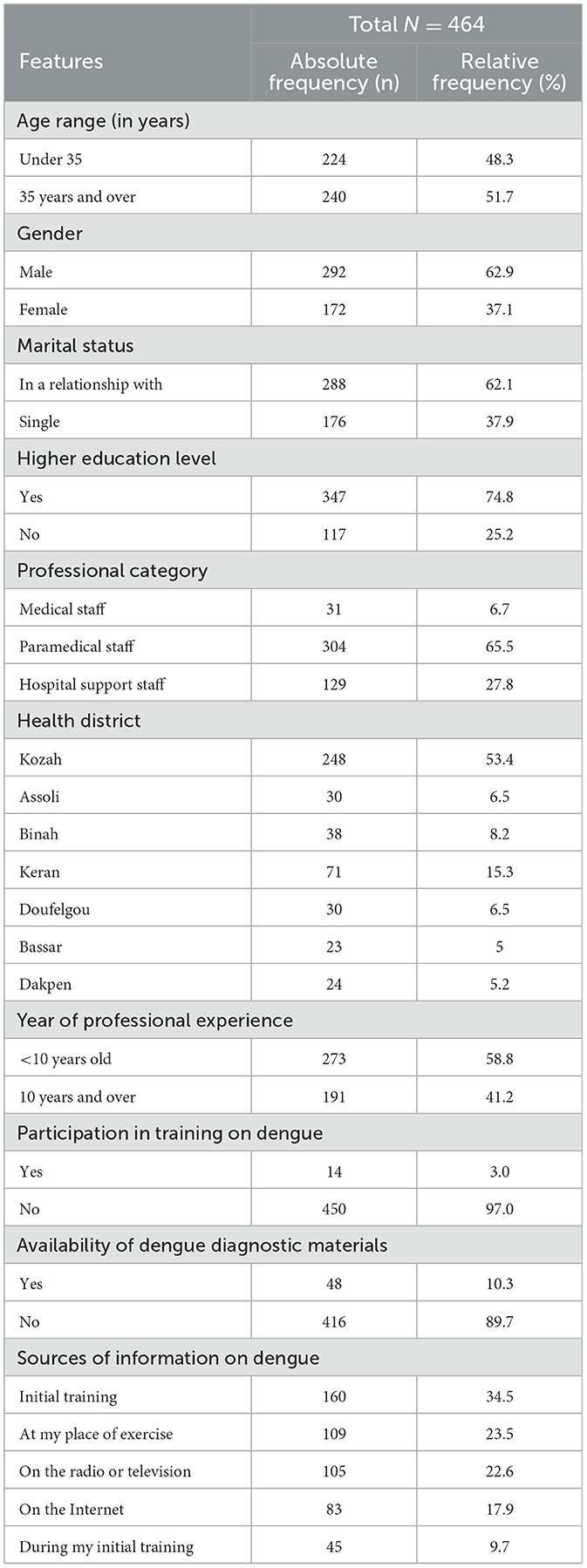
Table 1. Sociodemographic characteristics and organizational environment (N = 464).
A significant proportion of participants (70.5%) were aware of dengue fever. Regarding specific knowledge, 40.7% were familiar with the infectious agent of dengue, and 43.8% knew its incubation period. Additionally, 51.3% recognized the clinical signs, 62.1% knew the vector, and 69.6% were aware of preventive methods for dengue fever. The median knowledge score for dengue was 5.0 with an interquartile range of 2.5–7.5. Almost half of the participants, 49.1%, met the criteria for good knowledge of dengue, as defined by the 60% threshold (Table 2).
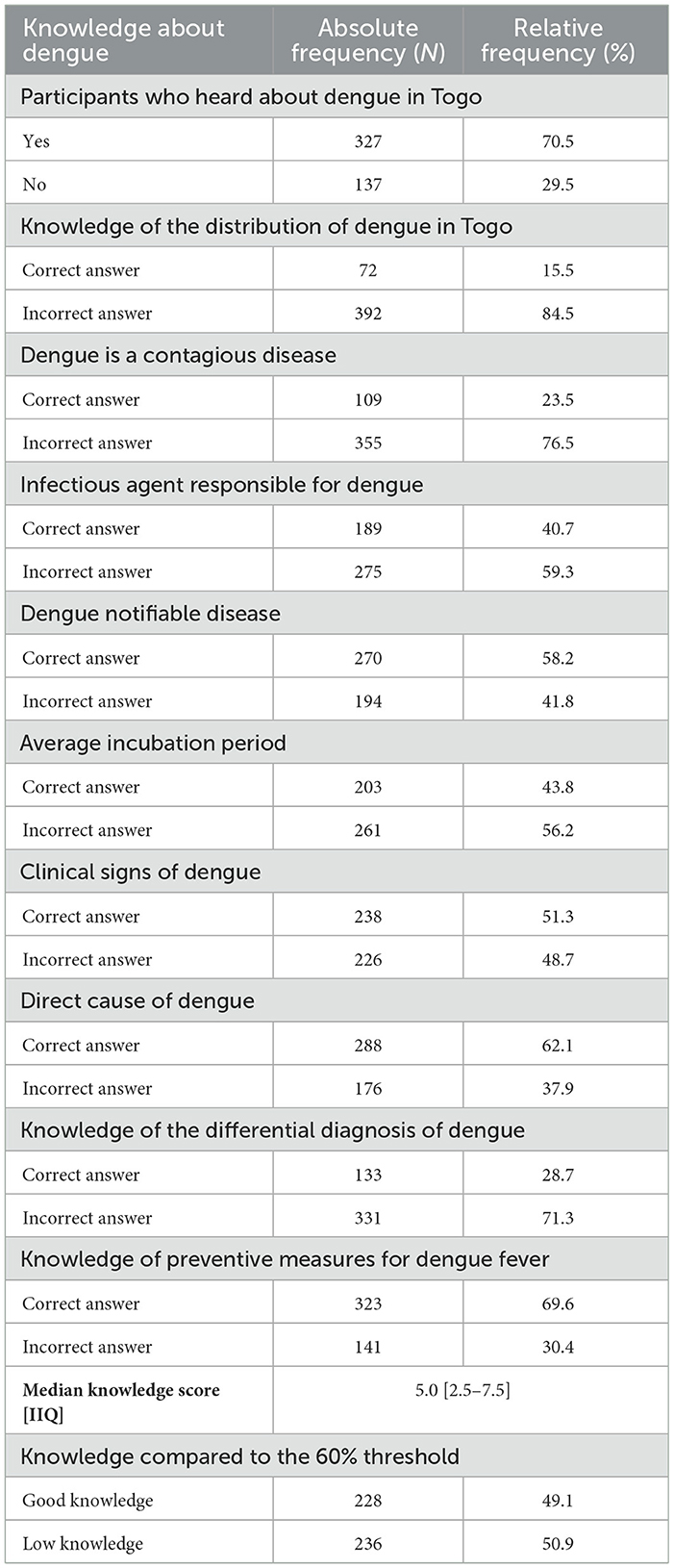
Table 2. Description of knowledge about dengue fever among participants (N = 464).
Regarding attitudes, 59.3% of participants strongly agreed they could recognize a suspected dengue case, 71.8% felt confident in implementing preventive measures, and 44.2% believed they could identify vulnerable targets for dengue. Conversely, only 55 participants (11.9%) expressed confidence in their ability to diagnose dengue fever. The median attitude score among respondents was 2.0, ranging from 0 to 4, with an interquartile range of 1.0–3.0. Overall, 30% of the participants were categorized as having a positive attitude toward dengue management, based on the 60% threshold for positive attitudes (Table 3).
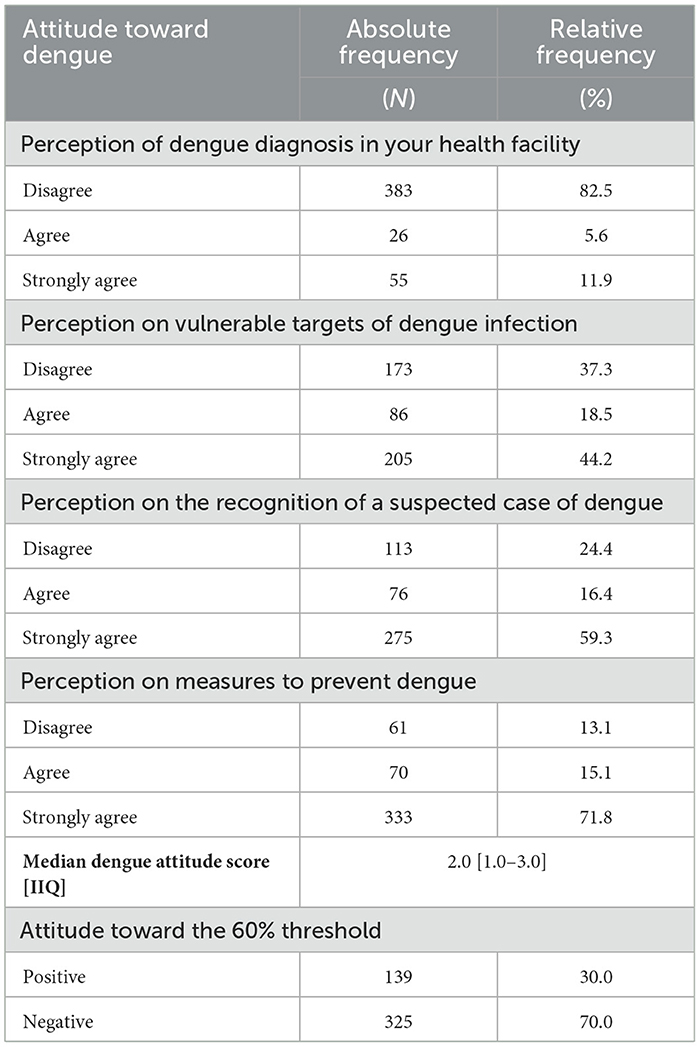
Table 3. Distribution of respondents according to attitudes toward dengue (N = 464).
In this study, 55.2% (256 participants) reported having encountered a suspected case of dengue fever. Among these, 64.1% (164 participants) demonstrated correct practices in diagnosing dengue, utilizing rapid diagnostic tests or serology. Furthermore, 9.4% (24 participants) had successfully managed a confirmed dengue case. The median score for dengue-related practices was 1.0, with an interquartile range (IQR) of 0.0 to 1.0, and scores ranging from a minimum of 0 to a maximum of 3. Only 9.4% (24 participants) were considered to have adequate diagnostic and treatment practices according to the 60% threshold (Table 4).
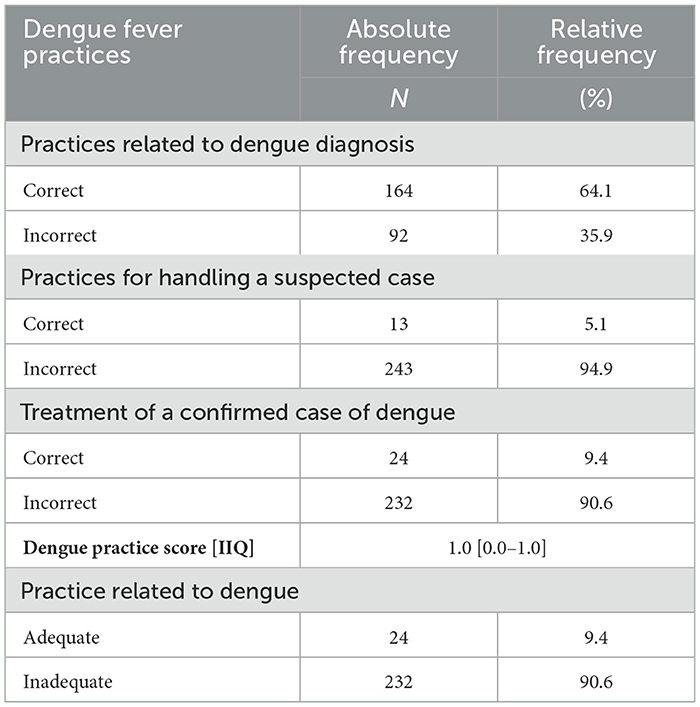
Table 4. Distribution of respondents according to dengue practices (N = 256).
Multivariate logistic regression analysis revealed several factors significantly associated with good knowledge of dengue. Male healthcare professionals were more likely to possess good knowledge compared to females (aOR = 1.94; CI 95% = [1.26–3.00]). Similarly, university-educated healthcare workers were more likely to have good knowledge than others (aOR = 1.92; CI 95% = [1.14–3.26]). Coupled healthcare professionals also had good knowledge of dengue (aOR = 2.18; CI 95% = [1.38–3] 47) compared to single ones; paramedics and medical staff were more likely to have good knowledge of dengue with aOR = 1.88 [1.13–3.16] and aOR = 6.53; CI 95% = [2.32–21.6] respectively. Furthermore, participants with more than 10 years of experience were 2.3 times less likely to have good knowledge than respondents with <10 years of professional experience. In addition, the availability of dengue diagnostic equipment was associated with good dengue-related knowledge aOR = 2.19; CI 95% [1.13–4.39].
About factors linked to positive attitudes, the availability of dengue diagnostic equipment was significantly associated with a positive attitude toward dengue (aOR = 2.94; IC 95% = [1.46–5.98]). medical staff had a positive attitude compared to other professional categories (aOR = 4.81; IC 95% = [1.86–12.8]). In addition, staff in the six other districts compared with those in the Kozah district had a better positive attitude to dengue fever (aOR = 2.8; CI 95% = [1.751–4.55]). Finally, healthcare professionals with good knowledge of dengue fever were more likely to have a positive attitude toward dengue compared with those with poor knowledge (aOR = 6.06; CI 95% = [3.71–10.2]).
In terms of factors associated with adequate dengue diagnosis and treatment practices, healthcare staff who had received dengue training in the last 3 years were more likely to have adequate dengue practice (aOR = 8.14; CI 95% = [1.72–36.0]). Information on factors associated with dengue CAP among health professionals in the Kara region is presented in Table 5.

Table 5. Factors associated with knowledge, attitudes and practices related to dengue.
This 2022 study in Kara, northern Togo, found that 49.1% of healthcare professionals had good knowledge of dengue fever, a figure similar to the 47.1% reported by Zida-compaoré et al. in 2021 in Lomé, southern Togo (20). These results suggest a relatively low level of dengue knowledge among Togolese healthcare workers, lower than figures reported elsewhere. For instance, Yusuf et al. in Ethiopia (2019) found 59.6% good knowledge (29), while Koonisetty in Turkey and Oche et al. in Nigeria (2021) reported 69.0% and 87.8%, respectively (19, 28). The limited knowledge in Togo may be attributed to factors like insufficient ongoing training for healthcare personnel and inadequate dengue awareness among both healthcare staff and the public community. Additionally, the infrequent encounter with dengue cases in Togo, as opposed to recent epidemics in other countries that have prompted increased learning, might contribute to this knowledge gap (31–33). The presence of dengue diagnostic equipment was significantly linked to better knowledge (aOR = 2.19; CI 95% [1.13–4.39]). However, only 10.3% of surveyed professionals reported having access to rapid dengue diagnostics. This scarcity could contribute to the underreporting of dengue, which has epidemic potential in Kara, as seen in national health statistics (34). Similar patterns of underreporting were observed in many non-endemic countries, possibly due to the low prevalence of reported cases in Africa despite conducive climatic conditions for dengue transmission (2, 35). Therefore, enhancing diagnostic access and affordability is crucial for the early detection of dengue in Togo.
In our study, only 30.0% of surveyed healthcare workers exhibited a positive attitude toward dengue fever, possibly reflecting the low proportion of good knowledge about dengue among participants. This correlation mirrors findings from a 2020 Malaysian study, where 46.8% of healthcare personnel had a positive attitude toward dengue, paralleling the 50.7% with good knowledge (36). Similarly, a 2019 Ethiopian study reported a 48% rate of positive attitudes among healthcare workers (29), whereas a 2021 Nigerian study by Oche et al. found a significantly higher rate of 93.2% positive attitudes, aligned with 87.8% good knowledge (28). These comparisons underscore the link between knowledge of dengue and positive attitudes toward its management among healthcare providers. Regarding factors influencing positive attitudes toward dengue fever, our multivariate analysis indicated that medical staff were more likely to exhibit positive attitudes than other professional groups (aOR = 4.81; CI 95% = [1.86–12.8]), a finding consistent with studies by Zida-Compaor et al. (20) in Togo, Oche et al. (28) in Nigeria, and Mohammed Yusuf and Abdurashid Ibrahim (29) in Ethiopia. This trend could be attributed to the frontline role of medical staff in managing dengue cases, fostering more positive attitudes toward the condition compared to other healthcare professionals. Moreover, the presence of dengue diagnostic tools was notably correlated with a favorable attitude, as indicated by an adjusted odds ratio (aOR) of 2.94 and a 95% confidence interval (CI) of [1.46–5.98]. This finding aligns with the work of Wong et al. (37) in Malaysia, who documented an aOR of 3.09 [1.27–7.5]. Such evidence highlights the critical role of ready access to rapid diagnostic tests at health facilities in fostering positive attitudes among healthcare workers toward dengue. Furthermore, healthcare professionals with comprehensive knowledge of dengue fever were significantly more inclined to demonstrate a positive attitude compared to their less-informed peers, with an aOR of 6.06; CI 95% = [3.71–10.2], affirming consistency with previous literature (19, 28, 29).
In our investigation, a mere 9.4% of healthcare professionals with experience handling dengue cases demonstrated sufficient dengue-related practices, a strikingly low figure relative to those reported in existing research. For comparison, Yusuf and colleagues identified that in Ethiopia in 2019, 48% of surveyed healthcare workers exhibited appropriate dengue-related practices based on a 60% cut-off (29). Similarly, using a 70% cut-off, Nikookar et al. reported that in Iran in 2023, an impressive 73.0% of participants had good practices (38). The scant proportion of adequate dengue practices in our study could primarily be attributed to the reported unavailability of dengue diagnostic equipment within the participants' health region. Furthermore, the observed deficiency in ongoing training, coupled with the lower scores in knowledge and attitudes, may contribute to the limited extent of adequate practices. Notably, healthcare professionals who had received training on dengue in the past 3 years were significantly more likely to engage in adequate dengue practices, as evidenced by an adjusted odds ratio (aOR) of 8.14 and a 95% confidence interval (CI) of [1.72–36.0]. The implications of our results highlight the critical need for targeted interventions to ensure the availability of dengue diagnostic equipment in health facilities in the Kara region. Secondly, it is essential to invest in comprehensive and ongoing training programs on dengue management. In addition, the promotion of multidisciplinary approaches that involve coordinated efforts in surveillance, vector control and community engagement can help mitigate the impact of dengue in the Kara region. Health professionals can play a key role in disseminating accurate information and promoting preventive behavior about dengue among the population (39).
Some potential limitations that could affect the accuracy and reliability of the results were identified and controlled before the study was carried out. These were selection bias, social desirability bias and statistical analysis limitation. With regard to selection bias, the study attempted to minimize these threats by including all health professionals working in all health facilities in the Kara region with exhaustive recruitment. Concerning social desirability bias, this was possible due to the face-to-face administration of the questionnaire. Participants might feel obliged to answer in an acceptable way or in accordance with the majority opinion in order to please, rather than answering honestly and objectively. To avoid this, the interviewers were trained to administer the questionnaire in order to reassure participants that their anonymity, confidentiality and freedom of expression would be preserved in accordance with the ethical and deontological rules of research. Similarly, the questionnaire was administered in an office with only the participant facing the interviewer, to avoid the influence of colleagues and limit social desirability bias. For the statistical analysis, we set a significance level of 0.05 based on the literature review and given that our study was exploratory in nature. We did not make any corrections in order to guarantee comparability with the data found in the literature, which used the same 0.05 threshold (16, 20, 28, 38). Despite these limitations, most of which were anticipated and corrected, our results were consistent with those of Ida et al. in Lomé and can therefore be generalized to Togo (20).
In conclusion, our study highlighted alarming gaps in dengue diagnosis and treatment practices among health professionals in the Kara region. This finding highlights the urgent need for targeted interventions to address the challenges of improving access to diagnostic equipment, strengthening training programs and improving public awareness. Our results also pave the way for other avenues of research into dengue, particularly within the community, with a view to advancing dengue prevention and control. This includes developing robust surveillance systems to monitor the incidence of dengue and identify early warning signs of dengue epidemics. In addition, efforts to monitor vectors need to be stepped up in order to track mosquito populations and the dynamics of disease transmission. Finally, socio-behavioral research is needed to understand the perceptions, knowledge and practices of communities in terms of dengue prevention and control in the Kara region.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Bioethics Committee for Health Research. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
RT: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. AD: Methodology, Supervision, Writing – review & editing. WZ-C: Investigation, Methodology, Validation, Writing – review & editing. MB: Methodology, Supervision, Visualization, Writing – review & editing. AS: Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – review & editing. RK: Investigation, Methodology, Writing – review & editing. AB: Investigation, Methodology, Writing – review & editing. MT: Data curation, Formal analysis, Supervision, Visualization, Writing – review & editing. GG: Investigation, Validation, Writing – review & editing. FG-K: Conceptualization, Project administration, Supervision, Validation, Writing – review & editing. FD: Supervision, Validation, Writing – review & editing. JT: Conceptualization, Supervision, Validation, Writing – review & editing. AF: Conceptualization, Methodology, Resources, Supervision, Validation, Visualization, Writing – review & editing. DE: Conceptualization, Methodology, Resources, Supervision, Validation, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors would like to thank all the teaching staff at the Institute of Health and Development and the WHO TDR program for research on diseases of poverty and for their significant involvement in the success of this study. We would also like to thank the Regional Health Director of Kara and all his staff, as well as the Head of the Public Health Department at the University of Lomé and all the public health residents who helped us carry out this study. Finally, I would like to thank the UEMOA (West African Economic and Monetary Union) commission for the excellence scholarship.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1375773/full#supplementary-material
1. Guzman MG, Harris E. Dengue. Lancet Lond Engl. (2015) 385:453–65. doi: 10.1016/S0140-6736(14)60572-9
2. Bhatt S, Gething PW, Brady OJ, Messina JP, Farlow AW, Moyes CL, et al. The global distribution and burden of dengue. Nature. (2013) 496:504–7. doi: 10.1038/nature12060
3. World Health Organization. Dengue in Africa: emergence of DENV-3, Côte d'Ivoire, 2008. Wkly Epidemiol Rec. (2009) 84:85–8.
4. World Health Organization (WHO). Integrating Neglected Tropical Diseases into Action for Global Health and Development: Fourth WHO Report On Neglected Tropical Diseases. Geneva: World Health Organization (2017). p. 272.
5. Calon J. The fight against neglected tropical diseases. Pharmaceut Sci. (2016) dumas-01485672.p 117.
6. Pilly E. ECN. Pilly 2020: Infectious and Tropical Diseases Prep. ECN, All Infectious Disease Items/Work From the College of Infectious and Tropical Diseases Scholars, CMIT; [coordinators of the 2020 edition Catherine Chirouze, Olivier Épaulard, Rozenn Le Berre]. 6th edition. Paris: Edition Alinéa Plus (2019).
7. World Health Organization. Dengue and Severe Dengue. (2023). Available online at: https://www.who.int/en/news-room/fact-sheets/detail/dengue-and-severe-dengue (accessed March 5, 2022).
8. World Health Organization. Dengue Guidelines for Diagnosis, Treatment, Prevention and Control : New Edition. Geneva: World Health Organization (2009). Available online at: https://apps.who.int/iris/handle/10665/44188 (accessed July 6, 2022).
9. World Health Organization. UNICEF/UNDP/World Bank/WHO Special Program for Research and Training in Tropical Diseases. Guide to the clinical management of dengue fever. Geneva: World Health Organization (2013). Available online at: https://apps.who.int/iris/handle/10665/85736 (accessed May 18, 2023).
10. Stephenson JR. The problem with dengue. Trans R Soc Trop Med Hyg. (2005) 99:643–6. doi: 10.1016/j.trstmh.2005.05.003
11. World Health Organization. Global Strategy for Dengue Prevention and Control 2012–2020. Geneva: World Health Organization (2012). Available online at: http://apps.who.int/iris/bitstream/10665/75303/1/9789241504034_eng.pdf (accessed February, 3, 2022).
12. Runge-Ranzinger S, Kroeger A, Olliaro P, McCall PJ, Sánchez Tejeda G, Lloyd LS, et al. Dengue contingency planning: from research to policy and practice. PLoS Negl Trop Dis. (2016) 10:e0004916. doi: 10.1371/journal.pntd.0004916
13. Wong LP, AbuBakar S, Chinna K. Community knowledge, health beliefs, practices and experiences related to dengue fever and its association with IgG seropositivity. PLoS Negl Trop Dis. (2014) 8:e2789. doi: 10.1371/journal.pntd.0002789
14. World Health Organization. Enhancing-Dengue-Diagnosis-and-Case-Management. (2023). Available online at: https://www.who.int/activities/enhancing-dengue-diagnosis-and-case-management (accessed April, 2023).
15. Teixeira M G, Barreto M L. Diagnosis and management of dengue. BMJ. (2009) 339:b4338 doi: 10.1136/bmj.b4338
16. Giang HTN, Sayed AM, Dang T, Iqtadar S, Tuan NM, Khiem NT, et al. Survey of knowledge, attitude and practice of healthcare professionals on dengue transmission, diagnosis and clinical classification. BMC Infect Dis. (2021) 21:1130. doi: 10.1186/s12879-021-06816-y
17. Syed M, Saleem T, Syeda UR, Habib M, Zahid R, Bashir A, et al. Knowledge, attitudes, and practices regarding dengue fever among adults of high and low socioeconomic groups. J Pak Med Assoc. (2010) 60:243–7.
18. Hamed M. Knowledge, attitude, and practices toward dengue fever among the public: a cross-sectional study in the Western region of Saudi Arabia. Front Public Health. (2024) 12:1327427. doi: 10.3389/fpubh.2024.1327427
19. Koonisetty KS, Aghamohammadi N, Urmi T, Yavaşoglu SI, Rahman MS, Nandy R, et al. Assessment of knowledge, attitudes, and practices regarding dengue among physicians: a web-based cross-sectional survey. Behav Sci Basel Switz 21 juill. (2021) 11:105. doi: 10.3390/bs11080105
20. Zida-Compaore WIC, Gbeasor-Komlanvi FA, Tchankoni MK, Sadio AJ, Konu YR, Agbonon A, et al. Knowledge and practices among healthcare workers regarding dengue in Togo. J Public Health Afr. (2023) 13:1937 doi: 10.4081/jphia.2022.1937
21. Ridde V, Agier I, Bonnet E, Carabali M, Dabiré KR, Fournet F, et al. Presence of three dengue serotypes in Ouagadougou (Burkina Faso): research and public health implications. Infect Dis Poverty. (2016) 5:23. doi: 10.1186/s40249-016-0120-2
22. Seogo PH, Bicaba BW, Yameogo I, Moussa G, Charlemangne KJ, Ouadraogo S, et al. Ampleur de la dengue dans la ville de Ouagadougou, Burkina-Faso, 2016. J Interv Epidemiol Public Health. (2021) 4:1. doi: 10.37432/jieph.supp.2021.4.3.03.1
23. Lee JS, Mogasale V, Lim JK, Ly S, Lee KS, Sorn S, et al. A multi-country study of the economic burden of dengue fever based on patient-specific field surveys in Burkina Faso, Kenya, and Cambodia. PLoS Negl Trop Dis 28 févr. (2019) 13:e0007164. doi: 10.1371/journal.pntd.0007164
24. Sawadogo S, Baguiya A, Yougbare F, Bicaba BW, Nebie K, Millogo T, et al. Seroprevalence and factors associated with IgG anti-DENV positivity in blood donors in Burkina Faso during the 2016 dengue outbreak and implications for blood supply. Transfus Med Oxf Engl. (2020) 30:37–45. doi: 10.1111/tme.12646
25. Zida-Compaore WIC, Gnatou GYS, Agoro S, Togan R, Tchankoni MK, Gbeasor-Komlanvi FA, et al. Séroprévalence de la dengue chez des patients fébriles dans la région de la Kara au Togo, (2022). Rev DÉpidémiologie Santé Publique sept. (2023) 71:102008. doi: 10.1016/j.respe.2023.102008
26. Presentation of the Kara region. Togo Politics. (2020). Available online at: https://togopolitique.org/presentation-de-la-region-kara (accessed April 15, 2022).
27. Essi MJ, Oudou N. The Knowledge, attitudes, practices survey in research. Health Sci Dis. (2013) 14:2.
28. Oche OM, Yahaya M, Oladigbolu RA, Ango JT, Okafoagu CN, Ezenwoko Z, et al. A cross-sectional survey of knowledge, attitude, and practices toward dengue fever among health workers in a tertiary health institution in Sokoto state, Nigeria. J Fam Med Prim Care. (2021) 10:3575–83. doi: 10.4103/jfmpc.jfmpc_327_21
29. Mohammed Yusuf A, Abdurashid Ibrahim N. Knowledge, attitude and practice towards dengue fever prevention and associated factors among public health sector health-care professionals: in Dire Dawa, eastern Ethiopia. Risk Manag Healthc Policy. (2019) 12:91–104. doi: 10.2147/RMHP.S195214
30. Kazaura M. Knowledge, attitude and practices about dengue fever among adults living in Pwani Region, Tanzania in 2019. Afr Health Sci. (2020) 20:1601–9. doi: 10.4314/ahs.v20i4.12
31. Gupta N, Murhekar MV, Poornima V, Saravanakumar V, Sukumaran K, Anandaselvasankar A, et al. Epidemiology of dengue in India: a systematic review and meta-analysis. PLoS Negl Trop Dis. (2019) 13:e0007760. doi: 10.1371/journal.pntd.0006618
32. Abdulaziz MM, Ibrahim A, Ado M, Ameh C, Umeokonkwo C, Sufyan MB, et al. Prevalence and factors associated with dengue fever among febrile patients attending secondary health facilities in Kano metropolis, Nigeria. Afr. J. Clin Exp Microbiol. (2020) 21:340–8. doi: 10.4314/ajcem.v21i4.11
33. Mahmood R, Benzadid MS, Weston S, Hossain A, Ahmed T, Mitra DK, et al. Dengue outbreak 2019: clinical and laboratory profiles of dengue virus infection in Dhaka city. Heliyon. (2021) 7:e07183. doi: 10.1016/j.heliyon.2021.e07183
34. Ministry of Health. Yearbook of Health Statistics, 2021. (2022). Available online at: https://sante.gouv.bj/assets/ressources/pdf/Annuaire%20statistiques%202021%20MS_VF.pdf (accessed 20 July, 2023).
35. Sharp TM, Moreira R, Soares MJ, Miguel da Costa L, Mann J, DeLorey M, et al. Underrecognition of dengue during 2013 epidemic in Luanda, Angola. Emerg Infect Dis. (2015) 21:1311–6. doi: 10.3201/eid2108.150368
36. Selvarajoo S, Liew JWK, Tan W, Lim XY, Refai WF, Zaki RA, et al. Knowledge, attitude and practice on dengue prevention and dengue seroprevalence in a dengue hotspot in Malaysia: a cross-sectional study. Sci Rep 12 juin. (2020) 10:9534. doi: 10.1038/s41598-020-66212-5
37. Wong LP, Shakir SMM, Atefi N, AbuBakar S. Factors affecting dengue prevention practices: nationwide survey of the Malaysian public. PLOS ONE. (2015) 10:e0122890. doi: 10.1371/journal.pone.0122890
38. Nikookar SH, Moosazadeh M, Fazeli-Dinan M, Zaim M, Sedaghat MM, Enayati A. Knowledge, attitude, and practice of healthcare workers regarding dengue fever in Mazandaran Province, northern Iran. Front Public Health 4 juill. (2023) 11:1129056. doi: 10.3389/fpubh.2023.1129056
Keywords: dengue, knowledge, attitudes, practices, health professional, Togo
Citation: Togan RM, Diallo AI, Zida-Compaoré WIC, Ba MF, Sadio AJ, Konu RY, Bakoubayi AW, Tchankoni MK, Gnatou GY-S, Gbeasor-Komlanvi FA, Diongue FB, Tine JAD, Faye A and Ekouévi DK (2024) Knowledge, attitudes, and practices of health care professionals regarding dengue fever: need for training and provision of diagnostic equipment in Togo in 2022, a cross-sectional study. Front. Public Health 12:1375773. doi: 10.3389/fpubh.2024.1375773
Received: 24 January 2024; Accepted: 21 May 2024;
Published: 10 June 2024.
Edited by:
Antonino Maniaci, Kore University of Enna, ItalyReviewed by:
Eustachio Cuscianna, University of Bari Aldo Moro, ItalyCopyright © 2024 Togan, Diallo, Zida-Compaoré, Ba, Sadio, Konu, Bakoubayi, Tchankoni, Gnatou, Gbeasor-Komlanvi, Diongue, Tine, Faye and Ekouévi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roméo Mèdéssè Togan, cm9jb2V1cjIwMDBAZ21haWwuY29t
†ORCID: Roméo Mèdéssè Togan orcid.org/0000-0003-2715-2031
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.