 Júlio A. Costa1*
Júlio A. Costa1* Susana Vale2,3Rita Cordovil4,5
Susana Vale2,3Rita Cordovil4,5 Luís P. Rodrigues6Vasco Cardoso1Rui Proença7Manuel Costa1Carlos Neto5
Luís P. Rodrigues6Vasco Cardoso1Rui Proença7Manuel Costa1Carlos Neto5 João Brito1José Guilherme1,8
João Brito1José Guilherme1,8 André Seabra1
André Seabra1- 1Portugal Football School, Portuguese Football Federation, FPF, Oeiras, Portugal
- 2Politécnico do Porto - Escola Superior de Educação, Porto, Portugal
- 3CIAFEL/ITR - Universidade do Porto, Porto, Portugal
- 4CIPER, Faculdade de Motricidade Humana, Universidade de Lisboa, Lisboa, Portugal
- 5Faculdade de Motricidade Humana, Universidade de Lisboa, Lisboa, Portugal
- 6Instituto Politécnico de Viana do Castelo, Escola Superior de Desporto e Lazer, SPRINT, Melgaço, Portugal
- 7School D. Carlos I, Sintra, Portugal
- 8Faculty of Sport, Centre of Research, Education, Innovation and Intervention in Sport, University of Porto, Porto, Portugal
Objective: The “Super Quinas” project evaluated the effectiveness of an intervention program to improve physical activity, aerobic fitness, sleep, and motor competence on children in primary school.
Methods: The experimental group (n = 19) enrolled in a 12-week intervention program (one more extra-curricular activity class of 60 min per week) compared to the CG (n = 19), all aged 9–10 years. Physical activity (PA) and sleep were measured by accelerometry, and aerobic fitness was measured by Children’s Yo-Yo test (YYIR1C) during the 1st week (PRE), the 6th week (DUR), and the 12th week (POST) of the intervention program. Motor Competence in PRE and POST intervention was also assessed by the Motor Competence Assessment (MCA) instrument. Heart rate (HR, assessed using HR monitors), and enjoyment level were recorded during all intervention program classes. A linear mixed model analysis (i.e., within-subject analyses) was performed.
Results: Comparing the EG and CG in DUR and POST, the EG spent ~18 min and ~ 34 min more time in moderate to vigorous physical activity (MVPA) per day (p < 0.001); had ~44 min and ~ 203 min less sedentary time per day (p < 0.001); performed more 44 and 128 m in the Children’s Yo-Yo test compared to CG (p < 0.001) and slept more 17 and 114 min per night (p < 0.001). In POST motor competence was significantly better (27%) in the EG compared to CG (p < 0.001). The %HRmax during the extra-curricular classes ranged between 65 and 81% (i.e., light to moderate intensities), and the enjoyment between fun and great fun.
Conclusion: Our findings suggest that adding one more extra-curricular activity class of 60 min per week for 12 weeks effectively increased the levels of physical activity, aerobic fitness, sleep duration, and motor competence in children aged 9–10 years.
1 Introduction
Childhood physical activity is a global concern, with declining levels observed in many countries around the world (1). Portugal is no exception and has struggled with the challenge of declining physical activity levels among its youth (2). For instance, in Portugal overweight and obesity levels remain cautious, with one in three children in school-age are overweight (2, 3). Research from the latest round of the WHO European Childhood Obesity Surveillance Initiative carried out in 2018–2020 indicates that 29% of children aged 7–9 years in the participating countries were found to be living with overweight (including obesity – according to WHO definitions) (2, 3). This trend has raised significant public health concerns due to its profound impact on health and well-being of children. Research has consistently indicated that insufficient physical activity during childhood is associated with a range of adverse health outcomes, including obesity, cardiovascular disease, and metabolic disorders (4–7).
Given the critical importance of developing active lifestyles early in life, school-based interventions have emerged as a promising avenue for promoting physical activity (PA) among school-age children (8–10). These interventions often adopt multifaceted approaches, targeting not only PA levels, but also health related parameters, such as sleep, aerobic fitness, and motor competence (4, 10). Such comprehensive strategies recognize that these aspects of health are intertwined and can mutually influence each other (11, 12).
Aerobic fitness is a robust indicator of cardiovascular health and overall fitness, while motor competence, encompassing skills such as stability, locomotor and manipulative tasks, underpins a child’s ability to effectively engage in physical activities (13, 14). In fact, the development of motor competence is most crucial during childhood and school years, contributing to a solid foundation for a lifelong physical health (14, 15). School is the only shared environment for the entire age cohort of children and adolescents, hence offering the most powerful context to promote motor competence and physical fitness (16).
Additionally, sleep is emerging as a critical factor in the PA-health relationship (17). Inadequate sleep patterns have been linked to reduced PA levels in children (18, 19) while increased PA has been associated with improved sleep duration and quality, creating a reciprocal relationship between these two essential health behaviors (20, 21). In fact, an adequate amount of good sleep duration and efficiency is important for optimal health and functioning throughout life. Normal ranges for sleep duration in childhood have been published from several parts of the world (19); however, this has mostly been assessed by parental reports rather than objective measures. Moreover, within any population there is a wide range of sleep duration, and the potential consequences of reduced sleep have received little attention in community-based studies of children (18, 19). It is also important to note that, an association between reduced sleep and obesity in children has been noted (22, 23). However, little research has focused on what role environmental or behavioral factors such as daily exercise might play in the relationship between PA and sleep duration, especially in Portugal.
By examining these interconnected health parameters, we intent to get a comprehensive understanding of the effectiveness of a school-based PA intervention program in promoting overall health and well-being.
Thus, the aims of this study were to assess a school-based PA intervention program conducted on children in primary school, and to assess the impact of this intervention program on PA levels, sleep patterns, aerobic fitness, and motor competence. We hypothesized that adding one additional extra-curricular activity class of 60 min per week (i.e., 120 min of physical education per week in total), over a period of three months (i.e., 12 weeks), would significantly improve PA levels, sleep patterns, aerobic fitness, and motor competence on children in primary school.
2 Materials and methods
2.1 Participants and study design
The participants of this study were part of the pilot project “Super Quinas,” a 12-week intervention program focusing to increase daily PA levels, sleep patterns, aerobic fitness, and motor competence on children in primary school.
This pilot project was conducted in 44 schools across the country (i.e., in Portugal), and involved over 1,600 school-age children (6 to 10 years old). It took place between January and March 2023 at several school facilities, during extra-curricular activities and led by physical education teachers.
All 1,600 children completed the MCA the PRE test in the 1st week and the POST test in the 12th week. Additionally, a sub-group of 38 children underwent more specific tests (i.e., PA, sleep, body composition and aerobic fitness) for a detailed analysis of the impact of this intervention project (Figure 1).
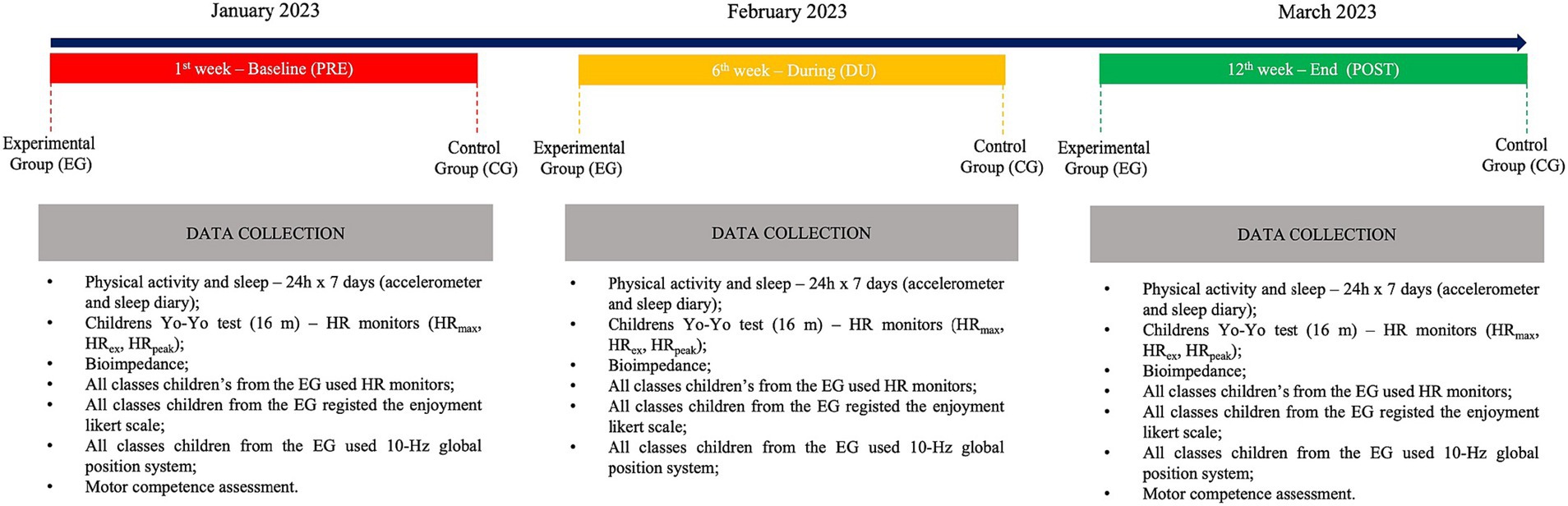
Figure 1. Study design of the “Super Quinas” physical intervention program in primary school.
The experimental group (EG) comprised 8 girls and 11 boys (n = 19), while the control group (CG) included 9 girls and 10 boys (n = 19), with a mean age of 9.1 years and belonging to the 4th grade primary school. This study was conducted in one of the 44 primary schools located in Sintra (Portugal), under the supervision of one member of the research group (J.A.C.) and one physical education teacher. The school was chosen for convenience due to location and facilitation of data collection and analysis. It was chosen children from the 4th grade due to the available and interested of their parents to participate in the sub-group analyses. The use of medication or the presence of a pathology or clinical condition in which PA is contraindicated were considered as exclusion criteria. No children were excluded by the exclusion criteria mentioned above.
Sample size calculations were performed a priori for within-subject analyses using the G*Power software version 3.1.9.6, considering an effect size 0.25, a statistical power of 0.95 at p < 0.05. A sample size of at least 14 in each group was required.
Therefore, the present study focused on the analysis of a specific subgroup of children.
The EG was enrolled in 12-week intervention program, which included 120 min of physical activities per week (comprising 60 min of their usual physical education lesson plus an additional 60 min from the “Super Quinas” intervention program). The CG maintained their regular schedule, involving a 60-min physical educational lesson, and 60-min of an extra-curricular activity class per week (i.e., languages, art, or other non-PA).
In the intervention (i.e., for the EG), each 60-min session was organized into three parts related to different individual and group pre-sports games as described below:
1. The first part (~20 min) primarily focused on individual work emphasizing general motor skills. The goal was to promote body awareness through tasks like running, jumping, balancing, crawling, and climbing. Additionally, it aimed to enhance the body and ball relationship, incorporating ball manipulations, dribbling different types of balls, controlling the ball, and throwing or kicking at fixed and moving targets;
2. The second part (~30 min) centered on collaborative work in pairs or small groups. It aimed to further promote body awareness and the relationship with the ball;
3. The third part (~10 min) concentrated on group activities with all the group and included pre-sports games and small sided games that combined various actions such as passing, reception, dribbling, shooting, offense, or defense.
Weekly PA, sleep and aerobic fitness were measured, in January (PRE; 1st week), in February (DUR; 6th week) and in March (POST; 12th week) for the EG and CG. Motor competence was measured in PRE and POST, for the EG and CG. Heart rate (HR), external load, and sessions enjoyment level (1, no fun to 5, great fun) were recorded in all extra-curricular activity classes (i.e., 12 sessions in total) of the intervention program for the EG.
Prior to data collection, participants and their parents/legal guardians were informed about the study details (purpose, duration, type of intervention, risks and benefits). In fact, it is important to mention that in case of any injury or unexpected outcomes/results, the parents/legal guardians would be informed to guide their children to their respective family doctors/pediatricians, as indicated in the approved ethical document. They were also informed that they could withdraw from the study at any time, without any consequences. No child dropped out of the study. Written informed consent was obtained from the participants’ legal representatives and verbal assent was obtained from the children. The study was approved by the Ethical Committee of the Portugal Football School, Portuguese Football Federation (nr. CEPFS 17.2022).
2.2 Variables and measuring instruments
2.2.1 Body composition
Body composition was assessed using an InBody 270 bio-impedance scale with an 8 Electrode Tetrapolar Electrode System with frequencies of 20 and 100 kHz. This allowed for the measurement of weight, body fat mass (%) and body mass index (BMI) (24). A portable stadiometer (Seca 213, Germany) was used to measure height. All measurements were conducted with participants lightly dressed (wearing only underwear and t-shirt) and barefoot.
2.2.2 Physical activity and sleep
To estimate daily PA a tri-axial accelerometer (ActiGraph, model GT3X, Acticorp Co., Pensacola, FL, United States) was used at baseline (i.e., PRE), at the middle of the intervention program (i.e., DUR) and at the end of the study (i.e., POST). Participants wore the accelerometer during 7 consecutive days (i.e., Monday to Sunday) for each moment (i.e., at PRE, DUR, and POST).
A flexible elastic belt was securely fastened around the waist of each child. Children were asked to wear the accelerometer continuously for 24-h, with removal only during bathing, water-based activities, and in exceptional cases such as engaging in contact sports such as martial arts, where there was a risk of injury.
In the data analysis phase, records of PA performed on at least 4 days were considered, comprising 3 days during the week and 1 day over the weekend. Valid records needed a minimum of 8 h of recording per day (25, 26). Wear time validation was calculated using Troiano defaults (27, 28).
Accelerometer data files were collected according to the, respectively, cut point chosen to record the spontaneous and intermittent activities of children more accurately (25, 26). Evenson Children cut-points (25), validated cut-points recommended for children, were used to estimate time spent in sedentary, light, moderate, and vigorous intensity activity in children: light (101 to ≥2,295 counts per min), moderate (≥ 2,296 counts per min), and vigorous intensity (≥ 4,012 counts per min) PA (26, 29–31).
Sleep monitoring was assessed using the same accelerometers employed for PA measurements. However, during night sleep, participants were asked to wear the accelerometers on their non-dominant wrist (32, 33). Sleep variables were recorded every night over 7 consecutive days for each assessment point (i.e., at PRE, DUR and POST). Data was analyzed with the same software, using the Sadeh’s algorithm (34, 35). Sleep indices included sleep duration (amount of sleep in hours) and sleep efficiency (percentage of time in bed that was spent asleep) (35), which were analyzed according to the National Sleep Foundation (36, 37). A sleep duration <8 h was considered an indicator of inappropriate sleep duration, and a sleep efficiency ≤65% was considered an inappropriate sleep quality for children (36, 37).
2.2.3 Aerobic fitness
The Children’s Yo-Yo test (YYIR1C) was measured during PRE (1st week), DUR (6th week), and POST (12th week) for the EG and CG. YYIR1C was developed for accounting for differences in running economy in children and has recently been reported to be a reliable and valid (construct validity) test for children’s of either sex (38, 39). This test uses the same acoustic progression, but shorter distance compared to Yo-Yo intermittent recovery test in its level 1 (YYIR1) version (38–40). Indeed, in the YYIR1C the children shuttle-run between two lines positioned 16 m apart, instead of 20 m, and walk over 4 m (instead of 5 m) in the 10s active recovery period (41, 42).
YYIR1C was performed at the school gym at the same time of the day, to account for circadian variation in human performance. All children were acquainted with the assessment procedures during dedicated physical education lessons in the week preceding the study.
2.2.4 Motor competence assessment
Motor competence was assessed using the MCA test battery (15, 43), which comprises six tests, two for each component of motor competence: stability (lateral jumps and shifting platforms), locomotor (standing long jump and 10 m shuttle run), and manipulative (ball kicking velocity and ball throwing velocity). All tests are quantitative (product oriented), without a marked developmental (age) ceiling effect, and based on the child’s feasible execution of motor tasks.
In this study, testing conditions were arranged prior to beginning assessments, and children performed all tests in small groups (usually about five children per task). All participants completed a 10-min general and standardized warm-up before beginning the tests (14, 15). Examiners were previously trained in administering all tests, and the following requirements were standardized: (a) a proficient demonstration of each test technique was provided along with a verbal explanation; (b) every participant experimented with each task before the actual test administration; (c) the instructions emphasized that children should try to perform the task at their maximum capacity (e.g., “as fast as possible” for the stability tests and 4 ×10 shuttle run; “as far as possible” for the standing long jump; and “as hard as possible” for the manipulative tests); and (d) motivational, but no verbal feedback was provided (14, 15).
Results on each test of the three subscales were transformed into a percentile value by age and sex, according to the MCA norms (15). MCA subscales scores resulted from the average of the percentile values of the two constitutive tests, and the Total MCA score was calculated by the average of the subscales’ scores. This means that al MCA scores (tests, susbscales, and total MCA) represent percentile positions according to age and sex.
2.2.5 Heart rate
HR data during extra-curricular activity classes for the EG was recorded in real time at 5 s intervals by short-range radio telemetry (Firstbeat Sports, Jyvaskyla, Finland). The monitors were attached to the children using an adjustable elastic chest strap. Data was transferred to a computer using the corporative software Firstbeat Sports Server version 4.7.3.1. HRmax, which was considered as the highest value reached during the YYIR1C, served as the standard to establish the intensity zone of moderate to very hard at ≥70% HRmax (44). The software quantified the time spent at this intensity zone (i.e., ≥ 70% HRmax) during physical education sessions, and data was presented as the percentage relative to the total training time. The software also calculated the percentage relative to the individual HRmax (%HRmax) for the intensity zone as mentioned previously. The HR recording was not interrupted during the exercise transitions because the teacher organized the physical education sessions so that these breaks were not longer than 1 min.
2.2.6 External load
Children used 10-Hz global position system (GPS) pods during extra-curricular activity classes (STATSports Apex, Northern Ireland) (45). In order to avoid inter-unit error, each child wore the same GPS unit throughout the data collection (46). Data were subsequently downloaded and adjusted to extra-curricular activity class exposure using corporate software (STATSports Apex, Northern Ireland). Total distance was used as an external load variable (47).
2.2.7 Enjoyment level
Activities enjoyment was ascertained for the EG at the end of all extra-curricular activity class through a 5-points Likert scale (1, nothing fun; 2, little fun; 3, indifferent; 4, fun; 5, very fun). At the end of each class, each child was given a sheet with pictograms of human faces (i.e., emojis), which illustrate 5 levels of emotion (48). The child chose the one that most closely related to the enjoyment level felt during the proposed activities.
2.3 Statistical analyses
Sample distribution was tested using the Shapiro–Wilk test for PA, sleep, aerobic fitness, body composition and motor competence, for the EG and CG at PRE, DUR, and POST moments.
A linear mixed model analysis was performed to examine differences in moderate to vigorous PA (MVPA), sleep duration and efficiency indices, total distance performed in the aerobic fitness test and the total motor competence between the EG vs. CG at PRE, DUR and POST moments. A α-level of 0.05 was set as the level of significance for statistical comparisons. The PRE, DUR, and POST moments were included as a fixed effect and player identity (subject ID) as the random effect, between EG vs. CG.
Furthermore, among the recommended variance–covariance structure models, compound symmetry was selected according to the smallest Akaike Information Criterion assessment (49) based on the Maximum Likelihood method. Pairwise comparisons (Bonferroni) were used to show the mean differences for MVPA, sleep duration and efficiency, total distance performed in the aerobic fitness test and the total motor competence between EG vs. CG.
3 Results
Table 1 reports the anthropometric characteristics of the participants. No significant differences were found between EG vs. CG for all anthropometric measures (p > 0.05) in PRE moment. In the POST moment, children from the EG showed less weight, a lower fat mass percentage and a lower BMI compared to the CG (p ≤ 0.05).
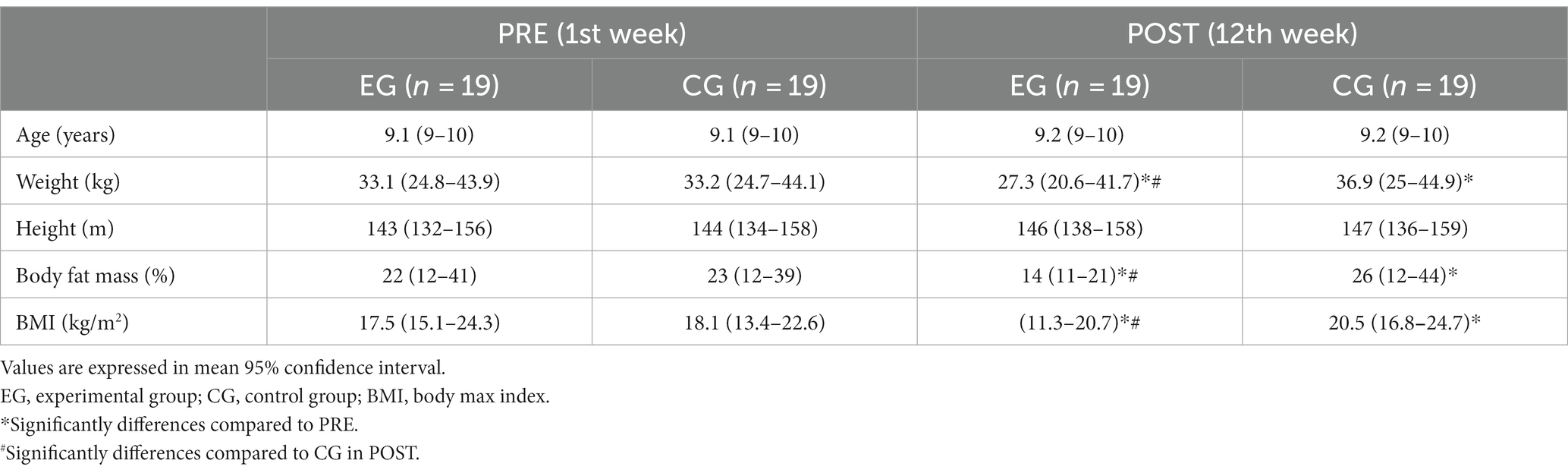
Table 1. Participants’ anthropometric characteristics (n = 38).
There were no significant differences between groups (EG vs. CG) regarding PA, sedentary time, aerobic fitness, sleep duration and efficiency and motor competence, in PRE test (Figure 1). For the DUR and POST test moments, results show that EG spent more time in moderate to vigorous PA (MVPA) (DUR, more ~18 min; POST, more ~34 min) and less time in sedentary (DUR, less ~44 min; POST, less~203 min) per day, compared to the CG (p < 0.001). Children from the EG performed more 44 m and 128 m in the YYIR1C and slept more 17 and 114 min per night compared to CG (DUR (p < 0.05) and POST (p < 0.001), respectively) (Figure 2). No significant differences were found between EG vs. CG for sleep efficiency.
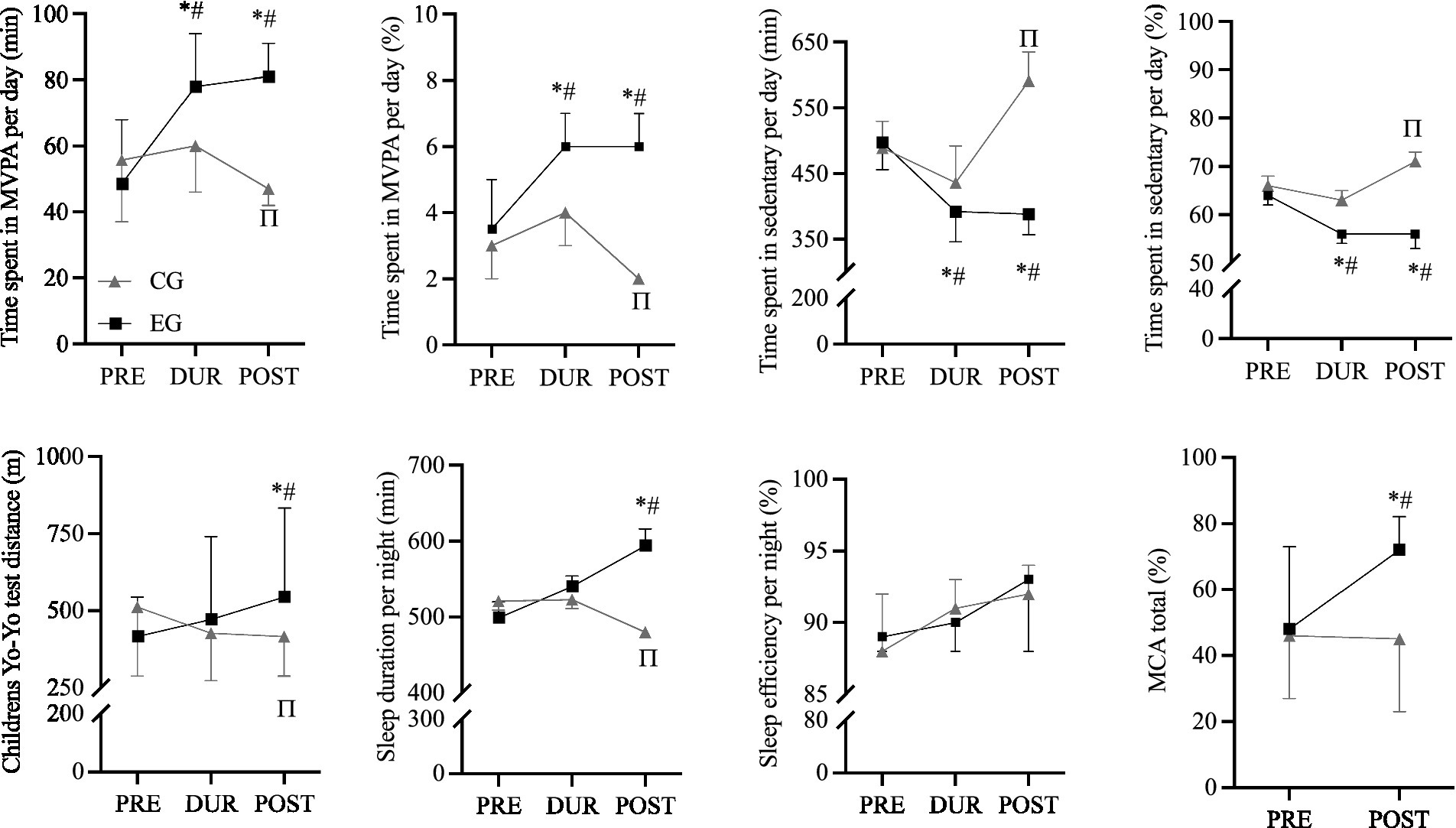
Figure 2. Descriptive data (Control group [CG] n = 19; Experimental group [EG] n = 19) responsiveness for time spent in moderate to vigorous physical activity (MVPA) per day; time spent in sedentary per day; Children’s Yo-Yo test (YYIR1C); sleep duration and sleep efficiency per night, and motor competence assessment (MCA) during PRE (1st week), DUR (6th week) and POST (12th week), in primary school children. Black lines (EG) and gray lines (CG) show group mean (95% confidence interval) during each evaluated moment PRE, DUR and POST. *Significantly different compared to PRE-EG. # Significantly different compared to POST-CG. Π Significantly different compared to PRE-CG.
Regarding motor competence, significant differences were found between groups in POST test of evaluation. Motor competence was significantly better (i.e., more 27%) in the EG compared to CG (p < 0.001) (Figure 2).
When comparing PRE vs. POST test moments, results show that the CG decreased 1% (~ 9 min) of time in MVPA per day, spent 5% (~102 min) more time in sedentary time per day, performed less 96 m in the YYIR1C and slept less 41 min per night (p < 0.001) (Figure 2).
Regarding the EG, children increased by 3% (~33 min) in MVPA time per day, spent 8% (~110 min) less in sedentary time per day; performed more 128 m in the YYIR1C and slept more 95 min per night (p < 0.001) (Figure 2). No significant differences were found between EG vs. CG for sleep efficiency, in both groups (Figure 2).
Regarding MC, children from EG had significantly better motor competence scores (i.e., more 24%) in POST than in PRE (p < 0.001) (Figure 1). No significant differences were found for motor competence scores from CG between PRE and POST (p ≤ 0.05).
During the classes, the % HRmax ranged between 65 and 81% (i.e., light to moderate intensities) and total distance ranged between 1,360–1,627 m (Figure 3).
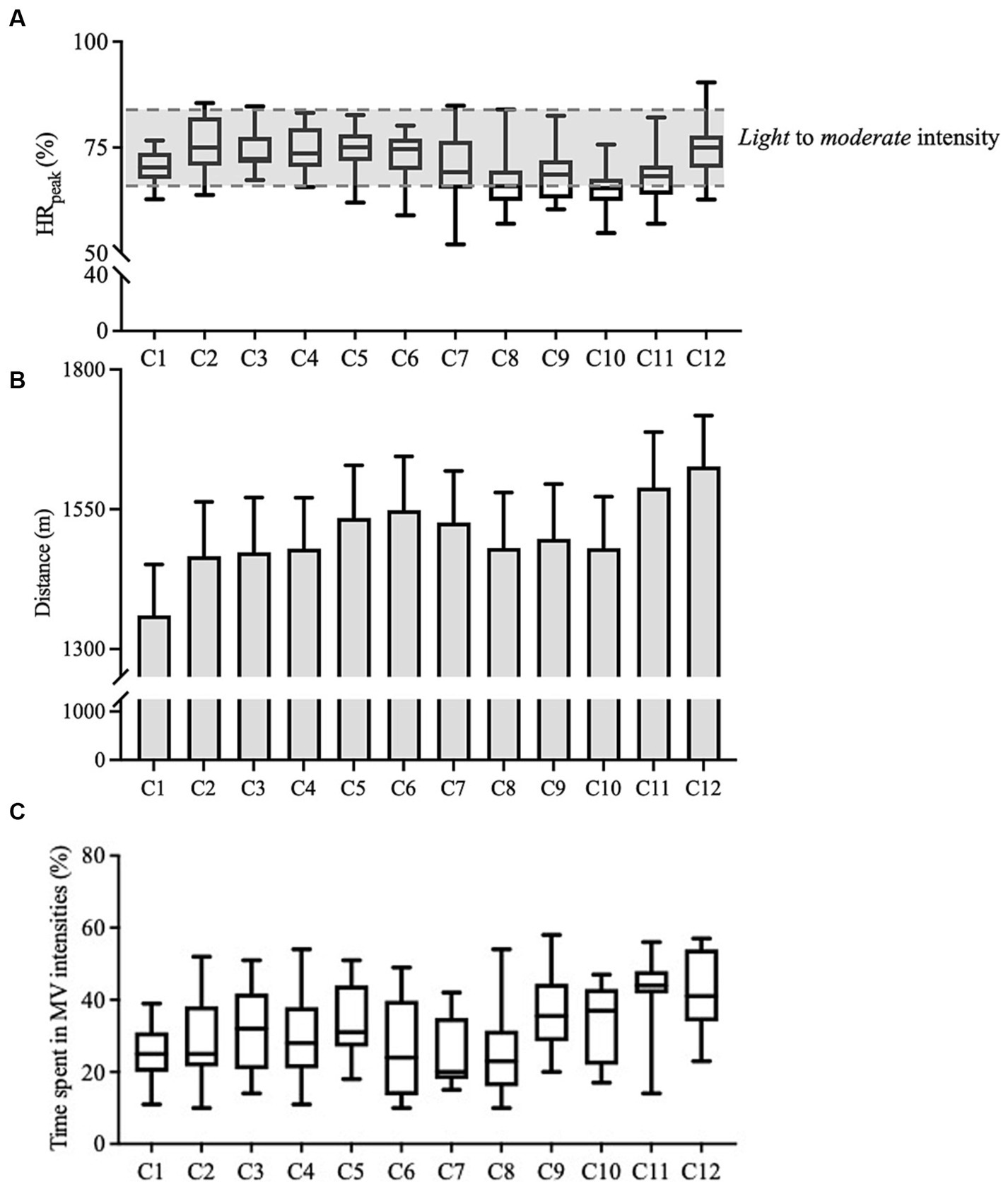
Figure 3. Descriptive data (Experimental group; n = 19) responsiveness for % heart max (%HRmax), external load variables and the responsiveness for time spent in moderate to very hard (i.e., ≥ 70% of heart rate max) during 12-week intervention (one physical education session of 60 min per week), in primary school children. Graphic (A–C) Black lines show group mean (95% confidence interval) data. C, class; TD, total distance.
The time spent above 70% HRmax ranged between 15 and 60% (i.e., moderate to very hard).
Enjoyment ranged between 4 and 5 (i.e., fun–great fun). All children gave a 5 (great fun) in all extra-curricular activity classes with exception of one child that gave a 4 (fun) in the 4th extra-curricular activity class.
4 Discussion
The aim of this research was to present the findings of a school-based PA intervention program conducted among primary school children, assessing its impact on PA levels, sleep patterns, aerobic fitness, and MC. The comparison between the EG and CG at PRE and POST intervention moments revealed a significant and positive impact on several parameters, among primary school children, corroborating the study hypothesis. In general, the EG not only showed statistically significant improvements in weight, body fat mass, and body mass index but also exhibited positive changes in PA levels, aerobic fitness, and sleep duration, when compared to the CG. These improvements bring the EG closer to or in line with the WHO recommendations for children (50) in this specified age group (i.e., 9–10 years), indicating the effectiveness of the intervention program “Super Quinas.” These findings are also aligned with existing scientific literature that emphasizes the importance of PA interventions in improving overall health and well-being in children (4, 8, 10).
Regarding body composition, it is important to highlight that EG children showed significantly lower values of weight, body fat mass and body mass index in POST compared to PRE. This is in accordance with other school-based PA interventions: 11-week (51, 52), 12-week (53) and 6-month intervention (54). All these school-based PA studies have shown potential for yielding positive effects on body composition.
4.1 Physical activity, sleep, and aerobic fitness
It is well known that cardiovascular disease risk factors are associated with lower levels of PA and highly associated with a lower level of fitness in children (55). However, it is important to note that interventions focusing on PA within a school-based setting can potentially enhance both PA and fitness among healthy young individuals (16, 56). The most recent results from Portugal’s 2021 Report Card on Physical Activity for Children and Adolescents shows that less than 30% of children and adolescents achieve physical activity guidelines (2). In the present study, it was possible to find that the EG demonstrated a significant increase in MVPA compared to the CG, both at DUR and POST intervention moments. Moreover, the EG spent approximately 2% more time in MVPA per day at PRE, with this difference increasing to 4% in the POST intervention period. Accordingly, on sedentary time, the EG also exhibited substantial reductions compared to the CG, i.e., at PRE, the EG spent 7% less time in sedentary activities per day, which further increased to 15% in the POST period. This aligns with previous research indicating that structured exercise programs can effectively promote MVPA, contributing to improved cardiovascular fitness and overall health (57). Additionally, it also reinforces the importance of reducing sedentary behavior, as excessive sedentary has been linked to various health risks (58). In the current study, the EG improved the moderate to vigorous MVPA from PRE to POST intervention moments, approaching or reaching the WHO recommendations for children (50).
Regarding children’s sleep, children from the EG showed significantly more sleep duration at POST moment, with a significantly increase of 114 min, when compared to CG. The observed increase in sleep duration in the EG is consistent with research that suggests a bidirectional relationship between PA and sleep (17). Engaging in a regular PA can positively affect sleep duration by reducing anxiety and stress levels, promoting the release of endorphins, and contributing to better sleep patterns (59). This natural enhancement in sleep duration due to increased PA aligns with the findings of the current study. A study by Rhodes et al. (59) highlighted how PA can improve sleep quality and duration in children, indicating that an adequate sleep duration is essential for recovery and overall health, and exercise interventions have been shown to positively impact sleep quality and duration (17, 59).
It is also important to mention that PA and sleep could also be associated with the exercise intensity (60). In the present study the exercise intensity (monitored as a % HRmax) revealed that the EG maintained intensities between 65 and 81% of HRmax, indicating light to moderate intensities. This level of exercise intensity falls within the range typically recommended for promoting overall health and well-being in children’s (61). This level of exercise intensity encourages participation in a wider range of activities, contributing to an active and healthy lifestyle. The relationship between exercise intensity and sleep in children is also significant. The findings in the current study indicate that children in the EG experienced an increase in sleep duration following the intervention. The maintenance of light to moderate exercise intensities may have contributed to this positive effect on sleep. Research has shown that exercise at moderate intensities can enhance the overall quality and duration of sleep in children (62). For instance, Alnawwar et al. (62) have demonstrated that engaging in moderate-intensity physical exercise can result in improved sleep patterns, reducing the risk of sleep disturbances. Furthermore, light-moderate exercise intensities may help children fall asleep more easily and experience deeper, more restorative sleep (62).
Concerning the aerobic fitness, the YYIR1C test was significantly higher in the EG compared to CG at POST intervention revealing a better aerobic fitness after the 12-week intervention. This effect has been associated with a lower risk of cardiometabolic diseases, obesity, diabetes, and other health problems during the entire life cycle (63). Other studies have reported similar effects of intervention programs on aerobic fitness performance in children after 6 weeks (40), 11 weeks (52, 64) and 10 months (65).
4.2 Motor competence and enjoyment assessment
Motor competence is a crucial aspect of child development as it encompasses a range of fundamental movement skills that are essential for participating in PA and sports (14, 15). These skills include running, jumping, throwing, catching, and balance, among others. Motor competence is associated with a child’s overall physical development, coordination, and ability to engage in various physical activities. The findings of the present study showed that a school-based PA intervention had a positive impact on motor competence in primary school children. This is an important result because it aligns with the goals of physical education programs, which aim to improve children’s fundamental motor skills and physical literacy. Research supports the idea that well-designed PA interventions can enhance motor competence in children (20). A study conducted by Barnett et al. (4) found that structured PA programs in schools can significantly improve motor skills and fundamental movement abilities in children. In the current study, the EG displayed a 27% improvement in motor competence compared to the CG at POST intervention period. This emphasizes the effectiveness of exercise interventions in motor coordination, as found in the scientific literature (20, 66). Moreover, these results suggests that the intervention had a meaningful and positive impact on children’s motor skills. Such improvements in motor competence can have far-reaching benefits, not only in terms of PA and sports participation but also in promoting physical confidence and a lifelong interest in maintaining an active and healthy lifestyle (4, 67).
Finally, it is important to highlight children from the EG also reported high enjoyment levels, ranging from 4 to 5 on a scale of 1 (fun) to 5 (great fun). This suggests that the exercise program was fun and enjoyable, which is crucial for long-term adherence to PA programs (68).
Additionally, it is important to note that there are other factors that might influence PA levels, sleep patterns, aerobic fitness, and MC in children among primary school. Such as the cultural norms; socioeconomic disparities (e.g., access to recreational facilities and sleep environment); the educational system (e.g., school schedules and how the educational systems focus on promoting overall well-being); the technology and screen time (i.e., integration of technology in educational settings can influence sedentary behavior and impact both PA and sleep patterns); the parental involvement (e.g., modeling behaviors and sleep practices); the community and social support (e.g., community programs and social connections) and public health initiatives (e.g., government policies and accessibility of healthcare). Thu, all these factors are relevant for implementing and adapting the intervention, and tailored strategies would be necessary under certain social conditions.
5 Strengths and limitations
It is important to acknowledge the strengths and limitations of this study. It contributes to the existing knowledge by exploring the potential of a school-based intervention to improve the PA levels, sleep patterns, aerobic fitness, and motor competence among primary school children, which, to the best of our knowledge, has not been previously undertaken. Moreover, the use of objective instruments (e.g., accelerometers and HR monitors), further strengthened the design of our study. Overall, these strengths contribute to the robustness and credibility of our study’s findings.
Regarding the limitations, the sample size was small and not randomly assigned, which can increase the risk of bias. Activities outside school were not controlled in the analysis, nor the socioeconomic status or the presence of siblings in the family. Moreover, it is also very important to consider as limitation the fact that data were not analyzed according to the sex distribution (i.e., stratified analysis by sex) neither by location clusters.
6 Conclusion
Our findings indicate that adding one more physical education lesson of 60 min per week (i.e., a total of 120 min of physical education weekly), over three months (i.e., 12 weeks), resulted in significant improvements in PA levels, sleep patterns, aerobic fitness, and motor competence in children aged 9–10 years. Thus, this study highlights the role of the school-based programs as important determinants of PA levels in elementary schoolchildren. These data reinforce and justify that priority should be given to the development of national action programs that encourage the adoption of healthier lifestyles and to the creation of structural and environmental conditions favorable to children’s health.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethical Committee of the Portugal Football School, Portuguese Football Federation (nr. CEPFS 17.2022). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
JC: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. SV: Conceptualization, Data curation, Investigation, Methodology, Software, Writing – review & editing, Formal analysis. RC: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – review & editing. LR: Writing – review & editing, Investigation. VC: Investigation, Writing – review & editing. RP: Conceptualization, Visualization, Writing – review & editing, Data curation. MC: Conceptualization, Investigation, Validation, Visualization, Writing – review & editing, Supervision. CN: Conceptualization, Investigation, Supervision, Validation, Visualization, Writing – review & editing. JB: Conceptualization, Investigation, Validation, Visualization, Writing – review & editing, Supervision. JG: Conceptualization, Formal analysis, Investigation, Validation, Visualization, Writing – review & editing, Supervision. AS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, Funding acquisition, Resources.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by the Portuguese Football Federation.
Acknowledgments
The authors would like to acknowledge the children, parents or legal guardians, and teachers from the primary school D. Carlos I, Municipality of Sintra, Portugal.
Conflict of interest
“Super Quinas” is a registered trademark of the Portuguese Football Federation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Wang, Y, and Lobstein, T. Worldwide trends in childhood overweight and obesity. Int J Pediatr Obes. (2006) 1:11–25. doi: 10.1080/17477160600586747
2. Pizarro, A, Oliveira-Santos, JM, Santos, R, Ribeiro, JC, Santos, MP, Coelho-E-Silva, M, et al. Results from Portugal's 2022 report card on physical activity for children and youth. J Exerc Sci Fit. (2023) 21:280–5. doi: 10.1016/j.jesf.2023.05.002
3. WHO (2022). WHO regional Office for Europe. Report on the fifth round of data collection, 2018–2020: WHO European childhood obesity surveillance initiative (COSI) Copenhagen 2022.
4. Barnett, LM, Jerebine, A, Keegan, R, Watson-Mackie, K, Arundell, L, Ridgers, ND, et al. Validity, reliability, and feasibility of physical literacy assessments designed for school children: a systematic review. Sports Med. (2023, 2023) 53:1905–29. doi: 10.1007/s40279-023-01867-4
5. Dumith, SC, Gigante, DP, Domingues, MR, and Kohl, HW 3rd. Physical activity change during adolescence: a systematic review and a pooled analysis. Int J Epidemiol. (2011) 40:685–98. doi: 10.1093/ije/dyq272
6. Janssen, I, and Leblanc, AG. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act. (2010) 7:40. doi: 10.1186/1479-5868-7-40
7. Mitchell, JA, Pate, RR, Beets, MW, and Nader, PR. Time spent in sedentary behavior and changes in childhood BMI: a longitudinal study from ages 9 to 15 years. Int J Obes. (2013) 37:54–60. doi: 10.1038/ijo.2012.41
8. Morgado, MC, Sousa, M, Marques, C, Coelho, AB, Costa, JA, and Seabra, A. Effects of physical activity and nutrition education on the gut microbiota in overweight and obese children. Children (Basel). (2023) 10:10. doi: 10.3390/children10071242
9. Salmon, J, Booth, ML, Phongsavan, P, Murphy, N, and Timperio, A. Promoting physical activity participation among children and adolescents. Epidemiol Rev. (2007) 29:144–59. doi: 10.1093/epirev/mxm010
10. Santos, F, Sousa, H, Gouveia, ER, Lopes, H, Peralta, M, Martins, J, et al. School-based family-oriented health interventions to promote physical activity in children and adolescents: a systematic review. Am J Health Promot. (2023) 37:243–62. doi: 10.1177/08901171221113836
11. Chaput, JP, Gray, CE, Poitras, VJ, Carson, V, Gruber, R, Olds, T, et al. Systematic review of the relationships between sleep duration and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. (2016) 41:S266–82. doi: 10.1139/apnm-2015-0627
12. Hands, B, and Larkin, D. Physical activity measurement methods for young children: a comparative study. Meas Phys Educ Exerc Sci. (2006) 10:203–14. doi: 10.1207/s15327841mpee1003_5
13. Robinson, LE, Stodden, DF, Barnett, LM, Lopes, VP, Logan, SW, Rodrigues, LP, et al. Motor competence and its effect on positive developmental trajectories of health. Sports Med. (2015) 45:1273–84. doi: 10.1007/s40279-015-0351-6
14. Rodrigues, LP, Stodden, DF, and Lopes, VP. Developmental pathways of change in fitness and motor competence are related to overweight and obesity status at the end of primary school. J Sci Med Sport. (2016) 19:87–92. doi: 10.1016/j.jsams.2015.01.002
15. Rodrigues, LP, Luz, C, Cordovil, R, Bezerra, P, Silva, B, Camoes, M, et al. Normative values of the motor competence assessment (MCA) from 3 to 23 years of age. J Sci Med Sport. (2019) 22:1038–43. doi: 10.1016/j.jsams.2019.05.009
16. Neil-Sztramko, SE, Caldwell, H, and Dobbins, M. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst Rev. (2021) 9:CD007651. doi: 10.1002/14651858.CD007651.pub2
17. Kredlow, MA, Capozzoli, MC, Hearon, BA, Calkins, AW, and Otto, MW. The effects of physical activity on sleep: a meta-analytic review. J Behav Med. (2015) 38:427–49. doi: 10.1007/s10865-015-9617-6
18. Carson, V, Tremblay, MS, Chaput, JP, and Chastin, SF. Associations between sleep duration, sedentary time, physical activity, and health indicators among Canadian children and youth using compositional analyses. Appl Physiol Nutr Metab. (2016) 41:S294–302. doi: 10.1139/apnm-2016-0026
19. Nixon, GM, Thompson, JM, Han, DY, Becroft, DM, Clark, PM, Robinson, E, et al. Short sleep duration in middle childhood: risk factors and consequences. Sleep. (2008) 31:71–8. doi: 10.1093/sleep/31.1.71
20. Holfelder, B, and Schott, N. Relationship of fundamental movement skills and physical activity in children and adolescents: a systematic review. Psychol Sport Exerc. (2014) 15:382–91. doi: 10.1016/j.psychsport.2014.03.005
21. Ortega, FB, Ruiz, JR, Castillo, MJ, and Sjostrom, M. Physical fitness in childhood and adolescence: a powerful marker of health. Int J Obes. (2008) 32:1–11. doi: 10.1038/sj.ijo.0803774
22. Eisenmann, JC, Ekkekakis, P, and Holmes, M. Sleep duration and overweight among Australian children and adolescents. Acta Paediatr. (2006) 95:956–63. doi: 10.1080/08035250600731965
23. Sekine, M, Yamagami, T, Handa, K, Saito, T, Nanri, S, Kawaminami, K, et al. A dose-response relationship between short sleeping hours and childhood obesity: results of the Toyama birth cohort study. Child Care Health Dev. (2002) 28:163–70. doi: 10.1046/j.1365-2214.2002.00260.x
24. Miller, RM, Chambers, TL, Burns, SP, and Godard, MP. Validating InBody® 570 multi-frequency bioelectrical impedance analyzer versus DXA for body fat percentage analysis.: 3576 board #15 June 4, 8: 00 AM - 9: 30 AM. Med Sci Sports Exerc. (2016) 48:991. doi: 10.1249/01.mss.0000487979.68551.d7
25. Evenson, KR, Catellier, DJ, Gill, K, Ondrak, KS, and Mcmurray, RG. Calibration of two objective measures of physical activity for children. J Sports Sci. (2008) 26:1557–65. doi: 10.1080/02640410802334196
26. Migueles, JH, Cadenas-Sanchez, C, Ekelund, U, Delisle Nystrom, C, Mora-Gonzalez, J, Lof, M, et al. Accelerometer data collection and processing criteria to assess physical activity and other outcomes: a systematic review and practical considerations. Sports Med. (2017) 47:1821–45. doi: 10.1007/s40279-017-0716-0
27. Kuritz, A, Mall, C, Schnitzius, M, and Mess, F. Physical activity and sedentary behavior of children in afterschool programs: an accelerometer-based analysis in full-day and half-day elementary schools in Germany. Front Public Health. (2020) 8:463. doi: 10.3389/fpubh.2020.00463
28. Troiano, RP. Large-scale applications of accelerometers: new frontiers and new questions. Med Sci Sports Exerc. (2007) 39:1501. doi: 10.1097/mss.0b013e318150d42e
29. Cooper, AR, Goodman, A, Page, AS, Sherar, LB, Esliger, DW, Van Sluijs, EM, et al. Objectively measured physical activity and sedentary time in youth: the international children's accelerometry database (ICAD). Int J Behav Nutr Phys Act. (2015) 12:113. doi: 10.1186/s12966-015-0274-5
30. Trost, SG, Loprinzi, PD, Moore, R, and Pfeiffer, KA. Comparison of accelerometer cut points for predicting activity intensity in youth. Med Sci Sports Exerc. (2011) 43:1360–8. doi: 10.1249/MSS.0b013e318206476e
31. Steene-Johannessen, J, Hansen, BH, Dalene, KE, Kolle, E, Northstone, K, Møller, NC, et al. Variations in accelerometry measured physical activity and sedentary time across Europe - harmonized analyses of 47,497 children and adolescents. Int J Behav Nutr Phys Act. (2020) 17:38. doi: 10.1186/s12966-020-00930-x
32. Alsaadi, SM, Mcauley, JH, Hush, JM, Bartlett, DJ, Mckeough, ZM, Grunstein, RR, et al. Assessing sleep disturbance in low back pain: the validity of portable instruments. PLoS One. (2014) 9:e95824. doi: 10.1371/journal.pone.0095824
33. Smith, C, Galland, B, Taylor, R, and Meredith-Jones, K. ActiGraph GT3X+ and Actical wrist and hip worn accelerometers for sleep and wake indices in young children using an automated algorithm: validation with polysomnography. Front Psych. (2019) 10:958. doi: 10.3389/fpsyt.2019.00958
34. Meltzer, LJ, Walsh, CM, Traylor, J, and Westin, AM. Direct comparison of two new actigraphs and polysomnography in children and adolescents. Sleep. (2012) 35:159–66. doi: 10.5665/sleep.1608
35. Sadeh, A, Sharkey, KM, and Carskadon, MA. Activity-based sleep-wake identification: an empirical test of methodological issues. Sleep. (1994) 17:201–7. doi: 10.1093/sleep/17.3.201
36. Hirshkowitz, M, Whiton, K, Albert, SM, Alessi, C, Bruni, O, DonCarlos, L, et al. National Sleep Foundation's sleep time duration recommendations: methodology and results summary. Sleep Health. (2015) 1:40–3. doi: 10.1016/j.sleh.2014.12.010
37. Ohayon, M, Wickwire, EM, Hirshkowitz, M, Albert, SM, Avidan, A, Daly, FJ, et al. National Sleep Foundation's sleep quality recommendations: first report. Sleep Health. (2017) 3:6–19. doi: 10.1016/j.sleh.2016.11.006
38. Povoas, SC, Castagna, C, Soares, JM, Silva, PM, Lopes, MV, and Krustrup, P. Reliability and validity of Yo-Yo tests in 9- to 16-year-old football players and matched non-sports active schoolboys. Eur J Sport Sci. (2016a) 16:755–63. doi: 10.1080/17461391.2015.1119197
39. Povoas, SCA, Castagna, C, Da Costa Soares, JM, Silva, P, Coelho, ESM, Matos, F, et al. Reliability and construct validity of Yo-Yo tests in untrained and soccer-trained schoolgirls aged 9-16. Pediatr Exerc Sci. (2016b) 28:321–30. doi: 10.1123/pes.2015-0212
40. Bendiksen, M, Williams, CA, Hornstrup, T, Clausen, H, Kloppenborg, J, Shumikhin, D, et al. Heart rate response and fitness effects of various types of physical education for 8- to 9-year-old schoolchildren. Eur J Sport Sci. (2014) 14:861–9. doi: 10.1080/17461391.2014.884168
41. Ahler, T, Bendiksen, M, Krustrup, P, and Wedderkopp, N. Aerobic fitness testing in 6- to 9-year-old children: reliability and validity of a modified Yo-Yo IR1 test and the Andersen test. Eur J Appl Physiol. (2012) 112:871–6. doi: 10.1007/s00421-011-2039-4
42. Bendiksen, M, Ahler, T, Clausen, H, Wedderkopp, N, and Krustrup, P. The use of Yo-Yo intermittent recovery level 1 and Andersen testing for fitness and maximal heart rate assessments of 6- to 10-year-old school children. J Strength Cond Res. (2013) 27:1583–90. doi: 10.1519/JSC.0b013e318270fd0b
43. Luz, C, Rodrigues, LP, Almeida, G, and Cordovil, R. Development and validation of a model of motor competence in children and adolescents. J Sci Med Sport. (2016) 19:568–72. doi: 10.1016/j.jsams.2015.07.005
44. Muntaner-Mas, A, Vidal-Conti, J, Salmon, J, and Palou-Sampol, P. Associations of heart rate measures during physical education with academic performance and executive function in children: a cross-sectional study. Int J Environ Res Public Health. (2020) 17:1–12.doi: 10.3390/ijerph17124307
45. Beato, M, Devereux, G, and Stiff, A. Validity and reliability of global positioning system units (STATSports viper) for measuring distance and peak speed in sports. J Strength Cond Res. (2018) 32:2831–7. doi: 10.1519/JSC.0000000000002778
46. Gaudino, P, Iaia, FM, Alberti, G, Hawkins, RD, Strudwick, AJ, and Gregson, W. Systematic bias between running speed and metabolic power data in elite soccer players: influence of drill type. Int J Sports Med. (2014) 35:489–93. doi: 10.1055/s-0033-1355418
47. Castagna, C, Krustrup, P, D'ottavio, S, Pollastro, C, Bernardini, A, and Araujo Povoas, SC. Ecological validity and reliability of an age-adapted endurance field test in young male soccer players. J Strength Cond Res. (2019) 33:3400–5. doi: 10.1519/JSC.0000000000002255
48. Motl, RW, Dishman, RK, Saunders, R, Dowda, M, Felton, G, and Pate, RR. Measuring enjoyment of physical activity in adolescent girls. Am J Prev Med. (2001) 21:110–7. doi: 10.1016/S0749-3797(01)00326-9
49. Akaike, H. A new look at the statistical model identification. IEEE Trans Autom Control. (1974) 19:716–23. doi: 10.1109/TAC.1974.1100705
50. Bull, FC, Al-Ansari, SS, Biddle, S, Borodulin, K, Buman, MP, Cardon, G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. (2020) 54:1451–62. doi: 10.1136/bjsports-2020-102955
51. Larsen, MN, Terracciano, A, Moller, TK, Aggestrup, CS, Buono, P, Krustrup, P, et al. An 11-week school-based "health education through football" programme improves musculoskeletal variables in 10-12-yr-old Danish school children. Bone Rep. (2023) 18:101681. doi: 10.1016/j.bonr.2023.101681
52. Orntoft, C, Fuller, CW, Larsen, MN, Bangsbo, J, Dvorak, J, and Krustrup, P. 'FIFA 11 for Health' for Europe. II: effect on health markers and physical fitness in Danish schoolchildren aged 10-12 years. Br J Sports Med. (2016) 50:1394–9. doi: 10.1136/bjsports-2016-096124
53. Vasconcellos, F, Seabra, A, Cunha, F, Montenegro, R, Penha, J, Bouskela, E, et al. Health markers in obese adolescents improved by a 12-week recreational soccer program: a randomised controlled trial. J Sports Sci. (2016) 34:564–75. doi: 10.1080/02640414.2015.1064150
54. Seabra, A, Katzmarzyk, P, Carvalho, MJ, Seabra, A, Coelho, ESM, Abreu, S, et al. Effects of 6-month soccer and traditional physical activity programmes on body composition, cardiometabolic risk factors, inflammatory, oxidative stress markers and cardiorespiratory fitness in obese boys. J Sports Sci. (2016) 34:1822–9. doi: 10.1080/02640414.2016.1140219
55. Andersen, LB, Bugge, A, Dencker, M, Eiberg, S, and El-Naaman, B. The association between physical activity, physical fitness and development of metabolic disorders. Int J Pediatr Obes. (2011) 6:29–34. doi: 10.3109/17477166.2011.606816
56. Kriemler, S, Meyer, U, Martin, E, Van Sluijs, EM, Andersen, LB, and Martin, BW. Effect of school-based interventions on physical activity and fitness in children and adolescents: a review of reviews and systematic update. Br J Sports Med. (2011) 45:923–30. doi: 10.1136/bjsports-2011-090186
57. Warburton, DE, Nicol, CW, and Bredin, SS. Health benefits of physical activity: the evidence. CMAJ. (2006) 174:801–9. doi: 10.1503/cmaj.051351
58. Biswas, A, Oh, PI, Faulkner, GE, Bajaj, RR, Silver, MA, Mitchell, MS, et al. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: a systematic review and meta-analysis. Ann Intern Med. (2015) 162:123–32. doi: 10.7326/M14-1651
59. Rhodes, RE, Guerrero, MD, Vanderloo, LM, Barbeau, K, Birken, CS, Chaput, JP, et al. Development of a consensus statement on the role of the family in the physical activity, sedentary, and sleep behaviours of children and youth. Int J Behav Nutr Phys Act. (2020) 17:74. doi: 10.1186/s12966-020-00973-0
60. Fonseca, A, De Azevedo, CVM, and Santos, RMR. Sleep and health-related physical fitness in children and adolescents: a systematic review. Sleep Sci. (2021) 14:357–65. doi: 10.5935/1984-0063.20200125
61. Jago, R, Sebire, SJ, Turner, KM, Bentley, GF, Goodred, JK, Fox, KR, et al. Feasibility trial evaluation of a physical activity and screen-viewing course for parents of 6 to 8 year-old children: Teamplay. Int J Behav Nutr Phys Act. (2013) 10:31. doi: 10.1186/1479-5868-10-31
62. Alnawwar, MA, Alraddadi, MI, Algethmi, RA, Salem, GA, Salem, MA, and Alharbi, AA. The effect of physical activity on sleep quality and sleep disorder: a systematic review. Cureus. (2023) 15:e43595. doi: 10.7759/cureus.43595
63. Laurson, KR, Eisenmann, JC, and Welk, GJ. Development of youth percent body fat standards using receiver operating characteristic curves. Am J Prev Med. (2011) 41:S93–9. doi: 10.1016/j.amepre.2011.07.003
64. Skoradal, MB, Purkhus, E, Steinholm, H, Olsen, MH, Orntoft, C, Larsen, MN, et al. "FIFA 11 for health" for Europe in the Faroe Islands: effects on health markers and physical fitness in 10- to 12-year-old schoolchildren. Scand J Med Sci Sports. (2018) 28:8–17. doi: 10.1111/sms.13209
65. Larsen, MN, Nielsen, CM, Helge, EW, Madsen, M, Manniche, V, Hansen, L, et al. Positive effects on bone mineralisation and muscular fitness after 10 months of intense school-based physical training for children aged 8-10 years: the FIT FIRST randomised controlled trial. Br J Sports Med. (2018) 52:254–60. doi: 10.1136/bjsports-2016-096219
66. Santner, A, Kopp, M, and Federolf, P. Partly randomised, controlled study in children aged 6-10 years to investigate motor and cognitive effects of a 9-week coordination training intervention with concurrent mental tasks. BMJ Open. (2018) 8:e021026. doi: 10.1136/bmjopen-2017-021026
67. Barnett, LM, Van Beurden, E, Morgan, PJ, Brooks, LO, and Beard, JR. Childhood motor skill proficiency as a predictor of adolescent physical activity. J Adolesc Health. (2009) 44:252–9. doi: 10.1016/j.jadohealth.2008.07.004
Keywords: sedentarism, childhood, exercise, physical activity program, health
Citation: Costa JA, Vale S, Cordovil R, Rodrigues LP, Cardoso V, Proença R, Costa M, Neto C, Brito J, Guilherme J and Seabra A (2024) A school-based physical activity intervention in primary school: effects on physical activity, sleep, aerobic fitness, and motor competence. Front. Public Health. 12:1365782. doi: 10.3389/fpubh.2024.1365782
Edited by:
Jennifer K. Frediani, Emory University, United StatesReviewed by:
Isabel Rada, Universidad del Desarrollo, ChileJuris Porozovs, University of Latvia, Latvia
Copyright © 2024 Costa, Vale, Cordovil, Rodrigues, Cardoso, Proença, Costa, Neto, Brito, Guilherme and Seabra. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Júlio A. Costa, amFoZGNAaG90bWFpbC5jb20=