 Santo Fruscione1*
Santo Fruscione1* Ginevra Malta1
Ginevra Malta1 Maria Gabriella Verso1Anna Calascibetta1Daniela Martorana2
Maria Gabriella Verso1Anna Calascibetta1Daniela Martorana2 Emanuele Cannizzaro1
Emanuele Cannizzaro1- 1PROMISE Department, University of Palermo, Palermo, Italy
- 2Department of Orthopedics, Hospital Company ‘Ospedali Riuniti Villa Sofia-Cervello’, Palermo, Italy
Introduction: Work-related stress is an occupational risk that has been linked to the development of cardiovascular disease (CVD). While previous studies have explored this association in various work contexts, none have focused specifically on logistics and distribution personnel. These workers may be exposed to significant job stress, which potentially increases the risk of CVD.
Methods: In this study, we aimed to examine the relationship between work-related stress and cardiovascular risk in a sample of 413 healthy workers of a logistics and distribution company. To assess work-related stress and cardiovascular risk, we used the organisational well-being questionnaire proposed by the Italian National Anti-Corruption Authority, the Framingham Heart Study General Cardiovascular Disease (CVD) Risk Prediction Score and the WHO General Wellbeing Index (WHO-5).
Results: Our results revealed that individuals with low job support had a significantly higher CVD risk score and lower well-being index than those reporting high job support. Furthermore, workers with high-stress tasks showed higher well-being index scores than those with passive tasks. Approximately 58% of the subjects were classified as low CVD risk (CVD risk <10%), approximately 31% were classified as moderate risk (CVD risk between 10 and 20%) and 11% were considered high risk (CVD risk >20%). The overall median CVD risk for the population was moderate (6.9%), with individual scores ranging from 1 to 58%.
Discussion: Further analyses confirmed the protective effect of work support, also identifying physical inactivity, regular alcohol consumption and low educational level as factors contributing to an increased risk of CVD. Interestingly, factors such as job control and work support demonstrated a positive impact on psychological well-being. These results emphasise the importance of intervention strategies aimed at promoting health in the workplace. By addressing these combined factors, organisations can effectively reduce the risk of CVD and improve the general well-being of their workforce.
1 Introduction
Cardiovascular diseases (CVD) occurring in adulthood are mainly caused by a combination of modifiable and non-modifiable factors (1). These diseases are the leading cause of death in developed countries (2).
Among the factors that can be changed, behaviours such as smoking, unhealthy eating habits, lack of physical activity and stress have been identified as significant factors (3, 4). However, although there is international consensus that work-related stress is a major health and safety challenge in modern society, its connection to cardiovascular risk is not yet fully understood. With the ageing of the world’s population and considering its particular impact on certain occupations, it is expected that an increasing number of workers will develop chronic diseases during their working lives, with a significant impact on essential services for the general population (5).
In recent years, also due to the SARS-CoV-2 pandemic with increased sedentary behaviour, workplace health promotion has become a crucial issue on an international scale (6, 7). In Italy, a recent agreement between the Italian Society of Occupational Medicine (SIML) and the Ministry of Health emphasises the role of occupational physicians in the implementation of strategies for the prevention of chronic non-communicable diseases among workers and citizens (8). These strategies include the implementation of screening and the promotion of healthier lifestyles. To ensure the effectiveness of these strategies, it is important to first explore the relationships between organisational factors, psychological well-being and general health status in different work environments. It is precisely as a result of the COVID-19 pandemic and its variants that the concept of psychological well-being has also been reinforced in relation to the work dimension (9). In fact, psychological stress was able to lead to erroneous behaviour and addictions, such as those to alcohol, which could also negatively influence the individual’s working life (10).
It will be necessary to identify the groups of workers who may be more susceptible to health problems and to design specific workplace health promotion programmes (11). Despite the well-established association between work-related stress and cardiovascular risk factors such as metabolic syndrome or hypertension, very few studies have examined this association in specific occupations (12–14). To our knowledge, few studies have been conducted on a sector as heterogeneous and varied as logistics and distribution, which has experienced an increase in the demand for labour in recent years. This complex system involves a large number of people, from drivers to warehousemen and administrative staff. Managing this workforce, ensuring their well-being and optimising their performance is a significant operational challenge. In summary, the logistics and distribution sector is a very intricate web of processes, technologies, regulations and human resources (15, 16). It is constantly evolving to meet the needs of a rapidly changing world and the associated complexities require constant innovation and adaptation to ensure timely and reliable delivery of items to individuals and businesses.
To assess work-related stress, validated methods use self-administered questionnaires such as the Effort/Reward Imbalance (ERI) and the Job Demand-Control (JDC), which are highly reliable (16, 17). In particular, Karasek’s job demand-control model, although proposed in 1979, remains relevant today, using a system that identifies job demand and job control as key risk factors for employee well-being (18). Work demand refers to quantitative aspects such as workload and time pressure, while work control, or ‘decision latitude’, refers to workers’ ability to control their workload and schedules. Combining these two dimensions, Karasek classified jobs into four categories: high-stress jobs (high demand and low control), low-stress jobs (low demand and high control), passive jobs (low demand and low control) and active jobs (high demand and high control) (19). The JDC model was further extended to include job support as a third component. According to the theorisation of the model, jobs characterised by high demands, low control and low social support are the most detrimental to workers’ well-being (20). In our study, we used a cross-sectional design to investigate the relationship between work-related stress, employees’ general perception of emotional well-being and cardiovascular risk among workers with different tasks in a logistic and distribution company.
A secondary objective was to identify indicators of the effectiveness of health promotion programmes aimed at encouraging healthy lifestyles in this specific organisational context.
2 Materials and methods
During the annual occupational health surveillance programme conducted in 2023, our study focused on the recruitment of workers in a logistics and distribution company of southern Italy (21).
Out of a total of over 1,000 employees, we successfully recruited 413 workers as explicated in Figure 1. The selection of subjects included those who were to undergo the occupational health surveillance programme during the study period from January 2023 to September 2023. Inclusion criteria included: an age between 18 and 65 years and at least 3 years of employment. The exclusion criteria were: previous ischaemic cardiovascular diseases, dysmetabolic diseases, Body Mass Index (BMI) > 35, treatment with psychotropic substances (22). The exclusion criteria are specifically designed to ensure that the study accurately assesses the impact of work-related stress on cardiovascular disease risk. By excluding individuals with previous ischemic cardiovascular diseases, the study aims to isolate the effects of work stress from pre-existing cardiovascular conditions. Similarly, excluding those with dysmetabolic diseases and severe obesity addresses confounders that independently increase cardiovascular disease risk, ensuring the focus remains on how work stress contributes to new cardiovascular issues. Excluding participants on psychotropic substances further clarifies this relationship by removing the potential influence of medications on heart health. This strategic selection enhances the study’s precision in investigating how occupational stress uniquely affects cardiovascular disease risk among logistics and distribution workers.
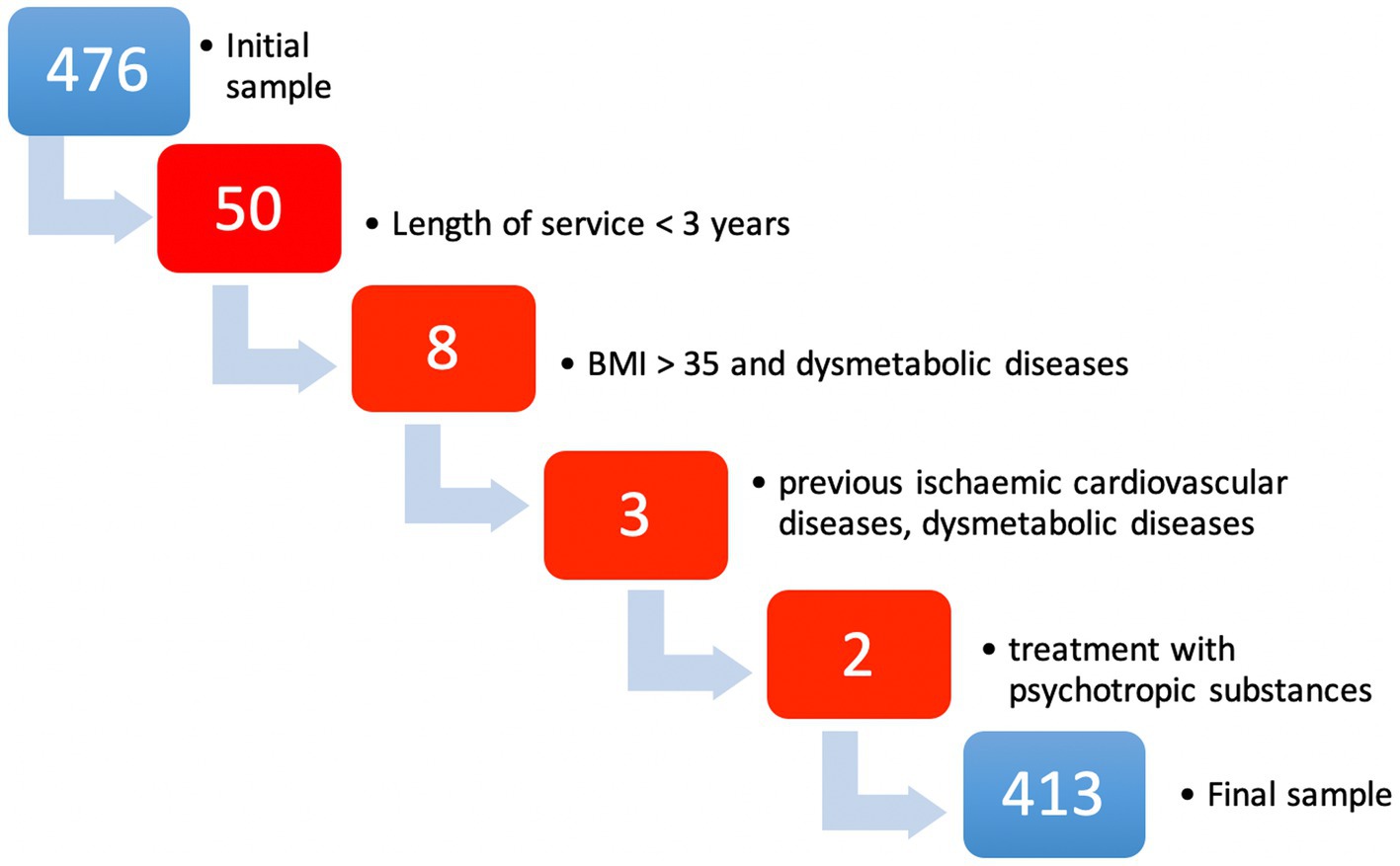
Figure 1. Flowchart about sample selection according to exclusion criteria.
Figure 1 shows the exclusion criteria and the number of persons excluded for each cause.
During the clinical examination, eligible subjects were informed about the objectives of the study and asked to provide written consent for participation. The logistics and distribution company operates throughout the province of Palermo, carrying out most of its receiving and sorting activities within a single facility. The workers were divided into two work shifts: fixed day shifts (reference group consisting of staff with predominantly administrative tasks) and variable shifts including night shifts (reference group consisting of production, in-house processing and drivers).
Various data were extracted from the medical records of each study subject, including age, education level, job duties, length of employment, work shifts, BMI, resting heart rate, systolic and diastolic blood pressure, medical history and current drug treatments. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured by an experienced physician using a manual sphygmomanometer after the subjects had remained supine for 2 min making sure that they do not having consumed coffee or smoked cigarettes for at least the last 2 h before the measurement. We defined obesity as subjects with a BMI greater than 30 kg/m2 and set the threshold for hypertension at SBP ≥ 140 mmHg or DBP ≥ 90 mmHg (22, 23). Each subject also completed a standardised self-administered questionnaire, which assessed work-related stress and included information on lifestyle habits such as smoking, alcohol intake, recreational physical activity and coffee consumption.
We classified the lifestyle, personal and professional variables as follows:
• Smoking habits: Current vs. former smokers or individuals who have never smoked.
• Recreational physical activity: regular exercisers, defined as those who engage in physical activity at least twice a week, as opposed to sporadic exercisers (less than twice a week) or non-practitioners.
• Alcohol intake: abstinent (who strictly abstain from drink), sporadic drinkers (who consume less than one alcoholic unit per day, as in the case of social drinking), daily drinkers (who consume at least one alcoholic unit per day).
• Coffee intake: low consumers (one or no cup per day), medium consumers (two to four cups per day) and high consumers (more than four cups per day).
• Type of shift work: Permanent daytime (who works only day time, morning or afternoon, for 6 h) and shift workers (who works nighttime, for 12 h).
• Education: lower education (primary schools), middle education (secondary schools) and higher education (bachelor’s, master’s and doctoral degrees).
• Tasks: administrative staff, call centre operators, production staff, distribution staff.
2.1 Stress assessment and occupational well-being
All participants in the study completed a self-administered questionnaire that included the questionnaire on organisational well-being proposed by the Italian National Anti-Corruption Authority (24). The questionnaire consists of several subscales, including the part on organisational wellbeing, the degree of sharing of the evaluation system and the evaluation of the hierarchical superior. To assess the reliability of each subscale, Cronbach’s α values were calculated, which were 0.81, 0.68 and 0.73, respectively, for organisational well-being, the degree of sharing of the evaluation system and the evaluation of the hierarchical superior (25).
Karasek’s taxonomy of jobs was used, which classifies various jobs into four different categories: passive jobs (low demands and low job control), low-tension jobs (low demands and high job control), high-tension jobs (high demands and low job control) and active jobs (high demands and high job control) (18). This classification is based on the combination of the demand and job control scores, comparing them with the median values in a two-by-two matrix. In addition, we classified the four categories of the work taxonomy according to high or low support from colleagues. Work support scores above or below the median were used to define high and low work support, respectively.
To measure the well-being of the study participants, we used the WHO-Five Well-Being Index (WHO-5), consisting of five items (26). These items assess feelings of cheerfulness, good mood, calmness, relaxation, vigour, freshness when waking up and engagement in daily activities. Participants rated each item on a 5-point scale ranging from 0 (never) to 5 (always), indicating the perceived frequency of experiencing each item over the past 2 weeks. The raw score was obtained by summing the individual scores for the five items. The theoretical range of the raw score is from 0 (indicating no well-being) to 25 (indicating maximum well-being). The internal reliability of this well-being subscale, as assessed by Cronbach’s α, was 0.84.
2.2 Cardiovascular risk assessment
We used the individual SCORE2 score calculation to calculate the absolute risk of CVD, expressed as a percentage probability, for each study participant (27). This score takes into account various concomitant risk factors, including gender, age, diabetes, smoking, systolic blood pressure, total cholesterol, and continent. The 10-year risk estimate provided by this model represents the probability of developing a significant CVD event, such as coronary death, myocardial infarction, coronary insufficiency, angina, ischaemic stroke, haemorrhagic stroke, transient ischaemic attack, peripheral artery disease or heart failure (28). It should be noted that this particular model is specifically applicable to individuals aged between 40 and 89 years who did not have a pre-existing diagnosis of CVD at baseline clinical examination (29).
It should be noted that individuals under 40 years of age are by definition identified as being at low cardiovascular risk unless there are congenital malformations or diseases (27).
Since blood lipid levels are not part of routine workplace health surveillance, we chose to use BMI instead, as recommended for the simplified Framingham Study risk scoring model BMI was calculated, based on the data declared in the anamnestic section of the questionnaire, according to which, by dividing the weight expressed in kilogrammes (kg) with the height expressed in metres squared, a value is obtained that indicates the extent of body weight, distinguishing the following conditions: severely underweight (BMI < 16.5), underweight (BMI between 16.00 and 18.49), normal weight (BMI between 18.5 and 24.99), overweight (BMI between 25.00 and 29.99), mild obesity—class I (BMI between 30.00 and 34.99), medium obesity—class II (BMI between 35.00 and 39.99), severe obesity—class III (BMI > 40.00) (22, 28). The CVD risk was then classified as low (<10%), moderate (10–20%) or high (>20%).
2.3 Statistical analysis
To analyse the data, we used various statistical techniques, including parametric and non-parametric descriptive techniques. To compare differences between the study groups, we used analysis of variance (ANOVA) or the Kruskal-Wallis test and Spearman correlation was used analysing the relationship between variables (30, 31).
To explore the relationship between work-related stress and the risk of CVD, we constructed a multiple regression model (32). This model considered various factors, such as job demands, job control and job support scores, while adjusting for education, alcohol intake, recreational physical activity and DBP. Furthermore, we used a linear regression model to predict the well-being index, taking into account work-related stress scores together with age, duration of employment, level of education, alcohol intake, smoking habit, BMI, SBP and DBP. In another regression model, we examined the predictive value of Karasek’s categories and job support, instead of stress scores, for both CVD risk and well-being. In this analysis, we also included shift time as an independent variable.
Statistical analysis was performed with the RStudio software (33). It was not necessary to receive confirmation from the Ethical Committee as the activity is ruled by the Law Decree (DL) 81/08 within the health promotion actions. However, all participants were fully informed about the study and written informed consent was obtained from those who chose to participate. The questionnaires were anonymous, coded and securely stored by the principal investigator (MC), who was the only person authorised to access them. The questionnaires were kept separate from the clinical records of each participant. The study complied with the principles of the Declaration of Helsinki (34).
3 Results
Table 1 provides an overview of the main characteristics of the study participants.
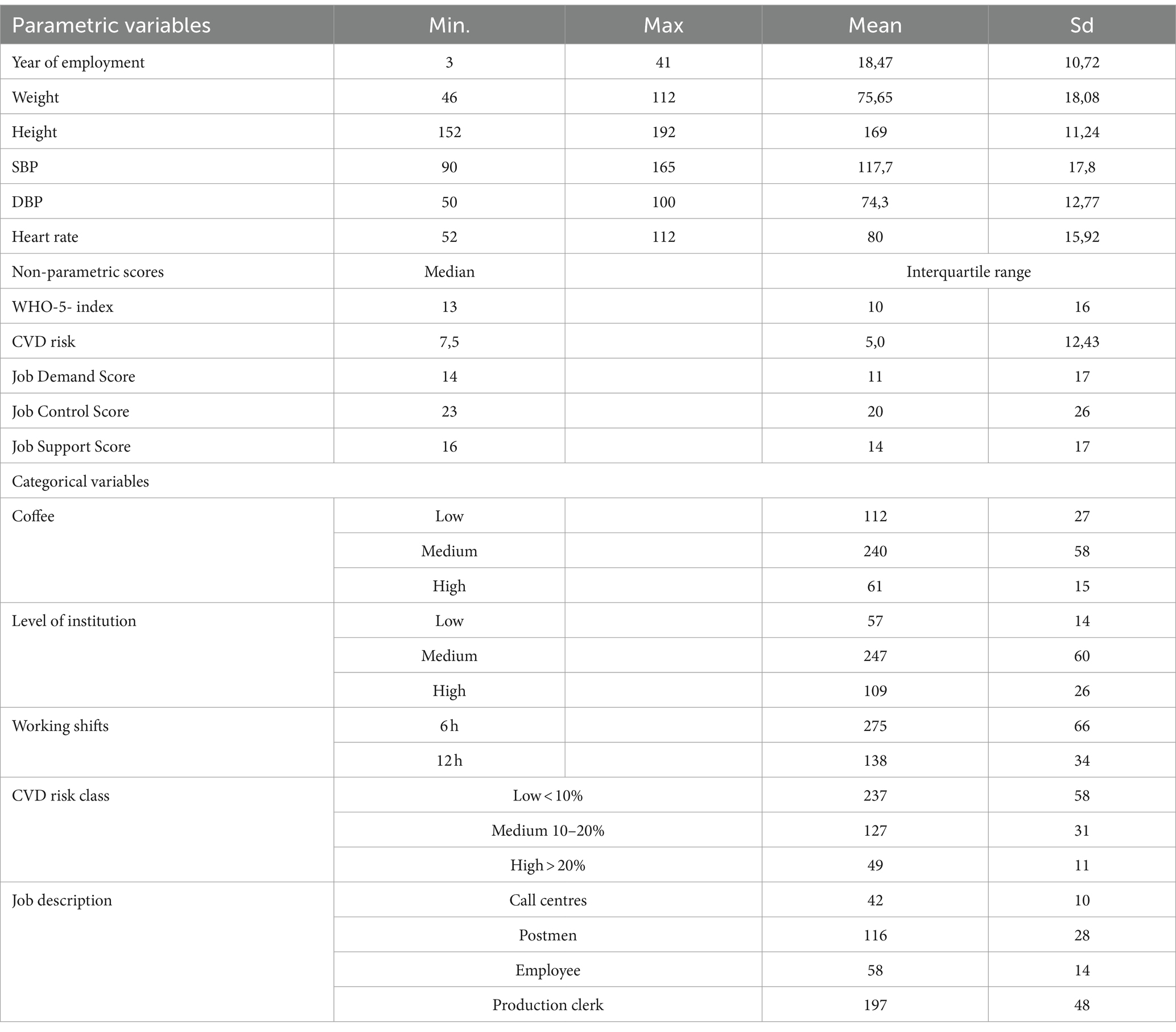
Table 1. The study population encompassed 413 participants, and data were accessible for all selected variables.
Among the 413 participants, 234 were male (57%) and 179 (35) female, the mean age was 43.27 years (standard deviation [sd] 13.23) and the mean BMI was 26.18 (sd 4.62).
Approximately 30% of the study population were habitual smokers, while 59% were classified as overweight. In addition, 16% of the participants regularly drank alcohol and 67% regularly engaged in recreational physical activity. It was found that 24.6% of the participants suffered from hypertension.
Figure 2 presents the distribution of the study subjects according to Karasek’s categories and job support categories. Passive jobs were less common, accounting cumulatively (call centres and office workers) for 28% of the sample, with none of the jobs falling into the low-voltage categories. Karasek’s categories were further divided according to job support, with 46% falling into the low-support category and 54% into the high-support category. The cut-off points for the work demand, control and support scores according to Karasek’s categorisation were 13, 24 and 15, respectively.
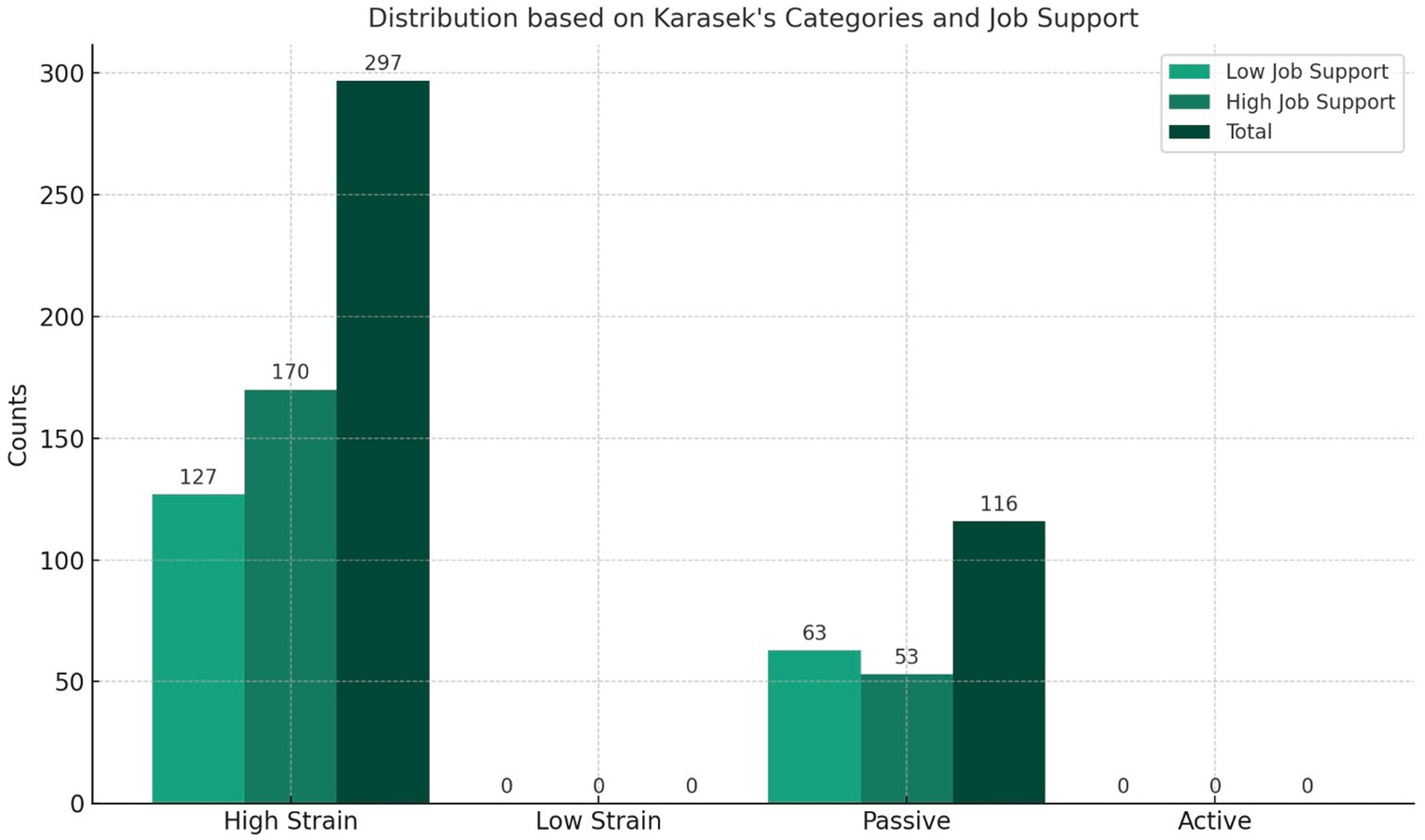
Figure 2. The overall study population’s distribution based on Karasek’s categories and Job support categories.
The subjects in the different Karasek and work support categories had similar characteristics in terms of age, duration of employment, BMI, SBP, DBP and heart rate (HR; not shown in the tables).
The study population was classified into different CVD risk levels in Table 2. Approximately 58% of the subjects were classified as low CVD risk (CVD risk <10%), approximately 31% were classified as moderate risk (CVD risk between 10 and 20%) and 11% were considered high risk (CVD risk >20%). The overall median CVD risk for the population was moderate (6.9%), with individual scores ranging from 1 to 58% (30).
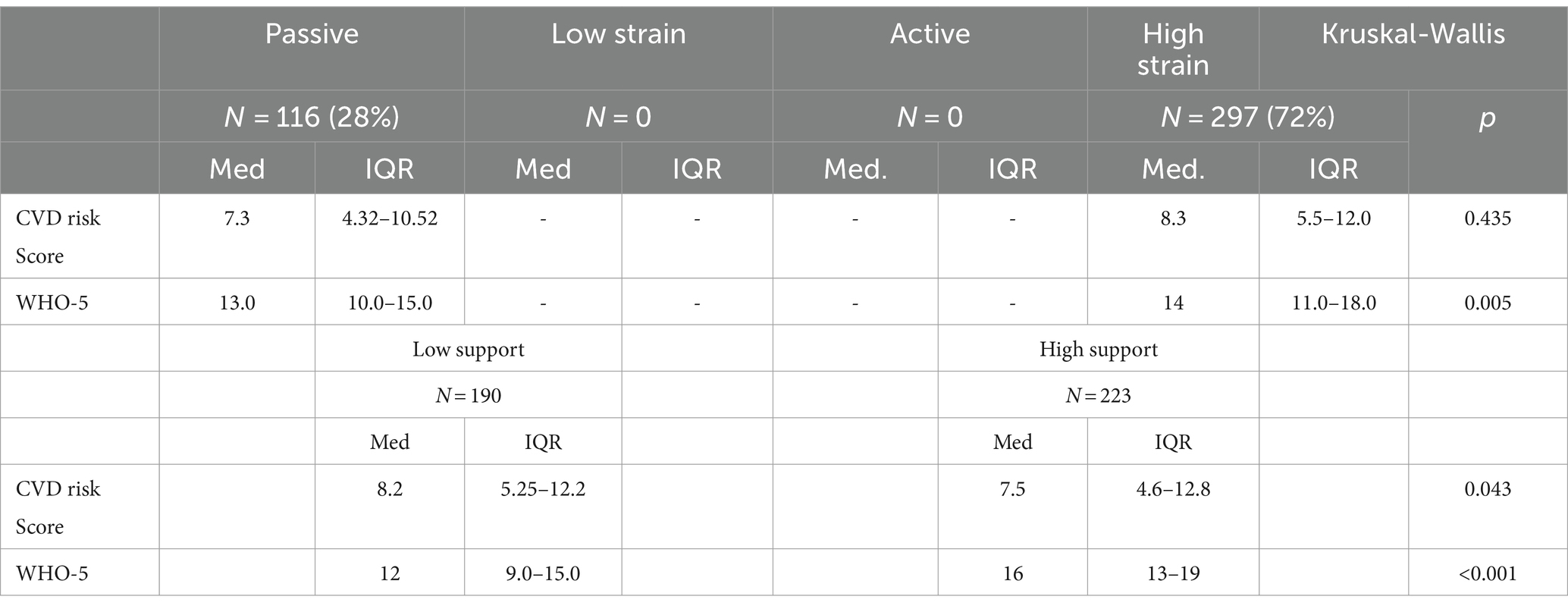
Table 2. Results from the Kruskal-Wallis test comparing CVD risk and WHO-5 among Karasek’s categories and Job support categories in the overall study population.
The passive job category showed lower values in the WHO well-being index than high-stress jobs (p = 0.005), as observed in Table 2.
The average CVD risk score did not exceed the low threshold in either of Karasek’s two categories in our sample. A low level of work support was moderately, but significantly associated with increased CVD risk scores and lower WHO well-being index, compared to high work support (Table 2; Figure 3).
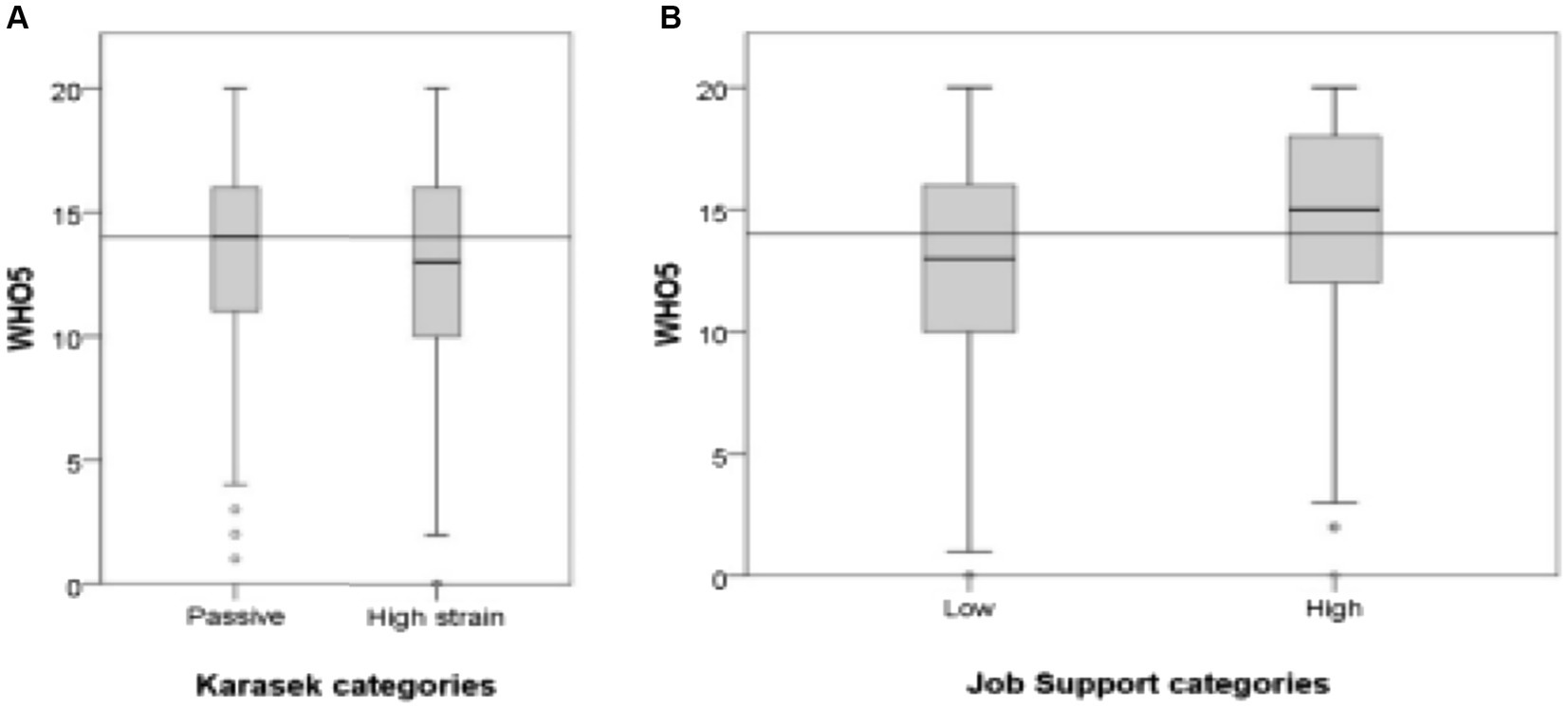
Figure 3. Primary median (depicted by the grey line) and box plots illustrating general well-being (WHO-5): within the four Karasek’s categories (A); and across job support categories (B).
The correlation matrix shown in Table 3 indicates that the CVD risk score was positively correlated with regular alcohol consumption (p = 0.023) and higher resting heart rate (p < 0.001), and negatively correlated with leisure-time physical activity (p ≤ 0.001), well-being index (p ≤ 0.001) and work support score (p = 0.037). In contrast, the WHO-5 well-being index was positively correlated with job control (p < 0.001) and job support (p < 0.001), and negatively correlated with job demand (p = 0.047).
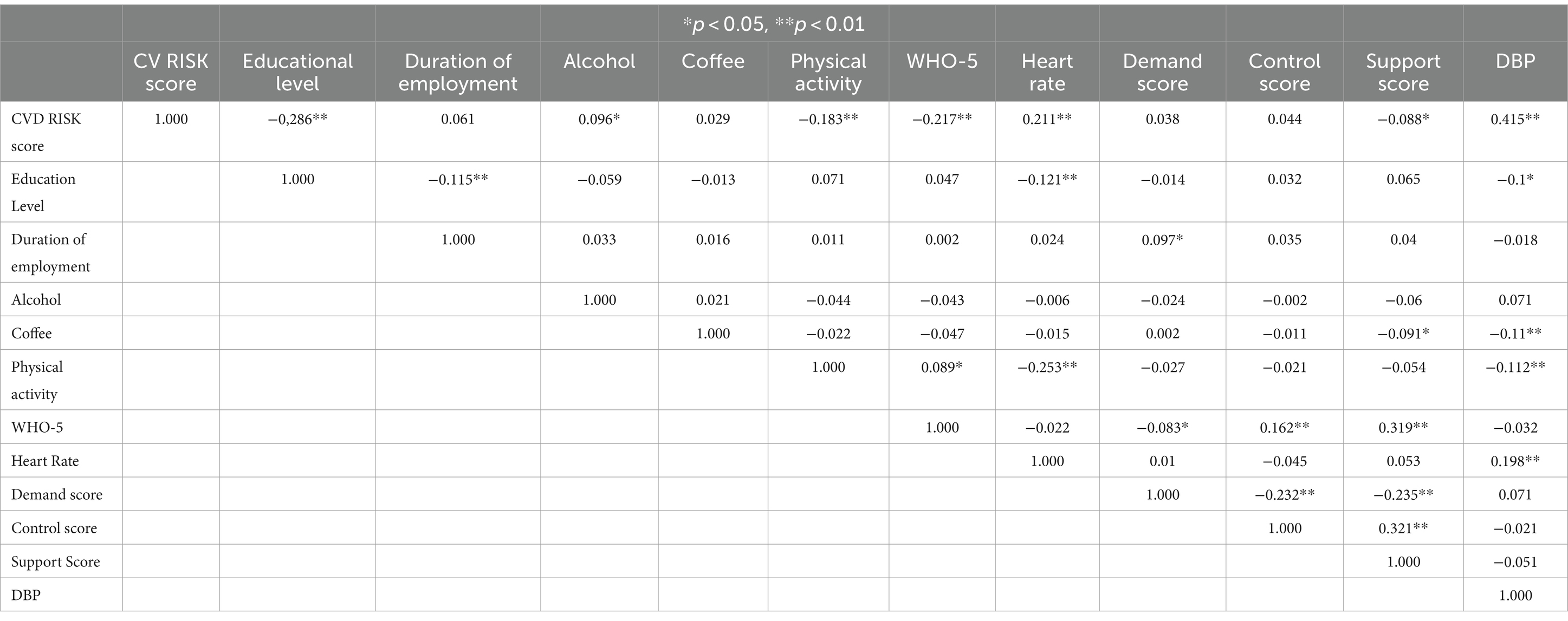
Table 3. Spearman correlation matrix (*p < 0.05; **p < 0.01).
DBP showed a strong correlation with SBP (Pearson’s correlation coefficient = 0.702, p < 0.001, not shown in Table 3) and a moderate correlation with CVD risk (Table 3).
The linear regression model for predicting CVD risk showed a negative effect of systolic blood pressure, low education level and physical inactivity, which tended to increase the risk of CVD. In contrast, a higher work support score protected against CVD risk, as did abstention or occasional consumption of alcoholic beverages (Table 4). The median values of the expected CVD risk, classified according to work support and Karasek categories, are presented in Table 5. When Karasek’s categories were entered instead of job application, control and support scores in the regression model for predicting CVD risk, no significant impact on CVD risk was observed (R2 = 0.279; adjusted R2 = 0.265).
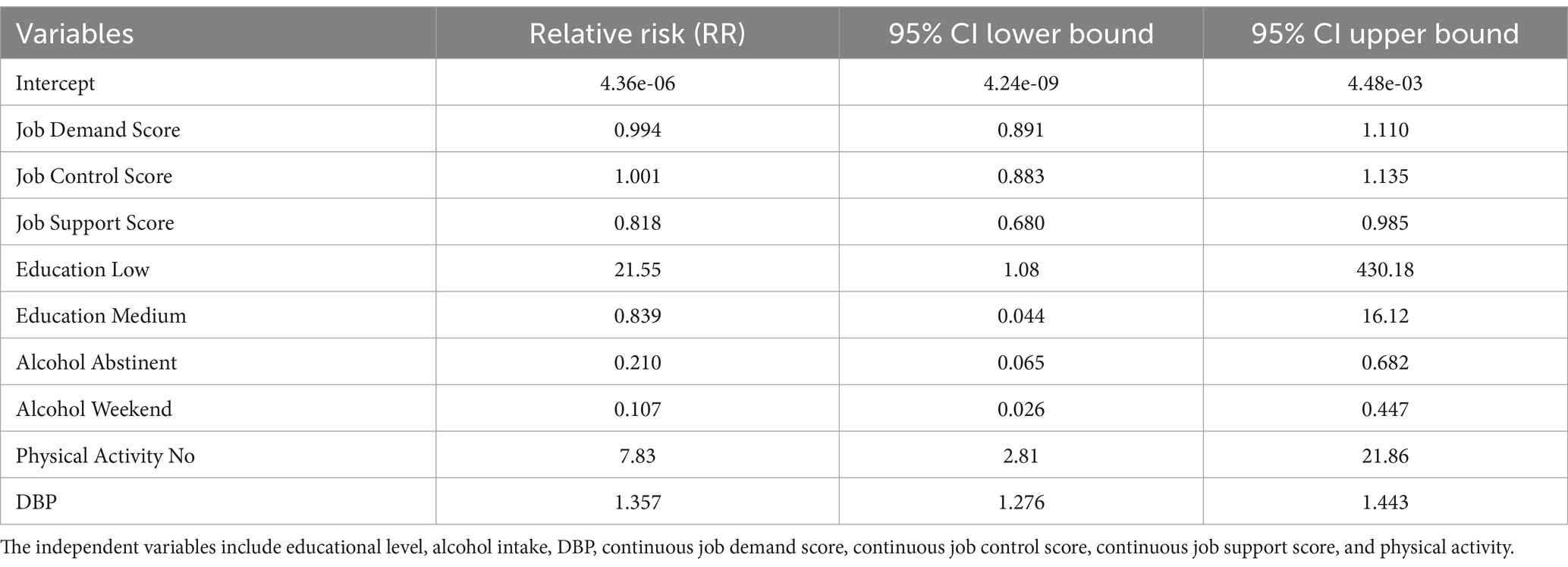
Table 4. Table summarising the Relative Risks (RR) and 95% Confidence Intervals for the variables considered.
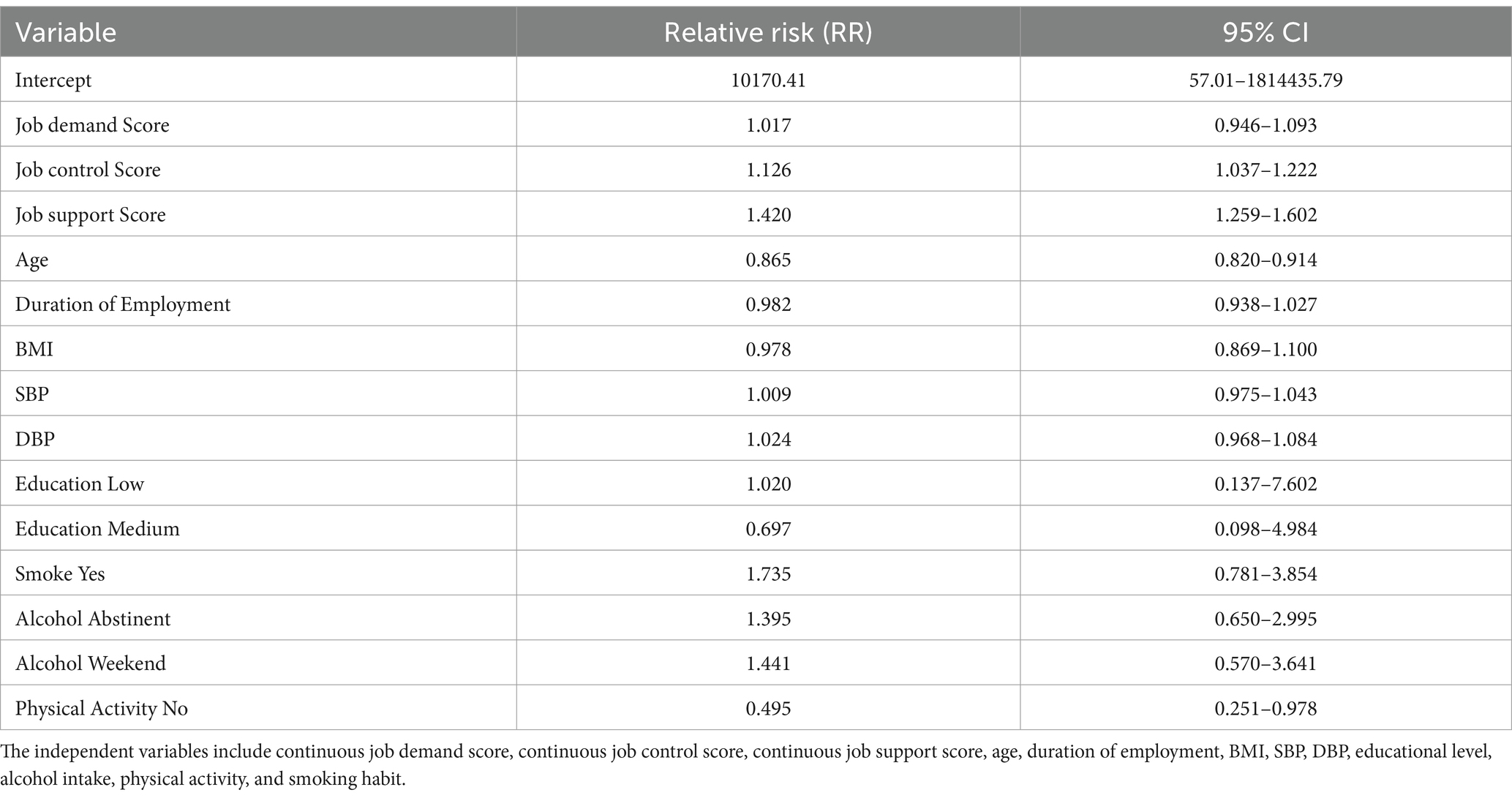
Table 5. Multiple linear regression model forecasting WHO-5 well-being (R2 = 0.1661; adjusted R2 = 0.1447).
A high score in work control and work support showed a positive effect on well-being, while older age and physical inactivity showed a negative effect (Table 5).
The median predicted CVD risk scores in the four Karasek categories and the two job support categories, based on the linear regression model, are shown in Table 6.

Table 6. Predicted median CVD risk scores in the four Karasek’s categories and the two job support categories, as per the linear regression model outlined in Table 4.
4 Discussion
In line with previous studies, our survey suggests a correlation between work support and lower CVD risk (36). Our results support the hypothesis that certain dimensions of work-related stress may have an impact on CVD risk (37). Specifically, modifiable and non-modifiable risk factors may contribute to an increased likelihood of developing CVD and experiencing decreased well-being in work environments where peer support is lacking (38, 39). In contrast, general well-being and work support have been reported to increase long-term survival rates among individuals with chronic heart disease (40).
Based on Karasek’s classical dimensions, when analysing the levels of work-related stress, the study population showed a three-quarter distribution represented by high-stress job categories. However, compared to similar studies conducted on mixed populations using the same assessment method, the median scores for job demands and job control in our logistics support company were higher (14 vs. 12 for job demands; 23 vs. 18 for job control). It is worth noting that high-stress jobs have been consistently associated with detrimental health outcomes, such as cardiac autonomy imbalance indicated by Heart Rate Variability, hypertension and metabolic syndrome (41–43). In our study population, we observed an impact of job stress on perceived well-being, but not statistically significant on CVD risk. It is conceivable that working in a company that provides distribution support does not involve physically demanding tasks that significantly influence the perception of job stress (44). With regard to the other known risk factors for CVD, our results are in line with previous reports showing a protective effect of education (35, 45). Education is often used as a surrogate for socioeconomic status in epidemiological studies, which in turn implies a higher likelihood of performing high-stress, low-control and low-support jobs (46).
Our results are also consistent with previous research indicating a possible influence of work-related stress dimensions on psychological well-being, independent of other potential confounders such as shift work. In fact, night shifts could lead to alterations in circadian rhythms with an increased risk of developing sleep disorders and psychiatric disorders (47, 48). However, it is possible that other factors not considered, such as domestic stress or job-specific factors (e.g., security personnel), influenced our results (49). In our study population, the prevalence of current smokers (30%) and overweight individuals (55.6%) exceeded the national averages in Italy (19.3 and 54.8%, respectively) (50, 51). We also observed a clear protective role of regular recreational physical activity in reducing the risk of CVD. Therefore, the implementation of health promotion strategies aimed at physical activity and smoking cessation in these workers could contribute to improved well-being and productivity (52, 53). Several workplaces have successfully introduced health promotion strategies focusing on physical activity and smoking cessation and achieved significant cardiovascular risk reduction (54–58). In our study population, the average probability of experiencing a major cardiovascular event within 10 years was 6.9 per cent. After suffering a major cardiovascular event, occupational physicians must consider the economic and social consequences for workers, including the ability to return to work, fitness for work, loss of productivity and loss of job skills (59). Simple CVD risk calculation tools, such as the one used in our study, can help occupational physicians identify otherwise healthy workers who may be susceptible to developing CVD during routine workplace health surveillance. These workers may in fact not feel the need to consult a medical specialist. Finally, the average age of our study population was 43.27 years (sd 13.23), suggesting a significant trend towards an ageing workforce, even in the logistics support sector. The ageing of the workforce is a shared reality in most developed economies and can have a negative impact on labour productivity (60). Consequently, active ageing has become a major concern in occupational medicine and public health (61, 62). It is important to recognise certain limitations that affect the interpretation of our results.
The cross-sectional design of our study inherently prevents drawing firm conclusions. In discussing the limitations of a study focused on a single logistics company, there are main concerns regarding the generalisability of the results. The applicability to different sectors suggests that the results obtained from a specific company in the logistics sector may not be directly applicable to other sectors or work contexts. Each sector has its own unique dynamics, work stresses, and working conditions that may affect worker well-being and health risks differently. Without a critical examination of how these results would translate to different contexts, the extent of their applicability remains uncertain. In addition, focusing on a single company raises questions about the representativeness of the study within the logistics sector as a whole. Working practices, company culture, and stress factors may vary significantly between companies within the same sector. This study may therefore reflect the peculiarities of that company’s specific working environment rather than providing a general picture applicable to all logistics companies.
To address these limitations, it would be useful to conduct comparative studies that include a wider range of companies within the logistics sector and, ideally, studies that examine different sectors to assess the consistency of the observed effects. In addition, subgroup analysis within the current study could provide insights into how various factors (such as type of work, age of workers, or level of education) influence the relationship between working conditions and worker well-being. These steps could improve the generalisability and applicability of the results to broader contexts.
Furthermore, we could not assess the role of stress and social support at home, which might interact with work-related stress to increase cardiovascular risk. Despite these limitations, an advantage of our study was to focus on the general mental and physical health status of the working population by combining the assessment of work-related stress with that of CVD risk. Adopting such a holistic approach allows occupational physicians to address modifiable factors, such as work stress management through work organisation interventions, as well as lifestyle factors. The current research contributes to the investigation of the intricate relationship between the theoretical frameworks that predict CVD risk and any observed early changes that precede disease manifestation to establish preventive strategies. Our findings propose that various dimensions of work-related stress have the potential to influence both CVD risk and the psychological well-being of individuals in the workforce. Modifiable factors such as coworker support, decision-making autonomy, nature of work performed, and shift work schedules should be considered when attempting to mitigate CVD risk through interventions targeting organisational stress and promoting healthy lifestyles. In recent years, the ageing of the workforce is a multifaceted phenomenon that requires careful consideration and new proactive strategies such as prevention campaigns for smoking, alcohol abuse and proper nutrition (63, 64). Occupational physician must adapt their practice to meet the health needs of workers at different stages of their careers. By embracing age diversity and implementing prevention policies, companies can capitalise on the strengths of a multi-generational workforce, fostering a culture of inclusion and innovation.
In addition to domestic stress and shift work, there may be numerous other unmeasured or unconsidered factors that could influence the results, such as pre-existing health conditions, lifestyle (e.g., diet, physical activity), and social support. Domestic stress, whether stemming from family responsibilities, financial concerns, or interpersonal conflicts, can take a toll on one’s cardiovascular well-being. Research indicates that chronic stress contributes to hypertension, inflammation, and other risk factors for heart disease (64). Employees with pre-existing health conditions, such as hypertension, diabetes, or obesity, face additional hurdles in maintaining cardiovascular health in the workplace. Healthy lifestyle choices, including balanced nutrition, regular sleep cycle and regular physical activity, play a pivotal role in preventing cardiovascular disease (65). Yet, busy work schedules and sedentary office environments often present barriers to maintaining these habits (66). Finally, social support plays a critical role in mitigating the impact of stress and promoting cardiovascular health. Strong support networks in the workplace can buffer against the negative effects of stress, providing individuals with resources and encouragement to cope effectively. Employers can facilitate social connections among employees through team-building activities, mentorship programs, and open communication channels. By fostering a supportive and inclusive work environment, employers can contribute to the overall well-being of their workforce and reduce the burden of cardiovascular disease (66). The lack of control for these factors may introduce bias into the results and limit the ability to attribute observed effects with certainty to the variables of interest studied. To overcome these limitations, future studies should consider adopting a more holistic approach that includes a wide range of potential confounders and utilises methods of data collection and statistical analysis capable of handling the complexity of interactions between various factors. This would improve the internal validity of the study and the relevance of its findings, providing a more complete and accurate understanding of the impact of job stress and other factors on worker well-being. In conclusion, further investigation, using a longitudinal study design but also correlation with biohumoral parameters as done in other studies, will be indispensable to affirm the hypothesis that specific indicators of work-related stress and general well-being may predict susceptibility to the development of cardiovascular diseases (67).
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was not required for the studies involving humans because Since the normal diagnostic care pathway was not changed, no therapies or drugs were administered, ethics committee approval was not required. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SF: Data curation, Formal analysis, Investigation, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. GM: Conceptualization, Data curation, Formal analysis, Investigation, Supervision, Writing – review & editing. MV: Data curation, Supervision, Validation, Visualization, Writing – review & editing. AC: Resources, Supervision, Validation, Visualization, Writing – review & editing. DM: Formal analysis, Supervision, Validation, Visualization, Writing – review & editing. EC: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
Authors thanks Luigi Cirrincione for the support provided.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ciumărnean, L, Milaciu, MV, Negrean, V, Orășan, OH, Vesa, SC, Sălăgean, O, et al. Cardiovascular risk factors and physical activity for the prevention of cardiovascular diseases in the elderly. Int J Environ Res Public Health. (2021) 19:207. doi: 10.3390/ijerph19010207
2. World Health Statistics (2022). Monitoring health for the SDGs Sustainable Development Goals-WHO. Accessed on 04 December 2023 at link: https://www.who.int/publications/i/item/9789240051157
3. Kondo, T, Nakano, Y, Adachi, S, and Murohara, T. Effects of tobacco smoking on cardiovascular disease. Circ J. (2019) 83:1980–5. doi: 10.1253/circj.CJ-19-0323
4. Elagizi, A, Kachur, S, Carbone, S, Lavie, CJ, and Blair, SN. A review of obesity, physical activity, and cardiovascular disease. Curr Obes Rep. (2020) 9:571–81. doi: 10.1007/s13679-020-00403-z
5. Tian, YE, Cropley, V, Maier, AB, Lautenschlager, NT, Breakspear, M, and Zalesky, A. Heterogeneous aging across multiple organ systems and prediction of chronic disease and mortality. Nat Med. (2023) 29:1221–31. doi: 10.1038/s41591-023-02296-6
6. Costantino, C, Cannizzaro, E, Verso, MG, Tramuto, F, Maida, CM, Lacca, G, et al. SARS-CoV-2 infection in healthcare professionals and general population during "first wave" of COVID-19 pandemic: a cross-sectional study conducted in Sicily. Italy Front Public Health. (2021) 9:644008. doi: 10.3389/fpubh.2021.644008
7. Cirrincione, L, Plescia, F, Ledda, C, Rapisarda, V, Martorana, D, Lacca, G, et al. COVID-19 pandemic: new prevention and protection measures. Sustain For. (2022) 14:4766. doi: 10.3390/su14084766
8. Protocollo di Intesa tra Società Italiana di Medicina del Lavoro, Farmaindustria, Assogenerici”. Quotidiano Sanità (2019). Accessible on 29 February 2024 at link: https://www.quotidianosanita.it/allegati/allegato5773402.pdf
9. Maida, CM, Tramuto, F, Di Naro, D, Randazzo, G, Stefanelli, P, et al. First detection of SARS-CoV-2 a.23.1 sub-lineage in migrants arriving to Italy via the Mediterranean Sea and public health implications. Travel Med Infect Dis. (2021) 43:102142. doi: 10.1016/j.tmaid.2021.102142
10. Cannizzaro, E, Cirrincione, L, Malta, G, Fruscione, S, Mucci, N, Martines, F, et al. The influence of the COVID-19 pandemic emergency on alcohol use: a focus on a cohort of Sicilian workers. Int J Environ Res Public Health. (2023) 20:4613. doi: 10.3390/ijerph20054613
11. Talini, D, and Baldasseroni, A. Workplace health promotion. Med Lav. (2019) 110:321–4. doi: 10.23749/mdl.v110i4.8525
12. Santana, AIC, Merces, MCD, Magalhães, LBNC, Costa, ALB, and D'Oliveira, A. Association between metabolic syndrome and work: an integrative review of the literature. Rev Bras Med Trab. (2020) 18:185–93. doi: 10.47626/1679-4435-2020-511
13. Ledda, C, Cinà, D, Matera, S, Mucci, N, Bracci, M, and Rapisarda, V. High HOMA-IR index in healthcare shift workers. Medicina (Kaunas). (2019) 55:186. doi: 10.3390/medicina55050186
14. Rapisarda, V, Cannizzaro, E, Barchitta, M, Vitale, E, Cinà, D, Minciullo, F, et al. A combined multidisciplinary intervention for Health promotion in the workplace: a pilot study. J Clin Med. (2021) 10:1512. doi: 10.3390/jcm10071512
15. Pang, Q, Fang, M, Wang, L, Mi, K, and Su, M. Increasing Couriers' job satisfaction through social-sustainability practices: perceived fairness and psychological-safety perspectives. Behav Sci (Basel, Switzerland). (2023) 13:125. doi: 10.3390/bs13020125
16. Qiu, XY, Dai, H, Yu, XT, Wu, CL, and Qiu, YB. Zhonghua lao dong wei sheng zhi ye bing za zhi = Zhonghua laodong weisheng zhiyebing zazhi =. Chinese J Indus Hygiene Occup Dis. (2019) 37:446–9. doi: 10.3760/cma.j.issn.1001-9391.2019.06.010
17. Häusser, JA, Schulz-Hardt, S, and Mojzisch, A. The active learning hypothesis of the job-demand-control model: an experimental examination. Ergonomics. (2014) 57:23–33. doi: 10.1080/00140139.2013.854929
18. Magnavita, N. Two tools for health surveillance of job stress: the Karasek job content questionnaire and the Siegrist effort reward imbalance questionnaire. G Ital Med Lav Ergon. (2007) 29:667–70.
19. Alves, MG, Hökerberg, YH, and Faerstein, E. Trends and diversity in the empirical use of Karasek's demand-control model (job strain): a systematic review. Rev Bras Epidemiol. (2013) 16:125–36. doi: 10.1590/s1415-790x2013000100012
20. Canivet, C, Choi, B, Karasek, R, Moghaddassi, M, Staland-Nyman, C, and Östergren, PO. Can high psychological job demands, low decision latitude, and high job strain predict disability pensions? A 12-year follow-up of middle-aged Swedish workers. Int Arch Occup Environ Health. (2013) 86:307–19. doi: 10.1007/s00420-012-0766-4
21. Perini, F. Il decreto legislativo n. 81/2008. Sulla tutela della salute e della sicurezza nei luoghi di lavoro [The legislative decree n. 81/2008 on health and safety in workplaces]. Epidemiol Prev. (2008) 32:201–4.
22. Weir, CB, and Jan, A. BMI classification percentile and cut off points In: StatPearls. Treasure Island, FL: StatPearls Publishing (2024).
23. Krause, T, Lovibond, K, Caulfield, M, McCormack, T, and Williams, B. Guideline development group. Management of hypertension: summary of NICE guidance. BMJ. (2011) 343:d4891. doi: 10.1136/bmj.d4891
24. Emanuel, F, Bertola, L, and Colombo, L. The evaluation of organizational well-being in the public sector: an integration of the ANAC questionnaire. Med Lav. (2018) 16:132–44. doi: 10.23749/mdl.v109i2.6669
25. Alkhadim, GS. Cronbach's alpha and semantic overlap between items: a proposed correction and tests of significance. Front Psychol. (2022) 13:815490. doi: 10.3389/fpsyg.2022.815490
26. Topp, CW, Østergaard, SD, Søndergaard, S, and Bech, P. The WHO-5 well-being index: a systematic review of the literature. Psychother Psychosom. (2015) 84:167–76. doi: 10.1159/000376585
27. SCORE2 working group and ESC Cardiovascular risk collaboration. SCORE2 risk prediction algorithms: new models to estimate 10-year risk of cardiovascular disease in Europe. Eur Heart J. (2021) 42:2439–54. doi: 10.1093/eurheartj/ehab309
28. Hageman, SHJ, Petitjaen, C, Pennells, L, Kaptoge, S, Pajouheshnia, R, Tillmann, T, et al. Improving 10-year cardiovascular risk prediction in apparently healthy people: flexible addition of risk modifiers on top of SCORE2. Eur J Prev Cardiol. (2023) 30:1705–14. doi: 10.1093/eurjpc/zwad187
29. Hemann, BA, Bimson, WF, and Taylor, AJ. The Framingham risk score: an appraisal of its benefits and limitations. Am Heart Hosp J. (2007) 5:91–6. doi: 10.1111/j.1541-9215.2007.06350.x
30. Armstrong, RA, Eperjesi, F, and Gilmartin, B. The application of analysis of variance (ANOVA) to different experimental designs in optometry. Ophthalmic Physiol Opt. (2002) 22:248–56. doi: 10.1046/j.1475-1313.2002.00020.x
31. Guo, S, Zhong, S, and Zhang, A. Privacy-preserving Kruskal-Wallis test. Comput Methods Programs Biomed. (2013) 112:135–45. doi: 10.1016/j.cmpb.2013.05.023
32. Marill, KA. Advanced statistics: linear regression, part II: multiple linear regression. Acad Emerg Med. (2004) 11:94–102. doi: 10.1197/j.aem.2003.09.006
33. Core Team R. R: A language and environment for statistical computing. (2024). Available at: https://www.R-project.org/
34. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. (2013) 310:2191–4. doi: 10.1001/jama.2013.281053
35. Schultz, WM, Kelli, HM, Lisko, JC, Varghese, T, Shen, J, Sandesara, P, et al. Socioeconomic status and cardiovascular outcomes: challenges and interventions. Circulation. (2018) 137:2166–78. doi: 10.1161/CIRCULATIONAHA.117.029652
36. Cesana, G, Sega, R, Ferrario, M, Chiodini, P, Corrao, G, and Mancia, G. Job strain and blood pressure in employed men and women: a pooled analysis of four northern italian population samples. Psychosom Med. (2003) 65:558–63. doi: 10.1097/01.psy.0000041473.03828.67
37. Kivimäki, M, and Kawachi, I. Work stress as a risk factor for cardiovascular disease. Curr Cardiol Rep. (2015) 17:630. doi: 10.1007/s11886-015-0630-8
38. Restrepo, J, and Lemos, M. Addressing psychosocial work-related stress interventions: a systematic review. Work. (2021) 70:53–62. doi: 10.3233/WOR-213577
39. Sara, JD, Prasad, M, Eleid, MF, Zhang, M, Widmer, RJ, and Lerman, A. Association between work-related stress and coronary heart disease: a review of prospective studies through the job strain. Effort-Reward Balance, and Organiz Justice Models J Am Heart Assoc. (2018) 7:e008073. doi: 10.1161/JAHA.117.008073
40. Kubzansky, LD, Huffman, JC, Boehm, JK, Hernandez, R, Kim, ES, Koga, HK, et al. Positive psychological well-being and cardiovascular disease: JACC Health promotion series. J Am Coll Cardiol. (2018) 72:1382–96. doi: 10.1016/j.jacc.2018.07.042
41. Thayer, JF, Yamamoto, SS, and Brosschot, JF. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int J Cardiol. (2010) 141:122–31. doi: 10.1016/j.ijcard.2009.09.543
42. Babu, GR, Jotheeswaran, AT, Mahapatra, T, Mahapatra, S, Kumar, A Sr, Detels, R, et al. Is hypertension associated with job strain? A meta-analysis of observational studies. Occup Environ Med. (2014) 71:220–7. doi: 10.1136/oemed-2013-101396
43. Li, W, Yi, G, Chen, Z, Dai, X, Wu, J, Peng, Y, et al. Is job strain associated with a higher risk of type 2 diabetes mellitus? A systematic review and meta-analysis of prospective cohort studies. Scand J Work Environ Health. (2021) 47:249–57. doi: 10.5271/sjweh.3938
44. Cortés-Denia, D, Isoard-Gautheur, S, Lopez-Zafra, E, and Pulido-Martos, M. Effects of vigor at work and weekly physical activity on job stress and mental health. Sci Rep. (2022) 12:16025. doi: 10.1038/s41598-022-19966-z
45. Petrelli, A, Sebastiani, G, Di Napoli, A, Macciotta, A, Di Filippo, P, et al. Education inequalities in cardiovascular and coronary heart disease in Italy and the role of behavioral and biological risk factors. Nutr Metab Cardiovasc Dis. (2022) 32:918–28. doi: 10.1016/j.numecd.2021.10.022
46. Cohen, SS, Mumma, MT, Ellis, ED, and Boice, JD Jr. Validating the use of census data on education as a measure of socioeconomic status in an occupational cohort. Int J Radiat Biol. (2022) 98:587–92. doi: 10.1080/09553002.2018.1549758
47. Cirrincione, L, Plescia, F, Malta, G, Campagna, M, Lecca, LI, Skerjanc, A, et al. Evaluation of correlation between sleep and psychiatric disorders in a population of night shift workers: a pilot study. Int J Environ Res Public Health. (2023) 20:3756. doi: 10.3390/ijerph20043756
48. Malta, G., Fruscione, S., Albano, G.D., Zummo, L., Zerbo, S., et al. (2023). Shift work and altered sleep: A complex and joint interaction between neurological and occupational medicine. Euromediterranean Biomedical Journal.
49. Consoli, SM. Stress professionnel et infarctus du myocarde [occupational stress and myocardial infarction]. Presse Med. (2015) 44:745–51. doi: 10.1016/j.lpm.2015.05.006
50. Abitudine al fumo - Sorveglianza Passi. ISS. (2024). Available at: https://www.epicentro.iss.it/passi/dati/fumo#:~:text=In%20Italia%2C%20la%20maggioranza%20degli,consumano%20pi%C3%B9%20di%20un%20pacchetto
51. Masocco, M, Minardi, V, Contoli, B, Minelli, G, Manno, V, Cobellis, L, et al. Sovrappeso e obesità nella popolazione adulta in Italia: trend temporali, differenze socio-anagrafiche e regionali con focus sulla Regione Campania. Boll Epidemiol Naz. (2023) 4:1–8. doi: 10.53225/BEN_059
52. An, HY, Chen, W, Wang, CW, Yang, HF, Huang, WT, and Fan, SY. The relationships between physical activity and life satisfaction and happiness among young, middle-aged, and older adults. Int J Environ Res Public Health. (2020) 17:4817. doi: 10.3390/ijerph17134817
53. Espinosa-Salas, S, and Gonzalez-Arias, M. Behavior modification for lifestyle improvement In: StatPearls. Treasure Island, FL: StatPearls Publishing (2024).
54. Makar, O, and Siabrenko, G. Influence of physical activity on cardiovascular system and prevention of cardiovascular diseases (review). Georgian Med News. (2018) 285:69–74.
55. Ger0man, C, Makarem, N, Fanning, J, Redline, S, Elfassy, T, et al. Sleep, sedentary behavior, physical activity, and cardiovascular Health: MESA. Med Sci Sports Exerc. (2021) 53:724–31. doi: 10.1249/MSS.0000000000002534
56. Franco, M, Cooper, RS, Bilal, U, and Fuster, V. Challenges and opportunities for cardiovascular disease prevention. Am J Med. (2011) 124:95–102. doi: 10.1016/j.amjmed.2010.08.015
57. Matera, S, Filetti, V, Rapisarda, V, Kaźmierczak-Siedlecka, K, Rapisarda, L, Dounias, G, et al. Workplace health promotion: results of a combined multidisciplinary intervention over a long period - preliminary results. Eur Rev Med Pharmacol Sci. (2023) 27:9346–54. doi: 10.26355/eurrev_202310_33962
58. Caponnetto, P, Maglia, M, Floresta, D, Ledda, C, Vitale, E, Polosa, R, et al. A randomized controlled trial to compare group motivational interviewing to very brief advice for the effectiveness of a workplace smoking cessation counseling intervention. J Addict Dis. (2020) 38:465–74. doi: 10.1080/10550887.2020.1782564
59. Oldridge, NB. Economic burden of physical inactivity: healthcare costs associated with cardiovascular disease. Eur J Cardiovasc Prev Rehabil. (2008) 15:130–9. doi: 10.1097/HJR.0b013e3282f19d42
60. Ross, D. Ageing and work: an overview. Occup Med (Lond). (2010) 60:169–71. doi: 10.1093/occmed/kqq029
61. Robertson, A, and Tracy, CS. Health and productivity of older workers. Scand J Work Environ Health. (1998) 24:85–97. doi: 10.5271/sjweh.284
62. Health, TLP. Ageing: a 21st century public health challenge? Lancet Public Health. (2017) 2:e297. doi: 10.1016/S2468-2667(17)30125-1
63. Beach, B. Ageing populations and changing worlds of work. Maturitas. (2014) 78:241–2. doi: 10.1016/j.maturitas.2014.05.011
64. Rudnicka, E, Napierała, P, Podfigurna, A, Męczekalski, B, Smolarczyk, R, and Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas. (2020) 139:6–11. doi: 10.1016/j.maturitas.2020.05.018
65. Lo Coco, D, Cupidi, C, Mattaliano, A, Baiamonte, V, Realmuto, S, and Cannizzaro, E. REM sleep behavior disorder in a patient with frontotemporal dementia. Neurolog Sci: Official J Italian Neurolog Society and of the Italian Society of Clin Neurophysiol. (2012) 33:371–3. doi: 10.1007/s10072-011-0702-5
66. Golaszewski, NM, LaCroix, AZ, Godino, JG, Allison, MA, Manson, JE, King, JJ, et al. Evaluation of social isolation, loneliness, and cardiovascular disease among older women in the US. JAMA Netw Open. (2022) 5:e2146461. doi: 10.1001/jamanetworkopen.2021.46461
Keywords: occupational medicine and hygiene, risk, job, cardiovascular prevention, occupational health, prevention
Citation: Fruscione S, Malta G, Verso MG, Calascibetta A, Martorana D and Cannizzaro E (2024) Correlation among job-induced stress, overall well-being, and cardiovascular risk in Italian workers of logistics and distribution. Front. Public Health. 12:1358212. doi: 10.3389/fpubh.2024.1358212
Edited by:
Stefano Palermi, University of Naples Federico II, ItalyReviewed by:
Sofiane Kab, INSERM US11 Cohortes Epidémiologiques en population, FranceVenerando Rapisarda, University of Catania, Italy
Copyright © 2024 Fruscione, Malta, Verso, Calascibetta, Martorana and Cannizzaro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Santo Fruscione, c2FudG8uZnJ1c2Npb25lQHVuaXBhLml0