 Delong Chen1
Delong Chen1 Guanggao Zhao1*
Guanggao Zhao1* Jinmei Fu2Sunli Shun2
Jinmei Fu2Sunli Shun2 Liqiang Su3
Liqiang Su3 Zihao He4Ruiming Chen1Tianle Jiang1Xuewen Hu1Yunong Li1Fanchao Shen1
Zihao He4Ruiming Chen1Tianle Jiang1Xuewen Hu1Yunong Li1Fanchao Shen1- 1School of Physical Education, Nanchang University, Nanchang, China
- 2Jiangxi Sports Science and Medicine Center, Nanchang, China
- 3Physical Education College, Jiangxi Normal University, Nanchang, China
- 4School of Sports and Human Sciences, Beijing Sport University, Beijing, China
Background: It has been suggested that higher levels of fundamental motor skills (FMS) promote the physical health of preschool-aged children. The impacts of structured and unstructured interventions on FMS in children aged 10–16 years have been widely acknowledged in previous studies. However, there is a lack of relevant studies in preschool-aged children.
Objective: This meta-analysis aimed to compare the effects of structured and unstructured interventions on FMS in preschool-aged children.
Methods: The PubMed, Web of Science, and Google Scholar databases were searched from inception to 1 November 2023 to identify experiments describing structured and unstructured interventions for FMS in preschool-aged children. The Downs and Black Checklist was used to assess the risk of bias. A random effects model was used for the meta-analysis to evaluate the pooled effects of interventions on FMS. Subgroup analyses based on the duration and characteristics of the intervention were conducted to identify sources of heterogeneity.
Results: A total of 23 studies with 4,068 participants were included. There were 12 studies examining structured interventions, 9 studies examining unstructured interventions, and 6 studies comparing structured vs. unstructured interventions. The risk of bias in the included studies was generally low. All interventions significantly improved FMS in preschool-aged children compared to control treatments (p < 0.05). Structured interventions had more significant effects on locomotor skills (LMSs) in preschool-aged children than unstructured interventions (Hedges’ g = 0.44, p = 0.04). The effects of structured interventions were strongly influenced by the total intervention duration, such that long-term interventions were more effective (Hedge’s g = 1.29, p < 0.001).
Conclusion: Structured interventions play a crucial role in enhancing FMS among young children, especially when considering LMSs. These interventions require consistent and repeated practice over time to reach proficiency.
Systematic review registration:: PROSPERO, identifier number CRD42023475088, https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023475088.
1 Introduction
Fundamental motor skills (FMS) are the basis for children to perform more complex movements (1). Furthermore, achieving FMS can ensure normal development and help to maintain health (2). FMS are usually divided into locomotor skills (LMS) (e.g., running and jumping) and object control skills (OCS) (e.g., catching and throwing) (1). In addition, FMS are closely related to the maintenance of physical activity levels (3), physical fitness (4), overweight and obesity (5), rapid brain development and neuromuscular maturity (6), cognitive and social development (2), and other developmental indicators. FMS are considered the foundation for an active lifestyle (7).
FMS among children—especially jumping ability—have declined over a 13-year period, according to a trend survey (8). Moreover, 9.2% of children exhibited below-average FMS scores (9), with lower FMS scores observed in poverty areas compared to low-poverty areas (10, 11). Because early school age is considered a window of opportunity for developing FMS (12), it is important to promote FMS during the first years of life (13). While all children develop a rudimentary fundamental motor pattern over time, mature patterns of FMS do not develop naturally (14). Implementing effective FMS interventions in school-aged children helps maintain a healthy level and reduces the risk of future adverse conditions.
Currently, the World Health Organization (WHO) (15), the National Association for Sport and Physical Education (NASPE) (16), and organizations such as the National Physical Activity Plan Alliance (NPAPA) (17) emphasize the importance of structured and unstructured activities for preschool-aged children to achieve health requirements. Structured interventions include school physical education (PE), school/club sports programs, and active after-school care. Unstructured interventions include active travel, active play, and informal games. Previous studies have shown that structured interventions are more effective than unstructured interventions in terms of improving FMS in girls aged 10–16 years (18).
Previous meta-analyses focused solely on summarizing the effects of either structured or unstructured interventions on FMS in preschool-aged children. Notably, studies have examined the impact of PE on FMS in preschool-aged children (19) and the influence of active play on FMS (20). However, no meta-analyses have examined both structured and unstructured interventions. While some experimental studies have compared these structured and unstructured interventions in preschool settings, they have yielded inconsistent results (21, 22). Therefore, it is necessary to consolidate and analyze the effects of existing structured and unstructured interventions on FMS in preschool-aged children.
This meta-analysis examined the impacts of structured and unstructured interventions on the development of FMS in preschool-aged children. This research aimed to establish a foundational understanding for future targeted health promotion interventions.
2 Methods
The study was performed in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines (23). The inclusion/exclusion criteria and analytical methods were specified and registered in PROSPERO (http://www.crd.york.ac.UK/PROSPERO) before the study was initiated (PROSPERO reference number CRD42023475088).
2.1 Search strategy
The PubMed, Web of Science, and Google Scholar electronic databases were searched from inception to 1 November 2023. The search strategy was developed based on the eligibility criteria and outcomes of interest. In addition, the bibliographies of all eligible original papers and reviews were manually searched. The search terms were as follows: ‘fundamental motor skills’, ‘gross motor skills’, ‘locomotor skills’, ‘object* skills’, and ‘young children’. The search strategies and results returned for each database are shown in the Supplementary Table S1. Two researchers independently identified relevant articles by screening titles and reviewing abstracts (CDL and CRM). Two reviewers (CDL and CRM) examined the full texts of the articles for eligibility.
2.2 Inclusion and exclusion criteria
We developed the following inclusion criteria in accordance with the PICOS approach (24): (1) participants: preschoolers (2–6 years of age); (2) interventions: any type of structured or unstructured intervention aimed at increasing FMS; (3) control group: usual child care or kindergarten classes or another intervention strategy; (4) outcome: inclusion of FMS test metrics (total FMS score [total FMS], LMS, and OCS); (5) study design: an intervention trial with an intervention duration longer than 4 weeks (randomized controlled trial [RCT], cluster randomized controlled trials [CRT], or comparative studies in which the sample is randomized, and non-RCTs).
The exclusion criteria were as follows: (1) literature not published in Chinese or English; (2) reviews or studies missing key data; (3) non-controlled studies; and (4) non-controlled trials.
2.3 Data extraction
One author (CDL) extracted the following information from each eligible study: study background (name of the first author, year, and study location), sample characteristics (number of participants, age of participants, and number of girls and boys), design [intervention (RCT or non-RCT)], and instruments used to assess FMS outcomes. We also recorded the number of weeks of intervention, the duration and frequency of the interventions, and the descriptions of the interventions.
2.4 Criteria for risk of bias assessment
Two researchers (CRM and JTL) individually evaluated the risk of bias for each eligible study. Any disagreements were resolved through a consensus meeting. To determine the interrater agreement for the risk of bias assessment, the percentage agreement between the evaluators (CRM and JTL) was calculated. SPSS software version 26.0 (IBM Corporation, Armonk, NY, United States) was used to calculate the intraclass correlation coefficient (ICC) analysis.
Two independent researchers (CRM and JTL) assessed the full studies for bias using the Downs and Black checklist (25). The Downs and Black Checklist was used to evaluate the risk of bias for non-randomized and randomized control trials. The checklist consists of 27 items. The majority of questions were rated as either “yes” (= 1) or “unable to determine/no” (= 0), except for item five, which was rated on a 3-point scale (yes = 2, partial = 1, and no = 0). The maximum score was 32, with higher scores indicating better quality. The quality of the studies was classified as excellent (≥26), good (18–23), fair (13–17), or poor (≤14).
2.5 Meta-analysis of intervention studies
A meta-analysis was performed using STATA 15.0 statistical software (produced by Stata Corp, https://www.stata.com/). When different studies used different measurement methods and tools, Hedges’ g and 95% CI were used to measure the effect size. According to Cohen’s (1988) classification of effect sizes, a value less than 0.2 indicates a small effect, a value between 0.2 and 0.79 indicates a medium effect, and a value greater than or equal to 0.80 indicates a large effect (26). Calculations were performed using the Cochrane Handbook method for assessing the effective sample size for CRT (27). The ICC was estimated to be 0.031 (28). The sample sizes calculated using this method are presented in Supplementary Table S2. The pooled ES of the effect was determined using random effects models. A p-value of <0.05 and 95% confidence intervals (CIs) were used as criteria for identifying significant differences. Additionally, to understand the effectiveness of the intervention modality, we compared the changes from baseline to endpoint data between groups. The formulas for the mean and SD from pre- to post-change values were as follows: Meanchange = Meanpost – Meanpre and SDchange = SQRT [(SDpre2 + SDpost2) – (2 × Corr × SDpre × SDpost)], with the correlation coefficient set at 0.5 based on the Cochrane Collaboration Handbook guidelines (29). To distinguish the effect errors caused by different clusters, subgroup analyses were performed based on different outcome indicators (total FMS, LMS, and OCS). In multiarm studies (21, 22), the experimental group is compared to the control group in pairs (e.g., in a three-arm study, experimental group 1 is compared to the control group, experimental group 2 is compared to the control group, and experimental group 1 is compared to experimental group 2). Moreover, in the meta-analysis, the sample size of the control group was recorded only once during the statistical analysis to avoid artificially inflating the true sample size (21, 22).
Heterogeneity (i.e., the degree of variation between studies) was determined using the I2 statistic. I2 values <25, 50, and 75% were considered to indicate low, moderate, and high heterogeneity, respectively (30). To evaluate the likelihood of publication bias, funnel plots were generated, and Egger’s test was performed.
2.6 Subgroup analyses
First, we classified three outcome indicators (total FMS, LMS, and OCS). We subsequently conducted subgroup analyses based on the characteristics of the different interventions. Since structured interventions have a defined dose and duration, we used different intervention durations for the corresponding subgroup analysis. The total intervention duration was divided into three categories: (0, 1,100) min, (1,100, 3,000) min, and (3,000, +∞) min.
Unstructured interventions involve many steps, and according to the characteristics of the intervention, they can be divided into changing the environment, providing official policy guidance, and an unstructured curriculum.
3 Results
3.1 Selection process
A total of 51,440 relevant studies were retrieved, and 23 works were ultimately included based on the inclusion and exclusion criteria. The screening process is shown in Figure 1. In total, 14 randomized controlled trials (22, 31–43), eight cluster randomized controlled trials (21, 44–50), and one clinical trial (51) were included in the meta-analysis.
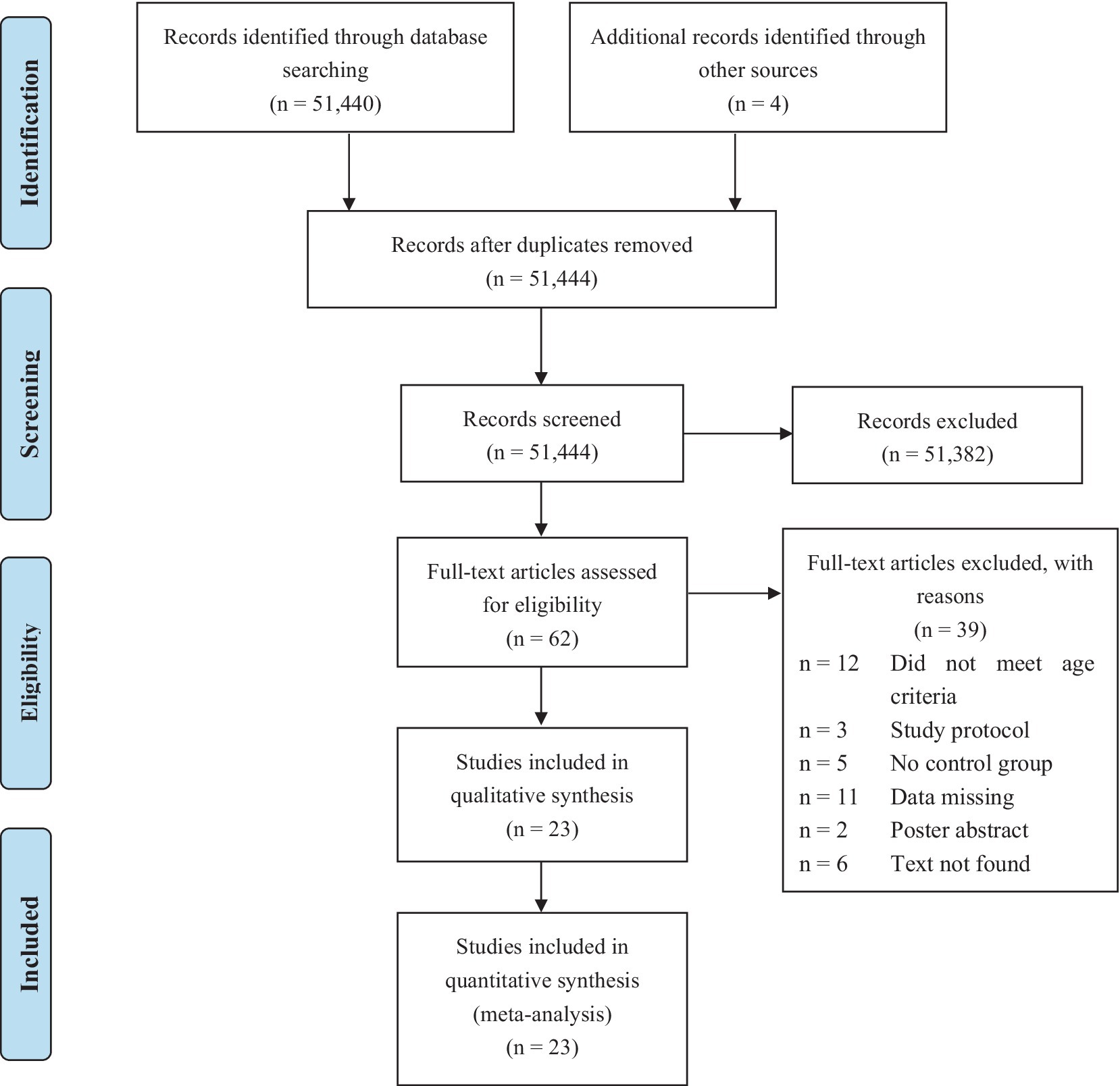
Figure 1. PRISMA flow chart of the search results and articles identified for inclusion.
3.2 Basic features of the included studies
The 23 studies included in this meta-analysis are described in detail in Table 1. There were 12 structured intervention studies (21, 22, 31, 33, 36, 37, 42, 43, 45, 47, 49, 51), 9 unstructured intervention studies (21, 22, 32, 35, 40, 41, 44, 46, 48), and 5 structured vs. unstructured intervention studies (21, 22, 34, 38, 39, 50), 2 of which were 3-arm trials (21, 22). The sample characteristics were included as follows: 23 studies involved a total of 4,068 preschool-aged children aged 3–6 years, with sample sizes ranging from 27 to 648. Two studies focused on preschoolers at risk e.g., exposure to biological risks (chronic diseases, genetic diseases, etc.), or environmental risks (single parenthood, poverty, etc.) (34, 35); one study focused on malnourished preschoolers (41); and one study involved only a sample of girls (38); the rest of studies included normal, healthy samples. The results characteristics were included as follows: 17 studies provided total FMS data (21, 22, 31–33, 37, 41–51), 9 studies provided LMS data (21, 32, 39, 40, 46–49, 51), and 12 studies provided OCS data (21, 32, 34–36, 38, 40, 46–49, 51). A total of 9 of the 17 studies reporting total FMS included both LMS scores and OCS scores. Exposures and comparison conditions were described as follows: the majority of studied interventions had a duration ranging from 8 to 24 weeks, and two studies included interventions longer than 24 weeks (25 weeks (51) and 36 weeks (44)). Notably, the structured intervention studies included in this meta-analysis described the intervention doses and the intervention durations ranged from 300 to 7,200 min. Among the unstructured intervention studies, five included details regarding intervention doses, with durations ranging from 300 to 21,600 min (21, 22, 32, 35, 41). In four studies (40, 44, 46, 48), due to the intervention involving the physical environment, space, and other factors, the dose could not be estimated. Intervention intensity was not reported in all studies; for example, participants were required to maintain intensity markers such as 50–80% of the maximum heart rate during the intervention.
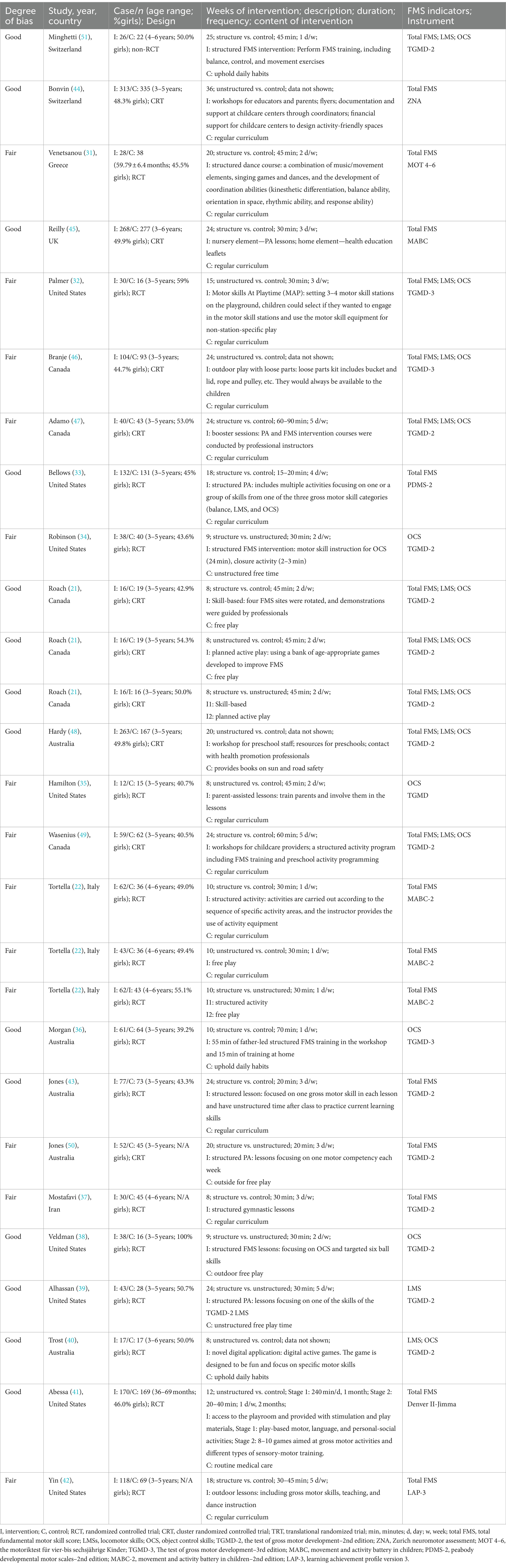
Table 1. Basic characteristics of the included studies.
3.3 Meta-analysis results
The results of this study are described in detail in Table 2. As shown in Supplementary Figure S1 and in the forest plots for all comparisons, the included study interventions had significant effects on the total FMS, LMS, and OCS in preschool-aged children (p < 0.05). The structured intervention was more effective than the unstructured intervention in improving the LMS (p < 0.05). No significant publication bias was detected based on Egger’s test for total FMS (p = 0.10), LMS (p = 0.10), or OCS (p = 0.06). The funnel plot is shown in Supplementary Figures S2–S4.
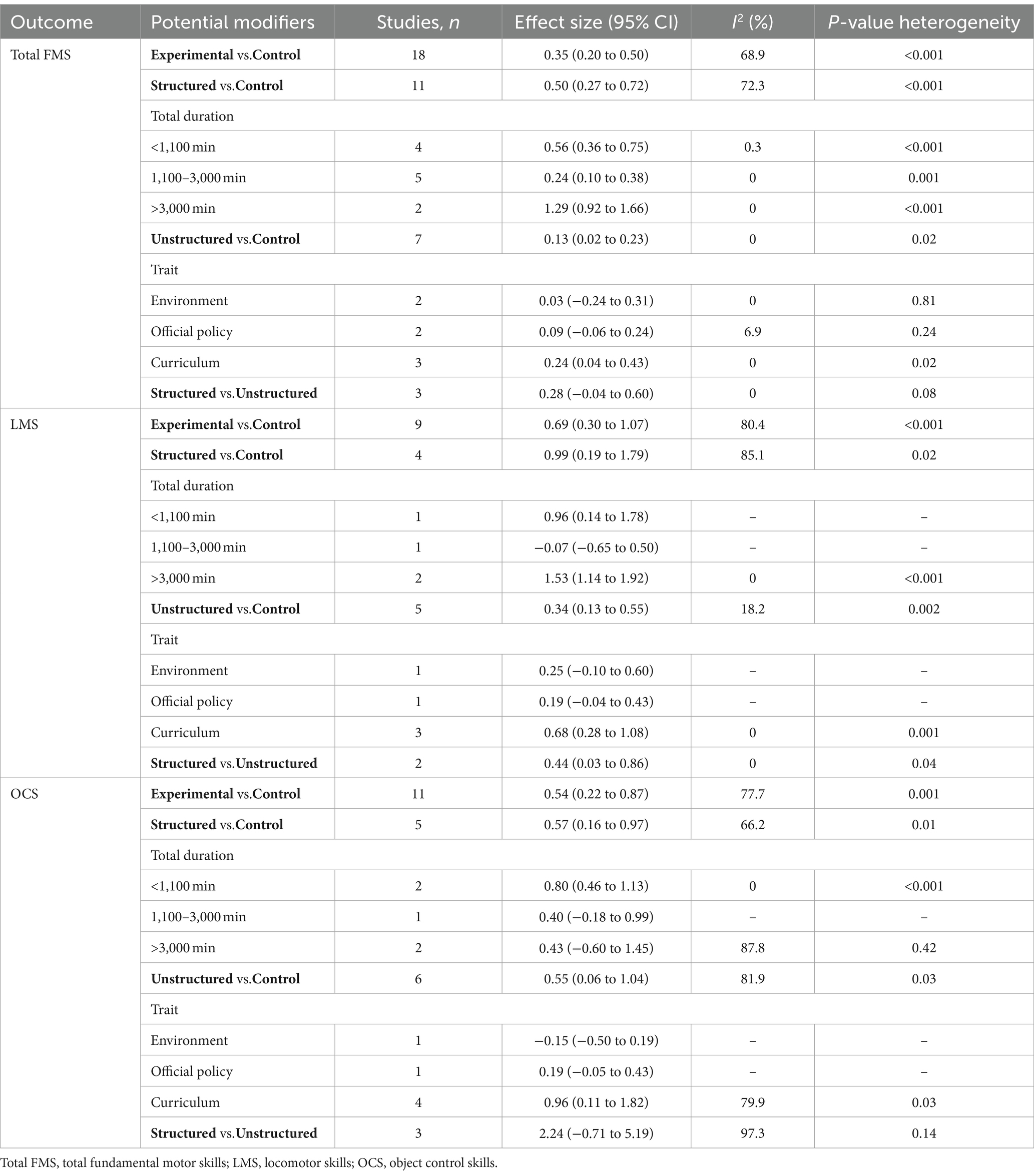
Table 2. Subgroup analyses on the effect of intervention on FMS in preschool children.
3.3.1 Total FMS
In total, 16 studies reported total FMS (21, 22, 31–33, 37, 41–49, 51). Compared with the control group, the interventions had a medium effect size (Hedge’s g = 0.35, 95% CI = 0.20–0.50, I2 = 68.9%, p < 0.001).
Total FMS data were reported in 11 structured intervention studies (22, 31, 33, 37, 42, 43, 45, 47, 49, 51). Compared with the control group, the structured interventions had a medium-sized effect on FMS (Hedge’s g = 0.50, 95% CI = 0.27–0.72, I2 = 72.3%, p < 0.001). Furthermore, when considering the total intervention duration, interventions with a duration of 300–1,100 min (Hedge’s g = 0.56) (22, 33, 37), 1,100–3,000 min (Hedge’s g = 0.24) (31, 42, 43, 45, 51), and 3,000–7,200 min (Hedge’s g = 1.29, 49, 51) had significant effects on FMS in preschool-aged children. There was a low level of heterogeneity (I2 < 25%).
Total FMS data were reported from six unstructured intervention studies (22, 32, 41, 44, 46, 48). Compared with the control group, the unstructured interventions had a small-sized effect on FMS (Hedge’s g = 0.13, 95% CI = 0.02–0.23, I2 = 0%, p = 0.02). Subgroup analysis based on intervention characteristics indicated that only the unstructured curriculum (Hedge’s g = 0.24) (21, 32, 41) had a significant effect on the preschool total FMS (p = 0.02). There was no heterogeneity between studies (I2 = 0%).
Three studies comparing structured vs. unstructured interventions reported total FMS data (21, 22, 50). There was no significant difference in the total FMS score between the structured intervention and unstructured intervention groups (p = 0.08).
3.3.2 LMS
Eight studies reported LMS data (21, 32, 40, 46–49, 51). Compared with the control group, the interventions had a medium-sized effect on LMS (Hedge’s g = 0.69, 95% CI = 0.30–1.07, I2 = 80.4%, p < 0.001).
Four structured intervention studies reported LMS data (21, 47, 49, 51). Compared with the control group, the structured interventions had a medium-sized effect on LMS (Hedge’s g = 0.99, 95% CI = 0.19–1.79, I2 = 85.1%, p = 0.02). Subgroup analysis based on the total duration of the intervention revealed that interventions with a duration greater than 3,000 min (Hedge’s g = 1.53) (47, 49) had a significant effect on LMS in preschool-aged children. There was no heterogeneity between studies (I2 = 0%).
Five unstructured intervention studies reported LMS data (21, 32, 40, 46, 48). Compared to the control group, the unstructured interventions had a medium-sized effect on LMS (Hedge’s g = 0.34, 95% CI = 0.13–0.55, I2 = 18.2%, p = 0.002). Subgroup analysis based on intervention characteristics indicated that only the unstructured curriculum (Hedge’s g = 0.68) (21, 32, 40) had a significant effect on LMS in preschool-aged children (p < 0.001). There was no heterogeneity between studies (I2 = 0%).
Two studies comparing structured and unstructured interventions reported LMS data (21, 39). Compared with unstructured interventions, structured interventions had a medium-sized effect on LMS in preschool-aged children (Hedge’s g = 0.44, 95% CI = 0.03–0.86, I2 = 0%, p = 0.04).
3.3.3 OCS
n total, 11 studies reported OCS data (21, 32, 35, 36, 40, 46–49, 51). Compared with the control group, the interventions had a medium-sized effect on OCS (Hedge’s g = 0.54, 95% CI = 0.22–0.87, I2 = 77.7%, p = 0.001).
Five structured intervention studies reported OCS data (21, 36, 47, 49, 51). Compared with the control group, the structured interventions had a medium-sized effect on OCS (Hedge’s g = 0.57, 95% CI = 0.16–0.97, I2 = 66.2%, p = 0.01). Subgroup analysis based on the total intervention duration revealed that interventions with a total duration of less than 1,100 min (Hedge’s g = 0.80) (21, 36) had a significant effect on OCS in preschool-aged children. There was no heterogeneity between studies (I2 = 0%).
Six unstructured intervention studies reported OCS data (21, 32, 35, 40, 46, 48). Compared with the control group, unstructured interventions had a medium-sized effect on OCS (Hedge’s g = 0.55, 95% CI = 0.06–1.04, I2 = 81.9%, p = 0.03). Subgroup analysis based on intervention characteristics revealed that only the unstructured curriculum (Hedge’s g = 0.96) (21, 32, 35, 40) had a significant effect on OCS in preschool-aged children (p = 0.03). There was a high degree of heterogeneity between studies (I2 = 79.9%).
Three structured vs. unstructured studies reported OCS data (21, 34, 38). There was no significant difference between the structured and the unstructured intervention in terms of OCS in preschool-aged children (p = 0.14).
3.4 Risk of bias assessment
The two researchers exhibited a high degree of consistency regarding the risk of bias assessment (ICC = 0.78). Overall, seven RCTs showed a fair risk of bias (22, 31, 32, 34, 35, 37, 42). All four CRTs showed a fair risk of bias (46, 47, 49, 50). Furthermore, the non-RCTs showed a good risk of bias (51). Details of the risk of bias assessment are shown in Supplementary Table S3.
4 Discussion
The included studies explored the effects of various interventions [childcare environment (52), teacher leadership (19), parental involvement (53), etc.] on FMS indicators in preschool-aged children. However, the use of various interventions leads to a high risk of heterogeneity. Therefore, using a more macro perspective (structured vs. unstructured interventions) may be a feasible approach. This study attempted to analyze trials of structured and unstructured interventions targeting FMS indicators in preschool-aged children. The effects of the structured and unstructured interventions on the FMS index of preschool-aged children were compared. After analyzing 19 intervention trials, we found that after active intervention, the FMS of preschool-aged children can be significantly improved (total FMS: Hedge’s g = 0.35; LMS: Hedge’s g = 0.69; OCS: Hedge’s g = 0.54). This study is consistent with previous studies showing that interventions targeting FMS in preschool-aged children are beneficial (54). Relevant reports show that the level of FMS mastery is still low in preschool-aged children (8, 10, 11). Both structured and unstructured interventions improved FMS in preschool-aged children. However, preschool is the period during which children develop FMS (1, 12). Selecting more efficient intervention measures for this age group is still a challenge among scholars. Similarly, there are no relevant reports on whether structured intervention or unstructured intervention is the better choice for improving the FMS in preschool-aged children. This study is the first known meta-analysis to investigate the effects of structured vs. unstructured interventions on the development of FMS in preschool-aged children.
4.1 Effects of structured and unstructured interventions on total FMS in preschool-aged children
This study examined 11 structured intervention studies to determine their effect on FMS in preschool-aged children. The results showed that structured interventions had a significant positive impact on the total FMS in preschool-aged children (Hedge’s g = 0.50, 95% CI = 0.27–0.72, I2 = 72.3%, p < 0.001). The significance of adult leadership within structured interventions lies in its capacity to deliver verbal cues, thereby influencing children’s motor behavior (55). In structured classes, it is essential to provide not only positive feedback but also negative feedback, verbal instructions, demonstrations, and effective organization of practice. The synthesis of this series of functions ultimately fosters the refinement of children’s motor skills (56, 57). Previous studies have suggested that the number of intervention sessions per week is the main reason for the heterogeneity of structured intervention effects (3 per week) (19). However, in this study, the duration of interventions was used as the segmentation point. The results showed that intervention duration and effect size had a “√” type relationship. That is, interventions with a duration of less than 3,000 min (Hedge’s g = 1.29) had the largest effect size, followed by interventions lasting more than 1,100 min (Hedge’s g = 0.56), and those lasting between 1,100 and 3,000 min (Hedge’s g = 0.24) had the smallest effect size. All the studies conducted had low heterogeneity. This may be attributed to the learning characteristics of preschool-aged children. Young learners exhibit high intrinsic motivation and a strong interest in acquiring new knowledge (58). Nevertheless, repetitive instruction on the same content tends to diminish enthusiasm for learning, leading to reduced compliance. Research suggests that short-duration interventions (<1,100 min) may be more effective than medium-duration interventions (1100–3,000 min). Additionally, the two long-term interventions (7,200 min) in this study were considerably longer than those in the remaining studies (<3,000 min), thus enabling extended practice and skill development among children (47, 49). This phenomenon may explain the greater effect size observed in the long-term intervention group. Consequently, emphasizing the necessity for repetitive teaching, practice, and reinforcement of FMS becomes crucial. These findings are consistent with expert opinions in the field, indicating that FMS need to be actively taught and consistently reinforced since they do not appear to develop naturally and maintain themselves automatically (14, 59).
In addition to structured interventions, seven unstructured intervention studies were included. The results showed that unstructured interventions significantly improved the total FMS (Hedge’s g = 0.13, 95% CI = 0.02–0.23, I2 = 0%, p = 0.02) in preschool-aged children. Previous studies did not integrate research on unstructured interventions targeting FMS in preschool-aged children and instead used only single-feature literature or systematic reviews (20, 60). However, consistent with those studies, unstructured interventions have health benefits for preschoolers. Unstructured interventions are considered a potential measure for enhancing children’s physical activity and improving their overall development (61, 62). However, some studies have suggested that unstructured interventions can have significant effects only in small samples (62). However, this study revealed that in unstructured interventions involving a large sample, some studies still showed significant improvement in total FMS in preschool-aged children (41, 44, 48). Thus, sample size is not a major factor in the effect of unstructured interventions. A comparison of the results of the included studies revealed that only exercise interventions directly targeting preschool-aged children could affect total FMS. Teachers and caregivers, providing children with ideological courses, or increasing the content of children’s physical activity environment may have more effects on children’s physical, psychological, and other developmental indicators (63–65). After further analysis, we found that unstructured interventions were distinguished based on intervention characteristics. Only unstructured curriculum interventions had a significant effect on total FMS in preschool-aged children. Research suggests that vigorous active play is a good measure for promoting the development of FMS in preschool-aged children (66). Organizations, such as the WHO (67), explicitly require active play for preschoolers. The reason is that in energetically active play, children can fully run, jump, and play (61). The development of children’s athletic ability is strong. In addition, role-playing between peers can more fully mobilize children’s enthusiasm and enable them to develop in games (68).
By analyzing three studies of structured vs. unstructured interventions, this study revealed that structured interventions were not significantly better than unstructured interventions at improving total FMS in preschool-aged children (p = 0.08). Structured interventions are controlled in design, and well-structured, repetitive exercise regimens are often performed. However, it is not yet clear whether the structured interventions will also have the same benefits on other indicators of physical development (69). Moreover, child development indicators are not limited to FMS. Therefore, the use of structured interventions in practice should consider more comprehensive design content. Interventions should avoid focusing too closely on the development of one indicator while neglecting the common development of other health indicators. In contrast, although the effects of unstructured interventions on total FMS in preschool-aged children were not as strong as the effects of structured interventions, the former approach still yielded significant positive effects. Moreover, unstructured interventions have positive effects on many child health indicators (70). The rational use of unstructured interventions is feasible.
4.2 Effects of structured and unstructured interventions on LMS and OCS in preschool-aged children
The findings of this study indicate that both structured and unstructured interventions exert significant impacts on the LMS and OCS of preschool-aged children. However, it is imperative to acknowledge the potential influence of the number of included studies and methodological variations between LMS and OCS research on the obtained results. Prior research has highlighted that LMSs, such as running and jumping, constitute fundamental components of children’s daily activities (71), and numerous motor interventions, encompassing both structured and unstructured interventions, have been found to promote these skills. This highlights the significant potential for both types of interventions to enhance LMS in preschool-aged children when administered correctly. This study posits that structured interventions outperform unstructured interventions in enhancing LMS in preschool-aged children. This superiority is evident both through direct and indirect comparisons, which consistently indicate that structured interventions yield more favorable outcomes. Furthermore, as proposed by JD Goodway, children’s acquisition of proficient LMS is contingent upon guidance and/or practice (72). In the absence of appropriate guidance, children may fail to master LMS even throughout their adolescent years (73). This highlights the crucial role of structured interventions, particularly guidance, in fostering the development of LMS in preschool children.
On the other hand, the results for control skills, such as throwing and catching, were similar under both structured and unstructured interventions. In indirect comparisons, the effects of structured (Hedge’s g = 0.57) and unstructured (Hedge’s g = 0.55) interventions compared to the control group were similar. Similarly, direct comparisons did not reveal significant differences (Hedge’s g = 2.24, 95% CI = -0.71–5.19, I2 = 97.3%, p = 0.14). This suggests that the development of control skills may require a more complex intervention design (34). The current study found that the allocation of time in structured curricula may be one of the factors influencing the development of OCS. Niko S. Wasenius’s study allocated more intervention time to LMS practice, with only 33% of the time devoted to OCS practice (49). Another study provided additional control skills, such as balls and bats (44). Although structured and unstructured interventions produced similar results in promoting overall motor skill performance, only motor skills showed superior results in structured practice compared to unstructured practice.
Other results showed that increasing outdoor amusement equipment did not lead to a significant improvement in FMS in preschool-aged children, which is consistent with the findings of previous research (22, 46, 74). It should be noted that this study included only a few studies on changing the environment, which may not provide a clear explanation. Additionally, the implementation of outdoor amusement equipment varies greatly, and it is crucial to carefully evaluate and design intervention strategies to determine the positive effects of FMS in preschool-aged children (22). Therefore, it cannot be denied that changing the environment has a positive impact on FMS in preschool-aged children, but further research is needed to fully understand the extent of this impact.
4.3 Limitations of the study
Although there are several novel findings in this study, there are still several limitations. For example, the studies included in this meta-analysis used different types of motor interventions. In addition, this study only referred to the duration of the intervention and did not refer to the intensity of the intervention. However, there are no clear reports on the intensity of intervention, and the results only provide good guidance on the duration of intervention. Moreover, data, such as physical activity and other related indicators, were not collected in this study, so there was no analysis of how these factors may affect FMS.
5 Conclusion
Scientific interventions are necessary to improve FMS in young children. Well-designed structured interventions are more suitable than natural development for the improvement of FMS in young children, especially when considering LMSs. Moreover, FMS in young children need to be practiced repeatedly for a long time to achieve proficiency.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
Author contributions
DC: Writing – original draft. GZ: Writing – review & editing. JF: Writing – review & editing. SS: Writing – review & editing. LS: Writing – review & editing. ZH: Writing – review & editing. RC: Data curation, Writing – review & editing. TJ: Software, Writing – review & editing. XH: Software, Writing – review & editing. YL: Software, Writing – review & editing. FS: Software, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by the National Social Science Foundation of China (21BTY088), the 14th Five-Year Plan of Social Science in Jiangxi Province (22TY20D), the Special Project for Postgraduate Student Innovation in Jiangxi Province (YC2021-S024), and the Special Project for Postgraduate Student Innovation in Jiangxi Province (YC2022-S031).
Acknowledgments
We would like to express our sincere gratitude to Nanchang University, Jiangxi Sports Science Medical Centre, Jiangxi Normal University, and Beijing Sport University for their invaluable support in this research endeavor. Furthermore, we extend our deepest appreciation to the National Social Science Foundation and the Jiangxi Provincial Foundation for their generous financial support. Finally, we would like to acknowledge all the esteemed authors for their commendable contributions to this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1345566/full#supplementary-material
References
1. Goodway, JD, Ozmun, JC, and Gallahue, DL. Understanding motor development: Infants, children, adolescents, adults Jones & Bartlett Learning (2019).
3. Iivonen, KS, Sääkslahti, AK, Mehtälä, A, Villberg, JJ, Tammelin, TH, Kulmala, JS, et al. Relationship between fundamental motor skills and physical activity in 4-year-old preschool children. Percept Mot Skills. (2013) 117:627–46. doi: 10.2466/10.06.PMS.117x22z7
4. Barnett, LM, Van Beurden, E, Morgan, PJ, Brooks, LO, and Beard, JR. Does childhood motor skill proficiency predict adolescent fitness? Med Sci Sports Exerc. (2008) 40:2137–44. doi: 10.1249/MSS.0b013e31818160d3
5. Chowdhury, SD, Wrotniak, BH, and Ghosh, T. Association between body mass index and motor competence in Santal children of Purulia District, India. J Mot Behav. (2017) 49:349–54. doi: 10.1080/00222895.2016.1219308
6. Stodden, DF, Goodway, JD, Langendorfer, SJ, Roberton, MA, Rudisill, ME, Garcia, C, et al. A developmental perspective on the role of motor skill competence in physical activity: an emergent relationship. Quest. (2008) 60:290–306. doi: 10.1080/00336297.2008.10483582
7. Lubans, DR, Morgan, PJ, Cliff, DP, Barnett, LM, and Okely, AD. Fundamental movement skills in children and adolescents: review of associated health benefits. Sports Med. (2010) 40:1019–35. doi: 10.2165/11536850-000000000-00000
8. Hardy, LL, Barnett, L, Espinel, P, and Okely, AD. Thirteen-year trends in child and adolescent fundamental movement skills: 1997-2010. Med Sci Sports Exerc. (2013) 45:1965–70. doi: 10.1249/MSS.0b013e318295a9fc
9. Aye, T, Oo, KS, Khin, MT, Kuramoto-Ahuja, T, and Maruyama, H. Gross motor skill development of 5-year-old kindergarten children in Myanmar. J Phys Ther Sci. (2017) 29:1772–8. doi: 10.1589/jpts.29.1772
10. Roscoe, CMP, James, RS, and Duncan, MJ. Accelerometer-based physical activity levels, fundamental movement skills and weight status in British preschool children from a deprived area. Eur J Pediatr. (2019) 178:1043–52. doi: 10.1007/s00431-019-03390-z
11. Xia, X, Chao, L, Nan, C, Yin, X, Zheng, H, and Zhang, S. Fundamental motor skills of kindergarten children in different environments and ethnic groups in Northwest China. BMC Pediatr. (2022) 22:423. doi: 10.1186/s12887-022-03497-7
12. Clark, JE, and Humphrey, JH. Motor Development: Research & Reviews. Vol. 2. National Association for Sport and Physical Education. (2002).
13. Gil Madrona, P, Romero Martínez, SJ, Sáez-Gallego, NM, and Ordóñez Camacho, XG. Psychomotor limitations of overweight and obese five-year-old children: influence of body mass indices on motor, perceptual, and social-emotional skills. Int. J. Environ. Res. Public Health. (2019) 16:427. doi: 10.3390/ijerph16030427
14. Logan, SW, Robinson, LE, Wilson, AE, and Lucas, WA. Getting the fundamentals of movement: a meta-analysis of the effectiveness of motor skill interventions in children. Child Care Health Dev. (2012) 38:305–15. doi: 10.1111/j.1365-2214.2011.01307.x
15. World Health Organization. Guidelines on physical activity, sedentary behaviour, and sleep for children under 5 years of age. Geneva: AAHPERD Publications (2019).
16. Clark, JE, Clements, RL, Guddemi, M, Morgan, DW, Pica, R, Pivarnik, JM, et al. Active start: a statement of physical activity guidelines for children birth to five years ERIC (2002).
17. Katzmarzyk, PT, Denstel, KD, Beals, K, Carlson, J, Crouter, SE, McKenzie, TL, et al. Results from the United States 2018 report card on physical activity for children and youth. J Phys Act Health. (2018) 15:S422–4. doi: 10.1123/jpah.2018-0476
18. Hardy, LL, O'Hara, BJ, Rogers, K, St George, A, and Bauman, A. Contribution of organized and nonorganized activity to children's motor skills and fitness. J Sch Health. (2014) 84:690–6. doi: 10.1111/josh.12202
19. van Capelle, A, Broderick, CR, van Doorn, N, Ward, RE, and Parmenter, BJ. Interventions to improve fundamental motor skills in pre-school aged children: a systematic review and meta-analysis. J Sci Med Sport. (2017) 20:658–66. doi: 10.1016/j.jsams.2016.11.008
20. Johnstone, A, Hughes, AR, Martin, A, and Reilly, JJ. Utilising active play interventions to promote physical activity and improve fundamental movement skills in children: a systematic review and meta-analysis. BMC Public Health. (2018) 18:789. doi: 10.1186/s12889-018-5687-z
21. Roach, L, and Keats, M. Skill-based and planned active play versus free-play effects on fundamental movement skills in preschoolers. Percept Mot Skills. (2018) 125:651–68. doi: 10.1177/0031512518773281
22. Tortella, P, Haga, M, Lorås, H, Fumagalli, GF, and Sigmundsson, H. Effects of free play and partly structured playground activity on motor competence in preschool children: a pragmatic comparison trial. Int J Environ Res Public Health. (2022) 19:7652. doi: 10.3390/ijerph19137652
23. Moher, D, Liberati, A, Tetzlaff, J, and Altman, DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Open Med. (2009) 3:e123–30. doi: 10.1016/j.ijsu.2010.02.007
24. Liberati, A, Altman, DG, Tetzlaff, J, Mulrow, C, Gøtzsche, PC, Ioannidis, JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. (2009) 339:b2700. doi: 10.1136/bmj.b2700
25. Downs, SH, and Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. (1998) 52:377–84. doi: 10.1136/jech.52.6.377
27. Cumpston, M, Li, T, Page, MJ, Chandler, J, Welch, VA, Higgins, JP, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev. (2019) 10:Ed000142. doi: 10.1002/14651858.Ed000142
28. Parker, K, Nunns, M, Xiao, Z, Ford, T, and Ukoumunne, OC. Intracluster correlation coefficients from school-based cluster randomized trials of interventions for improving health outcomes in pupils. J Clin Epidemiol. (2023) 158:18–26. doi: 10.1016/j.jclinepi.2023.03.020
29. Deeks, JJ, Higgins, JP, and Altman, DG. Analysing Data and Undertaking Meta-Analyses. Cochrane Handbook for Systematic Reviews of Interventions. (2008). p. 243–296.
30. Higgins, JP, Thompson, SG, Deeks, JJ, and Altman, DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
31. Venetsanou, F, and Kambas, A. How can a traditional Greek dances programme affect the motor proficiency of pre-school children? Res Dance Educ. (2004) 5:127–38. doi: 10.1080/14617890500064019
32. Palmer, KK, Miller, AL, Meehan, SK, and Robinson, LE. The motor skills at playtime intervention improves children's locomotor skills: a feasibility study. Child Care Health Dev. (2020) 46:599–606. doi: 10.1111/cch.12793
33. Bellows, LL, Davies, PL, Anderson, J, and Kennedy, C. Effectiveness of a physical activity intervention for head start preschoolers: a randomized intervention study. Am J Occup Ther. (2013) 67:28–36. doi: 10.5014/ajot.2013.005777
34. Robinson, LE, and Goodway, JD. Instructional climates in preschool children who are at-risk. Part I: object-control skill development. Res Q Exerc Sport. (2009) 80:533–42. doi: 10.1080/02701367.2009.10599591
35. Hamilton, M, Goodway, J, and Haubenstricker, J. Parent-assisted instruction in a motor skill program for at-risk preschool children. Adapt Phys Act Q. (1999) 16:415–26. doi: 10.1123/apaq.16.4.415
36. Morgan, PJ, Grounds, JA, Ashton, LM, Collins, CE, Barnes, AT, Pollock, ER, et al. Impact of the 'Healthy youngsters, healthy Dads' program on physical activity and other health behaviours: a randomised controlled trial involving fathers and their preschool-aged children. BMC Public Health. (2022) 22:1166. doi: 10.1186/s12889-022-13424-1
37. Mostafavi, R, Ziaee, V, Akbari, H, and Haji-Hosseini, S. The effects of SPARK physical education program on fundamental motor skills in 4-6 year-old children. Iran. J Pediatr. (2013) 23:216–9.
38. Veldman, SL, Palmer, KK, Okely, AD, and Robinson, LE. Promoting ball skills in preschool-age girls. J Sci Med Sport. (2017) 20:50–4. doi: 10.1016/j.jsams.2016.04.009
39. Alhassan, S, Nwaokelemeh, O, Ghazarian, M, Roberts, J, Mendoza, A, and Shitole, S. Effects of locomotor skill program on minority preschoolers' physical activity levels. Pediatr Exerc Sci. (2012) 24:435–49. doi: 10.1123/pes.24.3.435
40. Trost, SG, and Brookes, DSK. Effectiveness of a novel digital application to promote fundamental movement skills in 3- to 6-year-old children: a randomized controlled trial. J Sports Sci. (2021) 39:453–9. doi: 10.1080/02640414.2020.1826657
41. Abessa, TG, Worku, BN, Wondafrash, M, Girma, T, Valy, J, Lemmens, J, et al. Effect of play-based family-centered psychomotor/psychosocial stimulation on the development of severely acutely malnourished children under six in a low-income setting: a randomized controlled trial. BMC Pediatr. (2019) 19:336. doi: 10.1186/s12887-019-1696-z
42. Yin, Z, Parra-Medina, D, Cordova, A, He, M, Trummer, V, Sosa, E, et al. Míranos! Look at us, we are healthy! An environmental approach to early childhood obesity prevention. Child Obes. (2012) 8:429–39. doi: 10.1089/chi.2011.0125
43. Jones, RA, Okely, AD, Hinkley, T, Batterham, M, and Burke, C. Promoting gross motor skills and physical activity in childcare: a translational randomized controlled trial. J Sci Med Sport. (2016) 19:744–9. doi: 10.1016/j.jsams.2015.10.006
44. Bonvin, A, Barral, J, Kakebeeke, TH, Kriemler, S, Longchamp, A, Schindler, C, et al. Effect of a governmentally-led physical activity program on motor skills in young children attending child care centers: a cluster randomized controlled trial. Int J Behav Nutr Phys Act. (2013) 10:90. doi: 10.1186/1479-5868-10-90
45. Reilly, JJ, Kelly, L, Montgomery, C, Williamson, A, Fisher, A, McColl, JH, et al. Physical activity to prevent obesity in young children: cluster randomised controlled trial. BMJ. (2006) 333:1041. doi: 10.1136/bmj.38979.623773.55
46. Branje, K, Stevens, D, Hobson, H, Kirk, S, and Stone, M. Impact of an outdoor loose parts intervention on Nova Scotia preschoolers' fundamental movement skills: a multi-methods randomized controlled trial. AIMS Pub Health. (2022) 9:194–215. doi: 10.3934/publichealth.2022015
47. Adamo, KB, Wilson, S, Harvey, AL, Grattan, KP, Naylor, PJ, Temple, VA, et al. Does intervening in childcare settings impact fundamental movement skill development? Med Sci Sports Exerc. (2016) 48:926–32. doi: 10.1249/MSS.0000000000000838
48. Hardy, LL, King, L, Kelly, B, Farrell, L, and Howlett, S. Munch and move: evaluation of a preschool healthy eating and movement skill program. Int J Behav Nutr Phys Act. (2010) 7:80. doi: 10.1186/1479-5868-7-80
49. Wasenius, NS, Grattan, KP, Harvey, ALJ, Naylor, PJ, Goldfield, GS, and Adamo, KB. The effect of a physical activity intervention on preschoolers' fundamental motor skills - a cluster RCT. J Sci Med Sport. (2018) 21:714–9. doi: 10.1016/j.jsams.2017.11.004
50. Jones, RA, Riethmuller, A, Hesketh, K, Trezise, J, Batterham, M, and Okely, AD. Promoting fundamental movement skill development and physical activity in early childhood settings: a cluster randomized controlled trial. Pediatr Exerc Sci. (2011) 23:600–15. doi: 10.1123/pes.23.4.600
51. Minghetti, A, Donath, L, Zahner, L, Hanssen, H, and Faude, O. Beneficial effects of an intergenerational exercise intervention on health-related physical and psychosocial outcomes in Swiss preschool children and residential seniors: a clinical trial. PeerJ. (2021) 9:e11292. doi: 10.7717/peerj.11292
52. Wick, K, Leeger-Aschmann, CS, Monn, ND, Radtke, T, Ott, LV, Rebholz, CE, et al. Interventions to promote fundamental movement skills in childcare and kindergarten: a systematic review and Meta-analysis. Sports Med. (2017) 47:2045–68. doi: 10.1007/s40279-017-0723-1
53. Riethmuller, AM, Jones, RA, and Okely, AD. Efficacy of interventions to improve motor development in young children: a systematic review. Pediatrics. (2009) 124:e782–92. doi: 10.1542/peds.2009-0333
54. Han, A, Fu, A, Cobley, S, and Sanders, RH. Effectiveness of exercise intervention on improving fundamental movement skills and motor coordination in overweight/obese children and adolescents: a systematic review. J Sci Med Sport. (2018) 21:89–102. doi: 10.1016/j.jsams.2017.07.001
55. Rodríguez-Guerrero, YI, Gil-Madrona, P, Pilar León, M, and Vásquez-Cruz, AE. Relationship between fine/gross motor skills and language and math development in Colombian Caribbean children: a study in Barranquilla. Infant Child Dev. (2023) 32:e2430. doi: 10.1002/icd.2430
56. Medeiros, P, Capistrano, R, Zequinão, MA, Silva, SAD, Beltrame, TS, and Cardoso, FL. EXERGAMES as a tool for the acquisition and development of motor skills and abilities: a systematic review. Rev Paul Pediatr. (2017) 35:464–71. doi: 10.1590/1984-0462/;2017;35;4;00013
57. von Suchodoletz, A, Lee, DS, Henry, J, Tamang, S, Premachandra, B, and Yoshikawa, H. Early childhood education and care quality and associations with child outcomes: a meta-analysis. PLoS One. (2023) 18:e0285985. doi: 10.1371/journal.pone.0285985
58. Cordova, DI, and Lepper, MR. Intrinsic motivation and the process of learning: beneficial effects of contextualization, personalization, and choice. J Educ Psychol. (1996) 88:715–30. doi: 10.1037/0022-0663.88.4.715
59. Morgan, PJ, Barnett, LM, Cliff, DP, Okely, AD, Scott, HA, Cohen, KE, et al. Fundamental movement skill interventions in youth: a systematic review and meta-analysis. Pediatrics. (2013) 132:e1361–83. doi: 10.1542/peds.2013-1167
60. Comeras-Chueca, C, Marin-Puyalto, J, Matute-Llorente, A, Vicente-Rodriguez, G, Casajus, JA, and Gonzalez-Aguero, A. The effects of active video games on health-related physical fitness and motor competence in children and adolescents with healthy weight: a systematic review and Meta-analysis. Int J Environ Res Public Health. (2021) 18:6965. doi: 10.3390/ijerph18136965
61. Truelove, S, Vanderloo, LM, and Tucker, P. Defining and measuring active play among Young children: a systematic review. J Phys Act Health. (2017) 14:155–66. doi: 10.1123/jpah.2016-0195
62. O'Dwyer, MV, Fairclough, SJ, Ridgers, ND, Knowles, ZR, Foweather, L, and Stratton, G. Effect of a school-based active play intervention on sedentary time and physical activity in preschool children. Health Educ Res. (2013) 28:931–42. doi: 10.1093/her/cyt097
63. Honrubia Montesinos, C, Gil Madrona, P, Losada Puente, L, Brian, A, and Saraiva, L. The relationship between early childhood teachers’ professional development in physical education and Children’s fundamental movement skills. Early Educ Dev. (2023) 1-14:1–14. doi: 10.1080/10409289.2023.2221766
64. Sáez Sánchez, MB, Gil Madrona, P, and Martínez, LM. Desarrollo psicomotor y su vinculación con la motivación hacia el aprendizaje y el rendimiento académico en Educación Infantil. Revista de educación. (2021)
65. Simón-Piqueras, JÁ, Cano-Noguera, F, Zamorano-García, D, and Gil-Madrona, P. Efecto de un programa de iniciación a la natación basado en juegos motores acuáticos sobre la autoestima corporal y socio afectiva en niñas y niños de 5 y 6 años de edad. Revista Electrónica Interuniversitaria de Formación del Profesorado. (2023) 26:75–88. doi: 10.6018/reifop.570041
66. Oppici, L, Stell, FM, Utesch, T, Woods, CT, Foweather, L, and Rudd, JR. A skill acquisition perspective on the impact of exergaming technology on foundational movement skill development in children 3-12 years: a systematic review and Meta-analysis. Sports Med Open. (2022) 8:148. doi: 10.1186/s40798-022-00534-8
67. Bull, FC, Al-Ansari, SS, Biddle, S, Borodulin, K, Buman, MP, Cardon, G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. (2020) 54:1451–62. doi: 10.1136/bjsports-2020-102955
68. Foulkes, JD, Knowles, Z, Fairclough, SJ, Stratton, G, O'Dwyer, M, Ridgers, ND, et al. Effect of a 6-week active play intervention on fundamental movement skill competence of preschool children. Percept Mot Skills. (2017) 124:393–412. doi: 10.1177/0031512516685200
69. Ginsburg, KR. The importance of play in promoting healthy child development and maintaining strong parent-child bonds. Pediatrics. (2007) 119:182–91. doi: 10.1542/peds.2006-2697
70. Gil-Madrona, P, Romero-Martínez, SJ, and Roz-Faraco, CC. Extracurricular physical activities and the condition of being an only child as a conditioning factor in the psychomotor development of 5-year-old children. Front Pediatr. (2021) 9:684418. doi: 10.3389/fped.2021.684418
72. Goodway, JD, and Branta, CF. Influence of a motor skill intervention on fundamental motor skill development of disadvantaged preschool children. Res Q Exercise Sport. (2003) 74:36–46. doi: 10.1080/02701367.2003.10609062
73. Goodway, JD, and Suminski, R. Learner and environmental constraints influencing fundamental motor skill development of at-risk Hispanic preschoolers. Res Q Exercise Sport. (2003) 74:31.
Keywords: structured, unstructured, fundamental motor skills, preschool children, meta-analysis
Citation: Chen D, Zhao G, Fu J, Shun S, Su L, He Z, Chen R, Jiang T, Hu X, Li Y and Shen F (2024) Effects of structured and unstructured interventions on fundamental motor skills in preschool children: a meta-analysis. Front. Public Health. 12:1345566. doi: 10.3389/fpubh.2024.1345566
Edited by:
Herbert Ugrinowitsch, Federal University of Minas Gerais, BrazilReviewed by:
Liu Yueying, Affiliated Hospital of Jiangnan University, ChinaPedro Gil-Madrona, University of Castilla-La Mancha, Spain
Crislaine Rangel Couto, Federal University of Minas Gerais, Brazil
Copyright © 2024 Chen, Zhao, Fu, Shun, Su, He, Chen, Jiang, Hu, Li and Shen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guanggao Zhao, emhhb2dnMjAwMkAxNjMuY29t