
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Public Health , 28 February 2024
Sec. Life-Course Epidemiology and Social Inequalities in Health
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1345273
 Alessandra Galiè1*†
Alessandra Galiè1*† Anni McLeod2†
Anni McLeod2† Zoë A. Campbell1
Zoë A. Campbell1 Nicholas Ngwili1
Nicholas Ngwili1 Zelalem G. Terfa3
Zelalem G. Terfa3 Lian F. Thomas1,4,5
Lian F. Thomas1,4,5One Health research and intervention outcomes are strongly influenced by gender dynamics. Women, men, girls, and boys can be negatively affected by gender-based disadvantage in any of the three One Health domains (animal, human, and environmental health), and where this occurs in more than one domain the result may be a compounding of inequity. Evidence worldwide shows that women and girls are more likely to suffer from such gender-based disadvantage. A thoughtfully implemented One Health intervention that prioritizes gender equity is more likely to be adopted, has fewer unintended negative consequences, and can support progress toward gender equality, however there is limited evidence and discussion to guide using a gender lens in One Health activities. We propose a framework to identify key gender considerations in One Health research for development – with a focus on Low-and Middle-Income Countries. The framework encourages developing two types of research questions at multiple stages of the research process: those with a bioscience entry-point and those with a gender entry-point. Gender considerations at each stage of research, institutional support required, and intervention approaches is described in the framework. We also give an applied example of the framework as it might be used in One Health research. Incorporation of gender questions in One Health research supports progress toward more equitable, sustainable, and effective One Health interventions. We hope that this framework will be implemented and optimized for use across many One Health challenge areas with the goal of mainstreaming gender into One Health research.
There is currently a drive within the international community to integrate gender considerations into research, policy, and practice. This includes research and development activities in any of the three domains of One Health: animal, human, and environmental health. One Health recognizes the constantly evolving relationship between animals, humans, and the environment (1). The One Health High-Level Expert Panel (OHHLEP) states that “the health of humans, domestic and wild animals, plants, and the wider environment (including ecosystems) are closely linked and interdependent” (2). Motivation for integrating gender considerations is based on a growing appreciation that the social context in which problems occur influences research outcomes and therefore the effectiveness of development interventions in both disseminating relevant innovations and ensuring the benefits are equitably shared among the stakeholders.
The One Health Panel’s conceptualization of One Health (2) highlights the importance of equity and inclusivity, as do an earlier paper by (3) – although neither specifically mention gender- and a paper by Laing et al. (4). Van Patter et al. (5) argue that One Health researchers need to understand the political economies that often cause health disparities to progress toward equity. They further argue that integrating feminist thought into One Health research can help identify ‘the complexities and interconnections of power and difference that impact each of the three pillars of One Health’ (page 4).
Equitable access to appropriate innovations and to the associated benefits is paramount in gender equality, whereby men, women, boys, and girls have equal access to resources and opportunities that meet their needs, priorities, and interests. ‘Gender’ is a key organizing principle in society unconsciously used by people worldwide as a means of making sense of who we are in relation to the other (6). Gender, as well as other identity markers like age, ethnic group, religion, marital status, and caste influences the power you have in relation to others, the behaviors considered appropriate in a particular time or place, your roles and responsibilities, and your access to resources and opportunities (7, 8). Hierarchal relationships whereby some groups of people are given more privilege than others do not just affect interactions between individuals, they are entrenched in systems including human health and veterinary services, government institutions, schools and universities, and the economy. Gender analysis engages in such complex social dynamics which shape the differences in preferences, needs, and capacities we may see between women and men. Gender analysis is different from gender-disaggregated data collection which entails recording differences between women and men (the ‘what’) without any analysis of gender dynamics and norms that shape such gender differences (the ‘how’ and ‘why’ behind the ‘what’).
In this paper, we limit our discussion to women and men as the two main gender groups of interest based on the extensive body of literature on inter-gender differences between these two groups, particularly with respect to agriculture and rural livelihoods. However, we fully acknowledge that gender-diverse people often experience specific forms of discrimination (9). We believe that the process of developing questions on gender proposed in our framework would be valid for gender-diverse people and we would encourage other researchers to explore this possibility and include gender-diverse options.
In this paper, we provide some illustrative examples of the importance of gender considerations within key health challenges where a One Health approach is relevant. Women in lower- and middle-income countries, for example, are often disproportionately affected by zoonotic and infectious diseases due to their gender-based roles in domestic activities and animal production. In Uganda, practices associated with risk of transmission of Rift Valley fever such as handling raw meat or consumption of unpasteurized milk were influenced by gendered social roles (10, 11). In rural South Africa, men may be more exposed to risks associated with hunting and slaughtering wildlife and rodent control (12). In West Africa, outbreaks of Ebola, an emerging zoonotic disease, disproportionately affected the economic and social lives of young women, in particular. Closed schools led to increased pregnancies out of wedlock. After the 2015 outbreak, a policy established that ‘visibly pregnant girls’ would be unable to re-enroll in school, leading to a drop in girls’ access to education (13). Early evidence from the COVID-19 pandemic identified increased risk of mortality for men, possibly due to sex-based immunological differences or gender-based differences such as patterns of smoking or gendered hygiene practices (10).
An additional complexity is that due to social and gender norms (see definition below), health care workers in many countries are predominantly women, which put them at greater risk of contracting COVID-19 (14, 15). In rural Nepal, gender norms affected healthcare seeking behaviors and the likelihood of being prescribed and taking antibiotics, which are relevant to the (re)-emergence of antimicrobial resistance (16). In light of these and other studies, researchers have made a case for considering gender issues to minimizing food safety risks in livestock value chains (17) and for improved One Health research in pastoralist systems (18), noting the scarcity of frameworks that embed gender in One Health (19). While analytical frameworks for gender in human health already exist (20, 21), appropriate frameworks to support the integration of gender considerations across all three domains of One Health are currently lacking.
Building on the momentum from recent discussion and publications, we propose a framework highlighting key gender considerations across One Health research. This article is structured as follows:
• Section 2 defines One Health as applied to the development of the framework.
• Section 3 summarizes arguments for gender considerations in One Health research.
• Section 4 provides a brief description of methods.
• Section 5 describing an overview of the framework structure, gender considerations at each stage of one health research including institutional support required and intervention approaches.
• Section 6 presents an applied example of the framework as it might be used in One Health research on Taenia solium, the pork tapeworm.
• Section 7 provides the conclusion.
The definition of One Health has evolved over time; common ideas can be found across many sources, but emphasis has varied among institutions and according to context (22, 23). In 2021, a common definition was agreed by the One Health High Level Expert Panel (OHHLEP) (2). We used OHHLEP’s definition (below and Figure 1) as a starting point for developing a gender in One Health framework:
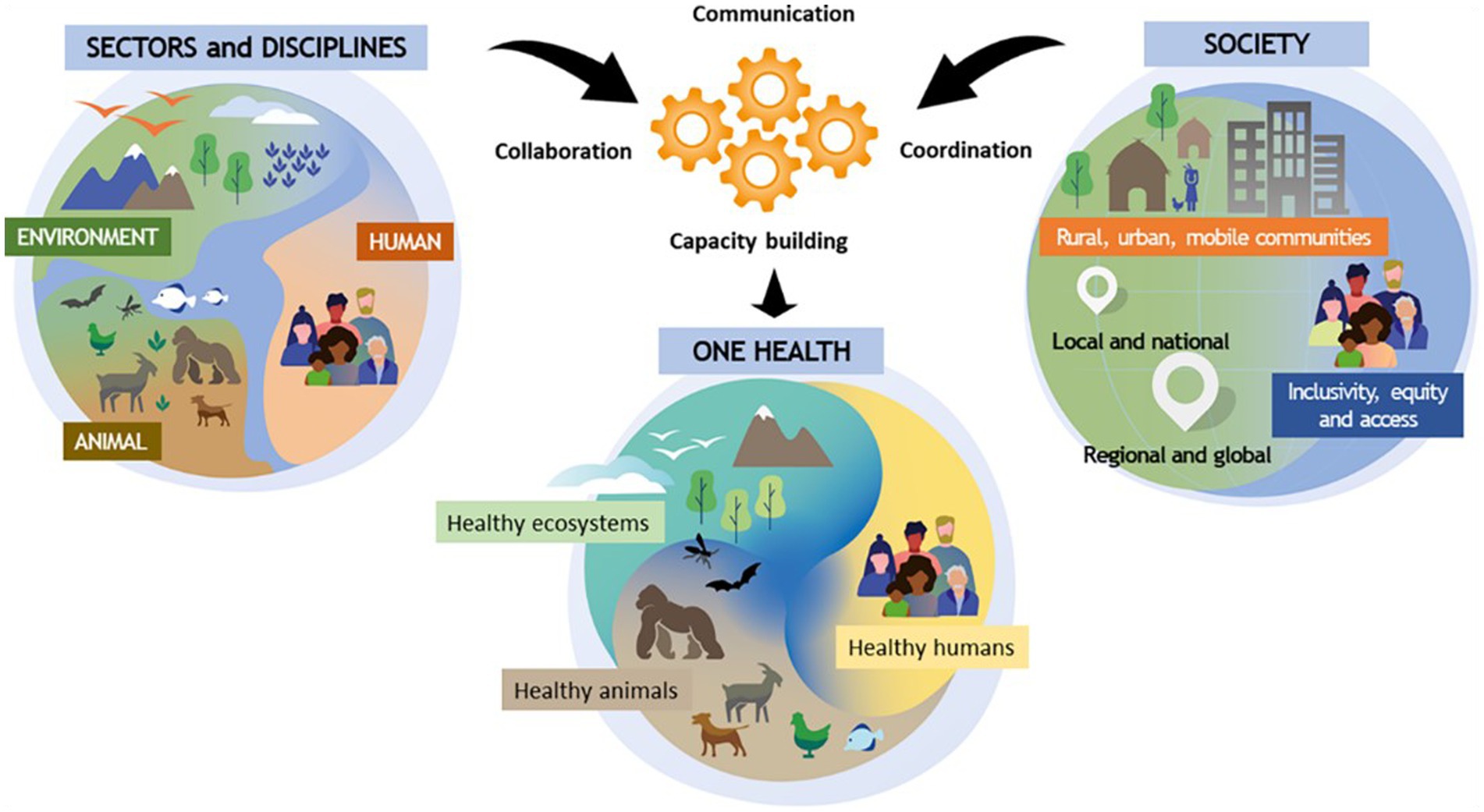
Figure 1. One Health as described by OHHLEP.
“One Health is an integrated, unifying approach that aims to sustainably balance and optimize the health of people, animals, and ecosystems.
It recognizes the health of humans, domestic and wild animals, plants, and the wider environment (including ecosystems) are closely linked and interdependent.
The approach mobilizes multiple sectors, disciplines, and communities at varying levels of society to work together to foster well-being and tackle threats to health and ecosystems, while addressing the collective need for clean water, energy and air, safe and nutritious food, taking action on climate change, and contributing to sustainable development.”
A One Health approach “mobilizes multiple sectors, disciplines and communities at varying levels of society to work together to foster well-being and tackle threats to health and ecosystems” with ‘Equality, inclusivity and access’ being identified as a key enabler of this process (2). A recent compilation of One Health Core Competencies by the Network for Ecohealth and One Health included ‘Social, cultural and gender equity and inclusiveness’ as a core value for teams working in this space, re-emphasizing the need for explicit consideration of gender in One Health (4). A recent analysis demonstrated a correlation between improved gender equity indicators and positive indicators of social and ecosystem performance and, whilst not proving a casual link, demonstrates the complex interplay between social, health and environmental outcomes (24).
Embedding gender and other identity markers into One Health research aids in better understanding risks at the human-animal-environment interface (25) and identifying possible synergies, such as the potential to improve detection of emerging zoonotic diseases by widening access of previously underserved groups of livestock keepers to veterinary extension service providers. It also helps to identify possible compromises and trade-offs, which can aid in decision-making about which interventions to prioritize and maximize on the “added” value of One Health to inform policies toward addressing disproportionate burden of diseases.
One of the biggest challenges in including gender considerations in One Health research is the breadth and complexity of the One Heath subject area. As OHHLEP’s definition implies, a One Health approach can be applied to a multitude of research areas and topics. Each health domain includes gender-relevant issues, and additional issues arise when we consider the interfaces between domains of One Health. While gender considerations are relevant to each of the three health domains separately, in the framework proposed here we focus on gender considerations that are relevant at the interface between at least two or all the three health domains. Such considerations may reveal how gender-based disadvantage has a compounding effect across the three health domains. For example, disadvantaged access to and control over land for women or poorer individuals may expose them to environments with a higher risk of zoonotic disease and increase their chances of infection. If their livestock are infected by a zoonotic disease, these groups or individuals may lack access to animal health care, with negative consequences on the productivity of their livestock. Lost income from their livestock assets could influence their ability to seek medical care, exponentially increasing the negative impacts of such initial exposure to risky environments for these individuals – as compared to others who are better positioned to reduce exposure to risks by accessing needed resources and services.
Conversely, applying a gender lens while identifying and applying One Health solutions provides an opportunity to address gender-based discrimination across the three health domains and avoid the spiraling negative impacts described above. For example, improving vaccination coverage for zoonoses through a gender responsive approach to vaccine delivery and knowledge transfer has the potential to improve environmental and human health outcomes through improved animal health (26). Other types of inequality may influence the ways in which women and men, boys and girls, experience disadvantage or privilege (7). By taking into account identity markers (e.g., ethnicity, age, religion) that may be relevant in a given context, gender analysis can reveal axes and processes of inequality between women and men, and, also, across women and across men (21). An approach or solution that applies in one social context may work less well or be more difficult to apply in a different context. It is always advisable to conduct gender analyses with an intersectional lens, meaning that more than one source of inequality is considered. For a practical example of this approach (see Tavenner, 2022).
The complexity of One Health interventions means they inherently require trade-offs or compromises. For example, when controlling zoonotic diseases, there may be a range of possible options, such as vaccinating livestock or humans; treating livestock or humans; changing to livestock management practices; or applying hygiene measures in slaughterhouses, food retailers, or homes. Considering gendered impacts in addition to economic considerations can guide selection of control measures. A One Health intervention focusing on disease control and livestock intensification may increase household income and food security for men, but have no improvement in food security for children, with negative consequences on women’s workload and nearby wildlife communities. Including gender considerations gives a more complete picture of the potential benefits and consequences of the proposed activities, identifies how benefits and risk are distributed, and tries to suggest interventions that will allow everyone in the community to benefit.
Interventions or activities that change the status quo, redistribute resources, or require time or labor to implement may bring negative, unintended consequences for less privileged groups of people. On the other hand, interventions that reflect the status quo may reproduce and aggravate gender disadvantaged labor allocation and resource distribution patterns. In a meta-analysis of the impact of livestock interventions on indicators of women’s empowerment, the most common negative consequence was an increase in women’s workload (27), as reported by a dairy intensification project in Uganda, for example (28). Family members who do not see the benefits of an innovation may oppose its adoption in the household, undermining the effectiveness of an intervention, as in the case of East Coast Fever infection and treatment method in Kenya (29). Increase in workload can be an acceptable change if it brings commensurate benefits (30). Gender analysis can help appreciate what intervention is more likely to bring equitable benefits in a given context. At the bare minimum, a One Health intervention should aim to “do no harm,” which is only possible if a project is considering the impact of gender dynamics and other identity markers to monitor for and mitigate potential unintended consequences.
The framework was developed by the co-authors through a series of discussions, which allowed the drafting of an initial framework. From here, literature review and subsequent discussions were used to refine and finalize the final framework. The co-authors are all researchers with experience implementing gender and/or One Health research.
The framework is designed to support development of key gender questions for the application of a gender lens to One Health research and to frame a discussion among multi-disciplinary researchers. The questions we are proposing are as simple and non-prescriptive as we can make them, given the complexity of the topic. We also indicate programmatic measures to be put in place for gender research to be supported effectively. We do not provide models, tools, methods, suggestions for specific interventions, or policy recommendations because these can only be shaped by projects based on the evidence that emerges when applying the proposed research questions. We consider four stages of research for development, beginning from the diagnostic stage when (1) a given situation is explored with a gender lens in order to (2) identify priority issues that need to be researched; to (3) producing evidence that is necessary for designing One Health interventions that respond to gendered needs and priorities; and leading finally to (4) framing of recommendations for wider-scale changes (shown in the top of Figure 2).
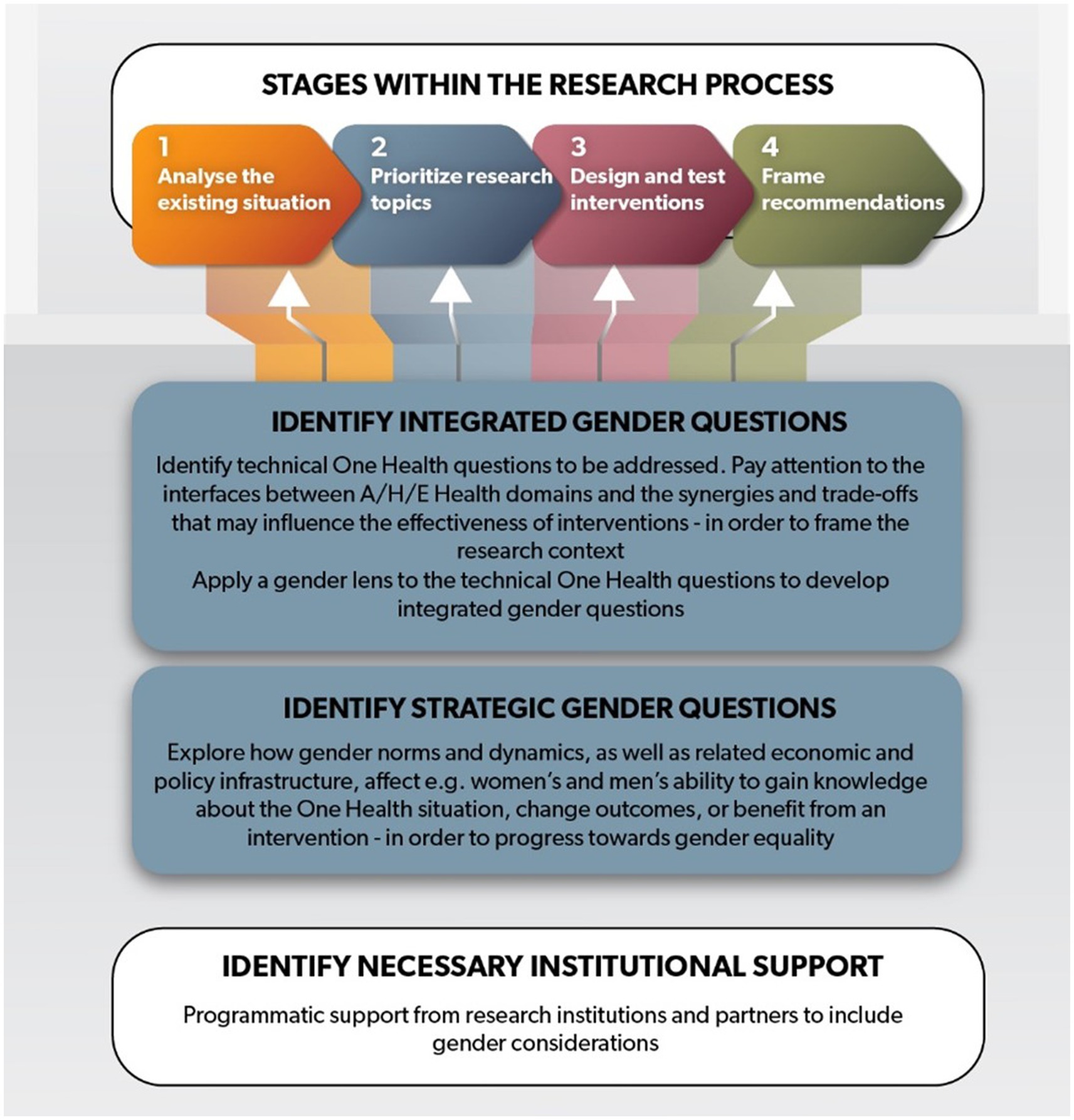
Figure 2. A framework for gender in One Health research. Every research stage involves identifying both integrated and strategic gender research questions and having underlying institutional support.
Research projects that incorporate gender considerations early and throughout the lifecycle of the research tend to have more successful and meaningful gender analyses and have the opportunity to identify and mitigate negative unintended consequences or help progress toward gender equality (8). At each research stage, the framework encourages researchers to identify gender research questions in two categories. For the first category, a technical question from a One Health domain or the interface between two domains is the entry point to thinking about gender issues. Gender issues are integrated in the technical ones to improve the latter’s relevance and effectiveness. For example, “what are the animal and human health impacts of zoonotic disease x?” might be a technical question at the interface between human and animal health. Asking “how are these impacts apportioned between men and women, boys and girls?” adds gender nuance. These types of questions may feel familiar to bioscientists, veterinarians, and epidemiologists.
For the second category, gender is the entry point applied to a technical issue. In this case, the intended outcome is often progression toward gender equality (although such research can also be necessary to improve a technical intervention). For example, asking “to what extent do gender norms affect the ability of men, women, boys, and girls to reduce the impact they experience from zoonotic disease x?” address the same One Health issue as the previous questions, namely impact of disease, but it puts gender concerns at the heart of the question. These types of questions may feel more familiar to social scientists and gender researchers.
Both integrated and strategic research questions are explained below in more detail. As previously mentioned, formulating research questions is an activity best for an interdisciplinary team because of the breadth of experience required to identify research questions in both technical and social categories and the inherently interdisciplinary nature of the One Health approach. The extent to which the final set of research questions will span both categories depends on the goals and objectives of the project, the expertise of the implementors, and the financial support and timeline. Underlying the process is identifying appropriate institutional support (as shown in white in Figure 2). The specific research questions identified, and the extent of institutional support required will help determine the most appropriate intervention approach. We discuss each component of the framework in more detail below.
Next, we describe each of the four stages of research in more detail. They are presented as a linear flow, but in some cases, it may be a more iterative and circular process whereby the results in one stage suggest returning to a previous stage. Institutional support and intervention approaches are also discussed.
Here the existing situation is explored, to identify where research may be needed. This enables researchers and practitioners to understand differences in exposures, preferences and priorities of men, women, girls, boys taking into account other social identity markers. Integrating gender considerations at this stage ensures that technical One Health questions are positioned within their social context in later stages of the research. This is also a good time to begin anticipating potential consequences and trade-offs of any proposed interventions or activities.
Integrating gender considerations at this stage affects the choice of One Health research topics by taking into account needs and preferences of men and women (across other individual markers). It also informs the way research is designed and undertaken and how interventions are implemented. For example, the choice of topic may be influenced by the priority that women, men, boys, and girls place on different livestock species, or their different exposure to health and environmental risks at home and along livestock value chains; other factors such as poverty, ethnicity and disability may also affect their priorities. The design of a research project on food safety or zoonotic disease control within households may be influenced by our understanding of gender norms, which affect household members’ knowledge of a problem and their ability to change what they do.
Assessing how a planned intervention may interact with local gender dynamics and norms, and consequently how effective and equitable it may be in the benefit it brings, is important to improve the intervention at the development stage. Assessing the performance of the actual intervention on the ground, with a gender lens, can help refine it for both effectiveness and equity outcomes for new rounds of ground testing before scaling. In the “Intervention approaches” section, we further describe two types of approaches that can be used in gender research.
Recommendations for the scaling of successful One Health interventions needs to be based on the evidence that emerges from the testing of interventions (stage 3). Because gender dynamics and norms are context specific, scaling of pilot interventions to other geographical areas can bring new complications as new gender dynamics may be at play. Recommendations need to carefully consider to what extent the findings produced by this framework can be generalized and how, in line with best practices of qualitative research.
Here, we describe the two categories of gender research questions that can be considered for inclusion in more detail, as shown in the blue boxes in Figure 2.
“Integrated” gender questions explore the way problems and proposed interventions may differently affect women, men, boys, and girls. They take a technical livestock topic as an entry point and bring a gender lens to that topic. For example, integrating gender considerations into a tool to assess which forage varieties are a good fit for a community allows the identification of varieties appropriate for a given farm where women’s labor is more prevalent than men’s. Using a One Health example, gender roles in hunting wild animals, cleaning carcasses, and managing livestock may affect the way zoonotic diseases are passed between wildlife and livestock and to different members of a household; a successful intervention will need to identify, target, and communicate with those most involved in all of these roles.
“Strategic” gender questions are questions where gender issues are the focus of the study and the entry point to solving a One Health problem. They take a specific gender issue as an entry point and explore the wider gender norms and dynamics that drive the reasons for gendered differences. For example, a strategic gender question might aim to understand how changes in empowerment may differ between women and men, girls and boys in livestock communities. The decisions each person is able to make can affect the way they use environmental resources such as water or roadside forage, and the extent to which they are able to change what they do to make more effective use of resources or reduce their workload. Strategic gender questions may help to identify ways to leverage One Health interventions to progress toward gender equality.
To appreciate the importance of both strategic and integrated gender questions it is important to acknowledge that gender equity and One Health interventions are mutually supporting goals. Equitable One Health interventions are more likely to be successful when all actors are supported to adopt them, and when they see the benefits they may gain. One Health interventions, on the other hand, are essential to progress toward gender equity to avoid that the possible spiraling effects of gender-based discrimination across the three health domains strongly disadvantage a gender group (Figure 3).

Figure 3. The interrelation between gender equity and One Health.
‘Gender norms’ are an important focus of gender strategic research. Gender norms are the unwritten rules that define and normalize as appropriate given identities, roles and actions for a gender. Gender norms affect who can do what kind of work, control what types of assets and make what level of decisions. They vary by context and time (8). Studying gender norms is essential to understand the processes behind gender-based discrimination.
Table 1 develops the concept of integrated and strategic gender questions by providing examples of typical questions that might be applied at each research stage of One Health.
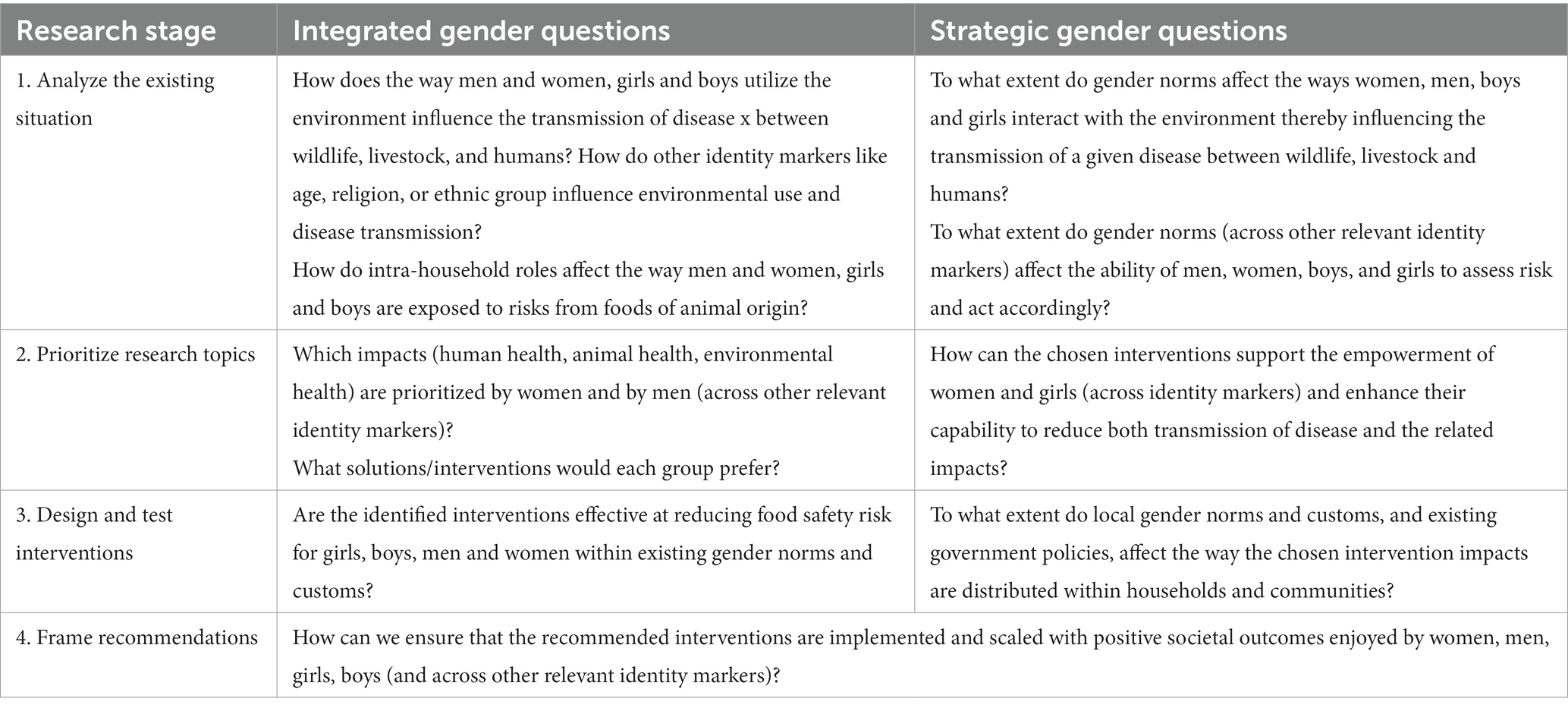
Table 1. Key integrated and strategic gender questions at each research stage of One Health.
Many of the questions included in the framework and Table 1 are qualitative given the exploratory nature of gender research in One Health at this point in time (when little is known still, about the ways in which gender dynamics and norms are relevant to One Health). However, depending on the methods used, they could also be answered quantitatively. Qualitative evidence can support the identification of key gender issues that can then be further explored using a combination of qualitative and quantitative research methods (31).
Institutional support is essential for integrating gender into research and effectively implementing the framework, so we explicitly include it as one of the components of the framework. It underpins all research stages. Institutional support includes arrangements with donors, capacity and willingness of the research institution to support gender research and interdisciplinary projects, and relationships with implementing partners which could include universities, non-governmental organizations (NGOs), government agencies, or private sector. An essential element of institutional support is ensuring that social science and gender expertise is included within research teams at all stages of the process. Following best practices in gender research has budget implications. For example, field research is designed in a way that allows men and women to be separately interviewed or separately consulted. This may involve additional staffing and inclusion of both men and women on data collection teams. Communities may be facilitated to discuss gender roles [such as the community conversations used by the One Health for Humans, Animals, Environment, and Livelihoods (HEAL) project (31)]. Analysis of qualitative data may require transcription and/or translation, which is time consuming and costly.
In our framework, Stage 3 is about identifying key gender questions for the designing and testing interventions that respond to gendered needs, priorities, and dynamics. Here we provide additional information about the type of interventions that could be considered for a project after reviewing the integrated and strategic research findings.
Two main types of intervention approaches that respond to gendered evidence are accommodative and transformative. Accommodative approaches develop interventions that reflect the existing gender dynamics and norms (e.g., engaging farm women in identifying sick animals and men vets in providing and administering veterinary drugs in a community where this is the typical division of labor). Transformative approaches address and challenge gender discriminating norms, practices, and beliefs [e.g., involving women farmers in identifying sick animals and also striving to engage women – who may be interested in providing animal health services but may be discouraged by gender norms to do so – thereby providing business opportunities for them (32)]. In a project aimed at improving the uptake of animal vaccines in northern Ghana, addressing restrictive gender norms at the project outset was essential to create a conducive social environment for animal vaccines to be adopted by the communities (32). Restrictive norms discouraged women farmers from rearing livestock, assigned only men the burden of providing for the household, and prevented women from working as veterinarians. Gender strategic questions are particularly important to develop transformative approaches by exploring, for example, gendered aspirations and challenges to empowerment.
The next section shows how the framework can be applied in practice, using a worked example.
To illustrate the application of the framework, we have used an example of research into the control of Taenia solium cysticercosis (T. solium), popularly known as the pork tapeworm. T. solium is an internal parasite which causes disease in humans and pigs. It is one of the leading causes of acquired epilepsy for people in endemic areas (33), primarily low- and middle-income countries in sub-Saharan Africa, Latin America, and Southeast Asia (34). The burden of this disease has been estimated as approximately 2.78 million Disability Adjusted Life Years (DALYs) globally (35). T. solium causes three diseases: taeniasis and neurocysticercosis in humans and porcine cysticercosis in pigs (36). Humans acquire taeniasis (a tapeworm infection) when they eat raw or undercooked pork meat contaminated with cysticerci, the larval form of T. solium. When ingested, the cysticerci establish in the intestine of humans, become adult tapeworms, and shed eggs in human feces that can infect in turn other humans and pigs by direct contact or by indirect contamination of water or food. Figure 4 illustrates typical transmission routes.

Figure 4. Taenia solium transmission routes. Reused with permission from (38).
The likelihood of transmission of T. solium is influenced by factors including the proximity of people to the pigs they are rearing, how the pigs are kept (e.g., production system and housing), access to restrooms and sanitation facilities, hygiene practices, and dietary practices and preferences. Gender dynamics and the social context shape the differentiated roles women and men have in pig production with implications on exposure to disease. For example, in a recent study in Vietnam, both women and men were found to participate in the pig value chain but performed different tasks. Women did more routine husbandry activities such as cleaning pens and pork processing while men were more responsible for disease management, slaughtering, and large-scale farming (37).
Although gender disaggregated data on disease burden are not yet readily available, preliminary data suggest the burden of T. solium infections may vary by gender. In a study of hospital patients in Ecuador, there were differences in the presentation of neurocysticercosis, with female patients harboring more transitional cysts (those with inflammation surrounding them, indicative of a greater immune response). These transitional cysts put women at higher risk of developing servere complications such as encephalitis (39). It is not known the extent to which these differences are related to biological differences between males and females; to gendered differences in risk factors for infection such as access to healthcare, and other social determinants of health; or to the interaction of all of these factors.
When analyzing the existing situation, integrated and strategic gender questions can be used to explore some of the above issues, as demonstrated in Table 2.
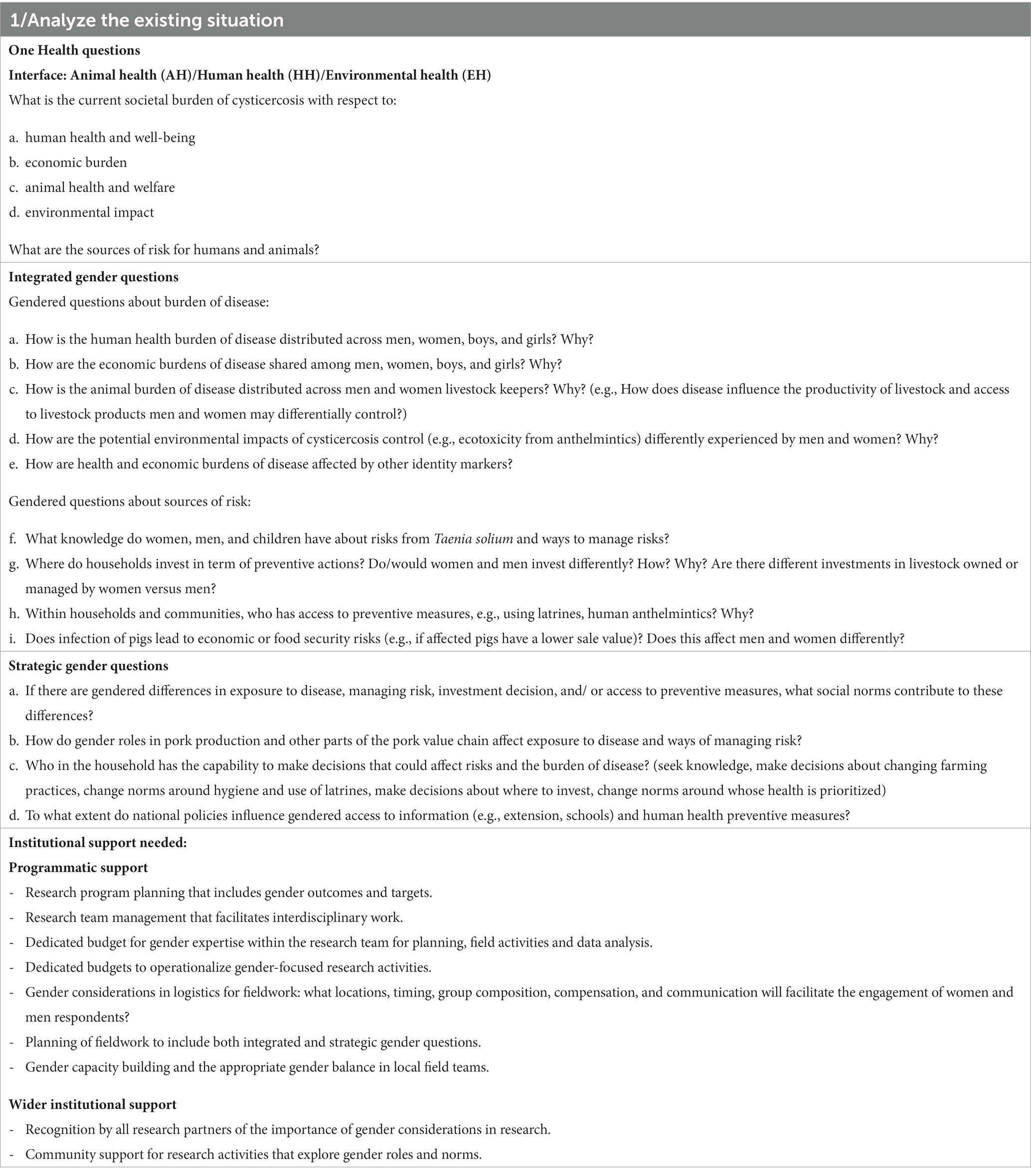
Table 2. Applying the gender and one health framework to Taenia solium: Research Stage 1.
Stage 2 of the research process involves continuing to define and prioritize research topics, which in this case study, was interpreted as prioritizing control measures. Reducing the risk associated with pork consumption in the developing world is a public health priority as laid out in the World Health Organization roadmaps for Neglected Tropical Diseases (40, 41). Prevention and control measures to break the cycle of infection can potentially include household hygiene (e.g., use of latrines, handwashing), pharmaceutical treatment of infected pigs and/or humans, or vaccination of pigs (42). In recent years, research efforts have focused on testing known interventions and understanding the barriers to control. Appropriately identifying the people and groups to target is important to underpin success of interventions. The best way to do this is to consider the needs and preferences of the target audience even when selecting the choice of interventions to be tested. Table 3 shows examples of integrated and strategic gender questions that may guide the choice of T. solium control measures to be investigated. The necessary institutional support is also listed; although this may be similar at each stage, explicitly considering it at each stage ensures that it is not forgotten.

Table 3. Applying the gender and one health framework to Taenia solium: Research Stage 2.
In Stage 3, questions are asked so that interventions are designed and tested in gender-equitable ways. Based on the produced evidence projects can decide whether to take a gender accommodative and/or a gender transformative approach. For example, if the evidence shows that gender norms hinder men’s ability to engage in household hygiene practices, then an intervention may be designed to address such gender norms.
Site-specific contextual issues affect implementation and uptake of the interventions. Some aspects of the context include understanding the socioeconomic aspects encompassing gender related issues of the target population as described in Ngwili et al. (36). Gender norms and customs may also create barriers to adoption of control practices like the use of toilets and access to information on improved pig husbandry (36, 43). Addressing these gender-related issues requires a multifaceted approach. Gender considerations become very important due to issues related to decision making and control of resources within the households. For example, interventions focusing on health education may need to consider gender dynamics in the household (who makes decisions about health in the household) so that knowledge uptake translates to change in practices. Men may have control over who attends the training sessions even if they are not involved in actual implementation of the new practices. Some interventions such as the mass distribution of anthelminthic drugs often target children but will need support from parents (both men and women) to be effective (44, 45). These and other lessons on how failure to understand gender dynamics can affect implementation and uptake of interventions against T. solium have been discussed in two previous studies (25, 36).
Table 4 shows the framework applied to Stage 3 of the framework, designing and testing T. solium control measures.
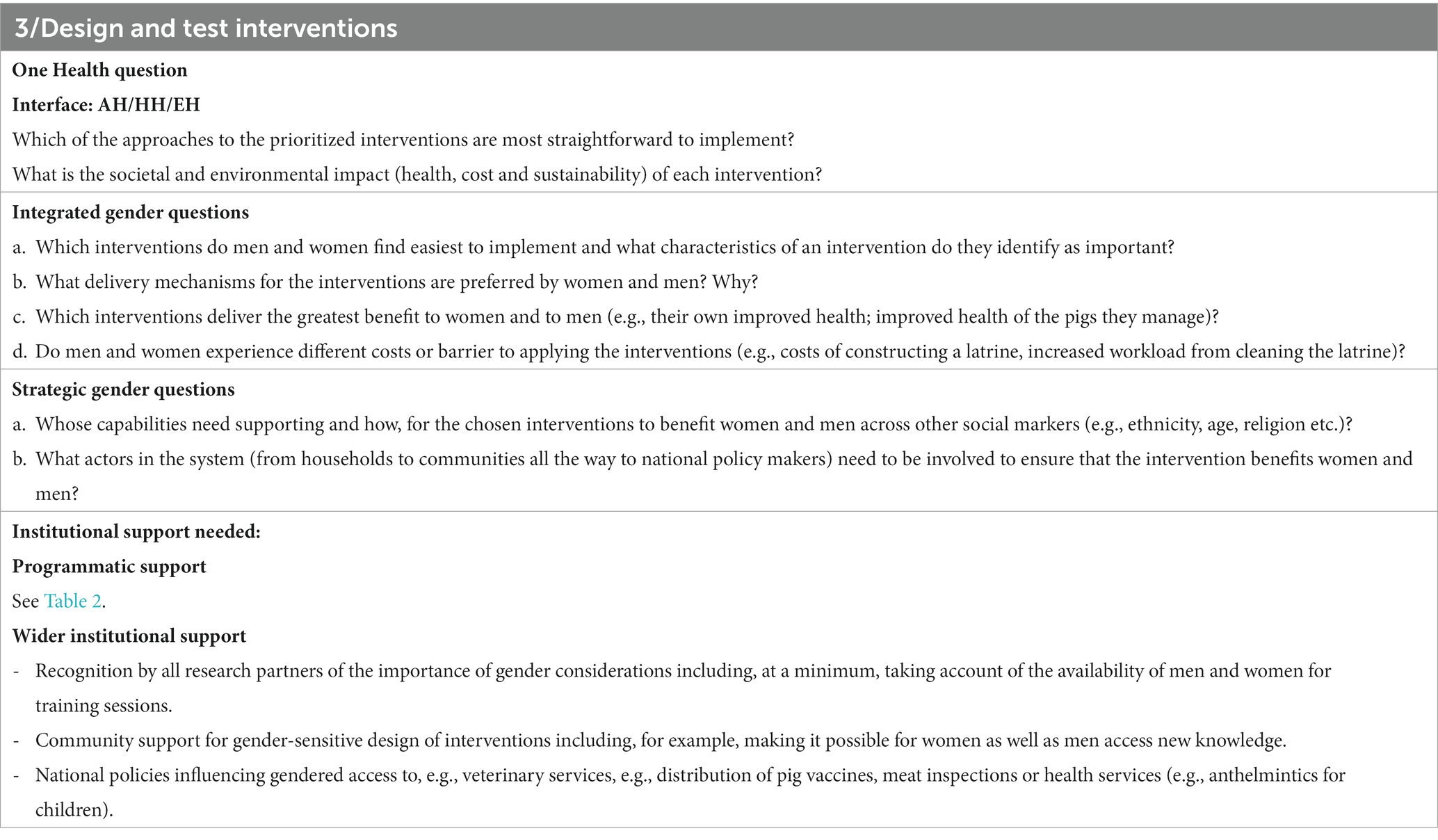
Table 4. Applying the gender and one health framework to Taenia solium: Research Stage 3.
Stage 4, the final research stage included in the framework, involves including considerations that help framing the recommendations arising from the previous three stages – these might involve, for example, scaling up of applied research to test implementations in a wider range of situation, or taking research findings into a delivery phase. Table 5 illustrates how research-to-delivery recommendations for T. solium control can acknowledge gender dynamics. At this stage, instead of integrated and strategic questions, we recommend including integrated and strategic gender considerations, which should influence the way the research findings are taken forward.
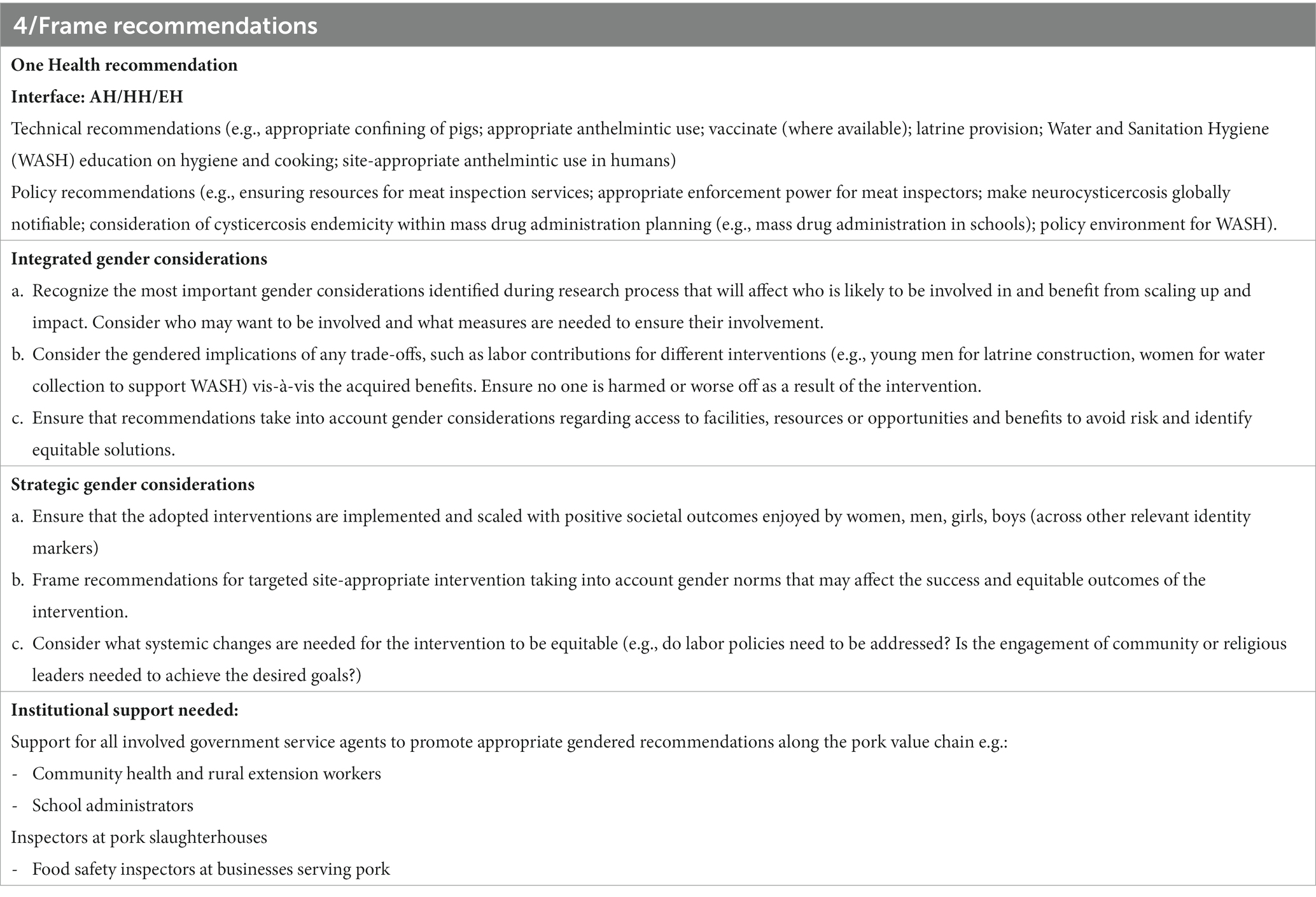
Table 5. Applying the gender and one health framework to Taenia solium: Research Stage 4.
We have presented a framework to include gender considerations in One Health research. The framework helps to highlight both why gender considerations are relevant to One Health and how One Health can help progress toward gender equality; it suggests key gender questions that may be asked to appreciate how gender dynamics may interact with a One Health intervention; and it illustrates the application of the questions to research into the control of T. solium. Acknowledging, and gaining a deep understanding of the influence of gender dynamics can help interventions be adopted, minimize negative consequences, and support progression to a more equitable society. This framework supports conversations within interdisciplinary teams, emphasizing the need to consider gender throughout the lifecycle of the research project, develop both integrated and strategic gender questions, and to acquire appropriate institutional support. The inclusion of strategic research questions – which use gender as an entry-point and whose findings can inform gender transformative approaches – supports One Health teams to challenge the existing gender norms that limit the ability for some groups of people to adopt and benefit from interventions. Such efforts are vital if One Health is to improve ‘equality, inclusiveness and access’ as a societal mechanism for the improvement of health across human, animal and environmental domains as urged by the OHHLEP definition of One Health.
AG: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing. AM: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. ZC: Visualization, Writing – review & editing. NN: Writing – review & editing. ZT: Writing – review & editing. LT: Conceptualization, Methodology, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. We are thankful for the support by the German Federal Ministry for Economic Cooperation and Development through the One Health Research, Education and Outreach Centre in Africa (OHRECA); the Sustainable Animal Productivity for Livelihoods, Nutrition and Gender Inclusion (SAPLING) Initiative, and the One Health Initiative which are grateful for the support of CGIAR Trust Fund Contributors. We thank all donors and organizations who globally supported its work through their contributions to the CGIAR Trust Fund https://www.cgiar.org/funders/.
Thank you to Annabel Slater at the International Livestock Research Institute (ILRI) for designing Figure 2.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Evans, BR , and Leighton, FA . A history of one health. Rev Sci Tech. (2014) 33:413–20. doi: 10.20506/rst.33.2.2298
2. Adisasmito, WB , Almuhairi, S , Behravesh, CB , Bilivogui, P , Bukachi, SA , Casas, N, et al. One health: a new definition for a sustainable and healthy future. PLOS Pathog. (2022) 18:e1010537. doi: 10.1371/journal.ppat.1010537
4. Laing, G , Duffy, E , Anderson, N , Antoine-Moussiaux, N , Aragrande, M , Luiz Beber, C, et al. Advancing one health: updated core competencies. CABI One Heal. (2023). doi: 10.1079/cabionehealth.2023.0002
5. Van Patter, LE , Linares-Roake, J , and Breen, AV . What does one health want? Feminist, posthuman, and anti-colonial possibilities. One Heal Outlook. (2023) 5:1–9. doi: 10.1186/s42522-022-00076-9
6. Ridgeway, CL , and Correll, SJ . Unpacking the gender system. Gend Soc. (2004) 18:510–31. doi: 10.1177/0891243204265269
7. Tavenner, K , Crane, TA , Bullock, R , and Galiè, A . Intersectionality in gender and agriculture: toward an applied research design. Gend Technol Dev. (2022) 26:385–403. doi: 10.1080/09718524.2022.2140383
8. Galiè, A , Pyburn, R , Baltenweck, I , and Quintero, S . Institutional and theoretical learning on gender analysis through the CGIAR research program on livestock. Nairobi, Kenya: International Livestock Research Institute (ILRI). (2022).
9. Secretary-General; UN . Human rights council. Protection against violence and discrimination based on sexual orientation and gender identity. (2019). Available at: https://digitallibrary.un.org/record/3823802
10. Baudin, M , Jumaa, AM , Jomma, HJE , Karsany, MS , Bucht, G , Näslund, J, et al. Association of Rift Valley fever virus infection with miscarriage in Sudanese women: a cross-sectional study. Lancet Glob Heal. (2016) 4:e864–71. doi: 10.1016/S2214-109X(16)30176-0
11. Namatovu, J , Campbell, Z , and Ouma, E . The role of gender dimensions in the transmission and control of Rift Valley fever in Uganda. Nairobi, Kenya (2021). Available at: https://hdl.handle.net/10568/111784
12. Kurpiers, LA , Schulte-Herbrüggen, B , Ejotre, I , and Reeder, DM . Bushmeat and emerging infectious diseases: lessons from Africa In: Angelici FM, editor. Problematic wildlife. Cham: Springer International Publishing (2016). 507–51.
13. Bandiera, O , Buehren, N , Goldstein, M , Rasul, I , and Smurra, A . The economic lives of young women in the time of Ebola: Lessons from an empowerment program [internet]. Washington, DC: World Bank (2019).
14. Wenham, C , Smith, J , Davies, SE , Feng, H , Grépin, KA , Harman, S, et al. Women are most affected by pandemics — lessons from past outbreaks. Nature. (2020) 583:194–8. doi: 10.1038/d41586-020-02006-z
15. Wenham, C , Smith, J , and Morgan, R . COVID-19: the gendered impacts of the outbreak. Lancet. (2020) 395:846–8. doi: 10.1016/S0140-6736(20)30526-2
16. Jones, N , Mitchell, J , Cooke, P , Baral, S , Arjyal, A , Shrestha, A, et al. Gender and antimicrobial resistance: what can we learn from applying a gendered Lens to data analysis using a participatory arts case study? Front Glob Women’s Heal. (2022) 3:3. doi: 10.3389/fgwh.2022.745862/full
17. Colverson, KE , Harris, LC , Galie, A , Moore, EV , Munoz, O , McKune, SL, et al. Evolution of a gender tool: WEAI, WELI and livestock research. Glob Food Sec. (2020) 26:100375. doi: 10.1016/j.gfs.2020.100375
18. Eba, E , Wieland, B , Flintan, F , Njiru, N , and Baltenweck, I . Gender and One Health context analysis for HEAL. Nairobi, Kenya: International Livestock Research Institute (ILRI). (2020).
19. International Livestock Research Institute (ILRI) . International livestock research institute. ILRI annual report. (2019). Available at: https://www.ilri.org/research/annual-report/2019/
20. Morgan, R , Davies, SE , Feng, H , Gan, CCR , Grépin, KA , Harman, S, et al. Using gender analysis matrixes to integrate a gender lens into infectious diseases outbreaks research. Health Policy Plan. (2022) 37:935–41. doi: 10.1093/heapol/czab149
21. World Health Organization . Gender and health. (2023). Available at: https://www.who.int/health-%0D%0Atopics/gender#tab=tab_1
22. Rüegg, SR , Buttigieg, SC , Goutard, FL , Binot, A , Morand, S , Thys, S, et al. Editorial: concepts and experiences in framing, integration and evaluation of one health and EcoHealth. Front Vet Sci. (2019) 6:155. doi: 10.3389/fvets.2019.00155/full
23. Lerner, H , and Berg, C . A comparison of three holistic approaches to health: one health, EcoHealth, and planetary health. Front Vet Sci. (2017) 4:163. doi: 10.3389/fvets.2017.00163/full
24. Cataldo, C , Bellenghi, M , Masella, R , and Busani, L . One health challenges and actions: integration of gender considerations to reduce risks at the human-animal-environmental interface. One Heal. (2023) 16:100530. doi: 10.1016/j.onehlt.2023.100530
25. de Coster, T , Van Damme, I , Baauw, J , and Gabriël, S . Recent advancements in the control of Taenia solium: a systematic review. Food Waterborne Parasitol. (2018) 13:e00030. doi: 10.1016/j.fawpar.2018.e00030
26. Omondi, I , Galiè, A , Teufel, N , Loriba, A , Kariuki, E , and Baltenweck, I . Women’s empowerment and livestock vaccination: evidence from Peste des Petits ruminants vaccination interventions in northern Ghana. Animals. (2022) 12:2–24. doi: 10.3390/ani12060717
27. Quisumbing, A , Cole, S , Elias, M , Faas, S , Galiè, A , Malapit, H, et al. Measuring Women’s empowerment in agriculture: innovations and evidence. Glob Food Sec. (2023) 38:100707. doi: 10.1016/j.gfs.2023.100707
28. Bain, C , Ransom, E , and Halimatus’adiyah, I . ‘Weak winners’ of Women’s empowerment: the gendered effects of dairy livestock assets on time poverty in Uganda. J Rural Stud. (2018) 61:100–9. doi: 10.1016/j.jrurstud.2018.03.004
29. Jumba, H , Teufel, N , Baltenweck, I , de Haan, N , Kiara, H , and Owuor, G . Use of the infection and treatment method in the control of East Coast fever in Kenya: does gender matter for adoption and impact? Gend Technol Dev. (2020) 24:297–313. doi: 10.1080/09718524.2020.1829359
30. Galiè, A , and Kantor, P . From gender analysis to transforming gender norms: using empowerment pathways to enhance gender equity and food security in Tanzania In: Njuki J, Parkins J, Kaler A, editors. Transforming gender and food security in the global south. London: International Development Research Centre (IDRC) and Routledge (2016)
31. Mwakanyamale, D , Cole, S , Heckert, J , John, I , Fischer, G , Seymour, G, et al. A process guide for the development of a mixed-methods research tool for measuring and understanding intra-household decision making. (2022). Available at: https://ebrary.ifpri.org/digital/collection/p15738coll2/id/136594
32. Njiru, N , Galiè, A , Wanyoike, F , Tawanda, M , Boonabaana, B , Bisikwa, J, et al. Exploration of gender dynamics in the production and marketing of forage technologies in Kenya. Front Animal Sci. (2023) 4:1113243. doi: 10.3389/fanim.2023.1113243
33. Ndimubanzi, PC , Carabin, H , Budke, CM , Nguyen, H , Qian, Y-J , Rainwater, E, et al. A systematic review of the frequency of Neurocyticercosis with a focus on people with epilepsy. PLoS Negl Trop Dis. (2010) 4:e870. doi: 10.1371/journal.pntd.0000870
34. Ouma, E , Dione, M , Mtimet, N , Lule, P , Colston, A , Adediran, S, et al. Demand for Taenia solium Cysticercosis vaccine: lessons and insights from the pig production and trading nodes of the Uganda pig value chain. Front Vet Sci. (2021) 8:611166. doi: 10.3389/fvets.2021.611166/full
35. Havelaar, AH , Kirk, MD , Torgerson, PR , Gibb, HJ , Hald, T , Lake, RJ, et al. World health organization global estimates and regional comparisons of the burden of foodborne disease in 2010. PLoS Med. (2015) 12:e1001923. doi: 10.1371/journal.pmed.1001923
36. Ngwili, N , Johnson, N , Wahome, R , Githigia, S , Roesel, K , and Thomas, L . A qualitative assessment of the context and enabling environment for the control of Taenia solium infections in endemic settings. PLoS Negl Trop Dis. (2021) 15:e0009470. doi: 10.1371/journal.pntd.0009470
37. Nguyen-Thi-Duong, N , Pham-Van, H , Duong-Nam, H , Nguyen-Thi-Thu, H , Ninh-Xuan, T , Dang-Xuan, S, et al. Gender-focused analysis and opportunities for upgrading within Vietnam’s smallholder pig value chains. Front Vet Sci. (2022) 9:906915. doi: 10.3389/fvets.2022.906915/full
38. Soare, C , Garcia-Ara, A , Seguino, A , Uys, M , and Thomas, LF . Maximising Societal Benefit From the Control of Neglected Zoonoses: identifying synergies and trade-offs in the control of taenia solium. Front. Vet. Sci. (2022) 8. doi: 10.3389/fvets.2021.794257
39. Kelvin, EA , Carpio, A , Bagiella, E , Leslie, D , Leon, P , Andrews, H, et al. The association of host age and gender with inflammation around neurocysticercosis cysts. Ann Trop Med Parasitol. (2009) 103:487–99. doi: 10.1179/000349809X12459740922291
40. Savioli, L , and Daumerie, D . Accelerating work to overcome the global impact of neglected tropical diseases: a roadmap for implementation. Geneva, Switzerland: World Heal Organ (2012).
41. World Health Organization . Ending the neglect to attain the sustainable development goals: A rationale for continued investment in tackling neglected tropical diseases 2021–2030. Geneva, Switzerland: WHO (World Health Organization) (2022).
42. Bardosh, K , Inthavong, P , Xayaheuang, S , and Okello, AL . Controlling parasites, understanding practices: the biosocial complexity of a one health intervention for neglected zoonotic helminths in northern Lao PDR. Soc Sci Med [Internet]. (2014) 120:215–23. doi: 10.1016/j.socscimed.2014.09.030
43. Thys, S , Mwape, KE , Lefèvre, P , Dorny, P , Marcotty, T , Phiri, AM, et al. Why latrines are not used: communities’ perceptions and practices regarding latrines in a Taenia solium endemic rural area in eastern Zambia. PLoS Negl Trop Dis. (2015) 9:e0003570. doi: 10.1371/journal.pntd.0003570
44. Mitchell, E , Kelly-Hanku, A , Krentel, A , Romani, L , Robinson, LJ , Vaz Nery, S, et al. Community perceptions and acceptability of mass drug administration for the control of neglected tropical diseases in Asia-Pacific countries: a systematic scoping review of qualitative research. PLoS Negl Trop Dis. (2022) 16:e0010215. doi: 10.1371/journal.pntd.0010215
45. Akinsolu, FT , Abodunrin, OR , Olagunju, MT , Adewole, IE , Rahman, NO , Dabar, AM, et al. Community perception of school-based mass drug administration program for soil-transmitted helminths and schistosomiasis in Ogun state, Nigeria. PLoS Negl Trop Dis. (2023) 17:e0011213. doi: 10.1371/journal.pntd.0011213
Keywords: gender, One Health, framework, T. solium, equity
Citation: Galiè A, McLeod A, Campbell ZA, Ngwili N, Terfa ZG and Thomas LF (2024) Gender considerations in One Health: a framework for researchers. Front. Public Health. 12:1345273. doi: 10.3389/fpubh.2024.1345273
Edited by:
Myer Glickman, Office for National Statistics, United KingdomReviewed by:
Henrik Lerner, Marie Cederschiöld University, SwedenCopyright © 2024 Galiè, McLeod, Campbell, Ngwili, Terfa and Thomas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alessandra Galiè, YS5nYWxpZUBjZ2lhci5vcmc=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.