 Ning Sulistiyowati1Dwi Hapsari Tjandrarini1
Ning Sulistiyowati1Dwi Hapsari Tjandrarini1 Christiana Rialine Titaley2*Bertha J. Que2
Christiana Rialine Titaley2*Bertha J. Que2 Puti Sari Hidayangsih1
Puti Sari Hidayangsih1 Suparmi1Sudikno Sudikno1
Suparmi1Sudikno Sudikno1 Yuni Purwatiningsih1Lely Indrawati1Selma Siahaan1
Yuni Purwatiningsih1Lely Indrawati1Selma Siahaan1 Windy Pradita Adyarani3
Windy Pradita Adyarani3- 1Research Center for Public Health and Nutrition, National Research and Innovation Agency, Bogor, Indonesia
- 2Faculty of Medicine, Pattimura University, Ambon, Indonesia
- 3Bekasi General Hospital, Bekasi, Indonesia
Background: Infections continue to be a major cause of death among children under the age of five worldwide. This study aimed to identify the factors associated with the development of multiple infectious diseases in children aged 24–59 months in Indonesia.
Methods: Data from the 2018 Basic Health Research conducted by the Ministry of Health, Republic of Indonesia, were used. Information from 39,948 children aged 24–59 months was analyzed. The outcome variable was the development of multiple infectious diseases, that is, acute respiratory infections, pneumonia, pulmonary tuberculosis, diarrhea, and hepatitis, in the month before the survey. Factors significantly associated with multiple types of infectious diseases were examined using logistic regression.
Results: The study found that 76.6% of children aged 24 to 59 months in Indonesia had at least one type of infectious disease. The likelihood of developing multiple types of infectious diseases increased in children whose parents did not practice appropriate handwashing with soap and running water [adjusted odds ratio (aOR) = 1.16, p < 0.001], those who received supplemental food (aOR = 1.38, p < 0.001), those with poor nutritional status (aOR = 1.12, p < 0.001), and those living in urban areas (aOR = 1.07, p = 0.045).
Conclusion: Improving caregivers’ awareness of adequate child healthcare practices, in addition to nutrition-sensitive and specific interventions to improve children’s nutritional status, is required to prevent children from contracting multiple types of infectious diseases.
1 Introduction
In 2019, approximately 5.3 million children under 5 years of age died, mostly from preventable causes (1). Globally, premature birth and birth complications (such as birth asphyxia/trauma), acute respiratory infections (ARIs), diarrhea, and malaria continue to be the leading causes of preventable death among children under 5 years of age (1, 2). In Indonesia, pneumonia (14.5%) and diarrhea (9.8%) were the leading causes of death among children aged 29 days to 11 months (3). Indonesia Basic Health Research in 2018 reported that 2.1 and 6.8% of children under 5 years of age have ever been diagnosed with pneumonia and diarrhea, respectively (4).
Multiple factors are reportedly associated with the occurrence of infectious diseases among children under 5 years of age. This includes a lack of access to and availability of health services, leading to delayed treatment and prolonged disease occurrence and severity (5, 6). Poor environmental health, such as a lack of safe water and sanitation, also contributes to child morbidity (7–9). At the same time, appropriate handwashing practice has been identified as one of the most prominent and affordable hygiene practices for reducing infectious diseases, such as diarrhea and respiratory infections (10).
Moreover, malnutrition has been reported to be the underlying reason for an increased risk of bacterial gastrointestinal and respiratory infections (11). A previous study highlighted the reciprocal association between malnutrition and infection because malnourished children are more likely to become infected, and recurrent infections frequently contribute to malnutrition (12). Malnutrition makes children more vulnerable to disease and death (13). Although substantial progress has been made in reducing childhood malnutrition globally, Indonesia still faces high levels of malnutrition. The National Nutritional Survey conducted in 2021 showed that a quarter of underweight children in Indonesia were stunted (24.4%), 7.1% were wasted, and 17% were underweight (14).
Various studies have investigated the relationship between nutritional status and morbidity (12, 15, 16); however, few have explored the determinants of multiple infectious diseases among children in Indonesia. Therefore, using nationally representative data, this study aimed to examine factors associated with the development of multiple infectious diseases in children aged 24 to 59 months in Indonesia. Policymakers and program managers could use the findings to design and implement evidence-based strategies to improve children’s health status by controlling factors contributing to the development of multiple infections among children in Indonesia.
2 Methods
2.1 Data sources
Data were obtained from the 2018 Basic Health Research conducted by the Ministry of Health, Republic of Indonesia. Using the multistage sampling method, the 2018 Basic Health Research was conducted in all 34 provinces of Indonesia, representing Indonesia’s district/city level. A detailed explanation of the survey method is provided elsewhere (4).
In this analysis, only information from children aged 24–59 months was used. Children in this age range were expected to have completed their basic immunization schedule beyond their lactation period (up to 23 months of age). Information from 39,948 children aged 24–59 months was analyzed. Data were obtained from household interviews and anthropometric measurements of the children.
This analysis used two anthropometric measurements in children aged 24–59 months: body weight and height/length. During data collection, the anthropometric measurements were performed by two personnel. The first person acted as the measurer, and the second person recorded the results. Height measuring devices measured the children’s heights with a measuring capacity of 2 m and an accuracy of 0.1 cm. Body weight was measured using a digital scale with a precision of 0.1 kg. All field personnel were trained to standardize the measurement procedures in the field.
2.2 Outcome variable
The dependent variable in this analysis was a history of multiple infectious diseases in children aged 24–59 months. Infectious diseases examined were ARIs, pneumonia, tuberculosis (TB), diarrhea, and hepatitis. This variable was classified into two groups: none or single type if the child had never or developed only one type of infectious disease, and multiple types if the child had two or more types of infectious disease in the past month.
2.3 Independent variables
Independent variables were divided into four categories: (1) environmental factors; (2) parents’ high-risk behaviors; (3) children’s nutritional status; and (4) provision of supplementation and immunization (Figure 1). Environmental factors included type of residence (urban/rural) and housing density. The housing density variable was constructed based on two criteria: a minimum housing area of 8 m2 per person, and the number of children under 5 years living in a house. The first category of housing density was children in the house, which met the minimum housing area criteria and had a maximum of two children in the house. The second category included children who did not meet the minimum housing area criteria or with two or more children under the age of 5 years in the house or both.
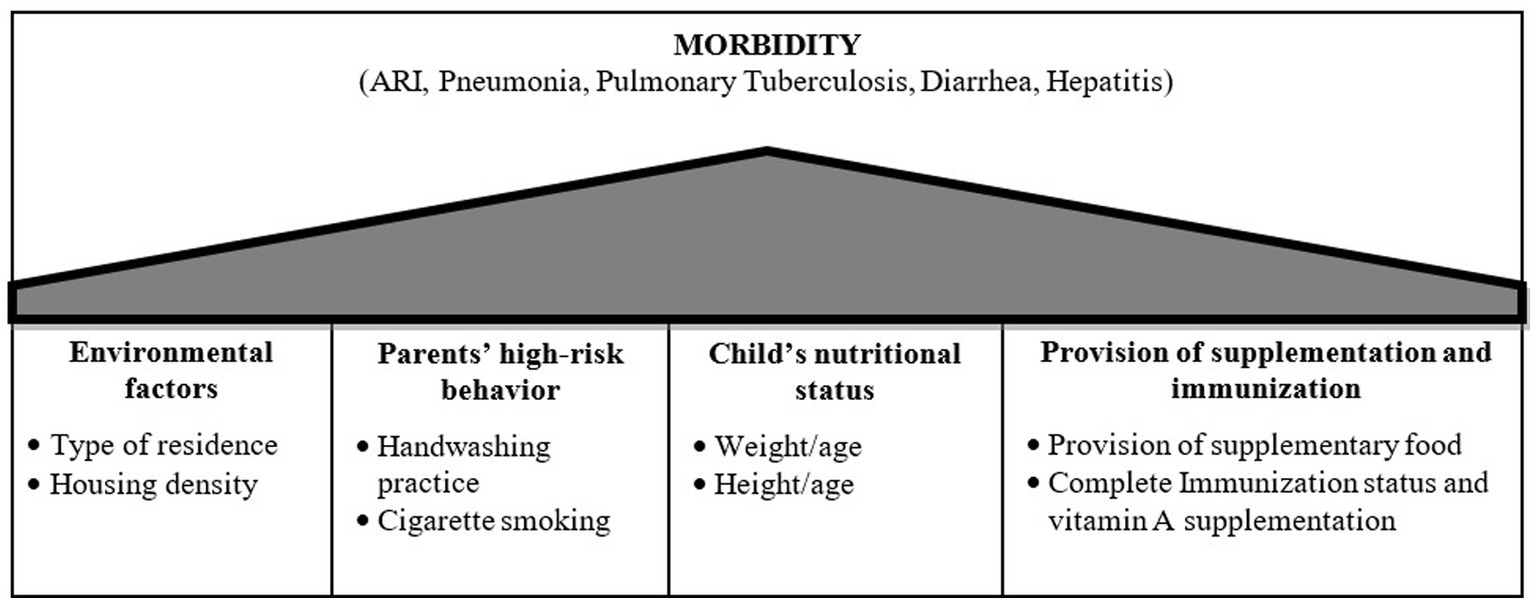
Figure 1. The analytical framework of factors associated with the frequent occurrence of infectious diseases in children under 5 years old in Indonesia.
Two variables were used in a high-risk behavior group: parents’ handwashing practices and cigarette smoking behavior. Parents’ handwashing practices consisted of two categories: (1) appropriate, that is, washing hands with soap and running water; and (2) inappropriate, if otherwise. Cigarette smoking behavior also consisted of two categories: (1) both parents who had never smoked cigarettes; and (2) if otherwise.
Two variables as the children’s nutritional status indicators were used, i.e., weight/age and height/age (17). For the weight/age indicator, the children were classified into either normal (the Z-score ≥ −2.0 to Z-score ≤ 2.0), overnutrition (Z-score was >2.0), or undernutrition (Z-score was <−2). For the children’s height/age indicator, they were categorized as either normal (Z-score ≥ −2.0) or short (Z-score < −2) (17).
Two variables used for the provision of supplementation and immunization were: (1) provision of supplementary food (yes/no), which was one of the government programs to complement the nutritional needs of children to achieve optimal weight gain, according to their age (18); and (2) the combined childhood immunization status and vitamin A supplementation, which was based on whether the child received childhood immunization up to 11 months of age (HB0, BCG, DPT/HB/HIB 1, 2, 3, polio 1, 2, 3, 4, or IPV 1, 2, 3, and measles) (19) and vitamin A supplementation usually provided every 6 months (20). This variable consisted of the following categories: (1) received all types of childhood immunization and vitamin A supplementation; (2) received all types of childhood immunization, but never received vitamin A supplementation; (3) never received or incomplete childhood immunization and ever received vitamin A supplementation; and (4) received incomplete/never received childhood immunization and never received vitamin A supplementation.
2.4 Data analysis
In the first stage, data analysis was performed by examining the distribution of each variable used and then examining each potential predictor’s distribution against childhood morbidity as the outcome variable. Logistic regression analysis was used to examine the factors associated with childhood morbidity. A multivariate logistic regression analysis was performed using a stepwise method to assess the association between each potential predictor and childhood morbidity. The final model consisted of variables significantly related to the study outcome at a significance level of 0.05. The statistical software SPSS v.24, suitable for analyzing complex sample data, was used. All estimates were weighted for sampling probabilities.
2.5 Ethics clearance
The 2018 Basic Health Research of Indonesia was approved by the Health Research Ethics Committee of the National Institute of Research and Development, Ministry of Health, Republic of Indonesia (No.: LB.02.01/2/KE.024/2018, July 28, 2017). Informed consent was obtained from all the respondents and they signed an informed consent form before data collection.
3 Results
Information from 39,948 children aged 24–59 months available from the 2018 Basic Health Research of Indonesia was used in this analysis. Figure 2 shows the characteristics of the children analyzed in this study. In the past month, 51.2% of the children had at least two types of infectious diseases. The most commonly reported infectious diseases were upper respiratory tract infections and pneumonia, whereas hepatitis and pulmonary TB were rarely reported (Figure 3). Most children lived in urban areas, >65% did not receive vitamin A supplementation, and 58.3% had parents who smoked cigarettes. Most parents reported appropriate hand-washing practices (washing their hands with soap and running water). Additionally, the prevalence of stunting and being underweight was 31.2 and 19.1%, respectively.
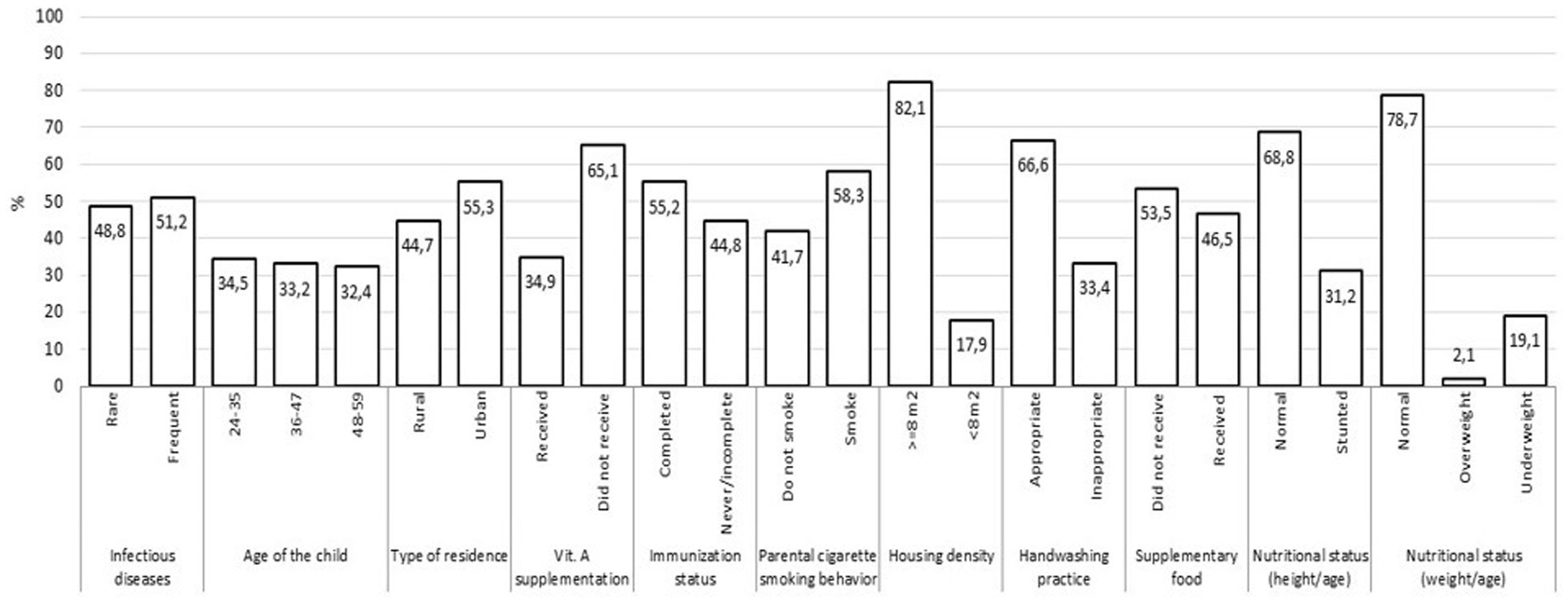
Figure 2. Characteristics of children aged 24–59 months, The 2018 Indonesia basic health survey.
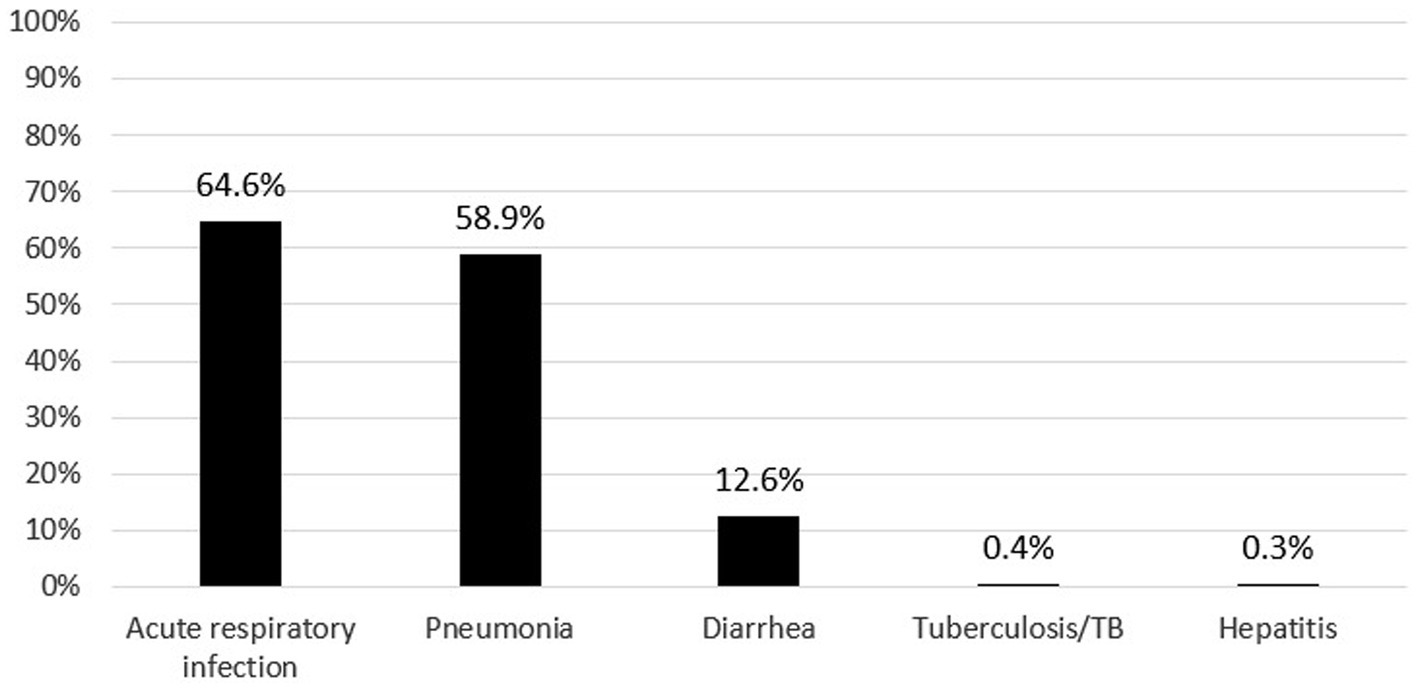
Figure 3. The prevalence of infectious disease in children aged 25–59 months in Indonesia, the 2018 Indonesia basic health survey.
Table 1 shows the distribution of potential predictors based on the occurrence of infectious diseases in the past month. The percentage of children with multiple infectious diseases in the past month increased in children whose parent smoked cigarettes and those whose parents did not have proper handwashing practices. Based on bivariate analysis, the factors significantly associated with the development of multiple types of infectious diseases were handwashing practices, immunization status, vitamin A supplementation, supplemental food, and child nutrition status.
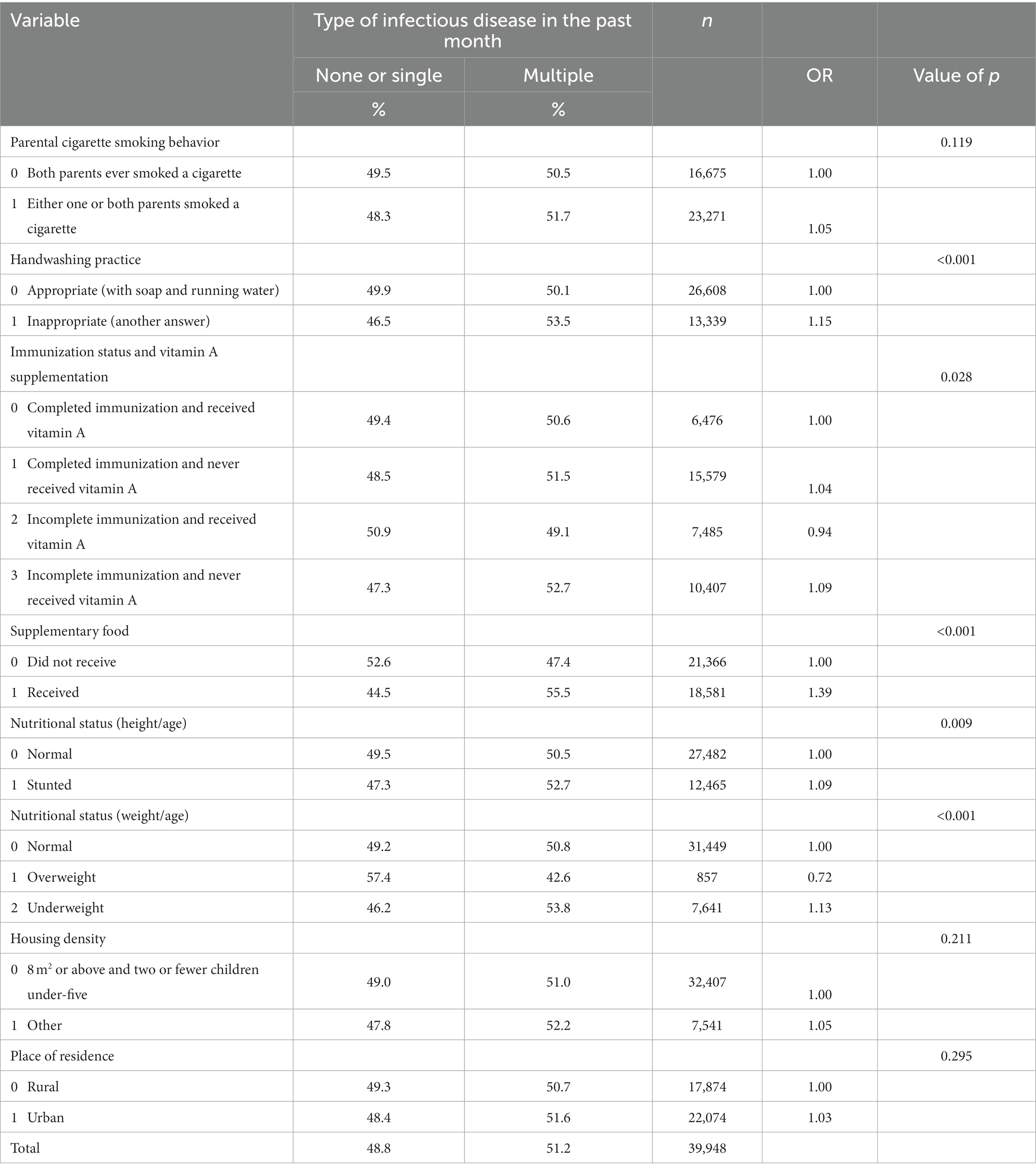
Table 1. Frequency distribution variables by the occurrence of infectious diseases in children under five in Indonesia, The 2018 Indonesia basic health survey.
Table 2 shows four factors significantly associated with developing multiple infectious diseases in the past month after controlling for all predictors. The odds of developing multiple types of infectious diseases increased in parents who had inappropriate handwashing practices [adjusted odds ratio (aOR) = 1.16, 95% confidence interval (CI): 1.09–1.24, p < 0.001], children receiving supplemental food (aOR = 1.38, 95% CI: 1.30–1.47, p < 0.001) and in underweight children (aOR = 1.12, 95% CI: 1.04–1.20, p < 0.001). However, the odds were lower in children who were overweight (aOR = 0.73, 95% CI: 0.59–0.91, p < 0.001) than those with normal weight. Infants from urban areas also had a higher odds of developing multiple types of infectious diseases than those from rural areas (aOR = 1.07, 95% CI: 1.00–1.14, p = 0.045).
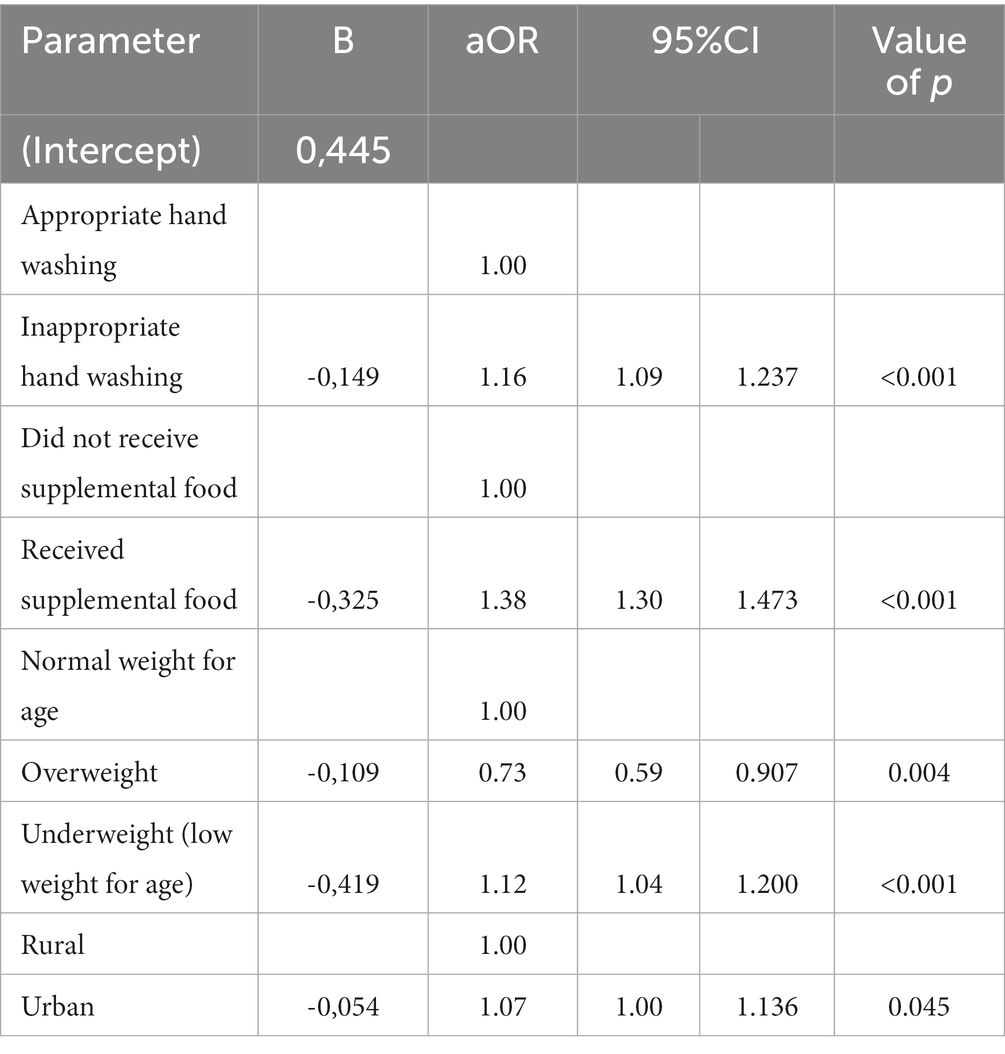
Table 2. Selected model of factors associated with frequent occurrence of infectious diseases amongst children aged 24–59 months in Indonesia, The 2018 Indonesia Basic Health Survey.
4 Discussion
4.1 Role of nutritional status in preventing infectious diseases
The importance of adequate nutrition to prevent children from infectious diseases was confirmed in this analysis. Underweight children were more likely to develop multiple infectious diseases. An underweight status usually mirrors recent and severe weight loss due to poor nutrient intake (21). This is supported by previous studies showing that undernourished children are more vulnerable to infectious diseases that adversely affect their survival (15). The relationship between undernutrition and infectious diseases is reciprocal (11, 15, 22). Undernutrition also worsens infectious diseases because it negatively affects the immune system, which is essential for protecting children from infectious agents (23). Previous studies have shown that undernourished children frequently experience respiratory infections, diarrhea, measles, and malaria, which are characterized by long and progressive disease courses (22). A Punjab-Pakistan study reported a relationship between diarrhea and underweight status in toddlers (24). Previous studies have shown that underweight children (weight/age) are more likely to experience diarrhea than normal-weight children (25, 26). A high prevalence of pneumonia among undernourished children has also been reported in Cambodia, and the duration of inpatient care due to pneumonia has increased with the increased severity of malnutrition (27). Previous literature reported that viral and bacterial skin infections were also prevalent in children (28). Insufficient nutritional status could impair the biological and structural integrity of the skin, leading to a compromised skin barrier (29). Nevertheless, due to the limited data available in the 2018 Basic Health Research, we could not incorporate skin infections into our analysis. Therefore, future studies that undertake a thorough examination of various infectious diseases, including skin infections, which are frequently observed in children are recommended.
Although several studies have reported the protective role of supplemental food in preventing child’s mortality (30) and infectious diseases (31, 32), this analysis showed that children who received supplemental food were more likely to experience multiple infectious diseases. It is highly likely that the children who received supplemental food in this study had poor nutritional status, including wasted or underweight children (33). Furthermore, several challenges have been reported in implementing this supplementary feeding program, including an unclear duration of administration (34). Poor adherence to supplementary feeding programs has emerged as an issue (35). All these conditions could contribute to an increased risk of infectious diseases among recipients of supplemental food.
These findings reflect the need for nutrition-specific and sensitive interventions that address the immediate and underlying causes of undernutrition to improve children’s nutritional status (36). Optimizing nutrition intake early in life to ensure the best start and provide long-term benefits complemented by multifaceted approaches to prevent and reduce undernutrition at the individual, household, and community levels is required (37).
4.2 Improving handwashing practices to prevent infectious diseases
Handwashing with soap is one of the most effective ways to prevent the transmission of infectious diseases (38). The availability of clean water is essential to support appropriate handwashing practices. The availability of clean water is associated with higher hygiene sanitation coverage and a lower risk of diarrheal diseases (39, 40). A study in India reported that washing hands before and after preparing food, defecating, and cleaning dishes significantly reduced the likelihood of diarrhea by >70% and respiratory infections by >56% (10). Mothers or caregivers who did not wash their hands at key times had an increased risk of experiencing acute diarrhea than those who practiced appropriate handwashing (41). A review reported that interventions promoting handwashing could reduce diarrhea episodes by approximately 30%, comparable to providing clean water in low-income areas (40). This indicates that improving the community’s access to handwashing facilities, soaps, and clean water is vital. This should also be complemented by interventions to promote community awareness, as mothers with sufficient knowledge would have more appropriate hand-washing practices than those with low levels of knowledge (42). Health workers should use every contact opportunity to educate mothers on the need to wash their hands with soap and running water, particularly at critical times, to reduce the risk of infection in children.
4.3 Importance of addressing children in urban areas
This analysis found an increased likelihood of developing infectious diseases among children living in urban areas. This aligns with previous studies that showed that children under 5 years of age living in urban areas have a higher risk of developing ARIs (43). Wahyuningsih (44) reported that the prevalence of ARI in Indonesia remained high over the years in urban areas, which was related to the physical environment of houses, including the adequacy of ventilation and sufficient sunlight in the house. Air pollution in urban areas is also associated with ARI in children (45). A previous study reported an increased risk of diarrhea in children owing to the high accessibility and availability of unsafe ready-to-eat foods with high microbial loads in urban areas (46). This emphasizes the need for health promotion program interventions to empower mothers in urban areas to make informed choices for and other caregivers about the selection and preparation of healthy food for children under 5 years old and to control various risk factors for infectious diseases related to their living environment.
4.4 Strengths and limitations of the study
This analysis provides national estimates of infectious diseases among children under 5 years of age in Indonesia. The large sample size used in this analysis provided adequate statistical power to examine the association between various predictors of infectious diseases. However, it is important to acknowledge several limitations of this study. Since this was a secondary analysis, our choice of variables was constrained by their availability within the dataset. Unfortunately, variables like measles or skin infections, which have been previously linked to malnutrition (29), were absent from the datasets and, consequently, had to be omitted from our analysis. The cross-sectional design did not allow the examination of potential causes and effects, but only the association between the variables examined. Another limitation was that the history of infectious diseases was based on the respondents’ recall ability and knowledge of the illnesses experienced by the children.
5 Conclusion
The findings show an association between inappropriate child healthcare practices (inappropriate handwashing practices and inadequate nutritional status of children) and residence type with frequent occurrence of infectious diseases in children aged 24–59 months in Indonesia. This indicates the need for multifaceted interventions to reduce infectious diseases in children under five. Effective health-promotion strategies are required for caregivers to raise awareness about the importance of appropriate childcare, including handwashing practices to prevent children from developing infectious diseases and ensuring access to clean water. Additionally, nutrition-sensitive, and nutrition-specific intervention strategies are essential to address children’s nutritional status. In urban areas, efforts to minimize the potential risk factors for infectious diseases should be a priority for health authorities and the community in general. Further research is recommended to explore different types of infections prevalent in children, including skin infections, which were not covered in our current dataset but are known to be common in this age group. This extended research could provide valuable insights for developing more targeted and effective health interventions.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Health Research Ethics Committee of the National Institute of Research and Development, Ministry of Health, Republic of Indonesia. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
NS: Conceptualization, Writing – original draft. DT: Formal analysis, Methodology, Writing – review & editing. CT: Resources, Writing – review & editing. BQ: Resources, Writing – review & editing. PH: Formal analysis, Writing – review & editing. S: Resources, Writing – review & editing. SdS: Resources, Writing – review & editing. YP: Resources, Writing – review & editing. LI: Resources, Writing – review & editing. SeS: Writing – review & editing. WA: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We thank the Ministry of Health Republic of Indonesia, for allowing us to use the Basic Health Research dataset in this analysis. We are grateful to all teams of experts and consultants, study supervisors, research team members, and the data collection team for their support and involvement in this study. The authors gratefully acknowledge all study participants for their participation in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Perin, J , Mulick, A , Yeung, D , Villavicencio, F , Lopez, G , Strong, KL, et al. Global, regional, and national causes of under-5 mortality in 2000–19: an updated systematic analysis with implications for the sustainable development goals. Lancet Child Adolesc Heal. (2022) 6:106–15. doi: 10.1016/S2352-4642(21)00311-4
2. United nations inter-agency Group for Child Mortality Estimation In: Levels & Trends in child mortality report 2022. Geneva: United Nations Children’s Fund. (2022)
3. Ministry of Health Republic of Indonesia . Indonesia Health Profile 2021. Jakarta: Ministry of Health Republic of Indonesia. (2022).
4. Ministry of Health Republic of Indonesia . The 2018 Indonesia basic Health Research report. Jakarta: Badan Penelitian dan Pengembangan Kesehatan (2018).
5. Guzmán, IB , Cuesta, JG , Trelles, M , Jaweed, O , Cherestal, S , van Loenhout, JAF, et al. Delays in arrival and treatment in emergency departments: women, children and non-trauma consultations the most at risk in humanitarian settings. PLoS One. (2019) 14:1–15. doi: 10.1371/journal.pone.0213362
6. Pajuelo, MJ , Anticona Huaynate, C , Correa, M , Mayta Malpartida, H , Ramal Asayag, C , Seminario, JR, et al. Delays in seeking and receiving health care services for pneumonia in children under five in the Peruvian Amazon: a mixed-methods study on caregivers’ perceptions. BMC Health Serv Res. (2018) 18:1–11. doi: 10.1186/s12913-018-2950-z
7. Alaa, H , Shah, SA , and Khan, AR . Prevalence of diarrhoea and its associated factors in children under five years of age in Baghdad. Iraq Open J Prev Med. (2014) 4:17–21. doi: 10.4236/ojpm.2014.41004
8. Nira, NK , Pramono, D , and Naning, R . Risk factors of pneumonia among under five children in Purbalingga District. Central Java Province Trop Med J. (2013) 3:128–35. doi: 10.22146/tmj.5864
9. Takele, K , Zewotir, T , and Ndanguza, D . Risk factors of morbidity among children under age five in Ethiopia. BMC Public Health. (2019) 19:1–9. doi: 10.1186/s12889-019-7273-4
10. Khan, KM , Chakraborty, R , Brown, S , Sultana, R , Colon, A , Toor, D, et al. Association between handwashing behavior and infectious diseases among low-income community children in urban New Delhi, India: a cross-sectional study. Int J Environ Res Public Health. (2021) 18:1–4. doi: 10.3390/ijerph182312535
11. Rodríguez, L , Cervantes, E , and Ortiz, R . Malnutrition and gastrointestinal and respiratory infections in children: a public health problem. Int J Environ Res Public Health. (2011) 8:1174–205. doi: 10.3390/ijerph8041174
12. Walson, JL , and Berkley, JA . The impact of malnutrition on childhood infections. Curr Opin Infect Dis. (2018) 31:231–6. doi: 10.1097/QCO.0000000000000448
13. Fan, Y , Yao, Q , Liu, Y , Jia, T , Zhang, J , and Jiang, E . Underlying causes and co-existence of malnutrition and infections: an exceedingly common death risk in Cancer. Front Nutr. (2022) 9:1–11. doi: 10.3389/fnut.2022.814095
14. Ministry of Health Republic of Indonesia. Results of the Indonesian nutritional status study (SSGI) for 2021. Jakarta: Health Development Policy Agency. (2021).
15. Katona, P , and Katona-Apte, J . The interaction between nutrition and infection. Clin Infect Dis. (2008) 46:1582–8. doi: 10.1086/587658
16. Hondru, G , Wieringa, FT , Poirot, E , Berger, J , Som, SV , Theary, C, et al. The interaction between morbidity and nutritional status among children under five years old in Cambodia: a longitudinal study. Nutrients. (2019) 11:1–12. doi: 10.3390/nu11071527
17. WHO . WHO child growth standards: length /height-for-age, weight-for-age, weight-for-length, weight-forheight and body mass index-for-age. Methods and development. Geneva, Switzerland: World Health Organization (WHO). (2006).
18. Ministry of Health Republic of Indonesia . Technical instructions for giving supplementary food (toddlers - pregnant women - school children). Jakarta: Petunjuk Tek. PMT (2017).
19. Ministry of Health of the Republic of Indonesia In: Technical instructions National Childhood Immunization Month. Jakarta: Ministry of Health of the Republic of Indonesia. (2021)
20. Ministry of Health Republic of Indonesia. Vitamin a supplementation integrated management guide. Jakarta: Ministry of Health of the Republic of Indonesia (2016).
21. Dipasquale, V , Cucinotta, U , and Romano, C . Acute malnutrition in children: pathophysiology, clinical effects and treatment. Nutrients. (2020) 12:1–9. doi: 10.3390/nu12082413
22. Schaible, UE , and Kaufmann, SHE . Malnutrition and infection: complex mechanisms and global impacts. PLoS Med. (2007) 4:0806–12. doi: 10.1371/journal.pmed.0040115
23. Asfaw, M , Wondaferash, M , Taha, M , and Dube, L . Prevalence of undernutrition and associated factors among children aged between six to fifty nine months in Bule Hora district. South Ethiopia BMC Public Health. (2015) 15:1–9. doi: 10.1186/s12889-015-1370-9
24. Kumar, R , Abbas, F , Mahmood, T , and Somrongthong, R . Prevalence and factors associated with underweight children: a population-based subnational analysis from Pakistan. BMJ Open. (2019) 9:e028972–13. doi: 10.1136/bmjopen-2019-028972
25. Gasgaw, TA , and Walie, YM . Prevalence and determinate factors of diarrhea morbidity among under five children in shake zone, Southwest Ethiopia, a community based cross-sectional study. Arch Comm Med Public Heal. (2019) 5:008–14. doi: 10.17352/2455-5479.000046
26. Melese, B , Paulos, W , Astawesegn, FH , and Gelgelu, TB . Prevalence of diarrheal diseases and associated factors among under-five children in Dale District, Sidama zone, southern Ethiopia: a cross-sectional study. BMC Public Health. (2019) 19:1–10. doi: 10.1186/s12889-019-7579-2
27. Arpitha, G , Rehman, M , and Ashwitha, G . Effect of severity of malnutrition on pneumonia in childern aged 2 M-5Y at a tertiary care center in Khammam, Andhra Pradesh: a clinical study. Sch J Appl Med Sci. (2014) 2:3199–203. doi: 10.36347/sjams.2014.v02i06.069
28. García, E , Halpert, E , Borrero, E , Ibañez, M , Chaparro, P , Molina, J, et al. Prevalence of skin diseases in children 1 to 6 years old in the city of Bogota, Colombia. World Allergy Organ J. (2020) 13:100484. doi: 10.1016/j.waojou.2020.100484
29. Pandit, V , and Udaya, K . A cross sectional study of nutritional dermatoses among malnourished children in a tertiary care Centre. Indian J Paediatr Dermatol. (2021) 22:226–30. doi: 10.4103/ijpd.IJPD_13_20
30. Khan, JR , and Awan, N . A comprehensive analysis on child mortality and its determinants in Bangladesh using frailty models. Arch Public Heal. (2017) 75:1–10. doi: 10.1186/s13690-017-0224-6
31. Vaivada, T , Gaffey, MF , and Bhutta, ZA . Promoting early child development with interventions in health and nutrition: a systematic review. Pediatrics. (2017) 140:4308. doi: 10.1542/peds.2016-4308
32. Bhutta, ZA , Das, JK , Rizvi, A , Gaffey, MF , Walker, N , Horton, S, et al. Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost? Lancet. (2013) 382:452–77. doi: 10.1016/S0140-6736(13)60996-4
33. Ministry of Health Republic of Indonesia . Guidelines for providing additional recovery food for undernourished toddlers. Jakarta: Ministry of Health Republic of Indonesia. (2011).
34. Indriati, R , Nugraheni, SA , and Kartini, A . Supplementary feeding program evaluation restoration malnourished in children under five in the district Wonogiri seen from input and process aspects. J Manaj Kesehat Indonesia. (2015) 3:18–26. doi: 10.14710/jmki.3.1.2015.%25p
35. Udoh, EE , Umoh, RA , Edem, KB , Okpokowuruk, FS , Udo, EN , Nwazuluoke, BN, et al. Effect of adherence to follow-up on recovery from moderate acute malnutrition among under-fives in a supplementary feeding programme. Malays J Nutr. (2022) 28:295–303. doi: 10.31246/mjn-2021-0040
36. Ruel, MT , and Alderman, H . Nutrition-sensitive interventions and programmes: how can they help to accelerate progress in improving maternal and child nutrition? Lancet. (2013) 382:536–51. doi: 10.1016/S0140-6736(13)60843-0
37. Keats, EC , Das, JK , Salam, RA , Lassi, ZS , Imdad, A , Black, RE, et al. Effective interventions to address maternal and child malnutrition: an update of the evidence. Lancet Child Adolesc Heal. (2021) 5:367–84. doi: 10.1016/S2352-4642(20)30274-1
38. Bogale, D , Id, O , and Mekonnen, AG . Availability and factors influencing community level handwashing facility in Ethiopia: implication for prevention of infectious diseases. PLoS One. (2021) 16:1–13.
39. Zerbo, A , Castro Delgado, R , and Arcos, GP . Water sanitation and hygiene in sub-Saharan Africa: coverage, risks of diarrheal diseases, and urbanization. J Biosaf Biosecur. (2021) 3:41–5. doi: 10.1016/j.jobb.2021.03.004
40. Mengistie, B , Berhane, Y , and Worku, A . Prevalence of diarrhea and associated risk factors among children under-five years of age in eastern Ethiopia: a cross-sectional study. Open J Prev Med. (2013) 3:446–53. doi: 10.4236/ojpm.2013.37060
41. Fenta, A , Alemu, K , and Angaw, DA . Prevalence and associated factors of acute diarrhea among under-five children in Kamashi district, western Ethiopia: community-based study. BMC Pediatr. (2020) 20:1–7. doi: 10.1186/s12887-020-02138-1
42. Dagne, H , Bogale, L , Borcha, M , Tesfaye, A , and Dagnew, B . Hand washing practice at critical times and its associated factors among mothers of under five children in debark town, Northwest Ethiopia, 2018. Ital J Pediatr. (2019) 45:120. doi: 10.1186/s13052-019-0713-z
43. Chakrabarti, S , Khan, MT , Kishore, A , Roy, D , and Scott, SP . Risk of acute respiratory infection from crop burning in India: estimating disease burden and economic welfare from satellite and national health survey data for 250 000 persons. Int J Epidemiol. (2019) 48:1113–24. doi: 10.1093/ije/dyz022
44. Wahyuningsih, S , Raodhah, S , and Basri, S . Acute respiratory infection (ARI) in toddlers in the coastal area of Kore Village, Sanggar District. Bima Regency Higiene. (2017) 3:97–105.
45. Wu, I-P , Liao, S-L , Lai, S-H , and Wong, KS . The respiratory impacts of air pollution in children: global and domestic (Taiwan) situation. Biom J. (2022) 45:88–94. doi: 10.1016/j.bj.2021.12.004
Keywords: infectious diseases, handwashing practice, supplemental food, nutritional status, type of residence, Indonesia basic health research
Citation: Sulistiyowati N, Tjandrarini DH, Titaley CR, Que BJ, Hidayangsih PS, Suparmi, Sudikno S, Purwatiningsih Y, Indrawati L, Siahaan S and Adyarani WP (2024) Suboptimal child healthcare practices and the development of multiple infectious diseases in children aged 24–59 months. Front. Public Health. 12:1340559. doi: 10.3389/fpubh.2024.1340559
Edited by:
Francis Thaise A. Cimene, University of Science and Technology of Southern Philippines, PhilippinesReviewed by:
Karim A. Mohamed Al-Jashamy, SEGi University, MalaysiaRegina Fölster-Holst, University Medical Center Schleswig-Holstein, Germany
Copyright © 2024 Sulistiyowati, Tjandrarini, Titaley, Que, Hidayangsih, Suparmi, Sudikno, Purwatiningsih, Indrawati, Siahaan and Adyarani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christiana Rialine Titaley, Y2hyaXN0aWFuYV9yaWFsaW5lQHlhaG9vLmNvbQ==