 Fang Chen
Fang Chen Qing Hua Xu*
Qing Hua Xu*- Anhui Center for Disease Control and Prevention, Hefei, Anhui, China
Objective: This study aimed to investigate the knowledge, attitude, and practice (KAP) regarding disinfection and hand hygiene, along with associated influencing factors among childcare facilities staff during the COVID-19 pandemic in Anhui, and to provide information for developing disinfection and hand hygiene strategies for childcare facilities.
Methods: A web-based cross-sectional study was conducted among Anhui Province residents in China in September 2020. In this study, 60 childcare facilities in two cities of Anhui Province were selected using the convenient sampling method for questionnaires. The questionnaires were distributed through a web-based platform. The disinfection and hand hygiene KAP scores among childcare facilities staff were calculated, and their influencing factors were analyzed. The accuracy rates of knowledge, attitude, and practice of behavior were calculated and analyzed.
Results: A total of 1,029 participants were included in the study. The disinfection and hand hygiene knowledge, attitude and practice ranged from approximately 5 to 23, 1 to 5, 3 to 13, respectively. The score of urban areas was higher than that of rural areas. Higher education levels and more years of working were associated with higher scores. Additionally, staff who received training or supervision had higher scores than those without. The categories with the lowest knowledge accuracy rate (46.3%), lowest attitude accuracy rate (4.2%), and “always” practice rate (5.3%) among childcare facility staff were all related to the question categories concerning the appropriate range of disinfectants for use. The accuracy rates of hand hygiene knowledge and attitude among the childcare facility staff were high (83.7%-99.6%), but the “always” practice rate was in the middle range (63.0%).
Conclusion: The disinfection and hand hygiene knowledge among childcare facilities staff was inadequate during the COVID-19 pandemic in Anhui. Continuous implementation of education and training, particularly in rural areas, is essential. Establishing a monitoring system to assess usage effectiveness and adverse reactions in China is critical. Interventions should focus on increasing compliance with hand hygiene practices. Further research should explore the training and intervention of disinfection and hand hygiene, the safety of disinfection measures, and more operational hand hygiene methods in childcare facilities.
Introduction
Childcare facilities, catering to children aged 0 to 6 years old, are often hotspots for clusters or outbreaks of acute gastroenteritis, hand, foot, and mouth disease, and influenza (1–3). During the COVID-19 pandemic, clusters of COVID-19 infections have occurred in childcare facilities (4). Disinfection is an important measure to cut off transmission, and hand hygiene is the most important, effective, and economical measure to prevent and control infection rates. The World Health Organization (WHO) recommends environmental cleaning, disinfection, and hand hygiene for the prevention and control of infectious diseases (5). However, studies have revealed that the implementation of these measures has not been satisfactory. Additionally, the unqualified environment disinfection and hand hygiene among children and teachers have been identified as risk factors for enterovirus infection in childcare facilities (6).
During the COVID-19 pandemic, the prevention and control measures of infectious diseases, such as disinfection and hand hygiene, have been promoted by many countries. Although residents exhibited good knowledge and attitude toward these measures, the behavior status was not satisfied. Some studies indicated that factors such as gender, age, and education level influenced behavior, with good knowledge and attitude serving as prerequisites for proper behavior (7, 8). Caregivers and teachers serve as a critical barrier in safeguarding children's health, while simultaneously emphasizing the importance of their own self-protection, and also play an important role for children getting and implementing health measures (9, 10). However, limited studies have been conducted on knowledge, attitude, and practice (KAP) toward disinfection and hand hygiene among childcare facilities staff. Some studies on knowledge and its intervention have exhibited differences in the knowledge rate among childcare facilities staff in different areas, with significant increases observed in knowledge rates to a high level after training (11, 12). Hand hygiene behaviors among childcare facilities staff were related to their knowledge, perception, habits, and interactions with children (13). During the COVID-19 pandemic, a KAP study on the prevention and control of hand, foot, and mouth disease among childcare facilities staff, including several disinfection and hand hygiene measures, exhibited that the staff possessed a low level of knowledge, but their attitude was positive. While a few staff practiced at a high level (14), it is suggested that the characteristics of disinfection and hand hygiene KAP among childcare facilities staff differed from those of the general public probably.
In China, childcare facilities have been listed as important institutions for the prevention and control of COVID-19 by the government. These institutions are required to perform environmental cleaning, disinfection, and hand hygiene (15). However, there is a lack of systematic surveillance and studies on KAP of childcare facilities staff. Understanding the disinfection and hand hygiene KAP among childcare facilities staff and discussing the improving measures are important steps to enhance environmental disinfection and hand hygiene as well as prevention and control of infectious disease among childcare facilities staff. This study was conducted based on a survey project of the disinfection practices in childcare facilities in Anhui Province in September 2022. The study aimed to investigate the disinfection and hand hygiene KAP among childcare facilities staff in two cities and analyze the influencing factors. This study also identified the gaps mainly among the knowledge, attitude, and practice, but not the scores of every part of knowledge, attitude, and practice, or total score and the relationship of the three as usual, to provide a scientific basis for the implementation and evaluation of intervention activities at every link in the future.
Materials and methods
Study setting and design
This study was a web-based cross-sectional study conducted among residents of Anhui Province, China, during the COVID-19 pandemic, in September 2020.
Sampling and sample size
A stratified sampling method was employed to select one city from the south and another from the north of Anhui Province. In each selected city, 3 districts were chosen and, within each district, 10 childcare facilities in each district were selected using a convenient sampling method to conduct the study. The childcare facilities included in this study comprised nurseries and kindergartens of all levels and types, catering to children aged 0–6 years.
Assuming that 80%(p) of staff were at a high level of disinfection and hand hygiene knowledge (16, 17), with a type Ierror (α) of 0.05 and the permissible error (d) of 0.1 p, considering 10% expected missing and incomplete responses in the online survey and the childcare facilities administrators participating in distribution work. The minimum sample size was 120 per district, with the sample size calculation formula (n = ) for the status study.
Questionnaire preparation and description
The questionnaires focused on disinfection and hand hygiene were developed based on existing research literature. The content validities of the questionnaire were reviewed by four experts (three experts in disinfection and one epidemiologist; Senior Doctor), each of whom provided separate comments. The researcher collected these comments and revised the questionnaire accordingly. A pre-survey was conducted among 20 staff members of childcare facilities staff, who completed the questionnaire and reported whether it was easy to understand. Based on their feedback, modifications were made and the formal questionnaire was formed.
The questionnaire primarily included the following contents: socio-demographic data and the method of access to knowledge (11 questions), disinfection and hand hygiene knowledge (8 questions), attitude (5 questions), and behavior (7 questions) on the purpose, object, method, timing of disinfection and hand hygiene. There were 31 questions in total.
The questionnaire scoring system is described as follows: first, in the knowledge questions, each correct response was scored “1,” while incorrect response/not sure was scored “0.” Second, in the attitude questions, a positive (correct) response was scored “1,” while a negative/neutral response was scored “0.” Third, in the practice questions, for multiple-choice questions, the number of correct responses was classified as positive, moderate, and negative behavior, scored “2”, “1,” and “0”, while for single-choice questions, the behavior implemented “always”, “sometimes,” and “never” were scored “2”, “1,” and “0”, respectively. The total score for KAP was 42, incorporating 23 points for knowledge, 5 points for attitude, and 14 points for practice.
Cronbach's alpha test was conducted using SPSS version 20.0 to check the reliability of the questionnaire and was found to be 0.765 (The multiple choice questions were split into several corresponding single choice data when exported from the WJX platform automatically).
Data collection
The questionnaires were distributed to respondents via the questionnaire platform powered by www.wjx.cn (WJX) and WeChat app in September 2022, after being approved by the local education administration. Informed consent was obtained from all participants. Within each childcare facility, three staff members from the departments of administrative management, childcare, healthcare, cleaning and disinfection, and food and beverage support completed the questionnaires; all staff answered if there were fewer than three staff members in a department. A total of 1,036 respondents were obtained, with 1,029 valid responses, resulting in a response rate of 99.3%.
The childcare facilities' character data (urbanicity, owned) were provided by local education administration and were assigned to response data exported from the WJX platform by researchers, depending on the name of the childcare facilities in response data, to avoid misunderstanding of the facility information by staff.
Data analysis
All the collected data in the “WJX” platform were exported to a master Excel spreadsheet (Microsoft Office 2007) for cleaning and coding before being imported into Statistical Package for Social Sciences (IBM SPSS20.0). Numbers and percentages were used to describe the categorical variables. When calculating the accuracy rate, the multiple-choice question was considered correct if it received a total score. The median (Q1, Q3) was used to describe continuous variables such as the KAP score of different groups. The Mann–Whitney test and the Kruskal–Wallis test were used for analyzing knowledge scores among different groups. The chi-square tests were used for analyzing trained or supervised percentages among various groups. A P-value of < 0.05 was considered statistically significant.
Ethical considerations
This study was approved by the Ethics Committee of Anhui Provincial Center for Disease Control and Prevention. The title and purpose of the study were presented at the beginning of the questionnaire. The contents did not include any personal identifiers. Informed consent was obtained from all participants in this study. Privacy and confidentiality of all information were strictly maintained.
Results
Information on survey objects
A total of 1,029 participants in 60 childcare facilities were included in the study. Of these, 97.7% of participants were female participants, mainly aged between 17 and 66 years, 46.4% were below 30 years old, 41.0% held junior college diplomas, 87.1% were majors in childcare and education, and 42.3% were working for 3 to 9 years. Additionally, 56.1% and 43.9% of participants resided in Bozhou City and Huangshan City, respectively; 70.8% were in urban areas; and 73.8% were in public childcare facilities (Table 1).
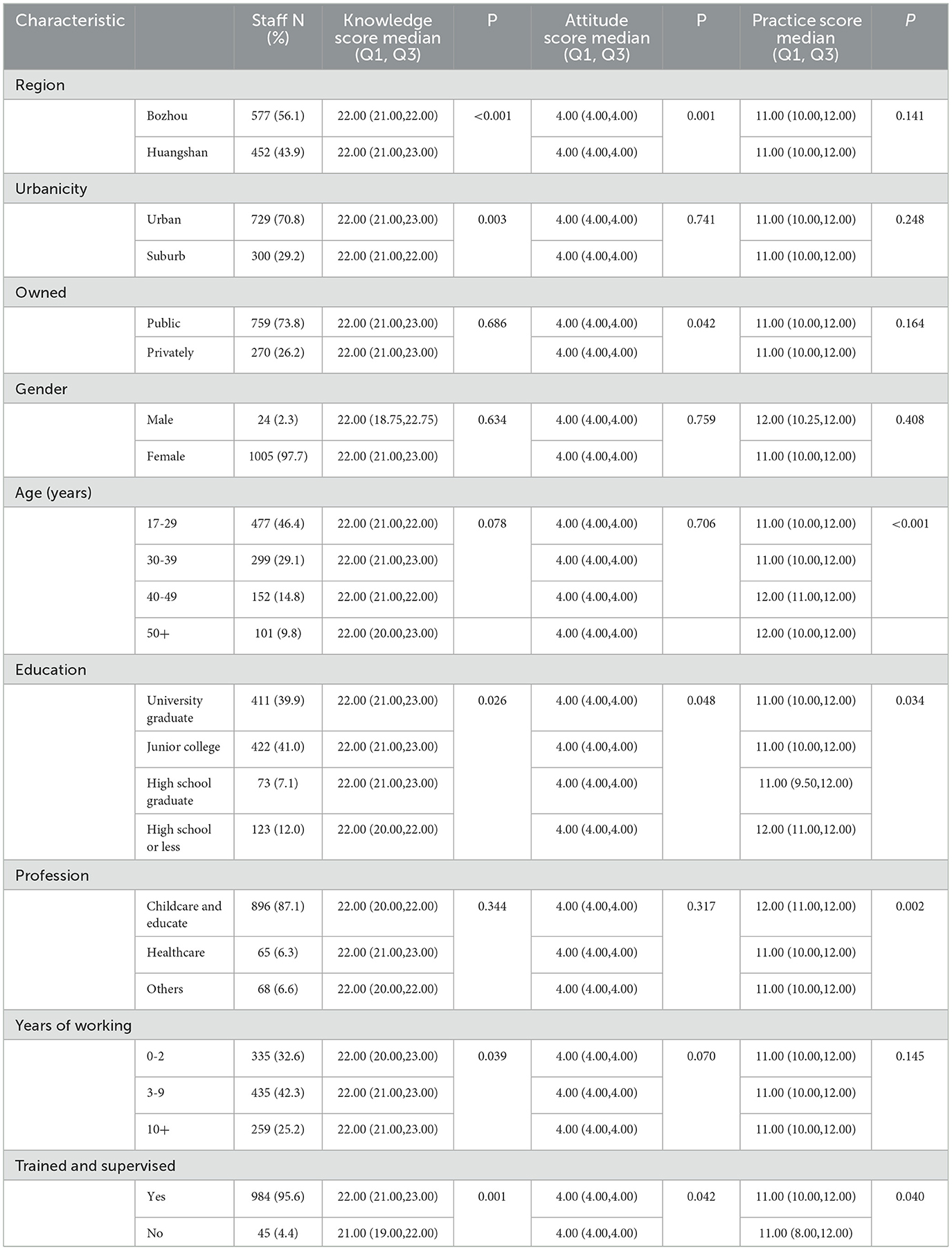
Table 1. The scores of disinfection and hand hygiene KAP among childcare facilities staff, Anhui Province, China, September 2022 (n = 1,029).
Disinfection and hand hygiene KAP score and influencing factors
The disinfection and hand hygiene knowledge score ranged between approximately 5 and 23. The different characteristics of staff were compared to determine the influencing factors in the scores of disinfection and hand hygiene knowledge. Scores in Huangshan were significantly higher than that in Bozhou; in urban areas, scores were significantly higher than that in suburban areas (P < 0.001 and P = 0.003, respectively). Higher education levels and the more years of working were significantly associated with higher scores (P = 0.026 and P = 0.039, respectively). The scores for staff with training or supervision were significantly higher than those for those without (P = 0.001). Scores of staff, whether in public or privately owned facilities and irrespective of gender or professions, were found to be non-significant.
The disinfection and hand hygiene attitude scores ranged from approximately 1 to 5. Scores of staff were different significantly with different regions, whether facilities were public or privately owned, and whether they received education and training or supervision (P = 0.001, P = 0.042, P = 0.048, and P = 0.042, respectively). Scores of staff with urban or suburb, gender, ages, professions, and years of working were found to be non-significant.
The disinfection and hand hygiene practice score ranged from approximately 3 to 13. Scores of staff with different ages, educations, professions, and training or supervision were significantly different (P < 0.001, P = 0.034, P = 0.002 and P = 0.040, respectively). Scores of staff with different regions, urban or suburban settings, public or privately owned facilities, gender, or years of working were found to be non-significant (Table 1).
Disinfection and hand hygiene knowledge questionnaire
Among the questions of knowledge, the highest accuracy was in the category of “Know the purpose of disinfection was cutting off transmission” (99.9%), followed by “Know that disinfectant should be used within the expiration date” (99.6%), and “Know that surfaces of environmental objects need to be cleaned at first and then disinfected” (98.5%). The lowest accuracy category was “Know that alcohol disinfectants could not be used for all infectious diseases” (46.3%) (Table 2).
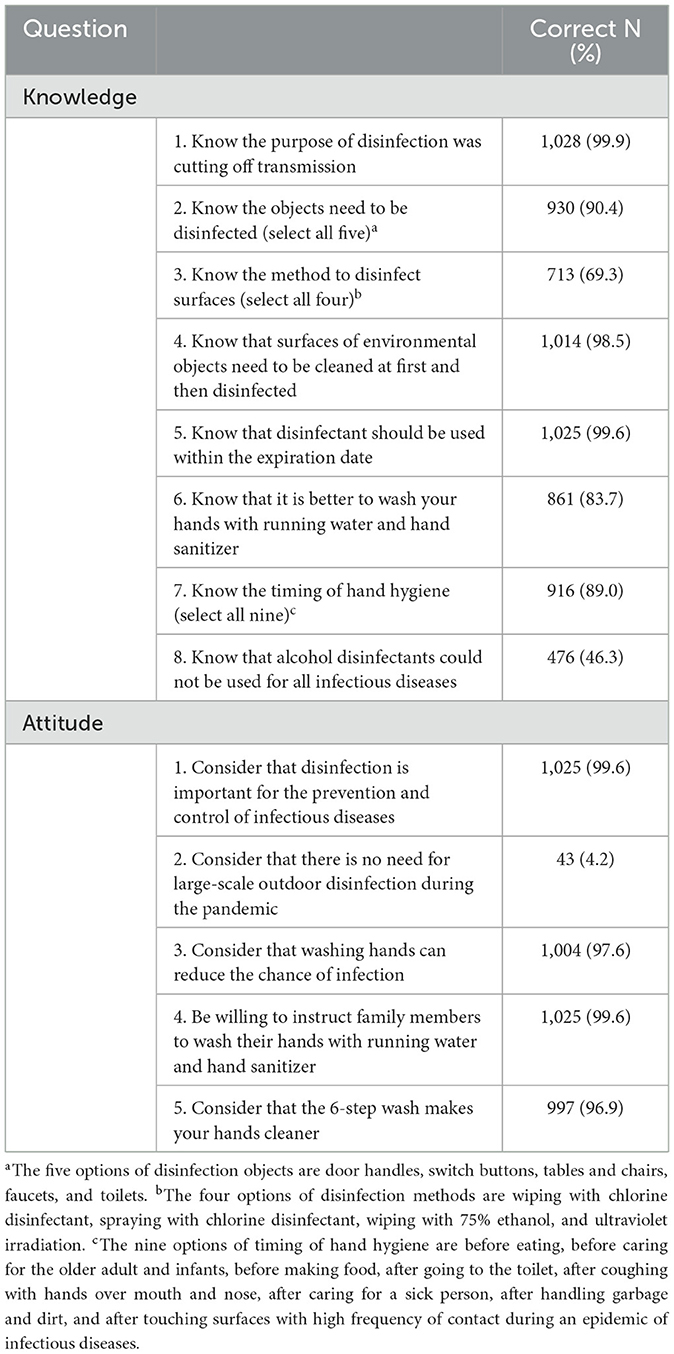
Table 2. The categories of disinfection and hand hygiene knowledge and attitude among childcare facilities staff, Anhui Province, China, September 2022 (n = 1,029).
Disinfection and hand hygiene attitude questionnaire
Among the questions of attitude, the highest accuracy of childcare facilities staff was “Consider that disinfection is important for the prevention and control of infectious diseases” and “Be willing to instruct family members to wash their hands with running water and hand sanitizer” (97.6% and 99.6% respectively). The lowest accuracy was “Consider that there is no need for large-scale outdoor disinfection during the pandemic” (46.3%) (Table 2).
The technical support of disinfection and hand hygiene knowledge
Comparing the staff trained or supervised or not in different characteristics, the percentage of staff receiving training or supervision in urban areas was significantly higher than that in rural (χ2 = 24.913, P < 0.001) (Table 3).
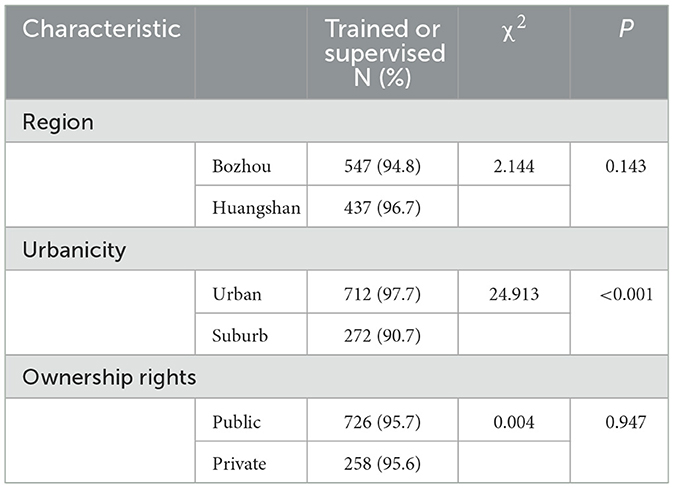
Table 3. The technical support of disinfection and hand hygiene knowledge among childcare facilities staff, Anhui Province, China, September 2022 (n = 1,029).
The method of access to disinfection and hand hygiene knowledge
The primary source of disinfection and hand hygiene knowledge for childcare facilities staff was training organized by facilities themselves (84.8%). Following that were training organized by superior institutions (77.9%). Other sources included WeChat accounts (77.7%), technical departments (70.8%), Television (59.9%), websites (58.5%), poster brochures (57.4%), and radio (50.0%).
Disinfection and hand hygiene practice questionnaire
Among the childcare facilities staff, 80.9% reported having prepared more than two kinds of disinfectants at home since 2020, 92.7% disinfected more than three kinds of objects for prevention, 74.0% cleaned first and then disinfected always, 74.4% wore masks and gloves when using chlorine disinfectant always, 89.7% washed hands when coming back from public places always, 63.0% washed hands with 6 steps always, while 5.3% never “sprayed alcohol to disinfect air since 2020” (Table 4).
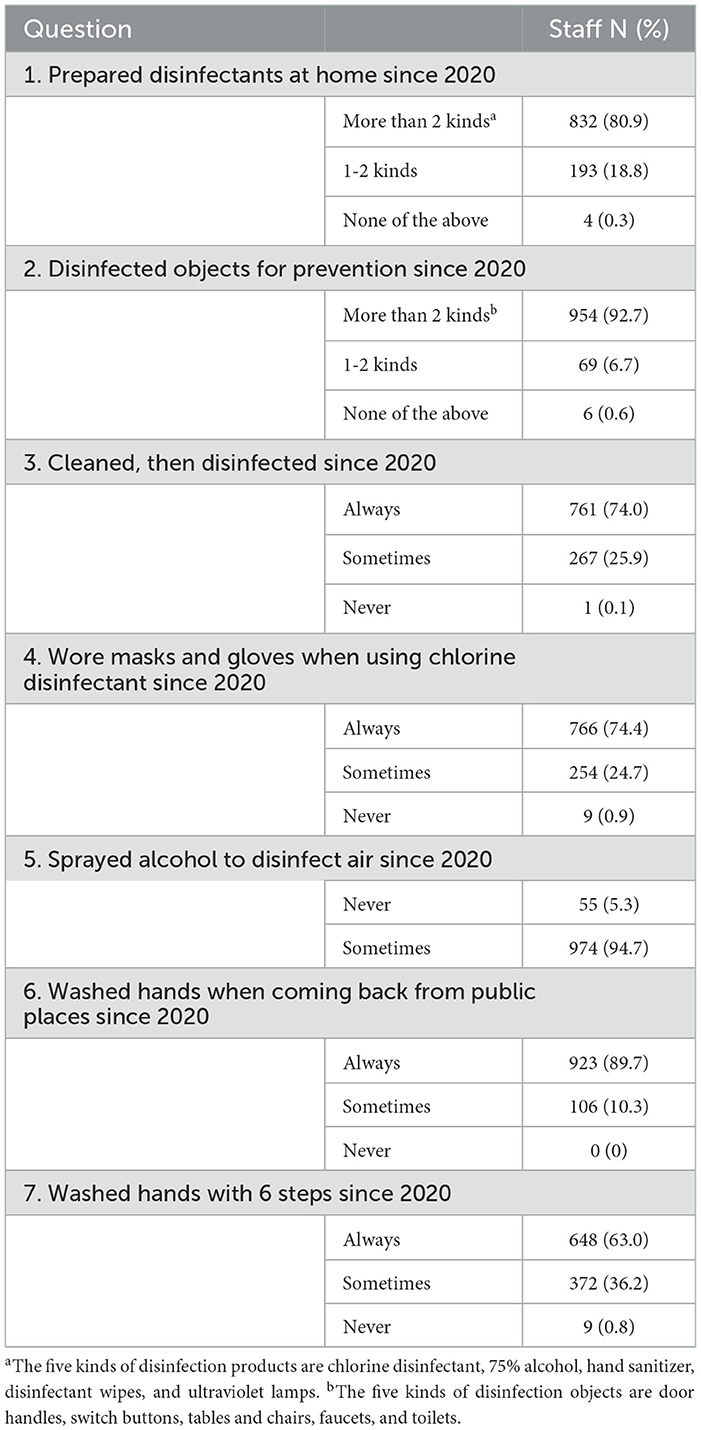
Table 4. The questions of disinfection and hand hygiene practices among childcare facilities staff, Anhui Province, China, September 2022 (n = 1,029).
Discussion
The results of this study showed a significant correlation between the higher educational level of the childcare facilities staff and their higher score, which was consistent with the survey results of resident adults and children's parents (8, 18). This result suggests that staff with a higher degree of education may possess a better understanding and mastery of knowledge. The results of this study showed that the education level of the childcare facilities staff mainly consisted of junior college (41.0%) and university graduates (39.9%), which was consistent with the survey results in China (12, 19). However, this finding was inconsistent with the research in other countries, such as Singapore, where the education of the staff mainly consisted of secondary school and diploma courses (14, 20). Although the effect of the educational level of childcare facilities staff on the implementation of hygiene measures among children has not been reported, some studies showed that the education level of parents was positively correlated with the hand hygiene behavior of students (21). Childcare facilities staff play a vital role in taking care and teaching children, akin to children's parents. The educational level of staff should be considered in the health care work of the childcare facilities. This study showed that the childcare facilities staff were predominantly female individuals (97.7%) and mainly aged from 17 to 29 years old (46.4%), which was consistent with other studies (12, 14, 22). This demographic trend may be attributed the characteristics and caring needs of children (20). However, this study showed that there was no significant difference in the knowledge scores of the staff by gender and age. This aspect was inconsistent with the research of the resident, which showed that the older and female individuals were more compliant with COVID-19 prevention and control measures (7). The results of this study also showed that the more the years of working, the higher the score significantly. The scores of staff with training or supervision were significantly higher than those without training or supervision. This difference may be due to different health promotion models between the public and childcare facilities staff. This study revealed that the training rate was 84.8% in facilities and 77.9% by higher level organizations among the staff. Organized training was more targeted and definitely showed effectiveness in improving the disinfection and hand hygiene knowledge of childcare facilities staff.
The results of this study showed that the disinfection and hand hygiene knowledge scores of staff were significantly different between the two cities, and the scores in urban childcare facilities were significantly higher than those in rural childcare facilities. This finding was partly consistent with the survey results of public adults in America and Saudi Arabia, which demonstrated that it was different among different cities because of the COVID-19 situation probably. At the same time, there was no difference between rural and urban areas (7, 16). The difference between rural and urban areas in this study was consistent with the survey results of hand hygiene knowledge of kindergarten teachers in Zhejiang, Shanghai, China, during the COVID-19 pandemic (19, 22). This result may be due to the low educational level of staff from rural childcare facilities in China, and they were short of the ability and opportunity to acquire relevant knowledge (19). This study also showed that the percentage of staff in rural childcare facilities who received disinfection and hand hygiene technical training or supervision was significantly lower than that in urban areas. However, the spread rate of infectious disease clusters in rural schools was higher than that in urban areas, while the qualified rate of disinfection in rural schools was lower than that in urban areas (23, 24). Therefore, childcare facilities in rural areas were critical segments to improve the control and prevention strategies for infectious disease in China. Moreover, the results of this study showed that scores of staff with different regions, public or privately owned, education, and training or supervision were significantly different. Scores of staff with different ages, educations, professions, and training or supervision were significantly different. The influencing factors that influenced attitude and practice were inconsistent with that of knowledge, except for training and supervision. This aspect highlighted the importance of training and supervision effort and should be more targeted.
The results of this study demonstrated that the lowest knowledge accuracy rate of childcare facilities staff was about the usable range of disinfectants: The accuracy rate of “Know that alcohol disinfectants could not be used for all infectious diseases” was 46.3%. The lowest attitude and behavior accuracy were consistent with that of knowledge. “Consider that there is no need for large-scale outdoor disinfection during the pandemic” was the lowest accuracy rate for attitude (4.2%), and “Never sprayed alcohol to disinfect air since 2020” was the lowest accuracy rate for practice (5.3%). Although the Chinese government promoted work requirements such as the “seven No's” principle of disinfection and the application scope and use method of common disinfectants (25), this study showed inadequate implementation in childcare facilities. According to a survey among 154 countries, China is one of the countries with the highest use of disinfectants during the COVID-19 pandemic, alcohol-based and chlorine-based disinfectants were reported to be the most widely used. The most commonly reported health problems, including skin and respiratory issues, were related to the two disinfectants mentioned earlier (26). The reasons for health problems included misuse and overuse of disinfectants (26, 27). During the COVID-19 pandemic, alcohol poisoning accounted for 8.5% of children in the pediatric emergency department of a hospital in Turkey, indicating a higher incidence compared to before the pandemic (28). This study highlighted the dangers posed to both staff and children if disinfectants were misused. In the United Kingdom and the United States, there are monitoring systems for poisoning caused by exposure to disinfectants (27, 29), it is helpful to evaluate and provide guidance to the public on the proper use of disinfectants. It is suggested that China also needs to establish and improve a monitoring system covering the use of disinfectants, disinfection effectiveness, and adverse reactions.
The results of this study showed that although the accuracy rate of hand hygiene knowledge among the childcare facility staff was high—“Know that it is better to wash your hands with running water and hand sanitizer” and “Know the timing of hand hygiene” were 83.7% and 89.0%, respectively—the attitude of staff was positive too. The support rate of “Consider that the 6-step wash makes your hands cleaner” was 96.9%, the “always” practice rate of “Washed hands when coming back from public places from 2020” was 89.7%, which was consistent with the survey results of rural adults from 3 provinces in China (17), and it was higher than the rate of adult residents from Ghana (61.5%−66.5%) (8). However, the practice rate of “ Wash hands with six steps since 2020” was not high, with “always” measured at 63.0%. The rate was lower than the implementation rate (79%−87%) of adults who “always” washed their palms, back of hands, between the fingers, fingertips, and thumbs during the partial block in Saudi Arabia 2020 (30). It may be related to the trend of the pandemic, and the difference between respondents. Furthermore, washing hands with six steps needs more time, as the rate of washing at least 20 times was not high (51.7%) in rural adults from 3 provinces in China (17). This finding is similar to the responsibilities of medical workers as childcare facility staff take care of children, and their hand hygiene compliance should be improved. Some studies investigated disinfection and hand hygiene knowledge in childcare facilities. While the intervention methods varied significantly, such as training and publicity, facility improvement, and interest stimulation, the effectiveness remained inconsistent (31–33). To improve the operability of hand hygiene, some studies in medical institutions showed that three-step techniques with hand rubbing (1. covering all surfaces of the hands, 2. rotationally rubbing the fingertips in the palm of the alternate hand, and 3. rotationally rubbing both thumbs) resulted in higher compliance with both hand hygiene indications and technique compared to the six steps. As the results of the microbiological analyses exclude inferiority, the conventional six steps could be safely replaced by a simpler hand hygiene technique. Three-step techniques were simpler, faster, and easier to popularize among the public (34). However, whether three steps with water and handwashing work similarly or not, and the effects on infectious disease control and prevention in the community need to be studied. Moreover, childcare facilities should be accompanied by specifically structured, model surveillance studies that further clarify outstanding questions about infectious disease events and hygiene control (10).
Limitation
In this study, a stratified multi-stage and convenient sampling method was adopted to select districts and childcare institutions, but not randomly. The reason for this was the lack of a perfect disinfection work monitoring system in childcare facilities in our province, leading to varying study conditions and degree of cooperation among different districts. As a result, the knowledge accuracy rate, attitude support rate, and compliance level of childcare facilities staff in this study may be better than the provincial average level. Therefore, the analysis and discussion were mainly conducted from the perspective of the facilities' character, working modes, and other notable limitations.
Conclusion
During the COVID-19 pandemic, the disinfection and hand hygiene knowledge among childcare facilities staff was found to be inadequate, especially in rural areas where training and publicity should be strengthened. However, the attitude and knowledge of the staff were mostly consistent. Hand hygiene compliance should be improved. We recommend establishing a comprehensive monitoring system that includes the usage, effectiveness, and adverse reactions related to disinfection, along with evaluating and guiding the public in the proper use of disinfectants in China. Furthermore, effective intervention measures should be taken to enhance staff compliance with hand hygiene. Further research should be considered on the training and intervention of disinfection and hand hygiene, the safety of disinfection measures, and more operational hand hygiene methods in childcare facilities.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author: aHNjZjExOUAxNjMuY29t.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants in accordance with the national legislation and the institutional requirements.
Author contributions
FC: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. QX: Conceptualization, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by the Disinfection Research Project of Chinese Preventive Medicine Association (XD2022-Z-07).
Acknowledgments
We would like to thank the participants for their generous participation in this study. We would also like to thank Kang Yang, Hao Fei Lin, He Fang Fang, Yu Yu Wen, Pei Ru Xu, who participated in distributing the WJX questionnaire in the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mattison CP, Calderwood LE, Marsh ZA, Wikswo ME, Balachandran N, Kambhampati AK, et al. Childcare and School Acute Gastroenteritis Outbreaks: 2009-2020. Pediatrics. (2022) 150:e2021056002. doi: 10.1542/peds.2021-056002
2. Weng XJ, Wang R, Wang XY, Li N, Yu L, Zhang YP. Epidemiological characteristics of communicable disease related public health emergencies in schools (child care settings) in China, 2014–2016. Dis Surveillance. (2019) 34:446–50.
3. Qian LZ, Jin RY, Lv WJ. Surveillance and analysis of epidemic situation of school infectious diseases in Ruian City from 2014 to 2018. Anhui J Prev Med. (2021) 1, 45–47. doi: 10.19837/j.cnki.ahyf.2021.01.011
4. Lopez AS, Hill M, Antezano J, Vilven D, Rutner T, Bogdanow L, et al. Transmission Dynamics of COVID-19 Outbreaks Associated with Child Care Facilities - Salt Lake City, Utah, April-July 2020(J). Morbid Mortal Wkly Rep. (2020) 69:1319–23. doi: 10.15585/mmwr.mm6937e3
5. Lisa Bender. Key Messages and Actions for COVID-19 Prevention and Control in Schools (n.d), UNICEF, WHO, IFRC. (2020). Available online at: https://www.who.int/publications/m/item/key-messages-and-actions-for-covid-19-prevention-and-control-in-schools (accessed January 22, 2024).
6. Sun JY, Cui H Y, Qian QQ. Analysis of infection risk factors in close contacts of HFMD in childcare facilities in Xicheng District Beijing. Chinese J Sch Health. (2015) 06:939–941.
7. Almutairi AF, BaniMustafa A, Alessa YM, Almutairi SB, Almaleh Y. Public Trust and Compliance with the Precautionary Measures Against COVID-19 Employed by Authorities in Saudi Arabia. Risk Manag Healthc Policy. (2020) 13:753–60. doi: 10.2147/RMHP.S257287
8. Omari R, Zotor F, Baah-Tuahene S, Arthur W. Handwashing knowledge, attitudes, and practices in Ghana. J Prev Med Hyg. (2022) 63:E59–68. doi: 10.15167/2421-4248/jpmh2022.63.1.2271
9. Watson J, Cumming O, Aunger R, Deola C, Chase RP, Dreibelbis R. Child handwashing in an internally displaced persons camp in Northern Iraq: A qualitative multi-method exploration of motivational drivers and other handwashing determinants. PLoS ONE. (2020) 15:e0228482. doi: 10.1371/journal.pone.0228482
10. Walger P, Heininger U, Knuf M, Exner M, Popp W, Fischbach T, et al. Children and adolescents in the CoVid-19 pandemic: Schools and daycare centers are to be opened again without restrictions. The protection of teachers, educators, carers and parents and the general hygiene rules do not conflict with this. GMS Hyg Infect Control. (2020)15:Doc11. doi: 10.3205/dgkh000346
11. Jang Y, Zhou LJ, Guan JJ. Effect evaluation of scenario simulation training in disinfection related knowledge training for caregivers in kindergartens. Shanghai Med. (2022) 43:54–57.
12. Wang XJ, Wang T, Shen TY. Knowledge of disinfection and isolation and level of prevention and control of infectious diseases among childcare workers in kindergartens in Xicheng District of Beijing. Occup and Health. (2019) 35:1554–7. doi: 10.13329/j.cnki.zyyjk.2019.0411
13. Zomer TP, Erasmus V, van Empelen P, Looman C, van Beeck EF, Tjon-A-Tsien A, et al. Sociocognitive determinants of observed and self-reported compliance to hand hygiene guidelines in child day care centers. Am J Infect Control. (2013) 41:862–7. doi: 10.1016/j.ajic.2012.11.023
14. Wang MX, Pang J. The knowledge, attitudes and practices of hand, foot, and mouth disease prevention strategies amongst parents and educators of children under 5 years amidst COVID-19 pandemic: A cross-sectional study. Front Public Health. (2022) 10:908004. doi: 10.3389/fpubh.2022.908004
15. National Health Commission. Prevention and control Plan of Novel coronavirus pneumonia [S]. 3th edition, Beijing: National Health Commission (2020). Available online at: http://www.nhc.gov.cn/xcs/zhengcwj/202001/470b128513fe46f086d79667db9f76a5.shtml (accessed November 9, 2023).
16. Brown LG, Hoover ER, Barrett CE, Vanden Esschert KL, Collier SA, Garcia-Williams AG. Handwashing and disinfection precautions taken by U.S. adults to prevent coronavirus disease 2019, Spring 2020. BMC Res Notes. (2020) 13:550. doi: 10.1186/s13104-020-05398-3
17. Zheng Z, Liang C, Li Z, Wu Y, Lin B, Fang J. Mask-wearing and handwashing behaviors of Chinese rural residents during the pandemic of COVID-19: a cross-sectional survey. Int J Environ Res Public Health. (2022) 20:779. doi: 10.3390/ijerph20010779
18. Leung MW, O'Donoghue M, Suen LK. Personal and household hygiene measures for preventing upper respiratory tract infections among children: a cross-sectional survey of parental knowledge, attitudes, and practices. Int J Environ Res Public Health. (2022) 20:229. doi: 10.3390/ijerph20010229
19. Zhou WY, Mao LX. Investigation on the hygiene and disinfection status of migrant workers' children's kindergartens and the knowledge of hand hygiene of kindergarten teachers. Chinese Rural Health Service Administration. (2015) 02:193–4.
20. Mahadzar AS, Rahman HA. Knowledge, Attitude and practice towards hand, foot and mouth disease (HFMD) among nursery governesses in Klang Valley, Selangor. Malays J Med Health Sci. (2019) 15:407.
21. Almoslem MM, Alshehri TA, Althumairi AA, Aljassim MT, Hassan ME, Berekaa MM. Handwashing Knowledge, Attitudes, and Practices among Students in Eastern Province Schools, Saudi Arabia. J Environ Public Health. (2021) 2021:6638443. doi: 10.1155/2021/6638443
22. Fan JH, Ji XF, Zhang CY, Tian L, Jiang N, Huang LL, et al. Investigation and analysis on the effect of disinfection training of SARS-CoV-2 in schools of Shanghai. Chinese J Disinf. (2022) 7:5003.
23. Zhao LH. Epidemiological characteristics of school public health emergencies in Haizhou District, Lianyungang City, 2016- 2021. Jiangsu J Prev Med. (2022) 05:580–2. doi: 10.13668/j.issn.1006-9070.2022.05.027
24. Zou YM, Liu YH, Wang HS, You YQ, Lan CJ, Zhu D. Disinfection quality of secondary and primary schools and kindergartens in Wuxi. Chinese J Sch Health. (2021) 2 :291–293. doi: 10.16835/j.cnki.1000-9817.2021.02.032
25. National Health Commission. Notice to carry out comprehensive and accurate environmental hygiene and disinfection work. Beijing: National Health Commission. (2020). Available online at : https://www.gov.cn/xinwen/2020-06/18/content_5520232.htm (accessed November 9, 2023).
26. Hashemi F, Hoepner L, Hamidinejad FS, Haluza D, Afrashteh S, Abbasi A, et al. A comprehensive health effects assessment of the use of sanitizers and disinfectants during COVID-19 pandemic: a global survey. Environ Sci Pollut Res Int. (2023) 30:72368–88. doi: 10.1007/s11356-023-27197-6
27. Chang A, Schnall AH, Law R, Bronstein AC, Marraffa JM, Spiller HA, et al. Cleaning and Disinfectant Chemical Exposures and Temporal Associations with COVID-19 - National Poison Data System, United States, January 1, 2020-March 31, 2020. MMWR Morb Mortal Wkly Rep. (2020) 69:496–8. doi: 10.15585/mmwr.mm6916e1
28. Salman H, Salman Z, Akçam M. Childhood Poisoning During the COVID-19 Pandemic. Turk Arch Pediatr. (2023) 58:268–73. doi: 10.5152/TurkArchPediatr.2023.22247
29. Cook MA, Brooke N. Event-Based Surveillance of Poisonings and Potentially Hazardous Exposures over 12 Months of the COVID-19 Pandemic. Int J Environ Res Public Health. (2021) 18:11133. doi: 10.3390/ijerph182111133
30. Al-Wutayd O, Mansour AE, Aldosary AH, Hamdan HZ, Al-Batanony MA. Handwashing knowledge, attitudes, and practices during the COVID-19 pandemic in Saudi Arabia: A non-representative cross-sectional study. Sci Rep. (2021) 11:16769. doi: 10.1038/s41598-021-96393-6
31. Serra ME. Prevention of respiratory infections at day care centers: recommendations and systematic review of the evidence. Arch Argent Pediatr. (2014) 112:323–31. doi: 10.5546/aap.2014.eng.323
32. Gudnason T, Hrafnkelsson B, Laxdal B, Kristinsson KG. Does hygiene intervention at day care centres reduce infectious illnesses in children? An intervention cohort study. Scand J Infect Dis. (2013) 45:397–403. doi: 10.3109/00365548.2012.749424
33. Or PP, Ching PT, Chung JW. Can Flu-Like Absenteeism in Kindergartens Be Reduced Through Hand Hygiene Training for Both Parents and Their Kindergarteners? J Prim Care Community Health. (2020) 11:2150132719901209. doi: 10.1177/2150132719901209
Keywords: disinfection, hand hygiene, childcare facilities, knowledge, attitude, practice, COVID-19
Citation: Chen F and Xu QH (2024) Disinfection and hand hygiene knowledge, attitude, and practices among childcare facilities staff during the COVID-19 pandemic in Anhui, China: a cross-sectional study. Front. Public Health 12:1335560. doi: 10.3389/fpubh.2024.1335560
Received: 09 November 2023; Accepted: 11 March 2024;
Published: 04 April 2024.
Edited by:
Mahlagha Dehghan, Kerman University of Medical Sciences, IranReviewed by:
Mohammad Ali Zakeri, Rafsanjan University of Medical Sciences, IranAsma Ghonchehpour, Kerman University of Medical Sciences, Iran
Copyright © 2024 Chen and Xu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qing Hua Xu, eHFoMTEyNkBzaW5hLmNvbQ==