 An-Qi Wang
An-Qi Wang Wen-Di Cheng2
Wen-Di Cheng2 Ya-Shuang Luo
Ya-Shuang Luo Hai-Yin Wang
Hai-Yin Wang- 1School of Public Health, Shandong Second Medical University, Weifang, Shandong, China
- 2Department of Health Technology Assessment, Shanghai Health Development Research Center (Shanghai Medical Information Center), Shanghai, China
- 3School of Public Health, Shanghai University of Traditional Chinese Medicine, Shanghai, China
Background: China faces various public health emergencies, and emergency responders at the Centers for Disease Control and Prevention (CDC emergency responders) are a mainstay in responding to public health emergencies. Career resilience can help CDC emergency responders to effectively respond to and recover from public health emergencies, but there is no specific measurement instrument available. In this study, we aimed to develop and conduct an initial validation of the career resilience instrument for CDC emergency responders in China within the context of public health emergencies from a process perspective.
Methods: Based on a survey conducted in Shanghai, interpretive phenomenological analysis (IPA), which is a qualitative research approach to describing and analyzing individual experiences, was used to analyze the interview texts to develop the initial career resilience instrument for CDC emergency responders. The initial career resilience instrument was revised through two rounds of expert consultation. Cronbach’s α coefficient and exploratory factor analysis were used to test the reliability and validity of the revised career resilience instrument.
Results: The initial career resilience instrument for CDC emergency responders contained three first-level measurement dimensions, 9 second-level measurement dimensions, and 52 measurement items. After expert consultation, the first-level and second-level measurement dimensions were not revised, 13 measurement items were deleted or revised, and six measurement items were added, resulting in 48 measurement items. The revised career resilience instrument was tested for good reliability and validity.
Conclusion: Career resilience for CDC emergency responders can be regarded as a set of protective factors and dynamic processes that can be cultivated and intervened in cognitive, affective, and behavioral dimensions to improve their ability to respond to and recover from public health emergencies.
1 Introduction
In recent years, with the outbreak of severe acute respiratory syndrome (SARS), the global spread of H1N1, the Ebola virus disease (EVD) epidemic in West Africa, the global pandemic of corona virus disease 2019 (COVID-19), and the frequent occurrence of various emergencies, the international community has entered a period of high risk of public health emergencies (1). China, a large country with a population of 1.41 billion, has a high population density and experiences frequent movement of its population within and outside the country, coupled with global warming and rapid urbanization, meaning that China faces greater risks and challenges in terms of public health emergencies (2). Since the outbreak of SARS, China has continued to improve its response mechanism for public health emergencies and accelerate the reform of its public health system (3). The Centers for Disease Control and Prevention (CDC) in China, an important public health agency, have also been in the public spotlight in regard to a series of reforms, mainly concerning managing and responding to public health emergencies through pre-event surveillance and risk assessment, the coordination of resources and provision of epidemiological technical services during events, and post-event summary and analysis to safeguard public health (4, 5). Emergency responders at the Centers for Disease Control and Prevention (CDC emergency responders) are the main force that undertakes the health emergency work of the CDC. CDC emergency responders are those normally undertaking routine work at the CDC, and assuming responsibility for health emergency response and disposal work in the event of public health emergencies, such as comprehensive coordination, sampling, laboratory testing, epidemiological investigation, and disinfection (6). CDC emergency responders face excessive workloads, the risk of viral infection, negative emotions, and turnover intentions during public health emergencies, when individuals need powerful forces to recover to a normal psychological state and work performance level (7, 8). These powerful forces are the same individual characteristics, regulatory processes, and social supports that McLarnon identified in his research, suggesting that they be defined as resilience, where individuals rely on these characteristics, processes, and support systems to recover to pre-event levels of performance and well-being (9).
The application of resilience in the career field is known as “career resilience” and was first proposed by London as a component of career motivation (10). The continued study of career resilience is necessary because every employee experiences adverse events in the workplace, and resilience can help employees cope with and bounce back from adversity to achieve positive outcomes and well-being (11, 12). However, there is not yet a unified perspective on the operational definition of career resilience. The trait perspective views career resilience as a characteristic or ability relating to combatting career adversity, coping with work stress, and adapting to environmental change (13–15). The outcome perspective views career resilience as achieving favorable outcomes in the face of adversity or stress in the workplace, including recovery to a normal work state or growth toward a new ordered state (16, 17). The process perspective views career resilience as the positive and effortful process by which individuals adapt to and recover from adversity in the workplace, involving their initial responses in the early stages of adverse events, individual protective factors, and self-regulatory processes (18, 19). We assume that the process perspective can more comprehensively describe the dynamic development process of resilience, which contains the connotative elements in the trait and outcome perspectives. Therefore, in this study, we attempted to develop the career resilience measurement instrument for CDC emergency responders from a process perspective.
King and Rothstein (20) have provided a more comprehensive and cogent view of career resilience from a process perspective. In the King and Rothstein (20) model, career resilience has been conceptualized as a dynamic process of individual-environment interaction, involving a higher-order, multidimensional construct of cognitive, affective, and behavioral protective factors and self-regulatory processes (20). These resilience processes are provoked by individual initial responses to an adverse event in the workplace and influenced by individual protective factors and social support resources, leading to self-regulation and recovery from an adverse event (21). Specifically, career resilience entails (a) individual protective factors, such as positive cognitive, affective, and behavioral characteristics; (b) social support resources; (c) initial responses following an adverse event; and (d) self-regulatory processes, such as positive self-cognitive, self-affective, and self-behavioral regulation, as well as related recovery outcomes (20). This model was developed to capture the key elements and processes by which individuals recover from adversity in the workplace, suggesting that resilience can be elicited through the management of an individual’s thoughts, feelings, and actions to cope with various adverse events and poor experiences in the workplace (9).
Previous studies rarely explored the connotative elements and measurement instruments of career resilience from a process perspective, much less developed context-and population-specific career resilience instruments with CDC emergency responders as the subject of study. Using the King and Rothstein (20) model as a guide, this study explores where career resilience for CDC emergency responders should be measured in the context of public health emergencies, particularly in the face of major public health emergencies. Thus, the aim of this study was to (a) develop the career resilience instrument for CDC emergency responders, and (b) conduct an initial validation of the developed career resilience instrument.
2 Methods
2.1 Study design
This study was conducted in three phases: (a) Face-to-face, in-depth, semi-structured interviews were conducted with the sampled CDC emergency responders, and the initial career resilience instrument for CDC emergency responders was generated by analyzing the interview texts. (b) Through consultation with experts in the field of health emergencies, the initial career resilience instrument for CDC emergency responders was revised and improved based on the importance ratings and revision opinions of the experts. (c) The reliability and validity of the revised career resilience instrument for CDC emergency responders were validated.
2.2 Sampling and data collection
Participants in this study were included according to the selection criteria provided below, and each participant understood the purpose of this survey and agreed to participate in it. The survey could be terminated at any time if the participant did not want to continue participating in the survey while it was in progress. The participants in this study were from Shanghai, the center city of China, with 16 districts, a total area of 6340.5 square kilometers, and a resident population of 24.76 million in 2022. From March to May 2022, Shanghai was under closed management in response to COVID-19, in which CDC emergency responders played an important role.
First, the criteria for selecting the interview subjects in this study were as follow: we included those who (a) were engaged in health emergency-related work at the CDC for 2 years or more, (b) had participated in health emergency response and disposal of public health emergencies, and worked for a cumulative duration of 14 days or more, and (c) volunteered and agreed to participate in the interviews. In accordance with the above criteria, 10 emergency responders were sampled from each of the three district-level CDCs in central, suburban, and far-suburban Shanghai, serving as the interview subjects for this study, finally, 30 interview subjects were selected. The interview centered on “CDC emergency responders’ literacy characteristics, main tasks, difficulties encountered, ways of overcoming difficulties, changes in thoughts and feelings, adjustments in work status, etc.” Each interview subject was interviewed once in a face-to-face, in-depth, semi-structured interview, with three interviewers using the same interview outline (refer to the detailed interview outline in Additional File 1), which was audio-recorded in its entirety, with the interview subject’s permission. For these three interviewers, one acted as the lead interviewer, and the other two were responsible for transcribing and supplementing. At the end of the interview, it was determined that each interview lasted between 20 and 40 min, and the interview data were organized promptly. If the interview subject did not allow audio-recording, the two interview transcribers compared what was transcribed and, in case of disagreement, could first seek confirmation from the lead interviewer. If the lead interviewer was unable to provide confirmation, the interview subject could be asked to confirm the information again to ensure accuracy and form a complete text. If the interview subject allowed audio-recording, it could be transcribed into a text by listening to the audio-recording repeatedly. Thirty interview texts were eventually collected.
Second, the criteria for selecting the experts to be consulted were as follow: the participants had to have (a) been engaged in health emergency-related work for 5 years or more, (b) carried out research work related to health emergencies, and (c) volunteered and agreed to participate in this survey. Based on the above criteria, 25 experts were sampled for this study, 24 of whom completed the consultation form, and two rounds of consultation were conducted with these experts. The initial career resilience instrument for CDC emergency responders, generated based on the interview text, was subjected to the first round of expert consultation, in which experts scored the importance of each dimension and item on a scale of 1–5, with higher scores representing greater affirmation of significance and importance. The initial career resilience instrument was revised through the first round of expert consultation, and the revised instrument was subjected to the second round of expert consultation, in which, again, the scores were rated on a scale of 1–5 according to importance.
Finally, we compiled the career resilience instrument, as revised through expert consultations, into a questionnaire and validated its reliability and validity after sampling CDC emergency responders to complete the questionnaire. The sampled CDC emergency responders fitted the following criteria: they (a) were involved in responding to public health emergencies, (b) worked in emergency-related operational departments at CDC, and (c) volunteered and agreed to participate in filling out this questionnaire. There are 16 district-level CDCs in Shanghai, and we randomly sampled 80–120 CDC emergency responders using the above criteria from each district CDC to fill out the questionnaire anonymously. For each questionnaire, we performed strict quality control procedures and eliminated questionnaires with incomplete key information and contradictory logic, ultimately leading to 1,286 valid questionnaires.
2.3 Data analysis
Interpretive phenomenological analysis (IPA) is a widely used qualitative research approach for describing and analyzing the subjective perceptions and experiences of individuals, revealing the meaning of each individual experience, comparing commonalities and differences, and then reducing the description of the individual experience to the essential elements and features of the things (22). We first used IPA to analyze the collected interview texts. To ensure the reliability of the analysis results, two researchers analyzed the interview texts in a back-to-back format. Where the two researchers’ analyses differed, a third researcher was asked to exercise judgment in order to determine the final analysis results. This study followed the steps of IPA (23, 24): firstly, the interview texts were read repeatedly, and initial notes and comments were made on valuable textual information. Secondly, the repetitive and similar initial notes and comments were merged and summarized to form the main comments, based on which sub-themes were extracted and named. Finally, associations between sub-themes were searched for, similar sub-themes were clustered into theme groups, and these theme groups were streamlined and refined to produce themes. As all the interview texts were analyzed and correlations between themes were explored in the above process, the IPA steps of “analyzing the information of the next subject, looking for thematic patterns between each other” were not repeated.
Second, this study applied the expert positivity coefficient, expert authority coefficient, and expert coordination coefficient to evaluate the expert consultations. The expert positivity coefficient refers to the degree of interest and cooperation of experts in this study, which is reflected through the valid response rate for the expert consultation form, and usually a response rate of 70% or more indicates a good expert positivity coefficient (25). The expert authority coefficient is reflected by the experts’ familiarity with the study and the judgment basis, and the mean value of the familiarity score and judgment basis score is the expert authority coefficient, which is above 0.7, indicating reliable results (25). The familiarity was set at five levels, ranging from “very familiar” to “very unfamiliar,” with scores of 1, 0.8, 0.6, 0.4, and 0.2, respectively, and the judgment basis was divided into four dimensions, namely, work experience, theoretical analysis, reference literature, and intuitive feeling. Each dimension was divided into three levels,namely, large, medium, and small, and the specific scores are shown in Table 1. The expert coordination coefficient is generally calculated using Kendall’s W (W), which is used to reflect the degree of coordination of the experts’ opinions regarding the content of the consultation. The W-value is between 0 and 1, and after several rounds of expert consultation, the W-value generally fluctuates at around 0.5. The significance of the W-value is tested using χ2, and a W-value that is statistically significant (p < 0.05) indicates that the degree of coordination of the opinions among experts is good (25). In addition, we adopted the boundary value method to screen the indicators, and according to the importance ratings (ranging from 1 to 5) and revised opinions of the experts, the indicators with “the mean value of importance less than 4, and the coefficient of variation greater than 0.25″ were deleted or revised (26, 27).
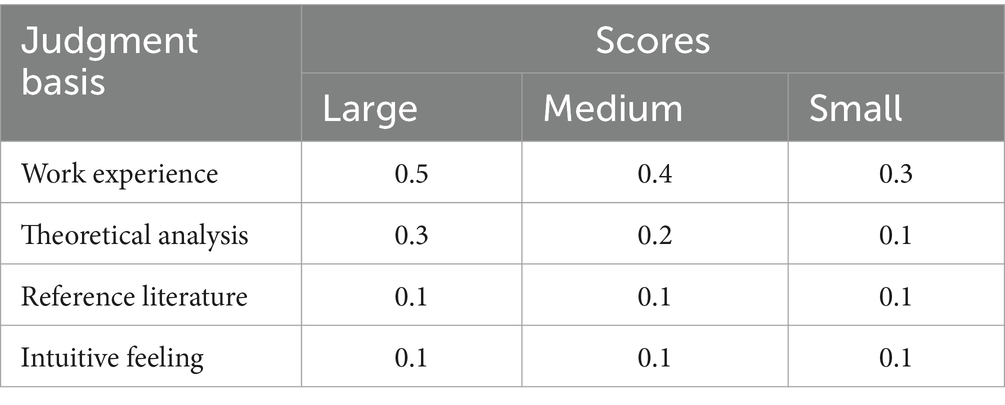
Table 1. Scale for assigning scores to the expert judgment basis.
Third, for the career resilience instrument, as revised by the expert consultations, we used Cronbach’s α coefficient to test its reliability and exploratory factor analysis to determine its structural validity. A Cronbach’s α coefficient greater than 0.7 indicates good reliability, and in exploratory factor analysis, a Kaiser-Meyer-Olkin (KMO) value greater than 0.7 and a p-value less than 0.05 indicate that it is suitable for factor analysis (28). In this study, the principal component method was used for factor extraction, the maximum variance method was used for factor rotation, and the number of factors was determined based on the eigenvalue being greater than 1. The items with a factor loading greater than 0.4 were considered appropriate.
3 Results
3.1 Demographic characteristics
3.1.1 Demographic characteristics of the interview subjects
Of the 30 interviewed subjects, 13 were male, accounting for 43.33%. The majority were 31–35 years old, amounting to 36.67%. The academic qualifications and majors were predominantly a postgraduate degree and preventive medicine, accounting for 63.33 and 93.33%, respectively. The titles and positions were mainly middle level and common staff, accounting for 53.33 and 80.00%, respectively. Working tenure was mostly 6–10 years, accounting for 36.67%. The specific demographic characteristics of the interviewed subjects are shown in Table 2.
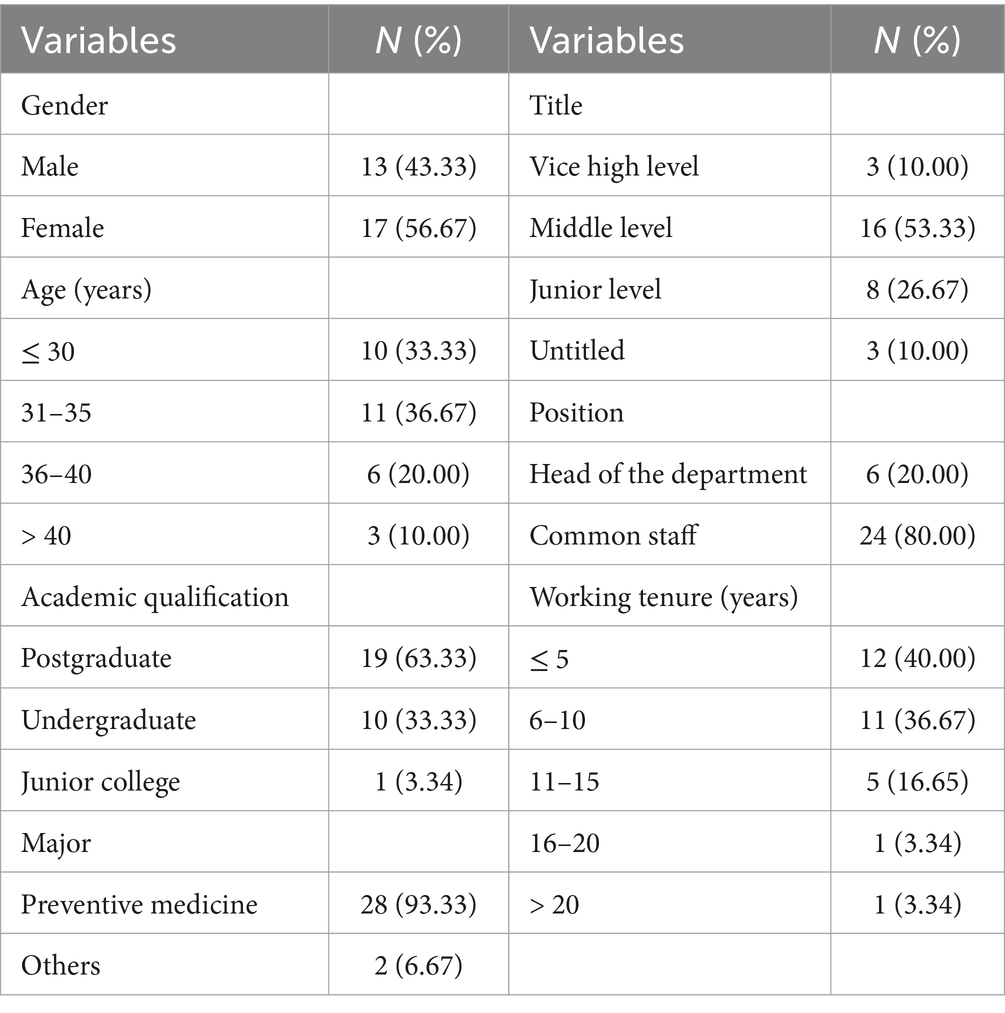
Table 2. Demographic characteristics of interview subjects (N = 30).
3.1.2 Demographic characteristics of the experts consulted
Two rounds of consultation were conducted with 24 experts in this study. The experts consulted were mainly female, accounting for 58.33%, and mostly 36–40 years old, accounting for 41.67%. The academic qualifications and majors were predominantly a postgraduate degree and preventive medicine, accounting for 70.83 and 87.50%, respectively. Titles and positions were mainly middle level and head of the department, accounting for 54.17 and 66.66%, respectively. Working tenure was mostly 11–15 years, accounting for 37.50%. The specific demographic characteristics of the experts consulted are shown in Table 3.
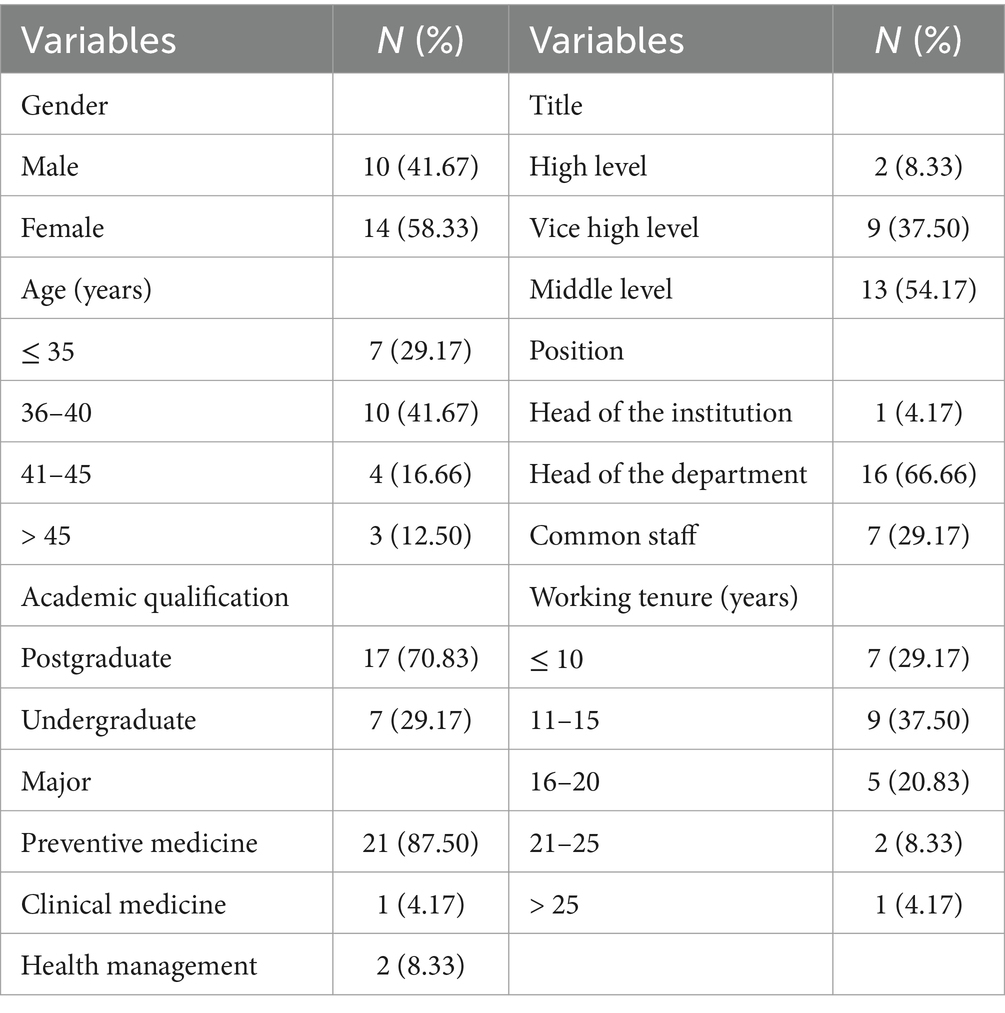
Table 3. Demographic characteristics of the experts consulted (N = 24).
3.1.3 Demographic characteristics of the CDC emergency responders sampled from 16 district-level CDCs in Shanghai
Of the 1,286 CDC emergency responders sampled, 543 (42.22%) were male, and there were more participants under the age of 30 and between 31 and 40 years of age, accounting for 38.18 and 37.56%, respectively. The academic qualifications and majors were predominantly undergraduate and preventive medicine, accounting for 65.32 and 79.47%, respectively. The majority of the titles and positions were middle level and common staff, accounting for 41.68 and 85.07%, respectively, while the majority of the working tenure was less than 5 years, accounting for 39.42%. The specific demographic characteristics of the sampled CDC emergency responders are shown in Table 4.
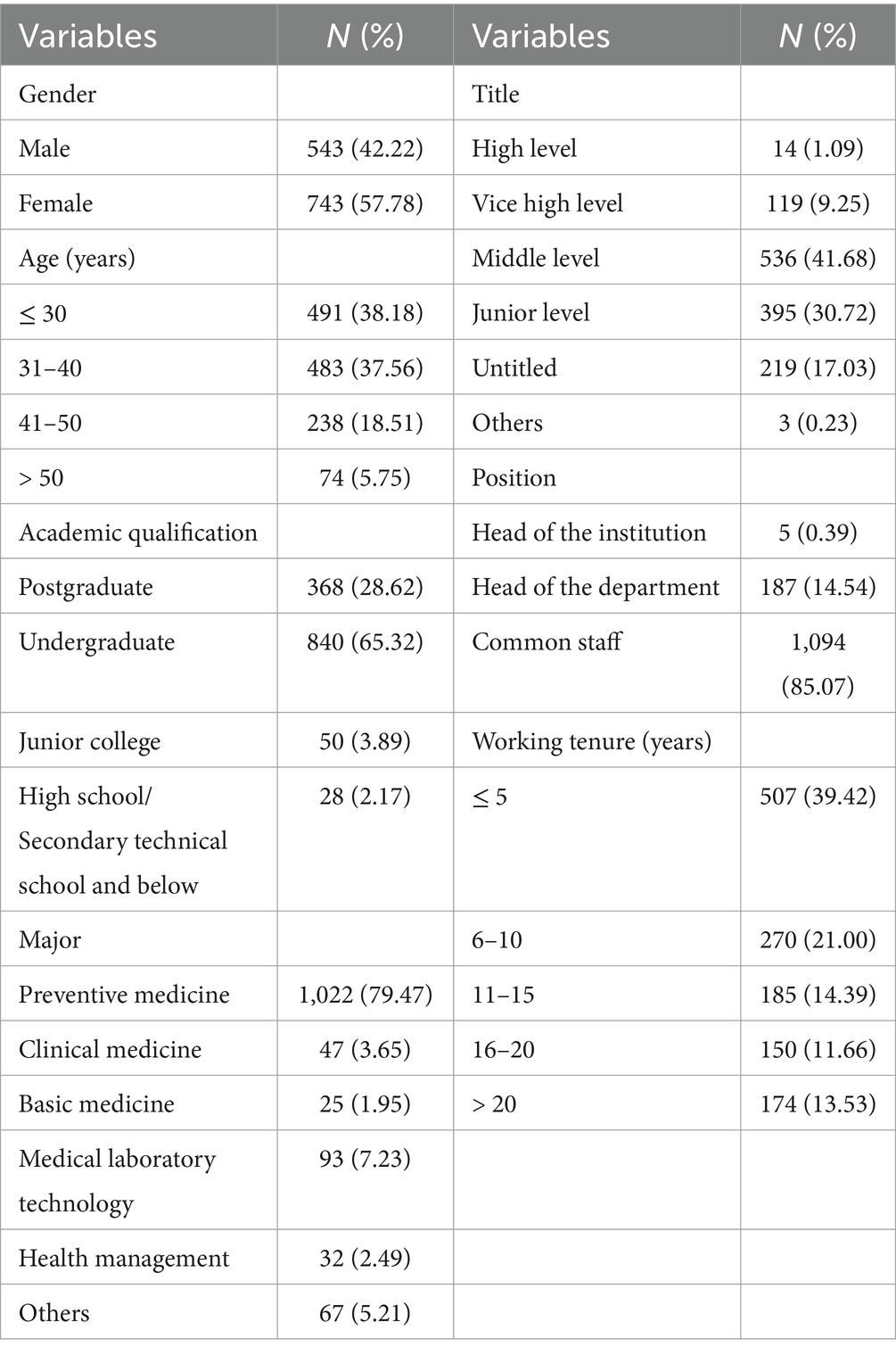
Table 4. Demographic characteristics of the CDC emergency responders sampled from 16 district-level CDCs in Shanghai (N = 1,286).
3.2 Interview text analysis results
IPA was used in this study to analyze the interview texts. The researchers read the interview texts repeatedly to fully familiarize themselves with these texts and acquire an overall impression of the situation described by the interview subjects. On this basis, with an open mind, initial notes and comments were made on the original statements in the interview texts that were related to the theme of this study. The collected interview texts of the 30 interview subjects extracted 567 original statements related to the theme of this study, and these original statements were subjected to initial notes and comments. Subsequently, repetitions and similarities of the 567 initial notes and comments were merged and collated, resulting in 52 main comments. Nine sub-themes were extracted by iterating through and reflecting on the 52 main comments and referring to the King and Rothstein model (20). The nine sub-themes were clustered into three theme groups by searching for correlations between them. The three theme groups were streamlined and refined into three themes with reference to Duchek’s resilience model (29), which elaborates that resilience consists of the ability to anticipate an unexpected event, cope during an unexpected event, and adapt afterward.
3.2.1 Theme 1: anticipatory resilience
In this study, anticipatory resilience referred to the CDC emergency responders’ resilience characteristics possessed before public health emergencies, which could be a guide and facilitator allowing individuals to clearly define their roles, maintain stable emotions, and quickly enter the “wartime” state when emergencies occurred. Anticipatory resilience included four sub-themes: career cognitive characteristics, career affective characteristics, career behavioral characteristics, and resource acquisition ability.
3.2.1.1 Sub-theme 1: career cognitive characteristics
The career cognitive characteristics of CDC emergency responders mainly concerned self-efficacy, sense of meaning in work, etc., which could play a guiding and normative role with respect to individuals changing their cognition of roles, clarifying their role positions, and taking on their role’s function in response to public health emergencies. The career cognitive characteristics contained seven main comments, which are presented in Supplementary Table S1 in Additional File 1.
3.2.1.2 Sub-theme 2: career affective characteristics
The CDC emergency responders were characterized by stable emotions, calmness, and patience with respect to dealing with problems and a passion for work. These characteristics could serve as facilitators and safeguards with regard to allowing individuals to quickly regulate negative emotions and focus on tasks during a response to public health emergencies. There were four main comments on the career affective characteristics, which are shown in Supplementary Table S1 in Additional File 1.
3.2.1.3 Sub-theme 3: career behavioral characteristics
The career behavioral characteristics of CDC emergency responders primarily involved planning, execution, adaptability, innovation, and learning, which could play leading and protective roles in enabling individuals to quickly adjust to the behaviors required in a “wartime” scenario when responding to public health emergencies. The career behavioral characteristics included nine main comments, which are shown in Supplementary Table S1 in Additional File 1.
3.2.1.4 Sub-theme 4: resource acquisition ability
The resource acquisition ability of CDC emergency responders included both instrumental and affective resource acquisition abilities, with six main comments on resource acquisition ability, as shown in Supplementary Table S1 in Additional File 1.
3.2.2 Theme 2: coping resilience
In this study, coping resilience referred to the active self-regulation of CDC emergency responders during their response to public health emergencies, adapting to the emergency work state, and completing emergency tasks flexibly and efficiently. Coping resilience involved four sub-themes: stress responses, self-cognitive regulation, self-affective regulation, and self-behavioral regulation.
3.2.2.1 Sub-theme 5: stress responses
In the initial occurrence of a public health emergency, the CDC emergency responders faced stress with a range of responses, including behavioral, cognitive, emotional, and physiological responses. The stress responses consisted of five main comments, as shown in Supplementary Table S2 in Additional File 1.
3.2.2.2 Sub-theme 6: self-cognitive regulation
Self-cognitive regulation involved CDC emergency responders’ efforts with respect to re-examining a problem, adjusting their cognition about unfavorable circumstances, and changing their ways of conceiving the problems while responding to public health emergencies in order to adjust and adapt to emergencies promptly. There were four main comments on self-cognitive regulation, as shown in Supplementary Table S2 in Additional File 1.
3.2.2.3 Sub-theme 7: self-affective regulation
During the response phase of public health emergencies, CDC emergency responders regulated their negative emotions and work stress and maintained a calm, stable, optimistic, and confident emotional state. There were five main comments on self-affective regulation, which can be seen in Supplementary Table S2 in Additional File 1.
3.2.2.4 Sub-theme 8: self-behavioral regulation
During the response phase of public health emergencies, the CDC emergency responders quickly adjusted from a routine behavioral status to “wartime” emergency behavior to complete the emergency tasks. There were eight main comments on self-behavioral regulation, which can be seen in Supplementary Table S2 in Additional File 1.
3.2.3 Theme 3: recovery resilience
In this study, recovery resilience referred to the ability the of CDC emergency responders to recover from the “wartime” state after the public health emergency response had ceased, as well as their ability to summarize and learn from the emergencies and reflect on their improvement. Recovery resilience included one sub-theme: adaptive outcomes.
3.2.3.1 Sub-theme 9: adaptive outcomes
Adaptive outcomes referred to the ability of CDC emergency responders to recover to their original state, learn and reflect on emergencies, and even reach a new state of equilibrium after a public health emergency response was completed. There were four main comments on the adaptive outcome, as shown in Supplementary Table S3 in Additional File 1.
3.2.4 Initial career resilience instrument
The CDC emergency responders’ connotative components of career resilience in the context of public health emergencies were collected based on the interview text and included the career characteristics of CDC emergency responders, individual stress responses and state regulation during public health emergencies, and recovery and growth after public health emergencies. Therefore, this study developed the initial career resilience instrument for CDC emergency responders by collating and analyzing the interview texts, with 52 main comments serving as the specific measurement items, nine sub-themes serving as the second-level measurement dimensions, and three themes serving as the first-level measurement dimensions.
3.3 Expert consultation results
We compiled the initial career resilience instrument for CDC emergency responders into an expert consultation form, where experts scored the importance of each measurement dimension and each measurement item on a scale of 1–5, with higher scores being considered more appropriate for measuring career resilience.
3.3.1 Basic information on expert consultations
Twenty-five expert consultation forms were sent out for the first round of expert consultation, of which 24 were returned, representing a valid response rate of 96%. In the second round of expert consultations, 24 expert consultation forms were sent out and 24 were returned, with a valid response rate of 100%. The valid response rates for both rounds of expert consultation were above 70%, indicating a high expert positivity coefficient. The authority coefficients of the two rounds of expert consultation were 0.880 and 0.886, respectively, which were both above 0.7, indicating that the results of expert consultation were reliable. The expert coordination coefficients for the first-level and second-level measurement dimensions were 0.420 and 0.423 in the first round of expert consultation and did not change in the second round. The expert coordination coefficients of the measurement items were 0.306 and 0.421 in the first and second rounds of expert consultation, respectively. In the second round of expert consultation, the expert coordination coefficients of each measurement dimension and measurement item were close to 0.5, with p < 0.001, indicating that the experts’ consultation opinions were relatively consistent. Table 5 presents basic information on the expert consultations.
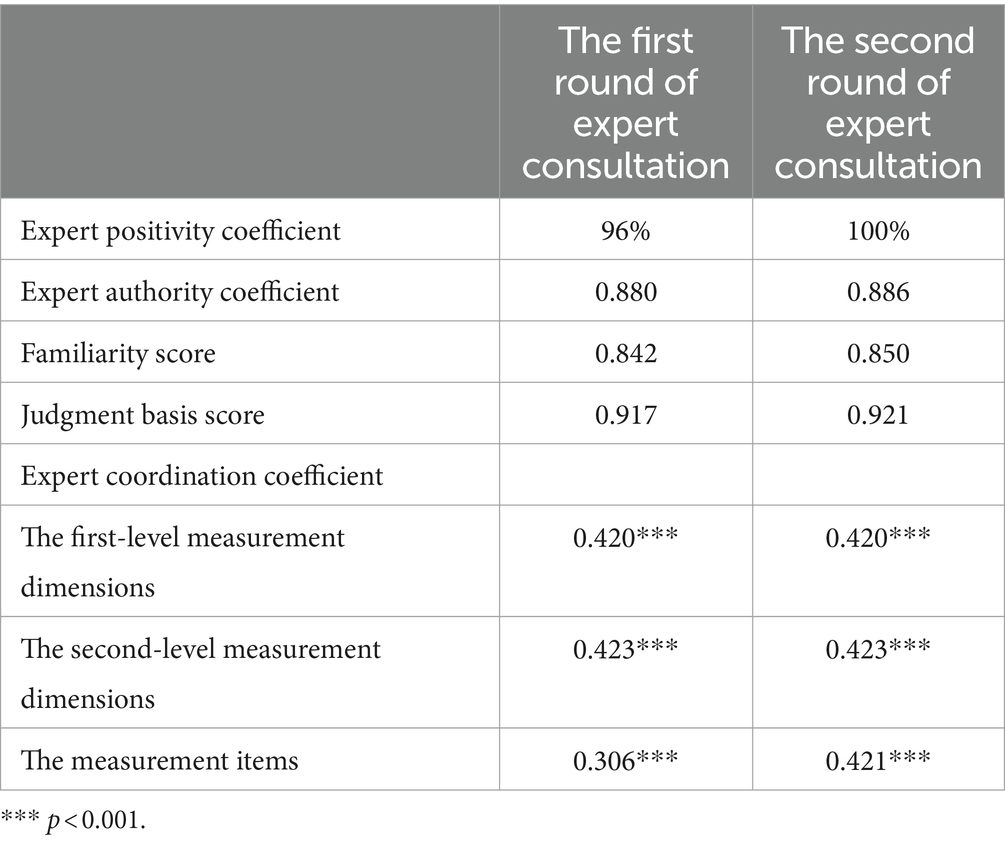
Table 5. Basic information on expert consultation.
3.3.2 Expert revisions to the initial instrument
Measurement dimensions and items were deleted or revised based on the following criterion: a “mean value of importance less than 4 and coefficient of variation greater than 0.25.” The results of both rounds of expert consultation showed that the mean values of importance for the first-level and second-level measurement dimensions were greater than 4 and that the coefficients of variation were less than 0.25, so they were not deleted or revised.
For the measurement items, in the first round of expert consultation, there were 13 items with a mean value of importance less than 4 and a coefficient of variation greater than 0.25. These 13 items were deleted or revised. For example, the item “Ensure coordination of tasks and resources in health emergency response” had a mean value of 2.958 and a coefficient of variation of 0.323, and the experts recommended its deletion because the majority of emergency responders’ tasks and resources are carried out according to regulations or are assigned by their leaders, in which individual coordination plays a minor role, and thus they item does not fully capture the meaning of career resilience. The experts’ specific revision opinions on these items are presented in Supplementary Table S4 in Additional File 1.
Moreover, in the first round of expert consultation, the experts suggested adding the following six items. For the dimension “Career behavioral characteristics,” one item for “Adapting proactively to changes in health emergency work” was added. For the dimension “Self-cognitive regulation,” two items for “During the response to public health emergencies, controlling negative thoughts and believing in good results” and “During the response to public health emergencies, adjusting thoughts and focusing on problems that need to be solved” were added. For the dimension “Self-behavioral regulation,” three items for “During the response to public health emergencies, being able to adjust quickly from the usual work pace to high-intensity work,” “During the response to public health emergencies, proactively reconciling work and family and focusing on the completion of emergency tasks,” and “During the response to public health emergencies, adjusting the way of obtaining information, and proactively collecting and analyzing information on emergencies” were added.
After revision through the first round of expert consultation, all measurement items were subjected to a second round of expert consultation, with a mean value of importance greater than 4 and a coefficient of variation less than 0.25 for all of them, so none of the items were deleted, and only minor revisions were made to the wording and presentation of a few items. The career resilience instrument for CDC emergency responders, as revised by the expert consultation, contained three first-level measurement dimensions, 9 second-level measurement dimensions, and 48 measurement items.
3.4 Reliability and validity test results
3.4.1 Reliability test results
The reliability of the career resilience instrument for CDC emergency responders, as revised via expert consultations, was tested using Cronbach’s α coefficient. The results showed that the Cronbach’s α coefficient for the entire instrument was 0.969; the Cronbach’s α coefficient for the three first-level dimensions of anticipatory resilience, coping resilience, and recovery resilience were 0.956, 0.921, and 0.910 respectively; and the Cronbach’s α coefficient for the 9 second-level dimensions of career cognitive characteristics, career affective characteristics, career behavioral characteristics, resource acquisition ability, stress responses, self-cognitive regulation, self-affective regulation, self-behavioral regulation, and adaptive outcomes were 0.928, 0.913, 0.954, 0.925, 0.871, 0.943, 0.956, 0.961, and 0.910, respectively. The Cronbach’s α coefficients for each dimension were all above 0.8, indicating good reliability of the instrument. Table 6 demonstrates the Cronbach’s α coefficients for each dimension.
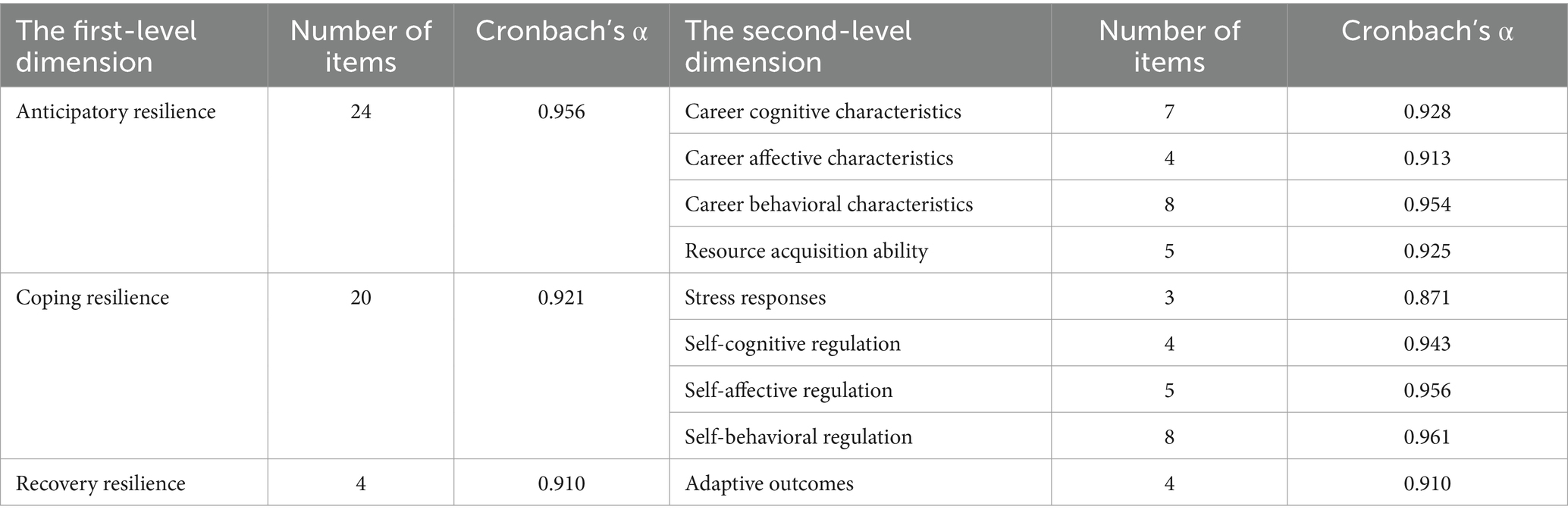
Table 6. The Cronbach’s α coefficients for each dimension.
3.4.2 Validity test results
The exploratory factor analysis was first conducted on the instrument of anticipatory resilience, and the results showed that the KMO value was 0.941, with a p-value of less than 0.001, rendering it suitable for factor analysis. Four factors were extracted from the 24 items, which were in line with the pre-defined results, and named career behavioral characteristics (with eight items), career cognitive characteristics (with seven items), resource acquisition ability (with five items), and career affective characteristics (with four items). The variance percentages of the four factors were 24.522, 21.171, 16.952, and 12.942%, respectively, and the factor loading values of the items corresponding to the four factors were 0.678 ~ 0.850, 0.764 ~ 0.858, 0.697 ~ 0.803, and 0.701 ~ 0.806, respectively. All the factor loading values were above 0.65, indicating good structural validity. Table 7 presents the factor loading values of anticipatory resilience items.
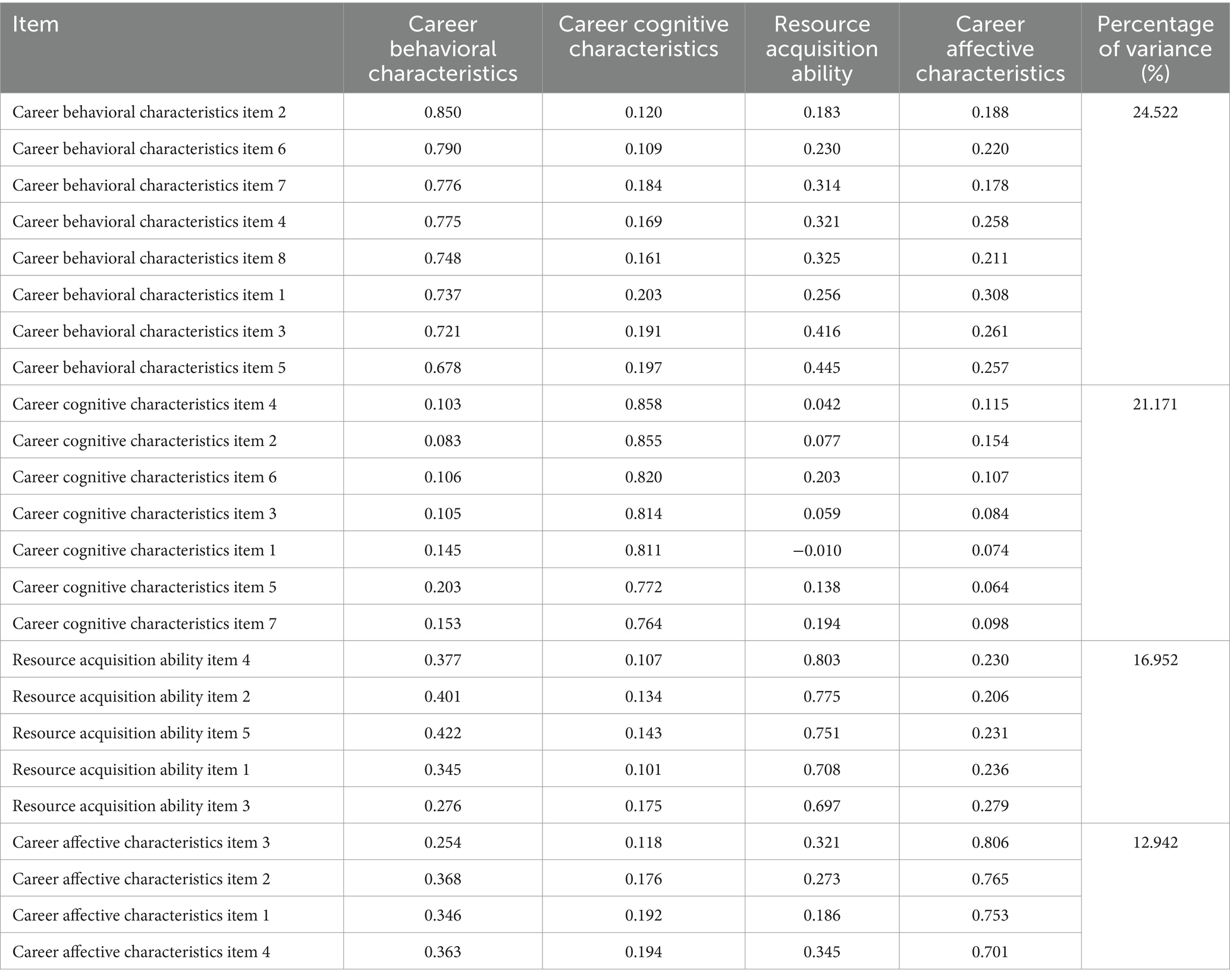
Table 7. Factor loading matrix of anticipatory resilience items.
Then, an exploratory factor analysis was conducted on the instrument of coping resilience, which needed to be normalized as the three items of the pre-set stress responses were set in reverse, and the results after processing showed that the KMO value was 0.907, with a p-value of less than 0.001, rendering it suitable for factor analysis. Four factors were extracted from the 20 items, which were in line with the pre-defined results, and named self-behavioral regulation (with eight items), self-affective regulation (with five items), self-cognitive regulation (with four items), and stress responses (with three items). The variance percentages of the four factors were 31.413, 21.567, 17.208, and 11.976%, respectively, and the factor loading values of the items corresponding to the four factors were 0.819 ~ 0.877, 0.795 ~ 0.902, 0.858 ~ 0.875, and 0.821 ~ 0.895,respectively.All the factor loading values were above 0.75, indicating good structural validity. Table 8 presents the factor loading values of coping resilience items.
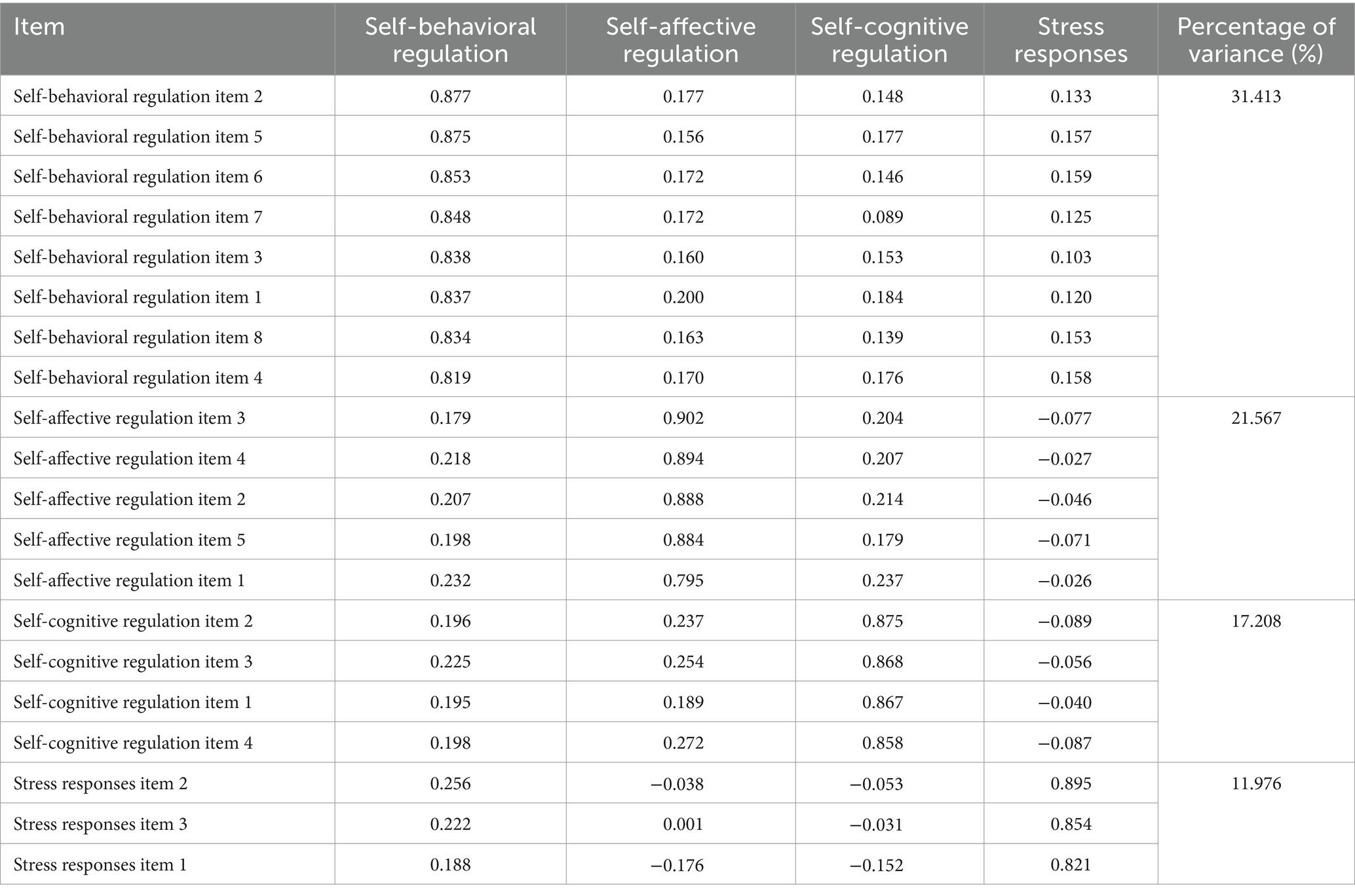
Table 8. Factor loading matrix of coping resilience items.
Finally, an exploratory factor analysis was conducted on the instrument of recovery resilience, and the results showed that the KMO value was 0.836, with a p-value of less than 0.001, rendering it suitable for factor analysis. Since only one factor was extracted, no further factor rotation was performed, which was in line with the pre-defined results, and named adaptive outcomes (with four items). The cumulative variance percentage of this single factor was 79.115%, and the factor loading values of each item ranged from 0.865 to 0.911. All the factor loading values were above 0.85, indicating good structural validity. Table 9 presents the factor loading values of recovery resilience items.
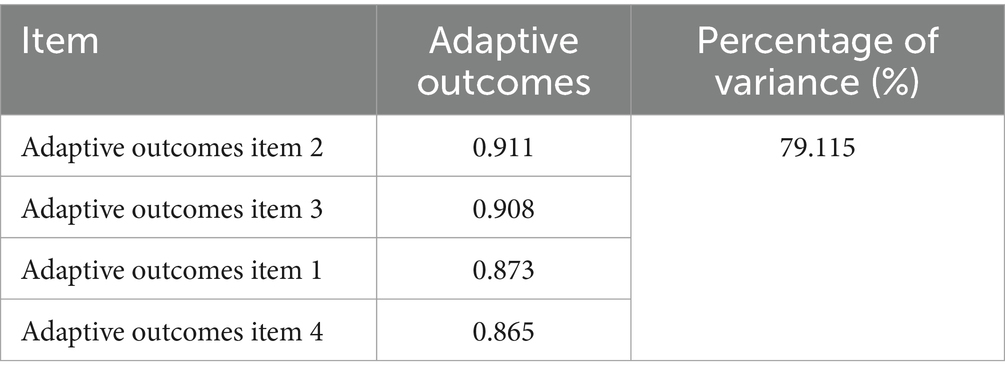
Table 9. Factor loading matrix of recovery resilience items.
4 Discussion
4.1 Summary of main findings
Career resilience is a means of helping CDC emergency responders to recover to normal functioning and performance after experiencing public health emergencies, especially major public health emergencies. A growing number of studies are pointing to the widespread impact of developing a validated career resilience assessment instrument, which can guide the design of resilience intervention strategies to fully exploit the effective functioning and optimal performance of resilience when experiencing an adverse event in the workplace (9, 30). Using the King and Rothstein (20) model as a theoretical guide, this study is the first to develop a career resilience instrument for CDC emergency responders in China within the context of public health emergencies from a process perspective and to conduct an initial validation of the developed instrument.
We first sampled 30 CDC emergency responders for face-to-face, in-depth, semi-structured interviews in three district-level CDCs in Shanghai. The interview texts were collated and analyzed using IPA, and 52 main comments, nine sub-themes, and three themes were eventually extracted, from which we constructed the initial career resilience instrument for CDC emergency responders. Secondly, we compiled the initial career resilience instrument into an expert consultation form and invited 24 experts to conduct two rounds of consultation. The expert positivity coefficients, expert authority coefficients, and expert coordination coefficients were all within the ideal value range, and revisions were proposed for 13 measurement items, while six measurement items were added. Further, we compiled the instrument revised by experts into a questionnaire and randomly sampled 1,286 CDC emergency responders in Shanghai, using the questionnaires they filled in for reliability and validity analyses. Additional, reliability and structural validity were examined using Cronbach’s α coefficient and exploratory factor analysis, respectively, which are widely used in the development and validation of instruments (9, 28). The results of this study showed that all the Cronbach’s α coefficients were above 0.85, and the factor loadings in exploratory factor analysis were above 0.65, and there were no double loadings, indicating good results for reliability and validity validation. In this study, the career resilience instrument for CDC emergency responders with three first-level measurement dimensions, 9 second-level measurement dimensions, and 48 measurement items was generated.
4.2 Theoretical implications
The theoretical implication of this study is guided by the King and Rothstein (20) model to develop the career resilience instrument for CDC emergency responders in China within the context of public health emergencies from a process perspective. Most previous studies developed instruments to measure career resilience from the trait and outcome perspectives. The trait perspective is a static and isolated way to assess career resilience, which tends to ignore the environmental or contextual factors of individuals’ recovery from adversity, and does not adequately consider the dynamic and developmental attributes of resilience (31, 32). The outcome perspective is a simple way to assess career resilience, and the outcomes achieved in different situational contexts and adverse events are also quite variable (31, 32). Therefore, considering the limitations of the trait and outcome perspectives, in this study, we developed the career resilience measurement instrument from a process perspective, describing protective individual characteristics, internal and external interactions and self-regulatory processes, and adaptive outcomes and employing a variable-centered approach to reveal the dynamic process of an individual’s breakdown from equilibrium to reintegration into equilibrium. In addition, career resilience in the healthcare field has mostly been studied with nurses, and primary healthcare professionals (28, 33–37), while basically, no studies are available regarding CDC emergency responders. This study introduces career resilience to the group of CDC emergency responders in hopes of focusing on the mental health and work status of this group, so that they can better respond to public health emergencies and protect public health.
4.3 Practical implications
Resilience is not an entirely innate and unchanging characteristic or trait, on the contrary, it stems from the normative functioning of the human adaptive system and is constituted by ordinary rather than specialized processes, meaning that it can be cultivated (38). This provides the possibility of intervening and cultivating career resilience and a more positive prospect for employees to adapt to various complex work situations. The following provides some practical implications around the exploration of this study.
Firstly, in terms of cognition, it is important to improve self-efficacy through the continuous upgrading of professional skills and actively perceive the value and meaning of work to enrich job satisfaction (39). These actions are conducive to the fact that CDC emergency responders can perceive the good side of an undesirable work environment, refrain from thinking nonsense, and make cognitive regulations in the event of an adverse event such as a public health emergency. Secondly, in terms of affection, health professionals involved in the response to emerging infectious disease outbreaks and major public health emergencies may often feel nervous, fearful, anxious, and powerless (40). This suggests that CDC emergency responders need to learn how to control their emotions and find ways to release their negative emotions, such as confiding in others and being physically active, which can help to regulate negative emotions during emergencies. It has been confirmed that emotional regulation is an unavoidable form of self-regulation when individuals are challenged, and it is used in combination with self-cognitive and self-behavioral regulations to maintain an internal equilibrium (41). Thirdly, in terms of behavior, CDC emergency responders need to acquire cutting-edge knowledge, constantly try new ways to solve problems, prioritize, and plan and schedule work well. One study noted that a sense of control over work schedules is a strong predictor of emotional resilience (42). These can help CDC emergency responders to make timely behavioral adjustments and carry out the actions required for emergencies.
Fourthly, it has been noted that good social networks, such as family support, affirmation from colleagues and leaders, and teamwork, are strongly associated with high levels of resilience (43, 44). This indicates that individuals should actively build a good social network and maintain a balance between interpersonal and work environments. Fifthly, CDC emergency responders should also actively learn to take stock of their work experience after an emergency response is completed. This can be achieved by reconceptualizing work and life, changing priorities, improving interpersonal relationships, enhancing professional competence, and learning ways in which to regulate and release emotions in order to increase resilience levels and respond to more challenges in the future (45).
5 Limitations and future research
Although this study has strengths, it still has some limitations. Firstly, the respondents for this study were from Shanghai and nationwide was not conducted, which somewhat interferes with the reliability and generalizability of this study. Therefore, there is a need to sample more areas of China in the future to further test the reliability and validity of this instrument, thereby accumulating more evidence regarding the validity and use of the developed career resilience instrument and determining its reliability and validity for a wider sample. In addition, the use this instrument to assess career resilience among CDC emergency responders in other countries will be attempted to expand its use if possible. Secondly, in this study, we only developed a career resilience instrument for CDC emergency responders and did not explore the antecedent and outcome variables of career resilience in depth. Therefore, future research is required to further explore the influencing factors and outcome effects of CDC emergency responders’ career resilience, which will also serve to further refine this career resilience instrument.
6 Conclusion
In this study, we attempted to develop the career resilience instrument for CDC emergency responders and initially validated its good reliability and validity. This study further opens up the application field of career resilience, and provides additional ways and support for assessing career resilience. This study also shows that career resilience can be regarded as a set of protective factors and dynamic processes that can be acquired through the cultivation of individual characteristics and self-regulation in cognitive, affective, and behavioral dimensions, enabling effective responses to and recovery from adverse events in the workplace.
Data availability statement
The original data presented in this study has been included in the article, further inquiries can be directed to the corresponding authors on reasonable request.
Author contributions
A-QW: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Validation, Writing – original draft, Writing – review & editing. W-DC: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft. Y-YF: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Writing – original draft. Y-SL: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft. JL: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft. H-YW: Conceptualization, Funding acquisition, Project administration, Resources, Supervision, Validation, Visualization, Writing – review & editing. C-LJ: Conceptualization, Funding acquisition, Project administration, Resources, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by Natural Science Foundation of Shanghai 2021 “Science and Technology Innovation Action Plan” (grant number: 21ZR1458800) and the Graduate Student Research Grant from Weifang Medical University.
Acknowledgments
We owe a special debt of gratitude to all the professors and editors in Frontiers in Public Health, whose hard work benefited us a lot and academically reviewed the paper.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1327738/full#supplementary-material
References
1. Hao, JJ, Ren, JJ, Wu, QH, Hao, Y, Sun, H, Ning, N, et al. Identifying factors associated with risk assessment competencies of public health emergency responders. Int J Environ Res Public Health. (2017) 14:597. doi: 10.3390/ijerph14060597
2. Tong, MXL, Hansen, A, Hanson-Easey, S, Xiang, J, Cameron, S, Liu, Q, et al. Public health professionals' perceptions of the capacity of China's CDCs to address emerging and re-emerging infectious diseases. J Public Health. (2021) 43:209–16. doi: 10.1093/pubmed/fdz070
3. Jiao, ML, Ning, N, Wu, QH, Peters, DH, Hao, Y, Li, Y, et al. Determinants of emergency response responsibility perceptions in the local public health workforce after China's health sector restructuring. BMC Health Serv Res. (2015) 15:339. doi: 10.1186/s12913-015-1003-0
4. Ding, F, Li, Q, and Jin, LM. Experience and practice of the emergency operations center, Chinese Center for Disease Control and Prevention: a case study of response to the H7N9 outbreak. Infect Dis Poverty. (2021) 10:4. doi: 10.1186/s40249-020-00789-x
5. Ren, JJ, Wu, QH, Hao, YH, Ferrier, A, Sun, H, Ding, D, et al. Identifying weaknesses in national health emergency response skills and techniques with emergency responders: a cross-sectional study from China. Am J Infect Control. (2017) 45:e1–6. doi: 10.1016/j.ajic.2016.10.001
6. Ma, JY. Analysis of the current situation of job satisfaction and influence factors among health emergency workers in disease prevention and control institutions in Jilin province. Changchun: Jilin University (2022).
7. Klomp, RW, Jones, L, Watanabe, E, and Thompson, WW. CDC's multiple approaches to safeguard the health, safety, and resilience of Ebola responders. Prehosp Disaster Med. (2020) 35:69–75. doi: 10.1017/S1049023X19005144
8. Shan, Y, Liu, GW, Zhou, CQ, and Li, S. The relationship between CDC personnel subjective socioeconomic status and turnover intention: a combined model of moderation and mediation. Front Psych. (2022) 13:908844. doi: 10.3389/fpsyt.2022.908844
9. McLarnon, MJW, and Rothstein, MG. Development and initial validation of the workplace resilience inventory. J Pers Psychol. (2013) 12:63–73. doi: 10.1027/1866-5888/a000084
10. Zhang, H. Research on the occupational resilience of community social workers from the perspective of life course theory. Chongqing: Southwest Unversity (2022).
11. Luthans, F, Avey, JB, Avolio, BJ, and Peterson, SJ. The development and resulting performance impact of positive psychological capital. Hum Resour Dev Q. (2010) 21:41–67. doi: 10.1002/hrdq.20034
12. LUTHANS, F, AVOLIO, BJ, AVEY, JB, and NORMAN, SM. Positive psychological capital: measurement and relationship with performance and satisfaction. Pers Psychol. (2007) 60:541–72. doi: 10.1111/j.1744-6570.2007.00083.x
13. Ashby, SE, Ryan, S, Gray, M, and James, C. Factors that influence the professional resilience of occupational therapists in mental health practice. Aust Occup Ther J. (2013) 60:110–9. doi: 10.1111/1440-1630.12012
14. Brown, T. The response to COVID-19: occupational resilience and the resilience of daily occupations in action. Aust Occup Ther J. (2021) 68:103–5. doi: 10.1111/1440-1630.12721
15. Cai, Z, Mao, Y, Gong, T, Xin, Y, and Lou, J. The effect of servant leadership on work resilience: evidence from the hospitality industry during the COVID-19 period. Int J Environ Res Public Health. (2023) 20:1322. doi: 10.3390/ijerph20021322
16. Greifer, AN. Occupational resilience: protective factors among clinical social workers. Lansing: Michigan State University (2004).
17. Hively, JD. Resilience among school psychologists: applying positive psychology to burnout prevention. Fresno: California State University (2003).
18. Delgado, C, Roche, M, Fethney, J, and Foster, K. Workplace resilience and emotional labour of Australian mental health nurses: results of a national survey. Int J Ment Health Nurs. (2020) 29:35–46. doi: 10.1111/inm.12598
19. Mishra, P, and McDonald, K. Career resilience: an integrated review of the empirical literature. Hum Resour Dev Rev. (2017) 16:207–34. doi: 10.1177/1534484317719622
20. King, GA, and Rothstein, MG. Resilience and leadership: the self-management of failure In: MG Rothstein and RG Burke, editors. Self-management and leadership development. Camberley: Edward Elgar Publishing (2010). 361–94.
21. King, GA, Brown, EG, and Smith, LK. Resilience: learning from people with disabilities and the turning points in their lives. Westport, CT: Praeger (2003).
22. Tuffour, I. A critical overview of interpretative phenomenological analysis: a contemporary qualitative research approach. J Healthc Commun. (2017) 2:52. doi: 10.4172/2472-1654.100093
23. Larkin, M, Watts, S, and Clifton, E. Giving voice and making sense in interpretative phenomenological analysis. Qual Res Psychol. (2006) 3:102–20. doi: 10.1191/1478088706qp062oa
24. Smith, JA, Flowers, P, and Larkin, M. Interpretative phenomenological analysis: theory, method, and research. London: SAGE (2009).
25. Zhu, XP. Construction of credit evaluation index system for non-public medical institutions. Beijing: Beijing University of Chinese Medicine (2018).
26. Ge, JL, Geng, SS, Chen, X, et al. Development of the general practitioner management of age-related hearing loss system. Chin. Gen. Pract. (2022) 25:4318–25. doi: 10.12114/j.issn.1007-9572.2022.0310
27. Yin, XY, Hao, CB, Zhu, Y, et al. Development of index system for assessing parent's ability on child injury prevention by Delphi consultation. Chin J School Health. (2022) 43:1086–9. doi: 10.16835/j.cnki.1000-9817.2022.07.030
28. Norouzinia, R, Yarmohammadian, MH, Ferdosi, M, Masoumi, G, and Ebadi, A. Development and psychometric evaluation of the emergency nurses' professional resilience tool. PLoS One. (2022) 17:e269539. doi: 10.1371/journal.pone.0269539
29. Duchek, S. Organizational resilience: a capability-based conceptualization. Bus Res. (2020) 13:215–46. doi: 10.1007/s40685-019-0085-7
30. Yousself, CM, and Luthans, F. Positive organizational behavior in the workplace: the impact of hope, optimism, and resilience. J Manag. (2007) 33:774–800. doi: 10.1177/0149206307305562
31. Li, X. A study on manager's career resilience: construct and relationship with its antecedents and outcomes. Tianjin: Nankai University (2010).
32. Zhang, WL. Study on the career resilience of college counsellors. Xi'an: Shaanxi Normal University (2016).
33. Aqtam, I, Ayed, A, Toqan, D, Salameh, B, Abd Elhay, ES, Zaben, K, et al. The relationship between stress and resilience of nurses in intensive care units during the COVID-19 pandemic. Inquiry. (2023) 60:1–8. doi: 10.1177/00469580231179876
34. Eley, E, Jackson, B, Burton, C, and Walton, E. Professional resilience in GPs working in areas of socioeconomic deprivation: a qualitative study in primary care. Br J Gen Pract. (2018) 68:e819–25. doi: 10.3399/bjgp18X699401
35. Foster, K, Roche, M, Giandinoto, JA, and Furness, T. Workplace stressors, psychological well-being, resilience, and caring behaviours of mental health nurses: a descriptive correlational study. Int J Ment Health Nurs. (2020) 29:56–68. doi: 10.1111/inm.12610
36. Robertson, HD, Elliott, AM, Burton, C, Iversen, L, Murchie, P, Porteous, T, et al. Resilience of primary healthcare professionals: a systematic review. Br J Gen Pract. (2016) 66:e423–33. doi: 10.3399/bjgp16X685261
37. Wang, AQ, Tang, CH, Song, J, Fan, CX, Wang, WC, Chen, ZM, et al. Association of individual resilience with organizational resilience, perceived social support, and job performance among healthcare professionals in township health centers of China during the COVID-19 pandemic. Front Psychol. (2022) 13:1061851. doi: 10.3389/fpsyg.2022.1061851
38. Masten, AS. Ordinary magic: resilience processes in development. Am Psychol. (2001) 56:227–38. doi: 10.1037//0003-066x.56.3.227
39. Hosseini, M, Ghasemi, S, and Hejazi, S. Exploring the impacts of caring for hospitalized COVID-19 patients on nurses: a qualitative descriptive study. Iran J Nurs Midwifery Res. (2023) 28:160–6. doi: 10.4103/ijnmr.ijnmr_49_22
40. Marcolongo, F, Ottaviani, M, Romano, P, Bonassi, S, Garramone, A, Infarinato, F, et al. The role of resilience and coping among Italian healthcare workers during the COVID-19 pandemic. Med Lav. (2021) 112:496–505. doi: 10.23749/mdl.v112i6.12285
41. Delgado, C, Evans, A, Roche, M, and Foster, K. Mental health nurses' resilience in the context of emotional labour: an interpretive qualitative study. Int J Ment Health Nurs. (2022) 31:1260–75. doi: 10.1111/inm.13037
42. Matheson, C, Robertson, HD, Elliott, AM, Iversen, L, and Murchie, P. Resilience of primary healthcare professionals working in challenging environments: a focus group study. Br J Gen Pract. (2016) 66:e507–15. doi: 10.3399/bjgp16X685285
43. Connelly, DM, Garnett, A, Snobelen, N, Guitar, N, Flores-Sandoval, C, Sinha, S, et al. Resilience amongst Ontario registered practical nurses in long-term care homes during COVID-19: a grounded theory study. J Adv Nurs. (2022) 78:4221–35. doi: 10.1111/jan.15453
44. Nasaif, H, Aldiabat, K, Alshammari, M, Albloushi, M, Alblooshi, SM, and Yaqoob, S. The lived experiences of nurses caring for patients with COVID-19 in Arabian gulf countries: a multisite descriptive phenomenological study. Glob Qual Nurs Res. (2023) 10:1682244972. doi: 10.1177/23333936231155052
Keywords: career resilience, emergency responders, center for disease control and prevention, public health emergency, measurement instrument
Citation: Wang A-Q, Cheng W-D, Fu Y-Y, Luo Y-S, Li J, Wang H-Y and Jin C-L (2024) Development and initial validation of the career resilience instrument for CDC emergency responders in China within the context of public health emergencies: based on a survey conducted in Shanghai. Front. Public Health. 12:1327738. doi: 10.3389/fpubh.2024.1327738
Edited by:
Biagio Solarino, University of Bari Aldo Moro, ItalyReviewed by:
Gul Muhammad Baloch, Keele University, United KingdomMuhammad Waseem, Lincoln Medical Center, United States
Copyright © 2024 Wang, Cheng, Fu, Luo, Li, Wang and Jin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hai-Yin Wang, d2FuZ2hhaXlpbkBzaGRyYy5vcmc=; Chun-Lin Jin, amluY2h1bmxpbkBzaGRyYy5vcmc=
†These authors have contributed equally to this work