 Bashayer Ebraheem Al-Wagdi1,2
Bashayer Ebraheem Al-Wagdi1,2 Mohammed Khaled Al-Hanawi1,3*†
Mohammed Khaled Al-Hanawi1,3*†- 1Department of Health Services and Hospital Administration, Faculty of Economics and Administration, King Abdulaziz University, Jeddah, Saudi Arabia
- 2Physical Therapy Department, Ahad Rafidah General Hospital, Abha, Saudi Arabia
- 3Health Economics Research Group, King Abdulaziz University, Jeddah, Saudi Arabia
Background: The increasing adoption of sedentary lifestyles and cultural shifts has fostered unhealthy habits and decreased physical activity, consequently exacerbating the prevalence of diabetes. Diabetes is currently one of the top 10 diseases worldwide, contributing significantly to both mortality and morbidity. Since diabetes hinges on self-care, possessing the right knowledge, attitude, and habits related to the disease is paramount. This study, therefore, aims to examine the knowledge, attitude, and practice of diabetes among the population of Saudi Arabia.
Methods: The study utilized data from a cross-sectional study conducted via an online self-reported questionnaire among the general population of Saudi Arabia. The study primarily used univariate and multivariable regression data analyses. Univariate analysis was employed to compile social and demographic statistics frequencies, while One-way analysis of variance (ANOVA) was used to assess mean differences in knowledge, attitudes, and practices scores. Furthermore, a multivariable linear regression analysis was executed to identify factors associated with knowledge, attitudes, and practices.
Results: The mean score for diabetes knowledge was 17.79 (SD = 5.39, range: 0–29), with an overall accuracy rate of 61.34%. The mean attitude score for diabetes was 2.33 (SD = 1.91, range: 0–7), while the mean score for diabetes practices was 2.58 (SD = 1.28, range: 0–4). The multivariate analyses reveal distinct variations in knowledge, attitudes, and practices of diabetes among participants based on their gender, education, marital status, income, diabetes patient status, and having a medical field-related education.
Conclusion: High knowledge scores do not necessarily equate to positive attitudes and practices related to diabetes. There is need for intensified care and the implementation of specialized educational programs that emphasize the importance of having the right attitude and engaging in the good diabetes practices.
Introduction
Over the years, the prominence of non-communicable diseases (NCDs) has remained a global concern. These diseases represent chronic illnesses that are characterized by their non-infectious and non-contagious nature, encompassing health conditions such as cardiovascular diseases, various forms of cancer, diabetes, and chronic respiratory diseases (1, 2). Demographic, economic, and environmental shifts, along with the COVID-19 pandemic, have exacerbated the prevalence of NCDs. COVID-19 has notably increased the susceptibility of individuals with NCDs to severe illness and mortality (3). In 2019, NCDs accounted for approximately 74% of the total global mortality, amounting to an estimated 40 million deaths (3). This highlights the global need for strategies in healthcare management aimed at reducing the prevalence of NCDs.
Diabetes is among the NCDs increasingly presenting challenges to countries, regardless of their developmental stage (4). Constituting a chronic metabolic disorder characterized by insufficient insulin production or the body’s ineffective use of insulin, diabetes ranks among the top 10 diseases contributing to mortality and morbidity (5, 6). An estimated 5 million deaths in the global population aged 20–79 were linked to diabetes in 2015 (7). The high mortality rates can be ascribed to the numerous complications associated with diabetes, including brain diseases, renal failure, vision impairment, cardiovascular problems, and limb amputations (8). This is exacerbated by the growing trend toward sedentary lifestyles and cultural shifts, which have introduced unhealthy habits and reduced physical activity (9, 10). Prioritizing the mitigation of risk factors is crucial in addressing the prevalence of diabetes.
Existing literature shows high diabetes prevalence among older individuals and those with lower education, whereas it is more common among individuals with higher incomes. The aging process reduces physical activity and weakens the immune system, thereby presenting healthcare access challenges and increasing the disease burden among the older adult (11, 12). Hence, diabetes prevalence differs among age groups, with the older adult experiencing a greater risk in contrast to younger individuals. In terms of education, individuals with lower levels of education may encounter increased exposure to risk factors and greater susceptibility to diabetes in comparison to those with higher levels of education (13–15). Education plays a vital role in raising awareness, but individuals with lower levels of education tend to have limited access to information (16, 17). Nonetheless, owing to sedentary lifestyles, numerous studies suggest a higher prevalence of diabetes among individuals with higher income levels (18, 19).
Despite specific socio-economic traits exhibiting higher prevalence, diabetes remains a burgeoning global public health challenge, profoundly affecting the population’s quality of life and well-being. The diabetic patient population is projected to exceed 700 million by 2045 (20). These statistics underscore the mounting pressure that the healthcare system will confront, leading to escalated healthcare costs, including both out-of-pocket expenses and insurance expenditures (21–23). Urgent action is required to implement strategies that can effectively address the prevalence, treatment, and management of diabetes. Since misconceptions about NCDs such as diabetes can increase the risk of complications, a sound understanding of the disease is essential for effective management. Insufficient knowledge, attitude, and practice regarding diabetes frequently correlate with unfavorable health outcomes (24). Patients well-informed about diabetes and its complications are more likely to seek appropriate treatment and healthcare (25).
A diagnostic tool employed to assess participants’ understanding, attitudes, and behaviors related to a specific phenomenon is referred to as a knowledge, attitude, and practice (KAP) study (26). It explores behaviors and practices by gathering data on what is understood, believed, and enacted in connection to a specific subject (27). KAP studies on diabetes delineate patient characteristics and the factors influencing their diabetes-related knowledge, attitudes, and practices (28). They uncover misconceptions about diabetes within the population that could impede preventive and curative programs as well as behavioral changes (27). Apart from serving as effective baselines for intervention programs, KAP studies inform the development of effective health education programs and techniques.
While KAP studies on diabetes have been conducted, additional research is essential, as inadequate KAP studies could heighten the risk of inadequate guidance and flawed intervention programs. This is especially needed for the Kingdom of Saudi Arabia (KSA), given its overburden healthcare system and a high prevalence of NCDs (29–31). The country ranks second in the Middle East and seventh worldwide in terms of diabetes prevalence (32). The lifestyle changes accompanying development have accentuated a higher incidence of obesity and increased susceptibility to diabetes in the country. Despite the severity of the situation, the majority of diabetes KAP studies have focused on either diabetes patients, specific regions or urban areas, or particular population subgroups. Findings from such studies may not consistently reflect the broader public accurately. This study seeks to contribute to the existing diabetes KAP literature by utilizing cross-sectional data collected from the general population of Saudi Arabia through self-reported questionnaires. By employing both univariate and multivariate regression data analyses, the study seeks to assess the level of diabetes KAP and how it varies across socio-demographic factors in Saudi Arabia. It is one of the few studies that offer a comprehensive examination, encompassing estimates from the general population, individuals with medical knowledge, and diabetes patients, while exploring variations across social and demographic factors.
Methodology
Study design and sample
This cross-sectional study was carried out targeting the general population of Saudi Arabia covering all administrative regions in the country, from 25 July 2023 to 5 September 2023. Data were collected online, via a self-reported questionnaire, using SurveyMonkey. Taking into account the widespread internet, and social media usage among individuals in Saudi Arabia (33), a link to the survey was shared with respondents through Twitter and WhatsApp groups. Participants were also requested to pass the link to their contact and ask them to participate in the study.
The study aimed to maximize reach and gather data from a wide range of respondents, as larger the target sample size, the higher the external validity and the greater the generalizability of the study (34). According to the most recent KSA census, the population of Saudi Arabia is 32,175,224 (35). To achieve the study’s objectives and ensure sufficient statistical power, a representative target sample size was calculated using a sample size calculator (36). The calculator determined that 385 participants would be needed, considering a margin of error of ±5%, a confidence level of 95%, a response distribution of 50%, and a population size of 32,175,224 individuals.
Study instrument
The study used a validated questionnaire related to knowledge, attitudes, and practices regarding diabetes (37). The author B.A. translated the questionnaire from English to Arabic, then translated back to English by M.K.A to ensure the meaning of the content. The Arabic version of the questionnaire was used to collect the data.
Prior to proceeding with the online questionnaire, participants were presented with a clear explanation of the study’s purpose on the first page. They were explicitly notified that they had the freedom to withdraw from the study at any point without providing a reason. Additionally, participants were assured that all the information and opinions they provided would be treated as anonymous and kept confidential. To be eligible for participation, individuals had to be residents of Saudi Arabia, aged 18 years or older, understand the questionnaire’s content, and willingly agree to take part in the study. They were also required to have a proper understanding of the questionnaire’s content and. Online informed consent was obtained from participants before they were able to proceed with the questionnaire.
The questionnaire consisted of four primary sections. The first section gathered general information and information on respondents’ sociodemographic characteristics, including gender, age, marital status, education level, education related to medical, whether participants suffer from a diabetes, work status, and monthly income level. The second section assessed participants’ knowledge of diabetes. This section included items on risk factors, diagnosis, prevention, and complications of diabetes. The third section assessed participants’ attitudes toward diabetes using seven questions related to adherence to treatment of diabetes. The final section of the questionnaire assessed the respondents’ practices. This section consisted of four questions related practices related to diabetes.
Dependent variables
To measure knowledge about diabetes, participants were presented with a series of knowledge items and asked to provide their responses. Incorrect or uncertain answers (marked as “do not know”) were assigned a score of zero, while correct responses were given a score of one. The total knowledge score ranged from zero to 29, with higher scores indicating a greater knowledge of diabetes. The internal reliability of the knowledge items was assessed using Cronbach’s α coefficient, which yielded a value of 0.84. This indicates a high level of internal reliability (38).
Attitudes were measured by calculating scores based on respondents’ answers to each attitudinal question. The total attitude scores ranged from zero to 7, with higher scores indicating more positive attitudes. The internal reliability of the attitudinal items was assessed using Cronbach’s α coefficient, which yielded a value of 0.76. This indicates a satisfactory level of internal reliability.
In the section on practices, respondents were asked to indicate “yes” or “no” in response to the items. A score of one was assigned to answers that reflected good practices, while a score of zero was assigned to answers that indicated otherwise. The total practice score ranged from zero to 4, with higher scores indicating positive practices.
Independent variables
General information, socioeconomic and demographic characteristics including gender, age, marital status, education level, education related to medical, whether participants suffer from a diabetes, work status, and monthly income were used as independent variables. Gender was coded as a binary variable, where it takes the value of 1 if the respondent is men and 0 if women. The age variable was categorized into two groups: ≤40 years old (reference category), and ≥ 40 years old as an age of ≥40 is considered to be the typical age for the onset of diabetes (39). Marital status was recorded as a binary variable, with a value of one indicating marriage and zero indicating any other status. Education was divided into three categories: high school or below (reference category), college/university degree, and postgraduate degree. Education related to medical field where it takes the value of 1 if respondent has education related to medical field and 0 if not. Suffering from diabetes takes the takes the value of 1 if yes and 0 if not. Work status was broken down into unemployed (reference category), government employee, non-government employee, self-employed, students, and retiree. Monthly income, denominated in Saudi Riyal (SR) with an exchange rate of USD 1 = SR 3.75, was grouped into four categories: less than SR 7,000 (reference category), SR 7,000 to less than SR 10,000, SR 10,000 to less than SR 15,000, and SR 15,000 or more.
Analysis methods
The data analysis in this study consisted primarily of univariate and multivariable regression analyses. Univariate analysis was employed to summarize the frequency distribution of social and demographic variables. To assess differences in mean values for knowledge, attitudes, and practice scores, one-way analysis of variance (ANOVA) was utilized.
Furthermore, a multivariable linear regression analysis was conducted to identify factors associated with knowledge, attitudes, and practice. This analysis aimed to determine the relationships between these variables and other relevant factors. STATA software (StataCorp LP, Texas, USA) was used to perform all the data analyses in this study.
Ethical considerations
All procedures performed in this study, involving human participants, complied with the institutional and/or national research committee ethical standards, and the 1964 Helsinki declaration and subsequent amendments or equivalent ethical standards. This study has been reviewed and approved by the King Abdulaziz University Research Ethics Committee and was designed and performed in accordance with the ethical principles established by the university. Therefore, ethical approval was obtained from the Biomedical Ethics Research Committee, Faculty of Medicine, King Abdulaziz University (Ref-270-23). Online informed consent to participate was secured from all respondents who participated in the study. The data collection procedure was anonymous and as such no personal identifying information was collected.
Results
Social and demographic characteristics
A total of 646 participants completed the questionnaire. After excluding 29 respondents who did not provide complete answers for all the variables of interest, the final sample comprised 617 participants. The sociodemographic characteristics of the study participants are detailed in Table 1. The table shows that the mean diabetes knowledge score stood at 17.79 (SD = 5.39, ranging from 0 to 29), with an overall accuracy rate of 61.34% (calculated as 17.79 out of 29, multiplied by 100). Additionally, the mean attitude score regarding diabetes was 2.33 (SD = 1.91, ranging from 0 to 7), while the mean score for diabetes-related practices averaged at 2.58 (SD = 1.28, ranging from 0 to 4).
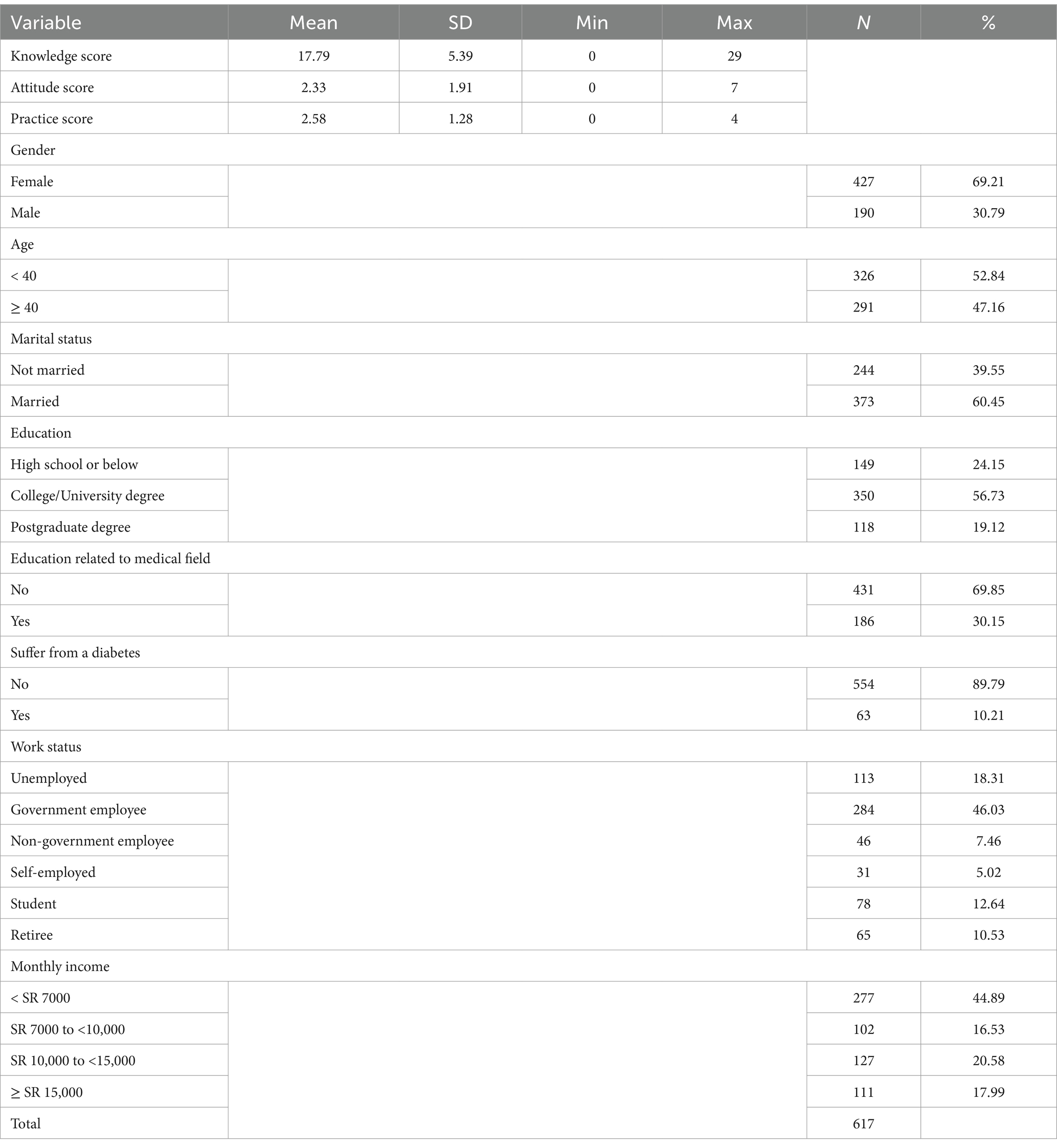
Table 1. Social and demographic characteristics of the study participants.
Table 1 provides a comprehensive summary of the social and demographic characteristics of the study participants where the majority of the sample consisted of women (69.21%), married (60.45%), and did not have diabetes (89.79%). More than half of the participants (52.84%) were below 40 years of age, and the majority (56.73%) held a college or university degree. Respondents were categorized based on their monthly income, with 277 (44.89%) falling into the group earning less than SR 7,000, and 111 (17.99%) belonging to the group earning SR 15,000 or more. In terms of employment status, 113 (18.31%) were unemployed, and 65 (10.53%) were retired.
Tables 2–4 offer an overview of the responses related to KAP regarding diabetes. Table 2 provides a comprehensive breakdown of participants’ knowledge about specific diabetes-related topics and their understanding of how these issues operate and relate to the disease. In contrast, Table 3 outlines the attitudes held by participants toward diabetes, and Table 4 consolidates the practices in which participants engage concerning diabetes.

Table 2. Responses to the questionnaire on diabetes knowledge.
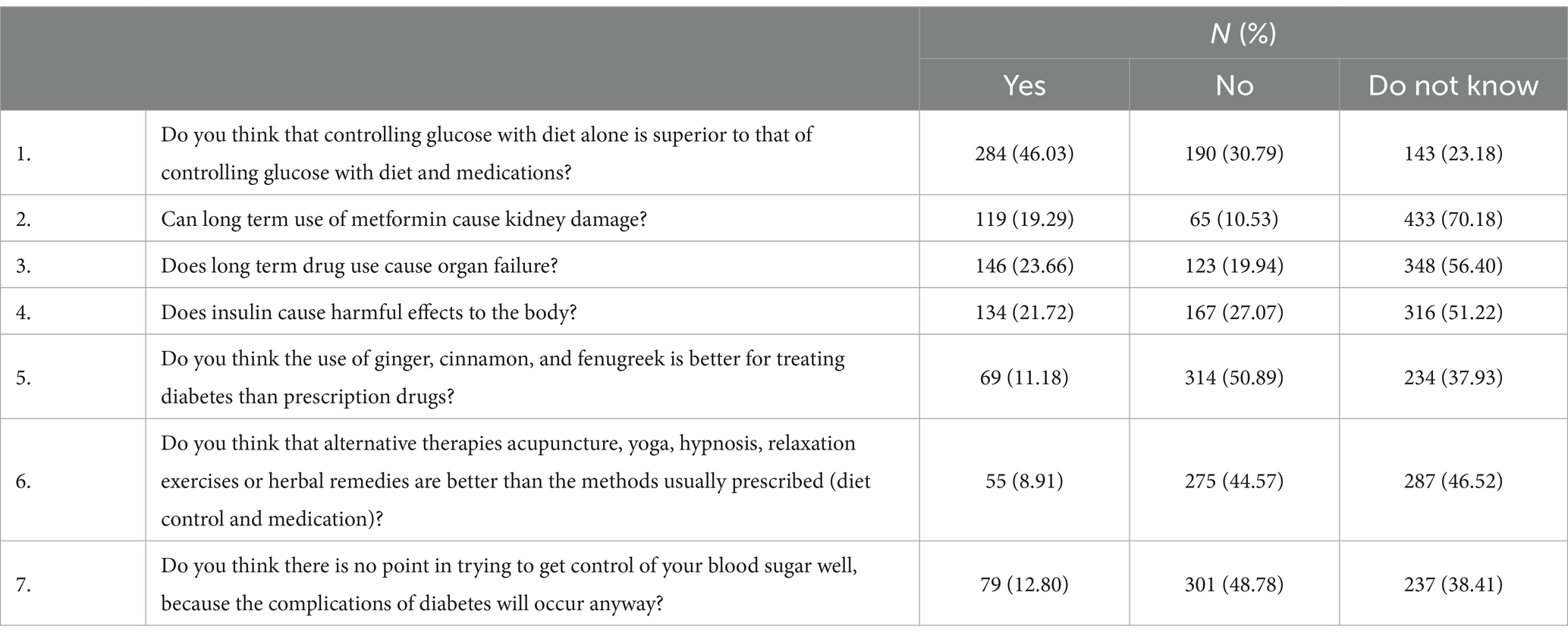
Table 3. Response to attitudinal questions regarding diabetes.

Table 4. Practices related to diabetes.
Table 2 provides an overview of the responses pertaining to diabetes knowledge. It highlights the areas where much of the sample demonstrates a strong understanding of diabetes-related concepts and those areas where knowledge appears to be lacking. For instance, 67.26% of respondents exhibit a clear understanding of the dynamics of blood sugar in diabetes, while 32.74% lack this knowledge. In contrast, 63.21% of participants are uncertain about whether diabetes can be cured through treatment with only 36.79% of participants giving the correct responses. In terms of diabetes mellitus risk factors, a significant portion of the sample possesses knowledge about the association between risk factors such as a family history of diabetes (83.31%), being overweight or obese (85.41%), and excessive sugar consumption (84.76%). However, it’s worth noting that a considerable number of respondents are unaware that a sedentary lifestyle (38.74%) and stress (28.53%) can also contribute to the risk of diabetes.
Furthermore, Table 2 reveals some key insights. Notably, 87.52% acknowledge the effectiveness of insulin injections in controlling blood sugar levels, but a mere 37.76% are informed about the potential blood sugar-regulating properties of herbs, ginger, and cinnamon. Moreover, 54.94% of the participants are unaware that diabetes can lead to complications such as heart attack, and 43.76% lack knowledge about the connection between diabetes and kidney failure. However, the majority of participants (87.84%) understand the link between a dysfunctional pancreas and the development of diabetes. The table highlights specific areas where educational programs concerning diabetes could concentrate their efforts to enhance knowledge as a part of the broader process aimed at reducing the prevalence of diabetes mellitus.
Table 3 presents responses to questions that shed light on the attitudes of the participants toward diabetes. The majority of participants expressed uncertainty regarding whether long-term use of metformin might result in kidney damage (70.18%) and whether extended drug use could potentially lead to organ failure (56.40%). Additionally, 51.22% were unsure about whether insulin could have detrimental effects on the body. The percentage of “do not know” responses in Table 3 outweighs both the positive and negative responses in most the questions, suggesting that participants do not hold strong attitudes or opinions on these specific issues.
Table 4 provides insights into the practices related to diabetes among the participants. A substantial proportion of the sample (84.44%) express their willingness to consider treatment if they or a family member were diagnosed with diabetes, while only 15.56% indicate that they would not consider it. Additionally, a significant percentage (60.29%) engage in daily physical activities, such as brisk walking, house chores, or stair climbing for 30–60 min, although a notable portion (39.71%) do not partake in such activities. When it comes to regular blood sugar monitoring, only 48.14% of participants do so (at least annually), while the majority (51.86%) do not. On a positive note, a significant percentage (64.83%) try to avoid refined sugar and sugary foods, which is commendable.
Differences in knowledge, attitudes, and practices toward diabetes
After examining the univariate statistics for each variable of interest, the study proceeded to further evaluate the disparities in the scores pertaining to KAP. The outcomes of this assessment are presented in Table 5.
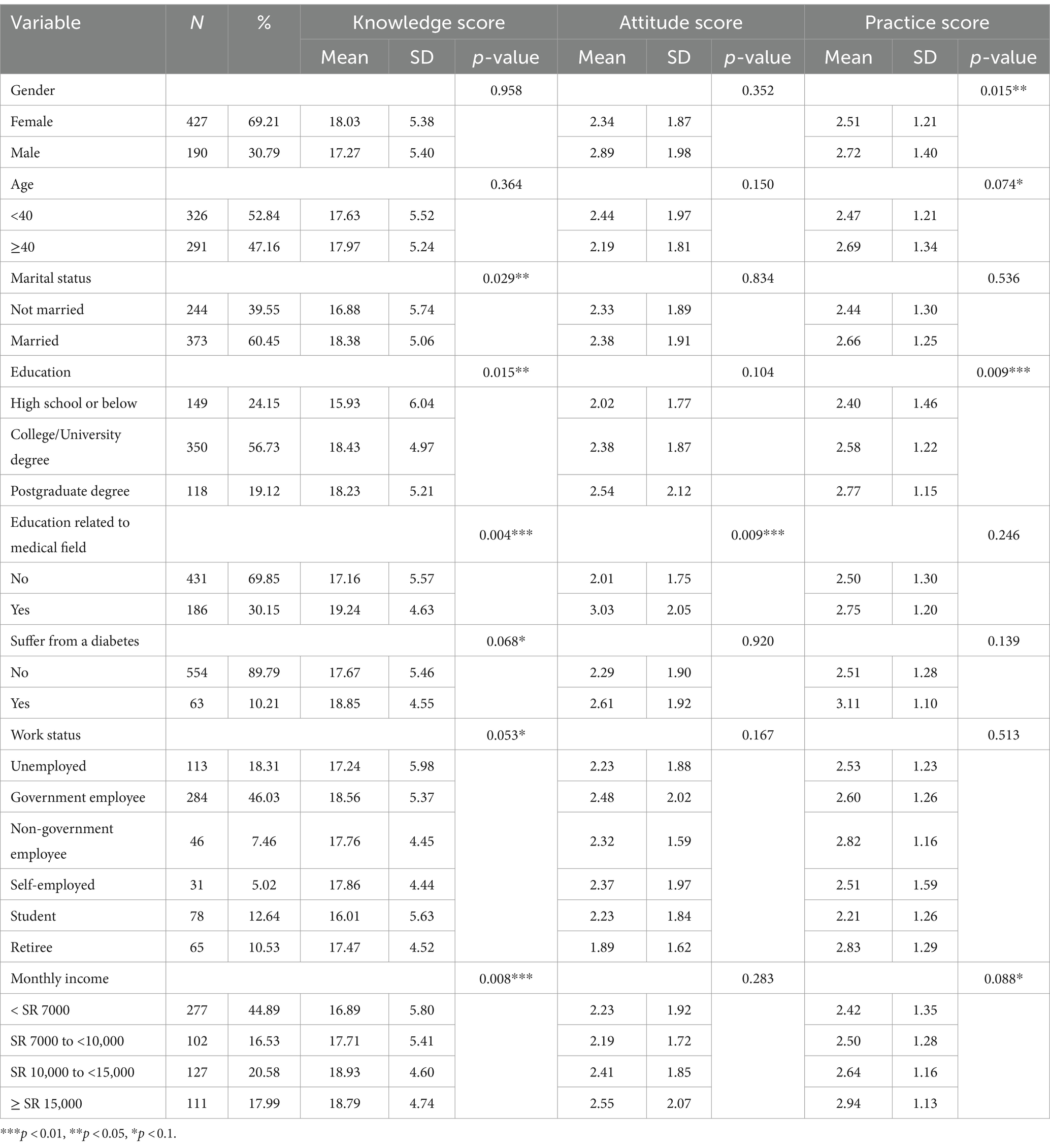
Table 5. Comparison of social and demographic characteristics, and mean diabetes score.
Table 5 shows that, except for gender and age, knowledge scores exhibit statistically significant differences across all other variables. For example, significant disparities exist in the mean knowledge scores concerning marital status (p < 0.05), educational background (p < 0.05), education related to the medical field (p < 0.01), diabetes diagnosis (p < 0.1), work status (p < 0.1), and monthly income (p < 0.01). These disparities point to variations in diabetes-related knowledge among various demographic characteristics. However, the variations in knowledge scores do not correspond to differences in attitude toward diabetes, as indicated by the lack of statistical significance between attitude scores and most socio-demographic variables, except for those with an educational background related to the medical field (p < 0.01). A similar pattern emerges when considering diabetes-related practices, with significant differences being evident across gender (p < 0.05), age (p < 0.1), educational background (p < 0.01), and income (p < 0.1). These findings are further examined using regression analysis.
Econometric results
In addition to the univariate and non-parametric analyses presented in earlier sections, the study also conducted regression analysis to further examine the KAP scores across several socio-demographic factors. Table 6 presents the results were higher scores indicate greater levels of knowledge, practices, and attitudes.
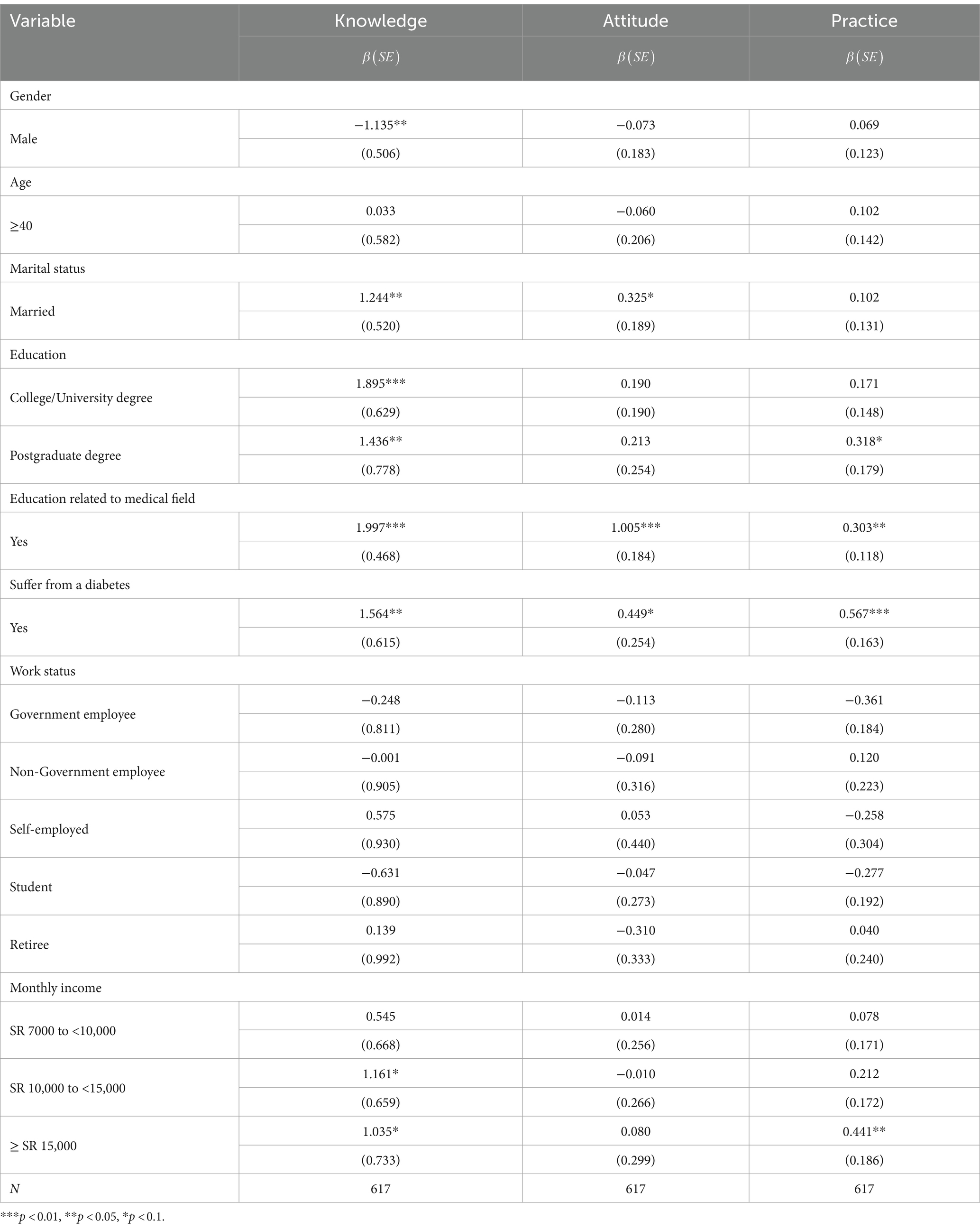
Table 6. Regression results of KAP-related factors for diabetes.
The results reveal variations in the levels of knowledge, attitudes, and practices among the population of the KSA, with certain socio-demographic variables showing significant associations, while others exhibit no significant impact. Table 6 demonstrates that there is no statistically significant difference in the levels of knowledge, attitudes, and practices related to diabetes when considering age and work status. This suggests that in matters concerning diabetes related KAP in Saudi Arabia, age, occupational status whether government, non-government, self-employed, student status, or retirement status have minimal bearing. However, Table 6 highlights significant differences in knowledge scores based on gender, marital status, educational background, medical field-related education, diabetes diagnosis, and income.
The findings indicate that males exhibit lower levels of knowledge (β = −1.135; p < 0.05) compared to females, while married individuals demonstrate higher levels of knowledge (β = 1.244; p < 0.05) in comparison to those who are unmarried. Likewise, Table 6 illustrates that possessing a college or university degree is linked to higher knowledge scores (β = 1.895; p < 0.01), in a similar manner, to having a postgraduate degree (β = 1.436; p < 0.05). Similarly, the pattern holds true for individuals with an education linked to a medical field and those experiencing diabetes. Those with a medical field-related education exhibit significantly higher levels of knowledge (β = 1.997; p < 0.01) compared to those without such an educational background. Likewise, individuals suffering from diabetes demonstrate more knowledge (β = 1.564; p < 0.05) compared to those without the condition. Furthermore, knowledge of diabetes is correlated with income, showing a significant disparity between participants with higher monthly income levels (β = 1.161; p < 0.1; β = 1.035; p < 0.1) and those with lower income levels, indicating that individuals with higher income possess greater knowledge.
When it comes to attitudes toward diabetes, significant differences are not observed across most socio-demographic variables, except in the cases of marital status, educational background related to the medical field, and those individuals suffering from diabetes. Table 6 shows that being married is linked to a more positive attitude (β = 0.325; p < 0.1) when compared to being unmarried. Similarly, having an educational background related to the medical field significantly enhances one’s attitude toward diabetes (β = 1.005; p < 0.01) in contrast to those without such an education. Furthermore, experiencing diabetes is associated with a more favorable attitude (β = 0.449; p < 0.1) compared to individuals who are not suffering from the disease.
Regarding diabetes-related practices, having a postgraduate degree (β = 0.318; p < 0.1), an educational background related to the medical field (β = 0.303; p < 0.05), living with diabetes (β = 0.567; p < 0.01), and having higher income levels (β = 0.441; p < 0.05) are all positively associated with the adoption of positive practices. In summary, as shown in Table 6, individuals with a medical background and those grappling with diabetes exhibit higher levels of KAP related to diabetes among the Saudi Arabian population. Moreover, there exists a direct correlation between higher levels of education and income and enhanced knowledge and practices related to diabetes.
Discussion
Recognizing the significance of self-care in diabetes management, this study employed cross-sectional data from the general population of the KSA to examine KAP of diabetes and their variations across socio-demographic factors in the Kingdom. Both univariate and multivariate analyses show that individuals suffering from diabetes exhibit higher KAP levels while those with a medical education demonstrate significantly greater knowledge (β = 1.997; p < 0.01), more positive attitudes (β = 1.005; p < 0.01), and better practices (β = 0.303; p < 0.05) related to diabetes. Furthermore, an increase in education and income is associated with higher knowledge and better diabetes management practices. In contrast to some prior research (40, 41), age and work status did not show significant differences in KAP related to diabetes. To enhance knowledge, attitudes, and practices toward diabetes management, the government should implement educational programs tailored to the relevant socio-demographic differences.
Drawing direct comparisons with existing literature can be challenging due to the varying focus on specific population segments and regions. However, general comparisons can still be made, particularly concerning socio-demographic characteristics. For example, both univariate and multivariate analyses indicated that married individuals, as compared to unmarried ones, exhibit higher knowledge (β = 1.244; p < 0.05) and more positive attitudes (β = 0.325; p < 0.1). Similar findings that linked marriage to increased knowledge and more positive attitudes have been reported in other studies (42, 43). This could be attributed to the fact that married individuals are more likely to have at least one family member who might be affected by the disease, unlike unmarried individuals. Existing literature suggests that those with a family history of diabetes tend to possess greater knowledge and exhibit more positive attitudes toward the condition (44, 45).
The observation that higher education correlates with increased knowledge is a recurring theme in literature. Consistent findings have been reported in various studies, such as those in Bangladesh (46), the Hail region of Saudi Arabia (47), and among diabetes patients in Nepal (48). Furthermore, this study has found that those with education related to medical field have higher knowledge (β = 1.997; p < 0.01), higher positive attitudes (β = 1.005; p < 0.01) and good practices (β = 0.303; p < 0.05) related to diabetes. The higher KAP score is likely a result of higher exposure to comprehensive diabetes information which, in turn, contributes to a more positive attitude (49). Self-care education is crucial for effective diabetes management as it helps correct misconceptions regarding diabetes treatment and management (37). Therefore, while there are multiple avenues to improve KAP regarding diabetes, one effective approach is providing training, workshops, and educational programs for those with low levels of education in Saudi Arabia.
The higher KAP scores related to diabetes among individuals with medical education also apply to diabetes patients. The findings reveal that diabetes patients possess more knowledge and exhibit a more positive attitude toward diabetes compared to those without the condition. Similar findings in other studies indicate that individuals who have either been diagnosed with the disease or have a family member with the condition tend to demonstrate greater knowledge, maintain a positive attitude, and engage in better practices, as they are exposed to more information while seeking to aid themselves or their relatives (6, 40).
In addition to higher education resulting in higher knowledge scores, the study also found that increased income was associated with greater level of knowledge about diabetes. This is possibly because individuals with higher income levels are likely to engage in sedentary lifestyles which could contribute to high diabetes prevalence, thereby increasing their likelihood of having more knowledge about the disease (41). Additionally, Gillani et al. (50) underscores that individuals with ample financial resources tend to exhibit more positive attitudes toward seeking treatment. In contrast, individuals with limited means require support and encouragement to enhance their participation. Financial constraints are linked to negative attitudes, highlighting the potential significance of family income in efforts to shape attitude changes (46).
The relationship between gender and KAP concerning diabetes has yielded mixed findings in the literature. While some studies have reported higher knowledge scores among males, as observed in Al Hasa district, Saudi Arabia (51), the United Arab Emirates (52), and Pakistan (50), it’s important to note that these results are not consistent across all studies. For example, this study, in contrast, has identified that males exhibit lower knowledge about diabetes compared to females (β = −1.135; p < 0.05). This could be attributed to the fact that women with higher knowledge about diabetes are selected in the sample. This observation aligns with similar findings in Qatar (8) and among university students in Jeddah, Saudi Arabia (53), where females demonstrated a stronger understanding of diabetes. Nevertheless, concerning diabetes management practices, the study revealed that males exhibited better practices than females, aligning with findings from Aljofan et al. (47) in Saudi Arabia and Gautam et al. (48) in Nepal. This could be attributed to the greater willingness of male participants to make lifestyle adjustments compared to females.
The study has certain limitations worth noting. Firstly, it relies on self-reported data, which can be susceptible to biases. For instance, the survey does not delve into how participants accessed diabetes information, which could be valuable for devising targeted publicity strategies for the disease. Additionally, while the study includes the general population, the sample consists of only 617 participants, potentially limiting the generalizability of the findings to the entire Saudi Arabian population. This sample size was constrained by time and resource limitations. Furthermore, the study’s design and sampling technique do not establish causality, so the results should be interpreted as associations rather than causal relationships. It’s also important to acknowledge that data collection occurred online, potentially excluding individuals who are not familiar with online surveys, and responses may be skewed toward those with higher levels of education and income. However, despite these constraints, the study offers valuable insights into knowledge, attitudes, and practices related to diabetes, which can inform the development of diabetes intervention and prevention strategies.
Conclusion
This study used cross-sectional data to examine knowledge, attitudes, and practices of diabetes among the population of Saudi Arabia and assess their variations across socio-demographic factors. Through univariate and multivariate analyses, the study reveals distinct variations in knowledge, attitudes, and practices of diabetes among participants based on their gender, education, marital status, income, diabetes patient status, and having a medical field-related education. Although knowledge scores are relatively high, attitudes and practices related to diabetes generally lag behind, highlighting the need to implement strategies that promote changes in attitude and healthy lifestyle practices to mitigate diabetes-related risks. The findings also suggest a necessity for heightened care and specialized educational programs for individuals who are unmarried, lack a medical field-related education, and have lower levels of education and income. As diabetes management heavily relies on self-care, the government should prioritize improving diabetes KAP scores to prevent additional complications and burdens that could strain the healthcare system.
Data availability statement
The datasets generated and/or analysed during the current study are not publicly available due to privacy and confidentiality agreements as well as other restrictions but are available from the corresponding author on reasonable request.
Ethics statement
All procedures performed in this study, involving human participants, complied with the institutional and/or national research committee ethical standards, and the 1964 Helsinki declaration and subsequent amendments or equivalent ethical standards. This study has been reviewed and approved by the King Abdulaziz University Research Ethics Committee and was designed and performed in accordance with the ethical principles established by the university. Therefore, ethical approval was obtained from the Biomedical Ethics Research Committee, Faculty of Medicine, King Abdulaziz University (Ref-270-23). Online informed consent to participate was secured from all respondents who participated in the study. The data collection procedure was anonymous and as such no personal identifying information was collected.
Author contributions
BA-W: Conceptualization, Data curation, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing. MA-H: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Validation, Writing – original draft, Writing – review & editing, Project administration, Supervision.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Adhikari, SP, Meng, S, Wu, Y-J, Mao, Y-P, Ye, R-X, Wang, Q-Z, et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: a scoping review. Infect Dis Poverty. (2020) 9:1–12. doi: 10.1186/s40249-020-00646-x
2. Mandil, AM, Alfurayh, NA, Aljebreen, MA, and Aldukhi, SA. Physical activity and major non-communicable diseases among physicians in Central Saudi Arabia. Saudi Med J. (2016) 37:1243–50. doi: 10.15537/smj.2016.11.16268
3. WHO. Access to NCD medicines: emergent issues during the COVID-19 pandemic and key structural factors. (2023). Available at: https://www.who.int/publications/i/item/9789240069442.
4. Animaw, W, and Seyoum, Y. Increasing prevalence of diabetes mellitus in a developing country and its related factors. PLoS One. (2017) 12:e0187670. doi: 10.1371/journal.pone.0187670
5. Shaw, JE, Sicree, RA, and Zimmet, PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. (2010) 87:4–14. doi: 10.1016/j.diabres.2009.10.007
6. Ahmad, S, and Ahmad, MT. Assessment of knowledge, attitude and practice among diabetic patients attending a health care facility in North India. Indian J Basic Appl Med Res. (2015) 4:501–9.
7. Ogurtsova, K, da Rocha, FJ, Huang, Y, Linnenkamp, U, Guariguata, L, Cho, NH, et al. IDF diabetes atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. (2017) 128:40–50. doi: 10.1016/j.diabres.2017.03.024
8. Al-Mutawaa, KA, Farghaly, AH, Nasir, R, Loares, AM, Skaroni, I, Al-Thani, M, et al. Level of knowledge, attitude and practice towards diabetes among nationals and long-term residents of Qatar: a cross-sectional study. BMJ Open. (2022) 12:e052607. doi: 10.1136/bmjopen-2021-052607
9. Flor, LS, and Campos, MR. The prevalence of diabetes mellitus and its associated factors in the Brazilian adult population: evidence from a population-based survey. Rev Bras Epidemiol. (2017) 20:16–29. doi: 10.1590/1980-5497201700010002
10. Hunt, KJ, and Schuller, KL. The increasing prevalence of diabetes in pregnancy. Obstet Gynecol Clin N Am. (2007) 34:173–99. doi: 10.1016/j.ogc.2007.03.002
11. Ayah, R, Joshi, MD, Wanjiru, R, Njau, EK, Otieno, CF, Njeru, EK, et al. A population-based survey of prevalence of diabetes and correlates in an urban slum community in Nairobi. Kenya BMC public health. (2013) 13:1–11. doi: 10.1186/1471-2458-13-371
12. Iser, BPM, Malta, DC, Duncan, BB, de Moura, L, Vigo, Á, and Schmidt, MI. Prevalence, correlates, and description of self-reported diabetes in brazilian capitals–results from a telephone survey. PLoS One. (2014) 9:e108044. doi: 10.1371/journal.pone.0108044
13. Vandenheede, H, Deboosere, P, Espelt, A, Bopp, M, Borrell, C, Costa, G, et al. Educational inequalities in diabetes mortality across Europe in the 2000s: the interaction with gender. Int J Public Health. (2015) 60:401–10. doi: 10.1007/s00038-015-0669-8
14. Asadi-Lari, M, Khosravi, A, Nedjat, S, Mansournia, M, Majdzadeh, R, Mohammad, K, et al. Socioeconomic status and prevalence of self-reported diabetes among adults in Tehran: results from a large population-based cross-sectional study (urban HEART-2). J Endocrinol Investig. (2016) 39:515–22. doi: 10.1007/s40618-015-0384-6
15. Addo, J, Agyemang, C, Aikins, A-G, Beune, E, Schulze, MB, Danquah, I, et al. Association between socioeconomic position and the prevalence of type 2 diabetes in Ghanaians in different geographic locations: the RODAM study. J Epidemiol Community Health. (2017) 71:633–9. doi: 10.1136/jech-2016-208322
16. Schillinger, D, Barton, LR, Karter, AJ, Wang, F, and Adler, N. Does literacy mediate the relationship between education and health outcomes? A study of a low-income population with diabetes. Public Health Rep. (2006) 121:245–54. doi: 10.1177/003335490612100305
17. Hale, NL, Bennett, KJ, and Probst, JC. Diabetes care and outcomes: disparities across rural America. J Community Health. (2010) 35:365–74. doi: 10.1007/s10900-010-9259-0
18. Mutyambizi, C, Booysen, F, Stokes, A, Pavlova, M, and Groot, W. Lifestyle and socio-economic inequalities in diabetes prevalence in South Africa: a decomposition analysis. PLoS One. (2019) 14:e0211208. doi: 10.1371/journal.pone.0211208
19. Richards, SE, Wijeweera, C, and Wijeweera, A. Lifestyle and socioeconomic determinants of diabetes: evidence from country-level data. PLoS One. (2022) 17:e0270476. doi: 10.1371/journal.pone.0270476
20. Saeedi, P, Petersohn, I, Salpea, P, Malanda, B, Karuranga, S, Unwin, N, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the international diabetes federation diabetes atlas. Diabetes Res Clin Pract. (2019) 157:107843. doi: 10.1016/j.diabres.2019.107843
21. Biswas, T, Islam, MS, Linton, N, and Rawal, LB. Socio-economic inequality of chronic non-communicable diseases in Bangladesh. PLoS One. (2016) 11:e0167140. doi: 10.1371/journal.pone.0167140
22. Al-Hanawi, MK, Mwale, ML, and Qattan, AM. Health insurance and out-of-pocket expenditure on health and medicine: heterogeneities along income. Front Pharmacol. (2021) 12:638035. doi: 10.3389/fphar.2021.638035
23. Al-Hanawi, MK. Decomposition of inequalities in out-of-pocket health expenditure burden in Saudi Arabia. Soc Sci Med. (2021) 286:114322. doi: 10.1016/j.socscimed.2021.114322
24. Alqahtani, M, Almutairi, FE, Albasseet, AO, and Almutairi, KE. Knowledge, attitude, and practice of diabetes mellitus among the saudi population in Riyadh, Saudi Arabia: a quantitative study. Cureus. (2020) 12:e6601. doi: 10.7759/cureus.6601
25. Mansy, W, Wajid, S, Alwhaibi, A, Alghadeer, SM, Alhossan, A, Babelghaith, S, et al. Assessing outpatients’ knowledge, attitude, and practice toward managing diabetes in Saudi Arabia. Inquiry. (2022) 59:00469580221082781. doi: 10.1177/00469580221082781
26. Abougalambou, SSI, AbaAlkhail, H, and Abougalambou, AS. The knowledge, attitude and practice among diabetic patient in central region of Saudi Arabia. Diabetes Metab Syndr Clin Res Rev. (2019) 13:2975–81. doi: 10.1016/j.dsx.2019.07.049
27. Kupitz, DG, Fenwick, E, Kollmann, KM, Holz, FG, and Finger, RP. Diabetes and diabetic retinopathy management in East Africa: knowledge, attitudes, and practices of hospital staff in Kenya. Asia Pac J Ophthalmol. (2014) 3:271–6. doi: 10.1097/APO.0b013e3182a83bfa
28. AshaRani, P, Abdin, E, Kumarasan, R, Kumar, FDS, Shafie, S, Jeyagurunathan, A, et al. Study protocol for a nationwide knowledge, attitudes and practices (KAP) survey on diabetes in Singapore’s general population. BMJ Open. (2020) 10:e037125. doi: 10.1136/bmjopen-2020-037125
29. Bawazir, A, Al-Surimi, K, Suwaidan, SD, AlShehri, AM, AlFarhan, AI, and Abolfotouh, MA. Capacity and readiness of primary health care centers for implementation of the basic strategy for prevention and control of non-communicable diseases in Saudi Arabia.: a case study from the Ministry of National Guard-Health Affairs, Riyadh, Saudi Arabia. Saudi Med J. (2019) 40:614–8. doi: 10.15537/smj.2019.6.24164
30. Al-Hanawi, MK, Alsharqi, O, Almazrou, S, and Vaidya, K. Healthcare finance in the Kingdom of Saudi Arabia: a qualitative study of householders’ attitudes. Appl Health Econ Health Policy. (2018) 16:55–64. doi: 10.1007/s40258-017-0353-7
31. Al-Hanawi, MK. Socioeconomic determinants and inequalities in the prevalence of non-communicable diseases in Saudi Arabia. Int J Equity Health. (2021) 20:1–13. doi: 10.1186/s12939-021-01510-6
32. Al Dawish, MA, Robert, AA, Braham, R, Al Hayek, AA, Al Saeed, A, Ahmed, RA, et al. Diabetes mellitus in Saudi Arabia: a review of the recent literature. Curr Diabetes Rev. (2016) 12:359–68. doi: 10.2174/1573399811666150724095130
33. AlMuammar, SA, Noorsaeed, AS, Alafif, RA, Kamal, YF, Daghistani, GM, Almuammar, S, et al. The use of internet and social media for health information and its consequences among the population in Saudi Arabia. Cureus. (2021) 13:e18338. doi: 10.7759/cureus.18338
34. Cavana, R, Delahaye, B, and Sekeran, U. Applied business research: Qualitative and quantitative methods. Milton, QLD: John Wiley & Sons (2001).
35. STATS. General Authority for Statistics: the Kingdom of Saudi Arabia (2023). Available at: https://www.stats.gov.sa/en/node.
36. RAOSOFT. Sample Size Calculator (2023). Available at: http://www.raosoft.com/samplesize.html.
37. Herath, H, Weerasinghe, N, Dias, H, and Weerarathna, T. Knowledge, attitude and practice related to diabetes mellitus among the general public in Galle district in southern Sri Lanka: a pilot study. BMC Public Health. (2017) 17:1–7. doi: 10.1186/s12889-017-4459-5
39. Al-Saeed, AH, Constantino, MI, Molyneaux, L, D’Souza, M, Limacher-Gisler, F, Luo, C, et al. An inverse relationship between age of type 2 diabetes onset and complication risk and mortality: the impact of youth-onset type 2 diabetes. Diabetes Care. (2016) 39:823–9. doi: 10.2337/dc15-0991
40. Alsous, M, Abdel Jalil, M, Odeh, M, Al Kurdi, R, and Alnan, M. Public knowledge, attitudes and practices toward diabetes mellitus: a cross-sectional study from Jordan. PLoS One. (2019) 14:e0214479. doi: 10.1371/journal.pone.0214479
41. Daba, A, and Yazew, T. Associated factors with knowledge, attitude and practices of type II diabetic patients in ambo university referral hospital. Ethiopia Am J Lab Med. (2020) 5:102–12. doi: 10.11648/j.ajlm.20200504.14
42. Alaofè, H, Hounkpatin, WA, Djrolo, F, Ehiri, J, and Rosales, C. Knowledge, attitude, practice and associated factors among patients with type 2 diabetes in Cotonou. Southern Benin BMC public health. (2021) 21:1–11. doi: 10.1186/s12889-021-10289-8
43. Asmelash, D, Abdu, N, Tefera, S, Baynes, HW, and Derbew, C. Knowledge, attitude, and practice towards glycemic control and its associated factors among diabetes mellitus patients. J Diabetes Res. (2019) 2019:1–9. doi: 10.1155/2019/2593684
44. Niguse, H, Belay, G, Fisseha, G, Desale, T, and Gebremedhn, G. Self-care related knowledge, attitude, practice and associated factors among patients with diabetes in Ayder comprehensive specialized hospital. BMC Res Notes. (2019) 12:1–7. doi: 10.1186/s13104-019-4072-z
45. Reid, M, Ml, R, Raubenheimer, J, and Walsh, C. Diabetes-related knowledge, attitude and practices (KAP) of adult patients with type 2 diabetes mellitus in the Free State province, South Africa. South Afr J Clin Nutr. (2019) 32:20–7. doi: 10.1080/16070658.2018.1468536
46. Islam, FMA, Chakrabarti, R, Dirani, M, Islam, MT, Ormsby, G, Wahab, M, et al. Knowledge, attitudes and practice of diabetes in rural Bangladesh: the Bangladesh population based diabetes and eye study (BPDES). PLoS One. (2014) 9:e110368. doi: 10.1371/journal.pone.0110368
47. Aljofan, M, Altebainawi, A, and Alrashidi, MN. Public knowledge, attitude and practice toward diabetes mellitus in hail region, Saudi Arabia. Int J Gen Med. (2019) 12:255–62. doi: 10.2147/IJGM.S214441
48. Gautam, A, Bhatta, DN, and Aryal, UR. Diabetes related health knowledge, attitude and practice among diabetic patients in Nepal. BMC Endocr Disord. (2015) 15:1–8. doi: 10.1186/s12902-015-0021-6
49. Thirunavukkarasu, A, Almulhim, AK, Albalawi, FA, Alruwaili, ZM, Almajed, OA, Alruwaili, SH, et al. Knowledge, attitudes, and practices towards diabetic retinopathy among primary care physicians of Saudi Arabia: a multicenter cross-sectional study. Healthcare. (2021) 9:1697. doi: 10.3390/healthcare9121697
50. Gillani, AH, Amirul Islam, FM, Hayat, K, Atif, N, Yang, C, Chang, J, et al. Knowledge, attitudes and practices regarding diabetes in the general population: a cross-sectional study from Pakistan. Int J Environ Res Public Health. (2018) 15:1906. doi: 10.3390/ijerph15091906
51. Khan, A, Lateef, N, Khamseen, M, Alithan, M, Khan, S, and Ibrahim, I. Knowledge, attitude and practice of ministry of health primary health care physicians in the management of type 2 diabetes mellitus: a cross sectional study in the Al Hasa District of Saudi Arabia, 2010. Niger J Clin Pract. (2011) 14:1–8.
52. Al-Maskari, F, El-Sadig, M, Al-Kaabi, JM, Afandi, B, Nagelkerke, N, and Yeatts, KB. Knowledge, attitude and practices of diabetic patients in the United Arab Emirates. PLoS One. (2013) 8:e52857. doi: 10.1371/journal.pone.0052857
Keywords: knowledge, attitude, practice, diabetes, Saudi Arabia, socio-demographic
Citation: Al-Wagdi BE and Al-Hanawi MK (2024) Knowledge, attitude and practice toward diabetes among the public in the Kingdom of Saudi Arabia: a cross-sectional study. Front. Public Health. 12:1326675. doi: 10.3389/fpubh.2024.1326675
Edited by:
Nyi Nyi Naing, Sultan Zainal Abidin University, MalaysiaReviewed by:
Joanna Wang, University of Technology Sydney, AustraliaChu Lin, Peking University People's Hospital, China
Copyright © 2024 Al-Wagdi and Al-Hanawi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohammed Khaled Al-Hanawi, bWthbGhhbmF3aUBrYXUuZWR1LnNh
†ORCID: Mohammed Khaled Al-Hanawi, orcid.org/0000-0002-8419-2219