 Clara Oliveras1,2,3,4*
Clara Oliveras1,2,3,4* Pol Bruguera1,2,3,4Imanol Cordero-Torres5
Pol Bruguera1,2,3,4Imanol Cordero-Torres5 Andrea Millán-Hernández3
Andrea Millán-Hernández3 Maria Teresa Pons-Cabrera1,2,3Pablo Rodrigo Guzmán Cortez1,2,3Marta Gómez-Ramiro2,5,6,7,8Mireia Vázquez2,5Roger Borràs9Maria Asenjo-Romero5
Maria Teresa Pons-Cabrera1,2,3Pablo Rodrigo Guzmán Cortez1,2,3Marta Gómez-Ramiro2,5,6,7,8Mireia Vázquez2,5Roger Borràs9Maria Asenjo-Romero5 Eduard Vieta2,6,10
Eduard Vieta2,6,10 Antoni Gual1,2,3,4
Antoni Gual1,2,3,4 Hugo López-Pelayo1,2,3,4Mercè Balcells-Oliveró1,2,3,4
Hugo López-Pelayo1,2,3,4Mercè Balcells-Oliveró1,2,3,4- 1Addictions Unit, Psychiatry and Psychology Service, ICN, Hospital Clinic Barcelona, Barcelona, Spain
- 2Department of Psychiatry and Clinical Psychology, Hospital Clínic de Barcelona, Barcelona, Spain
- 3Health and Addictions Research Group, Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain
- 4Red de Investigación en Atención Primaria de Adicciones (RIAPAd), Madrid, Spain
- 5Emergency Department, Hospital Clínic de Barcelona, Barcelona, Spain
- 6Centro de Investigación en Red de Salud Mental (CIBERSAM), Madrid, Spain
- 7Barcelona Clínic Schizophrenia Unit, Institute of Neuroscience, Hospital Clínic, University of Barcelona, IDIBAPS, Barcelona, Spain
- 8Psychiatry Service, Complejo Hospitalario Universitario de Vigo, SERGAS, Translational Neuroscience Research Group, Galicia Sur Health Research Institute (IISGS), Vigo, Spain
- 9Institute of Neuroscience and Medical Statistics Core Facility, Hospital Clínic de Barcelona, Barcelona, Spain
- 10Bipolar and Depressive Disorders Unit, Institute of Neuroscience, Hospital Clínic, University of Barcelona, IDIBAPS, Barcelona, Spain
Introduction: Alcohol-related problems increase the probability of frequent emergency department (ED) use. In this study, we compared the direct healthcare expenses incurred during a single visit among frequent and non-frequent ED users and analyzed the impact of alcohol-related issues in healthcare costs arising from ED usage.
Methods: The study relied on secondary analyses of economic data from a 1:1 matched case–control study with the primary aim of identifying the clinical characteristics of hospital ED frequent users in a Mediterranean European environment with a public, universal, and tax-funded health system. The participants ranged in age from 18 to 65 years and underwent ED visits at a high-complexity Spanish hospital (cases ≥5 times, controls <5) from December 2018 to November 2019. Each case was matched to a control with the same age, gender, and date of attendance at the ED. Clinical data and direct healthcare costs for a single ED visit were obtained by a retrospective review of the first electronic medical register. Costs and duration of stay were compared between cases and controls using paired-samples t-tests, and ED users with and without alcohol-related problems were compared using bivariate (independent-samples t-tests, one-way analysis of variance, Chi square tests, and multiple linear regression) and multivariate analyses (multiple linear regression models with backward stepwise selection algorithm, and dependent variable: total mean direct costs).
Results: Among 609 case–control pairs (total n = 1218), mean total healthcare direct costs per ED visit were 22.2% higher among frequent compared with non-frequent users [mean difference 44.44 euros; 95% confidence interval (CI) 13.4–75.5; t(608) = 2.811; p = 0.005]. Multiple linear regression identified length of stay, triage level, ambulance arrival, and the specialty discharging the patient as associated with total healthcare costs for frequent users. In bivariate analyses, a history of alcohol-related problems was associated with a 32.5% higher mean total healthcare costs among frequent users [mean difference 72.61 euros; 95% confidence interval 25.24–119.97; t(320.016) = 3.015; p = 0.003].
Conclusion: The findings confirm the high cost of frequent ED use among people with alcohol-related problems, suggesting that costs could be reduced through implementation of intervention protocols.
1 Introduction
Most patients use emergency departments (EDs) sporadically for isolated pathologies, but some patients use these services frequently, representing a disproportionate amount of healthcare costs (1). Although definitions of frequent ED use vary (2), a common definition is five or more visits annually (3). In high-income countries, the percentage of frequent users (FUs) of ED is between 0.3 and 8% of all patients who present to emergency services, representing up to 28% of all ED visits (4). FUs are not only heavy users of acute services, but they also frequently use other health services (5), which suggests that they are sicker and more vulnerable. This is supported by a higher-than-expected mortality (6). These factors are likely to increase healthcare system costs.
Drug use-related disorders and other psychiatric diseases seem to increase the probability of frequent ED use (7, 8), which is especially true for alcohol addiction (9).
From 1990 to 2017, there was a global increase in individual alcohol consumption, prevalence of current drinkers, and proportion of episodic heavy drinkers among adults, whereas the proportion of lifetime abstinence declined. These trends are anticipated to continue in the coming years (10). Patients with alcohol-related problems (ARPs) are less likely to use primary care services than the rest of the population (11), but they are more likely to use emergency services (12). Furthermore, alcohol-related ED visits seem to be increasing in frequency, duration, and resource consumption (13). For instance, patients with emergency department visits related to drug use are more likely to receive diagnostic tests, such as toxicology screenings (14).
As described for other psychiatric illnesses (15), ARPs predict higher costs, not only in the ED (16), but also in the entire healthcare network (17).
Currently, the majority of studies describing the characteristics of FUs have been conducted in English-speaking countries, such as the United States, Canada, Australia, or the United Kingdom (18–20), with fewer studies available from other regions (21). Globally, healthcare costs associated with frequent ED use have received less attention (2).
This manuscript presents the secondary analyses of economic data obtained from a case–control study with the primary objective of outlining the clinical characteristics of hospital ED FUs in a Mediterranean European country (Spain). The results of that study indicated that a history of ARPs [adjusted odds ratio = 1.82 (95% confidence interval [CI] 1.26–2.64), p = 0.001] increased the probability of frequent utilization of emergency services (22). The main aims of the secondary analyses presented in this manuscript were to compare direct healthcare costs of a single urgent visit between frequent and non-frequent users of hospital emergency services and to explore the role of ARPs in direct healthcare costs of frequent ED use in a universal, public, tax-financed national health system. A secondary objective was to investigate the factors influencing the direct costs of ED utilization among individuals who are non-frequent users.
2 Methods
2.1 Study design and setting
A retrospective matched case–control study was conducted to characterize the clinical profile of ED FUs at a tertiary hospital located in a metropolitan city (Barcelona) in Spain.
The ED is responsible for treating internal medicine, psychiatric, trauma, and surgical emergencies. Electronic health records are used to track all healthcare encounters within the center and provide access to clinical care data. The ED is located in a specific building of the hospital, and different levels of acute care are assigned to different floors. The Spanish healthcare system is public, universal, and free of charge (tax-financed; Beveridge model (23)).
The study adhered to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) Statement Checklist for case–control studies (24) (Supplementary material 1).
The main objective of the study was to determine the significance of alcohol-related issues in the frequent utilization of an ED at a general hospital in a European Mediterranean society with a public, universal, tax-funded healthcare system (Spain). Another objective was to investigate the influence of other drug use-related disorders on frequent ED use in this environment. The hypothesis for the main study was that a history of alcohol-related problems and other drug use-related disorders would increase the probability of frequent attendance at the ED.
In this article, the secondary analyses of economic data from the aforementioned study (22) are reported.
The local Ethics Committee for Clinical Research at the Hospital Clinic of Barcelona has granted ethical approval (HCB/2019/0717). The investigation was conducted in accordance with the guidelines on Good Clinical Practice (CPMP/ICH/135/95) and with the ethical principles stated in the Declaration of Helsinki 1964, as revised at the 64th World Medical Association General Assembly held in Fortaleza, Brazil, in October 2013.
2.2 Participant selection
All cases (FUs) were all adults (ages 18 to 65 years) who had at least five visits to the hospital ED from 1 December 2018 to 30 November 2019. Each case was matched by age, gender, and date of ED attendance to one control (a non-frequent user with <5 yearly ED visits during that period).
During the study period, the ED received 103,668 visits from 75,410 patients. As in previous studies (4), the initial ED attendance recorded in the electronic register from 1 December 2018 to 30 November 2019 was utilized to match, by date of presentation to the ED, each case with a control of the same age and gender, extract clinical characteristics, and calculate direct healthcare costs per urgent visit.
After electronically applying inclusion and exclusion criteria, we have identified 698 case–control pairs. Of these, 89 pairs were manually excluded, including 14 instances of duplicate cases and 75 instances of absence of a medical note. A final list of 609 case–control pairs was generated, giving a total sample size of 1218 (Figure 1).
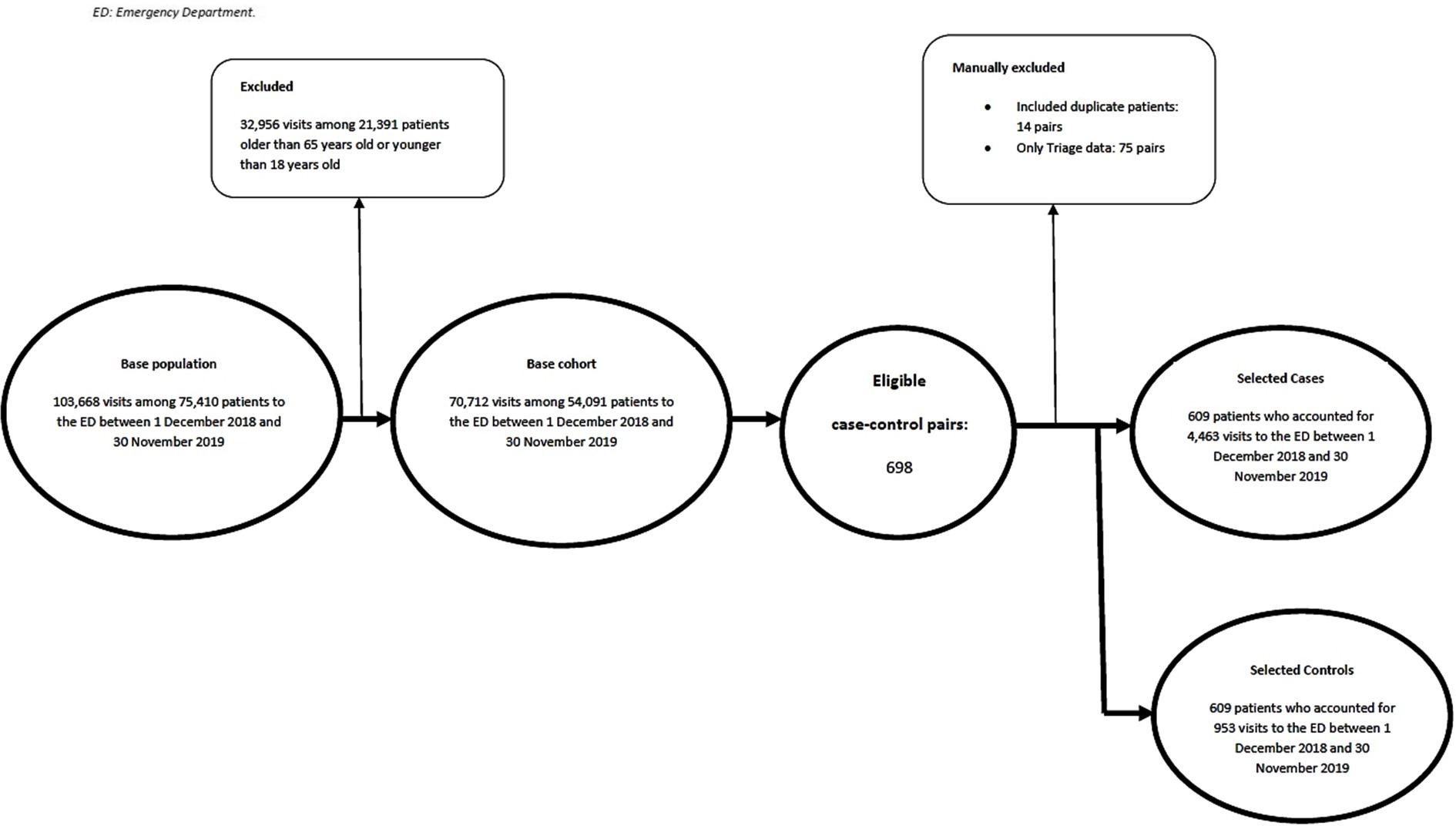
Figure 1. Flowchart of participant selection.
Before data extraction started, sample size calculations were performed based on estimates from previous studies (25). Assuming that 12% of controls would have a history of ARP, to detect a minimum odds ratio of 1.6 for emergency department frequent use with a power of 80% and a type I error of 0.5, a minimum of 567 case–control pairs with one matched control per case was needed, for a total sample size of 1158.
2.3 Methods of measurement
The variables obtained from each participant in the main case–control study are the following:
Outcome: frequent use of ED (≥5 visits to the ED from 1 December 2018 to 30 November 2019).
Exposures of interest include the history of any alcohol-related issues, as well as reports of other drug use-related disorders.
Covariates: age, gender, residence near the hospital, number of visits to the ED during a year, length of stay in the ED per visit (in minutes), night admission to the ED, ambulance arrival, report of other psychiatric comorbidity, report of organic comorbidity, report of alcohol drinking pattern, psychiatric assessment in the ED, social assessment in the ED, assessment by a non-psychiatric medical specialty in the ED, triage level at admission to the ED, type of specialty that discharged the patient from the ED, month of attendance at the ED, time of day at admission, type of psychiatric comorbidity, type of other drug use, situation at discharge.
To elaborate on a “Yes” in the variable “history of any alcohol-related problem,” the medical report had to include the history of diagnoses according to the International Classification of Diseases, Tenth Revision (ICD-10) (26) and the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (27), given in the table included in Supplementary material 2. The presence in the medical report of clinical presentations compatible with these pathologies, even if they were not coded through a standardized disease classification system, was also considered affirmative for the presence of ARPs. The reporting of other clinical conditions, such as accidents and trauma, when clearly related to alcohol use was also included as ARPs.
The following variables were automatically provided by the electronic health record system (SAP® software): age, gender, triage level at admission to the ED, month of attendance at the ED, time of day at admission, and length of stay (LoS). For other variables, in accordance with the general recommendations for this particular methodology (28), three team members conducted a chart data extraction. Two are psychiatrists specialized in addictions (CO and MTPC), and one is a nurse specialized in mental health (AMH). Prior to the commencement of extraction, all abstractors attended a meeting with the corresponding author (CO) to train in chart review methodology. If a condition was not mentioned, the abstractors documented that the condition was not present. Before formally beginning the extraction process, they reviewed 20 sample cases to assess reliability. This was confirmed by a Fleiss multi-rater Kappa statistic >0.6 for all variables. Throughout the extraction period, chart abstractors and senior researchers (AG, MB-O, HL-P) regularly met to resolve disputes and review coding rules.
Further details on the data extraction criteria are described elsewhere (22).
For the secondary analyses presented in this article, financial data on direct medical costs (in euros, €) per ED visit were obtained from the hospital’s financial department (Supplementary material 3).
2.4 Data analysis
The statistical analyses were performed using SPSS version 23.0 (IBM Corp., Armonk, NY, United States) and Stata 14 (StataCorp LLC, College Station, TX, United States). Data were summarized with descriptive analyses: continuous quantitative variables with total numbers, mean (M), and standard deviation (SD) and categorical variables with counts and percentages. To compare the costs and LoS between cases and controls, Student’s t-tests for paired samples were used.
Subsequently, the subgroups of frequent and non-frequent users were analyzed separately to ascertain which patient characteristics and professional interventions influence direct total costs per ED visit within each subgroup. ED users with ARPs were compared to users without ARPs using bivariate analyses (independent-samples t-tests, one-way analysis of variance, Chi-square tests, and multiple linear regression). In multivariate analyses, multiple linear regression models were used with total direct costs per ED visit as the dependent variable. Variables deemed clinically relevant and that were statistically significant (p < 0.05) for the dependent variable in bivariate analyses were incorporated into adjusted models employing a backward stepwise selection algorithm.
3 Results
3.1 Descriptive analyses
The sample included 609 case–control pairs (N = 1218; Tables 1–3). During the one-year period (1 December 2018 to 30 November 2019), controls accounted for 953 visits to the ED, whereas FUs accounted for 4,463 visits. The FUs visited the ED a mean of 7.34 (SD = 4.16) times per year (minimum of 5 and maximum of 42; 88.8% visited the ED ≤10 times during the study period). Controls presented a mean of 1.56 (SD = 0.87) times per year to the ED. The mean total direct expenses per ED visit were 244.87 € (SD = 268.86) among ED FUs and 200.43€ (SD = 310.12) among controls. There were no missing data.
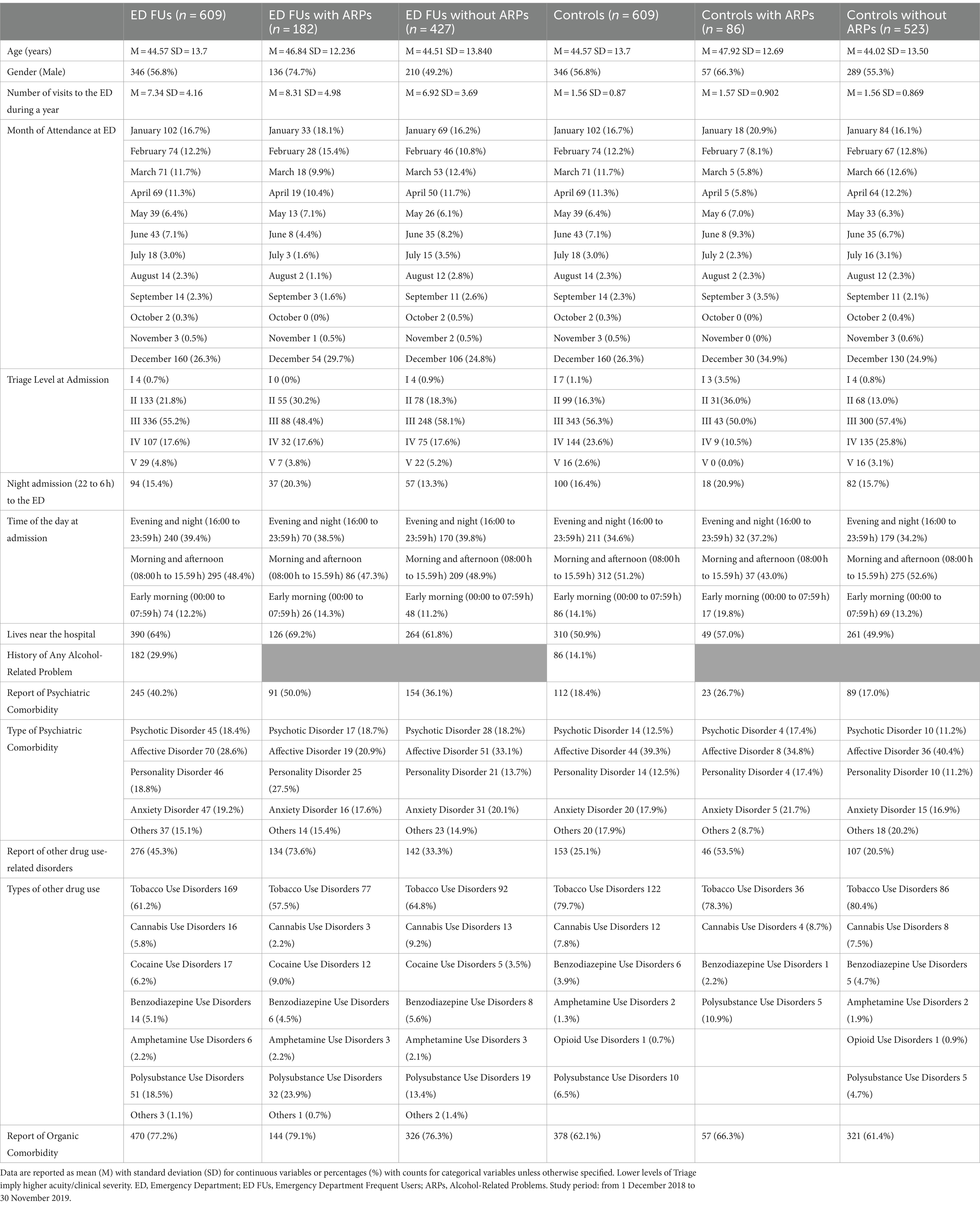
Table 1. Patient characteristics (clinical and sociodemographic data) of ED FUs (cases) vs. non-frequent users (controls): descriptive statistics.

Table 2. Professional interventions received in the ED by ED FUs (cases) vs. non-frequent users (controls): descriptive statistics.
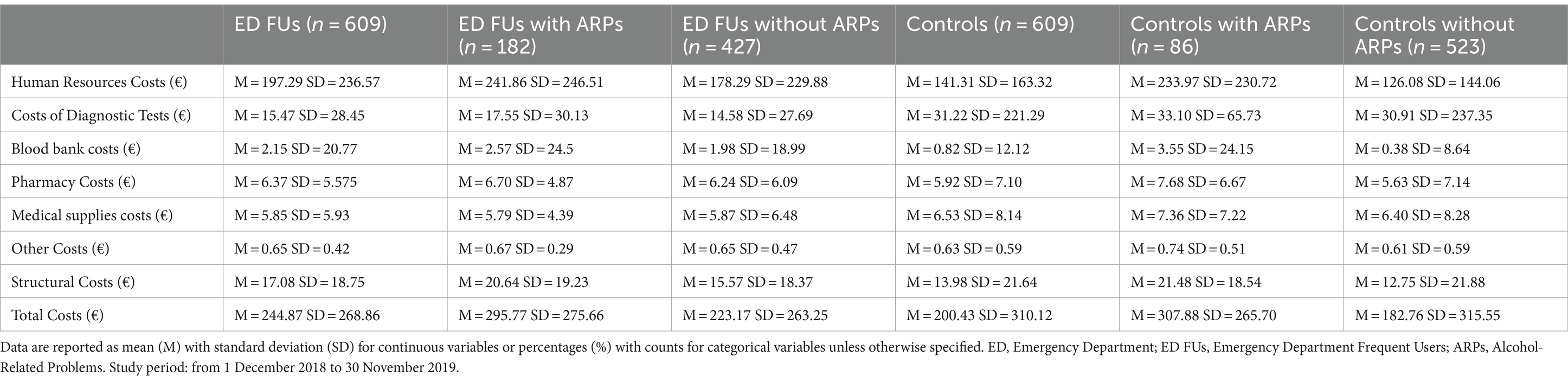
Table 3. Detailed healthcare costs per a single ED visit ED FUs (cases) vs. non-frequent users (controls): descriptive statistics.
3.2 Bivariate analyses
During the comparison of cases and controls in bivariate analyses, the mean total healthcare direct costs per ED visit were higher for FUs compared with non-frequent users [mean difference, 44.44 euros; 95% CI 13.4–75.5; t(608) = 2.811; p = 0.005]. The mean healthcare human resources costs for ED FU visits were higher by 55.97€ (95% CI 33.39–78.56) compared to costs for non-frequent users [t(608) = 4.868; p < 0.0005]. Mean LoS was longer for FUs by 142.117 minutes (95% CI 81.55–202.68) compared to non-frequent users [t (608) = 4.608, p = 0.0005].
In the bivariate analysis comparing ED FUs with and without ARPs and controls with and without ARPs, the mean total costs, healthcare human resources costs, and structural costs were higher, and the mean LoS was longer in the ARP groups from both FUs and non-frequent ED users (Table 4).
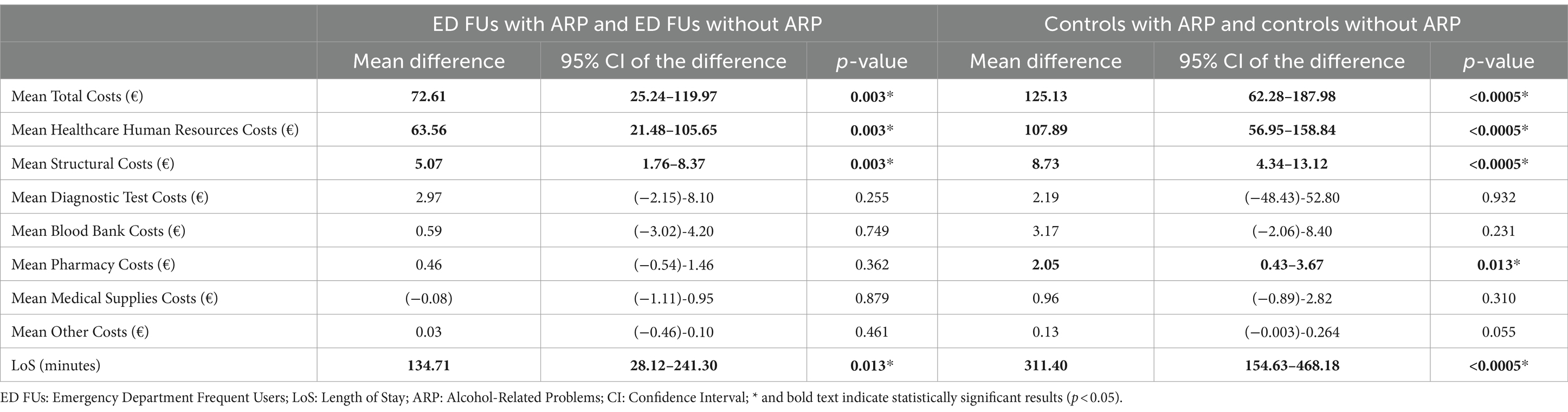
Table 4. Independent samples t-tests comparing ED FUs with and without ARP and non-frequent users of the ED with and without ARP.
3.3 Multivariate analyses
In a multiple linear regression model (Table 5) analyzing total costs per ED visit among FUs, we found that LoS, triage level, ambulance arrival, and the specialty that discharged the patient were significant predictors of direct costs. Longer LoS and ambulance arrival predicted higher costs per ED visit among FUs.
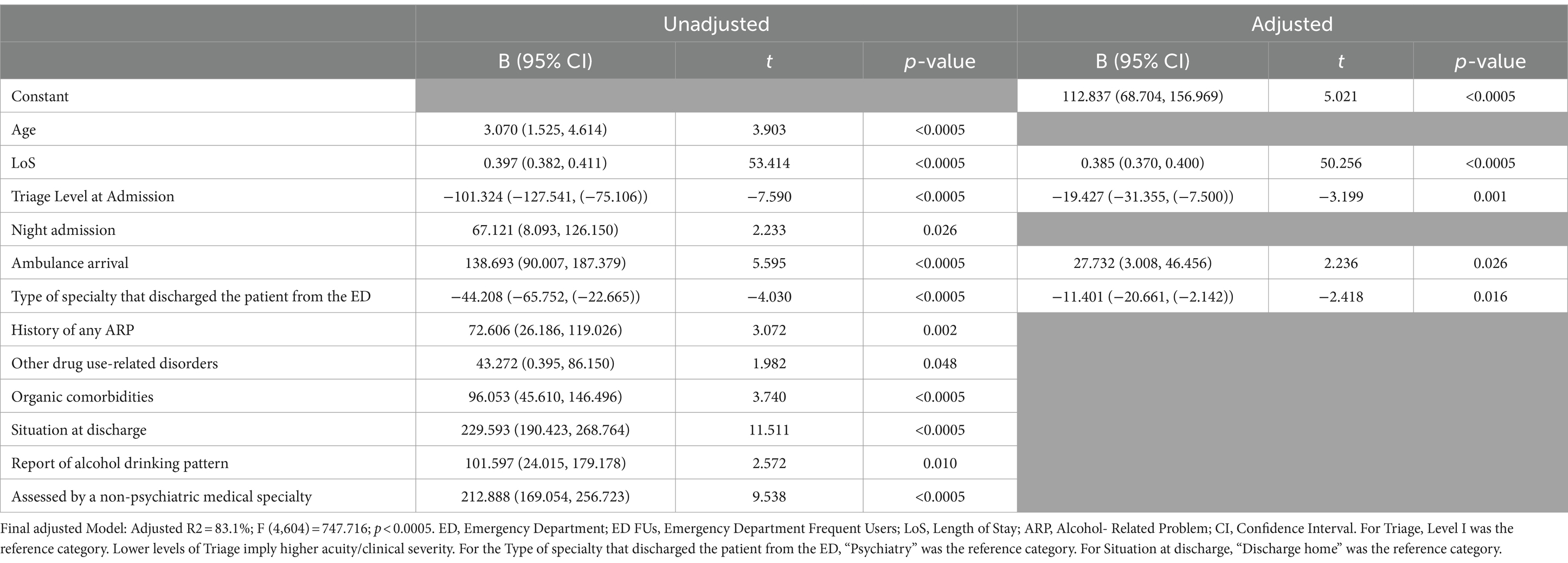
Table 5. Multiple linear regression models examining patient characteristics and professional interventions that influence direct total costs per ED visit among ED FUs.
Among non-frequent ED users (Table 6), the significant predictors identified in multivariate analysis were LoS, triage level, ambulance arrival, specialty that discharged the patient, and receiving assessment by a non-psychiatric medical specialty in the ED. The longer duration of LoS, ambulance arrival, and receiving assessment by a non-psychiatric medical specialty in the ED predicted higher costs per ED visit.
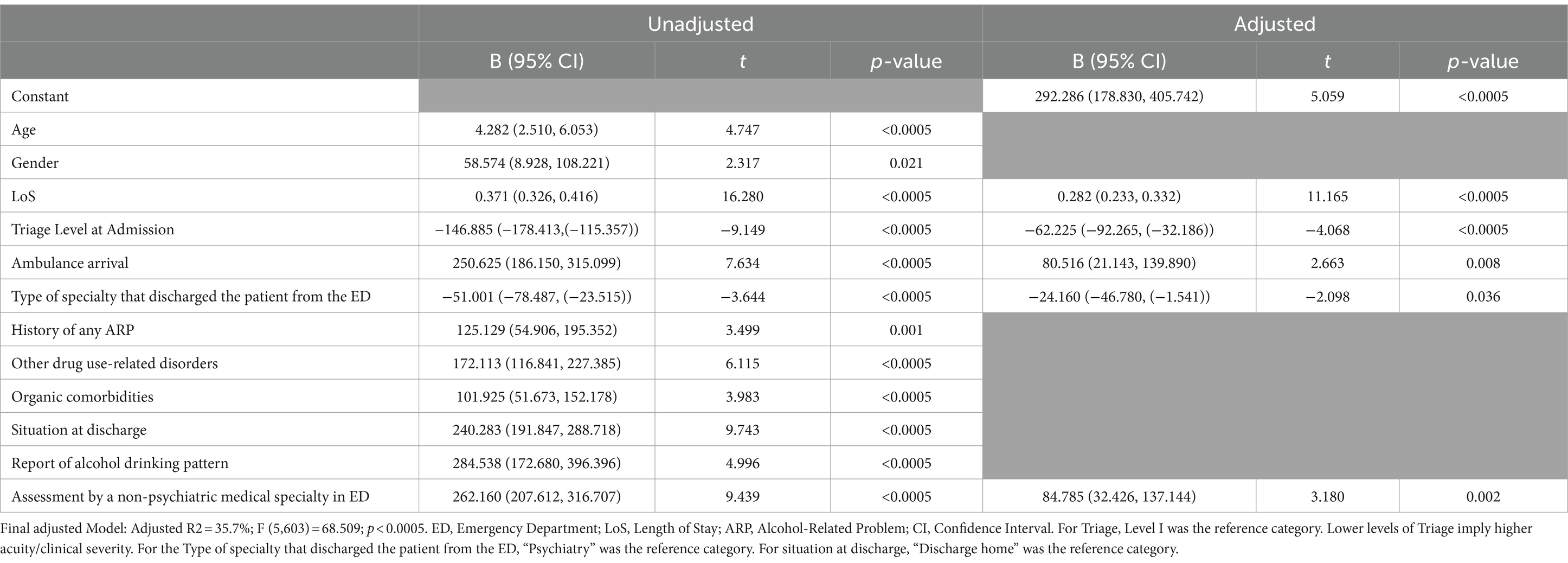
Table 6. Multiple linear regression models examining patient characteristics and professional interventions that influence direct total costs per ED visit among non-frequent ED users.
4 Discussion
To our knowledge, this investigation is one of the few to focus on understanding the influence of ARPs on healthcare costs related to frequent use of hospital emergency services in a public, universal, free-of-charge national health system.
In this secondary analysis, the mean direct total healthcare costs of a single ED visit in a general hospital were 22.2% more expensive among ED FUs compared to controls. It is clear that ED FUs present for emergency services much more frequently than do other patients and that, as a result, the total healthcare costs of this frequent use will be greater over time, as reported previously. A study conducted in the United States showed that, after a year, the global costs of attendance to emergency services were $10,465,216.07 among ED FUs compared with $1,012,610.21 among non-frequent ED users. However, past studies also pointed out that healthcare costs were similar for each ED visit between ED FUs and other users (29). Our results suggest that healthcare costs associated with ED frequent use are higher not only because of frequency but also because each consultation entails greater complexity, as indicated by the 37.6% longer mean LoS and 39.6% higher mean healthcare human resources costs for ED FUs compared with controls.
Results of bivariate analyses suggest that a history of ARPs was associated with an increase in mean total direct costs per visit among all ED users, raising mean human resources costs and LoS to an even greater degree among non-frequent users compared with FUs. Among ED FUs, a history of ARPs was linked to a 32.5% higher mean direct total cost per visit. Compared to ED FUs without ARPs, FUs with ARPs exhibited a 21.6% longer mean LoS, and each ED visit was 35.7% more expensive in terms of human resources costs. Among non-frequent users, ARPs were associated with a 68.5% higher mean direct total cost per visit. Compared with controls without ARPs, non-frequent users with ARPs had a mean LoS that was 93.3% longer, and each ED visit was 85.6% more expensive in terms of human resources costs. These results that suggest increased healthcare costs for patients with ARPs are similar to previously reported findings. In a Canadian sample of people with chronic diseases, psychiatric illnesses significantly increased the use of healthcare resources and their associated costs, whereas alcohol use disorders and other addictions had the highest rates of presentation to emergency services (15). In an Australian study involving ED patients, those who need extensive specialized treatment for alcoholism and other addictions attended the ED more frequently and incurred higher costs per visit. In addition, their hospital stays were usually longer (16). In a Catalan sample of adult primary healthcare patients, alcohol consumption was associated with increased charges from the public medical care system, showing a positive dose–response relationship (17).
The mean total direct cost per ED visit among ED FUs with ARPs was 295.77€ (SD = 275.66) in our analysis. Previous research on how ARPs affect frequent ED use–related costs is scarce, but estimates reported so far of healthcare costs for alcohol use–related ED presentations are generally higher. For instance, among ED users in the Netherlands, the average total expenses per patient seeking treatment for acute alcohol intoxication at the ED amounted to €1070 (encompassing estimated costs for ambulance transportation, ED visits, and hospital admission) (30). In an investigation involving adult ED users of a Belgian high-complexity hospital during a single year who attended the ED due to inebriety, the average estimated treatment cost was €541.32 per patient (31). However, most available estimates of urgent care costs related to alcohol use are reported from different countries, with distinct health systems and different costs of living.
In multivariate analyses, LoS, triage level, ambulance arrival, and type of specialty that discharged the patient were associated with total direct costs per ED visit among ED FUs in our sample. These factors were also associated with total direct costs among non-frequent users, as was undergoing assessment by a non-psychiatric medical specialty in the ED. According to these results, the most robust predictors of healthcare direct costs per ED visit would be the LoS, triage level, ambulance arrival, and discharge type of specialty for all users. The findings of the LoS and the triage level as predictors of ED healthcare costs are consistent with previous literature (32). Patients arriving by ambulance to the ED were noted to experience extended stays in the emergency services and incurred higher average expenses (33). The type of specialty that discharges the patient is also a predictor of ED healthcare costs, which is congruous with earlier evidence, as different types of diseases have been associated with diverse healthcare costs (34). Undergoing assessment by a non-psychiatric medical specialty is a predictor of costs among non-frequent users and is also consistent with previous knowledge. Multimorbidity is associated with an increased use of healthcare services, with associated costs (35). Nonetheless, given that ARPs were likely underreported in the reviewed charts, these results may underestimate emergency department costs attributable to ARPs.
4.1 Limitations
Some limitations of the current investigation should be noted. The first involves the case–control design, as retrospective data provide limited-quality evidence (28). Also, due to the focus of the original study on the relationship between substance use disorders and frequent ED use, clinical complexity was more finely assessed for substance use disorders and other psychiatric comorbidities and not so much for organic (non-psychiatric) medical comorbidities. Researchers were not blind to the study objectives or to the status of study participants (28). Since this is a single-center study, our findings might not be applicable to different contexts. Furthermore, variables of interest for this study could have been underreported in the charts. The literature suggests that psychiatric disorders (36), and especially addictions (25), are underreported in emergency medical reports. Therefore, it is possible that the findings underestimate the ED costs attributable to ARPs. Also, the estimates reflect only direct medical costs incurred only in the ED of one hospital, and the costs of using other resources of the healthcare system were not studied.
Despite these constraints, the academic background of abstractors equipped them with the expertise needed to precisely comprehend the subtleties of clinical data in the charts they reviewed. Additionally, they received standardized training in variable extraction and attended regular meetings with senior researchers to address disputes and review coding rules. Although prospective longitudinal studies provide higher-quality evidence, the clinical and social complexity of ED frequent users often makes long-term follow-up challenging. Retrospective designs are a useful initial approach for exploring large samples of this kind of patient.
Above all, the current study contributes to the limited body of research investigating expenses associated with frequent ED visits.
5 Conclusion
In a high-complexity public hospital, each FU attended the ED between 5 and 42 times per year, with an average of around 7 ED visits per patient. The mean direct total healthcare costs of a single ED visit were 22.2% higher among ED FUs than among matched, non-frequent users of emergency services. Given the association between a history of ARPs and a significantly increased likelihood of repeated emergency service use within the same sample, we propose that implementing targeted intervention protocols in the emergency room to address these issues simultaneously could mitigate the high healthcare costs associated with frequent ED use.
Prior presentations
Some of the data included in this manuscript was previously presented as a short oral communication under the title “El precio de la hiperfrecuentación de urgencias hospitalarias: ¿qué papel juegan el uso de alcohol y otras drogas?” in the 4th International Congress-XLIX Jornadas Nacionales Socidrogalcohol, which was held in Tenerife, Spain, between 6th and 8th October 2022, and as a short oral communication under the title “Influence of alcohol use and other addictive disorders in the costs of Emergency Department Frequent Use” in Lisbon Addictions 2022 (European Conference on Addictive Behaviors and Dependencies), which was held in Lisbon, Portugal, between 23rd and 25th November 2022.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary materials, further inquiries can be directed to the corresponding author.
Ethics statement
This study protocol was reviewed and approved by the local Ethics Committee for Clinical Research of Hospital Clinic de Barcelona, approval number HCB/2019/0717. The need for informed consent was waived by the Ethics Committee for Clinical Research of Hospital Clínic de Barcelona as the study consisted of a retrospective chart review of data routinely collected in daily clinical practice. This study was performed in accordance with the guidance on Good Clinical Practice (CPMP/ICH/135/95) and with the ethical principles stated in the Declaration of Helsinki 1964, as revised at the 64th World Medical Association (WMA) General Assembly in Fortaleza, Brazil, October 2013. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
CO: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing. PB: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Writing – review & editing. IC-T: Data curation, Software, Writing – review & editing. AM-H: Data curation, Investigation, Writing – review & editing. MTP-C: Data curation, Formal analysis, Investigation, Writing – review & editing. PRGC: Formal analysis, Writing – review & editing. MG-R: Formal analysis, Writing – review & editing. MV: Formal analysis, Writing – review & editing. RB: Formal analysis, Methodology, Supervision, Writing – review & editing. MAR: Writing – review & editing, Data curation, Software. EV: Writing – review & editing, Supervision. AG: Supervision, Writing – review & editing, Conceptualization, Methodology. HL-P: Conceptualization, Methodology, Supervision, Writing – review & editing, Formal analysis. MB-O: Conceptualization, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. MTP-C received funding by Contractes Clínic de Recerca “Emili Letang-Josep Font,” granted by Hospital Clínic de Barcelona, outside the submitted work. Red de Investigación en Atención Primaria de Adicciones, RIAPAd (RICORS), which is a project (RD21/0009/0010) funded by the Carlos III Institute, the European Regional Development Fund, and the Recovery, Transformation, and Resilience Plan.
Acknowledgments
The authors are grateful to Grup de Recerca Emergent, 2021 SGR 01158, AGAUR.
Conflict of interest
CO has received travel grants from Lundbeck, which had no bearing on the research of this study. PB has received honoraria from Lundbeck and travel grants from Pfizer, Lundbeck and Camurus, all outside the work of this manuscript. MTPC has received financial support for CME activities and travel funds from Lundbeck, Pfizer, and Esteve, outside the submitted work. MG-R has received funding unrelated to the present work for research projects and/or honoraria as a consultant or speaker from the following entities: Angelini, Janssen, Lundbeck, Otsuka, Sanofi-Aventis and Spanish Ministry of Science and Innovation- Instituto de Salud Carlos III. EV has received grants and served as consultant, advisor or CME speaker for the following entities: ABBiotics, AbbVie, Angelini, Biogen, Boehringer-Ingelheim, Celon Pharma, Dainippon Sumitomo Pharma, Ferrer, Gedeon Richter, GH Research, Glaxo-Smith Kline, Janssen, Lundbeck, Novartis, Orion Corporation, Organon, Otsuka, Sage, Sanofi-Aventis, Sunovion, Takeda, and Viatris, outside the submitted work. AG has received honoraria, research grants and travel grants from Lundbeck and D&A Pharma, which had no bearing on the research of this study. HL-P has received honoraria and travel grants from Lundbeck, which had no bearing on the research of this study. MB-O has received travel grants from Lundbeck and Camurus and CME-related honoraria from Novo Nordisk, all outside the subject of this article.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1322327/full#supplementary-material
References
1. Williams, RM. Frequent emergency department use in Sweden: implications for emergency medicine in the United States. Ann Emerg Med. (2001) 37:627–9. doi: 10.1067/mem.2001.115175
2. Pines, JM, Asplin, BR, Kaji, AH, Lowe, RA, Magid, DJ, Raven, M, et al. Frequent users of emergency department services: gaps in knowledge and a proposed research agenda. Acad Emerg Med. (2011) 18:e64–9. doi: 10.1111/j.1553-2712.2011.01086.x
3. Locker, TE, Baston, S, Mason, SM, and Nicholl, J. Defining frequent use of an urban emergency department. Emerg Med J. (2007) 24:398–401. doi: 10.1136/emj.2006.043844
4. Bieler, G, Paroz, S, Faouzi, M, Trueb, L, Vaucher, P, Althaus, F, et al. Social and medical vulnerability factors of emergency department frequent users in a universal health insurance system. Acad Emerg Med. (2012) 19:63–8. doi: 10.1111/j.1553-2712.2011.01246.x
5. Byrne, M, Murphy, AW, Plunkett, PK, McGee, HM, Murray, A, and Bury, G. Frequent attenders to an emergency department: a study of primary health care use, medical profile, and psychosocial characteristics. Ann Emerg Med. (2003) 41:309–18. doi: 10.1067/mem.2003.68
6. Hansagi, H, Olsson, M, Sjöberg, S, Tomson, Y, and Göransson, S. Frequent use of the hospital emergency department is indicative of high use of other health care services. Ann Emerg Med. (2001) 37:561–7. doi: 10.1067/mem.2001.111762
7. Meng, X, Muggli, T, Baetz, M, and D’Arcy, C. Disordered lives: life circumstances and clinical characteristics of very frequent users of emergency departments for primary mental health complaints. Psychiatry Res. (2017) 252:9–15. doi: 10.1016/j.psychres.2017.02.044
8. Moe, J, Kirkland, S, Ospina, MB, Campbell, S, Long, R, Davidson, A, et al. Mortality, admission rates and outpatient use among frequent users of emergency departments: a systematic review. Emerg Med J. (2016) 33:230–6. doi: 10.1136/emermed-2014-204496
9. Gual, A, and Drummond, C. Killing me softly: alcohol addiction today. Eur Neuropsychopharmacol. (2022) 57:30–2. doi: 10.1016/j.euroneuro.2021.12.008
10. Manthey, J, Shield, KD, Rylett, M, Hasan, OSM, Probst, C, and Rehm, J. Global alcohol exposure between 1990 and 2017 and forecasts until 2030: a modelling study. Lancet. (2019) 393:2493–502. doi: 10.1016/S0140-6736(18)32744-2
11. Miquel, L, Gual, A, Vela, E, Lligoña, A, Bustins, M, Colom, J, et al. Alcohol consumption and inpatient health service utilization in a cohort of patients with alcohol dependence after 20 years of follow-up. Alcohol Alcohol. (2016) 52:227–33. doi: 10.1093/alcalc/agw075
12. Chabert, J, Lambert, C, Cabé, J, Cherpitel, CJ, Rolland, B, Moustafa, F, et al. Could reasons for admission help to screen unhealthy alcohol use in emergency departments? A multicenter French study. Front. Psychiatry. (2023) 14:1–11. doi: 10.3389/fpsyt.2023.1271076
13. Mullins, PM, Mazer-Amirshahi, M, and Pines, JM. Alcohol-related visits to US emergency departments, 2001-2011. Alcohol Alcohol. (2016) 52:119–25. doi: 10.1093/alcalc/agw074
14. Beckerleg, W, and Hudgins, J. Substance use-related emergency department visits and resource utilization. West J Emerg Med. (2022) 23:166–73. doi: 10.5811/westjem.2022.1.53834
15. Sporinova, B, Manns, B, Tonelli, M, Hemmelgarn, B, Macmaster, F, Mitchell, N, et al. Association of mental health disorders with health care utilization and costs among adults with chronic disease. JAMA Netw Open. (2019) 2:1–14. doi: 10.1001/jamanetworkopen.2019.9910
16. Butler, K, Reeve, R, Arora, S, Viney, R, Goodall, S, van Gool, K, et al. The hidden costs of drug and alcohol use in hospital emergency departments. Drug Alcohol Rev. (2016) 35:359–66. doi: 10.1111/dar.12302
17. Miquel, L, Rehm, J, Shield, KD, Vela, E, Bustins, M, Segura, L, et al. Alcohol, tobacco and health care costs: a populationwide cohort study (n = 606 947 patients) of current drinkers based on medical and administrative health records from Catalonia. Eur J Pub Health. (2018) 28:674–80. doi: 10.1093/eurpub/ckx236
18. LaCalle, E, and Rabin, E. Frequent users of emergency departments: the myths, the data, and the policy implications. Ann Emerg Med. (2010) 56:42–8. doi: 10.1016/j.annemergmed.2010.01.032
19. Giannouchos, TV, Kum, HC, Foster, MJ, and Ohsfeldt, RL. Characteristics and predictors of adult frequent emergency department users in the United States: a systematic literature review. J Eval Clin Pract. (2019) 25:420–33. doi: 10.1111/jep.13137
20. Soril, LJJ, Leggett, LE, Lorenzetti, DL, Noseworthy, TW, and Clement, FM. Characteristics of frequent users of the emergency department in the general adult population: a systematic review of international healthcare systems. Health Policy (New York). (2016) 120:452–61. doi: 10.1016/j.healthpol.2016.02.006
21. Van Tiel, S, Rood, PPM, Bertoli-Avella, AM, Erasmus, V, Haagsma, J, Van Beeck, E, et al. Systematic review of frequent users of emergency departments in non-US hospitals: state of the art. Eur J Emerg Med. (2015) 22:306–15. doi: 10.1097/MEJ.0000000000000242
22. Oliveras, C, Bruguera, P, Cordero Torres, I, Millán Hernández, A, Pons, MT, Guzmán Cortez, PR, et al. Another round: influence of alcohol-related conditions and other drug use-related disorders in emergency department frequent use – a single-site matched case-control study in Spain. Eur Addict Res. (2024) 30:275–287. doi: 10.1159/000538987
23. Van Der Zee, J, and Kroneman, MW. Bismarck or Beveridge: a beauty contest between dinosaurs. BMC Health Serv Res. (2007) 7:1–11. doi: 10.1186/1472-6963-7-94
24. Vandenbroucke, JP, Von Elm, E, Altman, DG, Gøtzsche, PC, Mulrow, CD, Pocock, SJ, et al. Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. PLoS Med. (2007) 4:e297. doi: 10.1371/journal.pmed.0040297
25. Bruguera, P, Barrio, P, Oliveras, C, Vázquez, M, Soler, V, Nuño, L, et al. Detection and registration of alcohol use in the emergency department. Rev Esp Salud Publica. (2020) 94:E1–E8. doi: 10.4321/S1135-57272020000100021
26. World Health Organization. ICD-10: international statistical classification of diseases and related health problems. tenth revision, 2nd ed. Geneva (Switzerland): World Health Organization (2004).
27. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington, D.C.: American Psychiatric Publishing (2013).
28. Kaji, AH, Schriger, D, and Green, S. Looking through the retrospectoscope: reducing bias in emergency medicine chart review studies. Ann Emerg Med. (2014) 64:292–8. doi: 10.1016/j.annemergmed.2014.03.025
29. Ondler, C, Hegde, GG, and Carlson, JN. Resource utilization and health care charges associated with the most frequent ED users. Am J Emerg Med. (2014) 32:1215–9. doi: 10.1016/j.ajem.2014.07.013
30. Verheij, C, Rood, PPM, Deelstra, CK, Levendag, MLL, Koch, BCP, Polinder, S, et al. Emergency department visits due to intoxications in a Dutch university hospital: occurrence, characteristics and health care costs. PLoS One. (2019) 14:e0226029. doi: 10.1371/journal.pone.0226029
31. Verelst, S, Moonen, PJ, Desruelles, D, and Gillet, JB. Emergency department visits due to alcohol intoxication: characteristics of patients and impact on the emergency room. Alcohol Alcohol. (2012) 47:433–8. doi: 10.1093/alcalc/ags035
32. Ruger, JP, Richter, CJ, Spitznagel, EL, and Lewis, LM. Analysis of costs, length of stay, and utilization of emergency department services by frequent users: implications for health policy. Acad Emerg Med. (2004) 11:1311–7. doi: 10.1197/j.aem.2004.07.008
33. Ruger, JP, Richter, CJ, and Lewis, LM. Clinical and economic factors associated with ambulance use to the emergency department. Acad Emerg Med. (2006) 13:879–85. doi: 10.1197/j.aem.2006.04.006
34. Meerding, WJ, Bonneux, L, Polder, JJ, Koopmanschap, MA, and Van der Maas, PJ. Demographic and epidemiological determinants of healthcare costs in Netherlands: cost of illness study. Br Med J. (1998) 317:111–5. doi: 10.1136/bmj.317.7151.111
35. Johnston, MC, Crilly, M, Black, C, Prescott, GJ, and Mercer, SW. Defining and measuring multimorbidity: a systematic review of systematic reviews. Eur J Pub Health. (2019) 29:182–9. doi: 10.1093/eurpub/cky098
Keywords: healthcare costs, alcohol, psychiatry, emergency department, frequent users
Citation: Oliveras C, Bruguera P, Cordero-Torres I, Millán-Hernández A, Pons-Cabrera MT, Guzmán Cortez PR, Gómez-Ramiro M, Vázquez M, Borràs R, Asenjo-Romero M, Vieta E, Gual A, López-Pelayo H and Balcells-Oliveró M (2024) Effects of alcohol-related problems on the costs of frequent emergency department use: an economic analysis of a case–control study in Spain. Front. Public Health. 12:1322327. doi: 10.3389/fpubh.2024.1322327
Edited by:
Xiaozhen Lai, Peking University, ChinaReviewed by:
Giulia Caggiu, University of Milano-Bicocca, ItalyMark Attridge, Attridge Consulting, Inc., United States
Copyright © 2024 Oliveras, Bruguera, Cordero-Torres, Millán-Hernández, Pons-Cabrera, Guzmán Cortez, Gómez-Ramiro, Vázquez, Borràs, Asenjo-Romero, Vieta, Gual, López-Pelayo and Balcells-Oliveró. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Clara Oliveras, Y29saXZlcmFzQGNsaW5pYy5jYXQ=