 Narjes Hazar1
Narjes Hazar1 Mohammad Jokar
Mohammad Jokar Vahid Rahmanian
Vahid Rahmanian- 1Diabetes Research Center, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
- 2Young Researchers and Elite Club, Islamic Azad University of Karaj, Karaj, Iran
- 3Research Center for Non Communicable Disease, Jahrom University of Medical Sciences, Jahrom, Fars, Iran
- 4Center for Healthcare Data Modeling, Department of Biostatistics and Epidemiology, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
- 5Department of Public Health, Torbat Jam Faculty of Medical Science, Torbat Jam, Iran
Background: Diabetes mellitus (DM) poses a significant threat to public health, and the anticipated surge of over 100% in the age-standardized prevalence of type 2 diabetes in Iran between 2021 and 2050 underscores the pressing need for focused attention. The rationale for estimating the prevalence of type 2 diabetes in Iran becomes even more compelling when considering the potential cascading effects on the healthcare system, quality of life, and economic burden. The aim of this study was to estimate the prevalence and trends of DM from 1996 to 2023 in the Islamic Republic of Iran.
Methods: Up to July 2023, without deadlines, the search for appropriate articles in Persian and English. Iranian sources including SID, Magiran, and Element were included in the databases, along with foreign ones like PubMed/MEDLINE, Web of Science, Science Direct, Embase, Scopus, ProQuest, and Google Scholar. Using the JBI quality checklist, the study’s level of quality was evaluated. Version 14 of STATA was used to carry out the statistical analysis. The Dersimonian and Liard random-effects models were used because of heterogeneity. To investigate the causes of heterogeneity, subgroup analysis and univariate meta-regression were utilized. Sensitivity analysis was then carried out to see how each study’s findings affected the final findings. The prevalence pattern over time was also followed using cumulative meta-analysis.
Results: There were 53 studies in all, with a combined sample size of 1,244,896 people. Men were predicted to have a type 2 diabetes prevalence of 10.80% (95% CI: 9.1–12.4), while women were assessed to have a prevalence of 13.4% (95% CI: 11.6–15.3). Additionally, the prevalence of diabetes was much higher in the 55–64 age group, coming in at 21.7% (95% CI: 17.5–25.0). The anticipated prevalence of diabetes was 7.08% for 1988 to 2002, 9.05% for 2003 to 2007, 9.14% for 2008 to 2012, 15.0% for 2013 to 2017, and 13.40% for 2018 to 2023, among other time periods. Geographically, type 2 diabetes was most prevalent in Khuzestan (15.3%), followed by Razavi Khorasan (14.4%), Qazvin (14.3%), and Yazd (12.6%).
Conclusion: The prevalence of type 2 diabetes was estimated at 10.8%, highlighting variations across gender, age groups, and geographic regions that underscore the necessity for specific interventions. These findings advocate for proactive measures, including tailored screening and lifestyle modification programs. The notable temporal increase from 2013 to 2017 signals the need for policymakers and healthcare practitioners to develop effective strategies, anticipating and addressing the potential future burden on the healthcare system.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023437506, identifier: CRD42023437506.
1 Background
Diabetes is recognized as the primary cause of morbidity and mortality worldwide (1). It is a chronic and complex disease. According to estimates from the Global Burden of Disease study, diabetes was the eighth leading cause of mortality and disability worldwide in 2019, affecting nearly 460 million people (2) across all countries and age groups. The resulting medical expenses have placed a heavy pressure on healthcare systems. 537 million people worldwide are estimated to have diabetes according to predictions from the International Diabetes Federation from 2021 (3), with global healthcare spending expected to exceed $1,054 billion by 2045.The possibility of slowing the rise in diabetes prevalence by 2025 is less than 1% for women and significantly lower for males, despite worldwide efforts to manage and prevent the disease (4). While type 2 diabetes is characterized by a non-autoimmune progressive loss of adequate-cell insulin secretion against a background of metabolic syndrome and insulin resistance, type 1 diabetes is recognized by the American Diabetes Association (ADA) 2023 classification system as an autoimmune condition that results in pancreatic-cell destruction and complete insulin deficiency. Notably, the conventional categorization of diabetes type 1 as exclusively affecting children and type 2 as only affecting adults is no longer accurate (5). Age over 40, obesity, high blood pressure, an abnormal lipid profile, a lack of physical exercise, a history of gestational diabetes, smoking, and alcohol use are all risk factors for type 2 diabetes. Amputation of the lower limbs, blindness, retinopathy, nephropathy, and atherosclerotic cardiovascular disease are only a few of the serious consequences and organ damage that diabetic patients run the risk of (6).
The age-standardized global prevalence of type 2 diabetes is expected to surge significantly, increasing by 61.2% from 5.9% in 2021 to 9.5% in 2050, impacting a staggering 1.27 billion individuals worldwide. This prevalence exhibits notable variations across super-regions, ranging from 82.7% in North Africa and the Middle East to 30.3% in the high-income region. Moreover, the age-standardized prevalence of type 2 diabetes is projected to more than double in specific countries in North Africa and the Middle East between 2021 and 2050. These nations include Oman, United Arab Emirates, Syria, Iran, Libya, Sudan, and Saudi Arabia (7).
Various statistics on the prevalence of diabetes in Iran are available. A meta-analysis study conducted between 1996 and 2004 indicated that 24% of those over 40 had diabetes (8). Lower prevalence rates, however, have been found by more recent research. The prevalence of diabetes was found to be 26.1% in Yazd in 2015 (28% in women and 22.9% in men) (9), and 14.4% in Tehran’s population in 2017 (10). According to a study from the World Health Organization from 2020, Iran’s total prevalence of diabetes was 10.3%, with estimates for men and women of 9.6 and 11.1%, respectively. Obesity (24.9%), physical inactivity (31.9%), and overweight (60.5%) were the main risk factors for this illness in Iran. In light of anticipated surge in total diabetes prevalence, there is a compelling need to undertake a comprehensive analysis to assess and estimate the prevalence of diabetes in Iran. Such an analysis is vital for gaining insights into the specific challenges faced by Iran and for developing targeted strategies to address the growing impact of diabetes within the country. The aim of this study was to estimate the prevalence and trends of DM from 1996 to 2023 in the Islamic Republic of Iran.
2 Methods
2.1 Protocol and registration
According to the PRISMA-P 2020 guidelines for reporting items in systematic reviews and meta-analysis protocols, this systematic review and meta-analysis adhered to the process set out in that document. The study’s protocol was entered into the PROSPERO database and given the registration number CRD42023437506. The details can be accessed at: https://www.crd.york.ac.uk/prospero/#recordDetails.
2.2 Search strategy
The researchers conducted a time-unrestricted search for pertinent articles in Iranian databases including SID (Scientific Information Database), Magiran, and Element, as well as international databases such as PubMed/MEDLINE, Web of Science, ScienceDirect, Embase, Scopus, ProQuest, and Google Scholar from the inception of their investigation until July 2023. The search strategy utilized a combination of relevant keywords and controlled vocabulary specific to each database (Supplementary Table 1). In Iranian databases, Persian terms and their English equivalents were used, while in international databases, English-language terms were employed. The search strategy included both Persian and English-language publications. Boolean operators “AND” and “OR” were utilized to combine search terms effectively. Additionally, reference lists of identified articles were manually searched to ensure comprehensive coverage of relevant literature. The PRISMA flowchart (Figure 1) depicts the process of identifying and selecting relevant publications.
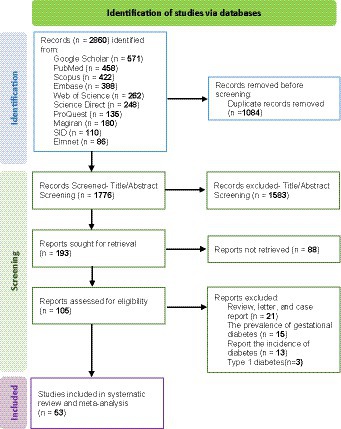
Figure. 1. PRISMA flowchart of studies included in this systematic review and meta-analysis.
2.3 Eligibility criteria
Studies required to be original full-text papers published in peer-reviewed journals up to July 2023, in either English or Persian, and done in Iranian settings in order to be included in this systematic review and meta-analysis. Furthermore, this systematic review and meta-analysis included cross-sectional studies that reported the prevalence of diabetes. Exclusion criteria were employed to filter out articles that did not adhere to specific requirements. Notably, non-observational studies, including short communications and review articles, were excluded. Additionally, studies with smaller sample sizes, non-random sampling techniques, and those involving a mixture of type 2 and type 1 diabetes were not considered for inclusion.
2.4 Study risk of bias assessment
Using the JBI quality assessment technique for prevalence studies (11), two reviewers provided a critical evaluation of the included papers. Nine characteristics make up this instrument, which evaluates many factors like suitable sampling, concise research descriptions, sufficient sample sizes, reliable procedures and measurements, and acceptable statistical analysis. For each parameter, a score of 1 was given for a “Yes” response and a score of 0 for a “No” or “Unclear” response. Each article’s mean score was calculated. The identity of the journal and the authors’ identities were not withheld from the reviewers as they independently assessed the research. The reliability value for the Cohen’s Kappa test, which was used to measure the inter-rater agreement, was 0.838 (p < 0.001), suggesting very good agreement between the two reviewers. The total possible score for each paper ranged from 0 to 9. Based on their overall scores, the studies were divided into three categories: low risk of bias (8, 9), moderate risk of bias (4–7), and high risk of bias (0–3). Conflicts between reviewers were resolved through consensus discussion. In cases where discrepancies arose in the assessment of individual studies, the two reviewers discussed their interpretations and reasons for scoring each criterion. If consensus could not be reached, a third independent reviewer was consulted to adjudicate the disagreement.
2.5 Selection process
This research employed a multi-step procedure to extract accurate data. All chosen articles were imported into EndNote X8, and duplicates were eliminated. Then, the two team members independently examined the remaining articles’ titles and abstracts to eliminate any irrelevant studies. The criteria for selection were based on reports pertinent to the research topic and consistent with methods of analytical study. The World Health Organization (WHO) criteria were used for diagnosing diabetes in this research (5).
2.6 Data extraction
During the data extraction process, the included studies’ pertinent data were retrieved, including the author (s)’ names, publication year, sample size, total positive number, location, age group, gender, study design, BMI, and prevalence. In cases where discrepancies arose between the two team members during data extraction, a consensus was reached through discussion and re-evaluation of the respective articles. If disagreements persisted, a third senior researcher was consulted to provide an impartial resolution.
2.7 Synthesis methods
STATA 14 was used for the statistical analysis in this meta-analysis. Using inverse variance and Cochran Q statistics, the degrees of heterogeneity among the included studies were assessed. Low, moderate, and high levels of heterogeneity were determined, respectively, by I2 values of less than 50%, between 50 and 80%, and higher than 80%. The Dersimonian and Liard random-effects models were used for the statistical analysis due to the heterogeneity. To learn more about the causes of heterogeneity, several methods were used, including subgroup analysis and univariate meta-regression. The One-out-remove method was used in the sensitivity analysis to determine the effect of each research on the final outcomes. Using Egger’s regression, publication bias was evaluated. The total estimate was modified using the trim-and-fill approach in order to account for the estimated number of studies that were lost to censorship (12). The trend of changes in prevalence over time was examined using a cumulative meta-analysis test. Using the ArcGIS 10.3 program, the regional distribution of type 2 diabetes prevalence throughout Iranian provinces was examined.
3 Results
3.1 Study selection
Based on the inclusion criteria, 2,860 articles from the available databases were chosen. Then, 1776 articles with repetitive titles and abstracts were further examined after 1,084 duplicate entries were eliminated. One hundred ninety three papers were eliminated after a full-text examination, leaving 107 publications to be evaluated for eligibility. The systematic review and meta-analysis comprised 53 papers in total (Figure 1).
3.2 Study characteristics
The features of the selected studies are presented in detail in Table 1. 53 studies in all were selected, 21 of which were done between 1988 and 2007 and 32 between 2013 and 2023.
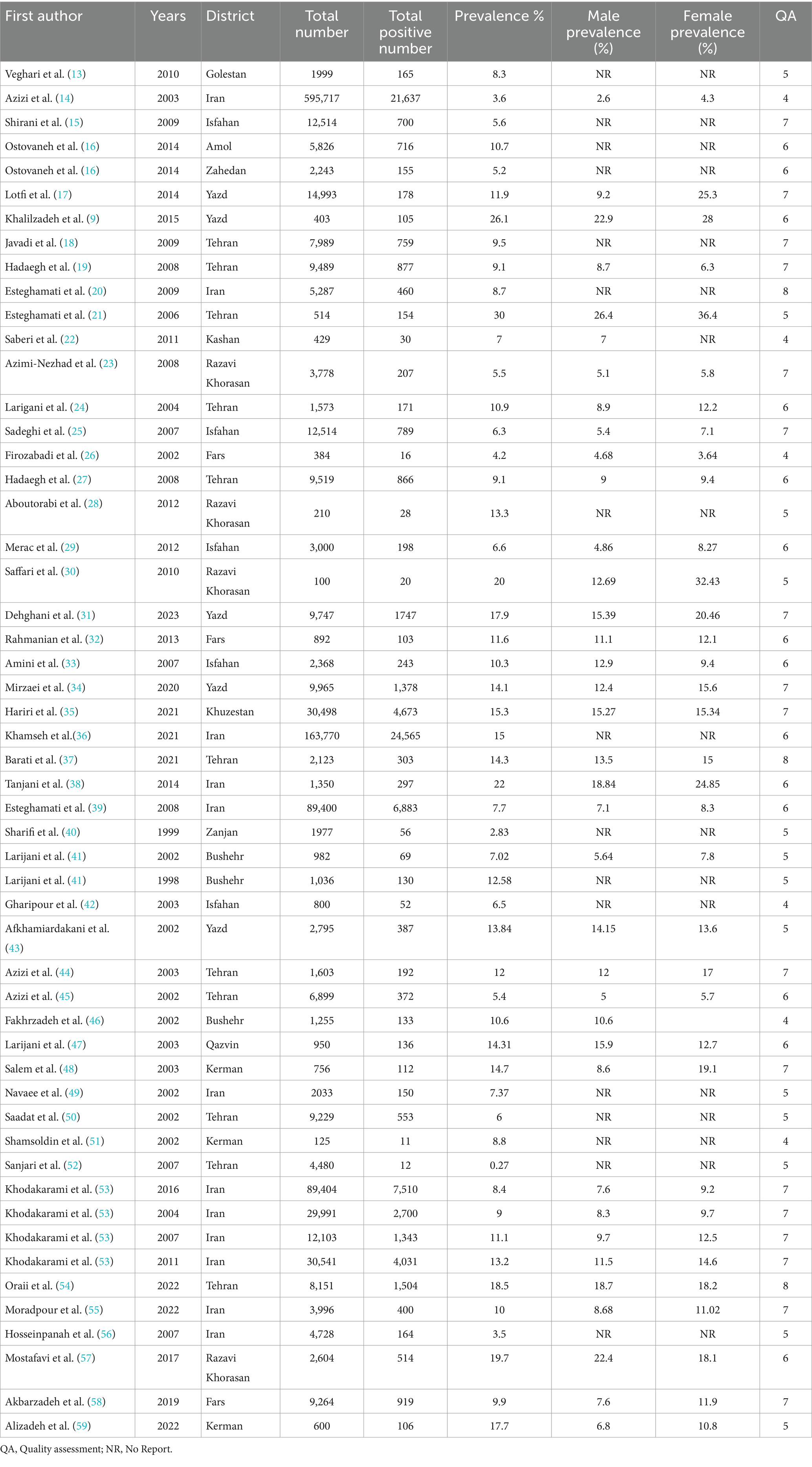
Table 1. Description of the studies included in the meta-analysis.
3.3 Risk of bias in studies
Fifty studies earned a score of 4–7 (moderate risk of bias) based on the quality evaluation score, whereas three studies received an 8–9 (low risk of bias) score (Table 1).
3.4 Results of syntheses
The study includes 53 studies with a total sample size of 1,244,896, of whom 89,979 tested positive for type 2 diabetes. Figure 2 shows that 10.80% (95% CI: 9.05–12.20%) of people have type 2 diabetes. However, there was a lot of statistical heterogeneity among the studies (I2 = 99.8%, Q statistic = 34073.31, df = 52, p < 0.0001, Tau-squared = 0.0024). By eliminating the one-by-one studies technique, we carried out a full sensitivity analysis, and the results showed that no one research had a substantial influence on the prevalence of diabetes; hence, the analysis did not allow us to discover any important studies in this regard (Table 2).
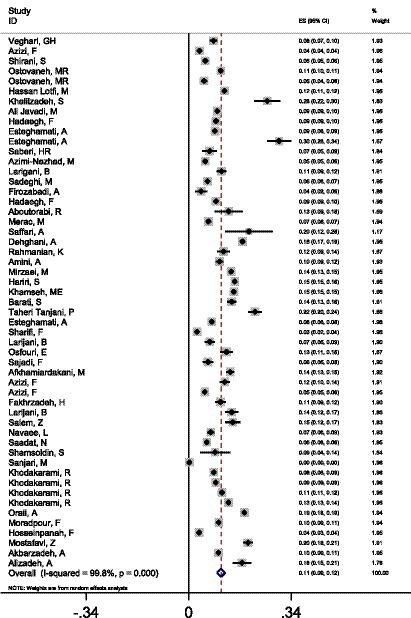
Figure 2. Forest plot analysis of diabetes prevalence in Iran, 1998–2023.
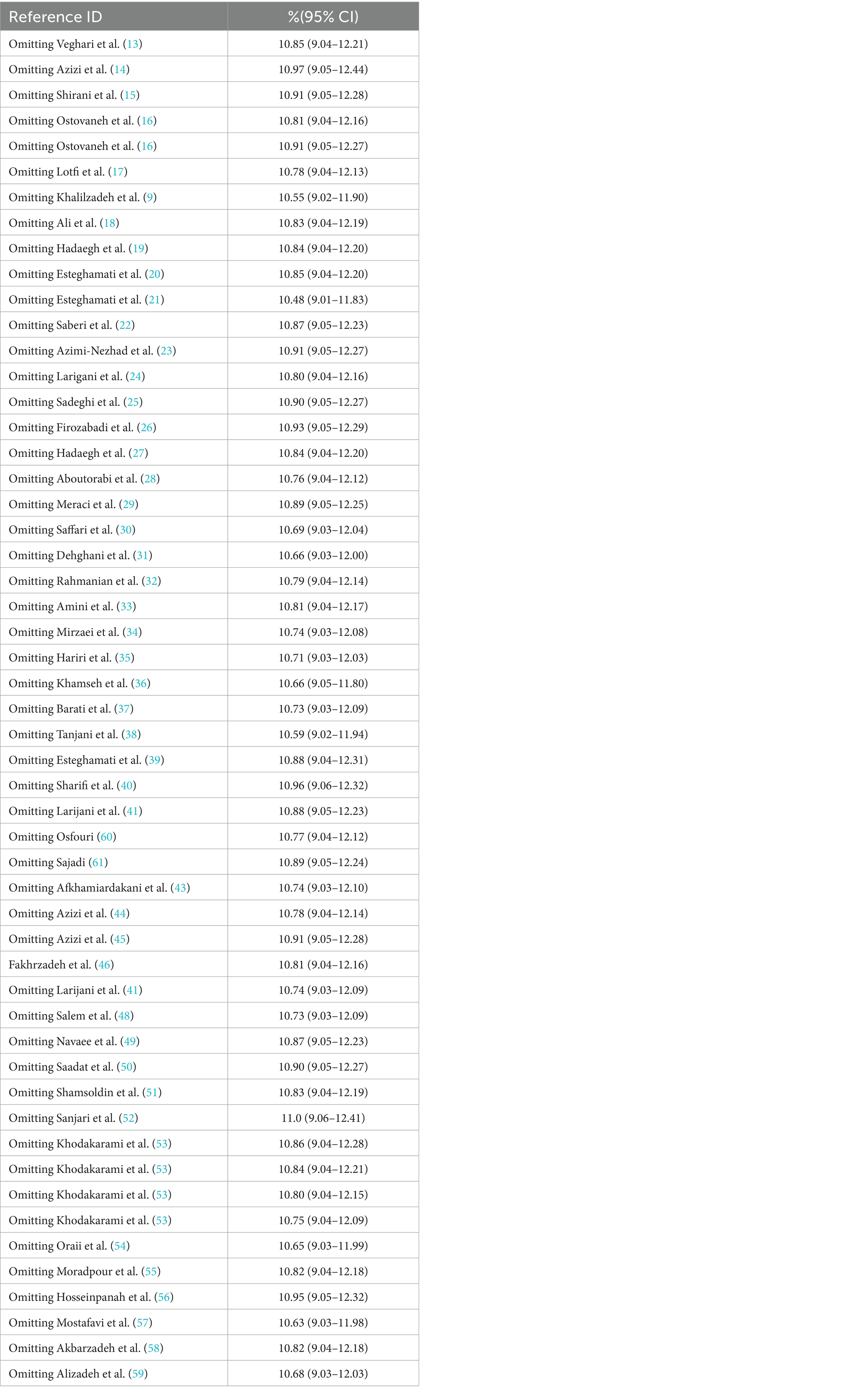
Table 2. Sensitivity analysis by removing one-by-one studies.
Additionally, the prevalence of diabetes was 14.4% (95% CI: 12.2–16.7) for people aged 45 to 55, 21.7% (95% CI: 17.5–25.0) for people aged 55 to 65, and 21.2% (95% CI: 10.7–31.7) for those aged 65 and above.
The prevalence of diabetes was also found to be related with obesity, with estimates of 8.4% (95% CI: 5–11.7), 12.4% (95% CI: 8.04–16.4), 17.4% (95% CI: 11.3–23.6), and 19% (95% CI: 7.2–30.2) in adults with a BMI of 18.5–24.9, 25–29.9, 30–34.9, and 35–39.9, respectively.
Moreover, there has been a notable rise in the incidence of diabetes throughout the last quarter-century. The prevalence of diabetes was assessed for five different time periods: 1988–2002, 2003–2007, 2008–2012, 2013–2017, and 2018–2023. The estimated prevalence rates for these years were 7.08% (95% CI: 5.09–9.06), 9.05% (95% CI: 7.08–11.10), 9.14% (95% CI: 8.36–9.91), 15.0% (95% CI: 11.40–18.60), and 13.40% (95% CI: 11.40–15.30), respectively (Table 3).
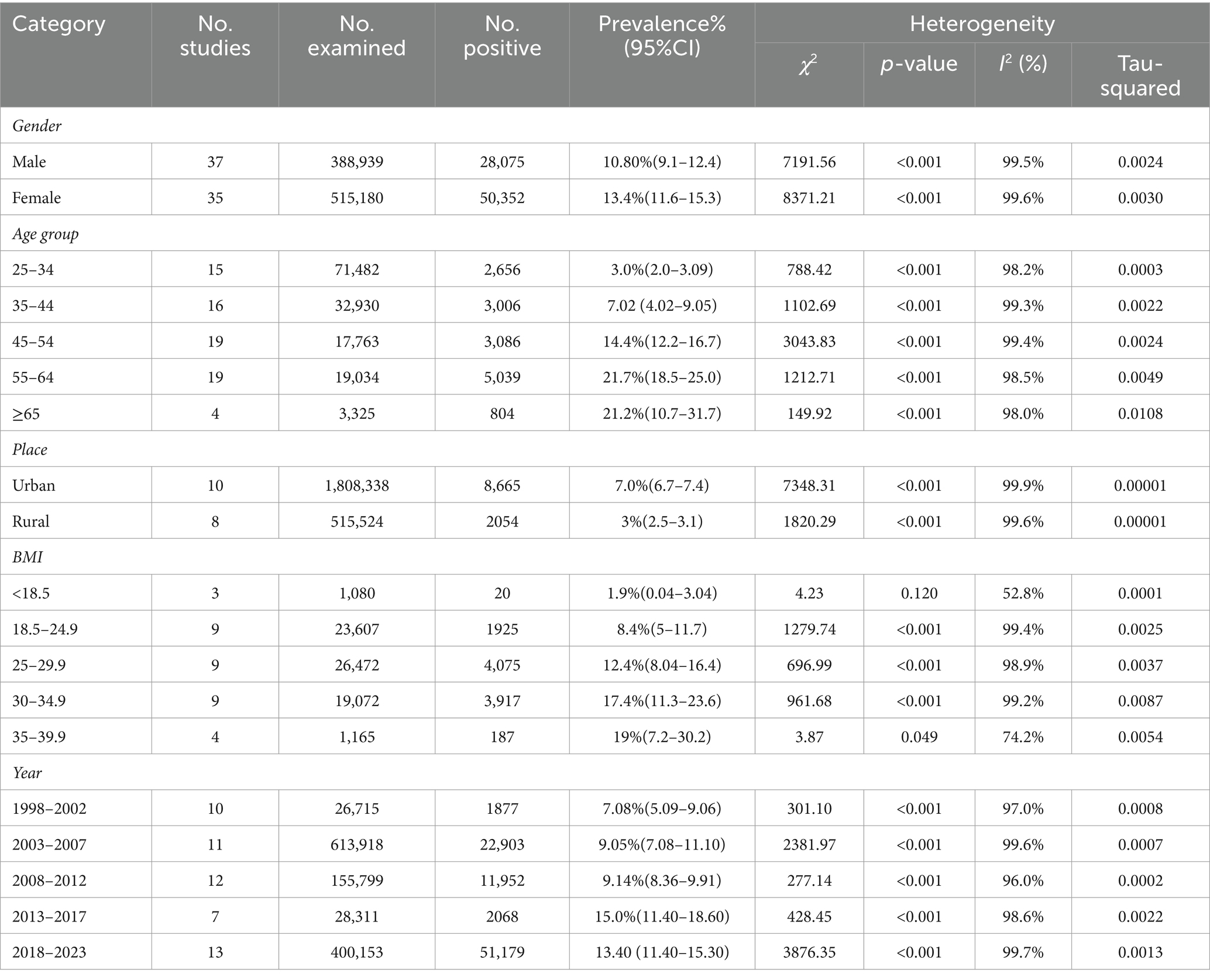
Table 3. Subgroup analysis of the prevalence of Diabetes in Iran, 1998–2023.
According to the findings of the subgroup analysis, it was seen that Khuzestan exhibited the greatest prevalence of type 2 diabetes, with a rate of 15.3%. This was closely followed by Razavi Khorasan, Qazvin, and Yazd, which reported rates of 14.4, 14.3, and 12.6%, respectively. The province of Mazandaran had a somewhat reduced incidence rate of 10.7%. In contrast, the prevalence rates of type 2 diabetes were comparatively lower in Fars (8.6%), Golestan (8.3%), Bushehr (8.1%), and Tehran (7.5%) among the population under study (Figure 3).
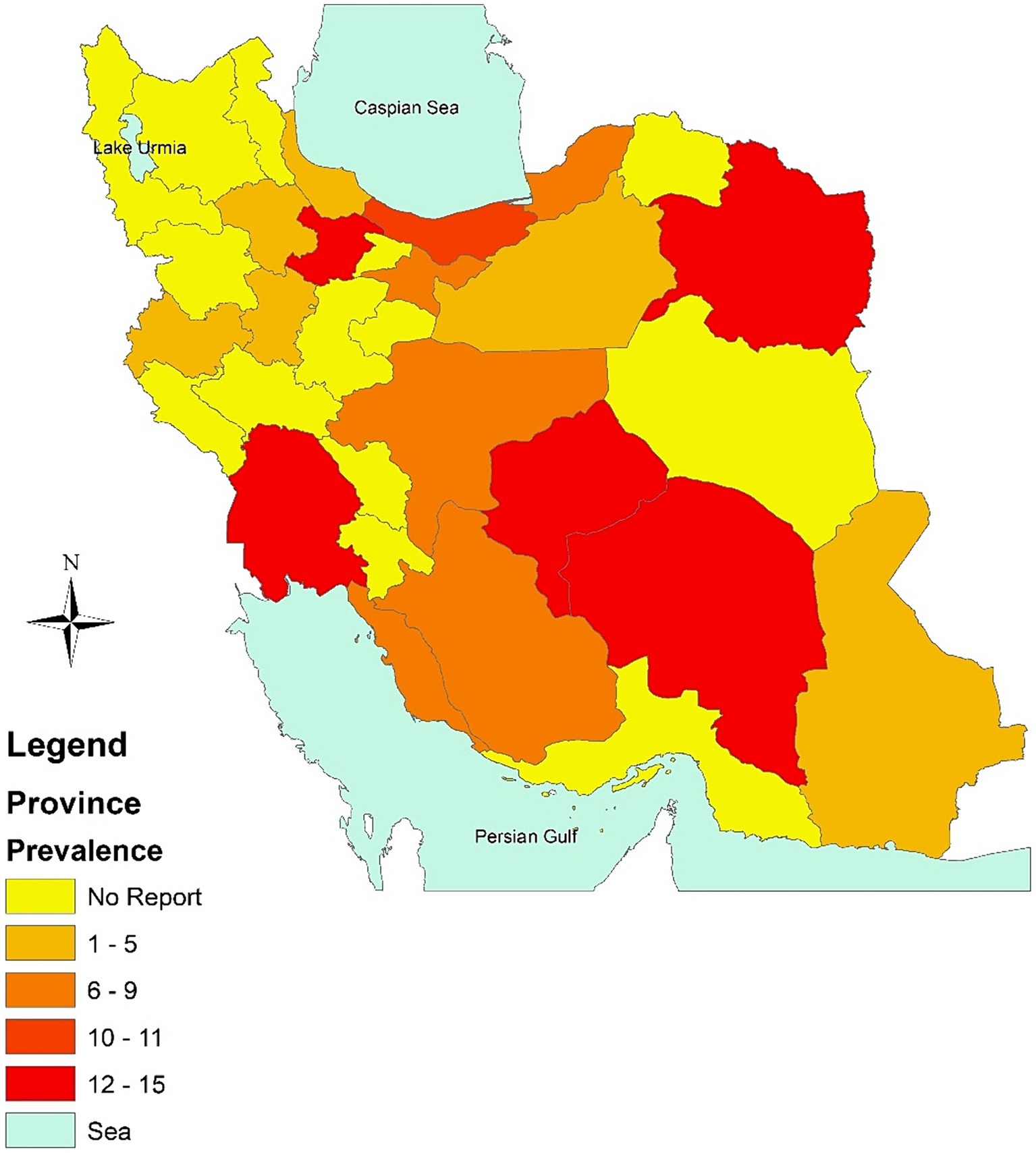
Figure 3. Prevalence of diabetes in Iran, 1998–2023 based on Province.
Univariate meta-regression was used to look into the causes of heterogeneity. According to the meta-regression analysis’s findings, a number of factors, including province (B = –0.005, P0.001), year (B = 0.0050, p = 0.020), gender (B = 0.0060, p = 0.022), age group (B = 0.164, p = 0.039), and BMI (B = 0.1174, p = 0.017), may be sources of heterogeneity (Table 4). The findings of the subgroup analysis showed that the prevalence of diabetes was 13.4% in women and 10.80% in men (95% confidence interval [CI]: 9.1–12.4).
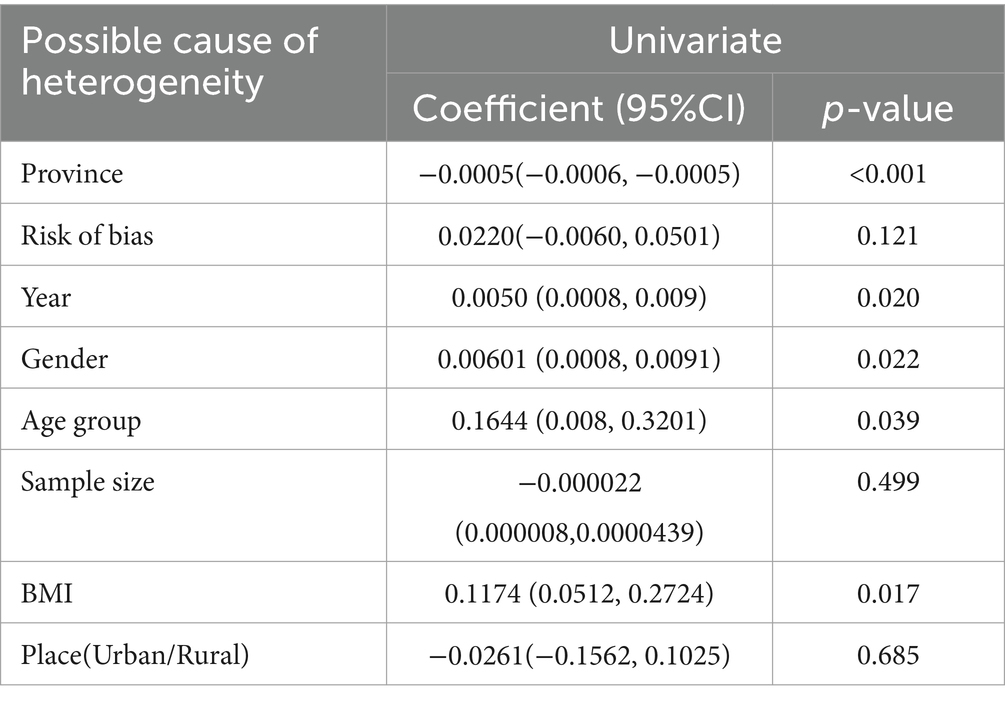
Table 4. Results of meta-regression analyses for identifying potential contributors to heterogeneity among studies in the meta-analysis.
In addition, the use of cumulative meta-analysis was applied to examine the pattern of changes in the prevalence of diabetes over a certain period. The findings of the cumulative meta-analysis demonstrate a progressive rise in the incidence of diabetes over a period of time (Figure 4).
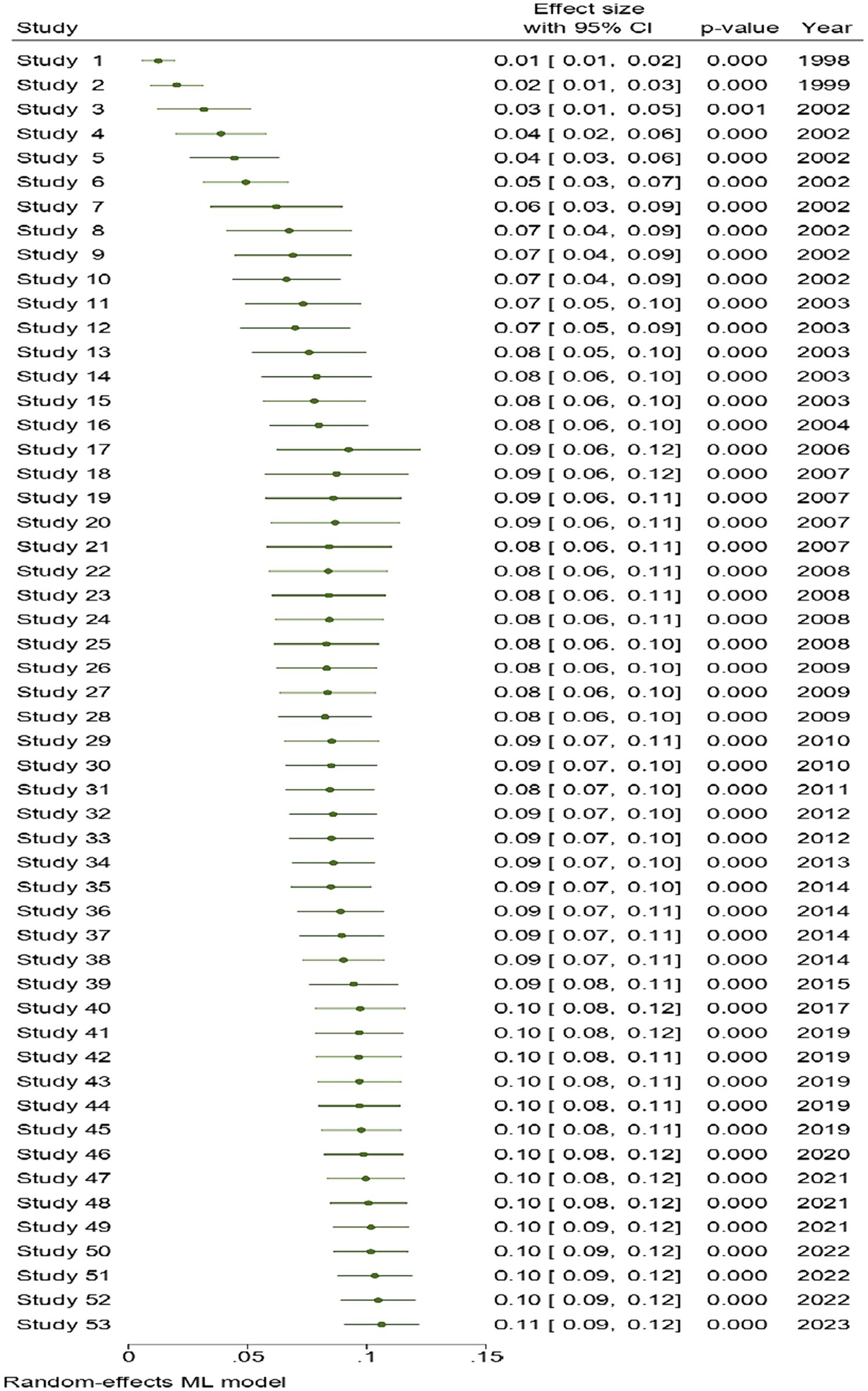
Figure 4. Cumulative meta-analysis results for examining the trend of changes in diabetes prevalence over time.
3.5 Reporting publication biases
Significant publication bias was found in the articles included in this meta-analysis, according to the findings of Egger’s regression test and asymmetry in the funnel plot (bias = 14.65, 95% CI: 7.37–21.92, p = 0.001) (Figure 5). This bias was corrected using a non-parametric Trim-and-fill model, which predicted that three potential studies on the prevalence of diabetes were left out of the meta-analysis. The estimated pooled prevalence of diabetes using this model, adjusted for random effects, was 10.2% (95% CI: 8.09–11.5) (Table 5).
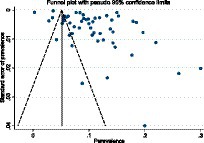
Figure. 5. Funnel plot with pseudo 95% confidence interval limits for the detection of publication bias.
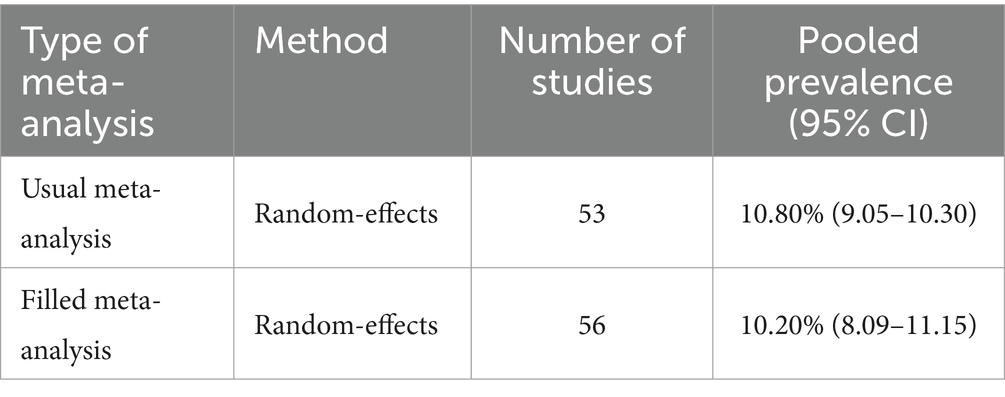
Table 5. Comparison of common and corrected meta-analysis results for publication bias.
4 Discussion
Between 1996 and 2023, every published study on the prevalence of type 2 diabetes among people in Iran was comprehensively reviewed. In this research, an effort was undertaken to extract the updated prevalence till 2023 for use by policymakers since a meta-analysis had previously published the pooled prevalence of diabetes from 1996 to 2004 (8).
The combined prevalence of diabetes among Iranians over 25 years old was 10.80% (95% CI: 9.05–12.20%), according to the findings of the current research. In other words, 1 in 10 adults over the age of 25 has diabetes. This figure was lower than that of Pakistan (14.62%) (62) and Afghanistan (12.13%) (63), two adjacent nations with comparable cultures, and higher than that of Nepal (8.4%) (64) and Bangladesh (7.8%) (65) in Africa. The lower age limit of participants in Nepal and Bangladesh (over 15 in Nepal and over 20 in Bangladesh) may partially account for the higher aggregated prevalence in Iran compared to Nepal and Bangladesh. However, the reasons for the lower prevalence of diabetes in Iran compared to Pakistan and Afghanistan with a comparable age range are unclear and may be attributable to differences in the age distribution, demographic characteristics, and lifestyle of the population. It is crucial to acknowledge that the observed differences in prevalence among these countries might be influenced by various factors, including differences in study methodologies, sample sizes, and population demographics. Therefore, a more detailed examination of these factors is needed to establish robust comparisons. Future research could delve deeper into the specific methodologies employed in each country, diagnostic criteria, and sampling techniques, as well as considering the age distribution and lifestyle factors, to provide a more comprehensive understanding of the observed variations.
The prevalence of type 2 diabetes in Iran was estimated to be 9.34% based on individual studies published between 1996 and 2004 and in persons over the age of 18 according to a meta-analysis (8). As an addendum to the aforementioned study, the prevalence of diabetes in adults aged 25 and older was estimated to be 10.8% in the present study. Moreover, subgroup analysis by publication year revealed that the five-year prevalence of diabetes was 7.08 (1998–2002), 9.05 (2003–2007), 9.14 (2008–2012), 15, and 13.4 (2018–2023). Upon closer analysis, we identified several factors that may contribute to the observed increase. Firstly, our data encompass various time periods, each representing distinct stages of diabetes awareness, screening, and diagnostic capabilities in Iran. The initiation of the National Diabetes Screening Program in 2006, coupled with advancements in detection and diagnosis, may have led to an increased identification of previously undiagnosed cases. To provide a more comprehensive perspective, the findings of a 2022 study based on data from the four periods of the national STEPs study, the prevalence of diabetes among adults aged 25–65 in 2004, 2007, 2011, and 2016 was 8.4, 11.1, and 13.2 percent, respectively (53). Consequently, it appears that the prevalence of diabetes in Iran has fluctuated over the past few years. The factors behind the rise of diabetes throughout time are complicated and multifaceted. One of them is the aging population, and as people live longer and age, diabetes will certainly afflict them more frequently (66). Additionally, lifestyle changes and an aging population are acknowledged contributors to the rising prevalence of diabetes. As people live longer and age, the likelihood of developing diabetes increases. According to some data, Iran’s population of people aged 60 and older will reach 20% in 2050 (67), exceeding 10% in 2022 (67). Moreover, the Iranian population has experienced an upsurge in diabetes risk factors such as obesity, sedentary behavior, and unhealthy dietary patterns (68–70).
As a result of steady advancements in diabetes detection and diagnosis over the years in Iran, the percentage of undiagnosed diabetes decreased from 45.7 to 24.7% during a period of seven years (71). As a result, it seems that the observed increase in the cumulative prevalence of diabetes over time in the current research is rather accurate.
The subgroup analysis reveals significant differences in the prevalence rates among provinces, with Khuzestan exhibiting the highest rate at 15.3%. The closely following rates in Razavi Khorasan, Qazvin, and Yazd, as well as the comparatively lower rates in Mazandaran, Fars, Golestan, Bushehr, and Tehran, offer insights into the geographical distribution of type 2 diabetes in Iran. One plausible explanation for the disparities in diabetes prevalence among provinces could be lifestyle differences. Variations in dietary habits, physical activity levels, and cultural practices may influence the prevalence of risk factors for type 2 diabetes. Future studies exploring the relationship between lifestyle factors and diabetes prevalence in specific regions could provide valuable insights. The socio-economic landscape of each province may also play a pivotal role. Disparities in income, education levels, and access to healthcare services can contribute to variations in diabetes prevalence. Furthermore, Differences in regional health policies and healthcare infrastructure might contribute to variations in diabetes prevalence. Assessing the effectiveness of existing health programs, accessibility of healthcare services, and the implementation of preventive measures could shed light on the impact of regional health policies on diabetes prevalence.
The subgroup analysis revealed an association between overweight obesity and diabetes. The prevalence of diabetes increases dramatically as body mass index (BMI) rises, so the prevalence of diabetes among those with a BMI between 35 and 39.9 was ten times that of those with a BMI below 18.5. The research performed on the association between diabetes and obesity demonstrates that overweight and obesity, especially when accompanied by abdominal obesity, is a significant risk factor for diabetes and prediabetes due to beta cell dysfunction and insulin resistance via three mechanisms (72): Increase in the production of cytokines such as tumor necrosis factor-alpha, resulting in a decrease in adiponectin (73); Misplaced deposition of lipids in the liver (74); and Mislocalization of lipids in the available research indicates that there has been a notable rise in the prevalence of obesity in Iran from 1990 to 2016, with a threefold increase seen over this time span. Furthermore, concomitant with the rise in population size and the increase in body mass index (BMI), there has been a nearly 11-fold surge in the prevalence of obesity throughout this timeframe (68). Furthermore, the findings of the STEPS research, which was done in 2016 on individuals aged 18 and above at a national level, yielded an estimated prevalence of 36.6% for overweight and 22.7% for obesity (75). In the meanwhile, a meta-analysis on the prevalence of overweight and obesity in Middle Eastern nations from 2000 to 2020 found that the prevalence of overweight was 33.92, and the prevalence of obesity was 22.41 (76). Adequate policies should be established to minimize these variables in the Iranian population to lower the incidence of type 2 diabetes, given the substantial prevalence and trend of overweight and obesity in Iran as a key risk factor for the disease. Implementing a robust public health strategy is essential to combat the escalating prevalence of obesity and mitigate the associated risks, particularly in reducing the incidence of type 2 diabetes among the Iranian population. This multifaceted approach includes launching culturally relevant public awareness campaigns to educate the public about the risks of obesity and its direct link to diabetes. Simultaneously, comprehensive and accessible nutritional education programs are crucial, focusing on balanced nutrition and the benefits of a healthy diet. To counteract sedentary lifestyles, initiatives promoting regular physical activity at community and workplace levels should be developed and incentivized. Widespread access to healthcare services, with a focus on preventative care for early detection and management of obesity-related conditions, is paramount. Advocacy for evidence-based policies, including regulations on food marketing, urban planning encouraging physical activity, and workplace wellness programs, is essential.
According to the findings of the current research, those aged 55 to 64 had a seven-fold higher incidence of diabetes than those aged 25 to 34. The age-specific prevalence in the 55 and older age group was found to be more than double that of those between the ages of 25 and 34 in a meta-analysis carried out in Afghanistan (63), a country next to Iran. Another Malaysian meta-analysis found that adults 60 years and older had a greater than tenfold increased risk of developing diabetes than those between the ages of 20 and 29 (77). There is no proof that the association between age and diabetes is inverse or nonexistent. As a result, it seems that the prevalence of diabetes rises with age across the board (78). Age-related physiological changes may have an impact on the prevalence of diabetes. Diabetes rates rise as people become older because of insulin resistance in the skeletal muscles brought on by changes in adiposity and physical inactivity on the one hand (79) and reduced secretory capacity and loss or malfunction of pancreatic beta cells on the other (80). Moreover, acknowledging the potential influence of lifestyle factors and healthcare access in different age groups is essential. Exploring the impact of dietary habits, physical activity levels, and healthcare-seeking behavior on diabetes prevalence within distinct age brackets would offer valuable insights.
In this research, women had a greater prevalence of diabetes [13.4 percent (11.6–15.3)] than males (10.80%, 9.1–12.4). Similar studies carried out in nearby nations and nations sharing a similar culture revealed that the prevalence of diabetes was higher in women than in men in some nations, including Turkey (81), Pakistan (62), and Nepal (64), while in Bangladesh the prevalence was slightly higher in men than in women (65). There was no distinction between the sexes in Cameron (82). Although women were more likely to have diabetes than males in the majority of the studies included in this meta-analysis, the situation was reversed in six of them. There may be a number of reasons for the varied frequency in the two genders. Estrogen, a female hormone important for insulin sensitivity and glucose metabolism, is one of these elements. As a result, low estrogen levels, particularly during menopause, might raise insulin resistance and diabetes risk (78). Obesity and way of life are other variables that determine the differing prevalence between the sexes. A Middle Eastern meta-analysis found that women are more likely than males to suffer from general obesity, which is a significant risk factor for developing diabetes (76). Stress, physical inactivity, and a diet high in processed foods and sugar are additional risk factors for type 2 diabetes that are more common in women (83). However, males are more likely to develop visceral fat buildup and abdominal obesity, both of which are risk factors for diabetes (84). In addition to the above indicated elements, gender differences exist in healthcare seeking behavior. Relevant research have shown that males often postpone going to the doctor when they are ill and use the less extensive array of healthcare services (85). Women are more likely than males to seek medical attention when they are unwell, which increases the likelihood that their condition will be discovered (86, 87). Moreover, the impact of cultural expectations and societal norms on gender-specific health behaviors cannot be overlooked. Societal pressures may influence both men and women in distinct ways, affecting their dietary choices, stress levels, and propensity for physical activity. Understanding these cultural dynamics is vital for tailoring effective public health interventions. Additionally, healthcare-seeking behavior disparities between genders may be shaped by socio-cultural factors. Delving into the reasons behind delayed medical visits among men and the more proactive approach of women toward healthcare utilization can provide valuable insights. Cultural perceptions of health, gender roles, and accessibility to healthcare services play pivotal roles in shaping these behaviors. A comprehensive exploration of the synergistic effects of lifestyle, obesity, and healthcare-seeking behavior, embedded within the broader context of cultural and societal influences, will contribute to a more nuanced understanding of gender disparities in diabetes prevalence.
5 Strengths
The following are some of this study’s advantages: First of all, the research includes a large number of studies, totaling 1,244,896 people in the sample. The reliability and generalizability of the results are greatly improved by the size of the sample. Secondly, by expanding the analysis to encompass data through 2023, the research provides a critical update to a prior meta-analysis. More updated information on the incidence of type 2 diabetes in Iran is provided by this extension. Last but not least, using cumulative meta-analysis enables tracing the historical trend in diabetes prevalence, giving important historical context.
6 Limitations
The limitations of the current meta-analysis should be taken into account when interpreting the findings. First, age-specific prevalence was not reported in two-thirds of the papers that made up this meta-analysis. If the contribution of participants under 40 years old in these studies is significant, the prevalence of diabetes in the present study may have been underestimated. The prevalence of diabetes is typically 5–10% in people under the age of 40, and it rises sharply from that age and above. Second, several studies failed to indicate whether individuals with diabetes were diagnosed with type 2 or another kind. Since type 2 diabetes affects more than 90% of diabetes patients, the analyzed condition was referred to as type 2 diabetes in the publications that were included. Third, since there was a significant level of heterogeneity in the current analysis, 99.8 of the variations in the prevalence estimate were due to the heterogeneity across studies rather than chance. Although we used meta-regression to track out its source and subgroup analysis to somewhat lessen its impact, it may still have an impact on the study’s overall estimate and conclusions.
7 Conclusion
In conclusion, our comprehensive meta-analysis spanning the period from 1996 to 2023 reveals a noteworthy estimated prevalence of 10.8% for type 2 diabetes in Iran. This alarming prevalence underscores the urgency of addressing this public health challenge. The observed variations across gender, age groups, and geographic regions emphasize the need for nuanced, targeted interventions. Our findings call for the implementation of proactive measures, including tailored screening programs and lifestyle modification initiatives. Policymakers and healthcare practitioners should take heed of the temporal trends, especially the significant increase from 2013 to 2017, prompting the development of effective strategies to mitigate the future burden on the healthcare system.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number (s) can be found in the article/Supplementary material.
Ethics statement
We diligently adhered to ethical principles for our systematic review and meta-analysis studies throughout this research. The study protocol obtained official approval from the Ethics Committee of Torbat Jam Faculty of Medical Sciences, with the assigned code IR.TRJUMS.REC.1401.004.
Author contributions
NH: Formal analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing. MJ: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Validation, Writing – original draft. NN: Data curation, Investigation, Methodology, Writing – original draft. SH: Data curation, Investigation, Methodology, Software, Writing – original draft. VR: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1322072/full#supplementary-material
Abbreviations
JBI, Joanna Briggs Institute; SID, Scientific Information Database; WHO, World Health Organization; STEPS, Stepwise approach to non-communicable disease risk factor surveillance; CI, Confidence Interval; BMI, Body Mass Index; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
References
1. Zheng, Y, Ley, SH, and Hu, F. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol. (2018) 14:88–98. doi: 10.1038/nrendo.2017.151
2. Psychiatry GMDCJTL. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet Psychiatry. (2022) 9:137–50. doi: 10.1016/S2215-0366(21)00395-3
3. Ogurtsova, K, Guariguata, L, Barengo, NC, Ruiz, PL-D, Sacre, JW, Karuranga, S, et al. IDF diabetes Atlas: Global estimates of undiagnosed diabetes in adults for 2021. Diab Res Clin Pract. (2022) 183:109118. doi: 10.1016/j.diabres.2021.109118
4. Zhou, B, Lu, Y, Hajifathalian, K, Bentham, J, Di Cesare, M, Danaei, G, et al. Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants. Lancet. (2016) 387:1513–30. doi: 10.1016/S0140-6736(16)00618-8
5. ElSayed, NA, Aleppo, G, Aroda, VR, Bannuru, RR, Brown, FM, Bruemmer, D, et al. Classification and diagnosis of diabetes: standards of Care in Diabetes-2023. Diab Rev. (2023) 46:S19–40. doi: 10.2337/dc23-S002
6. Esteghamati, A, Etemad, K, Koohpayehzadeh, J, Abbasi, M, Meysamie, A, Noshad, S, et al. Trends in the prevalence of diabetes and impaired fasting glucose in association with obesity in Iran: 2005–2011. Diabetes Res Clin Pract. (2014) 103:319–27. doi: 10.1016/j.diabres.2013.12.034
7. Ong, KL, Stafford, LK, McLaughlin, SA, Boyko, EJ, Vollset, SE, Smith, AE, et al. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the global burden of disease study 2021. Lancet. (2023) 402:203–34. doi: 10.1016/S0140-6736(23)01301-6
8. Haghdoost, A, Rezazadeh Kermani, M, and Sadghirad, B. Prevalence of type 2 diabetes in the Islamic Republic of Iran: Systematic review and meta-analysis. Baradaran HJE-EMHJ. (2009) 15:591–9.
9. Khalilzadeh, S, Afkhami-Ardekani, M, and Afrand, MJ. High prevalence of type 2 diabetes and pre-diabetes in adult Zoroastrians in Yazd, Iran: a cross-sectional study. Electron Phys. (2015) 7:998. doi: 10.14661/2015.998-1004
10. Rashedi, V, Asadi-Lari, M, Delbari, A, Fadayevatan, R, Borhaninejad, V, Foroughan, MJD, et al. Prevalence of diabetes type 2 in older adults: findings from a large population-based survey in Tehran, Iran (urban HEART-2). Diabetes Metab Syndr. (2017) 11:S347–50. doi: 10.1016/j.dsx.2017.03.014
11. Munn, Z, Moola, S, Lisy, K, Riitano, D, and Tufanaru, C. Systematic reviews of prevalence and incidence. JBI Man Evid Synth. (2020):5.1-5.
12. Borenstein, M, Hedges, LV, Higgins, JP, and Rothstein, HR. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res Synth Methods. (2010) 1:97–111. doi: 10.1002/jrsm.12
13. Veghari, G, Sedaghat, M, Joshaghani, H, Hoseini, SA, Niknezad, F, Angizeh, A, et al. Association between socio-demographic factors and diabetes mellitus in the north of Iran: a population-based study. Int J Diabetes Mell. (2010) 2:154–7. doi: 10.1016/j.ijdm.2010.09.001
14. Azizi, F, Guoya, M, Vazirian, P, Dolatshati, P, and Habbibian, S. Screening for type 2 diabetes in the Iranian national programme: a preliminary report. East Mediterr Health J. (2003) 9:1122–7. doi: 10.26719/2003.9.5-6.1122
15. Shirani, S, Kelishadi, R, Sarrafzadegan, N, Khosravi, A, Sadri, G, Amani, A, et al. Awareness, treatment and control of hypertension, dyslipidaemia and diabetes mellitus in an Iranian population: the IHHP study. East Mediterr Health J. (2009) 15:1455–63.
16. Ostovaneh, MR, Zamani, F, Sharafkhah, M, Ansari-Moghaddam, A, Khaleghi, NA, Saeedian, FS, et al. Prevalence of metabolic syndrome in Amol and Zahedan, Iran: a population based study. Arch Iran Med. (2014) 17:477–82.
17. Lotfi, MH, Saadati, H, and Afzali, G. Prevalence of diabetes in people aged≥ 30 years: the results of screen-ing program of Yazd Province, Iran, in 2012. J Res Health Sci. (2013) 14:88–92.
18. Javadi, MA, Katibeh, M, Rafati, N, Dehghan, MH, Zayeri, F, Yaseri, M, et al. Prevalence of diabetic retinopathy in Tehran province: a population-based study. BMC Ophthalmol. (2009) 9:1–8. doi: 10.1186/1471-2415-9-12
19. Hadaegh, F, Bozorgmanesh, MR, Ghasemi, A, Harati, H, Saadat, N, and Azizi, F. High prevalence of undiagnosed diabetes and abnormal glucose tolerance in the Iranian urban population: Tehran lipid and glucose study. BMC Int Health Hum Rights. (2008) 8:1–7. doi: 10.1186/1471-2458-8-176
20. Esteghamati, A, Meysamie, A, Khalilzadeh, O, Rashidi, A, Haghazali, M, Asgari, F, et al. Third national surveillance of risk factors of non-communicable diseases (SuRFNCD-2007) in Iran: methods and results on prevalence of diabetes, hypertension, obesity, central obesity, and dyslipidemia. BMC Public Health. (2009) 9:1–10. doi: 10.1186/1471-2458-9-167
21. Esteghamati, A, Abbasi, M, Nakhjavani, M, Yousefizadeh, A, Basa, AP, and Afshar, HJCD. Prevalence of diabetes and other cardiovascular risk factors in an Iranian population with acute coronary syndrome. Cardiovasc Diabetol. (2006) 5:1–6. doi: 10.1186/1475-2840-5-15
22. Saberi, HR, Moravveji, AR, Fakharian, E, Kashani, MM, and Dehdashti, ARJD. Prevalence of metabolic syndrome in bus and truck drivers in Kashan, Iran. Diabetol Metab Syndr. (2011) 3:1–5. doi: 10.1186/1758-5996-3-8
23. Azimi-Nezhad, M, Ghayour-Mobarhan, M, Parizadeh, M, Safarian, M, Esmaeili, H, Parizadeh, S, et al. Prevalence of type 2 diabetes mellitus in Iran and its relationship with gender, urbanisation, education, marital status and occupation. Singapore Med J. (2008) 49:571.
24. Ardeshir Larijani, MB, Mortaz Hejri, S, Pourabrahim, R, Nouri, M, Hashem, R, Shushtari Zadeh, P, et al. Prevalence of type 2 diabetes and impaired fasting glucose (IFG) in the population aged 25-64 years residing in the population research center of Tehran University of Medical Sciences. Iran J Diab Metab. (2008) 1:49–52.
25. Sadeghi, M, Roohafza, H, Shirani, S, Poormoghadas, M, Kelishadi, R, Baghaii, A, et al. Diabetes and associated cardiovascular risk factors in Iran: the Isfahan Healthy Heart Programme. Ann Acad Med Singap. (2007) 36:175.
26. Firouzabadi, A, and Momen, T. Prevalence of diabetes in hospitalized patients with bipolar disorder. Ideas Behav. (2002) 8:2–6.
27. Hadaegh, FBM, Harati, H, Saadat, N, and Azizi, F. High prevalence of diabetes and abnormal glucose tolerance in urban Iranians aged over 20 years: determining an effective screening strategy for un-diagnosed diabetes. Iran J Endocrinol Metabol. (2008) 9:384–91.
28. Aboutorabi, RAH, Rajabian, R, Golshan, A, and Shakeri, H. Study of diabetes in patients with urinary tract stones. J North Khorasan Univ Med Sci. (2012) 4:139–44. doi: 10.29252/jnkums.4.2.139
29. Mohammadreza Meraci, AF, and Nejad, MB. Investigating the prevalence of high blood pressure, type 2 diabetes mellitus and related risk factors according to a large general study in Isfahan-using multivariate logistic regression model. J Health Syst Res. (2012) 8:193–203.
30. Safaari, A, Saboori, SH, Hanieh, H, and Moshakat, M. Comparison of the prevalence of diabetes and its influencing factors in patients with cirrhosis compared to the general population. J Med Sci Islamic Azad Univ Mashhad. (2010) 4:259–66.
31. Dehghani, A, Korozhdehi, H, Hossein Khalilzadeh, S, Fallahzadeh, H, and Rahmanian, VJ. Prevalence of diabetes and its correlates among Iranian adults: Results of the first phase of Shahedieh cohort study. Health Sci Rep. (2023) 6:e1170. doi: 10.1002/hsr2.1170
32. Rahmanian, K, Shojaei, M, and Jahromi, AS. Relation of type 2 diabetes mellitus with gender, education, and marital status in an Iranian urban population. Rep Biochem Mol Biol. (2013) 1:–64.
33. Amini, M, and Janghorbani, M. Diabetes and impaired glucose regulation in first-degree relatives of patients with type 2 diabetes in Isfahan, Iran: prevalence and risk factors. Rev Diabet Stud. (2007) 4:169–76. doi: 10.1900/RDS.2007.4.169
34. Mirzaei, M, Rahmaninan, M, Mirzaei, M, Nadjarzadeh, A, and Dehghani tafti, AA. Epidemiology of diabetes mellitus, pre-diabetes, undiagnosed and uncontrolled diabetes in Central Iran: results from Yazd health study. BMC Int Health Hum Rights. (2020) 20:1–9. doi: 10.1186/s12889-020-8267-y
35. Hariri, S, Rahimi, Z, Hashemi-Madani, N, Mard, SA, Hashemi, F, Mohammadi, Z, et al. Prevalence and determinants of diabetes and prediabetes in southwestern Iran: the Khuzestan comprehensive health study (KCHS). BMC Endocr Disord. (2021) 21:1–11. doi: 10.1186/s12902-021-00790-x
36. Khamseh, ME, Sepanlou, SG, Hashemi-Madani, N, Joukar, F, Mehrparvar, AH, Faramarzi, E, et al. Nationwide prevalence of diabetes and prediabetes and associated risk factors among Iranian adults: analysis of data from PERSIAN cohort study. Diabetes Ther. (2021) 12:2921–38. doi: 10.1007/s13300-021-01152-5
37. Barati, S, Sadeghipour, P, Ghaemmaghami, Z, Mohebbi, B, Baay, M, Alemzadeh-Ansari, MJ, et al. Warning signals of elevated prediabetes prevalence in the modern Iranian urban population. Prim Care Diabetes. (2021) 15:472–9. doi: 10.1016/j.pcd.2021.04.002
38. Tanjani, PT, Moradinazar, M, Mottlagh, ME, and Najafi, F. The prevalence of diabetes mellitus (DM) type II among Iranian elderly population and its association with other age-related diseases, 2012. Ann Gerontol Geriatr. (2015) 60:373–9. doi: 10.1016/j.archger.2014.11.012
39. Esteghamati, A, Gouya, MM, Abbasi, M, Delavari, A, Alikhani, S, Alaedini, F, et al. Prevalence of diabetes and impaired fasting glucose in the adult population of Iran: National Survey of Risk Factors for Non-Communicable Diseases of Iran. BMC Endirol Disord. (2008) 31:96–8. doi: 10.2337/dc07-0959
40. Sharifi, F, Aghaei, M, Derakhshandeh, J, and Jabbari, Y. Study of the status of glucose tolerance test in individuals over 30 years old in rural areas of Zanjan province. J Adv Med Biomed Res. (1999) 36:4–8.
41. Larijani, B, and Osfouri, E. Prevalence of type 2 diabetes and impaired glucose tolerance in individuals aged 30-64 years in Bushehr city based on the criteria of the World Health Organization and the American Diabetes Association. Iran J Diab Metab. (2002) 1:119–22.
42. Gharipour, M, Mohammadifard, N, Asgary, S, and Naderi, G. The prevalence of obesity and cardiovascular risk factors in Isfahan. Sci Inform Datab. (2003) 7:53–64.
43. Ardakani, MA, Vahidi, S, Vahidi, A, and Ahmadiyeh, MH. Epidemiological indicators of diabetes in adults aged 30 years and older in the city of Yazd province. J Shahid Sadoughi Univ Med Sci. (2002) 9:1–8.
44. Azizi, F, Emami, H, Salehi, P, Ghanbarian, A, Mirmiran, P, Mirbolooki, M, et al. Cardiovascular risk factors in the elderly: THE Tehran Lipid and Glucose study. J Cardiovasc Risk. (2003) 10:65–73. doi: 10.1177/174182670301000111
45. Azizi, F, Saadat, N, Salehi, P, and Emami, H. Association of glucose intolerance with blood pressure indicators, body mass index, and waist-to-hip ratio in the urban population of Tehran. Iran J Endocrinol Metab. (2002) 3:247–56.
46. Fakhrazadeh, H, Faridnia, P, Mohaqeq, M, Pour-Ebrahim, R, and Nouri, M. Lipid and glucose metabolism disorders in employees of Khark Island oil industry. Iranian journal of. Diabetes Metab. (2002) 1:125–31.
47. Maleckzadeh, H, Pazhouhi, M, Samavat, T, Hojatzadeh, A, Ghasemi, A, Baradar, JR, et al. Prevalence of diabetes mellitus & impaired glucose tolerance of population aged over 25 in Qazvin. J Qazvin Univ Med Sci. (2003) 7:41–5.
48. Salem, Z, Nashat, A, Bagherian, K, Sheikh-Fathollahi, M, and Sajjadi, MA. Prevalence of type 2 diabetes in the population over 30 years old in Rafsanjan city. J Rafsanjan Univ Med Sci. (2003) 3:11–7.
49. Sadghi, M, Roohafza, H, Asgary, S, Sadry, G, Bahonar, A, Amani, A, et al. Prevalence of high blood pressure and its relation with cardiovascular risk factors. J Hum Hypertens. (2003) 7:46–52.
50. Saadat, N, Emami, H, Salehi, P, and Azizi, F. Comparison of ADA and WHO criteria for diagnosing metabolic disorders in the Tehran urban population: Tehran lipid and glucose study. Iran J Endocrinol Metab. (2002) 4:1–8.
51. Shamsaldini, S, and Saberi, S. Prevalence of diabetes and impaired glucose tolerance in patients with vitiligo in Kerman city. Avicenna J Clin Med. (2002) 8
52. Sanjari, M, Hedayati, M, and Azizi, F. Prevalence of type 2 diabetes mellitus in 3–19 age group in east of Tehran in 2001. Iran J Endocroniol Metab. (2004) 6:119–26.
53. Khodakarami, R, Abdi, Z, Ahmadnezhad, E, Sheidaei, A, and Asadi-Lari, MJ. Prevalence, awareness, treatment and control of diabetes among Iranian population: results of four national cross-sectional STEPwise approach to surveillance surveys. BMC Int Health Hum Rights. (2022) 22:1216. doi: 10.1186/s12889-022-13627-6
54. Oraii, A, Shafiee, A, Jalali, A, Alaeddini, F, Saadat, S, Masoudkabir, F, et al. Prevalence, awareness, treatment, and control of type 2 diabetes mellitus among the adult residents of Tehran: Tehran cohort study. BMC Endocr Didord. (2022) 22. doi: 10.1186/s12902-022-01161-w
55. Moradpour, F, Rezaei, S, Piroozi, B, Moradi, G, Moradi, Y, Piri, N, et al. Prevalence of prediabetes, diabetes, diabetes awareness, treatment, and its socioeconomic inequality in west of Iran. Sci Rep. (2022) 12:17892. doi: 10.1038/s41598-022-22779-9
56. Hosseinpanah, F, Rambod, M, Sarvghadi, F, Tohidi, M, Hedayati, M, Azizi, F, et al. Population attributable risk for diabetes associated to obesity in Iranian adults. BMC Public Health. (2007) 9:91–7.
57. Mostafavi, Z, and Mostafavian, Z. Prevalence of diabetes type 2 and relationship of it with anthropometric measures in urban population of Mashhad during 2011–2013. Health Sci Rep. (2015) 6:e1170
58. Akbarzadeh, A, Salehi, A, Vardanjani, HM, Poustchi, H, Gandomkar, A, Fattahi, MR, et al. Epidemiology of adult diabetes mellitus and its correlates in pars cohort study in Southern Iran. Arch Iran Med. (2019) 22:633–9.
59. Alizadeh, A, Danesh, P, Maleki, A, and Javaheri, F. Gender differences in incidence of type 2 diabetes and related psychosocial factors. J Commun Health Res. (2022) 11:117–25. doi: 10.18502/jchr.v11i2.10000
60. Osfouri, E. [Diabetes mellitus and impaired glucose tolerance (IGT) in 30–64 years old population of Booshehr Harbor]. Tebb-e-Jonoob [South Medicine Journal], (1998) 3:209–16 [In Farsi].
61. Sajadi, F. [Prevalence of type II diabetes mellitus and its association with cardiovascular risk factors in Isfahan population]. Journal of Isfahan University of Medical Sciences, (2003) 46:68–73 [In Farsi].
62. Akhtar, S, Nasir, JA, Abbas, T, and Sarwar, A. Diabetes in Pakistan: a systematic review and meta-analysis. Pak J Med Sci. (2019) 35:1173–8. doi: 10.12669/pjms.35.4.194
63. Akhtar, S, Nasir, JA, Javed, A, Saleem, M, Sajjad, S, Khan, M, et al. The prevalence of diabetes in Afghanistan: a systematic review and meta-analysis. BMC Public Health. (2021) 21:941. doi: 10.1186/s12889-021-10993-5
64. Gyawali, B, Sharma, R, Neupane, D, Mishra, SR, van Teijlingen, E, and Kallestrup, P. Prevalence of type 2 diabetes in Nepal: a systematic review and meta-analysis from 2000 to 2014. Glob Health Action. (2015) 8:29088. doi: 10.3402/gha.v8.29088
65. Akhtar, S, Nasir, JA, Sarwar, A, Nasr, N, Javed, A, Majeed, R, et al. Prevalence of diabetes and pre-diabetes in Bangladesh: a systematic review and meta-analysis. BMJ Open. (2020) 10:e036086. doi: 10.1136/bmjopen-2019-036086
66. Bansal, N, Dhaliwal, R, and Weinstock, RS. Management of diabetes in the elderly. Med Clin North Am. (2015) 99:351–77. doi: 10.1016/j.mcna.2014.11.008
67. Doshmangir, L, Khabiri, R, and Gordeev, VS. Policies to address the impact of an ageing population in Iran. Lancet. (2023) 401:1078. doi: 10.1016/S0140-6736(23)00179-4
68. Djalalinia, S, Mehdipour, P, Mohajer, B, Mohebi, F, Larijani, B, Sepanlou, SG, et al. Levels and trends of BMI, obesity, and overweight at national and sub-national levels in Iran from 1990 to 2016; a comprehensive pooled analysis of half a million individuals. Arch Iran Med. (2021) 24:344–53. doi: 10.34172/aim.2021.51
69. Mohebi, F, Mohajer, B, Yoosefi, M, Sheidaei, A, Zokaei, H, Damerchilu, B, et al. Physical activity profile of the Iranian population: STEPS survey, 2016. BMC Public Health. (2019) 19:1266. doi: 10.1186/s12889-019-7592-5
70. Ghassemi, H, Harrison, G, and Mohammad, K. An accelerated nutrition transition in Iran. Public Health Nutr. (2002) 5:149–55. doi: 10.1079/PHN2001287
71. Noshad, S, Afarideh, M, Heidari, B, Mechanick, JI, and Esteghamati, A. Diabetes Care in Iran: where we stand and where we are headed. Ann Glob Health. (2015) 81:839–50. doi: 10.1016/j.aogh.2015.10.003
72. Klein, S, Gastaldelli, A, Yki-Järvinen, H, and Scherer, PE. Why does obesity cause diabetes? Cell Metab. (2022) 34:11–20. doi: 10.1016/j.cmet.2021.12.012
73. Deng, Y, and Scherer, PE. Adipokines as novel biomarkers and regulators of the metabolic syndrome. Ann N Y Acad Sci. (2010) 1212:E1–e19. doi: 10.1111/j.1749-6632.2010.05875.x
74. Larson-Meyer, DE, Newcomer, BR, Ravussin, E, Volaufova, J, Bennett, B, Chalew, S, et al. Intrahepatic and intramyocellular lipids are determinants of insulin resistance in prepubertal children. Diabetologia. (2011) 54:869–75. doi: 10.1007/s00125-010-2022-3
75. Djalalinia, S, Saeedi Moghaddam, S, Sheidaei, A, Rezaei, N, Naghibi Iravani, SS, Modirian, M, et al. Patterns of obesity and overweight in the Iranian population: findings of STEPs 2016. Front Endocrinol. (2020) 11:42. doi: 10.3389/fendo.2020.00042
76. Okati-Aliabad, H, Ansari-Moghaddam, A, Kargar, S, and Jabbari, N. Prevalence of obesity and overweight among adults in the Middle East countries from 2000 to 2020: a systematic review and Meta-analysis. J Obes. (2022) 2022:1–18. doi: 10.1155/2022/8074837
77. Akhtar, S, Nasir, JA, Ali, A, Asghar, M, Majeed, R, and Sarwar, A. Prevalence of type-2 diabetes and prediabetes in Malaysia: a systematic review and meta-analysis. PLoS One. (2022) 17:e0263139. doi: 10.1371/journal.pone.0263139
78. Yan, Z, Cai, M, Han, X, Chen, Q, and Lu, H. The interaction between age and risk factors for diabetes and prediabetes: a community-based cross-sectional study. Diabetes Metab Syndr Obes. (2023) 16:85–93. doi: 10.2147/DMSO.S390857
79. Karakelides, H, Irving, BA, Short, KR, O'Brien, P, and Nair, KS. Age, obesity, and sex effects on insulin sensitivity and skeletal muscle mitochondrial function. Diabetes. (2010) 59:89–97. doi: 10.2337/db09-0591
80. De Tata, V. Age-related impairment of pancreatic Beta-cell function: pathophysiological and cellular mechanisms. Front Endocrinol (Lausanne). (2014) 5:138. doi: 10.3389/fendo.2014.00138
81. Satman, I, Yilmaz, T, Sengül, A, Salman, S, Salman, F, Uygur, S, et al. Population-based study of diabetes and risk characteristics in Turkey. Diabetes Care. (2002) 25:1551–6. doi: 10.2337/diacare.25.9.1551
82. Bigna, JJ, Nansseu, JR, Katte, JC, and Noubiap, JJ. Prevalence of prediabetes and diabetes mellitus among adults residing in Cameroon: a systematic review and meta-analysis. Diabetes Res Clin Pract. (2018) 137:109–18. doi: 10.1016/j.diabres.2017.12.005
83. Kautzky-Willer, A, Harreiter, J, and Pacini, G. Sex and gender differences in risk, pathophysiology and complications of type 2 diabetes mellitus. Endocr Rev. (2016) 37:278–16. doi: 10.1210/er.2015-1137
84. Nordström, A, Hadrévi, J, Olsson, T, Franks, PW, and Nordström, P. Higher prevalence of type 2 diabetes in men than in women is associated with differences in visceral fat mass. J Clin Endocrinol Metab. (2016) 101:3740–6. doi: 10.1210/jc.2016-1915
85. Galdas, PM, Cheater, F, and Marshall, P. Men and health help-seeking behaviour: literature review. J Adv Nurs. (2005) 49:616–23. doi: 10.1111/j.1365-2648.2004.03331.x
86. Jarrar, M, Abusalah, MAH, Albaker, W, al-Bsheish, M, Alsyouf, A, al-Mugheed, K, et al. Prevalence of type 2 diabetes mellitus in the general population of Saudi Arabia, 2000-2020: a systematic review and Meta-analysis of observational studies. Saudi J Med Med Sci. (2023) 11:1–10. doi: 10.4103/sjmms.sjmms_394_22
Keywords: epidemiology, diabetes mellitus, prevalence, meta-analysis, Iran
Citation: Hazar N, Jokar M, Namavari N, Hosseini S and Rahmanian V (2024) An updated systematic review and Meta-analysis of the prevalence of type 2 diabetes in Iran, 1996–2023. Front. Public Health. 12:1322072. doi: 10.3389/fpubh.2024.1322072
Edited by:
Youcef Shahali, Centre Hospitalier Universitaire de Besançon, FranceReviewed by:
Maryam Dadar, Razi Vaccine and Serum Research Institute, IranEhsan Shahrestanaki, Alborz University of Medical Sciences, Iran
Copyright © 2024 Hazar, Jokar, Namavari, Hosseini and Rahmanian. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vahid Rahmanian, VmFoaWQucmFobWFuaTEzOTJAZ21haWwuY29t