 Fatoumata Bintou Traoré1,2*
Fatoumata Bintou Traoré1,2* Cheick Sidya Sidibé3
Cheick Sidya Sidibé3 El Hadj Marouf Diallo2
El Hadj Marouf Diallo2 Bienvenu Salim Camara2,4
Bienvenu Salim Camara2,4 Sidikiba Sidibé2,4Alhassane Diallo5Nielé Hawa Diarra6
Sidikiba Sidibé2,4Alhassane Diallo5Nielé Hawa Diarra6 Birama Apho Ly7Mohamed Ali Ag Ahmed6
Birama Apho Ly7Mohamed Ali Ag Ahmed6 Kassoum Kayentao8Abdoulaye Touré9Alioune Camara10Alexandre Delamou2Hamadoun Sangho6Ibrahim Terera1
Kassoum Kayentao8Abdoulaye Touré9Alioune Camara10Alexandre Delamou2Hamadoun Sangho6Ibrahim Terera1- 1National Institute of Public Health, Bamako, Mali
- 2African Center of Excellence for the Prevention and Control of Communicable Diseases, Gamal Abdel Nasser University of Conakry, Conakry, Guinea
- 3Athena Institute for Research on Innovation and Communication in Health and Life Sciences, VU Amsterdam, Amsterdam, Netherlands
- 4Department of Public Health, Gamal Abdel Nasser University of Conakry, Conakry, Guinea
- 5Université de Montpellier, Montpellier, Languedoc-Roussillon, France
- 6Faculté de Médecine et d'Odontostomatologie, Université des Sciences, des Techniques et des Technologies de Bamako, Bamako, Mali
- 7Faculté de Pharmacie, Université des Sciences, Techniques et Technologies de Bamako, Bamako, Mali
- 8Malaria Research and Training Center, Mali International Center for Excellence in Research, University of Sciences, Techniques, and Technologies of Bamako, Bamako, Mali
- 9Center of Research and Training in Infectious Diseases, Gamal Abdel Nasser University of Conakry, Conakry, Guinea
- 10National Malaria Control Programme Conakry, Conakry, Guinea
Objectives: This study aimed to determine the prevalence and factors associated with maternal and neonatal sepsis in sub-Saharan Africa.
Methods: This systematic review and meta-analysis used the PRISMA guideline on sepsis data in sub-Saharan Africa. The bibliographic search was carried out on the following databases: Medline/PubMed, Cochrane Library, African Index Medicus, and Google Scholar. Additionally, the reference lists of the included studies were screened for potentially relevant studies. The last search was conducted on 15 October 2022. The Joanna Briggs Institute quality assessment checklist was applied for critical appraisal. Estimates of the prevalence of maternal and neonatal sepsis were pooled using a random-effects meta-analysis model. Heterogeneity between studies was estimated using the Q statistic and the I2 statistic. The funnel plot and Egger’s regression test were used to assess the publication bias.
Results: A total of 39 studies were included in our review: 32 studies on neonatal sepsis and 7 studies on maternal sepsis. The overall pooled prevalence of maternal and neonatal sepsis in Sub-Saharan Africa was 19.21% (95% CI, 11.46–26.97) and 36.02% (CI: 26.68–45.36), respectively. The meta-analyses revealed that Apgar score < 7 (OR: 2.4, 95% CI: 1.6–3.5), meconium in the amniotic fluid (OR: 2.9, 95% CI: 1.8–4.5), prolonged rupture of membranes >12 h (OR: 2.8, 95% CI: 1.9–4.1), male sex (OR: 1.2, 95% CI: 1.1–1.4), intrapartum fever (OR: 2.4, 95% CI: 1.5–3.7), and history of urinary tract infection in the mother (OR: 2.7, 95% CI: 1.4–5.2) are factors associated with neonatal sepsis. Rural residence (OR: 2.3, 95% CI: 1.01–10.9), parity (OR: 0.5, 95% CI: 0.3–0.7), prolonged labor (OR: 3.4, 95% CI: 1.6–6.9), and multiple digital vaginal examinations (OR: 4.4, 95% CI: 1.3–14.3) were significantly associated with maternal sepsis.
Conclusion: The prevalence of maternal and neonatal sepsis was high in sub-Saharan Africa. Multiple factors associated with neonatal and maternal sepsis were identified. These factors could help in the prevention and development of strategies to combat maternal and neonatal sepsis. Given the high risk of bias and high heterogeneity, further high-quality research is needed in the sub-Saharan African context, including a meta-analysis of individual data.
Systematic review registration: PROSPERO (ID: CRD42022382050).
Introduction
Maternal and neonatal sepsis is a generalized inflammatory response with systemic manifestations caused by one or more infectious agents (1), which occurs during pregnancy, childbirth, after abortion, or during the postpartum period (42 days) in women or in the first 28 days of life in newborns (2–4). Sepsis is a major cause of maternal and neonatal morbidity and mortality (2, 3, 5–9). It is the third leading cause of death in women and accounts for a quarter of neonatal deaths (1, 10–14). It is an obstacle to achieving the third Sustainable Development Goal (SDG), which aims to reduce maternal and neonatal mortality and morbidity (15). Low- and middle-income countries (LICs) are particularly affected by maternal and neonatal sepsis (11, 16, 17). In sub-Saharan Africa (SSA), it is estimated to be responsible for 130,000 maternal deaths and 300,000 neonatal deaths per year, although this may be an underestimation (2, 18). These deaths reflect a number of challenges, including policy, poverty, health inequalities, and the health system (19). However, few data are available on the prevalence and factors associated with sepsis across the continuum from pregnancy to postpartum or post-abortion, making it difficult to make a real estimation of maternal and neonatal sepsis in these countries (2, 10, 11). In the literature, the factors associated with maternal and neonatal sepsis are diverse, including prolonged labor, failure to perform antenatal consultation (ANC), prolonged rupture of membranes, history of infection in the mother, repeated vaginal examinations, intrapartum fever, gestational age, parity, type of delivery, prematurity, chorioamnionitis, meconium-stained amniotic fluid, Apgar score < 7, low birth weight < 2.5 kg, resuscitation of the newborn, age of the newborn <7 days, and male sex (5–7, 20–23).
Prevention, early recognition of signs, and rapid and appropriate management of cases are the main factors associated with a reduction in the morbidity and mortality associated with maternal and neonatal sepsis (5, 11, 24–26). A recent meta-analysis carried out in SSA in 2022 identified several risk factors for neonatal sepsis (27) but did not explore the magnitude of neonatal and/or maternal sepsis nor the factors associated with maternal sepsis. Other studies have shown that the prevalence of maternal sepsis was 39% in Ethiopia (28), 12.20% in Keyna (29), and 20% in Tanzania (30); for neonatal sepsis, it was 77.9 in Ethiopia (31), 20.5% in South Africa (32), 49.8 in Tanzania (33), 37.6 in Nigeria (34), and 17.5 in Ghana (35). Although these single studies reported data on the prevalence and factors associated with maternal and neonatal sepsis, there are no regionally representative pooled data on the magnitude and factors associated with maternal and neonatal sepsis in SSA. However, a better understanding of the burden and a synthesis of the evidence on the factors associated with maternal and neonatal sepsis are needed to optimize prevention strategies and management guidelines against this scourge. The aim of this systematic review with meta-analysis was to estimate the prevalence and factors associated with maternal and neonatal sepsis in sub-Saharan Africa. To the best of our knowledge, this is the first systematic review and meta-analysis to examine both the prevalence of and factors associated with maternal and neonatal sepsis in SSA. It aimed to answer the following questions:
What is the prevalence of maternal and neonatal sepsis in sub-Saharan Africa?
What are the associated factors with maternal and neonatal sepsis in sub-Saharan Africa?
Materials and methods
This systematic review was reported in accordance with PRISMA (Preferred Reporting Item for Systematic Review and Meta-analysis) guidelines (36). The protocol for this review was developed and registered in the “International prospective register of systematic reviews PROSPERO” (ID: CRD42022382050).
Search strategies
To identify eligible studies, Medline/PubMed, Cochrane Library, African Index Medicus, and Google Scholar databases were searched. We also conducted manual searches of the bibliographic references of included studies and meta-analyses. The adapted PECO format was used for this systematic review. This PECO included population (P), exposure (E), comparison (C), and outcome (O), as shown in Table 1. It consisted of using all the identified keywords and indexing terms to search different databases. All the search terms used and the MeSH terms for the search were added, as well as the Boolean operators, to guarantee the exhaustiveness of the search process. Key terms defining the same concept were introduced using the “OR” operator, and the “AND” operator was used to introduce different concepts.
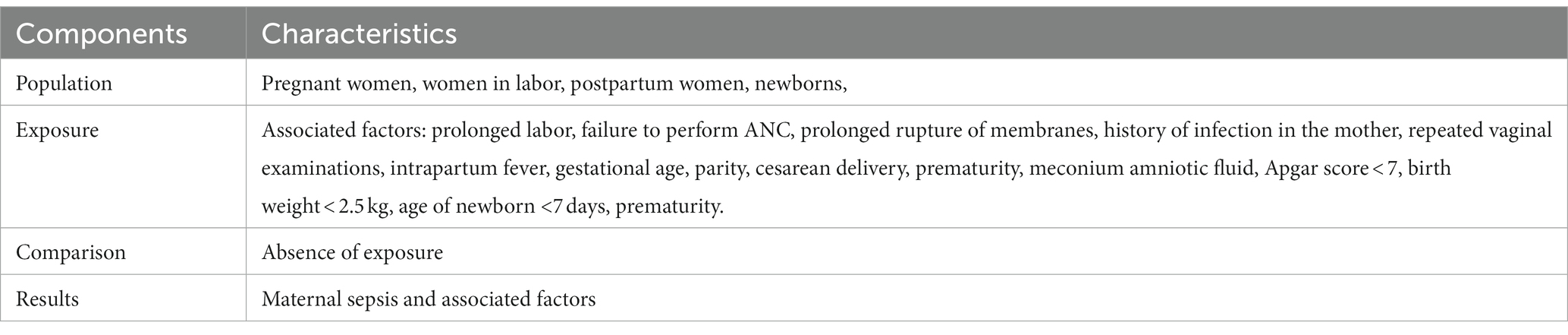
Table 1. PECOT framework for the review objective.
Selection of studies/eligibility criteria
The result of bibliographic searches carried out on the various search tools was exported to Zotero, where duplicates were identified and removed using the Duplicates command and manually also removed during the screening. The study selection process followed two evaluation stages (37). The first evaluation was based on an examination of the titles and abstracts of the articles. The titles and abstracts that were outside the scope of the study were excluded. The second assessment consisted of examining the full text of eligible studies. The entire process was carried out by two reviewers (FBT and NHD). They independently performed abstract screening and full-text study selection, where both authors had to approve the inclusion of the study in the systematic review. The reference lists of the included studies were screened for potentially relevant studies (38).
Studies reporting on the prevalence and/or at least one factor associated with maternal and/or neonatal sepsis in SSA in pregnant women from 28 weeks of amenorrhea (SA), postpartum women up to 42 days after delivery, post-abortion women, and newborns within 28 days of birth were included. Cross-sectional, cohort, and case–control studies on the prevalence, frequency, and factors associated with maternal and neonatal sepsis in SSA published in French and English between January 2012 and October 2022 were included. Qualitative studies, systematic reviews, and case series were excluded from the analysis, but the reference lists of these were screened.
Assessment of study quality and risk of bias
The quality of the included studies was assessed by two authors (FBT and NHD) using the Joanna Briggs Institute (JBI) quality assessment checklist (39). For cross-sectional studies, the following criteria were used: (1) conformity between target population and source population; (2) appropriate sampling technique; (3) representativeness of the sample; (4) description of the subject and context of the study; (5) data analysis with sufficient sample coverage; (6) valid methods for identifying the condition; (7) standard and reliable way of measuring the condition for all participants; (8) appropriate statistical test; and (9) adequate response rate. When items received a score ≥ 6 out of 9, they were considered to be of high quality. The following were used to assess cohort studies: (1) similarity of groups, (2) similarity of exposure measurement, (3) validity and reliability of measurement, (4) identification of confounders, (5) strategies for dealing with confounders, (6) adequacy of groups/participants at study entry, (7) validity and reliability of measured outcomes, (8) sufficient duration of follow-up, (9) completeness of follow-up or description of reasons for loss to follow-up, (10) strategies for dealing with incomplete follow-up, and (11) adequacy of statistical analysis. The criteria used to evaluate case–control studies are (1) comparable groups, (2) appropriateness of cases and controls, (3) criteria for identifying cases and controls, (4) standard exposure measurement, (5) similarity of exposure measurement for cases and controls, (6) treatment of confounding factors, (7) strategies for treating confounding factors, (8) standard evaluation of results, (9) appropriateness of duration of exposure, and (10) appropriateness of statistical analysis (see Table 2).
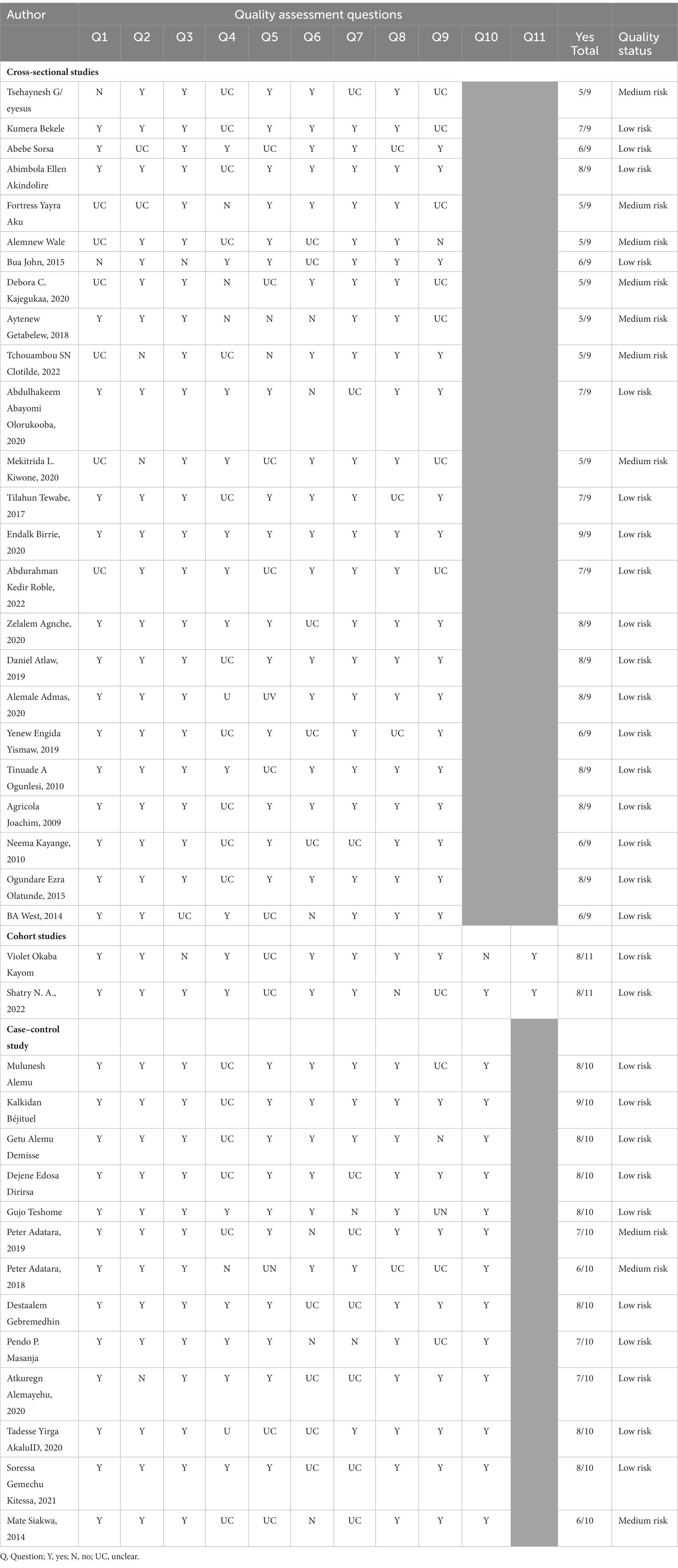
Table 2. Quality assessment results of included studies in sub-Saharan Africa from January 2002–October 2022 using the Joanna Briggs Institute (JBI) quality appraisal checklist.
Data extraction
Two authors (FBT and NHD) independently extracted data using a tested form on Microsoft Excel. If discrepancies between data extractors continued, a third reviewer (EMD) was involved. Data extracted included author name and year of publication, country, study period, study setting, study design, study population, sample size, type of sepsis (maternal or neonatal), prevalence of neonatal sepsis, prevalence of maternal sepsis, and risk bias.
For the associated factors, data were extracted on the age of the newborn, Apgar score, gestational age, birth weight, resuscitation of the newborn at birth, sex of the newborn, antenatal consultation (ANC), presence of prolonged rupture of membranes, repeated vaginal examinations, intrapartum fever, gestational age, parity, type of delivery, prematurity, meconium amniotic fluid, history of infection in the mother, maternal fever, type of delivery, and prolonged labor.
Statistical analysis
Data were entered into Microsoft Excel and then exported into Stata version 17 software. We pooled maternal and neonatal sepsis prevalence estimates using a random-effects meta-analysis model because it accounts for variability between studies. We examined the heterogeneity of effect size using the Q statistic and the I2 statistic (40). An I2 value ≥ 50% was considered strong heterogeneity, and a random-effects model was used (41, 42). The random-effect RELM method was mainly used. The funnel plot and Eggers’s regression test were used to check for publication bias (43). To complete the tests for publication bias, we added the Begg and Thompson tests on R software. Forest plots were used to display the results graphically. A subgroup analysis was performed according to study design (prospective or retrospective), sepsis diagnostic criteria (clinic or clinic and biology), risk of bias (low or moderate), and different regions of SSA (East, West, or South Africa).
Results
A total of 2,638 titles were screened (2,033 from PubMed, 58 from the African Index of Medicus, 41 from Cochrane, and 506 from Google Scholar). After removing duplicates, 2,145 studies remained. Evaluation of titles and abstracts led to the exclusion of 2,019 studies. Nine studies were excluded because the full text was not available. The full-text review involved 126 studies. The number of articles retained for inclusion was 39. The reasons for the exclusion of 87 studies were the lack of availability of the variable of interest and the difference in the target population (Figure 1).
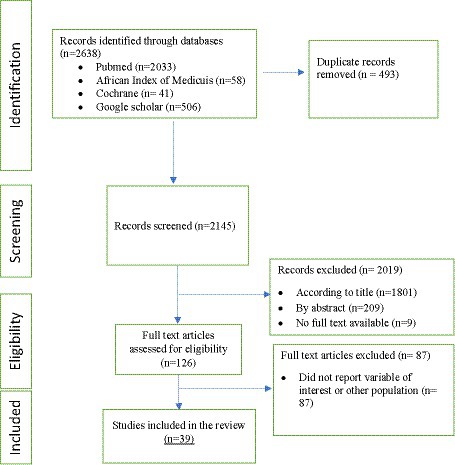
Figure 1. PRISMA flow diagram describing the results of study selection.
Characteristics of the studies included in the meta-analysis
A total of 39 studies were included in our review: 32 studies of neonatal sepsis and 7 studies of maternal sepsis. There were 24 cross-sectional studies (22, 30–34, 44–60), 13 case–control studies (28, 35, 61–69), and 2 cohorts (29, 70).
Twenty-one studies were from Ethiopia (28, 31, 44–46, 49, 51–56, 60–64, 66, 68, 69, 71), five from Tanzania (22, 30, 33, 67, 72), five from Nigeria (34, 47, 59, 73, 74), four from Ghana (35, 48, 65, 75), two from Uganda (50, 70), one from Kenya (29), and one from South Africa (32). The total study population was 12,777, including 10,494 newborns and 2,283 women. After quality assessment, 30 studies had a low risk of bias and 9 had a medium risk of bias (see Table 3).
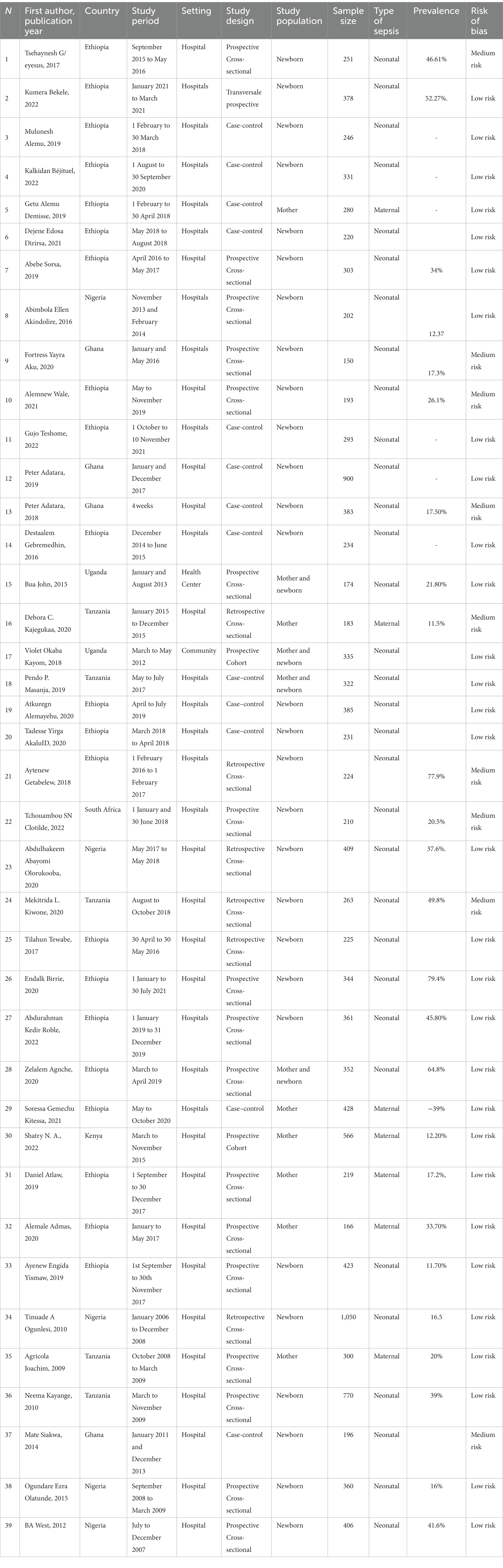
Table 3. Characteristics of included studies.
Prevalence of maternal sepsis
The pooled prevalence of maternal sepsis in SSA was 19.21% (95% CI, 11.46–26.97). Significant heterogeneity was observed between studies (I2 = 93.26%, p < 0.000). A random effects model was used to measure pooled prevalence. The highest prevalence was reported by Alemale et al. (54) (33.7%) and the lowest by Debora et al. (22) (11.5%); Figure 2 shows the details.
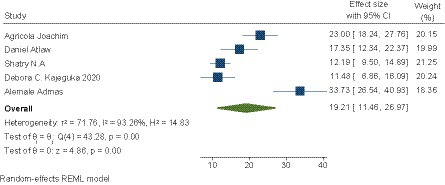
Figure 2. Pooled prevalence of maternal sepsis in SSA.
Subgroup analysis of the prevalence of maternal sepsis
A subgroup analysis of the prevalence of maternal sepsis was carried out according to the diagnostic criteria for sepsis (clinical or clinical and biological). It was 25.33 (9.28–41.38) for sepsis based on clinical signs and 15.43 (8.28–22.58) for sepsis based on clinical signs and biology (22, 29, 30). See Table 4 for details.

Table 4. Sub-group analysis of the prevalence of maternal sepsis in sub-Saharan Africa.
Prevalence of neonatal sepsis
The pooled prevalence of neonatal sepsis in SSA was 36.02% (95% CI, 26.68–49.36). A significant heterogeneity between the included studies was observed (I2 = 99.1%, p < 0.000). Therefore, a random effects model was used to estimate the pooled prevalence. The prevalence ranged from 11.1 (56) up to 77.9% (31) (see Figure 3).
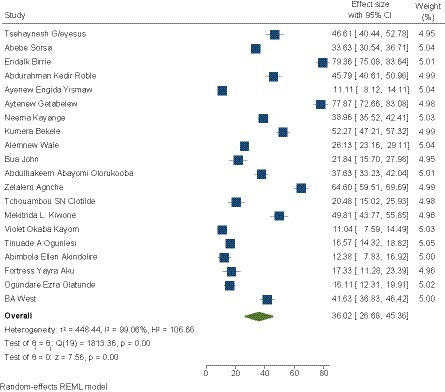
Figure 3. Pooled prevalence of neonatal sepsis in SSA.
Subgroup analysis of the prevalence of neonatal sepsis
A subgroup analysis of prevalence was performed according to the design (prospective and retrospective), subdivision of SSA (East, West, or South Africa), definition of sepsis (clinical when diagnostic based on clinical signs or clinical and biological when diagnostic based on clinical signs and confirmed by biological tests), and risk of bias (low or moderate).
Depending on the design, the prevalence of neonatal sepsis was 32.88 (22.35–43.41) for prospective studies and 45.46 (25.97–64.94) for retrospective studies. According to the diagnostic criteria for sepsis, it was 44.11 (27.33–60.90) for sepsis based on clinical signs and 31.25 (22.24–40.26) for sepsis based on clinical signs and biology. According to the subdivision, the prevalence of neonatal sepsis was 42.96 (30.75–55.16) in East Africa, 23.59 (15.53–33.65) in West Africa, and 20.48 (15.0–25.93) in South Africa. The prevalence of neonatal sepsis was 34.45 (23.93–44.98) for studies with a low risk of bias and 39.69 (21.58–57.80) for studies with a medium risk of bias (see Table 5).
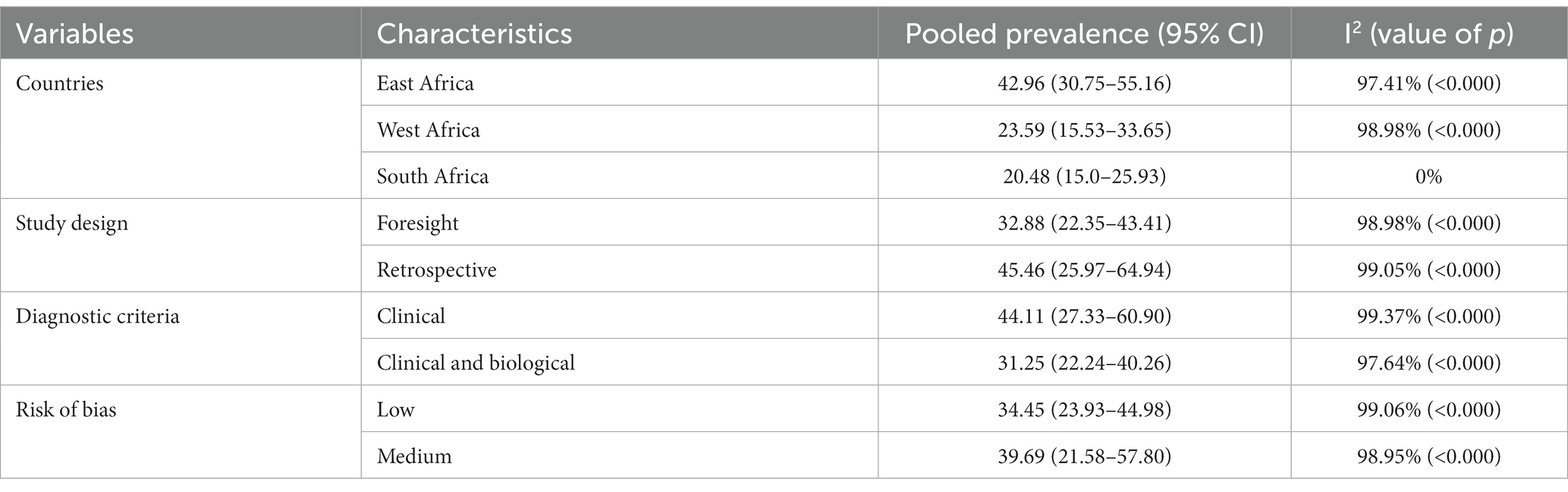
Table 5. Sub-group analysis of the prevalence of neonatal sepsis in sub-Saharan Africa.
Publication bias
We assessed publication bias using the funnel plot and Egger’s regression test (76). Compared with the maternal sepsis studies, a visual asymmetrical distribution was observed, and Egger’s regression test (value of p = 0.01) indicated the presence of a publication bias (see Figure 4). We did not use the Begg and Thompson tests due to the number of studies less than 10.
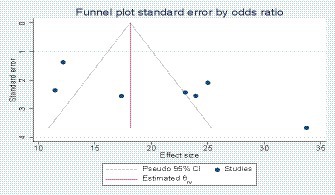
Figure 4. Funnel plot showing publication bias in maternal sepsis studies.
For the study concerning neonatal sepsis, we assessed publication bias using the funnel plot, Egger’s regression test, Begg’s test, and Thompson test. The diagrams showed asymmetry, and the result of Egger’s test showed the presence of bias (p = 0.04; see Figure 5). However, Begg’s test (value of p = 0.06) and the Thompson test (value of p = 0.14) did not reject the city Ho. Therefore, the asymmetry on the funnel plot is reflected much more by a small study effect than by a publication bias.

Figure 5. Funnel plot showing publication bias d in neonatal sepsis studies.
Meta-analysis of factors associated with maternal sepsis
A total of eight risk factors were included in the meta-analysis: place of residence for 3 studies (22, 28, 63), parity for 3 studies (22, 30, 54), mode of delivery for 5 studies (22, 28, 54, 60, 63), prolonged labor for 5 studies (22, 28, 29, 54, 63), multiple vaginal examinations for 3 studies (28, 29, 63), performance of ANC for 4 studies (28, 54, 60, 63), history of urinary tract infection for 3 studies (22, 29, 30), and level of education for 4 studies (28, 29, 60, 63). Table 6 shows the details.
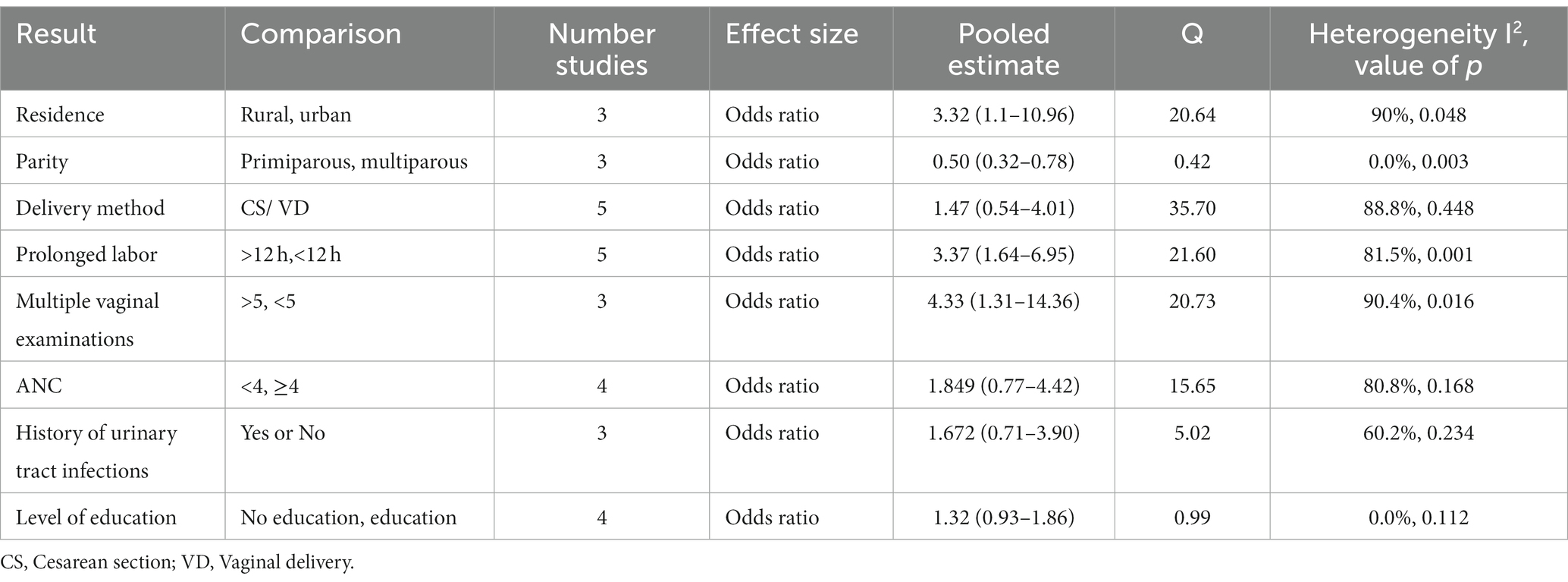
Table 6. Risk factors included in the meta-analysis for maternal sepsis.
Meta-analysis of factors associated with neonatal sepsis
A meta-analysis was carried out for 15 risk factors classified into maternal and neonatal factors. The maternal factors were history of urinary tract infection in the mother (13 studies) (31, 45, 53, 55, 56, 61, 62, 65, 66, 68–71), parity (10 studies) (31, 45, 48, 53, 56, 61, 62, 65, 67, 68), prolonged labor (5 studies) (31, 53, 62, 69, 73), intrapartum fever (13 studies) (31, 45, 48, 52, 55, 56, 61, 64, 66, 68, 70, 72, 73), multiple vaginal examinations (7 studies) (45, 53, 61, 64, 66–68), performance of ANC (13 studies) (45, 48, 50, 55, 61, 64, 65, 67–71), prolonged rupture of membranes (18 studies) (31, 33, 45, 46, 52, 53, 56, 61, 62, 65–73), and mode of delivery (14 studies) (31, 32, 35, 44, 46, 48, 52, 61, 62, 64, 66–68, 72). The neonatal factors reported were Apgar (18 studies) (31, 33–35, 44–46, 48, 52, 56, 61, 62, 64–66, 68, 69, 71), prematurity (17 studies) (31, 33–35, 44–46, 50, 52, 53, 61, 62, 64–67, 71), meconium amniotic fluid (12 studies) (31, 45, 46, 52, 61, 64–69, 72), birth weight (17 studies) (31–35, 44–48, 52, 53, 61, 62, 64–69, 72), neonatal resuscitation (09 studies) (33–35, 52, 53, 62, 65, 66, 71), neonatal age < 7 days (11 studies) (36, 38, 48, 53, 57, 65, 66, 69, 72, 75), and neonatal sex (14 studies) (32, 34, 35, 45, 46, 48, 53, 55, 61, 62, 65, 66, 72, 73) (see Table 7).
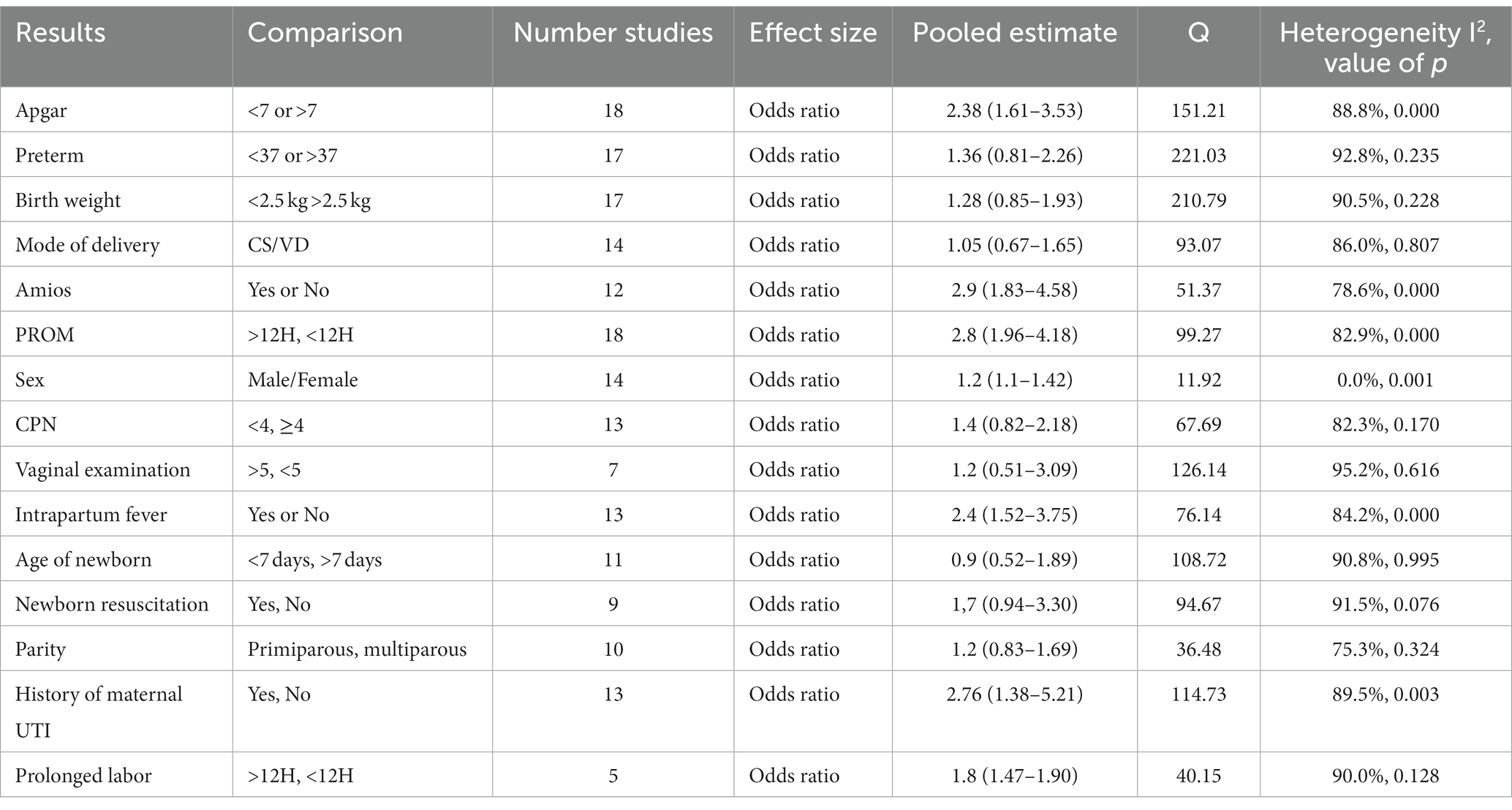
Table 7. Risk factors included in the meta-analysis for neonatal sepsis.
Associated factors with maternal and neonatal sepsis
Factors associated with maternal sepsis
Rural residence (OR: 2.32, IC 95%: 1.01–10.9, I2 = 90.3%), parity (OR: 0.5, IC95%: 0.3–0.7, I2 = 0%), prolonged labor (OR: 3.4, IC95%: 1.6–6.9, I2 = 81.5%), and multiple vaginal examinations (OR: 4.4, IC95%: 1.3–14.3, I2 = 90.4%) were independently associated with maternal sepsis.
Factors associated with neonatal sepsis
The meta-analysis identified 6 factors as being significantly associated with neonatal sepsis, including Apgar score < 7 (OR: 2.4, CI95%: 1.6–3.5, I2 = 88.8%), the presence of meconium in the amniotic fluid (OR: 2.9, CI95%: 1.8–4.5, I2 = 78.6%), prolonged rupture of membranes >12 h (OR: 2.8, IC95%: 1.9–4.1, I2 = 82.9%), male sex (OR: 1.2, IC95%: 1.1–1.4, I2 = 0%), intrapartum fever (OR: 2.4, IC95%: 1.5–3.7, I2 = 84.2%), and history of urinary tract infection in the mother (OR: 2.76, IC95%: 1.4–5.2, I2 = 89.5%).
Discussion
Knowledge of the burden and risk factors of maternal and neonatal sepsis is crucial for developing preventive measures and reducing maternal and neonatal mortality. This systematic review with meta-analysis filled the gaps in the literature on the prevalence of maternal and neonatal sepsis and associated factors in SSA. Based on 39 studies included in the final analysis, we found a pooled prevalence of 19.21% for maternal sepsis and 36.02% for neonatal sepsis. However, considerable heterogeneity was observed.
Factors such as rural residence, parity, prolonged labor, and multiple vaginal examinations significantly increased the risk of maternal sepsis in our study. The factors associated with neonatal sepsis in this review are classified into maternal and neonatal factors. Maternal factors such as prolonged rupture of membranes > 12 h, intrapartum fever, and history of maternal urinary tract infection and neonatal factors such as Apgar score < 7, presence of meconium in amniotic fluid, and male sex were significantly associated with neonatal sepsis. Our estimate confirms that maternal and neonatal sepsis is a major public health problem in SSA. The pooled prevalence of maternal sepsis in our review is in line with other reviews conducted in 2009 (77) and 2021 (20). This high prevalence can be explained by various factors, such as the coverage of childbirth in health facilities, the asepsis and hygiene of surfaces and materials used, the personal hygiene of pregnant women, and certain harmful practices. Our study is the first to examine both the extent and the factors associated with maternal and neonatal sepsis, which sets it apart from other reviews. It identified other factors, such as rural residence and parity, which were not identified in the 2022 review or the WHO guidelines (78). Our results could serve as a broader database for the development of interventions for the prevention and management of maternal and neonatal sepsis.
All the maternal sepsis studies included were from East Africa. The subgroup analysis of the prevalence of maternal sepsis ranged from 15.43% based on clinical signs and biology to 25.33% based on clinical signs.
The subgroup analysis of the prevalence of neonatal sepsis varied from one subdivision to another. East Africa recorded the highest prevalence, 42.96%, which was higher than the pooled prevalence. This could be explained by the weakness of the health system, the quality of services offered, and socio-cultural factors. The under-analysis of sepsis in other parts of Africa, due to the small number of studies carried out there, masks a probable high prevalence in these countries, as areas of high prevalence in these countries have probably not been covered by the small number of studies published. The prevalence of neonatal sepsis was 44.11% for the diagnostic criterion based on clinical signs and 31.25% for clinical signs and biology. Despite the various subgroup analyses, they did not make it possible to explore the source of the heterogeneity. This could be explained by the heterogeneous definition of sepsis in the different studies. The clinical signs differed from one study to another, as did the laboratory tests, which is why a meta-analysis of the individual data was necessary to identify a single algorithm.
The factors associated with maternal sepsis in our review are partly in accordance with a review of the literature in other systematic reviews in 2009 and 2022 (27, 77), where the risk factors identified were intrapartum maternal fever, multiple vaginal examinations, foul-smelling vaginal discharge, prematurity, prolonged rupture of membranes, prolonged labor, and multiple vaginal touches.
Living in a rural area was significantly associated with maternal sepsis. Women living in rural areas were 2.3 times more likely to develop sepsis than those living in urban areas. The possible explanation could be poor hygiene levels, lack of water sources, poor cord care, overcrowding in homes, and low education level of mothers in rural areas (73, 75, 79). Another possible explanation could be the fact that mothers living in urban areas are close to health facilities and have various means of transport to get to these facilities, and the availability of qualified staff and adequate technical platforms in urban areas. A vaginal examination ≥ 5 times was significantly associated with maternal sepsis. The probability of maternal sepsis was 4.4 times higher in women who had undergone a vaginal examination ≥ 5 times compared with those who had not. During vaginal examinations, there is a high likelihood of microorganisms ascending from the lower to the upper genital tract, which can lead to sepsis. Simple interventions accepted to reduce the incidence of maternal sepsis are using sterile and aseptic technical equipment by providers (hand washing, sterile drapes and instruments, and sterile gloves).
The factors associated with neonatal sepsis in our review are in line with other reviews in Pakistan (78), East Africa (21), SSA (27), and India (80), which reported maternal factors such as intrapartum maternal fever, prolonged rupture of water membranes, gestational age < 37 weeks, prolonged labor, multiple vaginal touches, history of maternal urinary tract infection and low socioeconomic status, neonatal factors such as resuscitation at birth, low birth weight < 2.5 kg, Apgar score < 7, absence of crying immediately after birth, meconium-stained amniotic fluid, and male sex.
Intrapartum fever was significantly associated with maternal sepsis. The probability of maternal sepsis was 2.4 times higher in women with a fever during pregnancy than in those without a fever. Intrapartum fever is suggestive of a maternal infection that is transmitted to the baby in utero or during passage through the genital tract, leading to sepsis.
Membrane rupture > 12 h significantly increased the risk of neonatal sepsis, and a history of urinary tract infection in the mother was significantly associated with neonatal sepsis. The water membrane protects the upper genital tract; when it is ruptured, bacteria can proliferate through the dilated cervix into the upper internal genital tract, causing infection. These pathogens also colonize the birth canal, which could contaminate the newborn during passage through the canal. Intrapartum antibiotic prophylaxis has been recommended as an effective practice for at-risk mothers to reduce sepsis worldwide (81).
Having an Apgar score < 7 significantly increased the risk of neonatal sepsis. As a result, the probability of neonatal sepsis was 2.4 times higher in neonates with an Apgar score < 7 compared with those with an Apgar score > 7. This finding is consistent with studies from Iraq (82) and Indonesia (83). Neonates with low Apgar scores tend to have a poor adaptation to extrauterine life due to the stress experienced during labor and therefore are more prone to infection. In addition, resuscitation procedures following birth asphyxia tend to expose newborns to pathogenic microbes. In our study, however, we did not assess birth asphyxia as a risk factor for neonatal sepsis.
Male sex has been identified as a factor associated with neonatal sepsis, and this finding has been made in the journals in India and SSA. However, we suggest further research into this factor to give a more rational explanation.
Strengths and limitations
Our review used an appropriate search strategy, with the combination of global and regional databases reducing the risk of missing relevant regional studies. Duplicate screening and data extraction, as well as rigorous quality assessment of included data and subgroup analysis, was also performed. The relatively high number of included studies for neonatal sepsis is a strength. The number of articles included was small for maternal sepsis (7), which may limit the generalizability of the results. Most of the studies were cross-sectional, which could be a limitation. The majority of studies included in this systematic review were from East Africa, which may affect the generalizability of our results to sub-Saharan Africa. There were also publication biases between studies and a high degree of heterogeneity. We believe that this is an important subject that has not been sufficiently explored and that a meta-analysis of individual data will be necessary.
Conclusion
In our review, the prevalence of maternal and neonatal sepsis was high. Several factors were significantly associated with this prevalence, which could help prevent maternal and neonatal sepsis by developing appropriate standard infection prevention techniques, reducing certain harmful practices, and reducing susceptibility to infection by improving maternal health through nutritional supplementation and treating infections during pregnancy. However, there is a need for evidence on other important risk factors for maternal and neonatal sepsis, including in the community. Given the high risk of bias and high heterogeneity, further high-quality research is needed in the sub-Saharan African context.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
FT: Conceptualization, Formal analysis, Investigation, Methodology, Software, Supervision, Writing – original draft, Writing – review & editing. CS: Conceptualization, Methodology, Writing – review & editing. ED: Conceptualization, Writing – review & editing, Investigation. BC: Investigation, Methodology, Writing – review & editing. SS: Software, Writing – review & editing, Formal analysis. ADi: Formal analysis, Validation, Writing – review & editing. ND: Conceptualization, Investigation, Writing – review & editing. BL: Methodology, Writing – review & editing. MA: Conceptualization, Writing – review & editing. KK: Formal analysis, Software, Supervision, Writing – review & editing. AT: Supervision, Writing – review & editing. AC: Writing – review & editing. ADe: Supervision, Validation, Writing – review & editing. HS: Supervision, Validation, Writing – review & editing. IT: Formal analysis, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the West African Network of African Center of Excellence on Infectious Diseases (WANIDA); however, the institution played no role in the study design, data collection, data analysis, or writing of the article. The corresponding author was responsible for the data and submission of the article for publication.
Acknowledgments
The authors thank the West African Network of African Center of Excellence on Infectious Diseases (WANIDA) for support. We thank colleagues of the National Institute of Public Health and those of the African Center of Excellence for Prevention and Control of Communicable Diseases for their support during this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors declared no conflicts of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Galvão, A, Braga, AC, Gonçalves, DR, Guimarães, JM, and Braga, J. Sepsis during pregnancy or the postpartum period. J Obstet Gynaecol. (2016) 36:735–43. doi: 10.3109/01443615.2016.1148679
2. Otu, A, Nsutebu, EF, Hirst, JE, Thompson, K, Walker, K, and Yaya, S. How to close the maternal and neonatal sepsis gap in sub-Saharan Africa. BMJ Glob Health. (2020) 5:e002348. doi: 10.1136/bmjgh-2020-002348
3. Sands, K, Spiller, OB, Thomson, K, Portal, EAR, Iregbu, KC, and Walsh, TR. Early-onset neonatal Sepsis in low- and middle-income countries: current challenges and future opportunities. Infect Drug Resist. (2022) 15:933–46. doi: 10.2147/IDR.S294156
4. Assemie, MA, Alene, M, Yismaw, L, Ketema, DB, Lamore, Y, Petrucka, P, et al. Prevalence of neonatal Sepsis in Ethiopia: a systematic review and Meta-analysis. Int J Pediatr. (2020) 2020:e6468492:1–9. doi: 10.1155/2020/6468492
5. Kendle, AM, Salemi, JL, Tanner, JP, and Louis, JM. Delivery-associated sepsis: trends in prevalence and mortality. Am J Obstet Gynecol. (2019) 220:391.e1–391.e16. doi: 10.1016/j.ajog.2019.02.002
6. Beck, C, Gallagher, K, Taylor, LA, Goldstein, JA, Mithal, LB, and Gernand, AD. Chorioamnionitis and risk for maternal and neonatal Sepsis: a systematic review and Meta-analysis. Obstet Gynecol. (2021) 137:1007–22. doi: 10.1097/AOG.0000000000004377
7. Tesfaye, T, Samuel, S, and Lera, T. Determinants of puerperal sepsis among postpartum women at public hospitals of Hawassa city, southern Ethiopia: institution-based unmatched case-control study. Heliyon. (2023) 9:e14809. doi: 10.1016/j.heliyon.2023.e14809
8. Fleischmann-Struzek, C, Goldfarb, DM, Schlattmann, P, Schlapbach, LJ, Reinhart, K, and Kissoon, N. The global burden of paediatric and neonatal sepsis: a systematic review. Lancet Respir Med. (2018) 6:223–30. doi: 10.1016/S2213-2600(18)30063-8
9. Reinhart, K, Daniels, R, Kissoon, N, Machado, FR, Schachter, RD, and Finfer, S. Recognizing Sepsis as a Global Health priority — a WHO resolution. N Engl J Med. (2017) 377:414–7. doi: 10.1056/NEJMp1707170
10. HAA, AL-K, and Hameed, RH. Sepsis during pregnancy in the postpartum duration. J Crit Rev. (2020) 7:2435–9.
11. Bonet, M, Brizuela, V, Abalos, E, Cuesta, C, Baguiya, A, Chamillard, M, et al. Frequency and management of maternal infection in health facilities in 52 countries (GLOSS): a 1-week inception cohort study. Lancet Glob Health. (2020) 8:e661–71. doi: 10.1016/S2214-109X(20)30109-1
12. Brizuela, V, Bonet, M, Romero, CLT, Abalos, E, Baguiya, A, Fawole, B, et al. Early evaluation of the ‘STOP SEPSIS!‘WHO global maternal Sepsis awareness campaign implemented for healthcare providers in 46 low, middle and high-income countries. BMJ Open. (2020) 10:e036338. doi: 10.1136/bmjopen-2019-036338
13. Brizuela, V, Cuesta, C, Bartolelli, G, Abdosh, AA, Abou Malham, S, Assarag, B, et al. Availability of facility resources and services and infection-related maternal outcomes in the WHO global maternal Sepsis study: a cross-sectional study. Lancet Glob Health. (2021) 9:e1252–61. doi: 10.1016/S2214-109X(21)00248-5
14. Say, L, Chou, D, Gemmill, A, Tunçalp, Ö, Moller, AB, Daniels, J, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. (2014) 2:e323–33. doi: 10.1016/S2214-109X(14)70227-X
15. Ebener, S, Stenberg, K, Brun, M, Monet, JP, Ray, N, Sobel, HL, et al. Proposing standardised geographical indicators of physical access to emergency obstetric and newborn care in low-income and middle-income countries. BMJ Glob Health. (2019) 4:e000778. doi: 10.1136/bmjgh-2018-000778
16. Hug, L, Alexander, M, You, D, and Alkema, L. National, regional, and global levels and trends in neonatal mortality between 1990 and 2017, with scenario-based projections to 2030: a systematic analysis. Lancet Glob Health. (2019) 7:e710–20. doi: 10.1016/S2214-109X(19)30163-9
17. Nyenga, AM. Trends in neonatal mortality in Lubumbashi (Democratic Republic of Congo) from 2011 to 2018. Pediatr Surg. (2019) 2:5. doi: 10.4236/oje.2021.115029
18. Hall, J, Adams, NH, Bartlett, L, Seale, AC, Lamagni, T, Bianchi-Jassir, F, et al. Maternal disease with group B Streptococcus and serotype distribution worldwide: systematic review and Meta-analyses. Clin Infect Dis. (2017) 65:S112–24. doi: 10.1093/cid/cix660
19. Yaya, S, Bishwajit, G, Okonofua, F, and Uthman, OA. Under five mortality patterns and associated maternal risk factors in sub-Saharan Africa: a multi-country analysis. PLoS One. (2018) 13:e0205977. doi: 10.1371/journal.pone.0205977
20. Melkie, A, and Dagnew, E. Burden of puerperal sepsis and its associated factors in Ethiopia: a systematic review and meta-analysis. Arch Public Health. (2021) 79:216. doi: 10.1186/s13690-021-00732-y
21. Abate, BB, Kasie, AM, Reta, MA, and Kassaw, MW. Neonatal sepsis and its associated factors in East Africa: a systematic review and meta-analysis. Int J Public Health. (2020) 65:1623–33. doi: 10.1007/s00038-020-01489-x
22. Kajeguka, DC, Mrema, NR, Mawazo, A, Malya, R, and Mgabo, MR. Factors and causes of puerperal Sepsis in Kilimanjaro, Tanzania: a descriptive study among postnatal women who attended Kilimanjaro Christian medical Centre. East Afr Health Res J. (2020) 4:158–62. doi: 10.24248/eahrj.v4i2.639
23. Chepchirchir, MV, Nyamari, J, and Keraka, M. Associated factors with puerperal Sepsis among reproductive age women in Nandi County, Kenya. JMRH. (2017) 5:9348. doi: 10.22038/jmrh.2017.9348
24. Edwards, W, Dore, S, van Schalkwyk, J, and Armson, BA. Prioritizing maternal Sepsis: National Adoption of an obstetric early warning system to prevent morbidity and mortality. J Obstet Gynaecol Can. (2020) 42:640–3. doi: 10.1016/j.jogc.2019.11.072
25. Cheshire, J, Jones, L, Munthali, L, Kamphinga, C, Liyaya, H, Phiri, T, et al. The FAST-M complex intervention for the detection and management of maternal sepsis in low-resource settings: a multi-site evaluation. BJOG Int J Obstet Gynaecol. (2021) 128:1324–33. doi: 10.1111/1471-0528.16658
26. Shifera, N, Dejenie, F, Mesafint, G, and Yosef, T. Risk factors for neonatal sepsis among neonates in the neonatal intensive care unit at Hawassa university comprehensive specialized hospital and Adare general Hospital in Hawassa City, Ethiopia. Front Pediatr. (2023) 11:671. doi: 10.3389/fped.2023.1092671
27. Bech, CM, Stensgaard, CN, Lund, S, Holm-Hansen, C, Brok, JS, Nygaard, U, et al. Risk factors for neonatal sepsis in sub-Saharan Africa: a systematic review with meta-analysis. BMJ Open. (2022) 12:e054491. doi: 10.1136/bmjopen-2021-054491
28. Kitessa, SG, Teferi Bala, E, Makuria, M, and Senbeta Deriba, B. Determinants of puerperal sepsis at public hospitals in West Ethiopia: a case-control study. Front Womens Health. (2021) 6. doi: 10.15761/FWH.1000207
29. Naima, S. Magnitude and risk factors for puerperal Sepsis at the Pumwani maternity hospital. [Thesis]. University of Nairobi; (2017). Available at:http://erepository.uonbi.ac.ke/handle/11295/101747
30. Joachim, A, Matee, MI, Massawe, FA, and Lyamuya, EF. Maternal and neonatal colonisation of group B streptococcus at Muhimbili National Hospital in Dar Es Salaam, Tanzania: prevalence, risk factors and antimicrobial resistance. BMC Public Health. (2009) 9:437. doi: 10.1186/1471-2458-9-437
31. Getabelew, A, Aman, M, Fantaye, E, and Yeheyis, T. Prevalence of neonatal Sepsis and associated factors among neonates in neonatal intensive care unit at selected governmental hospitals in Shashemene town, Oromia regional State, Ethiopia, 2017. Int J Pediatr. (2018) 2018:1–7. doi: 10.1155/2018/7801272
32. Clotilde, TS, Motara, F, and Laher, AE. Prevalence and presentation of neonatal sepsis at a paediatric emergency department in Johannesburg, South Africa. Afr J Emerg Med. (2022) 12:362–5. doi: 10.1016/j.afjem.2022.07.013
33. Kiwone, ML, Chotta, NS, Byamungu, D, and Mghanga, FP. Prevalence and factors associated with neonatal sepsis among hospitalized newborns at Ruvuma, southern Tanzania. South Sudan Med J. (2020) 13:86–9.
34. Olorukooba, AA, Ifusemu, WR, Ibrahim, MS, Jibril, MB, Amadu, L, and Lawal, BB. Prevalence and factors associated with neonatal Sepsis in a tertiary hospital, north West Nigeria. Niger Med J. (2020) 61:60–6. doi: 10.4103/nmj.NMJ_31_19
35. Adatara, P, Afaya, A, Salia, SM, Afaya, RA, Kuug, AK, Agbinku, E, et al. Risk factors for neonatal Sepsis: a retrospective case-control study among neonates who were delivered by caesarean section at the trauma and specialist hospital, Winneba, Ghana. Biomed Res Int. (2018) 2018:1–7. doi: 10.1155/2018/6153501
36. Moher, D, Liberati, A, Tetzlaff, J, and Altman, DG. Preferred reporting items for systematic reviews and Meta-analyses: the PRISMA statement. Ann Intern Med. (2009) 151:264–9. doi: 10.7326/0003-4819-151-4-200908180-00135
37. Vu-Ngoc, H, Elawady, SS, Mehyar, GM, Abdelhamid, AH, Mattar, OM, Halhouli, O, et al. Quality of flow diagram in systematic review and/or meta-analysis. PLoS One. (2018) 13:e0195955. doi: 10.1371/journal.pone.0195955
38. Madrid, L, Seale, AC, Kohli-Lynch, M, Edmond, KM, Lawn, JE, Heath, PT, et al. Infant group B streptococcal disease incidence and serotypes worldwide: systematic review and Meta-analyses. Clin Infect Dis. (2017) 65:S160–72. doi: 10.1093/cid/cix656
39. Munn, Z, Moola, S, Riitano, D, and Lisy, K. The development of a critical appraisal tool for use in systematic reviews addressing questions of prevalence. Int J Health Policy Manag. (2014) 3:123–8. doi: 10.15171/ijhpm.2014.71
40. Higgins, JP, and Thompson, SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21:1539–58. doi: 10.1002/sim.1186
41. Higgins, JPT, Thompson, SG, Deeks, JJ, and Altman, DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
42. Huang, X, Chen, M, Fu, R, He, W, He, Y, Shentu, H, et al. Efficacy of kangaroo mother care combined with neonatal phototherapy in newborns with non-pathological jaundice: a meta-analysis. Front Pediatr. (2023) 11:1098143. doi: 10.3389/fped.2023.1098143
43. Egger, M, Davey Smith, G, Schneider, M, and Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ. (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
44. G/eyesus, T, Moges, F, Eshetie, S, Yeshitela, B, and Abate, E. Bacterial etiologic agents causing neonatal sepsis and associated risk factors in Gondar, Northwest Ethiopia. BMC Pediatr. (2017) 17:137. doi: 10.1186/s12887-017-0892-y
45. Bekele, K, Bekele, F, Edosa, D, Mekonnen, M, and Benayew, M. Magnitude and associated factors of neonatal sepsis among neonates admitted to neonatal intensive care unit of northern Oromia hospitals, Ethiopia: a multicenter cross-sectional study. Ann Med Surg. (2022) 78:103782. doi: 10.1016/j.amsu.2022.103782
46. Sorsa, A. Epidemiology of neonatal Sepsis and associated factors implicated: observational study at neonatal intensive care unit of Arsi university teaching and referral hospital, south East Ethiopia. Ethiop J Health Sci. (2019) 29:333–42. doi: 10.4314/ejhs.v29i3.5
47. Akindolire, AE, Tongo, O, Dada-Adegbola, H, and Akinyinka, O. Etiology of early onset septicemia among neonates at the university college hospital, Ibadan, Nigeria. J Infect Dev Ctries. (2016) 10:1338–44. doi: 10.3855/jidc.7830
48. Aku, FY, Akweongo, P, Nyarko, KM, Mensah, LG, Amegan-Aho, K, Kumi, L, et al. Factors associated with culture proven neonatal sepsis in the ho municipality 2016. Pan Afr Med J. (2020) 36:281. doi: 10.11604/pamj.2020.36.281.20408
49. Wale, A, Chelkeba, L, Wobie, Y, and Abebe, A. Treatment outcome and associated factors of neonatal Sepsis at Mizan Tepi university teaching hospital, south West Ethiopia: a prospective observational study. Pediatric Health Med Ther. (2021) 12:467–79. doi: 10.2147/PHMT.S322069
50. John, B, David, M, Mathias, L, and Elizabeth, N. Risk factors and practices contributing to newborn sepsis in a rural district of eastern Uganda, august 2013: a cross sectional study. BMC Res Notes. (2015) 8:339. doi: 10.1186/s13104-015-1308-4
51. Tewabe, T, Mohammed, S, Tilahun, Y, Melaku, B, Fenta, M, Dagnaw, T, et al. Clinical outcome and risk factors of neonatal sepsis among neonates in Felege Hiwot referral hospital, Bahir Dar, Amhara regional State, north West Ethiopia 2016: a retrospective chart review. BMC Res Notes. (2017) 10:265. doi: 10.1186/s13104-017-2573-1
52. Roble, AK, Ayehubizu, LM, and Olad, HM. Neonatal Sepsis and associated factors among neonates admitted to neonatal intensive care unit in general hospitals, eastern Ethiopia 2020. Clin Med Insights Pediatr. (2022) 16:117955652210983. doi: 10.1177/11795565221098346
53. Agnche, Z, Yenus Yeshita, H, and Abdela, GK. Neonatal Sepsis and its associated factors among neonates admitted to neonatal intensive care units in primary hospitals in Central Gondar zone, Northwest Ethiopia, 2019. Infect Drug Resist. (2020) 13:3957–67. doi: 10.2147/IDR.S276678
54. Admas, A, Gelaw, B, BelayTessema, WA, and Melese, A. Proportion of bacterial isolates, their antimicrobial susceptibility profile and factors associated with puerperal sepsis among post-partum/aborted women at a referral Hospital in Bahir Dar, Northwest Ethiopia. Antimicrob Resist Infect Control. (2020) 9:14. doi: 10.1186/s13756-019-0676-2
55. Birrie, E, Sisay, E, Tibebu, NS, Tefera, BD, Zeleke, M, and Tefera, Z. Neonatal Sepsis and associated factors among newborns in Woldia and Dessie comprehensive specialized hospitals, north-East Ethiopia, 2021. Infect Drug Resist. (2022) 15:4169–79. doi: 10.2147/IDR.S374835
56. Yismaw, AE, Abebil, TY, Biweta, MA, and Araya, BM. Proportion of neonatal sepsis and determinant factors among neonates admitted in University of Gondar comprehensive specialized hospital neonatal intensive care unit Northwest Ethiopia 2017. BMC Res Notes. (2019) 12:542. doi: 10.1186/s13104-019-4587-3
57. Ogunlesi, TA, and Ogunfowora, OB. Predictors of mortality in neonatal septicemia in an underresourced setting. J Natl Med Assoc. (2010) 102:915–22. doi: 10.1016/S0027-9684(15)30710-0
58. Ogundare, E, Akintayo, A, Aladekomo, T, Adeyemi, L, Ogunlesi, T, and Oyelami, O. Presentation and outcomes of early and late onset neonatal sepsis in a Nigerian hospital. Afr Health Sci. (2019) 19:2390–9. doi: 10.4314/ahs.v19i3.12
59. West, BA, and Peterside, O. Sensitivity pattern among bacterial isolates in neonatal septicaemia in port Harcourt. Ann Clin Microbiol Antimicrob. (2012) 11:7. doi: 10.1186/1476-0711-11-7
60. Atlaw, D, Seyoum, K, Handiso, D, and Berta, M. Puerperal sepsis and associated factors among women attending postnatal care service at University of Gondar Referral Hospital. Int J Pregnancy Child Birth. (2019) 5:190–5. doi: 10.15406/ipcb.2019.05.00175
61. Alemayehu, A, Alemayehu, M, Arba, A, Abebe, H, Goa, A, Paulos, K, et al. Predictors of neonatal Sepsis in hospitals at Wolaita Sodo town, southern Ethiopia: institution-based unmatched case-control study, 2019. Int J Pediatr. (2020) 2020:1–10. doi: 10.1155/2020/3709672
62. Bejitual, K, Fikre, R, Ashegu, T, and Zenebe, A. Determinants of neonatal sepsis among neonates admitted to the neonatal intensive care unit of public hospitals in Hawassa City administration, Sidama region, Ethiopia, 2020: an unmatched, case-control study. BMJ Open. (2022) 12:e056669. doi: 10.1136/bmjopen-2021-056669
63. Demisse, GA, Sifer, SD, Kedir, B, Fekene, DB, and Bulto, GA. Determinants of puerperal sepsis among post partum women at public hospitals in west SHOA zone Oromia regional STATE, Ethiopia (institution BASEDCASE control study). BMC Pregnancy Childbirth. (2019) 19:95. doi: 10.1186/s12884-019-2230-x
64. Teshome, G, Hussen, R, Abebe, M, Melaku, G, Wudneh, A, Molla, W, et al. Factors associated with early onset neonatal sepsis among neonates in public hospitals of Sidama region, southern Ethiopia, 2021: unmatched case control study. Ann Med Surg. (2022) 81:104559. doi: 10.1016/j.amsu.2022.104559
65. Adatara, P, Afaya, A, Salia, SM, Afaya, RA, Konlan, KD, Agyabeng-Fandoh, E, et al. Risk factors associated with neonatal Sepsis: a case study at a specialist Hospital in Ghana. Sci World J. (2019) 2019:1–8. doi: 10.1155/2019/9369051
66. Gebremedhin, D, Berhe, H, and Gebrekirstos, K. Risk factors for neonatal Sepsis in public hospitals of Mekelle City, North Ethiopia, 2015: unmatched case control study. PLoS One. (2016) 11:e0154798. doi: 10.1371/journal.pone.0154798
67. Masanja, PP, Kibusi, SM, and Mkhoi, ML. Predictors of early onset neonatal Sepsis among neonates in Dodoma, Tanzania: a case control study. J Trop Pediatr. (2020) 66:257–66. doi: 10.1093/tropej/fmz062
68. Akalu, TY, Gebremichael, B, Desta, KW, Aynalem, YA, Shiferaw, WS, and Alamneh, YM. Predictors of neonatal sepsis in public referral hospitals, Northwest Ethiopia: a case control study. PLoS One. (2020) 15:e0234472. doi: 10.1371/journal.pone.0234472
69. Dirirsa, DE, Dibaba Degefa, B, and Gonfa, AD. Determinants of neonatal sepsis among neonates delivered in Southwest Ethiopia 2018: a case-control study. SAGE Open Med. (2021) 9:205031212110270. doi: 10.1177/20503121211027044
70. Kayom, VO, Mugalu, J, Kakuru, A, Kiguli, S, and Karamagi, C. Burden and factors associated with clinical neonatal sepsis in urban Uganda: a community cohort study. BMC Pediatr. (2018) 18:355. doi: 10.1186/s12887-018-1323-4
71. Alemu, M, Ayana, M, Abiy, H, Minuye, B, Alebachew, W, and Endalamaw, A. Determinants of neonatal sepsis among neonates in the northwest part of Ethiopia: case-control study. Ital J Pediatr. (2019) 45:150. doi: 10.1186/s13052-019-0739-2
72. Kayange, N, Kamugisha, E, Mwizamholya, DL, Jeremiah, S, and Mshana, SE. Predictors of positive blood culture and deaths among neonates with suspected neonatal sepsis in a tertiary hospital, Mwanza-Tanzania. BMC Pediatr. (2010) 10:39. doi: 10.1186/1471-2431-10-39
73. Ogunlesi, TA, Ogunfowora, OB, Osinupebi, O, and Olanrewaju, DM. Changing trends in newborn sepsis in Sagamu, Nigeria: bacterial aetiology, risk factors and antibiotic susceptibility. J Paediatr Child Health. (2011) 47:5–11. doi: 10.1111/j.1440-1754.2010.01882.x
74. Ogundare, E, Akintayo, A, Florence, D, Okeniyi, J, Adeyemi, A, Ogunlesi, T, et al. Neonatal Septicaemia in a rural Nigerian hospital: Aetiology, presentation and antibiotic sensitivity pattern. Br J Med Med Res. (2016) 12:1–11. doi: 10.9734/BJMMR/2016/22325
75. Siakwa, M, Kpikpitse, D, Mupepi, S, and Semuatu, M. Neonatal Sepsis in rural Ghana: a case control study of risk factors in a birth cohort. Peer Reviewed Articles. (2014); Available at:https://scholarworks.gvsu.edu/kcon_articles/43
76. Sterne, JAC, Sutton, AJ, Ioannidis, JPA, Terrin, N, Jones, DR, Lau, J, et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. (2011) 343:d4002. doi: 10.1136/bmj.d4002
77. Seale, AC, Mwaniki, M, Newton, CRJC, and Berkley, JA. Maternal and early onset neonatal bacterial sepsis: burden and strategies for prevention in sub-Saharan Africa. Lancet Infect Dis. (2009) 9:428–38. doi: 10.1016/S1473-3099(09)70172-0
78. Alam, MM, Saleem, AF, Shaikh, AS, Munir, O, and Qadir, M. Neonatal sepsis following prolonged rupture of membranes in a tertiary care hospital in Karachi, Pakistan. J Infect Dev Ctries. (2014) 8:067–73. doi: 10.3855/jidc.3136
79. Onyedibe, KI, Utoh-Nedosa, AU, Okolo, M, Onyedibe, KIO, Ita, OI, Udoh, UA, et al. Impact of socioeconomic factors on neonatal Sepsis in Jos. Nigeria Jos J Med. (2012) 6:54–8.
80. Murthy, S, Godinho, MA, Guddattu, V, Lewis, LES, and Nair, NS. Risk factors of neonatal sepsis in India: a systematic review and meta-analysis. PLoS One. (2019) 14:e0215683. doi: 10.1371/journal.pone.0215683
81. Tewari, V. Current evidence on prevention and Management of Early Onset Neonatal Sepsis. J Infect Dis Ther. (2016) 4:2–5.
82. Mohamed, DA, Ibrahim, SA, and Suleman, SK. Risk factors associated with early and late-onset of neonatal Sepsis in Duhok City. Erbil J Nurs Midwifery. (2020) 3:1–10. doi: 10.15218/ejnm.2020.01
Keywords: maternal sepsis, neonatal sepsis, prevalence, associated factors, sub-Saharan Africa
Citation: Traoré FB, Sidibé CS, Diallo EHM, Camara BS, Sidibé S, Diallo A, Diarra NH, Ly BA, Ag Ahmed MA, Kayentao K, Touré A, Camara A, Delamou A, Sangho H and Terera I (2024) Prevalence and factors associated with maternal and neonatal sepsis in sub-Saharan Africa: a systematic review and meta-analysis. Front. Public Health. 12:1272193. doi: 10.3389/fpubh.2024.1272193
Edited by:
Fathiah Zakham, University of Helsinki, FinlandReviewed by:
Surajudeen Bello, Nasarawa State Ministry of Health, NigeriaConcepcion De Alba-Romero, University Hospital October 12, Spain
Copyright © 2024 Traoré, Sidibé, Diallo, Camara, Sidibé, Diallo, Diarra, Ly, Ag Ahmed, Kayentao, Touré, Camara, Delamou, Sangho and Terera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fatoumata Bintou Traoré, dGZhdG91bWF0YWJAZ21haWwuY29t