
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 13 March 2024
Sec. Life-Course Epidemiology and Social Inequalities in Health
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1270906
This article is part of the Research TopicEmerging Global Population Health Risks: From Epidemiological PerspectivesView all 14 articles
 Maria Ramos Monserrat1,2,3*
Maria Ramos Monserrat1,2,3* Jeronia Ramón Molinas3
Jeronia Ramón Molinas3 Marta Fuster Truyol2Aina Bonet Manresa2Trinidad Planas Juan1,2Juan José Montaño Moreno2,3María de los Ángeles Pérez Martín1Patricia Ruíz Armengol1Almudena Personat Labrador4Carlota María Lamilla Buades1Verónica María Carrión García1Miguel Salvá Garví1
Marta Fuster Truyol2Aina Bonet Manresa2Trinidad Planas Juan1,2Juan José Montaño Moreno2,3María de los Ángeles Pérez Martín1Patricia Ruíz Armengol1Almudena Personat Labrador4Carlota María Lamilla Buades1Verónica María Carrión García1Miguel Salvá Garví1 Catalina Nuñez Jiménez1,2
Catalina Nuñez Jiménez1,2 Elena Cabeza Irigoyen1,2
Elena Cabeza Irigoyen1,2Background: Crises and health policies to tackle them can increase health inequalities. We explored the scope and usefulness of helplines set up during the COVID-19 crisis and characterised the vulnerability of their users. This study explored the geographic and socioeconomic effects of the telephone helplines set up by the Balearic Islands Government and aimed to characterise the vulnerability of their users.
Methods: Telephonic survey combined with a geographical analysis of a sample of calls made between 15th of March and 30th of June of 2020 to five helplines: COVID-19 general information; psychological, social (minimum vital income), labour (temporary employment regulation), and housing (rental assistance) helps. The questionnaire included sociodemographic and housing characteristics, type of problem, and if it was solved or not. We used multinomial regression to explore factors associated with having solved the problem. We calculated the standardised rate of calls by municipality using Chi-squared and z-test to test differences.
Results: 1,321 interviews from 2,678 selected (231 excluded, 608 untraceable, and 518 refusals). 63.8% of women, 48.7% were born in another country. They had no internet at home in 3.1%, only on the phone in 17.3%. The 23.5% had no income at home. The Problem was solved in 25.4%, and partly in 30.9%. Factors associated with not solving the problem were not having income at home (p = 0.021), labour (p = 0.008), economic (p = 0.000) or housing (p = 0.000) problems. People from 55 of 67 municipalities did at least one call. The highest rates of calls were from coastal tourist municipalities.
Conclusion: Helplines reached most of the territory of the Balearic Islands and were used mainly in tourist municipalities. It probably has not been helpful for families with more significant deprivation. Digital inequalities have emerged.
• Helplines probably have not been helpful for the most vulnerable families in the COVID-19 crisis.
• Digital inequalities have emerged during the COVID19 pandemic that should be addressed without waiting for a new crisis.
In the COVID-19 crisis, some of the public health measures adopted, namely the lockdown policies, have exacerbated health inequalities, as happened or occurred in other pandemics (1, 2). Therefore, COVID-19 has been qualified as a “syndemic,” as it interacts with and exacerbates the consequences of the social determinants of health (3).
Since the start of the COVID-19 pandemic, many efforts have been made to identify population groups that were more vulnerable to severe COVID-19 infection or death. However, the identification and support of more vulnerable groups in terms of social and economic consequences (2, 4) should have been equally important in terms of resourcing and advocacy, because their vulnerability was exacerbated by the pandemic (5, 6).
There were many uncertainties in the COVID-19 pandemic, and the Geographic Information Systems (GIS) was essential to understand and predict the disease’s evolution, track human movements, detect and help vulnerable groups, and formulate and examine health policy interventions (7).
The Spanish Government set up different actions to reduce the social and economic consequences of COVID-19, the so-called Social Shield. These actions included ensuring a minimum vital income and enforcing measures of temporary employment regulation (8). Concurrently, the Balearic Islands Government launched phone helplines to offer information about COVID-19, to provide psychological support, and help to complete applications for the social assistance measures mentioned above, as well as a website compiling all the information related to COVID-19.1
This study explored the geographic and socioeconomic effects of the telephone helplines set up by the Balearic Islands Government and aimed to characterise the vulnerability of their users.
Descriptive study that combined a telephonic survey and a geographical analysis.
Residents in the Balearic Islands, Spain (1,171,543 inhabitants in 2020, 50.1% women). The Balearic Islands inhabited are four: Mallorca (77.9% of the Balearic Islands’ population), Menorca (8.2%), Ibiza (12.9%), and Formentera (1%). Palma is the capital city (36.1% of the Balearic Islands’ population) (9).
We selected a non-probabilistic convenience sample of telephone numbers from Balearic Islands residents who have called during the period of strict lockdown in Spain (between the 15th of March and the 30th of June 2020). We included the following helplines: COVID-19 general information; psychological help; social help, for minimum vital income; labour help, for applying to temporary employment regulation (ERTE, in Spanish) and housing rental help. Furthermore, we excluded the lines addressed to women victims of gender based violence (GBV) and minors to avoid putting them in danger. The criteria for selecting the sample were numbers that call to more lines, numbers that call more times to each line, and those that call for social and housing help. We assumed that we would include the most vulnerable people in this way. We made as many calls as we could with the resources we had. We included both mobile and landline numbers.
A team of trained health professionals called the numbers selected and interviewed the respondents’ after asking for informed consent. We made three attempts on different days and hours. The only exclusion criterion for the interview was that the phone number corresponded to a municipal service or business consultancy instead of a citizen. Interviews took place between the 1st of August 2020 and the 31st of March 2021, and they were recorded.
The research team drew up the questionnaire used (Annex 1).
(1) Sociodemographic characteristics: age, sex, country of birth, and municipality or neighbourhood of residence; number, age, and labour situation of persons living at home; (2) housing conditions: m2 of the house; access or not to exterior spaces at home (balcony, terrace, and garden); access to the internet in the house or on the mobile phone, and (3) reason for the call: type of problem or problems they called for, and if the problem they have called for was solved or not (yes, no, partly yes, and partly no).
We performed a descriptive statistical analysis with relative frequencies, a bivariate analysis with a Chi-square (X2) test to explore factors associated with the variable if the problem they have called for was solved, and multinomial regression, as the dependent variable had three categories. The software used was SPSS 17.0.
We allocated the calls according to the municipality and neighbourhood (only for Palma) on a map. Then, we calculated the rate of calls by municipality and neighbourhood by population, and we standardised them based on the overall rate for the Balearic Islands. We applied a global X2 test with a continuity correction for island, municipality, and neighbourhood to analyse the differences between the observed and the expected calls based on the total number of registered calls and the population sizes. Next, we applied an individual z-test with a continuity correction (10), controlling the alpha error through the Bonferroni correction for each island, municipality, and neighbourhood. Finally, we built a Geographical Information System (GIS) combining the information about the calls by municipality or neighbourhood (number, rate, and standardised rates) with socioeconomic information by censual section: income rates and Gini index by census section (11), and we compared the patterns visually. The software programmes used were ArcGis and QGis.
Between 15 March 2020 and 30 June 2020, 42,532 telephone numbers called to the helplines: 11.1% for COVID-19 general information, 2.0% for psychological help, 20.5% for social help, 51.4% for labour help and 24.8% for housing rental help. A sample of 2,678 numbers was selected (6.4%) (Supplementary Table 1). Finally, 1,321 interviews were performed, as 231 cases were excluded, 608 were untraceable and 518 were refusals to participate.
The sociodemographic and housing conditions of persons interviewed are shown in Table 1. Two out of three were women, with an average age of 42.25 (SD: 11.141). Half were born in another country (46 different countries). The most frequent countries of origin were Spain (667 cases), followed by Argentina (113 cases), Colombia (108 cases), Ecuador (50 cases), Morocco (36 cases) and Italy (36 cases). They lived with an average of 2.77 persons (SD: 1.423), more frequently with children (43.7%) than with aged people (10.5%). Houses had <80 m2 in 54.7% of cases, with an average of co-habitants of 2.77 (SD: 1.423), without any exterior space in 16.4% of cases and access to the internet in 3.9%, or only on the mobile phone in 17.3%. The problems they called for were mainly economic, followed by labour and housing. 23.5% of interviewers declared that they had no income at home, and in 21.3% of cases, there was someone in the house in ERTE. Only 7% of the people interviewed said they had a psychological problem.
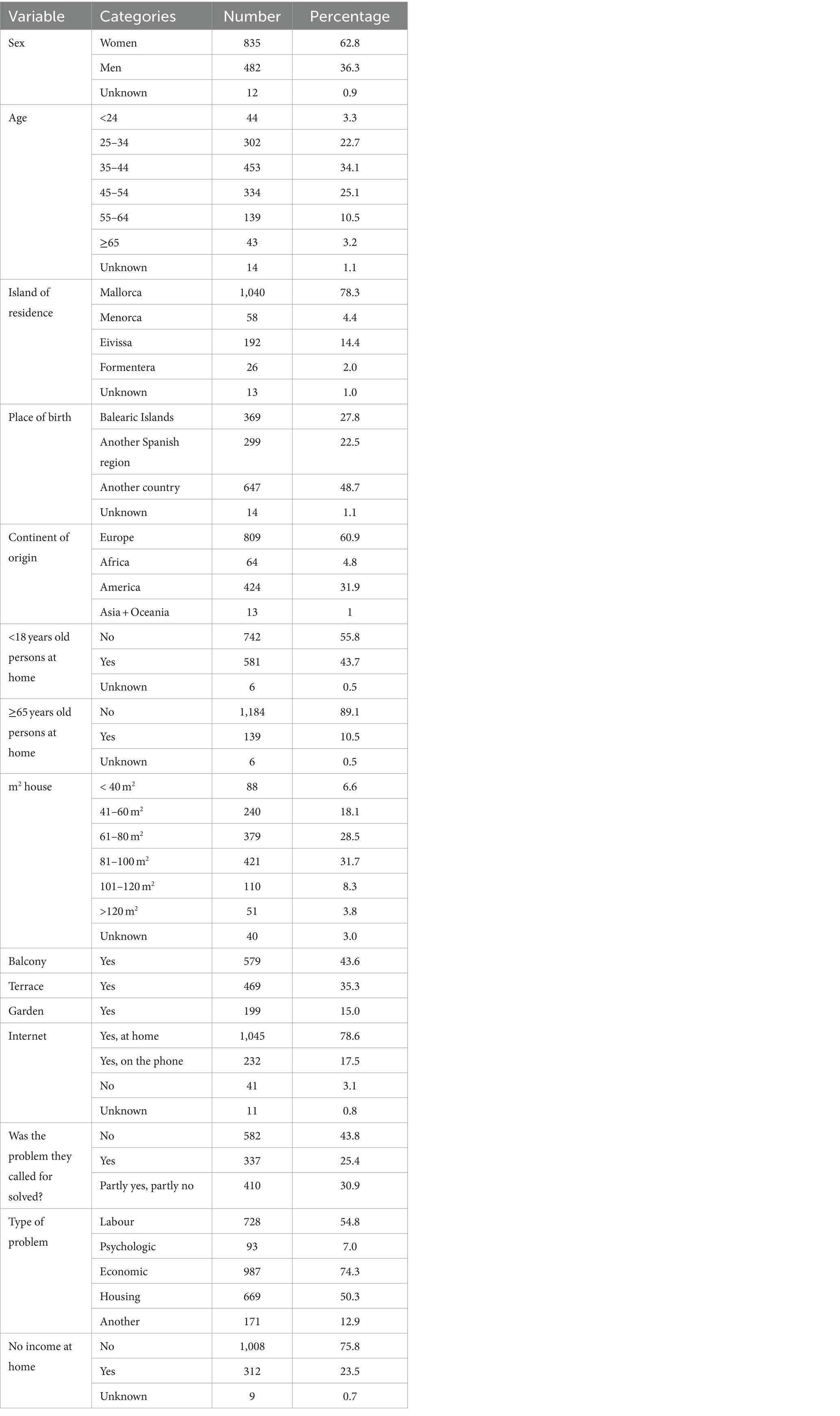
Table 1. Description of persons interviewed (N = 1,321).
Issues leading the call were solved in 25.4% of cases and partly solved in 30.9%. The factors associated with not solving the problem were in the unadjusted analysis: having no income at home (p < 0.001), having no internet (p < 0.05), having children at home (p < 0.01) and having no one in ERTE (p < 0.05). After the multinomial regression, factors associated with not solving the problem were having no income at home (p < 0.05) or if the problem was of labour (p < 0.005), economic (p < 0.001) or housing (p < 0.001) (Table 2).
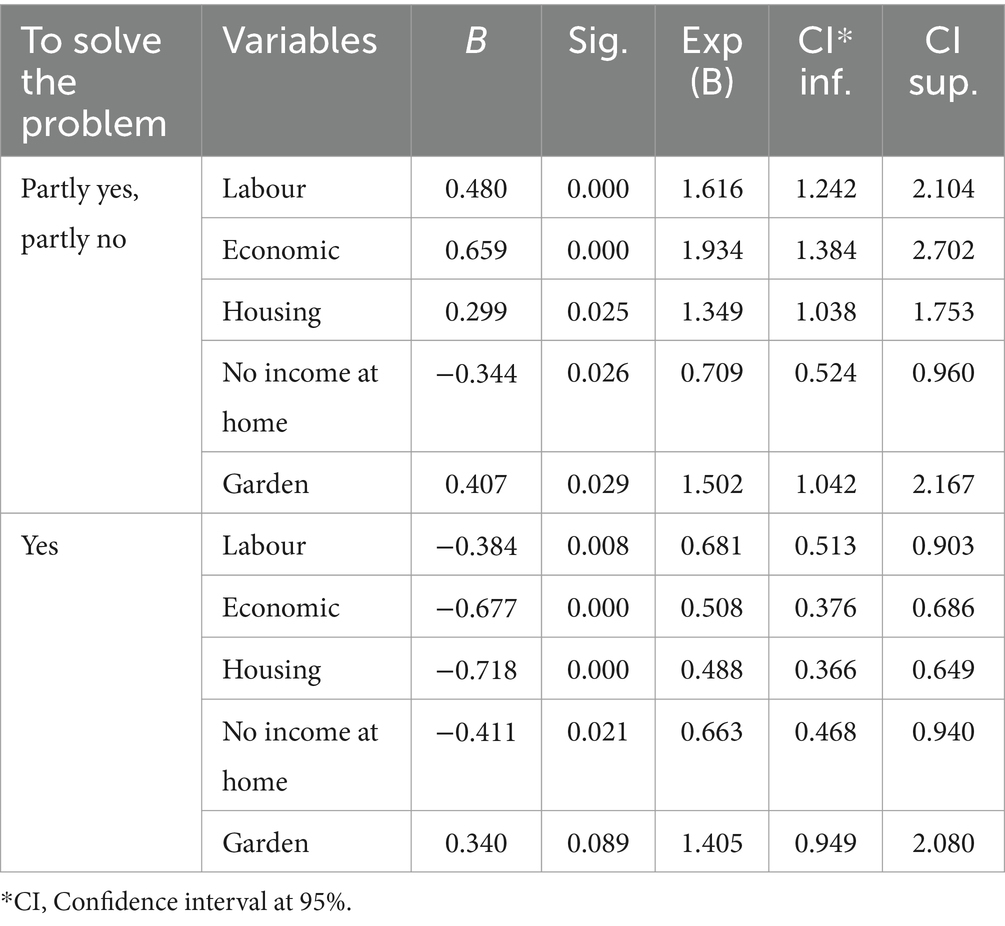
Table 2. Multinomial regression of factors associated with not solving the problem (No, as reference).
Regarding geographical distribution, a 78.3% of calls were from Mallorca, 4.4% from Menorca, 14.4% from Ibiza and 2% from Formentera. The number of calls was higher than expected in Formentera (p < 0.05). Instead, it was significantly lower than expected in Menorca (p < 0.05).
At least one call was made from 55 municipalities and none from 12 (11 of Mallorca and one of Menorca). Nearly, a half of the calls (46.4%) were made from Palma city. After standardisation of call rates, we observed that the municipalities with lower calls or no calls were municipalities with low population and high income in the Tramuntana mountain range or with lower income in the interior of the island of Mallorca (Figure 1). Instead, the municipalities with the highest call rates (Figure 2) were tourist municipalities on the coast or near Palma. There were significant differences between the observed calls and the expected calls by each municipality (p < 0.005). Only six municipalities presented rates significantly over expected (p < 0.05), and only one lower than expected (p < 0.05), apart from the 12 without calls.
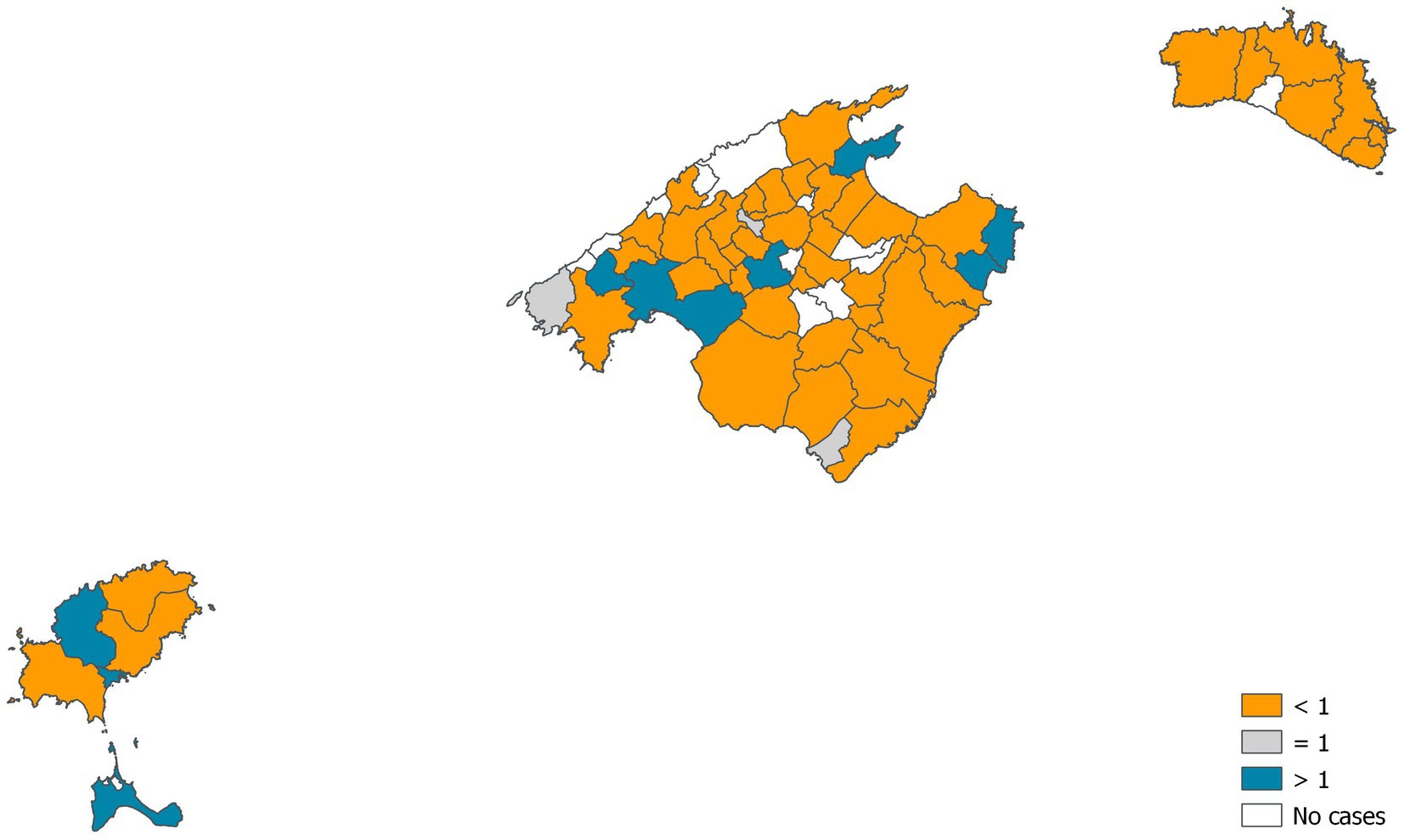
Figure 1. Standardised rates of calls by municipalities.
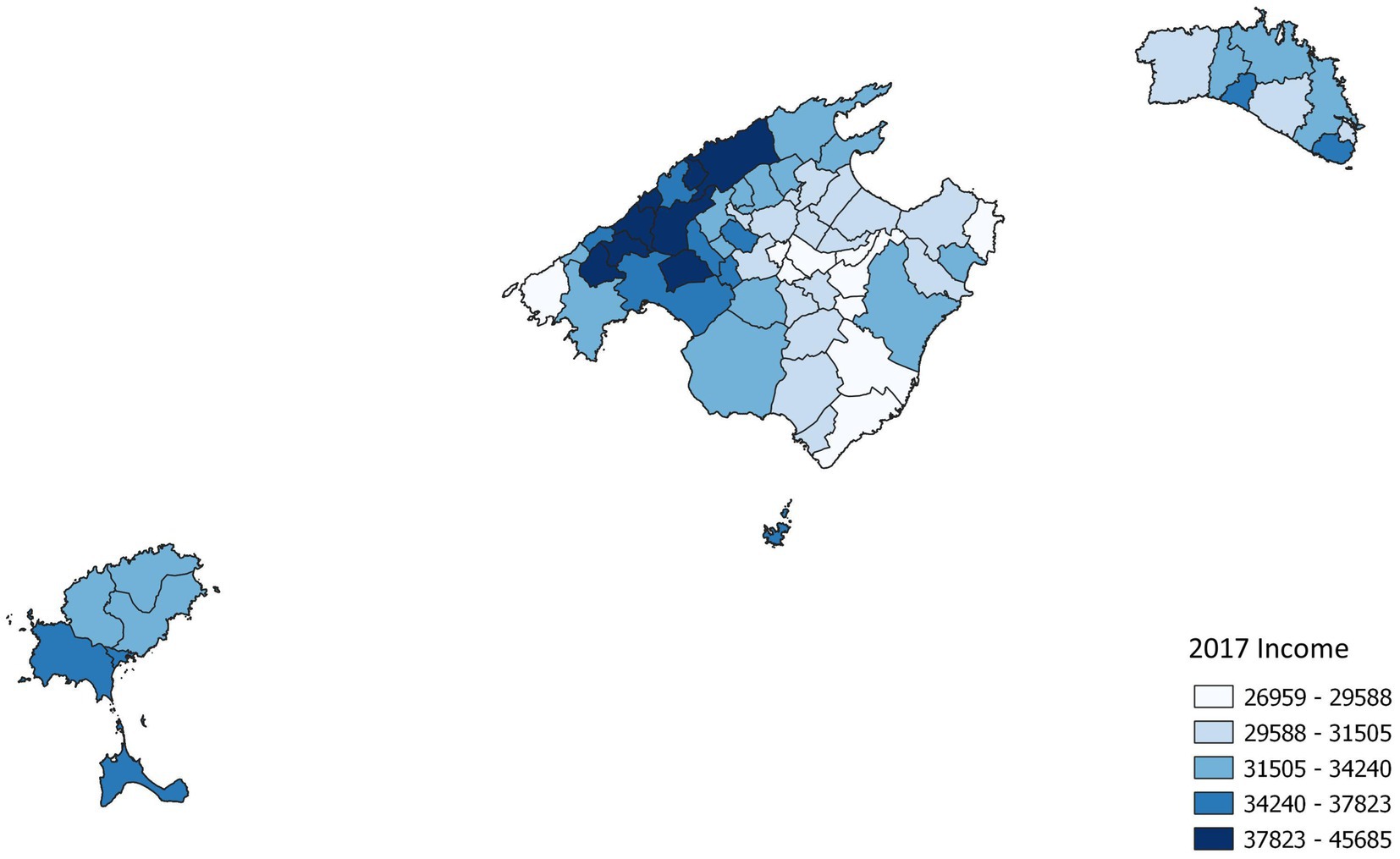
Figure 2. Income rates by municipalities.
In Palma city, there were calls from 71 of 88 neighbourhoods. The neighbourhoods with rates under the expected number of calls or without calls were sparsely populated and in a situation of extreme wealth or poverty. Whilst neighbourhoods with the highest rates of calls were underprivileged and populated. There were significant differences between the observed calls and the expected calls by neighbourhood (p < 0.005). Only five neighbourhoods presented rates significantly higher than expected (p < 0.05).
When comparing standardised calls with income rates and the Gini index, we did not observe clear patterns for municipalities or neighbourhoods in Palma (Supplementary Figures 1–4).
We have observed that the phone helplines covered all islands and most municipalities. However, there were significant differences in their use, being higher in touristic areas. It is coherent with the economy of the Balearic Islands, based on tourism. The main reported problems were economic, labour and housing, all three interconnected and related to the interruption of tourism activities, mainly bars, restaurants and hotels.
Users of the lines were working-age people, mainly women and immigrants, reinforcing the vulnerability of immigrant people, especially women (12) working in the domestic environment (13). The absence of older people both among the persons interviewed and among the people who live with them, which we attribute to the fact that they have a pension. Our results support the idea that the social consequences of the COVID-19 crisis are associated with young age, female gender and poor economic conditions (14).
Psychological helplines were used less than expected, despite, lockdowns negatively impacting mental Health and economic difficulties are significant stressors in these situations (15). Our results suggest that offering and announcing a psychological helpline is not enough to help the people with psychological distress during a global health crisis like COVID-19, especially when the visits to the health centres are discouraged to prevent the spreading of the disease. Indeed, the stressors are related to gender, economic difficulties, worry about work, lack of information, trust in the institutional response and fear of infection (14–18).
We have identified a non-negligible percentage of people who declared no income, and this circumstance was associated with not having solved the problem through the helpline. Therefore, we hypothesise that the helplines could not help the families that need them most, that is, the families with severe financial difficulties emerge as the most vulnerable (19). We believe that a combined approach to this population group through community networks and agents (20) from day 1 of the crisis could have mitigated the social consequences of COVID-19. In the Balearic Islands, we have done it as a strategy to reduce the cases. However, we discovered that these families had difficulties maintaining lockdown conditions due to housing and employment issues.
At the same time, there is also a non-negligible percentage of people without internet at home, having it only on their phone. In this pandemic, the importance of digital inequalities has emerged as a new public health challenge (21). Smartphones have proven to be a valuable tool for searching for health information, social support between peers (4, 13) and rapid assessment of people’s needs (22) or mental health state (16). Nevertheless, we have seen in this study that smartphones are insufficient for applying for official help. Beaunoyer and colleagues have proposed strategies for reducing digital inequalities, targeting both individuals’ access and use of technologies and the messages’ quality, understandability, and acceptability (21). In the Balearic Islands, social workers have been overwhelmed trying to help people apply for official help, and the Government provided laptops to schoolchildren without them. Nevertheless, there is much work to do to reduce digital inequities in order to prepare for future crises through the joint work of Technology, Education and Social Services departments with municipalities.
We designed the study in April–May 2020, the interviews started in September 2020, and we presented the results in the second half of 2021. This time span is undoubtedly too long and has been useless for this crisis, although it can teach us things for the future. We suggest designing a global strategy to evaluate helplines, using rapid online surveys (16, 22), probably immediately after the call, as commercial companies do.
One of the problems we have had is that we expected that the phone companies would provide us with the geographical location of all the calls. Finally, this was not possible, so we had to work with a sample asking for this information during the interviews. The questionnaire included only the municipality and neighbourhood, as we were afraid that people would not feel comfortable giving us their address. However, we verified that people had no problem giving us their address during the fieldwork. Addresses would allow us to do a more accurate geographic analysis, especially to compare the call rates with economic layers. We believe that the lack of visual correlation of call rates with socioeconomic information is due to the imprecision of the unit used for call rates (municipality or neighbourhood) as the unit for socioeconomic information was the census section. Therefore, we have suffered the modifiable area unit problem or ecological fallacy (23).
We believe that the combination of methodologies has been a wise choice, especially the inclusion of geographic analysis to evaluate a public health measure as the development of different helplines to mitigate the social and economic effects of a health crisis such as COVID-19. We have also used qualitative methods (24) to investigate the problems for which people called into these lines.
As far as we know, this is the first study that aims to evaluate the geographical and social effectiveness of different helplines during a health crisis. Other authors have explored the scope and usefulness but only of psychological helplines (25, 26). Other authors had used helpline calls during the COVID-19 crisis as a proxy for the mental health status of the population, observing that the number of calls increased when the restrictive measures were implemented and decreased when such measures were revoked (27).
COVID-19 has changed the world and provided an opportunity to improve it (28), although how tourism is coming back to the Balearic Islands makes us doubt it. For future pandemics, as we know that “those most vulnerable will be the hardest hit” (29), the core idea that “this size does not fit all” (30) should be applied from the beginning. The collection of socioeconomic data of cases could aid (31) but probably it will not be enough. It is necessary to be closer to the people that suffer, and primary care professionals, social workers and mental health specialists are well positioned to do it. Significant coordination between them would be convenient for a future crisis (32).
The helplines set up by the Balearic Islands to mitigate the social and economic consequences of COVID-19 arrived at all islands, and most municipalities, but they have probably been no help for the most deprived families. Migrants, women, workers in the tourism sector and especially families without any income were the most vulnerable groups. Digital inequalities have emerged, and they should be addressed without waiting for a new crisis. At the same time, it seems crucial to deal with collaborative efforts between public health, primary health care, social work, and mental health sectors. The development of a global strategy for evaluating the helplines using rapid online surveys could also identify the most vulnerable groups affected by the sanitary crisis.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Balearic Islands Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
MR: Conceptualization, Data curation, Formal Analysis, Investigation, Project administration, Validation, Writing – original draft. JR: Conceptualization, Methodology, Supervision, Visualization, Writing – review & editing. MF: Data curation, Formal Analysis, Investigation, Methodology, Visualization, Writing – review & editing. AB: Data curation, Investigation, Validation, Writing – review & editing. TP: Investigation, Writing – review & editing. JM: Formal Analysis, Methodology, Writing – review & editing. MP: Investigation, Writing – review & editing. PR: Investigation, Writing – review & editing. AP: Investigation, Writing – review & editing. CL: Investigation, Writing – review & editing. VC: Investigation, Writing – review & editing. MS: Data curation, Methodology, Validation, Writing – review & editing. CN: Investigation, Writing – review & editing. EC: Conceptualization, Methodology, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. IdISBa, grant number COVID-19/2 have funded the study.
We are deeply grateful to all persons interviewed for their time and story. We hope that their situation improves soon.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1270906/full#supplementary-material
1. Marmot, M, and Allen, J. COVID-19: exposing and amplifying inequalities. J Epidemiol Community Health. (2020) 74:jech-2020-214720–2. doi: 10.1136/jech-2020-214720
2. Wright, L, Steptoe, A, and Fancourt, D. Are we all in this together? Longitudinal assessment of cumulative adversities by socioeconomic position in the first 3 weeks of lockdown in the UK. J Epidemiol Community Health. (2020) 74:jech-2020-214475–8. doi: 10.1136/jech-2020-214475
3. Bambra, C, Riordan, R, Ford, J, and Matthews, F. The COVID-19 pandemic and health inequalities. J Epidemiol Community Health. (2020) 74:jech-2020-214401–5. doi: 10.1136/jech-2020-214401
4. Park, HJ, and Leeb, JB. The role of social work for foreign residents in an epidemic: the MERS crisis in the Republic of Korea. Soc Work Public Health. (2016) 31:656–64. doi: 10.1080/19371918.2016.1160352
5. Glover, RE, van Schalkwyk, MC, Akl, EA, et al. A framework for identifying and mitigating the equity harms of COVID-19 policy interventions. J Clin Epidemiol. (2020) 128:35–48. doi: 10.1016/j.jclinepi.2020.06.004
6. The Lancet. Redefining vulnerability in the era of COVID-19 (editorial). Lancet. (2020) 395:1089. doi: 10.1016/S0140-6736(20)30757-1
7. Franch-Pardo, I, Napoletano, BM, Rosete-Verges, F, and Billa, L. Spatial analysis and GIS in the study of COVID-19. A review. Sci Total Environ. (2020) 739:140033. doi: 10.1016/j.scitotenv.2020.140033
8. Subdirección General de Promoción, Prevención y Calidad (2021). Dirección General de Salud Pública. Ministerio de Sanidad. Equidad en salud y COVID-19. Available at: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/COVID19_Equidad_en_salud_y_COVID-19.pdf [Accessed April 08, 2021).
9. Institut d’Estadística de les Illes Balears (IBESTAT) (2021). Estadísticas de población. Padrón. Available at: https://ibestat.caib.es/ibestat/estadistiques/poblacio/padro/2acef6cf-175a-4826-b71e-8302b13c1262 (Accessed April 08, 2021).
10. Regidor, E, de Mateo, S, Rodríguez, C, and Gutiérrez-Fisac, JL. An evaluation of the statistical significance and calculation of the confidence interval for the standardized mortality ratio. Gac Sanit. (1993) 7:237–43. doi: 10.1016/S0213-9111(93)71156-5
11. Instituto Nacional de Estadística (INE) (2021). Atlas de distribución de renta de los hogares. Available at: https://www.ine.es/experimental/atlas/experimental_atlas.htm (Accessed January 09, 2021).
12. Wenham, C, Smith, J, and Morgan, R. COVID-19: the gendered impacts of the outbreak. Lancet. (2020) 395:846–8. doi: 10.1016/S0140-6736(20)30526-2
13. Liem, A, Wang, C, Wariyanti, Y, Latkin, CA, and Hall, BJ. The neglected health of international migrant workers in the COVID-19 epidemic. Lancet. (2020) 7:E20. doi: 10.1016/S2215-0366(20)30076-6
14. Jacques-Aviñó, C, López-Jiménez, T, Medina-Perucha, L, de Bont, J, Gonçalves, AQ, Duarte-Salles, T, et al. Gender-based approach on the social impact and mental health in Spain during COVID-19 lockdown: a cross-sectional study. BMJ Open. (2020) 10:e044617. doi: 10.1136/bmjopen-2020-044617
15. Brooks, SK, Webster, RK, Smith, LE, Woodland, L, Wessely, S, Greenberg, N, et al. The psychological impact of quarantine and how to reduce it: rapid review of evidence. Lancet. (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
16. Ripoll, J, Contreras-Martos, S, Esteva, M, Soler, A, and Serrano-Ripoll, MJ. Mental health and psychological wellbeing during the COVID-19 lockdown: a longitudinal study in the Balearic Islands (Spain). J Clin Med. (2021) 10:3191. doi: 10.3390/jcm10143191
17. González-Sanguino, C, Ausín, B, Castellanos, MA, Saiz, J, López-Gómez, A, Ugidos, C, et al. Mental health consequences during the initial stage of the 2020 coronavirus pandemic (COVID-19) in Spain. Brain Behav Immun. (2020) 87:172–6. doi: 10.1016/j.bbi.2020.05.040
18. Prati, G. Mental health and its psychosocial predictors during national quarantine in Italy against the coronavirus disease 2019 (COVID-19). Anxiety Stress Coping. (2021) 34:145–56. doi: 10.1080/10615806.2020.1861253
19. Douglas, M, Katikireddi, SV, and McKee, M. Mitigating the wider health effects of covid-19 pandemic response. BMC Dermatol. (2020) 369:m1557. doi: 10.1136/bmj.m1557
20. Ministerio de Sanidad Redes comunitarias en la crisis de COVID-19. Available at: https://www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/Estrategia/docs/ImplementacionLocal/Redes_comunitarias_en_la_crisis_de_COVID-19.pdf (Accessed October 08, 2021).
21. Beaunoyer, E, Dupéré, S, and Guitton, MJ. COVID-19 and digital inequalities: reciprocal impacts and mitigation strategies. Comput Hum Behav. (2020) 111:106424. doi: 10.1016/j.chb.2020.106424
22. Geldsetzer, P. Use of rapid online surveys to assess People's perceptions during infectious disease outbreaks: a cross-sectional survey on COVID-19. J Med Internet Res. (2020) 22:e18790. doi: 10.2196/18790
23. Sáenz, HM. Revisando los métodos de agregación de unidades espaciales: MAUP, algoritmos y un breve ejemplo. Estud Demográfic Urban. (2016) 31:385–411. doi: 10.24201/edu.v31i2.1592
24. Labrador, AP, Juan, TP, Martín, MÁP, Armengol, PR, García, VMC, and Monserrat, MJR. Vulnerabilidad sobrevenida. El impacto social de la Covid-19. Rev ROL Enferm. (2023) 46:9–17.
25. Hermida, JRF, Santolaya, F, and García-Vera, MP. The COVID-19 psychological helpline of the Spanish Ministry of Health and Spanish psychological association: characteristics and demand. Rev Esp Salud Publ. (2020) 94:e202010138.
26. Turkington, R, Mulvenna, M, Bond, R, Ennis, E, Potts, C, Moore, C, et al. Behavior of callers to a crisis helpline before and during the COVID-19 pandemic: quantitative data analysis. JMIR Mental Health. (2020) 7:e22984. doi: 10.2196/22984
27. Arendt, F, Markiewitz, A, Mestas, M, and Scherr, S. COVID-19 pandemic, government responses, and public mental health: investigating consequences through crisis hotline calls in two countries. Soc Sci Med. (2020) 265:113532. doi: 10.1016/j.socscimed.2020.113532
28. Ahmad, A, Mueller, C, and Tsamakis, K. Covid-19 pandemic: a public and global mental health opportunity for social transformation? BMJ. (2020) 369:m1383. doi: 10.1136/bmj.m1383
29. Smith, JA, and Judd, J. COVID-19: vulnerability and the power of privilege in a pandemic (editorial). Health Promot J Austral. (2020) 31:158–60. doi: 10.1002/hpja.333
30. Sominsky, L, Walkera, DW, and Spencer, SJ. One size does not fit all – patterns of vulnerability and resilience in the COVID-19 pandemic and why heterogeneity of disease matters. Brain Behav Immun. (2020) 87:1–3. doi: 10.1016/j.bbi.2020.03.016
31. Khalatbari-Soltani, S, Cumming, RC, Delpierre, C, et al. Importance of collecting data on socioeconomic determinants from the early stage of the COVID-19 outbreak onwards. J Epidemiol Community Health. (2020) 74:jech-2020-214297–23. doi: 10.1136/jech-2020-214297
Keywords: social determinants of health, COVID-19, helplines, inequalities, territory
Citation: Ramos Monserrat M, Ramón Molinas J, Fuster Truyol M, Bonet Manresa A, Planas Juan T, Montaño Moreno JJ, Pérez Martín MdlÁ, Ruíz Armengol P, Personat Labrador A, Lamilla Buades CM, Carrión García VM, Salvá Garví M, Nuñez Jiménez C and Cabeza Irigoyen E (2024) Assessing the social impacts of the COVID-19 crisis using phone helplines. The case of the Balearic Islands, Spain. Front. Public Health. 12:1270906. doi: 10.3389/fpubh.2024.1270906
Edited by:
Cyrille Delpierre, INSERM Public Health, FranceReviewed by:
Tahmineh Mokhtari, Chinese Academy of Sciences (CAS), ChinaCopyright © 2024 Ramos Monserrat, Ramón Molinas, Fuster Truyol, Bonet Manresa, Planas Juan, Montaño Moreno, Pérez Martín, Ruíz Armengol, Personat Labrador, Lamilla Buades, Carrión García, Salvá Garví, Nuñez Jiménez and Cabeza Irigoyen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Ramos Monserrat, bXJhbW9zQGRnc2FuaXRhLmNhaWIuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.