 Yiran Deng
Yiran Deng Xianliang Wang*
Xianliang Wang*- School of Physical Education, Shandong University, Jinan City, China
Objective: This meta-analysis aimed to examine the effect of high-intensity interval training on cardiorespiratory fitness in children and adolescents with overweight or obesity, and to explore the optimal dose of high-intensity interval training to improve cardiorespiratory fitness in children and adolescents with overweight or obesity.
Methods: Randomized controlled trials on the effects of HIIT on cardiorespiratory fitness in children and adolescents with overweight or obesity were retrieved from six electronic databases, including PubMed, Web of Science, Cochrane Library, CNKI, Wanfang, and VIP. The quality assessment of the included studies was conducted following the revised quality evaluation method based on the PRISMA principles. Keywords for literature search mainly include high-intensity interval, cardiorespiratory fitness, overweight, obese, children, and adolescent, etc.
Results: (1) A total of 18 studies, comprising 581 participants (288 in the intervention group and 293 in the control group), were included and all of them were of moderate to high quality. (2) HIIT had a positive effect on the cardiorespiratory fitness levels of in children and adolescents with overweight or obesity (SMD = 0.91; 95% CI: 0.66, 1.15; p < 0.00001). (3) The improvement in cardiorespiratory fitness was more significant when the HIIT intervention lasted for more than 10 weeks (SMD = 1.04; 95% CI: 0.74, 1.34; p < 0.00001), was conducted 3 times per week, with 2 to 8 sets per session (SMD = 1.13; 95% CI: 0.71, 1.55; p < 0.00001), and maintained a ratio of approximately 1:1 between exercise and rest intervals (SMD = 1.11; 95% CI: 0.73, 1.50; p < 0.00001).
Conclusion and recommendations: (1) Long-term HIIT can improve cardiorespiratory fitness in children and adolescents with overweight or obesity. (2) To achieve significant improvements in cardiorespiratory fitness in a short period, children and adolescents with overweight or obesity can engage in HIIT programs lasting for more than 10 weeks, conducted 3 times per week, with 2 to 8 sets per session, and a ratio of approximately 1:1 between exercise and rest intervals.
Systematic Review Registration: Identifier: INPLASY202350033.
1 Introduction
Childhood and adolescent obesity and overweight have become a global public health concern. Severe obesity and overweight significantly reduce an individual’s cardiorespiratory fitness (CRF). CRF, as one of the important indicators of physical health, is crucial for maintaining overall health and quality of life. Numerous studies have demonstrated a close association between low CRF levels and increased all-cause mortality rates and the incidence of various cancers (1, 2). Additionally, children and adolescents in their developmental stage who experience prolonged low levels of cardiorespiratory fitness are at a higher risk of cardiovascular and metabolic diseases in adulthood (3, 4). Over the years, Traditional long-duration aerobic exercise (similar to a marathon) has been regarded as a crucial means to reduce fat and promote cardiorespiratory health. Engaging in over 60 min of physical exercise daily can help maintain healthy cardiorespiratory function, and when combined with dietary control or medication, it produces a potent synergistic effect on improving cardiorespiratory fitness and physical health levels in children and adolescents. However, due to high academic pressure and increased entertainment distractions, modern children and adolescents find it challenging to allocate dedicated time for physical exercise beyond school physical education classes. This is where high-intensity interval training (HIIT) comes into play as a time-efficient, highly effective, and rapidly impactful exercise modality, gradually gaining popularity among the general population.
High-intensity interval training (HIIT) is a form of exercise training that involves brief periods of intense, maximal, and explosive movements followed by lower-intensity exercise or rest intervals for recovery (5–7). Previously, HIIT has been proven to have a significant effect on obesity intervention and cardiorespiratory fitness improvement in adults as an emerging, efficient, and time-saving exercise method (8, 9). Existing research suggests that the mechanisms by which HIIT influences body fat content and cardiorespiratory function may involve enhanced fat oxidation after high-intensity exercise and an increase in the secretion of certain hormones. For example, studies by Burgomaster (10) and Talanian (11) have demonstrated that HIIT can increase fatty acid oxidation capacity, thereby accelerating fat consumption to achieve weight control. Additionally, the substantial secretion of catecholamines during HIIT exercise is also a crucial factor in driving the reduction of visceral fat. Another significant mechanism is that HIIT may reduce energy intake by suppressing appetite, consequently decreasing fat accumulation (12). In recent years, related studies and systematic reviews have indicated that HIIT has a beneficial impact on improving cardiorespiratory fitness in obese or overweight children and adolescents (13–15). There is a strong correlation between high levels of childhood obesity, elevated blood pressure, decreased cardiorespiratory fitness, and a lack of physical activity (16). Compared with traditional sports programs, HIIT is short-term, interesting and acceptable. It is a method that can efficiently improve the physical fitness and cardiorespiratory fitness of children and adolescents. Therefore, it is particularly important to explore the effect of high-intensity interval training on cardiorespiratory fitness in children and adolescents with overweight or obesity, and the optimal dose of high-intensity interval training to improve cardiorespiratory fitness in children and adolescents with overweight or obesity.
Currently, although the positive impact of high-intensity interval training on cardiorespiratory health levels has been confirmed (17–19), and there have been controlled experiments and systematic reviews on children and adolescents with overweight or obesity (20–22), the results of the above studies have not reached a consensus. Specifically, there is significant variation in the intervention effects of high-intensity interval training on cardiorespiratory fitness in children and adolescents with overweight or obesity. For example, Abdessalem Koubaa and Brooke Starkoff found that the CRF of participants in the HIIT group was only 10 to 14% higher than that of the control group at the end of their experiments, while Wing Chung Patrick Lau’s research showed that the HIIT group had a CRF value nearly 25% higher than the control group. We believe this discrepancy is closely related to differences in exercise protocols and intervention dosages in experimental designs. Additionally, with the evolution of high-intensity interval exercise, numerous recent studies have emerged on the impact of high-intensity interval training on cardiorespiratory fitness in children and adolescents with overweight or obesity. However, none of these studies have been included in a new systematic review or meta-analysis to expand our understanding of the effects of high-intensity interval training on cardiorespiratory fitness in this population. Furthermore, the existing research has not identified the optimal dose–response relationship of high-intensity interval training in improving cardiorespiratory health levels in children and adolescents with overweight or obesity.
Therefore, this study employs a Meta-analysis method, ensuring methodological quality, to quantitatively analyze randomized controlled trials involving high-intensity interval training for improving cardiorespiratory health levels in children and adolescents with overweight or obesity. The main objectives are to explore two key questions: (1) the overall impact of high-intensity interval training on improving cardiorespiratory fitness in children and adolescents with overweight or obesity, and (2) the optimal dose–response relationship of high-intensity interval training in enhancing cardiorespiratory health levels in children and adolescents with overweight or obesity. This study aims to provide objective evidence for future physical practice and health interventions aimed at improving cardiorespiratory health levels in children and adolescents with overweight or obesity.
2 Research methods
2.1 Literature search
Six electronic databases, including PubMed, Web of Science, Cochrane Library, CNKI, Wanfang, and VIP, were selected to search for randomized controlled trials (RCTs) on the effects of high-intensity interval training (HIIT) on cardiorespiratory fitness in overweight and obese children and adolescents. The search period ranged from the inception of the databases to March 31, 2023. A combination of subject terms and free-text terms was used to construct the search strategy. The English search strategy was as follows: (“high-intensity interval” OR “high-intensity interval” OR “high intensity intermittent” OR “high-intensity intermittent” OR HIIT) AND (“cardiorespiratory fitness” OR “maximal oxygen uptake” OR “peak oxygen uptake” OR CRF) AND (“children” OR “adolescent”) AND (“obese” OR “overweight”). The Chinese search strategy was as follows: SU = (“High-intensity interval training “+ “HIIT”) AND SU = “Children” + “adolescents” + “pediatric” AND SU = (“obesity” + “overweight”) AND SU = (“cardiorespiratory fitness” + CRF). A total of 1,676 relevant articles were retrieved from the electronic databases. After removing 647 duplicate articles, 1,049 articles remained for further analysis.
2.2 Inclusion and exclusion criteria
Two researchers independently assessed the inclusion and exclusion of articles. In cases of disagreement, a third researcher was consulted to reach a consensus through group discussion. The following criteria were used to include studies:
Population: the participants were children and adolescents with overweight or obesity (aged 7–17 years) without prior professional training; The participants did not have acute or chronic diseases.
Intervention: the intervention in the experimental group was HIIT.
Comparison: the intervention in the control group was normal routine or traditional aerobic training.
Outcome: the primary outcome was VO2max. The outcome measures included VO2max or tests from which VO2max values could be indirectly calculated; Secondary outcomes are duration of intervention, intervention period, frequency of intervention, etc.
Study design: published randomized controlled trials (RCTs) were eligible for inclusion, and nonrandomized studies were excluded.
2.3 Literature screening
Based on the search and removal of duplicates, 1,049 articles were obtained. Two researchers screened the titles and abstracts and conducted a full-text review, following the inclusion and exclusion criteria. A total of 1,011 articles were excluded, and ultimately, 18 articles were included in the meta-analysis. The process of literature screening is shown in Figure 1.
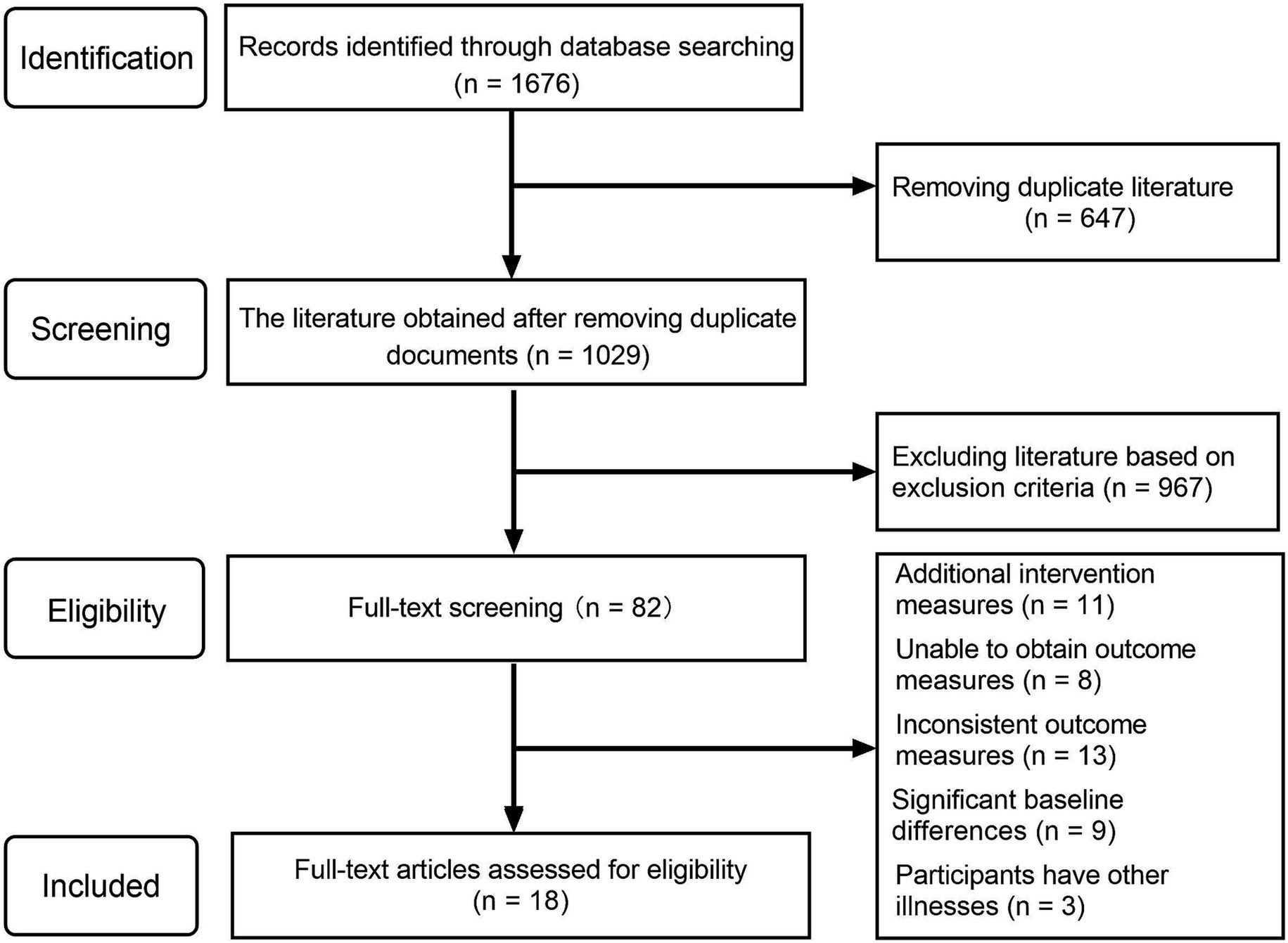
Figure 1. PRISMA flow diagram.
2.4 Characteristics of included studies
The included 18 studies were coded for their characteristics using Excel software. The following features were extracted: author, publication year, sample size, participant age, intervention dose (load time, rest time, number of intervention sets, intervention frequency, intervention duration), and outcome measures (as shown in Table 1). All 18 included studies were RCTs published after 2013. The total sample size of the studies was 581, with 288 participants in the intervention group (ranging from 7 to 23 participants per group) and 293 participants in the control group (ranging from 6 to 26 participants per group). The number of intervention sets varied from 2 to 20, and the intervention duration ranged from 4 to 24 weeks. The intervention frequency was consistent across all studies, with interventions conducted 3 times per week. Regarding outcome measures, except for three studies (Lau, Bogataj, Cvetkovic) that used the YO-YO test to indirectly estimate VO2 max, the remaining 15 studies directly measured VO2 max. The unit of measurement for VO2 max in all included studies was ml/min/kg.
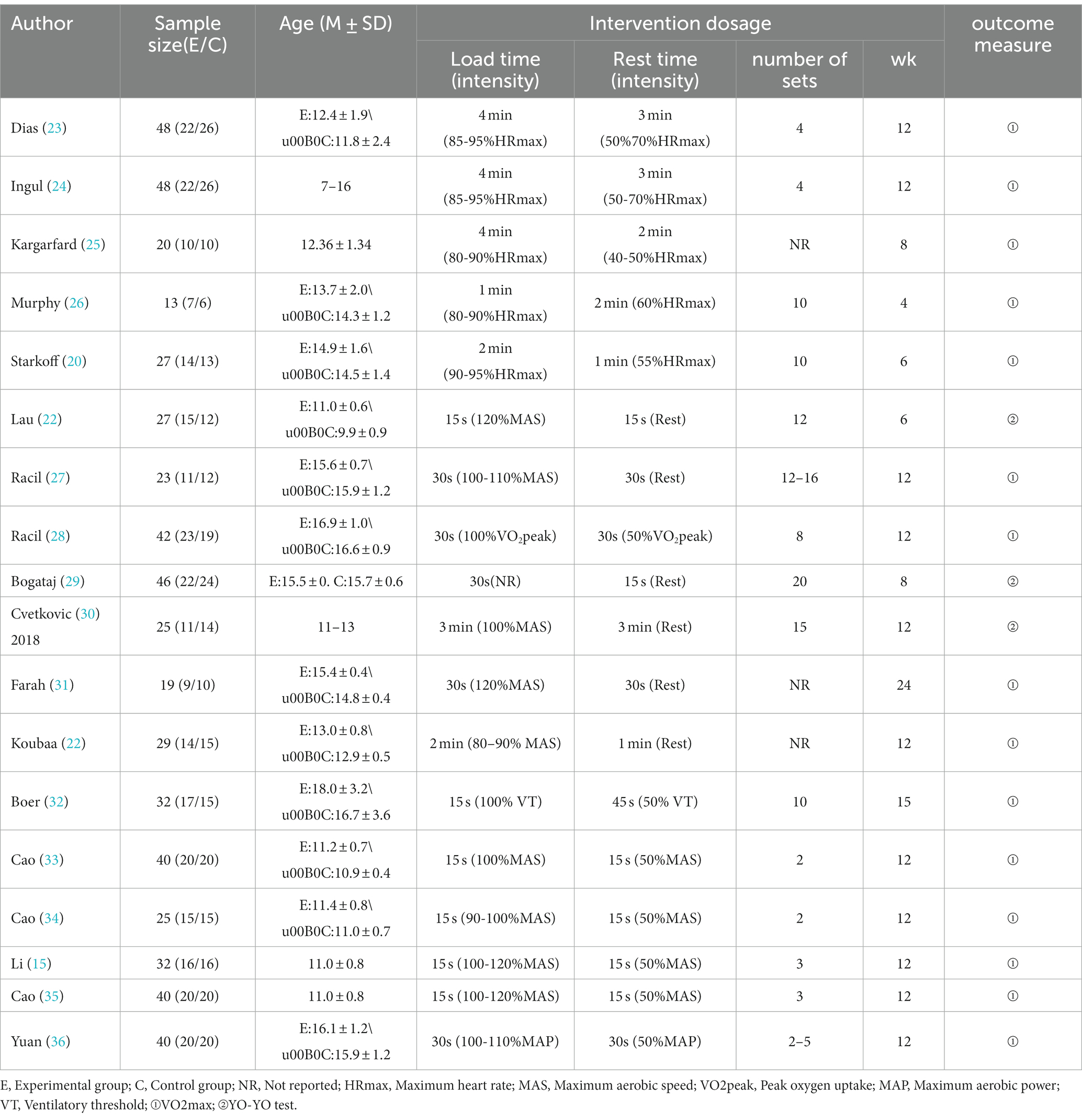
Table 1. Basic characteristics of included literature.
2.5 Quality assessment
The quality assessment of the included studies was conducted by two researchers independently, referring to the quality evaluation method revised based on the PRISMA principles by Buchheit (37). The included studies were categorized into three levels of risk: high risk (0–3 points), medium risk (4–6 points), and low risk (7–8 points) based on the cumulative evaluation score. The assessment included eight criteria: (1) clear inclusion criteria, (2) random allocation, (3) no significant baseline differences between groups, (4) blinding of outcome assessors, (5) all participants received the intended intervention or intention-to-treat analysis was performed, (6) dropout or lost to follow-up rate < 20% with detailed reasons, (7) sample size meeting the calculation requirements, and (8) reporting of effect size, precision, and results for each group (as shown in Table 2).
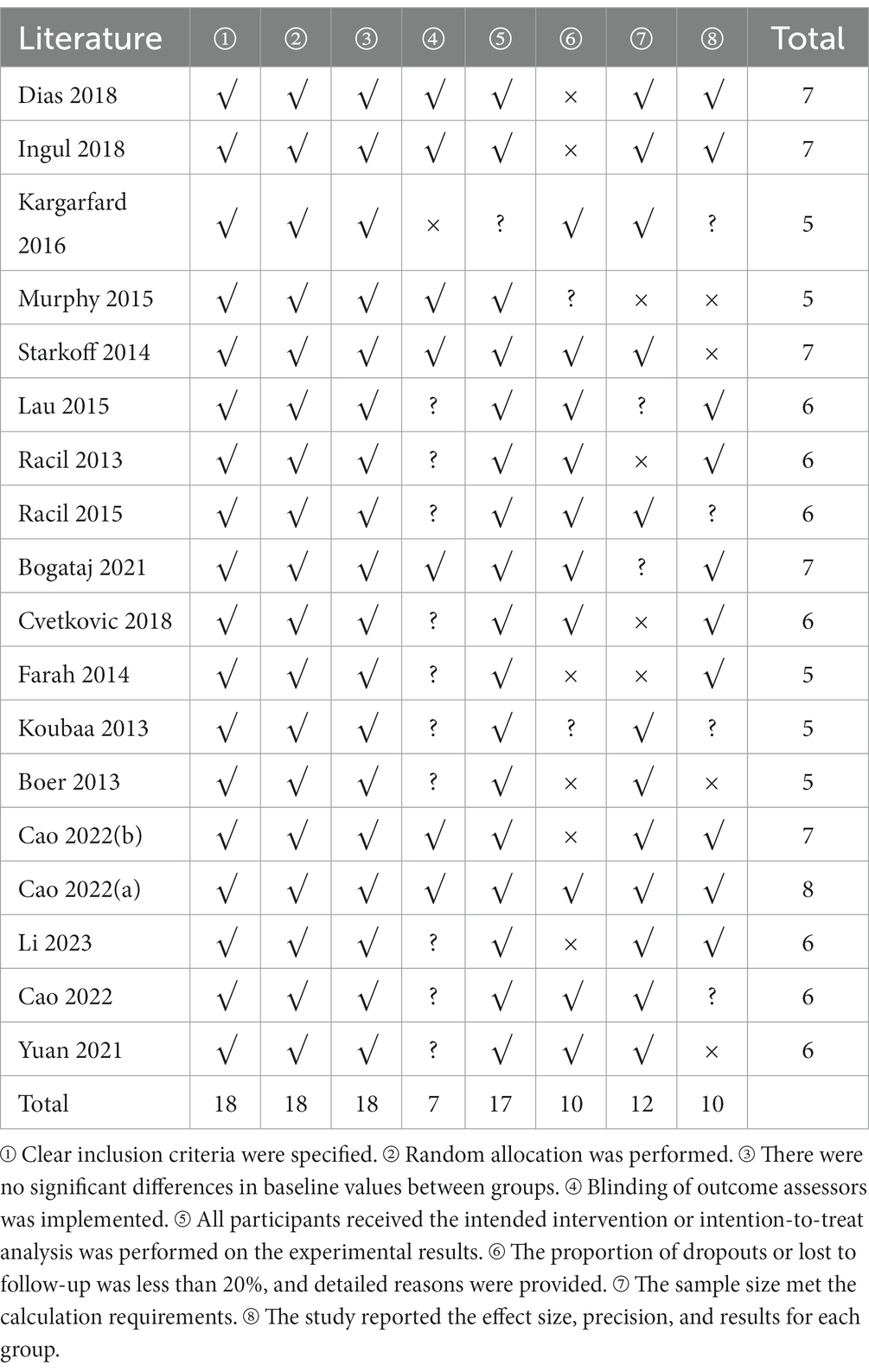
Table 2. Risk of bias evaluation of the included literature.
2.6 Data analysis
Review Manager 5.4 and Stata 17 software were used for the meta-analysis in this study. Since the included studies had continuous variables and inconsistent outcome measures, the statistical analysis was conducted using the standardized mean difference (SMD) and its 95% confidence interval (CI). A value of p < 0.05 was considered statistically significant. Additionally, Cochran’s Q test and the I2 statistic were employed to determine the magnitude of heterogeneity among studies: I2 < 25% indicates low heterogeneity, 25% < I2 < 50% indicates moderate heterogeneity, and I2 > 50% indicates high heterogeneity. A significance level of p < 0.05 indicates significant heterogeneity. Only when I2 < 50% and P > 0.05, a fixed-effects model can be used for analysis; otherwise, a random-effects model is applied. Egger’s test and funnel plots were used to assess publication bias among the included studies. If publication bias was detected, the trim and fill method was employed to assess the stability of the combined results. Additionally, sensitivity analyses were conducted using two methods to ensure the reliability of the results: (1) switching between random-effects and fixed-effects models and reanalyzing all statistical results, and (2) assessing the significant influence of each individual study by sequentially excluding one study at a time.
3 Results
3.1 Quality assessment results
After assessing the quality of the 18 included studies, it was found that 6 studies were classified as low risk (7–8 points), 12 studies were classified as medium risk (4–6 points), and no studies were classified as low quality (0–3 points). All 18 studies met the low-risk requirements in terms of inclusion criteria, random allocation, and baseline comparability. Regarding blinding, only 7 studies implemented blinding of outcome assessors, reducing the potential bias introduced by researchers’ subjective intentions. In terms of intervention implementation, only 1 study did not provide a detailed description of the intervention. Regarding dropout and description, all 18 studies reported the number of dropouts and the reasons, but 8 studies had dropout rates exceeding 20% of the original sample size. In terms of reporting results, 8 studies only reported the numerical values of outcome measures before and after the intervention, without reporting the effect size. Overall, the average risk of bias evaluation score for the included studies was 6.1, indicating a medium risk level. This suggests that future experimental studies should control dropout rates and conduct further statistical analysis on the changes in outcome measures, in addition to implementing blinding, to improve the methodological quality of study designs.
3.2 Effect of high-intensity interval training on cardiorespiratory fitness in children and adolescents with overweight or obesity
First, a test for heterogeneity was conducted on the 18 included studies, revealing moderate heterogeneity (I2 = 46%, p = 0.02). Therefore, a random-effects model was used to examine the overall effect size. According to Cohen’s criteria, effect sizes of 0.2 indicate a small effect, 0.2–0.8 indicate a moderate effect, and above 0.8 indicate a large effect. The overall pooled effect size of the 18 studies was d = 0.91. The two-tailed test result (p < 0.00001) and the 95% CI (0.66, 1.15) both indicated statistical significance. These findings demonstrate that high-intensity interval training significantly improves the cardiorespiratory fitness level of children and adolescents with overweight or obesity (Figure 2).
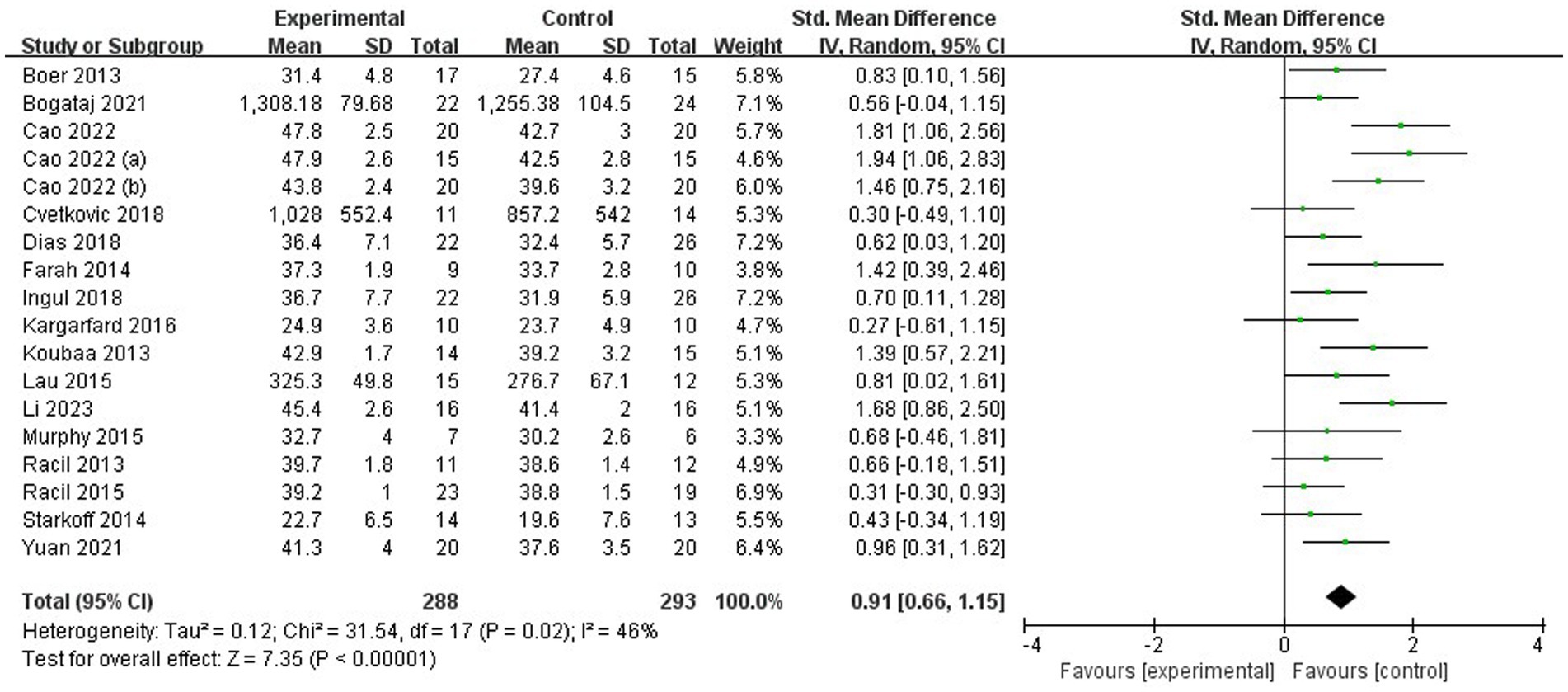
Figure 2. Meta-analysis forest plot.
3.3 Sources of heterogeneity
Based on the overall effect size analysis, it was observed that the included studies exhibited moderate heterogeneity (I2 = 46%, p = 0.02). To explore the sources of heterogeneity, this study conducted meta-regression analyses using intervention duration, number of intervention sets, load time, rest time, and load/rest time ratio as independent variables (as shown in Table 3).
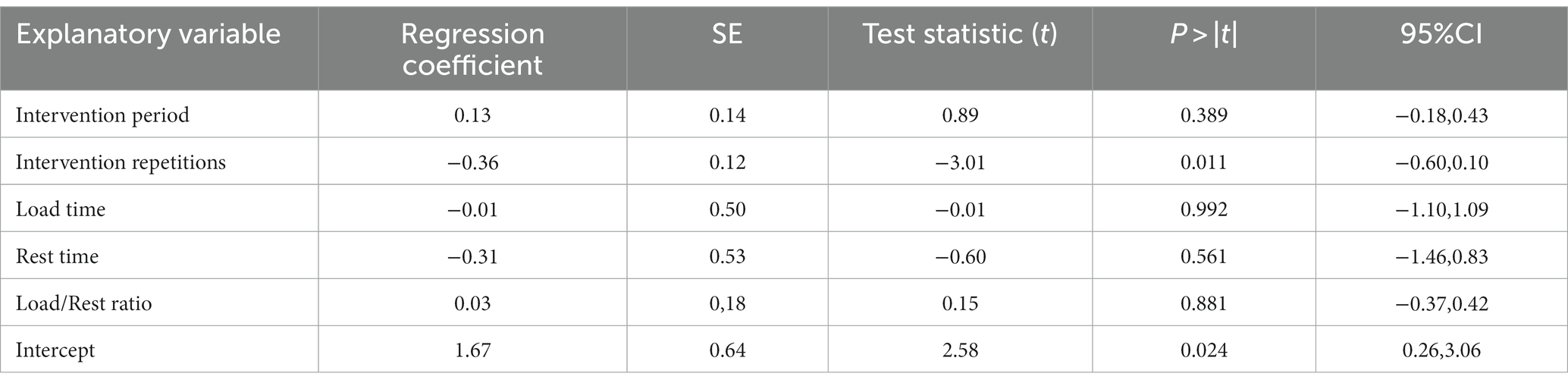
Table 3. Overview of meta-regression results.
The results of the meta-regression analysis indicate that the intervention duration, load time, rest time, and load/rest time ratio subgroups all have p values >0.05, indicating no significant differences. However, the subgroup analysis of the number of intervention sets showed a p value of 0.011 < 0.05, suggesting that the number of intervention sets is one of the sources of heterogeneity in this study. Additionally, based on the results of the meta-regression, a more detailed subgroup analysis can be conducted to explore the dose–response relationship of high-intensity interval training on improving cardiorespiratory fitness in children and adolescents with overweight or obesity.
3.4 Assessment of publication bias
To ensure the scientific rigor and validity of the research findings, an assessment of publication bias was conducted for the included studies. When the number of studies included in the meta-analysis exceeds 10, publication bias can be assessed using a funnel plot, along with Begg’s test and Egger’s test for quantitative evaluation. Firstly, based on the distribution of the 18 included studies in the funnel plot (Figures 3, 4), the results show that the effect sizes of most studies are evenly distributed on both sides of the average effect value, indicating a balanced distribution. Although there may be some slight bias toward the right side in a few individual studies, it is unlikely to have a significant impact on the overall results. Secondly, both Begg’s test (Z = 0.72, p = 0.472) and Egger’s test (t = 1.47, p = 0.161) yielded p values greater than 0.05. Therefore, it can be concluded that there is no apparent publication bias among the included studies, and the data analysis results are considered scientifically sound and rigorous.
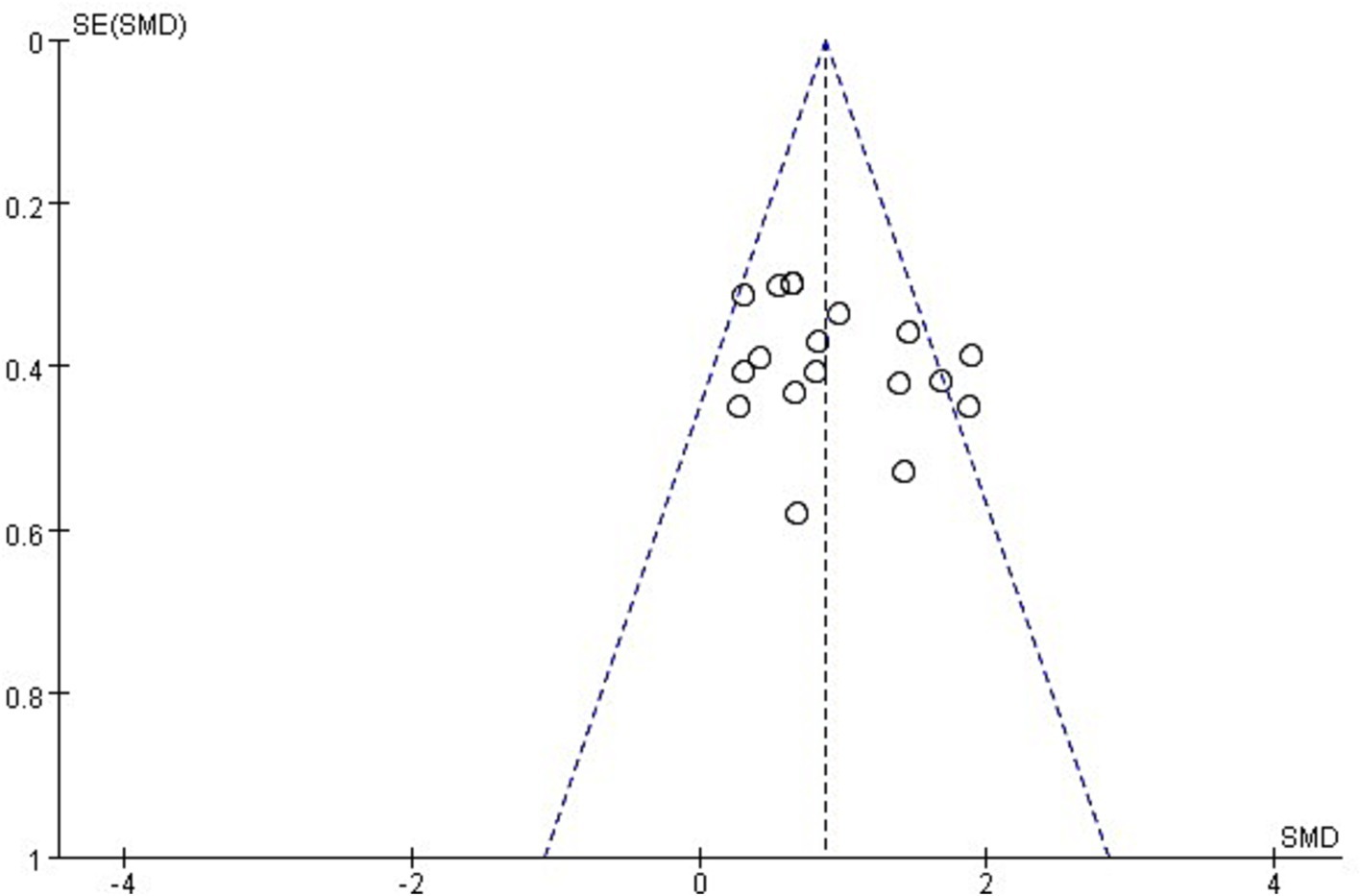
Figure 3. Funnel plot of publication bias.
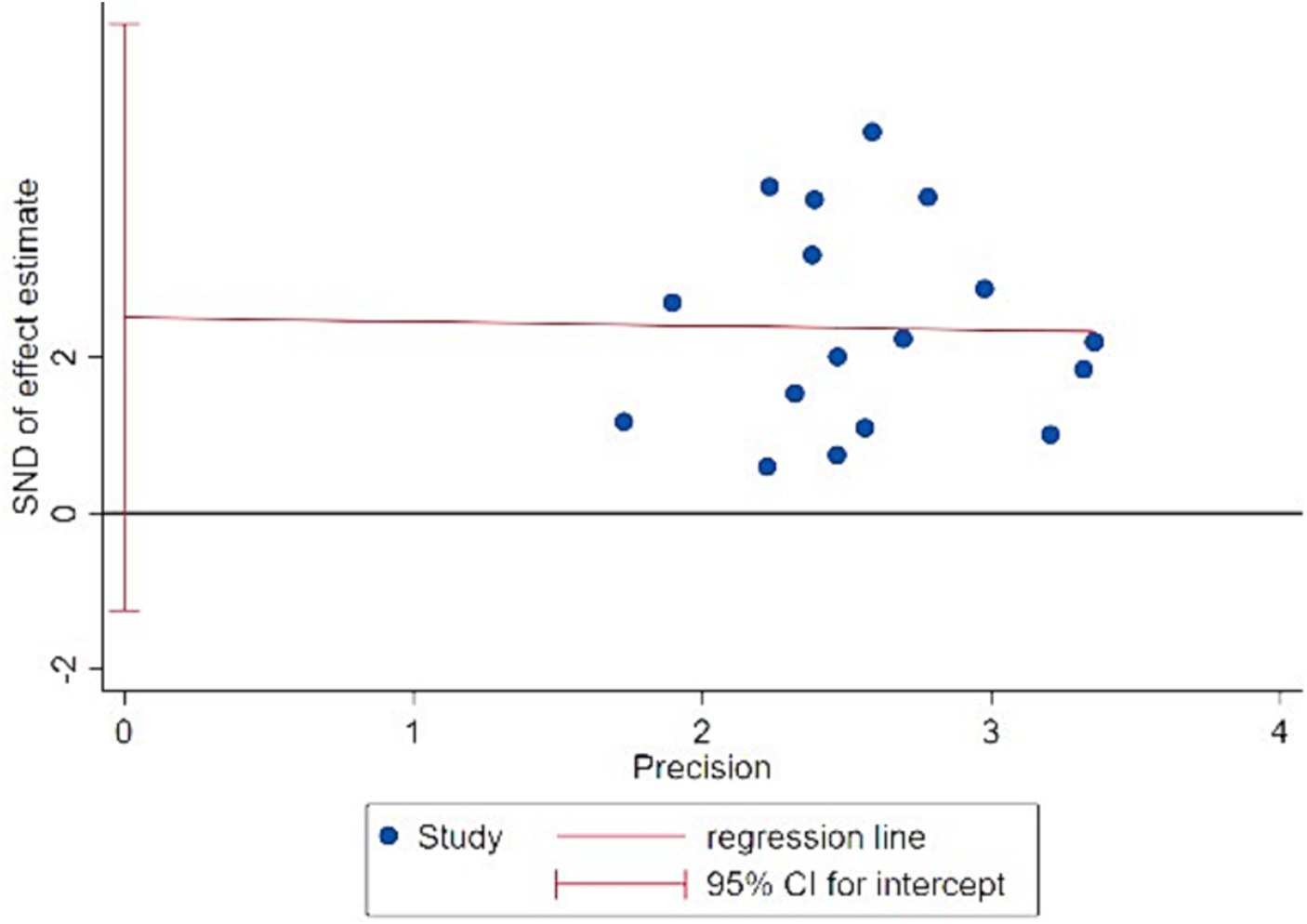
Figure 4. Egger test results chart.
3.5 Sensitivity analysis quality assessment results
To assess the reliability of this study, a sensitivity analysis was conducted by performing statistical analyses using both random-effects and fixed-effects models. The results showed that there were no significant changes in the statistical results after swapping between the two models. This indicates that the findings of the study are robust and not heavily influenced by the choice of the model.
Furthermore, a leave-one-out sensitivity analysis was conducted to examine the potential impact of each individual study on the overall results. The results showed that after removing each individual study, the range of the pooled effect size (SMD) was between 0.95 and 0.84, which still falls within the range of a large effect. The range of I2 was between 50 and 34%, and the p values were all less than 0.00001. This indicates that the removal of any single study had minimal impact on the overall effect size, and the results remained statistically significant. The analysis confirms the stability and reliability of this study.
3.6 Dose–response relationship of high-intensity interval training to improve cardiorespiratory fitness in children and adolescents with overweight or obesity
After confirming the significant positive effect of high-intensity interval training on cardiorespiratory fitness in children and adolescents with overweight or obesity, this study conducted a subgroup analysis to explore the dose–response relationship between high-intensity interval training and the improvement in cardiorespiratory fitness in this population. The analysis was conducted based on intervention duration, intervention frequency, single-bout exercise duration, single-bout rest duration, and load/rest ratio (Table 4). Since all included studies had an intervention frequency of 3 times per week, intervention frequency was not analyzed as a separate subgroup.
1) Intervention duration: in this subgroup, a total of 581 participants were included. The effect sizes among the three subgroups showed moderate heterogeneity (I2 = 57.9%), indicating that intervention duration has some influence on the relationship between high-intensity interval training and the improvement in cardiorespiratory fitness among children and adolescents with overweight or obesity. Specifically, high-intensity interval training with a duration of more than 10 weeks produced the largest effect size: SMD = 1.04, 95% CI (0.74, 1.34), p < 0.00001. The subgroup with an intervention duration of 4–8 weeks had the next highest effect size: SMD = 0.62, 95% CI (0.13, 1.12), p = 0.01. The subgroup with an intervention duration of 8–10 weeks had the smallest effect size: SMD = 0.46, 95% CI (−0.03, 0.95), p = 0.07, although it was not statistically significant.
2) Intervention frequency: in this subgroup, a total of 581 participants were included. The effect sizes among the three subgroups showed moderate heterogeneity (I2 = 49.2%), indicating that intervention frequency has some influence on the relationship between high-intensity interval training and the improvement in cardiorespiratory fitness among children and adolescents with overweight or obesity. High-intensity interval training with 2–8 intervention sets per session produced the largest effect size: SMD = 1.13, 95% CI (0.71, 1.15), p < 0.00001. The subgroup with 8–12 intervention sets had the next highest effect size: SMD = 0.80, 95% CI (0.47, 1.14), p < 0.00001. The intervention effect gradually decreased as the number of intervention sets increased, with the smallest effect size observed in the subgroup with more than 12 intervention sets: SMD = 0.57, 95% CI (0.23, 0.93), p < 0.001.
3) Single bout exercise duration: in this subgroup, a total of 581 participants were included. The effect sizes among the three subgroups showed high heterogeneity (I2 = 62.7%), indicating that single-bout exercise duration has some influence on the relationship between high-intensity interval training and the improvement in cardiorespiratory fitness among children and adolescents with overweight or obesity. The subgroup with a single bout exercise duration of 15 s to 1 min produced the largest effect size: SMD = 1.09, 95% CI (0.76, 1.42), p < 0.00001. The subgroup with a single bout exercise duration of 1–2 min had the next highest effect size: SMD = 0.84, 95% CI (0.22, 1.45), p = 0.008. The subgroup with a single bout exercise duration of 3 min or more had the smallest effect size: SMD = 0.53, 95% CI (0.19, 0.87), p = 0.002. The trend observed in the effect sizes of these three subgroups suggests that the intervention effect gradually decreases with longer single-bout exercise duration.
4) Single bout rest duration: in this subgroup, a total of 581 participants were included. The effect sizes among the three subgroups showed high heterogeneity (I2 = 51.3%), indicating that single-bout rest duration has some influence on the relationship between high-intensity interval training and the improvement in cardiorespiratory fitness among children and adolescents with overweight or obesity The subgroup with a single bout rest duration of 15 s to 1 min produced the largest effect size: SMD = 10.9, 95% CI (0.76, 1.42), p < 0.00001. The subgroup with a single bout rest duration of 1–2 min had the next highest effect size: SMD = 0.69, 95% CI (0.16, 1.21), p = 0.01. The subgroup with a single bout rest duration of 3–4 min had the smallest effect size: SMD = 0.54, 95% CI (0.08, 1.00), p = 0.02. The trend observed in the effect sizes of these three subgroups suggests that longer single-bout rest duration leads to weaker intervention effects.
5) Load/rest ratio: in this subgroup, a total of 581 participants were included. The effect sizes among the three subgroups showed high heterogeneity (I2 = 41.6%), indicating that the load/rest ratio has some influence on the relationship between high-intensity interval training and the improvement in cardiorespiratory fitness among children and adolescents with overweight or obesity. The subgroup with a load/rest ratio of 1 produced the largest effect size: SMD = 1.11, 95% CI (0.73, 1.50), p < 0.00001. The subgroup with a load/rest ratio less than 1 had the next highest effect size: SMD = 0.78, 95% CI (0.17, 1.40), p = 0.01. The subgroup with a load/rest ratio greater than 1 had the smallest effect size: SMD = 0.65, 95% CI (0.34, 0.96), p < 0.0001.
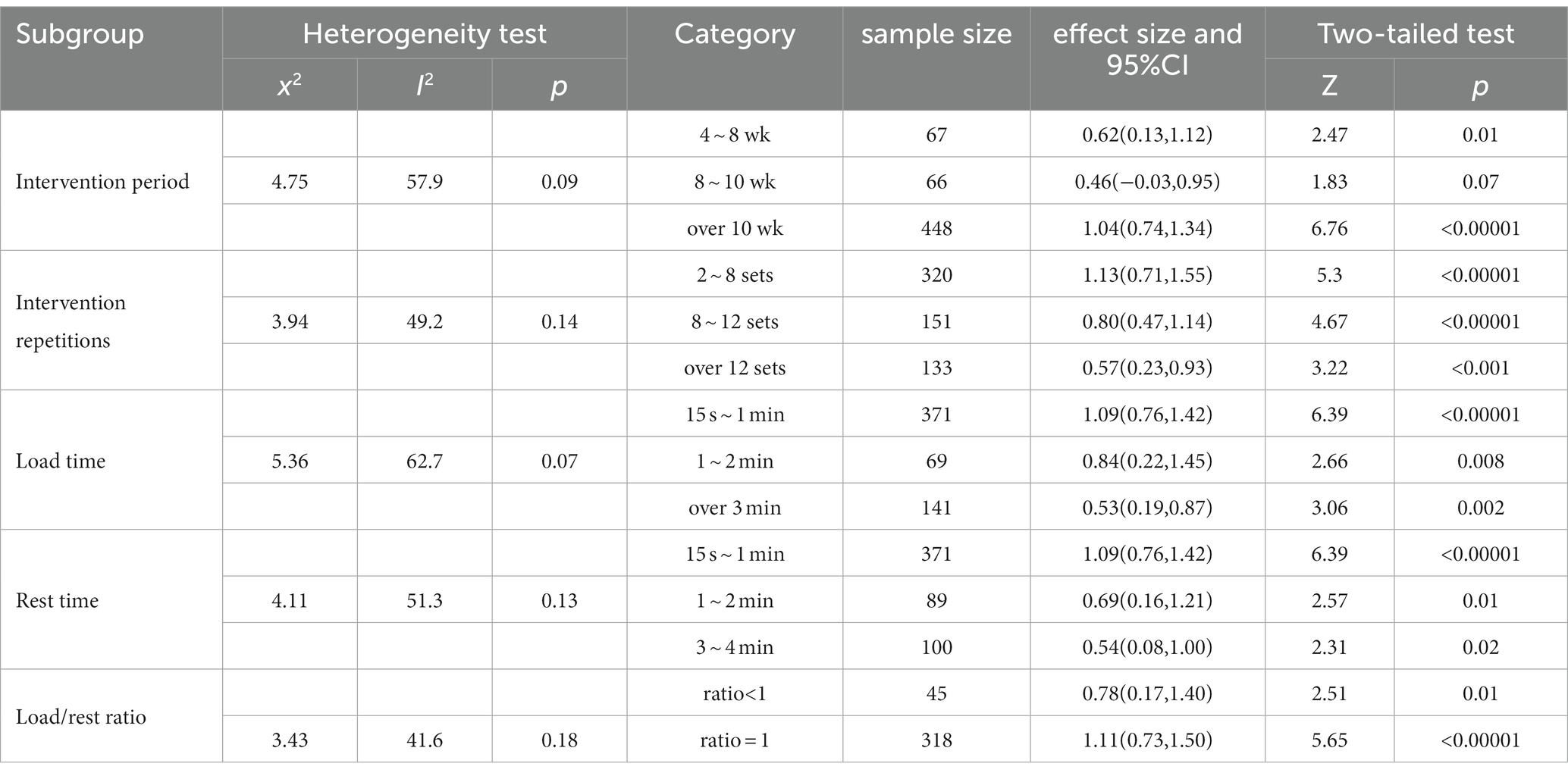
Table 4. Dose-effect relationship between high-intensity interval exercise pairs and cardiorespiratory fitness in children and adolescents with overweight or obesity.
4 Discussion
4.1 Analysis of the effect of high-intensity interval training on cardiorespiratory fitness in children and adolescents with overweight or obesity
Overall, high-intensity interval training has a significant positive effect on cardiorespiratory fitness levels in children and adolescents with overweight or obesity. This finding is consistent with previous meta-analyses and systematic reviews (38–40). Based on the synthesis of existing meta-analyses and relevant research evidence, this study concludes that high-intensity interval training has a positive effect on improving cardiorespiratory fitness levels in children and adolescents with overweight or obesity.
Regarding the mechanisms underlying the rapid improvement of cardiorespiratory fitness through high-intensity interval training, studies in the cardiovascular and skeletal muscle domains provide some insights (Figure 5). After high-intensity exercise, plasma parameters, maximal cardiac output, stroke volume, and hemoglobin levels all show significant increases. Research by Jan Helgerud (41) and Ulrik Wisløff (42) found that after a long period of HIIT training, subjects experienced an increase in cardiac output, and their maximal oxygen uptake (VO2max) was approximately 10% higher than the baseline. Furthermore, they observed significant improvements in plasma and hemoglobin levels as well as improved endothelial function in the HIIT intervention group, leading to enhanced oxygen transport efficiency and more efficient training effects in a shorter training time. Increased mitochondrial density and improved oxygen utilization in skeletal muscles may be another important reason for the significant enhancement of cardiorespiratory fitness through HIIT. In fact, related studies have confirmed that HIIT is more effective than traditional training methods in improving skeletal muscle oxidative capacity (43). From the perspective of the molecular adaptive mechanisms of skeletal muscle oxidative capacity, HIIT can activate the activity of AMPK and MAPK exercise-responsive kinases (44, 45), and increase the mRNA quantity of PGC-1α, a transcriptional factor that regulates mitochondrial oxidative function. This joint activation leads to increased transcription of mitochondrial genes and protein accumulation, resulting in the generation of more mitochondrial substances and enhancing the aerobic and anaerobic capacities of the body, ultimately improving cardiorespiratory fitness (46). In addition to the adaptive changes in the cardiovascular system and skeletal muscles, changes in ventilatory function also play a significant role in the improvement of cardiorespiratory fitness through HIIT. In intense exercise, increasing respiratory rate and depth are effective methods to obtain more energy supply. Compared to traditional training methods, HIIT can more closely simulate the respiratory rhythm and pattern of the body under high-intensity exercise scenarios, promoting adaptive improvements in ventilatory function and enhancing cardiorespiratory fitness. Studies by Ana Carolina Corte de Araujo in Brazil and Zu XiuMing in China have supported these observations. They found that obese children and adolescents who underwent HIIT interventions for more than 12 weeks showed significantly lower systolic and diastolic blood pressure and significant improvements in respiratory parameters, such as respiratory rate and alveolar ventilation (47, 48).
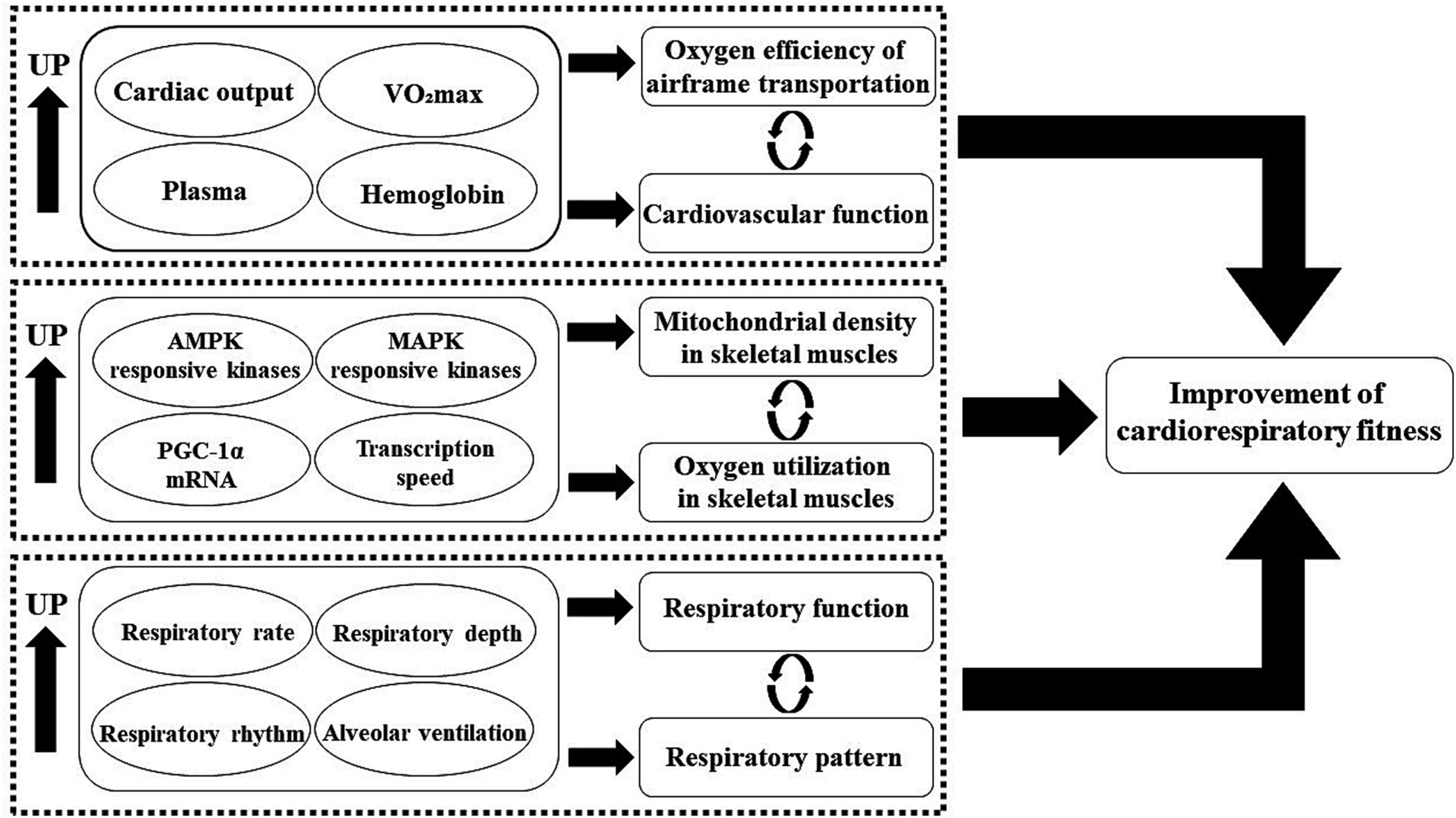
Figure 5. Mechanism of high-intensity interval training improving cardiorespiratory fitness in children and adolescents with overweight or obesity.
4.2 Analysis of the dose–response relationship of high-intensity interval training to improve cardiorespiratory fitness in children and adolescents with overweight or obesity
Based on the effects of intervention duration on the improvement of cardiorespiratory fitness in children and adolescents with overweight or obesity, interventions lasting more than 10 weeks had the largest effect size, followed by interventions lasting 4–8 weeks, and interventions lasting 8–10 weeks had the smallest effect size. Previous studies have shown that after a HIIT training period of more than 3 weeks, subjects’ cardiorespiratory function can improve by about 3 to 33% (49). As research on the optimal dose–response relationship of HIIT progresses, it has been suggested that the training period should be extended appropriately while ensuring that the total duration of each session is not less than 16 min, and the training intensity should be maintained above 7 METs (50). From the perspective of functional adaptation, long-duration high-intensity interval training can better adjust the high-energy phosphate bonds and reserves in skeletal muscles, leading to an improved oxidative potential. Considering that children and adolescents are still in the growth and development stage, their positive metabolic adaptations to physical exercise occur rapidly but have a relatively short duration. Therefore, this study suggests that high-intensity interval training lasting more than 10 weeks is likely to have the best effect on improving cardiorespiratory fitness in children and adolescents with overweight or obesity, given that other conditions are appropriate.
In terms of the number of intervention sets, 2–8 sets resulted in the largest effect size, while 8–12 sets and more than 12 sets had moderate effect sizes, showing a gradual decrease in effect size with an increasing number of intervention sets. It indicates that the intervention effect does not improve with an increasing number of sets. This may be because excessive exercise and alternating intervals can lead to fatigue in the sympathetic and parasympathetic nervous systems, weakening the central adaptation effect and reducing the intervention effect (14). Additionally, the baseline level of physical activity in most children and adolescents with overweight or obesity is not high, so increasing the number of intervention sets will significantly raise the exercise intensity. This not only fails to enhance their physical fitness and cardiorespiratory fitness but also may harm their health. Therefore, the results suggest that high-intensity interval training with 2–8 sets achieves the best effect on improving cardiorespiratory fitness in children and adolescents with overweight or obesity, and the number of exercise sets should be controlled to avoid excessive exercise.
Regarding the single-bout exercise duration and rest duration, the largest effect sizes were observed within the range of 15 s to 1 min, while durations of 1–2 min and 3 min or more resulted in moderate effect sizes, with a gradual decrease in effect size with longer durations. This indicates that longer exercise and rest durations do not necessarily lead to better results. Prolonged exercise and rest durations deviate from the essence of high-intensity interval training and make it more similar to traditional aerobic training, which hinders the rapid and effective recovery of the body and nervous system, consequently affecting the intervention effect. This is supported by the subgroup analysis of the exercise/rest duration ratio (14). When the ratio was 1:1, the intervention effect reached its maximum. It is evident that solely emphasizing exercise duration, rest duration, or intervention frequency is not scientifically appropriate for improving cardiorespiratory fitness in children and adolescents with overweight or obesity. Only when multiple influencing factors are synergistically adapted can an ideal intervention effect be achieved (38).
Although the meta-analysis suggests that high-intensity interval training interventions lasting over 10 weeks, with a frequency of 3 times per week, 2–8 sets per session, and a ratio of exercise duration to rest duration of approximately 1:1, may be the most effective for improving cardiorespiratory fitness in children and adolescents with overweight or obesity, caution should be exercised in generalizing these dose–response recommendations for the following reasons: (1) The number of included studies in this analysis was limited, and the risk of literature omission exists due to the subjective preferences and limited experience of the researchers. Further validation of the effectiveness of these results is required. (2) The included studies were conducted in different countries and regions, and the effects may vary due to factors such as different races, social backgrounds, cultural differences, and lifestyle habits among participants. Therefore, the broad application of these dose–response recommendations in improving cardiorespiratory fitness in children and adolescents with overweight or obesity needs to be further investigated through future research and experiments, considering controlling other intervention factors, to explore the effects of different intervention doses on cardiorespiratory fitness.
4.3 Limitations and shortcomings of the study health, physics and mathematics references
This study primarily investigated the optimal dose–response relationship of high-intensity interval training for improving cardiorespiratory fitness in children and adolescents with overweight or obesity. Although the study strictly followed the PRISMA guidelines, there are still some limitations and shortcomings: (1) It is possible that not all relevant previous studies were comprehensively and carefully searched and included. (2) Despite the absence of significant result biases based on publication bias tests and sensitivity analyses, there may still be potential risks of bias considering the limited number of included studies, the shortage of intervention methods, and the low proportion of high-quality studies. (3) Some included studies used the Level 1 YO-YO test to measure outcome indicators. Although this measurement method can provide the subjects’ VO2max values, the testing process may introduce uncontrollable biases, resulting in some errors in the results of this study.
5 Conclusion and recommendations
After conducting a meta-analysis of published literature to assess the impact and dose–response relationship of high-intensity interval training on cardiorespiratory fitness in children and adolescents with overweight or obesity, the study results indicate the following: (1) High-intensity interval training can significantly enhance cardiorespiratory fitness levels in children and adolescents with overweight or obesity. (2) The research suggests that, to achieve a substantial improvement in cardiorespiratory fitness in a short period, children and adolescents with overweight or obesity should engage in high-intensity interval training for more than 10 weeks, 3 times per week, with 2 to 8 sets each time. The single load time-to-interval time ratio should be maintained at around 1:1.
Additionally, based on the research results, we propose the following three recommendations: (1) Schools should provide students with sufficient space and time for physical activities, especially for children and adolescents with overweight or obesity, who require more attention. For instance, in regular physical education classes, beyond traditional activities, it is essential to integrate short-duration, multi-set, and enjoyable high-intensity interval training, considering the individual characteristics and developmental stages of overweight and obese children and adolescents. This can subtly help them enhance physical fitness and promote health. (2) After school, parents should collaboratively establish detailed plans for extracurricular physical exercises with the school and students. Encouraging and supervising students to complete the designated amount of daily physical exercise, alongside their academic tasks, will sustain and expand the positive impact of school physical education on improving students’ physical fitness. (3) In the future, there should be higher-quality and larger-sample experimental studies conducted in schools. Under the premise of ensuring methodological quality, designing more detailed and feasible experimental plans will help identify intervention strategies and long-term mechanisms to enhance cardiorespiratory fitness and overall health in overweight and obese adolescents.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
YD: Conceptualization, Data curation, Formal analysis, Project administration, Resources, Software, Validation, Visualization, Writing – original draft. XW: Funding acquisition, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The design of the study and collection, analysis were supported by National key research and development program [2020YFC2006804].
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Blair, SN, Kohl, HW, Paffenbarger, RS, Clark, DG, Cooper, KH, and Gibbons, LW. Physical fitness and all-cause mortality. A prospective study of healthy men and women. JAMA. (1989) 262:2395–401. doi: 10.1001/jama.262.17.2395
2. Laukkanen, JA, Kurl, S, Salonen, R, Rauramaa, R, and Salonen, JT. The predictive value of cardiorespiratory fitness for cardiovascular events in men with various risk profiles: a prospective population-based cohort study. Eur Heart J. (2004) 25:1428–37. doi: 10.1016/j.ehj.2004.06.013
3. Sawada, SS, Lee, I-M, Naito, H, Kakigi, R, Goto, S, Kanazawa, M, et al. Cardiorespiratory fitness, body mass index, and cancer mortality: a cohort study of Japanese men. BMC Public Health. (2014) 14:1012. doi: 10.1186/1471-2458-14-1012
4. Sui, X, LaMonte, MJ, and Blair, SN. Cardiorespiratory fitness as a predictor of nonfatal cardiovascular events in asymptomatic women and men. Am J Epidemiol. (2007) 165:1413–23. doi: 10.1093/aje/kwm031
5. Allameh Tabataba’i University, Faculty of Sport Science, Department of Exercise Physiology, Core Research of Health Physiology and Physical Activity, Tehran, Iran, Tayebi SM, Siahkouhian M, University of Mohaghegh Ardabili, Faculty of Educational Science, Department of Exercise Science, Ardabil, Iran, Keshavarz M, Tarbiat Modares University, Faculty of Humanities, Department of Exercise Science, Tehran, Iran, Yousefi M, Avicenna Fertility Center, Department of Midwifery, Tehran, Iran. The effects of high-intensity interval training on skeletal muscle morphological changes and denervation gene expression of aged rats. Monten J Sports Sci Med. (2019) 8:39–45. doi: 10.26773/mjssm.190906
6. Niazi, S, Tayebi, SM, Costa, PB, Mirdar, S, and Hamidian, G. Effects of six weeks of high-intensity interval training on HIF-1α protein expression in lung tissues and apoptosis of pulmonary system in male Wistar rats. Ann App Sport Sci. (2023) 11:1203. doi: 10.52547/aassjournal.1203
7. Tayebi, SM, Siahkouhian, M, Keshavarz, M, Mahdian, R, Mollanouri Shamsi, M, and Shahbazi, S. The effects of high intensity interval training on Mir-23a expression and related factors involved in muscular atrophy of aged rats. International journal of applied exercise. Phys Ther. (2019) 8:170–6. doi: 10.30472/ijaep.v8i1.347
8. Zhao, GG, Cao, W, Shu, LQ, Zhang, L, Zhang, JM, and Zhu, Z. The impact of high-intensity interval training and moderate-intensity continuous training on cardiorespiratory fitness in overweight and obese adults: A Meta-analysis. J Capital University of Physical Educ Sport. (2018) 30:186–92. doi: 10.14036/j.cnki.cn11-4513.2018.02.020
9. Cao, M, Zhuang, J, Quan, MH, Xu, Q, and Wang, JY. Effects of high-intensity interval training and moderate-intensity continuous training for cardiorespiratory fitness improvements in healthy young adults. CHINA SPORT SCI TECHNOL. (2018) 54:62–8. doi: 10.16470/j.csst.201804008
10. Burgomaster, KA, Hughes, SC, Heigenhauser, GJF, Bradwell, SN, and Gibala, MJ. Six sessions of sprint interval training increases muscle oxidative potential and cycle endurance capacity in humans. J Appl Physiol. (2005) 98:1985–90. doi: 10.1152/japplphysiol.01095.2004
11. Talanian, JL, Galloway, SDR, Heigenhauser, GJF, Bonen, A, and Spriet, LL. Two weeks of high-intensity aerobic interval training increases the capacity for fat oxidation during exercise in women. J Appl Physiol. (2007) 102:1439–47. doi: 10.1152/japplphysiol.01098.2006
12. Bilski, J, Teległów, A, Zahradnik-Bilska, J, Dembiński, A, and Warzecha, Z. Effects of exercise on appetite and food intake regulation. Med Sport. (2009) 13:82–94. doi: 10.2478/v10036-009-0014-5
13. Zhou, HX. Effects of high-intensity interval training and continuous aerobic training on body composition and cardiorespiratory fitness of healthy and obese adolescents: A Meta analysis. Sport Sci Res. (2021) 42:77–93. doi: 10.12064/ssr.20210111
14. Liu, JX, Fang, W, Wang, DZ, and Ma, XD. HIIT promotes the health of children and adolescents: research status, mechanism and feasibility. China Sport Sci. (2019) 39:61–72. doi: 10.16469/j.css.201908007
15. Li, S, Cao, M, Zhou, Y, and Tang, YC. Effects of high-intensity interval training on visceral adipose tissue and cardiorespiratory fitness in children with obesity. J Phys Educ. (2023) 30:138–44. doi: 10.16237/j.cnki.cn44-1404/g8.20230324.002
16. Domaradzki, J, Koźlenia, D, and Popowczak, M. Prevalence of positive effects on body fat percentage, cardiovascular parameters, and cardiorespiratory fitness after 10-week high-intensity interval training in adolescents. Biology. (2022) 11:424. doi: 10.3390/biology11030424
17. Starkoff, B, Bonny, A, Hoffman, R, and Devor, S. Estimated aerobic capacity changes in adolescents with obesity following high intensity interval exercise. Int J Kinesiology & Sports Sci. (2014) 2:2202–946. doi: 10.7575/aiac.ijkss.v.2n.3p.1
18. Koubaa, A. Effect of intermittent and continuous training on body composition cardiorespiratory fitness and lipid profile in obese adolescents. iosrphr. (2013) 3:31–7. doi: 10.9790/3013-32103137
19. Lau, WC, Wong, DP, Ngo, J, Liang, Y, and Kim Chang-Gyun Kim, H. Effects of high-intensity intermittent running exercise in overweight children. Eur J Sport Sci. (2015) 15:182–90. doi: 10.1080/17461391.2014.933880
20. Eddolls, WTB, McNarry, MA, Stratton, G, Winn, CON, and Mackintosh, KA. High-intensity interval training interventions in children and adolescents: A systematic review. Sports Med. (2017) 47:2363–74. doi: 10.1007/s40279-017-0753-8
21. Delgado-Floody, P, Latorre-Román, P, Jerez-Mayorga, D, Caamaño-Navarrete, F, and García-Pinillos, F. Feasibility of incorporating high-intensity interval training into physical education programs to improve body composition and cardiorespiratory capacity of overweight and obese children: A systematic review. J Exerc Sci Fit. (2019) 17:35–40. doi: 10.1016/j.jesf.2018.11.003
22. Domaradzki, J, Rokita, A, Koźlenia, D, and Popowczak, M. Optimal values of body composition for the lowest risk of failure in Tabata Training’s effects in adolescents: A pilot study. Biomed Res Int. (2021) 2021:6675416. doi: 10.1155/2021/667541611
23. Dias, KA, Ingul, CB, Tjønna, AE, Keating, SE, Gomersall, SR, Follestad, T, et al. Effect of high-intensity interval training on fitness, fat mass and Cardiometabolic biomarkers in children with obesity: A randomised controlled trial. Sports Med. (2018) 48:733–46. doi: 10.1007/s40279-017-0777-0
24. Ingul, CB, Dias, KA, Tjonna, AE, Follestad, T, Hosseini, MS, Timilsina, AS, et al. Effect of high intensity interval training on cardiac function in children with obesity: A randomised controlled trial. Prog Cardiovasc Dis. (2018) 61:214–21. doi: 10.1016/j.pcad.2018.01.012
25. Kargarfard, M, Lam, ETC, Shariat, A, Asle Mohammadi, M, Afrasiabi, S, Shaw, I, et al. Effects of endurance and high intensity training on ICAM-1 and VCAM-1 levels and arterial pressure in obese and normal weight adolescents. Phys Sportsmed. (2016) 44:208–16. doi: 10.1080/00913847.2016.1200442
26. Murphy, A, Kist, C, Gier, AJ, Edwards, NM, Gao, Z, and Siegel, RM. The feasibility of high-intensity interval exercise in obese adolescents. Clin Pediatr (Phila). (2015) 54:87–90. doi: 10.1177/0009922814528038
27. Racil, G, Ounis, O, Hammouda, O, Kallel, A, Zouhal, H, Chamari, K, et al. Effects of high vs. moderate exercise intensity during interval training on lipids and adiponectin levels in obese young females. Eur J Appl Physiol. (2013) 113:2531–40. doi: 10.1007/s00421-013-2689-5
28. Racil, G, Zouhal, H, Elmontassar, W, Abderrahman, A, Sousa, M, Chamari, K, et al. Plyometric exercise combined with high-intensity interval training improves metabolic abnormalities in young obese females more so than interval training alone. Appl Physiol Nutr Metab. (2015) 41:103–9. doi: 10.1139/apnm-2015-0384
29. Bogataj, Š, Trajković, N, Cadenas-Sanchez, C, and Sember, V. Effects of school-based exercise and nutrition intervention on body composition and physical fitness in overweight adolescent girls. Nutrients. (2021) 13:238. doi: 10.3390/nu13010238
30. Cvetkovic, N, Stojanović, E, Stojiljkovic, N, Nikolić, D, Scanlan, A, and Milanović, Z. Exercise training in overweight and obese children: recreational football and high-intensity interval training provide similar benefits to physical fitness. Scand J Med Sci Sports. (2018) 28:18–32. doi: 10.1111/sms.13241
31. Farah, BQ, Ritti-Dias, RM, Balagopal, P, Hill, JO, and Prado, WL. Does exercise intensity affect blood pressure and heart rate in obese adolescents? A 6-month multidisciplinary randomized intervention study. Pediatric. Obesity. (2014) 9:111–20. doi: 10.1111/j.2047-6310.2012.00145.x
32. Boer, PH, Meeus, M, Terblanche, E, Rombaut, L, De Wandele, I, Hermans, L, et al. Does exercise intensity affect blood pressure and heart rate in obese adolescents? A 6-month multidisciplinary randomized intervention study. Clin Rehabil. (2013) 28:221–31. doi: 10.1177/0269215513498609
33. Cao, M, Tang, Y, Li, S, and Zou, Y. Effects of high-intensity interval training and moderate-intensity continuous training on Cardiometabolic risk factors in overweight and obesity children and adolescents: A Meta-analysis of randomized controlled trials. IJERPH. (2021) 18:11905. doi: 10.3390/ijerph182211905
34. Cao, M, Tang, Y, and Zou, Y. Integrating high-intensity interval training into a school setting improve body composition, cardiorespiratory fitness and physical activity in children with obesity: A randomized controlled trial. JCM. (2022) 11:5436. doi: 10.3390/jcm11185436
35. Cao, M, Tang, YC, Li, S, and Zhou, Y. Effects of high-intensity interval training on body composition, cardiorespiratory fitness and blood indicators of children with obesity: A randomized controlled trial Chin. J Sports Med. (2022) 41:109–17. doi: 10.16038/j.1000-6710.2022.02.007
36. Yuan, LL. Effects of high-intensity interval exercise on cardiorespiratory fitness and body composition and blood lipid levels in overweight or obese male adolescents. Chin J Phys Med Rehabil. (2021) 43:251–3. doi: 10.1097/01.REO.0000000000000296
37. Costigan, SA, Eather, N, Plotnikoff, RC, Taaffe, DR, and Lubans, DR. High-intensity interval training for improving health-related fitness in adolescents: a systematic review and meta-analysis. Br J Sports Med. (2015) 49:1253–61. doi: 10.1136/bjsports-2014-094490
38. Martin-Smith, R, Cox, A, Buchan, D, Baker, J, Grace, F, and Sculthorpe, N. High intensity interval training (HIIT) improves cardiorespiratory fitness (CRF) in healthy, overweight and obese adolescents: A systematic review and Meta-analysis of controlled studies. Int J Environ Res Public Health. (2020) 17:2955. doi: 10.3390/ijerph17082955
39. Zhu, L, and Liu, JX. Effectiveness of high - intensity interval training on cardiorespiratory fitness in overweight and obese adolescent meta - analysis. J Military Physical Educ Sports. (2020) 39:96–101. doi: 10.13830/j.cnki.cn44-1129/g8.2020.01.022
40. Deng, JW, and Cao, L. Reviews on high-intensity interval training for health promotion in children and adolescents. China Sport Sci Technol. (2019) 55:21–34. doi: 10.16470/j.csst.2019020
41. Helgerud, J, Høydal, K, Wang, E, Karlsen, T, Berg, P, Bjerkaas, M, et al. Aerobic high-intensity intervals improve VO2max more than moderate training. Med Sci Sports Exerc. (2007) 39:665–71. doi: 10.1249/mss.0b013e3180304570
42. Wisløff, U, Støylen, A, Loennechen, JP, Bruvold, M, Rognmo, Ø, Haram, PM, et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: a randomized study. Circulation. (2007) 115:3086–94. doi: 10.1161/CIRCULATIONAHA.106.675041
43. Tremblay, A, Simoneau, JA, and Bouchard, C. Impact of exercise intensity on body fatness and skeletal muscle metabolism. Metabolism. (1994) 43:814–8. doi: 10.1016/0026-0495(94)90259-3
44. Little, JP, Gillen, JB, Percival, ME, Safdar, A, Tarnopolsky, MA, Punthakee, Z, et al. Low-volume high-intensity interval training reduces hyperglycemia and increases muscle mitochondrial capacity in patients with type 2 diabetes. J Appl Physiol. (2011) 111:1554–60. doi: 10.1152/japplphysiol.00921.2011
45. Gibala, MJ, McGee, SL, Garnham, AP, Howlett, KF, Snow, RJ, and Hargreaves, M. Brief intense interval exercise activates AMPK and p38 MAPK signaling and increases the expression of PGC-1alpha in human skeletal muscle. J Appl Physiol (1985). (2009) 106:929–34. doi: 10.1152/japplphysiol.90880.2008
46. Little, JP, Safdar, A, Bishop, D, Tarnopolsky, MA, and Gibala, MJ. An acute bout of high-intensity interval training increases the nuclear abundance of PGC-1α and activates mitochondrial biogenesis in human skeletal muscle. Am J Physiol Regul Integr Comp Physiol. (2011) 300:R1303–10. doi: 10.1152/ajpregu.00538.2010
47. Zhu, XM. Effects of endurance training and high-intensity interval training on health-related indexs of obese children. Southwest Defense Med. (2014) 24:408–11. doi: 10.3969/j.issn.1004-0188.2014.04.023
48. Corte, A, Roschel, H, Picanço, A, Prado, D, Villares, S, Sá Pinto, A, et al. Similar health benefits of endurance and high-intensity interval training in obese children. PloS One. (2012) 7:e42747. doi: 10.1371/journal.pone.0042747
49. Wen, D, Utesch, T, Wu, J, Robertson, S, Liu, J, Hu, G, et al. Effects of different protocols of high intensity interval training for VO2max improvements in adults: A meta-analysis of randomised controlled trials. J Sci Med Sport. (2019) 22:941–7. doi: 10.1016/j.jsams.2019.01.013
50. Wang, K, Zhu, Y, Wong, SH-S, Chen, Y, Siu, PM-F, Baker, JS, et al. Effects and dose–response relationship of high-intensity interval training on cardiorespiratory fitness in overweight and obese adults: a systematic review and meta-analysis. J Sports Sci. (2021) 39:2829–46. doi: 10.1080/02640414.2021.1964800
Keywords: high-intensity interval training, obesity, children and adolescents, cardiorespiratory fitness, dose–response relationship
Citation: Deng Y and Wang X (2024) Effect of high-intensity interval training on cardiorespiratory in children and adolescents with overweight or obesity: a meta-analysis of randomized controlled trials. Front. Public Health. 12:1269508. doi: 10.3389/fpubh.2024.1269508
Edited by:
Stevo Popovic, University of Montenegro, MontenegroReviewed by:
Jarosław Domaradzki, Wroclaw University of Health and Sport Sciences, PolandIván Rentería, Universidad Autónoma de Baja California, Mexico
Seyed Morteza Tayebi, Allameh Tabataba’i University, Iran
Predrag R Bozic, Serbian Institute of Sport and Sports Medicine (SISSM), Serbia
Copyright © 2024 Deng and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xianliang Wang, d2FuZ3hpYW5saWFuZ0BzZHUuZWR1LmNu