
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 21 February 2024
Sec. Substance Use Disorders and Behavioral Addictions
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1203631
This article is part of the Research TopicSubstance Use Disorder: Above and Beyond AddictionView all 32 articles
 Folefac D. Atem1,2*
Folefac D. Atem1,2* Meagan A. Bluestein3Baojiang Chen1,3Melissa B. Harrell3,4,5
Meagan A. Bluestein3Baojiang Chen1,3Melissa B. Harrell3,4,5 Sarah E. Messiah2,4Arnold E. Kuk3
Sarah E. Messiah2,4Arnold E. Kuk3 Adriana Pérez1,3
Adriana Pérez1,3Introduction: To examine if perceptions of harmfulness and addictiveness of hookah and cigarettes impact the age of initiation of hookah and cigarettes, respectively, among US youth. Youth (12-17 years old) users and never users of hookah and cigarettes during their first wave of PATH participation were analyzed by each tobacco product (TP) independently. The effect of perceptions of (i) harmfulness and (ii) addictiveness at the first wave of PATH participation on the age of initiation of ever use of hookah was estimated using interval-censoring Cox proportional hazards models.
Methods: Users and never users of hookah at their first wave of PATH participation were balanced by multiplying the sampling weight and the 100 balance repeated replicate weights with the inverse probability weight (IPW). The IPW was based on the probability of being a user in their first wave of PATH participation. A Fay’s factor of 0.3 was included for variance estimation. Crude hazard ratios (HR) and 95% confidence intervals (CIs) are reported. A similar process was repeated for cigarettes.
Results: Compared to youth who perceived each TP as “a lot of harm”, youth who reported perceived “some harm” had younger ages of initiation of these tobacco products, HR: 2.53 (95% CI: 2.87-4.34) for hookah and HR: 2.35 (95% CI: 2.10-2.62) for cigarettes. Similarly, youth who perceived each TP as “no/little harm” had an earlier age of initiation of these TPs compared to those who perceived them as “a lot of harm”, with an HR: 2.23 (95% CI: 1.82, 2.71) for hookah and an HR: 1.85 (95% CI: 1.72, 1.98) for cigarettes. Compared to youth who reported each TP as “somewhat/very likely” as their perception of addictiveness, youth who reported “neither likely nor unlikely” and “very/somewhat unlikely” as their perception of addictiveness of hookah had an older age of initiation, with an HR: 0.75 (95% CI: 0.67-0.83) and an HR: 0.55 (95% CI: 0.47, 0.63) respectively.
Discussion: Perceptions of the harmfulness and addictiveness of these tobacco products (TPs) should be addressed in education campaigns for youth to prevent early ages of initiation of cigarettes and hookah.
Many studies have been conducted to assess the prevalence of tobacco product (TP) use in youth, and several studies have suggested risk factors for initiation including previous substance use, lack of awareness, and socioeconomic status (1, 2). Moreover, initiation of TP use is associated with decreased perceptions of harmfulness (3); however, other studies have shown that most youth who initiated cigarette use were aware of the risks associated with these TPs (4). Nonetheless, most of the studies on the impact of harmfulness and addictiveness have focused on the initiation of TP use with binary outcomes (yes/no) (3, 5, 6). Rather than analyzing the initiation as a yes/no answer, monitoring participants over time until some of them experience the event of interest improves precision and decreases bias (7). In a 2022 longitudinal study using Population Assessment of Tobacco and Health (PATH) data, the impact of the perceptions of hookah harmfulness and addictiveness on the age of initiation was examined among never users during their initial participation in the PATH study (8). However, analyses excluded the youth who reported hookah use during their first wave of PATH participation. This type of study design that involves only never users at the outset of the study and follows them prospectively until the occurrence of the event of interest is referred to as an incident cohort design (9). According to Cain et al. (9), excluding these participants may result in biased estimates. In this study, we aimed to incorporate both participants who had already initiated each TP use at their first wave of PATH participation and never users of each TP at that same wave. This approach allowed us to separately investigate their perceptions of hookah and cigarettes regarding their harmfulness and addictiveness at the age of initiation (9). Employing a survival analysis study design, participants were followed until they initiated the TP use (8, 10). To comprehend the impact of the perceptions of harmfulness and addictiveness on the age of initiation for hookah and cigarette use among the youth population, we carefully balanced the effects of users and never users at their first wave of PATH participation through the inverse probability weighting (IPW) method (11, 12). The strength of this approach is that it does not exclude users from the analysis and balances between covariates such as sex and race/ethnicity between users and never users (13, 14).
We performed secondary data analysis using the PATH data, which is a longitudinal study of tobacco use in the US (15). This study began during 2013–2014 with annual samples collected until 2017; when samples were collected every 2 years a complex stratified area probability sampling method was employed to generate a nationally representative sample of youth and adults in the US (15, 16). We included youth (aged 12–17 years) data from waves 1–4 (wave 1: 2013–2014, wave 2: 2014–2015, wave 3: 2015–2016, and wave 4: 2016–2017). Shadow youth participants, that is, youth aged 9–11 years at wave 1, entered the study once they turned 12 at wave 2 and wave 3, respectively. All youth who turned 18 years in the subsequent waves were invited to participate in the adult study, and their follow-up data as adults were included in the analyses (15, 16). The institutional review board approval for this study was obtained from the Committee for the Protection of Human Subjects at the University of Texas Health Science Center at Houston (protocol number HSC-SPH-17-0368).
In the first wave of participation (waves 1–4), participants were asked the following question: “Have you ever smoked tobacco in a hookah, even one or two puffs?,” and the response options were “yes,” “no,” and “I do not know” (15). In waves 1–4, using PATH, youth respondents were asked the following question: “Have you ever smoked a cigarette, even one or two puffs?,” and the response options were “yes,” “no,” and “I do not know (15, 16). These analyses were limited to participants that responded “yes” or “no.”
The restricted-use PATH data do not provide the date of birth information for youth participants; however, it does provide the participants’ age in years at each wave and the number of weeks between the waves. For each participant, we created a lower and an upper age bound for each TP outcome. At the first wave of PATH participation, youths were asked the following question: “Have you ever smoked tobacco in a hookah, even one or two puffs?,” and the response options were “yes” and “no.” Those who answered “yes” were asked another question: “Age when first tried smoking a hookah, even one or two puffs?” This recalled age of initiation as indicated by the youth is what we labeled “recalled age.” Similar questions were asked about cigarettes, separately.
The lower age bound for the youth who indicated the use of TPs at their first wave of PATH participation was their recalled age of initiation, while the upper age bound was the age at the first wave of PATH participation (17).
For never users of each TP at their first wave of PATH participation, the lower age bound was the participants’ age at the first wave of PATH participation plus the number of weeks between the first wave and the last wave the participant reported non-use of each TP. For those who initiated the TP after the first wave of PATH participation, the upper age bound was the age at the lower bound plus the number of weeks between the lower bound and the first wave the participant reported the initiation of each TP (18). Never users during the study period were considered right-censored, that is, their upper bound age of initiation was unbounded (19).
PATH assessed perceptions of harmfulness and addictiveness of hookah and cigarettes individually for youth in their first wave of PATH participation (waves 1–3). The perceptions of harmfulness of cigarettes and hookah in waves 1–3 were only assessed among the youth participants who had heard of each TP at each wave. Since all users of a TP at their first wave of PATH participation must have heard of the TP, never users, those who had not heard of each TP, were excluded. The following question was used to measure the perceptions of harmfulness: “How much do you think people harm themselves when they smoke/use [TP]?” (16). The response options included (i) “no harm”; (ii) “little harm”; (iii) “some harm”; (iv) “a lot of harm”; (v) “do not know”; and (vi) “refused.” These responses were recoded as “no/little harm,” “some harm,” and “a lot of harm.” The participants who answered “do not know” and “refused” were not included in the analysis.
Similarly, the perceptions of addictiveness of each TP were assessed at the first wave of PATH participation, using the questions, “How likely is someone to become addicted to shisha or hookah tobacco?” or “How likely is someone to become addicted to cigarettes?” (16). The response options included (i) “very unlikely”; (ii) “somewhat unlikely”; (iii) “neither likely nor unlikely”; (iv) “somewhat likely”; (v) “very likely”; (vi) “do not know”; and (vii) “refused.” We excluded those who responded with “do not know” and “refused” from our analyses. The variables were recoded as follows: “very/somewhat unlikely,” “neither likely nor unlikely,” and “somewhat/very likely.” Similarly, the youth who had not heard of each TP were excluded from the analyses.
Sex was classified as female or male, and this variable was imputed by PATH using the household information at wave 1 (16). Race was assessed as white, Black, Asian, and other (including multi-racial). Ethnicity was categorized as either Hispanic or non-Hispanic. In our analyses, compared to the previous publications, we categorized race/ethnicity into four categories, with non-Hispanic white as the reference: non-Hispanic white, Hispanic, non-Hispanic Black, and non-Hispanic other (Asian, multi-race, and other races) (19, 20, 21).
A two-phase secondary analysis for understanding the perceptions of harmfulness and addictiveness at the age of initiation of hookah or cigarette use was conducted among the youth who participated in PATH (aged 12–17 years) at their first wave of PATH participation (waves 1–3) (16). In the first phase, we employed the IPW method, considering the probability of being a user, to balance the confounding effects related to sex and race/ethnicity between users and never users of each TP at their first wave of PATH participation (12). The primary goal of IPW is to create a pseudo-population where the distribution of sex and race/ethnicity is balanced across TP users and never users at their first wave of PATH participation, similar to what might be observed in a randomized controlled trial. This weighting technique helps in mitigating the biases that could arise due to sex and race/ethnicity or uneven distribution of characteristics among TP users and never users at their first wave of PATH participation, thereby allowing for more accurate estimations of treatment effects or associations between variables.
The IPW technique uses propensity score to balance the characteristics of users and never users of each TP (hookah and cigarettes) by weighing each individual in the analysis (22).
Specifically, we developed a weight known as IPW by fitting a logistic regression with the binary indicator variable (yes/no) for users versus never users at the first wave of PATH participation for each TP with sex and race/ethnicity as the covariates (12, 23).
Thus, the propensity score, defined as p(K) = Pr(Z = 1 | K), is the conditional probability of being a user of hookah (yes/no) at the first wave of PATH participation, that is, Z = 1 for users of hookah at their first wave of PATH participation and Z = 0 for never users of hookah at their first wave of PATH participation. K refers to the measured covariates, that is, sex and race/ethnicity. The p(K) is estimated using a logistic regression for the probability of being a user of hookah at the first wave of PATH participation with sex and race/ethnicity as covariates, and its estimate (output) represented the predictive value from this model. Then, weights are assigned for users and never users of each TP by exemplifying the case for hookah. Hookah users at their first wave of PATH participation were assigned a weight: w(K) = 1/p(K), whereas never users of hookah were assigned a weight: w(K) = 1/1-p(K) (11, 12, 23). Weight assignment was repeated for cigarette users and non-users at the first wave of PATH participation. Next, we created a new set of composite weights by (1) multiplying the IPW with the PATH sampling weight and (2) multiplying the IPW with the 100 balance replicate weights (24, 25). This new set of composite weights is expected to minimize the bias due to the lack of randomization in being a user or never user at the first wave of PATH participation (24). Differences in perceptions of harmfulness and addictiveness were explored by fitting composite weighted Cox proportional hazards regression models to interval-censored data with a constant baseline hazard function, which represents the instantaneous rate of initiation of a TP within the interval. Hazard ratios (HR), serving as indicators for the likelihood of TP initiation between groups, were estimated, and their respective 95% confidence intervals (CI) were reported (26, 27). The hazard function and non-parametric estimators for each significant level by perceptions of harmfulness and addictiveness, separately from the Cox proportional hazards regression models, were estimated (28–30). A type I error level of 0.05 was used. For each TP, Statistical Analysis System (SAS version 9.4) macros were developed.
Weighted summary statistics for demographic characteristics for PATH youth (aged 12–17 years at their first wave of PATH participation) are shown in Table 1. The sample size for the users and never users (waves 1–3) for each of the TPs was as follows: 16,564 youth (representing 30,85,8,246 US youth) for hookah, and 17,689 youth (representing 32,982,770 US youth) for cigarettes. Among these youth, 5.9% ever used hookah and 10.7% ever used cigarettes by their first wave of PATH participation. The average age of participants in their first wave of PATH participation was 13.9 years for these TPs. The distribution of sex was almost evenly distributed, with girls accounting for approximately 49.1% of the hookah sample and 48.8% of the cigarette sample. The racial/ethnic distribution among various TP usage was notably consistent, with approximately 54% being non-Hispanic white, 23% Hispanic, 13% non-Hispanic Black, and 10% falling into the non-Hispanic other category. The majority of youth perceived both hookah and cigarettes as harmful, with 52.3% reporting “a lot of harm” for hookah and 83.3% for cigarettes. Additionally, a considerable percentage of youth perceived hookah (75.3%) and cigarettes (81.5%) to be “somewhat/ very likely” in terms of addictiveness.
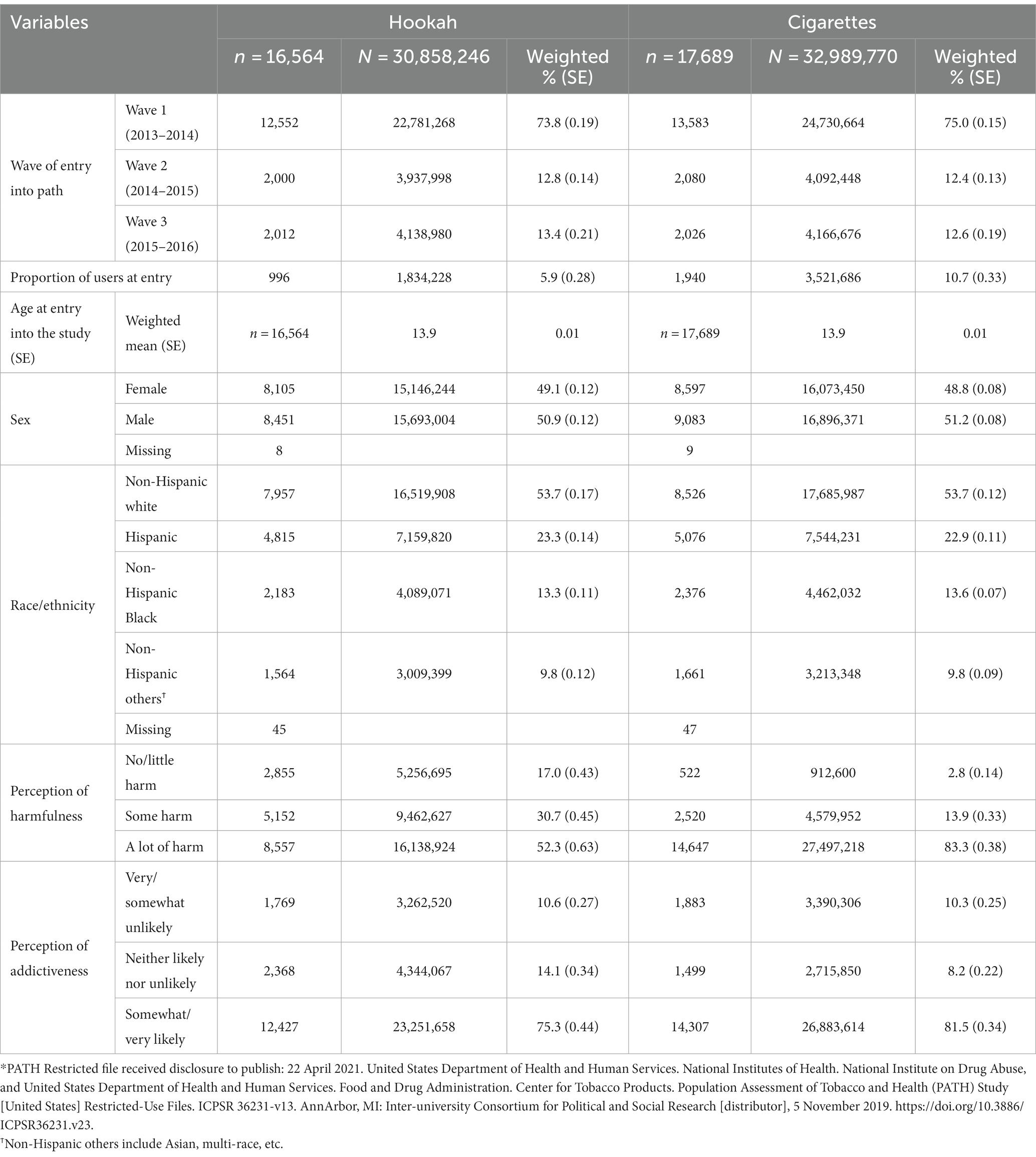
Table 1. Demographic characteristics of users and never users of each TP in PATH USA youth (aged 12–17 years).
In Table 2, we present the adjusted hazard ratios and their 95% CIs exploring the impact of the perceptions of harmfulness and addictiveness on the age of initiation of each TP using the composite weight and the 100 composite BRR weights. Adjusted hazard ratios are balanced by sex and race/ethnicity. The findings revealed distinct patterns regarding perceptions of harm and addictiveness influencing the initiation of hookah and cigarette use among youth. Youth perceiving hookah as having “no/little harm” showed a strikingly higher likelihood (123%, HR, 2.23, 95% CIs, 1.82–2.73) of being more prone to initiate hookah use earlier compared to those perceiving it as having “a lot of harm.” Similarly, those perceiving hookah as having “some harm” were 253% (HR: 3.53, 95% CI: 2.87–4.34) more likely to initiate use at younger ages than those perceiving “a lot of harm.”
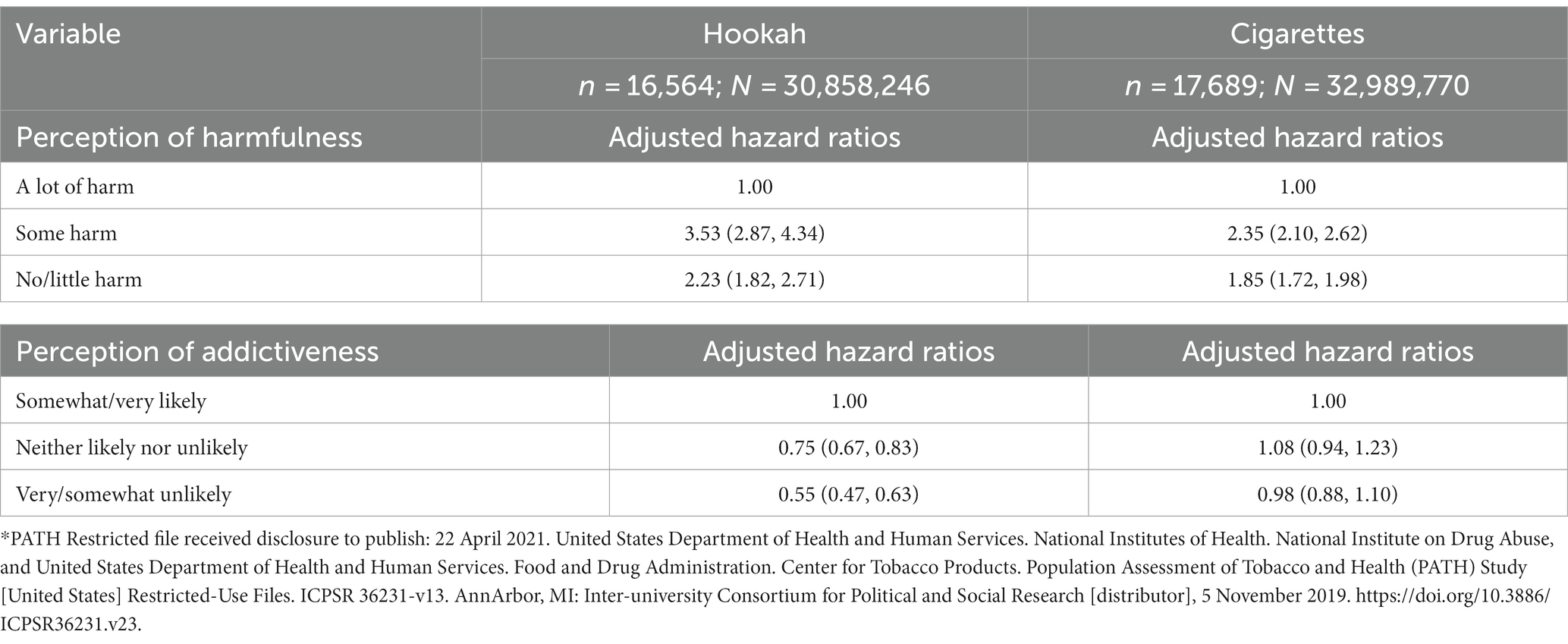
Table 2. Hazard ratios (and 95% confidence intervals) for the association between perceptions of harmfulness and addictiveness and the age of initiation of hookah and cigarette use.
Regarding the addictiveness perceptions, the youth who reported feeling “very/somewhat unlikely” were 45% (HR: 0.55, 95% CI: 0.47–0.63) less likely to initiate hookah use early compared to those feeling “somewhat/very likely.” Meanwhile, those with “neither likely nor unlikely” perceptions were 25% (HR: 0.75, 95% CI: 0.67–0.83) less inclined to initiate hookah use at a younger age compared to those perceiving addictiveness as “somewhat/very likely.” Concerning cigarettes, youth perceiving “no/little harm” and “some harm” were notably 85% higher for early age of initiation (HR: 1.85, 95% CI: 1.72-1.98) and 135% (HR: 2.35, 95% CI: 2.10-2.62) respectively, as compared to those perceiving cigarettes as having “a lot of harm”.
Table 3 shows the hazard function and its 95% CI of ever use of each of these TPs stratified by three categorized classes of the perceptions of harmfulness. For all three TPs, initiation increases as the perceptions of harmfulness decrease from “a lot of harm” to “no/little harm.” By the age of 17 years, the proportion of youth who perceived “a lot of harm” from hookah and initiated it was 3.4% (95% CI, 2.8–4.1), those who perceived “some harm” and initiated it was 10.8% (95% CI, 9.1–11.8), and those who perceived “no/little harm” and initiated it was 27.7% (95% CI, 25.0–30.3). Moreover, by the age of 17 years, the proportion of youth who perceived “a lot of harm” in cigarettes and initiated them was 22.9% (95% CI, 20.2–25.6), those who perceived “some harm” and initiated them was 40.0% (95% CI, 33.3–45.7), and those who perceived “no/little harm” and initiated them was 42.1% (95% CI, 36.1–48.1).
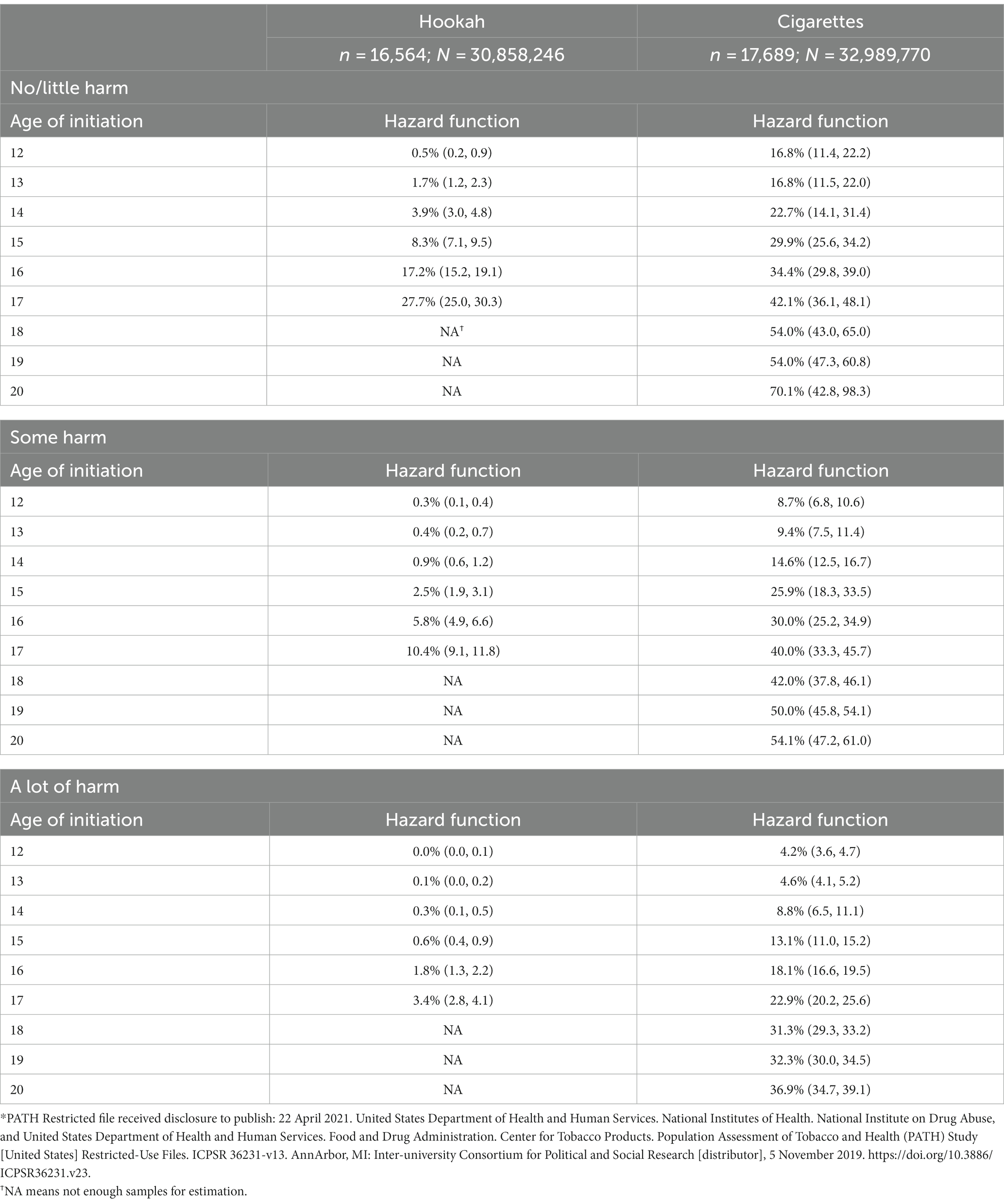
Table 3. Estimated hazard function (95% confidence interval) of the age of initiation of ever TP use outcomes by perceptions of harmfulness of PATH USA youth.
Table 4 shows the hazard functions and its 95% CIs of ever use of each of these TPs stratified by three categorized classes of the perceptions of addictiveness. The results limited to the strata that are significantly different from the reference class “somewhat/very likely” perception of addictiveness were presented. Our results showed that, by the same age, the proportion of initiation of hookah increases as the perception of addictiveness decreases from “somewhat/very likely” to “very/somewhat unlikely.” For example, by the age of 17 years, 5.2% (95% CI: 4.4–6.0) of youth were estimated to initiate hookah among those who reported “somewhat/very likely” perceptions of addictiveness for hookah, 16.2% (95% CI: 14.0–18.4) of youth were estimated to initiate hookah among those who reported “neither likely nor unlikely” perceptions of addictiveness, and 38.8% (95% CI: 30.5–37.1) of youth were estimated to initiate hookah among those who reported “very/somewhat unlikely” perceptions of addictiveness.
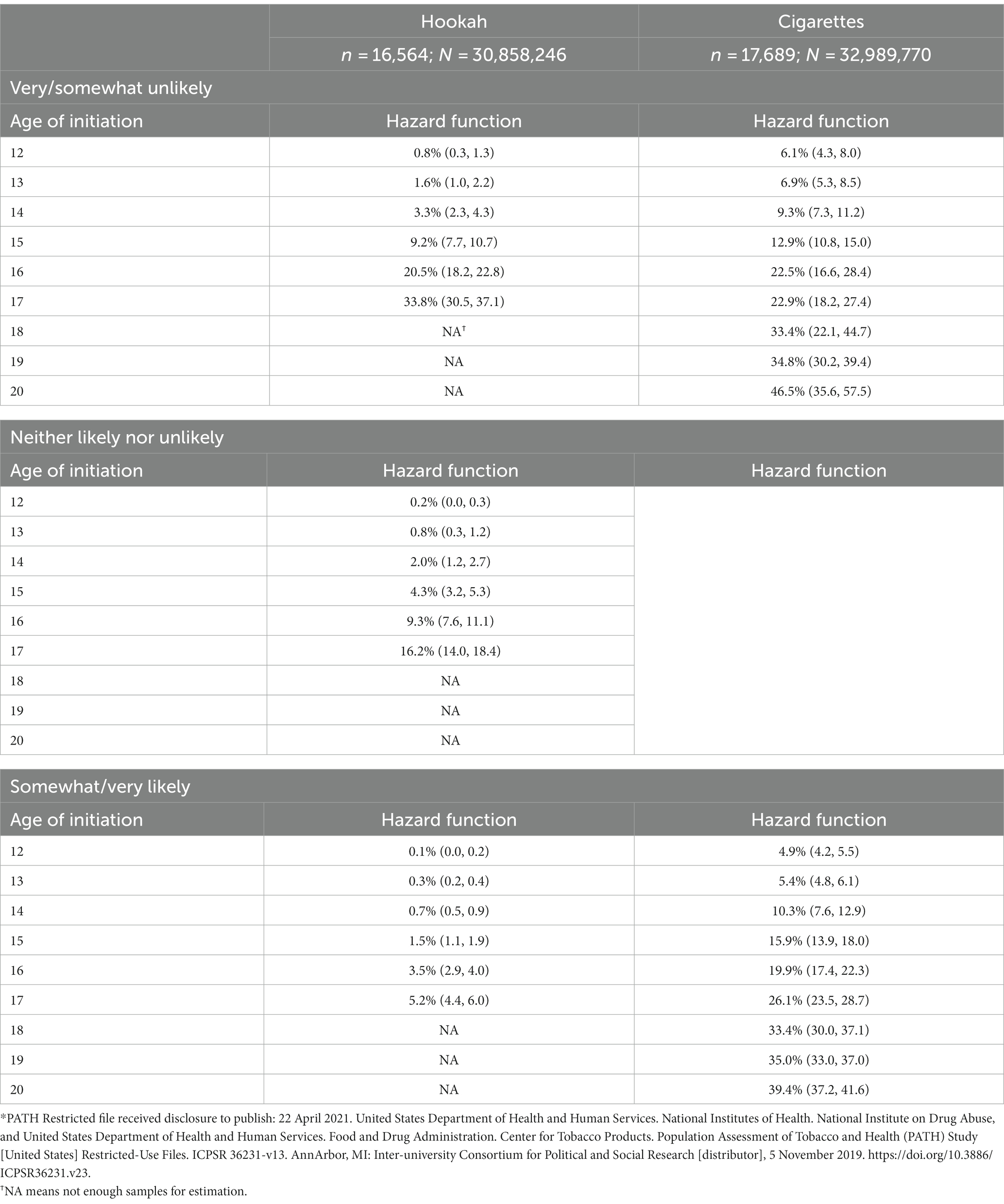
Table 4. Estimated hazard function (95% confidence interval) of the age of initiation of ever TP use outcomes by perceptions of addictiveness of PATH USA youth.
In this study, we examined the association between the youth perceptions of harmfulness and addictiveness and the age of initiation of ever use of hookah and cigarettes. These two TPs reported more than 5% ever use at the first wave of PATH participation. Each TP product was examined independently to understand how youth’s perceptions of harmfulness and addictiveness influence the age of initiation of each of these TPs. This study differs significantly from the two previous studies (8, 10) in two ways. First, the dataset analyzed by Chen et al. (10) and Kuk et al. (8) was limited to non-users of TPs at their first wave of PATH participation, while we included both users and non-users of each TP at the first wave of PATH participation, separately, in this study. Second, in the previous two studies, the analyses took advantage of the PATH sampling weights and the 100 balance replicate weights; however, in this study, we created composite weights by multiplying the IPW with the PATH sampling weight and multiplying the IPW with the 100 balance replicate weights. In our inverse probability approach, we aimed to achieve equilibrium in sex and race/ethnicity distributions. This balancing act mirrors block randomization based on sex and race/ethnicity. The goal is to ensure that any observed disparities between groups are not attributed to differences in sex or race/ethnicity but instead reflect the impact of other factors under examination.
The findings from the previous studies indicated that, when youth perceived these tobacco products as less harmful, they tended to initiate their use at earlier ages. Our results support this trend with a nuanced twist: the likelihood of initiating ever use of cigarette and hookah at younger ages follows the order of “some harm” > “no/little harm” > “a lot of harm.”
Moreover, a previous study revealed that a lower perceived risk was linked to the likelihood of ever using hookah (31). Our study, in conjunction with this research, highlights the potential impact of educating youth about the potential harmfulness and addictiveness of hookah, which could significantly decrease its consumption. Overall, the analysis results suggest that educating these young individuals about the potential risks associated with these tobacco products might prove beneficial in altering their perceptions of them.
This nationally representative US sample, combined with a causal analytical approach that balanced users and non-users during their initial participation in the PATH study, offered valuable insights into how perceptions of harmfulness and addictiveness influence the age of hookah and cigarette initiation. Moreover, our longitudinal study design strengthens the validity of findings, illustrating a robust and consistent relationship between risk perceptions and the age at which individuals initiate hookah and cigarette use.
A potential limitation in the design of this study is that the perceptions of harmfulness and addictiveness were recorded at the first wave of PATH participation, where users of each TP were recorded after the initiation, while never users of each TP were recorded before the initiation. Despite these measurement issues, we do not think this will have a tremendous effect on our results since we assumed the exposure does not change over time in the model (32, 33). Another potential drawback is with the recalled age of initiation for users at their first wave of PATH participation because these users might not precisely know when they initiated the TP. However, in one of our previous publications, we performed a sensitivity analysis where we replaced the recalled age of initiation with a uniform six “6” as the lower age bound under the assumption that the participants were at least 6 years old when they initiated each of these products. The results showed insignificant differences using the recalled age and the uniform six “6” as the lower age bound for these TPs (17), indicating that recall bias was minimal.
Our findings highlight the importance of the perceptions of harmfulness and addictiveness in the age of initiation of hookah and cigarettes. The perceptions of harmfulness and addictiveness of these TPs should be addressed in education campaigns for youth to prevent earlier ages of initiation of these products.
The datasets presented in this article are not readily available because we used the restricted data from Population Assessment of Tobacco and Health (PATH) study, 2013–2017. Any researcher could assess the data after completing the necessary paperwork. Requests to access the datasets should be directed to bmFoZGFwLXZkZS1zdXBwb3J0QHVtaWNoLmVkdQ==.
FA, MH, SM and AP wrote the protocol. BC, MB, AK, and AP conducted literature search and data compilation. FA analyzed the data and wrote the first draft of the manuscript. MH, SM, and AP supervised and redrafted the manuscript. FA and AP assembled the final draft and circulated it to all the authors who read and agreed on the final submitted draft.
A grant supported the research reported in this publication to AP from the National Cancer Institute (NCI) and the FDA Center for Tobacco Products (CTP) under the grant number R01CA234205 and a diversity supplement to FA by the National Cancer Institute of the National Institutes of Health under Award Number R01CA234205-S1 supported this research.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ambrose, BK, Rostron, BL, Johnson, SE, Portnoy, DB, Apelberg, BJ, Kaufman, AR, et al. Perceptions of the relative harm of cigarettes and e-cigarettes among US youth. Am J Prev Med. (2014) 47:S53–60. doi: 10.1016/j.amepre.2014.04.016
2. Palamar, JJ, Zhou, S, Sherman, S, and Weitzman, M. Hookah use among US high school seniors. Pediatrics. (2014) 134:227–34. doi: 10.1542/peds.2014-0538
3. Chaffee, BW, and Cheng, J. Tobacco product initiation is correlated with cross-product changes in tobacco harm perception and susceptibility: longitudinal analysis of the population assessment of tobacco and Health youth cohort. Prev Med. (2018) 114:72–8. doi: 10.1016/j.ypmed.2018.06.008
4. Mattingly, DT, Tompkins, LK, Rai, J, Sears, CG, Walker, KL, and Hart, JL. Tobacco use and harm perceptions among Appalachian youth. Prev Med Rep. (2020) 18:101089. doi: 10.1016/j.pmedr.2020.101089
5. Bernat, D, Gasquet, N, Wilson, KOD, Porter, L, and Choi, K. Electronic cigarette harm and benefit perceptions and use among youth. Am J Prev Med. (2018) 55:361–7. doi: 10.1016/j.amepre.2018.04.043
6. Ganz, O, Johnson, AL, Cohn, AM, Rath, J, Horn, K, Vallone, D, et al. Tobacco harm perceptions and use among sexual and gender minorities: findings from a national sample of young adults in the United States. Addict Behav. (2018) 81:104–8. doi: 10.1016/j.addbeh.2018.01.032
7. Cook, NR, and Ware, JH. Design and analysis methods for longitudinal research. Annu Rev Public Health. (1983) 4:1–23. doi: 10.1146/annurev.pu.04.050183.000245
8. Kuk, AE, Bluestein, MA, Chen, B, Harrell, M, Spells, CE, Atem, F, et al. The effect of perceptions of hookah harmfulness and addictiveness on the age of initiation of hookah use among population assessment of tobacco and health (PATH) youth. Int J Environ Res Public Health. (2022) 19:5034. doi: 10.3390/ijerph19095034
9. Cain, KC, Harlow, SD, Little, RJ, Nan, B, Yosef, M, Taffe, JR, et al. Bias due to left truncation and left censoring in longitudinal studies of developmental and disease processes. Am J Epidemiol. (2011) 173:1078–84. doi: 10.1093/aje/kwq481
10. Chen, B, Spells, CE, Bluestein, MA, Kuk, AE, Harrell, MB, and Pérez, A. The association of perceptions of harmfulness and addictiveness on the age of initiation of cigar product use among youth: findings from the population assessment of tobacco and Health (PATH) study, 2013–2017. Front Public Health. (2022) 10. doi: 10.3389/fpubh.2022.882434
11. Austin, PC, and Stuart, EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat Med. (2015) 34:3661–79. doi: 10.1002/sim.6607
12. Rotnitzky, A. Inverse probability weighted methods In:. Longitudinal data analysis : Chapman and Hall/CRC (2008). 467–90.
13. Austin, PC. Assessing covariate balance when using the generalized propensity score with quantitative or continuous exposures. Stat Methods Med Res. (2019) 28:1365–77. doi: 10.1177/0962280218756159
14. Imai, K, and Ratkovic, M. Covariate balancing propensity score. J Royal Stat Soc. (2014) 76:243–63. doi: 10.1111/rssb.12027
15. Hyland, A, Ambrose, BK, Conway, KP, Borek, N, Lambert, E, Carusi, C, et al. Design and methods of the population assessment of tobacco and Health (PATH) study. Tob Control. (2017) 26:371–8. doi: 10.1136/tobaccocontrol-2016-052934
16. United States Department of Health and Human Services, National Institute of Health, National Institute 458 on Drug Abuse, Food and Drug Administration, Center for Tobacco Products. (2021). Population 459 Assessment of Tobacco and Health (PATH) Study [United States] Restricted-Use Files, User 460 Guide: Inter-university Consortium for Political and Social Research, 461 doi: 10.3886/ICPSR36231.v37
17. Atem, FD, Bluestein, MA, Harrell, MB, Chen, B, Messiah, SE, Kuk, AE, et al. Precise Estimation for the Age of Initiation of Tobacco Use Among U.S. Youth: Finding from the Population Assessment of Tobacco and Health (PATH) Study, 2013–2017. Biostat Biomet Open Access J. (2022) 11. doi: 10.19080/bboaj.2022.11.555801
18. Pérez, A, Bluestein, M, Chen, B, Perry, CL, and Harrell, MB. Prospectively estimating the age of initiation of e-cigarettes among US youth: findings from the population assessment of tobacco and Health (PATH) study, 2013-2017. J Biomet Biostat. (2020) 11
19. Pérez, A, Kuk, AE, Bluestein, MA, Harrell, MB, Perry, CL, and Chen, B. Prospective estimation of the age of initiation of hookah use among youth: findings from the population assessment of tobacco and Health (PATH) study waves 1-4 (2013-2017). Addict Behav. (2021) 117:106838. doi: 10.1016/j.addbeh.2021.106838
20. Chen, B, Sterling, KL, Bluestein, MA, Kuk, AE, Harrell, MB, Perry, CL, et al. Age of initiation of cigarillos, filtered cigars and/or traditional cigars among youth: findings from the population assessment of tobacco and Health (PATH) study, 2013–2017. PLoS One. (2020) 15:e0243372. doi: 10.1371/journal.pone.0243372
21. Kasza, KA, Edwards, KC, Tang, Z, Stanton, CA, Sharma, E, Halenar, MJ, et al. Correlates of tobacco product initiation among youth and adults in the USA: findings from the PATH study waves 1–3 (2013–2016). Tob Control. (2020) 29:s191–202. doi: 10.1136/tobaccocontrol-2020-055671
22. Curtis, LH, Hammill, BG, Eisenstein, EL, Kramer, JM, and Anstrom, KJ. Using inverse probability-weighted estimators in comparative effectiveness analyses with observational databases. Med Care. (2007) 45:S103–7. doi: 10.1097/MLR.0b013e31806518ac
23. Matsouaka, RA, and Atem, FD. Regression with a right-censored predictor using inverse probability weighting methods. Stat Med. (2020) 39:4001–15. doi: 10.1002/sim.8704
24. DuGoff, EH, Schuler, M, and Stuart, EA. Generalizing observational study results: applying propensity score methods to complex surveys. Health Serv Res. (2014) 49:284–303. doi: 10.1111/1475-6773.12090
25. Leas, EC, Benmarhnia, T, Strong, DR, and Pierce, JP. Effects of menthol use and transitions in use on short-term and long-term cessation from cigarettes among US smokers. Tob Control. (2021) doi: 10.1136/tobaccocontrol-2021-056596
26. Goodall, RL, Dunn, DT, and Babiker, AG. Interval-censored survival time data: confidence intervals for the non-parametric survivor function. Stat Med. (2004) 23:1131–45. doi: 10.1002/sim.1682
27. Ng, MP. A modification of Peto's nonparametric estimation of survival curves for interval-censored data. Biometrics. (2002) 58:439–42. doi: 10.1111/j.0006-341X.2002.00439.x
28. Turnbull, BW. The empirical distribution function with arbitrarily grouped, censored and truncated data. J Royal Stat Soc. (1976) 38:290–5.
29. Fay, R. E. (1989). Theory and application of replicate weighting for variance calculations. In: Paper presented at the Proceedings of the Survey Research Methods Section of the American Statistical Association, 212–7.
31. Cooper, M, Pacek, LR, Guy, MC, Barrington-Trimis, JL, Simon, P, Stanton, C, et al. Hookah use among US youth: a systematic review of the literature from 2009 to 2017. Nicotine Tob Res. (2019) 21:1590–9. doi: 10.1093/ntr/nty135
32. Finkelstein, DM, Goggins, WB, and Schoenfeld, DA. Analysis of failure time data with dependent interval censoring. Biometrics. (2002) 58:298–304. doi: 10.1111/j.0006-341X.2002.00298.x
Keywords: tobacco, addictiveness, harmfulness, truncation, interval censoring, weighted survival analysis
Citation: Atem FD, Bluestein MA, Chen B, Harrell MB, Messiah SE, Kuk AE and Pérez A (2024) Application of inverse weighting analysis to assess the association of youth perceptions with the age of initiation of tobacco products. Front. Public Health. 12:1203631. doi: 10.3389/fpubh.2024.1203631
Edited by:
Muthuraju Sangu, University of Houston, United StatesReviewed by:
Yasmine Sherafat, California State University, San Marcos, United StatesCopyright © 2024 Atem, Bluestein, Chen, Harrell, Messiah, Kuk and Pérez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Folefac D. Atem, Rm9sZWZhYy5ELkF0ZW1AdXRoLnRtYy5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.