 Feras Kasabji1
Feras Kasabji1 Ferenc Vincze1
Ferenc Vincze1 Kinga Lakatos1
Kinga Lakatos1 Anita Pálinkás2
Anita Pálinkás2 László Kőrösi3
László Kőrösi3 László Ulicska4
László Ulicska4 Karolina Kósa5
Karolina Kósa5 Róza Ádány1,2
Róza Ádány1,2 János Sándor1,2*
János Sándor1,2*- 1Department of Public Health and Epidemiology, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
- 2ELKH-DE Public Health Research Group, Department of Public Health and Epidemiology, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
- 3National Health Insurance Fund, Budapest, Hungary
- 4Deputy State Secretariat for Social Inclusion, Ministry of Interior, Budapest, Hungary
- 5Department of Behavioral Sciences, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
Introduction: Spatially segregated, socio-economically deprived communities in Europe are at risk of being neglected in terms of health care. In Hungary, poor monitoring systems and poor knowledge on the health status of people in these segregated areas prevent the development of well-informed effective interventions for these vulnerable communities.
Aims: We used data available from National Health Insurance Fund Management to better describe health care performance in segregated communities and to develop more robust monitoring systems.
Methods: A cross-sectional study using 2020 health care data was conducted on each general medical practice (GMP) in Hungary providing care to both segregated and nonsegregated (complementary) adult patients. Segregated areas were mapped and ascertained by a governmental decree that defines them as within settlement clusters of adults with low level of education and income. Age, sex, and eligibility for exemption certificate standardized indicators for health care delivery, reimbursement, and premature mortality were computed for segregated and nonsegregated groups of adults and aggregated at the country level. The ratio of segregation and nonsegregation specific indicators (relative risk, RR) was computed with the corresponding 95% confidence intervals (95% CI).
Results: Broad variations between GMPs were detected for each indicator. Segregated groups had a significantly higher rate of health care service use than complementary groups (RR = 1.22, 95% CI: 1.219;1.223) while suffering from significantly reduced health care reimbursement (RR = 0.940, 95% CI: 0.929;0.951). The risk of premature mortality was significantly higher among segregated patients (RR = 1.184, 95% CI: 1.087;1.289). Altogether, living in a segregated area led to an increase in visits to health care services by 18.1% with 6.6% less health spending.
Conclusion: Adults living in segregated areas use health care services more frequently than those living in nonsegregated areas; however, the amount of health care reimbursement they receive is significantly lower, suggesting lower quality of care. The health status of segregated adults is remarkably lower, as evidenced by their higher premature mortality rate. These findings demonstrate the need for intervention in this vulnerable group. Because our study reveals serious variation across GMPs, segregation-specific monitoring is necessary to support programs sensitive to local issues and establish necessary benchmarks.
1 Introduction
Segregation, whether residential, racial, or otherwise, is a recognized risk factor for ill health and inequity. Various studies have explored segregation and its impact on health (1–7) and found pronounced inequality in health care outcomes between segregated and nonsegregated areas, including but not limited to overall infant and adult mortality, high-risk pregnancies, and exposure to communicable diseases (7, 8). Reasons for these disparities range from environmental factors, such as sanitation facilities and pollution, to lifestyle factors, such as poor housing situations, crowding, and habits such as poor diets, smoking, and low physical activity (9, 10).
The relationship between segregation and health is well documented. However, the specific association of segregation with health care delivery and reimbursement policies is still understudied. A prominent example of this is the Roma people in Europe, who constitute the largest ethnic minority in Europe (11, 12) and in Hungary (13), where they make up 94% of inhabitants in segregated areas (14). Data regarding their health are limited. However, it is estimated that Roma have a 10-year shorter life expectancy (15) and are at higher risk of coronary and chronic diseases (16, 17). It makes them among the most relevant health equity concerns in Europe and prompts many studies to investigate segregated Roma access to and use/misuse of health care services (18–22). However, these studies have fallen short of explaining the determinants of the observed health losses. This shortfall has contributed to the failure of governments to implement effective equity-targeted policies, as evidenced by the current dissimilarity in health between Roma and non-Roma populations (23).
A major constraint of any Roma-focused study is the inability to accurately identify Roma ethnicities in local demographics or estimate their health statistics, mainly due to ethical issues and the unavailability of a clear-cut method to do so (24–26). These limitations generate unguided financial policies and governance, leading to considerable inequality in health delivery and outcomes both geographically and among population groups (27, 28). This situation gives rise to the need for more robust monitoring and intervention programs, both of which require a clearer picture of the variability in health care delivery and reimbursement.
Moreover, even though Roma are overrepresented in segregated communities in Hungary, the non-Roma population of the segregates lives in equal socioeconomic deprivation, and interventions should therefore be sensitive to this situation and the local environment and aim to help the vulnerable population regardless of ethnic background.
As a result, current inclusion policies shift the focus from Roma people to segregated communities regardless of ethnicity, to avoid any ethical concerns surrounding the identification of different ethnic groups as well as monitoring their health status, in accordance with the Hungarian national social inclusion strategies (29).
In Hungary, the National Institute of Health Insurance Fund Management (NIHIFM) is the organization operating the country’s official health monitoring system. Every month, NIHIFM evaluates all general medical practices (GMPs) by a limited set of performance indicators (30, 31), which then affect GMP financing through a pay-for-performance system. More data on primary health care operations are collected but not utilized by the NIHIFM, leaving an untapped reservoir of data that could be useful for research.
Using the protected data within the NIHIFM system, aggregated indicators can be produced for segregated areas where most inhabitants are Roma and other vulnerable groups that are cared for by identifiable institutions, achieved by linking the geographical location of segregation with the health-insured population living there. These aggregated statistics can then be used to investigate the most vulnerable subgroup of Roma by evaluating geographical inequality (32, 33), thus bypassing legal and ethical limitations. The governmental decree’s definition of segregation utilizes census data, focusing on income and education measures rather than Roma ethnicity, which enables the study of segregation related issues and leads to conclusions indirectly related to Roma.
The purpose of our study was (1) to use the available but untapped NIHIFM data as a means to describe patient inequality in health delivery and reimbursement between segregated communities (where the most vulnerable populations with extremely high Roma representation reside) and nearby nonsegregated areas; (2) to outline the variability of this inequality across different Hungarian GMPs that serve both segregated and nonsegregated areas; and (3) to aid in the conceptualization and implementation of a new equality-oriented monitoring system.
2 Methods
2.1 Setting
The study utilized person-level health records, and evaluated GMP-level-aggregated indicators. All Hungarian GMPs (N = 4,359) who delivered care for adults were investigated. Each of them were contracted with the NIHIFM (the only health insurance institute in Hungary). The NIHIFM provided data on 2020 for secondary analysis on the health care use, reimbursement, and health status of adults belonging to the GMPs.
2.2 Design
A cross-sectional study of Hungarian GMPs providing care to segregated adults was performed. Segregated areas (SAs) were mapped and ascertained by applying the classification of a governmental decree that defines them as within settlement clusters of adults between the ages of 18 and 59 with a high proportion with at most primary-level education and no active income. Accordingly, the NIHIFM classified each household as either an SA or nonsegregated area [complementary area (CA)], which were mutually exclusive. Using addresses, any adult of at least 18 years of age could therefore be defined as living in an SA or CA. GMPs without patients living in an SA were excluded from the analysis.
2.2.1 Outcome indicators
2.2.1.1 Health care delivery
Health care delivery rates for multiple services were calculated as the number of patients who used the health service per patient belonging to a GMP for the previous 12 months. The delivery indicators included (1) the number of general practitioner visits, (2) outpatient service use without computed tomography or magnetic resonance imaging (CT/MRI) services, (3) CT/MRI services, and (4) hospitalization.
2.2.1.2 Health care reimbursement
Per capita reimbursement was calculated for these services as health insurance spending (in Euros) per patient belonging to the general medical practice for the previous 12 months. With the addition of medication costs, and since the NIHIFM finances GMPs per capita irrespective of the number of patient visits, this measure was not included among the reimbursement indicators, as it does not influence variability in GMP average per capita financing.
2.2.1.3 Premature mortality
All-cause premature mortality was defined as all deaths of adults below 65 years of age who had not changed their GMP in the past 5 years. This restriction was applied to exclude those who died in the care of a new GMP who did not manage their health prior to their death.
2.3 Statistical analysis
Standardized performance measures were calculated using the national average as a reference. Indicators for SAs and CAs were indirectly standardized by age (applied age groups: 18–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75–79, and 80 and above), sex and, eligibility for an exemption certificate. Exemption certificates are issued by the local municipalities to patients with disadvantageous socioeconomic status and chronic diseases (if recommended by GPs) and ensure free of charge access to medicines and medical devices. If GMPs provided care to more than one settlement, the observed and expected values were summarized to obtain GMP specific SA and CA measures. Dividing GMP-level observed values over expected values resulted in standardized risk ratios for SAs (SRsa) and CAs (SRca) for each indicator and GMP (32, 34–36). These GMP-level data were aggregated further to obtain country level standardized measures for SAs and CAs.
Relative performance in SAs was described by the risk ratio (RR), which was calculated by the SRsa/SRca ratio for each GMP and for the whole country along with 95% confidence intervals (95% CIs). Impact measures such as excess number of cases in the SAs, percentage of risk attributable to segregation in the population of SAs (attributable risk), and percentage of risk attributable to segregation in the population of the entire country (population attributable risk) were computed using nationally and locally adjusted standardized ratios.
3 Results
The studied population consisted of 7,385,641 adults (3,456,560 men and 3,929,081 women), with 2,071 identified segregated areas hosting 283,876 adults (139,507 men; 144,369 women). Demographic structure varied widely between the SA and CA populations (Figure 1). The mean age was notably lower among those living in SAs (total: 43.3 years; men: 42.2 years; women: 44.4 years) than among those living in CAs (total: 50.4 years; men: 48.5 years; women: 52.1 years). The older adult dependency ratio (the proportion of older adult individuals aged 65 or above among individuals aged 15 and above) was remarkably lower in SAs (15.4%) than in CAs (33.7%).
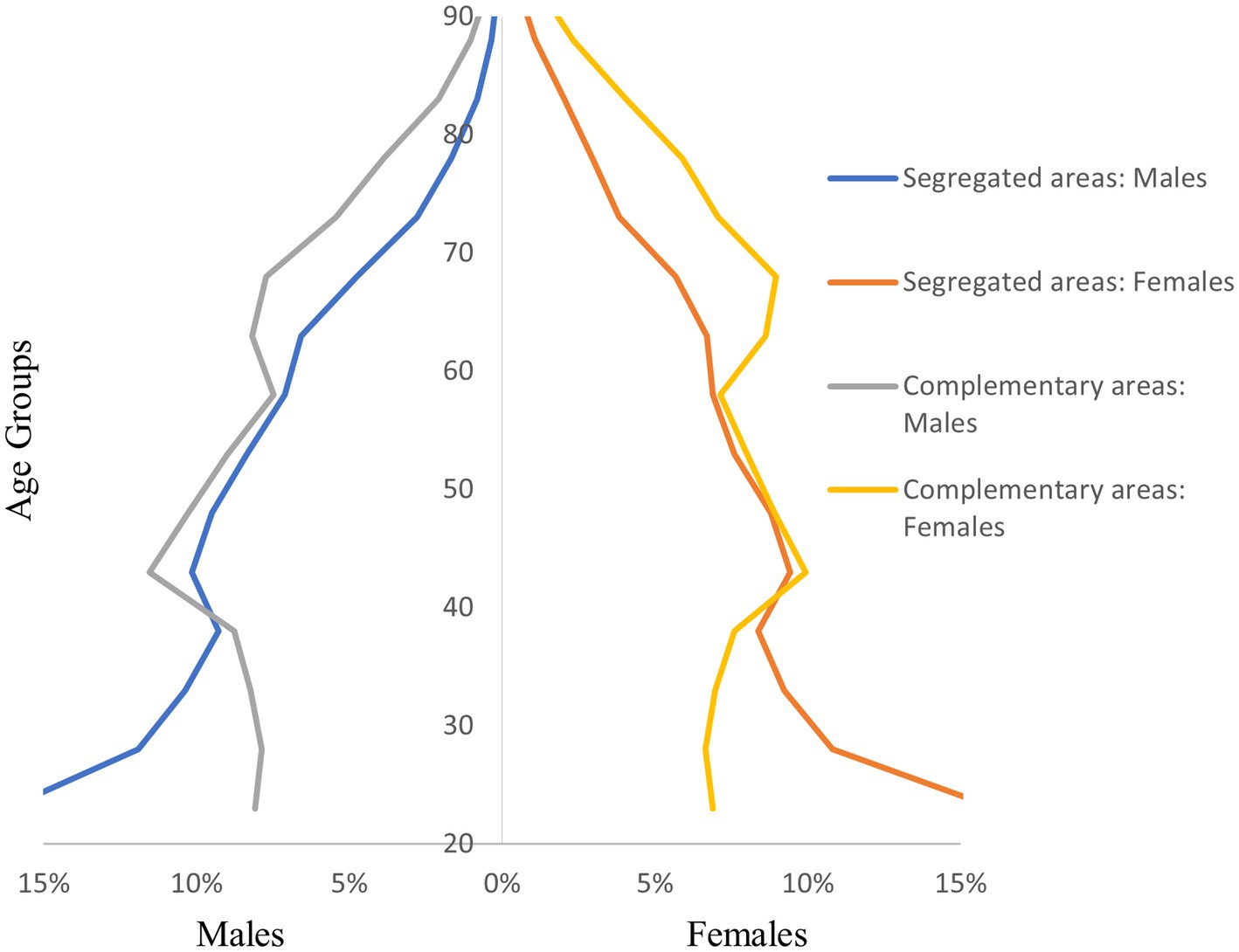
Figure 1. Demographic structure of the segregated and complementary populations.
The distribution of the number of segregated patients belonging to a GMP was highly varied across the standardized health care delivery, health care reimbursement, and premature mortality indicators (Figures 2–4). The highest level of heterogeneity of both episode and reimbursement indicators for relative GMP performance was observed in imaging examinations. Outpatient service use showed the highest variability.

Figure 2. Distribution of segregated adult patients according to the relative health care delivery ratio among Hungarian GMPs.
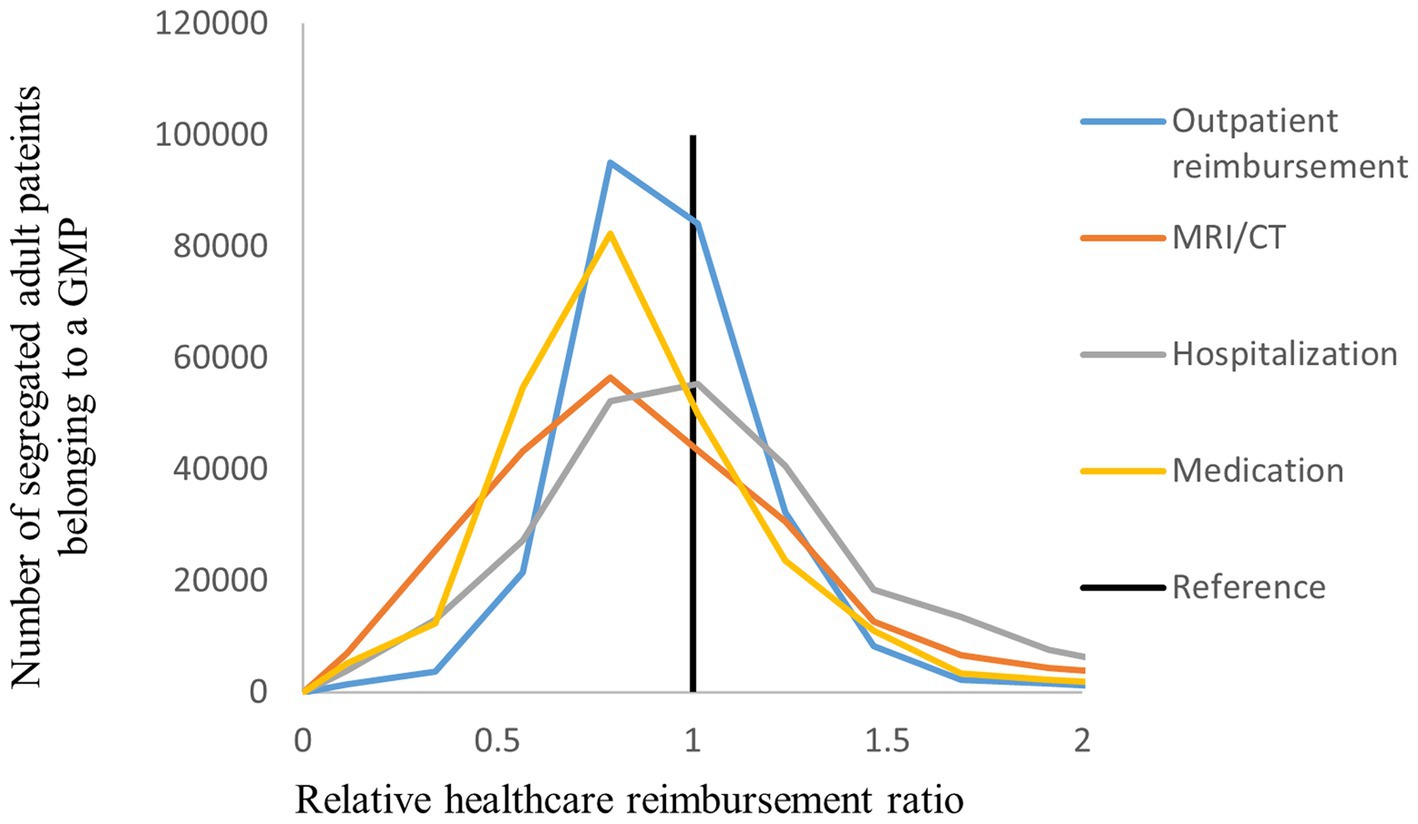
Figure 3. Distribution of segregated adult patients according to the relative health care reimbursement ratio among Hungarian GMPs.
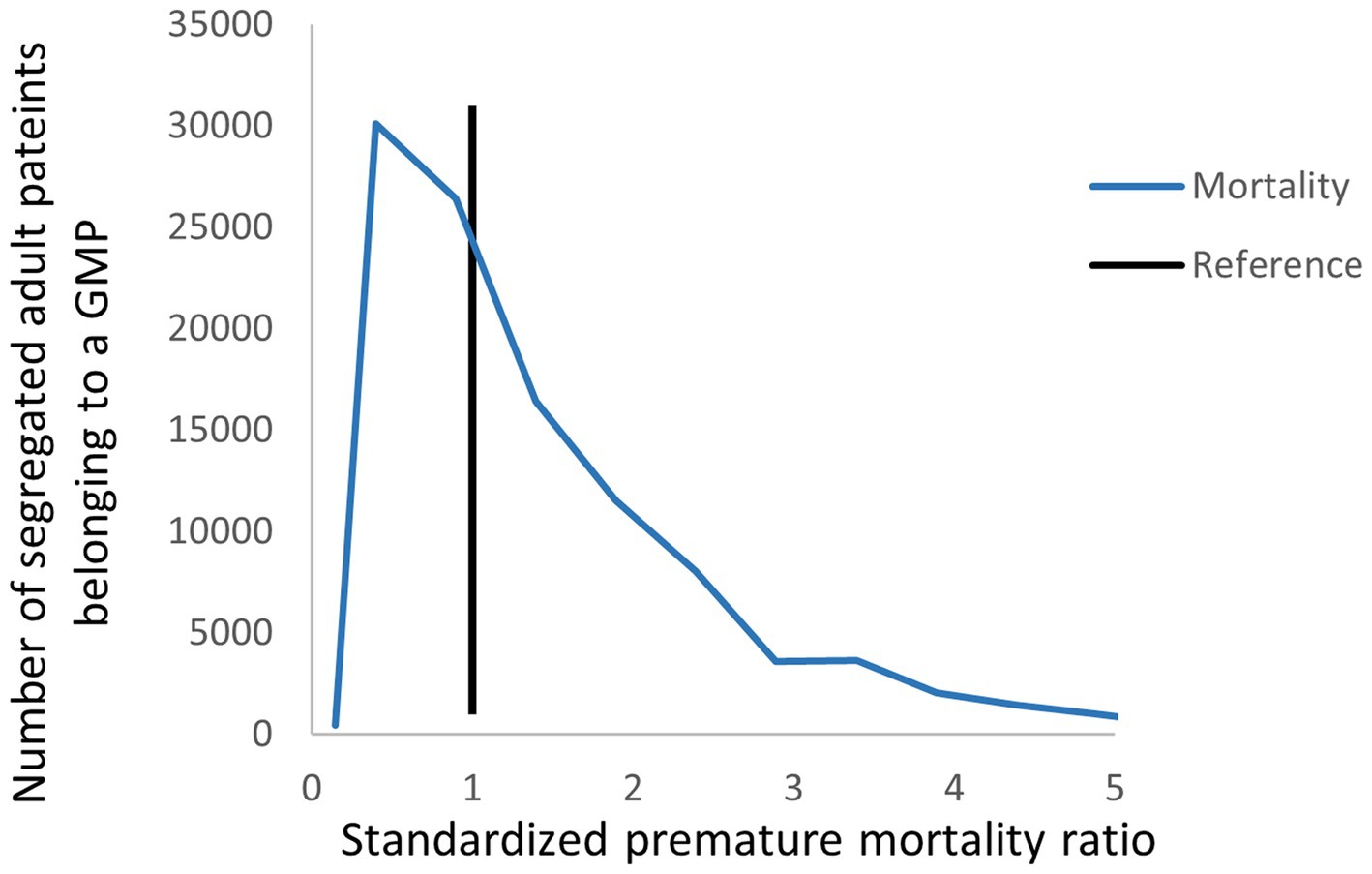
Figure 4. Distribution of segregated adult patients according to the relative premature mortality ratio among Hungarian GMPs.
3.1 Health care delivery
According to the standardized relative indicators aggregated for the whole country (Table 1) segregated groups had a significantly higher rate of health care services use than their complementary counterparts (RR = 1.222, 95% CI: 1.220;1.223). Specifically, for individual services provided to segregated patients, the number of GP visits per person per year (RR = 1.251, 95% CI: 1.249;1.253) and the number of hospital admissions per year exceeded those for complementary patients (RR = 1.250, 95% CI: 1.237;1.264). on the other hand, segregated patients experienced a significantly reduced number of treatments per year in outpatient service centers (RR = 0.948, 95% CI: 0.943;0.953) and imaging examinations (RR = 0.935, 95% CI: 0.920;0.950) compared to their counterparts.
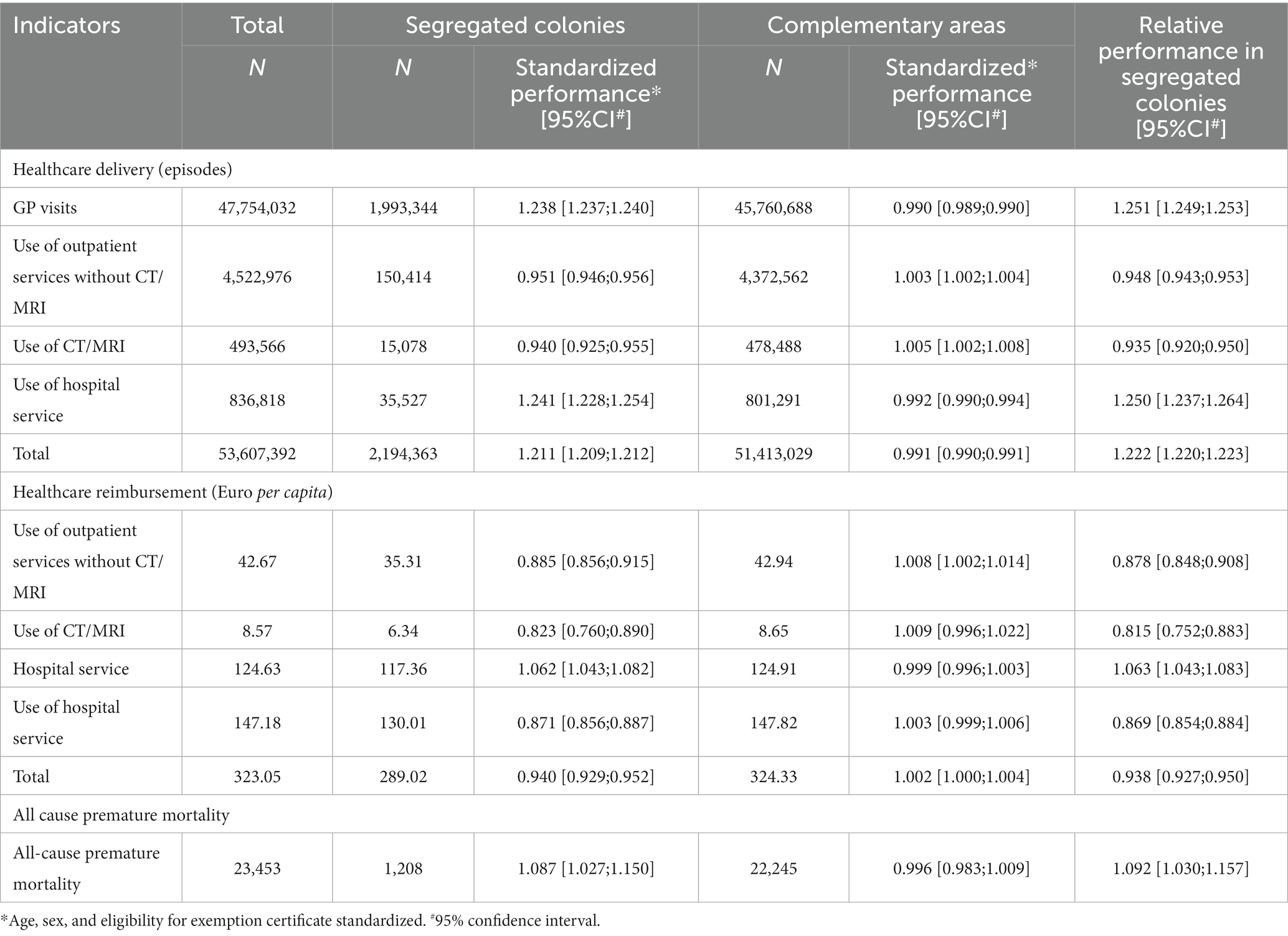
Table 1. Relative health care delivery, reimbursement, and all-cause premature mortality among Hungarian adults provided by general medical practices situated in a segregated or complementary area.
Regarding attributable risk (Table 2), patients living in an SA were associated with an increase in visits to health care services by 18.1% (95% CI: 18.0;18.2), with a population-attributable risk of 0.742% when comparing with CAs. Considering the number of episodes, the number of GP visits showed broad inequality, with an estimation of 400,024 (95% CI: 397,811;402,234) excess visits made per year. Hospital service use also had an excess of 7,116 (95% CI: 6,819;7,410), a 20% increase compared to residence in a CA. Meanwhile, the number of outpatient services used and CT/MRI examinations were lower by 8,241 (95% CI: 9,045;7,441) and 1,046 (95% CI: 7,911;306), respectively.
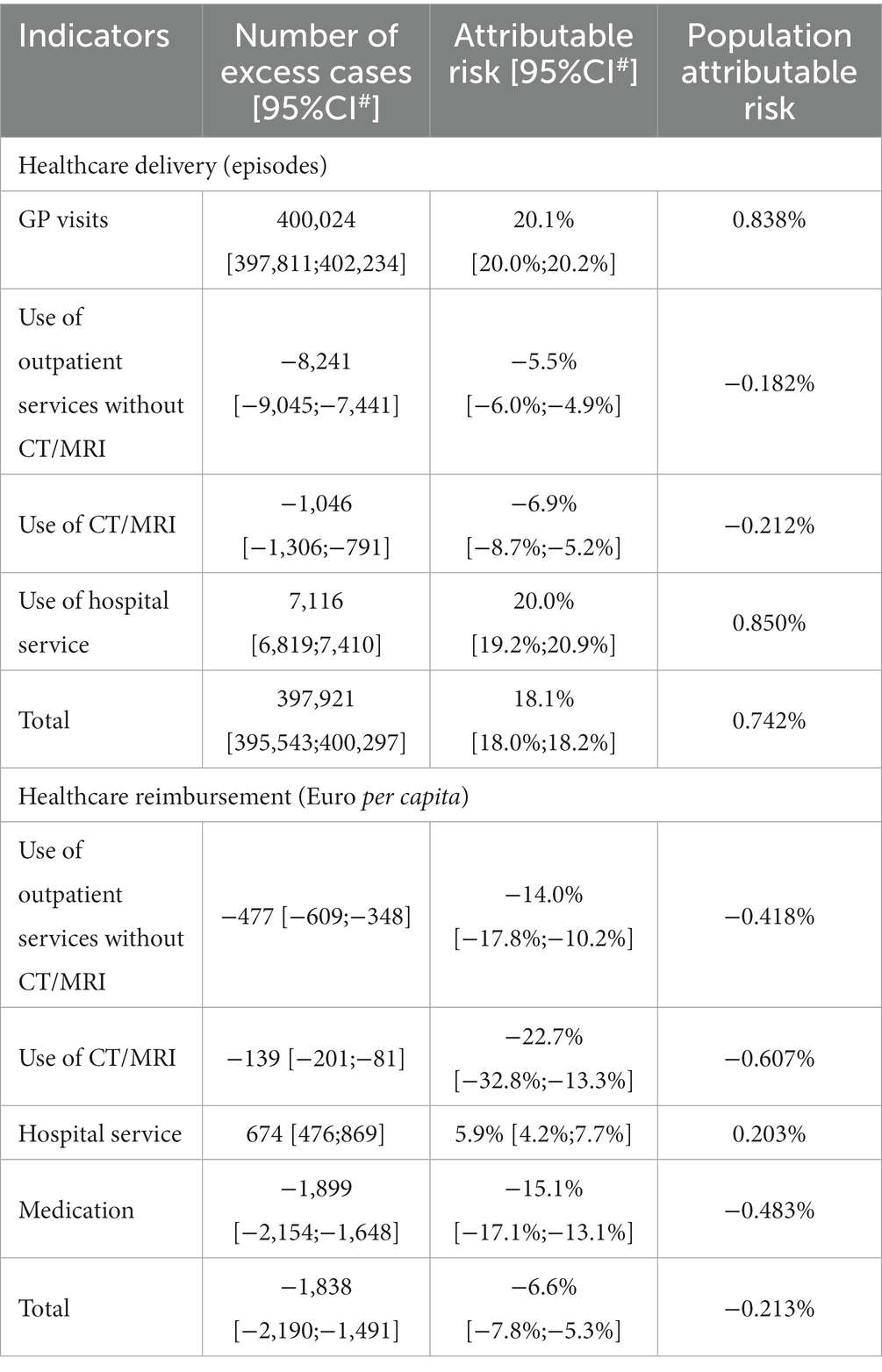
Table 2. Impact of segregation among adults living in segregated areas (number of excess cases and attributable risk) and in the whole adult population of Hungary (population attributable risk).
3.2 Health care reimbursement
Health care reimbursement also had significant dissimilarities depending on whether patients lived in SAs or CAs (Table 1). Total health services reimbursement for a GMP was significantly reduced for SA patients (RR = 0.938, 95% CI: 0.927;0.950). Specifically, GMPs exhibited significantly lower reimbursement per year for outpatient services to SA patients (RR = 0.878, 95% CI: 0.848;0.908), MRI/CT examinations (RR = 0.815, 95% CI: 0.752;0.883), and medications (RR = 0.869, 95% CI: 0.854;0.884). Hospitalization reimbursement, on the other hand, showed higher spending on segregated groups (RR = 1.063, 95% CI: 1.043;1.083).
Providing care to segregated patients lowered health care reimbursement by 6.6% (95% CI: 7.8;5.3) (Table 2) when compared to complementary groups, with a population-attributable risk of −0.213%. This finding is predominantly attributed to medication-related NIHIFM reimbursement, where the per capita yearly cost was lower for SA patients by 1,899 EUROs (95% CI: 2,154;1,648) compared to CA patients.
3.3 All-cause premature mortality
The age-and sex-standardized premature mortality among the SA population was significantly higher than that in the CA population (RR = 1.092, 95% CI: 1.030;1.157) (Table 1). The estimated 101.544 (95% CI: 37.355;162.213) excess cases in the SA population corresponded to 8.406% (95% CI: 3.092;13.428). The population level impact was estimated to be 0.433%.
4 Discussion
4.1 Main findings
Our study reveals variation and statistically significant dissimilarity in health care use, reimbursement, and premature mortality across Hungarian GMPs, pointing to causes of the existing health gap between segregated people and their counterparts living in complementary areas.
A characteristic health care use pattern of adults living in segregated areas was identified. People living in SAs use health care services more frequently than those living in CAs; however, the amount of health care reimbursement paid for their care is significantly lower, suggesting lower quality of care.
In the case of primary care, crude indicators show that segregated groups had a higher rate of GP appointments, which corresponds with other studies from Europe (37, 38). And publications on the poorer health status of residents of segregations (32, 35, 36).
However, the services of outpatient and imaging centers were notably less utilized by segregated groups, which correlates with a significant reduction in GMPs’ reimbursement compared to complementary groups. This difference, coupled with the fact that people living in SAs have poorer health status and a likely greater need for outpatient services, implies the underutilization of these services by segregated groups.
This finding helps explain the increase in hospital service utilization in SA groups paralleled with an increase in reimbursement; since outpatient services (including advanced and specialized tests and treatments) are required to diagnose, reverse, or halt the progression of chronic diseases, which can otherwise go undetected until a more serious prognosis requires hospitalization. Moreover, this discrepancy could also be due to the poorer health and greater needs of people living in SAs. Numerous studies have reported increased hospital admissions, avoidable and otherwise, in segregated minorities (32, 39, 40).
The health status of adults living in segregation was significantly poorer than that of adults living in complementary areas, as evidenced by their higher premature mortality rate, corroborating other studies showing the same conclusion (17, 34, 35). Their poorer health may be an outcome of their lower socioeconomic status and unhealthy lifestyles (10, 41) combined with the provision of lower-quality health care (30).
4.2 Strengths and limitations
The major strength of our study was the inclusion of all Hungarian adults living in SAs or in CAs. Because the Hungarian GMPs are required to contract with NIHIFM, detailed reimbursement and health data were available for each subject. Therefore, there was no selection bias in our study. Further, the proper quality of data was ensured by the standard NIHIFM protocols for data collection (42).
The present study results reflect estimations of health care use and mortality of Roma living in SAs, since Roma constitute 94% of the inhabitants of these areas (14). It is presumable that the Roma and non-Roma adults in SAs follow similar lifestyle and have similar health status. Consequently, the SA specific indicators can be considered as proxy estimations for those Roma who live in segregated areas.
Unfortunately, the health care use indicators of our study were not adjusted for the health needs and health status of the investigated populations, to which the observed differences in health care use could be partially attributed. The higher premature mortality shows that the health status is worse in SAs, consequently leading to more intensive use of health care services in these areas. In this context, the higher frequency of GP visits and hospital admissions can be considered an adequate response to the higher health care needs, while the lower utilization of outpatient services in SAs is inconsistent, suggesting a potential malfunction in the system, where fewer outpatient services were provided than necessary. Our results do not identify the mechanisms behind the observed inequalities, calling for more detailed pathway analyses to propose interventions that could help lessen the present inequality.
Data available for our analysis were from 2020. That year was seriously affected by COVID-19. The first case in Hungary was detected on 04/03/2020 (43). The consecutive epidemiologic measures profoundly impacted health care operation (44). Consequently, our results predominantly reflect health care inequality during the COVID-19 epidemic. However, the compared groups of SAs and CAs shared the same settlements, geographical access to health care, and GP who was ultimately responsible for the gate-keeping of treatment pathways. Therefore, any differences between SAs and CAs in health care use or reimbursement should be minimized. Nevertheless, vaccination coverage was lower in SAs, suggesting that the COVID-19 epidemic contributed to some of the observed health care use and reimbursement inequalities (45). Altogether, the inequality pattern observed in our study should be further investigated in years not affected by the epidemic to substantiate the findings of our investigation.
4.3 Implications
Our findings indicate a significant association between segregation and severe health care issues, as demonstrated by country level aggregated relative risk measures. Notably, these problems largely stem from the local setting as evidenced by the varying levels of inequality at the local GMP-level. Some GMPs exhibit pronounced local inequalities, while others show no such disparities (Supplementary Table S1).
A monitoring system could distinguish between GMPs with and without local bias, and could monitor the time trend of country level inequality. At present, there is no monitoring system, to inform stakeholders neither at local nor at the country level. Consequently, there is a pressing need for monitoring systems specific to SAs. Our investigation demonstrates not only the feasibility of segregation oriented monitoring but also suggests indicators for this purpose. However, it is evident that additional indicators are required to understand the processes leading to the observed disparities in premature mortality, health care use, and insurance reimbursement. This monitoring system could support the National Social Inclusion Strategy of the Hungarian government (29), and as Roma are overrepresented in SAs, it could contribute to the programs aimed at improving the health status of the Roma population. The effectiveness of interventions could be enhanced by considering self-declared Roma ethnicity (available from census data) in defining SAs.
5 Conclusion
This analysis showed that (1) in the Hungarian health system, there are varying degrees of GMP-level dissimilarity in both health services delivery and reimbursement, in addition to varying health status between people living in SAs and CAs; this suggests that residence in an SA is a strong factor impacting the health care services system. Furthermore, (2) some Hungarian GMPs seemed to provide equal care to their inhabitants, while others show varied levels of inequality. We suggest that further studies are required to investigate such variations and local factors affecting the quality of care provided to segregated populations. According to our findings (3) any decision-making on interventions related to SAs should take the local (GMP-level) environment into consideration.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: the datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. Requests to access these datasets should be directed to amFub3Muc2FuZG9yQG1lZC51bmlkZWIuaHU=.
Ethics statement
The protocol to produce segregation-specific indicators was approved by the Office of the Commissioner for Fundamental Rights (AJB-3147/2013), the general director of the NHIF (E0101/215-3/2014), and the Hungarian National Authority for Data Protection and Freedom of Information (NAIH/2015/826/7N). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
FK prepared the literature review, analyzed, interpreted the data, and prepared the draft of the manuscript. FV prepared the primary database. LK helped with conception and data base preparation. RÁ helped with conception and study design. JS elaborated on the design, interpreted the results, and finalized the manuscript. All authors read and approved the final manuscript.
Funding
This study was carried out in the framework of the “Routine monitoring for the health status and health care use in the Hungarian segregated colonies” program (BM/6327-3/2021, FEIF/951/2021-ITM), supported by the Deputy State Secretariat for Social Inclusion, Ministry of Interior (https://2010-2014.kormany.hu/en/ministry-of-interior), and the Stipendium Hungaricum Scholarship Program (grant SHE-26763-004/2020 to FK). The project was co-financed by the Eötvös Loránd Research Network (TKCS-2021/32).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1152555/full#supplementary-material
Abbreviations
GMP, General medical practice; GP, General practitioner; NHIF, National Health Insurance Fund; NIHIFM, National Institute of Health Insurance Fund Management; SA, Segregated areas; CA, Complementary areas; CI, Confidence interval; IQR, Inter quartile range; CT, Computed tomography; MRI, Magnetic resonance imaging.
References
1. Jacobs, DE. Environmental health disparities in housing. Am J Public Health. (2011) 101:S115–22. doi: 10.2105/AJPH.2010.300058
2. European Commission, Executive Agency for Health and Consumers. (2013). Health inequalities in the EU: final report of a consortium - Consortium lead: Sir Michael Marmot, European Commission. Available at: https://data.europa.eu/doi/10.2772/34426. (Accessed April 23, 2023).
3. European Union Agency for Fundamental Rights. (2013). Inequalities and multiple discrimination in access to and quality of healthcare. LU: Publications Office. Available at: https://data.europa.eu/doi/10.2811/17523. (Accessed April 23, 2023).
4. Kramer, MR, and Hogue, CR. Is segregation bad for your health? Epidemiol Rev. (2009) 31:178–94. doi: 10.1093/epirev/mxp001
5. Kawachi, I, and Berkman, LF. Neighborhoods and health. Oxford: Oxford University Press (2003). 369 p.
6. Subramanian, SV, Acevedo-Garcia, D, and Osypuk, TL. Racial residential segregation and geographic heterogeneity in black/white disparity in poor self-rated health in the US: a multilevel statistical analysis. Soc Sci Med. (2005) 60:1667–79. doi: 10.1016/j.socscimed.2004.08.040
7. Beck, AF, Edwards, EM, Horbar, JD, Howell, EA, McCormick, MC, and Pursley, DM. The color of health: how racism, segregation, and inequality affect the health and well-being of preterm infants and their families. Pediatr Res. (2020) 87:227–34. doi: 10.1038/s41390-019-0513-6
8. Acevedo-Garcia, D. Residential segregation and the epidemiology of infectious diseases. Soc Sci Med. (2000) 51:1143–61. doi: 10.1016/S0277-9536(00)00016-2
9. Kozubik, M, Van Dijk, JP, and Odraskova, B. Roma housing and eating in 1775 and 2013: a comparison. Int J Environ Res Public Health. (2018) 15:588. doi: 10.3390/ijerph15040588
10. Kolarčik, P, Geckova, AM, Orosova, O, van Dijk, JP, and Reijneveld, SA. Predictors of health-endangering behaviour among Roma and non-Roma adolescents in Slovakia by gender. J Epidemiol Community Health. (2010) 64:1043–8. doi: 10.1136/jech.2009.092098
11. Ringold, D, Orenstein, MA, and Wilkens, E. Roma in an expanding Europe: Breaking the poverty cycle. Washington, DC: World Bank Publications (2005). 270 p.
12. Parekh, N, and Rose, T. Health inequalities of the Roma in Europe: a literature review. Cent Eur J Public Health. (2011) 19:139–42. doi: 10.21101/cejph.a3661
13. KSH. Hungarian Central Statistical Office. Available at: http://www.ksh.hu/nepszamlalas/tables_regional_00. (Accessed February 12, 2021).
14. Kósa, K, Daragó, L, and Adány, R. Environmental survey of segregated habitats of Roma in Hungary: a way to be empowering and reliable in minority research. Eur J Pub Health. (2011) 21:463–8. doi: 10.1093/eurpub/ckp097
15. BeszélŐ. (2004) Babusik Ferenc írása 2004/10. Available at: http://beszelo.c3.hu/04/10/14babusik.htm. (Accessed September 7, 2021).
16. Sudzinova, A, Nagyova, I, Rosenberger, J, Studencan, M, Vargova, H, Middel, B, et al. Seven years’ mortality in Roma and non-Roma patients after coronary angiography. Eur J Pub Health. (2015) 25:765–9. doi: 10.1093/eurpub/ckv057
17. Vincze, F, Földvári, A, Pálinkás, A, Sipos, V, Janka, EA, Ádány, R, et al. Prevalence of chronic diseases and activity-limiting disability among Roma and non-Roma people: a cross-sectional, census-based investigation. Int J Environ Res Public Health. (2019) 16:3620. doi: 10.3390/ijerph16193620
18. McFadden, A, Siebelt, L, Gavine, A, Atkin, K, Bell, K, Innes, N, et al. Gypsy, Roma and Traveller access to and engagement with health services: a systematic review. Eur J Pub Health. (2018) 28:74–81. doi: 10.1093/eurpub/ckx226
19. Jarcuska, P, Bobakova, D, Uhrin, J, Bobak, L, Babinska, I, Kolarcik, P, et al. Are barriers in accessing health services in the Roma population associated with worse health status among Roma? Int J Public Health. (2013) 58:427–34. doi: 10.1007/s00038-013-0451-8
20. Hanssens, LGM, Devisch, I, Lobbestael, J, Cottenie, B, and Willems, S. Accessible health care for Roma: a gypsy’s tale a qualitative in-depth study of access to health care for Roma in Ghent. Int J Equity Health. (2016) 15:38. doi: 10.1186/s12939-016-0327-7
21. Földes, ME, and Covaci, A. Research on Roma health and access to healthcare: state of the art and future challenges. Int J Public Health. (2012) 57:37–9. doi: 10.1007/s00038-011-0312-2
22. Arora, VS, Kühlbrandt, C, and McKee, M. An examination of unmet health needs as perceived by Roma in central and Eastern Europe. Eur J Pub Health. (2016) 26:737–42. doi: 10.1093/eurpub/ckw004
23. European Commission. (2011) An EU Framework for National Roma Integration Strategies up to 2020. EUR Lex. Available at: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:52011DC0173. (Accessed October 15, 2021).
24. Tremlett, A, and Mc Garry, A. Challenges facing researchers on Roma minorities in contemporary Europe. European Centre for Minority Issues (ECMI): 19. ECMI Research Papers. (2013) 19:1–12.
25. Kósa, K, and Adány, R. Studying vulnerable populations: lessons from the Roma minority. Epidemiol Camb Mass. (2007) 18:290–9. doi: 10.1097/01.ede.0000258919.15281.4f
26. European Commission. Communication from the commission to the European Parliament, the council, the European economic and social Committee of the Regions: An EU framework for National Roma Integration Strategies up to 2020. (2011).
27. Gaal, P, Szigeti, S, Csere, M, Gaskins, M, and Panteli, D. Hungary health system review. Health Syst Transit. (2011) 13:1–266.
28. OECD. (2019). Policies EO on HS and. Hungary: country health profile 2019. Available at: https://www.oecd-ilibrary.org/content/publication/4b7ba48c-en. (Accessed October 5, 2021).
29. Government of Hungary. National Social Inclusion Strategy and the government action plan on its implementation between 2015 and 2017. Budapest, Hungary: Government of Hungary (2015).
30. Kovács, N, Varga, O, Nagy, A, Pálinkás, A, Sipos, V, Kőrösi, L, et al. The impact of general practitioners’ gender on process indicators in Hungarian primary healthcare: a nation-wide cross-sectional study. BMJ Open. (2019) 9:e027296. doi: 10.1136/bmjopen-2018-027296
31. Kovács, N, Pálinkás, A, Sipos, V, Nagy, A, Harsha, N, Kőrösi, L, et al. Factors associated with practice-level performance indicators in primary health Care in Hungary: a Nationwide cross-sectional study. Int J Environ Res Public Health. (2019) 16:3153. doi: 10.3390/ijerph16173153
32. Sándor, J, Pálinkás, A, Vincze, F, Kovács, N, Sipos, V, Kőrösi, L, et al. Healthcare utilization and all-cause premature mortality in Hungarian segregated Roma settlements: evaluation of specific indicators in a cross-sectional study. Int J Environ Res Public Health. (2018) 15:1835. doi: 10.3390/ijerph15091835
33. Bekele, BB, Bogale, B, Negash, S, Tesfaye, M, Getachew, D, Weldekidan, F, et al. Public health interventions on prescription redemptions and secondary medication adherence among type 2 diabetes patients: systematic review and meta-analysis of randomized controlled trials. J Diabetes Metab Disord. (2021) 20:1933–56. doi: 10.1007/s40200-021-00878-0
34. Kósa, Z, Moravcsik-Kornyicki, Á, Diószegi, J, Roberts, B, Szabó, Z, Sándor, J, et al. Prevalence of metabolic syndrome among Roma: a comparative health examination survey in Hungary. Eur J Pub Health. (2015) 25:299–304. doi: 10.1093/eurpub/cku157
35. Kósa, Z, Széles, G, Kardos, L, Kósa, K, Németh, R, Országh, S, et al. A comparative health survey of the inhabitants of Roma settlements in Hungary. Am J Public Health. (2007) 97:853–9. doi: 10.2105/AJPH.2005.072173
36. Sándor, J, Kósa, Z, Boruzs, K, Boros, J, Tokaji, I, McKee, M, et al. The decade of Roma inclusion: did it make a difference to health and use of health care services? Int J Public Health. (2017) 62:803–15. doi: 10.1007/s00038-017-0954-9
37. Uiters, E, Devillé, WLJM, Foets, M, and Groenewegen, PP. Use of health care services by ethnic minorities in the Netherlands: do patterns differ? Eur J Pub Health. (2006) 16:388–93. doi: 10.1093/eurpub/ckl040
38. van der Gaag, M, van der Heide, I, Spreeuwenberg, PMM, Brabers, AEM, and Rademakers, JJDJM. Health literacy and primary health care use of ethnic minorities in the Netherlands. BMC Health Serv Res. (2017) 17. doi: 10.1186/s12913-017-2276-2
39. Dalla Zuanna, T, Spadea, T, Milana, M, Petrelli, A, Cacciani, L, Simonato, L, et al. Avoidable hospitalization among migrants and ethnic minority groups: a systematic review. Eur J Pub Health. (2017) 27:861–8. doi: 10.1093/eurpub/ckx113
40. Vaughan Sarrazin, MS, Campbell, ME, Richardson, KK, and Rosenthal, GE. Racial segregation and disparities in health care delivery: conceptual model and empirical assessment. Health Serv Res. (2009) 44:1424–44. doi: 10.1111/j.1475-6773.2009.00977.x
41. Belak, A, Madarasova Geckova, A, van Dijk, JP, and Reijneveld, SA. Why don’t segregated Roma do more for their health? An explanatory framework from an ethnographic study in Slovakia. Int J Public Health. (2018) 63:1123–31. doi: 10.1007/s00038-018-1134-2
42. Hungarian Government. (1999). Government decree on the detailed rules for the financing of health services from the health insurance fund – collection of effective legislation. Available at: https://net.jogtar.hu/jogszabaly?docid=99900043.kor. (Accessed December 17, 2023).
43. Kemenesi, G, Kornya, L, Tóth, GE, Kurucz, K, Zeghbib, S, Somogyi, BA, et al. Nursing homes and the elderly regarding the COVID-19 pandemic: situation report from Hungary. GeroScience. (2020) 42:1093–9. doi: 10.1007/s11357-020-00195-z
44. Bekele, BB, Alhaffar, BA, Wasnik, RN, and Sándor, J. The effect of the COVID-19 pandemic on the social inequalities of health care use in Hungary: a nationally representative cross-sectional study. Int J Environ Res Public Health. (2022) 19:2258. doi: 10.3390/ijerph19042258
Keywords: cross-sectional, segregation, inequality, healthcare, health reimbursement, general medical practitioner, Hungary
Citation: Kasabji F, Vincze F, Lakatos K, Pálinkás A, Kőrösi L, Ulicska L, Kósa K, Ádány R and Sándor J (2024) Cross-sectional comparison of health care delivery and reimbursement between segregated and nonsegregated communities in Hungary. Front. Public Health. 12:1152555. doi: 10.3389/fpubh.2024.1152555
Edited by:
Hanadi Hamadi, University of North Florida, United StatesReviewed by:
Anandadeep Mandal, University of Birmingham, United KingdomAurora Tafili, University of Alabama at Birmingham, United States
Copyright © 2024 Kasabji, Vincze, Lakatos, Pálinkás, Kőrösi, Ulicska, Kósa, Ádány and Sándor. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: János Sándor, amFub3Muc2FuZG9yQG1lZC51bmlkZWIuaHU=