 Min Chen
Min Chen Yantao Liu1,2,3
Yantao Liu1,2,3 Xue Yang
Xue Yang Jiaqi Ni
Jiaqi Ni
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 23 March 2023
Sec. Health Economics
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.990181
Objective: To analyze the inpatient cost of hematopoietic stem cell transplantation (HSCT) in children, so as to support clinical decision-making.
Methods: Study population were children who received HSCT in a tertiary children’s hospital (Sichuan, China) between 1st January 2020 and 31st December 2021. The median and interquartile range (IQR) of total cost at 100 days post transplantation were calculated. Subgroup analyses were conducted based on age, gender, transplantation types, and post-transplant complications. The cost differences between subgroups were analyzed to determine whether it had an impact on the total costs.
Results: A total of 142 pediatric patients were included in the study with a total cost of 250721.78 yuan (197019.16–315740.52, 1 yuan equals to around 0.15 US dollars). Drug costs accounted for 51.85% of the total cost, followed by medical service costs (12.57%) and treatment expenses (12.24%). In terms of transplantation types, the cost of autologous transplantation was lower than that of allogeneic transplantation (115722.98 yuan vs. 256043.99 yuan, p < 0.05), and the cost of human leukocyte antigen (HLA) complete matched was lower compared with that of partial matched (213760.88 yuan vs. 294044.84 yuan, p < 0.05). As for post-transplant complications, cases with <3 types of complications cost less than those with ≥3 types (212893.25 yuan vs. 286064.60 yuan, p < 0.05), and those with severity ≤ grade 2 cost less than those > grade 2 (235569.37 yuan vs. 280061.58 yuan, p < 0.05). Age and gender of patients did not lead to statistical differences in the total cost, while the transplantation types and post-transplant complications influenced the total cost.
Conclusion: The total cost at 100 days post transplantation associated with HSCT treatment were substantial for pediatric patients. The HLA compatibility between donors and recipients, and post-transplant complications were important factors affecting the total cost.
Hematopoietic stem cell transplantation (HSCT) is the procedure conducted after completely or partially destroyed the patient’s hematopoietic and immune systems with chemotherapy and / or radiological procedure, then donors’ or autologous healthy hematopoietic stem cells are transplanted to rebuild the patient’s hematopoietic and immune functions (1–3). With the advancement of supportive care and pre-transplant procedures, HSCT has become an effective treatment for hematological diseases such as lymphoma, multiple myeloma and leukemia, and non-hematological diseases such as genetic diseases (4).
HSCT is a significant financial burden for most families, which impacts the quality of life of the whole family (5). Previous studies revealed that many factors affected the total cost of HSCT, which included transplantation types, length of hospitalization, and pre-transplant treatments, etc. (6) Graft vs. host disease (GvHD), infection, disease recurrence and other post-transplant complications led to increased inpatient costs and even the failure of transplantation (6–8). Severe sepsis, acute respiratory failure, endotracheal intubation, total parenteral nutrition (TPN) could double the total cost (8).
A comprehensive search was conducted in databases including Cochrane Library, PubMed, Embase, NHS EED, HTA, CBM, CNKI, Wanfang, and VIP. Literature related to HSCT mainly came from the United States, Japan, Germany and other developed countries. Among them, only four studies were conducted in pediatric patients (9–12). In China, to the best of our knowledge, very limited data has been published on costs associated with HSCT in pediatric patients. The aim of this study is to fill this gap by investigating costs associated with HSCT based on claims data from a Chinese study population, so as to support clinical decision-making and health administrative regulations.
Data was obtained from the electronic medical record system of a tertiary children’s hospital (Sichuan, China). All pediatric patients who received HSCT between 1st January 2020 and 31st December 2021 were included. Literature reported that the direct medical costs of HSCT peaked in the first quarter post transplantation. The costs of 100 days post transplantation accounted for 75% of the total cost within 1 year post transplantation (12, 13). Therefore, the data collection time was the period after initial hospitalization to 100 days post transplantation. Patients with incomplete or missed medical records were excluded.
Medical records were retrospectively reviewed for patients’ demographic data (medical registration number, name, gender, age), admission date, discharge date, date of engraftment, duration of hospital stay, main diagnosis and inpatient expenses. The components of inpatient expenses included medical services, treatments and operations, nursing services, laboratory and diagnostic services, medications, blood products, etc.
Excel 2013 was adopted for data entry and classification, and SPSS 17.0 was used for statistical analysis. Cost data was classified into subgroups based on the patient’s medical information (age, gender, transplantation types, post-transplant complications, etc.), and the cost differences between subgroups were analyzed to determine whether it had an impact on the total cost of HSCT.
Shapiro–Wilk Normality test was performed on the data of each subgroup, and the data did not conform to the normal distribution if p < 0.05. Independent sample t-test was used for the data conforming to the normal distribution, and independent sample nonparametric test was used for the data not conforming to the normal distribution to compare the differences between subgroups. p < 0.05 represented statistically significant differences between subgroups.
A total of 1,322 hospital admissions with 208 pediatric patients were initially retrieved. After removing cases with incomplete medical records, 142 patients were finally included in the study, with 86 boys and 56 girls. The median age was 5 years old, and the median length of hospital stay post transplantation was 51 [43–63] days. In terms of disease types, 14 types were obtained. Leukemia was the most common type of disease receiving HSCT, which included 36 cases of acute myeloid leukemia, 23 cases of acute lymphoblastic leukemia, 7 cases of mixed leukemia, and 6 cases of chronic myeloid leukemia. Anemia was the second common type of disease receiving HSCT with 45 cases, including 24 cases of aplastic anemia and 21 cases of thalassemia. Other malignant diagnoses included solid tumors, leukodystrophy, congenital keratosis, lymphoproliferative diseases, mucopolysaccharide storage diseases, myelodysplastic syndromes, platelet dysfunction, and immune deficiencies with increased IgM. Related information including transplantation types, post-transplant complications and severity classification was shown in Table 1.
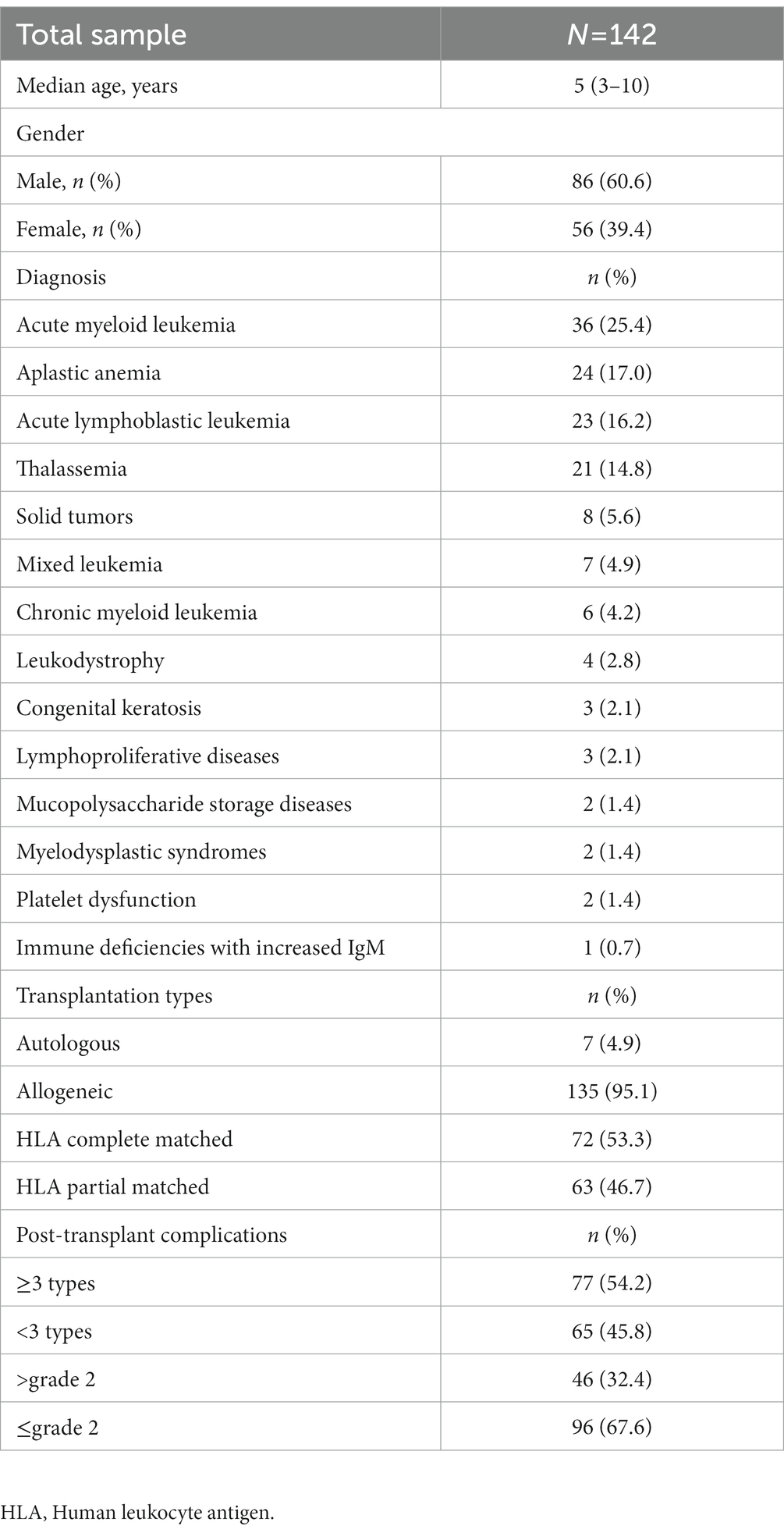
Table 1. Patient and transplant characteristics.
Direct health care costs were divided into 9 categories: (1) total costs; (2) medical service costs; (3) treatment expenses (surgical and non-surgical methods); (4) nursing service fees; (5) laboratory and diagnostic costs; (6) drug costs; (7) supportive care expenses (including blood transfusion fees, albumin fees, globulin fees, coagulation factor fees, cytokine fees, etc.); (8) material fees; (9) others. The costs were tested for normality, and the results showed that all the costs did not conform to the normal distribution (p < 0.05). The total cost of HSCT was 250721.78 yuan (197019.16−315740.52, 1 yuan equals to around 0.15 US dollars). Drug costs accounted for 51.85% of the total cost, followed by medical service costs (12.57%) and treatment expenses (12.24%; Table 2).
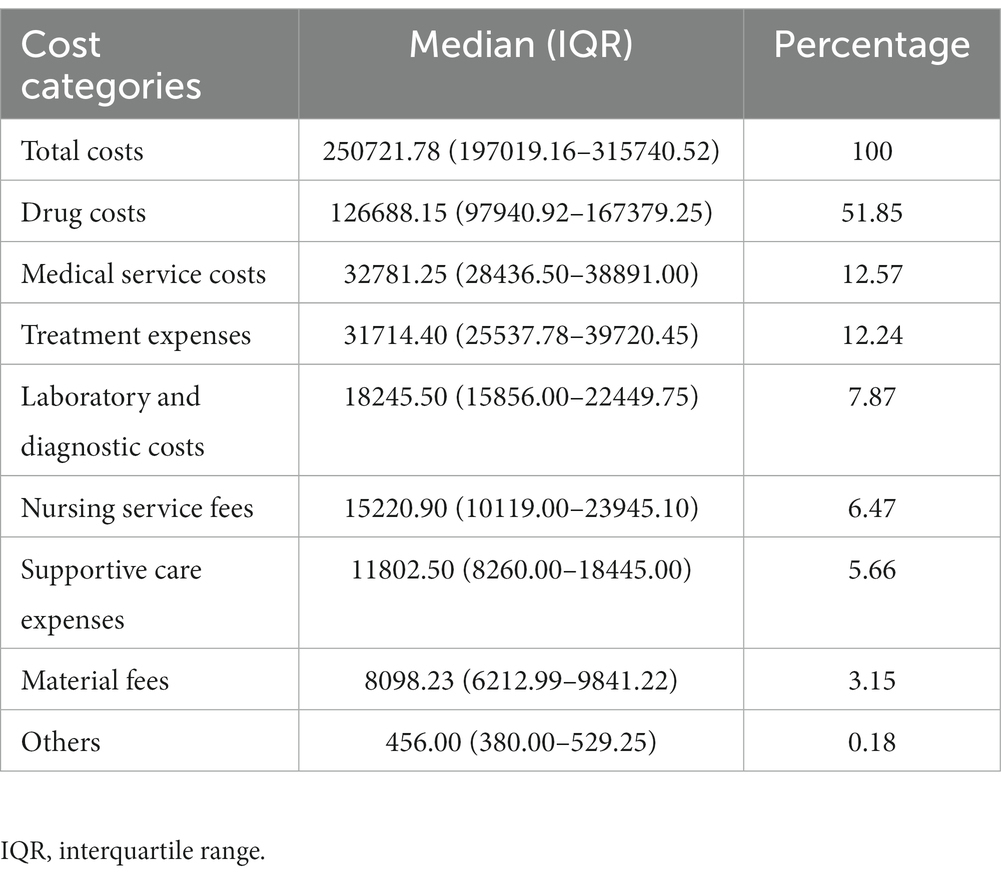
Table 2. Direct health care costs with hematopoietic stem cell transplantation.
Cost data was classified into subgroups based on the patient’s age, gender, transplantation types, and post-transplant complications. The cost differences between subgroups were analyzed to determine how these factors affected the total cost of HSCT.
Results revealed no significant differences of the costs between the 1- to 5-year-old and the 6- to16-year-old groups. Same results were observed between the male and female groups (p > 0.05), which indicated that age and gender did not influence the cost of HSCT (Table 3).
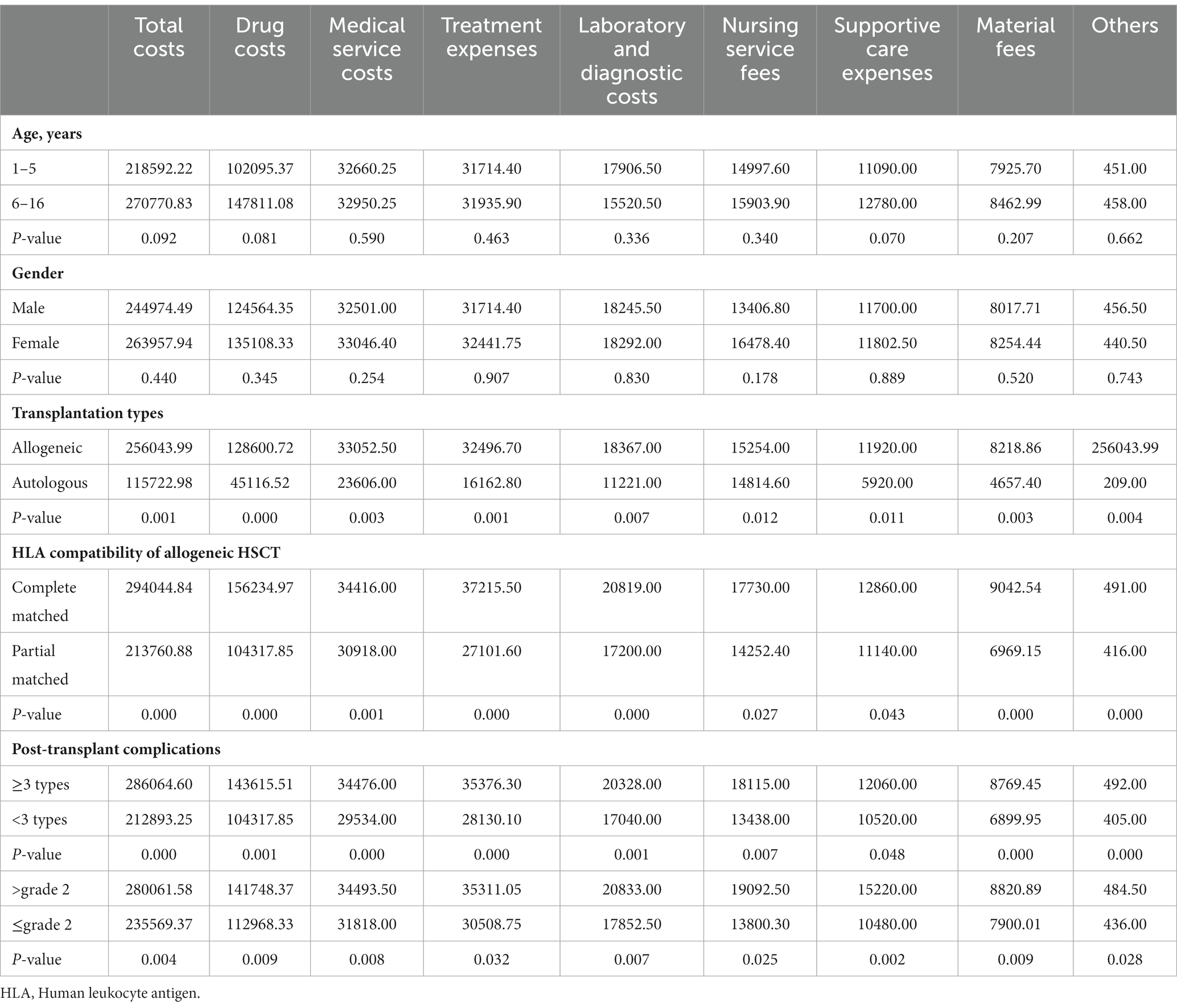
Table 3. Subgroup analysis of costs with hematopoietic stem cell transplantation.
Subgroup analysis in different transplantation types showed statistically significant differences in the costs between allogeneic hematopoietic stem cell transplantation (allogeneic HSCT) and autologous hematopoietic stem cell transplantation (autologous HSCT). In addition, human leukocyte antigen (HLA) fully matched and partially matched groups revealed similar differences (p < 0.05). The cost of autologous HSCT was lower than that of allogeneic HSCT, and the cost of HLA fully matched HSCT was lower than that of partially matched among allogeneic HSCT (Table 3).
In terms of complications after HSCT, 129 (90.8%) cases had infections, 87 (61.3%) cases experienced oral mucosal ulcer, 69 (48.6%) cases reported engraftment syndrome, 50 (35.2%) cases reported acute GvHD, 27 (19.1%) cases had hemorrhagic cystitis, 2 (1.4%) cases experienced hepatic portal vein occlusion, and 2 (1.4%) cases had graft dysfunction.
Subgroup analysis of different post-transplant complications revealed statistically significant differences in the costs between patients experienced ≥3 types of complications and those with <3. Similar results were observed in patients reported complication severity > grade 2 and those ≤grade 2. Complications were graded based on NCI Common Terminology Criteria for Adverse Events (CTCAE, version 4.03; Supplementary material) grading scale (14) and the Mount Sinai Acute GvHD International Consortium (MAGIC) grading system (Supplementary Figure 1) (15, 16). If the complication fell into inconsistent grade between the two grading scale, it was classified according to the higher level. The more types of complications experienced, and the more severe complications were, the higher the cost of HSCT (Table 3).
HSCT is an effective treatment for a variety of hematological and non-hematological diseases (9). The direct medical costs within 100 days after HSCT treatment in 142 Chinese children were analyzed for the first time. Moreover, the effects of age, gender, transplantation types, and post-transplant complications on the costs were discussed in subgroups. The total cost was 250721.78 yuan (197019.16−315740.52), of which the drug costs were 126688.15 yuan (97940.92−167379.25), followed by medical service costs of 32781.25 yuan (28436.50–38891.00) and treatment expenses of 31714.40 yuan (25537.78−39720.45). In China, the per capita GDP in 2021 was 80,976 yuan, and the transplantation cost exceeded 3 times of the per capita GDP, which was a substantial financial burden for most families. Drug costs accounted for the highest proportion in HSCT cost, which was consistent with findings from other published literature (6, 13, 17). A study including 162 patients who received HSCT in India showed that age and gender did not affect the cost, which was confirmed by our study (6). Moreover, our study revealed that the transplantation types and post-transplant complications would cause differences in the total cost.
Hematopoietic stem cells mainly origin from bone marrow, peripheral blood, and umbilical cord blood. Based on the source of donors, HSCT can be categorized as autologous HSCT and allogeneic HSCT. Allogeneic HSCT can be further categorized as relative-related and non-relative related allogeneic HSCT based on the relationship between donors and recipients. According to compatibility of HLA between donors and recipients, relative-related allogeneic HSCT can be further categorized as haploid allogeneic HSCT and homozygous allogeneic HSCT (1). Limited studies were conducted regarding the costs of different transplantation types. Kanate et al. performed a retrospective study to evaluate the costs of double umbilical cord blood transplants (dUCBT) and haploid allogeneic HSCT for adult patients in the first 100 days post transplantation. Haploid allogeneic HSCT showed a significantly lower total costs compared with dUCBT (18). A study conducted in Nepal reported the costs were $5,200, $10,000, and $13,300 for autologous HSCT, homozygous allogeneic HSCT, and haploid allogeneic HSCT, respectively (19). Compared with allogeneic HSCT, autologous HSCT has fewer restrictions on age, fewer post-transplant complications, faster recovery and higher quality of life, and transplantation is not limited by donors (4, 20). Among the 142 patients included in this study, only 7 cases (4.9%) received autologous HSCT, and 135 cases (95.1%) received allogeneic HSCT. Compared with developed countries, the proportion of autologous HSCT was relatively low (4). The cost of autologous HSCT is lower than that of allogeneic HSCT (115722.98 yuan vs. 256043.99 yuan). In addition, the cost of HLA fully matched HSCT was lower than that of partially matched (213760.88 yuan vs. 294044.84 yuan).
The occurrence of post-transplant complications is one of the main reasons for the high cost of HSCT. A retrospective study of 1,831 adult patients who received HSCT in the United States showed that 70% patients experienced complications. The most common complications were mucositis, neutropenia with fever, and infections. The incidence of acute organ failure, acute GvHD and death was relatively low (10%), however, it greatly increased inpatient cost and length of hospital stay (21). In contrast, another study showed that acute GvHD within 2 months after transplantation did not increase the cost (22). In this study, 97.2% pediatric patients experienced post-transplant complications. The incidence of infection, oral mucositis, engraftment syndrome and acute GvHD was relatively high (90.8%, 61.3%, 48.6%, and 35.2%, respectively). Among them, 77 patients (54.2%) were complicated with ≥3 types of complications. The cost of HSCT in those with ≥3 complications increased by around 34% compared with those with <3 complications (286064.60 vs. 212893.25 yuan). The cost of HSCT with complication severity > grade 2 increased by about 19% compared with those ≤grade 2 (280061.58 vs. 235569.37 yuan), which indicated that the increase in the types and severity of complications led to an increase in the cost.
Some limitations were identified in the study. The sample size was relatively small with 142 patients. In addition, we focused on direct medical expenses during hospitalization. Outpatient visits and non-medical expenses, including transportation and accommodation expenses were not discussed. Moreover, the collection time period was 100 days after transplantation, which resulted in the lack of long-term follow-up data. Further research using larger and randomized controlled trials will be required to confirm the long-term cost. Studies showed the disease types, such as acute leukemia and aplastic anemia, and pre-transplant treatments would affect the cost (23). Hou et al. reported that low dose cyclophosphamide (CTX) combined with thoracic and abdominal radiotherapy improved the efficacy without increasing the incidence of HSCT complications. In contrast, large dose of CTX was related to the high incidence of GvHD. Adding anti-thymocyte globulin on the basis of the original regimen may reduce the incidence of GvHD (24). A retrospective study performed in pediatric HSCT patients revealed that the risk of pneumatosis intestinalis increased in patients receiving steroid therapy, patients with gastrointestinal GvHD, and patients relying on nasogastric tube feeds for >50% of total daily nutrition (25). Yang et al. reported that patients with mismatched blood type, CMV infection and elderly age had an increased risk of poor graft function post HSCT (26). Our study did not conduct the subgroup analyses based on these factors due to the limited sample size, which demanded further investigation.
Hematopoietic stem cell transplantation in children is an expensive health-care intervention. Allogeneic HSCT (especially those with HLA partial matched), and more types of post-transplant complications will result in an increase in the total cost. Selection of proper donor, adoption of appropriate immunotherapy post transplantation, preventing infection, and early transition to outpatient visits may be worthwhile to reduce the total cost.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by West China Second University Hospital Ethical Committee. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
MC and JN: study design and protocol preparation and manuscript drafting. YL: data collection. YH: data analysis. XY, JN, and MC: data interpretation. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.990181/full#supplementary-material
1. Ashfaq, K, Yahaya, I, Hyde, C, Andronis, L, Barton, P, Bayliss, S, et al. Clinical effectiveness and cost-effectiveness of stem cell transplantation in the management of acute leukaemia: a systematic review. Health Technol Assess. (2010) 14:1–141. doi: 10.3310/hta14540
3. Jiang, Q, Zhang, H, Yang, L, Luo, H, Miao, Q, and Deng, X. Haploid hematopoietic stem cell transplantation in the treatment of 23 leukemia cases. Chin J Tissue Engineer Res. (2016) 20:4218–25.
4. Cheng, T, Dong, F, Fu, R, Han, M, Hao, S, and Jiang, E. Standard for autologous hematopoietic stem cell transplantation. Chin Med Biotechnol. (2022) 17:75–93.
5. Yu, S, Ye, J, and Liu, J. Hematopoietic stem cell transplantation. China Med Pharmacy. (2011) 1:9–12.
6. Sharma, SK, Choudhary, D, Gupta, N, Dhamija, M, Khandelwal, V, Kharya, G, et al. Cost of hematopoietic stem cell transplantation in India. Med J Hematol Infect Dis. (2014) 6:e2014046. doi: 10.4084/mjhid.2014.046
7. Yin, G, Li, J, and Miu, K. Advances in research on implantation failure of hematopoietic stem cell transplantation. J Nanjing Med Univ Nat Sci. (2020) 40:141–6.
8. Saito, AM, Cutler, C, Zahrieh, D, Soiffer, R, Ho, VT, Alyea, EP, et al. Costs of allogeneic hematopoietic cell transplantation with high-dose regimens. Biol Blood Marrow Transplant. (2008) 14:197–207. doi: 10.1016/j.bbmt.2007.10.010
9. Madero, L, González, VM, Ramirez, M, Quintero, V, Benito, A, and Díaz, MA. Clinical and economic comparison of allogeneic peripheral blood progenitor cell and bone marrow transplantation for acute lymphoblastic leukemia in children. Bone Marrow Transplant. (2000) 26:269–73. doi: 10.1038/sj.bmt.1702516
10. Lin, YF, Lairson, DR, Chan, W, Du, XL, Leung, KS, Kennedy-Nasser, AA, et al. The costs and cost-effectiveness of allogeneic peripheral blood stem cell transplantation versus bone marrow transplantation in pediatric patients with acute leukemia. Biol Blood Marrow Transplant. (2010) 16:1272–81. doi: 10.1016/j.bbmt.2010.03.016
11. Barr, RD. Costs and consequences of stem cell transplantation in children. Pediatr Transplant. (2003) 7:7–11. doi: 10.1034/j.1399-3046.7.s3.1.x
12. Mayerhoff, L, Lehne, M, Hickstein, L, Salimullah, T, Prieur, S, Thomas, SK, et al. Cost associated with hematopoietic stem cell transplantation: a retrospective claims data analysis in Germany. J Compar Effective Res. (2019) 8:121–31. doi: 10.2217/cer-2018-0100
13. Cho, SK, McCombs, J, Punwani, N, and Lam, J. Complications and hospital costs during hematopoietic stem cell transplantation for non-Hodgkin lymphoma in the United States. Leuk Lymphoma. (2019) 60:2464–70. doi: 10.1080/10428194.2019.1581932
14. National Institutes of Health. Common terminology criteria for adverse events. (2010). Available at: https://evs.nci.nih.gov/ftp1/CTCAE/About.html (Accessed 13 December 2022).
15. Schoemans, HM, Lee, SJ, Ferrara, JL, Wolff, D, Levine, JE, Schultz, KR, et al. EBMT-NIH-CIBMTR task force position statement on standardized terminology & guidance for graft-versus-host disease assessment. Bone Marrow Transplant. (2018) 11:1401–15. doi: 10.1038/s41409-018-0204-7
16. Stem cell application group, Chinese Society of Hematology, Chinese Medical Association. Chinese consensus of allogeneic hematopoietic stem cell transplantation for hematological disease (III) -acute graft-versus-host disease. Zhonghua Xue Ye Xue Za Zhi. (2020) 7:529–36.
17. Jaime-Pérez, JC, Heredia-Salazar, AC, Cantú-Rodríguez, OG, Gutiérrez-Aguirre, H, Villarreal-Villarreal, CD, Mancías-Guerra, C, et al. Cost structure and clinical outcome of a stem cell transplantation program in a developing country: the experience in Northeast Mexico. Oncologist. (2015) 20:386–92. doi: 10.1634/theoncologist.2014-0218
18. Kanate, AS, Szabo, A, Raj, RV, Bower, K, Grulke, R, Shah, N, et al. Comparison of graft acquisition and early direct charges of haploidentical related donor transplantation versus umbilical cord blood transplantation. Biol Blood Marrow Transplant. (2019) 7:1456–64.
19. Poudyal, BS, Tuladhar, S, Neupane, S, Sapkota, S, Pandit, S, Shrestha, PR, et al. Hematopoietic stem cell transplantation in Nepal: international partnership, implementation steps, and clinical outcomes. Transplant Cell Ther. (2022) 28:268–75. doi: 10.1016/j.jtct.2022.02.011
20. Orsi, C, Bartolozzi, B, Messori, A, and Bosi, A. Event-free survival and cost-effectiveness in adult acute lymphoblastic leukaemia in first remission treated with allogeneic transplantation. Bone Marrow Transplant. (2007) 40:643–9. doi: 10.1038/sj.bmt.1705790
21. Svahn, BM, Remberger, M, Alvin, O, Karlsson, H, and Ringdén, O. Increased costs after allogeneic haematopoietic SCT are associated with major complications and re-transplantation. Bone Marrow Transplant. (2012) 47:706–15. doi: 10.1038/bmt.2011.162
22. Rivera-Franco, MM, Leon-Rodriguez, E, and Castro-Saldaña, HL. Costs of hematopoietic stem cell transplantation in a developing country. Int J Hematol. (2017) 106:573–80. doi: 10.1007/s12185-017-2278-1
23. Broder, MS, Quock, TP, Chang, E, Reddy, SR, Agarwal-Hashmi, R, Arai, S, et al. The cost of hematopoietic stem-cell transplantation in the United States. Am Health Drug Benefits. (2017) 10:366–74.
24. Hou, H, Yao, YH, Lu, J, Xiao, PF, Bian, XN, Liu, H, et al. Treatment of four cases of Fanconi anemia by allogeneic hematopoietic stem cell transplantation with low intensity conditional regimen. Zhonghua Xue Ye Xue Za Zhi. (2018) 3:231–5.
25. Frolova Gregory, P, Angus, J, Brothers, AW, Gray, AN, Skeen, K, Gooley, T, et al. Risk factors for development of pneumatosis intestinalis after Pediatric hematopoietic stem cell transplantation: a single-Center case-control study. Transplant Cell Ther. (2022) 11:785.e1–7.
Keywords: hematopoietic stem cell transplantation, cost analysis, children, China, developing country
Citation: Chen M, Liu Y, Yang X, Hong Y and Ni J (2023) Cost analysis of childhood hematopoietic stem cell transplantation in Sichuan, China. Front. Public Health. 11:990181. doi: 10.3389/fpubh.2023.990181
Edited by:
Hai Fang, Peking University, ChinaReviewed by:
Fei-Fei Tang, Peking University People's Hospital, ChinaCopyright © 2023 Chen, Liu, Yang, Hong and Ni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jiaqi Ni, amlhcWluaTAwN0AxNjMuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.