
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 09 March 2023
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.963464
 Vasco Ricoca Peixoto1*
Vasco Ricoca Peixoto1* André Vieira1Pedro Aguiar1Alexis Sentis2Carlos Carvalho3Daniel Rhys Thomas4Alexandre Abrantes1
André Vieira1Pedro Aguiar1Alexis Sentis2Carlos Carvalho3Daniel Rhys Thomas4Alexandre Abrantes1 Carla Nunes1
Carla Nunes1Introduction: In Portugal, COVID-19 laboratory notifications, clinical notifications (CNs), and epidemiological investigation questionnaires (EI) were electronically submitted by laboratories, clinicians, and public health professionals, respectively, to the Portuguese National Epidemiological Surveillance System (SINAVE), as mandated by law. We described CN and EI completeness in SINAVE to inform pandemic surveillance efforts.
Methods: We calculated the proportion of COVID-19 laboratory-notified cases without CN nor EI, and without EI by region and age group, in each month, from March 2020 to July 2021. We tested the correlation between those proportions and monthly case counts in two epidemic periods and used Poisson regression to identify factors associated with the outcomes.
Results: The analysis included 909,720 laboratory-notified cases. After October 2020, an increase in the number of COVID-19 cases was associated with a decrease in the submissions of CN and EI. By July 2021, 68.57% of cases had no associated CN nor EI, and 96.26% had no EI. Until January 2021, there was a positive correlation between monthly case counts and the monthly proportion of cases without CN nor EI and without EI, but not afterward. Cases aged 75 years or older had a lower proportion without CN nor EI (aRR: 0.842 CI95% 0.839–0.845). When compared to the Norte region, cases from Alentejo, Algarve, and Madeira had a lower probability of having no EI (aRR;0.659 CI 95%0.654–0.664; aRR 0.705 CI 95% 0.7–0.711; and aRR 0.363 CI 95% 0.354–0.373, respectively).
Discussion: After January 2021, CN and EI were submitted in a small proportion of laboratory-confirmed cases, varying by age and region. Facing the large number of COVID-19 cases, public health services may have adopted other registry strategies including new surveillance and management tools to respond to operational needs. This may have contributed to the abandonment of official CN and EI submission. Useful knowledge on the context of infection, symptom profile, and other knowledge gaps was no longer adequately supported by SINAVE. Regular evaluation of pandemic surveillance systems' completeness is necessary to inform surveillance improvements and procedures considering dynamic objectives, usefulness, acceptability, and simplicity.
Facing the large number of COVID-19 cases public health services may have adopted other registry strategies including new surveillance and management tools to respond to operational needs.
In Portugal, the established National Epidemiological Surveillance System (SINAVE) (1, 2) was updated to include COVID-19 laboratory notifications (LNs), submitted by the laboratories, clinical notifications (CNs), submitted by the clinicians or public health professionals in local-level public health units, and epidemic investigation (EI) questionnaires, submitted by the public health professionals or under their supervision, according to EU regulations and national law. These components are mandatory by law (2), which states that CN must be submitted within 24 h of diagnosis (2) and the EI and contact tracing must be initiated within 24 h of acknowledgment of the case by the public health services. LN, CN, and EI must be recorded in SINAVE digital platform (3). COVID-19 management teams at the local public health services had to verify LN, ensure the existence of a CN, submit an EI questionnaire in SINAVE, and initiate contact tracing. If a CN was not submitted by a clinician, public health services should guarantee their submission with the necessary information (3).
Clinical notifications include symptoms, comorbidities, outcomes, and basic epidemiological information. EI could only be registered if a CN was submitted. EI registries included both CN information and epidemiological information regarding the context of infection, epidemiological link, association with outbreaks, travel history, workplace, and activities; however, they did not allow for the recording of contact tracing lists and there was no national system for recording of contact tracing activities and results until the development of TRACE COVID-19 (4). This platform was created to support contact tracing and follow-up of contacts (including self-reporting of symptoms), case management at home, symptom recording, and follow-up by clinicians. This platform was regularly updated to include more functions throughout the pandemic. CN and EI records could be updated or corrected by Health Authorities at the local level (in public health units), regional level (Health Regional Administrations' Public Health Department), and national level (by the Portuguese Directorate-General of Health—DGS).
The importance of surveillance system's attributes evaluation, such as acceptability, simplicity, internal completeness, sensitivity, internal data validity, timeliness, usefulness, and others, resurfaced with COVID-19. The performance of surveillance systems considering these attributes is relevant because they determine the following: the quality of information, the behavior of data providers, and data quality. This will have an impact on research and routine surveillance to inform strategic decision-making.
We identified few reported COVID-19 surveillance system evaluations for COVID-19 (5–7) focusing on the attributes proposed by the European Centre for Disease Prevention and Control (ECDC) (8) and Centers for Disease Control and Prevention (CDC) (9). Some focus on laboratory surveillance but evaluate the internal completeness of demographic and epidemiological variables (10). We found no reports of internal completeness of submission of different components of surveillance (clinical notification, epidemiological investigation questionnaires/contact tracing) and their changes over time by age and region. The ECDC has issued guidance for surveillance system evaluation and data quality monitoring that stresses the importance of evaluating system internal completeness through time in face of changing pandemic context, guidelines, and evolving surveillance systems and tools (8).
In Portugal, after October 2020, there was a large increase in cases that made it necessary for public health services to adapt and quickly escalate capacity for collecting information and submitting clinical notifications (CNs), epidemiological investigation (EI) questionnaires in SINAVE, and for contact tracing.
During this high-incidence period, many healthcare workers and professionals from other sectors, including military personnel, were mobilized to aid in epidemiological investigation activities and contact tracing.
The changes in procedures and demand in different pandemic phases, the different strategies to cope with increased demand in different regions, and the emergence of parallel contact tracing tools that worked as concurrent surveillance systems with operational tools for COVID-19, triggered the importance of evaluating the completeness of SINAVE in an evolving epidemic context.
In this study, we aimed at describing the completeness of SINAVE regarding the submission of clinical notification and epidemiological investigation questionnaires and to understand the associated factors to inform future evaluation needs and potential risks in pandemic surveillance.
We used a database including all COVID-19 laboratory-confirmed cases in Portugal from 3 March 2020 until 16 July 2021. This database is compiled by the Portuguese Directorate General of Health (DGS) and includes all first positive laboratory notifications for each patient. It also contains information related to CN and EI questionnaires for each LN if they were submitted. EI questionnaires can only be recorded and submitted if a clinical notification is previously submitted.
We described the proportion of cases without CN nor EI and without EI overall (regardless of CN) in time, place, and person. We identified the factors associated with these outcomes in multivariable analysis using Poisson regression and presented adjusted relative risks, 95% confidence intervals, and p-value.
Finally, we calculated the Pearson correlation coefficient and respective p-value between the number of cases in each month and the proportion of cases with EI questionnaires by region in two different periods (before and after January 2021, the largest peak of hospitalizations by COVID-19) and presented coefficient variation from one period to another.
The analyzed outcomes were as follows: laboratory-confirmed cases without CN nor EI; laboratory-confirmed cases without EI overall (regardless of submission of clinical notification).
We described both the outcomes by sex, age, and health region in each month. Age was categorized into four groups (<25; 25–49; 50–74; ≥75). Region was categorized according to the county of occurrence and, when not available, the county of residence was used.
We calculated the proportion of cases for each outcome in the different health regions and plotted the monthly proportion of LN without CN nor EI and without EI overall including the number of cases in each month by region for visual comparison of trends in completeness and case numbers. We calculated the proportion of each outcome by month for different age groups.
We conducted univariable and multivariable analyses for both outcomes for each category of the associated factors and calculated prevalence by category and adjusted relative risks (aRRs), 95% confidence intervals (95%CIs), and respective p-values.
Statistical analysis was conducted in Stata (version 14, StataCorp, College Station, Texas, US). All analyses used 95% CI and considered a p < 0.05 as statistically significant.
All positive 909,720 laboratory notifications (LNs) between 3 March 2020 and 16 July 2021 were included in the analysis. Of those, 486,451 (53.47%) had no CN nor EI and 762,512 (83.82%) had no EI overall.
We observed that, with a rise in cases starting in October 2020, in most regions, there was a large increase in the proportion of cases with no CN nor EI and without EI overall (Figure 1).
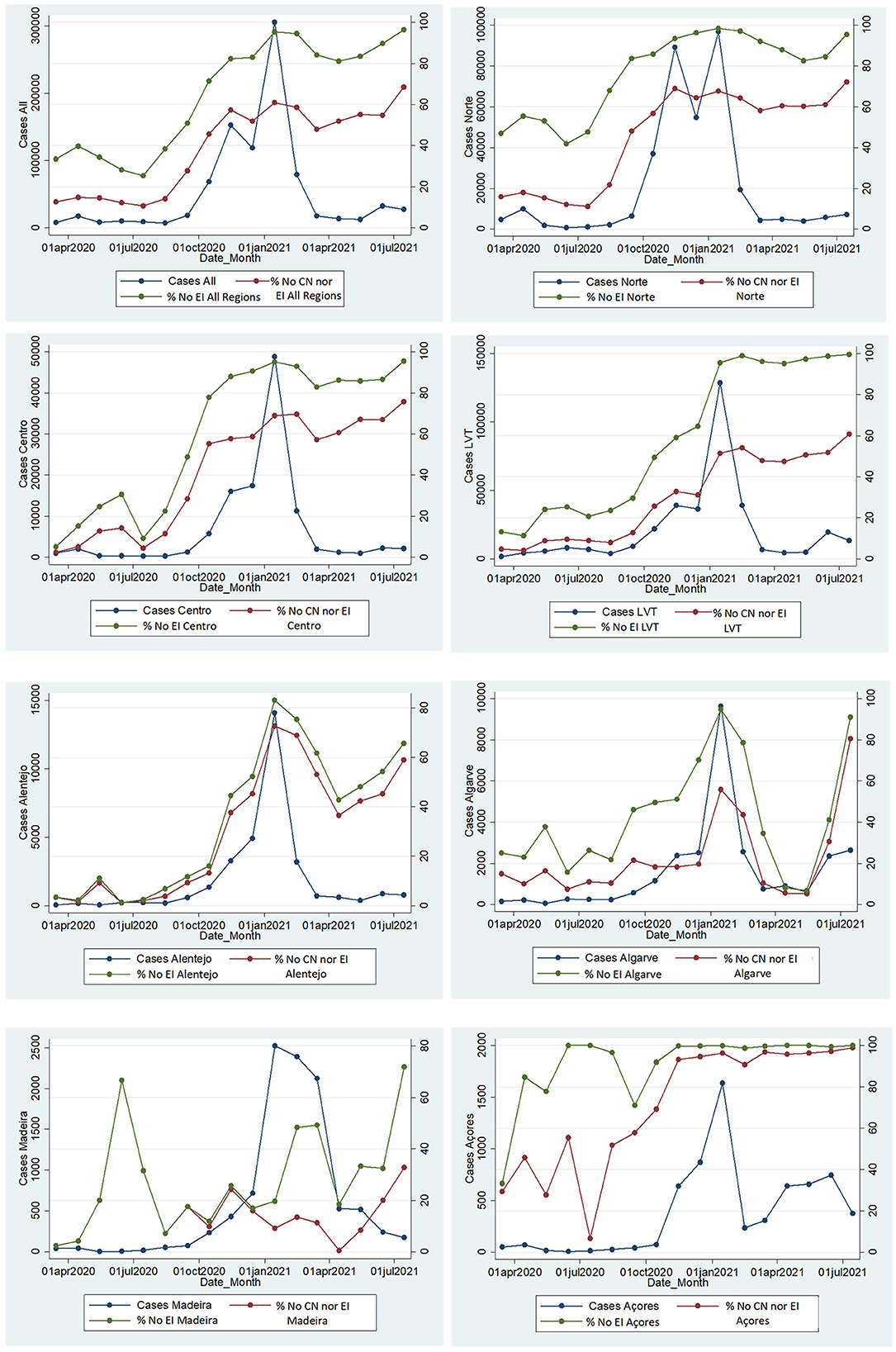
Figure 1. Monthly laboratory-confirmed cases and proportion of cases without clinical notification or epidemic investigation questionnaire submitted (No CN nor EI), and proportion of cases without EI questionnaires overall (No EI) by month in each Region and in Portugal, SINAVE, Portugal March 2020–July 2021. Cases: A total number of cases with a laboratory notification. No CN nor EI: cases without clinical notification and without EI questionnaire. No EI: cases without a submitted epidemic investigation questionnaire overall (regardless of clinical notification).
Even before the large increase in case numbers after October 2021, some regions had higher proportions of cases without EI such as North, LVT, and Center.
After stringent control measures in January to contain the spread, there has been a steep reduction in cases in all regions, with a slower reduction in Madeira. Even though in regions such as Algarve and Alentejo, there was a reduction in the proportion of cases without CN nor EI and without EI overall, in most regions, these proportions remained above 60 and 80%, respectively.
Age ≥75 had lower proportions of cases without clinical notification nor EI questionnaires and without EI overall. However, differences between age groups were larger for the proportions of cases without CN nor EI. The EI questionnaire was missing in high proportions of cases in all age groups, and even though there was a mild reduction in February, March, and April 2021, there was a rise in all age groups reaching levels close to 90% for those above 75 and close to 100% for other age groups in the last analyzed month.
Those above 75 had a lower prevalence of cases without CN nor EI (31.48%), approximately half of any other age group (Figure 2). We found large differences between regions. Lisbon Algarve and Madeira had a smaller proportion of cases without CN nor EI. Overall, after September 2021, there was an increase in cases without CN nor EI that remained high every month afterward (above 50% in most months until July 2021).
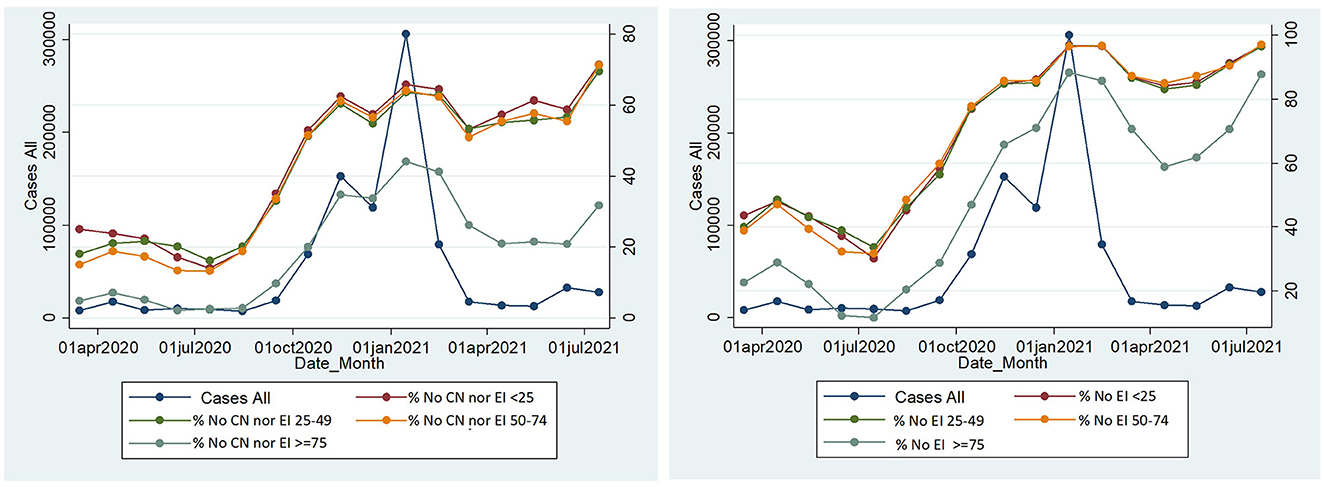
Figure 2. Monthly number of cases and proportion of cases without CN nor EI by age group (left) and Monthly number of cases and proportion of cases without EI overall (regardless of CN) in each month, by age group in Portugal, SINAVE, Portugal March 2020–July 2021. Cases: A total number of cases with a laboratory notification. No CN|EI: cases without clinical notification or epidemic investigation questionnaire submitted. No EI: cases without a submitted epidemic investigation questionnaire overall (regardless of clinical notification).
Cases without EI overall were 33.5% in March 2020 and remained below 40% until August 2020. In September, there was an increase in the proportion of cases without EI that remained above 80% after November 2020. Similar to the cases without CN nor EI those aged ≥ 75 had a smaller proportion of cases without EI overall (Tables 1, 2).
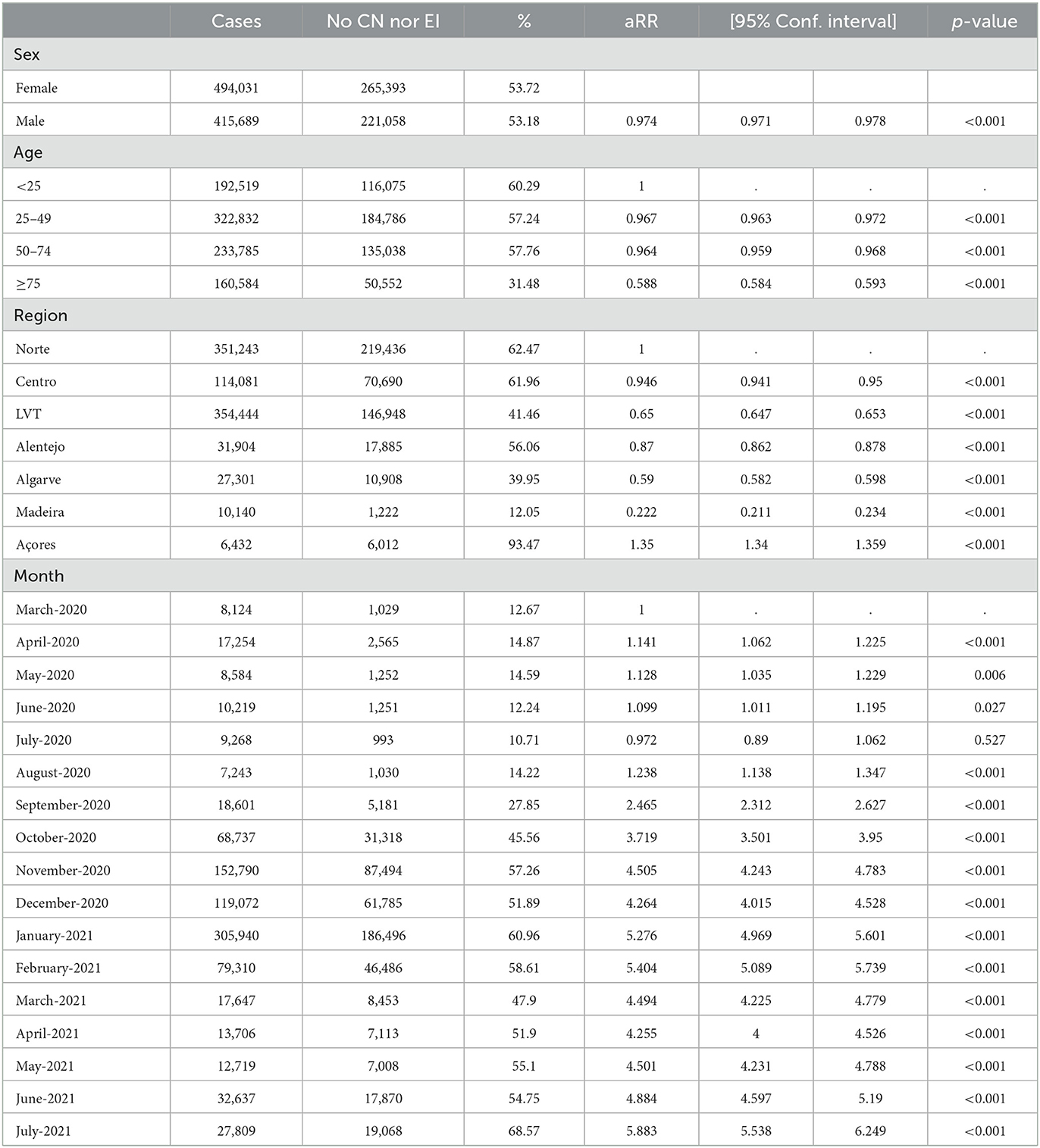
Table 1. Univariable and multivariable analyses for the outcome No CN nor EI, among laboratory notifications using Poisson regression in Portugal, SINAVE, Portugal March 2020–July 2021.
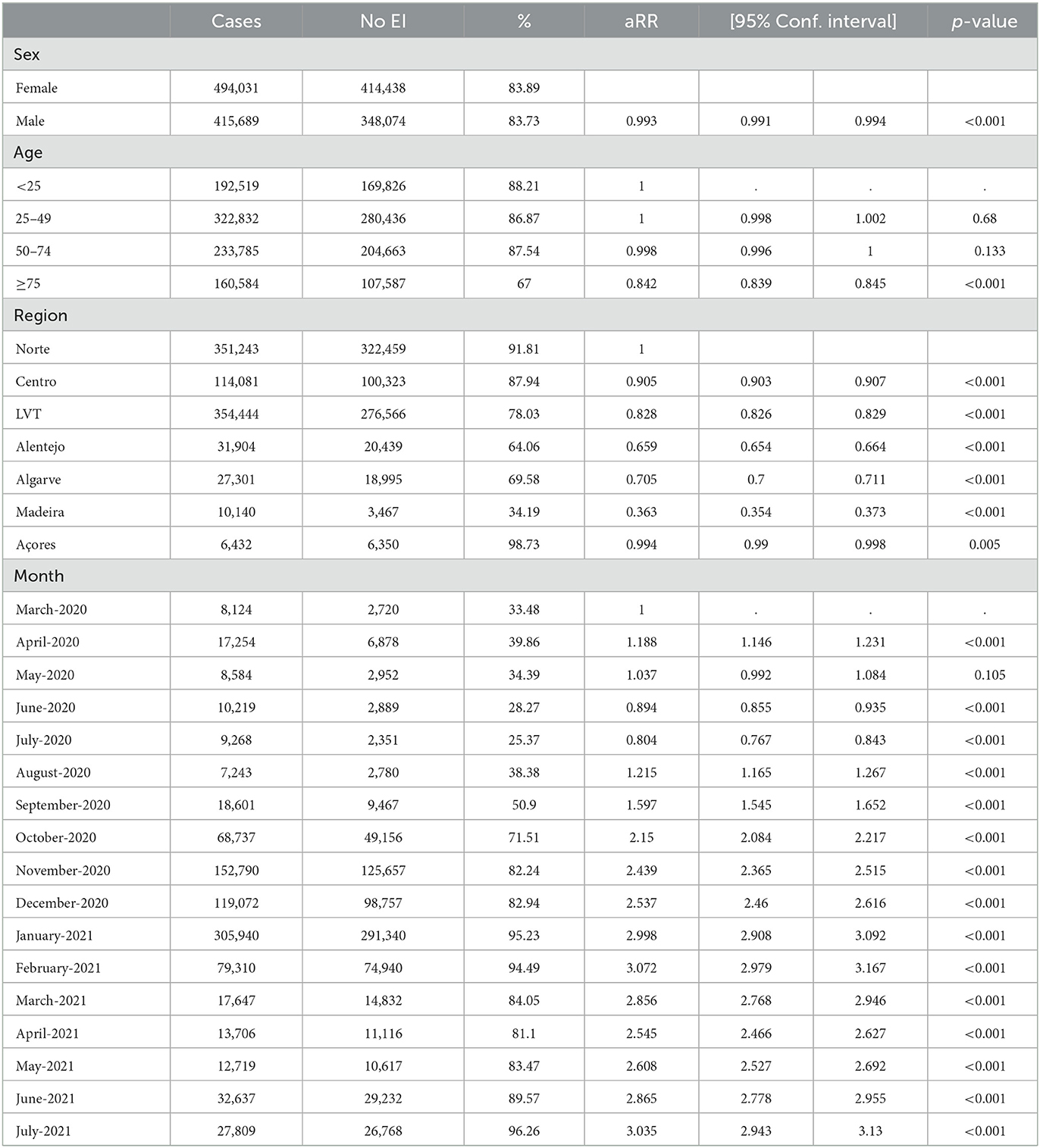
Table 2. Univariable and multivariable analyses for the outcome without epidemiological investigation questionnaires overall—with or without clinical notification questionnaires among laboratory notifications, using poisson regression in Portugal, SINAVE, Portugal March 2020–July 2021.
Alentejo, Algarve, and Madeira had the lowest proportions of cases without EI overall as they recovered completeness temporarily after the peak of the second epidemiological wave. Cases aged 75 years or older had a lower proportion without CN or EI (aRR: 0.842 CI95% 0.839–0.845). When compared to the Norte region, cases from Alentejo, Algarve, and Madeira had a lower probability of having no EI (aRR; 0.659 CI 95%0.654–0.664; aRR 0.705 CI 95% 0.7–0.711; and aRR 0.363 CI 95% 0.354–0.373, respectively).
Before January 2021, there was a strong and significant correlation between the number of cases in each month and the proportion of cases without CN nor EI and without EI overall. After January 2021, a reduction in cases was not followed by a reduction or increase in the proportion of cases for either outcome as the Pearson correlation coefficient was low in these periods and not statistically significant (Table 3).
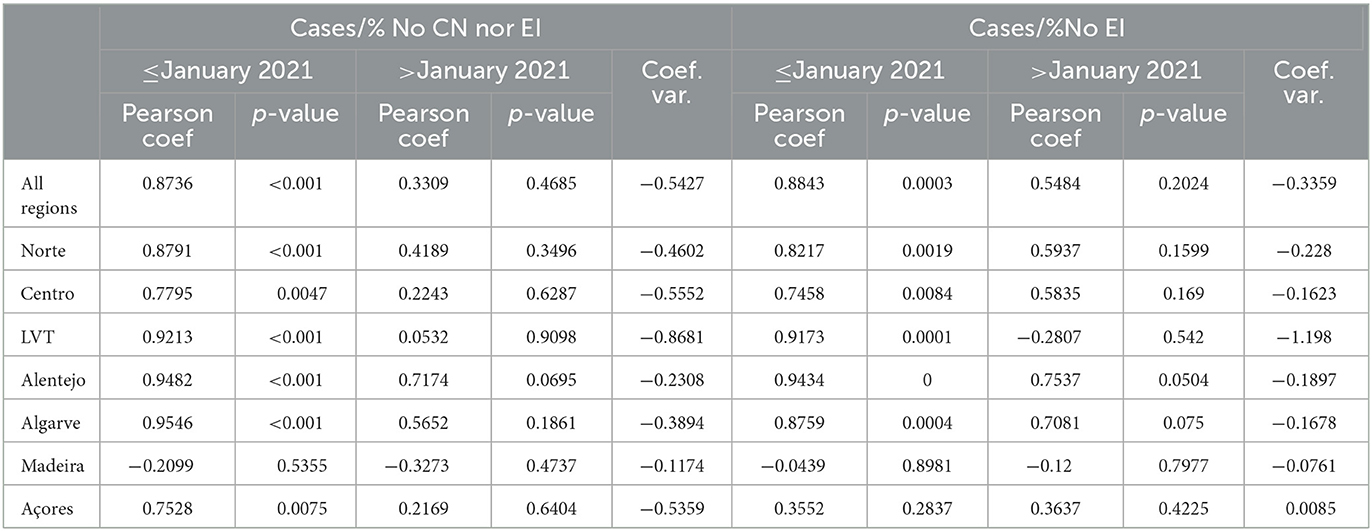
Table 3. Pearson correlation coefficient between the number of cases and proportion of cases without CN nor EI (left) and between cases and proportion of cases without EI questionnaires (right) by region in two different periods.
There has been a very large reduction in the completeness of SINAVE for clinical notification and epidemiological investigation questionnaire submission throughout the pandemic. This reduction started with increasing case numbers after September. We found relevant differences in the outcomes of interest in different age groups, regions, and time periods, which should generate hypothesis on its motifs and contribute to after-action reviews (11) of COVID-19 surveillance and lessons learned for surveillance systems in future pandemics.
There was a correlation between the incidence of cases and the proportion of cases without clinical notification nor EI and without EI questionnaires overall until January. After that, even though case incidence went down, in most regions and age groups, there was only a very mild reduction in these proportions implying changes in the practice of clinicians and public health units that may have prioritized other forms of epidemiological registries.
A lower proportion of cases without CN nor EI in those above 74 can be justified by a higher probability of clinical notification in settings of nursing homes and long-term care facilities because these tend to have closer surveillance by public health units in articulation with the physicians contracted by these institutions.
We can hypothesize that the differences in regions are attributable to different coping capacities with a surge of cases and different strategies adopted toward the use of SINAVE digital platforms for submitting clinical notifications and EI questionnaires during the second wave and after the reduction of cases that started in February 2021. With the rise in cases in October, contact tracing teams were reinforced with professionals from the health sector and others (military, municipal services, etc.), but they may have lacked access to the SINAVE platform. On the other hand, another COVID-19 information system for case management and contact tracing (TRACECOVID-19) had been implemented in April 2020 and acquired new features that generated operational tasks for primary care clinicians (who followed up with patients with COVID-19 by phone) and for public health units (contact tracing association of cases with contacts, contacts follow-up tasks, and automated SMS communication and SARS-CoV-2 test prescrition). Different regions and public health units may have used different platforms to register CN and EI information. All of this may have contributed to an abandonment of clinical notification and EI questionnaires in the SINAVE digital platform, the mandatory, legal framework surveillance system in Portugal.
Even in the first wave, it is apparent that many public health units struggled with submitting EI questionnaires in SINAVE. In the first five pandemic months, even though most laboratory-confirmed cases had a clinical notification, cases without EI questionnaires were above 25%. These values were above 40% in the North region, which implies that in this region, even at the beginning of the pandemic, there was a lower usage of the platform for CN and EI submissions.
The SINAVE digital platform did not allow for the recording of contacts generated by the cases while TRACE COVID-19 came to integrate this function after February 2021, which may have contributed to a shift in platform usage. SINAVE clinical notification included information on testing, symptoms, comorbidities, outcomes, and basic epidemiological context while the EI form included information on (work/institutional/educational context, epidemiological link, origin/context of infection, associated outbreak, travel history, and case classification). Completeness became more limited after October 2021 and especially after January 2020 for most regions and age groups. This has implications in terms of accurate symptom profiling in different epidemiological periods in face of pharmacological and non-pharmacological interventions, in terms of describing the origins and context of infection and unknown sources of infection, in understanding the risk factors over time for different severity outcomes, and in the ability of the surveillance system to measure the impact of changes in policy and of control strategies, including vaccine effectiveness for different outcomes, such as symptomatic disease.
After February 2021, only Algarve and Alentejo had a relevant reduction in the proportion of cases without CN nor EI and cases without EI overall. This may imply that after the surge in demand, these regions made an effort to maintain a high proportion of submitted clinical notifications and EI questionnaires in SINAVE, something that other regions did not do. However, in June and July, even these regions had relevant increases in the proportion of laboratory notifications without clinical notification and epidemiological investigation questionnaires.
These findings should be discussed considering the objectives of the surveillance system and the need for maximizing its usefulness, acceptability, and flexibility in face of evolving epidemiological needs and variations in demand during epidemic surges. The usefulness of specific variables must be evaluated as they should regularly generate useful knowledge for practice and policy. If they do not, they should neither increase the system's burden nor reduce its simplicity and acceptability. Flexibility is also important so that changes are implemented in a fast way to remove unnecessary tasks and variables and add those that become relevant while facilitating operational tasks for data providers at the local-level public health units and healthcare.
We must be aware that surveillance of a pandemic such as COVID-19 is a challenge due to uncertainty and knowledge gaps and due to different information and operational needs that must be anticipated, considering efficiency and acceptability.
Evaluation of surveillance system attributes with a focus on usefulness, while monitoring changes in completeness, timeliness, and data quality over time is of utmost importance. It allows anticipation of the need to change or integrate surveillance, to increase acceptability by maximizing efficiency, and to give feedback to the operational level while guaranteeing that the system is serving its objectives. Usefulness should be maximized in terms of operational management of cases and outbreaks, and in terms of generating quality data to inform decisions and allow applied epidemiological research beyond surveillance routine outputs to further understand the disease and inform policy and practice.
However, SINAVE-specific surveillance and research objectives for COVID-19 have not been publicly and formally defined even though SINAVE legal and technical framework defines general objectives for all notifiable diseases (1).
These findings must raise awareness of the potential of pandemics to disrupt surveillance systems and induce changes in their use, with consequences in terms of the availability of centralized and complete data. We also raise awareness of the importance of frequent evaluation and monitoring of the performance of the surveillance systems considering objectives and usefulness, both operational (case and outbreak investigation and transmission control) and strategic (information for policy). Evaluation of various attributes of surveillance systems for COVID-19 and other pandemics must be promoted to inform and anticipate the necessary changes in surveillance systems architecture and procedures and maximize their value.
Other evaluations of surveillance systems for COVID-19 suggest that public health institutes should improve physicians' and public health units' participation in the system by improving access to data, providing support and feedback that is useful in daily work in the field and that evaluation of surveillance systems for COVID-19 should be conducted in a systematic way (5).
To our knowledge, few studies have analyzed the completeness of clinical and public health notification components of surveillance among all laboratory-confirmed cases in a country for COVID-19.
These findings have implications in terms of the cost-effectiveness of surveillance systems. Concrete public health action and policy were less robustly supported by SINAVE due to the low completeness of clinical notification and EI questionnaires. Other COVID-19 information systems such as TRACE-COVID-19 could be considered in terms of defining the future approach to COVID-19 surveillance in Portugal. Patients autonomous submission of relevat clinical and epidemiological information should be considered in different contexts.
Low completeness of surveillance systems and gaps in collected information weakens health policy and practice, understanding of transmission patterns, clinical presentation, and risk factors for infection and disease severity over time, and evaluation of the impact of control interventions (contact tracing, vaccination, and others).
Improvements to surveillance systems must be driven by public health objectives and should be evaluated rigorously to determine their effects and costs. These objectives need to be clear and fully described to evaluate whether the system remains fit for purpose over time.
For COVID-19 as well as future pandemic threats and other notifiable diseases in Portugal, it is important to advance toward one centralized, robust surveillance system that can gather all relevant data (linking different platforms and health registries (primary care, hospitals, vaccination registries, contact tracing platforms, and prescriptions) to maximize usefulness, simplicity, and acceptability, considering different objectives and stakeholders.
Routine monitoring of system performance and conduction of evaluations of the surveillance system is of utmost importance in pandemics. The surveillance system's attribute indicators should be closely monitored, reported, and discussed considering information needs and knowledge gaps in different pandemic periods. Pandemics have a large impact on health, society, and economy, and knowledge of surveillance systems functioning and attributes is critical to facilitate planning, propose changes, and interpret surveillance findings adequately (12).
The data analyzed in this study is subject to the following licenses/restrictions: DGS Portugal COVID-19 Surveillance SINAVE Dataset. It's been shared with the academia under a protocol during the COVID-19 pandemic. Requests to access these datasets should be directed to DGS, Portugal.
Ethical review and approval was not required for this study of routine, anonymized surveillance data, in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
VR: design, analysis, and writting of first draft. AV: reviews. PA: desing, analysis, and reviews. AA: design and reviews. DR, CC, AS, and CN: discussion and reviews. All authors contributed to the article and approved the submitted version.
The present publication was funded by Fundação Ciência e Tecnologia, IP national support through CHRC (UIDP/04923/2020).
AS was employed by company Epiconcept.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Assembleia, da República. Lei 81/2009, 2009-08-21—DRE—Institui Um Sistema de Vigilância Em Saúde Pública, Que Identifica Situações de Risco, Recolhe, Actualiza, Analisa e Divulga Os Dados Relativos a Doenças Transmissíveis e Outros Riscos Em Saúde Pública, Bem Como Prepara Planos de Contingência Face a Situações de Emergência Ou Tão Graves Como de Calamidade Pública. Assembleia da Républica. Available online at: https://dre.pt/pesquisa/-/search/488301/details/maximized?print_preview=print-preview (accessed February 15, 2019).
2. Ministério, da Saúde. Portaria 22/2016, 2016-02-10—DRE—Primeira Alteração à Portaria n.o 248/2013, de 5 de Agosto, Que Aprova o Regulamento de Notificação Obrigatória de Doenças Transmissíveis e Outros Riscos Em Saúde Pública. Available online at: https://dre.pt/home/-/dre/73535989/details/maximized?p_auth=G7lbFhw2 (accessed February 15, 2019).
3. DGS. Norma no 015/2020 de 24/07/2020 Atualizada a 19/02/2021 COVID-19: Rastreio de Contactos. Available online at: https://covid19.min-saude.pt/wp-content/uploads/2021/02/i027197.pdf (accessed September 23, 2021).
4. SNSS. Trace COVID-19. Available online at: https://www.spms.min-saude.pt/2020/07/trace-covid-19/ (accessed September 23, 2021).
5. Norwegian Institute of Public Health. Final Report From a One-Year Evaluation of Notifiable Diseases Surveillance During the COVID-19 Epidemic—NIPH. Available online at: https://www.fhi.no/en/publ/2021/Final-report-one-year-evaluation-notifiable-diseases-surveillance-during-COVID-19-epidemic/ (accessed September 21, 2021).
6. Tamiru A, Regassa B, Alemu T, Begna Z. The performance of COVID-19 surveillance system as timely containment strategy in Western Oromia, Ethiopia. BMC Public Health. (2021) 21:2297. doi: 10.1186/s12889-021-12380-6
7. Awekeya H, Dubik SD, Amegah K, Ashinyo A, Wuobar F, Kaitoo E, et al. An evaluation of COVID-19 surveillance system in New Juaben South Municipality of Ghana: a cross-sectional study. Pan Afr Med J. (2021) 40:206. doi: 10.11604/pamj.2021.40.206.30715
8. European Centre for Disease Prevention Control. Data Quality Monitoring and Surveillance System Evaluation—A Handbook of Methods and Applications. Stockholm: ECDC (2014). Available online at: https://ecdc.europa.eu/en/publications-data/data-quality-monitoring-and-surveillance-system-evaluation-handbook-methods-and (accessed July 24, 2019).
9. Centers for Disease Control Prevention. Updated Guidelines for Evaluating Public Health Surveillance Systems: Recommendations From the Guidelines Working Group. MMWR (2001) 50. Available online at: https://stacks.cdc.gov/view/cdc/13376 (accessed April 1, 2022).
10. Clare T, Twohig KA, O'Connell AM, Dabrera G. Timeliness and completeness of laboratory-based surveillance of COVID-19 cases in England. Public Health. (2021) 194:163–6. doi: 10.1016/j.puhe.2021.03.012
11. European Centre for Disease Prevention Control. Best Practice Recommendations for Conducting After-Action Reviews to Enhance Public Health Preparedness. Stockholm: ECDC (2018). Available online at: https://ecdc.europa.eu/en/publications-data/best-practices-framework-undertaking-after-action-review-aar (accessed September 23, 2021).
Keywords: COVID-19, completeness, surveillance attribute, epidemic surveillance, surveillance system evaluation, notifications
Citation: Ricoca Peixoto V, Vieira A, Aguiar P, Sentis A, Carvalho C, Rhys Thomas D, Abrantes A and Nunes C (2023) COVID-19 surveillance: Large decrease in clinical notifications and epidemiological investigation questionnaires for laboratory-confirmed cases after the 2nd epidemic wave, Portugal March 2020–July 2021. Front. Public Health 11:963464. doi: 10.3389/fpubh.2023.963464
Received: 07 June 2022; Accepted: 30 January 2023;
Published: 09 March 2023.
Edited by:
Reza Lashgari, Shahid Beheshti University, IranReviewed by:
Mengchun Gong, Southern Medical University, ChinaCopyright © 2023 Ricoca Peixoto, Vieira, Aguiar, Sentis, Carvalho, Rhys Thomas, Abrantes and Nunes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vasco Ricoca Peixoto, dnJmLnBlaXhvdG9AZW5zcC51bmwucHQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.