 Loys Lene da Costa Siqueira
Loys Lene da Costa Siqueira Karla de Melo Batista2
Karla de Melo Batista2
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 18 December 2023
Sec. Injury Prevention and Control
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1330451
Introduction: Intimate Partner Violence (IPV) is a significant public health issue, characterized by being a highly stressful experience for its victims. The relationship between IPV and stress creates a harmful cycle with broad health implications, affecting individuals and society at large. Despite its significance, there's a noticeable lack of research on this topic, especially regarding IPV throughout one's life and during the pandemic.
Objective: To verify the association between perceived stress and the history of intimate partner violence throughout life and during the COVID-19 pandemic.
Materials and methods: Analytical cross-sectional epidemiological study with a sample of 1,086 women. Sociodemographic information and violence history, assessed using the World Health Organization Violence Against Women (WHO VAW STUDY), along with perceived stress measured by the short version of the Perceived Stress Scale (PSS), were collected. The sampling process unfolded through multiple stages. For bivariate analyses, the t-test and ANOVA were performed, whereas for multivariate analyses simple and multiple linear regression were performed. The software Stata® version 15.1 and R® were used.
Results: Women who reported having suffered intimate partner violence throughout their lives had higher means of stress (18.49), with an average increase of 4 points without adjustments and 3.5 points after adjustments for sociodemographic variables. Similarly, during the COVID-19 pandemic (19.01), stress increased by an average of 3.3 points, which was reduced to 2.8 points after adjustments.
Conclusion: The results indicate an association between intimate partner violence and an increase in women's perceived stress, both throughout life and during the pandemic. The importance of preventive approaches, promoting gender equality and preventing IPV from the early stages of life is highlighted. In addition, they underscore the urgency of evidence-based interventions of a comprehensive nature to deal with this complex issue in a careful and effective manner. The cross-sectional nature of this study limits the inference of causality, and an additional limitation is acknowledged concerning information bias. This bias relates to the multifaceted issues surrounding the concept of violence, potentially influencing the accuracy of participants' information and complicating the measurement of violence.
Intimate Partner Violence (IPV) is one of the most frequent forms of abuse committed against women. It is also identified as an important global public health concern. This form of violence is characterized by harmful physical, sexual, and/or psychological behaviors, and may even involve economic abuse and control over the victim (1). The World Health Organization (WHO) findings indicate that around 1 in 3 (30%) of women worldwide have faced intimate partner violence during their lifetime. Furthermore, globally, intimate partners account for up to 38% of all homicides targeting women (2). Similarly, in Brazil, IPV is also a concern, with 23% of women being subjected to physical and/or sexual violence by an intimate partner throughout life (3). Additionally, a study conducted in Vitória, Espírito Santo (ES), on IPV throughout life reported that 57.6% of women were victims of psychological violence, 39.3% of physical violence, and 18% of sexual violence (4).
We should also consider the scenario of the Corona Virus Disease 2019 (COVID-19) pandemic, which began in 2020. As pointed out in the literature, during this period, violence against women increased, largely due to the necessary control measures, such as social isolation, which significantly impacted women (5). Thus, violence against women remains a latent threat to both public health and women's health and wellbeing during times of crisis. The threat of violence faced by women and their children in emergency situations, such as the COVID-19 pandemic, cannot in any way be underestimated (6).
Considering this, note that IPV has wide-ranging negative consequences affecting physical, sexual/reproductive, mental, and behavioral health (1), and representing a highly stressful experience for its victims (7). Stress is an inevitable consequence of this experience for women (8), and it can persist or worsen even after the relationship ends (9). Stress refers to the adaptive biological and psychological changes that occur in response to external demands (10). Although the literature highlights short-term stress as positive and adaptive, increasing performance and improving immune function (11), in contrast, the long-term stress response is related to dysregulation of the immune system (12).
Chronic and unstoppable stress can result in damage to physical and mental health, such as anxiety disorders, depression, cardiovascular diseases, obesity, metabolic syndrome, type 2 diabetes mellitus, atherosclerosis, neurovascular degenerative disease, osteopenia, osteoporosis, and insomnia (13). Note that the theory of stress, coping, and adaptation of Lazarus et al. (14), presents stress as the consequence of perception of individuals that the demands are superior to their ability to manage them. The stress related to IPV is unique, especially due to the so-called cycle of violence that occurs in these experiences (7). Stress perception is a widely used measure to interpret or evaluate the psychological component in the response to stressors (15), including IPV (7).
Understanding stress in the most diverse sociodemographic, cultural, and social groups contributes to preventing adversities directly related to it and to other broad health problems in the world. Thus, investigating the way people perceive stressful situations in their lives is essential for computing psychological stress in health and disease around the world (16). Also, few studies, especially in Brazil, address the relationship between stress and IPV. Therefore, this cross-sectional epidemiological study, considering sociodemographic information, aimed to verify the association between perceived stress and the history of intimate partner violence throughout life and during the COVID-19 pandemic. We screened for a history of violence using the World Health Organization Violence Against Women (WHO VAW STUDY), and the short version of the Perceived Stress Scale (PSS) was employed to assess perceived stress.
We recognize that the biology of stress is not merely an “emergency system” but rather a continuous system in which the body and the brain adjust to our routine experiences, regardless of whether we perceive them as stressful or not. These experiences encompass our adherence/lack of adherence to our circadian cycle, whether we are introverted or extroverted, and if we live in a noisy and insecure environment or have access to nature and sources of peace and tranquility (17, 18).
In common terms, “good stress” refers to short-duration experiences controlled by the individual, generating positive feelings and a sense of accomplishment. On the other hand, “bad stress” or simply “being stressed” is the opposite, associated with experiences beyond the individual's control, often prolonged, recurring, emotionally draining, and physically exhausting or dangerous (19). This type of chronic and uncontrollable stress is not only negative but can become toxic, resulting in prolonged physical and mental health damage (17, 18). It is observed, therefore, that stress arises from the interaction of the individual with the environment, representing a globally significant health issue (20).
The health consequences of exposure to IPV are vast. The hypothetical pathways through which intimate partner violence leads to distinct forms of morbidity and mortality include the direct route of violence resulting in injuries and death (21). Acute or immediate physical injuries, such as bruises, abrasions, lacerations, punctures, burns, and bites, as well as fractures and broken bones or teeth, are highlighted. Furthermore, there are more severe injuries with the potential to lead to disabilities, involving body parts such as the head, eyes, ears, chest, and abdomen, and long-term health problems, frail health status, and death, as related to Acquired Immunodeficiency Syndrome (AIDS) or feminicide (22).
Beyond the direct pathway, there is a more indirect route mediated by stress responses. Complex biological mechanisms connect exposure to violence to different adverse health outcomes through neural, neuroendocrine, and immune responses. Brain regions such as the hippocampus, amygdala, and prefrontal cortex undergo structural changes that have implications for mental health and cognitive performance. These alterations can result in mental disorders, somatoform disorders, or chronic pathologies, as well as other physical conditions (21). As mentioned earlier, stress is an inevitable consequence of IPV in women (8).
However, there is a shortage of studies on the relationship between the perception of stress and exposure to IPV, especially in the Brazilian context.
According to Lazarus et al.'s (14) theory of stress, coping, and adaptation, stress is a consequence of individual perception, considering subjectivity. This cognitive theory is grounded in evaluation, where the personal meaning (primary appraisal) of an event (stress) for the individual is assessed. Coping options are then considered, including the use of social support. Based on these assessments, the event is categorized as harm, threat, or challenge. Coping can be problem-focused or emotion-focused, and the outcome of this event can be favorable or unfavorable, resulting in positive emotion or distress, respectively (14, 23, 24).
It is inevitable to consider that there are various human experiences that can lead to stress, encompassing a wide variety of aspects and situations (25). However, stress related to IPV is unique, especially due to the cyclical nature of violence, characterized by a period of progressive tension followed by an act of violence, then a relatively calm phase, and again followed by progressive tension (7, 26). Other elements of the IPV experience, such as intensity, duration, the victim's perception of their situation, coexistence with the aggressor, the presence of other concurrent stressors, and post-traumatic symptoms, should be considered (7).
Survivors of IPV describe it as a chronic, overwhelming, emotional, and personal experience, standing out as a unique stressor in their lives. They face various challenges and obstacles in dealing with violence and associated stress, including difficulties related to the partner, lack of resources and limited support, a history of abusive relationships and other experiences of abuse, reluctance to label IPV as abuse, barriers in disclosing the incident, influence of personal and religious beliefs, and the presence of children (27).
Longitudinal data collected from a sample of 815 married women in rural Pakistan, 12 months postpartum, revealed that 8.5% of women reported experiencing physical IPV, 25.7% psychological IPV, and 25.1% sexual IPV in the last year, with 42.6% experiencing some form of IPV. Exposure to any form of IPV in the previous year (vs. none) and greater severity of IPV were associated with 3.43 and 2.57 points, respectively, of an increase in perceived stress. Physical, psychological, and sexual IPV, along with their relative severities, were independently associated with increased perceived stress (28).
Another study conducted with young adults in South Africa, investigating the association between IPV, psychosocial, sexual health, and gender-specific perceived stress, revealed that 60% of the participants were women. Higher perceived stress was observed among young women compared to young men. Additionally, young women who were victims of IPV exhibited higher levels of perceived stress (29).
A multiple mediation analysis involving 7,392 women, examining the impact of IPV, depressive symptoms, alcohol dependence, and perceived stress on the risk of cardiovascular disease over 30 years among young adult women (aged 24 to 32 years), revealed that 15% had experienced some form of IPV in the last year. Participants had, on average, moderate levels of perceived stress, few depressive symptoms, and little or no alcohol dependence. However, those exposed to IPV in the last year had statistically/significantly higher levels of perceived stress, an increase in depressive symptoms, and a higher risk of cardiovascular disease over 30 years (30).
The exposure to acute and chronic psychological stress has been associated with pathological conditions for both men and women; however, women are more vulnerable to the detrimental effects of stress (31). As some studies suggest, there is a strong link between psychological stress and cardiovascular diseases, with women having a higher sensitivity to the deleterious effects of stress system imbalances and stress hormone signaling (31, 32). They exhibit increased vascular reactivity to glucocorticoids, which could explain their elevated risk for stress-induced ischemia (33).
Previous studies have shown a significant association between stress-motivated eating and obesity, with women having a higher Body Mass Index (BMI) after stressful events compared to men (34, 35).
The influence of chronic stress on the HPA (hypothalamic-pituitary-adrenal) and HPO (hypothalamic-pituitary-ovarian) axes can have significant effects on reproduction. Hyperactivity of the HPA axis in response to prolonged stress results in hormonal imbalances, impacting body composition and insulin resistance. These changes, in turn, affect the functioning of the HPO axis, crucial for the maturation of reproductive organs and reproductive capacity. Changes in hormonal relationships, reduced oocyte competence, and impacts on fetal development may occur as a result of these alterations. Children of stressed mothers may present low birth weight, elevated anxiety, and dysfunction of the HPA axis (36–38). These studies highlight the numerous impacts of stress, especially in women.
Research, such as that conducted by Sangeetha et al. (26), suggests that expanding the investigation of IPV based on the Walker Cycle of Violence is a promising path to strengthen efforts to improve the wellbeing of women and eliminate the cycle of violence that makes them victims. Moreover, it raises awareness among women to leave abusive relationships and live independently. Therefore, it is crucial to consider the bidirectionality of violence and stress (7), where one can potentiate the other.
Thus, the combination of IPV and stress reveals a harmful cycle with disastrous impacts on health at various levels, from individual to societal (7). Despite the relevance of this phenomenon, the scarcity of studies on the topic, especially considering IPV throughout life and during the pandemic, limits the development of effective interventions and public policies for women exposed to violence, particularly in the context of Espírito Santo, Brazil. This gap represents an urgency in contemporary public health, and our pioneering study seeks to contribute to broader goals, such as the United Nations Sustainable Development Goals (SDGs) by 2030, promoting good health, wellbeing (Goal 3), and gender equality (Goal 5) to ensure the rights and health of women (39).
To verify the association between perceived stress and the history of intimate partner violence throughout life and during the COVID-19 pandemic.
Is there a significant association between perceived stress and the history of intimate partner violence throughout life and during the COVID-19 pandemic?
This study is part of a broader study called “Violência contra a mulherem Vitória, Espírito Santo: um estudo de base populacional” (Violence against women in Vitória, Espírito Santo: a population-based study). This is an analytical cross-sectional epidemiological study carried out in the municipality of Vitória, Espírito Santo (ES), Brazil. This municipality had its population estimated for 2021 at 369,534 people, and the female population aged 18 years or older was about 155,673 (40). According to data from the last census, in 2010, the municipal Human Development Index was 0.845. The territory has 97.123 km2 (41).
Prior to participation, explicit informed consent was obtained from all participants. This process, involving a written Informed Consent Form (ICF), ensured that participants were well-informed about the study's objectives and nature. The protection of anonymity was emphasized throughout. Interviews were conducted in participants' homes, in a private location, with only the interviewee and interviewer present, lasting an average of 30 min.
Data collection occurred between January and May 2022 and was performed by a team of properly trained female interviewers. Data were collected using tablets and managed with the assistance of the Research Electronic Data Capture (REDCap) electronic data capture tool. Field supervisors provided support to the team. The pilot study took place in December 2021, the data collected in it were not included in the final sample of the research. Fieldwork began after data analysis of the pilot study.
The sample was composed of women aged 18 years or older, living in the municipality of Vitória, with and without a history of violence (psychological, sexual, and/or physical) by an intimate partner. This was defined as the partner or ex-partner and/or current boyfriends if the couple maintains sexual relations, regardless of whether it was a formal union or not. Women who did not have the capacity to understand or communicate due to intellectual or sensory deficit and who, therefore, were unable to respond to the research data collection instruments were excluded from the study.
The sampling process occurred through multiple stages. The primary sampling unit was the census tracts of the municipality of Vitória provided by the 2010 Census conducted by the Brazilian Institute of Geography and Statistics (IBGE). The total number of households in the urban area of Vitória, Espírito Santo, in 2010 (108,515) was divided by 100 (the number of sectors to be visited) to obtain the systematic skip (1,085), ensuring proportional probability to the number of households and women within each sector.
Subsequently, the list was ordered by socioeconomic level, and the number 513 (between 1 and 1,085) was randomly selected using the R statistical program and Stata® software version 15.1, corresponding to the number belonging to the first defined sector. The selection of the remaining sectors (99) proceeded by adding the systematic skip of the initial sector (184) and so on, successively until the end of the listing. Once the selection of census tracts was completed, the selection of households occurred randomly from the list available online by the IBGE. In each household, a list of eligible women, i.e., those meeting the study's inclusion criteria, was created, and one woman was then randomly chosen to respond to the interview.
For calculating the sample size of this study, the estimate of stress prevalence of 47.5% (42) was considered to maximize the sample, with a confidence level of 95%, acceptable error of 5%, plus 10% for losses and 30% for confounding factors, reaching a sample size of 1,100 women. For the present research, the sample consisted of 1,086 women.
The controlled variables were: sociodemographic data age/age group (18–29; 30–39; 40–49; 50–59; 60 or more), race/color (White; Black; Mixed race; Yellow, and Indigenous), years of schooling (0–8; 9–11; 12 or more), family income (1sttertile– poorer; 2ndtertile and 3rdtertile– richer), marital status (married; consensual union; single; separated or widowed), status of the house (own; rented or other), religion (no; yes), paid work (no; yes), government aid (no; yes), and number of residents in the household (living alone; 2; 3; 4; 5 or more people).
In this study, two outcomes were addressed: the levels of Perceived Stress among women who suffered IPV (psychological, sexual, and/or physical) throughout life (yes/no) and the levels of stress among women who suffered IPV during the COVID-19 pandemic (yes/no), that is, in the last 24 months prior to the research, which included the period of occurrence of the two waves of COVID-19 in Brazil (2020/2021) (43).
Sociodemographic information was collected using a questionnaire that contained details specified in the independent variables. To screen for violence, the World Health Organization Violence Against Women (WHO VAW STUDY) (44) instrument was applied, translated and validated in Brazil, consisting of 13 questions, considering it present when the woman answered yes to one of the items for each type of VAW (psychological, sexual, or physical). To evaluate the Perceived Stress the short version of the Perceived Stress Scale (PSS) (15) was used, to evaluate the perceived stress regarding life experiences in the last month. The PSS is a Likert-type scale and has 10 questions with answer options ranging from zero to four (0 = never; 1 = almost never; 2 = sometimes; 3 = fairly often, and 4 = very often) for questions with negative connotations. On the other hand, questions with positive connotations have inverted scores (0 = 4, 1 = 3, 2 = 2, 3 = 1, and 4 = 0). The total of the scale is the sum of the scores of these 10 questions, and the score can range from 0 to 40. The scale, in Brazil, was translated and validated by Luft et al. (45) and its results are described in mean and standard deviation, a higher score indicates greater stress.
The descriptive analyses of sample characterization were expressed in absolute and relative frequencies and their respective confidence intervals (95%CI) for categorical variables. The mean was also used as a measure of central tendency for variables with normal distribution plus their respective standard deviation. For the bivariate analyses, the following tests were used: t-test for means when we had independent variables in dichotomous form and analysis of variance (ANOVA) to verify the association and present the means by categories. The significance level was 5%. In the multivariate analysis, simple and multiple linear regression was used, with the betas (β) expressed in the tables. A significance level of 20% was used for entering the multivariable model and a significance level of 5% for remaining in the final model.
Figure 1 shows the perceptions of stress, in the last month, of women who suffered violence (sexual, psychological, and/or physical) by an intimate partner throughout their lives. According to the data presented, 29% of the women reported being sad due to unexpected events. Regarding the ability to control irritations in their lives, 29% responded negatively. When it comes to confidence in their ability to solve personal problems, 69% said they did not feel confident. Note that 20% reported feeling this confidence occasionally.
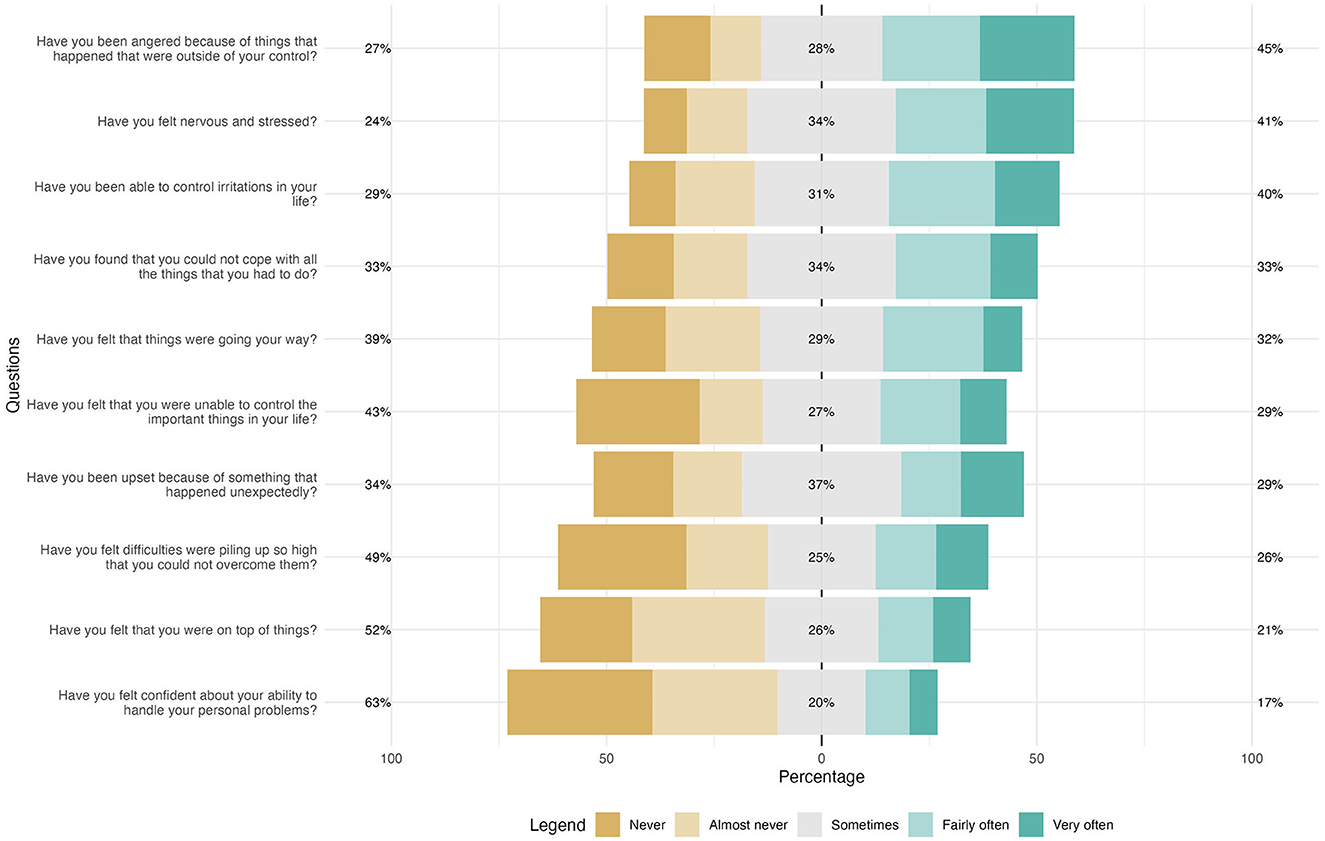
Figure 1. Perceived stress among women living in the municipality of Vitória who suffered intimate partner violence throughout their lives (N: 519). Vitória, ES, Brazil, 2022.
Perceived stress (Figure 2), in relation to life experiences in the last month, of women who suffered violence (sexual, psychological, and/or physical) by an intimate partner during the pandemic (last 24 months) revealed that 32% of women were sad due to unexpected events. Regarding the ability to manage irritations in their lives, 28% reported not being able to do so. In addition, 59% of women did not feel confident in their ability to solve personal problems, with 21% reporting feeling this confidence occasionally.
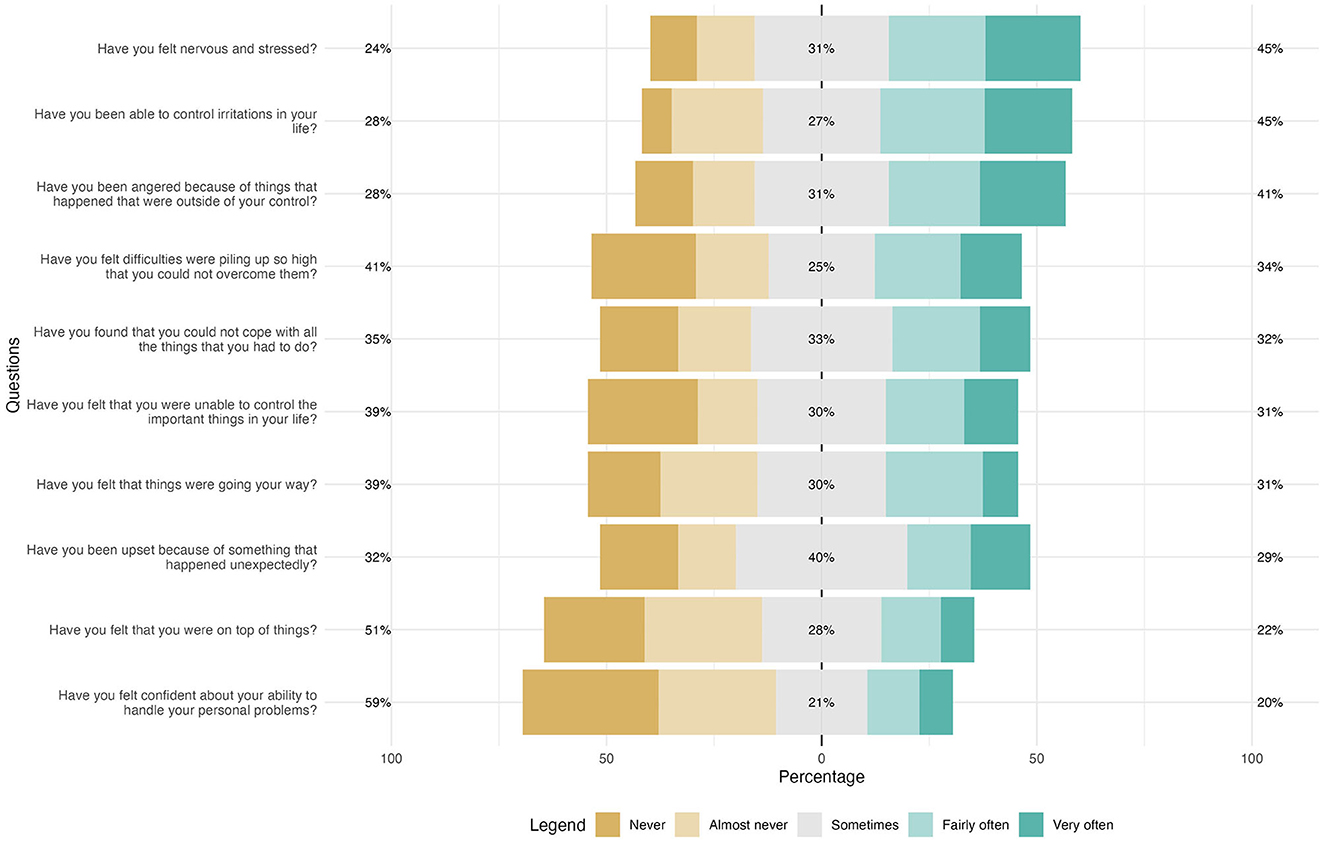
Figure 2. Perceived stress among women living in the city of Vitória who suffered intimate partner violence in the pandemic (last 24 months) (N: 231). Vitória, ES, Brazil, 2022.
Women who suffered intimate partner violence in their lives had higher mean stress (18.49) when compared with those who did not experience this condition (14.49). Analyzing the three types of violence separately (psychological/emotional, physical, and sexual), the experience of each of them was associated with higher averages of perceived stress. Regarding violence throughout life, physical violence had the highest average (19.26), followed by sexual violence (19.25), with the latter being very close, and psychological/emotional (18.60) (p < 0.001) (Table 1).
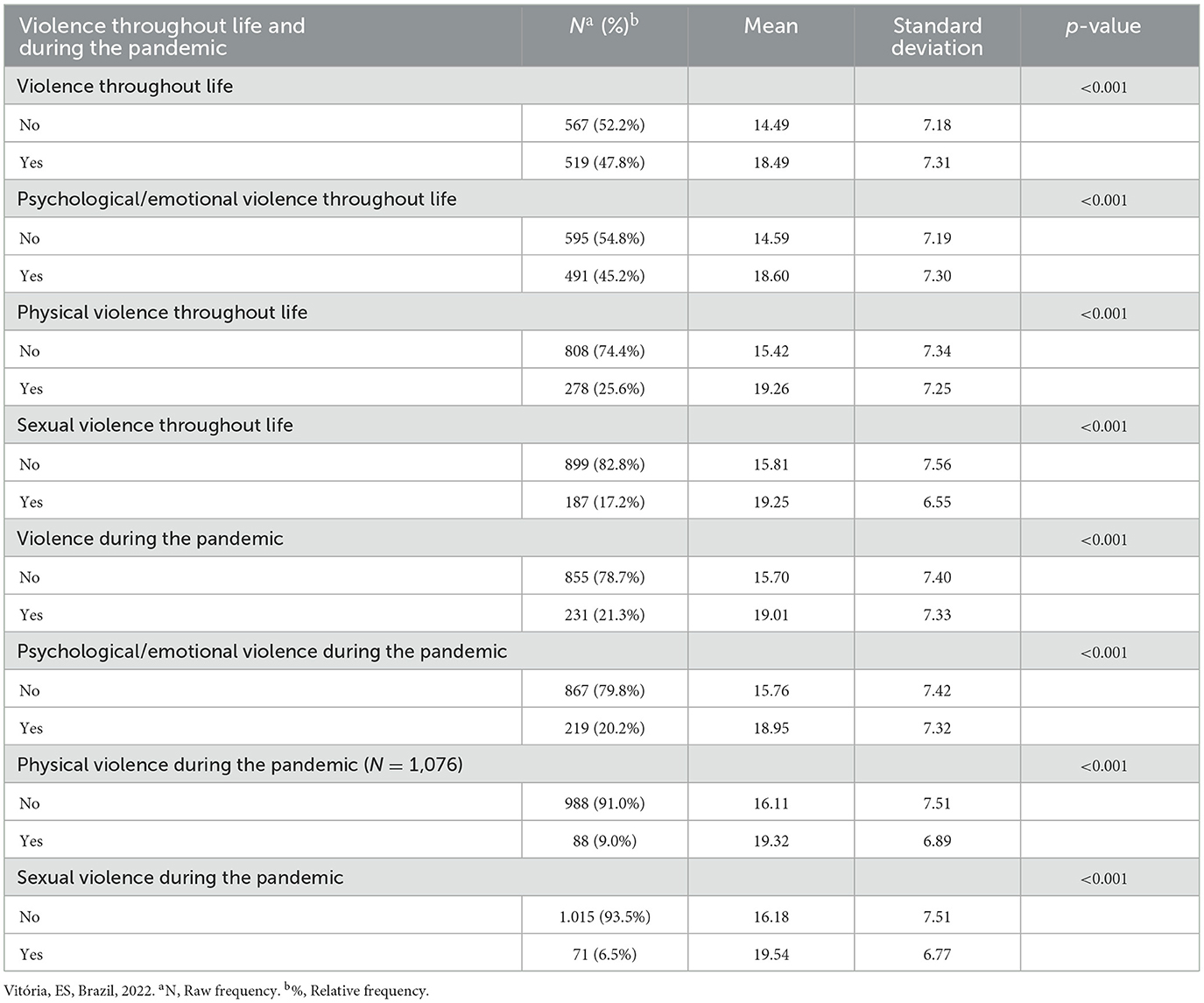
Table 1. Means and standard deviation of perceived stress according to violence throughout life and during the pandemic among women aged 18 years or older living in the municipality of Vitória (N: 1,086).
Similarly, experiencing violence practiced by a partner during the period of isolation due to the COVID-19 pandemic was associated with higher mean stress (19.01) compared with women who did not experience this (15.70). In the context of the pandemic, there was a shift from physical violence (19.32) to sexual violence (19.54), with the latter now having the highest average. The physical violence was followed immediately by psychological/emotional (18.95) (p < 0.001) (Table 1).
Table 2 shows that women who suffered violence by a partner in their lives presented, on average, 4 more points of stress than those who did not suffer violence, note that psychological/emotional violence stood out, also with an increase of 4 points, followed by physical violence with 3.8 and sexual violence with 3.4 (p < 0.001).

Table 2. Coefficients of simple regression of the relationship between the perceived stress among women living in the municipality of Vitória according to the occurrence of violence throughout life and during the pandemic (N = 1,086).
Similarly, victims during the pandemic recorded, on average, a 3.3 point increase in their stress levels compared with the group of non-victimized women. Sexual violence stood out in the significant increase in points in perceived stress, with 3.35 points, followed by physical violence with 3.2 and psychological/emotional violence, which also had an increase of 3.2 points (p < 0.001) (Table 2).
Table 3 shows the results obtained from the multiple linear regression analysis. Adjusting for sociodemographic variables, perceived stress remained associated with the occurrence of violence. Women who suffered violence from their intimate partner throughout their lives had, on average, 3.5 points more stress when compared with those who did not report this experience. Specifically, psychological/emotional violence stood out with the highest increase (β = 3.55), followed by physical violence (β = 3.49) and sexual violence (β = 3.08) (p < 0.001).
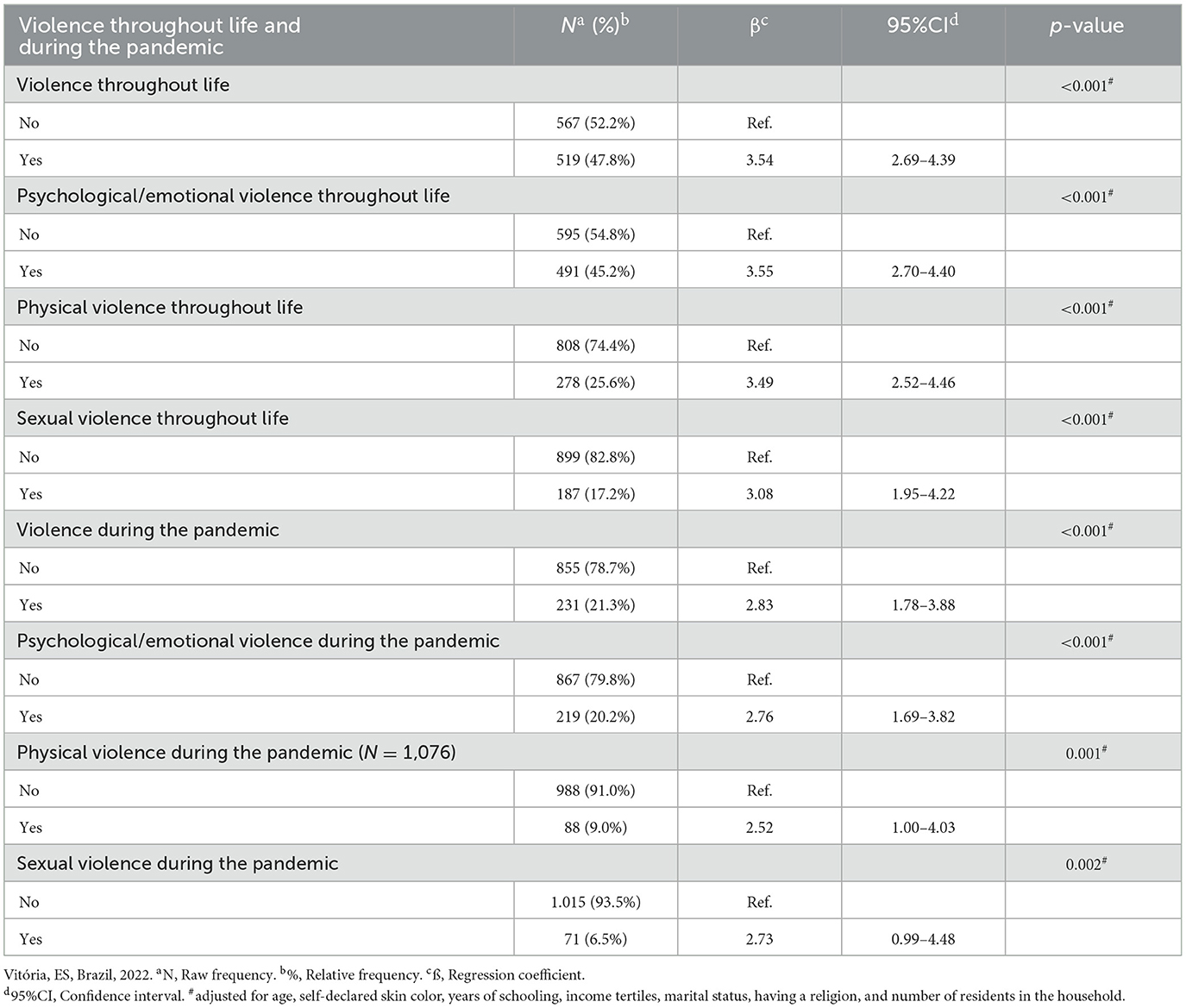
Table 3. Coefficients of the multiple regression of the relationship between the perceived stress among women living in the city of Vitória according to the occurrence of violence throughout life and during the pandemic (N = 1,086).
Similarly, victims during the pandemic showed, on average, 2.8 points more stress. Psychological/emotional violence also stood out in this context, with an increase of 2.76 points, followed by sexual violence with 2.7 and physical violence with 2.52 (p < 0.001) (Table 3).
Superior part of the form Superior part of the form.
The results of this study pointed to an association between experiencing IPV throughout life and higher levels of stress in the women interviewed. On average, the perceived stress increased by 4 points in women who were victims of IPV. Even after considering sociodemographic factors, this association persisted, with an average increase of 3.5 points. These findings are consistent with previous studies (28, 29) that evidenced the impact of IPV on perceived stress.
The IPV is an overwhelming stressor, both emotional and personal, leading the victim to be constantly in a state of alert. A study points out that dealing with IPV is compared to going into “survival mode,” and the experience has been described as an overflowing glass (27). These findings corroborate the view that IPV is a unique and chronic stressor (7), reinforcing the importance of addressing it in a differentiated way in the analysis of its impacts on the stress perceived by the victims.
A systematic review conducted by Yim and Kofman highlighted that IPV can influence health by both biological pathways, related to endocrine and immunological aspects, and psychological pathways, such as stress. According to the review's findings, some dysregulations in endocrine and immunoinflammatory markers are associated with IPV, as well as psychological stress, which emerges in new cases of IPV. This suggests that IPV may contribute to increased stress in victims, and at the same time, high levels of stress may also increase the likelihood of IPV occurring or persisting (7).
Findings during the COVID-19 pandemic showed an average increase of 3.3 points in perceived stress among women victims of IPV, and 2.8 points after adjusting for sociodemographic variables. These results corroborate a study conducted in the United States, which aimed to identify differences in the levels of resilience and perceived stress between groups. That study revealed that victims of IPV reported lower resilience and higher perceived stress. These findings provide empirical support for asserting that public health measures adopted to combat the spread of COVID-19 can have negative and unintended impacts, such as increasing the risk of experiencing IPV, and the associated mental health outcomes (46).
During the pandemic, the disintegration of social and protection networks, women's lower contact with family and friends, limited access to services, prolonged contact with family members, possible economic or job losses, school closures, and increased workload related to family and child-care were factors that significantly increased stress and risk of violence for women (6).
Since the beginning of the pandemic, the incidence of Violence Against Women (VAW) has worryingly increased, which has been described as the “shadow pandemic” (47). In times of pandemic, the increase in gender-based violence may not be adequately addressed and given the attention it deserves. Previous experiences with epidemics such as Ebola and Zika have shown that such crises tend to exacerbate existing inequalities, including those related to gender and economic status (48). The crisis has disproportionately impacted women, highlighting that the effects of crises are never gender-impartial, and COVID-19 is no exception. Women have also been particularly affected by the economic and social outcomes of the pandemic, resulting from pre-existing inequalities in terms of economic position and social status (49).
Regarding the specific types of violence, be it psychological/emotional, physical, or sexual, in our study, all were related to an increase in the victims' perceived stress, both throughout life and during the pandemic. The IPV, in general, has adverse impacts on women's physical and mental health. In addition, over time, exposure to different types and multiple episodes of abuse appears to result in a cumulative detrimental effect. Another important point highlighted is the tendency for the frequent coexistence of various types of violence: physical IPV is often accompanied by sexual IPV and is often associated with emotional abuse (1), which can intensify the onset of traumatic symptoms and other health issues in affected individuals (50).
Thus, recognizing IPV as a unique and complex stressor, differentiating it from other chronic stressors, is essential. Factors such as the cycle of violence, the intensity and duration of IPV, the history of other experiences of abuse, the co-occurrence of other stressors, the possible resulting trauma, and the maintenance of an intimate relationship with the perpetrator of the violence (7) should be considered in studying this phenomenon. They can also allow for a deeper understanding of the impacts of IPV on victims' perceived stress.
The results of this study reveal a significant association between IPV throughout life and during the COVID-19 pandemic and increased levels of stress perceived by women. This association underscores the importance of carefully considering policies and interventions in times of crisis, such as the pandemic, since solutions adopted for one problem may inadvertently generate other challenges. Recognizing that this relationship is not just limited to periods of crisis, but permeates women's lives in ongoing and damaging ways, is crucial. In this context, in addition to addressing the implications of IPV during crises such as the pandemic, we must recognize the long-term impact of this violence.
Combining efforts in prevention and intervention to address this complex issue more comprehensively and carefully is essential. Promoting gender equality and preventing IPV should be guidelines from the early stages of life, aiming at deconstructing gender stereotypes and promoting healthy relationships. Preventing IPV cannot be as a momentary response, but rather as an enduring commitment to building a society that respects, protects, and empowers all women.
The findings of this study also highlight the urgency of developing effective, evidence-based interventions to address IPV and mitigate its negative effects on women's health. Promoting safe environments and adequate support for IPV victims should be a priority to ensure women's wellbeing and protection. Building a just and egalitarian society requires continuous and collaborative efforts, where prevention and intervention go hand in hand to address IPV and its devastating consequences.
Our study in this location is the first to propose the investigation of the association between intimate partner violence (IPV) throughout a woman's life and during the COVID-19 pandemic, and the perceived stress in women. To attain significant goals, such as the SDGs objectives until 2030–specifically, promoting good health and wellbeing (Goal 3) and gender equality (Goal 5) to safeguard the rights and health of women–it is imperative to first recognize the existing problems.
The importance of a careful evaluation of the results of this study is emphasized due to its cross-sectional nature, which prevents the inference of causality. However, the study found an association between exposure to IPV and the outcome perceived stress, providing information that can serve as a basis for future investigations, as well as careful evaluation with the victims and subsequent interventions. In addition, another limitation of this research refers to the information bias, focusing on the multiple issues related to the concept of violence that can influence the accuracy of the information provided by the participants, which can lead to a difficulty in measuring violence; however, as a way of mitigating this problem, note that the interview was conducted in a private space and with only the interviewee and the interviewer. Despite their limitations, analytical cross-sectional epidemiological studies strongly contribute to identifying possible associations between variables.
This research contributes to advance knowledge on the relationship between IPV and perceived stress, as well as it represents a basis for further research in future studies. Research with a longitudinal design to investigate variations in stress perceptions over time and possible associations between IPV and women's health is advised.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The research was approved by the Research Ethics Committee of the Federal University of Espírito Santo (CEP/UFES), with opinion number 4.974.080, and was registered under the Certificate of Presentation for Ethical Appreciation (CAAE) number 41628820.6.0000.5060. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
LC: Conceptualization, Formal analysis, Investigation, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing. KM: Conceptualization, Supervision, Validation, Visualization, Writing – review & editing. FM: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Supervision, Validation, Visualization, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was supported by Fundação de Amparo à Pesquisa e Inovação do Espírito Santo (FAPES). Process 163/2021.
The authors would like to thank all the women who participated in this research.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. World Health Organization. Understanding and Addressing Violence Against Women: Intimate Partner Violence. World Health Organization and Pan American Health Organization (2012). Available online at: https://www.who.int/publications/i/item/WHO-RHR-12.36 (accessed November 15, 2022).
2. World Health Organization. Violence Against Women: Key Facts. Geneva: World Health Organization (2021). Available online at: https://www.who.int/news-room/fact-sheets/detail/violence-against-women (accessed November 13, 2023).
3. World Health Organization. Violence Against Women Prevalence Estimates, 2018: Global, Regional and National Prevalence Estimates for Intimate Partner Violence Against Women and Global and Regional Prevalence Estimates for Non-Partner Sexual Violence Against Women. Geneva: World Health Organization (2021). Available online at: https://apps.who.int/iris/handle/10665/341337 (accessed November 4, 2022).
4. Santos IB, dos Leite FMC, Amorim MHC, Maciel PMA, Gigante DP. Violência contra a mulher na vida: estudo entre usuárias da Atenção Primária. Ciên Saúde Colet. (2020) 25:1935–46. doi: 10.1590/1413-81232020255.19752018
5. Davies RL, Rice K, Rock AJ. The effects of COVID-19 social restrictions and subsequent informal support limitations on intimate partner violence: an opinion piece. Front Glob Womens Health. (2022) 3:829559. doi: 10.3389/fgwh.2022.829559
6. Organização Pan-American da Saúde. COVID-19 e a violência contra a mulher: o que o setor/sistema de saúde pode fazer (2020). Available online at: https://www.paho.org/pt/documents/covid-19-and-violence-against-women-what-health-sectorsystem-can-do (accessed November 07, 2022).
7. Yim IS, Kofman YB. The psychobiology of stress and intimate partner violence. Psychoneuroendocrinology. (2019) 105:9–24. doi: 10.1016/j.psyneuen.2018.08.017
8. Khodabakhshi-Koolaee A, Bagherian M, Rahmatizadeh M. Stress and coping strategies in women with and without intimate-partner violence experiences. J Client Centered Nurs Care. (2018) 4:29–36. doi: 10.32598/jccnc.4.1.29
9. Anderson D, Saunders D. Leaving an abusive partner: an empirical review of predictors, the process of leaving, and psychological well-being. Trauma Violence Abuse. (2003) 4:163–91. doi: 10.1177/1524838002250769
10. García-León MÁ, Pérez-Mármol JM, Gonzalez-Pérez R, Del Carmen García-Ríos M, Peralta-Ramírez MI. Relationship between resilience and stress: perceived stress, stressful life events, HPA axis response during a stressful task and hair cortisol. Physiol Behav. (2019) 202:87–93. doi: 10.1016/j.physbeh.2019.02.001
11. McEwen BS, Gianaros PJ. Stress- and allostasis-induced brain plasticity. Annu Rev Med. (2011) 62:431–45. doi: 10.1146/annurev-med-052209-100430
12. Dhabhar FS. Effects of stress on immune function: the good, the bad, and the beautiful. Immunol Res. (2014) 58:193–210. doi: 10.1007/s12026-014-8517-0
13. Chrousos GP. Stress and disorders of the stress system. Nat Rev Endocrinol. (2009) 5:374–81. doi: 10.1038/nrendo.2009.106
14. Lazarus RS, DeLongis A, Folkman S, Gruen R. Stress and adaptational outcomes: the problem confounded meseares. Am Psychol. (1985) 40:770–79. doi: 10.1037/0003-066X.40.7.770
15. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. (1983) 24:385. doi: 10.2307/2136404
16. Vallejo MA, Vallejo-Slocker L, Fernández-Abascal EG, Mañanes G. Determining factors for stress perception assessed with the perceived stress scale (PSS-4) in Spanish and other European samples. Front Psychol. (2018) 9:37. doi: 10.3389/fpsyg.2018.00037
17. McEwen BS. What is the confusion with cortisol? Chronic Stress. (2019) 3:247054701983364. doi: 10.1177/2470547019833647
18. McEwen BS, Akil H. Revisiting the stress concept: implications for affective disorders. J Neurosci. (2020) 40:12–21. doi: 10.1523/JNEUROSCI.0733-19.2019
19. McEwen BS. Physiology and neurobiology of stress and adaptation: central role of the brain. Physiol Rev. (2007) 87:873–904. doi: 10.1152/physrev.00041.2006
20. Ojha J, Bhandari T, Karki R. Job stress and its associated factors among working women in Pokhara Metropolitan, Nepal. J Sci Soc. (2020) 47:105. doi: 10.4103/jss.JSS_50_20
21. World Health Organization. Global and Regional Estimates of Violence Against Women: Prevalence and Health Effects of Intimate Partner Violence and Non-Partner Sexual Violence. Geneva: World Health Organization (2013). Available online at: https://www.who.int/publications/i/item/9789241564625 (accessed November 27, 2022).
22. World Health Organization. Understanding and Addressing Violence Against Women: Health Consequences. World Health Organization and Pan American Health Organization (2012). Available online at: https://www.who.int/publications/i/item/WHO-RHR-12.43 (accessed November 12, 2022).
23. Folkman S. The case for positive emotions in the stress process. Anxiety Stress Coping. (2008) 21:3–14. doi: 10.1080/10615800701740457
24. Lazarus RS, Folkman S. Stress Appraisal and Coping. New York, NY: Springer Pub. Co. (1984), p. 456.
25. Epel ES, Crosswell AD, Mayer SE, Prather AA, Slavich GM, Puterman E, et al. More than a feeling: a unified view of stress measurement for population science. Front Neuroendocrinol. (2018) 49:1. doi: 10.1016/j.yfrne.2018.03.001
26. Sangeetha J, Mohan S, Hariharasudan A, Nawaz N. Strategic analysis of intimate partner violence (IPV) and cycle of violence in the autobiographical text –when i hit you. Heliyon. (2022) 8:1–9. doi: 10.1016/j.heliyon.2022.e09734
27. Rizo CF. Intimate partner violence related stress and the coping experiences of survivors: “there's only so much a person can handle.” J Fam Viol. (2016) 31:581–93. doi: 10.1007/s10896-015-9787-6
28. Haight SC, Gallis JA, Chung EO, Baranov V, Bibi A, Frost A, et al. Stressful life events, intimate partner violence, and perceived stress in the postpartum period: longitudinal findings in rural Pakistan. Soc Psychiatry Psychiatr Epidemiol. (2022) 57:2193–205. doi: 10.1007/s00127-022-02354-3
29. Pakhomova TE, Dietrich JJ, Closson K, Smit J, Hornschuh S, Smith P, et al. Intimate partner violence, depression, and anxiety are associated with higher perceived stress among both young men and women in Soweto and Durban, South Africa. Front Reprod Health. (2021) 3:638116. doi: 10.3389/frph.2021.638116
30. Wright EN, Hanlon A, Lozano A, Teitelman AM. The impact of intimate partner violence, depressive symptoms, alcohol dependence, and perceived stress on 30-year cardiovascular disease risk among young adult women: a multiple mediation analysis. Prev Med. (2019) 121:47–54. doi: 10.1016/j.ypmed.2019.01.016
31. Mehta PK, Bess C, Elias-Smale S, Vaccarino V, Quyyumi A, Pepine CJ, et al. Gender in cardiovascular medicine: chest pain and coronary artery disease. Eur Heart J. (2019) 40:3819–26. doi: 10.1093/eurheartj/ehz784
32. Dhaibar HA, Cruz-Topete D. Predisposition of women to cardiovascular diseases: a side-effect of increased glucocorticoid signaling during the COVID-19 pandemic? Front Glob Womens Health. (2021) 2:606833. doi: 10.3389/fgwh.2021.606833
33. Lima BB, Hammadah M, Kim JH, Uphoff I, Shah A, Levantsevych O, et al. Association of transient endothelial dysfunction induced by mental stress with major adverse cardiovascular events in men and women with coronary artery disease. JAMA Cardiol. (2019) 4:988–96. doi: 10.1001/jamacardio.2019.3252
34. Laitinen J, Ek E, Sovio U. Stress-related eating and drinking behavior and body mass index and predictors of this behavior. Prev Med. (2002) 34:29–39. doi: 10.1006/pmed.2001.0948
35. Udo T, Grilo CM, Mckee SA. Gender differences in the impact of stressful life events on changes in body mass index. Prev Med. (2014) 69:49–53. doi: 10.1016/j.ypmed.2014.08.036
36. Joseph DN, Whirledge S. Stress and the HPA axis: balancing homeostasis and fertility. Int J Mol Sci. (2017) 18:2224. doi: 10.3390/ijms18102224
37. Richards JS, Pangas SA. The ovary: basic biology and clinical implications. J Clin Invest. (2010) 120:963–72. doi: 10.1172/JCI41350
38. Valsamakis G, Chrousos G, Mastorakos G. Stress, female reproduction and pregnancy. Psychoneuroendocrinology. (2019) 100:48–57. doi: 10.1016/j.psyneuen.2018.09.031
39. Nações Unidas Brasil. Objetivos de desenvolvimento sustentável. ONU Brasil (2022). Available online at: https://brasil.un.org/pt-br/sdgs (accessed November 14, 2023).
40. DATASUS. População residente: Espírito Santo (2021). Available online at: http://tabnet.datasus.gov.br/cgi/deftohtm.exe?ibge/cnv/popsvsbr.def (accessed November 19, 2023).
41. Instituto Brasileiro de Geografia e Estatística. Índice de desenvolvimento humano: BRASIL, Espírito Santo, Vitória. IBGE (2010). Available online at: https://cidades.ibge.gov.br/brasil/es/vitoria/pesquisa/37/30255?tipo=ranking (accessed February 17, 2023).
42. Souza ASR, Souza GFA, Souza GA, Cordeiro ALN, Praciano GAF, de Souza Alves AC, et al. Factors associated with stress, anxiety, and depression during social distancing in Brazil. Rev SaúdePública. (2021) 55:5. doi: 10.11606/s1518-8787.2021055003152
43. De Lima Osório F, Zuardi AW, Silveira ILM, de Souza Crippa JA, Hallak JEC, Lima KP, et al. Mental health trajectories of Brazilian health workers during two waves of the COVID-19 pandemic (2020–2021). Front Psychiatry. (2023) 14:1026429. doi: 10.3389/fpsyt.2023.1026429
44. Schraiber LB, Latorre MDRDO, França Jr I, Segri NJ, D'Oliveira AFPL. Validade do instrumento WHO VAW STUDY para estimar violência de gênero contra a mulher. Rev Saúde Pública. (2010) 44:658–66. doi: 10.1590/S0034-89102010000400009
45. Luft CDB, Sanches SDO, Mazo GZ, Andrade A. Versão brasileira da escala de estresse percebido: tradução e validação para idosos. Rev Saúde Pública. (2007) 41:606–15. doi: 10.1590/S0034-89102007000400015
46. Buttell F, Cannon CEB, Rose K, Ferreira RJ. COVID-19 and intimate partner violence: prevalence of resilience and perceived stress during a pandemic. Traumatology. (2021) 27:20–8. doi: 10.1037/trm0000296
47. United Nations Women. Mensuring the Shadow Pandemic: Violence Against Women During Covid-19 (2021). Available online at: https://data.unwomen.org/publications/vaw-rga (accessed December 06, 2022).
48. Thibaut F, Van Wijngaarden-Cremers PJM. Women's mental health in the time of Covid-19 pandemic. Front Glob Womens Health. (2020) 1:588372. doi: 10.3389/fgwh.2020.588372
49. United Nations Women and United Nations Development Programme. Government Responses to Covid-19: Lessons on Gender Equality for a World in Turmoil (2022). Available online at: https://www.unwomen.org/en/digital-library/publications/2022/06/government-responses-to-covid-19-lessons-on-gender-equality-for-a-world-in-turmoil (accessed November 28, 2022).
Keywords: violence against women, domestic violence, intimate partner violence, COVID-19, stress psychological, perceived stress
Citation: da Costa Siqueira LL, de Melo Batista K and Marabotti Costa Leite F (2023) Association between perceived stress and history of intimate partner violence throughout life and during the COVID-19 pandemic. Front. Public Health 11:1330451. doi: 10.3389/fpubh.2023.1330451
Received: 30 October 2023; Accepted: 27 November 2023;
Published: 18 December 2023.
Edited by:
A. Hariharasudan, Kalasalingam University, IndiaReviewed by:
S. Gnana Sanga Mithra, Vinayaka Missions Research Foundation (DU), IndiaCopyright © 2023 da Costa Siqueira, de Melo Batista and Marabotti Costa Leite. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Franciéle Marabotti Costa Leite, ZnJhbmNpZWxlbWFyYWJvdHRpQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.