
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 08 January 2024
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1327082
 Aina Huguet-Torres1,2
Aina Huguet-Torres1,2 Enrique Castro-Sánchez2,3,4*
Enrique Castro-Sánchez2,3,4* Laura Capitán-Moyano1,2
Laura Capitán-Moyano1,2 Cristian Sánchez-Rodríguez2,5
Cristian Sánchez-Rodríguez2,5 Miquel Bennasar-Veny1,2,6,7
Miquel Bennasar-Veny1,2,6,7 Aina M. Yáñez1,2,6
Aina M. Yáñez1,2,6Background: During the SARS-CoV-2 pandemic, nurses of primary health care has been an important role in Spain. Even so, the data obtained in the tracing have been scarcely used to investigate the possible mechanisms of transmission. Few studies focused on community transmission, evaluating the effectiveness of individual protective measures and exposure environment. The main aim of the study was to evaluate the association between individual protective measures and SARS-CoV-2 transmission in the community and to compare secondary attack rates in different exposure settings.
Methods: A case–control study from contact tracing of SARS-CoV-2 index patients. COVID-19 contact tracing was led by nurses at the COVID-19 Coordinating Centre in Majorca (Spain). During the systematic tracing, additional information for this study was collected from the index patient (social-demographic variables, symptoms, the number of close contacts). And also, the following variables from their close contacts: contact place, ventilation characteristics mask-wearing, type of mask, duration of contact, shortest distance, case-contact relationship, household members, and handwashing, the test result for SARS-CoV-2 diagnostic. Close contacts with a positive test for SARS-CoV-2 were classified as “cases” and those negative as “controls.”
Results: A total of 1,778 close contacts from 463 index patients were identified. No significant differences were observed between the sexes but between age groups. Overall Secondary Attack Rate (SAR) was 24.0% (95% CI: 22.0–26.0%), 36.9% (95% CI: 33.2–40.6%) in closed spaces without ventilation and 50.7% (95% CI: 45.6–55.8%) in exposure time > 24 h. A total of 49.2% of infections occurred among household members. Multivariate logistic regression analysis showed that open-air setting (OR 0.43, 95% CI: 0.27–0.71), exposure for less than 1 h (OR 0.19, 95% CI: 0.11–0.32), and wearing a mask (OR 0.49, 95% CI: 0.28–0.85) had a protective effect transmission of SARS-CoV-2 in the community.
Conclusion: Ventilation of the space, mask-wearing and shorter exposure time were associated with a lower risk of transmission in the community. The data obtained allowed an assessment of community transmission mechanisms and could have helped to improve and streamline tracing by identifying close contacts at higher risk.
The COVID-19 pandemic had an unprecedented impact on society, making it the pandemic with the greatest impact worldwide in recent times. SARS-CoV-2 shares multiple features with hitherto described coronaviruses, the secondary attack rate (SAR; the number of cases occurring within the incubation period following exposure to a primary case divided by the total susceptible persons (1)) of SARS-CoV-2 appears to be higher (26.3–39.3%, depending on the variant) (2) than infection by SARS-CoV (10.2%) (3) or MERS (4%) (2). The range of clinical signs and symptoms typically showcased by persons infected includes fever, cough, dyspnea, fatigue, and myalgias (4). Among the clinical symptoms reported in persons with coronavirus infection, the prevalence of coughing and its presumptive role in transmission dynamics have attracted attention (5). Although much of the evidence available refers to coughing and the projection of simulated aerosolized viral particles (5), a consensus on airborne transmission was not reached during the initial response to the pandemic (6).
Families and other close social and work contacts have been identified as important contributors towards the pandemic burden (7). Family members and relatives were the main transmission agents of SARS-CoV-2, regardless of whether they shared accommodation with the persons infected (8). However, whilst a systematic review exploring secondary attack rate in different exposure settings highlighted the higher attack rate at homes, social circles, and workplaces (9), most studies focused only on one environment of exposure, such as hospitals or health centers (10–15), households (16, 17), educational centers (18), or public transport (19). Few studies describe the transmission of SARS-CoV-2 related to settings where routine activities such as working, or practicing sports and exercising are carried out, and fewer consider environmental characteristics (ventilation) or factors related to the exposure to the infective agent (exposure time, distancing, etc.).
Wearing a facemask in public settings, maintaining social distance and hand washing are preventive measures and bundles of protective behaviors that had been used for SARS-COV-2 (16, 20–22), and other similar coronaviruses (23). Recent reviews concluded that the use of the face mask is effective in reducing the likelihood of transmission of respiratory pathogens that could include SARS-CoV-2, although most studies included were unrelated to this virus (16, 17). Consequently, we think that is relevant to investigate the effect of wearing a mask specifically in SARS-CoV-2 on the population. In terms of the optimal type of mask, a meta-analysis, found no benefit between different types of masks, with N95 and cloth masks obtaining similar results (17).
In addition to non-pharmacological interventions to address viral transmission, behavioral, social, and environmental factors have also proven vital in the pandemic (24). Contact tracing is an essential and widespread public health measure to mitigate the transmission of infectious diseases (25). During the COVID-19 pandemic, contact tracing was adopted by most countries (26) in addition to other preventive measures such as wearing masks, practicing physical and social distancing, and hand hygiene (27), and was found to be effective in limiting epidemic growth (28). In addition to the operational benefit for clinical and public health management, contact tracing generates a vast amount of data about transmission which could be useful to identify those individuals most at risk of infection (29). Close contact tracing of cases has been one of the main public health approaches to reduce transmission, hospital admissions, and mortality (30). Typically, contact tracing involves interviewing people who are infected to identify which other individuals might have been exposed to the virus, and isolation or quarantine of contact risk (31). Most frequently, the data generated during tracing activities are only used for operational and not research purposes (28).
We aimed to evaluate the association between individual protective measures in the population and SARS-CoV-2 transmission. Also, compare the secondary attack rate of COVID-19 across different settings, exposure, and characteristics.
An unmatched case–control study selecting the controls from the same population. COVID-19 contact tracing was led by nurses at the COVID-19 Coordinating Centre in Majorca (Balearic Islands, Spain). At the coordination center, all authorized diagnostic testing centers reported every diagnosed case there. Upon receiving this information, nurses contacted the positive patient. During this phone call, the infected patient’s health status was assessed, and close contact tracing was conducted. After concluding the call with the infected patient, close contacts were contacted to notify them of their situation, provide information about the required quarantine, and schedule diagnostic tests as necessary. During the systematic tracing, additional information for this study was collected from the index patient and their close contacts.
During the data collection period, the government of the Balearic Islands imposed mobility restrictions tailored to fluctuating thresholds of coronavirus cumulative incidence, thus allowing, or banning some social activities (32, 33) (both in Table 1). Also, the vaccination rate of the population in the age ranges of our sample was less than 50% (34). During data collection, Mallorca was between 2nd and 4th level of COVID-19 public health measures (“Control Situation” and “High Risk”) (35).
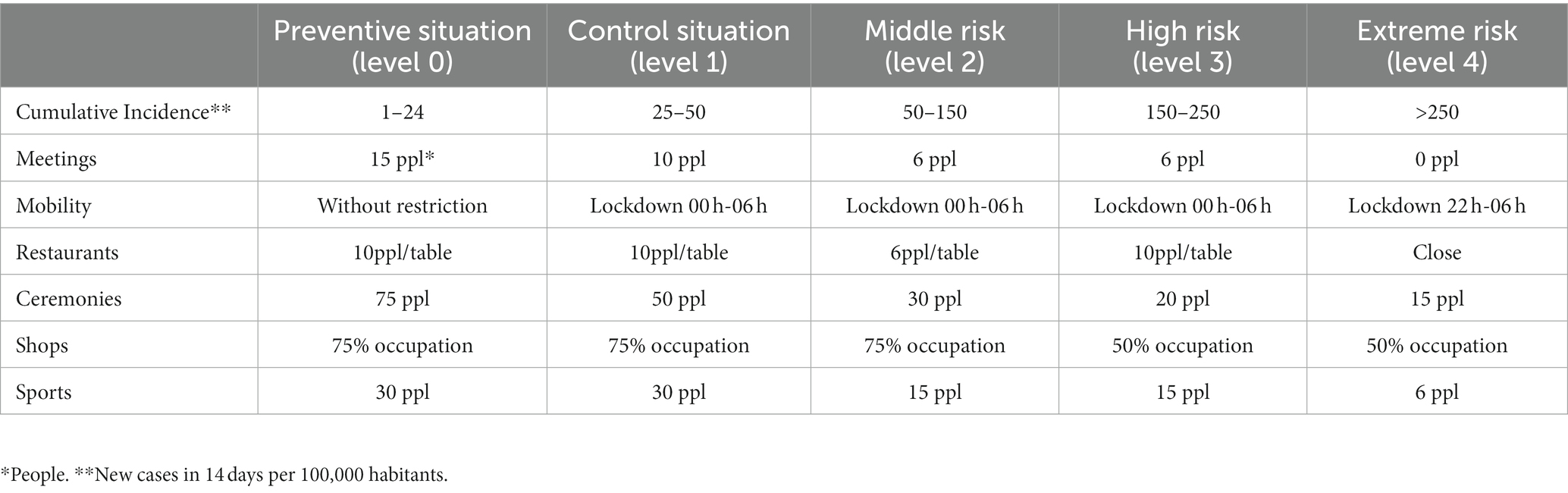
Table 1. Balearic Islands’ levels of COVID-19 public health measures.
An index patient was defined as a person with a new positive SARS-CoV2 test and unknown origin of their infection during contact tracing.
A ‘close contact’ was a person who (a) had been at the same place as a symptomatic index patient for at least 2 days prior to the onset of symptoms or (b) if the index patient was asymptomatic, at least 2 days prior to the positive diagnosis of the index patient. In addition, in both instances, close contacts should have been within 2 meters of the index patient for more than 15 min within 24 h as per the definition of the Ministry of Health (36).
In our study, cases were defined as those “close contacts” tested positive for SARS-CoV-2 by PCR or antigen test within 10 days after the last contact with the index patient. And controls were similar to cases but had a negative SARS-CoV-2 test result.
Both cases and controls were included in the study if they were older than 18 years and accepted to participate. Cases were excluded if they: (1) were symptomatic close contacts of the index patient, to avoid confusion on the transmission chain. The symptoms considered for exclusion as close contact for this study were the same as those identified as COVID-19 suspicion symptoms by the Spanish Ministry of Health (36); (2) were contacts institutionalized in nursing homes or long-term care facilities, and persons in contact with a healthcare setting (either as workers or patients/service users) -since they had different preventive measures-, and (3) had difficulties with telephone communication or understanding.
Accepting an alpha risk of 0.05 and a beta risk of 0.2 in a bilateral contrast, 327 cases and 1,636 controls are required to detect a minimum Odds Ratio of 1.5. It is assumed that the rate of exposure to the different variables collected in the control group will be at least 20%.
Therefore, the total sample will be at least 1,963 close contacts. Considering that each index patient can have an average of about 5 close contacts, about 400 index patients will be necessary.
The questionnaire for the index patients included social-demographic variables (age, sex, education level, profession, and professional status), symptoms and the number of close contacts. The questionnaire for close contacts asked about the environment or setting and exposure characteristics associated with SARS-CoV-2 transmission: contact place, ventilation characteristics (open-air, closed space with or without ventilation), mask-wearing, type of mask, duration of contact, shortest distance, case-contact relationship, household members, and handwashing. Social-demographic variables for close contacts were also collected. Finally, once the isolation period of the close contact ended, test results were retrieved from the electronic health records.
Recruitment of participants was conducted from February to June 2021. During this period, a total of 6,765 patients were reported to the tracking coordination center. We finally included 425 index patients which led to 2,050 close contacts of whom 1,778 were included after application of the inclusion and exclusion criteria.
Descriptive analysis with sociodemographic variables of index patients and close contacts was performed. Numerical variables were expressed by the mean and standard deviation (SD). Categorical variables were expressed by absolute and relative frequencies. The secondary attack rate with confidence intervals (95% CI) was estimated using the percentage of new cases (positive contacts) among all contacts to enable a comparison with secondary attack rate across the different ventilation characteristics and durations of contact. Logistic regression with random effects adjusted for the index patient was used to calculate Odds Ratios (ORs) and 95% CI to evaluate the association between SARS-CoV-2 infection and all studied factors.
All statistical tests were two-sided, and p values <0.05 were considered statistically significant. Statistical analysis was carried out using the Statistical Package for the Social Sciences (SPSS) version 26.0 (IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp).
The study adhered to the principles of the Declaration of Helsinki and legal regulations regarding data confidentiality and research involving human participants. The study protocol received approval from the Balearic Committee of Clinical Research Ethics (Ref. no: IB 4444/21). All participants were informed of the study’s purpose and procedures before providing their verbal consent to participate.
Our analysis included all new index patients and their contacts who met inclusion criteria reported to the contact tracing center of Majorca from February to June 2021. During the study period, after doing the contact tracing of all index patients who complied with the inclusion criteria, 2,050 close contacts from 463 index patients were identified. When the inclusion and exclusion criteria were applied, a total of 1,778 close contacts were offered to participate and were accepted (425 cases and 1,353 controls).
The mean age of index patients was 39.71 ± 15.26, and 53.1% were female. As for education level, 9.4% had not completed basic education or secondary education. Most index patients (59.5%) were office workers (20.5%), worked in the industrial sector (17.4%), or in bar and service workers (11.5%) (Supplementary Table 1). Headaches (51.4%) and cough (49.9%) were the symptoms most frequently reported by index patients, but 6% of them were asymptomatic (Figure 1). Mean close contacts per index patient were 4.43 ± 3.38, including all close contacts identified during the tracing process (n = 2,050).
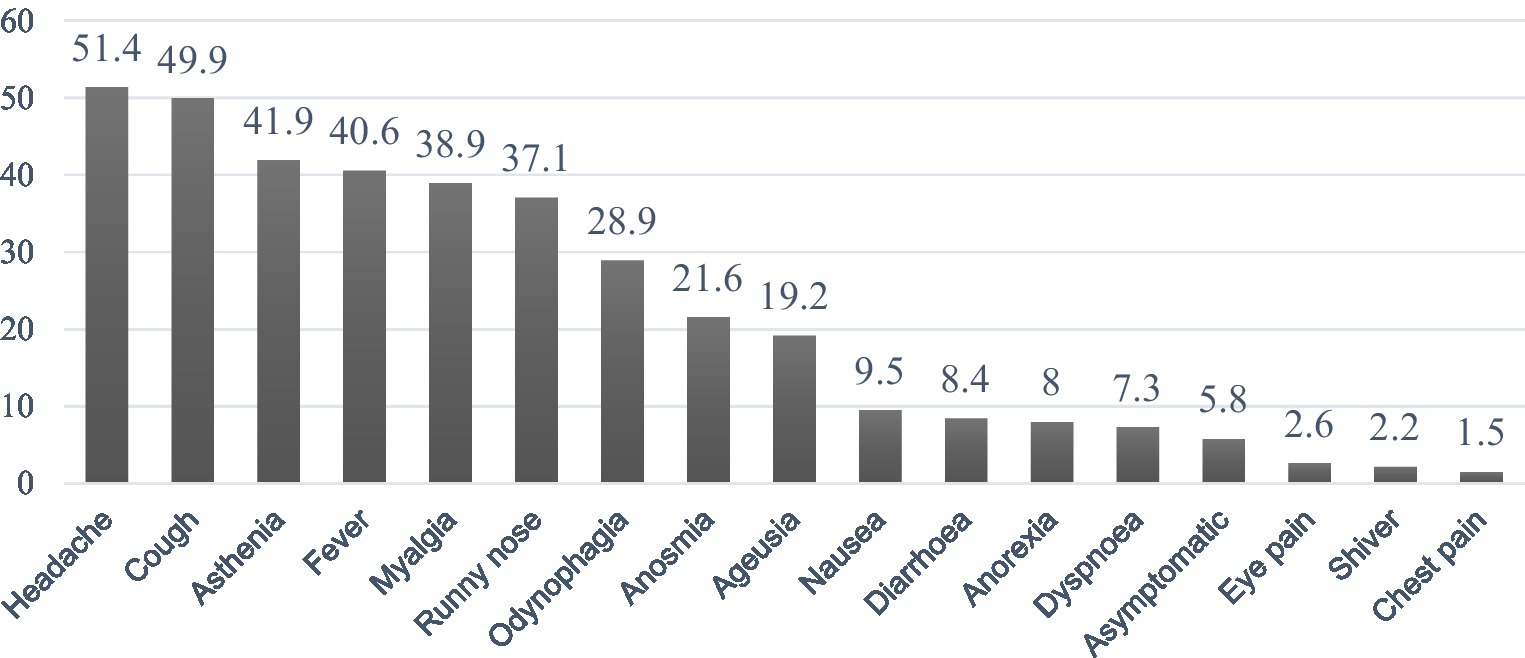
Figure 1. Index patient symptomatology before diagnostic (%). Index patients could have had more than one symptom.
The mean age of the contacts included in the study (n = 1,778) was 42.8 ± 17.4, and 53.6% were female (Table 2). Most contacts were family members (57.5), 33.6% shared accommodation, 23.7% were friends, and 13.8% were work colleagues. The accommodation was the main environment of exposure (67.3%). The 60.8% of contacts reported not wearing a mask when they were exposed to the index patient. Finally, the type of mask more frequently used (66.1%) was a surgical one.
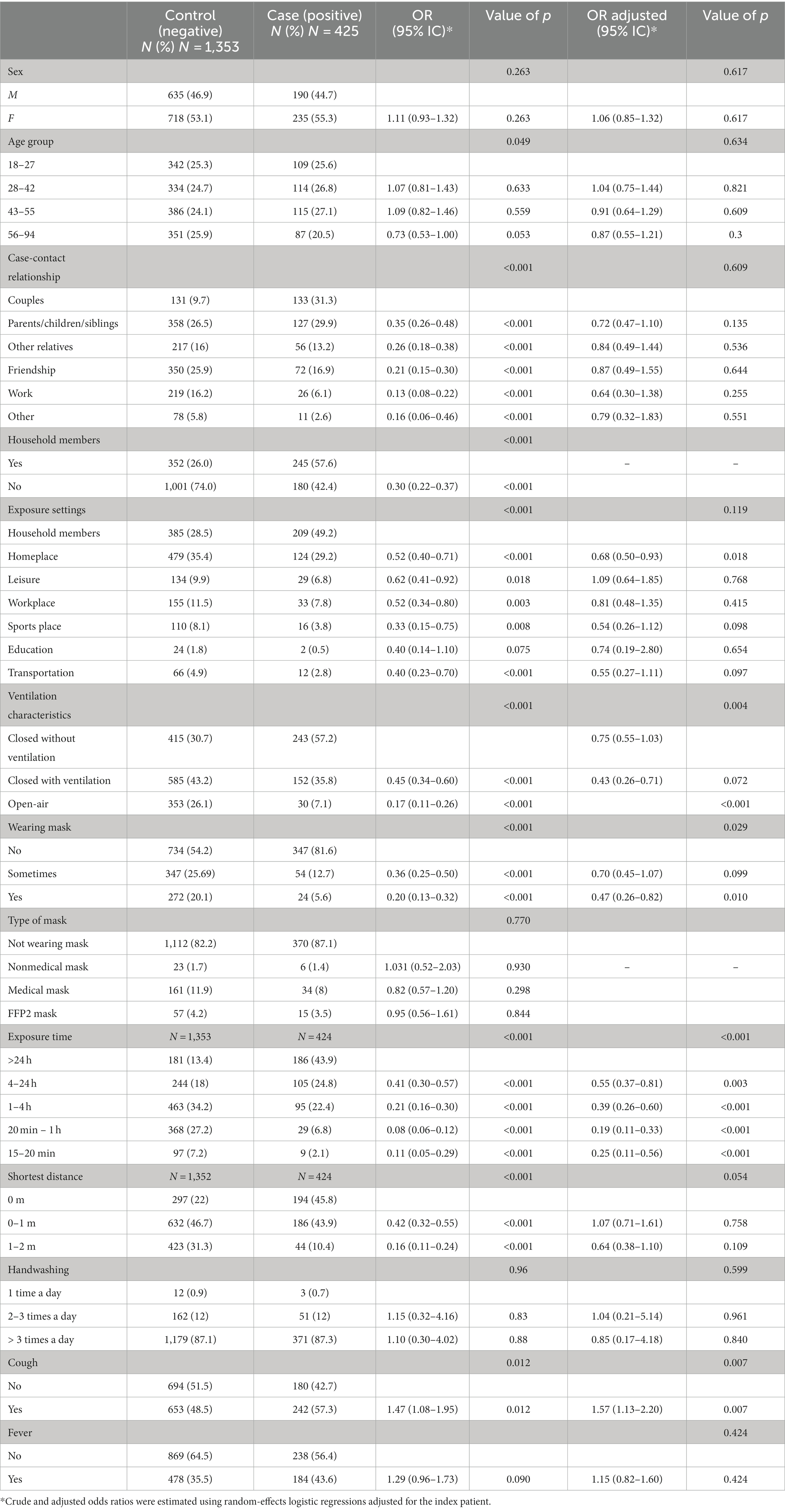
Table 2. Risk factors associated with SARS-CoV-2 infection among contacts of index patients (N = 1,778).
The secondary attack rate within the contacts was 24.0% (95% CI: 22.0–26.0%). According to ventilation characteristics, was: 7.8% (95% CI: 5.1–10.5%) in open-air, 20.6% (95% CI: 17.7–23.5%) in closed space with ventilation, and 36.9% (95% CI: 33.2–40.6%) in unventilated closed spaces. By exposure time, was: 8.5% (95% CI: 3.2–13.8%) for 15–20 min, 7.3% (95% CI: 4.7–9.9%) for 20 min–1 h, 17.0% (95% CI: 14.0–20.1%) 1–4 h, 30.1% (95% CI: 25.3–34.9%) for 4 h-24 h, and 50.7% (95% CI: 45.6–55.8%) for close contacts who stayed more than 24 h. Regarding the secondary attack rate in different exposure settings: among household members, it was 35.2% (95% CI: 31.3–39.0%), at home was 20.6% (95% CI: 17.3–23.8%), social settings 17.8% (95% CI: 11.9–23.7%), and finally, the work setting 17.6% (95% CI: 12.1–23.0%) (Table 3).
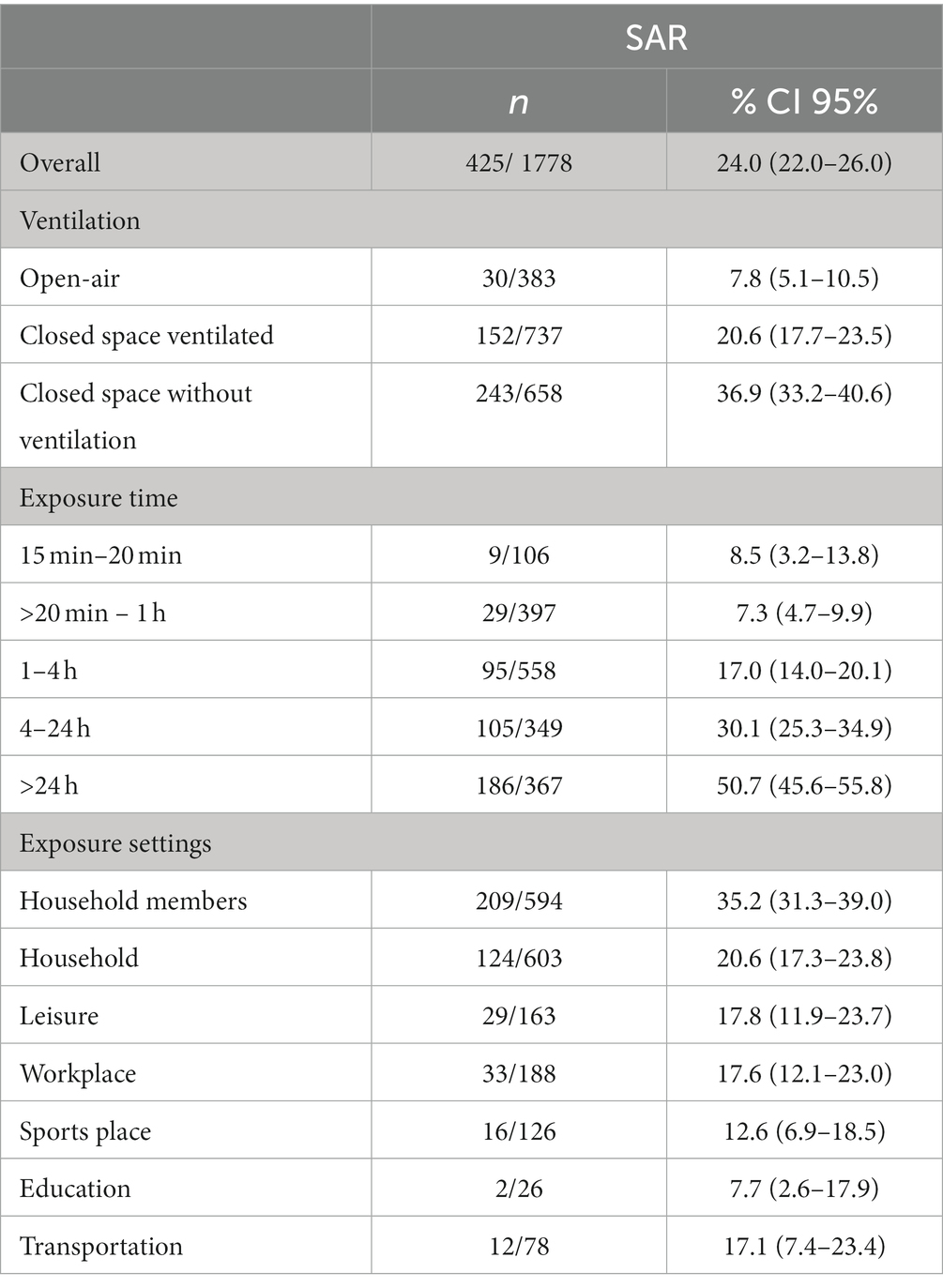
Table 3. Secondary attack rate within the contacts identified through tracing.
The bivariate analyses showed an inverse association between personal protective measures and exposure characteristics (exposure time and ventilation) and SARS-CoV-2 transmission. There were no differences between sex and infection of either index patients or close contacts who were subsequently infected. Among the close contacts, there was a close statistically significant difference for age group and SARS-CoV-2 transmission; OR 1.07 (95% CI: 0.81–1.1.43) between 28 and 42 years, 1.09 (95%CI: 0.82–1.46) for 43–55 years and 0.73 (95% CI: 0.53–1.00) for 56–94 years compared with 18–27 age group.
Contacts who shared accommodation with the index patient were more likely to be infected (OR for non-household members 0.30, 95% CI: 0.22–0.37). Similarly, when the exposure environment was analyzed, close contacts in homes, workplaces, and sites of leisure and socialization activities (bars and restaurants) were more likely to be infected compared to those who were exposed to transportation, education, and sports environments (p < 0.001).
Close contacts who were exposed in the open air were less likely to be infected (OR 0.17, 95% CI: 0.11–0.26) than those exposed to index patients in unventilated, closed spaces. Those contacts who maintained a physical distance between 1 and 2 meters were less likely to be infected (OR 0.16, 95% CI: 0.11–0.24) than close contacts who were closer than 1 m. Infection was less likely to occur among those spending less than 1 h with the index patient, compared to those close contacts who had spent more than 24 h (OR 0.08; 95% CI: 0.06–0.12). Cough and fever of the index patient were more likely to result in infection of the close contacts identified; OR 1.47; 95% CI: 1.08–1.95 and 1.29; 95% CI: 0.96–1.73, respectively. We did not find a statistically significant association between a particular type of face mask and infection, but wearing any mask was however associated with less risk of infection (p < 0.001) (Table 2).
In a multivariant analysis, adjusted odds ratio analyses showed that open-air setting (OR 0.43, 95% CI: 0.26–0.71), exposure for less than 1 h (OR 0.19, 95% CI: 0.11–0.33), and wearing a mask (OR 0.47, 95% CI: 0.26–0.82) had a protective effect against infection. Also, if the cough was present in index patients the likelihood of transmission to their close contacts increased (OR 1.57, 95% CI: 1.13–2.20). The multivariable analyses did not include the type of mask and those household members because of collinearity with wearing masks and relationships with index patient-contact, respectively (Table 2).
Our results characterized the transmission of COVID-19 in the community. Wearing face masks was effective in reducing this transmission, regardless of the type of masks used. Additional factors such as duration of exposure to a person with infection, and environmental ventilation, were also influential in community transmission, rather than the relationship with the index patient and the areas where exposure occurred. Our results emphasize the contribution of households and the sharing of accommodation towards the transmission dynamics of the pandemic. In this regard, we observed that limiting the time of exposure, increasing ventilation, and wearing any type of mask as much as possible would prevent SARS-CoV-2 transmission.
In our study, we did not observe a statistically significant difference regarding sex in the transmission of SARS-CoV-2 to close contacts. This finding is aligned with other already published studies (18). Similarly, we found no statistical differences regarding the age of contacts, whereas higher rates of infection among close contacts who were older have been reported (22, 37, 38). However, these studies were mainly conducted in 2020, when social awareness of compliance with personal protective measures to reduce the risk of infection was heightened (39). Our results could be explained by prevailing political narratives and directives towards protecting older adults, messages which were readily adopted by the population (40).
In our study, the overall secondary attack rate was ~24%, a slightly higher percentage, but similar to results typically conducted in households, ranging between 16.5 and 23.0% (22, 37, 41–43). However, environments such as boxing venues and nightclubs seem to have a higher secondary attack rate than households, whilst the workplace was associated with the lowest (42). Another community study focused on schools reported 9.2% secondary attack rate, slightly higher than our results (7.7%) (37). Our results provide evidence that the household was the environment with the higher risk of secondary attack rate within all daily settings. Similar findings have been obtained elsewhere (44, 45); household secondary attack rate was higher than global, followed by social (44).
Differences were found when the secondary attack rate was calculated for different exposure times and ventilation characteristics. Compared to outdoor spaces, secondary attack rate in closed unventilated spaces was almost 5 times higher. A study that assessed poor ventilation in a restaurant concluded that indeed ventilation in indoor spaces at restaurants had a lower risk than spaces without ventilation (46). Exposure time is a relevant variable in transmission; spending more than 4 h with an infected person has been observed to double the transmission rate. Our results were higher than those reported elsewhere for a time exposure of more than 60 min with a secondary attack rate of 24% (42). Contacts who spent more than 24 h in closed unventilated spaces tended to be household members, therefore, our results reinforce the idea that much of the growth in community transmission during the pandemic can be attributed to the household and close relatives (18).
We observed a higher risk of transmission among close contacts when the index patient had a cough. Previous evidence reflected simulated conditions (5, 47). The smaller cough droplets can reach longer distances (47), and sneezing projects more viral load than coughing (5). Our study showed similar results to in vitro studies who observed increased shedding of droplets containing SARs-CoV-2 when coughing, coinciding with increased transmission and infection of close contacts in the general population.
Mask-wearing could be one of the most important individual behaviors to reduce SARS-CoV-2 transmission, compared with other personal protective variables (hand hygiene washing and social distance). Other studies focused on SARS-CoV-2 were consistent with our results. Wearing a mask at home after illness onset reduces the transmission of SARS-CoV-2 (OR 0.30, 95% CI: 0.11–0.82) compared with people who never wear a mask (22).
The type of mask (cloth, surgical, FFP2) used during the exposure did not show statistically significant differences in the risk of transmission (42). Existing evidence suggests a gradient of protection, with N95 respirator use associated with viral infectious episodes for healthcare workers compared with surgical masks (48). Such reduction could be attributed to the higher risk of infection in a clinical setting compared to other social environments (49). In another study, masks indicated less effectiveness but still concludes that any type of mask minimizes the risk of transmission in the general population (50). Therefore, the type of mask perhaps will not be as important in the community as in health centers.
Household members accounted for more than half of all at-risk contacts who became infected, making the home the environment with the highest risk for SARS-CoV-2 transmission. A cohort study that compared households with other settings got similar results (45). In a multivariable model, household members had an OR of 8.1 (95% CI: 5.9–11.4) compared with shared transportation, enclosed space without direct contact, and conversation (45). Few studies analyzed all areas at the same time, which makes it difficult to compare the obtained results with existing ones.
Our study has some limitations due to the design and methods followed, which should encourage caution when interpreting the results. First, case–control studies may overestimate the magnitude of the effect seen when compared to relative risk (51). Secondly, we considered that each positive contact had been infected by an index patient, whereas it might be possible for some contacts to be infected by other individuals in the community unknown to the contact tracing team. Another limitation could be the exclusion of children could have led to an underestimated secondary attack rate in the educational environment. We understand that this population requires attention but due to the tracing logistics, we opted to exclude them from the study. Also, the contact tracing interview focused on the use of face masks but did not clarify whether such use was correct (i.e., mouth and nose covered), or whether the face mask was new or worn out, both factors which can compromise the efficacy of the mask (52). As well as the limitation of not to collect the vaccination status of our participants. Finally, we only asked participants about the symptoms included in the national protocol developed by the Ministry and did not ask about other symptoms experienced by the index patients such as sneezing, which could be associated with transmission independently from cough (47). Finally, selection bias for the close contacts could have affected this study because the index patients voluntarily named their close contacts, being likely to not have included every possible close contact.
Regarding the study strengths, most index patients diagnosed from February to June 2021 were included in the study. We included all COVID tests realized in Majorca during the period of study so the results could be generalized to the entire community. We designed the study to minimize the biases of case–control studies (complacency bias, and recall bias) (53). Complacency bias was minimized as the questionnaire was administered before the respondents were given the result of their test, avoiding any influence on their responses. Recall bias was minimized by contacting people at the time of their identification as close contacts, thus minimizing the time elapsed between the call and the day of exposure.
Our results provide evidence supporting individual and collective prevention and safety measures against coronavirus transmission. Understanding the association between the use of masks, ventilation of area, time exposure, and the transmission of SARS-CoV-2 could optimize the real-time contact tracing mechanisms and focus on the more at-risk population. Also, additional attention and resources could be allocated to close contacts of index patients with cough, which would be at higher risk of infection.
Our study may have been beneficial in assisting public institutions to better identify individuals most at risk, thereby optimizing the use of limited human resources in case tracing. Despite organizational difficulties and pressure on the health system and workforce during contact tracing, research opportunities were afforded to understand community mechanisms of transmission and thus improve this public health component. Studies replicating our experience should be embedded in contact tracing efforts, even during pandemic events, to refine policy or tracing decisions.
The dataset supporting the findings of this study is available in the Docsalut repository at https://hdl.handle.net/20.500.13003/20064, doi: 10.52207/docusalut.20064.
The studies involving humans were approved by Balearic Ethical Committee of Clinical Research (Ref. No: IB 4444/21). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
AH-T: Conceptualization, Data curation, Formal analysis, Investigation, Writing – original draft. EC-S: Formal analysis, Supervision, Writing – review & editing. LC-M: Data curation, Formal analysis, Writing – review & editing. CS-R: Data curation, Validation, Writing – review & editing. MB-V: Conceptualization, Formal analysis, Methodology, Validation, Writing – review & editing. AY: Conceptualization, Formal analysis, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by the Royal College of Nurses from the Balearic Islands (Ref. 2021-0564). This research was also supported by the Florence Nightingale fellowship program, Royal College of Nurses from the Balearic Islands and the Nursing and Physiotherapy Department, University of the Balearic Islands.
We thank all participants involved in providing information. We thank all professionals from COVID-19 Coordinating Centre for their support, especially Rocío Sánchez Rodríguez, Ana Belén Expósito Torres, Esther Granados Ramos, and María José Sastre Perea.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1327082/full#supplementary-material
1. Benenson, AS . Control of communicable diseases manual. Control of communicable diseases manual. 16th ed. Washington, DC: American Public Health Association (1995).
2. Drosten, C, Meyer, B, Müller, MA, Corman, VM, Al-Masri, M, Hossain, R, et al. Transmission of MERS-coronavirus in household contacts. N Engl J Med. (2014) 371:828–35. doi: 10.1056/NEJMoa1405858
3. He, X, Lau, EHY, Wu, P, Deng, X, Wang, J, Hao, X, et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat Med. (2020) 26:672–5. doi: 10.1038/s41591-020-0869-5
4. ISARIC Clinical Characterisation Group . COVID-19 symptoms at hospital admission vary with age and sex: results from the ISARIC prospective multinational observational study. Infection. (2021) 49:889–905. doi: 10.1007/s15010-021-01599-5
5. Agrawal, A, and Bhardwaj, R. Probability of COVID-19 infection by cough of a normal person and a super-spreader. Phys Fluids. (2021) 33:031704. doi: 10.1063/5.0041596
6. Jimenez, JL, Marr, LC, Randall, K, Ewing, ET, Tufekci, Z, Greenhalgh, T, et al. What were the historical reasons for the resistance to recognizing airborne transmission during the COVID-19 pandemic? Indoor Air. (2022) 32:e13070. doi: 10.1111/ina.13070
7. Cheng, VCC, Wong, SC, Chen, JHK, Yip, CCY, Chuang, VWM, Tsang, OTY, et al. Escalating infection control response to the rapidly evolving epidemiology of the coronavirus disease 2019 (COVID-19) due to SARS-CoV-2 in Hong Kong. Infect Control Hosp Epidemiol. (2020) 41:493–8. doi: 10.1017/ice.2020.58
8. Smith, SM, Sonego, S, Wallen, GR, Waterer, G, Cheng, AC, and Thompson, P. Use of non-pharmaceutical interventions to reduce the transmission of influenza in adults: a systematic review. Respirology. (2015) 20:896–903. doi: 10.1111/resp.12541
9. Koh, WC, Naing, L, Chaw, L, Rosledzana, MA, Alikhan, MF, Jamaludin, SA, et al. What do we know about SARS-CoV-2 transmission? A systematic review and meta-analysis of the secondary attack rate and associated risk factors. PLoS One. (2020) 15:e0240205. doi: 10.1371/journal.pone.0240205
10. Chavhan, SS, Adsul, B, Dhikale, PT, Kinge, K, Gokhale, C, Ingale, A, et al. Assessment of risk factors for COVID-19 in health care workers: a nested case-control study. J Assoc Physicians India. (2021) 69:11–2.
11. Dev, N, Meena, RC, Gupta, DK, Gupta, N, and Sankar, J. Risk factors and frequency of COVID-19 among healthcare workers at a tertiary care Centre in India: a case-control study. Trans R Soc Trop Med Hyg. (2021) 115:551–6. doi: 10.1093/trstmh/trab047
12. Lentz, RJ, Colt, H, Chen, H, Cordovilla, R, Popevic, S, Tahura, S, et al. Assessing coronavirus disease 2019 (COVID-19) transmission to healthcare personnel: the global ACT-HCP case-control study. Infect Control Hosp Epidemiol. (2021) 42:381–7. doi: 10.1017/ice.2020.455
13. Rosser, JI, Tayyar, R, Giardina, R, Kolonoski, P, Kenski, D, Shen, P, et al. Case-control study evaluating risk factors for SARS-CoV-2 outbreak amongst healthcare personnel at a tertiary care center. Am J Infect Control. (2021) 49:1457–63. doi: 10.1016/j.ajic.2021.09.004
14. Heinzerling, A, Stuckey, MJ, Scheuer, T, Xu, K, Perkins, KM, Resseger, H, et al. Transmission of COVID-19 to health care personnel during exposures to a hospitalized patient – Solano County, California, February 2020. MMWR Morb Mortal Wkly Rep. (2020) 69:472–6. doi: 10.15585/mmwr.mm6915e5
15. Radonovich, LJ Jr, Simberkoff, MS, Bessesen, MT, Brown, AC, Cummings, DAT, Gaydos, CA, et al. N95 respirators vs medical masks for preventing influenza among health care personnel: a randomized clinical trial. JAMA. (2019) 322:824–33. doi: 10.1001/jama.2019.11645
16. Chaabna, K, Doraiswamy, S, Mamtani, R, and Cheema, S. Facemask use in community settings to prevent respiratory infection transmission: a rapid review and meta-analysis. Int J Infect Dis. (2021) 104:198–206. doi: 10.1016/j.ijid.2020.09.1434
17. Chen, Y, Wang, Y, Quan, N, Yang, J, and Wu, Y. Associations between wearing masks and respiratory viral infections: a meta-analysis and systematic review. Front Public Health. (2022) 10:874693. doi: 10.3389/fpubh.2022.874693
18. Lim, C, Nam, Y, Oh, WS, Ham, S, Kim, E, Kim, M, et al. Characteristics of transmission routes of COVID-19 cluster infections in Gangwon Province, Korea. Epidemiol Infect. (2022) 150:e19. doi: 10.1017/S0950268821002788
19. Zhen, J, Chan, C, Schoonees, A, Apatu, E, Thabane, L, and Young, T. Transmission of respiratory viruses when using public ground transport: a rapid review to inform public health recommendations during the COVID-19 pandemic. S Afr Med J. (2020) 110:478–83. doi: 10.7196/SAMJ.2020.v110i6.14751
20. CDC . Coronavirus disease 2019 (COVID-19) prevention and treatment. Centres for Disease Control and Prevention. (2020) Available at: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html
21. WHO . Advice on the use of masks in the community, during home care and in health care settings in the context of the novel coronavirus (2019-nCoV) outbreak (2020).
22. Wang, Y, Tian, H, Zhang, L, Zhang, M, Guo, D, Wu, W, et al. Reduction of secondary transmission of SARS-CoV-2 in households by face mask use, disinfection and social distancing: a cohort study in Beijing, China. BMJ Glob Health. (2020) 5. doi: 10.1136/bmjgh-2020-002794
23. Cui, JLF, and Shi, ZL. Origin and evolution of pathogenic coronaviruses. Nat Rev Microbiol. (2019) 17:181–92. doi: 10.1038/s41579-018-0118-9
24. Rebar, AL, Lally, P, Verplanken, B, Diefenbacher, S, Kwasnicka, D, Rhodes, RE, et al. Changes in virus-transmission habits during the COVID-19 pandemic: a cross-national, repeated measures study. Psychol Health. (2022) 37:1626–45. doi: 10.1080/08870446.2022.2097682
25. Hossain, AD, Jarolimova, J, Elnaiem, A, Huang, CX, Richterman, A, and Ivers, LC. Effectiveness of contact tracing in the control of infectious diseases: a systematic review. Lancet Public Health. (2022) 7:e259–73. doi: 10.1016/S2468-2667(22)00001-9
26. Our World in Data . Which countries do COVID-19 contact tracing? (2022) Available at: https://ourworldindata.org/grapher/covid-contact-tracing?time=2022-04-17
27. WHO . WHO coronavirus (COVID-19) dashboard, measures (2022) Available at: https://covid19.who.int/measures
28. Fetzer, T, and Graeber, T. Measuring the scientific effectiveness of contact tracing: evidence from a natural experiment. Proc Natl Acad Sci U S A. (2021) 118. doi: 10.1073/pnas.2100814118
29. El-Sadr, WM, Platt, J, Bernitz, M, and Reyes, M. Contact tracing: barriers and facilitators. Am J Public Health. (2022) 112:1025–33. doi: 10.2105/AJPH.2022.306842
30. European Centre for Disease Prevention and Control . COVID-19 contact tracing: Country experiences and way forward. Copenhagen: WHO Regional Office for Europe and Stockholm: European Centre for Disease Prevention and Control (2022).
31. Thomas Craig, KJ, Rizvi, R, Willis, VC, Kassler, WJ, and Jackson, GP. Effectiveness of contact tracing for viral disease mitigation and suppression: evidence-based review. JMIR Public Health Surveill. (2021) 7:e32468. doi: 10.2196/32468
32. Butlletí Oficial de les Illes Balears (BOIB). Acord del Consell de Govern de 12 de març de 2021 pel qual s’estableixen els nivells d’alerta sanitària per illes que han de vigir a la comunitat autònoma de les Illes Balears i s’estableixen mesures excepcionals de prevenció del contagi de la COVID-19 aplicables temporalment a les illes. BOIB núm. 35. Secció III. Altres disposicions i actes administratius (2021). Available at: https://www.caib.es/eboibfront/ca/2021/11353/seccio-iii-altres-disposicions-i-actes-administrat/472
33. Butlletí Oficial de les Illes Balears (BOIB). Acord del Consell de Govern de 27 de novembre de 2020 pel qual s’estableixen els nivells d’alerta sanitària i s’aprova el nou Pla de Mesures Excepcionals de Prevenció, Contenció i Coordinació per fer Front a la Crisi Sanitària Ocasionada per la COVID-19. BOIB núm. 201. Secció III. Altres disposicions i actes administratius (2020). Available at: https://www.caib.es/eboibfront/ca/2020/11302/seccio-iii-altres-disposicions-i-actes-administrat/472
34. Balearic Islands Goverment (GOIB) . Visior COVID-19 Illes Balears (2023) Available at: https://www.caib.es/sites/covid-19/es/visor_covid-19_illes_balears/
35. Butlletí Oficial de les Illes Balears (BOIB). Acord del Consell de Govern d’11 de gener de 2021 pel qual s’estableixen els nivells d’alerta sanitària per illes que han de vigir a la comunitat autònoma de les Illes Balears, de conformitat amb l’Acord del Consell de Govern de les Illes Balears de 27 de novembre de 2020, i es disposen mesures excepcionals aplicables a l’illa de Mallorca i a la d’Eivissa. BOIB núm. 5. Secció III. Altres disposicions i actes administratius (2021). Available at: https://www.caib.es/eboibfront/ca/2021/11322/seccio-iii-altres-disposicions-i-actes-administrat/472
36. Ministerio de Sanidad. Estrategia de detección precoz, vigilancia y control de COVID-19. (2021). Available at: https://www.sanidad.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/COVID19_Estrategia_vigilancia_y_control_e_indicadores.pdf
37. Fung, HF, Martinez, L, Alarid-Escudero, F, Salomon, JA, Studdert, DM, Andrews, JR, et al. The household secondary attack rate of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2): a rapid review. Clin Infect Dis. (2021) 73:S138–45. doi: 10.1093/cid/ciaa1558
38. Luo, L, Liu, D, Liao, X, Wu, X, Jing, Q, Zheng, J, et al. Contact settings and risk for transmission in 3410 close contacts of patients with COVID-19 in Guangzhou, China: a prospective cohort study. Ann Intern Med. (2020) 173:879–87. doi: 10.7326/M20-2671
39. Ali-Saleh, O, and Obeid, S. Compliance with COVID-19 preventive guidelines among minority communities: the case of Israeli Arabs. J Racial Ethn Health Disparities. (2022) 10:1576–87. doi: 10.1007/s40615-022-01344-0
40. The Independent Scientific Advisory Group for Emergencies (SAGE) . Why supported isolation is crucial to break community transmission SAGE (2021) Contract No. 40.
41. Jing, QL, Liu, MJ, Zhang, ZB, Fang, LQ, Yuan, J, Zhang, AR, et al. Household secondary attack rate of COVID-19 and associated determinants in Guangzhou, China: a retrospective cohort study. Lancet Infect Dis. (2020) 20:1141–1150. doi: 10.1016/S1473-3099(20)30471-0
42. Doung-Ngern, P, Suphanchaimat, R, Panjangampatthana, A, Janekrongtham, C, Ruampoom, D, Daochaeng, N, et al. Case-control study of use of personal protective measures and risk for SARS-CoV 2 infection, Thailand. Emerg Infect Dis. (2020) 26:2607–16. doi: 10.3201/eid2611.203003
43. Madewell, ZJ, Yang, Y, Longini, IM Jr, Halloran, ME, and Dean, NE. Household transmission of SARS-CoV-2: a systematic review and Meta-analysis. JAMA Netw Open. (2020) 3:e2031756. doi: 10.1001/jamanetworkopen.2020.31756
44. Del Águila-Mejía, J, Wallmann, R, Calvo-Montes, J, Rodríguez-Lozano, J, Valle-Madrazo, T, and Aginagalde-Llorente, A. Secondary attack rate, transmission and incubation periods, and serial interval of SARS-CoV-2 omicron variant. Spain Emerg Infect Dis. (2022) 28:1224–8. doi: 10.3201/eid2806.220158
45. Ge, Y, Martinez, L, Sun, S, Chen, Z, Zhang, F, Li, F, et al. COVID-19 transmission dynamics among close contacts of index patients with COVID-19: a population-based cohort study in Zhejiang Province, China. JAMA Intern Med. (2021) 181:1343–50. doi: 10.1001/jamainternmed.2021.4686
46. Li, Y, Qian, H, Hang, J, Chen, X, Cheng, P, Ling, H, et al. Probable airborne transmission of SARS-CoV-2 in a poorly ventilated restaurant. Build Environ. (2021) 196:107788. doi: 10.1016/j.buildenv.2021.107788
47. El Hassan, M, Assoum, H, Bukharin, N, Al Otaibi, H, Mofijur, M, and Sakout, A. A review on the transmission of COVID-19 based on cough/sneeze/breath flows. Eur Phys J Plus. (2022) 137:1. doi: 10.1140/epjp/s13360-021-02162-9
48. Collins, AP, Service BC, Gupta, S, Mubarak, N, Zeini, IM, Osbahr, DC, et al. N95 respirator and surgical mask effectiveness against respiratory viral illnesses in the healthcare setting: a systematic review and meta-analysis. J Am Coll Emerg Physicians Open. (2021) 2:e12582. doi: 10.1002/emp2.12582
49. Nguyen, LH, Drew, DA, Graham, MS, Joshi, AD, Guo, CG, Ma, W, et al. Risk of COVID-19 among front-line health-care workers and the general community: a prospective cohort study. Lancet Public Health. (2020) 5:e475–83. doi: 10.1016/S2468-2667(20)30164-X
50. Silva, A, Almeida, AM, Freire, MEM, Nogueira, JA, Gir, E, and Nogueira, WP. Cloth masks as respiratory protections in the COVID-19 pandemic period: evidence gaps. Rev Bras Enferm. (2020) 73:e20200239. doi: 10.1590/0034-7167-2020-0239
51. Davies, HT, Crombie, IK, and Tavakoli, M. When can odds ratios mislead? BMJ. (1998) 316:989–91. doi: 10.1136/bmj.316.7136.989
52. Howard, J, Huang, A, Li, Z, Tufekci, Z, Zdimal, V, van der Westhuizen, HM, et al. An evidence review of face masks against COVID-19. Proc Natl Acad Sci U S A. (2021) 118. doi: 10.1073/pnas.2014564118
Keywords: SARS-CoV-2, contact tracing, hand disinfection, physical distancing, masks, ventilation, respiratory tract diseases
Citation: Huguet-Torres A, Castro-Sánchez E, Capitán-Moyano L, Sánchez-Rodríguez C, Bennasar-Veny M and Yáñez AM (2024) Personal protective measures and settings on the risk of SARS-COV-2 community transmission: a case–control study. Front. Public Health. 11:1327082. doi: 10.3389/fpubh.2023.1327082
Edited by:
Simon Ching Lam, Tung Wah College, Hong Kong SAR, ChinaReviewed by:
Hua Wei, The University of Manchester, United KingdomCopyright © 2024 Huguet-Torres, Castro-Sánchez, Capitán-Moyano, Sánchez-Rodríguez, Bennasar-Veny and Yáñez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Enrique Castro-Sánchez, ZW5yaXF1ZS5jYXN0cm8tc2FuY2hlekBicnVuZWwuYWMudWs=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.