
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health, 11 January 2024
Sec. Public Mental Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1305463
This article is part of the Research TopicCommunity Series in Mental Illness, Culture, and Society: Dealing with the COVID-19 Pandemic, volume VIIIView all 63 articles
 Verónica Martínez-Borba1,2
Verónica Martínez-Borba1,2 Laura Martínez-García1,2
Laura Martínez-García1,2 Óscar Peris-Baquero1,2
Óscar Peris-Baquero1,2 Jorge Osma1,2*
Jorge Osma1,2* Esther del Corral-Beamonte3
Esther del Corral-Beamonte3Objective: The COVID-19 pandemic has been emotionally challenging for the entire population and especially for people who contracted the illness. This systematic review summarizes psychological interventions implemented in COVID-19 and long COVID-19 patients who presented comorbid emotional disorders.
Methods and measures: 3,839 articles were identified in 6 databases and 43 of them were included in this work. Two independent researchers selected the articles and assessed their quality.
Results: 2,359 adults were included in this review. Severity of COVID-19 symptoms ranged from asymptomatic to hospitalized patients; only 3 studies included long COVID-19 populations. Similar number of randomized controlled studies (n = 15) and case studies (n = 14) were found. Emotional disorders were anxiety and/or depressive symptoms (n = 39) and the psychological intervention most represented had a cognitive behavioral approach (n = 10). Length of psychological programs ranged from 1–5 sessions (n = 6) to 16 appointments (n = 2). Some programs were distributed on a daily (n = 4) or weekly basis (n = 2), but other proposed several sessions a week (n = 4). Short (5–10 min, n = 4) and long sessions (60–90 min, n = 3) are proposed. Most interventions were supported by the use of technologies (n = 18). Important risk of bias was present in several studies.
Conclusion: Promising results in the reduction of depressive, anxiety and related disorders have been found. However, important limitations in current psychological interventions were detected (i.e., duration, format, length, and efficacy of interventions were not consistently established across investigations). The results derived from our work may help to understand clinical practices in the context of pandemics and could guide future efforts to manage emotional suffering in COVID-19 patients. A stepped model of care could help to determine the dosage, length and format of delivery for each patient.
Systematic review registration: PROSPERO 2022 CRD42022367227. Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022367227
The coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARSCoV-2), is considered one of the largest pandemics in world history and was declared a Public Health Emergency of International Concern by the World Health Organization (WHO) on January 30th, 2020 (1). COVID-19 symptoms range from asymptomatic or mild to severe (2), being fever, coughing, fatigue, and dyspnea the most prevalent physical symptoms of diagnosed patients (3). Thus, COVID-19 has caused high morbidity and mortality worldwide. As of 20 June 2023, it has affected more than 768 million people and caused nearly 7 million deaths (4). Special attention should be paid to COVID-19 patients who survive the pandemics but do not recover their initial state of health and report persistent and/or new physical symptoms 3 months after the initial infection, which has been referred by the WHO as post COVID-19 syndrome (5). Thus, more specifically, within this condition the most frequent reported symptoms have been brain fog, dizziness, loss of attention, confusion, chest pain, tachycardia, diarrhea, vomiting, general fatigue, dyspnea, and cough, among others (6).
The impact of the pandemic was observed not only in morbidity and mortality numbers; the pandemic situation and the measures taken during its duration, such as lockdown or reduction of social contact, have had a significant emotional impact on the entire population (7–11). It seems that it was a hard situation for millions of people, with a higher prevalence of psychological symptoms among those who suffered from the disease (12). One study found that patients who were quarantined due to COVID-19 infection showed psychological symptoms such as anxiety and depression symptomatology, lack of self-control and low levels of well-being and vitality (13). From all COVID-19 patients, a high proportion of mental health problems were observed in long or post COVID-19 populations, which presented high rates of persistent psychological distress (36%), anxiety disorders (22%), depression (21%), post-traumatic stress disorder (20%), and sleep disorders (35%) (12).
As we can see, there is a great variety and prevalence of physical and psychological symptoms related both directly to the COVID-19 infection and to the development of post COVID-19 syndrome after the infection. Thus, it has been claimed there is a need for multidisciplinary interventions to address the physical and psychological symptoms associated with COVID-19 (14). From a physical perspective, we found different systematic reviews and meta-analyses on the efficacy of antiviral treatments for the reduction of mortality and risk of hospitalization of patients infected with COVID-19 (15). Probiotics, prebiotics, synbiotics, and postbiotics for the modulation of the microbiota have been used in COVID-19 patients with the aim of reducing the severity and duration of symptoms such as dyspnea, olfactory dysfunction, nausea, vomiting, and gastrointestinal problems (16). In the case of the Post-COVID condition, specific rehabilitation programs have been developed with the input of multidisciplinary professionals (i.e., physiotherapists, occupational therapists, speech and language therapists, social workers, neuropsychiatrists, dieticians or nutritionists, among others) (17).
Similarly, from a psychological perspective, we found different systematic reviews in the field of psychological interventions for COVID-19 patients (18, 19). Promising results were found in the reduction of emotional suffering in COVID-19 patients, which suggest that psychological issues could be properly treated in the context of COVID-19 conditions. However, we noted some important limitations in these systematic reviews. First, some of them have summarized interventions focused mainly on COVID-19 patients which did not include long COVID conditions (18). Second, increased attention has been paid to severe cases (i.e., hospitalized patients) (19) or other non-COVID-19 populations (i.e., relatives, professionals, general populations) (20). Third, despite the well-known comorbidity between anxiety and depressive symptoms in COVID-19 patients, other systematic reviews addressed isolated depressive symptoms (21), or anxiety and related disorders (22).
With the aforementioned information in mind, to the best of our knowledge, this is the first systematic review which aims to explore and update the main characteristics of the psychological interventions delivered to patients with COVID-19 or long COVID-19 conditions and comorbid emotional disorders or symptoms. Results derived from this work may help to guide future clinical and research efforts conducted on the management of these patients.
According to the main objective of this systematic review, inclusion criteria to select the scientific articles were: (a) a psychological intervention was provided; (b) patients presented with COVID-19 or long-COVID-19 conditions; (c) changes in psychological outcomes were reported; (d) patients presented with emotional disorders or symptoms; (e) COVID-19 patients were the main participants; (f) the full text of the articles was written in English or Spanish. Similarly, pre-specified exclusion criteria included: (a) psychological program was not provided; (b) patients did not present with any form of COVID-19 condition; (c) psychological outcomes were not reported; (d) patients presented with severe mental disorders (i.e., psychotic disorders); (e) intervention was focused exclusively on relatives, professionals or general population. Other exclusion criteria had to do with manuscript type and the design of the study. This way, records were excluded for synthesis if they were not scientific articles (i.e., book chapters or conference papers) or they were protocol studies or trial registrations. Additionally, papers were excluded if they were systematic reviews/meta-analysis or if they do not provide efficacy data (i.e., theoretical description of interventions without efficacy results).
This systematic review has been conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses [PRISMA, (23). See Supplementary materials A, B]. The literature search was carried out in specialized databases in the field of mental health and health conditions. Specifically, literature searches were performed in WOS (Web of Science), Scopus, PubMed, PsycINFO, Cochrane and CINAHL. The following word combinations and Boolean operator were entered in the databases: “COVID-19 conditions” AND/OR “psychological interventions” AND/OR “psychological issues” (see a detailed description on Supplementary material C). No language or data restrictions were applied in the searches, which were conducted by two independent researchers (VM-B and LM-G) on June 14, 2023. In addition to the database search, reference lists of different systematic reviews and meta-analyses were also examined to identify the possible inclusion of articles that were not initially found in the databases.
Regarding the management of the results, we used the Mendeley platform (24), for the automatic elimination of duplicate results, and the Rayyan platform (25), for the subsequent review of the inclusion and exclusion criteria of the articles. For this purpose, two independent researchers (VM-B and LM-G) carried out the review of articles in two phases. The first consisted in checking the titles and abstracts of the articles to verify if they met the inclusion criteria. The second phase consisted in a complete reading of the articles selected in the first phase by the researchers to ensure that they, in fact, met the inclusion criteria. A third expert researcher (JO) was consulted when there were doubts about whether a specific article should be included or excluded.
To conduct the extraction of the information, a pre-specified list of outcomes was used by two independent authors (VM-B and LM-G). If there were any disagreements, a third author was consulted (JO). All studies included in the review were eligible for data extraction and synthesis. The pre-specified list was elaborated following the Cochrane recommendations (26). Additionally, in this systematic review we have include interpretation of results to identify whether improvements on psychological measures indicate a total recovery of symptoms (e.g., participants’ scores at post-intervention were below the clinical cut-off established for each questionnaire) or a partial recovery of symptoms (e.g., a decrease in the scores of psychological issues was observed but scores were above the clinical cut-off after the intervention). In this regard, some missing or unclear data was found in the extraction of the information. In some cases, the studies did not report the clinical cut-off that was used for a given questionnaire. To avoid reporting bias, we have checked if authors provided the reference of the questionnaire used in the study. If the reference of the questionnaire was reported, we used it as a cut-off. On the other hand, if the reference of the questionnaire was not mentioned, we used the original version of the questionnaire to determine whether a partial or a total recovery was obtained in this study.
In relation to presentation of results, we have reported the effect measure indicated in the study (i.e., means comparisons, effect sizes, reliable change index). Data presentation is supported by tables and was based on the information directly obtained from the article without converting the data. We have presented the information of such studies according to their design (case studies outcomes are reported in Table 1 while results from intervention studies with and without control group are presented in Table 2). No additional statistical analyses were calculated. Thus, meta-analysis, sub-group analysis and meta-regression and sensitivity analyses were not conducted. To avoid duplication and to reduce possible bias, authors pre-registered the review protocol in PROSPERO (CRD4202236722) on October 19, 2022.
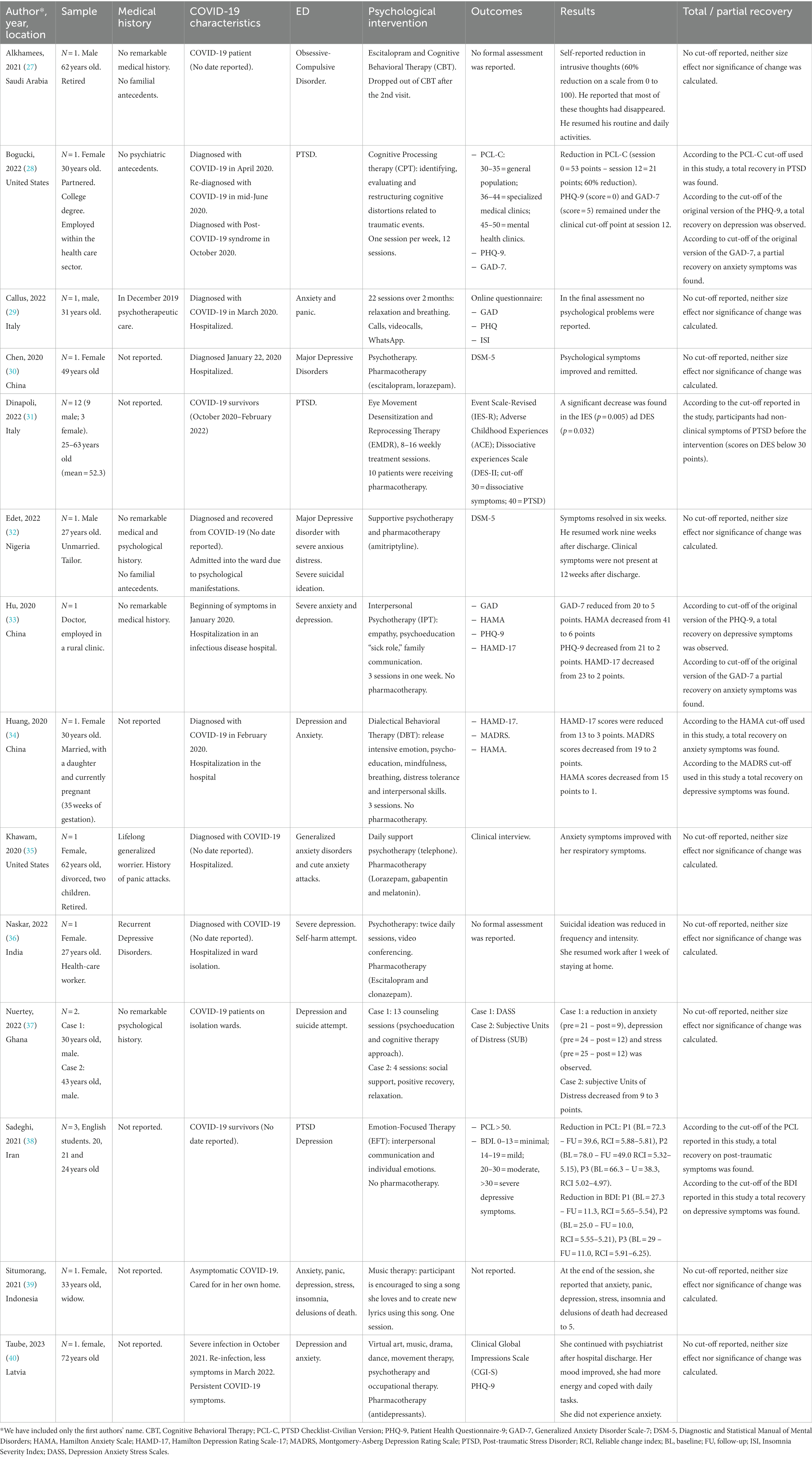
Table 1. Extraction of data for case studies (N = 14).

Table 2. Extraction of data for controlled and non-controlled studies (N = 29).
The analyses of the quality of the studies were performed by two independent researchers (VM-B and LM-G). We did not exclude any articles due to their study design (i.e., controlled intervention studies, observational cohort and cross-sectional studies, case–control studies, before-after with no control studies and case series studies). Consequently, the Study Quality Assessment Tool that was developed by the National Heart, Lung and Blood Institute (70) was employed.
As can be observed in Figure 1, a total of 3,839 records were identified from electronic searches on databases and additional searches on references of systematic reviews. Of those, 2,117 were kept after eliminating duplicated records. In the first phase of screening, 2000 were excluded looking at title and abstract; the most frequent exclusion criteria were a psychological intervention was not provided (n = 804) or the target intervention did not include COVID-19 patients (n = 858). In the second phase, a total of 117 full-text articles were assessed for eligibility and only 43 were included in this review for synthesis. Agreement between the two independent researchers in the selection of the studies was 98% (Cohen’s k = 0.75, substantial agreement).
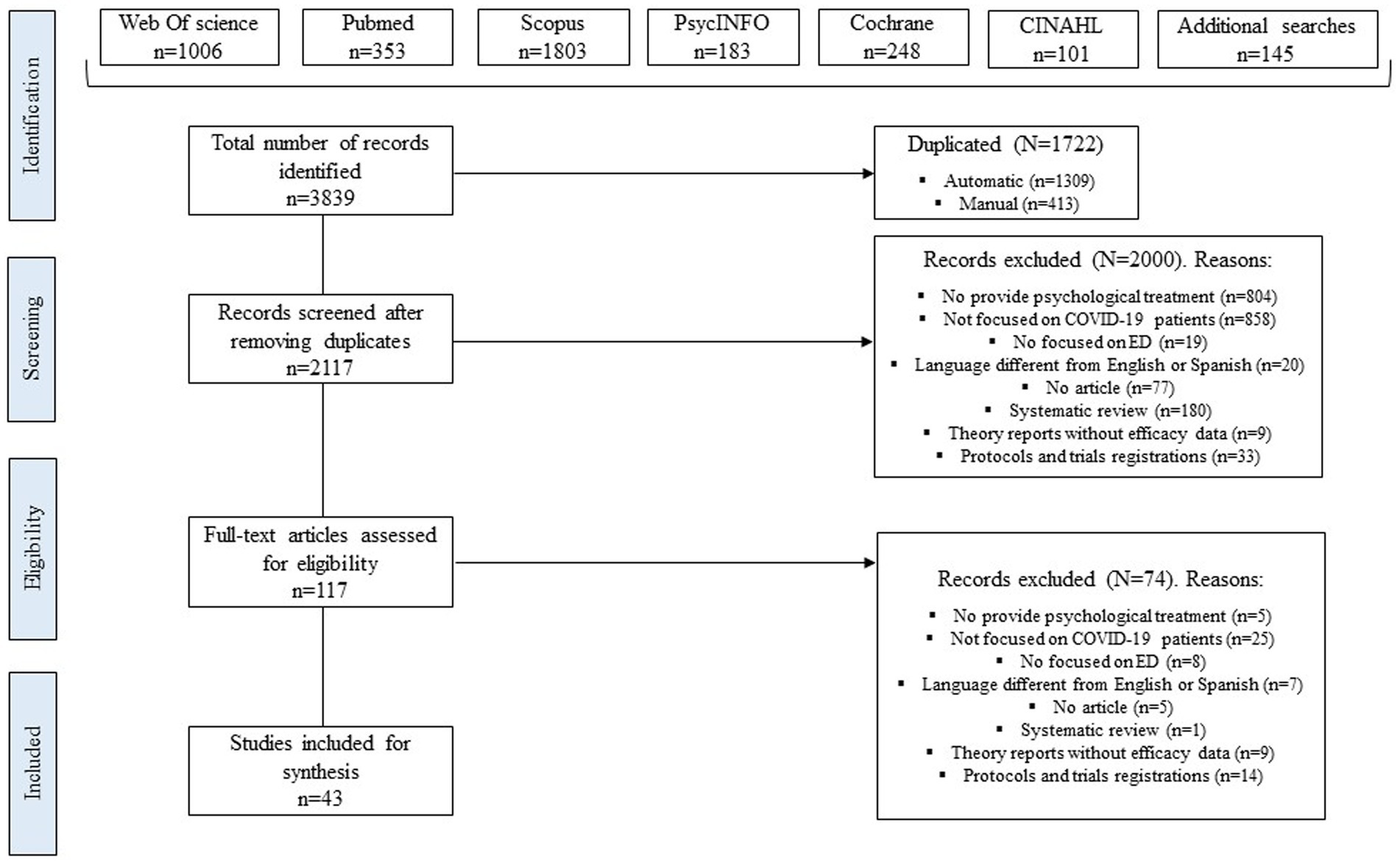
Figure 1. PRISMA flow diagram of included studies (23).
Characteristics of the 43 scientific studies included in this systematic review are reported in Table 1 (case studies) and Table 2 (intervention studies with and without control group). Sample size in the different studies ranged from 1 to 569. Across all the studies, a total of 2,359 participants were included. With regard to the age of participants, it ranged from 20 to 72 years old. Some studies (n = 6) did not provide participant’ age information (33, 50, 52, 63, 64, 66).
Most of the studies had been conducted in China (n = 15) (30, 33, 34, 45, 50, 52–55, 63, 64, 66–69), Iran (n = 6) (38, 47, 48, 58, 61, 62), Italy (n = 5) (29, 31, 41, 44, 57), India (n = 4) (36, 46, 56, 59), United States (n = 2) (28, 35), and Korea (n = 2) (49, 65). The remaining studies had been developed in Saudi Arabia (n = 1) (27), Nigeria (n = 1) (32), Indonesia (n = 1) (39), France (n = 1) (42), Turkey (n = 1) (43), Thailand (n = 1) (51), Latvia (n = 1) (40), Ghana (n = 1) (37), and Poland (n = 1) (60).
With regard to study design, the most common study design was randomized controlled trials (n = 15) (43, 45, 47, 50, 52–56, 58, 60–62, 64, 69) followed by case studies (n = 14) (27–40). Other study designs included pre-post studies without control group (n = 9) (41, 42, 44, 49, 57, 59, 63, 65, 67) and non-randomized studies with control group (n = 5) (46, 48, 51, 66, 68).
In relation to COVID-19 characteristics, as presented in Tables 1, 2, out of the total 43 studies, only three studies (two case studies and one pre-post study without control group) included long COVID-19 patients (28, 40, 44) while the remaining investigations were focused on COVID-19 patients.
The difference in the severity of COVID-19 symptoms is clearly appreciated across the studies. On the one hand, some studies focused on mildly-affected patients, namely participants who had recovered from COVID-19 symptoms (n = 5) (31, 32, 38, 47, 59), who were asymptomatic (n = 2) (39, 56), presented mild COVID-19 symptoms (n = 2) (54, 55) or were out of hospital (n = 3) (48, 58, 61). On the other hand, other interventions had been provided to COVID-19 patients who were hospitalized in isolation wards (n = 20) (29, 30, 33–37, 43, 46, 49–53, 60, 63–66, 68) or patients with severe symptoms in Intensive Care Units (n = 3) (42, 66, 67). Additional researches recruited participants from various settings and with different levels of severity of COVID-19 symptoms (n = 3) (41, 45) or did not specify the severity of the COVID-19 symptoms (n = 3) (27, 57, 69).
Regarding emotional disorders or symptoms addressed, the vast majority of studies were focused on depressive symptoms alone (30) or combined with anxiety (n = 15) (33, 34, 40–42, 44, 47, 48, 50–52, 55–57, 60), panic attacks (n = 6) (59, 62, 64, 66–68), suicidal ideation or self-harming attempts (n = 2) (36, 37) or post-traumatic stress disorder (PTSD) (n = 1) (38). On the other hand, six studies were focused on patients who presented with anxiety symptoms alone (43, 46, 53, 54, 58, 61) or combined it with panic attacks (29, 35).
The remaining studies addressed panic attacks alone (63) or combined with PTSD (69), PTSD alone (28, 31, 45), or obsessive-compulsive disorder (OCD) (27). Finally, two studies included patients with more than two diagnoses, namely depression, anxiety, panic attacks and suicidal attempts (39), depression, anxiety and suicidal attempts (32, 49) or depression, anxiety and PTSD (65).
Different psychological approaches were employed to manage the aforementioned psychological issues. Some studies (n = 10) were based on cognitive and behavioral principles [CBT alone (27, 49, 52); CBT + eye movement desensitization and reprocessing (EMDR) (44); CBT + mindfulness (55); CBT + relaxation (67); Cognitive Processing (28); Behavioral Therapy (50); dialectical-behavioral therapy (DBT) (34, 47)].
Other interventions had an interpersonal / relation approach (n = 4) [Interpersonal Therapy (33); emotion focused therapy based on interpersonal relationships (38, 41); relational intervention (57)]. Additional interventions included relaxation alone (n = 3) (53, 62, 66) or combined with mindfulness (64). Three studies used breathing techniques as the main component (29, 43, 56) while six interventions were based on providing psychoeducation, social support and additional relaxation and meditation techniques (46, 51, 54, 59, 61, 68).
The interventions with less representation were those based on music therapy (39, 40); compassion (48); positive psychology with hypnosis and Ericksonian principles (60, 69), narrative exposure therapy (45), EMDR (31, 42) and imagination (58). Four case studies (30, 32, 35, 36) and two pre-post studies without control group (63, 65) did not provide information about the type of psychotherapy that was applied. One study (37) described two different psychological programs, one of them based on CBT and the other focused on social support, positive recovery and relaxation training.
In terms of programs’ length, as shown in Tables 1, 2, short and long interventions were used. Some programs were implemented in only 1–5 sessions (33, 34, 39, 42, 53, 62) while others lasted 8–12 sessions (28, 31, 41, 45, 47, 48, 50) or had over 16 appointments (29, 57). The frequency of sessions also showed great variability. Some studies offered daily (36, 43, 52, 61) or weekly sessions (28, 31) while others proposed 2–3 sessions per week (44, 48, 57, 67). Again, some inconclusive results were found in the sessions duration, which ranged from 5–10 min (46, 47, 55, 56) to 60–90 min (44, 45, 48) (Tables 1, 2).
With regards to the format, some interventions had face-to-face appointments (47, 48, 52, 66) sometimes combined with online sessions (67). Other interventions used technology to provide the entire intervention. For example, seven studies used computerized programs which required the use of Internet-based solutions (45, 55, 57, 64) or videoconferencing (29, 36, 41). Four programs used group social messaging platforms (51, 54, 61, 68) and three studies used phone calls (35, 49, 65). Finally, some interventions were supported by the use of videos and audios (43, 56, 58, 66).
Different measures were used across studies to assess changes in psychological outcomes after the intervention. Instruments used to assess depressive symptoms included the PHQ (28, 29, 33, 40, 41, 64–67), HAMD-D (33, 34, 55, 64), the BDI (38, 47–49, 57), the HADS-D (42, 49, 50), the SDS (44, 45, 69) and the MADRS (34). Similarly, seven different instruments were used to assess anxiety symptoms, namely, HAMA (33, 34, 55, 57, 64), GAD (28, 29, 41, 46, 64–67), HADS-A (42, 49, 50, 60, 68), STAI (53, 54, 58, 61), BAI (43, 47, 48, 61), and SAS (44, 45, 63, 69). As can be seen in Table 2, some authors assessed both anxiety and depressive symptoms with two different instruments while others selected one isolated measure, such as the DASS, the SCL-90-R or the Mental Health Inventory, which includes the assessment of multiple outcomes (51, 52, 56, 57, 59, 62, 65).
Another outcome that was assessed in various studies was insomnia with instruments as the PQSI (45, 54, 66, 67), SRSS (53, 67), ISI (29, 49), AIS (55), ESS (57) or ad hoc questions (56). Additional outcomes assessed were posttraumatic symptoms (PCL-C) (28, 38, 45, 65), quality of life (WHOQOL) (43, 60, 62), social support (PSSS) (50), affect (PANAS) (68), and coping (Coping Modes questionnaire) (68). It is also remarkable that only one study used a COVID-19 specific measure, namely the MAC-RF, to assess COVID fears (42). The rest of the studies used clinical interviews (30, 32, 35), or did not inform about how they conducted the formal assessments (27, 36, 39).
Case studies found inconclusive results related to the intervention’s efficacy. Most case studies reported a reduction after the intervention on outcomes such as intrusive thoughts (27), post-traumatic symptoms (28, 31, 38), anxiety (28, 33–35, 37–40), depression (28, 33, 34, 37–39), general clinical symptoms (30, 32), suicidal ideation (36) and insomnia (39). However, some studies did not indicate the cut-off selected to establish the recovery of symptoms and no size effect or significance of change was calculated. Consequently, out of 14 case studies, only 4 interventions based on CBT components as well as interpersonal relationships actually reported a total recovery of post-traumatic, anxiety and depressive symptoms (28, 33, 34, 38).
Along the same lines, controlled and non-controlled interventions showed a reduction in anxiety, depression, insomnia, stress, PTSD and COVID-19 fears (Table 2). However, a total recovery of symptoms was only reported in 13 out of the 29 studies. More precisely, a total recovery from anxiety symptoms was found in two studies (51, 53), recovery from COVID-19 fears was found in one study (42) and a total recovery from insomnia was found in one study (54). With regard to total recovery on multiple outcomes, complete disappearance of anxiety and depression was found in three studies (41, 50, 60). Two studies found a total recovery from symptoms of depression and PTSD (45) or depression and stress (52). Additionally, total recovery from three symptoms (anxiety, depression and insomnia/stress) was found in four studies (56, 57, 66, 67).
As showed in Supplementary material D, the quality of case series studies was generally low (eight studies obtained 2 points out of 7 and two studies obtained 4 points). Only four studies could be classified as “good” (scores of 5–6 out of 9 points). For case studies rated as “poor,” the most important issues were related to the lack of information about the psychological intervention that was provided and not using valid and reliable measures. Other items that failed in almost all interventions were lack of follow-up assessments, not reporting statistical methods and poor results reports.
Supplementary material E shows the analyses of study quality for pre-post interventions without control group. All studies obtained scores from 4 to 7 points (out of 12 points) which may be interpreted as “fair” quality. The items that are more worrisome are item 4 (enrollment of potential participants), item 5 (sample size justification), item 6 (definition of the intervention), item 8 (blinded assessments), item 9 (dropouts) and item 11 (length of follow-up).
In third place, we analyzed randomized controlled trials. As shown in Supplementary material F, nine studies obtained scores of up to 7 points (out of 14) which could be interpreted as being “poor” quality studies. Another six studies were classified as “fair” studies because their total scores oscillated between 9 and 11 points. Just one study obtained 12 points, which indicated a “good” quality study. In general terms, RCT failed to provide proper information about participants and providers blinding to allocation, blinded assessments, adherence rates and pre-specified hypothesis.
The remaining five studies were non-randomized controlled interventions with control group. Although scores ranged from 6 to 8 points (out of 14), we considered that these interventions were of “good” quality because some items referred specifically to randomized studies (items 1–5). As these interventions were not described as randomized control trials, in most cases it was not possible to determine whether allocation and assessments were blinded. Additional shortcomings with these interventions were lack of information about adherence rates, sample size justification and lack of pre-specified hypothesis (Supplementary material G).
Coping with the physical and social consequences of the pandemics was a great challenge for the entire population (71), and especially for those suffering from COVID-19 or long COVID-19 conditions (7, 12). This resulted in the emergence of psychological interventions to alleviate the psychological impact of the pandemic (18). The main aim of this systematic review was to summarize and analyze the psychological interventions that are available for patients suffering any kind of COVID-19 conditions and comorbid emotional disorders. This study provides results from 43 studies including 2,359 participants.
Due to the magnitude of the COVID-19 pandemic, several economic investments have been executed (72) specially in developed countries. However, as stated in previous lines, only 26% of studies included in this review have been developed in western countries. It seems that, despite the availability of economic resources and although we already have psychological interventions available to be provided for health conditions (73, 74), research efforts are not reaching the entire globe and psychological interventions are not yet equally distributed. We expect that future research will allow psychological interventions to be implemented in different countries and cultures and reach all COVID-19 patients who need it.
Another important finding from this systematic review is that almost all psychological interventions were provided to COVID-19 patients and only 3 studies were focused on post COVID-19 or long COVID-19 populations. This contrasts with the high prevalence of long COVID-19 syndrome and the negative consequences of not caring for this population. Scientific evidence highlights that around 10–20% of COVID-19 patients might develop long COVID-19 (75) and, what is more important, it seems that post COVID-19 patients are at risk of emotional suffering and suicide (76). Fortunately, it seems that programs addressing physical and psychological issues may reduce the emotional suffering and the risk of suicide in post COVID-19 patients (76). Taking this into account, future psychological interventions should specifically include post COVID-19 patients and analyze whether the same intervention could be applied to all COVID-19 patients irrespective of the duration of the COVID-19 symptoms.
With respect to COVID-19 severity, we found in our systematic review that investigations included very heterogeneous participants, from asymptomatic to patients with severe COVID-19 symptoms. It has been postulated that length of hospitalization and severity of COVID-19 symptoms are associated with reduced quality of life (77) so there is no doubt that, if possible, psychological interventions should be provided during and after discharge. However, patients with mild but chronic physical symptoms may also experience an impact on their quality of life, especially those with pulmonary affections (78) so we propose that all COVID-19 patients should be offered both preventive psychological interventions and psychological treatment. As length and duration of sessions was not clearly established across interventions, a stepped model of care (79, 80) could serve to determine the dosage, length and format of delivery for each patient.
In relation to the delivery format, the COVID-19 pandemic has evidenced that current mental health services are insufficient to care for all people who suffer emotional disorders and has provided an opportunity to implement new models of care (81). Furthermore, the mobility restrictions and lockdowns associated with the pandemic impeded the provision of face-to-face sessions, which also favored the development of new models of care. These facts were clearly observed in our systematic review by the great number of interventions that used technology both as the main format of delivery or as a complement to onsite sessions. We strongly believe that the use of audio-visual content, which is usually requested by patients and professionals (82), could be extremely beneficial for COVID-19 patients because they usually present with memory and attentional deficits (83). In this sense, technology-based psychological interventions help to provide audio-visual content that could be always accessible (84). It facilitates the access of participants to the intervention whenever they need it, patients are able to review and repeat the content, which may in turn result in higher skills acquisition (85). Another important outcome from our work is that different questionnaires were employed to assess emotional disorders in COVID-19 patients. Most of the studies used well established instruments designed for general populations (i.e., PHQ, BAI, GAD, SDS). Nonetheless, it has also been claimed there is a need to select the most appropriate questionnaire according to the specific circumstances of the participants who are being evaluated (86). Consequently, during the pandemic, enormous effort were carried out to develop COVID-19 specific measures (87). We need to consider that some physical symptoms of COVID-19 and long COVID-19 conditions include loss of attention, confusion, fatigue, difficulties in taking decisions or insomnia due to pain (88). These symptoms usually overlap with the main criteria used to diagnose anxiety and depressive symptoms (89). Future research should consider whether the use of general questionnaires may result in an over diagnosis of emotional disorders in COVID-19 populations and if we need to conduct separate and extensive assessments including cognitive-specific measures and psychological in-depth interviews.
The aforementioned assessments allow researchers to evaluate the efficacy of the interventions. Different therapies, such as CBT, interpersonal psychotherapy, positive psychology and mind–body approaches, have been proposed to address emotional disorders in COVID-19 patients. Our results indicated that, in general terms, a reduction in emotional disorders is found after psychological interventions. It is remarkable that RCTs based on CBT seem to be one of the most convenient interventions for the reduction of emotional suffering in COVID-19 patients, demonstrated by the efficacy rates and the low risk of bias of these studies. While acknowledging this valuable information, these results may be interpreted with caution as several limitations have been detected in this review. First, only 43 studies have been conducted since the onset of the pandemic, and few countries are represented in those studies, which may compromise generalization of findings. Second, most studies found only a partial recovery of symptoms and it is difficult to establish if emotional recovery is attributable to the psychological intervention itself or to a recovery from the COVID-19 physical symptoms. Third, there is a lack of well-designed and rigorous RCT and, as indicated by our risk of bias analyses, a worrisome percentage of studies did not provide enough information about the intervention that was provided, especially in case studies. Another shortcoming with psychological interventions is their insufficient length (sometimes programs were based on only one session), the lack of proper follow-up assessments (which may help to determine whether the improvement achieved disappeared with time or if the improvements were maintained), the inadequate assessment protocols and the lack of transdiagnostic approaches that allow to address the factors contributing to the development and maintenance of emotional disorders (90).
In this sense, it is remarkable that none of the aforementioned interventions proposed the implementation of a transdiagnostic psychological intervention (91). Given that comorbidity between anxiety and depression is highly frequent in COVID-19 patients (92), we postulate the need to develop and implement transdiagnostic CBT interventions. These interventions target etiological and maintenance factors shared by distinct emotional disorders (90) instead of focusing on specific symptoms (e.g., the Unified Protocol for transdiagnostic treatment of emotional disorders) (93). In recent years, different systematic reviews and meta-analysis have been published regarding their efficacy when applied to individuals with emotional disorders (94) and it has also been applied recently with encouraging results to individuals with comorbid emotional disorders and health conditions, including people with long COVID-19 (95). Transdiagnostic psychological treatments have multiple advantages, for example, clinicians can use one single treatment protocol for a variety of emotional disorders and comorbid cases, thus it is easier to train clinicians and to disseminate evidence-based psychological treatments (96). Finally, another advantage is the possibility to deliverer it in cost-effective formats such as group or technology-based interventions (97).
Arguments shown in this work may help to understand current practices in the context of COVID-19 patients and may help to expand the field of research. However, this work is not exempt from some limitations. First, systematic reviews usually present potential risk of bias (selection, attrition, interpretation of results etc.) (98). Although we have followed PRISMA recommendations, have pre-registered our work in PROSPERO and have included two independent researchers across all the process, it is possible that some biases are still present. Second, our objective was to summarize psychological interventions in the context of COVID-19 patients and we did not exclude any study due to their quality. As a result, some studies included in this review were rated as “poor” or “fair” quality. Related with this, although some studies included in this review (n = 9) administered pharmacotherapy (i.e., antidepressants), none of them conducted statistical analyses comparing participants which were taking pharmacotherapy with psychotherapy and those that received only psychotherapy. Thus we can not determine the independent percentage of change attributable to each of these two treatments (e.g., psychotherapy and pharmacotherapy). Future studies administering drugs should include formal analyses comparing populations with and without pharmacotherapy prescription to obtain more reliable results. Third, we have not included study protocols nor registers in clinicaltrials.gov as previous reviews did (99) so it is possible that some psychological interventions which are currently being implemented, especially in long COVID-19 patients, were not included in our review. Finally, due to the heterogeneity in the studies, it was not possible to conduct a meta-analysis which could facilitate generalization and comparison of results.
Despite these limitations, this systematic review could be useful both for researchers and clinical practice by providing an overview of current psychological interventions for COVID-19 patients. According to our results, future interventions should include long COVID-19 participants, offer preventive and treatment protocols to all COVID-19 patients, use more sophisticated research designs, propose transdiagnostic interventions with long-term follow-ups, explore which are the best assessment protocols and use cost-effective formats (i.e., group and self-administered interventions based on the use of technologies).
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
VM-B: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft. LM-G: Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft. ÓP-B: Investigation, Writing – original draft. JO: Conceptualization, Data curation, Funding acquisition, Methodology, Project administration, Supervision, Writing – review & editing. EC-B: Funding acquisition, Project administration, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by Autonomous Government of Aragón (Departamento de Ciencia, Universidad y Sociedad del Conocimiento, [research group grant S31_23R]). The study is funded by Solutex GC S.L. “Call for industrial research business projects linked to the pharmaceutical sector” (idmf7202170008). The sponsors had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1305463/full#supplementary-material
1. World Health Orgnization [WHO]. WHO coronavirus disease (COVID-19) dashboard. WHO Heal Emerg Dashboard (2023)
2. Chilamakuri, R, and Agarwal, S. COVID-19: characteristics and therapeutics. Cells. (2021) 10:206. doi: 10.3390/cells10020206
3. al Maqbali, M, al badi, K, al Sinani, M, Madkhali, N, and Dickens, GL. Clinical features of COVID-19 patients in the first year of pandemic: a systematic review and Meta-analysis. Biol Res Nurs. (2022) 24:172–85. doi: 10.1177/10998004211055866
4. World Health Organization [WHO]. WHO coronavirus (COVID-19) dashboard. Glob Situat (2023) Available at: https://covid19.who.int/?mapFilter=deaths (Accessed July 25, 2023)
5. World Health Orgnization [WHO]. COVID-19: Clinical care. A Clin case Defin post COVID-19 Cond by a Delphi consensus, 6 Oct 2021 (2021) Available at: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (Accessed July 25, 2023)
6. Mehandru, S, and Merad, M. Pathological sequelae of long-haul COVID. Nat Immunol. (2022) 23:194–202. doi: 10.1038/s41590-021-01104-y
7. Vindegaard, N, and Benros, ME. COVID-19 pandemic and mental health consequences: systematic review of the current evidence. Brain Behav Immun. (2020) 89:531–42. doi: 10.1016/j.bbi.2020.05.048
8. Tang, F, Liang, J, Zhang, H, Kelifa, MM, He, Q, and Wang, P. COVID-19 related depression and anxiety among quarantined respondents. Psychol Health. (2021) 36:164–78. doi: 10.1080/08870446.2020.1782410
9. Ubillos-Landa, S, Puente-Martínez, A, and González-Castro, JL. Psychological withdrawal and mental health during the COVID-19 pandemic: a longitudinal study. Psychol Health. (2023) 38:1361–77. doi: 10.1080/08870446.2021.2019254
10. Morris, SG, Kudrna, L, and Martin, J. Mental health and life satisfaction among those advised to shield during the COVID-19 pandemic in the UK: a secondary analysis of the understanding society longitudinal study. Front Public Health. (2023) 11:1235903. doi: 10.3389/fpubh.2023.1235903
11. Barbalat, G, Tanguy Melac, A, Zante, E, Haesebaert, F, and Franck, N. Predictors of mental well-being over the first lockdown period due to the COVID-19 pandemic in France. A repeated cross-sectional study. Front Public Health. (2023) 11:1234023. doi: 10.3389/fpubh.2023.1234023
12. Khraisat, B, Toubasi, A, AlZoubi, L, Al-Sayegh, T, and Mansour, A. Meta-analysis of prevalence: the psychological sequelae among COVID-19 survivors. Int J Psychiatry Clin Pract. (2022) 26:234–43. doi: 10.1080/13651501.2021.1993924
13. Amin, S, Mehmood, W, Aman-Ullah, A, and Khan, MA. Corona-phobia violated human rights? Impact of COVID-19 on patient’s well-being. Int J Hum Rights Healthc. (2022). doi: 10.1108/IJHRH-05-2022-0048 [Epubh ahead of print].
14. O’Brien, H, Tracey, MJ, Ottewill, C, O’Brien, ME, Morgan, RK, Costello, RW, et al. An integrated multidisciplinary model of COVID-19 recovery care. Ir J Med Sci. (2021) 190:461–8. doi: 10.1007/s11845-020-02354-9
15. Wen, W, Chen, C, Tang, J, Wang, C, Zhou, M, Cheng, Y, et al. Efficacy and safety of three new oral antiviral treatment (molnupiravir, fluvoxamine and Paxlovid) for COVID-19:a meta-analysis. Ann Med. (2022) 54:516–23. doi: 10.1080/07853890.2022.2034936
16. Xavier-Santos, D, Padilha, M, Fabiano, GA, Vinderola, G, Gomes Cruz, A, Sivieri, K, et al. Evidences and perspectives of the use of probiotics, prebiotics, synbiotics, and postbiotics as adjuvants for prevention and treatment of COVID-19: a bibliometric analysis and systematic review. Trends Food Sci Technol. (2022) 120:174–92. doi: 10.1016/j.tifs.2021.12.033
17. Décary, S, De Groote, W, Arienti, C, Kiekens, C, Boldrini, P, Giuseppe Lazzarini, S, et al. Scoping review of rehabilitation care models for post COVID-19 condition. Bull World Health Organ. (2022) 100:676–88. doi: 10.2471/BLT.22.288105
18. Rahmati, F, and Khalili, R. Investigating the effectiveness of psychological interventions in response to stress, anxiety, and depression in coronavirus disease 2019 patients: a systematic review. J Educ Health Promot. (2022) 11:203–6. doi: 10.4103/jehp.jehp_923_21
19. Tasleem, A, Wang, Y, Li, K, Jiang, X, Krishnan, A, He, C, et al. Effects of mental health interventions among people hospitalized with COVID-19 infection: a systematic review of randomized controlled trials. Gen Hosp Psychiatry. (2022) 77:40–68. doi: 10.1016/j.genhosppsych.2022.04.002
20. Komariah, M, Amirah, S, Faisal, EG, Prayogo, SA, Maulana, S, Platini, H, et al. Efficacy of internet-based cognitive behavioral therapy for depression and anxiety among global population during the COVID-19 pandemic: a systematic review and meta-analysis of a randomized controlled trial study. Healthcare. (2022) 10:1224. doi: 10.3390/healthcare10071224
21. Chennapragada, L, Sullivan, SR, Hamerling-Potts, KK, Tran, H, Szeszko, J, Wrobleski, J, et al. International PRISMA scoping review to understand mental health interventions for depression in COVID-19 patients. Psychiatry Res. (2022) 316:114748. doi: 10.1016/j.psychres.2022.114748
22. Safieh, J, Broughan, J, McCombe, G, McCarthy, N, Frawley, T, Guerandel, A, et al. Interventions to optimise mental health outcomes during the COVID-19 pandemic: a scoping review. Int J Ment Health Addict. (2022) 20:2934–55. doi: 10.1007/s11469-021-00558-3
23. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. PLoS Med. (2021) 18:e1003583. doi: 10.1371/journal.pmed.1003583
25. Ouzzani, M, Hammady, H, Fedorowicz, Z, and Elmagarmid, A. Rayyan – a web and mobile app for systematic reviews. Syst Rev. (2016) 5:210. doi: 10.1186/s13643-016-0384-4
26. Li, T, Higgins, J, and Deeks, J. Collecting data In: J Higgins, J Thomas, J Chandler, M Cumpston, T Li, M Page, and V Welch, editors. Cochrane handbook for systematic reviews of interventions version 6.3. London: Cochrane (2022)
27. Alkhamees, AA. Obsessive–compulsive disorder post-COVID-19: A case presentation. Egypt J Neurol Psychiatr Neurosurg. (2021) 57:1–3. doi: 10.1186/s41983-021-00405-1
28. Bogucki, OE, and Sawchuk, CN. Cognitive processing therapy for posttraumatic stress disorder due to COVID-19-related traumas: a case study. Psychol Serv. (2022) 20:533–7. doi: 10.1037/ser0000630
29. Callus, E. Provision of psychological support to a 31-year-old man with SARS-CoV2-induced pneumonia during and after hospitalization: a clinical case report. Int J Environ Res Public Health. (2023) 20:757. doi: 10.3390/ijerph20010757
30. Chen, J, Tian, C, Cheng, X, Huang, Y, Tang, L, Wang, R, et al. A case of coronvirus disease 2019 with psychological disorders. Psychiatr Danub. (2020) 32:581–3. doi: 10.24869/psyd.2020.581
31. Dinapoli, L, Ferrarese, D, Belella, D, Carnevale, S, Camardese, G, Sani, G, et al. Psychological treatment of traumatic memories in COVID-19 survivors. Clin Psychol Psychother. (2023) 30:225–33. doi: 10.1002/cpp.2771
32. Edet, BE, Essien, EA, Ugobo, MB, Okafor, CJ, Olose, EO, and Essien, VA. Depression and suicidality in a COVID-19 patient: a case report from Calabar, Nigeria. West Afr J Med. (2022) 39:548–51.
33. Hu, C-C, Huang, J-W, Wei, N, Hu, S-H, Hu, J-B, Li, S-G, et al. Interpersonal psychotherapy-based psychological intervention for patient suffering from COVID-19: a case report. World J Clin Cases. (2020) 8:6064–70. doi: 10.12998/wjcc.v8.i23.6064
34. Huang, J-W, Zhou, X-Y, Lu, S-J, Xu, Y, Hu, J-B, Huang, M-L, et al. Dialectical behavior therapy-based psychological intervention for woman in late pregnancy and early postpartum suffering from COVID-19: a case report. J Zhejiang Univ Sci B. (2020) 21:394–9. doi: 10.1631/jzus.B2010012
35. Khawam, E, Khouli, H, and Pozuelo, L. Treating acute anxiety in patients with COVID-19. Cleve Clin J Med. (2020). doi: 10.3949/ccjm.87a.ccc016 [Epubh ahead of print].
36. Naskar, C, Grover, S, Sahoo, S, and Mehra, A. Managing a COVID-positive health-care worker with recent suicide attempt through telepsychiatry. Ann Indian Psychiatry. (2022) 6:99–101. doi: 10.4103/aip.aip_4_21
37. Nuertey, BD, Mumuni, K, Addai, J, Kunfah, S, Attibu, RI, Acquah, D, et al. Attempted suicide of two confirmed SARS-CoV-2 infected patients in an isolation facility and recommendations to prevent COVID-19 suicides: a case report. Pan Afr Med J. (2022) 41:245. doi: 10.11604/pamj.2022.41.245.29660
38. Sadeghi, M, Moradi, Z, and Ershadi, F. The clinical trial of COVID-19 patients: the effectiveness of emotion-focused therapy on post-traumatic stress and depression. Iran Red Crescent Med J. (2021) 23:e998. doi: 10.32592/ircmj.2021.23.10.998
39. Situmorang, DDB. “When the first session may be the last!”: a case report of the implementation of “rapid tele-psychotherapy” with single-session music therapy in the COVID-19 outbreak. Palliat Support Care. (2022) 20:290–5. doi: 10.1017/S1478951521001425
40. Taube, M. Depression and brain fog as long-COVID mental health consequences: difficult, complex and partially successful treatment of a 72-year-old patient—a case report. Front Psychiatry. (2023) 14:1153512. doi: 10.3389/fpsyt.2023.1153512
41. Biagianti, B, Lisi, I, Di Liberto, A, Turtulici, N, Foti, G, Zito, S, et al. Feasibility and preliminary efficacy of brief tele-psychotherapy for COVID-19 patients and their first-degree relatives. J Affect Disord. (2023) 330:300–8. doi: 10.1016/j.jad.2023.03.024
42. Brennstuhl, M-J, Pascale, T, Ann, RJ, Louise, TC, Lydia, P, Christine, R, et al. Treating COVID-19 patients with EMDR: a pilot study. Eur J Trauma Dissociation. (2022) 6:100276. doi: 10.1016/j.ejtd.2022.100276
43. Öner Cengiz, H, Ayhan, M, and Güner, R. Effect of deep breathing exercise with Triflo on dyspnoea, anxiety and quality of life in patients receiving covid-19 treatment: a randomized controlled trial. J Clin Nurs. (2021) 31:3439–53. doi: 10.1111/jocn.16171
44. Compagno, S, Palermi, S, Pescatore, V, Brugin, E, Sarto, M, Marin, R, et al. Physical and psychological reconditioning in long COVID syndrome: Results of an out-of-hospital exercise and psychological-based rehabilitation program. Int J Cardiol Heart Vasc. (2022) 41:101080. doi: 10.1016/j.ijcha.2022.101080
45. Fan, Y, Shi, Y, Zhang, J, Sun, D, Wang, X, Fu, G, et al. The effects of narrative exposure therapy on COVID-19 patients with post-traumatic stress symptoms: a randomized controlled trial. J Affect Disord. (2021) 293:141–7. doi: 10.1016/j.jad.2021.06.019
46. Ganesan, S, Balasubramanian, B, Krishnamurthy, P, Govindan, R, and Mani, N. Effects of tele-counseling on reducing anxiety levels of COVID-19 patients in isolation wards: an observational study. Indian J Psychol Med. (2023) 45:43–6. doi: 10.1177/02537176221139598
47. Torbati, AG, Imeni, M, and Abbaspour, S. Impact of dialectical behavior therapy on depression and anxiety in patients following COVID-19 discharge. Open Psychol J. (2022) 16:1–7. doi: 10.2174/18743501-v16-e2208191
48. Ghodrati-Torbati, AG, Abbaspour, S, and Zandi, A. Efficacy of psychoeducational intervention on depression and anxiety after discharge in patients with covid-19. J Public Health Dev. (2022) 20:209–20. doi: 10.55131/jphd/2022/200317
49. Kim, J-W, Stewart, R, Kang, S-J, Jung, S-I, Kim, S-W, and Kim, J-M. Telephone based interventions for psychological problems in hospital isolated patients with COVID-19. Clin Psychopharmacol Neurosci. (2020) 18:616–20. doi: 10.9758/cpn.2020.18.4.616
50. Kong, X, Kong, F, Zheng, K, Tang, M, Chen, Y, Zhou, J, et al. Effect of psychological–behavioral intervention on the depression and anxiety of COVID-19 patients. Front Psychiatry. (2020) 11:586355. doi: 10.3389/fpsyt.2020.586355
51. Lerthattasilp, T, Kosulwit, L, Phanasathit, M, Nuallaong, W, Tapanadechopone, P, Thanetnit, C, et al. Effect of an online psychological support group on patients with COVID-19 in a Thai field hospital: a real world study. J Health Res. (2021) 36:1040–6. doi: 10.1108/JHR-01-2021-0044
52. Li, J, Li, X, Jiang, J, Xu, X, Wu, J, Xu, Y, et al. The effect of cognitive behavioral therapy on depression, anxiety, and stress in patients with COVID-19: a randomized controlled trial. Front Psychiatry. (2020) 11:580827. doi: 10.3389/fpsyt.2020.580827
53. Liu, K, Chen, Y, Wu, D, Lin, R, Wang, Z, and Pan, L. Effects of progressive muscle relaxation on anxiety and sleep quality in patients with COVID-19. Complement Ther Clin Pract. (2020) 39:101132. doi: 10.1016/j.ctcp.2020.101132
54. Liu, Y, Yang, Y-Q, Liu, YY, Pei, S-L, Yang, H-H, Wu, J-J, et al. Effects of group psychological intervention combined with pulmonary rehabilitation exercises on anxiety and sleep disorders in patients with mild coronavirus disease 2019 (COVID-19) infections in a Fangcang hospital. Psychol Health Med. (2021) 27:333–42. doi: 10.1080/13548506.2021.1916956
55. Liu, Z, Qiao, D, Xu, Y, Zhao, W, Yang, Y, Wen, D, et al. The efficacy of computerized cognitive behavioral therapy for depressive and anxiety symptoms in patients with COVID-19: randomized controlled trial. J Med Internet Res. (2021) 23:e26883. doi: 10.2196/26883
56. Mahendru, K, Pandit, A, Singh, V, Choudhary, N, Mohan, A, and Bhatnagar, S. Effect of meditation and breathing exercises on the well-being of patients with SARS-CoV-2 infection under institutional isolation: a randomized control trial. Indian J Palliat Care. (2021) 27:490–4. doi: 10.25259/IJPC_40_21
57. Maresca, G, Formica, C, De Cola, MC, Lo Buono, V, Latella, D, Cimino, V, et al. Care models for mental health in a population of patients affected by COVID-19. J Int Med Res. (2022) 50:030006052210974. doi: 10.1177/03000605221097478
58. Parizad, N, Goli, R, Faraji, N, Mam-Qaderi, M, Mirzaee, R, Gharebaghi, N, et al. Effect of guided imagery on anxiety, muscle pain, and vital signs in patients with COVID-19: a randomized controlled trial. Complement Ther Clin Pract. (2021) 43:101335. doi: 10.1016/j.ctcp.2021.101335
59. Priyamvada, R, Ranjan, R, and Chaudhury, S. Efficacy of psychological intervention in patients with post-COVID-19 anxiety. Ind Psychiatry J. (2021) 30:41–S44. doi: 10.4103/0972-6748.328787
60. Rutkowski, S, Bogacz, K, Czech, O, Rutkowska, A, and Szczegielniak, J. Effectiveness of an inpatient virtual reality-based pulmonary rehabilitation program among COVID-19 patients on symptoms of anxiety, depression and quality of life: preliminary results from a randomized controlled trial. Int J Environ Res Public Health. (2022) 19:16980. doi: 10.3390/ijerph192416980
61. Shaygan, M, Yazdani, Z, and Rambod, M. The effect of interactive virtual psycho-educational interventions via social networks on self-efficacy and anxiety among patients infected with COVID-19 and living in home quarantine: a randomized control trial. Iran J Nurs Midwifery Res. (2023) 28:65–71. doi: 10.4103/ijnmr.ijnmr_451_21
62. Sotoudeh, HG, Alavi, SS, Akbari, Z, Jannatifard, F, and Artounian, V. The effect of brief crisis intervention package on improving quality of life and mental health in patients with COVID-19. Iran J Psychiatry. (2020) 15:205–12. doi: 10.18502/ijps.v15i3.3812
63. Sun, P, Fan, D-J, He, T, Li, H-Z, Wang, G, Zhang, X-Z, et al. The effects of psychological intervention on anxiety symptoms of COVID19-positive patients isolated in hospital wards. Eur Rev Med Pharmacol Sci. (2021) 25:498–502. doi: 10.26355/eurrev_202101_24421
64. Wei, N, Huang, B, Lu, SJ, Hu, JB, Zhou, XY, Hu, CC, et al. Efficacy of internet-based integrated intervention on depression and anxiety symptoms in patients with COVID-19. J Zhejiang Univ Sci B. (2020) 21:400–4. doi: 10.1631/jzus.B2010013
65. Won, G, Lee, HJ, Lee, JH, Choi, TY, Hong, H-L, and Jung, CY. Impact of a psychiatric consultation program on COVID-19 patients: an experimental study. Psychiatry Investig. (2023) 20:471–80. doi: 10.30773/pi.2022.0295
66. Xiao, CX, Lin, YJ, Lin, RQ, Liu, AN, Zhong, GQ, and Lan, CF. Effects of progressive muscle relaxation training on negative emotions and sleep quality in COVID-19 patients: a clinical observational study. Medicine (Baltimore). (2020) 99:e23185. doi: 10.1097/MD.0000000000023185
67. Yang, X, Yang, X, Kumar, P, Cao, B, Ma, X, and Li, T. Social support and clinical improvement in COVID-19 positive patients in China. Nurs Outlook. (2020) 68:830–7. doi: 10.1016/j.outlook.2020.08.008
68. Yuan, L-P, Yu, Z-H, Zhang, X-C, Zhang, W, Jin, L-L, Wang, Z, et al. The psychological effect of forming WeChat groups between medical staff and patients with COVID-19. Front Public Health. (2021) 9:586465. doi: 10.3389/fpubh.2021.586465
69. Zheng, T, Lin, J, Tu, L, Hu, J, and Wei, W. Correlation analysis of positive therapy based on high content image analysis technology on posttraumatic nerve growth in patients with COVID-19 in the context of intelligent medical treatment. Contrast Media Mol Imaging. (2022) 2022:9165764. doi: 10.1155/2022/9165764
70. National Heart Lung and Blood Institute [NHLBI]. Study quality assessment tools. (2021) Available at: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (Accessed March 25, 2020)
71. Lin, C-C, and Yeh, C-B. Psychological impacts of COVID-19 pandemic. J Med Sci. (2023) 43:1. doi: 10.4103/jmedsci.jmedsci_269_21
72. European Commission. Cohesion policy action against coronavirus. Reg Policy Funding (2023) Available at: https://ec.europa.eu/regional_policy/funding/coronavirus-response_en (Accessed July 28, 2023).
73. Thompson, RD, Delaney, P, Flores, I, and Szigethy, E. Cognitive-behavioral therapy for children with comorbid physical illness. Child Adolesc Psychiatr Clin N Am. (2011) 20:329–48. doi: 10.1016/j.chc.2011.01.013
74. McCombie, A, Gearry, R, Andrews, J, Mikocka-Walus, A, and Mulder, R. Computerised cognitive behavioural therapy for psychological distress in patients with physical illnesses: a systematic review. J Clin Psychol Med Settings. (2015) 22:20–44. doi: 10.1007/s10880-015-9420-0
75. World Health Organization [WHO]. Post COVID-19 condition (long COVID). (2022) Available at: https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition (Accessed January 9, 2023)
76. Simonetti, A, Bernardi, E, Janiri, D, Mazza, M, Montanari, S, Catinari, A, et al. Suicide risk in post-COVID-19 syndrome. J Pers Med. (2022) 12:2019. doi: 10.3390/jpm12122019
77. Kaso, AW, Tesema, HG, Hareru, HE, Kaso, T, Ashuro, Z, Talemahu, AA, et al. Health-related quality of life and associated factors among Covid-19 survivors. Experience from Ethiopian treatment centers. Infect Drug Resist. (2022) 15:6143–53. doi: 10.2147/IDR.S386566
78. Siboni, F, Alimoradi, Z, Atashi, V, Alipour, M, and Khatooni, M. Quality of life in different chronic diseases and its related factors. Int J Prev Med. (2019) 10:65. doi: 10.4103/ijpvm.IJPVM_429_17
79. Bower, P, and Gilbody, S. Stepped care in psychological therapies: access, effectiveness and efficiency. Br J Psychiatry. (2005) 186:11–7. doi: 10.1192/bjp.186.1.11
80. Cross, S, and Hickie, I. Transdiagnostic stepped care in mental health. Public Health Res Pract. (2017) 27:27. doi: 10.17061/phrp2721712
81. Yang, X. The impact of COVID-19 on access to mental health services and the use of teletherapy as an alternative form of treatment. Arch Clin Psychiatry. (2022) 49:23–30. doi: 10.15761/0101-60830000000423
82. Osma, J, Martínez-García, L, Prado-Abril, J, Peris-Baquero, Ó, and González-Pérez, A. Developing a smartphone app based on the unified protocol for the transdiagnostic treatment of emotional disorders: a qualitative analysis of users and professionals’ perspectives. Internet Interv. (2022) 30:100577–7. doi: 10.1016/j.invent.2022.100577
83. Velichkovsky, BB, Razvaliaeva, AY, Khlebnikova, AA, Manukyan, PA, and Kasatkin, VN. Attention and memory after COVID-19 as measured by neuropsychological tests: systematic review and meta-analysis. Acta Psychol. (2023) 233:103838. doi: 10.1016/j.actpsy.2023.103838
84. Stoll, J, Müller, JA, and Trachsel, M. Ethical issues in online psychotherapy: a narrative review. Front Psychiatry. (2020) 10:993. doi: 10.3389/fpsyt.2019.00993
85. Hardenberg, J, Rana, I, and Tori, K. Evaluating impact of repeated exposure to high Fidelity simulation: skills acquisition and stress levels in postgraduate critical care nursing students. Clin Simul Nurs. (2020) 48:96–102. doi: 10.1016/j.ecns.2020.06.002
86. Institute of Medicine. Overview of psychological testing In: Psychological testing in the Service of Disability Determination. Committee on Psychological Testing, Including Validity Testing, for Social Security Administration Disability Determinations. Washington (DC): National Academies Press (US) (2015). doi: 10.17226/21704
87. Cortez, PA, Joseph, SJ, Das, N, Bhandari, SS, and Shoib, S. Tools to measure the psychological impact of the COVID-19 pandemic: what do we have in the platter? Asian J Psychiatr. (2020) 53:102371. doi: 10.1016/j.ajp.2020.102371
88. Farooqi, M, Khan, A, Jacobs, A, D’Souza, V, Consiglio, F, Karmen, CL, et al. Examining the long-term sequelae of SARS-CoV2 infection in patients seen in an outpatient psychiatric department. Neuropsychiatr Dis Treat. (2022) 18:1259–68. doi: 10.2147/NDT.S357262
89. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-5). Washington, D.C: American Psychiatric Press (2013).
90. Barlow, D, Allen, L, and Choate, M. Toward a unified treatment for emotional disorders. Behav Ther. (2004) 35:205–30. doi: 10.1016/S0005-7894(04)80036-4
91. Osma, J, Martínez-García, L, Quilez-Orden, A, and Peris-Baquero, Ó. Unified protocol for the transdiagnostic treatment of emotional disorders in medical conditions: a systematic review. Int J Environ Res Public Health. (2021) 18:5077. doi: 10.3390/ijerph18105077
92. Klaser, K, Hompson, E, Nguyen, L, Sudre, C, and Al, E. Anxiety and depression symptoms after COVID-19 infection: results from the COVID symptom study app. J Neurol Neurosurg Psychiatry. (2021) 92:1254–8. doi: 10.1136/jnnp-2021-327565
93. Barlow, D, Farchione, T, Sauer-Zavala, S, Latin, H, Ellard, K, Bullis, J, et al. Unified protocol for transdiagnostic treatment of emotional disorders: therapist guide. 2nd ed. New York, NY: Oxford University Press (2018).
94. Cassiello-Robbins, CS, Southward, MW, Tirpak, JW, and Sauer-Zavala, S. A systematic review of unified protocol applications with adult populations: facilitating widespread dissemination via adaptability. Clin Psychol Rev. (2020) 78:101852. doi: 10.1016/j.cpr.2020.101852
95. Martínez-Borba, V, Peris-Baquero, O, Martínez-García, L, Osma, J, and del Corral, BE. Unified protocol application in patients with long COVID-19 conditions In: J Osma and T Farchione, editors. Applications of the unified protocol in health conditions. Oxford: Oxford University Press (2023)
96. Cassiello-Robbins, C, Murray-Latin, H, and Sauer-Zavala, S. The unified protocol: future directions In: D Barlow and T Farchione, editors. Applications of the unified protocol for transdiagnostic treatment of emotional disorders. Oxford: Oxford University Press (2018). 291–301.
97. Peris-Baquero, Ó, Moreno, JD, and Osma, J. Long-term cost-effectiveness of group unified protocol in the Spanish public mental health system. Curr Psychol. (2022) 42:22462–77. doi: 10.1007/s12144-022-03365-8
98. Owens, JK. Systematic reviews: brief overview of methods, limitations, and resources. Nurse Author Ed. (2021) 31:69–72. doi: 10.1111/nae2.28
Keywords: COVID-19 patients, long COVID-19 conditions, psychological interventions, systematic review, emotional disorders
Citation: Martínez-Borba V, Martínez-García L, Peris-Baquero &, Osma J and del Corral-Beamonte E (2024) Guiding future research on psychological interventions in people with COVID-19 and post COVID syndrome and comorbid emotional disorders based on a systematic review. Front. Public Health. 11:1305463. doi: 10.3389/fpubh.2023.1305463
Edited by:
Renato de Filippis, University Magna Graecia of Catanzaro, ItalyReviewed by:
Māris Taube, Riga Stradiņš University, LatviaCopyright © 2024 Martínez-Borba, Martínez-García, Peris-Baquero, Osma and del Corral-Beamonte. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jorge Osma, b3NtYUB1bml6YXIuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.