
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 22 January 2024
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1302669
This article is part of the Research TopicOn the Cusp of the Silent Wave of the Long COVID Pandemic: Why, what and how should we tackle this emerging syndrome in the clinic and population?View all 12 articles
 Daniel Tavares Malheiro1
Daniel Tavares Malheiro1 Sabrina Bernardez-Pereira1*
Sabrina Bernardez-Pereira1* Kauê Capellato Junqueira Parreira1João Gabriel Dias Pagliuso1Emerson de Paula Gomes1Daisa de Mesquita Escobosa1Carolina Ivo de Araújo1Beatriz Silva Pimenta1Vivian Lin1Silvana Maria de Almeida1Paula Tuma1Claudia Regina Laselva1Miguel Cendoroglo Neto1Sidney Klajner1Vanessa Damazio Teich1
Kauê Capellato Junqueira Parreira1João Gabriel Dias Pagliuso1Emerson de Paula Gomes1Daisa de Mesquita Escobosa1Carolina Ivo de Araújo1Beatriz Silva Pimenta1Vivian Lin1Silvana Maria de Almeida1Paula Tuma1Claudia Regina Laselva1Miguel Cendoroglo Neto1Sidney Klajner1Vanessa Damazio Teich1 Takaaki Kobayashi2Michael B. Edmond3
Takaaki Kobayashi2Michael B. Edmond3 Alexandre R. Marra1,2
Alexandre R. Marra1,2Background: Robust data comparing long COVID in hospitalized and non-hospitalized patients in middle-income countries are limited.
Methods: A retrospective cohort study was conducted in Brazil, including hospitalized and non-hospitalized patients. Long COVID was diagnosed at 90-day follow-up using WHO criteria. Demographic and clinical information, including the depression screening scale (PHQ-2) at day 30, was compared between the groups. If the PHQ-2 score is 3 or greater, major depressive disorder is likely. Logistic regression analysis identified predictors and protective factors for long COVID.
Results: A total of 291 hospitalized and 1,118 non-hospitalized patients with COVID-19 were included. The prevalence of long COVID was 47.1% and 49.5%, respectively. Multivariable logistic regression showed female sex (odds ratio [OR] = 4.50, 95% confidence interval (CI) 2.51–8.37), hypertension (OR = 2.90, 95% CI 1.52–5.69), PHQ-2 > 3 (OR = 6.50, 95% CI 1.68–33.4) and corticosteroid use during hospital stay (OR = 2.43, 95% CI 1.20–5.04) as predictors of long COVID in hospitalized patients, while female sex (OR = 2.52, 95% CI 1.95–3.27) and PHQ-2 > 3 (OR = 3.88, 95% CI 2.52–6.16) were predictors in non-hospitalized patients.
Conclusion: Long COVID was prevalent in both groups. Positive depression screening at day 30 post-infection can predict long COVID. Early screening of depression helps health staff to identify patients at a higher risk of long COVID, allowing an early diagnosis of the condition.
The World Health Organization (WHO) defines long COVID as the continuation or development of new symptoms 3 months after the initial SARS-CoV-2 infection, with these symptoms lasting for at least 2 months with no other explanation. Long COVID impacts various population groups, leading to a diverse array of signs and symptoms. Over 200 different symptoms have been reported that can have an impact on daily life activities (1). It poses a growing medical challenge due to the complexity and diversity of its long-term effects. The presence of respiratory, motor, cardiovascular, or psychological sequelae heightens the demand for physical rehabilitation services and psychosocial support. Consequently, long COVID is increasingly burdening the healthcare system. Apart from strengthening the primary healthcare system and its multidisciplinary teams, there is a need to enhance specialized care. Considering that middle-income countries may have limited access to healthcare systems with fewer resources compared to high-income countries, it is crucial to investigate the prevalence of long COVID in these middle-income countries.
The majority of studies on long COVID have been carried out in Europe and North America, focusing on patients who were hospitalized and later discharged (2, 3). The United States produced the largest number of related publications, followed by the United Kingdom. The top ten most frequent keywords cited in these publications are “fatigue,” “depression,” and “inflammation” (2). Long COVID appears to be more common among women, older adult individuals, and those with existing comorbidities and higher body mass index (BMI) (2). However, limited research has been conducted on the long-term predictors in patients from middle-income countries comparing hospitalized and non-hospitalized patients. A systematic literature review published in 2021 showed that the number of publications had the following geographic distribution: Europe (62%, 24/39), followed by Asia (23%, 9/39), North America (8%, 3/39) and the Middle East 8% (3/39) and none of the included studies were carried out in low-middle-income countries (4). Furthermore, another systematic literature review and meta-analysis comprising 139 studies, highlighted a limitation of the geographic homogeneity. Over 50% of publications originated from Europe, with, less than 5% representing studies in long COVID from Africa, Oceania and South America. This underscores the need for more data from low-middle income countries (5). The study postulates that the prevalence of long COVID may exhibit variations between hospitalized and non-hospitalized COVID-19 patients in middle-income countries. Additionally, specific demographic and clinical factors, including patient-reported outcomes variables, including aspects of mental health, may serve as predictors of long COVID. The relationship between depression and long COVID is still an ongoing area of research and results are not conclusive.
The primary objective of this research is to assess the prevalence of long COVID among both hospitalized and non-hospitalized patient cohorts. Furthermore, the study seeks to identify predictive and protective factors influencing the development of long COVID within these groups. This investigation also endeavors to evaluate the impact of long COVID on the quality of life among afflicted individuals in Brazil.
This was a single center, retrospective cohort study, which included all the hospitalized and non-hospitalized adult patients (with a confirmed diagnosis of COVID-19 at Hospital Israelita Albert Einstein (HIAE) from February 12, 2021 to July 25, 2022. The Brazilian Israelite Society Albert Einstein is a nonprofit healthcare, educational, and research organization, with headquarters in the city of São Paulo, managing diverse services from primary to tertiary care, in the public and private healthcare sectors. It operates 40 healthcare units, mainly in the state of São Paulo. In 2022, the private sector HIAE had 344,000 emergency department visits, 495,000 outpatient visits, and 62,000 hospital discharges. The institution manages a diverse healthcare system ranging from primary healthcare to tertiary care services in the public and private sectors.
Any hospitalized and non-hospitalized adult patients (18 or more years of age) with a laboratory-confirmed COVID-19 were included. The laboratorial confirmation was performed using RT-PCR on specimens obtained via naso-pharyngeal swab, according to the protocol instituted at HIAE.
Long COVID was defined according to WHO criteria as the continuation or development of new symptoms 3 months after the initial SARS-CoV-2 infection. The signs and symptoms included in long COVID were general signs and symptoms (fatigue), respiratory and cardiac symptoms (dyspnea, cough, chest pain), neurological symptoms (memory loss, headache, sleep problem), and other symptoms (anosmia, ageusia, motor problems and difficulties with activities of daily living). We collected data on the first SARS-CoV-2 infection recorded in our system and excluded patients who were subsequently diagnosed with re-infection documented in the electronic medical record.
All the hospitalized patients with COVID-19 were followed through telephone interviews run by a trained professional 30 days and 90 days after hospital discharge, If the subject was unreachable at first call, three attempts were made. Non-hospitalized patients were followed 30 days and 90 days after COVID-19 confirmation date, via text message or email.
Data were collected using an electronic medical record, and patient reported questionnaires. At baseline, demographic characteristics including age, sex, and BMI, and clinical information including symptoms on admission, disease duration from onset of symptoms and underlying comorbidities were collected. Intensive care unit admission, use of mechanical ventilation, length of hospital stay, and drug therapy (i.e., steroids, antibiotics, and remdesivir) were also collected for hospitalized patients.
At 30-day and 90-day follow-up, symptoms and the PHQ-2 questionnaire were collected in both groups, and the EuroQol-5D3L quality of life questionnaire and EuroQol visual analog scale (EQ-VAS) were collected only in the hospitalized patient group.
The EuroQol-5D3L is a generic instrument for measuring health-related quality of life which generates an EQ-5D index score from 1 (full health) to 0 (a state as bad as being dead). The EQ-VAS is a 0–100 scale where patients are asked to indicate their overall health, where the higher the value, the better. Patients with and without long COVID were analyzed according to change in the EQ-5D index score and EQ-VAS scale from 30 days to 90 days. Three categories were defined: improvement, no change and worsening (6).
The PHQ-2 addresses the frequency of depressed mood and anhedonia in the last two weeks and can be used as a first approach for diagnosing depression. If the score is 3 or greater, major depressive disorder is likely (7).
As only a small number of positive samples among our cases were sequenced, all individuals were classified according to the most prevalent variant. Due to the low number of Alpha cases, it was combined with the Gamma cases to form a single time period. The time period between February 12, 2021, to August 5, 2021 was considered the “Alpha/Gamma era”; August 6, 2021 to December 16, 2021 the “Delta era”; and December 17, 2021 to July 25, 2022, the “Omicron era” (8).
To compare the demographic characteristics of hospitalized and non-hospitalized patients among COVID-19 variant eras, the Pearson’s Chi-square and Fisher’s exact test were used for categorical variables and were summarized as counts and percentages (9). In addition, normality assumptions were tested by the Anderson-Darling normality test. If this test provided evidence against a normal distribution for a given continuous variable, the Wilcoxon-Mann–Whitney U test was used instead. Both were expressed as medians with IQR (Interquartile Range).
A logistic regression model was used to investigate which factor, either at baseline or follow-up day 30, was associated with long COVID at day 90 in the two groups (hospitalized and non-hospitalized patients). The variables selected to enter the multivariate model were those with significant associations on univariate analysis (p < 0.05). Dichotomous intervals for continuous variables such as age (≥60 years or < 60 years) and length of stay (≥21 days or < 21 days) were created for the models. For the purposes of logistic regression, the PHQ-2 response on day 30 was used. Some variables did not have full information for all observations, for instance PHQ2 ≥ 3 (n = 6) and obesity (n = 4) had a total of 281 patients (long COVID = 131 and no long COVID = 150) and these variables were removed from the hospitalized long COVID prediction model. Predictors for both models did not present variance inflation factors (VIF >10), indicating that collinearity was not a problem. Receiver Operating Characteristic (ROC) curve analysis was employed to evaluate the performance of the predictive model. The Area Under the ROC Curve (AUC) was calculated to assess the discriminatory ability of the model in distinguishing between long COVID and no long COVID. All results with p < 0.05 were considered statistically significant. Data was manipulated in Knime Analytics Software1 and all statistical analyses were performed in R (4.2.0 version)2 programming language. The R packages used in the analyses are described in Supplementary Data 1.
The study was approved by the HIAE Research Ethics Committee, protocol number 6.204.804, CAAE: 69689123.2.0000.0071, and the National Commission for Research Ethics.
During the study period, 1,409 patients with confirmed COVID-19 were included, of which 291 (20.65%) were hospitalized patients and 1,118 (79.35%) non-hospitalized patients (Figure 1).
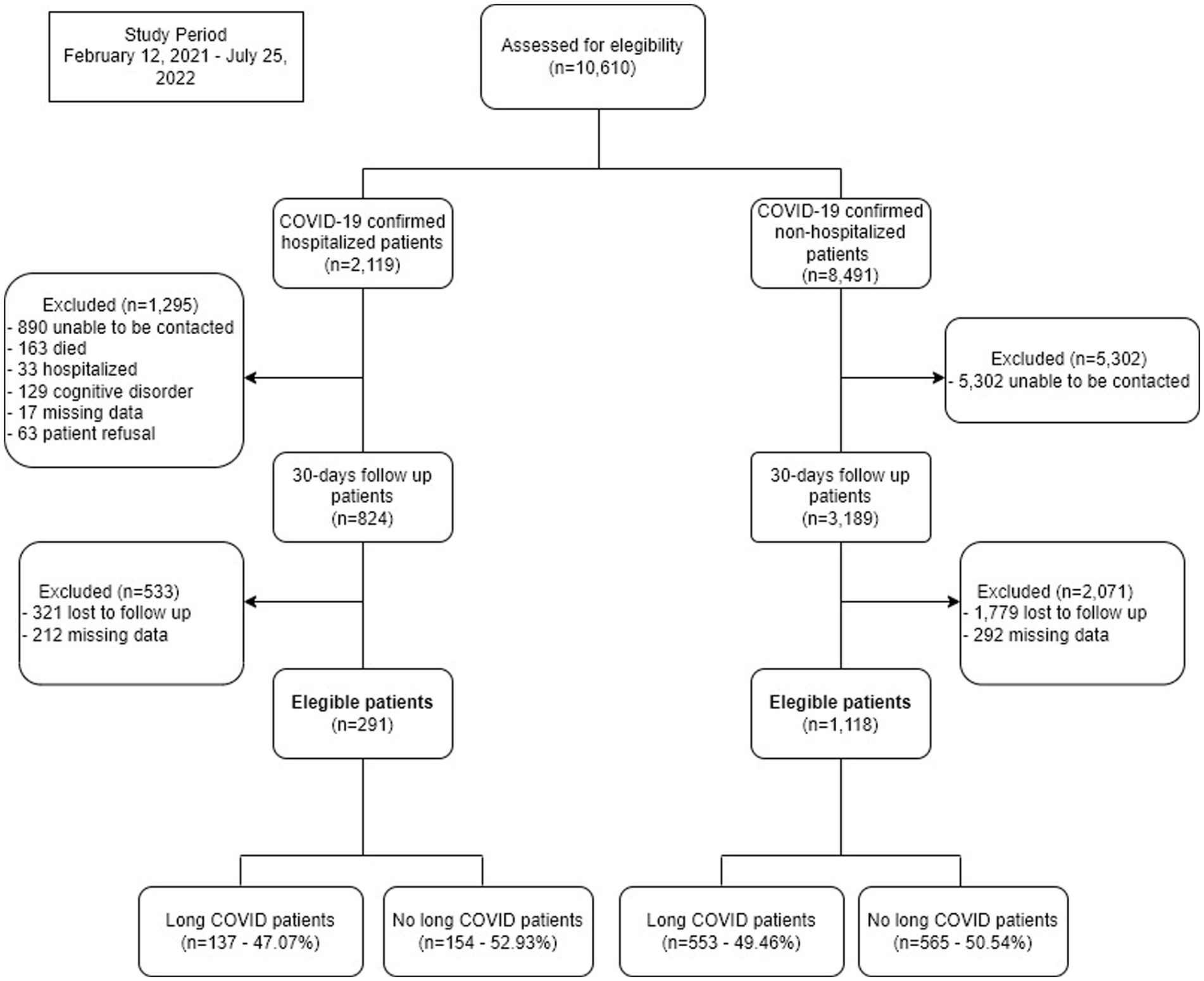
Figure 1. Study flowchart.
Table 1 summarizes the demographic and clinical characteristics of the eligible population in the two study groups (hospitalized and non-hospitalized) stratified by COVID-19 eras. Patients who were hospitalized were more likely to be older (median age 53.0 vs. 43.0 years old, p < 0.01) than non-hospitalized patients, regardless of variant, and had higher BMI (27.9 vs. 25.7 kg/m2, p < 0.01) in the Alpha/Gamma era. Hospitalized patients also had more comorbidities and the predominant symptoms on admission were cough (35.7% vs. 28.2%, p = 0.01), fever (55.7% vs. 20.5%, p < 0.01), myalgia (30.6% vs. 19.7%, p < 0.01), fatigue (32.0% vs. 25.1%, p = 0.02) and dyspnea (19.9% vs. 5.4%, p < 0.01) when compared to non-hospitalized patients. Regarding the clinical course among hospitalized patients, 42.3% required admission to the ICU, 9.6% received mechanical ventilation, 59.5% antibiotics, 69.8% steroids and 12.4% remdesivir. Patients admitted during the Alpha/Gamma era received proportionally more mechanical ventilation (14.6%, p = 0.01) and corticosteroids (93.4%, p < 0.01) (Supplementary Table 1).
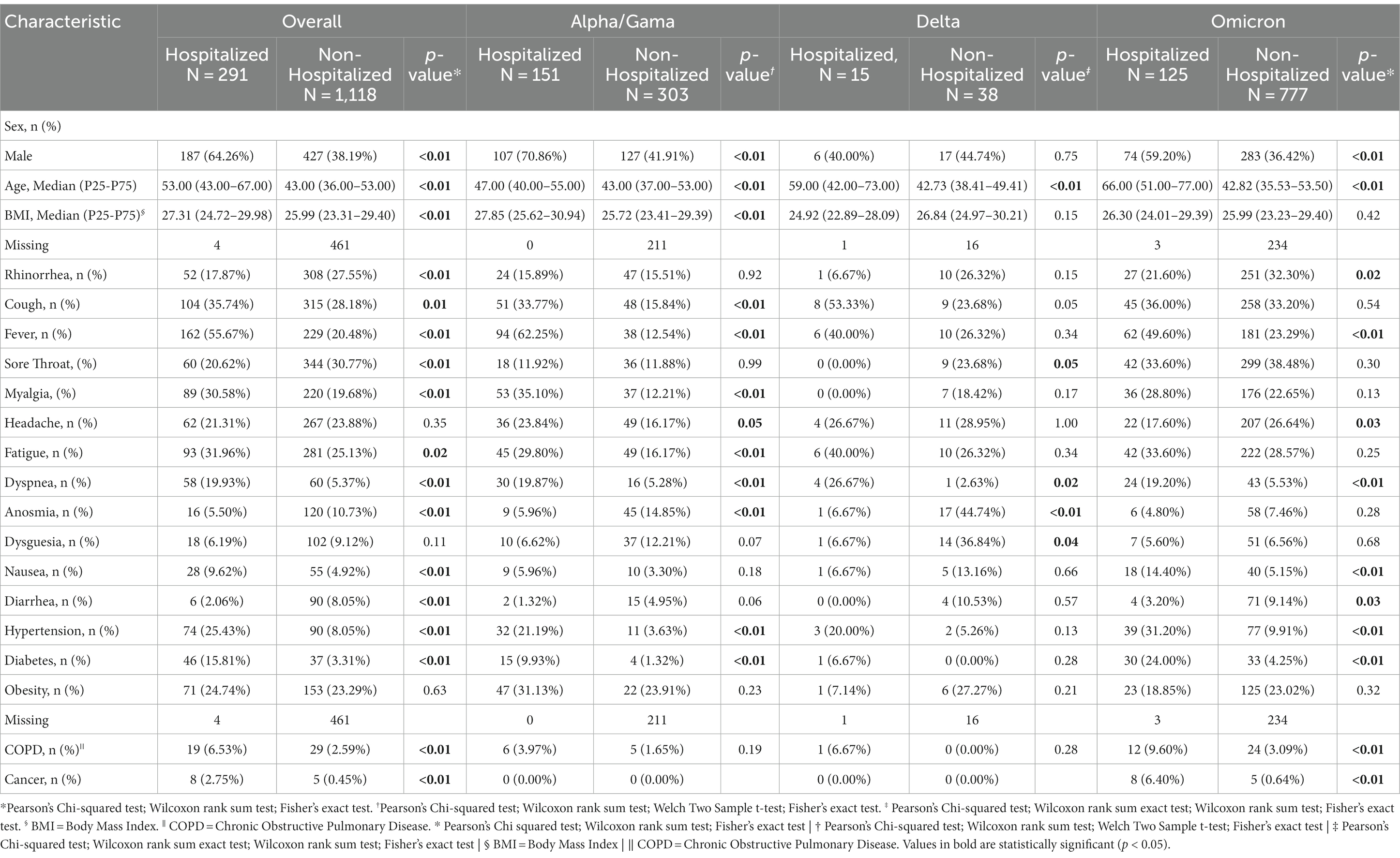
Table 1. Demographic and clinical characteristics of the eligible population by COVID-19 era.
The prevalence of long COVID was found to be 47.1% among hospitalized patients and 49.5% among non-hospitalized patients at 90 days. Among hospitalized patients, the prevalence of long COVID varied across different eras, with rates of 58.3% during the Alpha/Gamma era, 46.7% during the Delta era, and 33.6% during the Omicron era. Among non-hospitalized patients, the prevalence of long COVID was 50.83% during the Alpha/Gamma era, 63.16% during the Delta era, and 48.26% during the Omicron era. In hospitalized patients diagnosed with long COVID, the most common symptoms reported were memory loss (33.6%) and fatigue (30.7%). Among non-hospitalized patients, the prevalent symptoms included memory loss (45.8%), fatigue (46.5%), sleep disorders (32.4%) and headache (30.7%) (Supplementary Figure 1 provides further details).
The analysis of the change in the EQ-5D index score from 30 days to 90 days showed that patients with long COVID have a higher rate of worsening over time than those without long COVID (33.8% vs. 11.3%, p < 0.01) (Figure 2A). There was no significant difference for the EQ-VAS variation score in the same period (p = 0.45) (Figure 2B), however, the EQ-VAS score at 90 days was lower among patients with long COVID compared to those without this condition (Supplementary Figure 2).
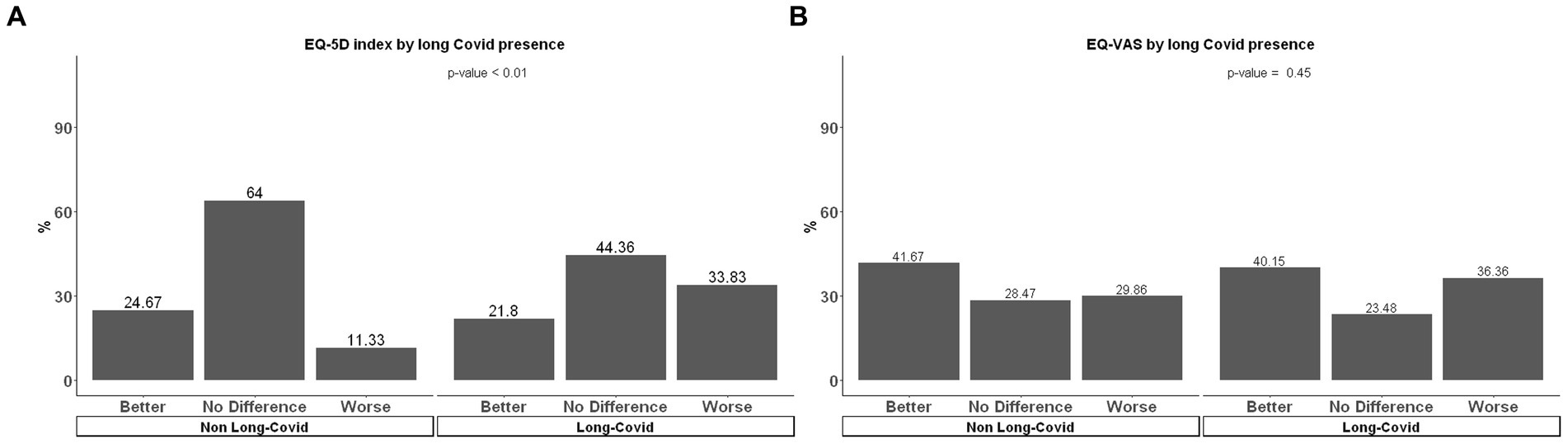
Figure 2. (A) EQ-5D index and (B) EQ-VAS change from 30 days to 90 days follow up for long COVID and no long COVID of hospitalized patients.
Multivariable logistic regression showed that predictors of long COVID among hospitalized patients were female sex (odds ratio [OR] = 4.50, 95% confidence interval (CI): [2.51–8.37]), hypertension (OR = 2.90 [1.52–5.69]), PHQ-2 ≥ 3 (OR = 6.50 [1.68–33.4]) and corticosteroid treatment during hospital stay (OR = 2.43 [1.20–5.04]) and a protective factor was Omicron era (OR = 0.40 [0.19–0.83]) (Table 2). Among non-hospitalized patients, predictors were female sex (OR = 2.52 [1.95–3.27]) and PHQ-2 > 3 (OR = 3.88 [2.52–6.16]) and a protective factor was age ≥ 60 years old (OR = 0.68 [0.48–0.97]) (Table 3).
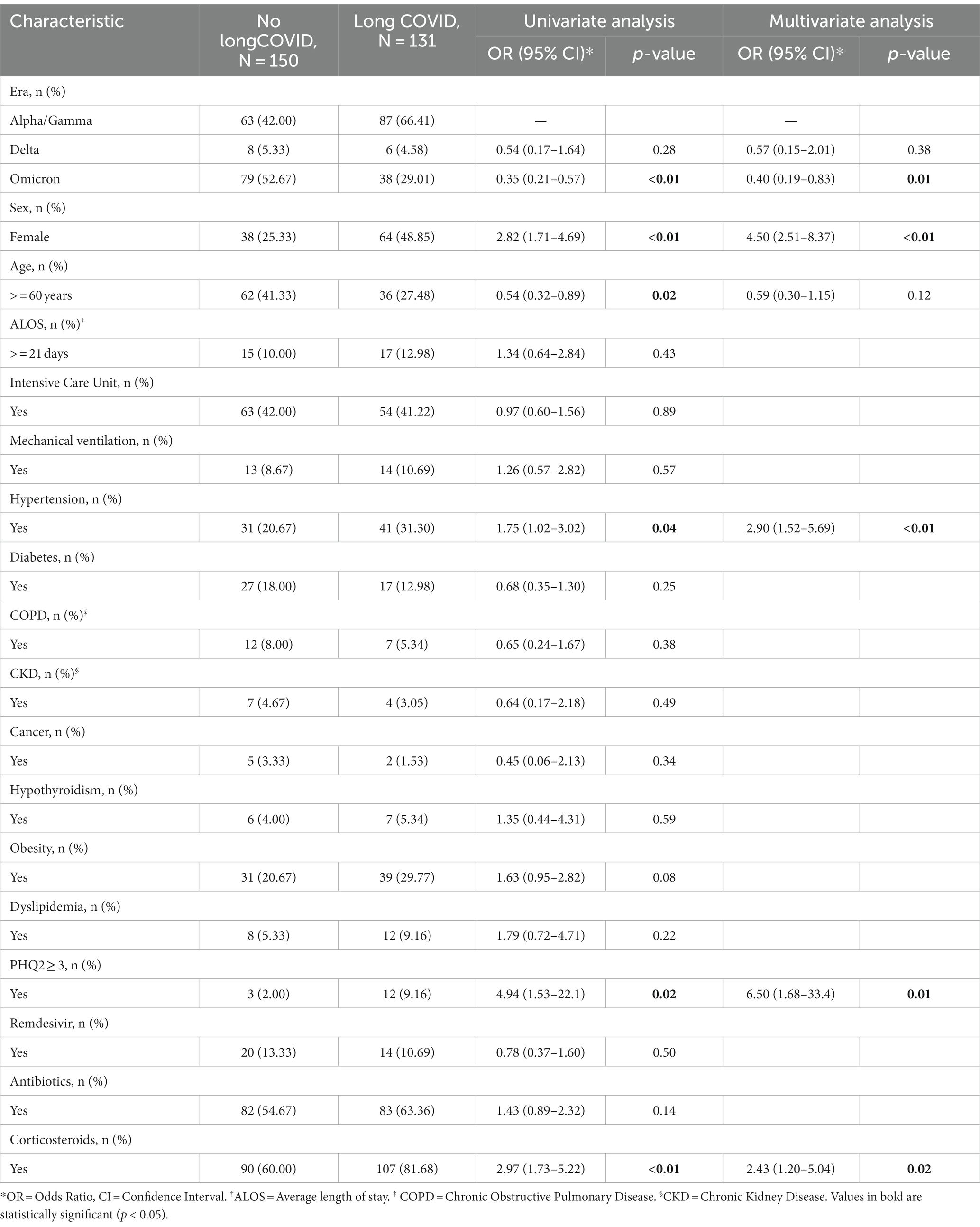
Table 2. Multivariate analysis of predictors for long COVID in hospitalized patients.
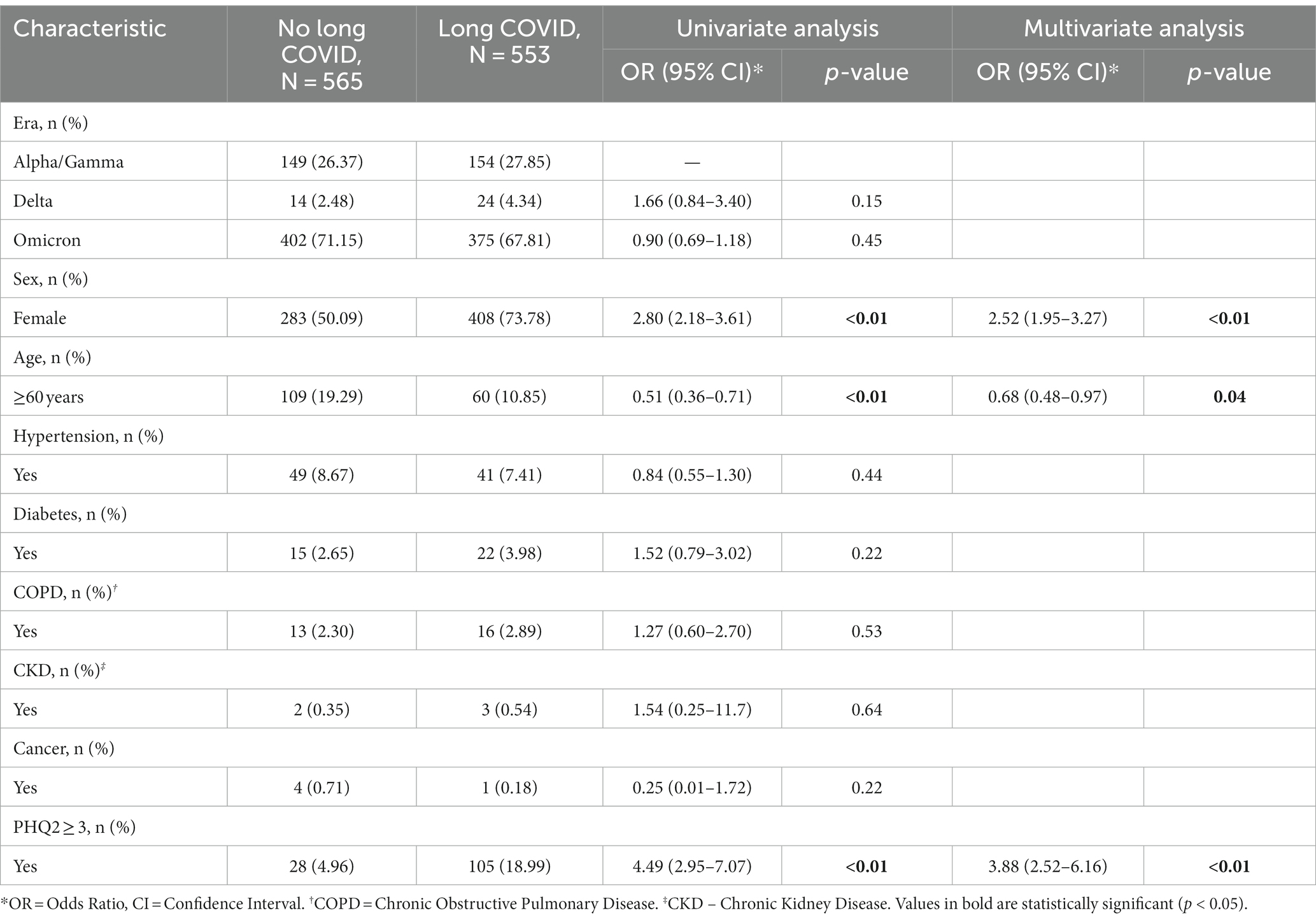
Table 3. Multivariate analysis of predictors for long COVID in non-hospitalized patients.
The ROC curve was employed to analyze the predictive power of the variables for the classification of long COVID. For the group of hospitalized patients, the analyzed variables were gender, age (> = 60 years), hypertension, PHQ2, and corticosteroid use, resulting in an area under the curve (AUC) value of 0.759 and a 95% confidence interval between 0.704 and 0.815. Regarding the group of outpatient patients, the available variables were gender, age (> = 60 years), and PHQ2, yielding an AUC value of 0.667 and a 95% confidence interval between 0.638 and 0.696 (Supplementary Figures 3, 4).
This study revealed that the prevalence of long COVID among hospitalized patients and non-hospitalized patients was 47.1 and 49.5%, respectively, at the 90 days after initial SARS-CoV-2 infection in a middle-income country. The prevalence of long COVID varied across different variant eras with the lowest prevalence seen in the Omicron era. Memory loss and fatigue were the most common symptoms for both groups. The factors associated with long COVID were female gender and positive screening for depression (PHQ-2 score) in both groups. The presence of hypertension also showed a risk for the development of long COVID among hospitalized patients while Omicron era infection was associated with a lower risk. Additionally, hospitalized patients with long COVID had a higher percentage of worsening quality of life measured by the EQ-5D index score at 90 days when compared to patients without long COVID.
A surveillance report of the European Centre for Disease Prevention and Control (ECDC), through a systematic review study and meta-analysis revealed a higher incidence of long COVID in patients admitted to the ICU. In this report overall prevalence of any post COVID-19 condition symptom was estimated at 51% in the community setting; 67% in the hospital setting; and 74% in the ICU setting (3). More recently, another systematic review signaled that the prevalence estimates of long COVID were significantly influenced by the severity of acute infection and being hospitalized (10). However, our results showed similar overall prevalence among non-hospitalized patients and hospitalized patients.
Interestingly, our study showed that the prevalence of long COVID was lowest during the Omicron era in hospitalized patients. A recent systematic review demonstrated that patients infected with the Omicron variant may have a lower risk of developing long COVID than those infected with other variants (11). However, the Omicron era was not shown to be a protective factor in non-hospitalized patients and further research is needed to understand the specific mechanisms underlying this observation and to determine if it holds true across different populations and settings.
Limited research exists on long COVID among hospitalized and non-hospitalized patients in middle-income countries. In Malaysia, common symptoms observed in both outpatients and inpatients include fatigue, brain fog, depression, anxiety, insomnia, and joint or muscle pain (12). However, in India, a single-center prospective observational cohort study highlighted fatigue, dyspnea, and weight loss as the predominant symptoms among hospitalized patients (13). A study in China found that at 6-month follow-up, fatigue or muscle weakness and sleep difficulties were the main symptoms observed in COVID-19 patients who had recovered. Patients with more severe illness had reduced lung function and a higher risk of psychological complications like anxiety and depression (14). In line with these findings and following similar results in high-income countries (2, 3, 15, 16), our study identified fatigue and memory loss as the most prevalent symptoms among both hospitalized and non-hospitalized patients. These results underscore the wide range of symptoms and the potential impact on various patient populations affected by long COVID.
Previous literatures showed that symptoms due to long COVID have a strong impact on quality of life of affected patients (17, 18). While our study found no difference in the EQ-VAS visual analog scale between patients with and without long COVID at 90 days compared to 30 days after COVID-19, the long COVID group exhibited a lower quality of life score according to the EuroQol-5D3L questionnaire. This contrasts with findings from a high-income country, where a Japanese report indicated that participants with long COVID had lower average scores on both the EQ-VAS and EuroQol-5D3L compared to those without long COVID (19). Gaspar et al. (20) in a study conducted in Portugal showed an association between the presence of long COVID and the deterioration of quality of life, assessed through the EQ-5D index, at 3-, 6-, and 9-months post-discharge. Further research is needed to better understand the long-term effects of COVID-19, including how it affects the quality of life of those with persistent symptoms.
Previous studies, including those conducted in low-and middle-income countries, have established a link between female gender and long COVID (12, 13, 21–23), However, it has not been previously reported that a positive depression screening at day 30 using a validated questionnaire could be a risk factor for diagnosing long COVID at day 90 (24, 25). Additionally, few studies have examined depression as a risk factor for COVID-19 or long COVID (26, 27). Taquet et al. showed a bidirectional association between COVID-19 and psychiatric disorder. Adults with a history of COVID-19 diagnosis have an approximately doubled risk of being newly diagnosed with a psychiatric condition than those without SARS-CoV-2 infection. On the other hand, having a diagnosis of psychiatric disorder in the year before the COVID-19 pandemic was associated with a 65% increased risk of COVID-19 (28). More recently, an investigation of factors associated with psychiatric outcomes in long COVID was published and it was shown that patients with long COVID are at increased risk for psychiatric disease, including depression, compared with those without long COVID (29). Conversely, Wang et al. found a strong association between symptoms of depression and anxiety, worry about COVID-19, loneliness, and perceived stress with the risk of long COVID. They note that their results should not be misinterpreted as being supportive of the hypothesis that symptoms of long COVID are psychosomatic since a significant number of patients without mental illness also develop long COVID (30).
The association between depression and long COVID may be explained by several factors. Inflammation and activation of the hypothalamic–pituitary–adrenal axis, which can lead to chronic immune suppression, can be generated by distress. Additionally, depression may lead to changes in the brain and nervous system, which could contribute to long COVID symptoms such as fatigue and cognitive impairment (31). This suggests that recommending mental health screening to support these patients might be warranted. The PHQ-2 is a simple and effective screening tool that can be used to assess depression symptoms. Early identification and treatment of depression may help prevent the development of long COVID and improve overall health outcomes.
While hypertension is known to increase the risk of severe COVID-19 illness, the underlying mechanisms are not fully understood (32). Hypertension may contribute to the development of long COVID by affecting cardiovascular health and immune function. Initially, there was a suggested link between the use of renin-angiotensin-aldosterone system (RAAS) inhibitors and mortality in severe SARS-CoV-2 infection due to interactions with the bradykinin pathway. However, subsequent evidence has not confirmed this hypothesis (33–37). Other studies have indicated that hypertension’s association with known risk factors such as advanced age, obesity, diabetes, cardiovascular disease, and chronic kidney disease could explain its role as a risk factor (38, 39). Limited research has been conducted on the role of hypertension as a predictor of long COVID and the impact of RAAS inhibitors on long-term symptoms. A recent study involving 414 patients indicated that hypertension appears to play a significant role in the persistence of long COVID symptoms. Among these individuals, 39.6% reported symptoms extending beyond 6 weeks post-infection. The study found that long COVID was notably higher in patients over 65 years old and those with various comorbidities, including Type II diabetes mellitus, dyslipidemia, coronary artery disease, asthma, and cancer. Specifically, hypertension showed an odds ratio of 2.59 and was statistically significant (p = 0.001), indicating a notable association with prolonged symptoms post-infection (40).
Similar to a study conducted in Italy, our results indicate that the severity of acute COVID-19 (ICU admission, prolonged length of stay, and use of mechanical ventilation) did not exert a substantial influence on the development of long-term COVID-19 (41). Interestingly, our findings showed that patients who received steroids during hospitalization were at greater risk of developing this condition. Likewise, a study from Southeastern Italy also demonstrated that corticosteroid therapy administered in the acute phase of COVID-19 might be associated with an increased risk of long COVID. One plausible hypothesis posited by the authors is that the administration of corticosteroids during the acute phase of illness may potentially contribute to the persistence of the virus within non-respiratory system among some patients reservoirs (24). To ascertain the potential association between corticosteroid utilization and an increased risk of prolonged COVID-19, along with its dependence on factors such as dosage, type, or duration of in-hospital steroid therapy, further comprehensive investigations are warranted.
The Omicron era was found to be associated with a lower risk of developing long COVID among hospitalized patients while age ≥ 60 years old was a protective factor among non-hospitalized patients, similar to that reported by Reme et al. (42). The findings of a study published in 2022 demonstrated that the mean number of post-COVID-19 symptoms was higher in patients infected with the Wuhan variant than in those infected with the Alpha or Delta variant (43). Meanwhile a correspondence published in the same year found a reduction in the odds of long COVID with the Omicron variant versus the Delta variant (44). This intriguing finding suggests that the emergence of different COVID-19 variants may influence the clinical course and outcomes of this disease, including the likelihood of experiencing long-term symptoms. Understanding the role of the new COVID-19 variants in long COVID may aid in tailoring treatment approaches and public health interventions to mitigate its long-term burden. This study has several strengths. Its innovative approach focuses on exploring long COVID within the context of a middle-income country, specifically in Brazil. By comparing occurrences and predictive factors between hospitalized and non-hospitalized patients, the study provides crucial insights into how the severity of the initial illness influences the manifestation and impact of long COVID on individuals. Moreover, the study delves into the use of patient-reported outcome measures and their long-term effects on conditions such as COVID, examining their influence on both quality of life and mental health.
Our study sheds light on the prevalence of long COVID in distinct patient groups and identifies potential predictors, including gender, underlying health conditions, and depression screening. These findings offer crucial information for comprehending, predicting, and managing long COVID in diverse patient cohorts. By focusing on a middle-income country, the research contributes to a more comprehensive understanding of long COVID by incorporating data from varied socioeconomic backgrounds.
This study has limitations due to its single institution setting and limited timeframe. The generalizability of the findings to broader populations may be limited. The reliance on clinical data and lack of exploration of certain factors, such as pre-existing conditions, especially presence of depression or mood disorder, may contribute to variations in outcomes and the prevalence of long COVID. Variables related to comorbidities were collected from the medical records; however, the Charlson Comorbidity Index was not routinely measured, so we did not use this information in our analysis. Socioeconomic data were not collected for this study. Additionally, the study’s retrospective nature and reliance on self-reported symptoms introduce biases and variability in reporting. Furthermore, the study did not thoroughly examine the impact of treatment regimens other than remdesivir, or vaccination status. Due to the sensitive nature of personal information within vaccination data, access to this information in national databases is limited under the General Data Protection Law established in 2020 in Brazil. Consequently, these data was not included in the analyses. As of July 2022, at the conclusion of the Omicron wave, approximately 90% of the population of the State of São Paulo had received the first dose of the COVID-19 vaccine. We believe this fact may have contributed to the protective outcome during the Omicron wave in the multivariate analysis. Moreover, our study did not specifically address the characteristics of patients diagnosed with the COVID variants (Alpha/Gamma, Delta, and Omicron). Given the evolving nature of the virus and the emergence of new variants, it is essential to recognize that the dynamics of long COVID may be influenced by factors specifically to each variant. Therefore, extrapolation of our findings to populations affected by more recent variants should be approached with caution, and further research is warranted to understand the implications of these variants on the manifestation and impact of long COVID.
Future research with larger cohorts and prospective designs is needed to validate these findings, explore the underlying mechanisms, and address these limitations for a more comprehensive understanding of long COVID.
In conclusion, approximately half of both hospitalized and non-hospitalized patients in Brazil developed long COVID 90 days after their initial COVID-19. The prevalence of long COVID differed among different strain eras, with fatigue and memory loss being the most frequently reported symptoms. We identified a significant association between a positive depression screening at day 30 and an increased risk of developing long COVID at day 90. These findings may highlight the importance of integrating depression screening into regular COVID-19 follow-ups at primary care clinics.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Ethics Committee of Hospital Israelita Albert Einstein – CEP/Einstein. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because the waiver of the use of informed consent is based on: i) being a retrospective observational study that utilized only medical records, institutional information systems, and/or other sources of data and clinical information available within the institution without the use of biological material anticipated; ii) because all data were handled and analyzed anonymously, without nominal participant identification; iii) because the study results will be presented in an aggregated manner, preventing individual participant identification; and iv) because it is a non-interventional study (without clinical interventions) and without alterations/influences in the participant’s routine/treatment, consequently posing no additional risks or harm to their well-being. Additionally, we will be unable to obtain consent from all participants in this research.
De-identified individual study data reported in this article can be requested upon application to investigator board via the corresponding author.
DMa: Conceptualization, Formal analysis, Methodology, Supervision, Writing – review & editing. SB-P: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. KP: Writing – original draft, Methodology, Formal analysis. JP: Conceptualization, Investigation, Writing – original draft. EP: Data curation, Formal analysis, Validation, Visualization, Writing – original draft. DMe: Data curation, Methodology, Project administration, Supervision, Writing – original draft. CA: Data curation, Project administration, Writing – original draft. BP: Data curation, Writing – original draft. VL: Writing – original draft. SA: Data curation, Validation, Writing – original draft. PT: Writing – review & editing. CL: Writing – review & editing. MN: Writing – review & editing. SK: Writing – review & editing. VT: Conceptualization, Resources, Writing – review & editing. TK: Writing – review & editing. ME: Writing – review & editing. AM: Conceptualization, Investigation, Methodology, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was supported by an internal grant from Hospital Israelita Albert Einstein and designed by the investigators.
The authors would like to express gratitude to all of the health professionals at Hospital Israelita Albert Einstein who were willing to donate their time to save lives.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1302669/full#supplementary-material
2. Jin, H, Lu, L, and Fan, H. Global trends and research hotspots in long COVID: a bibliometric analysis. Int J Environ Res Public Health. (2022) 19:3742. doi: 10.3390/ijerph19063742
3. European Centre for Disease Prevention and Control. Prevalence of post COVID-19 condition symptoms: a systematic review and meta-analysis of cohort study data stratified by recruitment setting. Stockholm: ECDC (2022).
4. Michelen, M, Manoharan, L, Elkheir, N, Cheng, V, Dagens, A, Hastie, C, et al. Characterising long COVID: a living systematic review. BMJ Glob Health. (2021) 6:e005427. doi: 10.1136/bmjgh-2021-005427
5. O’Mahoney, LL, Routen, A, Gillies, C, Ekezie, W, Welford, A, Zhang, A, et al. The prevalence and long-term health effects of long Covid among hospitalised and non-hospitalised populations: a systematic review and meta-analysis. EClinicalMedicine. (2022) 55:101762. doi: 10.1016/j.eclinm.2022.101762
6. Rabin, R, and de Charro, F. EQ-5D: a measure of health status from the euro Qol group. Ann Med. (2001) 33:337–43. doi: 10.3109/07853890109002087
7. Kroenke, K, Spitzer, RL, and Williams, JB. The patient health Questionnaire-2: validity of a two-item depression screener. Med Care. (2003) 41:1284–92. doi: 10.1097/01.MLR.0000093487.78664.3C
8. Marra, AR, Sampaio, VS, Ozahata, MC, Lopes, R, Brito, AF, Bragatte, M, et al. Risk factors for long coronavirus disease 2019 (long COVID) among healthcare personnel, Brazil, 2020–2022. Infect Control Hosp Epidemiol. (2023) 5:1–7. doi: 10.1017/ice.2023.95 [Epub ahead of print].
9. Lee, SW. Methods for testing statistical differences between groups in medical research: statistical standard and guideline of life cycle committee. Life Cycle. (2022) 2:e1. doi: 10.54724/lc.2022.e1
10. Woodrow, M, Carey, C, Ziauddeen, N, Thomas, R, Akrami, A, Lutje, V, et al. Systematic review of the prevalence of long COVID, open forum. Infect Dis. (2023) 10:ofad 233. doi: 10.1093/ofid/ofad233
11. Fernández-de-Las-Peñas, C, Notarte, KI, Peligro, PJ, Velasco, JV, Ocampo, MJ, Henry, BM, et al. Long-COVID symptoms in individuals infected with different SARS-CoV-2 variants of concern: a systematic review of the literature. Viruses. (2022) 14:2629. doi: 10.3390/v14122629
12. Moy, FM, Hairi, NN, Lim, ERJ, and Bulgiba, A. Long COVID and its associated factors among COVID survivors in the community from a middle-income country-an online cross-sectional study. PLoS One. (2022) 17:e0273364. doi: 10.1371/journal.pone.0273364
13. Nair, CV, Moni, M, Edathadathil, F, Prasanna, P, Pushpa Raghavan, R, Sathyapalan, DT, et al. Incidence and characterization of post-COVID-19 symptoms in hospitalized COVID-19 survivors to recognize Syndemic connotations in India: single-center prospective observational cohort study. JMIR Form Res. (2023) 7:e40028. doi: 10.2196/40028
14. Huang, C, Huang, L, Wang, Y, Li, X, Ren, L, Gu, X, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. (2021) 397:220–32. doi: 10.1016/S0140-6736(20)32656-8
15. Iqbal, FM, Lam, K, Sounderajah, V, Clarke, JM, Ashrafian, H, and Darzi, A. Characteristics and predictors of acute and chronic post-COVID syndrome: a systematic review and meta-analysis. EClinicalMedicine. (2021) 36:100899. doi: 10.1016/j.eclinm.2021.100899
16. Hetlevik, Ø, Wensaas, KA, Baste, V, Emberland, KE, Özgümüs, T, Håberg, SE, et al. Prevalence and predictors of post-COVID-19 symptoms in general practice - a registry-based nationwide study. BMC Infect Dis. (2023) 23:721. doi: 10.1186/s12879-023-08727-6
17. Malik, P, Patel, K, Pinto, C, Jaiswal, R, Tirupathi, R, Pillai, S, et al. Post-acute COVID-19 syndrome (PCS) and health-related quality of life (HRQoL)-a systematic review and meta-analysis. J Med Virol. (2022) 94:253–62. doi: 10.1002/jmv.27309
18. Román-Montes, CM, Flores-Soto, Y, Guaracha-Basañez, GA, Tamez-Torres, KM, Sifuentes-Osornio, J, González-Lara, MF, et al. Post-COVID-19 syndrome and quality of life impairment in severe COVID-19 Mexican patients. Front Public Health. (2023) 11:1155951. doi: 10.3389/fpubh.2023.1155951
19. Tsuzuki, S, Miyazato, Y, Terada, M, Morioka, S, Ohmagari, N, and Beutels, P. Impact of long-COVID on health-related quality of life in Japanese COVID-19 patients. Health Qual Life Outcomes. (2022) 20:125. doi: 10.1186/s12955-022-02033-6
20. Gaspar, P, Dias, M, Parreira, I, Gonçalves, HD, Parlato, F, Maione, V, et al. Predictors of long-COVID-19 and its impact on quality of life: longitudinal analysis at 3, 6 and 9 months after discharge from a Portuguese Centre. Acta Med Port. (2023) 24, 36:647–60. doi: 10.20344/amp.19047
21. Subramanian, A, Nirantharakumar, K, Hughes, S, Myles, P, Williams, T, Gokhale, KM, et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat Med. (2022) 28:1706–14. doi: 10.1038/s41591-022-01909-w
22. Munblit, D, Bobkova, P, Spiridonova, E, Shikhaleva, A, Gamirova, A, Blyuss, O, et al. Incidence and risk factors for persistent symptoms in adults previously hospitalized for COVID-19. Clin Exp Allergy. (2021) 51:1107–20. doi: 10.1111/cea.13997
23. Xiong, Q, Xu, M, Li, J, Liu, Y, Zhang, J, Xu, Y, et al. Clinical sequelae of COVID-19 survivors in Wuhan, China: a single-Centre longitudinal study. Clin Microbiol Infect. (2021) 27:89–95. doi: 10.1016/j.cmi.2020.09.023
24. Quaranta, VN, Portacci, A, Dragonieri, S, Locorotondo, C, Buonamico, E, Diaferia, F, et al. The predictors of long COVID in southeastern Italy. J Clin Med. (2023) 12:6303. doi: 10.3390/jcm12196303
25. Tsampasian, V, Elghazaly, H, Chattopadhyay, R, Debski, M, Naing, TKP, Garg, P, et al. Risk factors associated with post−COVID-19 condition: a systematic review and Meta-analysis. JAMA Intern Med. (2023) 183:566–80. doi: 10.1001/jamainternmed.2023.0750
26. Woodward, SF, Bari, S, Vike, N, Lalvani, S, Stetsiv, K, Kim, BW, et al. Anxiety, post–COVID-19 syndrome-related depression, and suicidal thoughts and behaviors in COVID-19 survivors: cross-sectional study. JMIR Form Res. (2022) 6:e36656. doi: 10.2196/36656
27. Fancourt, D, Steptoe, A, and Bu, F. Psychological consequences of long COVID: comparing trajectories of depressive and anxiety symptoms before and after contracting SARS-CoV-2 between matched long-and short-COVID groups. Br J Psychiatry. (2023) 222:74–81. doi: 10.1192/bjp.2022.155
28. Taquet, M, Luciano, S, Geddes, JR, and Harrison, PJ. Bidirectional associations between COVID-19 and psychiatric disorder: retrospective cohort studies of 62 354 COVID-19 cases in the USA. Lancet Psychiatry. (2021) 8:130–40. doi: 10.1016/S2215-0366(20)30462-4
29. Re’em, Y, Stelson, EA, Davis, HE, McCorkell, L, Wei, H, Assaf, G, et al. Factors associated with psychiatric outcomes and coping in long COVID. Nat Mental Health. (2023) 1:361–72. doi: 10.1038/s44220-023-00064-6
30. Wang, S, Quan, L, Chavarro, JE, Slopen, N, Kubzansky, LD, Koenen, KC, et al. Associations of depression, anxiety, worry, perceived stress, and loneliness prior to infection with risk of post-COVID-19 conditions. JAMA Psychiatry. (2022) 79:1081–91. doi: 10.1001/jamapsychiatry.2022.2640
31. Raony, Í, de Figueiredo, CS, Pandolfo, P, Giestal-de-Araujo, E, Oliveira-Silva Bomfim, P, and Savino, W. Psycho-neuroendocrine-immune interactions in COVID-19: potential impacts on mental health. Front Immunol. (2020) 11:1170. doi: 10.3389/fimmu.2020.01170
32. Peng, M, He, J, Xue, Y, Yang, X, Liu, S, and Gong, Z. Role of hypertension on the severity of COVID-19: a review. J Cardiovasc Pharmacol. (2021) 78:e648–55. doi: 10.1097/FJC.0000000000001116
33. Kreutz, R, Algharably, EAE, Azizi, M, Dobrowolski, P, Guzik, T, Januszewicz, A, et al. Hypertension, the renin–angiotensin system, and the risk of lower respiratory tract infections and lung injury: implications for COVID-19. Cardiovasc Res. (2020) 116:1688–99. doi: 10.1093/cvr/cvaa097
34. Hoffmann, M, Kleine-Weber, H, Schroeder, S, Krüger, N, Herrler, T, Erichsen, S, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cells. (2020) 181:271–280.e8. doi: 10.1016/j.cell.2020.02.052
35. Kumar, S, Nikravesh, M, Chukwuemeka, U, Randazzo, M, Flores, P, Choday, P, et al. Safety of ACEi and ARB in COVID-19 management: a retrospective analysis. Clin Cardiol. (2022) 45:759–66. doi: 10.1002/clc.23836
36. Li, J, Wang, X, Chen, J, Zhang, H, and Deng, A. Association of Renin-Angiotensin System Inhibitors with Severity or risk of death in patients with hypertension hospitalized for coronavirus disease 2019 (COVID-19) infection in Wuhan. China JAMA Cardiol. (2020) 5:825–30. doi: 10.1001/jamacardio.2020.1624
37. Semenzato, L, Botton, J, Drouin, J, Baricault, B, Vabre, C, Cuenot, F, et al. Antihypertensive drugs and COVID-19 risk: a cohort study of 2 million hypertensive patients. Hypertension. (2021) 77:833–42. doi: 10.1161/HYPERTENSIONAHA.120.16314
38. Iaccarino, G, Grassi, G, Borghi, C, Ferri, C, Salvetti, M, and Volpe, M. SARSRAS investigators age and multimorbidity predict death among COVID-19 patients: results of the SARS-RAS study of the Italian society of hypertension. Hypertension. (2020) 76:366–72. doi: 10.1161/HYPERTENSIONAHA.120.15324
39. Thakur, B, Dubey, P, Benitez, J, Torres, JP, Reddy, S, Shokar, N, et al. A systematic review and meta-analysis of geographic differences in comorbidities and associated severity and mortality among individuals with COVID-19. Sci Rep. (2021) 11:8562. doi: 10.1038/s41598-021-88130-w
40. Nair, P, Nair, CV, Kulirankal, KG, Corley, EM, Edathadathil, F, Gutjahr, G, et al. Characterization and predictive risk scoring of long COVID in a south indian cohort after breakthrough COVID infection; a prospective single Centre study. BMC Infect Dis. (2023) 23:670. doi: 10.1186/s12879-023-08600-6
41. Comelli, A, Viero, G, Bettini, G, Nobili, A, Tettamanti, M, Galbussera, AA, et al. Patient-reported symptoms and sequelae 12 months after COVID-19 in hospitalized adults: a multicenter long-term follow-up study. Front Med. (2022) 9:834354. doi: 10.3389/fmed.2022.834354
42. Reme, BA, Gjesvik, J, and Magnusson, K. Predictors of the post-COVID condition following mild SARS-CoV-2 infection. Nat Commun. (2023) 14:5839. doi: 10.1038/s41467-023-41541-x
43. Fernández-de-Las-Peñas, C, Cancela-Cilleruelo, I, Rodríguez-Jiménez, J, Gómez-Mayordomo, V, Pellicer-Valero, OJ, Martín-Guerrero, JD, et al. Associated-onset symptoms and post-COVID-19 symptoms in hospitalized COVID-19 survivors infected with Wuhan, alpha or Delta SARS-CoV-2 variant. Pathogens. (2022) 11:725. doi: 10.3390/pathogens11070725
Keywords: long COVID, mental health, depression screening, quality of life, middle income countries
Citation: Malheiro DT, Bernardez-Pereira S, Parreira KCJ, Pagliuso JGD, de Paula Gomes E, de Mesquita Escobosa D, de Araújo CI, Pimenta BS, Lin V, de Almeida SM, Tuma P, Laselva CR, Neto MC, Klajner S, Teich VD, Kobayashi T, Edmond MB and Marra AR (2024) Prevalence, predictors, and patient-reported outcomes of long COVID in hospitalized and non-hospitalized patients from the city of São Paulo, Brazil. Front. Public Health. 11:1302669. doi: 10.3389/fpubh.2023.1302669
Edited by:
Nuno Sepulveda, Warsaw University of Technology, PolandReviewed by:
Dong Keon Yon, Kyung Hee University, Republic of KoreaCopyright © 2024 Malheiro, Bernardez-Pereira, Parreira, Pagliuso, de Paula Gomes, de Mesquita Escobosa, de Araújo, Pimenta, Lin, de Almeida, Tuma, Laselva, Neto, Klajner, Teich, Kobayashi, Edmond and Marra. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sabrina Bernardez-Pereira, c2FicmluYS5iZXJuYXJkZXpAZWluc3RlaW4uYnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.