
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 15 November 2023
Sec. Children and Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1290567
 Sarah J. Greeven1Andrew M. Medellin2Janette M. Watkins1,3Cassandra J. Coble1
Sarah J. Greeven1Andrew M. Medellin2Janette M. Watkins1,3Cassandra J. Coble1 Julia E. Brunnemer4Paola A. Fernández Solá2Sandeep Dutta5James M. Hobson6
Julia E. Brunnemer4Paola A. Fernández Solá2Sandeep Dutta5James M. Hobson6 Justin M. Evanovich5
Justin M. Evanovich5 Vanessa M. Martinez Kercher3
Vanessa M. Martinez Kercher3 Kyle A. Kercher1*
Kyle A. Kercher1*Introduction: Physical activity yields significant benefits, yet fewer than 1 in 4 youth meet federal guidelines. Children in rural areas from low socioeconomic (SES) backgrounds face unique physical activity contextual challenges. In line with Stage 0 with the NIH Stage Model for Behavioral Intervention Development, the objective of the present study was to conduct a community-engaged needs assessment survey with middle school children and adults to identify perceptions, barriers, and facilitators of physical activity, sport, psychological needs, and nutrition from a multi-level lens.
Methods: A cross-sectional survey data collection was conducted with children (n = 39) and adults (n = 63) from one middle school community in the Midwestern United States. The child sample was 33% 6th grade; 51% 7th grade and was 49% female. The adult sample was primarily between 30 and 39 years old (70%) and comprised predominantly of females (85%). Multi-level survey design was guided by the psychological needs mini-theory within self-determination theory and aimed to identify individual perceptions, barriers, and facilitators in line with the unique context of the community.
Results: At the individual level, 71.8% of children and 82.2% of the overall sample (children and adults) were interested in new physical activity/sport programming for their school. Likewise, 89.7% of children and 96.8% of adults agree that PA is good for physical health. For basic psychological needs in the overall sample, relatedness was significantly greater than the autonomy and competence subscales. Children’s fruit and vegetable intake were below recommended levels, yet only 43.6% of children were interested in nutritional programming. Conversely, 61.5% indicated interest at increasing leadership skills. At the policy-systems-environmental level, the respondents’ feedback indicated that the condition and availability of equipment are areas in need of improvement to encourage more physical activity. Qualitative responses are presented within for physical activity-related school policy changes.
Discussion: Interventions addressing children’s physical activity lack sustainability, scalability, and impact due to limited stakeholder involvement and often neglect early behavioral intervention stages. The present study identified perspectives, barriers, and facilitators of physical activity, sport, psychological needs, and nutrition in a multi-level context and forms the initial campus-community partnership between scientists and community stakeholders.
Participating in the recommended amount of physical activity (PA) has well-established benefits for physical, psychological, and socioemotional health (1). Despite these benefits, there remains a lack of engagement in PA-related health behaviors among children, particularly those who come from rural and low-socioeconomic status (SES) households (2–4). The disparities between rural and low-SES groups are related to differences in access to PA facilities and resources, as well as existing barriers for transportation, built environment, and socioeconomic status (3, 5, 6). Multi-level (i.e., individual, interpersonal, and community) and multicomponent interventions targeting PA and other positive lifestyle behaviors present an opportunity to reduce inequalities between population groups (7) and are more likely to be successful than single component interventions (8). While many lifestyle interventions have been conducted, few have focused on rural populations and emphasized sustainable multi-level impact on PA-related outcomes, and many have neglected the early stages of human-centered intervention design (7, 9, 10). Instead, many initiatives have imposed researcher’s agendas without adequately taking the time to include stakeholders wants, preferences, and cultural norms. Therefore, while there is general understanding of population-level disparities (e.g., barriers of transportation, cost, lack of feeling welcome), there is a lack of understanding about how the needs manifest in context at the detailed level required to make intervention design decisions.
Numerous lifestyle interventions have been conducted in children, however the outcomes have been mixed and the impact has been limited (8, 11, 12). Community stakeholders are often left feeling frustrated due to short-term emphasis, little long-term benefit, and research teams do not develop the infrastructure to sustain efforts (13, 14). Many interventions fail to scale-up in real world settings (15); as such, early collaboration is recommended between community stakeholders and scientists when designing, implementing, or evaluating interventions (15). Additionally, the existing body of lifestyle intervention literature is limited by a lack of integration of children into the research process. A recent review found less than 1% of published studies of children’s health studies included any form of advice from children regarding their perspectives, preferences, or developmental needs during the research process (16). This lack of inclusion of children in the development of lifestyle interventions fails to take advantage of the recognized unique perspectives and ideas children can contribute that are otherwise unavailable to adult researchers (17, 18). A promising psychological needs-supportive intervention was conducted by Meerits et al. (19) to boost parents’ need-supportive behaviors and support children’s intrinsic motivation for physical activity. Prior literature also supports the use of influential role models as a promising strategy for shaping positive PA experiences for students in PA and physical education (20, 21).
To build on past research and fill in gaps within the existing lifestyle intervention literature, research programs are needed that (1) dedicate significant time to early stages of intervention development and (2) follow systematic/evidence-based intervention development processes. One such approach that addresses these concerns is the National Institute of Health (NIH) Stage Model for Behavioral Intervention Development which aims to support development and testing of interventions at scale in real world settings (22, 23). To progress effectively through the early stages of the NIH Stage Model, a series of preliminary work is essential, including but not limited to using survey methodology that collects input from multiple community stakeholders regarding their wants, preferences, and resources. Collectively, these preliminary steps incorporating elements of community-based participatory research (CBPR) and human-centered design in line with the NIH Stage Model, allow for the foundation of developing a mutually beneficial campus-community partnership aiming to make a lasting impact. We will leverage a campus-community partnership for its myriad benefits, including the valuable opportunity to create collaborative engagements, drawing on diverse perspectives and resources to address real-world challenges and improve the overall quality of research endeavors.
CBPR and the establishment of a campus-community partnership are promising strategies that require essential rapport building to be done in the early stages of the research process. The NIH defines CBPR as programs supporting collaborative interventions that include researchers and community members to address health conditions disproportionately affecting health disparity populations. Relatedly, effective campus-community partnerships require continued investment in shared understanding and usage of common language, rules, expectations, and accountability (24). Partnerships involving campus and community stakeholders, with sport and/or nutrition at the forefront of the collaborations, are growing rapidly and have been associated with the promotion of healthy behaviors (25–27). However, too often is the case where campus-community partnerships are based upon a model that operates with university stakeholders as experts approaching communities as problems to fix (28). Specific examples of inequitable collaboration have been observed in decision-making and short-term programs driven by funding and its accompanying rules (29). Working groups, with stakeholders of diverse identities and roles, operate within a web of active relationships and partnerships with complex dynamics that require effective management and on-going analysis (30–32).
The present study takes a sport-based youth development approach to early-stage intervention development and future testing. Sport-based youth development utilizes sports as a “hook” to promote youth lifestyle development, incorporating physical, social, and psychological components (33). The adoption of sport-based youth developmental programming is driven by its innovative nature, harnessing the inherent benefits and appeal of sports to address and satisfy children’s psychological needs more effectively than conventional exercise initiatives (34). When delivered appropriately, sports foster an environment conducive to self-growth, psychological well-being, and self-esteem in youth (35).
Therefore, we conducted a multilevel needs assessment survey in line with Stage 0 of the NIH Stage Model for Behavioral Intervention Development. Despite knowledge of the PA-based needs of children from the population level, we need to develop specific understanding of how the needs manifest themselves in context at the level of detail needed to make intervention design decisions (36). Further, each rural community is unique and appropriate CBPR requires researcher teams to build rapport and attempt to understand community context prior to intervening. Thus, the objective of the present study was to conduct a needs assessment survey with middle school children and adults to identify perceptions, attributes, barriers, and facilitators of PA/sport, nutrition, and policy-systems-environment (PSE) that are responsive to the community context and preferences. This needs assessment will serve as a starting point for examining the PA-related context with the current middle school partner prior to informing future intervention development and testing.
Three complementary theoretical elements were used to guide the present study: (1) the psychological needs satisfaction mini-theory from self-determination theory (37, 38), (2) the National Institute of Minority Health and Health Disparities’ Research Framework (22), and (3) the biopsychosocial model (39). The psychological needs satisfaction mini theory proposes that enhancing a child’s well-being can be achieved by promoting autonomy, competence, and relatedness (40, 41). By incorporating the psychological needs mini theory, we were able to empirically support our examination of the relationship between proposed intervention components, psychological needs, and study outcomes to inform a future exploratory pilot/feasibility study (42–45). The NIMHD Research Framework was used to conceptualize multilevel factors in the survey design and interpretation. The biopsychosocial model guided the interpretation of results as PA, sport participation, nutrition, lifestyle behaviors, and PSE questions/items all exist within a broader biopsychosocial context (39, 46). This integrated conceptual approach is presented in Figure 1 and described further in prior research (36).
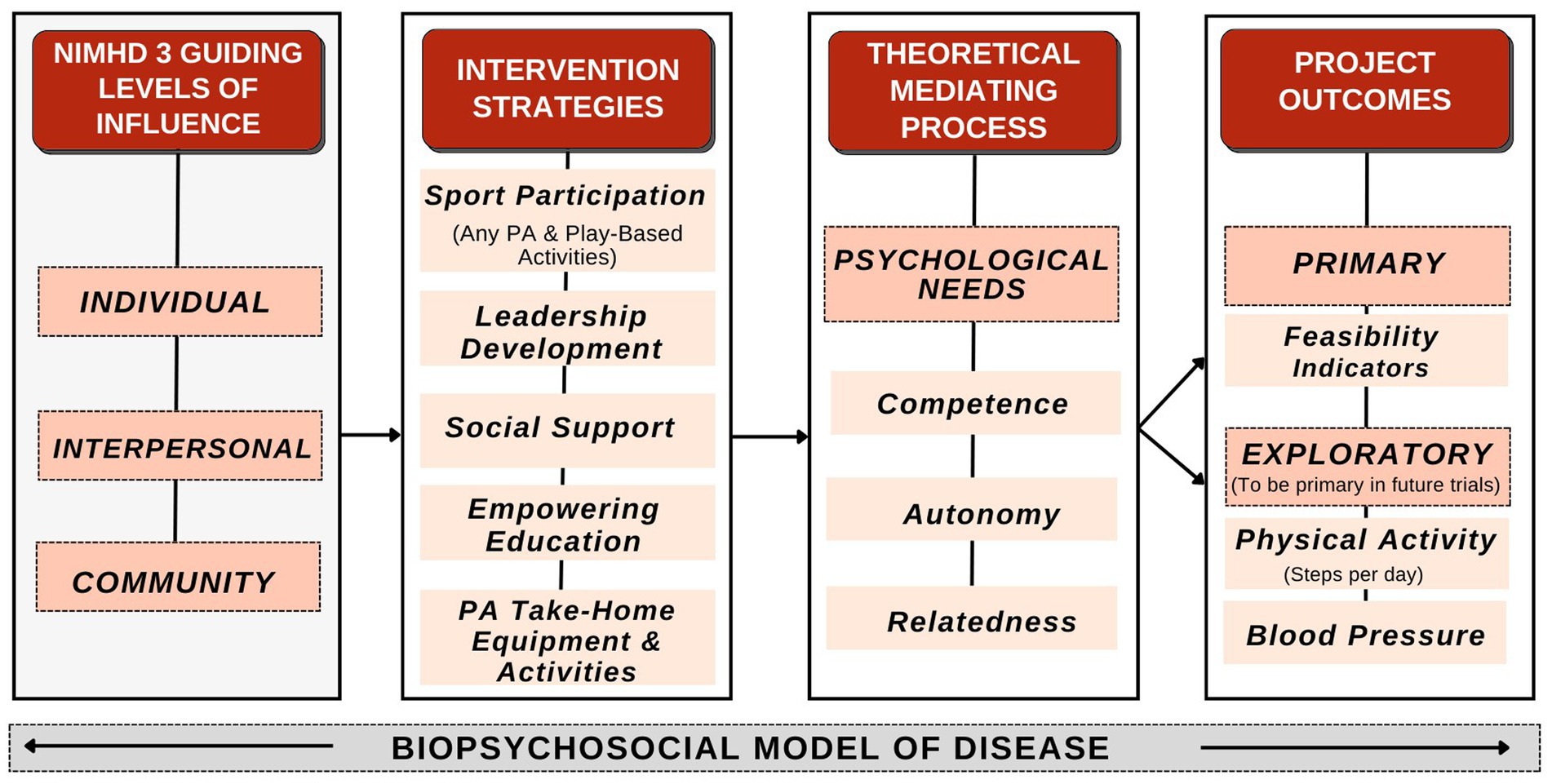
Figure 1. Hoosier sport conceptual framework.
This prospective cross-sectional cohort study included middle school children (n = 39) and adults (defined as parents, adult family members, adult caregivers of children, and/or teachers/administrators) (n = 63) from a rural community in Indiana during the 2023 spring semester. The school district serves approximately 800 students from predominantly low-income backgrounds. Of children living in the school district, 96% are non-Hispanic White (47). The district experiences high poverty as 52% of the residents live below the poverty line utilized by the Supplemental Nutrition Assistance Program Education (SNAP-Ed) (48), and the entire school system provides free breakfast and lunch for students with funding from the Department of Education. Moreover, geographical distance between homes, lack of access to physical activity resources, and unhealthy eating habits present significant barriers to positive health behaviors. While there are no specific estimates for physical inactivity among children in the target county, approximately 33% of adults in the Indiana community are physically inactive (47, 49).
Approval was obtained from the district school board and school stakeholders. There were separate inclusion criteria for children and adults. Children had to be enrolled at the middle school (i.e., 6th – 8th grade), attending school, and willing to participate in the survey. This age group was selected based on alignment in the campus-community partnership as well as a significant reduction in PA that has been observed in 6th grade students compared to other ages (50). Adults had to be parents, adult family members, and/or adult caregivers of children currently enrolled at the middle school or employed as teachers/administrators at the middle school and willing to participate in the survey. Adults were included to ensure a multi-level perspective from the target community was gained. There were no exclusion criteria for this study. All participants and their adult caregivers provided informed consent and assent (children). The Indiana University Institutional Review Board approved the study protocol (#18636).
After receiving consent from parents, we obtained assent from children before they participated in the study to ensure children fully understood the assent document information, including the purpose of the study, study requirements, and potential risks or benefits. Parental consent was collected remotely through an informed consent document distributed through Qualtrics survey software. Child assent and survey administration were conducted through Qualtrics and occurred in-person to increase compliance and understanding. The survey measures included demographics, the Physical Activity Questionnaire for Children (PAQ-C) (51–54), select items from the Expanded Food and Nutrition Education Program (EFNEP) Food and Physical Activity Behaviors Questionnaire (55), and Basic Psychological Needs in Exercise Scale (BPNES) (56, 57). Children were incentivized with a $10 gift card after completing the survey.
For the adult survey, we obtained consent and administered the survey remotely. Similar to the child survey, the adult surveys included demographics, questions from the EFNEP Food and Physical Activity Behaviors Questionnaire (55), BPNES (56, 57), as well as additional PSE questions from prior PA research (58). Adults were incentivized with a $10 e-gift card after completing the survey. All surveys included debriefing questions developed by survey methodologists from the Indiana University Center for Survey Research, encouraging participant feedback on survey methodology and assessing potential areas for improvement in future surveys. See the Measures section for additional details and see Supplemental materials S1, S2 for the complete child and adult surveys, respectively.
To assess physical activity and sport participation, participants completed the Physical Activity Questionnaire for Children (PAQ-C) (51, 54). The PAQ-C assessed PA during physical education class, recess, lunch, right after school, evening, weekends, and spare time. The PAQ-C consisted of ten items scored on a 5-point scale ranging from “no” activity being a 1 and “7 times or more” being a 5. A cumulative score of 1 indicates low PA, whereas a 5 indicates high PA (51, 54). In children, the PAQ-C has demonstrated good internal consistency, acceptable validity, and an adequate Cronbach’s alpha coefficient of 0.72–0.88 (52, 53). One complex PAQ-C question about PA on each of the past 7 days was omitted from the survey to reduce respondent burden.
Participants responded to two questions about perceived barriers to PA, sport, walking, running, bicycling, and exercising in their community. The response options were: Not enough areas/places to be physically active; Not enough sports teams/groups where I live; The places are run-down or do not have enough equipment; I cannot get to places to walk, run, bike, or be physically active easily; I’m not interested. These items were adapted from the Barriers to Being Active Quiz (59) to gain an understanding of specific barriers to PA/sport in the community.
Attitudes toward PA were assessed with three questions to get a sense of the respondents’ beliefs in the holistic value of PA for physical health, relationship building, and handling emotions. Interest in new types of PA-related programming was assessed with three questions about PA/sport programming, nutrition programming, and leadership programming. PA/sport and nutrition programming were assessed because those are two of the primary outcome areas of the program. Leadership programming was selected because school stakeholders expressed interest in leadership-specific programming to be included as part of the future intervention design. 4-point Likert scales were used for assessing attitudes and interest in new programming, ranging from “Not important/interested at all” to “Extremely important/interested.” Respondents moderately or extremely interested in PA/sport programming were categorized as agreeing and interested in new programming.
Questions from the EFNEP Food and Physical Activity Behaviors Questionnaire were used to assess dietary intake. Questions covered nutritional behaviors “over the last 7 days” and “yesterday.” Of the original 30 questions on the questionnaire, the research team selected eight questions for children and ten questions for adults to help ensure the survey will be feasible in terms of respondent burden. Response options allowed participants to select how often they consume various food and drink options. The EFNEP began in 1969, serves all states and U.S. territories, and reaches 450,000 low-income youth and 200,000 low-income adults each year (55, 60). The EFNEP consistently shows more than 90% of adults and 80% of youth report improved nutritional practices (60, 61).
Children and adults will rate the satisfaction of their psychological needs in exercise settings with the Basic Psychological Needs in Exercise Scale (BPNES). The BPNES measures psychological needs satisfaction in an exercise context based on autonomy, competence, and relatedness (56, 57, 62). The BPNES consists of 11 items that form a total score and three subscale scores for the degree to that the person experiences satisfaction of each of the three psychological needs. Scores are assessed on a 5-point Likert scale ranging from “I do not agree at all” to “I completely agree.” Four items assessed autonomy, four for competence, and three for relatedness (62). In adults, the BPNES has demonstrated adequate internal consistency with Cronbach’s alpha coefficients of 0.84 for autonomy, 0.81 for competence, and 0.92 for relatedness, as well as acceptable discriminant and predictive validity (57). The scale scores are also largely unaffected by social desirability bias and have demonstrated stability in repeated measures (57).
The adult survey included questions addressing the PSE level of influence. Questions assessed adults’ interest in PA, nutrition, positive behavioral programming, and perceptions of current school PA policies and interest in new school PA policies. PA environmental questions were informed by past research on perceived environmental variables that may influence PA (58, 63). As PA behaviors exist within an array of settings and levels of influence, questions focused on gaining an understanding of PA behaviors in various settings such as homes, neighborhoods, PA facilities, and parks. For the adult survey, PA-related questions were asked about programming and PA equipment they would like to see offered at the school. There was also a qualitative open-ended question asked to adults: “Do you think a new WRV school policy should be created to help WRV children be more physically active?” If respondents answered yes, then this item was presented: “Please describe the general idea or concept that you think a new policy should address.” These results are presented descriptively and categorized into themes identified by the research team in Table 1. See Supplemental materials S1, S2 for complete versions of the adult and child surveys, respectively.
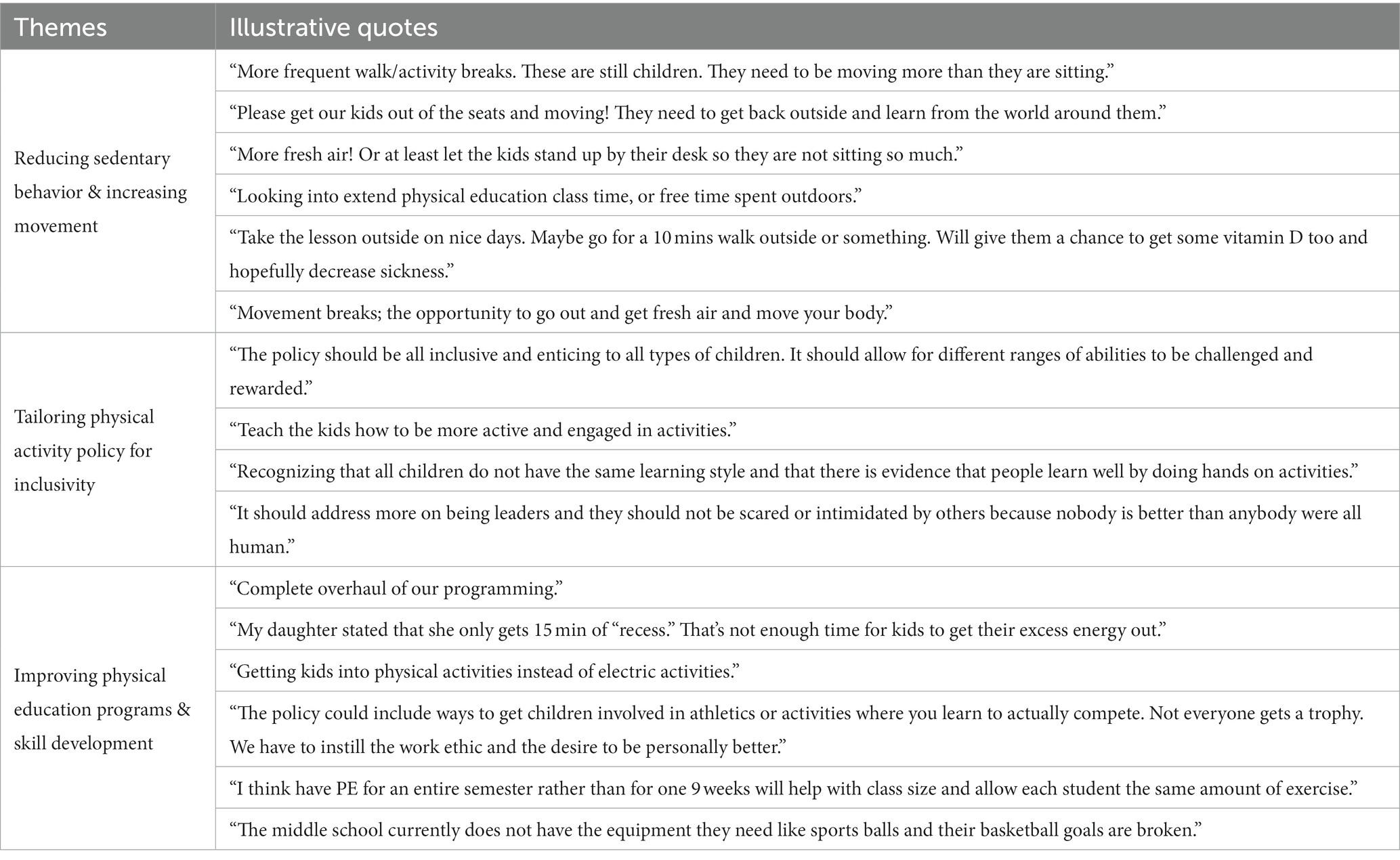
Table 1. Qualitative responses from parents policy-systems-environment questions.
Rather than hypothesis testing, the primary objective of the present study was to identify and describe opportunities, barriers, and facilitators to promote PA and healthy lifestyle behaviors in one rural middle school community. To accomplish this objective, the study team assessed the overall study sample, while from an exploratory standpoint also exploring differences between child and adult respondents for outcomes of interest (e.g., interest in programming). For descriptive statistics, frequencies and percentages were computed for each categorical variable, and means and standard deviations were calculated for continuous variables. Listwise deletion was used for handling missing data as any incomplete observations were dropped from analysis (n = 102), which reduced the total sample size to n = 39 children and n = 63 adults. A sensitivity analysis was conducted by running the analyses on the raw and final samples and the results were highly similar. Analyses were performed in R 4.0.3 (64) and the level of significance was set to alpha = 0.05 in the exploratory analyses.
A total of 102 respondents completed the survey (overall: n = 102; children: n = 39; adults: n = 63) out of a total 150 students at the middle school (response rate: 39/150 = 26%). The child sample was composed primarily of 6th and 7th grade students (33% 6th grade; 51% 7th grade) and was nearly equally distributed across biological sex (49% female). The adult sample was primarily between 30 and 39 years old (70%) and comprised predominantly of females (85%). The majority of respondents (96%) were Non-Hispanic White, with 37.0% having a high school diploma or lesser qualification, and 74.1% were married or living with a partner. Overall, 94% of participants identified as White. Table 2 provides detailed demographic data for the overall sample.
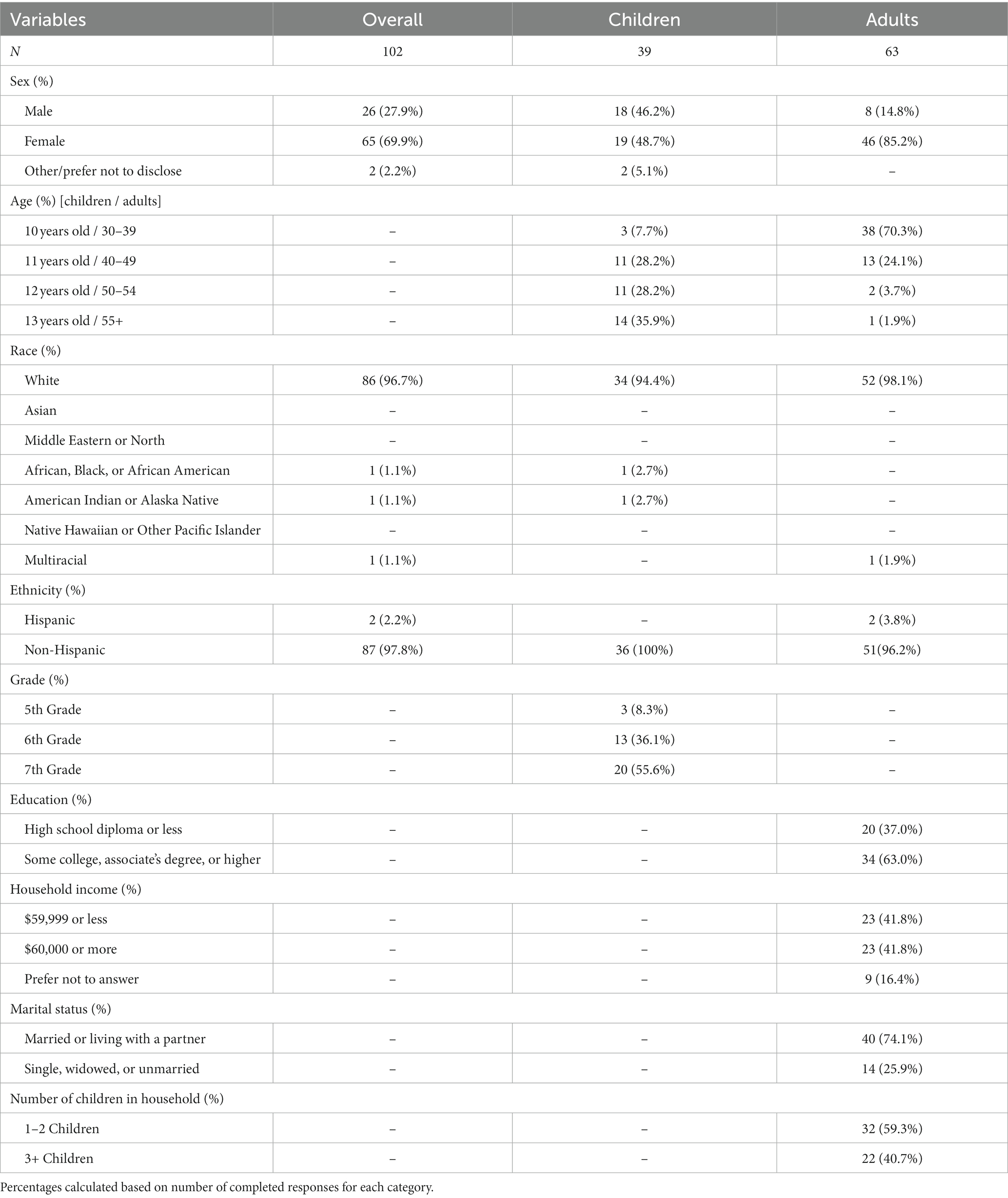
Table 2. Demographics.
Table 3 displays the types of PA and sports participated in by the child respondents. Our sample, including males and females, had a mean activity score of 2.96 which is consistent with past research that found means of between 2.85 to 3.16 for males and 2.56 to 2.79 for females (51). The score for the PAQ-C is between a 1 and 5 where a score of 1 indicates low PA and a score of 5 indicates high PA. The score of 2.96 shows a moderately active mean score for the child respondents (54). See Supplementary Table S2 for detailed item results for the PAQ-C. In the last 7 days, activities participated in most frequently (7+ times in the past week) by children were jogging and physical conditioning (11 respondents), followed by basketball and baseball/softball (7 respondents).
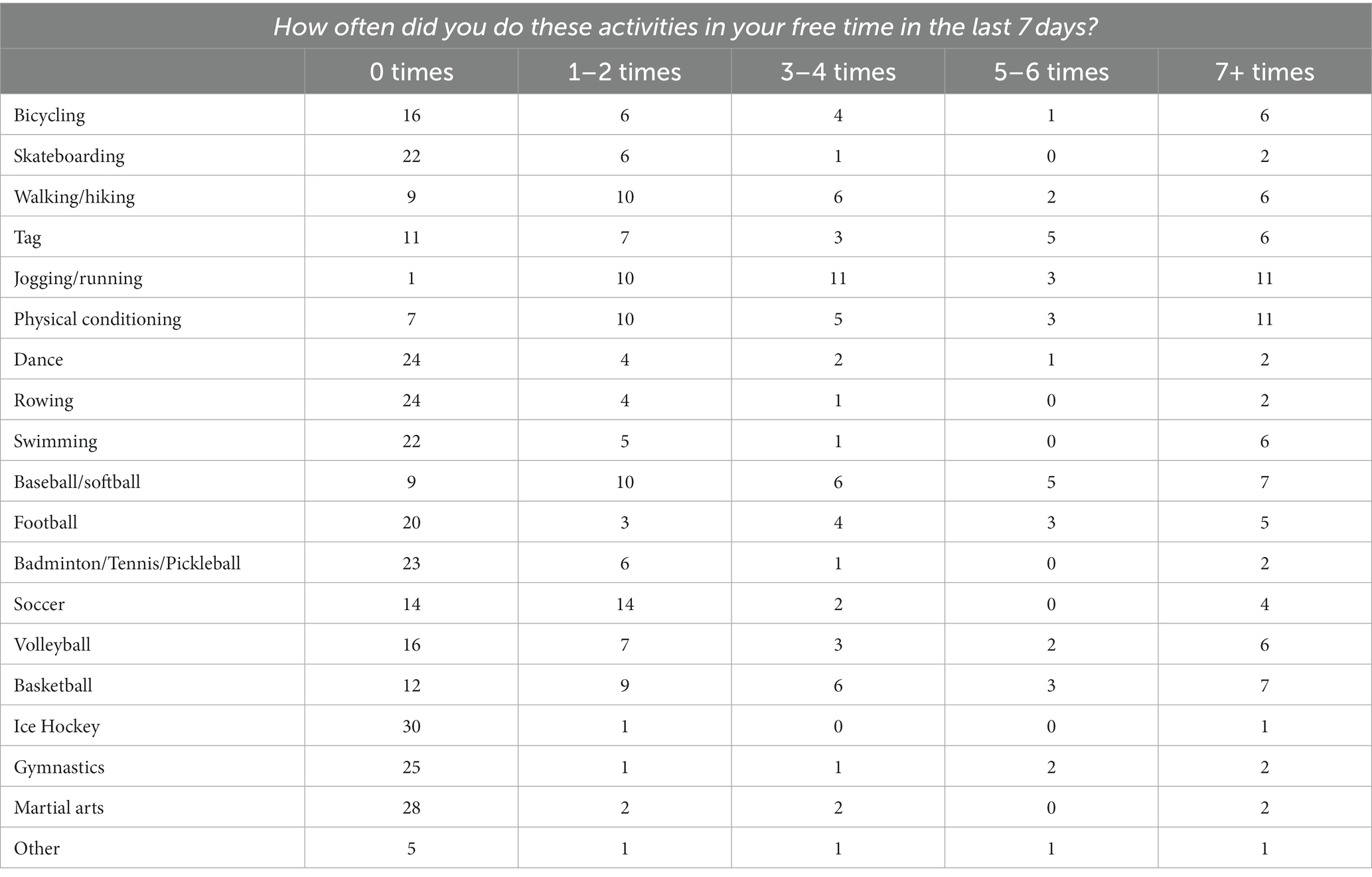
Table 3. Children’s physical activity and sport participation in the past week.
See Table 4 for barriers to PA and Table 5 for attitudes and interest in programming. Overall, participants perceived there were not enough areas to be physically active (47% of respondents) and the places to be active are run-down or do not have enough equipment (40%). For attitudes toward PA, a large majority of respondents believed PA is helpful for physical health (94.1% of respondents), relationship building (91.2%), and handling one’s emotions (87.3%). For interest in new programming at school in the overall sample, respondents were very interested in new PA/sport programming (82.2% of respondents), moderately interested in leadership programming (76.2%), and less interested in nutritional programming (67.0%; 43.6% of children). There were noticeable differences between children and adults in terms of interest in programming as adults were more interested in all three types of programming compared to the child group, but the pattern remained the same with PA/sport being favored, followed by leadership and nutrition programming.
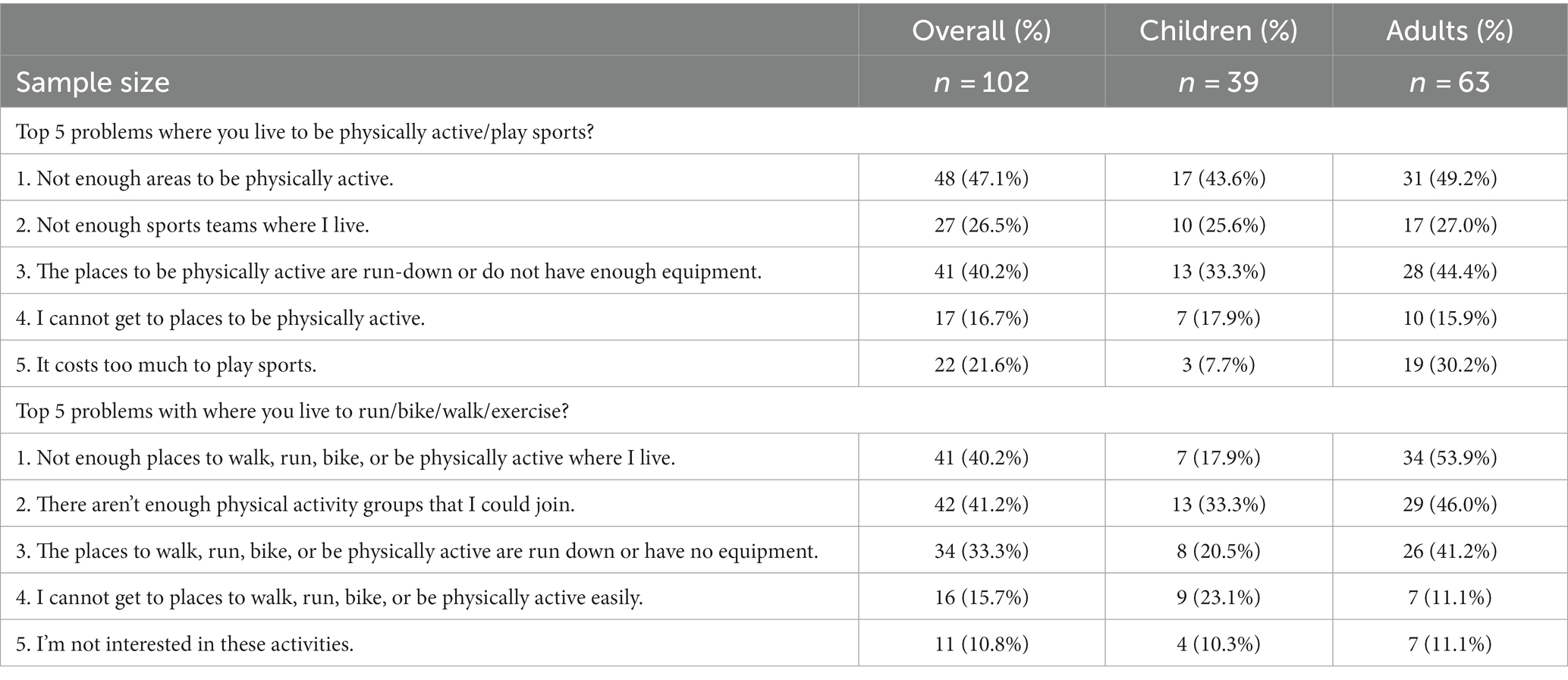
Table 4. Perceived barriers toward physical activity in the community.
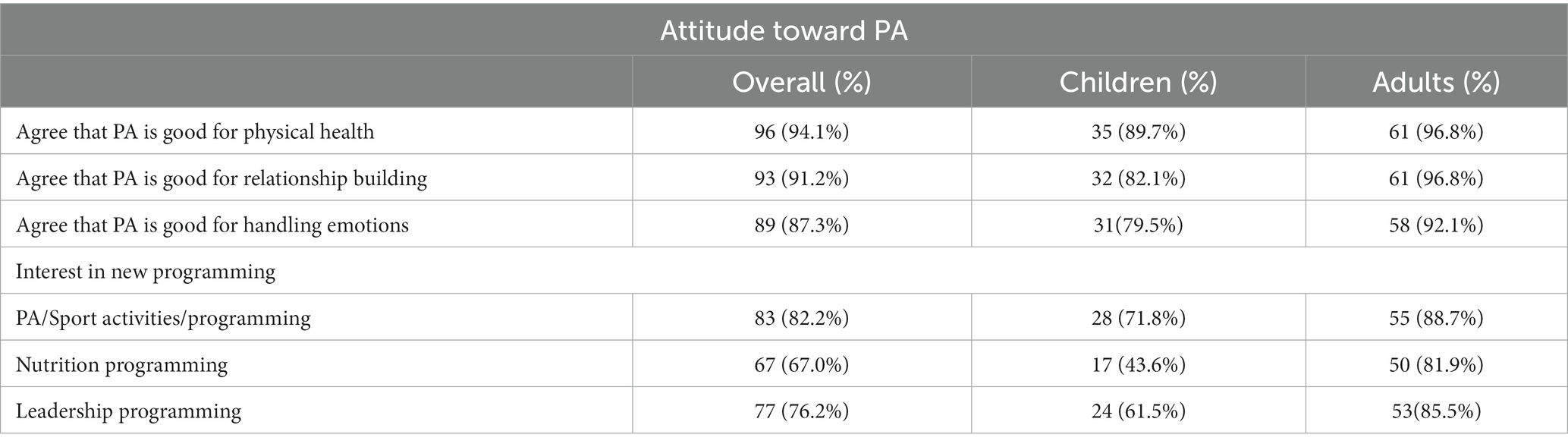
Table 5. Attitudes and interest in physical activity-related programming.
The top 3 sports/activities and sports equipment each group would like to see more of at their school are listed in Figure 2. The top sports that respondents would like to see at their school were baseball/softball (children), martial arts (adults), and basketball (overall sample). The top sports equipment desired by respondents were sports balls (children) and strength training equipment (adults and overall sample).
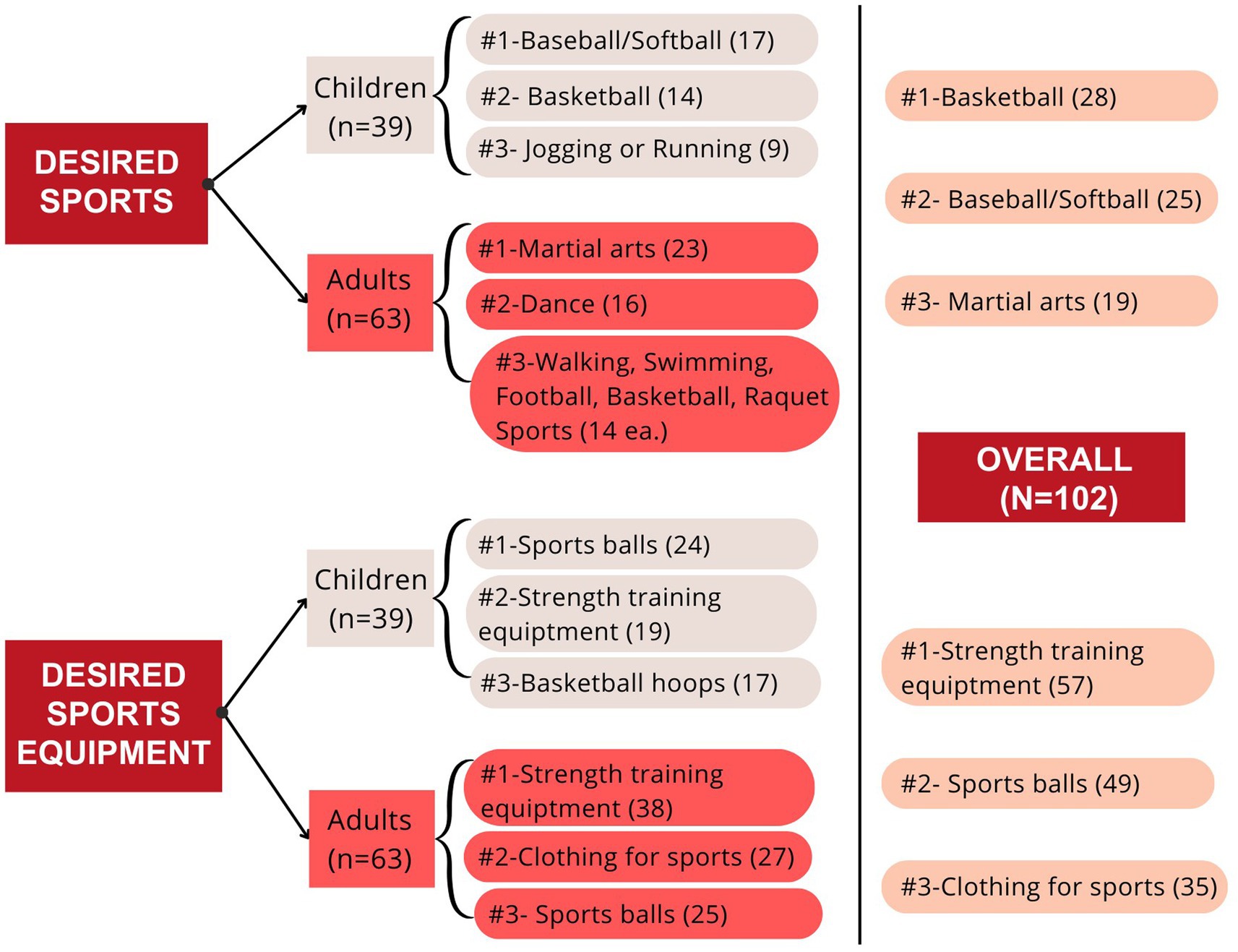
Figure 2. Ranking of top 3 desired sports/activities and equipment to have at school.
Table 6 illustrates results for nutritional behaviors based on the 7 days recall data from the overall sample, as well as specific breakdowns for child and adult respondents. The data from the child survey highlighted that fruit and vegetable intake were low in the past 7 days. 87.2% of children (34 out of 39 children) reported not consuming a daily serving of fruits and 97.4% did not consume a daily serving of vegetables (38 out of 39 children). 71.8% of children (28 out of 39 children) consumed red/orange vegetables on 0–2 days of the week. 76.9% of children (30 out of 39 children) consumed dark green vegetables on 0–2 days of the week. Children consumed at least one serving of fruit, red/orange vegetable, and dark green vegetables an average of 3.1 days (SD = 1.8), 1.5 days (SD = 1.6), and 1.3 days (SD = 1.5). Additionally, about 89.7% of children reported consuming sweetened beverages in the past week.
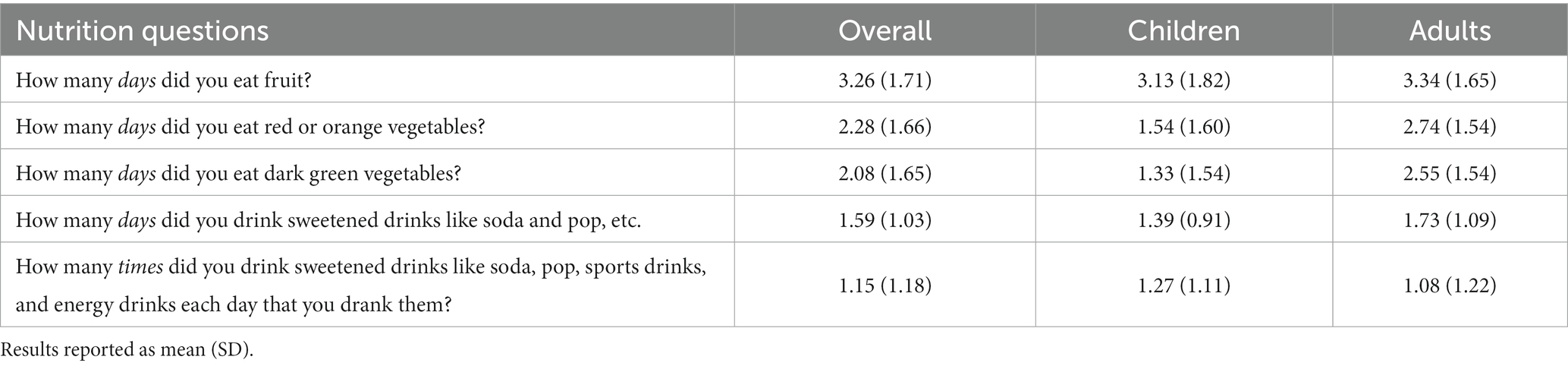
Table 6. 7 days food recall for child participants.
Table 7 displays the cumulative BPNES score as well as the subscale scores for autonomy, competence, and relatedness in the overall, child, and adult samples. For the overall sample, the cumulative score for the BPNES, combining all 11 items, had a mean score of 3.72 (SD = 0.99). The cumulative BPNES scores did not differ significantly between the child and adult groups. Further, the relatedness subscale score was also significantly greater in the adult group compared to the child group (p = 0.038). For children, the highest rated item was “I can easily talk to the people I am physically active with” [relatedness item]; and the lowest rated item was “I can do what I need to do to get what I want out of physical activity in my life” [competence item]. For adults, the highest rated item was “The relationships with the people I exercise with are friendly” [relatedness item]; and the lowest rated item was “I feel exercise is an activity which I do very well” [competence item].
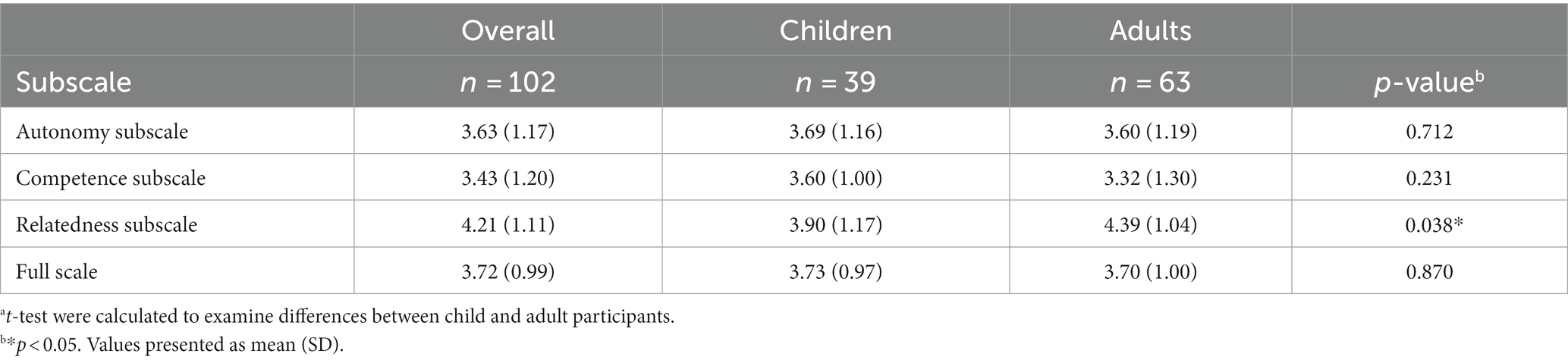
Table 7. Results for basic psychological needs satisfaction in exercise scalea.
Table 1 provides a summary of qualitative responses from adults to the question “Do you think a new WRV school policy should be created to help WRV children be more physically active? If they answered yes, then this item was presented: “Please describe the general idea or concept that you think a new policy should address.” 22 adults answered yes to the previous item (16 usable responses) and provided an idea or concept that were then categorized into three major themes: reducing sedentary behavior and increasing movement; tailoring physical activity policy for inclusivity; and improving physical education programs and skill development.
Although many interventions have been conducted to improve PA-related lifestyle behaviors in children, gaps remain in that stakeholders (including children) are often not part of the research process (16) and researchers neglect the early stages of intervention development where critical intervention design decisions are made (36). In line with evidence supporting collaboration between community members and scientists early in the intervention development process (15), this study focused on Stage 0 of the NIH Stage Model to conduct a needs assessment survey with children and adults from a rural Indiana middle school community. The survey focused on identifying perceptions, attributes, barriers, facilitators of PA/sport, nutrition, and PSE that are responsive to the community context. Key findings from this study were (1) a high level of interest in PA/sport programming; (2) basic psychological needs point to promising strengths to build upon and weaknesses to improve; (3) children’s nutritional behaviors were well below recommended levels and they are not very interested in nutrition programming; and (4) adults were engaged in providing ideas for PA-promoting school policy changes. These results are supported by previous work which found school-based PA interventions to be a successful mode for increasing health behaviors (7, 9). Furthermore, this study addresses two major knowledge gaps in literature by (1) establishing a campus-community partnership with a rural school community and (2) providing data to support the success of a multicomponent intervention to increase PA and healthy behaviors (7, 8, 10). The findings from this study will be discussed below and used to inform the next stages of human-centered intervention design prior to pilot/feasibility testing an intervention called Hoosier Sport in the partner middle school. In addition, within the title of our intervention, “Hoosier,” is a prideful term to describe a resident of Indiana.
Similar to nationally representative samples and prior PA literature (65, 66), children in the present study reported lower than recommended levels of physical activity participation. Past research has suggested that the steepest declines in physical activity may occur in 5th and 6th grade children compared to other ages (50). Thus, the present survey results combined with mandatory attendance in middle school point to the middle school as an impactful and promising intervention setting. Child respondents reported participating in many different sports and PAs on a weekly basis, and both children and adults were highly interested in new PA/sport programming being offered at their school (82.2% of overall respondents). Compared to national norms where nearly a quarter of public schools in the United States do not offer sports (23.5%) (67), the middle school in the present study offers 9 sports for girls and 7 sports for boys. Further, data from a nationally representative sample indicate that 33.6% of high poverty schools did not offer sports, compared to only 15.4% of low poverty schools not offering sports (67). Thus, despite being in a high poverty district, the school continues to value and offer a variety of sports to students.
Given the high number of sport/PA offerings from our school partner, it is promising that 72% of children surveyed and 82% of the overall sample are moderately or extremely interested in new sport/PA programming. Additionally, this high level of respondent interest is promising for subsequent intervention design stages, considering that community needs, wants, and preferences will be leveraged rather than preconceived ideas of exercise and sport needs from researchers. Further, an important differentiation between early-stage intervention development in the present study compared to more traditional exercise interventions is that the present study follows a sport-based youth development approach. Based on the high level of interest in new sport/PA programming, our approach looks promising for rooting early-stage intervention development in sport-based youth development and integrating basic psychological needs. Framing Hoosier Sport as a sport-based youth development intervention with strong foundations in basic psychological needs may provide a more promising approach than the more traditional intervention approach of targeting obesity and PA by requiring students to do PA for a total of 1 hour per day, which does not capitalize on fun, enjoyability, and positive psychology that may be more accessible through the power of sport. It may be possible that failing to create a fun and enjoyable PA/sport-related context could be a fundamental flaw of many past interventions targeting PA and related lifestyle behaviors.
Our second set of key findings were from the basic psychological needs satisfaction results. In both the child group and adult group, the relatedness subscale was significantly higher than the autonomy and competence subscales. This supports the emphasis by Howie et al. (68) on the potentially positive value of youth sport participation for social health (i.e., relatedness). In terms of future intervention development and evaluation, strong relatedness scores point to co-designing intervention protocol to build on the relatedness psychological need while focusing on improving competency and autonomy. For example, co-design teams may be able to use existing friendships, social supports, or peer-mentoring (i.e., relatedness) to support children in learning new skills (i.e., competence) such as dribbling sports balls in soccer or basketball, learning game rules, or achieving tangible goals in creative school activity programs. Lower competence scores point to an opportunity for competency building activities like SMART goal setting (69) and age-appropriate sport skill developmental activities. As the Hoosier Sport project begins to identify and select intervention strategies, behavioral classification systems targeting each psychological need could be used, as identified in recent research from Ahmadi et al. (70).
While the primary focus of Hoosier Sport is on children, the inclusion of results for adults is also important because children exist within the inseparable context of families and parents, which have a direct influence on child health behaviors (71–73). As these findings are used to develop future intervention protocol, the results from adult respondents are important to support targeting a multi-level intervention strategy with the possibility of influencing adult caregiver (e.g., lifestyle educational materials) and teacher (e.g., professional development training) psychological needs satisfaction. An example of a competency-based strategy that may have a positive impact on both teachers and parents is training on the LET US Play principles for enhancing PA (LET US Play stands for: eliminate Lines; avoid Elimination games; reduce Team sizes; minimize Uninvolved kids; adjusting Space, equipment, rules for maximizing PA). If our intervention protocol successfully targets improvements in exercise-related competency in parents and teachers, then children are likely to come in contact with and be influenced by those adults with increased PA-related competency. Further, our preliminary BPNES findings connect the present study to the greater body of psychological needs literature within self-determination theory and provide a concrete example of how the research design has integrated existing theoretical components into various stages of intervention design, implementation, and evaluation. Rigorous design and evaluation are currently lacking within existing sport for social development literature, as many of the programs have been implemented by health and/or non-profit agencies rather than research institutions (68).
The third key finding from the study was that despite nutrition behaviors being below national recommendations (e.g., fruit, vegetable, and sweetened drink intake), children are not very interested in nutrition programming. Only 43.6% of children were interested in new nutrition programming at school compared to 71.8 and 61.5% of children being interested in PA/sport and leadership programming, respectively. To overcome the lack of excitement around nutrition programming, our findings highlight the need for fun and engaging intervention design to target children’s psychological needs satisfaction (i.e., autonomy, competence, relatedness) in a nutritional context. If given the autonomous choice between participating in different types of health programming, children are unlikely to engage in nutrition programming unless it is designed in a fun and engaging way.
Further, the 7 days nutritional recall data from our child respondents highlighted a concerning nutritional situation and potential opportunity for intervention as 87.2% of children reported not consuming a daily serving of fruit; 97.4% of children reported not consuming a daily serving of vegetables; and 89.7% of children reported consuming sweetened beverages at least once in the past week. While the low levels of fruit and vegetable intake are well recognized from a high-level population perspective, these results offer important contextualization and implications in the target community. Rural residents are often under-represented in research, but these results illuminate significant health challenges which help to provide evidence for the rationale of including nutritional education, hands-on nutritional activities, and practical food tasting intervention strategies in our upcoming multicomponent PA-based intervention. The low levels of fruit and vegetable intake in the present study are similar, yet more stark, in comparison to findings from a recent study from the Centers for Disease Control & Prevention (74) which found that in Indiana 43.1% of children did not consume a daily serving of fruit, 53% of children did not consume a daily serving of vegetables, and 66.7% of children consumed sugary beverages at least once weekly. Compared to national norms, Indiana was approximately 5–10% worse with each of the three aforementioned nutritional indicators.
The final key finding based on the open-ended adult PSE responses is the need for new policies to enhance PA and nutrition among WRV children. After expressing interest in the need for improved PA policy, the respondents were then asked to clarify the fundamental concepts that the PA policy should entail. Of the 63 adult respondents, 22 provided responses, revealing three prominent themes: (1) reducing sedentary behavior and increasing movement; (2) customizing PA policies for inclusiveness; and (3) enhancing physical education programs by fostering interpersonal skill development. Regarding inclusivity, the PA policy will cater to diverse abilities and learning styles by promoting active engagement, leadership, and confidence-building activities. In addition, to enhance educational attainment during in-school programming, respondents recommended additional breaks during the day to allow for PA and energy release to maintain focus throughout the school day. Overall, the qualitative responses underscored the awareness and interest of adults in their children’s PA behaviors at school, emphasized an inclusive approach to PA, by recognized the potential value of PA/sport in teaching valuable life skills.
The findings from this study should be interpreted within the study limitations. The present study had a cross-sectional design, and thus causation should not be assumed; rather the study interpretation focused on descriptive statistics and correlation. The study had a non-representative sample, 94% White, but in this case, we were satisfied with that distribution since the community we are collaborating with matches that racial demographic distribution. Although a limitation of this study was that it was convenience sample, we attempted to increase representativeness of the sample by sending the initial study recruitment message to all middle school students through the school administrators, rather than recruiting through athletic groups (e.g., sports teams, at PE class). There was a lack of male representation in the adult sample (85% female); however, the child sample was made up of 49% of respondents identifying as female. Finally, we recognize that inclusivity is a challenge when developing interventions and not all children are interested in group-based physical activity. As such, the results from this survey will help to guide the development of our individualized PA-related goal setting process for future school-based PA interventions. Despite these limitations, the present study highlights a promising CBPR approach to early-stage intervention development that may help lead to more promising interventions putting target communities’ needs, wants, and preferences at the center of the research process. From a practical standpoint, the results from this study will directly inform our next step of intervention design during agenda planning for the human-centered participatory co-design process with children and adults from the partner middle school.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Indiana University Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
SG: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Validation, Writing – original draft, Writing – review & editing. AM: Conceptualization, Formal analysis, Methodology, Software, Visualization, Writing – original draft, Writing – review & editing. JW: Writing - reviewing & editing, Visualization, Project administration, Methodology, Supervision. CC: Conceptualization, Funding acquisition, Supervision, Writing – review & editing. JB: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Visualization, Writing – review & editing. PF: Conceptualization, Methodology, Visualization, Writing – review & editing. SD: Conceptualization, Investigation, Methodology, Resources, Writing – original draft, Writing – review & editing. JH: Writing - reviewing & editing, Data curation, Visualization, Resources, Project administration, Methodology, Supervision. JE: Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing. VM: Conceptualization, Funding acquisition, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. KK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the SNAP-Ed grant program within the Division of Nutrition and Physical Activity at the Indiana Department of Health, as well as the Indiana University Office of the Vice Provost of Research, and the Indiana University Center for Innovative Teaching and Learning.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1290567/full#supplementary-material
PA, physical activity; CBPR, community-based participatory research; BPNES, Basic Psychological Needs in Exercise Scale; EFNEP, Expanded Food and Nutrition Education Program; PSE, policy-systems-environment; NIH, National Institutes of Health; SNAP-Ed, Supplemental Nutrition Assistance Program Education.
1. U.S. Department of Health and Human Services. Physical activity guidelines for Americans. 2nd ed U.S. Government Printing Office (2019).
2. Liu, JH, Jones, SJ, Sun, H, Probst, JC, Merchant, AT, and Cavicchia, P. Diet, physical activity, and sedentary behaviors as risk factors for childhood obesity: an urban and rural comparison. Child Obes. (2012) 8:440–8. doi: 10.1089/chi.2012.0090
4. Kegler, MC, Gauthreaux, N, Hermstad, A, Arriola, KJ, Mickens, A, Ditzel, K, et al. Inequities in physical activity environments and leisure-time physical activity in rural communities. Prev Chronic Dis. (2022) 19:E40. doi: 10.5888/pcd19.210417
5. The Aspen Institute. (2021). Youth sports facts: sports participation and physical activity rates, Available at: https://www.aspenprojectplay.org/youth-sports-facts/participation-rates.
6. Johnson, JA 3rd, and Johnson, AM. Urban-rural differences in childhood and adolescent obesity in the United States: a systematic review and meta-analysis. Child Obes. (2015) 11:233–41. doi: 10.1089/chi.2014.0085
7. Messing, S, Rütten, A, Abu-Omar, K, Ungerer-Röhrich, U, Goodwin, L, Burlacu, I, et al. How can physical activity be promoted among children and adolescents? A systematic review of reviews across settings. Front Public Health. (2019) 7:55. doi: 10.3389/fpubh.2019.00055
8. Russ, LB, Webster, CA, Beets, MW, and Phillips, DS. Systematic review and meta-analysis of multi-component interventions through schools to increase physical activity. J Phys Act Health. (2015) 12:1436–46. doi: 10.1123/jpah.2014-0244
9. Demetriou, Y, Gillison, F, and McKenzie, TL. After-school physical activity interventions on child and adolescent physical activity and health: a review of reviews. Adv Phys Educ. (2017) 7:191–215. doi: 10.4236/ape.2017.72017
10. Pope, KJ, Whitcomb, C, Vu, M, Harrison, LM, Gittelsohn, J, Ward, D, et al. Barriers, facilitators, and opportunities to promote healthy weight behaviors among preschool-aged children in two rural U.S communities. BMC Public Health. (2023) 23:53. doi: 10.1186/s12889-022-14770-w
11. Naylor, P-J, Nettlefold, L, Race, D, Hoy, C, Ashe, MC, Wharf Higgins, J, et al. Implementation of school based physical activity interventions: a systematic review. Prev Med. (2015) 72:95–115. doi: 10.1016/j.ypmed.2014.12.034
12. Andermo, S, Hallgren, M, Nguyen, TTD, Jonsson, S, Petersen, S, Friberg, M, et al. School-related physical activity interventions and mental health among children: a systematic review and meta-analysis. Sports Med Open. (2020) 6:1–27. doi: 10.1186/s40798-020-00254-x
13. Albert, A, Islam, S, Haklay, M, and McEachan, RRC. Nothing about us without us: a co-production strategy for communities, researchers and stakeholders to identify ways of improving health and reducing inequalities. Health Expect. (2023) 26:836–46. doi: 10.1111/hex.13709
14. Holkup, PA, Tripp-Reimer, T, Salois, EM, and Weinert, C. Community-based participatory research: an approach to intervention research with a native American community. ANS Adv Nurs Sci. (2004) 27:162–75. doi: 10.1097/00012272-200407000-00002
15. Brandes, M, Brandes, B, Sell, L, Sacheck, JM, Chinapaw, M, Lubans, DR, et al. How to select interventions for promoting physical activity in schools? Combining preferences of stakeholders and scientists. Int J Behav Nutr Phys Act. (2023) 20:48. doi: 10.1186/s12966-023-01452-y
16. Sellars, E, Pavarini, G, Michelson, D, Creswell, C, and Fazel, M. Young people’s advisory groups in health research: scoping review and mapping of practices. Arch Dis Child. (2021) 106:698–704. doi: 10.1136/archdischild-2020-320452
17. Dennehy, R, Cronin, M, and Arensman, E. Involving young people in cyberbullying research: the implementation and evaluation of a rights-based approach. Health Expect. (2019) 22:54–64. doi: 10.1111/hex.12830
18. Larsson, I, Staland-Nyman, C, Svedberg, P, Nygren, JM, and Carlsson, IM. Children and young people’s participation in developing interventions in health and well-being: a scoping review. BMC Health Serv Res. (2018) 18:507. doi: 10.1186/s12913-018-3219-2
19. Meerits, PR, Tilga, H, and Koka, A. Web-based need-supportive parenting program to promote physical activity in secondary school students: a randomized controlled pilot trial. BMC Public Health. (2023) 23:1627. doi: 10.1186/s12889-023-16528-4
20. Bureau, JS, Howard, JL, Chong, JXY, and Guay, F. Pathways to student motivation: a meta-analysis of antecedents of autonomous and controlled motivations. Rev Educ Res. (2022) 92:46–72. doi: 10.3102/00346543211042426
21. Vasconcellos, D, Parker, PD, Hilland, T, Cinelli, R, Owen, KB, Kapsal, N, et al. Self-determination theory applied to physical education: a systematic review and meta-analysis. J Educ Psychol. (2020) 112:1444–69. doi: 10.1037/edu0000420
22. National Institute on Minority Health and Health Disparities. (2018). NIMHD research framework. Available at: https://www.nimhd.nih.gov/about/overview/research-framework/nimhd-framework.html.
23. National Institute on Aging. (2023). The NIH stage model: can it help us create better interventions? Available at: https://www.nia.nih.gov/research/blog/2023/03/nih-stage-model-can-it-help-us-create-better-interventions.
24. Parent, MM, and Harvey, J. Towards a management model for sport and physical activity community-based partnerships. Eur Sport Manag Q. (2009) 9:23–45. doi: 10.1080/16184740802461694
25. Bruening, JE, Fuller, RD, and Percy, VE. A multilevel analysis of a campus-community partnership. J Serv Learn High Educ. (2015) 4:n1
26. Toh, C, Chew, S, and Tan, C. Prevention and control of non-communicable diseases in Singapore: a review of national health promotion programmes. Singapore Med J. (2002) 43:333–9.
27. Cameron, C, Craig, C, Coles, C, and Cragg, S. Increasing physical activity: encouraging physical activity through school. Ottawa: Canadian Fit Lifestyle Res Inst (2003).
28. Boyer, EL. Scholarship reconsidered: priorities of the professoriate. Lawrenceville, NJ: Princeton University Press, ERIC (1990).
29. Bringle, RG, and Hatcher, JA. Campus–community partnerships: the terms of engagement. J Soc Issues. (2002) 58:503–16. doi: 10.1111/1540-4560.00273
30. Sandy, M, and Holland, BA. Different worlds and common ground: community partner perspectives on campus-community partnerships. Michigan J Community Serv Learn. (2006) 13:30–43.
31. Dötterweich, JA. Building effective community partnerships for youth development: lessons learned from ACT for youth. J Public Health Manag Pract. (2006) 12:S51–7. doi: 10.1097/00124784-200611001-00011
32. Walsh, D. Best practices in university-community partnerships: lessons learned from a physical-activity-based program. J Phys Educ Recreat Dance. (2006) 77:45–56. doi: 10.1080/07303084.2006.10597863
33. Perkins, DF, and Noam, GG. Characteristics of sports-based youth development programs. New Dir Youth Dev. (2007) 2007:75–84. doi: 10.1002/yd.224
34. Schneider, ML, and Kwan, BM. Psychological need satisfaction, intrinsic motivation and affective response to exercise in adolescents. Psychol Sport Exerc. (2013) 14:776–85. doi: 10.1016/j.psychsport.2013.04.005
35. Super, S, Hermens, N, Verkooijen, K, and Koelen, M. Examining the relationship between sports participation and youth developmental outcomes for socially vulnerable youth. BMC Public Health. (2018) 18:1012. doi: 10.1186/s12889-018-5955-y
36. Greeven, SJ, Fernández Solá, PA, (Martinez) Kercher, VM, Coble, CJ, Pope, KJ, Erinosho, TO, et al. Hoosier sport: a research protocol for a multilevel physical activity-based intervention in rural Indiana. Front Public Health. (2023) 11:1243560. doi: 10.3389/fpubh.2023.1243560
37. Deci, EL, and Ryan, RM. The general causality orientations scale: self-determination in personality. J Res Pers. (1985) 19:109–34. doi: 10.1016/0092-6566(85)90023-6
38. Deci, EL, and Ryan, RM. Intrinsic motivation and self-determination in human behavior. University of Rochester, Rochester, USA: Springer Science & Business Media (2013).
39. Engel, GL. The need for a new medical model: a challenge for biomedicine. Science. (1977) 196:129–36. doi: 10.1126/science.847460
40. Martela, F, and Riekki, TJJ. Autonomy, competence, relatedness, and beneficence: a multicultural comparison of the four pathways to meaningful work. Front Psychol. (2018) 9:1157. doi: 10.3389/fpsyg.2018.01157
41. Sebire, SJ, Jago, R, Fox, KR, Edwards, MJ, and Thompson, JL. Testing a self-determination theory model of children’s physical activity motivation: a cross-sectional study. Int J Behav Nutr Phys Act. (2013) 10:111. doi: 10.1186/1479-5868-10-111
42. Leenstra, T, Keeler, L, Arthur-Cameselle, J, and Russell, K. The peer mentor experience in a physical activity intervention for mental health. Mentor Tutoring: Partnersh Learn. (2019) 27:68–87. doi: 10.1080/13611267.2019.1583410
43. Ntoumanis, N, Ng, JYY, Prestwich, A, Quested, E, Hancox, JE, Thøgersen-Ntoumani, C, et al. A meta-analysis of self-determination theory-informed intervention studies in the health domain: effects on motivation, health behavior, physical, and psychological health. Health Psychol Rev. (2021) 15:214–44. doi: 10.1080/17437199.2020.1718529
44. Raabe, J, Schmidt, K, Carl, J, and Höner, O. The effectiveness of autonomy support interventions with physical education teachers and youth sport coaches: a systematic review. J Sport Exerc Psychol. (2019) 41:345–55. doi: 10.1123/jsep.2019-0026
45. Raedeke, TD, and Hayes, M. Feasibility of project mentor: a mentoring program based on self-determination theory for adolescents classified as overweight. Res Q Exerc Sport. (2023):1–14. doi: 10.1080/02701367.2023.2167912
46. John, JM, Haug, V, and Thiel, A. Physical activity behavior from a transdisciplinary biopsychosocial perspective: a scoping review. Sports Med Open. (2020) 6:49. doi: 10.1186/s40798-020-00279-2
47. University of Wisconsin Population Health Institute. (2022). County Health Rankings & Roadmaps. Available at: https://www.countyhealthrankings.org/explore-health-rankings/indiana/greene?year=2022
48. Feeding America. (2023). Food insecurity among overall (all ages) population in Greene County. Available at: https://map.feedingamerica.org/county/2019/overall/indiana/county/greene
49. Wang, Y, Min, J, Khuri, J, and Li, M. A systematic examination of the association between parental and child obesity across countries. Adv Nutr. (2017) 8:436–48. doi: 10.3945/an.116.013235
50. Friel, CP, Duran, AT, Shechter, A, and Diaz, KMUS. Children meeting physical activity, screen time, and sleep guidelines. Am J Prev Med. (2020) 59:513–21. doi: 10.1016/j.amepre.2020.05.007
51. Crocker, PR, Bailey, DA, Faulkner, RA, Kowalski, KC, and McGrath, R. Measuring general levels of physical activity: preliminary evidence for the physical activity questionnaire for older children. Med Sci Sports Exerc. (1997) 29:1344–9. doi: 10.1097/00005768-199710000-00011
52. Janz, KF, Lutuchy, EM, Wenthe, P, and Levy, SM. Measuring activity in children and adolescents using self-report: PAQ-C and PAQ-A. Med Sci Sports Exerc. (2008) 40:767–72. doi: 10.1249/MSS.0b013e3181620ed1
53. Marasso, D, Lupo, C, Collura, S, Rainoldi, A, and Brustio, PR. Subjective versus objective measure of physical activity: a systematic review and meta-analysis of the convergent validity of the physical activity questionnaire for children (PAQ-C). Int J Environ Res Public Health. (2021) 18:3413. doi: 10.3390/ijerph18073413
54. Kowalski, KC, Crocker, PR, and Donen, RM. The physical activity questionnaire for older children (PAQ-C) and adolescents (PAQ-A) manual. Coll Kinesiol Univ Sask. (2004) 87:1–38.
55. Murray, EK, Auld, G, Baker, SS, Barale, K, Franck, K, Khan, T, et al. Methodology for developing a new EFNEP food and physical activity behaviors questionnaire. J Nutr Educ Behav. (2017) 49:777–783.e1. doi: 10.1016/j.jneb.2017.05.341
56. Costa, LCAD, Maroco, J, and Vieira, LF. Validation of the basic psychological needs in exercise scale (BPNES). J Phys Educ. (2018) 28. doi: 10.4025/jphyseduc.v28i1.2847
57. Vlachopoulos, SP, and Michailidou, S. Development and initial validation of a measure of autonomy, competence, and relatedness in exercise: the basic psychological needs in exercise scale. Meas Phys Educ Exerc Sci. (2006) 10:179–201. doi: 10.1207/s15327841mpee1003_4
58. Sallis, JF, Johnson, MF, Calfas, KJ, Caparosa, S, and Nichols, JF. Assessing perceived physical environmental variables that may influence physical activity. Res Q Exerc Sport. (1997) 68:345–51. doi: 10.1080/02701367.1997.10608015
59. Health, U. D. o. & Human Services. (1999). Promoting physical activity: a guide for community action. Champaign, IL: Human Kinetics, 67–73.
60. United States Department of Agriculture National Institute of Food and Agriculture. (2023). About EFNEP. Available at: https://www.nifa.usda.gov/grants/programs/capacity-grants/efnep/about-efnep.
61. United States Department of Agriculture National Institute of Food and Agriculture. (2023). Expanded food and nutrition education program (EFNEP) FY2022 National Reports. United States Department of Agriculture.
62. Vlachopoulos, SP, Ntoumanis, N, and Smith, AL. The basic psychological needs in exercise scale: translation and evidence for cross-cultural validity. Int J Sport Exerc Psychol. (2010) 8:394–412. doi: 10.1080/1612197X.2010.9671960
63. Ausenhus, C, Gold, JM, Perry, CK, Kozak, AT, Wang, ML, Jang, SH, et al. Factors impacting implementation of nutrition and physical activity policies in rural schools. BMC Public Health. (2023) 23:308. doi: 10.1186/s12889-023-15176-y
64. Team, R. C. (2020). R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Available at: https://www.R-project.org/ [Google Scholar].
65. Chung, AE, Skinner, AC, Steiner, MJ, and Perrin, EM. Physical activity and BMI in a nationally representative sample of children and adolescents. Clin Pediatr. (2012) 51:122–9. doi: 10.1177/0009922811417291
66. van Sluijs, EMF, Ekelund, U, Crochemore-Silva, I, Guthold, R, Ha, A, Lubans, D, et al. Physical activity behaviours in adolescence: current evidence and opportunities for intervention. Lancet. (2021) 398:429–42. doi: 10.1016/S0140-6736(21)01259-9
67. Veliz, P, Snyder, M, and Sabo, D. The state of high school sports in America: an evaluation of the Nation’s Most popular extracurricular activity Eisenhower Park, East Meadow, NY: Women’s Sports Foundation. (2019).
68. Howie, EK, Daniels, BT, and Guagliano, JM. Promoting physical activity through youth sports programs: It’s social. Am J Lifestyle Med. (2020) 14:78–88. doi: 10.1177/1559827618754842
69. Doran, GT. There’sa SMART way to write management’s goals and objectives. Manag Rev. (1981) 70:35–6.
70. Ahmadi, A, Noetel, M, Parker, P, Ryan, RM, Ntoumanis, N, Reeve, J, et al. A classification system for teachers’ motivational behaviors recommended in self-determination theory interventions. J Educ Psychol. (2023). doi: 10.1037/edu0000783
71. Zecevic, CA, Tremblay, L, Lovsin, T, and Michel, L. Parental influence on young children’s physical activity. Int J Pediatr. (2010) 2010:468526:1–9. doi: 10.1155/2010/468526
72. Coto, J, Pulgaron, ER, Graziano, PA, Bagner, DM, Villa, M, Malik, JA, et al. Parents as role models: associations between parent and young children’s weight, dietary intake, and physical activity in a minority sample. Matern Child Health J. (2019) 23:943–50. doi: 10.1007/s10995-018-02722-z
73. Petersen, TL, Møller, LB, Brønd, JC, Jepsen, R, and Grøntved, A. Association between parent and child physical activity: a systematic review. Int J Behav Nutr Phys Act. (2020) 17:67. doi: 10.1186/s12966-020-00966-z
Keywords: human-centered design, multilevel intervention, youth, community-based participatory research, sport-based youth development, psychological needs, sport for development
Citation: Greeven SJ, Medellin AM, Watkins JM, Coble CJ, Brunnemer JE, Fernández Solá PA, Dutta S, Hobson JM, Evanovich JM, Martinez Kercher VM and Kercher KA (2023) Multilevel needs assessment of physical activity, sport, psychological needs, and nutrition in rural children and adults. Front. Public Health. 11:1290567. doi: 10.3389/fpubh.2023.1290567
Edited by:
Nicholas P. Hays, Nestle, SwitzerlandReviewed by:
Arne Kodal, Norwegian Research Institute (NORCE), NorwayCopyright © 2023 Greeven, Medellin, Watkins, Coble, Brunnemer, Fernández Solá, Dutta, Hobson, Evanovich, Martinez Kercher and Kercher. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kyle A. Kercher, a3lsa2VyY2hAaXUuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.