 Christina R. Davies
Christina R. Davies Charley A. Budgeon2
Charley A. Budgeon2 Kevin Murray
Kevin Murray
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 30 November 2023
Sec. Aging and Public Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1288760
This article is part of the Research TopicArts and Design in Public Health in a Digital Age: A Multidisciplinary PerspectiveView all 9 articles
Introduction: Evidence of the benefits of arts engagement to community wellbeing has been mounting since the 1990s. However, large scale, quantitative, epidemiological studies of the “arts–healthy aging” relationship, or the types of arts older adults voluntarily choose to engage in as part of their everyday life, for enjoyment, entertainment or as a hobby (vs. therapy or interventions) are limited. The aims of this study were to describe older adult recreational arts engagement via the Busselton Healthy Ageing Study (BHAS) cohort, and to determine if there was an association between arts engagement, general health and mental wellbeing.
Methods: Overall, 2,843 older adults (born 1946–1964) from the BHAS cohort (n = 5,107) who had completed a supplementary arts survey (n = 3,055, 60%) and had data on required variables were included in this study (93% of those eligible). The dependent variable was general health (SF12) and subjective mental wellbeing (Warwick-Edinburgh Mental Wellbeing Scale, WEMWBS). The independent variable was hours engaged in recreational arts in the last 12 months. A descriptive analysis followed by a linear regression analysis was conducted.
Results: The prevalence of recreational arts engagement in the last 12 months was 85% (mean = 132 h/year). Older adults engaged in the arts in a number of ways including attending events (79%), actively participating/making art (40%), as an arts society/club/organization member (20%), by learning about the arts (13%) or by volunteering/working in the arts (non-professional, 11%). When general health was assessed via the SF12, the average physical component score (PCS) was 50.1 (SD 8.9) and the average mental component score (MCS) was 53.6 (SD 8.3). When mental wellbeing was assessed, the average WEMWBS score was 54.9 (SD = 8.6). After adjustment for 12 demographic and lifestyle covariates, it was found that older adults who engaged in any recreational arts in the last 12 months had significantly higher WEMWBS scores and higher SF12 physical component scores than those who did not engage in the arts (0 h/year).
Discussion: Evidence of an arts-health relationship was found in this study. The suitability of the arts as a population based, healthy aging strategy to influence the mental wellbeing and general health of older adults should be investigated further.
For many people worldwide (1), a long life (60 years and beyond) is now an “expectation” rather than the exception (1, 2). However, as people age into older adulthood they are likely to experience events and risk factors (e.g., reduced income, disability, bereavement, social isolation, loneliness) which have the potential to adversely impact quality of life, health and wellbeing, e.g., loneliness is associated with mental ill-health, high blood pressure and heart disease (3–7). As a result, the 73rd World Health Assembly has called for urgent and concerted global action on healthy aging, especially sustainable solutions that are person-centered and prevention (rather than illness) focused. (3, 4). With an emphasis on self-expression, social inclusion, happiness, agency, enjoyment, and creativity (8–11), like recreational sport (an established health promotion strategy), in Australia, recreational arts engagement is starting to receive attention from government, industry, philanthropists, policy makers, health professionals, artists, and the general community as a public health and healthy aging strategy (10–12).
Recreational arts engagement is an umbrella term that describes the various ways individuals interact with the arts, as part of their everyday life, for enjoyment, entertainment, socially or as a hobby (13, 14). The arts includes a large number of activities/events and has been defined by Davies et al. (13, 15) via five art forms, these being:
• performing arts (e.g., playing a musical instrument, attending a concert, singing, dancing, listening to music);
• visual arts, design and craft (e.g., painting, drawing, pottery, jewelry making, attending an art exhibition);
• community and cultural festivals (i.e., festivals related to community events, national holidays, or events of religious or cultural significance, e.g., Diwali festival, community lantern events, Lunar New Year festivals);
• literature (e.g., storytelling, creative writing, reading novels, book clubs), and
• online, digital and electronic arts (e.g., photography, film making, animation, viewing a movie or e-concert).
Recreational arts engagement flows on a continuum from active involvement (e.g., making art) to receptive involvement (e.g., viewing art) (13, 15). Methods of engagement include (but are not limited to), making, performing, attending, learning about, listening to, viewing art (15) and can occur within a variety of settings, including but not limited to the home, workplaces, schools, community centers, museums, theaters, concert halls, art galleries, parks, places of worship, prisons, aged care facilities, and hospitals (13).
This study responds to the UK all-parliamentary enquiry into the “arts and wellbeing” which found that the arts can help to keep us well and support longer lives better lived (10). This study also responds to the Australian “National Arts and Health Framework” which was endorsed by both Health Ministers and Arts Ministers in every Australian state/territory to promote the integration of the arts into health policy and practice (16), and the recent Australian Royal Commission into aged care that found that many older Australians are isolated, lonely and lack the intellectual activity/resources needed to live a meaningful life (6, 17). Arts interventions and programs for older adults have been found to reduce depressed mood, social isolation, boredom; enhance feelings of joy, happiness, hope, self-worth, relaxation and improve quality of life (14, 18–23). In the general population, qualitative and quantitative studies have found that arts engagement increases perceptions of happiness, resilience, empathy, enjoyment, confidence, self-esteem, self-expression, knowledge, and self-reflection (8, 24–27). Given this, it is now time to assess the effectiveness of arts engagement as a non-pharmacological, healthy aging strategy, and if found to be effective, to utilize the arts in innovative public health policy and practice, like we do with recreational sport (28). While evidence and review of the benefits of arts engagement has been mounting for many years (11, 29–33), large scale, quantitative, epidemiological studies of the “recreational arts–healthy aging” relationship (rather than therapy or as part of an intervention) are limited (8). As a result, this study aimed to (1) describe how older Australian adults engage in recreational arts, and then (2) determine if there is an association between recreational arts engagement (hours per year), general health and mental wellbeing.
The study protocol (7) for the Busselton Healthy Ageing Study (BHAS) includes detailed health questionnaires and physical clinical assessments. All non-institutionalized adults (born 1946–1964) listed on the electoral roll as living within the City of Busselton local government electoral boundary were invited to participate (in Australia electoral roll registration is compulsory). Contact was made with 82% of those eligible of which 76% completed the BHAS study protocol at the survey center (n = 5,107, 45% male). This cohort provides good power cross-sectionally to study participant health and has similar prevalence of chronic conditions and disease risk factors to the Australian population (7, 34). Based on a previously established survey, arts engagement and mental wellbeing questions were included as a supplementary postal survey in 2015 (8). Permission to conduct this study was granted by the University of Western Australia Human Research Ethics Committee (RA/4/1/2203), and informed consent obtained from participants. Of the 5,107 BHAS cohort participants, 3,055 (60%) replied to the arts survey, of these 2,843 (93%) had the required variables to enable inclusion in this study.
The SF12 (Version 2, QualityMetric Incorporated) is a multipurpose, short-form measure of health status (35). The SF12 consists of 12 questions that measure eight health domains to assess physical health (PCS) and mental health (MCS). In this study, the PCS and MCS scores were computed and normalized according to published algorithms (35, 36). Scores range from 0 to 100 (mean = 50, SD = 10), with higher scores indicating better physical and mental health. The SF12 has been validated across a number of populations, conditions and has good test–retest reliability (35, 36). Permission to utilize the SF12 was granted under license T122450/OP005134.
Subjective mental wellbeing was measured using the 14 item Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS) (37). This scale includes hedonic (e.g., happiness, life satisfaction) and eudaimonic (e.g., positive relationships, psychological functioning) items which together measure mental wellbeing (38). WEMWBS was scored by summing responses to each of the 14 items. Population scores on WEMWBS approximate to a normal distribution, with a minimum score of 14 and a maximum score of 70 (population average = 51) (37). The scale has good validity, test–retest reliability, acceptability and internal consistency (37, 39). Permission to utilize WEMWBS was granted by the University of Warwick.
The independent variable in this study was total hours engaged in recreational arts in the last 12 months. Quantifying engagement by asking questions about (1) behavior in the last 12 months, and (2) measurement in terms of “time,” are common in the literature (8). As shown in Figure 1, arts engagement was measured by asking 14 questions about arts attendance (6 questions), arts participation/making (5 questions), learning (1 question), work/volunteering (1 question) and membership (1 question). For each survey item, respondents were asked if they had engaged in the arts in the previous 12 months (yes/no). If “yes,” they were asked to describe the activity or event. Respondents were then asked approximately how many days in the last 12 months they had engaged in each type of arts activity or event, followed by (on a typical day), how many hours they spent engaging.
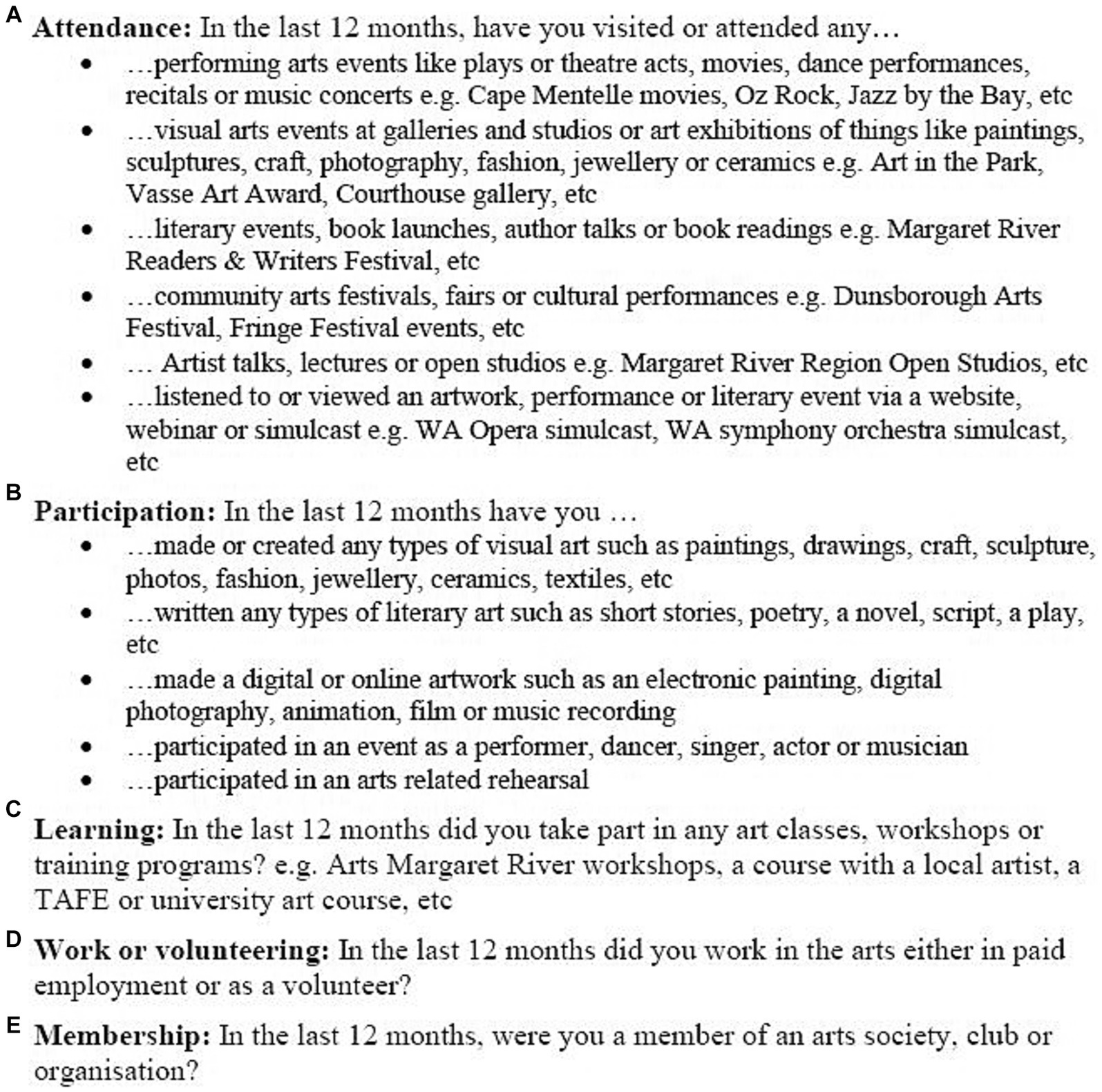
Figure 1. Arts survey questions.
To control for the influence of confounding or effect modification, information about 12 possible covariates to the recreational arts-healthy aging relationship were analyzed (Table 1). This included demographic variables (i.e., sex, age group, household income, education, marital status) and if in the last 12 months respondents experienced a separation/divorce, bereavement, engaged in sport (at least once a week for most weeks), attended religious services/events at a place of worship, partook in a holiday (two or more weeks), experienced financial difficulties or a serious illness.
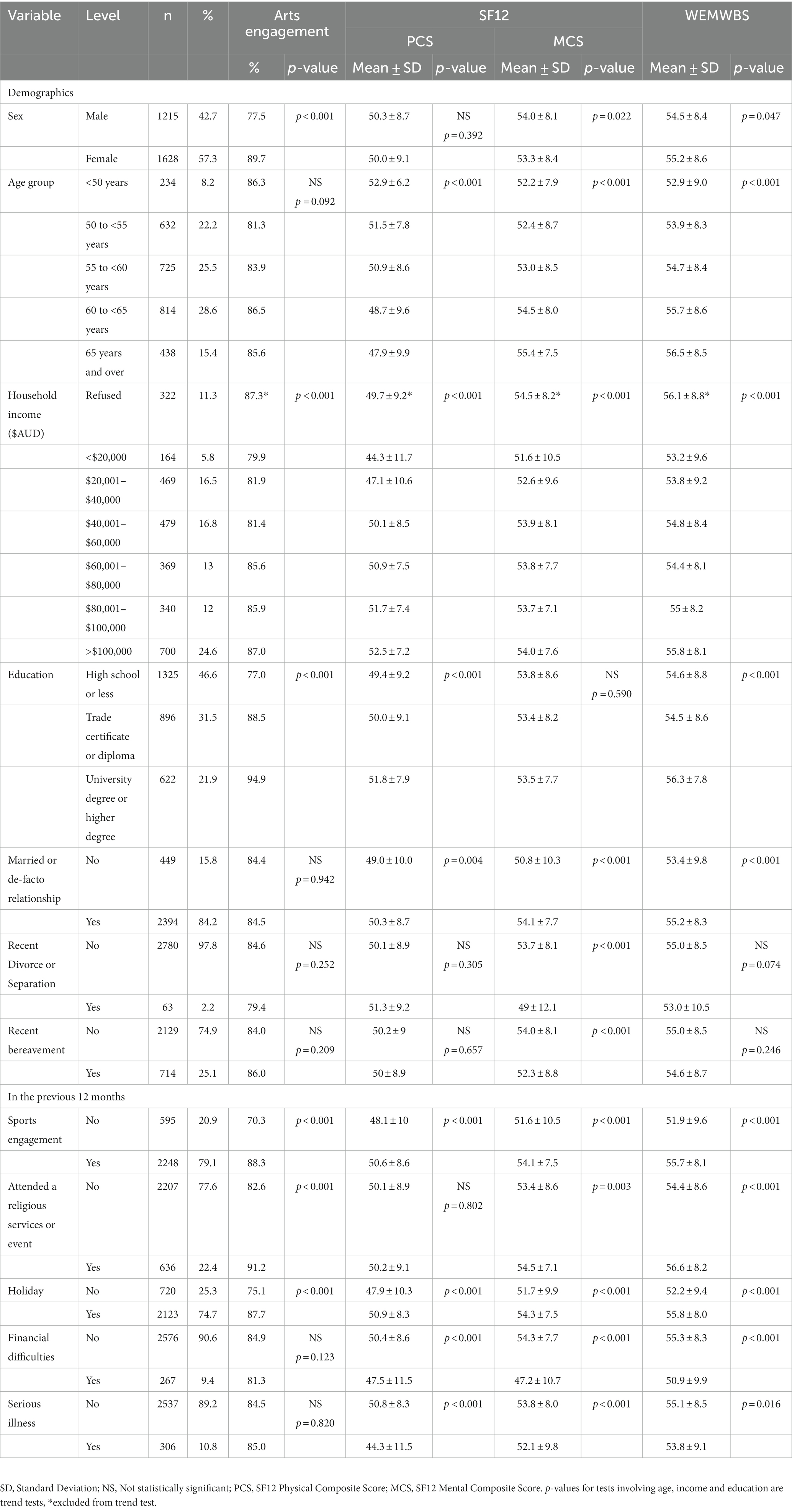
Table 1. BHAS cohort demographic, arts engagement, SF12 and WEMWBS characteristics (n = 2843).
The analyses were conducted using SAS® 9.4. Arts “attendance” in the previous 12 months was calculated based on respondent self-reported answers to one or more of the six survey items relating to attendance. Similarly, respondent “participation” was calculated based on responses to one or more of the five survey items related to participation. A respondent was considered to be engaged in the arts in the previous 12 months (prevalence) if they had attended, and/or participated, and/or took part in arts learning, and/or worked/volunteered in the arts (non-professional basis) and/or been a member of an arts organization, club or society. “Total days engaged in the arts in the previous 12 months” was calculated by summing the number of days respondents spent attending, participating, learning, working/volunteering or being a member. “Hours per day engaged in the arts in the previous 12 months,” was calculated by first multiplying hours on a typical day by number of days engaged in each arts activity over the last 12 months, this was then summed and the total divided by the sum of days engaged in each arts activity. “Hours per year engaged in the arts,” was calculated by multiplying hours on a typical day by number of days engaged in each activity in the previous 12 months and summing each sub-total.
Summary statistics were calculated for categorical variables and means and standard deviations for continuous variables. Chi-squared tests and trend tests were carried out to initially investigate the potential correlates of arts engagement. Linear regression was then used to investigate associations between arts engagement (hours per year), SF12 (PCS, MCS) and WEMWBS. As the distribution of arts engagement was positively skewed (i.e., 16% did not engage in the arts, median = 23 h/year, 75th percentile = 102 h/year), “hours per year engaged in the arts” was grouped into four categories: no art = 0 h/year, low arts engagement = 0.1 to 22.9 h/year, medium arts engagement = 23 to 101.9 h/year and high arts engagement = 102 or more hours/year (8). Overall, three models were fitted. The first model estimated the direct (unadjusted) effect of arts engagement (Model A). The second model (Model B) estimated the effect of arts engagement after adjustment for demographics. The third model (Model C) adjusted for demographics, plus separation/divorce, bereavement, sports engagement, religious activities, holidays, financial difficulties, and serious illness. Interactions between sex and arts engagement were also examined.
Table 1 shows cohort characteristics by demographics, arts engagement, SF12, and WEMWBS (n = 2,843). Overall, 57% of subjects were female. Most were married or in a de-facto relationship (84%), had not recently separated/divorced (98%), not suffered a recent bereavement (75%), not experienced financial difficulties (91%), and had not experienced a serious illness (89%). Approximately half of all subjects completed more than a high school education (53%) and half had an annual income greater than AUD$60,000 per year (50%). Most subjects engaged in sport (79%), had taken a holiday (75%), and had not attended a religious service/event (78%) in the last 12 months.
As shown in Table 2, in the previous 12 months, 79% of subjects had attended an arts event; 40% actively participated/made art; 13% took part in arts related learning; 11% worked or volunteered in the arts (non-professional basis) and 20% were an arts society/club member. In the previous 12 months, on average, respondents spent 17 h attending arts events; 57 h participating/making art; 10 h learning about the arts; 19 h working/volunteering in the arts (non-professional) and 30 h as an arts society/club member. Overall, the prevalence of recreational arts engagement in the cohort was 85%. The cohort spent an average of 132 h per year (SD 330, median 23) engaging in recreational arts activities or events. As the distribution of arts engagement hours was skewed it was grouped. Overall, 16% of respondents did not engage in the arts, 34% had low arts engagement (0.1–22.99 h/year), 25% had medium arts engagement (23–101.99 h/year) and 25% had high arts engagement (102 or more hours/year) (8). As shown in Table 1, females were significantly more likely to engage in recreational arts than males (p < 0.001). Recreational arts engagement also significantly increased by income (p < 0.001), education (p < 0.001), and was more likely in those who also engaged in sport (p < 0.001), who attended religious services/events (p < 0.001) and had taken a holiday (p < 0.001) in the previous 12 months.
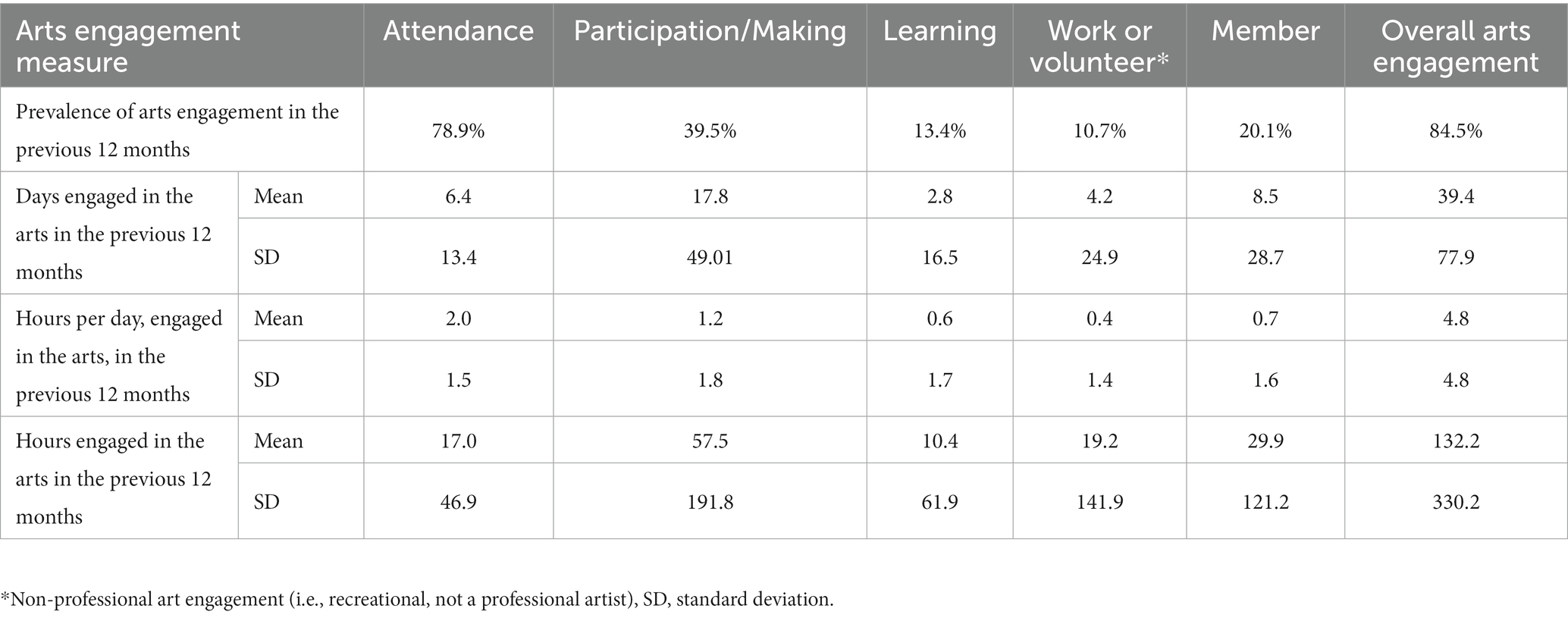
Table 2. BHAS cohort prevalence, days and hours engaged in the arts in the previous 12 months (n = 2,843).
The average SF12 physical component score (PCS) for respondents was 50.1 (SD 8.9) and the average mental component score (MCS) was 53.6 (SD 8.3). As shown in Table 1, PCS significantly decreased by age group (p < 0.001) and increased by income (p < 0.001), education (p < 0.001), and marital status (p = 0.004). MCS were higher in males (p = 0.02) and significantly increased by age group (p < 0.001), income (p < 0.001), marital status (p < 0.001) and not recently experiencing a divorce/separation (p < 0.001) or bereavement (p < 0.001). PCS and MCS were higher in those who engaged in sport (p < 0.001), had taken a holiday (n < 0.001), had no financial difficulties (p < 0.001) or serious illness (p < 0.001) in the previous 12 months. MCS was also higher in those who had attended a religious service/event in the last 12 months (p = 0.003).
As shown in Table 3, Model A (unadjusted), respondents who did not engage in the arts in the last 12 months (PCS 48.4, MCS 52.6), on average, had lower physical and mental component scores than those who had low (PCS 50.8, MCS 54.0), medium (PCS 50.8, MCS 53.6) or high (PCS 49.6, MCS 53.7) levels of recreational arts engagement. After adjustment for demographics, separation or divorce, bereavement, sports engagement, religious activities, holidays, financial difficulties, serious illness (Overall Test–2 groups, Model C) those who did not engage in the arts in the last 12 months (0 h/year) had significantly lower PCS than those who engaged in “any” recreational arts (mean difference − 1.1, 95% CI [−2.0, −0.2], p = 0.016) however a statistically significant difference in MCS was not found in the fully adjusted model (p = 0.337). There was no clear trend in PCS or MCS (unadjusted or adjusted) means with increasing category of arts engagement, with the “low” category of arts engagement having the highest means. Effect modification by sex was not found to be significant.
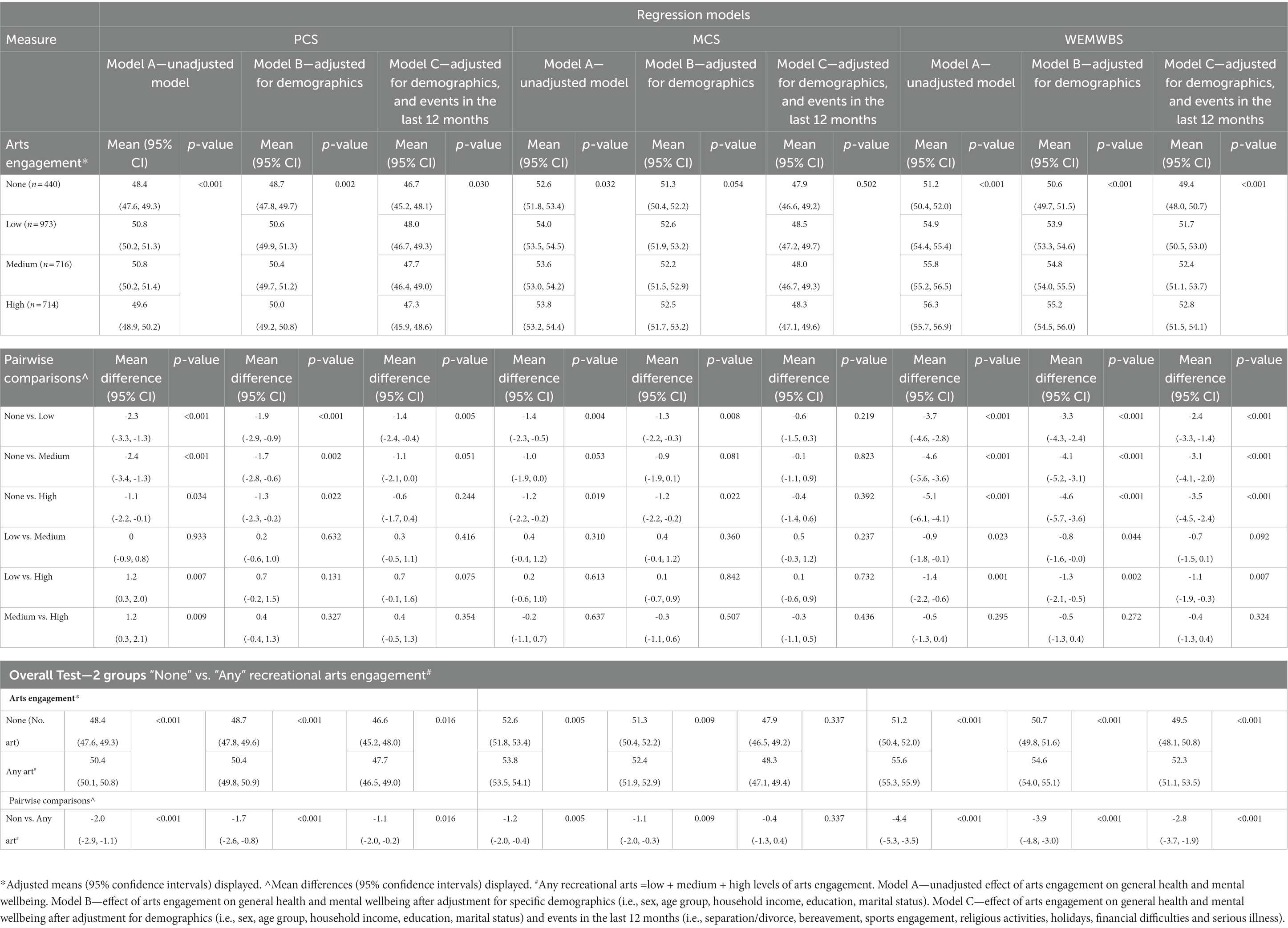
Table 3. Unadjusted and adjusted associations between recreational arts engagement (hrs/year), general health (SF12 PCS, MCS) and mental wellbeing (WEMWBS) (n = 2,843).
The WEMWBS mean score for the cohort was 54.9 (SD 8.6). As shown in Table 1, females had a higher average WEMWBS scores than males (p = 0.047), as did older compared to younger subjects (p < 0.001). Average WEMWBS scores also significantly increased by income (p < 0.001), education (p < 0.001) and marital status (p < 0.001) and were higher for those who engaged in sport (p < 0.001), attended a religious service/event (p < 0.001), had taken a holiday (n < 0.001), who had no financial difficulties (p < 0.001) or serious illness (p = 0.016) in the previous 12 months.
As shown in Table 3, Model A (unadjusted), older adults who engaged in low (54.9), medium (55.8) or high (56.3) levels of arts engagement in the last 12 months had significantly higher WEMWBS scores than those who did not engage in the arts (51.2). After adjustment for demographics, separation or divorce, bereavement, sports engagement, religious activities, holidays, financial difficulties, serious illness (Overall Test–2 groups, Model C), it was found that people who did not engage in recreational arts (0 h/year) had significantly lower WEMWBS scores than those who engaged in “any” recreational arts in the last 12 months (mean difference − 2.8, 95% CI [−3.7, −1.9], p < 0.001). In general, respondents who participated in any (low, medium or high) recreational arts had WEMWBS scores almost three points higher than those who did not engage in recreational arts. Further, there was evidence in both unadjusted and adjusted means of increasing WEMWBS scores with higher levels of arts engagement with the “high” category of arts engagement having the highest means. Effect modification by sex was not found to be significant.
This study contributes to the healthy aging literature and increases knowledge of the impact of recreational arts engagement on older adult mental wellbeing and general health. Encouraging older adults to “shift” their behavior to encourage actions that enhance wellbeing is a common health promotion strategy as this approach, at a population level, can benefit more older adults (overall) than targeting only specific groups. For example, a population approach to increasing physical health might be to encourage older adults to engage in adequate levels of exercise such as walking, balance and strength-based exercise. Likewise, population-based strategies to improve older adult mental wellbeing and general health could be to encourage recreational arts-based activities, programs and events in the community and in aged care, e.g., creative writing, book clubs, painting, pottery, knitting, coloring, photography, playing a musical instrument, singing, dancing, art classes, attending concerts, etc.
In this study, a significant association between arts engagement and mental wellbeing, as measured by WEMWBS, was found. This is consistent with the arts-mental health literature for both the general population and interventions with older adults (8, 40, 41). After adjustment for demographic and lifestyle factors, respondents who engaged in any recreational arts in the last 12 months had significantly higher WEMWBS scores than those who did not engage at all. Evidence of increasing WEMWBS scores with higher levels of arts engagement was found. Respondents with “high” arts engagement in the last 12 months (102 h or more/year, or 2 h or more/week) had average WEMWBS score 3.5 points higher than those who did not engage at all (0 h/year). WEMWBS responsiveness to change has been assessed at both the individual and population level for which a difference of three or more points can be considered meaningful (39).
When the association between arts engagement in the last 12 months, and general health was assessed, a weaker relationship was found for the SF12 physical component, but not for the mental health component. The impact of arts engagement on general health, as measured by the SF12, has had mixed findings in the literature. For example, some arts engagement studies have showed a significant increase in SF12 mental health component scores at 6-month follow-up (18, 42) but not at 12-month follow-up (18), and for SF12 physical component scores, no significant change at 6-month follow-up (18, 42) but “close to significant” (p = 0.06) change at 12-month follow-up (18). One explanation for our results and the literature, is that arts related physical health changes may take longer than 6 months to develop. Acknowledging that (1) our results are an association and not an indication of causality or relationship directionality (i.e., older adult arts engagement may improve mental wellbeing and/or older mental wellbeing may increase the likelihood of engagement in the arts), and (2) given the decline in our physical health as we age (3–7), rigorous research (e.g., RCTs, prospective cohort studies) is needed to assess whether recreational arts-based activities, programs and events can positively impact the physical health of older adults living in the community and in aged care. One possible explanation for our SF12 mental health component result and the literature, is that the mental health effects of arts engagement are short term, however, this is not consistent with our results for WEMWBS. Keeping in mind that when asked to self-report outcomes obtained from engaging in the arts, members of the general population are more likely to mention positive (e.g., happiness, relaxation, self-esteem) rather than negative outcomes (e.g., anxiety, frustration, disappointment) (25). Another explanation for the difference in results between WEMWBS and the SF12 mental health component, is because these surveys are measuring different mental health outcomes. The Warwick-Edinburgh Mental Wellbeing Scale was developed to measure positive mental health (39), that is, WEMWBS measures positive mental health or mental wellbeing, via hedonic (e.g., happiness) and eudaimonic questions (e.g., positive relationships) (37, 38). The mental health component of the SF12 however measures mental health functioning and low scores can be used as an indicator of ill-health (35). More research is needed to determine which mental health measures are most appropriate when conducting studies related to arts engagement.
Overall, this paper provides three important findings for government, industry, philanthropists, policy makers, health professionals, artists, older adults, with results generalizable to Australian states/territories and countries with similar mental-health, health and socio-demographic profiles to Australia. First, recreational arts engagement may have the potential to enhance the mental wellbeing and general health of older adults. Second, when engaging in creative activities and events, more research is needed to determine the “art dose” or the optimal amount of time older adults should spend engaging in the arts, e.g., in the general population (18 years and older) it has been suggested that two or more hours/week of arts engagement is associated with enhanced mental wellbeing (8). Third, in time, if the relationship between hours engaged in the arts, general health and mental wellbeing is found to be causal, there is potential for innovative, non-pharmacological, “arts-healthy aging” policy, programs, campaigns and strategies, such as those used to promote the health benefits of sport and physical activity to older Australians. For example, in Western Australia, Injury Matters and the Department of Health have implemented the “Stay on your Feet”® falls prevention campaign to promote the health benefits of physical activity to health professionals, older adults, and the friends and families of older adults (43).
Strengths of this study include its large sample size, high response, adjustment for a wide range of confounders and effect modifiers to the arts-healthy aging relationship and that the cohort is representative of the Australian population. A limitation of this study is that our analyses are cross-sectional and therefore preclude our ability to determine causality. For researchers to determine whether or not a causal relationship exists between arts engagement and healthy aging study designs that consider temporal order are needed (e.g., RCTs) (44). Enablers and barriers to the arts-healthy aging relationship should also be investigated (e.g., cost, access, someone to attend arts events with), as should the influence of arts engagement methods (i.e., active vs. receptive) to determine which elements have the most impact on mental wellbeing and general health.
The datasets presented in this article are not readily available. The Busselton Population Medical Research Institute (BPMRI) welcomes applications from researchers for data access which are considered by the BPMRI Scientific Research Committee.
The study was approved by the University of Western Australia Human Research Ethics Committee (RA/4/1/2203). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
CD: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. CB: Data curation, Formal analysis, Investigation, Project administration, Software, Writing – original draft, Writing – review & editing. KM: Data curation, Formal analysis, Funding acquisition, Investigation, Project administration, Software, Writing – original draft, Writing – review & editing. MH: Data curation, Investigation, Methodology, Resources, Software, Validation, Writing – original draft, Writing – review & editing. MK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. BHAS was supported by grants from the Government of Western Australia (Department of Jobs, Tourism, Science and Innovation and Department of Health), the Commonwealth Government (Department of Health), the City of Busselton and from private donations to the Busselton Population Medical Research Institute. CD was funded by the Ian Potter Foundation (31110974) and the Minderoo Foundation—Arts & Culture (2022/GR000916) and the Western Australian Future Health Research and Innovation Fund, which was an initiative of the Western Australian State Government. Warwick-Edinburgh Mental Wellbeing Scale was funded by the Scottish Executive National Programme for improving mental health and wellbeing, commissioned by NHS Health Scotland, developed by the University of Warwick and the University of Edinburgh, and was jointly owned by NHS Health Scotland, the University of Warwick and the University of Edinburgh.
We thank the Western Australian Country Health Service, and the BPMRI Busselton Health Study Centre staff and volunteers for survey operations, and the BPMRI Community Advisory Committee and the people of Busselton for their participation. We would like to thank the University of Warwick for granting permission to use the Warwick-Edinburgh Mental Wellbeing scale.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
WEMWBS, Warwick-Edinburgh Mental Wellbeing Scale; NS, Not statistically significant; SD, Standard Deviation; SF12, Short Form12; PCS, SF12 Physical Composite Score; MCS, SF12 Mental Composite Score; IQR, Interquartile range
1. World Health Organization. Ageing and health. Geneva: WHO (2021) Available at: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.
2. Higgs, P, and Gilleard, C. Frailty, abjection and the ‘othering’ of the fourth age. Health Sociol Rev. (2014) 23:10–9. doi: 10.5172/hesr.2014.23.1.10
3. United Nations- Department of Economic and Social Affairs. World population aging 2019. New York, NY: United Nations. (2020). Available at: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Report.pdf (Accessed October, 2020).
4. World Health Organisation. Decade of healthy ageing (2020-2030) (2020). Available at: https://www.who.int/ageing/decade-of-healthy-ageing.
5. National Institute on Aging. Social isolation, loneliness in older people pose health risks (2019). Available at: https://www.nia.nih.gov/news/social-isolation-loneliness-older-people-pose-health-risks.
6. Commonwealth of Australia. Royal commission into aged care quality and safety - interim report volume 1 Australian Government (2019) Available at: https://agedcare.royalcommission.gov.au/publications/Documents/interim-report/interim-report-volume-1.pdf.
7. The Busselton Healthy Ageing Study (BHAS) Investigator GroupJames, A, Hunter, M, Straker, L, Beilby, J, Bucks, R, et al. Rationale, design and methods for a community-based study of clustering and cumulative effects of chronic disease processes and their effects on ageing: the Busselton healthy ageing study. BMC Public Health. (2013) 13:1–12. doi: 10.1186/1471-2458-13-936,
8. Davies, C, Knuiman, M, and Rosenberg, M. The art of being mentally healthy: a study to quantify the relationship between recreational Arts engagement and mental well-being in the general population. BMC Public Health. (2016) 16:15. doi: 10.1186/s12889-015-2672-7
9. Smith, R. Spend (slightly) less on health and more on the arts. BMJ. (2002) 325:1432–3. doi: 10.1136/bmj.325.7378.1432
10. All-Party Parliamentary Group on Arts Health and Wellbeing. Creative health: the arts for health and wellbeing (short report) (2017). Available at: http://www.artshealthandwellbeing.org.uk/appg-inquiry/.
11. Davies, C, and Pescud, M. The Arts, creative industries and health: an evidence check rapid review brokered by the sax Institute for the Victorian Health Promotion Foundation. New South Wales: Sax Institute (2020).
12. Commonwealth of Australia. Revive: a place for every story, a story for every place – Australia’s cultural policy for the next five years. Canberra, ACT: Australian Government (2023) Available at: https://www.arts.gov.au/sites/default/files/documents/national-culturalpolicy-8february2023.pdf.
13. Davies, C, and Clift, S. Arts and Health Glossary - a summary of definitions for use in research, policy and practice. Front Psychol. (2022) 13:949685. doi: 10.3389/fpsyg.2022.949685
14. Archibald, M, and Kitson, A. Using the arts for awareness, communication and knowledge translation in older adulthood: a scoping review. Arts Health. (2019) 3:1–17. doi: 10.1080/17533015.2019.1608567
15. Davies, C, Rosenberg, M, Knuiman, M, Ferguson, R, Pikora, T, and Slatter, N. Defining arts engagement for population-based health research: art forms, activities and level of engagement. Arts Health. (2012) 4:203–16. doi: 10.1080/17533015.2012.656201
16. Standing Council on Health and Cultural Ministers. National arts and health framework (2014) Available at: http://mcm.arts.gov.au/national-arts-and-health-framework.
17. Pagone, T, and Care, BL. Dignity and respect: the final report of the royal commission into aged care quality and safety. Canberra, ACT: Commonwealth of Australia (2021) Available at: https://agedcare.royalcommission.gov.au/publications/final-report.
18. Greaves, C, and Farbus, L. Effects of creative and social activity on the health and well-being of socially isolated older people: outcomes from a multi-method observational study. J R Soc Promot Heal. (2006) 126:134–42. doi: 10.1177/1466424006064303
19. MacLeod, A, Skinner, M, Wilkinson, F, and Reid, H. Connecting socially isolated older rural adults with older volunteers through expressive arts. Can J Aging. (2016) 35:14–27. doi: 10.1017/S071498081500063X
20. Anderson, S, Fast, J, Keating, N, Eales, J, Chivers, S, and Barnet, D. Translating knowledge: promoting health through intergenerational community Arts programming. Health Promot Pract. (2017) 18:15–25. doi: 10.1177/1524839915625037
21. Petrovsky, DV, Sefcik, JS, and Cacchione, PZ. A qualitative exploration of choral singing in community-dwelling older adults. West J Nurs Res. (2020) 42:340–7. doi: 10.1177/0193945919861380
22. Fraser, K, O'Rourke, H, Wiens, H, Lai, J, Howell, C, and Brett-MacLean, P. A scoping review of research on the Arts, aging, and quality of life. Gerontologist. (2015) 55:719–29. doi: 10.1093/geront/gnv027
23. Edwards, L, and Owen-Booth, B. An exploration of engagement in community based creative activities as an occupation for older adults. Irish J Occup Ther. (2021) 49:51–7. doi: 10.1108/IJOT-05-2020-0009
24. Australia Council for the Arts. Connecting Australians: results of the national arts participation survey (2017). Available at: https://www.australiacouncil.gov.au/workspace/uploads/files/connecting-australians-natio-59520692c614a.pdf
25. Davies, C, Knuiman, M, Wright, P, and Rosenberg, M. The art of being healthy: a qualitative study to develop a thematic framework for understanding the relationship between health and the arts. BMJ Open. (2014) 4:e004790–10. doi: 10.1136/bmjopen-2014-004790
26. A New Approach (ANA). Transformative: impacts of culture and creativity acton ACT: produced by ANA think tank with lead delivery partner the Australian Academy of the Humanities. (2019). Available at: https://www.humanities.org.au/new-approach/report2/.
27. Boydell, KM, and Croguennec, J. A creative approach to knowledge translation: the use of short animated film to share stories of refugees and mental health. Int J Environ Res Public Health. (2022) 19. doi: 10.3390/ijerph191811468
28. McPhee, J, French, D, Jackson, D, Nazroo, J, Pendleton, N, and Degens, H. Physical activity in older age: perspectives for healthy ageing and frailty. Biogerontology. (2016) 17:567–80. doi: 10.1007/s10522-016-9641-0
29. White, M. Arts development in community health: a social tonic. Oxon: Radcliffe Publishing (2009).
30. Clift, S, and Camic, P eds. Oxford textbook of creative Arts, health, and wellbeing: international perspectives on practice, policy and research. Oxford: Oxford University Press (2016).
31. Zarobe, L, and Bungay, H. The role of arts activities in developing resilience and mental wellbeing in children and young people a rapid review of the literature. Perspect Public Health. (2017) 137:337–47. doi: 10.1177/1757913917712283
32. Fancourt, D, and Finn, S. What is the evidence on the role of the arts in improving health and well-being? A scoping review, health evidence network synthesis report 67. Copenhagen: WHO Regional Office for Europe (2019).
33. Zbranca, R, Dâmaso, M, Blaga, O, Kiss, K, Dascl, M, Yakobson, D, et al. CultureForHealth report: culture’s contribution to health and well-being: a report on evidence and policy recommendations for Europe. Brussels: Culture Action Europe (2022). Available at: https://www.cultureforhealth.eu/app/uploads/2023/02/Final_C4H_FullReport_small.pdf.
34. Hunter, M, Knuiman, M, Musk, B, Hui, J, Murray, K, Beilby, J, et al. Prevalence and patterns of multimorbidity in Australian baby boomers: the Busselton healthy ageing study. BMC Public Health. (2021) 21:1539. doi: 10.1186/s12889-021-11578-y
35. Ware, J, Kosinski, M, and Keller, S. SF-12: how to score the SF-12 physical and mental summary scales. 2nd ed. Boston, MA: The Health Institute, New England Medical Center (1995).
36. Ware, J, Kosinski, M, and Keller, S. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. (1996) 34:220–33. doi: 10.1097/00005650-199603000-00003
37. Stewart-Brown, S, and Janmohamed, K. Warwick-Edinburgh Mental Well-being Scale (WEMWBS) user guide: Version 1 (2008). Available at: http://www.cppconsortium.nhs.uk/admin/files/1343987601WEMWBS%20User%20Guide%20Version%201%20June%202008.pdf.
38. Clarke, A, Friede, T, Putz, R, Ashdown, J, Martin, S, Blake, A, et al. Warwick-Edinburgh Mental Well-Being Scale (WEMWBS): validated for teenage school students in England and Scotland. A mixed methods assessment. BMC Public Health. (2011) 11:487. doi: 10.1186/1471-2458-11-487
39. Maheswaran, H, Weich, S, Powell, J, and Stewart-Brown, S. Evaluating the responsiveness of the Warwick Edinburgh Mental Well-Being Scale (WEMWBS): group and individual level analysis. Health Qual Life Outcomes. (2012) 10:156. doi: 10.1186/1477-7525-10-156
40. Beauchet, O, Cooper-Brown, L, Hayashi, Y, Deveault, M, and Launay, C. Improving the mental and physical health of older community-dwellers with a museum participatory art-based activity: results of a multicentre randomized controlled trial. Aging Clin Exp Res. (2022) 34:1645–54. doi: 10.1007/s40520-022-02139-3
41. Beauchet, O, Bastien, T, Mittelman, M, Hayashi, Y, and Ho, AHY. Participatory art-based activity, community-dwelling older adults and changes in health condition: results from a pre-post intervention, single-arm, prospective and longitudinal study. Maturitas. (2020) 134:8–14. doi: 10.1016/j.maturitas.2020.01.006
42. Coulton, S, Clift, S, Skingley, A, and Rodriguez, J. Effectiveness and cost-effectiveness of community singing on mental health-related quality of life of older people: randomised controlled trial. Br J Psychiatry. (2015) 207:250–5. doi: 10.1192/bjp.bp.113.129908
43. Injury Matters, I. Stay on your feet: move, improve, remove. Leederville, WA: IM (2023). Available at: https://www.injurymatters.org.au/programs/stay-on-your-feet/.
Keywords: arts, general health, mental health, older adult, Warwick-Edinburgh Mental Wellbeing Scale, SF12
Citation: Davies CR, Budgeon CA, Murray K, Hunter M and Knuiman M (2023) The art of aging well: a study of the relationship between recreational arts engagement, general health and mental wellbeing in cohort of Australian older adults. Front. Public Health. 11:1288760. doi: 10.3389/fpubh.2023.1288760
Edited by:
Yao Song, Hong Kong Polytechnic University, Hong Kong SAR, ChinaReviewed by:
Helga Eggebø, Nordland Research Institute, NorwayCopyright © 2023 Davies, Budgeon, Murray, Hunter and Knuiman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christina R. Davies, Y2hyaXN0aW5hLmRhdmllc0B1d2EuZWR1LmF1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.