
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 19 January 2024
Sec. Clinical Diabetes
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1286056
This article is part of the Research TopicRecent Advances in Gestational Diabetes MellitusView all 12 articles
 Grammata Kotzaeridi1
Grammata Kotzaeridi1 Cécile Monod2
Cécile Monod2 Tina Linder1
Tina Linder1 Daniel Eppel1
Daniel Eppel1 Vera Seidel3
Vera Seidel3 Michael Feichtinger4Beatrice Mosimann2Valeria Filippi2
Michael Feichtinger4Beatrice Mosimann2Valeria Filippi2 Silke Wegener3
Silke Wegener3 Wolfgang Henrich3
Wolfgang Henrich3 Andrea Tura5
Andrea Tura5 Christian S. Göbl1,6*
Christian S. Göbl1,6*Introduction: Women with migration background present specific challenges related to risk stratification and care of gestational diabetes mellitus (GDM). Therefore, this study aims to investigate the role of ethnic origin on the risk of developing GDM in a multiethnic European cohort.
Methods: Pregnant women were included at a median gestational age of 12.9 weeks and assigned to the geographical regions of origin: Caucasian Europe (n = 731), Middle East and North Africa countries (MENA, n = 195), Asia (n = 127) and Sub-Saharan Africa (SSA, n = 48). At the time of recruitment maternal characteristics, glucometabolic parameters and dietary habits were assessed. An oral glucose tolerance test was performed in mid-gestation for GDM diagnosis.
Results: Mothers with Caucasian ancestry were older and had higher blood pressure and an adverse lipoprotein profile as compared to non-Caucasian mothers, whereas non-Caucasian women (especially those from MENA countries) had a higher BMI and were more insulin resistant. Moreover, we found distinct dietary habits. Non-Caucasian mothers, especially those from MENA and Asian countries, had increased incidence of GDM as compared to the Caucasian population (OR 1.87, 95%CI 1.40 to 2.52, p < 0.001). Early gestational fasting glucose and insulin sensitivity were consistent risk factors across different ethnic populations, however, pregestational BMI was of particular importance in Asian mothers.
Discussion: Prevalence of GDM was higher among women from MENA and Asian countries, who already showed adverse glucometabolic profiles at early gestation. Fasting glucose and early gestational insulin resistance (as well as higher BMI in women from Asia) were identified as important risk factors in Caucasian and non-Caucasian patients.
In parallel to the rising rates of metabolic disorders that affect the general and progressively more the reproductive-aged younger population, the prevalence of gestational diabetes mellitus (GDM) has increased over the last decades. Nowadays, the global prevalence of GDM ranges between 12 and 18% of pregnancies, with regional prevalence varying from 7% in North America to 27% in MENA countries (1–3). Thereby, hyperglycemia does not only elevate the risk of adverse outcome for women and offspring during pregnancy and at birth, but also the long-term risk of cardiovascular disease and type 2 diabetes (4).
It is known that the GDM prevalence markedly differs between different ethnic populations and hence, the region of origin has been recognized as a non-negligible risk factor. However, detailed data about each area and its specific role and importance are sparse and sometimes conflicting (4–9). Although Asian populations and women from the Sub-Saharan region have long been recognized as being at high risk of developing the disease, women from other regions are also often affected (3, 10, 11). For example, more recent evidence suggests an increased prevalence of GDM in pregnant women from the Middle East and North Africa countries as compared to other populations (3, 12). Migration has been steadily rising and the countries of origin have greatly diversified over the past years. As a consequence, women with migration background were reported to constitute up to 8–14% of the collective of pregnant women in two Nordic countries (8, 13). In this context, pregnant women with migration background (especially those from other continents) present specific challenges related to detection and care of GDM that need to be addressed (14). However, prospective studies, including information of clinical features, metabolic parameters and dietary habits in multiethnic cohorts are sparsely available.
Therefore, this study aims to investigate and refine the possible role of non-Caucasian ancestry for the development of GDM in a multiethnic European cohort. Moreover, ethnic specific differences in glucometabolic parameters and dietary habits at start of pregnancy as well as possible differences in their contribution for GDM development will be assessed in different ethnic groups.
The study design is reported in detail elsewhere (15). In short, pregnant women who participated in this prospective cohort study were recruited among patients attending the pregnancy outpatient clinic at the Department of Obstetrics and Gynaecology, Division of Obstetrics and feto-maternal Medicine, Medical University of Vienna between 2016 and 2019. Patients with preexisting diabetes (such as type 1 or type 2 diabetes) or those with early gestational glycated haemoglobin A1c (HbA1c) equal or exceeding 6.5% at study entry were excluded. Study participants were included at a median gestational age of 12.9 weeks, interquartile range (IQR) 12.3 to 13.6 weeks. An assessment of maternal characteristics (e.g., maternal age, parity, obstetric history, family history of diabetes, as well as women’s height and pregestational weight and body mass index (BMI)) were assessed at time of recruitment. Moreover, we collected detailed information about the country of origin of participating women and their parents. Therefore, we defined five geographical regions: Caucasian (n = 731), Middle East and North Africa (MENA, n = 195), Asia (n = 127), Sub Saharan African (SSA, n = 48) and Others and assigned each country present in our cohort to one region according to the definition of the NCD Risk Factors Collaboration (NCD-RisC) (16). We only included women whose parents’ countries of birth were known and situated within the same region and hence excluded 22 women. In the non-Caucasian cohort, about 88.2% of women were first generation migrants and 11.8% were second generation migrants. Table 1 gives an overview of the number of women included and their regions and countries of origin. Thereafter, participants were followed-up until delivery to assess status of GDM and pregnancy outcomes.
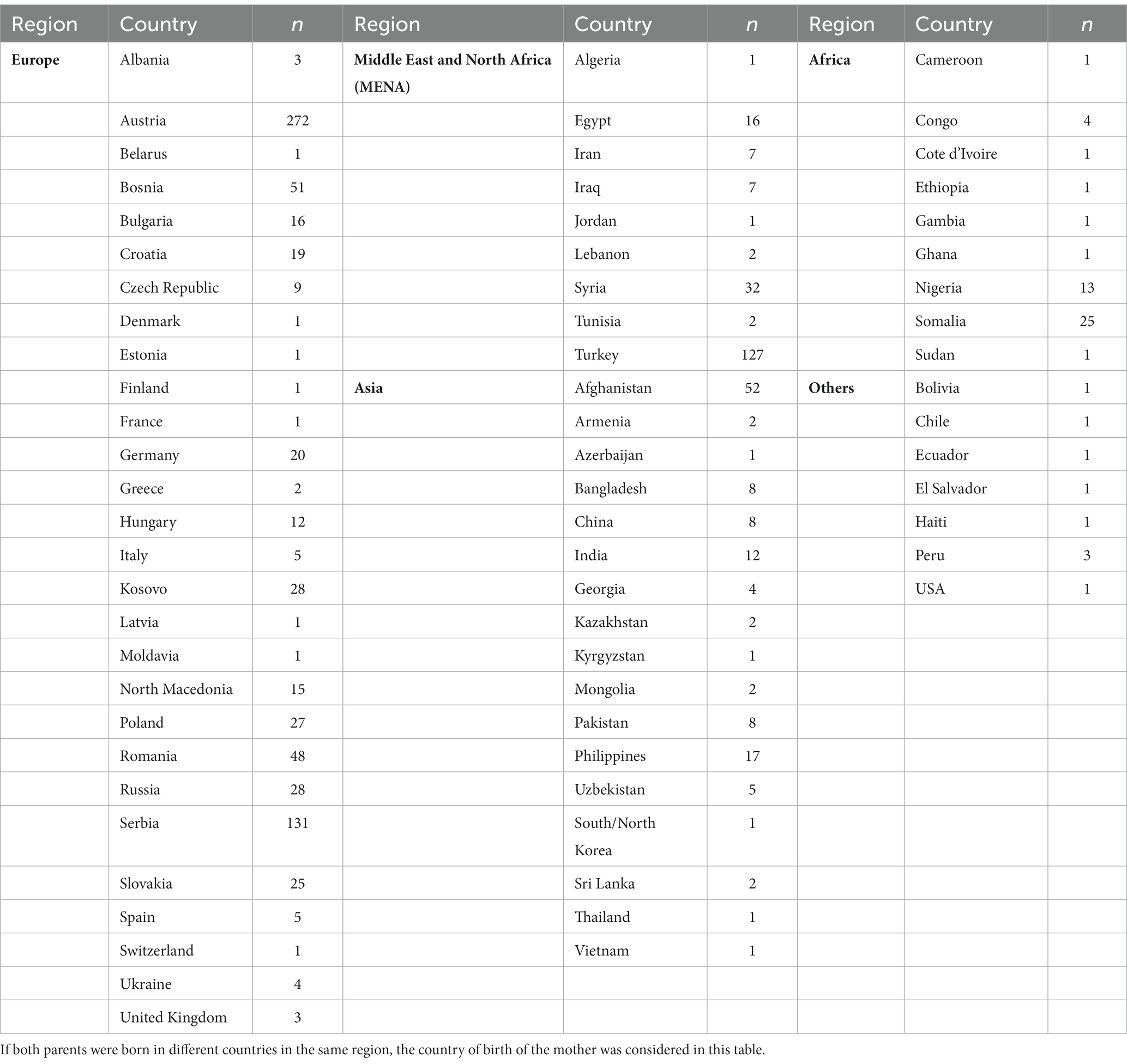
Table 1. List of countries and study participants included for each region.
At time of recruitment, fasting plasma glucose (FPG), insulin and HbA1c as well as triglycerides, total-cholesterol, LDL-cholesterol and HDL-cholesterol were assessed and the homeostasis model assessment of insulin resistance (HOMA-IR) was evaluated (17). Universal Screening of GDM was routinely performed by use of a 75 g 2 h oral glucose tolerance test (OGTT) in the late second or early third trimester. Thereby, the diagnosis of GDM was based on the cut-offs after oral glucose load proposed by the International Association of the Diabetes and Pregnancy Study Groups (IADPSG) criteria (18). The standard laboratory methods at our certified Department of Medical and Chemical Laboratory Diagnostics1 were used to determine all laboratory parameters in this study. According to the international and local guidelines, glucose measurements during the diagnostic OGTT were assessed by use of venous plasma blood samples at local public laboratories (19). Moreover, a food frequency questionnaire was used at time of inclusion to address dietary habits at the start of pregnancy (20).
The Ethics Committee of the Medical University of Vienna approved the study (EK 1937/2015). The study was performed in accordance with the Declaration of Helsinki. All participants gave written informed consent.
Continuous variables were reported as mean ± standard deviation and in case of skewed distributed data as median and interquartile ranges (IQR). These were compared by either Welch’s t-test (for two samples) and analysis of variance (for more than two samples), or rank based “nonparametric” inference such as the Kruskal Wallis Test, respectively. Categorical variables were summarized by counts and percentages and compared by binary logistic regression, whereby odds ratios and 95% Confidence Intervals (95%CI) were calculated for dichotomous outcomes (such as the development of GDM) by binary logistic regression. Multiple logistic regression was further used to identify a possible effect of non-Caucasian ethnicity on the risk of GDM adjusted for various confounders. Thereby, stepwise variable selection was used to identify the model with the lowest (i.e., best) Akaike’s information criterion (AIC). For comparison of more than two groups with one reference group we used Dunnett’s post hoc test to achieve a 95% coverage probability. We further used recursive partitioning to calculate variable importance metrics as the average difference in predictive accuracy before and after random permutation of the values of a predictor variable over 106 random decision trees (21). Statistical analysis was performed with R (version 4.2.2) and contributing packages (especially “multcomp,” “nparcomp” and “randomForest” as well as “ggplot2” for visualisations) (22, 23). A two-sided p-value of ≤0.05 was considered statistically significant. All reported p-values were interpreted in an explorative manner aiming to generate new hypotheses.
Characteristics of Caucasian and non-Caucasian study participants are provided in Table 2. Pregnant women of Caucasian origin were older, more often nulliparous and used assisted reproduction more frequently. Moreover, Caucasian mothers were more likely to smoke (or to be former smokers) and characterized by higher blood pressure and increased total-cholesterol, LDL-cholesterol but also HDL- and non-HDL-cholesterol as compared to non-Caucasian mothers at the beginning of pregnancy. In contrast, non-Caucasian women were more often multiparous, and showed higher BMI as well as a higher degree of insulin resistance associated with modestly higher HbA1c, fasting glucose and insulin levels. A more detailed comparison of early gestational metabolic parameters in pregnant women according to the regional origin is provided in the Supplementary Table S1, showing distinct differences between the investigated subgroups. Women from the MENA as well as those from the SSA region had higher BMI as compared to Caucasian mothers. Women from MENA countries were more insulin resistant with elevated fasting glucose and insulin levels, while women from SSA and Asia showed higher HbA1c but lower total- and non-HDL-cholesterol as compared to the Caucasian population. Distinct differences were also observed in dietary habits (Table 3). Non-Caucasian mothers consumed more rice, couscous or bulgur and legumes but less noodles, potatoes, vegetables, meat and fruits. However, a more detailed analysis of dietary habits according to the regional origin showed that especially women from the MENA regions consumed more carbohydrates such as bread, rice, couscous or bulgur, but were also eating more legumes as compared to Caucasian mothers. A higher rice, bulgur or couscous consumption was also observed in SSA and Asian mothers, whereas they were eating sweets less often.
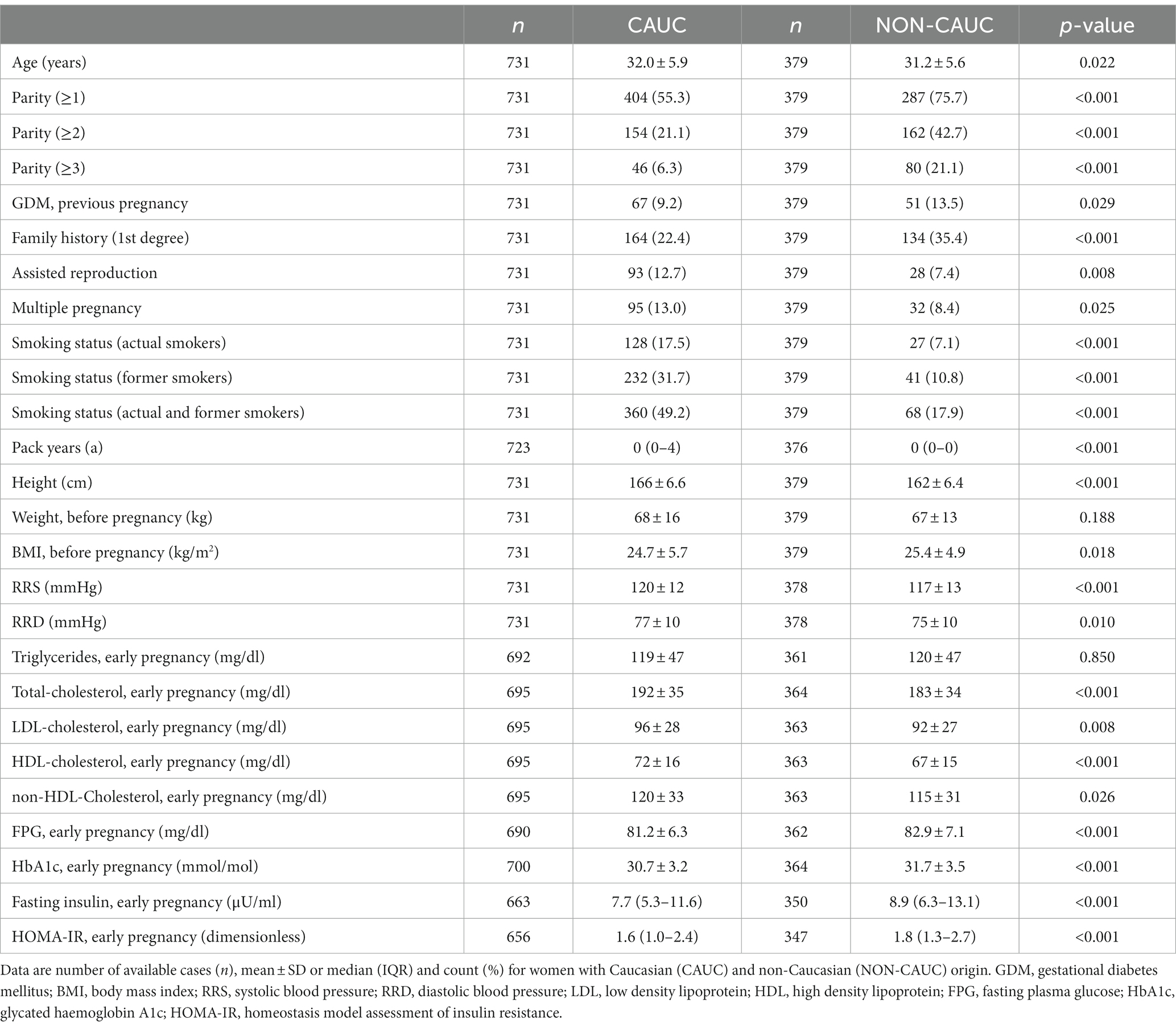
Table 2. Early gestational characteristics of women with Caucasian and non-Caucasian origin.
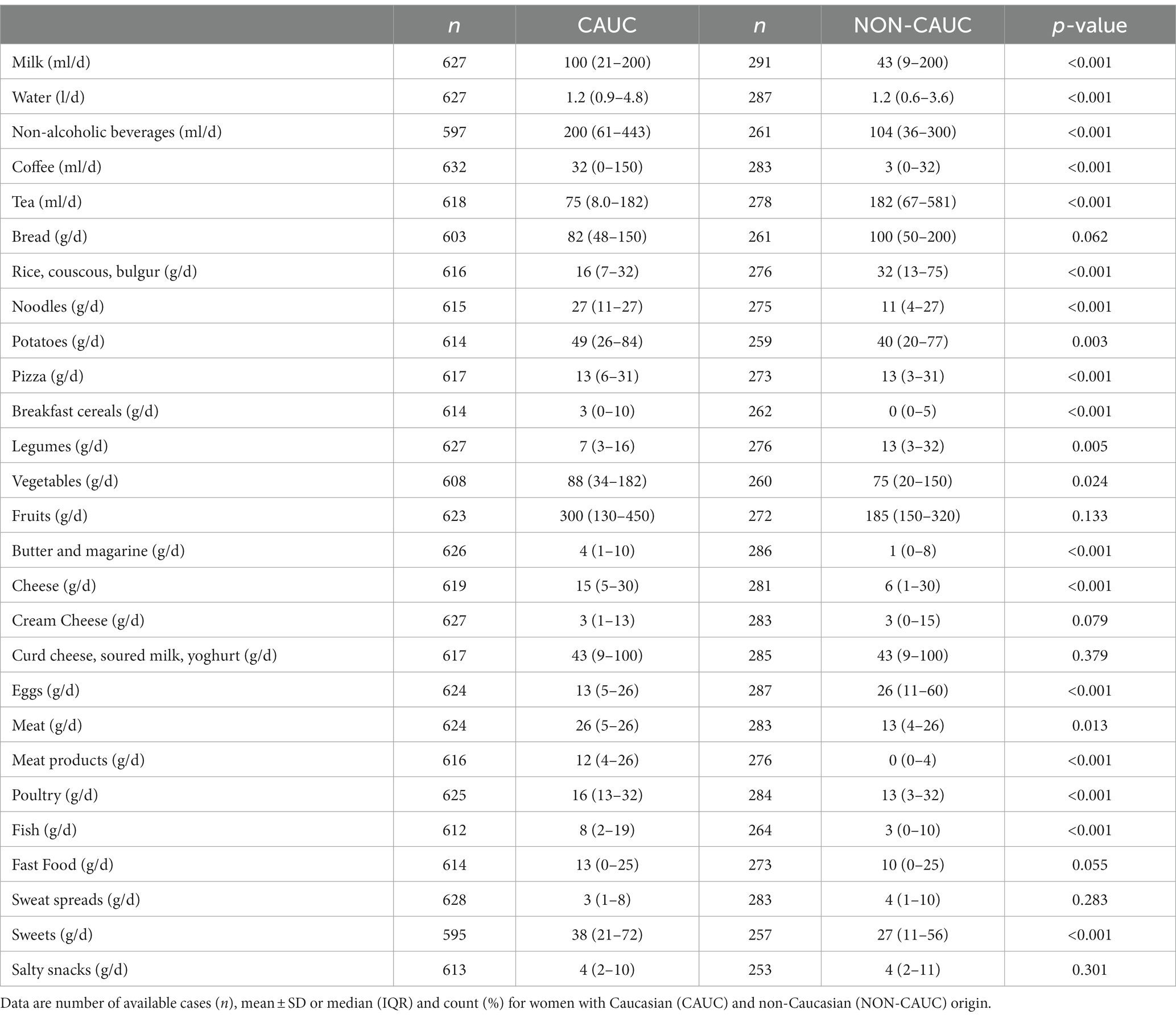
Table 3. Dietary habits at early pregnancy of women with Caucasian and non-Caucasian origin.
The prevalence of GDM was higher in non-Caucasian mothers as compared to the Caucasian population (n = 108, 28.5% vs. n = 128, 17.5%, OR 1.87, 95%CI 1.40 to 2.52, p < 0.001) and comparable results were observed after adjustment for maternal age and BMI (adjusted OR 1.90, 95%CI 1.41 to 2.58, p < 0.001). The results remained unchanged in a fully adjusted logistic regression model including the variables provided in Tables 2, 3 (adjusted OR 2.95, 95%CI 1.32 to 6.60, p = 0.008) as well as in a reduced model using stepwise selection (adjusted OR 3.38, 95%CI 1.74 to 6.60, p < 0.001). Likewise, non-Caucasian mothers showed higher glucose concentrations within the diagnostic OGTT vs. Caucasian mothers (OGTT glucose baseline: 83 ± 9 vs. 81 ± 10 mg/dL, p = 0.001; OGTT glucose 60′: 142 ± 37 vs. 132 ± 33 mg/dL, p < 0.001; OGTT glucose 120′: 113 ± 28 vs. 106 ± 25 mg/dL, p < 0.001) and required glucose lowering medications more often (n = 61, 56.5% vs. n = 53, 41.4%, p = 0.022 for non-Caucasian vs. Caucasian GDM patients, respectively). A detailed analysis of regional origin showed that the increased incidence of GDM was especially observed in MENA (OR 1.95, 95%CI 1.35 to 2.79, p < 0.001) and Asian mothers (OR 2.09, 95%CI 1.36 to 3.17, p < 0.001). However, no differences were observed in pregnancy outcomes including cesarean section rate (p = 0.919), international birth weight percentiles (p = 0.980) or the incidence of LGA offspring (p = 0.871) and the results remained unchanged when women with normal glucose tolerance were excluded. Likewise, we found no significant difference in LGA delivery in previous pregnancy.
Ethnically stratified variable importance metrics were calculated for 396 Caucasian (64 with GDM) and 114 non-Caucasian women (MENA: 63, 20 with GDM; ASIA: 46, 15 with GDM; SSA: 5, 1 with GDM) with complete information about baseline characteristics (as summarized in Table 2) and dietary habits (as summarized in Table 3). As visualized in Figure 1, fasting glucose as well as HOMA-IR achieved high variable importance scores in both Caucasian and non-Caucasian mothers. Pregestational BMI was a more important predictor in non-Caucasian mothers, whereas history of pregnancy with GDM was more important in Caucasian mothers. In general, dietary habits were of minor importance in both groups. The estimated out of bag error (as a measurement of prediction error of the random forest) was lower in Caucasian patients as compared to non-Caucasian mothers (16.7% vs. 26.1%). In a further analysis non-Caucasian mothers were stratified according to their regional origin and showed that fasting glucose was especially important in women from the MENA regions, whereas maternal pregestational BMI and insulin sensitivity status was more important in Asian mothers (Figure 2). Due to the restricted sample size women from the SSA region were excluded from this analysis.
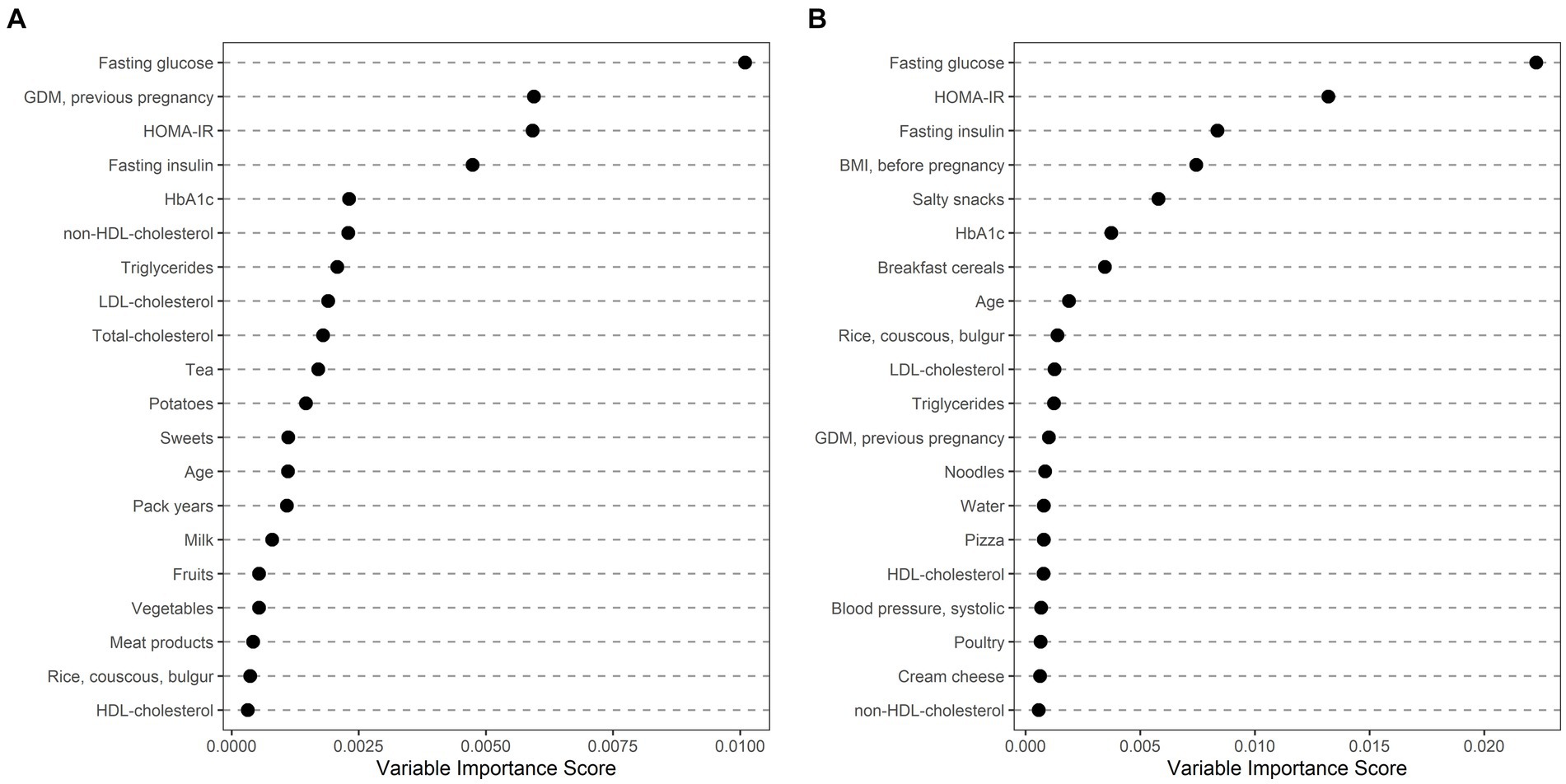
Figure 1. Ethnically stratified risk factors for GDM at early pregnancy showing variable importance scores for mothers with Caucasian (A) and non-Caucasian (B) origin. The first 20 variables with highest variable scores are shown.
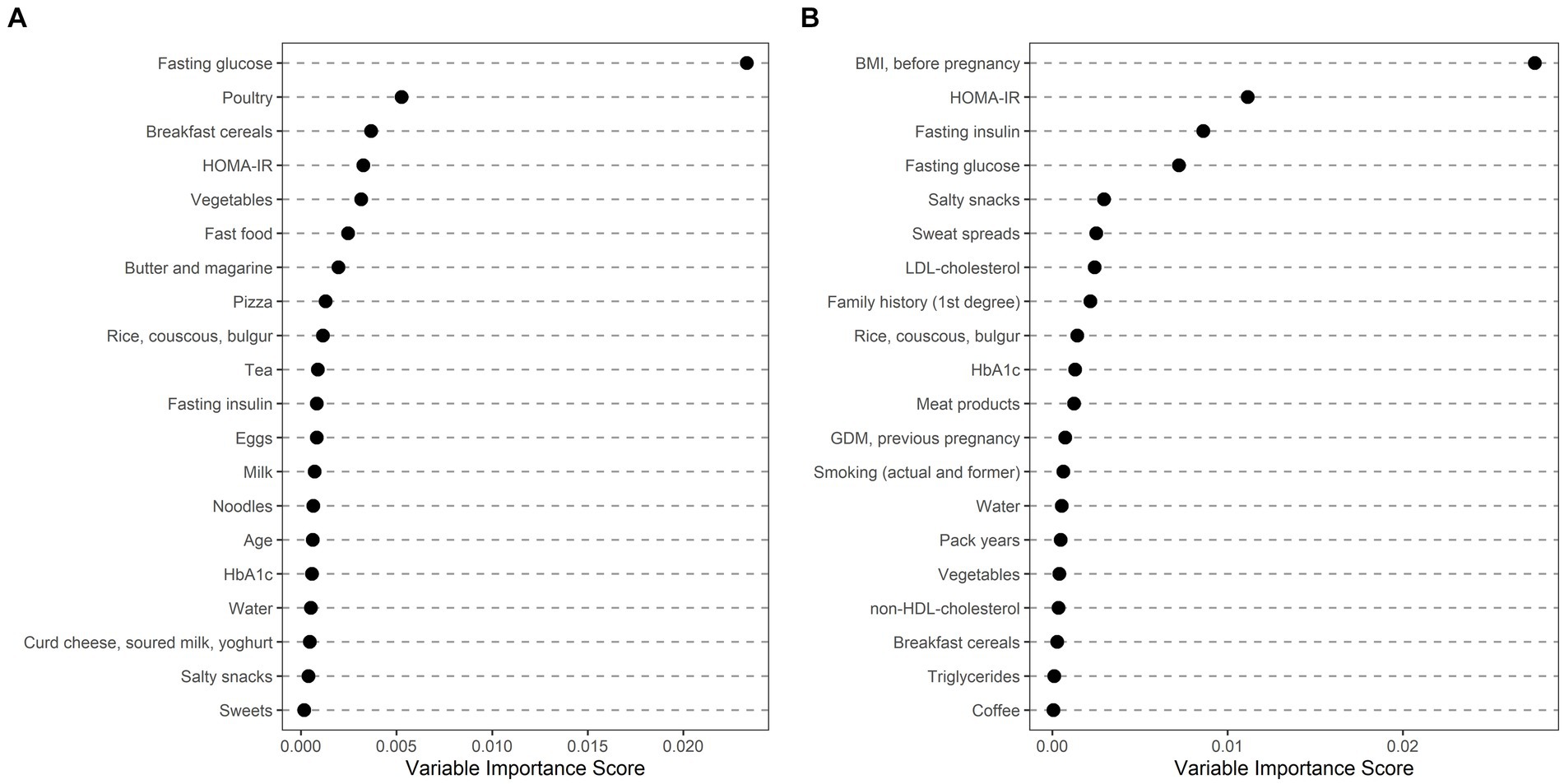
Figure 2. Ethnically stratified risk factors for GDM at early pregnancy showing variable importance scores for non-Caucasian mothers with Middle Eastern and Northern African (A) and Asian origin (B). The first 20 variables with highest variable scores are shown.
This study aimed to assess the role of ethnicity on the development of GDM in a prospectively assessed and well characterized multiethnic Central European cohort. We found that women with non-Caucasian ancestry, especially those with origin from the MENA and Asian countries have markedly increased risk as compared to Caucasian mothers. This is corroborated by results of some previous retrospective and register studies, suggesting a higher GDM incidence for specific ethnicities and minorities, such as South and East Asian, Indigenous Australian, African, Hispanics and Native Americans (24–28). Recently, Caputo et al. retrospectively analyzed data of 586 patients and found that despite being younger, GDM patients from “high migration pressure countries” required insulin treatment more often, what is also indicated for non-Caucasian mothers in our study (29). Likewise, a population based Norwegian register study identified substantially increased GDM incidence in immigrant women, whereby the risk for hyperglycemia increased in parallel to the length of residence in certain immigrant groups (9), suggesting, that the elevated risk in these mothers is not only attributable to a genetic predisposition (24).
In the present study, we also observed distinct differences in patient characteristics and clinical-metabolic features between Caucasian and non-Caucasian women. Thereby, non-Caucasian mothers had higher pregestational BMI, were more insulin resistant and showed an adverse glucometabolic risk profile with higher fasting glucose, and HbA1c already at start of gestation. In another study of reproductive-aged Austrian women, we previously found that women with origin from the MENA countries undergoing infertility treatment were more obese and, despite being younger as compared to Caucasian patients, showed impaired ovarian function, possibly explained by a higher incidence of Polycystic Ovarian Syndrome – a disease markedly triggered by impaired insulin sensitivity (30). This is comparable to our present study, indicating that especially women with origin from the MENA region had higher BMI as well as a higher degree of insulin resistance and consequently an increased risk for GDM development. Aside from the MENA population, we additionally observed an increased risk for GDM in mothers with Asian ancestry. This is in line with another recent register study, indicating that the risk of GDM is increased in mothers with South Asian and Chinese ethnicity, who had lower BMI as compared to the general Canadian population (11). Interestingly, Sharma et al. observed, that glucose metabolism remained markedly impaired after GDM pregnancy, in particular in Asian mothers, who showed impaired β-cell function, insulin action and clearance as compared to Nordic women (31).
Ethnically specific differences are often explained by different lifestyle habits, especially dietary patterns. Thereby, some authors suggested that “nutrition transition” towards an energy dense Western diet may promote the development of metabolic disorders and the requirement of glucose lowering medication in GDM patients (29, 32, 33). Dietary habits can also directly affect fetal development and growth and this effect can be possibly modulated by ethnicity. For example, Zulyniak et al. found that consumption of plant-based diet reduced infant birth weight in white Europeans, whereas it increased the risk for LGA infants in South Asians living in Canada (34). Another meta-analysis recently assessed the effect of healthy diet on GDM incidence and indicated significant associations between dietary patterns and GDM risk markedly in white European mothers, whereas no consistent evidence was observed in non-Caucasian populations, what may be explained by heterogenous use of dietary assessment tools (35). Differences in dietary patterns were also observed in our study, whereby non-Caucasian immigrants differed markedly from the Caucasian population. However, a detailed analysis of GDM risk factors indicated that dietary patterns had inferior variable importance scores as compared to other clinical-metabolic features, such as fasting glucose and maternal insulin resistance, showing consistently high predictive performance in Caucasian and non-Caucasian mothers. Of note, maternal pregestational BMI achieved notably higher importance for GDM prediction in Asian mothers. In line with our findings, Read et al. found that BMI increased the risk for GDM at far lower levels in South Asian and Chinese mothers, possibly indicating that limiting excess weight gain may be particular effective for GDM prevention in Asian mothers (11). This effect may be mediated by distinct metabolic profiles of Asian and white European women as recently suggested by another study (36).
Some advantages and limitations need to be addressed: Clinical and metabolic risk factors as well as dietary patterns were only assessed once at start of pregnancy, what may be seen as a limitation. However, the large sample size with a high proportion of non-Caucasian study participants and GDM cases is a clear advantage. In addition, the prospective character of the cohort study design allowed us to assess detailed information about ancestry (i.e., the parental country of origin) and allowed us to accurately determine patient’s ethnicity. Moreover, this is for our knowledge the first study including information of clinical features, metabolic parameters (such as early gestational insulin sensitivity) and dietary habits in a multiethnic cohort of pregnant women.
In summary, we identified distinct differences in dietary patterns and clinical metabolic features between Caucasian and non-Caucasian mothers, who showed a higher incidence of GDM and need of glucose lowering medications. GDM risk was highest in Asian mothers and those with origin from the MENA region. Fasting plasma glucose as well as maternal insulin resistance at start of pregnancy are important risk factors in both, Caucasian and non-Caucasian mothers, although, increased maternal BMI (even at lower levels) may be of particular importance in Asians. The information provided by our study is of clinical relevance to improve risk stratification and to provide “culturally appropriate care” (14) for non-Caucasian ethnicities indicating the need for further research in non-Caucasian populations.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the Ethics Committee of the Medical University of Vienna. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
GK: Writing – original draft, Writing – review & editing, Data curation, Project administration. CM: Writing – original draft, Writing – review & editing. TL: Data curation, Writing – review & editing. DE: Writing – review & editing. VS: Writing – review & editing. MF: Writing – review & editing. BM: Writing – review & editing. VF: Writing – review & editing. SW: Writing – review & editing. WH: Writing – review & editing. AT: Formal analysis, Writing – review & editing. CG: Conceptualization, Data curation, Formal analysis, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The researchers are indebted to the participants for their willingness to participate in the study and to the staff of the pregnancy outpatient clinic at the Department of Obstetrics and Gynaecology, Medical University of Vienna for their contribution.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1286056/full#supplementary-material
BMI, body mass index; FPG, fasting plasma glucose; GDM, gestational diabetes mellitus; HbA1c, glycated haemoglobin A1c; HDL-cholesterol, high density lipoprotein cholesterol; HOMA-IR, homeostasis model assessment of insulin resistance; IADPSG, International Association of the Diabetes and Pregnancy Study Groups; IQR, interquartile range; LDL-cholesterol, low density lipoprotein cholesterol; LGA, large for gestational age; MENA, Middle East and North Africa; NCD-RisC, Non-Communicable Diseases Risk Factors Collaboration; OGTT, oral glucose tolerance test; SSA, Sub Saharan African.
1. Sacks, DA, Hadden, DR, Maresh, M, Deerochanawong, C, Dyer, AR, Metzger, BE, et al. Frequency of gestational diabetes mellitus at collaborating centers based on IADPSG consensus panel-recommended criteria: the hyperglycemia and adverse pregnancy outcome (HAPO) study. Diabetes Care. (2012) 35:526–8. doi: 10.2337/dc11-1641
2. Huhn, EA, Massaro, N, Streckeisen, S, Manegold-Brauer, G, Schoetzau, A, Schulzke, SM, et al. Fourfold increase in prevalence of gestational diabetes mellitus after adoption of the new International Association of Diabetes and Pregnancy Study Groups (IADPSG) criteria. J Perinat Med. (2017) 45:359–66. doi: 10.1515/jpm-2016-0099
3. Wang, H, Li, N, Chivese, T, Werfalli, M, Sun, H, Yuen, L, et al. IDF Diabetes atlas: estimation of global and regional gestational diabetes mellitus prevalence for 2021 by International Association of Diabetes in pregnancy study Group’s criteria. Diabetes Res Clin Pract. (2022) 183:109050. doi: 10.1016/j.diabres.2021.109050
4. Hod, M, Kapur, A, Sacks, DA, Hadar, E, Agarwal, M, Di Renzo, GC, et al. The International Federation of Gynecology and Obstetrics (FIGO) initiative on gestational diabetes mellitus: a pragmatic guide for diagnosis, management, and care #. Int J Gynecol Obstet. (2015) 131:S173–211. doi: 10.1016/S0020-7292(15)30033-3
5. Shah, NS, Wang, MC, Freaney, PM, Perak, AM, Carnethon, MR, Kandula, NR, et al. Trends in gestational diabetes at first live birth by race and ethnicity in the US, 2011–2019. J Am Med Assoc. (2021) 326:660–9. doi: 10.1001/jama.2021.7217
6. Liu, B, Lamerato, LE, and Misra, DP. A retrospective analysis of the relationship between race/ethnicity, age at delivery and the risk of gestational diabetes mellitus. J Matern Fetal Neonatal Med. (2020) 33:2961–9. doi: 10.1080/14767058.2019.1566310
7. Webber, J, Charlton, M, and Johns, N. Diabetes in pregnancy: management of diabetes and its complications from preconception to the postnatal period (NG3). Br J Diabetes Vasc Dis. (2015) 15:107. doi: 10.15277/bjdvd.2015.029
8. Bastola, K, Koponen, P, Skogberg, N, Gissler, M, and Kinnunen, TI. Gestational diabetes among women of migrant origin in Finland-a population-based study. Eur J Pub Health. (2021) 31:784–9. doi: 10.1093/eurpub/ckab078
9. Strandberg, RB, Iversen, MM, Jenum, AK, Sørbye, LM, Vik, ES, Schytt, E, et al. Gestational diabetes mellitus by maternal country of birth and length of residence in immigrant women in Norway. Diabet Med. (2021) 38:e14493. doi: 10.1111/dme.14493
10. Gao, C, Sun, X, Lu, L, Liu, F, and Yuan, J. Prevalence of gestational diabetes mellitus in mainland China: a systematic review and meta-analysis. J Diabetes Investig. (2019) 10:154–62. doi: 10.1111/jdi.12854
11. Read, SH, Rosella, LC, Berger, H, Feig, DS, Fleming, K, Ray, JG, et al. BMI and risk of gestational diabetes among women of south Asian and Chinese ethnicity: a population-based study. Diabetologia. (2021) 64:805–13. doi: 10.1007/s00125-020-05356-5
12. Al-Rifai, RH, Abdo, NM, Paulo, MS, Saha, S, and Ahmed, LA. Prevalence of gestational diabetes mellitus in the Middle East and North Africa, 2000–2019: a systematic review, meta-analysis, and meta-regression. Front Endocrinol (Lausanne). (2021) 12:668447. doi: 10.3389/fendo.2021.668447
13. Kragelund Nielsen, K, Andersen, GS, Damm, P, and Andersen, AMN. Gestational diabetes risk in migrants. A Nationwide, register-based study of all births in Denmark 2004 to 2015. J Clin Endocrinol Metab. 105:2020, e692–e703. doi: 10.1210/clinem/dgaa024
14. Tzotzis, L, Hooper, M-E, Douglas, A, Kurz, E, Atchan, M, Spiller, S, et al. The needs and experiences of women with gestational diabetes mellitus from minority ethnic backgrounds in high-income nations: a systematic integrative review. Women Birth. (2023) 36:205–16. doi: 10.1016/j.wombi.2022.08.006
15. Kotzaeridi, G, Blätter, J, Eppel, D, Rosicky, I, Mittlböck, M, Yerlikaya-Schatten, G, et al. Performance of early risk assessment tools to predict the later development of gestational diabetes. Eur J Clin Investig. (2021) 51:e13630. doi: 10.1111/eci.13630
16. NCD Risk Factor Collaboration. Worldwide trends in diabetes since. A pooled analysis of 751 population-based studies with 4·4 million participants NCD risk factor collaboration (NCD-RisC) Europe PMC funders group. Lancet. (1980) 2016:387.
17. Matthews, DR, Hosker, JP, Rudenski, AS, Naylor, BA, Treacher, DF, and Turner, RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. (1985) 28:412–9. doi: 10.1007/BF00280883
18. International Association of D, Pregnancy Study Groups Consensus P. International Association of Diabetes and Pregnancy Study Groups Recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. (2010) 33:676–82. doi: 10.2337/dc09-1848
19. Schäfer-Graf, UM, Gembruch, U, Kainer, F, Groten, T, Hummel, S, Hösli, I, et al. Gestational diabetes mellitus (GDM) – diagnosis, treatment and follow-UpGuideline of the DDG and DGGG (S3 level, AWMF registry number 057/008, February 2018). Geburtshilfe Frauenheilkd. (2018) 78:1219–31. doi: 10.1055/a-0659-2596
20. Haftenberger, M, Heuer, T, Heidemann, C, Kube, F, Krems, C, and Mensink, GBM. Relative validation of a food frequency questionnaire for national health and nutrition monitoring. Nutr J. (2010) 9:36. doi: 10.1186/1475-2891-9-36
22. R Development Core Team. R Core Team. (2020). R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Available at: https://www.R-project.org/. R Foundation for Statistical Computing. 2019; 2.
23. Konietschke, F, Placzek, M, Schaarschmidt, F, and Hothorn, LA. Nparcomp: an R software package for nonparametric multiple comparisons and simultaneous confidence intervals. J Stat Softw. (2015) 64:1–17. doi: 10.18637/jss.v064.i09
24. Yuen, L, Wong, VW, and Simmons, D. Ethnic disparities in gestational diabetes. Curr Diab Rep. (2018) 18:68. doi: 10.1007/s11892-018-1040-2
25. Xiang, AH, Li, BH, Black, MH, Sacks, DA, Buchanan, TA, Jacobsen, SJ, et al. Racial and ethnic disparities in diabetes risk after gestational diabetes mellitus. Diabetologia. (2011) 54:3016–21. doi: 10.1007/s00125-011-2330-2
26. Dornhorst, A, Paterson, CM, Nicholls, JS, Wadsworth, J, Chiu, DC, Elkeles, RS, et al. High prevalence of gestational diabetes in women from ethnic minority groups. Diabet Med. (1992) 9:820–5. doi: 10.1111/j.1464-5491.1992.tb01900.x
27. Berkowitz, GS, Lapinski, RH, Wein, R, and Lee, D. Race/ethnicity and other risk factors for gestational diabetes. Am J Epidemiol. (1992) 135:965–73. doi: 10.1093/oxfordjournals.aje.a116408
28. Jaffe, A, Giveon, S, Rubin, C, Novikov, I, Ziv, A, and Kalter-Leibovici, O. Gestational diabetes risk in a multi-ethnic population. Acta Diabetol. (2020) 57:263–9. doi: 10.1007/s00592-019-01404-8
29. Caputo, M, Bullara, V, Mele, C, Samà, MT, Zavattaro, M, Ferrero, A, et al. Gestational diabetes mellitus: clinical characteristics and perinatal outcomes in a multiethnic population of North Italy. Int J Endocrinol. (2021) 2021:1–10. doi: 10.1155/2021/9474805
30. Feichtinger, M, Göbl, C, Weghofer, A, and Feichtinger, W. Reproductive outcome in European and middle eastern/north African patients. Reprod Biomed Online. (2016) 33:684–9. doi: 10.1016/j.rbmo.2016.09.003
31. Sharma, A, Lee-Ødegård, S, Qvigstad, E, Sommer, C, Sattar, N, Gill, JMR, et al. β-Cell function, hepatic insulin clearance, and insulin sensitivity in south Asian and Nordic women after gestational diabetes mellitus. Diabetes. (2022) 71:2530–8. doi: 10.2337/db22-0622
32. Popkin, BM. Nutrition transition and the global diabetes epidemic. Curr Diab Rep. (2015) 15:64. doi: 10.1007/s11892-015-0631-4
33. Popkin, BM, and Ng, SW. The nutrition transition to a stage of high obesity and noncommunicable disease prevalence dominated by ultra-processed foods is not inevitable. Obes Rev. (2022) 23:e13366. doi: 10.1111/obr.13366
34. Zulyniak, MA, De Souza, RJ, Shaikh, M, Desai, D, Lefebvre, DL, Gupta, M, et al. Does the impact of a plant-based diet during pregnancy on birth weight differ by ethnicity? A dietary pattern analysis from a prospective Canadian birth cohort alliance. BMJ Open. (2017) 7:e017753. doi: 10.1136/bmjopen-2017-017753
35. Fuller, H, Moore, JB, Iles, MM, and Zulyniak, MA. Ethnic-specific associations between dietary consumption and gestational diabetes mellitus incidence: a meta-analysis. PLOS Glob Public Health. (2022) 2:e0000250. doi: 10.1371/journal.pgph.0000250
Keywords: gestational diabetes mellitus, ethnicity, risk prediction, glucose levels, migration, risk stratification
Citation: Kotzaeridi G, Monod C, Linder T, Eppel D, Seidel V, Feichtinger M, Mosimann B, Filippi V, Wegener S, Henrich W, Tura A and Göbl CS (2024) The impact of regional origin on the incidence of gestational diabetes mellitus in a multiethnic European cohort. Front. Public Health. 11:1286056. doi: 10.3389/fpubh.2023.1286056
Edited by:
Guoju Li, Qingdao Women and Children’s Hospital, ChinaReviewed by:
Xinyu Zhao, Beijing Friendship Hospital, ChinaCopyright © 2024 Kotzaeridi, Monod, Linder, Eppel, Seidel, Feichtinger, Mosimann, Filippi, Wegener, Henrich, Tura and Göbl. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christian S. Göbl, Y2hyaXN0aWFuLmdvZWJsQG1lZHVuaXdpZW4uYWMuYXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.