 Jing Pang
Jing Pang Fuyi Tu
Fuyi Tu Yiwen Han1
Yiwen Han1
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 23 November 2023
Sec. Aging and Public Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1284959
This article is part of the Research TopicPromoting Healthy Aging Across the LifespanView all 39 articles
Background: Any form of physical activity is recommended for the older adults to maintain their physical function; however, the effect of daily activities on muscle function still needs to be investigated. Humans always use one dominant hand to perform tasks, providing a natural situation for research on the effect of daily activities on muscle function.
Methods: Five hundred and twenty-six healthy adults were recruited from the community in Beijing. Muscle strength was assessed using a handgrip dynamometer, lean mass, fat mass, bone area and bone mineral content of upper limbs were assessed using dual-energy X ray-absorptiometry. The results were compared between the dominant and non-dominant upper limbs.
Results: The dominant upper limb had better muscle strength, lean mass, bone area and bone mineral content than the non-dominant side. The difference in muscle strength and lean mass between the two upper limbs decreased with the advanced age. In older age, fat mass of upper limbs increased in men, but not in women.
Conclusion: Daily activities can maintain better muscle function in the dominant upper limb than in the non-dominant side; however, the delaying effect on age-related decline in muscle function was limited.
Sarcopenia is an adverse change in muscle across the whole lifetime, especially in older age. It is defined by the loss of muscle mass, and decreases in muscle strength and physical performance (1, 2). Older adults people with less muscle might have a higher risk of disability. Walking is a basic requirement for independent living, thus most studies have focused on the change of lower limbs with aging (3). There have been relatively fewer studies about the age-related decline in the upper limbs.
The upper limbs play important roles in everyday living, such as feeding, dressing, and grooming, which are critical tasks for independent living. The decline in upper limb strength may impact these activities and reduce quality of life (4, 5). In the Asian Working Group for Sarcopenia 2019 consensus, low muscle strength is defined as handgrip strength <28 kg for men and < 18 kg for women (6). Low handgrip strength is a simple and powerful predictor for future disability (7, 8) and falls (9–11). Similar to lower limb function, upper limb function also involves several physiological domains. A previous study demonstrated that performance in muscle strength, arm stability, dexterity, and coordination of the upper limbs significantly decreased with age (12). To study the upper limbs, handgrip strength is the most popular indicator for muscle function assessment (13). However, muscle strength is only one part of muscle performance, and how other muscle indicators change in the upper limbs with aging are unknown.
In contrast to the lower limbs, people usually have a dominant side when performing tasks using the upper limbs. The dominant side always has greater muscle strength than the non-dominant side (14). Several physical activities, such as doing housework and playing with balls, usually practice only one side of the upper limbs. Therefore, the comparison of muscle performance between the two upper limbs might provide guidance to evaluate the effect of daily activities on muscle function maintenance.
Muscle performance is a loosely defined concept that broadly includes muscle mass, muscle strength, and muscle composition (15). Herein, we compared several muscle indicators between the two upper limbs and observed the age-related changes in them. The results might help us to realize the relationship among daily activities, muscle function and aging, and give us a clue to determine which kind of muscle indicators could be used for early recognition and intervention in motor function decline. This can help us to optimize the intervention strategies for healthy aging.
The healthy subjects were volunteers to participant in this study. 538 Chinese adults (526 right-hand dominant and 12 left-hand dominant) aged 25–89 years were recruited from the community of Beijing in 2015. The proportion of left-dominant and right-dominant participants was imbalance; therefore we only analyzed the data of right-hand dominant participants (Table 1). A brief questionnaire, including basic demographic details, physical status, exercise, and medical history information was completed. Subjects who participated in regular strength training of the upper limbs (>1 time/week and > 10 min/time training) were excluded. The subjects’ informed consent was obtained to use their information in this study; and the study was approved by the Ethics Committee of Beijing Hospital (approval No. 2012BJYYEC-052-02).
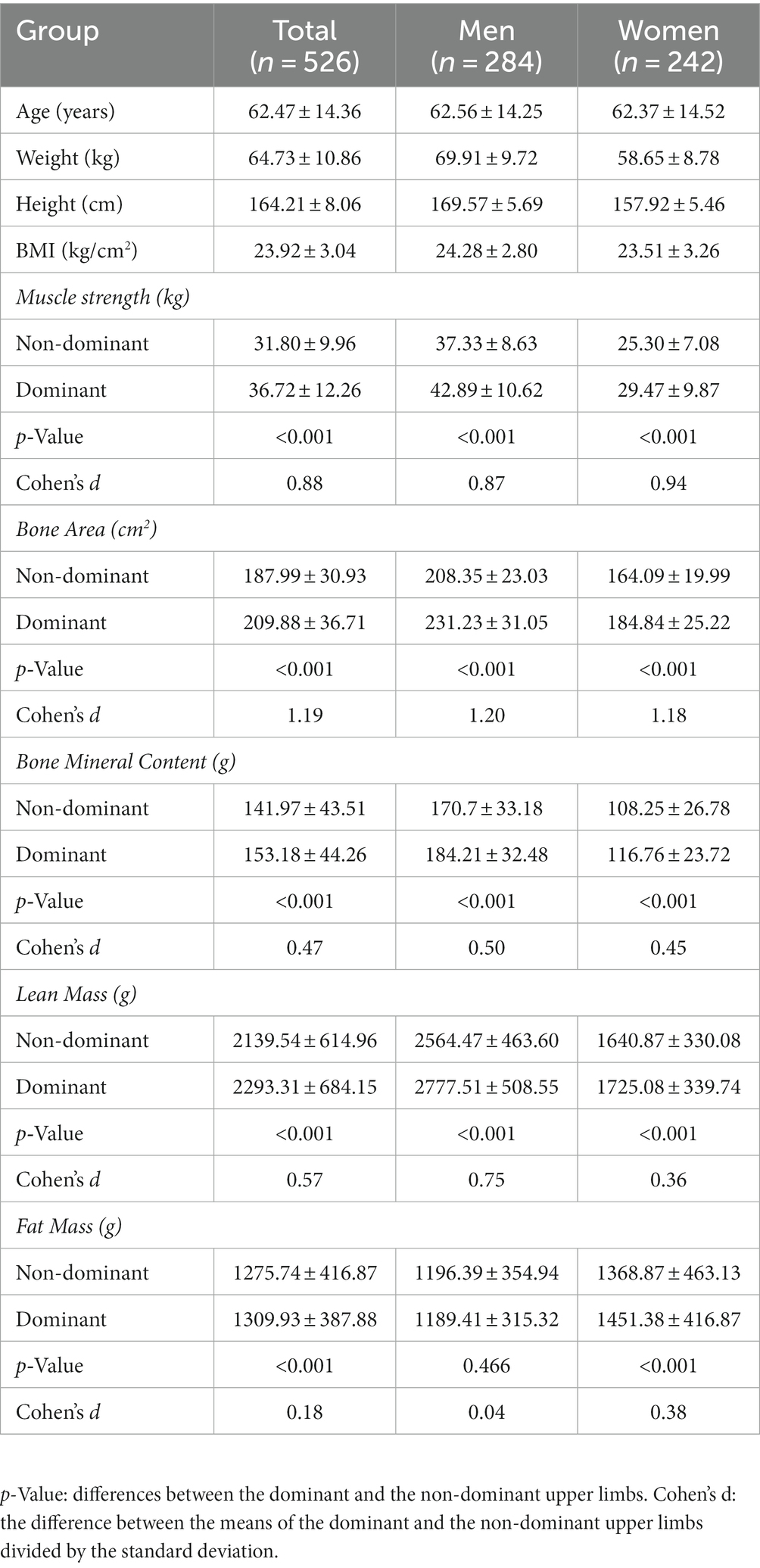
Table 1. Parameters of the dominant and non-dominant upper limbs in muscle performance between men and women (mean ± SD).
Handgrip strength (HS) was assessed in each hand using a JAMAR digital dynamometer (Sammons Preston, Chicago, IL, United States), which was measured twice for each hand and the higher value was used in the analysis.
All the participants completed the dual-energy X ray-absorptiometry (DEXA, Hologic QDR 4500A, Hologic) measurement in Beijing hospital. A standardized procedure for body composition detection and QDR software analysis were used. From DEXA scans, lean mass, fat mass, bone area and bone mineral content (BMC) of two upper limbs were evaluated.
Descriptive statistics were used to characterize the demographics and the measured variables of the subjects. All values are shown as the mean ± SD. The differences between the two upper limbs were compared using a paired t-test. A sample size of 29 achieves 90% power to detect a mean of paired differences of 3.0 with an estimated standard deviation of differences of 5.0 and with a significance level (alpha) of 0.05 using a two-sided paired t-test. The statistical analyses were carried out using SPSS 21.0 (IBM Corp., Armonk, NY, United States), and p < 0.05 was considered statistically significant.
For analysis the age-related patterns of muscle performance in two upper limbs, we employed the restricted cubic spline (RCS) to flexibly model and visualize the relationships between age and each indicator. RCS fitted a smooth and continuous curve for each indicator across the range of ages, allowing for cubic form changes in function at specific age points - 45, 55, 65 and 75 years - referred to as knot points. The curves obtained by RCS reflect the overall age-related changes of each indicator, and we further identified the change points at which abrupt changes occur in each indicator during ageing based on the fitted RCS curves. The segmented regression is a common choice for change point detection (16, 17). Given an initial guess for the change point, the segment regression fitted a piecewise linear function and updated the change point to minimize the gap between the two fitted intersecting lines. The process iterated until convergence is reached, ultimately yielding the optimal change point. The left and right slopes are calculated together with the estimated change point. The analyses of this part were performed using R (Version 4.3.1).
All the muscle performance indicators (muscle strength, lean mass, fat mass, bone area and bone mineral content) were exhibited significantly differences between the two upper limbs (p < 0.05, Table 1). The muscle strength, lean mass, bone area, and bone mineral content of the dominant upper limb were much higher than those of the non-dominant side both in male and female participants (p < 0.05, Table 1). In women, the dominant upper limb had more fat mass than the non-dominant one (p < 0.05); however, there was no difference in fat mass between the two sides in men.
In females, the dominant upper limb exhibited higher muscle strength, lean mass, fat mass, bone area, and bone mineral content than the non-dominant upper limb in each age group (Table 2). In males, the muscle strength, lean mass and bone area showed significant differences between the two upper limbs in each age group; however, there was no difference of bone mineral content and fat mass between the two sides in older group. We calculated the value of the dominant upper limb minus the non-dominant upper limb (D-value). The difference in muscle strength and lean mass between the two upper limbs decreased significantly with age both in male and female participants. Compared with those in 25–59 years old group, D-value for muscle strength in 75+ years old group decreased by 54% for males and 55% for females; D-value for lean mass in 75+ years old group decreased by 58% for males and 59% for females.
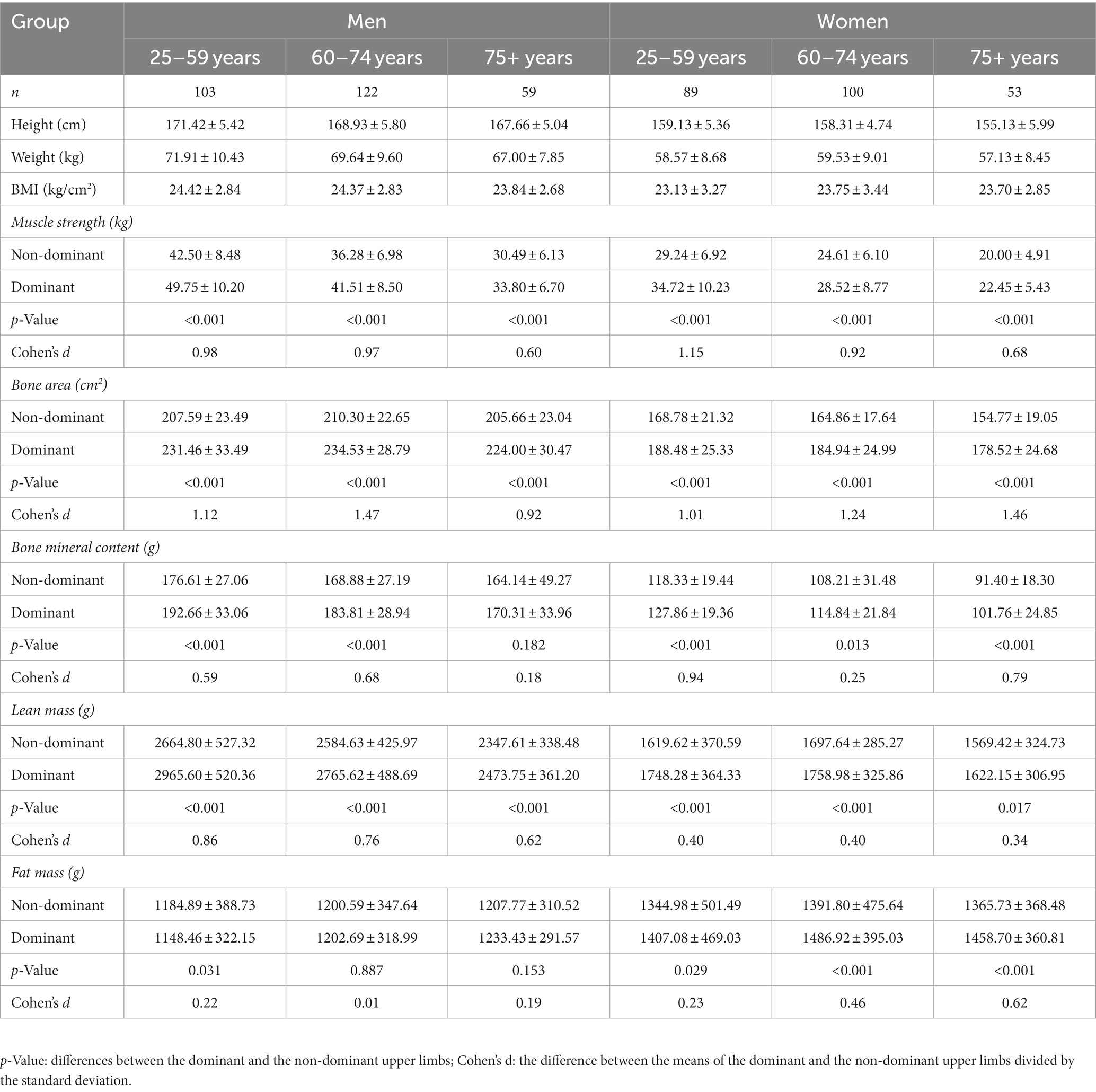
Table 2. Parameters of the dominant and non-dominant upper limbs in muscle performance within different age groups (mean ± SD).
We observed the trend of muscle performance indicators changed with age (Figure 1), analyzed the cutoff point of each indicator (Figure 2) and calculated the slope of them (Table 3). After 50 years old, the slope of muscle strength and lean mass in the dominant upper limb declined more significantly than those in the non-dominant upper limb both in males and females participants. The change of fat mass showed a sexual difference. After 50 years old, the fat mass of both upper limbs increased significantly in males, but decreased in females. In males, the slope of bone mineral content changed more significantly in the dominant upper limb than that in the non-dominant upper limb after 65 years old. In females, the age-related trend of bone mineral content was similar between the two upper limbs.
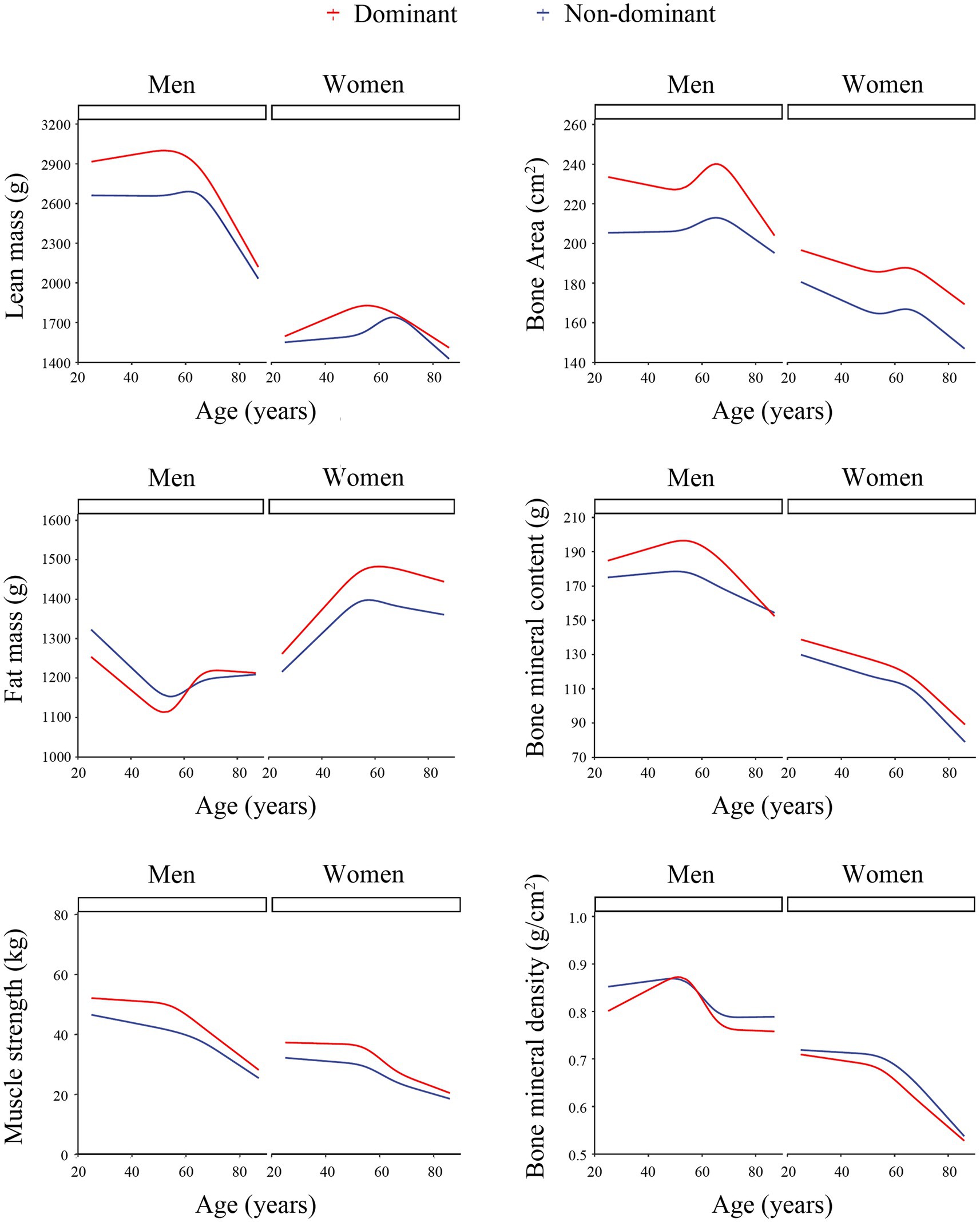
Figure 1. Age-related changes in muscle performance indicators between the two upper limbs. The curves obtained by the restricted cubic spline analysis. The red line represented the change of the dominant upper limb; the blue line represented the change of the non-dominant upper limb.
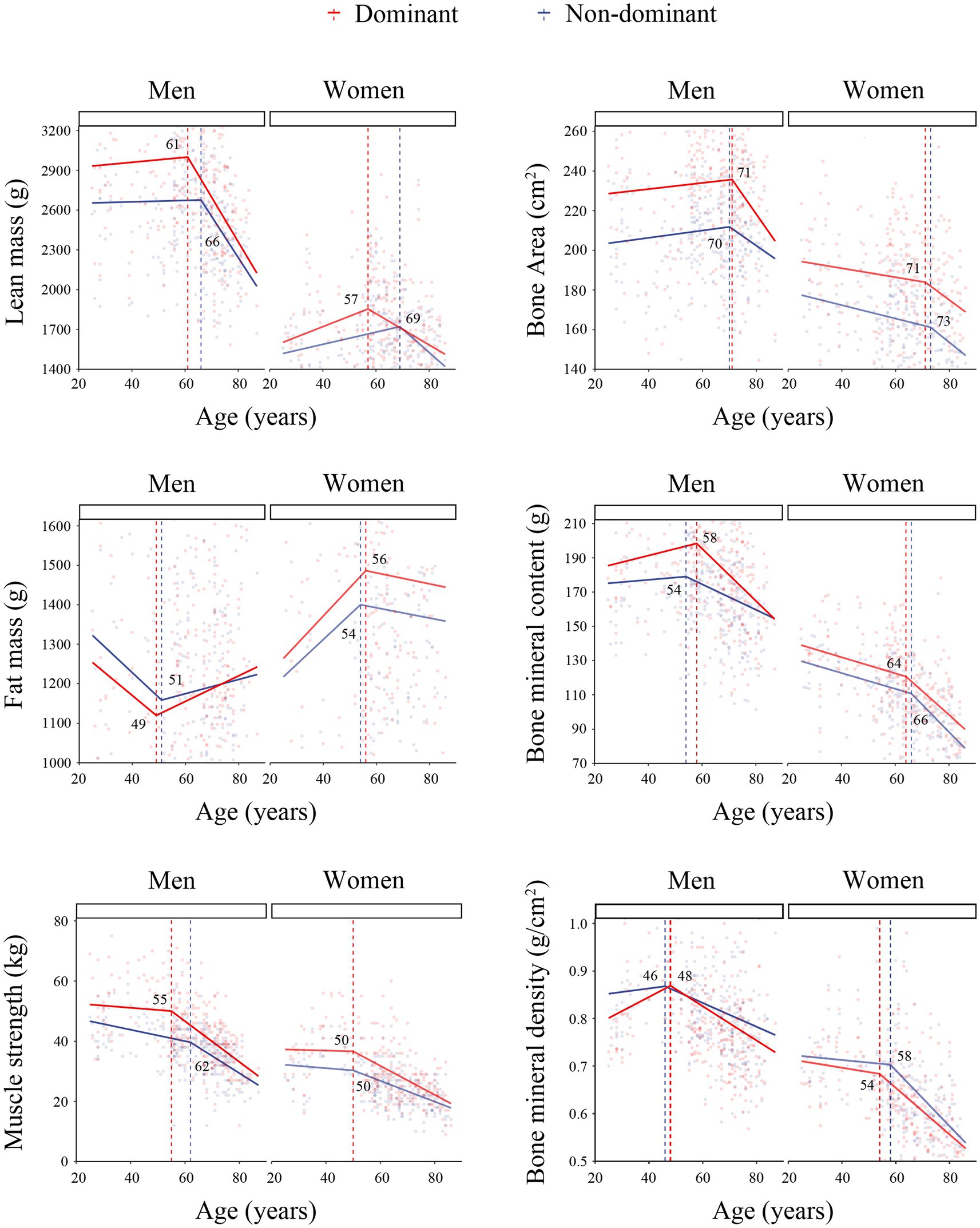
Figure 2. The cutoff points of muscle performance indicators changed with age. The age at the cutoff point was marked. The red line represented the change of the dominant upper limb; the blue line represented the change of the non-dominant upper limb.
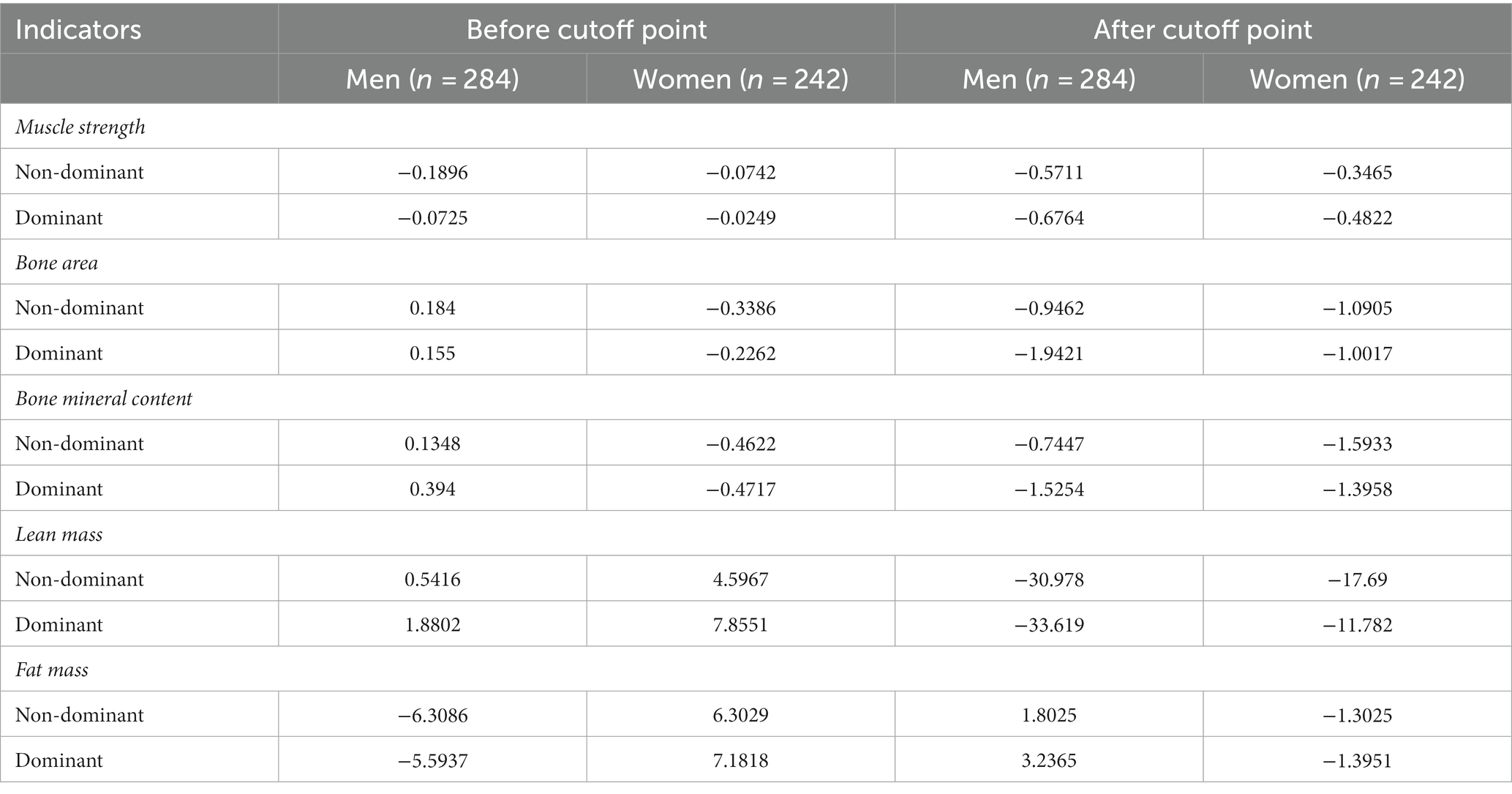
Table 3. The slope of age-related changes in muscle performance indicators.
Physical activity is important for physical function maintenance. People always have one dominant hand for carrying out daily tasks. The dominant hand is usually involved in more physical activity than the non-dominant hand, which might lead to different muscle performance between them. In this study, we compared several muscle performance indicators of the two upper limbs and found that the dominant upper limb maintained the better muscle performance than the non-dominant side, but the difference between the two sides decreased with the advanced age.
In this study, the handgrip strength of the dominant upper limb declined faster than that of the non-dominant upper limb in older age. Consistent with this, men had stronger handgrip strength than women, but the strength of men declined faster than that of women during aging (18, 19). Daily activities can increase muscle strength, but cannot prevent muscle aging. There may be two ways for muscle function maintenance: (1) doing more activities from young age to reserve high intrinsic ability; (2) engaging in more activities in old age for anti-aging.
Muscle strength and muscle mass are two important indicators for motor function assessment (1, 2); however, which indicator is more sensitive for sarcopenia early recognition still need to be investigated. In this study, both muscle strength and lean mass of upper limbs showed significant differences between the two sides and declined with age. In addition, we observed that muscle strength began to decline significantly at age 55 in men and age 50 in women, which was earlier than lean mass declined at age 61 in men and age 57 in women. This result supported the European consensus on Sarcopenia diagnosis revised in 2019, in which muscle strength detection was modified as an early screening indicator for muscle mass loss (2). Previous studies also found that physical intervention affected muscle strength, but had little effect on muscle mass (20, 21). According to these data, muscle strength might be more sensitive to reflect the change in muscle function than muscle mass.
The change of muscle composition, the loss of muscle mass and the infiltration of fat into muscle, was a main indicator for muscle quality evaluation and a cause of muscle function decline (22, 23). Here, the age-related change in fat mass showed a difference between the two sexes. In men, the dominant upper limb had little fat mass than the non-dominant side in young age, and the fat mass of both upper limbs increased after 50 years old. Contrary to men, the dominant upper limb had more fat mass than the non-dominant side from young to old in women. This sex difference might have been caused by hormone effect. The decrease of testosterone, which is a potent anabolic factor promoting muscle protein synthesis and muscular regeneration, may induce muscle composition changed (24).
Bone loss is a major risk for fall-related injury in older adults. Interestingly, the dominant upper limb had more bone area and bone mineral content than the non-dominant upper limb. Bone mineral density is a common indicator for bone health assessment, which is calculated by dividing bone mineral content by bone area. Previous studies had proved that high-intensity physical activity is an effective contributor to bone mineral density (25). Inconsistent with this, the bone mineral density of two upper limbs was similar in this study. These results suggested that daily activities might promote large bone area development in adolescent and maintained it into old age, but were not enough to increase bone mineral density.
This was the first study to use the difference in daily activities between the two upper limbs to determine the relationship among muscle performance, physical activity, and aging. In daily living, the dominant upper limb always completes more daily activities than the non-dominant side. Does this kind of physical activity slow the age-related decrease in muscle function? Our data showed that daily activities can promote high muscle function reserve, but cannot prevent muscle function decline with aging. In addition, the interaction of person and environment has been a focus of attention. Environmental factors, such as living arrangements, financial status, and electronics, may influence the lifestyle of older adults and have potential confounding impacts on muscle performance (26, 27). In this study, data on the amounts of physical activity and other influence factors were not investigated, thus more detailed analysis was missing. Further study may focus on the quantitative analysis between physical activity and muscle function maintenance during the aging process.
Muscle strength, lean mass, fat mass, bone area and bone mineral content were obviously different between the two upper limbs, and showed different aging patterns (Figure 3). In older adults, despite more regular use, the dominant hand’s muscle and bone quality was not protected against ageing. Additional exercise should be recommended for older adults to delay motor function decline and promote healthy aging. Comparison of the age-related trends of muscle performance indicators, fat mass increased earliest in men, and muscle strength declined first in women. The detection of muscle strength and fat mass may be useful for early recognition and intervention of motor function decline. Overall, as compared with the performance of the non-dominant upper limb, the dominant upper limb showed better muscle performance and bone quality from young to old. The long-term beneficial effect of daily activities on muscle and bone health was verified. Engaging in more physical activities at a younger age should be recommended to maintain independent living ability and decrease the occurrence of sarcopenia and falls later in life.
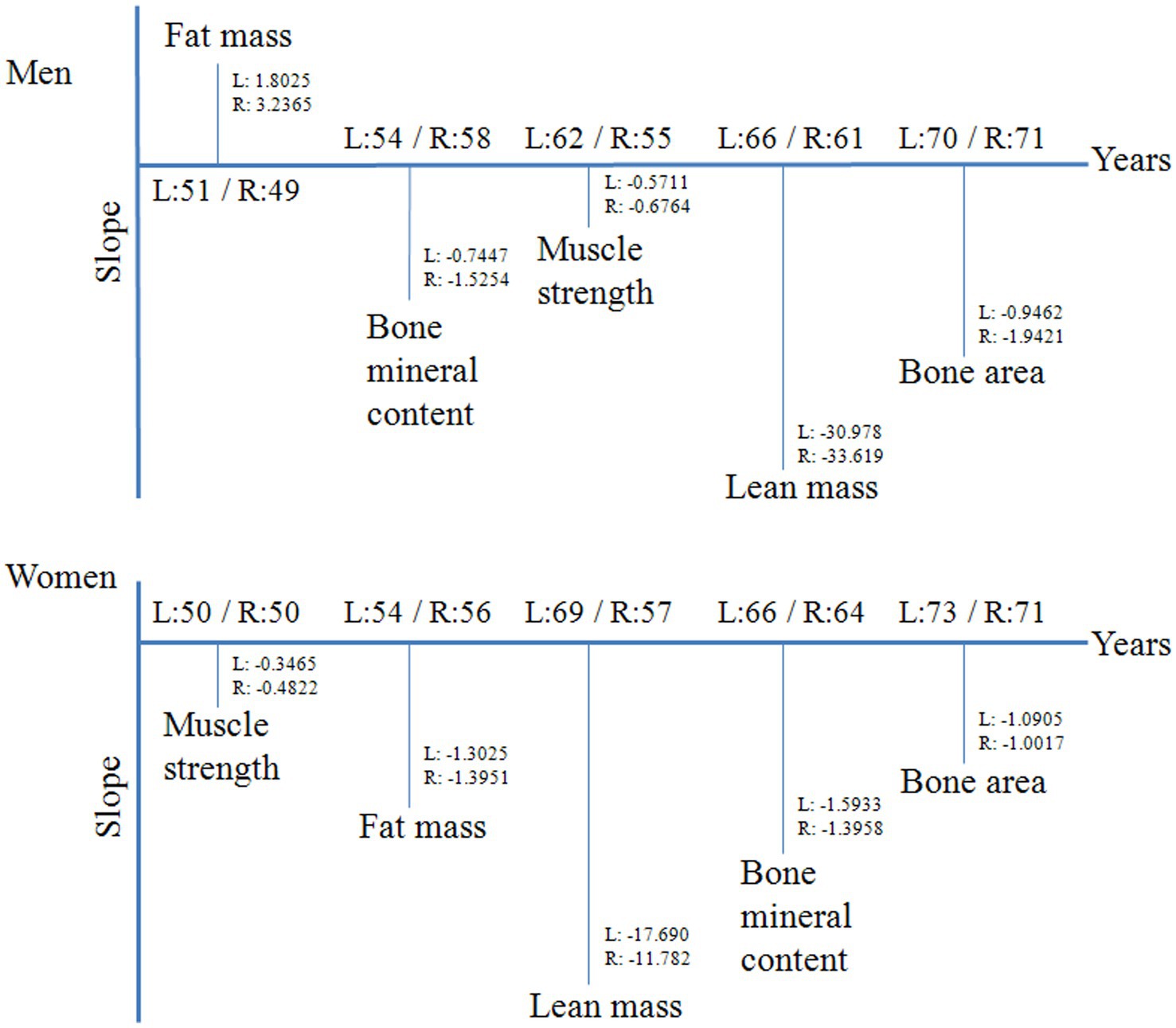
Figure 3. The key points of muscle performance indicators changed with age. The horizontal line marked the age of each indicator changed significantly. The vertical line marked the slope of each indicator changed after the cutoff point. L: the non-dominant upper limb; R: the dominant upper limb.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving humans were approved by the Ethics Committee of Beijing Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
JP: Funding acquisition, Investigation, Project administration, Writing – original draft, Writing – review & editing. FT: Data curation, Writing – original draft. YH: Investigation, Writing – original draft. EZ: Investigation, Writing – original draft. YZ: Investigation, Writing – original draft. TZ: Funding acquisition, Project administration, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by National Key R&D Program of China (2021YFE0111800), the National Natural Science Foundation of China (No. 81970745), and the Research Special Fund for Public Welfare Industry of Health (No. 201302008). All sources of funding received for the research being submitted.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Cruz-Jentoft, AJ, Baeyens, JP, Bauer, JM, Boirie, Y, Cederholm, T, Landi, F, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European working group on sarcopenia in older people. Age Ageing. (2010) 39:412–23. doi: 10.1093/ageing/afq034
2. Cruz-Jentoft, AJ, Bahat, G, Bauer, J, Boirie, Y, Bruyère, O, Cederholm, T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. (2019) 48:16–31. doi: 10.1093/ageing/afy169
3. Francis, P, Lyons, M, Piasecki, M, Mc Phee, J, Hind, K, and Jakeman, P. Measurement of muscle health in aging. Biogerontology. (2017) 18:901–11. doi: 10.1007/s10522-017-9697-5
4. Taekema, DG, Gussekloo, J, Maier, AB, Westendorp, RGJ, and de Craen, AJM. Handgrip strength as a predictor of functional, psychological and social health. A prospective population-based study among the oldest old. Age Ageing. (2010) 39:331–7. doi: 10.1093/ageing/afq022
5. Nguyen, NTT, Nguyen, TX, Nguyen, AT, Nguyen, TTH, Nguyen, TN, Nguyen, HTT, et al. A description of handgrip strength in the very older adult people living in rural Vietnam and its associatin with daily functions. Biomed Res Int. (2021) 2021:1–6. doi: 10.1155/2021/1237547
6. Chen, LK, Woo, J, Assantachai, P, Auyeung, T, Chou, M, Iijima, K, et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. (2020) 21:300–307.e2. doi: 10.1016/j.jamda.2019.12.012
7. Rantanen, T, Guralnik, JM, Foley, D, Masaki, K, Leveille, S, Gurb, JD, et al. Midlife hand grip strength as a predictor of old age disability. JAMA. (1999) 281:558–60. doi: 10.1001/jama.281.6.558
8. Giampaoli, S, Ferrucci, L, Cecchi, F, Lo Noce, C, Poce, A, Dima, F, et al. Hand-grip strength predicts incident disability in non-disabled older men. Age Ageing. (1999) 28:283–8. doi: 10.1093/ageing/28.3.283
9. Hiraoka, A, Tamura, R, Oka, M, Izumoto, H, Ueki, H, Tsuruta, M, et al. Prediction of risk of falls based on handgrip strength in chronic liver disease patients living independently. Hepatol Res. (2019) 49:823–9. doi: 10.1111/hepr.13322
10. Neri, S, Lima, R, Ribeiro, H, and Vainshelboim, B. Poor handgrip strength determined clinically is associated with falls in older women. J Frailty Sarcopenia Falls. (2021) 6:43–9. doi: 10.22540/JFSF-06-043
11. Pham, T, McNeil, JJ, Barker, AL, Orchard, SG, Newman, AB, Robb, C, et al. Longitudinal association between handgrip strength, gait speed and risk of serious falls in a community-dwelling older population. PLoS One. (2023) 18:e0285530. doi: 10.1371/journal.pone.0285530
12. Ingram, LA, Butler, AA, Walsh, LD, Brodie, MA, Lord, SR, and Gandevia, SC. The upper limb physiological profile assessment: description, reliability, normative values and criterion validity. PLoS One. (2019) 14:e0218553. doi: 10.1371/journal.pone.0218553
13. Bohannon, RW. Muscle strength: clinical and prognostic value of hand-grip dynamometry. Curr Opin Clin Nutr Metab Care. (2015) 18:465–70. doi: 10.1097/MCO.0000000000000202
14. Chen, C, McGee, CW, Rich, TL, Prudente, CN, and Gillick, BT. Reference values of intrinsic muscle strength of the hand of adolescents and young adults. J Hand Ther. (2018) 31:348–56. doi: 10.1016/j.jht.2017.05.012
15. Tieland, M, Trouwborst, I, and Clark, BC. Skeletal muscle performance and ageing. J Cachexia Sarcopenia Muscle. (2018) 9:3–19. doi: 10.1002/jcsm.12238
16. Muggeo, VMR. Estimating regression models with unknown break-points. Stat Med. (2003) 22:3055–71. doi: 10.1002/sim.1545
17. Zhou, J, Deng, Y, Shen, L, Wen, C, Yan, Q, Ning, D, et al. Temperature mediates continental-scale diversity of microbes in forest soils. Nat Commun. (2016) 7:12083. doi: 10.1038/ncomms12083
18. Abe, T, Thiebaud, RS, and Loenneke, JP. Age-related change in handgrip strength in men and women: is muscle quality a contributing factor? Age (Dordr). (2016) 38:28. doi: 10.1007/s11357-016-9891-4
19. Lauretani, F, Russo, CR, Bandinelli, S, Bartali, B, Cavazzini, C, DiIorio, A, et al. Age-associated changes in skeletall muscle and their effect on mobility: an operational diagnosis of sarcopenia. J Appl Physiol. (2003) 95:1851–60. doi: 10.1152/japplphysiol.00246.2003
20. Haider, S, Dorner, TE, Luger, E, Kapan, A, Titze, S, Lackinger, C, et al. Impact of a home-based physical and nutritional intervention program conducted by lay-volunteers on handgrip strength in prefrail and frail older adults: a randomized control trial. PLoS One. (2017) 12:e169613. doi: 10.1371/journal.pone.0169613
21. Tieland, M, Dirks, ML, van der Zwaluw, N, Verdijk, LB, van de Rest, O, de Groot, LC, et al. Protein supplementation increases muscle mass gain during prolonged resistance type exercise training in frail elderly people: a randomized, double-blind, placebo-controlled trial. J Am Med Dir Assoc. (2012) 13:713–9. doi: 10.1016/j.jamda.2012.05.020
22. Reinders, I, Murphy, RA, Brouwer, IA, Visser, M, Launer, L, Siggeirsdottir, K, et al. Muscle quality and myosteatosis: novel associations with mortality risk: the age, gene/environment susceptibility (AGES)-Reykjavik study. Am J Epidemiol. (2016) 183:53–60. doi: 10.1093/aje/kwv153
23. Heymsfield, SB, Gonzalez, MC, Lu, J, Jia, G, and Zheng, J. Skeletal muscle mass and quality: evolution of modern measurement concepts in the context of sarcopenia. Proc Nutr Soc. (2015) 74:355–66. doi: 10.1017/S0029665115000129
24. Anderson, LJ, Liu, H, and Garcia, JM. Sex differences in muscle wasting. Adv Exp Med Biol. (2017) 1043:153–97. doi: 10.1007/978-3-319-70178-3_9
25. Troy, KL, Mancuso, ME, Butler, TA, and Johnson, JE. Exercise early and often: effects of physical activity and exercise on women’s bone health. Int J Environ Res Public Health. (2018) 15:878. doi: 10.3390/ijerph15050878
26. Lien, WC, Guo, NW, Chang, JH, Lin, YC, and Kuan, TS. Relationship of perceived environmental barriers and disability in community-dwelling elderly in Taiwan—a population-based study. BMC Geriatr. (2014) 14:59. doi: 10.1186/1471-2318-14-59
27. Poppe, L, Bourdeaudhuij, ID, Verloigne, M, Shadid, S, Cauwenberg, JV, Compernolle, S, et al. Efficacy of a self-regulation-based electronic and mobile health intervention targeting an active lifestyle in adults having type 2 diabetes and in adults aged 50 years or older: two randomized controlled trials. J Med Internet Res. (2019) 21:e13363. doi: 10.2196/13363
Keywords: upper limbs, muscle strength, lean mass, fat mass, bone mineral content
Citation: Pang J, Tu F, Han Y, Zhang E, Zhang Y and Zhang T (2023) Age-related change in muscle strength, muscle mass, and fat mass between the dominant and non-dominant upper limbs. Front. Public Health. 11:1284959. doi: 10.3389/fpubh.2023.1284959
Edited by:
Miriam Rodriguez-Monforte, Ramon Llull University, SpainReviewed by:
Wei-Chih Lien, National Cheng Kung University, TaiwanCopyright © 2023 Pang, Tu, Han, Zhang, Zhang and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jing Pang, cGFuZ2ppbmczMTRAMTYzLmNvbQ==; Tiemei Zhang, dG16aGFuZzEyNkAxMjYuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.