 Ying Wang
Ying Wang Xue Wang1,2,3†
Xue Wang1,2,3† Buxin Han
Buxin Han Tianyong Chen
Tianyong Chen
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 27 November 2023
Sec. Aging and Public Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1280952
This article is part of the Research Topic Understanding and promoting factors which affect healthy ageing: Physical Activity, Sleep Patterns and nutritional habits View all 25 articles
Objectives: Older adults become more inactive and frailer with aging. Physical status is closely linked to mental health, but it is unclear which physical indicator is more strongly associated with depressive symptoms in older adults. The present study aimed to compare relationships between self-reported physical activity, physical frailty (muscle mass, muscle strength, and gait ability) and depressive symptoms in community male and female older adults.
Methods: A total of 1,180 adults aged 60 years and older were recruited to participate in this study from a Chinese community receiving annual check-up service from September 2018 to May 2019. Physical activity was assessed by the International Physical Activity Questionnaire (IPAQ). The Bio-electrical Impedance Analyzer was used to determine the muscle mass. As the indicators of muscle function, grip strength and gait ability were assessed by the dynamometer and Timed Up and Go Test (TUGT), respectively. The 15-item version of Geriatric Depression Scale (GDS-15) was used to examine depressive symptoms. Demographic variables, health status and sleep quality were collected using questionnaire.
Results: 11.8% men and 11.9% women reported depressive symptoms. Logistic regression showed that depressive symptoms was associated with low grip strength (OR = 2.42, 95% CI: 1.04–5.63), slow gait ability (OR = 3.60, 95% CI: 1.28–10.13) in older males, and associated with low level of self-reported physical activity (OR = 3.85, 95% CI: 2.00–7.42) in older females. No significant association was found between muscle mass and depressive symptoms.
Conclusion: There were gender differences in the relationship between physical activity, physical frailty, and depressive symptoms. Grip strength and gait ability may be a better indicator of frailty for predicting depressive symptoms in older men while physical activity may be useful in predicting depressive symptoms in older women.
It is well established that the health of body and mind are inextricably linked (1, 2). Older adults become more inactive and frailer with aging, and their psychological problems become more prominent (3). Previous studies have explored the relationship between physical status and depressive symptoms in older adults, while there are still some disagreements in the results using different indicators.
Mental health benefits conferred by physical activity are wildly recognized (4). In cross-sectional studies, researchers have found that insufficient physical activity predispose older adults to depressive symptoms and vice versa (5, 6). Longitudinal study also provided increasing clarity on the benefits of physical activity, showed that the odds of incident depression were 23% lower by meeting physical activity guidelines (7). Only a few previous studies failed to find the benefits of physical activity, and this may come from improper evaluation tools which easily exaggerate the amount of exercise (8). However, based on the gender differences in biological structure and function and in physical activity preference and attraction across the lifetime, some scholars began to pay attention to the gender difference in health benefits derived from physical activity (9). For example, it was found that the reduction of vigorous physical activity was associated with increased odds for depressive symptoms and higher level of recreational physical activity was associated with less depressive symptoms among older females, while there was no such correlation in men (10, 11).
More and more studies have linked physical frailty to higher risk of depressive symptoms in older adults (12, 13) as well, while associations between frailty using different indicators (such as muscle strength, gait ability and muscle mass) and depressive symptoms remain inconsistent. Brooks and colleagues found that grip strength was negatively associated with depressive symptoms among older adults in the American community (14). A study of six low-and-middle-income countries also suggested that adults over 50-year-old with lower grip strength suffer a higher prevalence of depressive symptoms (15). Both cross-sectional and longitudinal studies support this relationship in Japan (16). In Norway, it was found that older adults with lower gait ability suffered more depressive symptoms (17). In brief, majority of the literature support relationships between grip strength, gait ability and depressive symptoms, where grip strength and gait ability represent upper and lower physical capacity respectively. However, inconsistencies between studies raise concerns about whether there is a correlation between muscle mass and depressive symptoms. Wu et al. (18) found that both muscle mass and muscle strength were negatively correlated with depressive symptoms, the result of a national Korean study suggested no correlation between muscle mass and depressive symptoms in any age group (19). Moreover, there are great differences in muscle strength and muscle mass between men and women. The physiological difference may lead to a gender difference between frailty and depressive symptoms (20). Therefore, the predictive effect of physical activity and physical frailty on depressive symptoms in the older adults of different gender remains to be examined further.
In summary, the objectives of the present study were to: (i) investigate the association between physical activity, different indicators of frailty (muscle strength, gait ability and muscle mass) and geriatric depressive symptoms; and (ii) explore the possible gender differences in these relationships.
The participants in this study were community-dwelling older adults age 60 years or more. Between September 2018 and May 2019, a total of 1,180 sixty-year-olds were recruited from the community older adults receiving annual check-up service voluntarily at the Community Healthcare Center of Nanyingmen street, Heping District, Tianjin. Because blood samples were collected, the participants were instructed not to eat or drink anything before the examination. Exclusion criteria for participation included a history of major depression, unable to communicate, unable to complete grip strength or walking test (e.g., severe arthritis or surgery). A total of 1,180 older adults have participated in this study. Since there were 55 men and 80 women who did not have the body composition test, we interpolated the missing value using mean values of different genders and different age stages of the appendicular skeletal muscle mass. The study was approved by the Ethics Committee of the Institute of Psychology of the Chinese Academy of Sciences (IPCAS). All participants signed an informed consent.
The 15-item version of Geriatric Depression Scale (GDS-15) was administered to all participants (21). A validation study by Boey (22) supported the use of GDS-15 as a reliable measurement utilized among older adults in urban China. All items in the GDS-15 are rated by self-report and scores are summed, resulting in a possible total score of 0–15. We defined depressive symptoms as a score of 5 or more (23).
Physical activity was assessed using the Chinese version of International Physical Activity Questionnaire (IPAQ), a self-report instrument that assesses physical activity during the past seven days (24). A total physical activity score was calculated as the metabolic equivalent of energy per week (MET/week). MET per week for each participant were calculated as follows: Total activity (MET/ week) = (3.3 × walking minutes per day × walking days) + (4.0 × moderate activity minutes per day × moderate activity days) + (8.0 × vigorous activity minutes per day × vigorous activity days). There were high reliability and validity in IPAQ for Chinese population (25). A total score below 600 MET-min/w was coded as “low level of physical activity,” 600 to 3000 MET-min/w was coded as “moderate level of physical activity,” and above 3000 MET-min/w was coded as “high level of physical activity” (26).
Physical frailty was indicated by muscle strength, muscle mass and gait ability. Muscle strength of the dominant hand was performed with a hand-held dynamo-meter (GRIP-D; Takei, Niigata, Japan), since grip strength is closely related to total body strength and widely used to evaluate the muscle strength in older participants (27). The highest value from 3 trials in a standing position was used in the analysis.
The calculation of the muscle mass index was performed by dividing the appendicular skeletal muscle mass (ASM) by the body weight (ASM/ wt), differences related to height, sex, age and race were eliminated when using body weight as the denominator (28). The Bio-electrical Impedance Analyzer (INBody 720; Biospace Co., Ltd, Seoul, Korea) was used to determine the ASM, while participants standing on 2 metallic electrodes and held metallic grip electrodes. Muscle strength and muscle mass have been distributed according to quartile and conducted a sex-stratified analysis for the large gender gap.
Measurement of gait ability was performed by the Time Up and Go Test (TUGT) (29). It measures the time taken by a 6-meter walk, which requires participants to rise from a standard chair (with the height of 45 cm), walk three meters, turn around, walk back to the chair, and sit down without any device throughout.
Demographic information (marital status, sex, age and education), health (obesity and disease history) and sleep quality were assessed using questionnaire items. Body mass index (BMI), calculated as weight (kg)/height squared (m2), was used to indicate obesity (BMI ≥ 28: obesity = 1; BMI < 28: obesity = 0) (30). Sleep quality was assessed by one item and coded as 3 levels (1–3 were good, fair and poor).
All analyses were conducted using SPSS V.24.0, stratified by gender. Frequencies and percentages were computed for each demographic characteristic. Bivariate analyses with Chi-square test were used to explore the relevance of demographic variables, physical activity, physical frailty to depressive symptoms.
After adjusting for age, marital status, education, disease, sleep quality and obesity, logistic regression analysis was used to test relationships between indicators of physical status and depressive symptoms. Grip strength, gait ability, muscle mass and physical activity was added in model 1, model 2, model 3, and model 4, respectively. Afterwards, we added indicators of physical activity and physical frailty to the same model to test the independent association between each variable and depressive symptoms.
The characteristics and demographics of the participants are shown in Table 1. The analysis include data from 1,180 older adults, of whom 533 were men (mean age: 68.07 ± 6.47) and 647 were women (mean age: 66.52 ± 5.19). In addition, it is consistent with the basic situation of old adults in China that women have lower levels of education, higher rates of widowhood and obesity. Of all the participants, 11.9% were classified as being depressive symptoms. The proportions of depressive symptoms in men and women were 11.8 and 11.9% respectively, with no significant difference (χ2 = 0.01, P = 0.966).
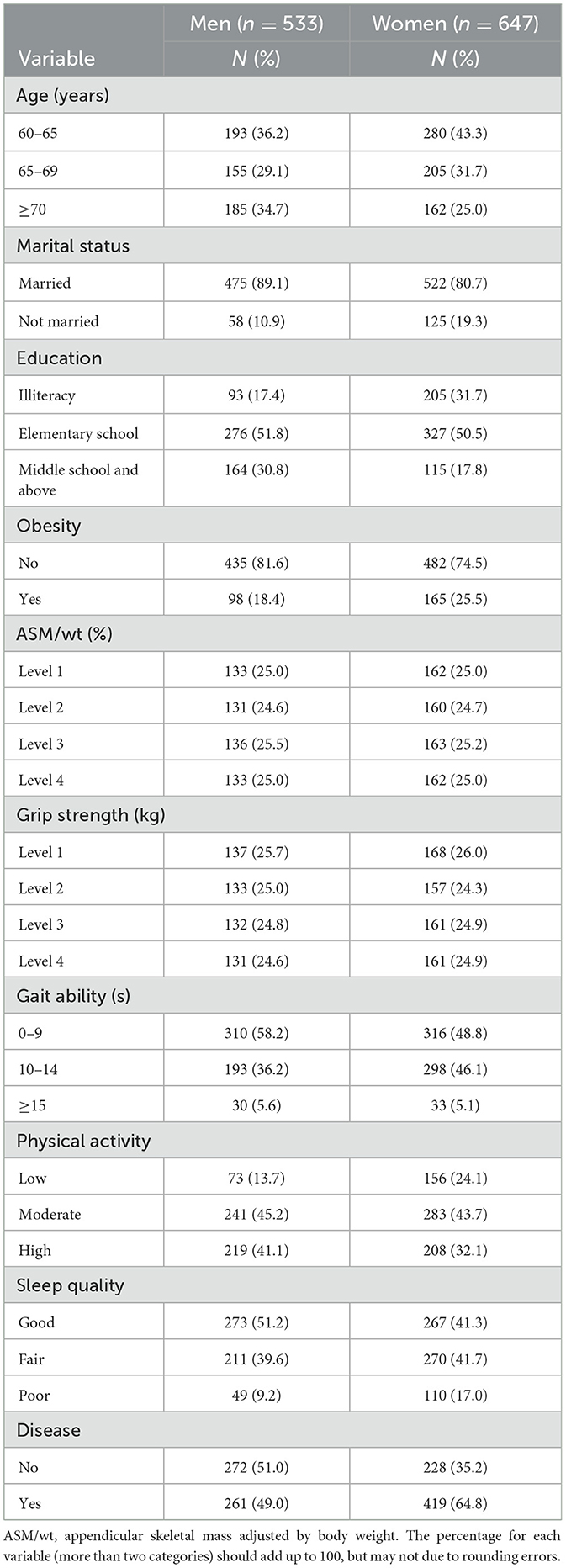
Table 1. Characteristics of the study population.
Chi-square tests were conducted to analysis associations between depressive symptoms and other variables. As shown in Table 2, a significant higher prevalence of depressive symptoms was observed in men with old age, no spouse, low grip strength, low gait ability and poor sleep quality (P < 0.05) and in women with old age, disease history, low grip strength, low physical activity and no spouse (P < 0.05).
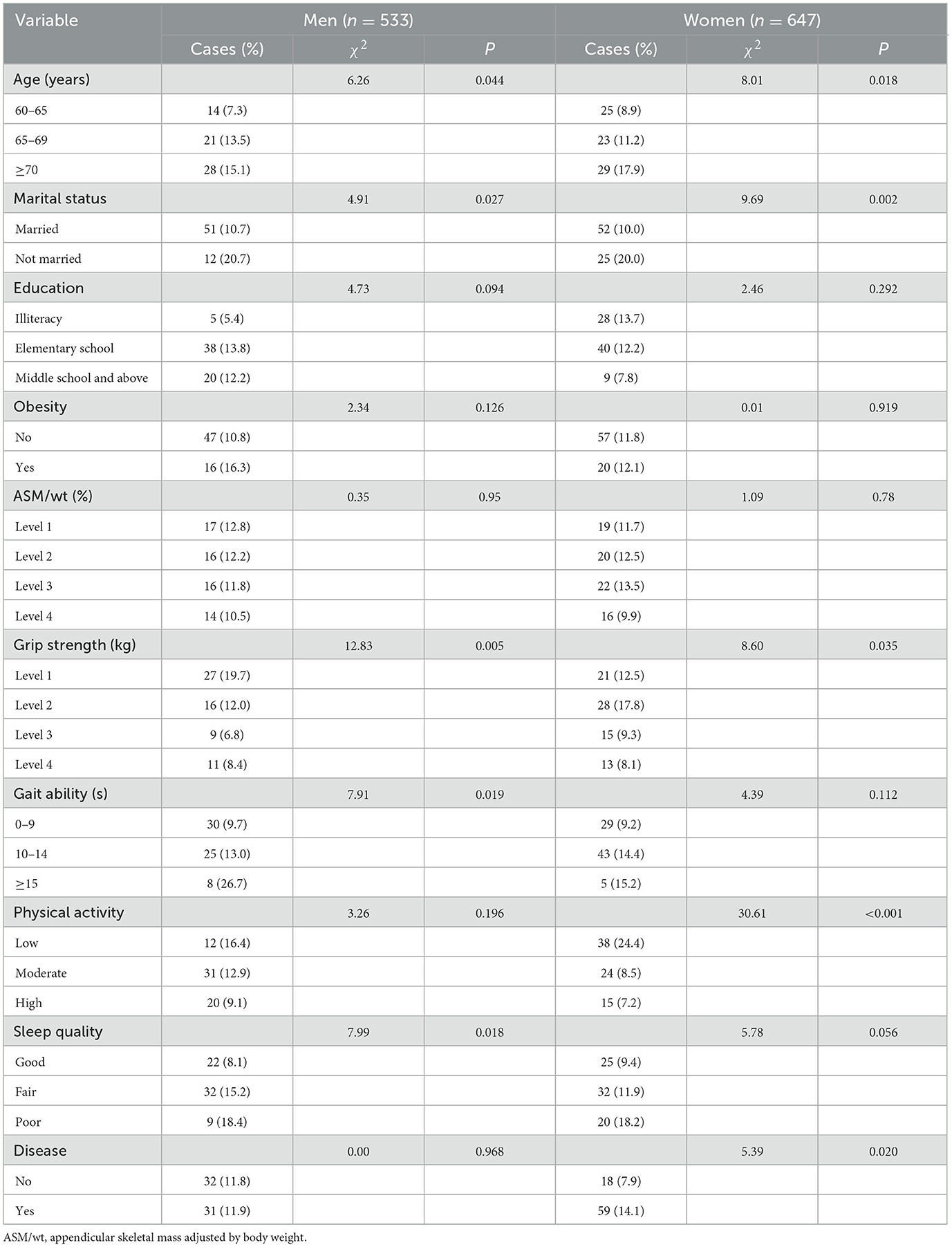
Table 2. Bivariate analyses of association between depressive symptoms and related factors.
ORs from the logistic regression model for depressive symptoms according to physical frailty and physical activity are shown in Tables 3, 4. Results showed that some indicators of physical frailty rather than physical activity have been linked to depressive symptoms in older males. Male participants with lower grip strength (OR = 2.42, 95% CI: 1.04–5.63) and lower gait ability (OR = 3.6, 95% CI: 1.28–10.13) had significant higher OR for depressive symptoms, but the role of muscle mass remains unclear. In addition, obesity and poor sleep quality were found to be a risk factor of depressive symptoms from all four models (Model 1: OR = 2.27, 95% CI: 1.14–4.51, P = 0.020; Model 1: OR = 3.53, 95% CI: 1.44–8.68, P = 0.006).
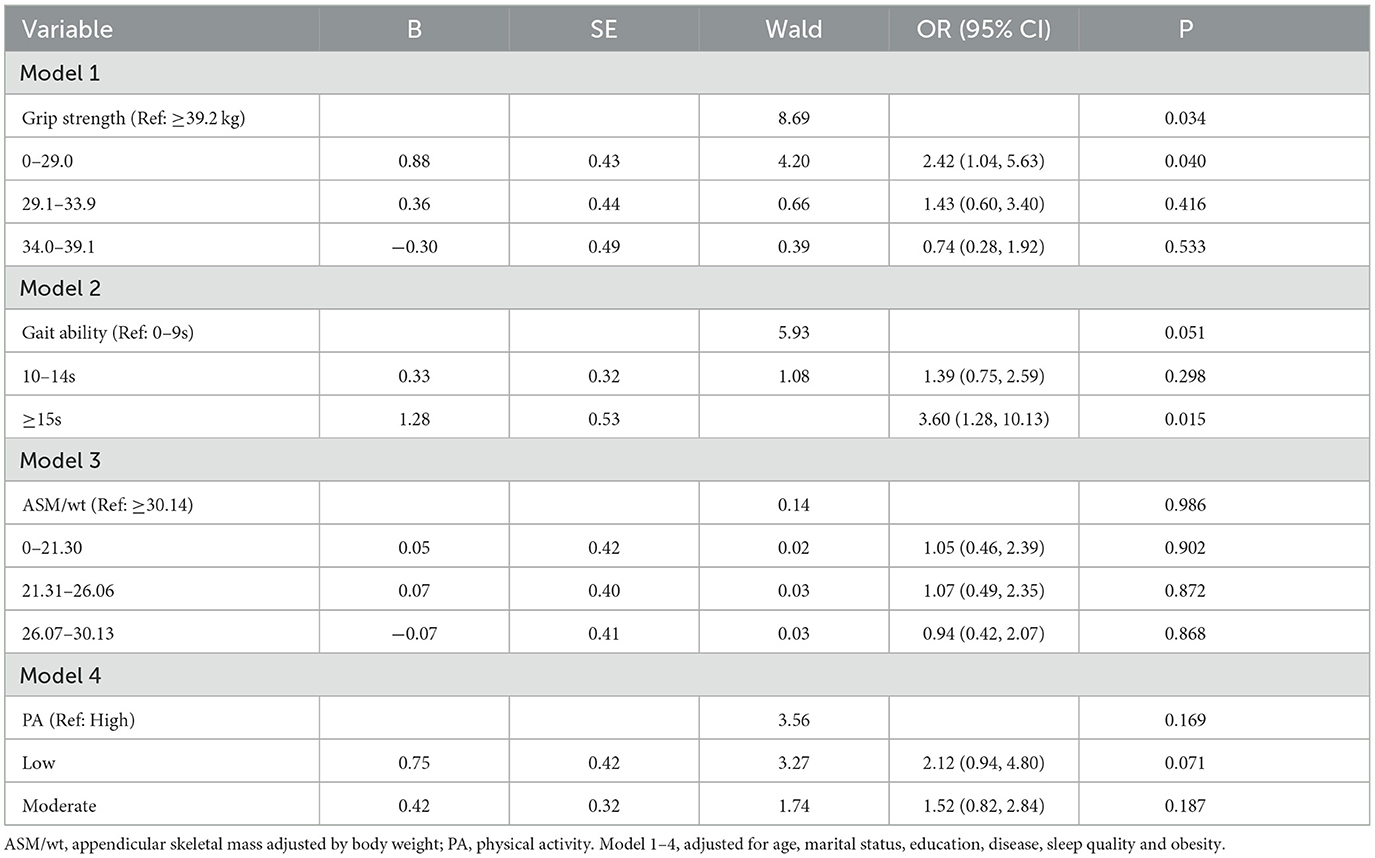
Table 3. Logistic regressions of physical activity, frailty on depressive symptoms in men.
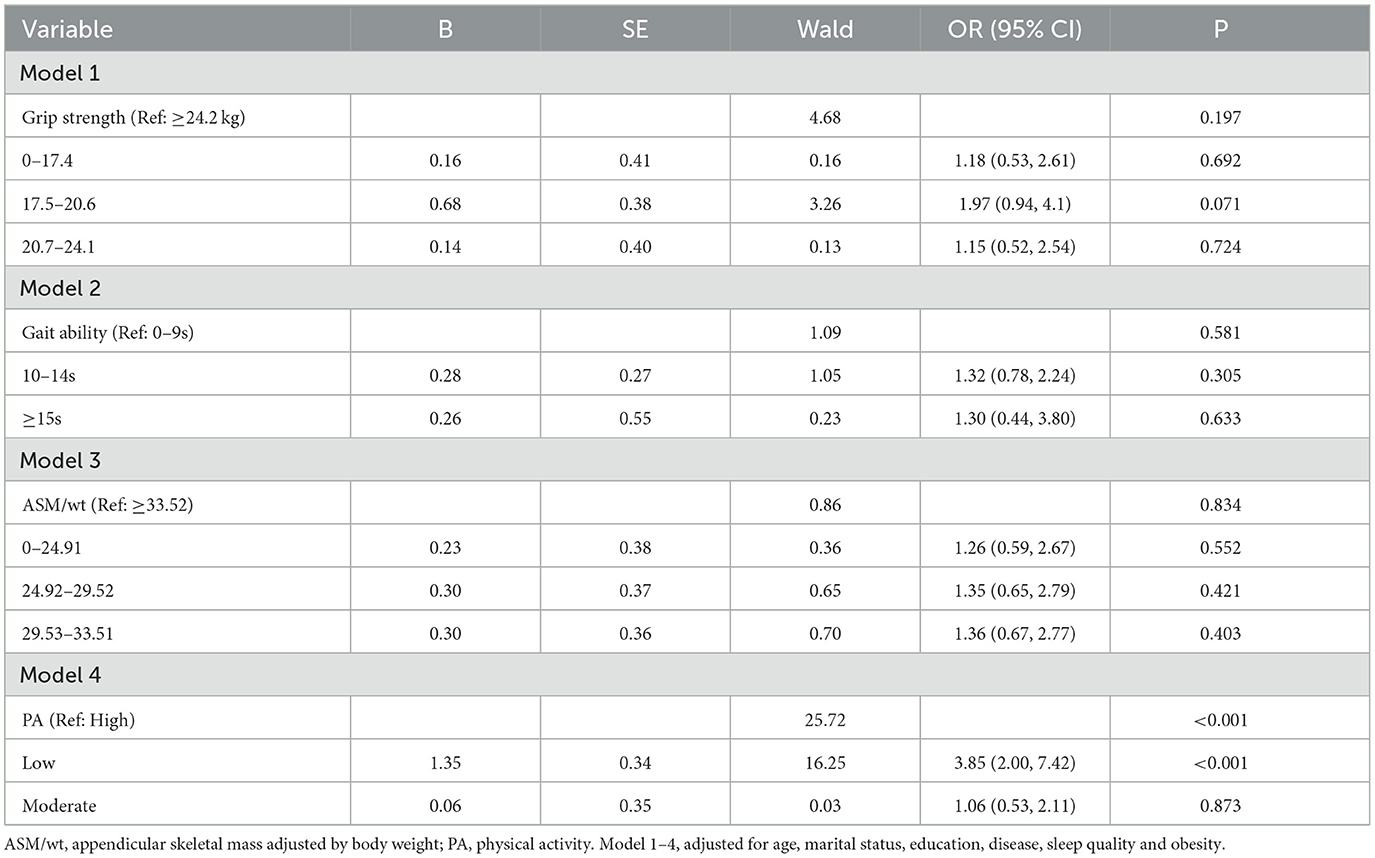
Table 4. Logistic regressions of physical activity, frailty on depressive symptoms in women.
For women group, no significant associations were found between muscle strength, muscle mass, gait ability and depressive symptoms. However, older females with low level of physical activity (<600 MET-min/w) were 3.85 times more likely to be depressed than that with high level of physical activity (more than 3000 MET-min/w). These effects still exist when we add physical activity and physical frailty in one model.
This is a community-based cross-sectional study aimed to explore the relationship between physical activity, physical frailty and geriatric depressive symptoms. The major findings are that lower amount of physical activity is significantly associated with depressive symptoms for older females, and depressive symptoms in the older males was associated with lower grip strength and lower gait ability.
The benefit of physical activity on health is widely recognized. Previous studies have shown that physical activity in later life can extend lifespan and reduce the risk of disability (31). Our results are in line with those studies advocating that physical activity is a protective factor against depressive symptoms in older participants (32, 33). Neuromolecular mechanisims that physical activity and antidepressants shared have been proposed in the past decade, including neurotrophic factor expression (34, 35), HPA axis response (36–38), anti-inflammatory effects (39, 40).
However, this effect was only observed in female participants in this study. Although previous researchers may not pay enough attention to gender differences, several studies analyzed by gender stratification showed similar results (10, 11, 41–43). An earlier study from Nepal, by contrast, only found this effect in men. Nevertheless, the effect was modest and researchers only used simple questions to assess the frequency of activity, which may undermine the credibility (44). The gender difference may partly be explained by psychological mechanisms of physical activity on depressive symptoms, such as increasing self-esteem, self-efficacy, and social support (45–48). It was found that physical activity with social attributes help alleviate depressive symptoms (49), while physical activity related to work, transport or domestic activity was not associated with depressive symptoms (50). From this perspective, women have stronger social connections than men and may be able to amplify the benefits of physical activity (51). On the other hand, the brain benefits from exercise also differ between men and women, with studies showing that daily walking improves hippocampal volume in women, but not in men (52). Due to the close connection between depressive symptoms and hippocampus (53), this may also be a potential physiological mechanism for gender differences.
The association between physical frailty and depressive symptoms is consistent with the observations of Ji et al. (54) and Liu et al. (55), showed that older persons with frailty are tend to have depressive symptoms. Muscle is closely associated with physical frailty, which is also a secretory organ (56) and contributes benefits on mental health via secretion of numerous myokines (57) and neurotrophic factor (58). Decline of muscle mitochondrial function is associated with depression as well (59). Malnutrition (60), hormonal imbalances (61), cardiovascular disease and inflammation (62) may also play a role in this relationship.
Maintaining muscle mass, improving muscle strength and physical function are important for preventing frailty (63, 64). However, not every indicator was associated with depressive symptoms in this study, and there were gender differences in the results. Previous studies exploring the relationship between muscle mass and depressive symptoms have yielded inconsistent results. Two studies reported associations between muscle mass and depressive symptoms, with one of them only found this relationship in male participants (18, 65). Unlike these two, the present study did not show significant association between them, which is consistent with a national Korean study (19). Unlike muscle mass, the predictive effects of muscle strength and gait ability on depressive symptoms were consistent with previous studies (66–68). On the one hand, the degree of physical frailty among community older adults in the present study may not be sufficient to trigger higher rate of depressive symptoms or more severe depressive symptoms, which may weaken the relationship of body and mind. On the other hand, it is possible that muscle function, rather than muscle mass, may be more closely related to health outcomes. For example, Chen et al. (69) found that it may be muscle function rather than muscle mass contribute to depression development via malnutrition. Arts et al. (70) also suggested that only performance-based physical frailty (encompassing gait ability and handgrip strength) was associated with higher levels of inflammatory markers and hence depression. Similarly, Newman et al. (71) clarified that low grip strength rather than muscle mass is associated with total mortality rates in late life.
As to the gender difference, these results are contrary to a recent study among rural older South Africans (72), but similar to a meta-analysis that found grip strength was associated with a reduced risk of depressive symptoms in male but not in female (73). The possible reason for gender difference may be related to the loss of skeletal muscle strength, with male muscle strength decreases earlier and faster than female (74, 75). Future research is needed to explore this issue.
This study explored the associations between physical activity, physical frailty and depressive symptoms in older adults, and provided support for the relationship of body and mind. The pathophysiology pathway between physical status and depressive symptoms is worth exploring because of the gender differences. Future studies on the relationship between body and mind may consider the two variables and pay attention to the possible gender differences. Furthermore, they can be used as supplementary indicators to identify the risk of depression in older persons, and also as a potential target for intervention. It is hoped that this study will contribute to a deeper understanding for the prevention and early detection of depression.
This study has some strengths. First, we collected data through an annual physical check-up, with large number of participants and good representativeness. Second, to the best of our knowledge, this is the first study to focus on different indicators of physical frailty and depressive symptoms from a gender perspective, which has helped us further understand the relationship between body and mind.
This study also has some limitations. First, this is a cross-sectional study, which is not sufficient to establish a causal relationship between physical activity, physical frailty and depressive symptoms. Longitudinal studies can be carried out in the future. Second, this study used a self-reported questionnaire to assess the physical activity of old adults in the past week. It is possible that a few participants were less involved than usual in the previous 7 days due to injury or other reasons, leading to a potential bias. Third, since this study is based on an annual physical check-up, we were not able to use objective measurements such as pedometers, which may reflect the physical activity of older adults more accurately.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Ethics Committee of the Institute of Psychology of the Chinese Academy of Sciences (IPCAS). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements.
YW: Validation, Writing – original draft, Writing – review & editing. XW: Data curation, Investigation, Methodology, Writing – original draft. XZ: Writing – review & editing, Writing – original draft. YS: Writing – review & editing. BH: Project administration, Supervision, Writing – review & editing. TC: Project administration, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the National Key Research and Development Program of China (2020YFC2003000) and the Scientific Foundation of Institute of Psychology, Chinese Academy of Sciences (E2CX3715CX).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Renoir T, Hasebe K, Gray L. Mind and body: how the health of the body impacts on neuropsychiatry. Front Pharmacol. (2013) 4:158. doi: 10.3389/fphar.2013.00158
2. Kong D, Solomon P, Dong XQ. Depressive symptoms and onset of functional disability over 2 years: a prospective cohort study. J Am Geriatr Soc. (2019) 67:S538–44. doi: 10.1111/jgs.15801
3. Mechling H, Netz Y. Aging and inactivity—capitalizing on the protective effect of planned physical activity in old age. Eur Rev Aging Phys Activity. (2009) 6:89–97. doi: 10.1007/s11556-009-0052-y
4. Pearce M, Garcia L, Abbas A, Strain T, Schuch FB, Golubic R, et al. Association between physical activity and risk of depression: a systematic review and meta-analysis. JAMA psychiatry. (2022) 79:550–9. doi: 10.1001/jamapsychiatry.2022.0609
5. Wołoszyn N, Wiśniowska-Szurlej A, Sozański B. An assessment of the relationship between the level of physical activity and the risk of falls and depression in older adults aged 60-75 years from the Podkarpackie region. Adv Rehab. (2018) 32:41–8. doi: 10.5114/areh.2018.77936
6. Wassink-Vossen S, Collard RM, Voshaar RCO, Comijs HC, de Vocht HM, Naarding P. Physical (in) activity and depression in older people. J Aff Disorders. (2014) 161:65–72. doi: 10.1016/j.jad.2014.03.001
7. McDowell CP, Dishman RK, Hallgren M, MacDonncha C, Herring MP. Associations of physical activity and depression: results from the Irish longitudinal study on ageing. Exp Gerontol. (2018) 112:68–75. doi: 10.1016/j.exger.2018.09.004
8. Cooper-Patrick L, Ford DE, Mead LA, Chang PP, Klag MJ. Exercise and depression in midlife: a prospective study. Am J Public Health. (1997) 87:670–3. doi: 10.2105/AJPH.87.4.670
9. Hands B, Larkin D, Cantell MH, Rose E. Male and female differences in health benefits derived from physical activity: implications for exercise prescription. J Womens Health Issues Care. (2016) 5:238. doi: 10.4172/2325-9795.1000238
10. Carroll DD, Blanck HM, Serdula MK, Brown DR. Obesity, physical activity, and depressive symptoms in a cohort of adults aged 51 to 61. J Aging Health. (2010) 22:384–98. doi: 10.1177/0898264309359421
11. Andrade-Gómez E, Martínez-Gómez D, Rodríguez-Artalejo F, García-Esquinas E. Sedentary behaviors, physical activity, and changes in depression and psychological distress symptoms in older adults. Dep Anxiety. (2018) 35:884–97. doi: 10.1002/da.22804
12. Collard R, Arts M, Schene A, Naarding P, Voshaar RO, Comijs H. The impact of frailty on depressive disorder in later life: findings from the Netherlands study of depression in older persons. Eur Psychiatry. (2017) 43:66–72. doi: 10.1016/j.eurpsy.2017.01.003
13. Chen LJ, Chen CY, Lue BH, Tseng MY, Wu SC. Prevalence and associated factors of frailty among elderly people in Taiwan. Int J Gerontol. (2014) 8:114–9. doi: 10.1016/j.ijge.2013.12.002
14. Brooks JM, Titus AJ, Bruce ML, Orzechowski NM, Mackenzie TA, Bartels SJ, et al. Depression and handgrip strength among US adults aged 60 years and older from NHANES 2011–2014. J Nutr Health Aging. (2018) 22:938–43. doi: 10.1007/s12603-018-1041-5
15. Ashdown-Franks G, Stubbs B, Koyanagi A, Schuch F, Firth J, Veronese N, et al. Handgrip strength and depression among 34,129 adults aged 50 years and older in six low-and middle-income countries. J Affect Disord. (2019) 243:448–54. doi: 10.1016/j.jad.2018.09.036
16. Fukumori N, Yamamoto Y, Takegami M, Yamazaki S, Onishi Y, Sekiguchi M, et al. Association between hand-grip strength and depressive symptoms: Locomotive Syndrome and Health Outcomes in Aizu Cohort Study (LOHAS). Age Ageing. (2015) 44:592–8. doi: 10.1093/ageing/afv013
17. Kyrdalen IL, Thingstad P, Sandvik L, Ormstad H. Associations between gait speed and well-known fall risk factors among community-dwelling older adults. Physiother Res Int. (2019) 24:e1743. doi: 10.1002/pri.1743
18. Wu H, Yu B, Meng G, Liu F, Guo Q, Wang J, et al. Both muscle mass and muscle strength are inversely associated with depressive symptoms in an elderly Chinese population. Int J Geriatr Psychiatry. (2017) 32:769–78. doi: 10.1002/gps.4522
19. Byeon CH, Kang KY, Kang SH, Kim HK, Bae EJ. Sarcopenia is not associated with depression in Korean adults: results from the 2010–2011 Korean national health and nutrition examination survey. Korean J Family Med. (2016) 37:37. doi: 10.4082/kjfm.2016.37.1.37
20. Wang J, Zhou X, Qiu S, Deng L, Li J, Yang L, et al. The Association between grip strength and depression among adults aged 60 years and older: a large-scaled population-based study from the longitudinal aging study in India. Front Aging Neurosci. (2022) 14:937087. doi: 10.3389/fnagi.2022.937087
21. Yesavage JA, Sheikh JI. 9/Geriatric depression scale (GDS) recent evidence and development of a shorter version. Clin Gerontol. (1986) 5:165–73. doi: 10.1300/J018v05n01_09
22. Boey KW. The use of GDS-15 among the older adults in Beijing. Clin Gerontol. (2000) 21:49–60. doi: 10.1300/J018v21n02_05
23. Burke WJ, Roccaforte WH, Wengel SP. The short form of the geriatric depression scale: a comparison with the 30-item form. J Geriatr Psychiatr Neurol. (1991) 4:173. doi: 10.1177/089198879100400310
24. Booth M. Assessment of physical activity: an international perspective. Res Q Exerc Sport. (2000) 71:114–20. doi: 10.1080/02701367.2000.11082794
25. Qu NN, Li KJ. Study on the reliability and validity of international physical activity questionnaire (Chinese Vision, IPAQ). Zhonghua Liu Xing Bing Xue za Zhi. (2004) 25:265–8.
26. Fan M, Lyu J, He P. Chinese guidelines for data processing and analysis concerning the international physical activity questionnaire. Zhonghua Liu Xing Bing Xue za Zhi. (2014) 35:961–4. doi: 10.3760/cma.j.issn.0254-6450.2014.08.019
27. Bohannon RW. Grip strength: an indispensable biomarker for older adults. Clin Interv Aging. (2019) 12:1681–91. doi: 10.2147/CIA.S194543
28. Baumgartner RN, Koehler KM, Gallagher D, Romero L, Heymsfield SB, Ross RR, et al. Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol. (1998) 147:755–63. doi: 10.1093/oxfordjournals.aje.a009520
29. Podsiadlo D, Richardson S. The timed “up & go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. (1991) 39:142–8. doi: 10.1111/j.1532-5415.1991.tb01616.x
30. Zhou B. Predictive values of body mass index and waist circumference to risk factors of related diseases in Chinese adult population. Zhonghua Liu Xing Bing Xue za Zhi. (2002) 23:5–10.
31. Marzetti E, Calvani R, Tosato M, Cesari M, Di Bari M, Cherubini A, et al. Physical activity and exercise as countermeasures to physical frailty and sarcopenia. Aging Clin Exp Res. (2017) 29:35–42. doi: 10.1007/s40520-016-0705-4
32. Kandola A, Ashdown-Franks G, Hendrikse J, Sabiston CM, Stubbs B. Physical activity and depression: towards understanding the antidepressant mechanisms of physical activity. Neurosci Biobehav Rev. (2019) 107:525–39. doi: 10.1016/j.neubiorev.2019.09.040
33. Schuch FB, Vancampfort D, Firth J, Rosenbaum S, Ward PB, Silva ES, et al. Physical activity and incident depression: a meta-analysis of prospective cohort studies. Am J Psychiatry. (2018) 175:631–48. doi: 10.1176/appi.ajp.2018.17111194
34. Castrén E, Rantamäki T. The role of BDNF and its receptors in depression and antidepressant drug action: reactivation of developmental plasticity. Dev Neurobiol. (2010) 70:289–97. doi: 10.1002/dneu.20758
35. Dinoff A, Herrmann N, Swardfager W, Gallagher D, Lanctôt KL. The effect of exercise on resting concentrations of peripheral brain-derived neurotrophic factor (BDNF) in major depressive disorder: a meta-analysis. J Psychiatr Res. (2018) 105:123–31. doi: 10.1016/j.jpsychires.2018.08.021
36. Chrousos GP. Stress and disorders of the stress system. Nat Rev Endocrinol. (2009) 5:374. doi: 10.1038/nrendo.2009.106
37. Fuqua JS, Rogol AD. Neuroendocrine alterations in the exercising human: implications for energy homeostasis. Metabolism. (2013) 62:911–21. doi: 10.1016/j.metabol.2013.01.016
38. Hötting K, Schickert N, Kaiser J, Röder B, Schmidt-Kassow M. The effects of acute physical exercise on memory, peripheral BDNF, and cortisol in young adults. Neural Plast. (2016) 2016:6860573. doi: 10.1155/2016/6860573
39. Eyre HA, Papps E, Baune BT. Treating depression and depression-like behavior with physical activity: an immune perspective. Front Psychiatry. (2013) 4:3. doi: 10.3389/fpsyt.2013.00003
40. Eyre HA, Baune BT. Assessing for unique immunomodulatory and neuroplastic profiles of physical activity subtypes: a focus on psychiatric disorders. Brain Behav Immun. (2014) 39:42–55. doi: 10.1016/j.bbi.2013.10.026
41. Mikkelsen SS, Tolstrup JS, Flachs EM, Mortensen EL, Schnohr P, Flensborg-Madsen T, et al. cohort study of leisure time physical activity and depression. Prev Med. (2010) 51:471–5. doi: 10.1016/j.ypmed.2010.09.008
42. Wang F, DesMeules M, Luo W, Dai S, Lagace C, Morrison H. Leisure-time physical activity and marital status in relation to depression between men and women: a prospective study. Health Psychol. (2011) 30:204. doi: 10.1037/a0022434
43. Zhang J, Yen ST. Physical activity, gender difference, and depressive symptoms. Health Serv Res. (2015) 21:1550–73. doi: 10.1111/1475-6773.12285
44. Gautam R, Saito T, Kai I. Leisure and religious activity participation and mental health: gender analysis of older adults in Nepal. BMC Public Health. (2007) 7:299. doi: 10.1186/1471-2458-7-299
45. Harvey SB, Hotopf M, Øverland S, Mykletun A. Physical activity and common mental disorders. The Br J Psychiatr. (2010) 197:357–64. doi: 10.1192/bjp.bp.109.075176
46. Legrand FD. Effects of exercise on physical self-concept, global self-esteem, and depression in women of low socioeconomic status with elevated depressive symptoms. J Sport Exerc Psychol. (2014) 36:357–65. doi: 10.1123/jsep.2013-0253
47. Ryan MP. The antidepressant effects of physical activity: mediating self-esteem and self-efficacy mechanisms. Psychol Health. (2008) 23:279–307. doi: 10.1080/14768320601185502
48. Wipfli B, Landers D, Nagoshi C, Ringenbach S. An examination of serotonin and psychological variables in the relationship between exercise and mental health. Scand J Med Sci Sports. (2011) 21:474–81. doi: 10.1111/j.1600-0838.2009.01049.x
49. Kleppang AL, Hartz I, Thurston M, Hagquist C. The association between physical activity and symptoms of depression in different contexts - a cross-sectional study of Norwegian adolescents. BMC Pub Health. (2018) 18:1368. doi: 10.1186/s12889-018-6257-0
50. Teychenne M, Ball K, Salmon J. Associations between physical activity and depressive symptoms in women. Int J Behav Nutr Phys Activity. (2008) 5:1–12. doi: 10.1186/1479-5868-5-27
51. Fässberg MM, Van Orden KA, Duberstein P, Erlangsen A, Lapierre S, Bodner E, et al. A systematic review of social factors and suicidal behavior in older adulthood. Int J Environ Res Pub Health. (2012) 9:722–45. doi: 10.3390/ijerph9030722
52. Varma VR, Chuang YF, Harris GC, Tan EJ, Carlson MC. Low-intensity daily walking activity is associated with hippocampal volume in older adults. Hippocampus. (2015) 25:605–15. doi: 10.1002/hipo.22397
53. Zhou H, Li R, Ma Z, Rossi S, Zhu X, Li J. Smaller gray matter volume of hippocampus/parahippocampus in elderly people with subthreshold depression: a cross-sectional study. BMC Psychiatry. (2016) 16:219. doi: 10.1186/s12888-016-0928-0
54. Ji L, Qiao X, Jin Y, Si H, Liu X, Wang C. Age differences in the relationship between frailty and depression among community-dwelling older adults. Geriatr Nursing. (2020) 41:485–9. doi: 10.1016/j.gerinurse.2020.01.021
55. Liu X, Wang C, Qiao X, Si H, Jin Y. Sleep quality, depression and frailty among Chinese community-dwelling older adults. Geriatr Nursing. (2021) 42:714–20. doi: 10.1016/j.gerinurse.2021.02.020
56. Pedersen BK, Febbraio MA. Muscle as an endocrine organ: focus on muscle-derived interleukin-6. Physiol Rev. (2008) 88:1379–406. doi: 10.1152/physrev.90100.2007
57. Giudice J, Taylor JM. Muscle as a paracrine and endocrine organ. Curr Opin Pharmacol. (2017) 34:49–55. doi: 10.1016/j.coph.2017.05.005
58. Pasco JA, Williams LJ, Jacka FN, Stupka N, Brennan-Olsen SL, Holloway KL, et al. Sarcopenia and the common mental disorders: a potential regulatory role of skeletal muscle on brain function? Curr Osteoporos Rep. (2015) 13:351–7. doi: 10.1007/s11914-015-0279-7
59. Brown PJ, Brennan N, Ciarleglio A, Chen C, Garcia CM, Gomez S, et al. Declining skeletal muscle mitochondrial function associated with increased risk of depression in later life. The Am J Geriatr Psychiatry. (2019) 27:963–71. doi: 10.1016/j.jagp.2019.03.022
60. Ulugerger Avci G, Suzan V, Bektan Kanat B, Unal D, Emiroglu Gedik T, Doventas A, et al. Depressive symptoms are associated with sarcopenia and malnutrition in older adults. Psychogeriatrics. (2023) 23:63–70. doi: 10.1111/psyg.12903
61. Li Z, Tong X, Ma Y, Bao T, Yue J. Prevalence of depression in patients with sarcopenia and correlation between the two diseases: systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. (2022) 13:128–44. doi: 10.1002/jcsm.12908
62. Vaughan L, Corbin AL, Goveas JS. Depression and frailty in later life: a systematic review. Clin Interv Aging. (2015) 18:1947–58. doi: 10.2147/CIA.S69632
63. Li M, Shi J, Zou CS, Tan X, Zhou BY, Duan CB, et al. Correlation of frailty severity with muscle mass and physical function in Chinese older adults: preliminary findings. Chin J Geriatr. (2017) 36:1313–7. doi: 10.3760/CMA.J.ISSN.0254-9026.2017.12.009
64. Corral-Pérez J, Ávila-Cabeza-de-Vaca L, González-Mariscal A, Espinar-Toledo M, Ponce-González JG, Casals C, et al. Risk and protective factors for frailty in pre-frail and frail older adults. Int J Environ Res Pub Health. (2023) 20:3123. doi: 10.3390/ijerph20043123
65. Nam Hoon K. Depression is associated with sarcopenia, not central obesity, in elderly korean men. J Am Geriatr Soc. (2011) 59:2062–8. doi: 10.1111/j.1532-5415.2011.03664.x
66. Szlejf C, Suemoto CK, Brunoni AR, Viana MC, Moreno AB, Matos SM, et al. Depression is associated with sarcopenia due to low muscle strength: results from the ELSA-Brasil study. J Am Med Dir Assoc. (2019) 20:1641–6. doi: 10.1016/j.jamda.2018.09.020
67. Hayashi T, Umegaki H, Makino T, Cheng XW, Shimada H, Kuzuya M. Association between sarcopenia and depressive mood in urban-dwelling older adults: a cross-sectional study. Geriatr Gerontol Int. (2019) 19:508–12. doi: 10.1111/ggi.13650
68. Chen L, Sheng Y, Qi H, Tang T, Yu J, Lv S. Correlation of sarcopenia and depressive mood in older community dwellers: a cross-sectional observational study in China. BMJ Open. (2020) 10:e038089. doi: 10.1136/bmjopen-2020-038089
69. Chen X, Han P, Song P, Zhao Y, Zhang H, Niu J, et al. Mediating effects of malnutrition on the relationship between depressive symptoms clusters and muscle function rather than muscle mass in older hemodialysis patients. J Nutr Health Aging. (2022) 26:461–8. doi: 10.1007/s12603-022-1778-8
70. Arts MH, Collard RM, Comijs HC, Naudé PJ, Risselada R, Naarding P, et al. Relationship between physical frailty and low-grade inflammation in late-life depression. J Am Geriatr Soc. (2015) 63:1652–7. doi: 10.1111/jgs.13528
71. Newman AB, Kupelian V, Visser M, Simonsick EM, Goodpaster BH, Kritchevsky SB, et al. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J Gerontol Series A Biol Sci Med Sci. (2006) 61:72–7. doi: 10.1093/gerona/61.1.72
72. Peltzer K. Hand grip strength and depression among rural older South Africans. Humanitas. (2022) 19:23–30. doi: 10.26555/humanitas.v19i1.10
73. Huang X, Ma J, Ying Y, Liu K, Jing C, Hao G. The handgrip strength and risk of depressive symptoms: a meta-analysis of prospective cohort studies. Q Life Res. (2021) 30:2467–74. doi: 10.1007/s11136-021-02858-6
74. Goodpaster BH, Park SW, Harris TB, Kritchevsky SB, Nevitt M, Schwartz AV, et al. The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study. J Gerontol Series A Biol Sci Med Sci. (2006) 61:1059–64. doi: 10.1093/gerona/61.10.1059
Keywords: physical activity, physical frailty, grip strength, depressive symptoms, older adults
Citation: Wang Y, Wang X, Zhu X, Sun Y, Han B and Chen T (2023) Physical activity, physical frailty and depressive symptoms among Chinese male and female older adults: do different indicators make a difference? Front. Public Health 11:1280952. doi: 10.3389/fpubh.2023.1280952
Received: 21 August 2023; Accepted: 08 November 2023;
Published: 27 November 2023.
Edited by:
Stevo Popovic, University of Montenegro, MontenegroReviewed by:
Juan Corral-Pérez, University of Cádiz, SpainCopyright © 2023 Wang, Wang, Zhu, Sun, Han and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tianyong Chen, Y2hlbnR5QHBzeWNoLmFjLmNu
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.