 Run Wang1
Run Wang1 Fang Zheng2
Fang Zheng2 Guiying Cao2Lloyd A. Goldsamt3Yan Shen1
Guiying Cao2Lloyd A. Goldsamt3Yan Shen1 Ci Zhang1Mengyao Yi1
Ci Zhang1Mengyao Yi1 Wenwen Peng1
Wenwen Peng1 Xianhong Li1*
Xianhong Li1*- 1Xiangya School of Nursing, Central South University, Changsha, Hunan, China
- 2Department of AIDS, The First Hospital of Changsha, Changsha, Hunan, China
- 3Rory Meyers College of Nursing, New York University, New York, NY, United States
Introduction: HIV and mental health problems are a global syndemic. One key issue is that the significant mental health problems among people vulnerable to acquiring or living with HIV have not been fully addressed. Access to social support has been one of the biggest challenges for HIV-positive men who have sex with men (HIV+ MSM). Lower social support has been linked to more severe depression symptoms. However, the mechanisms underlying the association between social support and depression in HIV+ MSM are unclear. Two possible mediators include hope and psychological flexibility. This study aimed to examine the relationship between social support and depression in HIV+ MSM and to explore the single mediating effects of hope and psychological flexibility and the chain mediating effect of these two variables on this relationship.
Methods: A convenience sample was used to recruit participants from the designated HIV/AIDS hospital in Changsha city, Hunan Province of China. A total of 290 HIV+ MSM completed questionnaires.
Results: Our findings showed that hope mediated the relationship between social support and depression in HIV+ MSM. Furthermore, the chain mediation model confirmed a direct negative association between social support and depression, but this relationship was largely mediated by the chain effects of hope and psychological flexibility.
Conclusions: Integrating hope and psychological flexibility into interventions may provide better mental health support for HIV+ MSM and improve their wellbeing and quality of life.
Introduction
Globally, there has been a rapid increase in HIV rates in men who have sex with men (MSM) in the last decade (1). The risk of HIV infection for MSM was 26 times higher than that of other adult males (2). China has a similar HIV epidemic trend. Among people newly diagnosed with HIV in China, the proportion of MSM increased from 1.5% in v2006 to 23.0% in 2019, making MSM the fastest-growing sub-group among those infected (3). Under the traditional Chinese cultural background of “filial piety,” homosexuality was morally unacceptable. Structural and psychological forms of stigma toward MSM, including social exclusion and marginalization, create cycles of co-occurring HIV and mental health disorders (4). Thus, Chinese HIV-positive MSM (HIV+ MSM) are even more vulnerable to mental health problems compared with other populations. The anxiety and depression rates among Chinese HIV+ MSM were 38.7 and 50.5% (5), respectively, while they were 25% (6) and 31% (7) among people living with HIV/AIDS (PLWHA) and 2.1 and 5.0% among the Chinese general population, respectively (8). Moreover, mental health problems among HIV+ MSM adversely impact HIV treatment outcomes and lower their quality of life. Depressive symptoms have consistently been found to predict HIV symptoms, drug resistance, and even mortality (4, 9–11). Evidence has also confirmed that poor mental health negatively affects treatment outcomes, including lowering CD4 counts and quality of life (9, 11). Given the highly stigmatized cultural background toward homosexuality, improving the mental health of Chinese HIV+ MSM remains challenging. Outcomes are influenced by patients' coping resources (e.g., social support) and coping responses (e.g., active and avoidant) according to the Stress-Processing Model (12). Among those influencing factors, access to social support has been widely proven to be one of the biggest challenges for PLWHA (13, 14). In addition, according to the Stress-Processing Model, the process of enhancing active coping responses (e.g., psychological flexibility and hope) is necessary for mental health, which may influence depressive symptoms (12). However, there is no research on the pathways between social support and depression among HIV+ MSM. Therefore, this study aims to explore the mediating mechanism of the relationship between social support and depression among HIV+ MSM by understanding the mediating factors to provide recommendations for improving the mental health of HIV+ MSM.
As the main resource of social support, family support could help HIV-infected individuals develop spiritual strength, establish life goals, reshape the meaning of life, and increase treatment adherence, thus enhancing the level of hope (15). Unfortunately, access to social support for HIV+ MSM is not encouraging. Evidence has shown that the availability of social support for Chinese HIV+ MSM was 20% lower than that of other adult males (13) due to HIV-related stigma. Furthermore, due to the fear of being stigmatized, HIV+ MSM were reluctant to access those available social resources (16, 17). Among HIV+ MSM, social support has been associated with reduced hopelessness, anxiety, and depressive symptoms. Evidence suggests that strong social support may reduce the risk of depression by up to 50% among HIV+ MSM (13). Moreover, African Americans living with HIV clearly expressed a desire for emotional and instrumental support and emphasized support as a mechanism to resist the negative effects of HIV-related stigma (18). However, Parcesepe et al. (19) suggested that there was no direct association between social support and psychological distress among PLWHA, which was inconsistent with previous studies. Social support may be indirectly associated with depression through other mediators. However, the evidence illustrating how social support may be positively linked to mental and physical health outcomes is less conclusive, although essential when designing effective interventions for HIV+ MSM (20, 21). Therefore, it is critical to explore potential pathways of social support and depression in HIV+ MSM.
Psychological flexibility might be a potential mediator in explaining how lower social support may lead to higher depression. According to the Stress-Processing Model, psychological flexibility plays an important role in improving mental health, which could not only directly reduce depression but also alleviate negative emotional experiences (22, 23). Psychological flexibility refers to the capacity of individuals to use psychological resources flexibly to adapt to different psychological needs or change their own points of view according to the environment (24). However, due to the life-long experience of sexual minority stress, HIV+ MSM demonstrate a lower level of psychological flexibility, leading them to keep their HIV infection a secret and consistently worry about being stigmatized (25, 26). Meanwhile, previous studies have confirmed that greater psychological flexibility was associated with optimal mental health (25–27). For example, a cross-sectional study among HIV+ MSM in the United States showed that psychological flexibility was an important predictor of mental health disorders (26), and lower psychological flexibility was associated with higher levels of depression (26). Despite growing evidence of the positive effects of psychological flexibility, the role of psychological flexibility in the relationship between social support and depression in people living with HIV remains unclear. Based on the existing evidence (28–30), this study hypothesized that psychological flexibility might become a mediator for HIV+ MSM's ability to access social support and reduce their depression.
Hope might be an additional potential mediator explaining the pathway from social support to depression. Social support is strongly associated with hope. As an intrinsic resource, social support, especially family support, could also strengthen hope. A study among 160 HIV-infected patients in Nepal showed that social support had a positive influence on hope, with higher social support associated with higher levels of hope (31). Evidence also indicates that hope is an important factor that affects the mental health of PLWHA (32–34). Liu et al. (34) conducted a study among 206 PLWHA and found that higher levels of hope could reduce depression symptoms, help PLWHA accept their HIV infection, and rationalize their sexual behavior. Individuals with higher levels of hope may possess a greater ability to cope with difficulties (34). Although no research has yet found a mediating role for hope between social support and depression among HIV+ MSM, it is a mediator between social support and quality of life in PLWHA (31), suggesting that hope may alleviate the negative impact of inadequate social support on quality of life. Given the association between social support and depression (31, 34), it was assumed that hope could also serve as a mediator between social support and depression among HIV+ MSM (35).
Moreover, the literature shows that hope is also associated with psychological flexibility (12). According to the Stress-Processing Model, hope as a positive psychological coping mechanism should be interrelated with depression (36), but this relationship could be mediated by psychological flexibility, as indicated by a study conducted among the general population in France during the COVID-19 lockdown period (35). Arslan et al. (37) also found that psychological inflexibility mediated the relationship between optimism-pessimism and depression among Turkish young adults, suggesting that hope and psychological flexibility may work together to alleviate depressive symptoms. However, few studies have neither examined the mediating roles of psychological flexibility and hope between social support and depression among HIV+ MSM, nor the combined impact of the two factors on depression, and the underlying mechanism of these associating variables remains unclear.
In summary, although the relationships among the variables of social support, psychological flexibility, hope, and depression have been examined separately, the role of psychological flexibility and hope in the impact of social support on depression among HIV+ MSM has not yet been thoroughly tested to date. We constructed a hypothetical model to test the relationship between social support and depression and the roles of psychological flexibility and hope among HIV+ MSM. Based on the previous evidence, we put forward four hypotheses: (1) social support might have a direct negative association with depression; (2) psychological flexibility would act as a mediator between social support and depression; (3) hope would act as a mediator between social support and depression; and (4) hope and psychological flexibility would jointly play a chain mediating role in the relationship between social support and depression. The hypothesized theoretical model is illustrated in Figure 1.
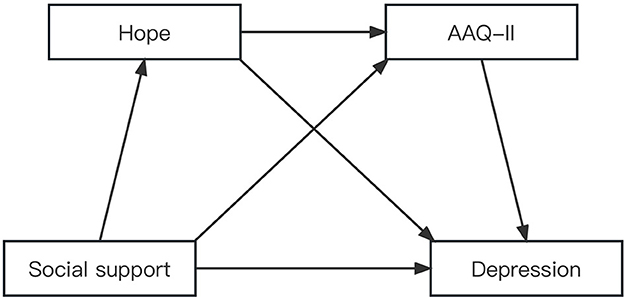
Figure 1. The theroetical models and hypotheses of social support. psychological flexibility, hope, and depression.
Methods
Study design and setting
This cross-sectional survey was conducted from June to October 2022. All participants were recruited from the designated HIV/AIDS hospital in Changsha city, Hunan Province of China. Hunan Province is located in south-central China, and the prevalence of HIV is consistent with the national level (38). As of October 2022, the reported cumulative number of surviving PLWHA in Hunan Province exceeded 50,000, and 5,463 were newly reported in 2022, of which 17% were infected through male-to-male sexual transmission, while in Changsha city, this proportion exceeded 50% (39).
Participants and recruitment
The target population for this study was MSM. The inclusion criteria were as follows: (a) male at birth; (b) self-reported ever having sex with men; (c) 18 years of age or older; (d) diagnosed with HIV infection by Western blot analysis; and (e) living in Hunan Province. Those who (a) had a cognitive impairment that limited their ability to understand and complete the study questionnaires and/or (b) were participating in other psychological interventions were excluded. Convenience sampling was used to recruit participants. The recruitment flier was posted at the hall of a community-based organization (CBO), which was located at the designated hospital. Those who were interested could contact a research assistant for screening. Some potential participants were also referred by the medical social worker from the CBO. This study was approved by the institutional review board of behavioral and nursing research in the Xiangya School of Nursing of Central South University (#E2022121).
Data collection
Data were collected using an online survey company (http://www.sojump.com), which had signed a contract with the study team to keep the data confidential. Informed consent was obtained from each participant before they started the online survey by scanning a QR code. Only when they clicked the “Informed and Agree” button and signed electronically, they could initiate the survey. IP addresses were used to prevent participants from completing multiple surveys. This survey took approximately 20 min to complete. Participants received 30 RMB (approximately US$5) as compensation for time spent filling out the survey. A total of 300 questionnaires were distributed, of which 290 were valid. Ten questionnaires (3.3%) were excluded due to participants dropping out in the middle of the process, resulting in an efficiency of 96.7%.
Measures
Socio-demographic and disease-related variables
Considering the potential influencing factors of depression (40–45), participants' socio-demographic information, including age, marital status, education level, employment, individual monthly income, and HIV-related information (including years of being diagnosed with HIV, years of antiviral treatment, HIV disclosure status, and drug side effects), was collected.
HIV transmission knowledge
A widely used 8-item questionnaire was adopted from “The China AIDS Prevention Supervision and Evaluation Framework Manual” (46). Responses are true or false, with one point for each correct answer. The total score ranges from 0 to 8. A total score of ≥6 indicates good awareness of HIV transmission. In this study, Cronbach's alpha was 0.72.
Depression
The Self-rating Depression Scale (SDS) developed by Zung (47) was used. This scale contains 20 items and is scored on a 4-point scale, ranging from “never (1) or occasionally” to “always (4)”. The total score is divided into three levels: low (48–57), moderate (58–67), and high (>72) (68). The higher score indicates a higher level of depressive symptoms. The SDS showed excellent reliability (Cronbach's alpha = 0.89) in China. In the current study, Cronbach's alpha of the scale was 0.82.
Social support
Social support was measured using the Social Support Rating Scale (SSRS), developed by Xiao Shuiyuan (69). The scale consists of 10 items, with a total score ranging from 12 to 66. The scale has been widely used in China (69). The higher the total score, the more the social support received. The Chinese SSRS has good validity and reliability (Cronbach's alpha = 0.82). In the current study, Cronbach's alpha of the scale was 0.76.
Psychological flexibility
The Acceptance and Action Questionnaire-II (AAQ-II) was used to evaluate the degree of psychological flexibility. Bond et al. (70) revised the AAQ-II scale from 9 items to 7 items, with a total score ranging from 7 to 49. Lower scores indicate lower experiential avoidance and higher psychological flexibility. Jing et al. (71) translated the 7-item scale and applied it to Chinese college students, and it demonstrated good reliability with Cronbach's alpha of 0.88. In the current study, Cronbach's alpha of the scale was 0.94.
Hope
The Herth Hope Index (HHI) was used to evaluate each participant's level of hope. The Chinese version of the scale was translated by Haiping and Zian (72). It consists of 12 items, with a total score ranging from 12 to 48. Higher scores indicate higher individual hope. The Chinese version of this scale had good reliability (Cronbach's alpha = 0.85). In the current study, Cronbach's alpha of the scale was 0.77.
Data analysis
The online questionnaire data were directly exported into an Epidata 3.1 database and cleaned. Statistical analyses were performed using IBM SPSS Statistics 26.0 and PROCESS 3.5.
First, descriptive statistics were calculated. Proportions and frequencies were calculated for the socio-demographic data and disease-related data. The Kolmogorov-Smirnov tests were used to check the normality of the study variables (social support, psychological flexibility, hope, and depression) (48). The mean (M) and standard deviation (SD) were calculated for the study variables if the data met the normal distribution. If not, the median and interquartile range (IQR) of the study variables were calculated. Second, we used Spearman's correlation coefficient to examine the relationships between all study variables among participants. Then, all variables, including socio-demographic and disease-related variables, social support, psychological flexibility, and hope, were entered into the multiple linear regression model to identify the independent correlates of depression among HIV+ MSM. Finally, for each pathway, we used a bias-corrected bootstrap method with 5,000 replications to examine the direct and indirect effects of HIV social support on depression (49). After adjusting covariates that were significant in multivariate regression analysis, the hypothetical single and chain mediation models were examined using PROCESS 3.5 developed by Hayes. Single mediation models of social support for depression through hope and psychological flexibility were examined using the PROCESS model 4 (50). The chain mediation model was carried out using PROCESS model 6 to examine the path between two mediators in sequence and the indirect effects of each mediator independently (49). If the 95% confidence interval did not include zero, the mediating effect was considered statistically significant. Statistical significance was set at P < 0.05.
Results
Common methods of bias control and testing
Harman's single-factor test was used to examine the common method biases, considering that the data were collected by questionnaire (51). The results showed that the characteristic root of these five factors was >1, and the first factor could explain 20.068%, which was 40% lower than the standard threshold value (51), which indicated that there was no serious common method bias problem in this study.
General information about the participants
A total of 300 questionnaires were accessed, of which 290 were valid and 10 were discarded. The average age of the participants was 27.71 years (SD = 0.417). Most of the participants were unmarried (90.3%) and held a college degree or above (71.4%). Only 9.7% of the participants had an individual monthly income >8,000 RMB (approximately US$1,110). Notably, 64.8% of them had been diagnosed with HIV for more than 6 months, and 50.3% reported 3–6 drug side effects. Less than 1/5 (17.6%) told their partners about their infection status. These data are shown in Table 1.
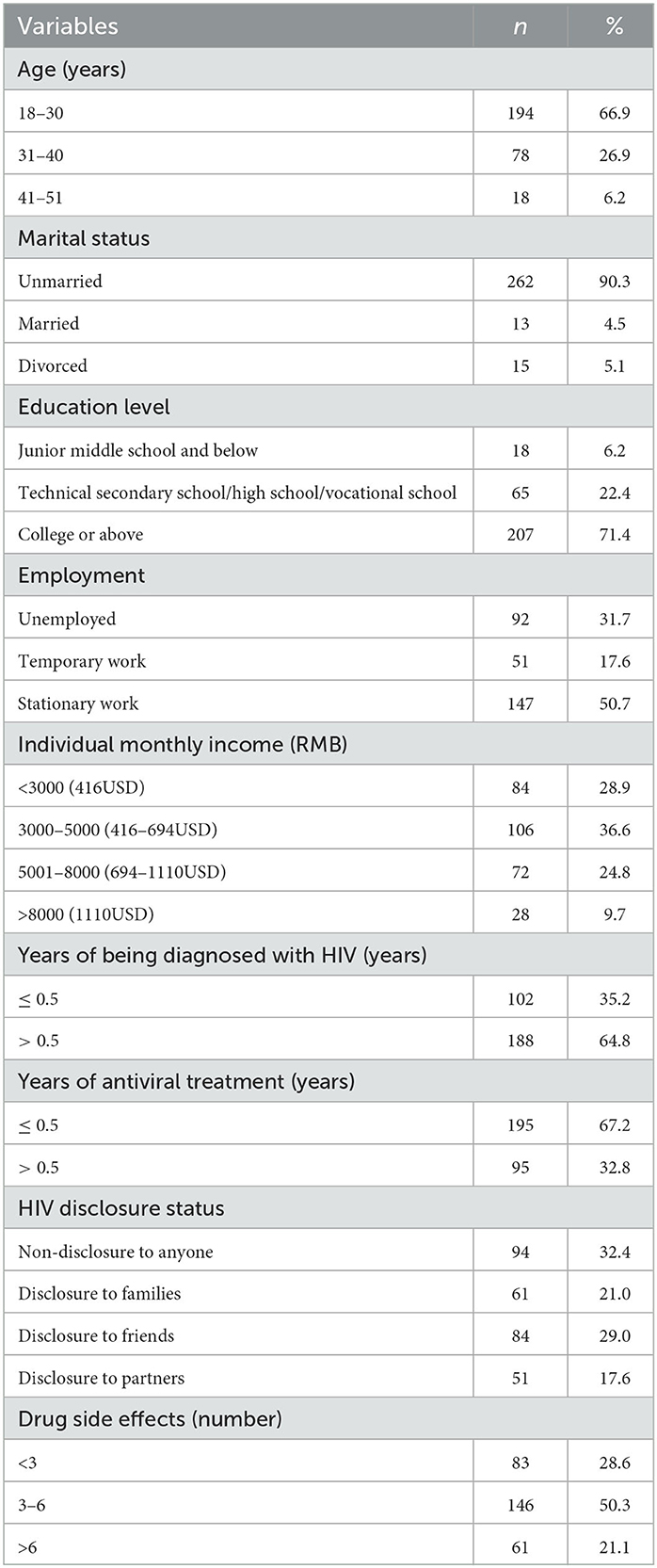
Table 1. General information of the participants (n = 290).
Description and bivariate correlations of study variables
As shown in Table 2, the mean scores of social support, psychological flexibility, hope, and depression were 25.71 ± 8.665, 28.94 ± 10.969, 34.00 ± 6.676, and 59.00 ± 14.749, respectively. According to these scores, 67.6% (195) had depressive symptoms, and 62.6% (122) of those with depressive symptoms had moderate to severe depressive symptoms.

Table 2. Mean, standard deviations, and correlations for study variables (N = 290).
Spearman's correlation coefficients between all study variables found that social support had a positive correlation with hope (r = 0.570, P < 0.01) and negative correlations with AAQ-II (r = −0.381, P < 0.01) and depression (r = −0.527, P < 0.01). Hope had a negative correlation with AAQ-II (r = −0.582, P < 0.01) and depression (r = −0.729, P < 0.01). Likewise, AAQ-II had a significant positive correlation with depression (r = 0.684, P < 0.01). Hypothesis 1 was verified.
Linear regression analysis
In the multiple linear regression model, we used depression as the dependent variable, and socio-demographic variables, disease-related factors, social support, psychological flexibility, and hope as independent variables. At the same time, we tested the collinearity of the independent variables, and the results showed that the tolerance of the independent variables was more than 0.1 and the variance inflation factor (VIF) was <10.0. Therefore, there was no multi-collinearity among independent variables. The results of the regression analysis showed that by controlling for the socio-demographic variables and disease-related factors, social support, psychological flexibility, and hope were significant influencing factors of depression for HIV+ MSM (Table 3). In addition to the study variables, age, individual monthly income, years of being diagnosed with HIV, HIV disclosure status, drug side effects, and HIV transmission knowledge score were also influential factors for depression in HIV+ MSM.
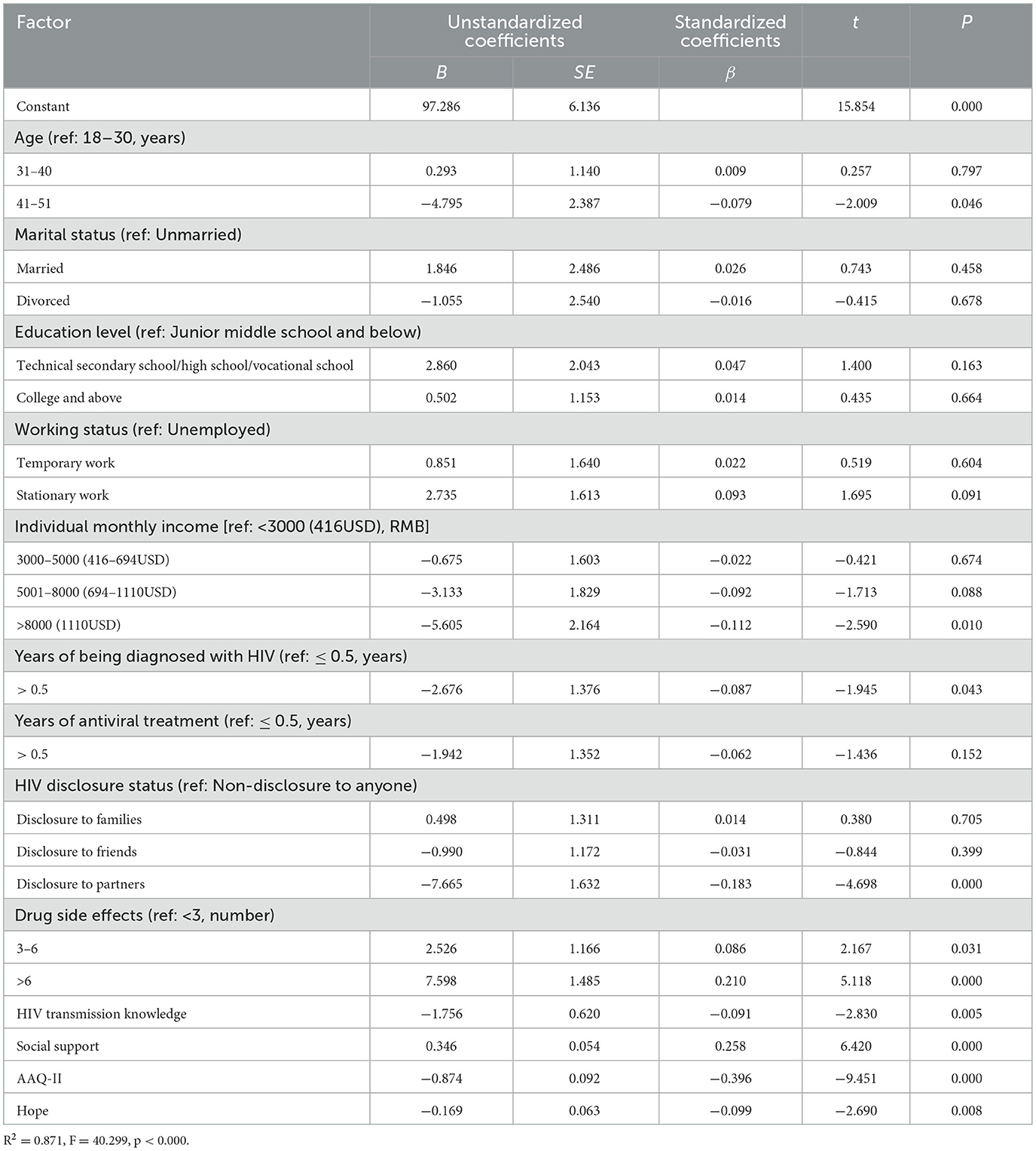
Table 3. Linear regression of factors associated with depression.
The single mediating effect of hope and psychological flexibility on the relationship between social support and depression
We examined the single mediation effect of psychological flexibility and hope on the relationship between social support and depression after controlling HIV disclosure and drug side effects, respectively. As shown in Figure 2, in the model with psychological flexibility as the single mediator, social support was positively associated with psychological flexibility (β = −0.238, P < 0.001), and psychological flexibility was negatively associated with depression (β = 0.564, P < 0.001). A significant indirect effect of social support on depression via psychological flexibility was found, and the mediating effect value was −0.134 [Bootstrap 95% CI: −0.235, −0.059]. Therefore, psychological flexibility played a partial mediating role between social support and depression. Hypothesis 2 was verified.
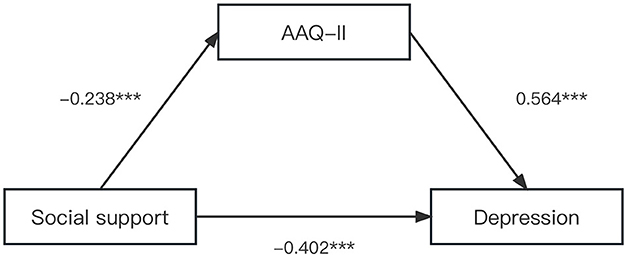
Figure 2. The single mediation role of psychological flexibility in the relationship between social support and depression. The solid line indicated significant path coefficients. ***p < 0.001.
As shown in Figure 3, in the model with hope as the mediator, social support was positively associated with hope (β = 0.319, P < 0.001), and hope was negatively associated with depression (β = –1.181, P < 0.001). A significant indirect effect of social support on depression via hope was found. The mediating effect of hope was −0.376 [Bootstrap 95% CI: −0.503, −0.266]. Hypothesis 3 was supported.
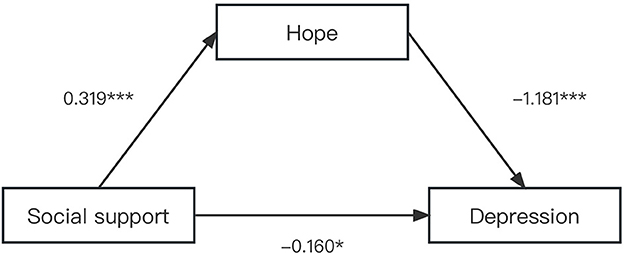
Figure 3. The single mediation role of hope in relationship between social support and depression. The solid line indicated significant path coefficients. ***p < 0.001 and *p < 0.05.
The chain mediating effect of hope and psychological flexibility on the relationship between social support and depression
Regression analysis was carried out on the chain intermediary effect model (52). Table 4 displays the coefficients and significance of each path in the chain mediation model. We found that social support was negatively associated with depression. The total effect was −0.537 [Bootstrap 95% CI: −0.760, −0.367], and the direct effect was −0.159 [Bootstrap 95% CI: −0.298, −0.020], which meant that the higher the level of social support, the lower the depressive symptoms were among HIV+ MSM. Therefore, hypothesis 1 was supported. Table 4 confirmed that social support had a direct and significant positive association with hope (β = 0.319, P < 0.001), while it had no significant association with psychological flexibility (β = −0.004, P = 0.966). Hope was negatively associated with depression (β = −0.927, P < 0.001) and positively associated with psychological flexibility (β = −0.735, P < 0.001). Psychological flexibility had a significant negative association with depression (β = 6.093, P < 0.001). Meanwhile, social support was still negatively associated with depression (β = −0.159, P < 0.05; Figure 4). It could be concluded that psychological flexibility and hope played an intermediary role between social support and depression. Hypotheses 1 and 3 were supported by data.
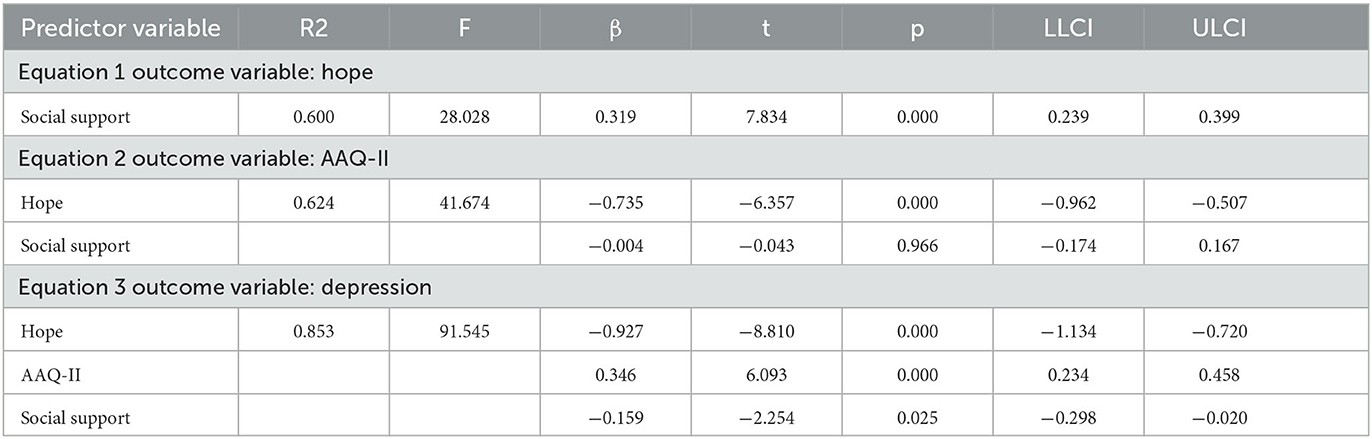
Table 4. Analysis of regression relationship of variables.
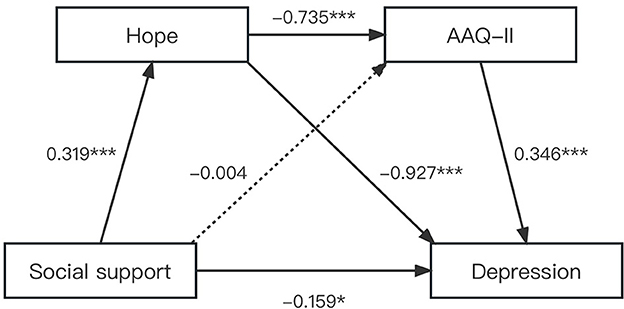
Figure 4. The chain mediation role of psychological flexibility in the relationship between social support and depression. The solid and dashed line indicated significant and non-significant path coefficients. ***p < 0.001 and *p < 0.05.
Table 5 shows the results of the chain mediation analyses and the effect size of the intermediary pathway, which indicated that the total indirect effect was −0.378 [Bootstrap 95% CI: −0.510, −0.273], while the direct effect was −0.159 [Bootstrap 95% CI: −0.298, −0.020], suggesting that the indirect effect was stronger than the direct effect. Specifically, the total indirect effect of the relationship between social support and depression included two pathways, and all specific mediating effects and chain mediating effects were significant. The indirect mediating effect of hope was −0.295 [Bootstrap 95% CI: −0.408, −0.203]. The bootstrap's 95% CI of the path did not contain zero, indicating that this indirect path was statistically significant. Importantly, the indirect effect of chain mediation from social support to depression via hope and psychological flexibility was significant, and the effect value was −0.082 [Bootstrap 95% CI: −0.129, −0.048]. The total indirect effect of psychological flexibility and hope accounted for 70.39% in the chain model, while the direct effect accounted for only 29.61% (Figure 4). Therefore, hypothesis 4 was supported.
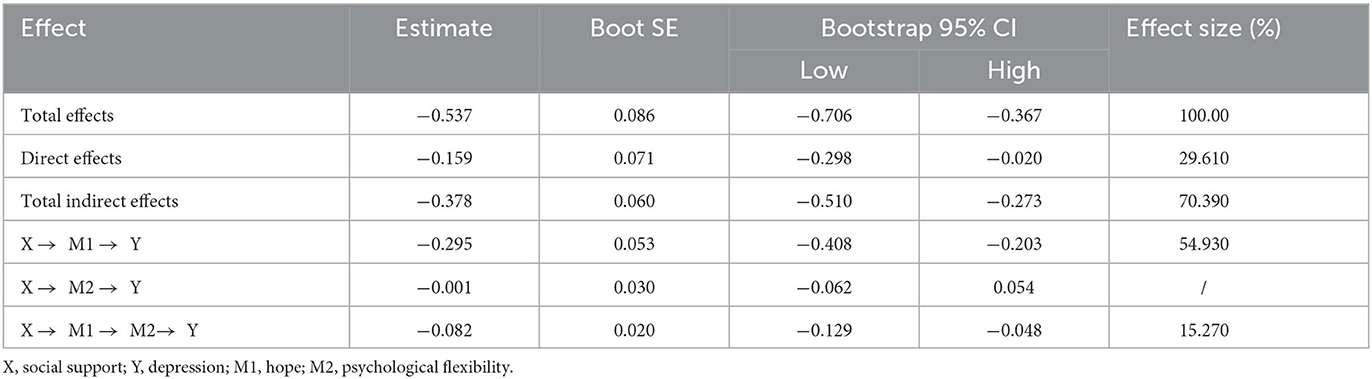
Table 5. Total, direct, and indirect effect of social support on depression though psychological flexibility and hope.
Discussion
This study explored the intermediary mechanism between social support and depression among Chinese HIV+ MSM based on the stress-processing model. The results supported the hypotheses and indicated that psychological flexibility and hope played a chain-medicating role in the association between social support and depression. In addition, the chain mediation analyses suggested a significant serial effect between psychological flexibility and hope.
In this study, the prevalence of depression among Chinese HIV+ MSM was 67.6% (196/290), which was much higher than that reported globally (43%) (7) and in other settings such as Vancouver, Canada (39.3%) (53) and the United States (40.8%) (54). Compared to the United States and European countries (55–57), China exhibits higher judgmental attitudes toward homosexuality due to traditional social norms and the Confucian philosophy that emphasizes heterosexual marriage and having sons to pass down the family name (58). Thus, the majority of Chinese people do not accept homosexuals and hold negative attitudes such as intolerance and avoidance toward MSM (59). When MSM get infected with HIV, they experience much more stress due to the HIV-related stigma, which adds to the homosexual stigma. HIV-related stigma in China is also higher than that in the West and some African countries (60, 61). As HIV infection is often considered to be associated with moral degradation or promiscuity, which leads to social discrimination and exclusion (40), Chinese PLWHA face more social condemnation, discrimination, and stigma (13, 59, 62, 63). Chinese PLWHA also experience higher stigma compared to some African countries, where HIV prevalence is very high, such as Kenya (22.02%), Zambia (23.38%), and Lesotho (25.48%) (64), and the public is not afraid of HIV as in China. The literature has confirmed that the dual stigma could lead to an increased prevalence of depression for HIV+ MSM. A meta-analysis found a 43% co-prevalence of depression and HIV infection among MSM, and HIV+ MSM were more likely to be depressed compared to HIV-negative MSM (65). In addition, evidence indicated that stigma and discrimination against sexual orientation and HIV infection were major sources of stress for HIV+ MSM (14, 66, 67). Therefore, HIV and depression among HIV+ MSM in China are syndemic, creating a vicious cycle in the HIV epidemic (20).
Moreover, as an isolated and marginalized group, HIV+ MSM perceived lower social support compared with that reported in previous studies (73, 74). In addition to the high dual stigma, which reduced the available social support resources, the concealment of their sexual orientation and HIV status also limited their access to those supporting resources. According to a recent meta-analysis, the disclosure rates for HIV+ MSM to their family, intimate friends, spouses, and regular sexual partners were low, at 43.42, 47.9, 56.8, and 43.2%, respectively (40). Chinese MSM usually face the dilemma of being exposed as gay men once informed of their HIV status, and they also fear hurting family feelings and wish to avoid embarrassment (75). Furthermore, the disclosure of HIV status causes familial exclusion, engenders a sense of social isolation, and gives rise to serious consequences such as impaired social roles and relationships, leading HIV+ MSM to experience less access to social support (76). Thus, medical staff should leverage proximity to facilitate early disclosure to help ensure HIV+ MSM receive adequate psychological care from their loved ones.
Consistent with hypothesis 3, this study found that hope partially mediated the relationship between social support and depression. Although the pathways have not been fully illuminated, some studies provided indirect support for them. For example, Masquillier et al. (15) confirmed that family functioning was positively associated with hope among PLWHA, and a supportive family could provide spiritual support to patients. The more patients felt being cared for by family members, the higher their level of hope. Furthermore, hope has a close association with anxiety and depression. Substantial evidence indicates that PLWHA with higher levels of hope have less depression and anxiety and a greater ability to cope with difficulties (31, 33, 34). The present study further supports these findings and suggests that social support, serving as an intrinsic resource, could strengthen hope, increase confidence, and ultimately reduce psychological distress, including depression.
This study found that psychological flexibility was not a mediator between social support and depression, which might be related to our sample characteristics and study methodology. Nevertheless, we found that social support did play an important role in reducing depression in HIV+ MSM, which was consistent with previous findings (13, 26). Furthermore, our most noteworthy finding was that social support had an effect on depression through the chain mediation of hope and psychological flexibility, which means that, with more social support, HIV+ MSM will first feel more hope and then increase psychological flexibility, which ultimately alleviates their depressive symptoms. These findings support our hypothesis and extend the existing evidence indicating that hope is a core dimension of recovery from mental disorders and negative coping styles (15). Nyoni et al. (77) conducted a study among 346 PLWHA in sub-Saharan Africa and suggested that perceived social support, especially family support, could enhance a sense of hope, establish a positive attitude, help them adapt to external changes, and then find appropriate self-regulation mechanisms, thereby reducing depressive symptoms. In addition, our study demonstrated a positive association between hope and psychological flexibility. Evidence confirmed that patients with higher levels of hope might have more conviction and motivation to face potentially traumatic events and thus have higher levels of psychological flexibility and resilience in the face of stress and difficulties (35). Similarly, Landstra et al. (26) also confirmed that some resilience-promoting resources, such as optimism, hope, and self-efficacy, could enhance psychological flexibility and ultimately reduce the incidence of depression. In addition, the stress process model (12) could explain this chain-mediating effect. The model suggests that an individual's perception of coping resources (e.g., social support) affects his or her hope and confidence in regulating stress, which in turn affects flexibility and adaptability in the face of stress and difficulties (e.g., psychological flexibility) and ultimately determines the extent to which mental disorders increase or decrease (78). Therefore, incorporating the concepts of hope and psychological flexibility into interventions can provide better mental health support for HIV+ MSM and improve their quality of life and wellbeing.
Inevitably, this study had several limitations that should be noted. First, the participants were only from one city in China, and thus the results might not be generalizable to HIV+ MSM populations in other geographic regions. Second, the cross-sectional and self-reported nature of the study might cause recall bias. In addition, this study only controlled for demographic and some disease-related variables; other potential influencing variables were not collected, such as coping strategies (79), which might affect the stability of the chain mediating model.
Despite these limitations, this study revealed the mediating role of psychological flexibility and hope between social support and depression, which has several implications for future research and practice. First, this study illustrates the need for interventions to improve the mental health of HIV+ MSM. Positive psychological interventions can play an important role in alleviating depressive symptoms and enhancing wellbeing in PLWHA (4, 20). Therefore, researchers need to adopt a positive perspective in addressing the mental health disorders of patients and explore new pathways for their psychological care. Future intervention studies can specifically target the psychological flexibility and hope of HIV+ MSM to improve their mental health and prevent HIV transmission. Second, a more conducive social environment should be created. Promoting social acceptance for MSM (10), reducing HIV-related discrimination and stigma, and improving social support (80) can provide emotional support to HIV+ MSM and reduce negative emotions (10, 13, 80). This underscores the importance of considering not only individual-level interventions but also social factors that affect the mental health of HIV+ MSM. In addition, public health policymakers should strive for clear policies and practices to promote social equity and medical convenience for MSM (76). For instance, expanding the PrEP transport network and HIV self-testing services can enhance the sustainability of PrEP among MSM (81, 82). Research conducted by Schanll et al. (82) highlights the high risk of HIV infection among young MSM (YMSM), underscoring the potential utility of HIV self-testing as a tool to ensure timely detection of infection and initiation of antiretroviral therapy. Finally, some current interventions focus only on social support (83), hope (15), or psychological flexibility (25) as ways to improve the mental health of PLWHA, but our study suggests that future interventions should combine the efforts to stimulate social support by increasing the level of hope and enhancing psychological flexibility. Integrated interventions are urgently needed to address structural barriers to accessing HIV prevention and treatment (84), thereby achieving the UNAIDS' 95-95-95 targets for ending AIDS by 2030 (85).
Conclusion
This study clarified the mediating pathway between social support and depression among Chinese HIV+ MSM. These findings indicated that hope and psychological flexibility play a chain-mediating role in this relationship and that hope also plays a single-mediating role. Given the mediating role of psychological flexibility and hope on depression among HIV+ MSM, interventions related to psychological flexibility and hope should be designed to enhance mental health among HIV+ MSM in China and other global settings.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving humans were approved by the Institutional Review Board of Behavioral and Nursing Research in the Xiangya School of Nursing of Central South University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
RW: Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Writing—original draft, Writing—review & editing, Software. FZ: Writing—review & editing. GC: Writing—review & editing. LG: Writing—review & editing. YS: Writing—review & editing. CZ: Writing—review & editing. MY: Writing—review & editing. WP: Writing—review & editing. XL: Writing—review & editing, Resources, Supervision.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by the National Natural Science Foundation of China, the funder was XL and the funding number was 72074226; and by the China Medical Board Open Competition Project, the funder was XL and the funding number was 22–465.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Cai R, Richardus JH, Looman CW, de Vlas SJ. Trends in high-risk sexual behaviors among general population groups in China: a systematic review. PLoS ONE. (2013) 8:e79320. doi: 10.1371/journal.pone.0079320
2. China, NHCotPsRo. New Progress in China's HIV Prevention and Treatment Efforts in 2019. http://www.nhc.gov.cn/jkj/s3586/201911/c2388ce70bdd404ea6dfcd886591784d.shtml (accessed November 30, 2019).
3. UNAIDS. Global HIV&AIDS Statistics-−2020 Fact Sheet. (2022) Available online at: https://www.unaids.org/en/resources/fact-sheet (accessed August 31, 2023).
4. Remien RH, Stirratt MJ, Nguyen N, Robbins RN, Pala AN, Mellins CA. Mental health and HIV/AIDS: the need for an integrated response. AIDS. (2019) 33:1411–20. doi: 10.1097/QAD.0000000000002227
5. Wei D, Wang X, You X, Luo X, Hao C, Gu J, et al. Prevalence of depression, anxiety and suicide among men who have sex with men in China: a systematic review and meta-analysis. Epidemiol Psychiatr Sci. (2020) 29:e136. doi: 10.1017/S2045796020000487
6. Rahmati J, Ahmadi S, Rezaei S, Hosseinifard H, Dehnad A, Shabaninejad H, et al. The worldwide prevalence of anxiety in acquired immune deficiency syndrome patients: a systematic review and meta-analysis. Med J Islam Repub Iran. (2021) 35:101. doi: 10.47176/mjiri.35.101
7. Rezaei S, Ahmadi S, Rahmati J, Hosseinifard H, Dehnad A, Aryankhesal A, et al. Global prevalence of depression in HIV/AIDS: a systematic review and meta-analysis. BMJ Supp Palliat Care. (2019) 9:404–12. doi: 10.1136/bmjspcare-2019-001952
8. China NHaHCotPsRo,. National Health Commission: Prevalence of Depression in China Reaches 2.1% Prevalence of Anxiety Disorders 4.98% (2020). Available online at: http://news.china.com.cn/txt/2020-12/23/content_77043277.htm (accessed December 23, 2020).
9. Langebeek N, Kooij KW, Wit FW, Stolte IG, Sprangers MAG, Reiss P, et al. Impact of comorbidity and ageing on health-related quality of life in HIV-positive and HIV-negative individuals. AIDS. (2017) 31:1471–81. doi: 10.1097/QAD.0000000000001511
10. Moges NA, Adesina OA, Okunlola MA, Berhane Y, Akinyemi JO. Psychological distress and its correlates among newly diagnosed people living with HIV in northwest Ethiopia: ordinal logistic regression analyses. Infect Dis. (2021) 14:1178633721994598. doi: 10.1177/1178633721994598
11. Xie J, Wang Z, Li Q, He Q, Xu G, Li Y, et al. Associations between antiretroviral therapy-related experiences and mental health status among people living with HIV in China: a prospective observational cohort study. AIDS Res Ther. (2021) 18:60. doi: 10.1186/s12981-021-00370-y
12. Steglitz J, Ng R, Mosha JS, Kershaw T. Divinity and distress: the impact of religion and spirituality on the mental health of HIV-positive adults in Tanzania. AIDS Behav. (2012) 16:2392–8. doi: 10.1007/s10461-012-0261-7
13. Yan H, Li X, Li J, Wang W, Yang Y, Yao X, et al. Association between perceived HIV stigma, social support, resilience, self-esteem, and depressive symptoms among HIV-positive men who have sex with men (MSM) in Nanjing, China. AIDS Care. (2019) 31:1069–76. doi: 10.1080/09540121.2019.1601677
14. Brown MJ, Gao C, Kaur A, Qiao S, Li X. Social support, internalized HIV stigma, resilience and depression among people living with HIV: a moderated mediation analysis. AIDS Behav. (2023) 27:1106–15. doi: 10.1007/s10461-022-03847-7
15. Masquillier C, Wouters E, Mortelmans D, Booysen Fle R. Families as catalysts for peer adherence support in enhancing hope for people living with HIV/AIDS in South Africa. J Int AIDS Soc. (2014) 17:18802. doi: 10.7448/IAS.17.1.18802
16. Henderson ER, Egan JE, Haberlen SA, Detels R, Teplin LA, Friedman MR, et al. Does social support predict depressive symptoms? A longitudinal study of midlife and older men who have sex with men from the multicenter AIDS. Cohort Study Ann LGBTQ Public Popul Health. (2021) 2:142–60. doi: 10.1891/LGBTQ-2020-0042
17. De Jesus M, Ware D, Brown AL, Egan JE, Haberlen SA, Palella FJ. Social-environmental resiliencies protect against loneliness among HIV-positive and HIV- negative older men who have sex with men: results from the Multicenter AIDS Cohort Study (MACS). Soc Sci Med. (2021) 272:113711. doi: 10.1016/j.socscimed.2021.113711
18. Buseh AG, Stevens PE. Constrained but not determined by stigma: resistance by African American women living with HIV. Women Health. (2006) 44:1–18. doi: 10.1300/J013v44n03_01
19. Parcesepe A, Tymejczyk O, Remien R, Gadisa T, Kulkarni SG, Hoffman S, et al. HIV-related stigma, social support, and psychological distress among individuals initiating ART in Ethiopia. AIDS Behav. (2018) 22:3815–25. doi: 10.1007/s10461-018-2059-8
20. Operario D, Sun S, Bermudez AN, Masa R, Shangani S, van der Elst E, et al. Integrating HIV and mental health interventions to address a global syndemic among men who have sex with men. Lancet HIV. (2022) 9:e574–e84. doi: 10.1016/S2352-3018(22)00076-5
21. Thoits PA. Mechanisms linking social ties and support to physical and mental health. J Health Soc Behav. (2011) 52:145–61. doi: 10.1177/0022146510395592
22. Lucas JJ, Moore KA. Psychological flexibility: positive implications for mental health and life satisfaction. Health Promot Int. (2020) 35:312–20. doi: 10.1093/heapro/daz036
23. Tindle R, Hemi A, Moustafa AA. Social support, psychological flexibility and coping mediate the association between COVID-19 related stress exposure and psychological distress. Sci Rep. (2022) 12:8688. doi: 10.1038/s41598-022-12262-w
24. McCracken LM. Committed action: an application of the psychological flexibility model to activity patterns in chronic pain. J Pain. (2013) 14:828–35. doi: 10.1016/j.jpain.2013.02.009
25. Kaijun H, Yan X, Yujie Z, Yifan Z. Research progress on the application of acceptance and commitment therapy in the psychological flexibility of people living with HIV/AIDS. Chinese J AIDS STD. (2023) 29:245–8. doi: 10.13419/j.cnki.aids.2023.02.29
26. Landstra JM, Ciarrochi J, Deane FP, Hillman RJ. Identifying and describing feelings and psychological flexibility predict mental health in men with HIV. Br J Health Psychol. (2013) 18:844–57. doi: 10.1111/bjhp.12026
27. Harrison A, Scott W, Timmins L, Graham CD, Harrison AM. Investigating the potentially important role of psychological flexibility in adherence to antiretroviral therapy in people living with HIV. AIDS Care. (2021) 33:337–46. doi: 10.1080/09540121.2020.1771263
28. Sundström FT, Lavefjord A, Buhrman M, McCracken LM. Assessing psychological flexibility and inflexibility in chronic pain using the multidimensional psychological flexibility inventory (MPFI). J Pain. (2022). doi: 10.1016/j.jpain.2022.11.010
29. Stotts AL, Villarreal YR, Klawans MR, Suchting R, Dindo L, Dempsey A, et al. Psychological flexibility and depression in new mothers of medically vulnerable infants: a mediational analysis. Matern Child Health J. (2019) 23:821–9. doi: 10.1007/s10995-018-02699-9
30. Elliott TR, Hsiao YY, Kimbrel NA, DeBeer BB, Gulliver SB, Kwok OM, et al. Resilience facilitates adjustment through greater psychological flexibility among Iraq/Afghanistan war veterans with and without mild traumatic brain injury. Rehabil Psychol. (2019) 64:383–97. doi: 10.1037/rep0000282
31. Yadav S. Perceived social support, hope, and quality of life of persons living with HIV/AIDS: a case study from Nepal. Qual Life Res. (2010) 19:157–66. doi: 10.1007/s11136-009-9574-z
32. Arnau RC, Rosen DH, Finch JF, Rhudy JL, Fortunato VJ. Longitudinal effects of hope on depression and anxiety: a latent variable analysis. J Pers. (2007) 75:43–64. doi: 10.1111/j.1467-6494.2006.00432.x
33. Abler L, Hill L, Maman S, DeVellis R, Twine R, Kahn K, et al. Hope matters: developing and validating a measure of future expectations among young women in a high hiv prevalence setting in rural south Africa (HPTN 068). AIDS Behav. (2017) 21:2156–66. doi: 10.1007/s10461-016-1523-6
34. Cong L, Kai Z, Xu HH, Li G, Chen Y, Luo L, et al. Study on the hope level and its influence factors of patients with HIV/AIDS who received antiretroviral therapy. Chin Nurs Manage. (2017) 17:1047–51. doi: 10.3969/j.issn.1672-1756.2017.08.010
35. Pellerin N, Raufaste E, Corman M, Teissedre F, Dambrun M. Psychological resources and flexibility predict resilient mental health trajectories during the French covid-19 lockdown. Sci Rep. (2022) 12:10674. doi: 10.1038/s41598-022-14572-5
36. Woldgabreal Y, Day A, Ward T. Linking positive psychology to offender supervision outcomes: the mediating role of psychological flexibility, general self-efficacy, optimism, and hope. Crim Justice Behav. (2016) 43:697–721. doi: 10.1177/0093854815620816
37. Arslan G, Yildirim M, Tanhan A, Buluş M, Allen KA. Coronavirus stress, optimism-pessimism, psychological inflexibility, and psychological health: psychometric properties of the coronavirus stress measure. Int J Ment Health Addict. (2021) 19:2423–39. doi: 10.1007/s11469-020-00337-6
38. Dan L. Hunan AIDS Epidemic Overall at a Low Epidemic Level 2021. (2021) Available online at: https://baijiahao.baidu.com/s?id=1717925890461098249&wfr=spider&for=pc (accessed December 01, 2021).
39. Prevention HPCFDCA,. Publicity Activities for 2022 “World AIDS Day” in Hunan Province. (2022) Available online at: http://www.hncdc.com/news/show/5441.html (accessed December 09, 2022).
40. Yu Y, Qin K, Xiao F, Cai H, Sun Y, Li J, et al. HIV Disclosure among sexually infected people living with HIV and AIDS in China: prevalence, influencing factors, and negative outcomes. AIDS Behav. (2022) 27:2411–29. doi: 10.1007/s10461-022-03968-z
41. Xiao L, Jing H, YU L, Shishi W, Ruiting Z, Kerong W, et al. Depression and its related factors of young-middle men who have sex with men with HIV infections. Chinese J AIDS STD. (2022) 28:494–7. doi: 10.13419/j.cnki.aids.2022.03.10
42. Seid S, Abdu O, Mitiku M, Tamirat KS. Prevalence of depression and associated factors among HIV/AIDS patients attending antiretroviral therapy clinic at Dessie referral hospital, South Wollo, Ethiopia. Int J Ment Health Syst. (2020) 14:55. doi: 10.1186/s13033-020-00389-0
43. Tan T, Zhou C, Lu R, Chen C, Bai C, Li L, et al. Depression and associated factors among men living with HIV/AIDS aged 50 years and over in Chongqing, China. J Multidiscip Healthc. (2022) 15:2033–40. doi: 10.2147/JMDH.S378956
44. Liu H, Zhao M, Ren J, Qi X, Sun H, Qu L, et al. Identifying factors associated with depression among men living with HIV/AIDS and undergoing antiretroviral therapy: a cross-sectional study in Heilongjiang, China. Health Qual Life Outcomes. (2018) 16:190. doi: 10.1186/s12955-018-1020-x
45. Mokwena KE, Mbatha NL. Social and demographic factors associated with postnatal depression symptoms among HIV-positive women in primary healthcare facilities, South Africa. Healthcare. (2021) 9:65. doi: 10.3390/healthcare9010065
46. Centers for Disease Control C,. China AIDS Prevention Supervision Evaluation Framework Manual. China Disease Prevention Control. (2009) Available online at: http://www.chinacdc.cn/jkzt/crb/azb/jszl_2219/201003/t20100322_24509.htm (accessed December 30, 2009).
47. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. (1965) 12:63–70. doi: 10.1001/archpsyc.1965.01720310065008
48. Das KR. A brief review of tests for normality. Am J Theor Appl Stat. (2016) 5:5. doi: 10.11648/j.ajtas.20160501.12
49. Peng, D. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. JASA. (2014) 109:1331. doi: 10.1111/jedm.12050
50. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. (2008) 40:879–91. doi: 10.3758/BRM.40.3.879
51. Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. (2003) 88:879–903. doi: 10.1037/0021-9010.88.5.879
52. Wen Z, Ye B. Analyses of mediating effects: the development of methods and models. Adv Psychol Sci. (2014) 5:5–19. doi: 10.3724/SP.J.1042.2014.00731
53. Chou FY, Armstrong HL, Wang L, Bacani N, Lachowsky NJ, Patterson TL, et al. A longitudinal analysis of cannabis use and mental health symptoms among gay, bisexual, and other men who have sex with men in Vancouver, Canada. J Affect Disord. (2019) 247:125–33. doi: 10.1016/j.jad.2019.01.015
54. Xiao L, Qi H, Wang YY, Wang D, Wilkinson M, Hall BJ, et al. The prevalence of depression in men who have sex with men (MSM) living with HIV: a meta-analysis of comparative and epidemiological studies. Gen Hosp Psychiatry. (2020) 66:112–9. doi: 10.1016/j.genhosppsych.2020.04.001
55. Newman PA, Reid L, Tepjan S, Akkakanjanasupar P. LGBT+ inclusion and human rights in Thailand: a scoping review of the literature. BMC Pub Health. (2021) 21:1816. doi: 10.1186/s12889-021-11798-2
56. Byne W. LGBT health: going strong as we begin our second year. LGBT Health. (2015) 2:1–2. doi: 10.1089/lgbt.2015.0010
57. Byne W. Resilience and action in a challenging time for LGBT rights. LGBT Health. (2018) 5:1–5. doi: 10.1089/lgbt.2017.0255
58. Chi Y, Huang D, Pachankis J, Valimaki M, Shen Y, Li X. Internalized sexual minority stigma is associated with HIV testing behavior among chinese men who have sex with men: a cross-sectional study. J Assoc Nurses AIDS Care. (2021) 32:578–88. doi: 10.1097/JNC.0000000000000205
59. Hong Y, Li X, Stanton B, Fang X, Lin D, Wang J, et al. Expressions of HIV-related stigma among rural-to-urban migrants in China. AIDS Patient Care STDS. (2008) 22:823–31. doi: 10.1089/apc.2008.0001
60. Tao J, Wang L, Kipp AM, Qian HZ, Yin L, Ruan Y, et al. Relationship of stigma and depression among newly HIV-diagnosed chinese men who have sex with men. AIDS Behav. (2017). doi: 10.1007/s10461-016-1477-8
61. Okonkwo N, Rwema JOT, Lyons C, Liestman B, Nyombayire J, Olawore O, et al. The relationship between sexual behavior stigma and depression among men who have sex with men and transgender women in kigali, rwanda: a cross-sectional study. Int J Ment Health Addict. (2022) 20:3228–43. doi: 10.1007/s11469-021-00699-5
62. Yang X, Li X, Qiao S, Li L, Parker C, Shen Z, et al. Intersectional stigma and psychosocial well-being among MSM living with HIV in Guangxi, China. AIDS Care. (2020) 32:5–13. doi: 10.1080/09540121.2020.1739205
63. Liu H, Hu Z, Li X, Stanton B, Naar-King S, Yang H. Understanding interrelationships among HIV-related stigma, concern about HIV infection, and intent to disclose HIV serostatus: a pretest-posttest study in a rural area of eastern China. AIDS Patient Care STDS. (2006) 20:133–42. doi: 10.1089/apc.2006.20.133
64. Cuadros DF, Abu-Raddad LJ. Geographical patterns of HIV sero-discordancy in High HIV prevalence countries in Sub-Saharan Africa. Int J Environ Res Public Health. (2016) 13:865. doi: 10.3390/ijerph13090865
65. Javanbakht M, Rosen A, Ragsdale A, Richter EI, Shoptaw S, Gorbach PM. Interruptions in mental health care, cannabis use, depression, and anxiety during the COVID-19 pandemic: findings from a Cohort of HIV-positive and HIV-negative MSM in Los Angeles, California. J Urban Health. (2022) 99:305–15. doi: 10.1007/s11524-022-00607-9
66. Sivasubramanian M, Mimiaga MJ, Mayer KH, Anand VR, Johnson CV, Prabhugate P, et al. Suicidality, clinical depression, and anxiety disorders are highly prevalent in men who have sex with men in Mumbai, India: findings from a community-recruited sample. Psychol Health Med. (2011) 16:450–62. doi: 10.1080/13548506.2011.554645
67. Yuvaraj A, Mahendra VS, Chakrapani V, Yunihastuti E, Santella AJ, Ranauta A, et al. HIV and stigma in the healthcare setting. Oral Dis. (2020) 26:103–11. doi: 10.1111/odi.13585
68. Duan QQ, Sheng L. Differential validity of SAS and SDS among psychiatric non-psychotic outpatients and their partners. Chinese Mental Health J. (2012) 26:676–9. doi: 10.3969/j.issn.1000-6729.2012.09.007
69. Yuan T, Mi H, Shui-Yuan X, Liang Z. Relation of quality of life to negative stressful life events and social support in rural elderly. Chinese Mental Health J. (2013) 27:734–8. doi: 10.3969/j.issn.1000-6729.2013.10.003
70. Bond FW, Hayes SC, Baer RA, Carpenter KM, Guenole N, Orcutt HK, et al. Preliminary psychometric properties of the acceptance and action questionnaire-II: a revised measure of psychological inflexibility and experiential avoidance. Behav Ther. (2011) 42:676–88. doi: 10.1016/j.beth.2011.03.007
71. Jing C, Yang J, Zhuo-Hong Z. Reliability and validity of the Chinese version of the acceptance and action questionnaire-second edition (AAQ-II) in college students. Chin Mental Health J. (2013) 27:873–7.
72. Haiping Z, Jian W. Social support and hope for haemodialysis patients. Chinese J Nurs. (2000) 5:49–51.
73. Berger BE, Ferrans CE, Lashley FR. Measuring stigma in people with HIV: Psychometric assessment of the HIV stigma scale. Res Nurs Health. (2001) 24:1–14. doi: 10.1037/t19334-000
74. Min X, Jin H, Honghong W, Min W, Xiaoping L, Liping W. Correlation between coping styles and social support in HIV-positive men who have sex with men. Chinese J AIDS STD. (2019) 25:476–9. doi: 10.13419/j.cnki.aids.2019.05.10
75. Xiao P. Under the Double Stigmas: HIV-Positive Gay Males' Experiences of HIV Infection Disclosure [Master thesis]. Guangzhou: South China Agricultural University (2017).
76. Yi L, Wu C. 'How can I fix my disrupted life?' Embodied experiences and biocitizenship among men who have sex with men living with HIV in China. Cult Health Sex. (2022) 21:1–15. doi: 10.1080/13691058.2022.2157884
77. Nyoni T, Nabunya P, Ssewamala FM. Perceived social support and psychological wellbeing of children orphaned by HIV/AIDS in Southwestern Uganda. Vulnerable Child Youth Stud. (2019) 14:351–63. doi: 10.1080/17450128.2019.1634855
78. Prado G, Feaster DJ, Schwartz SJ, Pratt IA, Smith L, Szapocznik J. Religious involvement, coping, social support, and psychological distress in HIV-seropositive African American mothers. AIDS Behav. (2004) 8:221–35. doi: 10.1023/B:AIBE.0000044071.27130.46
79. Banerjee N, Goodman ZT, McIntosh R, Ironson G. Cognition, coping, and psychological distress in HIV. AIDS Behav. (2022) 26:1074–83. doi: 10.1007/s10461-021-03462-y
80. Li J, Mo PK, Wu AM, Lau JT. Roles of self-stigma, social support, and positive and negative affects as determinants of depressive symptoms among hiv infected men who have sex with men in China. AIDS Behav. (2017) 21:261–73. doi: 10.1007/s10461-016-1321-1
81. Sharpe JD, Siegler AJ, Sanchez TH, Guest JL, Sullivan PS. Effects of mode of transportation on PrEP persistence among urban men who have sex with men. AIDS Care. (2023) 35:1411–9. doi: 10.1080/09540121.2023.2217375
82. Schnall R, Liu J, Kuhns LM, Pearson C, Scott Batey D, Bruce J, et al. A feasibility study of the use of HIV self-tests in young men who have sex with men. AIDS Care. (2023) 35:1279–84. doi: 10.1080/09540121.2022.2160864
83. Cabral HJ, Davis-Plourde K, Sarango M, Fox J, Palmisano J, Rajabiun S. Peer support and the HIV continuum of care: results from a multi-site randomized clinical trial in three urban clinics in the United States. AIDS Behav. (2018) 22:2627–39. doi: 10.1007/s10461-017-1999-8
84. Cluver LD, Sherr L, Toska E, Zhou S, Mellins CA, Omigbodun O, et al. From surviving to thriving: integrating mental health care into HIV, community, and family services for adolescents living with HIV. Lancet Child Adolesc Health. (2022) 6:582–92. doi: 10.1016/S2352-4642(22)00101-8
Keywords: HIV, men who have sex with men, social support, psychological flexibility, hope, depression
Citation: Wang R, Zheng F, Cao G, Goldsamt LA, Shen Y, Zhang C, Yi M, Peng W and Li X (2023) The relationship between social support and depression among HIV-positive men who have sex with men in China: the chain mediating role of psychological flexibility and hope. Front. Public Health 11:1271915. doi: 10.3389/fpubh.2023.1271915
Received: 03 August 2023; Accepted: 13 October 2023;
Published: 08 November 2023.
Edited by:
Ping Wu, Peking University, ChinaReviewed by:
Vsevolod Konstantinov, Penza State University, RussiaLu Yin, Chinese Academy of Medical Sciences and Peking Union Medical College, China
Copyright © 2023 Wang, Zheng, Cao, Goldsamt, Shen, Zhang, Yi, Peng and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xianhong Li, eGlhbmhvbmdfbGlAY3N1LmVkdS5jbg==