 Lilia Papst
Lilia Papst Christian Zickwolf
Christian Zickwolf Michael Käfer2
Michael Käfer2 Volker Beierlein
Volker Beierlein Volker Köllner
Volker Köllner- 1Psychosomatic Rehabilitation Research Group, Department of Psychosomatic Medicine, Center for Internal Medicine and Dermatology Charité – University Medicine Berlin, Berlin, Germany
- 2Mediclin Bliestal Clinics, Clinic for Psychosomatic Medicine, Blieskastel, Germany
- 3Department of Medical Psychology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
- 4Department of Psychosomatics and Behavioural Psychotherapy, Rehabilitation Centre Seehof, Teltow, Germany
Introduction: Work stress is a frequent factor in the development of depression. However, not only workplace environment, but also personal attitudes may affect stress experience. The aim of this study was to investigate the change sensitivity of occupational attitudes in psychosomatic inpatients and assess the relationship of changes to depressive symptom reduction.
Methods: The data set encompassed N = 1708 inpatients from two German psychosomatic rehabilitation clinics at admission and discharge. Responsivity of AVEM measures was evaluated by Bonferroni-corrected t-tests and Cohen’s dz effect sizes for paired samples. The relation of occupational behavior and experience patterns and depressive symptoms as assessed by the BDI-II questionnaire was calculated by Pearson correlation analysis of pre-post differential values.
Results: Changes in work attitudes were found on eight out of eleven AVEM subscales (Padj ≤ 0.001, Cohen’s dz = −0.45 to 0.43) and all AVEM coping styles. Most patients (57.4%) were classified to have a Burnout occupational coping style at admission. Changes following rehabilitation were most frequently observed from Burnout to Sparing coping styles (8.3%). Small to moderate associations between changes in occupational attitudes and depressive symptom reduction were found for all subscales (r = −0.39 to 0.25) except work ambition, and for occupational coping styles Burnout (r = 0.19), Sparing (r = −0.18) and Healthy (r = −0.10), but not Ambitious.
Discussion: The data support responsivity of occupational behavior and experience patterns within a psychosomatic rehabilitation setting. Correlations with depressive symptom reduction suggest that occupational attitudes are related but separate treatment targets.
1 Introduction
Work is the most frequently named source of stress in the general population in Germany (1). This poses a substantial public health issue as the presence of work-related stress increases the probability of a psychological diagnosis by two- to fourfold (2, 3), with depressive disorders being the most common diagnosis (4). Depressive disorders are associated with high personal as well as public costs. Among all diseases and all age groups, depression ranks 13th among the top causes of disease-adjusted life years globally (5). With a pooled life-time prevalence of a suicide attempt of 31%, it is associated with considerable mortality (6). Moreover, utilization of healthcare resources is increased in depressed individuals compared to the general population in Europe (RR = 5.4), as is the relative risk of work impairment (RR = 2.2) (7) and prolonged periods of sick leave (8).
Crucially, we distinguish two major aspects of work-related stress. On the one hand, there are external factors such as high workload, long working hours, lack of control, or job insecurity (9), i.e., factors describing objective aspects of occupational stress load. On the other hand, individual factors such as perfectionism (10, 11), over-commitment (12), or low self-efficacy (13, 14) may equally contribute to stress and depressive symptoms. Stress can therefore be understood as a transactional construct in that its experience is as much determined by the individual appraisal of a stressor – led by internalized beliefs and attitudes – as it is by the stressor itself (15).
The Assessment of Work-related Behavior and Experience Patterns questionnaire (AVEM) (16) allows for the evaluation of the individual’s beliefs and attitudes towards work. It distinguishes between Healthy (Type G), Sparing (Type S), Ambitious (Type A), and Burnout (Type B) patterns. The Healthy pattern is an indication of a healthy relationship towards work. It is characterized by strong but not excessive professional commitment, high resilience to stress and positive emotions. Individuals with a Sparing pattern report low work engagement but otherwise little issues in the other areas. The Ambitious pattern is marked by high effort and excessive job commitment that have no equivalent in life satisfaction. Finally, workers with a Burnout pattern experience being permanently overwhelmed, exhausted, and resigned. They are characterized by low work engagement, a lack in resistance to stress and strongly negative emotions. Previous investigations found that the Burnout pattern was positively associated with depressive symptoms and anxiety in medical students (17) and with self-reported stress experience in geriatric nurses (18).
Changes in occupational coping styles were observed following psychological interventions. One study on teachers revealed correlations between health improvement and decreases on AVEM scales willingness to work to exhaustion, striving for perfection, and the tendency for resignation in the face of failure, as well as with improved distancing ability, and inner calm and balance after participating in a Balint-type group intervention (19). In a randomized wait list control design, a pilot study on the effects of a mindfulness-based intervention on work-related behavior and experience patterns and depressive symptoms found that both depressive symptoms and individual attitudes such as willingness to work to exhaustion, striving for perfection, distancing ability, and inner calm and balance responded well to treatment, although overall risk patterns were less amenable to change (20).
In the current study, we investigated the responsivity of occupational behavior and experience patterns and their relationship to depressive symptom reduction in patients undergoing psychosomatic rehabilitation. Psychosomatic rehabilitation is a particular setting in that more than half of all patients may show a burnout-associated pattern (21) and are over-proportionately affected by symptom chronification and long sickness absence times (22, 23). Moreover, individuals with a burnout-associated coping style are discharged unfit for work significantly more often than individuals of any other work-related coping style (24). Using a large sample group, we therefore aimed to assess the extent of responsivity in occupational behavior and experience that may be expected in the psychosomatic rehabilitation setting. In addition, we investigated its relationship to depressive symptom reduction by assessing correlations with the BDI-II as a widely used measure of depressive symptoms. Due to previous findings (17, 18) we were particularly interested in the relationship of depressive symptom reduction and changes in the Burnout occupational coping style.
2 Materials and methods
The study was carried out as a multi-site correlation study in two German psychosomatic rehabilitation clinics.
2.1 Data acquisition
Data collection was performed as part of routine clinical diagnostics and rehabilitative interventions carried out according to German Pension Insurance (Deutsche Rentenversicherung) guidelines. Patients were asked for written broad consent on the use of clinical data for research purposes and informed about their rights to refuse data processing without indication of reasons or disadvantages to their treatment.
Approval by an ethics committee was waived in compliance with Brandenburg (§10 Datenschutz bei Forschungsvorhaben, https://bravors.brandenburg.de/de/verordnungen-215421) and Saarland (https://www.aerztekammer-saarland.de/files/164CC10E4F3/GV-0005%20Saarl%E4ndisches%20Krankenhausgesetz.pdf) state laws. A total of N = 1,708 psychosomatic patients (nclinic1 = 809, nclinic2 = 899) completed the self-report questionnaires Assessment of Work-related Behavior and Experience Patterns (Arbeitsbezogene Verhaltens- und Erlebensmuster, AVEM) (16) and the German version of the Beck Depression Inventory revised (BDI-II) (25) at admission (T0) and discharge (T1).
2.2 Measures
2.2.1 AVEM
The AVEM questionnaire captures factors work engagement, psychological resilience and work-related emotions. These arise from eleven scales: (1) work importance, (2) work ambition, (3) willingness to work to exhaustion, (4) striving for perfection, (5) ability to distance oneself, (6) tendency for resignation, (7) problem solving, (8) inner peace, (9) experience of success, (10) life satisfaction and (11) social support. Each scale is based on six items employing a 5-level response format (“strongly agree” to “strongly disagree”) with a range between 6 and 30. The AVEM has shown good reliability throughout all scales (Cronbach’s α between 0.78 and 0.87; split-half reliability between 0.76 and 0.90) and stability coefficients between 0.69 and 0.82 in a 3-month period. In addition, stanine patterns in the individual scales can be used to calculate probabilities for individuals to belong to work-related coping styles G (Healthy), S (Sparing), A (Ambitious), and B (Burnout) (16).
2.2.2 BDI-II
The Beck Depression Inventory (BDI-II) was developed to assess the severity of depressive symptoms. It comprises 21 questions on symptom frequency and severity within the last 2 weeks. Answers are given on a 4-level scale with response values ranging from 0 to 3. Item scores are summed up to a total score ranging from 0 to 63. The degree of depressive symptoms can be divided into four categories based on the BDI-II total score (0–13: no depression, 14–19: mild depression, 20–28: moderate depression, and 29–63: severe depression). The reliability (Cronbach’s alpha) was α = 0.93 in a sample of depressive patients in treatment, α = 0.92 in patients with primarily other mental disorders and α = 0.90 in a healthy population (25).
2.3 Data analysis
Data analysis was performed in R (Version 4.0.2) and R Studio (Version 1.3.959). Changes between T0 and T1 on AVEM scales were evaluated by t-tests for dependent samples followed by Bonferroni correction for multiple testing. Effect sizes were calculated using Cohen’s dz for paired samples. Patients’ AVEM work-related coping styles at admission as well as changes in classification at discharge were determined by probability scores that reflect the likelihood of group membership in the groups of the four types G/S/A/B. The highest probability scores, which indicate profile affiliation, were counted and converted into percentages, respectively. Associations between changes in AVEM scales and probability scores of work-related coping styles with changes in depressive symptoms as measured by BDI-II were investigated by calculating the Pearson correlation of their respective change scores (T1 – T0). For all statistical tests, the a priori defined α-error level to reject the null hypothesis H0 was P/Padj. > 0.05.
3 Results
3.1 Demographic data
Patient demographics are given in Table 1. The mean age in the sample group was 51.7 years (SD = 8.51).
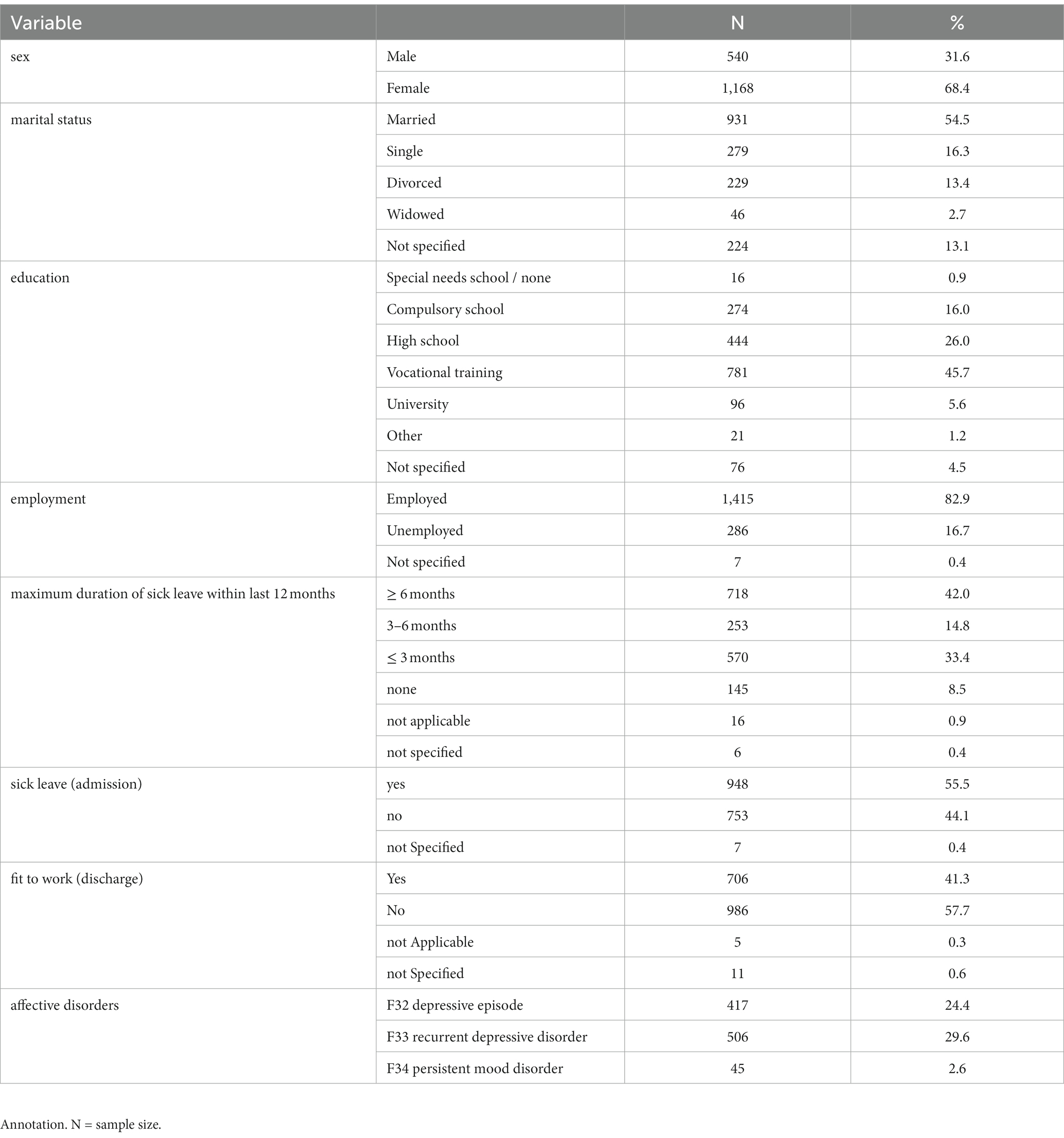
Table 1. Demographic data.
3.2 Occupational behavior and experience
Statistically significant changes between T0 and T1 were observed in 8 out of 11 AVEM scales following Bonferroni correction (work importance, work ambition, willingness to work to exhaustion, striving for perfection, ability to distance oneself, tendency for resignation, inner peace, and life satisfaction). Cohen’s dz effect sizes ranged from −0.45 (striving for perfection) to 0.43 (ability to distance oneself, life satisfaction). No statistically significant changes were observed on AVEM scales problem solving, experience of success and social support (Table 2).
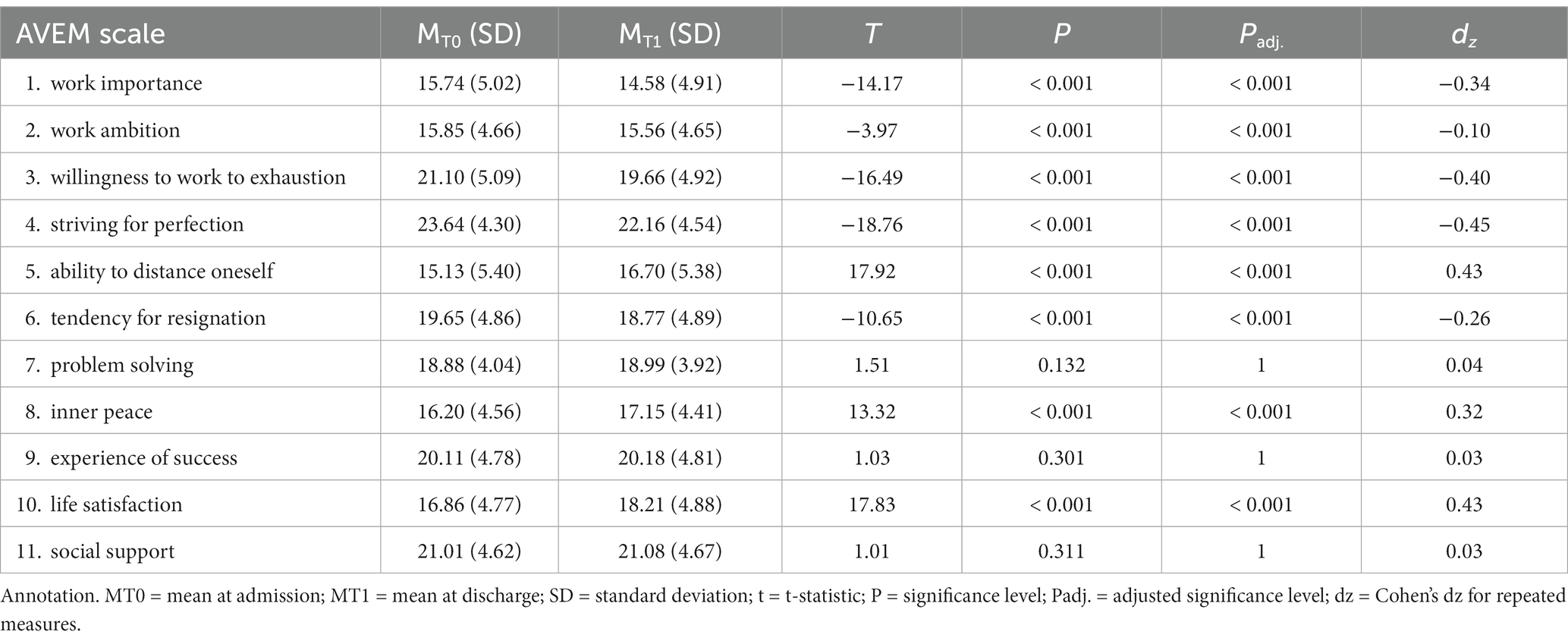
Table 2. Results of paired-sample t-Tests for changes in AVEM scores between admission (T0) and discharge (T1).
At 57.4%, the majority of psychosomatic patients presented with occupational risk pattern Type B (Burnout) at admission. The second most common pattern was risk pattern Type A (Ambitious) at 24.2%, followed by Type S (Sparing) at 13.3% and Type G (Healthy) at 5.1% (Figure 1). The highest increase (10.4%) towards discharge was observed in occupational pattern Type S, resulting in 23.7% of rehabilitants belonging to this group at T1. Out of these, 8.3% had been classified as Type B at admission. Type B remained the largest group at discharge (54.2%), with 45.8% of patients not having changed from T0, while 6.3% of scorers previously scored highest on Type A.
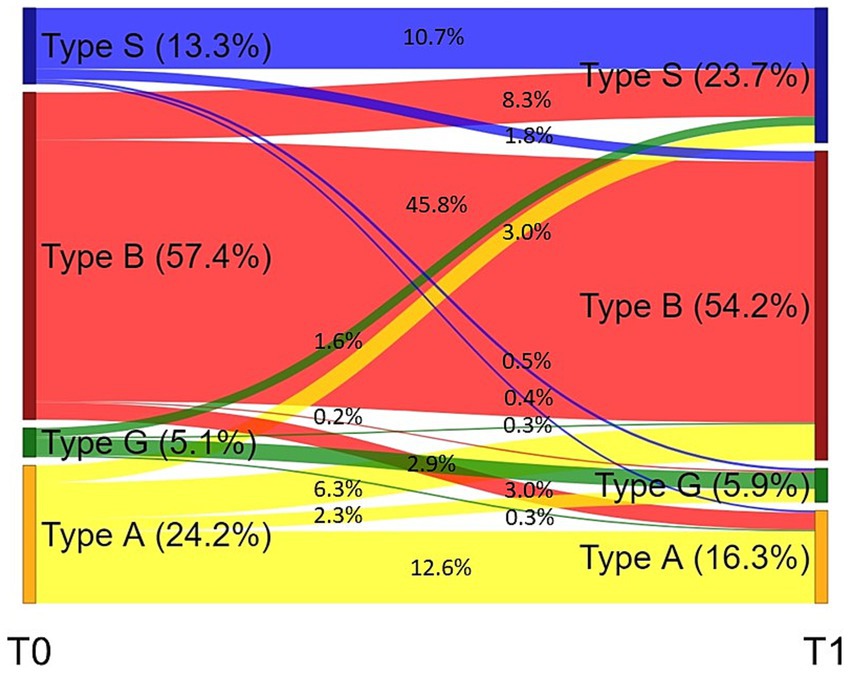
Figure 1. Sankey diagram of changes in occupational coping style from admission (T0) to discharge (T1). The diagram shows the percentage of patients belonging to occupational coping styles Type S (Sparing), Type B (Burnout), Type G (Healthy), and Type A (Ambitious) at admission (T0) and discharge (T1), as well as the percentage of patients changing occupational coping style between time points.
3.3 Depressive symptoms
A t-test for paired samples showed a statistically significant decrease in BDI-II scores (t (1707) = −46.4, p < 0.001, dz = −1.12) from admission (M = 24.7, SD = 12.0) to discharge (M = 13.7, SD = 12.4).
3.4 Association of changes in occupational behavior and experience with changes in depressive symptoms
Changes in BDI-II depressive symptom scores were statistically significantly associated with changes on all AVEM scales (−0.39 ≤ r ≤ 0.25, all p < 0.01) except for work ambition (Figure 2).
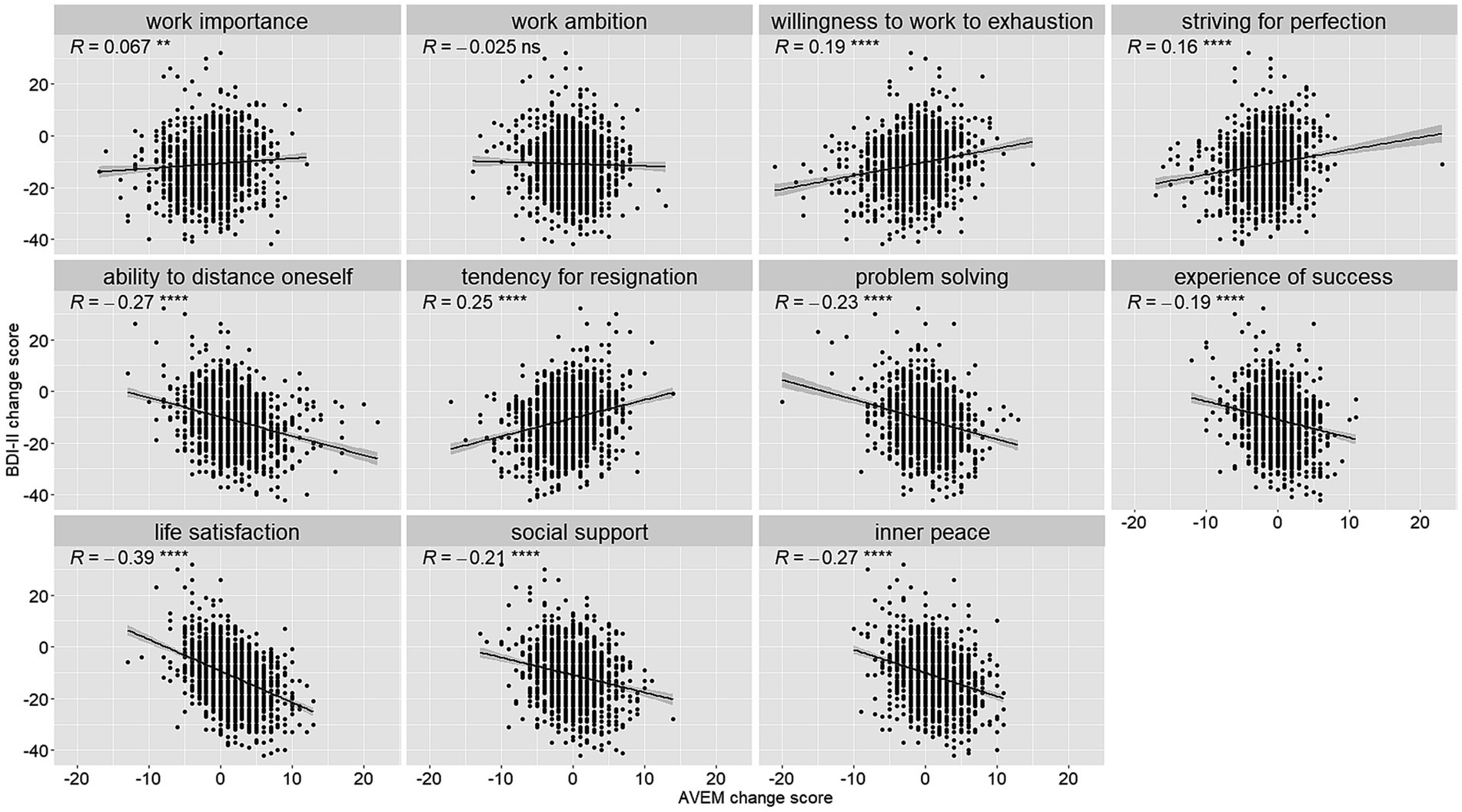
Figure 2. Scatter plots for AVEM scale and BDI-II change scores (T1-T0). Scatter plots show the relationship of change scores on AVEM scales with BDI-II change scores (T1-T0). Associations were determined by Pearson correlations, the level of statistical significance is indicated as ns = p > 0.05, ** = p < 0.01, **** = p < 0.0001.
Changes in BDI-II depressive symptoms were statistically significantly associated with changes in probability scores of all work-related coping patterns except for risk Type A (Figure 3).
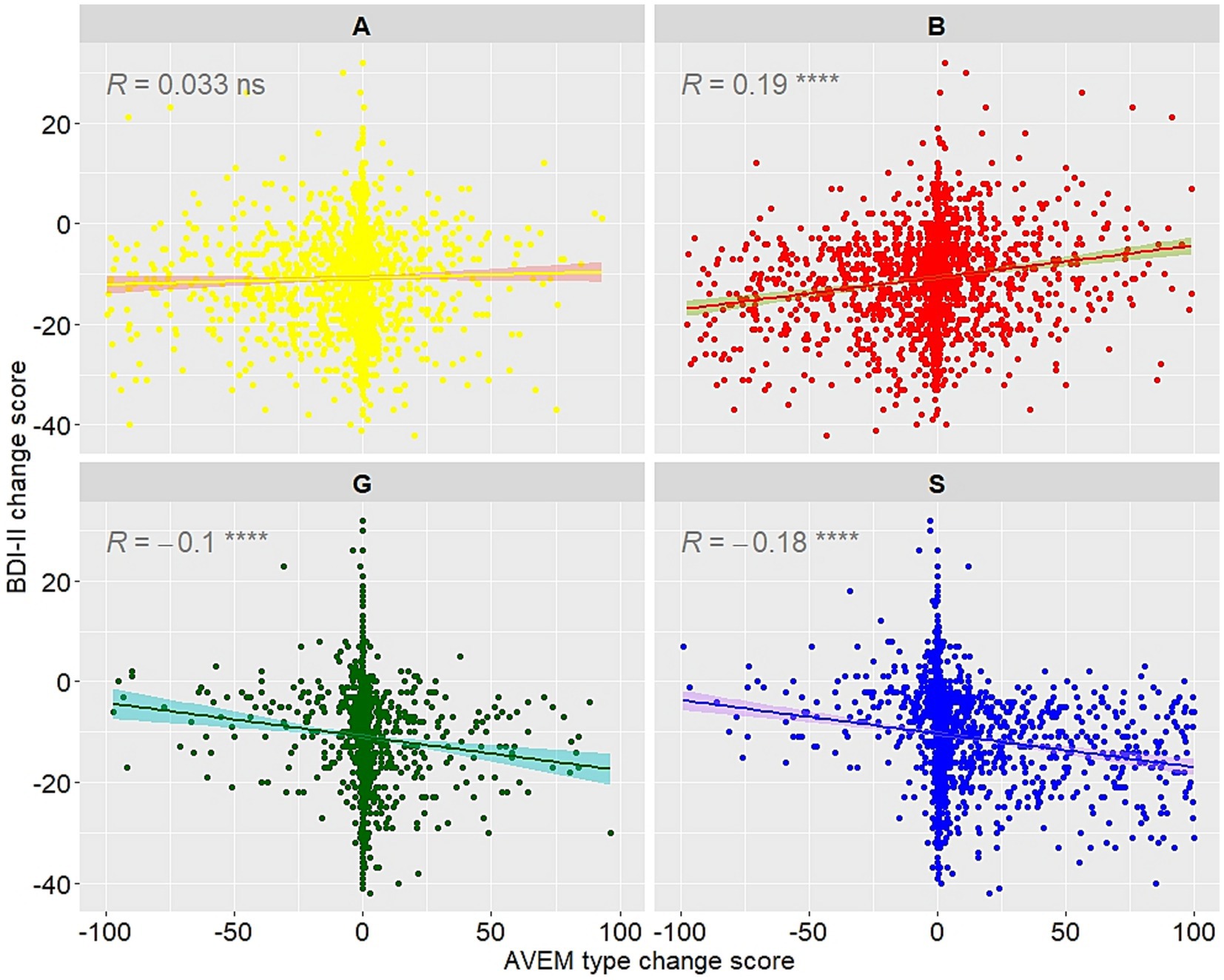
Figure 3. Correlation plots for AVEM work-related coping style probability change scores and BDI-II change scores (T1-T0). Scatter plots show the relationship of change scores in AVEM occupational coping style probabilities with BDI-II change scores (T1-T0). Associations were determined by Pearson correlations, the level of statistical significance is indicated as ns = p > 0.05, **** = p < 0.0001.
4 Discussion
Our findings indicate that AVEM scales are moderately responsive to change in a psychosomatic rehabilitation setting, which was evident from the pre-post differences in AVEM scales with small to medium effect sizes (0.10 < Cohen’s dz < 0.50). Regarding occupational coping styles, the majority of patients were classified as Risk Type B (57.4%) and Risk Type A (24.2%) at admission. Increases towards discharge were particularly noticeable in Type S (13.3% at T0 to 23.7% at T1). Despite the highest number of transitions from one occupational coping style to another (8.3% to Type S at T1), Type B remained the largest group at discharge. In addition, changes in AVEM scales and occupational coping styles showed small to medium correlations with reductions in depressive symptoms, except for AVEM scale work ambition and work-related coping style Type A (Ambitious). The directions of the correlations were consistent with their underlying concepts.
While an extensive research body on the malleability of occupational experience and behavior is missing, our findings fall in line with the effects reported by previous observational and intervention studies in clinical and non-clinical populations (19, 20). Reductions in work importance and work ambition not reported in previous studies may be a result of the specific population in psychosomatic rehabilitation. Psychosomatic patients frequently present with suffering from burnout due to overinvolvement with both wage labour as well as voluntary and care work (26). While a reduction on these traits may appear counterintuitive in the context of preserving and restoring earning capacity, in this specific group a reduced focus on work is important to prevent overexertion and foster healthy behaviors such as self-care. Indeed, previous investigations showed that interventions focusing on self-care yield results superior to interventions focussing on the improvement of stress resistance (27, 28).
Interestingly, some scales were consistently unresponsive in all investigations conducted to date, i.e., problem solving, experience of success and social support. We assume that the psychological variables underlying these scales may indeed be inaccessible to change experience during an inpatient treatment and are more likely to manifest as secondary effects in the long run. For instance, patients less willing to work to exhaustion may learn to correct imbalances in effort and reward (29), thus eventually experiencing more satisfaction with work and life in general. In addition, lower willingness to work to exhaustion may lead to a higher propensity to delegate tasks and thereby to a higher perception of social support. Moreover, patients may simply not encounter opportunities to experience improved problem-solving skills while still in rehabilitative treatment. Future investigations may address these possibilities by including a follow-up investigation.
Correlations of changes in occupational behavior and experience patterns and depressive symptoms moreover indicated largely independent constructs and not all expression patterns on the AVEM questionnaire were associated with changes in depressive symptom load. For instance, there was no association between changes in the scale work ambition and depressive symptoms. The scale is highly expressed in both Risk Type A and Type G indicating that its adaptiveness in the workplace is likely to be determined by accompanying factors. That is, Risk Type A may be maladaptive due to factors such as perfectionism or the inability to distance oneself from work rather than work ambition.
Meanwhile, the lack in association between changes in Risk Type A and depressive symptoms over the course of rehabilitation may be due to the specific change dynamics of the profile. That is, patients scoring highest on Risk Type A at admission were equally likely to develop towards both Type S and Risk Type B at discharge. While an adaptation of Type S may conceivably result in depressive symptom relief as patients practice more emotional distancing from work, a shift towards Risk Type B may indicate the breakdown of a dysfunctional coping style laying bare the underlying exhaustion and be associated with increased depressiveness. The latter trajectory of change may seem like a deterioration, but it is important to note that this breakdown may be a necessary development for some patients to eventually improve with respect to a healthier working style and better mental health (30).
Overall, the effects reported here may give researchers and practitioners a benchmark for the extent of changes in occupational beliefs and attitudes that may be expected in the psychosomatic rehabilitation setting. While effects were moderate, it is noteworthy that around 11% of psychosomatic inpatients changed dominant coping style from Risk Types B and A to Type S during rehabilitation. Given the degree of overall chronification in the study group and limited treatment duration of 5 weeks on average, this can be considered a rather high rate. The changes in overall work attitude are furthermore likely to translate into improved work performance (31) and reduced days of sick leave (32). These implications may be of interest to employers and policy makers as mental illness is responsible for both high direct financial costs such as medication, physician services and hospitalization as well as indirect costs through losses in productivity and income (33).
The low to moderate correlations with changes in depressive symptoms indicate that occupational beliefs and attitudes and depression need to be addressed individually within the context of rehabilitation as carry-over effects may be limited. This finding is in line with the separate coding of depressive disorders and the burnout syndrome within the International Classification of Disorders (ICD), which is supported by meta-analysis (34). However, it is unclear how well the constructs are treated as separate entities in practice, which may have potentially detrimental effects on the treatment outcome. Indeed, a review on intervention practices for depression in the workplace found none of the interventions to be effective in managing depression in this context (35). Perhaps interventions implementing work-related medical rehabilitation may be better tailored to suit the needs of these patients (36).
Lastly, while changes observed in our analyses are in line with previous investigations, a limitation of our study may be that we cannot exclude confounding effects owing to the test–retest stability of the AVEM questionnaire. In addition, the setting of the study did not allow for a randomized controlled trial with an untreated control group. Moreover, treatment plans included a disorder-specific group therapy for depressive disorders, but none for the burnout syndrome. Future studies on the topic may thus utilize more in-depth diagnostics to separate the constructs and include two treatment groups, i.e., offer manualized treatments for burnout and depressive disorders within a wait list control design in order to assess the effects on treatment outcomes.
5 Conclusion
Occupational behavior and experience patterns showed small to medium responsivity in a psychosomatic rehabilitation setting, with a particularly noteworthy rate of transitions from Type B to Type S occupational coping styles. Changes were accompanied by small but significant associations with a reduction in depressive symptoms. Occupational beliefs and attitudes can therefore be altered during standard rehabilitative treatment and change largely independently from depressive symptoms.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
LP: Conceptualization, Data curation, Formal analysis, Visualization, Writing – original draft, Writing – review & editing. CZ: Data curation, Investigation, Writing – review & editing. MK: Data curation, Investigation, Writing – review & editing, Project administration. VB: Data curation, Investigation, Validation, Writing – review & editing. VK: Conceptualization, Funding acquisition, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was performed within a grant by the German Federal Pension Fund (https://www.deutsche-rentenversicherung.de) awarded to VK (8011–106-31/31.127.2). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor WR declared a shared affiliation with the authors LP and VK at the time of review.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Meyer, B, Zill, A, and Dilba, D. Take it easy, Germany! TK study on the nation’s stress situation. Techniker Krankenkasse (2021). Available at: https://www.tk.de/techniker/unternehmensseiten/unternehmen/broschueren-und-mehr/stressstudie-2021-2026692. (Accessed January 10 2023).
2. Godin, I, Kittel, F, Coppieters, Y, and Siegrist, J. A prospective study of cumulative job stress in relation to mental health. BMC Public Health. (2005) 5:67. doi: 10.1186/1471-2458-5-67
3. Stansfeld, S, and Candy, B. Psychosocial work environment and mental health—a meta-analytic review. Scand J Work Environ Health. (2006) 32:443–62. doi: 10.5271/sjweh.1050
4. World Health Organization. (2017). Depression and Other Common Mental Disorders: Global Health Estimates. Geneva Available at: https://apps.who.int/iris/bitstream/handle/10665/254610/W?sequence=1 (Accessed January 10, 2023).
5. Vos, T, Lim, SS, Abbafati, C, Abbas, KM, Abbasi, M, Abbasifard, M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. (2020) 396:1204–22. doi: 10.1016/S0140-6736(20)30925-9
6. Dong, M, Zeng, L-N, Lu, L, Li, X-H, Ungvari, GS, Ng, CH, et al. Prevalence of suicide attempt in individuals with major depressive disorder: a meta-analysis of observational surveys. Psychol Med. (2019) 49:1691–704. doi: 10.1017/S0033291718002301
7. Jaffe, DH, Rive, B, and Denee, TR. The humanistic and economic burden of treatment-resistant depression in Europe: a cross-sectional study. BMC Psychiatry. (2019) 19:247. doi: 10.1186/s12888-019-2222-4
8. Demou, E, Smith, S, Bhaskar, A, Mackay, DF, Brown, J, Hunt, K, et al. Evaluating sickness absence duration by musculoskeletal and mental health issues: a retrospective cohort study of Scottish healthcare workers. BMJ Open. (2018) 8:e018085. doi: 10.1136/bmjopen-2017-018085
9. Stress Report Germany 2019. Mental demands, resources and well-being. 1st ed. Dortmund: Bundesanstalt für Arbeitsschutz und Arbeitsmedizin (2020).
10. Flett, GL, Nepon, T, Hewitt, PL, and Fitzgerald, K. Perfectionism, components of stress reactivity, and depressive symptoms. J Psychopathol Behav Assess. (2016) 38:645–54. doi: 10.1007/s10862-016-9554-x
11. Smith, MM, Sherry, SB, Ray, C, Hewitt, PL, and Flett, GL. Is perfectionism a vulnerability factor for depressive symptoms, a complication of depressive symptoms, or both? A meta-analytic test of 67 longitudinal studies. Clin Psychol Rev. (2021) 84:101982. doi: 10.1016/j.cpr.2021.101982
12. Khalid, A, Pan, F, Li, P, Wang, W, and Ghaffari, AS. The impact of occupational stress on job burnout among Bank employees in Pakistan, with psychological capital as a mediator. Front Public Health. (2020) 7:410. doi: 10.3389/fpubh.2019.00410
13. Lu, C, Siu, O, and Cooper, CL. Managers’ occupational stress in China: the role of self-efficacy. Personal Individ Differ. (2005) 38:569–78. doi: 10.1016/j.paid.2004.05.012
14. Yu, X, Wang, P, Zhai, X, Dai, H, and Yang, Q. The effect of Work stress on job burnout among teachers: the mediating role of self-efficacy. Soc Indic Res. (2015) 122:701–8. doi: 10.1007/s11205-014-0716-5
15. Lazarus, RS, and Folkman, S. Stress, appraisal, and coping. New York: Springer Publishing Company (2015).
16. Schaarschmidt, U, and Fischer, A. AVEM - an instrument for diagnosing different types of work - and health-related behavior and experience. ZDDP. (1997) 18:151–63.
17. Voltmer, E, Kötter, T, and Spahn, C. Perceived medical school stress and the development of behavior and experience patterns in German medical students. Med Teach. (2012) 34:840–7. doi: 10.3109/0142159X.2012.706339
18. Gutsch, C, Brinkmann, L, Frahm, G, Otto, AK, Bischoff, LL, Fenger, A, et al. Personal resources of geriatric nursing staff – results of a cross-sectional study. Gesundheitswesen. (2022) 84:301–9. doi: 10.1055/a-1341-1277
19. Braeunig, M, Pfeifer, R, Schaarschmidt, U, Lahmann, C, and Bauer, J. Factors influencing mental health improvements in school teachers. PLoS One. (2018) 13:e0206412. doi: 10.1371/journal.pone.0206412
20. Buxton, AE, Remmers, C, Köhling, J, and Michalak, J. Effects of a mindfulness-based depression treatment in a day hospital on vocational coping capacities of patients with Work-related conflicts. Verhaltenstherapie. (2022) 32:23–33. doi: 10.1159/000518693
21. Beierlein, V, Köllner, V, Neu, R, and Schulz, H. A screening-tool for three dimensions of Work-related behavior and experience patterns in the psychosomatic Rehabilitation – a proposal for a short-form of the occupational stress and coping inventory (AVEM-3D). Rehabilitation. (2016) 55:348–56. doi: 10.1055/s-0042-120232
22. Köllner, V. Rehabilitation in affective disorders. Rehabilitation. (2016) 55:395–410. doi: 10.1055/s-0042-118307
23. Brenner, L, Chrysanthou, S, and Köllner, V. When depression becomes chronic: possibilities and limits of rehabilitation. PiD - Psychotherapie im Dialog. (2021) 22:73–8. doi: 10.1055/a-1215-1996
24. Wittmann, C, Reischl, M, Welsch, K, Käfer, M, and Köllner, V. Diagnostic spectrum of somatic comorbidities in different AVEM patterns in psychosomatic rehabilitation. Z Psychosom Med Psychother. (2021) 114:58–67.
25. Hautzinger, M, Keller, F, and Kühner, C. Beck depression inventory: Revision (BDI-II). Frankfurt am Main: Harcourt Test Services (2006).
26. Köllner, V. The term burnout: meaningful use in psychotherapy. PiD - Psychotherapie im Dialog. (2018) 19:23–7. doi: 10.1055/a-0556-2420
27. Otto, J, and Linden, M. Regeneration orientation is better than resistance orientation in behaviour activation. Results from an intervention study with psychosomatic patients. Psychiatr Danub. (2017) 29:201–6. doi: 10.24869/psyd.2017.201
28. Wasilewski, J, Otto, J, and Linden, M. Promoting self-care instead of resistance orientation: therapeutic or side effect in regard to Work? Psychother. Psychosom. Med. Psychol. (2018) 68:417–22. doi: 10.1055/s-0043-118656
29. Siegrist, J, Starke, D, Chandola, T, Godin, I, Marmot, M, Niedhammer, I, et al. The measurement of effort–reward imbalance at work: European comparisons. Soc Sci Med. (2004) 58:1483–99. doi: 10.1016/S0277-9536(03)00351-4
30. Grumbach, K, Knox, M, Huang, B, Hammer, H, Kivlahan, C, and Willard-Grace, R. A longitudinal study of trends in burnout during primary care transformation. Ann. Fam. Med. (2019) 17:S9–S16. doi: 10.1370/afm.2406
31. Harari, D, Swider, BW, Steed, LB, and Breidenthal, AP. Is perfect good? A meta-analysis of perfectionism in the workplace. J Appl Psychol. (2018) 103:1121–44. doi: 10.1037/apl0000324
32. van de Leur, JC, Buhrman, M, Wallby, K, Karlström, A, and Johansson, F. Associations between improvements in psychological variables and subsequent sick leave among persons receiving a multimodal intervention for exhaustion disorder. BMC Public Health. (2023) 23:1–10. doi: 10.1186/s12889-023-16799-x
33. Gustavsson, A, Svensson, M, Jacobi, F, Allgulander, C, Alonso, J, Beghi, E, et al. Cost of disorders of the brain in Europe 2010. Eur Neuropsychopharmacol. (2011) 21:718–79. doi: 10.1016/j.euroneuro.2011.08.008
34. Koutsimani, P, Montgomery, A, and Georganta, K. The relationship between burnout, depression, and anxiety: a systematic review and meta-analysis. Front Psychol. (2019) 10:284. doi: 10.3389/fpsyg.2019.00284
35. Furlan, AD, Gnam, WH, Carnide, N, Irvin, E, Amick, BC III, DeRango, K, et al. Systematic review of intervention practices for depression in the workplace. J Occup Rehabil. (2012) 22:312–21. doi: 10.1007/s10926-011-9340-2
Keywords: depression, burnout, psychological, occupational health, occupational stress, working style
Citation: Papst L, Zickwolf C, Käfer M, Beierlein V and Köllner V (2023) Responsivity and relation to depressive symptoms of occupational behavior and experience patterns. Front. Public Health. 11:1271486. doi: 10.3389/fpubh.2023.1271486
Edited by:
Wulf Rössler, Charité University Medicine Berlin, GermanyReviewed by:
Jovica Jovanovic, University of Niš, SerbiaSílvio Manuel da Rocha Brito, Polytechnic Institute of Tomar (IPT), Portugal
Cristina Corina Bentea, Dunarea de Jos University, Romania
Copyright © 2023 Papst, Zickwolf, Käfer, Beierlein and Köllner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lilia Papst, bGlsaWEucGFwc3RAY2hhcml0ZS5kZQ==