 Liu Jia
Liu Jia Ming Ye
Ming Ye Hongliang Wang
Hongliang Wang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 12 October 2023
Sec. Occupational Health and Safety
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1270366
This article is part of the Research Topic Working and Absence from Work during the Pandemic View all 20 articles
Background: Facing the unknown virus, COVID-19 medical staff kept wearing thick personal protective equipment during their work in the early stage of the outbreak. The survey was designed to investigate the physical discomforts, the feeling of the work intensity and the related risk factors of the frontline medical staff during COVID-19 epidemic in the early outbreak.
Methods: An national survey was carried out in China from March 17th 2020 to March 20th 2020 by applying a standardized WeChat questionnaire survey. The doctors or nurses working in the wards for the confirmed COVID-19 patients on front-line were eligible to participate in the survey. Descriptive analysis and multivariate logistic regression analysis were used.
Results: A total number of 515 COVID-19 medical staff, including 190 physicians and 325 nurses participated in this survey. 375 medical staff (72.8%) experienced physical discomforts at work, mostly consist of dyspnea (45.8%), pain (41.0%), chest distress (24.1%), dizziness (18.8%), and weakness (17.5%), while wearing thick isolation clothes at work. The mean onset time and peak time of these symptoms were 2.4 h and 3.5 h after working, respectively. 337 medical staff (65.4%) suffered from sleep disorders. 51 medical staff (10%) were highly worried about being infected by COVID-19 even during their work breaks. 246 medical staffs (47.8%) felt high work intensity and the independent influential factors were the effective daily sleep time and anxiety levels at break time (p = 0.04).
Conclusion: The frontline medical staff during COVID-19 epidemic felt different physical discomforts when they wear thick isolation clothes at work in the early outbreak and they felt high work intensity. These precious data will help optimize the work management strategy to ensure the physical and mental health of medical staff in the face of similar outbreaks in future.
Since the outbreak of 2019 novel coronavirus (COVID-19) in Wuhan, Hubei province, China in late December 2019 (1–5), COVID-19 cases are still being continuously confirmed all over the world (6). This disease was transmitting so fast that the health-care system had been facing a sudden crisis. Moreover, the mortality rate was considerable in critically ill patients, as high as 61·5% (7). It is no doubt a huge challenge for medical staff never met before.
Reports showed that many health-care workers had been infected by COVID-19, and some of them had died (8–11). The mental stress of the health-care workers increased significantly when they cared for a large number of anxious COVID-19 patients with high-intensity work (12, 13). Lai (14) reported that health-care workers experiencing psychological burden, directly engaged in the diagnosis, treatment, and care for patients with COVID-19. Therefore, the medical staff for COVID-19 patients wore thick personal protective equipment (PPE) to protect themselves not being infected in the early outbreak in China, including three layers of medical hats, two layers of medical masks (N95 and surgical mask), eye protection (goggles or face screens), two layers of waterproof isolation clothing (a long fluid-impermeable gown and an operating coat), two layers of gloves, and two layers of shoe covers (Figure 1). This combination of PPE may cause increased work of breathing, reduced field of vision, muffled speech, difficulty hearing, and heat stress (15). Also, the medical staff who care for patients infected with COVID-19 are at a high risk of pressure injuries that caused by protective equipment in the prevention process (16). A growing concern regarding skin problems has been identified among healthcare workers during the COVID-19 pandemic (17–19), and the PPE-related skin injury can be serious (20). Daye (21) reported that skin problems were found to be 90.2%, the most common were dryness, itching, cracking, burning, flaking, peeling and lichenification. Severity of skin reaction was found to be significantly related to “hours per day of PPE use,” “consecutive days of PPE use,” and “female sex” (22). In the study by Proietti et al., prolonged use of PPE was a significant risk factor for developing skin related adverse events considering all the PPE considered (23). These occupational dermatoses caused by PPE in the ongoing COVID-19 pandemic are emerging occupational health challenges (24).

Figure 1. The COVID-19 medical staff wore thick personal protective equipment (PPE).
Therefore, the frontline medical staff faced great work stress and physical challenges during COVID-19 epidemic in the early outbreak. However, their physical discomforts and the feeling of the work intensity were not detailed described in previous studies. The survey was to comprehensively investigate their physical discomforts, the feeling of the work intensity and the related risk factors. When people face similar outbreaks in the future, these precious data may be learned from by the medical workers.
An anonymous investigation was carried out in China from March 17th 2020 to March 20th 2020 by applying a standardized anonymous WeChat questionnaire and the details are provided in the Supplementary material. The medical staff directly taking care of the confirmed COVID-19 patients were eligible to participate in the survey. The questionnaire consists of three parts. The first part is to collect basic characteristics, including demographic information and general work history. The second part is to investigate the physical discomforts of the COVID-19 medical staff at work. Other work related information were also included, such as work location, personal protective status, work time. The third part of the questionnaire collects information about the feeling of the work intensity and other mental state. Visual Analogue Scale (VAS) was used to evaluate the feeling of the work intensity levels, the anxiety levels of being infected by COVID-19 both at work and break time, and the adaptability levels to the COVID-19 related work (Figure 2). The feeling of the work intensity levels were further categorized into two groups according to the VAS scores, low-moderate intensity (VAS score: zero-five) and high intensity (VAS score: six-ten). Sleep disorder and the psychological interventions during the COVID-19 work period were also investigated.
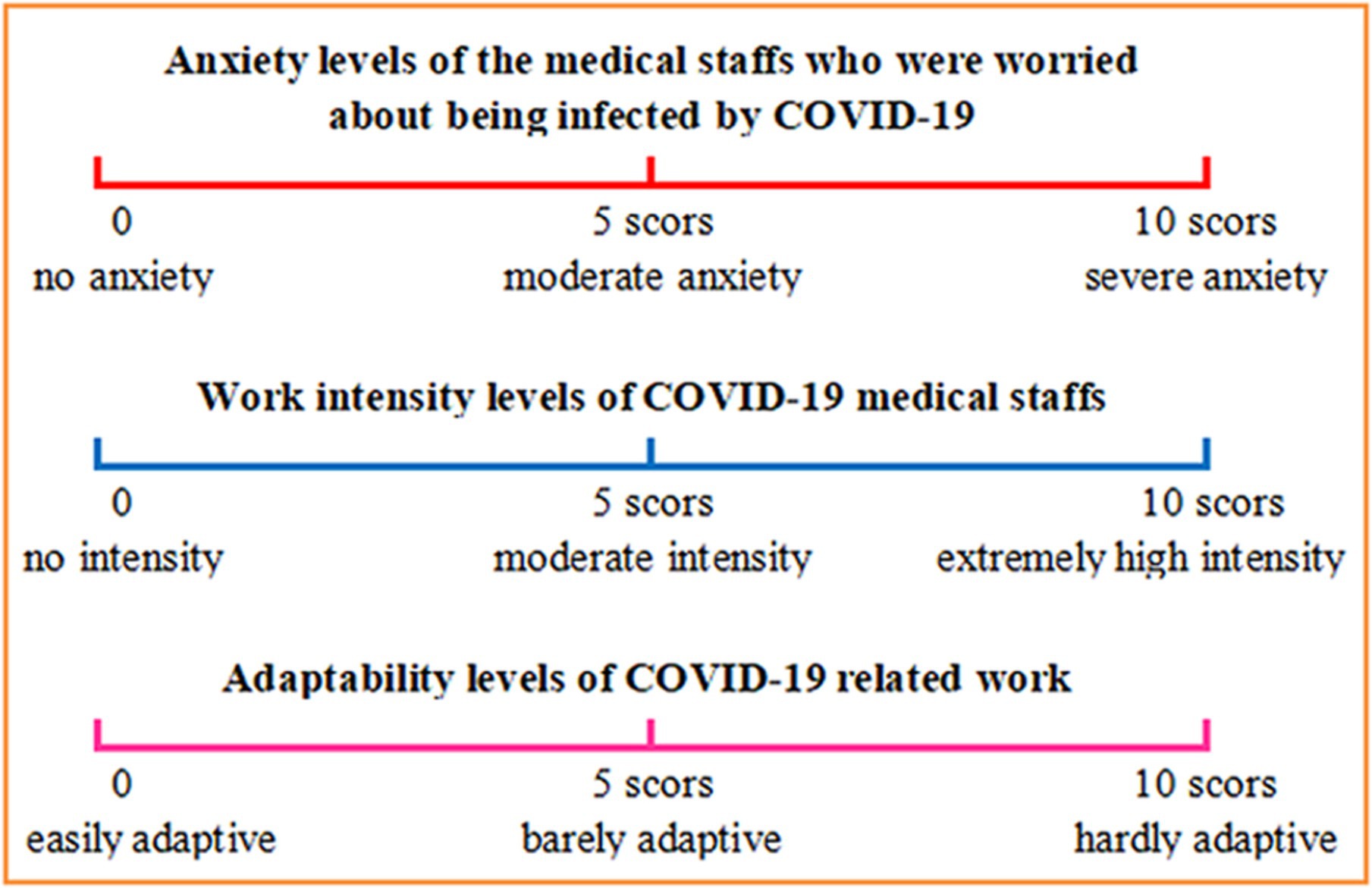
Figure 2. Visual Analogue Scale (VAS) used in the investigation.
Statistical analyses were performed using SPSS 22.0 software (SPSS Inc., Chicago, IL, United States). Quantitative variables were reported as mean with standard deviation or median with interquartile spacing (IQR). Qualitative data were described as values or percentages. A p < 0.05 was considered statistically significant.
Potential influential factors for feeling of the work intensity were identified firstly by univariate logistic regression analysis. Those factors with p < 0.05 were further included in a stepwise multivariate logistic regression analysis. Results were reported as the odds ratio (OR) with 95% confidence interval (CI).
A total number of 515 medical staff for COVID-19 [mean age, 34.5 (SD, 7.1) years; mean weight, 58.8 (SD, 18.0) kg; 190 (36.9%) physicians and 325 (63.1%) nurses], participated in this anonymous survey. As shown in Table 1, 389 medical staff (75.5%) came from Heilongjiang province, and 126 medical staff (24.5%) were from other provinces in China. 198 ICU medical staff accounted for 38.4% of all the participants in this survey. The rest of them were from respiratory department (63 medical staff, 12.2%), infectious disease department (15 medical staff, 2.9%), emergency department (11 medical staff, 2.1%), and other departments (228 medical staff, 44.3%). The medical staff mainly consisted of resident physicians and nurses (239 medical staff, 46.4%) and attending physicians and nurses (162 medical staff, 31.5%). Half of them had more than 10 years of work experience. The results showed that 39 medical staff (7.6%) had underlying physical diseases, such as hypertension or diabetes.

Table 1. Basic characteristics of 515 COVID-19 medical staffs.
Table 2 shows the work related information of the medical staff for COVID-19. All of them worn thick PPE at work (Figure 1). Most of them worked in Heilongjiang province (257 medical staff, 49.9%) or Hubei province (227 medical staff, 44.1%). None of the medical staff in this study was infected with COVID-19. Upon the time of the survey, these medical staff had continued working for COVID-19 patients for mean 26.3 [SD, 13.4] days. Nearly half of the medical staff (229 medical staff, 44.5%) had finished their rescue work for COVID-19 patients at the time of data collection.
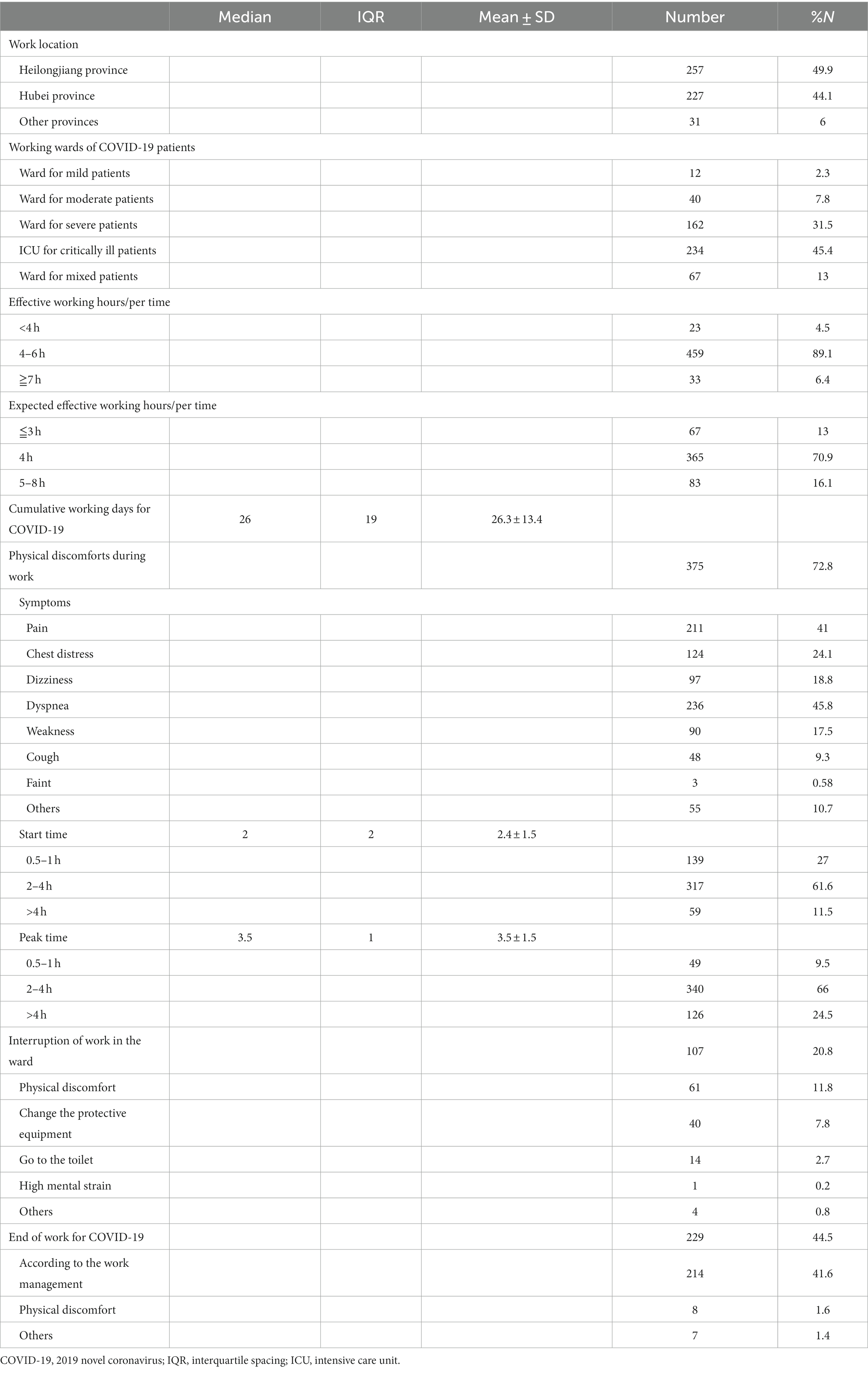
Table 2. Work status of 515 COVID-19 medical staffs.
375 medical staff (72.8%) felt physical discomforts while wearing thick isolation clothes at work, mostly consist of dyspnea (236 medical staff, 45.8%), pain (211 medical staff, 41.0%), chest distress (124 medical staff, 24.1%), dizziness (97 medical staff, 18.8%), and weakness (90 medical staff, 17.5%). The onset time [mean (SD)] and peak time [mean (SD)] of these symptoms were 2.4 [1.5] hours and 3.5 [1.5] hours after working, respectively. 27.0% of the medical staff felt obvious discomforts in 1 h. 20.8% of the medical staff had been forced to leave the wards during the working time because of several reasons, including feeling physical discomforts (61 medical staff, 11.8%), changing the protective equipment (40 medical staff, 7.8%), going to the toilet (14 medical staff, 2.7%), or other reasons (5 medical staff, 1.0%). The effective working hours/per time of 459 medical staff (89.1%) was four to 6 h, and 369 medical staff (70.9%) expected the effective working hours/per time to be 4 h.
The mental state of the medical staff for COVID-19 was shown in Table 3. 337 medical staff (65.4%) suffered from sleep disorders, and more than half of them had 6 h or less effective sleep per day. The VAS scores [mean (SD)] of anxiety levels of the medical staff who were worried about being infected by COVID-19 were 3.8 [2.9] at work and 2.6 [2.6] during break time, respectively. Only 131 medical staff (25%) were not anxious about the COVID-19 infection during breaks, whereas 51 medical staff (10%) were highly worried about being infected by COVID-19 even during breaks. 70 medical staff (13.6%) received psychological interventions during the COVID-19 work period. The VAS score (mean [SD]) of their feeling of the work intensity levels was 6.0 [2.2] and 246 medical staff (47.8%) felt high work intensity (VAS score ≧ six). However, most of the medical staff could adapt to the COVID-19 related work with the VAS score [mean (SD)]: 2.8[2.4] (Table 3). The feeling of the work intensity were further categorized into low-moderate intensity (VAS score: zero-five) and high intensity (VAS score: six-ten). Univariate and stepwise multivariate logistic regression analyses were performed to identify potential factors that were related to the work intensity. Comparisons were made between reference category and each of the remaining groups per characteristic.
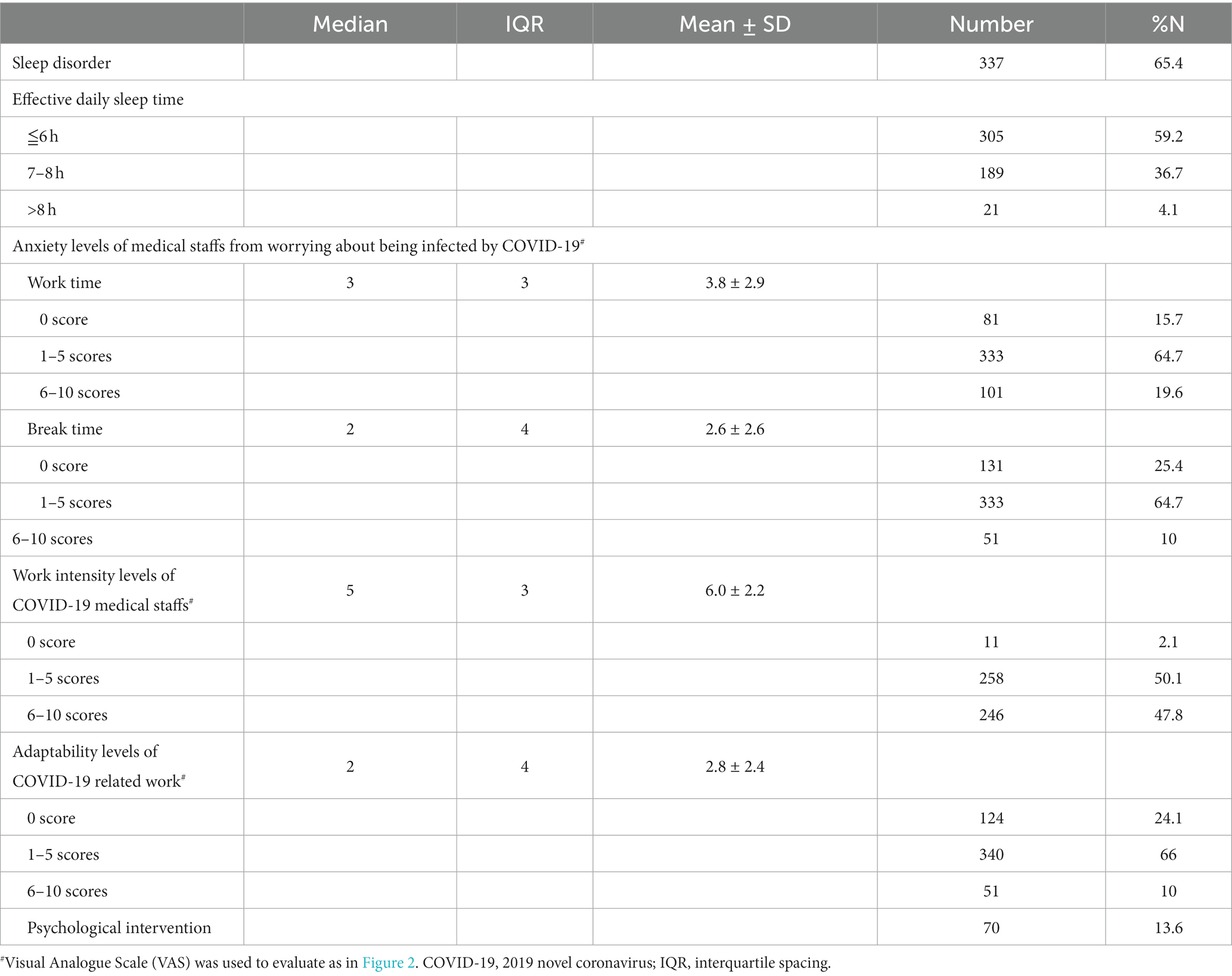
Table 3. Mental state of 515 COVID-19 medical staffs.
In Table 4, the results from univariate logistic regression analysis show that none of the basic characteristics of medical staff significantly affected their feeling of the work intensity. Work location, working wards for patients with different disease severity, effective working hours/per time, effective break time, and cumulative working days were also not associated with work intensity. In contrast, sleep disorder, effective daily sleep time, and anxiety levels of being infected by COVID-19 both at work time and break time were correlated with COVID-19 work intensity (p < 0.05). However, after adjusting for potential confounding factors through multivariate analysis, only effective daily sleep time and anxiety levels at break time were independent related factors for work intensity (p < 0.05). More specifically, the medical staff who were worried about being infected by COVID-19 with a VAS score of ≥six at break time felt a significantly higher work intensity than did those with a VAS score of zero (p = 0.04).
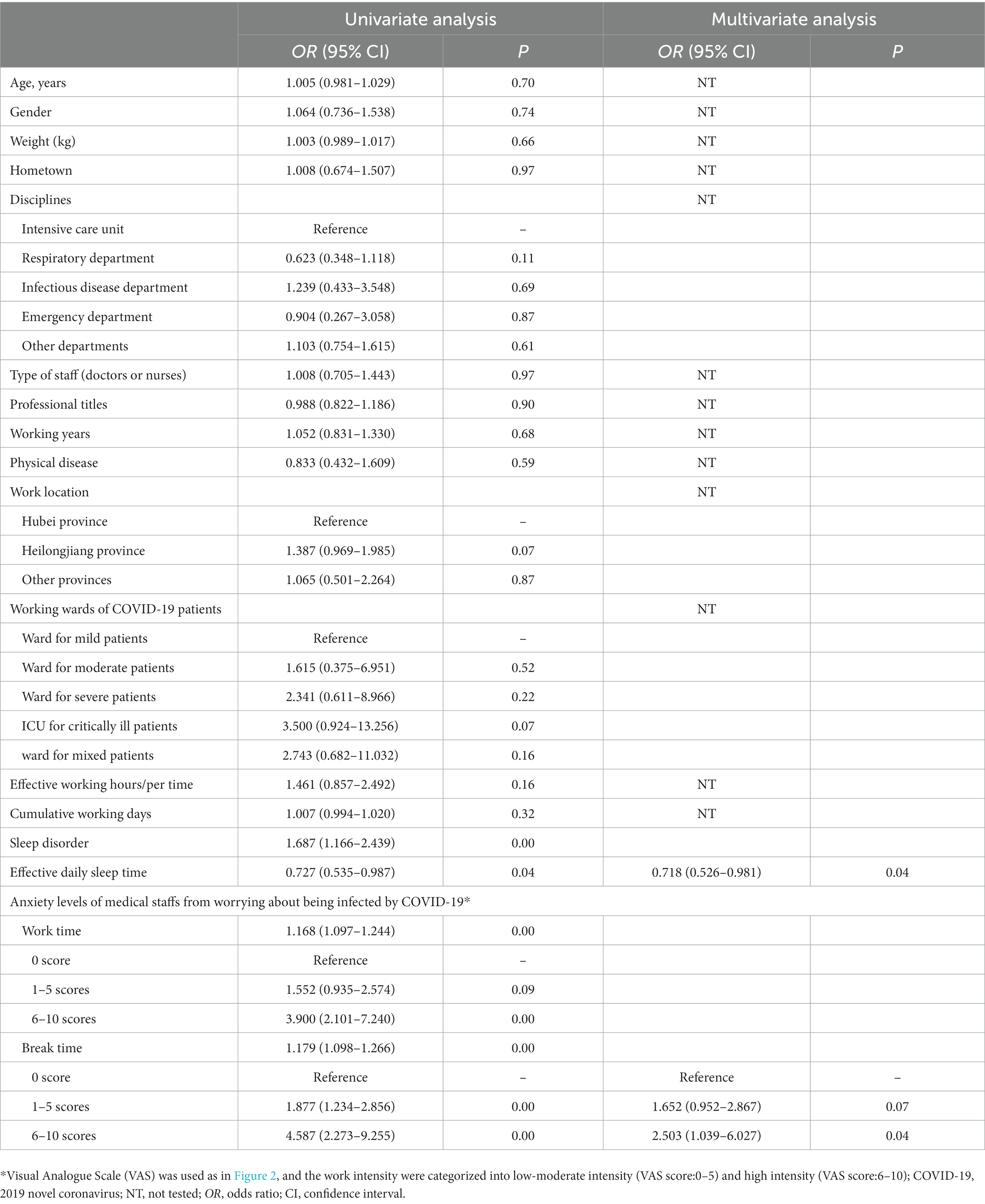
Table 4. Related factors for work intensity of COVID-19 medical staffs*.
As the continue increases of the confirmed COVID-19 cases worldwide, health-care systems globally could be operating at more than maximum capacity then and the health-care workers were every country’s most valuable resource (25). The medical staff were under great pressure in the early outbreak. In a district general hospital in south London, 128 (39%) of doctors experienced at least one sickness episode (26). However, there is no detailed description of the physical discomforts of the medical staff for COVID-19 during the early outbreak. Facing the unknown virus, COVID-19 medical staff kept wearing thick PPE during their work in the early stage of the outbreak. The survey showed that COVID-19 medical staff had different physical discomforts and they felt high work intensity.
The incidence of the physical discomforts related to PPE (such as dyspnea, pain, chest distress,etc.) was high in our survey and these effects were really inevitable. They are not caused by individual weakness; they are normal and expected reactions that any person will have when exposed to an unusual environment (15). Sahebi A also found that the prevalence of PPE-associated headache was relatively high, and the prevalence after and before the use of PPE was 48.27 and 30.47%, respectively (27). Adverse effects of PPE were associated with longer shift durations (28). In our study, PPE was worn for 4–6 h in 89.1% of the participants. Since the mean peak time of these physical discomforts was 3.5 h in our study, it indicates that the ideal working hours for the COVID-19 medical staff should be around 4 h every time. Also, 70.9% of them expected the effective working hours/per time to be 4 h. If PPE and human resources became sufficient, medical staff should take reasonable shifts to ensure physical health, otherwise the efficiency and quality of their work might decrease. However, due to the limitations of PPE or human resources, some of them had to work continuously for more than 6 h, which might easily cause distractions from their work. If working hours/per time cannot be shorten, some other work strategies should be applied.
Most of the medical staffs involved in the study worked for severe and critically ill patients, 162 medical staffs (31.5%) and 234 medical staffs (45.4%), respectively. When wearing thick isolate clothes, it is more difficult to perform procedures for COVID-19 patients, particularly for critically ill COVID-19 cases requiring complicated invasive procedures, such as tracheal intubation and arterial puncture/venipuncture. High frequency of performing these procedures would significantly increase the workload of the medical staffs and shorten their peak time of physical discomforts. Some measures might be beneficial for performing centralized treatments, and saving human resources, such as setting up a specialized procedure team, classifying patients being according to their severity. More work is needed to summarize and share the reasonable COVID-19 patient management.
The COVID-19 medical staff may experience considerable psychological distress due to providing direct patient care, vicarious trauma, quarantine, or self isolation (29, 30). Sleep disorders, in particular insomnia, have been commonly reported in frontline medical workers (31, 32). A meta-analysis, which included 98,533 medical staff from 71 studies, found the prevalence of insomnia among Chinese medical staff during the COVID-19 outbreak was generally high, especially for first-line workers (33). Our result showed that more than half of the medical staffs suffered from sleep disorders, and the effective daily sleep time was an independent influential factor for work intensity. These workers who had shorter effective daily sleep time during the COVID-19 work period felt higher work intensity. The medical staff were under high pressure even in the break time, which might be a major reason that lead to sleep disorder. The results indicated that only about 25% of medical staffs were not anxious about being infected by COVID-19, whereas 10% of them were highly worried about being infected by COVID-19 even during breaks. Moreover, anxiety levels of medical staffs at break time was an independent related factor for work intensity, and medical staffs with a VAS score of ≥six at break time felt a significantly higher work intensity than did those with a VAS score of zero. During the early phase of the pandemic in the Philippines, one-fourth of respondents reported moderate-to-severe anxiety and one-sixth reported moderate-to-severe depression and psychological impact (34). Besides, the workload of taking care of COVID-19 patients is very overwhelming, which challenges physical and mental limitations of medical staff all the time. Many other factors, such as change of living habit, food and environment in the isolation regions, would affect their effective sleep time, which in turn reduce the quality and productivity of their work. The risk of psychological effects from the COVID-19 pandemic is significant and manifests as stress, anxiety, depression, sleeplessness, and, in some cases, suicide (35). Therefore, it is of great importance to monitor the mental and psychological state of COVID-19 medical staffs, and provide professional psychological interventions as needed.
The psychological issues may induce healthcare workers experienced burnout during the pandemic. Ibar C found that 12% of the studied population showed burnout (52% doctors and residents, 19% nurses, 19% administrative personnel) and healthcare workers are subjected to increased levels of stress and burnout (36). Other than poor sleep, long working hours was a risk factor regarding an increase in personal burnout, work-related burnout levels and depression among health care professionals (37). The medical staff in China have been working for COVID-19 treatments in isolated areas for about 3 years. The mean continuous working days of medical staffs was 26.3 days during our survey time. However, health-care workers, unlike ventilators or wards, cannot run at 100% occupancy for long periods (25). Training workers about appropriate coping styles to adopt may be essential to enact prevention strategies to reduce burnout incidence in workers (38). Also, it is crucial to design an appropriate work schedule for medical staff, otherwise their health would be under risk and the work quality might also decrease.
Furthermore, Vancappel (39) reported that post-traumatic symptoms were also highly prevalent among French healthcare workers at the beginning of the COVID-19 crisis and they found a significant effect of the level of exposure to COVID-19 on affective symptoms. In the study by Oliver TL, the results implied that the COVID-19 pandemic had immediate effects on the eating patterns, weight changes, PA, and psychological factors of healthcare workers (40). In a large-scale survey during the COVID-19 pandemic, the results indicated that nurses who identified as women, working in ICUs, COVID-19 designated hospitals, and departments involved with treating COVID-19 patients had higher scores in mental health outcomes (41). Leaders within the hospital should investigate the working conditions and personal habits of all medical staff regularly and systematically during the COVID-19 pandemic and take any necessary preventive measures, such as improving resilience for nursing staff, in order to best care for their employees (37).
This study has several limitations. First, our investigation was carried out in the early stage of the outbreak of COVID-19 in China. The physical and mental state of the medical staff might be different in the later stage. Second, VAS score was first applied to evaluate the feeling of the work intensity of COVID-19 medical staff in this study. It was subjective and easy to implement, but further research is needed to confirm its effectiveness. Third, the details of the sleep disorders or the psychological intervention of the medical staff were not included in the questionnaire. In addition, this study fails to include the health-care workers who worked for fever clinics and who were in charge of infection surveillance. Their result of the data may be different.
The frontline medical staff for COVID-19 felt different physical discomforts when they wear thick isolation clothes at work in the early outbreak and they felt high work intensity. These precious data will help optimize the work management strategy to ensure the physical and mental health of medical staff in the face of similar outbreaks in future.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This study was deemed non-human-subjects research by the institutional Review Board (IRB) of the Harbin Medical University. As a result, ethical approval and written informed consent to participate in this study were not required for the study.
LJ: Data curation, Formal analysis, Writing – original draft, Writing – review & editing. MY: Data curation, Writing – review & editing. HoW: Data curation, Writing – review & editing. HuW: Data curation, Formal analysis, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors thank Shipeng Han for his help making the WeChat questionnaire. We also thank the medical staff who participated in this study during their busy jobs.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1270366/full#supplementary-material
1. Phelan, AL, Katz, R, and Gostin, LO. The novel coronavirus originating in Wuhan, China: challenges for Global Health governance. JAMA. (2020) 323:709–10. doi: 10.1001/jama.2020.1097
2. Chang, D, Lin, M, Wei, L, Xie, L, Zhu, G, Dela Cruz, CS, et al. Epidemiologic and clinical characteristics of novel coronavirus infections involving 13 patients outside Wuhan, China. JAMA. (2020) 323:1092–3. doi: 10.1001/jama.2020.1623
3. Wang, D, Hu, B, Hu, C, Zhu, F, Liu, X, Zhang, J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. (2020) 323:1061–9. doi: 10.1001/jama.2020.1585
4. Huang, C, Wang, Y, Li, X, Ren, L, Zhao, J, Hu, Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
5. Chen, N, Zhou, M, Dong, X, Qu, J, Gong, F, Han, Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. (2020) 395:507–13. doi: 10.1016/S0140-6736(20)30211-7
6. COVID-19 Dashboard. Center for Systems Science and Engineering (CSSE) at Johns Hopkins University, (2020). Available at: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6 (Accessed July 20, 2023).
7. Yang, X, Yu, Y, Xu, J, Shu, H, Xia, J, Liu, H, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet. Respir Med. (2020) 8:475–81. doi: 10.1016/S2213-2600(20)30079-5
8. Wei, XS, Wang, XR, Zhang, JC, Yang, WB, Ma, WL, Yang, BH, et al. A cluster of health care workers with COVID-19 pneumonia caused by SARS-CoV-2. J Microbiol Immunol Infect. (2021) 54:54–60. doi: 10.1016/j.jmii.2020.04.013
9. Zhan, M, Qin, Y, Xue, X, and Zhu, S. Death from Covid-19 of 23 health Care Workers in China. N Engl J Med. (2020) 382:2267–8. doi: 10.1056/NEJMc2005696
10. Himmelstein, DU, and Woolhandler, S. Health insurance status and risk factors for poor outcomes with COVID-19 among U.S. health care workers: a cross-sectional study. Ann Intern Med. (2020) 173:410–2. doi: 10.7326/M20-1874
11. Wander, PL, Orlov, M, Merel, SE, and Enquobahrie, DA. Risk factors for severe COVID-19 illness in healthcare workers: too many unknowns. Infect Control Hosp Epidemiol. (2020) 41:1369–70. doi: 10.1017/ice.2020.178
12. Wang, H, Wang, S, and Yu, K. COVID-19 infection epidemic: the medical management strategies in Heilongjiang Province, China. Crit Care. (2020) 24:107. doi: 10.1186/s13054-020-2832-8
13. Li, Y, Wang, H, and Jiao, J. The application of strong matrix management and PDCA cycle in the management of severe COVID-19 patients. Crit Care. (2020) 24:157. doi: 10.1186/s13054-020-02871-0
14. Lai, J, Ma, S, Wang, Y, Cai, Z, Hu, J, Wei, N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open. (2020) 3:e203976. doi: 10.1001/jamanetworkopen.2020.3976
15. Ruskin, KJ, Ruskin, AC, Musselman, BT, Harvey, JR, Nesthus, TE, and O'Connor, M. COVID-19, personal protective equipment, and human performance. Anesthesiology. (2021) 134:518–25. doi: 10.1097/ALN.0000000000003684
16. Yu, JN, Wu, BB, Feng, LP, and Chen, HL. COVID-19 related pressure injuries in patients and personnel: a systematic review. J Tissue Viability. (2021) 30:283–90. doi: 10.1016/j.jtv.2021.04.002
17. Silva, LFMD, Almeida, AGA, Pascoal, LM, Santos Neto, M, Lima, FET, and Santos, FS. Skin injuries due to personal protective equipment and preventive measures in the COVID-19 context: an integrative review. Lesões de pele por Equipamentos de Proteção individual e medidas preventivas no contexto da COVID-19: revisão integrativa. Rev Lat Am Enfermagem. (2022) 30:e3551. doi: 10.1590/1518-8345.5636.3551
18. Sarfraz, Z, Sarfraz, A, Sarfraz, M, Felix, M, Bernstein, JA, Fonacier, L, et al. Contact dermatitis due to personal protective equipment use and hygiene practices during the COVID-19 pandemic: a systematic review of case reports. Ann Med Surg. (2022) 74:103254. doi: 10.1016/j.amsu.2022.103254
19. Barnawi, GM, Barnawi, AM, and Samarkandy, S. The Association of the Prolonged use of personal protective equipment and face mask during COVID-19 pandemic with various dermatologic disease manifestations: a systematic review. Cureus. (2021) 13:e16544. doi: 10.7759/cureus.16544
20. Dowdle, TS, Thompson, M, Alkul, M, Nguyen, JM, and Sturgeon, ALE. COVID-19 and dermatological personal protective equipment considerations. Proc. (2021) 34:469–72. doi: 10.1080/08998280.2021.1899730
21. Daye, M, Cihan, FG, and Durduran, Y. Evaluation of skin problems and dermatology life quality index in health care workers who use personal protection measures during COVID-19 pandemic. Dermatol Ther. (2020) 33:e14346. doi: 10.1111/dth.14346
22. Nguyen, C, Young, FG, McElroy, D, and Singh, A. Personal protective equipment and adverse dermatological reactions among healthcare workers: survey observations from the COVID-19 pandemic. Medicine. (2022) 101:e29003. doi: 10.1097/MD.0000000000029003
23. Proietti, I, Borrelli, I, Skroza, N, Santoro, PE, Gualano, MR, Bernardini, N, et al. Adverse skin reactions to personal protective equipment during COVID-19 pandemic in Italian health care workers. Dermatol Ther. (2022) 35:e15460. doi: 10.1111/dth.15460
24. Keng, BMH, Gan, WH, Tam, YC, and Oh, CC. Personal protective equipment-related occupational dermatoses during COVID-19 among health care workers: a worldwide systematic review. JAAD Int. (2021) 5:85–95. doi: 10.1016/j.jdin.2021.08.004
25. Lancet, T. COVID-19: protecting health-care workers. Lancet. (2020) 395:922. doi: 10.1016/S0140-6736(20)30644-9
26. Khorasanee, R, Grundy, T, Isted, A, and Breeze, R. The effects of COVID-19 on sickness of medical staff across departments: a single Centre experience. Clin Med. (2021) 21:e150–4. doi: 10.7861/clinmed.2020-0547
27. Sahebi, A, Hasheminejad, N, Shohani, M, Yousefi, A, Tahernejad, S, and Tahernejad, A. Personal protective equipment-associated headaches in health care workers during COVID-19: a systematic review and meta-analysis. Front Public Health. (2022) 10:942046. doi: 10.3389/fpubh.2022.942046
28. Tabah, A, Ramanan, M, Laupland, KB, Buetti, N, Cortegiani, A, Mellinghoff, J, et al. Personal protective equipment and intensive care unit healthcare worker safety in the COVID-19 era (PPE-SAFE): an international survey. J Crit Care. (2020) 59:70–5. doi: 10.1016/j.jcrc.2020.06.005
29. Wu, PE, Styra, R, and Gold, WL. Mitigating the psychological effects of COVID-19 on health care workers. CMAJ. (2020) 192:E459–60. doi: 10.1503/cmaj.200519
30. Kang, L, Li, Y, Hu, S, Chen, M, Yang, C, Yang, BX, et al. The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. Lancet. Psychiatry. (2020) 7:e14. doi: 10.1016/S2215-0366(20)30047-X
31. Ferini-Strambi, L, Zucconi, M, Casoni, F, and Salsone, M. COVID-19 and sleep in medical staff: reflections, clinical evidences, and perspectives. Curr Treat Options Neurol. (2020) 22:29. doi: 10.1007/s11940-020-00642-4
32. Tang, L, Yu, XT, Wu, YW, Zhao, N, Liang, RL, Gao, XL, et al. Burnout, depression, anxiety and insomnia among medical staff during the COVID-19 epidemic in Shanghai. Front Public Health. (2023) 10:1019635. doi: 10.3389/fpubh.2022.1019635
33. Hu, N, Deng, H, Yang, H, Wang, C, Cui, Y, Chen, J, et al. The pooled prevalence of the mental problems of Chinese medical staff during the COVID-19 outbreak: a meta-analysis. J Affect Disord. (2022) 303:323–30. doi: 10.1016/j.jad.2022.02.045
34. Tee, ML, Tee, CA, Anlacan, JP, Aligam, KJG, Reyes, PWC, Kuruchittham, V, et al. Psychological impact of COVID-19 pandemic in the Philippines. J Affect Disord. (2020) 277:379–91. doi: 10.1016/j.jad.2020.08.043
35. Shah, M, Roggenkamp, M, Ferrer, L, Burger, V, and Brassil, KJ. Mental health and COVID-19: the psychological implications of a pandemic for nurses. Clin J Oncol Nurs. (2021) 25:69–75. doi: 10.1188/21.CJON.69-75
36. Ibar, C, Fortuna, F, Gonzalez, D, Jamardo, J, Jacobsen, D, Pugliese, L, et al. Evaluation of stress, burnout and hair cortisol levels in health workers at a university hospital during COVID-19 pandemic. Psychoneuroendocrinology. (2021) 128:105213. doi: 10.1016/j.psyneuen.2021.105213
37. Chu, WM, Ho, HE, Lin, YL, Li, JY, Lin, CF, Chen, CH, et al. Risk factors surrounding an increase in burnout and depression among health care professionals in Taiwan during the COVID-19 pandemic. J Am Med Dir Assoc. (2023) 24:164–170.e3. doi: 10.1016/j.jamda.2022.12.010
38. Rossi, MF, Gualano, MR, Magnavita, N, Moscato, U, Santoro, PE, and Borrelli, I. Coping with burnout and the impact of the COVID-19 pandemic on workers' mental health: a systematic review. Front Psych. (2023) 14:1139260. doi: 10.3389/fpsyt.2023.1139260
39. Vancappel, A, Jansen, E, Ouhmad, N, Desmidt, T, Etain, B, Bergey, C, et al. Psychological impact of exposure to the COVID-19 sanitary crisis on French healthcare workers: risk factors and coping strategies. Front Psych. (2021) 12:701127. doi: 10.3389/fpsyt.2021.701127
40. Oliver, TL, Shenkman, R, Diewald, LK, Bernhardt, PW, Chen, MH, Moore, CH, et al. A year in the life of U.S. frontline health care workers: impact of COVID-19 on weight change, physical activity, lifestyle habits, and psychological factors. Nutrients. (2022) 14:4865. doi: 10.3390/nu14224865
Keywords: COVID-19, medical staff, physical discomforts, work intensity, risk factors
Citation: Jia L, Ye M, Wang H and Wang H (2023) Physical discomforts, feeling of the high work intensity and the related risk factors of the frontline medical staff during COVID-19 epidemic: an early-outbreak, national survey in China. Front. Public Health. 11:1270366. doi: 10.3389/fpubh.2023.1270366
Edited by:
Milan Milosevic, University of Zagreb, CroatiaReviewed by:
Salvatore Zaffina, Bambino Gesù Children's Hospital (IRCCS), ItalyCopyright © 2023 Jia, Ye, Wang and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huaiquan Wang, d2hxMTY4OEAxMjYuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.