 Josefa L. Martinez-Brockman1,2*
Josefa L. Martinez-Brockman1,2* Amber Hromi-Fiedler3
Amber Hromi-Fiedler3 Deron Galusha1,2
Deron Galusha1,2 Carol Oladele1,2
Carol Oladele1,2 Lisbette Acosta1
Lisbette Acosta1 O. Peter Adams4Rohan G. Maharaj5
O. Peter Adams4Rohan G. Maharaj5 Cruz M. Nazario6Maxine Nunez7Marcella Nunez-Smith1,2
Cruz M. Nazario6Maxine Nunez7Marcella Nunez-Smith1,2 Rafael Pérez-Escamilla3 and on behalf of the ECHORN Writing Group
Rafael Pérez-Escamilla3 and on behalf of the ECHORN Writing Group- 1Equity Research and Innovation Center, Yale School of Medicine, New Haven, CT, United States
- 2Department of Internal Medicine, Yale School of Medicine, New Haven, CT, United States
- 3Department of Social and Behavioral Sciences, Yale School of Public Health, New Haven, CT, United States
- 4Department of Family Medicine, Faculty of Medical Sciences, University of the West Indies, Cave Hill, Cave Hill, Barbados
- 5Department of Paraclinical Sciences, University of the West Indies, Saint Augustine, Trinidad and Tobago
- 6Department of Biostatistics and Epidemiology, Graduate School of Public Health, University of Puerto Rico at Medical Sciences Campus, San Juan, Puerto Rico
- 7School of Nursing, University of the Virgin Islands, St. Thomas, US Virgin Islands
Background: Globally, 1.3 billion people were considered food insecure as of 2022. In the Caribbean region, the prevalence of moderate or severe food insecurity was 71.3% as of 2020, the highest of all subregions in Latin America. Experienced based measurement scales, like the Latin American and Caribbean Food Security Scale, are efficient measurement tools of food insecurity used globally. The Eastern Caribbean Health Outcomes Research Network (ECHORN) Cohort Study is a population-based longitudinal cohort study in the two Caribbean U.S. territories of Puerto Rico and the U.S. Virgin Islands, as well as in Barbados and Trinidad & Tobago. The purpose of this research was to examine the demographic, psychosocial, behavioral, and environmental risk factors associated with household food insecurity (HFI) among adults ≥40 years of age in the ECHORN cohort.
Methods: A cross-sectional analysis of baseline ECHORN cohort study data was conducted. The primary outcome was household food insecurity (none, mild, moderate/severe). A total of 16 known and potential risk factors were examined for their association with HFI. The ANOVA and chi-square statistics were used in bivariate analysis. Ordinal logistic regression was used for the multivariable and sex stratified analyses.
Results: More than one-quarter of the sample (27.3%) experienced HFI. In bivariate analyses, all risk factors examined except for sex, were significantly associated with HFI status. In the multivariable analysis, all variables except sex, education, marital status, smoking status, and residing in Puerto Rico were significant predictors of HFI in the adjusted model. In sex stratified analysis, depression, food availability, self-rated physical health, and island site were significantly associated with increased odds of worsening HFI for women, but not for men. Source of potable water was an important risk factor for both men and women.
Discussion: The prevalence of HFI in the ECHORN cohort study is comparable to other studies conducted in the region. While women did not have an increased risk of HFI compared to men, a different set of risk factors affected their vulnerability to HFI. More research is needed to understand how water and food security are interrelated in the ECHORN cohort.
1 Introduction
The World Health Organization (WHO) defines food security as “a situation that exists when all people, at all times, have physical, social and economic access to sufficient, safe and nutritious food that meets their dietary needs and food preferences for an active and healthy life” (1). Globally, 1.3 billion people were considered food insecure as of 2022, with an increase of nearly 119 million people due to the pandemic in 2021 (2). Measuring food insecurity through household food insecurity (HFI) experience-based measurement scales continues to be the method of choice to assess food insecurity globally, compared to other methods like household expenditure surveys or dietary intake assessments (3). In adults worldwide, HFI has been associated with chronic diseases such as diabetes (4–6), hypertension (7) and overweight (8). In women and adults in low-income households, there is robust evidence of an association between HFI and malnutrition globally (8–13). Among children, HFI has been associated with childhood obesity (4, 14), stunting (15), malnutrition (15–18) as well as disability and/or injury (4).
In the Caribbean region, the prevalence of moderate or severe food insecurity was 71.3 percent in 2020, the highest of all subregions in Latin America when measured using the Food Insecurity Experience Scale (19). In this region, HFI has been associated with HIV/AIDS in Haitian adults (20, 21), HIV in adults in the Dominican Republic (22), and malnutrition in adults from both the Dominican Republic and Haiti (6, 22). HFI is associated with lower household income, physical disability, and having an underweight body mass index among adults in Trinidad & Tobago (23, 24). In Barbados, HFI is associated with disability and/or injury (4), and in Puerto Rico the Covid-19 pandemic worsened food insecurity in many households (24). In children in the Caribbean, HFI has been associated with child disability, family divorce or separation, and increased child healthcare needs in Caribbean households with children in the Eastern Caribbean Child Vulnerability Study (4). Among adolescents in a five-country study that included Trinidad & Tobago, HFI was associated with negative psychological and behavioral outcomes (25). In rural Haiti, HFI was associated with childhood malaria (26).
Household food insecurity must be considered in the context of water security (27–29). There is a consistent relationship between water and food insecurity. Indeed, in a study conducted in 27 sites in 21 low-and middle-income countries, the Household Water Insecurity Experiences (HWISE) Scale revealed an association between increasing rates of household water insecurity and decreasing availability and quality of food in the household (27, 28, 30). HFI is exacerbated by water insecurity through the direct limitation of food options that can be prepared due to a lack of potable water (31) and by directly limiting the budget for household food items due to the need to pay for treatment of potable water (28). Water insecurity is also associated with non-communicable diseases such as malaria, obesity, diabetes, and hypertension (32).
Existing cross-sectional and prospective epidemiologic studies that have examined risk factors for food insecurity are primarily focused on the United States or other high resource settings. In the U.S. these risk factors include having a lower level of education, never being married or being divorced/separated, being young, renting, or being African American or Hispanic (33, 34). Few epidemiologic studies exist that examine risk factors for food insecurity in the Caribbean region. The Eastern Caribbean Health Outcomes Research Network (ECHORN) Cohort Study is an ongoing population-based longitudinal cohort study designed to follow adults 40 years of age and older in the two Caribbean U.S. territories of Puerto Rico and the U.S. Virgin Islands, as well as in the nations of Barbados and Trinidad & Tobago. Its primary purpose is to measure the prevalence and incidence of diabetes, cancer, and heart disease as well as known and potential risk factors including food insecurity. The Caribbean region has the highest burden of non-communicable diseases, compared to Latin America, the U.S., and Canada. In fact, the U.S. Caribbean territories of Puerto Rico and the U.S. Virgin Islands are home to nearly 3.4 million Americans, yet we know very little regarding the risk factors for HFI and the relationship between HFI and non-communicable diseases on these islands. ECHORN is the first multi-country, intergenerational cohort study in the region designed to examine non-communicable disease outcomes and their known and potential risk factors. The purpose of this research was to examine the demographic, psychosocial, behavioral, and environmental risk factors associated with household food insecurity among adults ≥40 years of age in the ECHORN cohort.
2 Methods
The ECHORN study protocol was reviewed and approved by the Institutional Review Boards at Yale University, the University of Puerto Rico Medical Sciences Campus, the University of the Virgin Islands, the University of the West Indies – Cave Hill, and St. Augustine (Trinidad) campuses, and the Ministry of Health of Trinidad and Tobago. All participants provided their fully informed consent prior to initiating study procedures. The current analysis was approved by the Data Access and Scientific Review committee of the ECHORN Cohort Study.
2.1 Sample
Eligible participants at baseline were 40 years of age and older, English or Spanish speaking, able to provide informed consent, non-institutionalized at the time of data collection, had reliable contact/residential information, were semi-permanent or permanent residents of the island for 10 or more years, and had no plans to permanently relocate in the next 5 years.
The sampling methodology for the baseline ECHORN cohort (n = 2,961) has been described in detail elsewhere (35). Briefly, in Trinidad, Puerto Rico, and Barbados, stratified multistage probability sampling was used to empanel the baseline cohort between 2013 and 2018. In the US Virgin Islands simple random sampling was used across the islands of St. Thomas St. Croix and Saint John. Participants visited a community assessment center, centrally located on each island site, for their baseline assessment. After informed consent was obtained, participants were asked to complete a health survey, a clinical assessment, and provide a blood sample for immediate testing to identify markers of disease. The health survey consisted of questions pertaining to health status and chronic disease history, health behaviors, diet, household food insecurity, access to health care, migration history, social support, health networks, neighborhood factors, and demographic information. The cross-sectional sample used in this analysis included all participants with household food insecurity data at baseline and non-missing values for the examined risk factors (n = 1,939).
2.2 Primary outcome
The primary outcome was household food insecurity as measured by the Latin American and Caribbean Food Security Scale (or ELCSA by its Spanish acronym) (34). The 9-item ELCSA scale for adults (Table 1) is a household-level experiential food security scale and is scored by assigning 1-point to each affirmatively answered yes/no question. Next, responses are divided into the following categories: food secure (score of 0), mild food insecurity (score of 1–3), moderate (4–6), and severe food insecurity (score of 7–9). Respondents with moderate and severe food insecurity scores (4–9) were grouped into a single category.
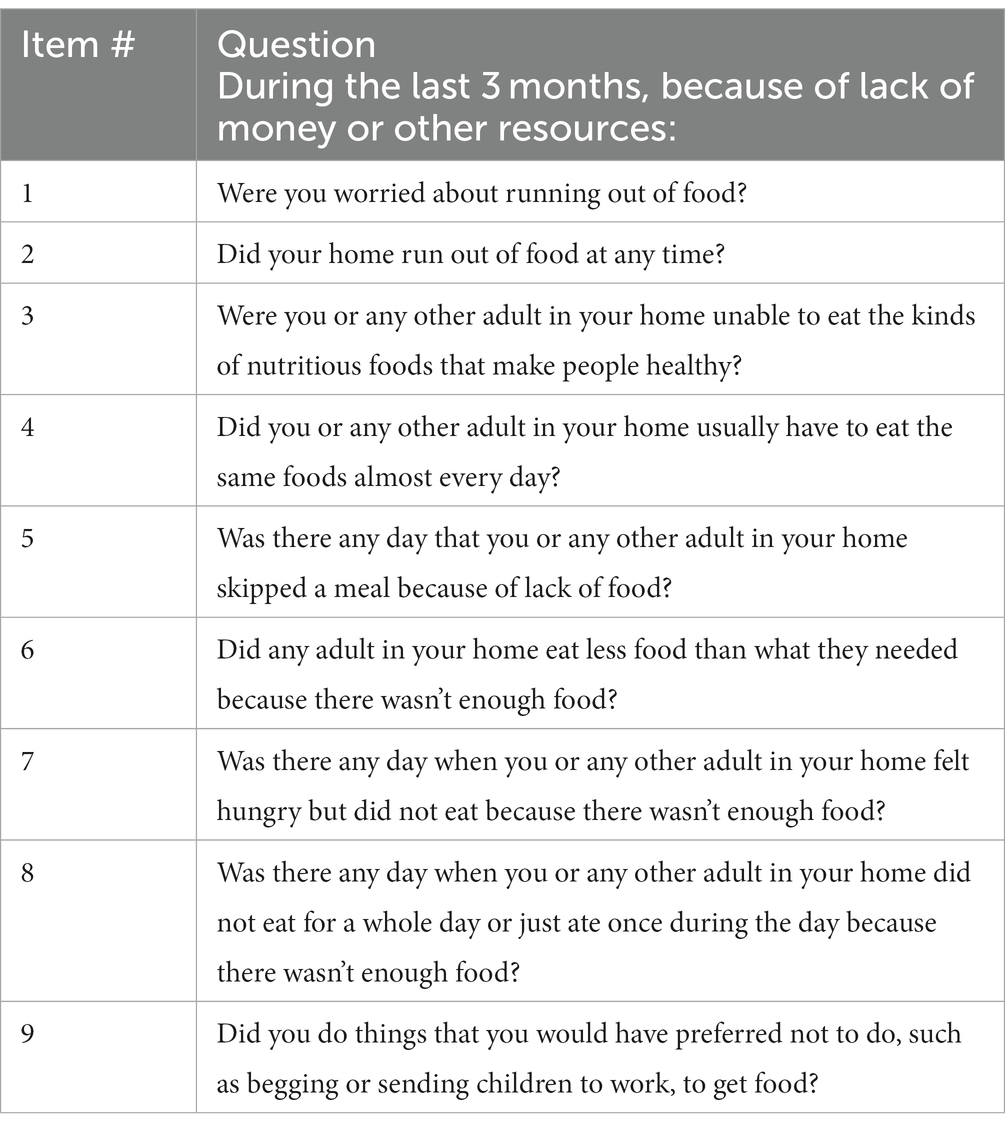
Table 1. Latin American and Caribbean household food security scale items.
2.3 Independent variables
Sixteen risk factors were chosen and examined based on existing literature and potential risk factors specific to this population, based on experience working in the region. Demographic factors included age at baseline interview (continuous), sex, level of education, perceived economic status, marital status, island site (Puerto Rico, USVI, Trinidad, or Barbados), home ownership status (Yes/No), and whether the participant had moved in the past year (Yes/No). Sex was measured on the baseline survey using the following question, “What sex were you at birth?” Educational attainment was measured using the question, “What is the highest year of school that you completed?” Responses were categorized into less than high school (or secondary school), high school graduate, some college, and college and higher. Perceived economic status was measured using an adapted version of the World Gallup Poll® question: “Please look at this figure, with steps numbered from 1 at the bottom to 10 at the top. Suppose the top of the ladder represents the richest people of this island and the bottom represents the poorest people of this island. Taking into consideration your current personal situation, what is the number of the step on which you would place yourself?” Responses ranged from 1 poor to 10 high and were categorized into bottom, middle, and top quantiles. Marital status was measured by asking “What is your current relationship status” and responses categorized into married, single, separated/divorced, or widowed.
Psychosocial factors included were emotional support, and depression. Emotional support was measured using the PROMIS Emotional Support short form (36). Responses were dichotomized (Yes/No) as to whether each participant had a low emotional support score, meaning less than 12. Depression (Yes/No) was measured by the Patient Health Questionnaire (PHQ-2) (37, 38).
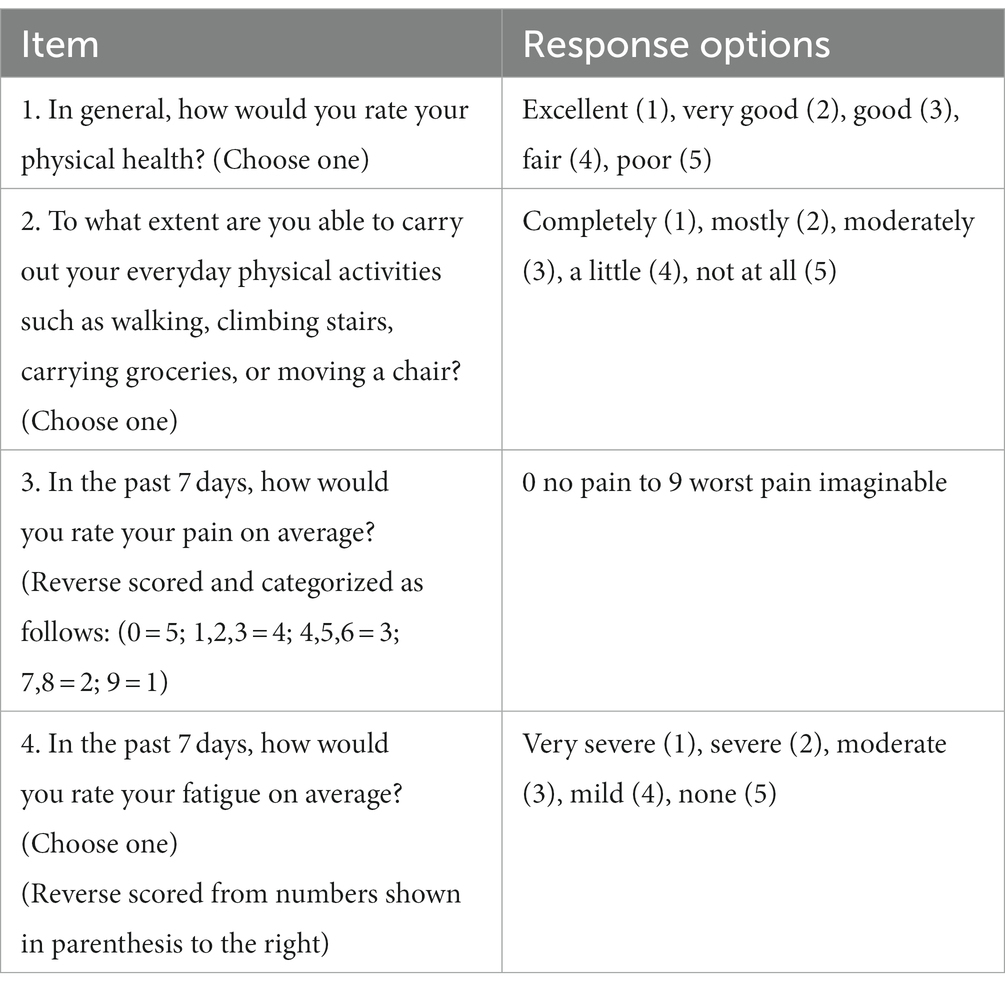
Behavioral factors included current smoking and self-reported physical health scores. Current smoking status (Yes/No) was measured using two variables: “Have you EVER smoked any tobacco product, such as cigarettes, cigars, or tobacco pipe? Yes/No. Those that answered Yes were asked “Do you still smoke cigarettes, cigars, or tobacco pipe regularly? By regularly we mean at least 20 cigarettes or 1 cigar or half an ounce sachet of loose tobacco per month.” The PROMIS Global Physical Health score was used to assess participant reported physical health (39, 40). The score ranges from 4 to 20, with 4 being poor health and 20 excellent health. The score was created using 4 items (Table 2).
Environmental factors included fruit and vegetable availability and quality, mode of transportation to the grocery store, and water source as a proxy for water security. Fruit and vegetable availability and quality were measured as follows: “Thinking about food resources in your neighborhood, how often are a large selection of fresh fruits and vegetables, excluding provisions, available in my neighborhood?” and “Thinking about food resources in your neighborhood, how often are the fresh fruits and vegetables in your neighborhood of high quality?” Responses were dichotomized into never/rarely/sometimes or usually/always. Mode of transportation to the grocery store was measured with a single item: “What is the most typical way you travel to the store for your groceries?” and responses were dichotomized: drive own car/ride with friend/family or take the bus/taxi/bike/walk. Water insecurity was measured by a single item asking about source of potable water: “What is the main source of water supply for members of your household? This item was used as a proxy for water insecurity. Responses were dichotomized as water secure (water piped into dwelling) and water insecure (water not piped into dwelling).
2.4 Analysis
Rasch modeling was used to assess the ELCSA scale’s psychometric properties since this was the first time the scale was being used in the ECHORN Cohort. The Rasch model is a 1-parameter item response model, a modeling technique that is consistently applied in studies using the ELCSA and other food insecurity scales (26, 41–43). RASCH modeling was completed using the full data set (n = 2,961). The model was run in the following ways: (1) On the full sample using all 9 ELCSA items; (2) on the full sample using 8 of 9 ELCSA items (removing number 9—begging); (3) on the sample from each island (using all 9 items and 8 items as above); (4) removing individual participants identified as outliers—both on the full sample using all 9 items and for each island site using the 9-item scale. Unidimensionality of the scale by island was further assessed using Differential Item Functioning (DIF). DIF analysis was performed to compare scale performance for each island to the full sample. Measure, Infit values, and differences in item performance were assessed by island site. A detailed description of the RASCH results can be found in Supplementary material.
Next, univariate and bivariate analyses were conducted to determine the prevalence of household food insecurity, describe the overall sample by each risk factor, and to examine the association between household food insecurity and each risk factor. Study variables were summarized using means and standard deviations or frequency distributions for the total sample and by level of household food insecurity. The analysis of variance and the chi-square test were used to examine the association between potential risk factor variables and household food insecurity. Tetrachoric and polychoric correlation coefficients were also examined to determine whether collinearity existed between specific study variables: education, perceived economic status, water supply (which may be a marker for economic status in the Caribbean region), and home ownership. Finally, multivariable ordinal logistic regression was then used to determine the association between household food insecurity (mild to moderate/severe) and each risk factor holding all other variables constant. The analysis was first conducted for the full sample, then stratified by sex as women are more likely to experience HFI than men (44).
3 Results
3.1 Rasch modeling results
Rasch modeling of the ELCSA scale in the ECHORN sample indicated that the full 9-item scale for adults used with the full cohort (rather than by island site) was the best fit. The Cronbach’s Alpha for the scale was 0.90. Figure 1 shows the ELCSA scale item infit values. Each item is shown along the X-axis and the item infit value on the Y-axis. Infit is a fit statistic that is less sensitive to outliers and more sensitive to observations near the respondent’s ability level (45). Acceptable infit values range from 0.7 to 1.3 (46). All 9-items of the ELCSA scale had acceptable infit values in the ECHORN sample. This means that the infit values demonstrate that the items measure the same construct and are independent of one another. Further information on the psychometric validity of the scale—as demonstrated through item prevalence, item severity, and differential item functioning by island site—is presented in Supplementary material.
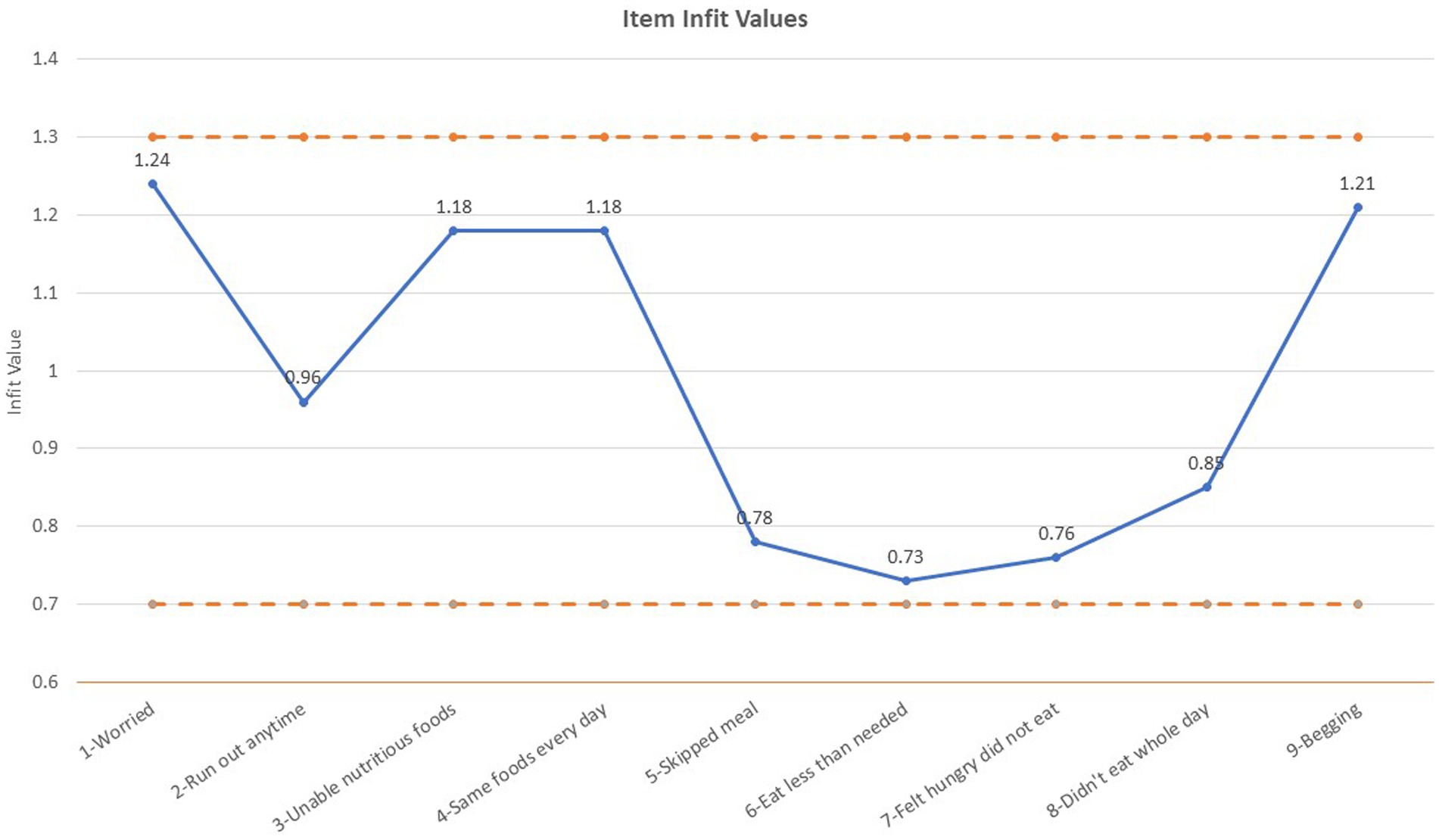
Figure 1. ELCSA item infit values.
3.2 Univariate and bivariate analysis
The final sample size consisted of 1,939 individuals with a baseline household food insecurity score and non-missing data for the examined risk factors. More than one-quarter of the sample (27.3%) experienced some level of household food insecurity (17.0% mild, 10.3% moderate or severe). Respondents were on average 57 years of age (S.D. 10.5) and nearly two-thirds were female. Nearly one-third had no high school education, 41% were married, nearly two-thirds owned their own home and 50% rated themselves in the middle economic quartile of their respective island. Nearly 15% of respondents did not have water piped directly into their homes (Table 3, total column). Correlation coefficients ranged from −0.04 to 0.23, indicating that collinearity was not present between education, perceived economic status, water supply, and home ownership.
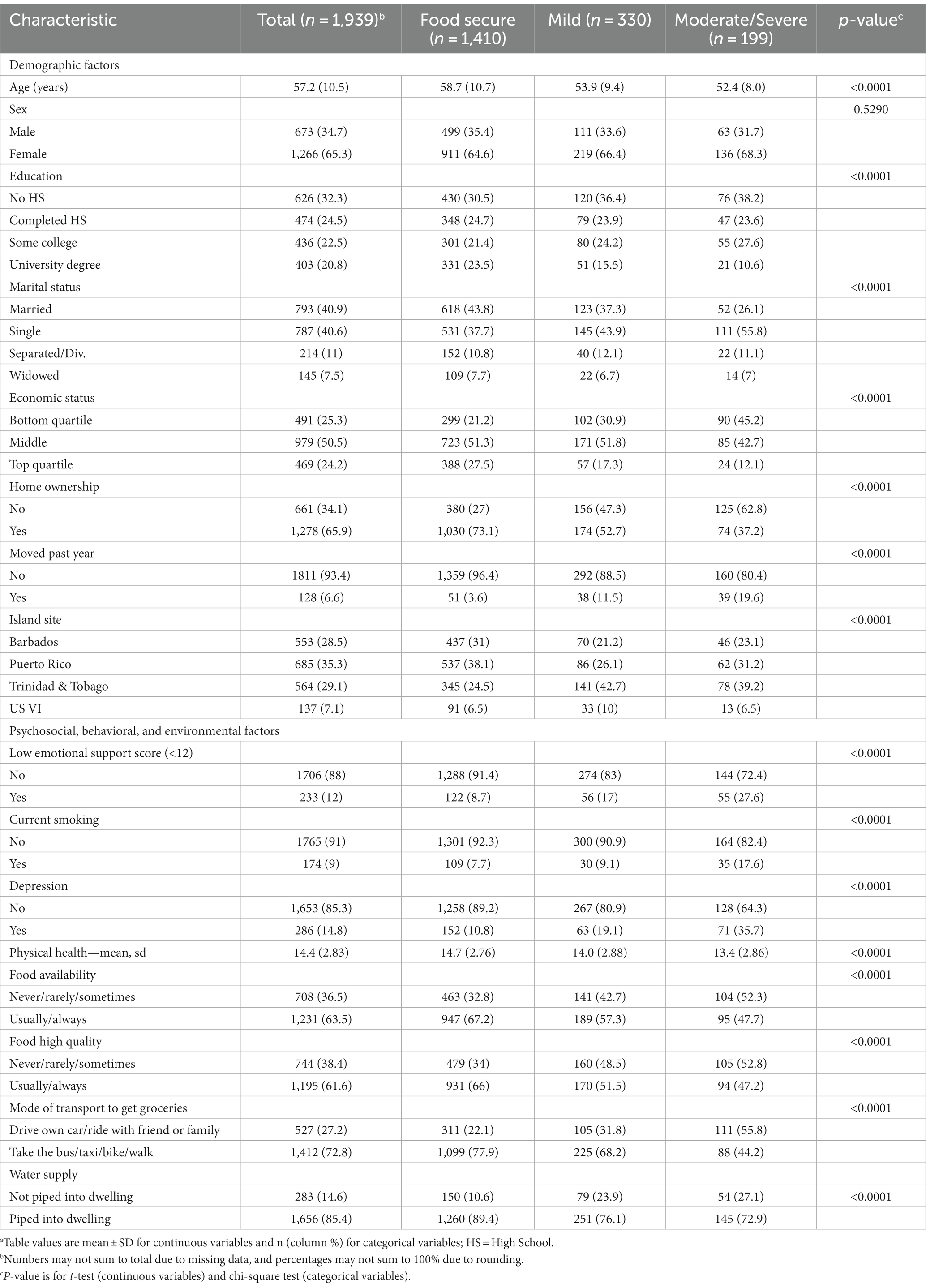
Table 3. Risk factors for household food insecurity by HFI status (n = 1,939)a.
In bivariate analyses, all risk factors examined, except for sex were significantly associated with household food security status (Table 3). Those who were food secure were 4.8–6.3 years older than those who had mild or moderate/severe food insecurity. Those who reported that they had not completed high school or college, were single, did not own a home, moved in the past year, or had a self-reported economic status in the bottom quantile were more likely to report food insecurity than their counterparts. Participants in Trinidad were more likely to report food insecurity compared to the other three island sites. The prevalence of water insecurity was 14.5% in this sample. A dose response relationship with water insecurity was found such that food insecurity worsened as the proportion of respondents who did not have potable water piped directly into their dwelling increased.
3.3 Multivariable analysis
The multivariable analysis modeled the odds of worsening household food insecurity (mild to moderate/severe; Table 4). Increasing age was protective against experiencing worsening HFI in this sample. All variables except sex, education, marital status, smoking status, and residing in Puerto Rico (compared to Barbados) were significant predictors of HFI in the adjusted model. Sex was not associated with HFI in either the unadjusted or the adjusted model. In the adjusted model, those who were depressed had 71% increased odds (OR: 1.71; 95% CI: 1.28–2.28) of worsening HFI compared to those who were not depressed. Those who did not have water piped directly into their dwelling had 59% increased odds of worsening HFI compared to those with water piped directly into their home (OR 1.59; 95% CI: 1.17–2.17).
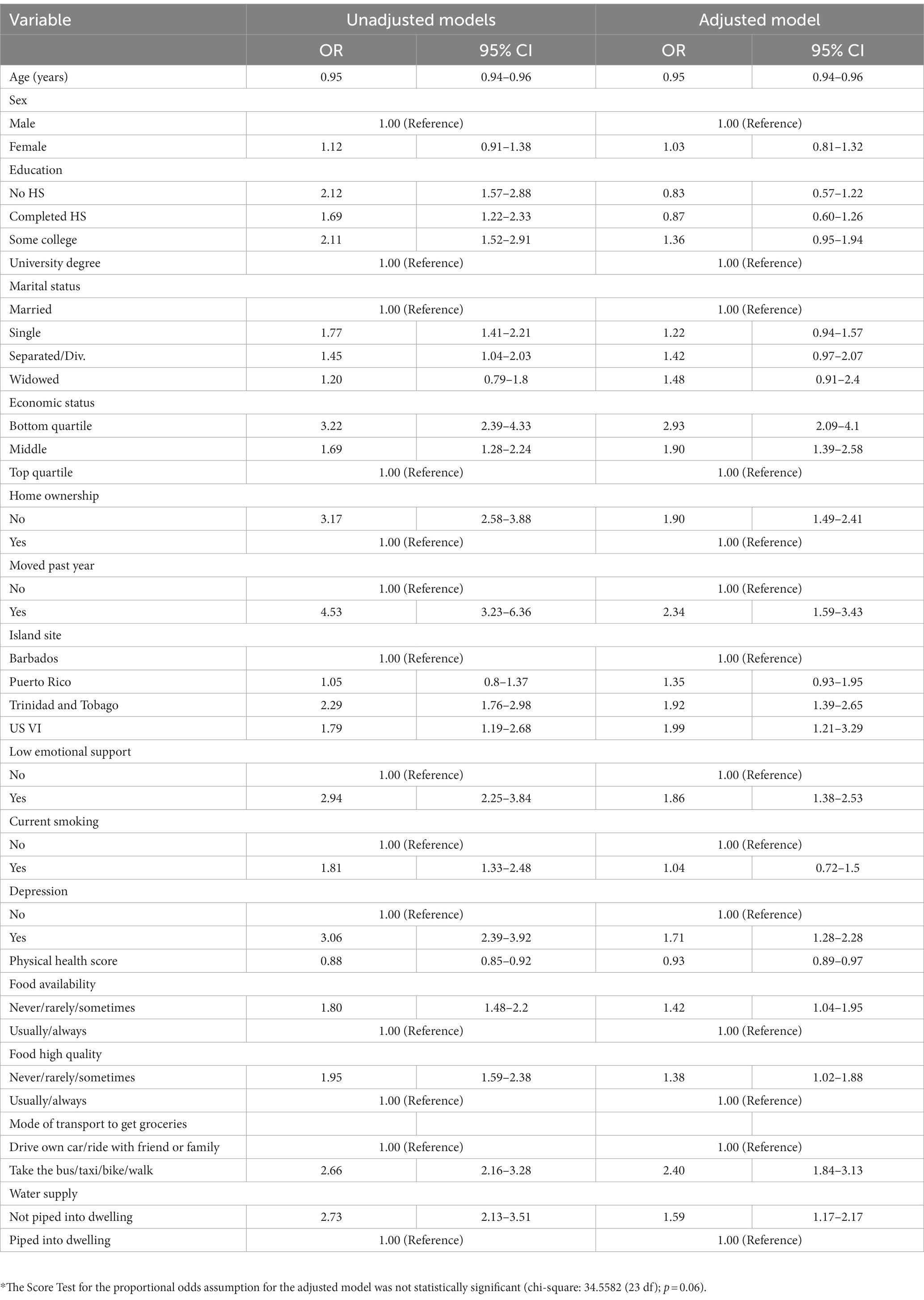
Table 4. Unadjusted and adjusted associations between risk factors and household food insecurity (N = 1,939)*.
3.4 Sex stratified analysis
In the sex stratified analysis, age was a significant protective factor against worsening HFI; however, there was a greater protective effect for women compared to men (Table 5). For every 1-year increase in age, women were 6% less likely to experience worsening HFI, while men were 3% less likely. Self-reported economic status in the middle or bottom quantiles, not owning a home, having moved in the past year, low emotional support, lack of car or ride to get to the grocery store, and lack of water piped directly into the home were significantly associated with worsening HFI among both men and women. Education, marital status, current smoking status, and access to high quality foods were not associated with worsening HFI in men or women.
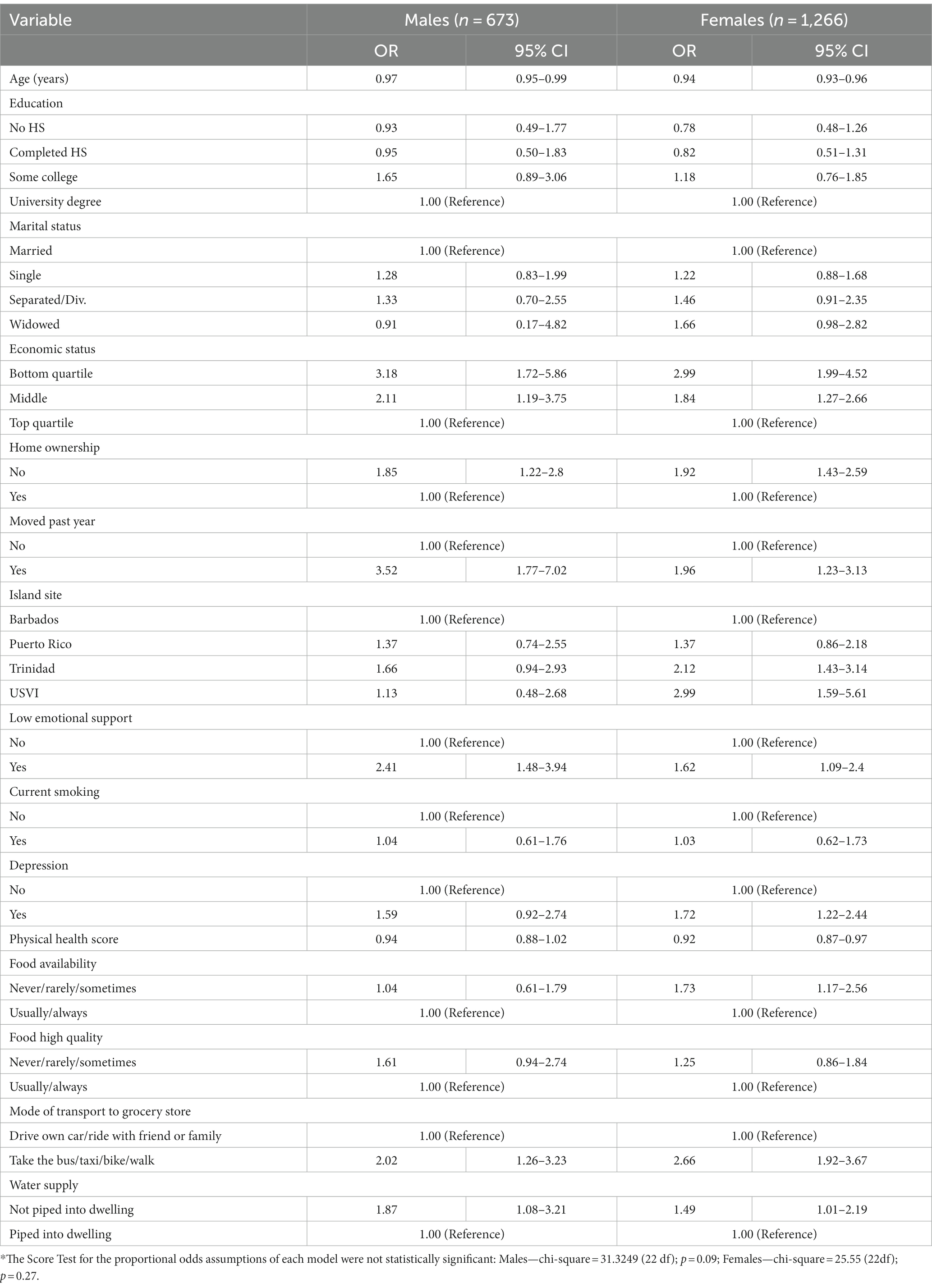
Table 5. Adjusted associations between risk factors and household food insecurity, stratified by sex (n = 1,939)*.
Depression, food availability, self-rated physical health, and island site were significantly associated with increased odds of worsening HFI for women, but not for men. Women who screened positive for depression had 72% increased odds of worsening HFI (OR: 1.72; CI: 1.22–2.44) compared to those without depressive symptoms. This is compared to 59% increased odds among men; however, this effect estimate was not statistically significant (OR: 1.59; CI: 0.92–2.74).
4 Discussion
This study aimed to examine demographic, psychosocial, behavioral, and environmental factors associated with HFI in a four-island Caribbean cohort. Identified demographic risk factors included younger age, lack of home ownership, and lack of stable housing. Psychosocial and behavioral risk factors included were depression, low emotional support, and poor self-rated physical health. Environmental risk factors included lack of food availability, lack of high-quality foods, and lack of water piped directly into the home. Our findings demonstrate that the prevalence of household food insecurity in the ECHORN Cohort is comparable to other studies that have been conducted in the region. A study of adults in Trinidad, showed a 25.0% prevalence of HFI and found that lower household income and physical disability were each independently associated with HFI (23). Another study conducted in households with children in three Eastern Caribbean countries (Barbados, St. Lucia, and St. Vincent and the Grenadines), that examined HFI as an exposure, showed a prevalence of HFI of 33.0% and found that food insecure households were more likely to include a chronically ill parent, among other factors (4). With respect to populations living with infectious diseases, the prevalence of HFI is even higher. Fifty-eight percent of people living with HIV in the Dominican Republic reported experiencing severe HFI (22). Finally, in a study of women with young children in Haiti, 98% of the sample had some level of food insecurity. This study found that severe food insecurity was a significant risk factor for clinical malaria (26).
The findings presented above differ from the existing literature in important ways. First, women are more likely to experience HFI than men, globally (47); however, sex was not associated with HFI in our bivariate or multivariable analyses. Given that female sex is a known risk factor for HFI in other regions of the world, a sex stratified analysis was conducted to understand how risk factors for HFI might differ by sex in this sample. In stratified analyses we found that women who screened positive for depression, had poorer self-rated physical health, and who did not think fresh fruits and vegetables were readily available had increased odds of worsening HFI. The existing literature demonstrates an association between HFI and depressive symptoms, anxiety, poor coping strategies, and risky behavior among women (48). The directionality of the association between depression and HFI is undetermined and while these findings do not directly fill that gap, they add to the body of literature demonstrating an association between mental health and HFI. Furthermore, women with poor self-rated physical health may have both physical and economic limitations that contribute to their food insecurity status. Future research should explore longitudinal associations between depression, self-rated physical health, food availability and HFI.
Furthermore, this study adds to the growing body of literature examining the association between water and food insecurity. Source of potable water-a proxy for water insecurity-was a significant predictor of HFI for both men and women, such that those without water piped directly into their home had an increased odds of experiencing HFI. We did not find evidence of multicollinearity between water source and other indicators of socioeconomic status such as education, perceived economic status, and home ownership, suggesting that source of potable water is an independent risk factor for HFI in this sample. To our knowledge, this is the first multi-country study in the Caribbean region to examine the association between water security and HFI. Recent scholarship on water and food security suggests collecting more and better data on water insecurity, including prevalence data (49). We will continue to explore the relationship between water and food security and corresponding health outcomes in subsequent waves of data collection for the ECHORN cohort.
4.1 Study strengths and limitations
We used a validated and well-tested measure of household food insecurity for this research and confirmed its robust psychometric properties in the ECHORN cohort. We also examined known and potential risk factors for HFI (based on our knowledge of the region), which allowed us to identify important risk factors specific to the populations under study. This research fills a gap in the literature with respect to identifying and understanding risk factors for household food insecurity in the Caribbean region, and strongly calls for applying the lessons learned in these settings to the design of similar policy relevant studies in other regions of the world. Importantly, we present evidence of a link between source of potable water, a proxy for water security, and household food insecurity in the ECHORN cohort. These findings have important implications for understanding how to improve the governance of food and water security systems and the coordination needed between them.
With respect to study limitations, the cross-sectional nature of this analysis only allows us to draw conclusions about the association between the studied risk factors and household food insecurity in the region, without comment on causality. In addition, these findings pertain to the ECHORN cohort study sites only and cannot be extrapolated to other nations or territories in region.
5 Conclusion
This cross-sectional, multi-country study was designed to identify risk factors for household food insecurity in the Eastern Caribbean. The findings fill a gap in the literature with respect to understanding risk factors for HFI and have important implications for future research and policy in this area. Future research should examine these risk factors longitudinally, with a focus on understanding the transition from a food secure to a food insecure state over time in the ECHORN cohort. Additional work will examine whether household food insecurity is associated with specific cardiometabolic conditions in the cohort and what role water security also plays in these relationships.
Data availability statement
The datasets generated and analyzed for this study are available upon request to the ECHORN Data Access and Scientific Review committee (https://www.echorn.org/request-echorn-data).
Ethics statement
This study was approved by the Institutional Review Boards at Yale University, the University of Puerto Rico Medical Sciences Campus, the University of the Virgin Islands, the University of the West Indies – Cave Hill, and St. Augustine (Trinidad) campuses, and the Ministry of Health of Trinidad and Tobago. This study were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JM-B: Conceptualization, Formal analysis, Methodology, Project administration, Supervision, Visualization, Writing – original draft, Writing – review & editing. AH-F: Formal analysis, Methodology, Software, Supervision, Writing – review & editing. DG: Data curation, Formal analysis, Methodology, Writing – review & editing. CO: Writing – review & editing. LA: Writing – original draft, Writing – review & editing. OA: Data curation, Funding acquisition, Resources, Writing – review & editing. RM: Data curation, Funding acquisition, Resources, Writing – review & editing. CN: Data curation, Funding acquisition, Resources, Writing – review & editing. MN: Data curation, Funding acquisition, Resources, Writing – review & editing. MN-S: Data curation, Funding acquisition, Resources, Writing – review & editing. RP-E: Conceptualization, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This publication was supported by the National Institute on Minority Health and Health Disparities through the Eastern Caribbean Health Outcomes Research Network (ECHORN)-U24MD006939 and through the Yale Transdisciplinary Collaborative Center for Health Disparities Research focused on Precision Medicine (Yale-TCC)-U54MD010711. Support was also provided by CTSA Grant Number KL2 TR001862 and KL2 RR024138 from the National Center for Advancing Translational Science (NCATS), a component of the National Institutes of Health (NIH). The contents are solely the responsibility of the authors and do not necessarily represent the official view of NIH.
Acknowledgments
We would like to thank the ECHORN research teams on each island site for their tireless efforts in establishing and maintaining this cohort. We would also like to thank the ECHORN cohort study participants for entrusting us with their health information.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer AJ declared a shared affiliation, though no other collaboration, with one of the authors RM to the handling editor.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1269857/full#supplementary-material
References
1. World Health Organization (WHO). Definition of Food Insecurity (2009). Available at: https://web.archive.org/web/20040806144802/http://www.who.int/trade/glossary/story028/en/.
2. Zereyesus, YA, Cardell, L, Valdes, C, Ajewole, K, Zeng, W, Beckman, J, et al. International food security assessment, 2022–32. United States: Department of Agriculture (USDA) (2022).
3. Pérez-Escamilla, R, and Segall-Corrêa, AM. Food insecurity measurement and indicators. Rev Nutr. (2008) 21:15s–26s. doi: 10.1590/S1415-52732008000700003
4. Racine, EF, Jemison, K, Huber, LR, and Arif, AA. The well-being of children in food-insecure households: results from the eastern Caribbean child vulnerability study 2005. Public Health Nutr. (2009) 12:1443–50. doi: 10.1017/S1368980008004229
5. McClain, AC, Cory, H, and Mattei, J. Childhood food insufficiency and adulthood cardiometabolic health conditions among a population-based sample of older adults in Puerto Rico. SSM Popul Health. (2022) 17:101066. doi: 10.1016/j.ssmph.2022.101066
6. Rasul, R, Rouzier, V, Sufra, R, Yan, LD, Joseph, I, Mourra, N, et al. Extreme food insecurity and malnutrition in Haiti: findings from a population-based cohort in Port-Au-Prince, Haiti. Nutrients. (2022) 14:4854. doi: 10.3390/nu14224854
7. Pérez-Escamilla, R, Villalpando, S, Shamah-Levy, T, and Méndez-Gómez, HI. Household food insecurity, diabetes and hypertension among Mexican adults: results from Ensanut 2012. Salud Publica Mex. (2014) 56 Suppl 1:s62–70. doi: 10.21149/spm.v56s1.5167
8. Basiotis, PP, and Lino, M. Insight 26: July 2002: food insufficiency and prevalence of overweight among adult women. Fam Econ Nutr Rev. (2003) 15:55–8.
9. Shariff, ZM, and Khor, G. Obesity and household food insecurity: evidence from a sample of rural households in Malaysia. Eur J Clin Nutr. (2005) 59:1049–58. doi: 10.1038/sj.ejcn.1602210
10. Shariff, ZM, and Lin, KG. Indicators and nutritional outcomes of household food insecurity among a sample of rural Malaysian women. Pak J Nutr. (2004) 3:50–5. doi: 10.3923/pjn.2004.50.55
11. Ihab, A, Rohana, A, and Manan, W. Concept and measurements of household food insecurity and its impact on malnutrition: a review. Int Med J. (2015) 22:509–16.
12. Jayatissa, R, Herath, HP, Perera, AG, Dayaratne, TT, De Alwis, ND, and Nanayakkara, HPLK. Impact of COVID-19 on child malnutrition, obesity in women and household food insecurity in underserved urban settlements in Sri Lanka: a prospective follow-up study. Public Health Nutr. (2021) 24:3233–41. doi: 10.1017/S1368980021001841
13. Orewa, S, and Iyanbe, C. Household food insecurity in Nigeria: an assessment of the present status of protein–energy malnutrition among rural and low-income urban households. J Appl Sci Res. (2009) 5:1615–21.
14. Ortiz-Marrón, H, Ortiz-Pinto, MA, Lanza, MU, Pujadas, GC, Pino, VV, Cortés, SB, et al. Household food insecurity and its association with overweight and obesity in children aged 2 to 14 years. BMC Public Health. (2022) 22:1930. doi: 10.1186/s12889-022-14308-0
15. Betebo, B, Ejajo, T, Alemseged, F, and Massa, D. Household food insecurity and its association with nutritional status of children 6–59 months of age in east Badawacho District, South Ethiopia. J Environ Public Health. (2017) 2017:1–17. doi: 10.1155/2017/6373595
16. Drammeh, W, Hamid, NA, and Rohana, A. Determinants of household food insecurity and its association with child malnutrition in sub-Saharan Africa: a review of the literature. Curr Res Nutr Food Sci J. (2019) 7:610–23. doi: 10.12944/CRNFSJ.7.3.02
17. Osei, A, Pandey, P, Spiro, D, Nielson, J, Shrestha, R, Talukder, Z, et al. Household food insecurity and nutritional status of children aged 6 to 23 months in Kailali District of Nepal. Food Nutr Bull. (2010) 31:483–94. doi: 10.1177/156482651003100402
18. Dhamija, G, Ojha, M, and Roychowdhury, P. Hunger and health: reexamining the impact of household food insecurity on child malnutrition in India. J Dev Stud. (2022) 58:1181–210. doi: 10.1080/00220388.2022.2029419
19. FAO P, WFP U. Latin America and the Caribbean–regional overview of food security and nutrition 2021: statistics and trends. Santiago: FAO (2021).
20. Rebick, GW, Franke, MF, Teng, JE, Gregory Jerome, J, and Ivers, LC. Food insecurity, dietary diversity, and body mass index of HIV-infected individuals on antiretroviral therapy in rural Haiti. AIDS Behav. (2016) 20:1116–22. doi: 10.1007/s10461-015-1183-y
21. Richterman, A, Leandre, F, Jerome, JG, Tsai, AC, and Ivers, LC. Mortality over long-term follow-up for people with HIV receiving longitudinal care and antiretroviral therapy in rural Haiti: open forum infectious diseases Oxford University Press (2020) 7:1–8. doi: 10.1093/ofid/ofaa328
22. Derose, KP, Ríos-Castillo, I, Fulcar, MA, Payán, DD, Palar, K, Escala, L, et al. Severe food insecurity is associated with overweight and increased body fat among people living with HIV in the Dominican Republic. AIDS Care. (2018) 30:182–90. doi: 10.1080/09540121.2017.1348597
23. Gulliford, MC, Mahabir, D, and Rocke, B. Food insecurity, food choices, and body mass index in adults: nutrition transition in Trinidad and Tobago. Int J Epidemiol. (2003) 32:508–16. doi: 10.1093/ije/dyg100
24. Ostolaza, C, Rosas, C, García-Blanco, AM, Gittelsohn, J, and Colón-Ramos, U. Impact of the COVID-19 pandemic on food insecurity in Puerto Rico. J Hung Environ Nutr. (2023) 18:380–95. doi: 10.1080/19320248.2021.1997857
25. Pengpid, S, and Peltzer, K. Food insecurity is associated with multiple psychological and behavioural problems among adolescents in five Caribbean countries. Psychol Health Med. (2023) 28:291–304. doi: 10.1080/13548506.2021.2019813
26. Pérez-Escamilla, R, Dessalines, M, Finnigan, M, Pachón, H, Hromi-Fiedler, A, and Gupta, N. Household food insecurity is associated with childhood malaria in rural Haiti. J Nutr. (2009) 139:2132–8. doi: 10.3945/jn.109.108852
27. Bethancourt, HJ, Swanson, ZS, Nzunza, R, Young, SL, Lomeiku, L, Douglass, MJ, et al. The co-occurrence of water insecurity and food insecurity among Daasanach pastoralists in northern Kenya. Public Health Nutr. (2023) 26:693–703. doi: 10.1017/S1368980022001689
28. Brewis, A, Workman, C, Wutich, A, Jepson, W, Young, S, Network, HWIERC, et al. Household water insecurity is strongly associated with food insecurity: evidence from 27 sites in low-and middle-income countries. Am J Hum Biol. (2020) 32:e23309. doi: 10.1002/ajhb.23309
29. Young, SL, Frongillo, EA, Jamaluddine, Z, Melgar-Quinonez, H, Perez-Escamilla, R, Ringler, C, et al. Perspective: the importance of water security for ensuring food security, good nutrition, and well-being. Adv Nutr. (2021) 12:1058–73. doi: 10.1093/advances/nmab003
30. Young, SL, Boateng, GO, Jamaluddine, Z, Miller, JD, Frongillo, EA, Neilands, TB, et al. The household water InSecurity experiences (HWISE) scale: development and validation of a household water insecurity measure for low-income and middle-income countries. BMJ Glob Health. (2019) 4:e001750. doi: 10.1136/bmjgh-2019-001750
31. Collins, SM, Mbullo Owuor, P, Miller, JD, Boateng, GO, Wekesa, P, Onono, M, et al. ‘I know how stressful it is to lack water!‘exploring the lived experiences of household water insecurity among pregnant and postpartum women in western Kenya. Glob Public Health. (2019) 14:649–62. doi: 10.1080/17441692.2018.1521861
32. Razzaghi, H, Martin, DN, Quesnel-Crooks, S, Hong, Y, Gregg, E, Andall-Brereton, G, et al. 10-year trends in noncommunicable disease mortality in the Caribbean region. Rev Panam Salud Publica. (2019) 43:1–11. doi: 10.26633/RPSP.2019.37
33. Coleman-Jensen, A, Gregory, C, and Singh, A. Household food security in the United States in 2013. USDA-ERS economic research. Report. (2014) 173. doi: 10.2139/ssrn.2504067
34. Gundersen, C. Food insecurity is an ongoing national concern. Adv Nutr. (2013) 4:36–41. doi: 10.3945/an.112.003244
35. Spatz, ES, Martinez-Brockman, JL, Tessier-Sherman, B, Mortazavi, B, Roy, B, Schwartz, JI, et al. Phenotypes of hypertensive ambulatory blood pressure patterns: design and rationale of the ECHORN hypertension study. Ethn Dis. (2019) 29:535–44. doi: 10.18865/ed.29.4.535
36. Measures, PH. PROMIS emotional support short form v2.0 (2016). Available at: https://www.healthmeasures.net/index.php?option=com_instruments&task=Search.pagination&Itemid=992.
37. Löwe, B, Kroenke, K, and Gräfe, K. Detecting and monitoring depression with a two-item questionnaire (PHQ-2). J Psychosom Res. (2005) 58:163–71. doi: 10.1016/j.jpsychores.2004.09.006
38. Arroll, B, Goodyear-Smith, F, Crengle, S, Gunn, J, Kerse, N, Fishman, T, et al. Validation of PHQ-2 and PHQ-9 to screen for major depression in the primary care population. Ann Fam Med. (2010) 8:348–53. doi: 10.1370/afm.1139
39. Hays, RD, Bjorner, JB, Revicki, DA, Spritzer, KL, and Cella, D. Development of physical and mental health summary scores from the patient-reported outcomes measurement information system (PROMIS) global items. Qual Life Res. (2009) 18:873–80. doi: 10.1007/s11136-009-9496-9
40. Hays, RD, Spritzer, KL, Schalet, BD, and Cella, D. PROMIS®-29 v2. 0 profile physical and mental health summary scores. Qual Life Res. (2018) 27:1885–91. doi: 10.1007/s11136-018-1842-3
41. Garcia, J, Hromi-Fiedler, A, Mazur, RE, Marquis, G, Sellen, D, Lartey, A, et al. Persistent household food insecurity, HIV, and maternal stress in peri-urban Ghana. BMC Public Health. (2013) 13:1–9. doi: 10.1186/1471-2458-13-215
42. Nord, M. Introduction to item response theory applied to food security measurement: Basic concepts, parameters, and statistics. Technical Paper Rome: FAO (2014).
43. Villagómez-Ornelas, P, Hernández-López, P, Carrasco-Enríquez, B, Barrios-Sánchez, K, Pérez-Escamilla, R, and Melgar-Quiñónez, H. Validez estadística de la Escala Mexicana de seguridad alimentaria y la Escala Latinoamericana y Caribeña de seguridad alimentaria. Salud Publica Mex. (2014) 56 Suppl 1:s5–s11. doi: 10.21149/spm.v56s1.5160
44. Schlüssel, MM, Silva, AAM, Pérez-Escamilla, R, and Kac, G. Household food insecurity and excess weight/obesity among Brazilian women and children: a life-course approach. SciELO Public Health. (2013) 29:219–26. doi: 10.1590/S0102-311X2013000200003
45. Bond, TG, and Fox, CM. Applying the Rasch model: Fundamental measurement in the human sciences. Mahwah, New Jersey: Psychology Press (2013).
46. Hackett, M, Melgar-Quinonez, H, and Uribe, MCA. Internal validity of a household food security scale is consistent among diverse populations participating in a food supplement program in Colombia. BMC Public Health. (2008) 8:1–9. doi: 10.1186/1471-2458-8-175
47. Broussard, NH. What explains gender differences in food insecurity? Food Policy. (2019) 83:180–94. doi: 10.1016/j.foodpol.2019.01.003
48. Ivers, LC, and Cullen, KA. Food insecurity: special considerations for women. Am J Clin Nutr. (2011) 94:1740S–4S. doi: 10.3945/ajcn.111.012617
Keywords: food insecurity, household food insecurity, Caribbean region, U.S. territories, ELCSA
Citation: Martinez-Brockman JL, Hromi-Fiedler A, Galusha D, Oladele C, Acosta L, Adams OP, Maharaj RG, Nazario CM, Nunez M, Nunez-Smith M, Pérez-Escamilla R and on behalf of the ECHORN Writing Group (2023) Risk factors for household food insecurity in the Eastern Caribbean Health Outcomes Research Network cohort study. Front. Public Health. 11:1269857. doi: 10.3389/fpubh.2023.1269857
Edited by:
Marianella Herrera-Cuenca, Central University of Venezuela, VenezuelaReviewed by:
Monica Ewomazino Akokuwebe, North-West University, South AfricaAfiya John, The University of the West Indies St. Augustine, Trinidad and Tobago
Aline Ferreira, Federal University of Rio de Janeiro, Brazil
Copyright © 2023 Martinez-Brockman, Hromi-Fiedler, Galusha, Oladele, Acosta, Adams, Maharaj, Nazario, Nunez, Nunez-Smith, Pérez-Escamilla and on behalf of the ECHORN Writing Group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Josefa L. Martinez-Brockman, am9zZWZhLm1hcnRpbmV6QHlhbGUuZWR1