
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 24 January 2024
Sec. Public Health Policy
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1268888
 Inês Vaz-Pinto1*
Inês Vaz-Pinto1* Enrique Ortega2
Enrique Ortega2 Ivan Chivite3María Butí4,5Juan Turnes-Vázquez6Vítor Magno-Pereira7,8Miguel Rocha9
Ivan Chivite3María Butí4,5Juan Turnes-Vázquez6Vítor Magno-Pereira7,8Miguel Rocha9 Jorge Garrido10Catarina Esteves-Santos1Mafalda Guimaraes1Tomás Mourão1María Martínez Roma2
Jorge Garrido10Catarina Esteves-Santos1Mafalda Guimaraes1Tomás Mourão1María Martínez Roma2 Vanessa Guilera3Jordi Llaneras-Artigues4
Vanessa Guilera3Jordi Llaneras-Artigues4 Ana Barreira-Díaz4Santiago Pérez Cachafeiro6Sandra Daponte Angueira6
Ana Barreira-Díaz4Santiago Pérez Cachafeiro6Sandra Daponte Angueira6 Elisa Xavier7Mariana Vicente9
Elisa Xavier7Mariana Vicente9 Gema Garrido10Maria Teresa Heredia10Diogo Medina11Miguel García Deltoro2
Gema Garrido10Maria Teresa Heredia10Diogo Medina11Miguel García Deltoro2Background: Around 57,000 people in Spain and Portugal currently living with HIV or chronic hepatitis C are unaware of their infection. The COVID-19 pandemic severely disrupted screening efforts for these infections. We designed an intervention to increase and sustain opportunistic blood-borne virus (BBV) screening and linkage to care (SLTC) by implementing the TEST model.
Methods: The Plan Do Study Act (PDSA) method of quality improvement (QI) was implemented in 8 healthcare organizations (HCOs), including four hospitals, two clusters of community health centers, and two community-based organizations (CBOs). Baseline assessment included a review of BBV SLTC practices, testing volume, and results 12 months before the intervention. Changes in BBV testing rates over time were measured before, during, and after the COVID-19 lockdowns in 2020. A mixed ANOVA model was used to analyze the possible effect on testing volumes among HCOs over the three study periods.
Intervention: BBV testing was integrated into normal clinical flow in all HCOs using existing clinical infrastructure and staff. Electronic health record (EHR) systems were modified whenever possible to streamline screening processes, implement systemic institutional policy changes, and promote QI.
Results: Two years after the launch of the intervention in screening practices, testing volumes increased by 116%, with formal healthcare settings recording larger increases than CBOs. The start of the COVID-19 lockdowns was accompanied by a global 60% decrease in testing in all HCOs. Screening emergency department patients or using EHR systems to automate screening showed the highest resilience and lowest reduction in testing. HCOs recovered 77% of their testing volume once the lockdowns were lifted, with CBOs making the fullest recovery. Globally, enhanced screening techniques enabled HCOs to diagnose a total of 1,860 individuals over the research period.
Conclusions: Implementation of the TEST model enabled HCOs to increase and sustain BBV screening, even during COVID-19 lockdowns. Although improvement in screening was noted in all HCOs, additional work is needed to develop strong patient linkage to care models in challenging times, such as global pandemics.
Reaching and testing those at risk of infection with blood-borne viruses (BBV) such as human immunodeficiency virus (HIV), hepatitis B virus (HBV), or hepatitis C virus (HCV) remains a public health challenge in the Iberian Peninsula. An estimated 19,600 and 2,800 people living with HIV in Spain and Portugal, respectively, are unaware of their infection, and one in two receive their diagnosis at a late stage (CD4+ T cell count <350 cells/mm3 at diagnosis) (1–3). Similarly, an estimated 22,500 and 12,300 people living with chronic HCV in Spain and Portugal, respectively are unaware of their infection (4, 5). The prevalence of chronic HBV infection is estimated at 0.7% for both countries: 331,400 people live with chronic hepatitis B in Spain and 72,000 in Portugal, an unknown proportion of whom remain undiagnosed (6). Late BBV diagnosis is problematic not just for affected individuals, due to increased morbidity and mortality, but also for society, due to missed opportunities to break transmission (7).
Screening, a cornerstone of secondary prevention, is essential to reduce BBV prevalence and prevent further transmission (8). To date, BBV screening has typically followed traditional models, requiring dedicated staff and resources outside routine clinical practice (3). Instead of integrating screening into the regular provision of care for all eligible patients, traditional approaches often rely on a case-by-case decision, which may reinforce the stigma associated with testing for these infections.
National and international guidelines alike recommend enhancing BBV screening and linkage to care (SLTC) practices. In its evidence-based guidance on integrated BBV testing, the European Center for Disease Prevention and Control (ECDC) calls on countries to increase testing coverage and uptake in order to achieve the UN's epidemic control goals for 2030 (9–11). The Spanish Ministry of Health recommends HIV screening in sexually active individuals between the ages of 20 and 59 who present at primary care facilities, require a blood-draw for any clinical reason, and live in a Spanish province where HIV incidence in the previous 3 years has been above the 75th percentile (12). While it limits its recommendations on HCV screening to persons with a history of exposure to the virus or other known risk factors, the Spanish Ministry of Health recognizes that this strategy has not adequately addressed the undiagnosed population, and is currently undertaking a clinical efficacy and cost-effectiveness analysis of a birth cohort screening strategy for the Spanish population (13). The Portuguese General Directorate for Health, meanwhile, recommends screening patients aged 18 to 64 for HIV at least once in their lifetime, and progressively screening high prevalence population groups for HCV (14, 15).
Despite these recommendations, implementation of BBV SLTC in formal healthcare organizations (HCO) in Spain and Portugal is low and heterogeneous when compared to the role played by community-based organizations (CBO), relative to their size and resources (16).
In 2020, the advent of the SARS-CoV-2 pandemic led to decreased access to BBV prevention services and testing as health systems diverted resources toward fighting a global health crisis (17). Surveys of HIV specialists found that 53% to 58% were now treating patients with SARS-CoV-2 infection, as infectious disease specialists, internal medicine specialists and other healthcare personnel were needed to manage the pandemic (18, 19). In addition, 35% of survey respondents also reported disruptions in HIV testing services. Similar disruptions were noted for viral hepatitis screening (20). This disruption in screening programs and decelerated linkage to care could worsen BBV control (21, 22).
HCOs in different cities across the US have successfully used the TEST model to promote system changes and expand SLTC in various settings (23–27). TEST consists of 4 guiding pillars for enhanced SLTC: T, Testing and linkage integrated into the normal clinical flow, using existing clinical infrastructure and staff to create efficiencies; E, Electronic health record (EHR) modification, enhancing efficiencies within EHR and other technologies to facilitate appropriate screening; S, Systemic policy change, implementing institutional and regional policy change to support screening and linkage to care; and T, Training, feedback and continuous quality improvement. Training was performed on all organizations involving (1) a refresher on the basics of HIV and viral hepatitis infection and care, and (2) instructions on how to enroll patients in screening, including appropriate language for opt-out. Program data was utilized to track progress, to identify areas for improvement, and to support staff training (28). In other words, the aim of TEST is to take advantage of visits to medical facilities to offer eligible individuals on-the-spot testing for viruses while blood work is processed for other reasons. This opportunistic screening approach reduces patient biases while respecting their right to decline this or any other common clinical investigations (29).
The aim of this multi-center quality improvement intervention was to increase and sustain opportunistic BBV screening by implementing the TEST model. The project involved 8 HCOs, including 4 hospitals, 2 clusters of primary care centers, and 2 CBOs.
Eight organizations in Spain and Portugal participated in the study during different periods: Hospital de Cascais Dr. José de Almeida (further refered to as HCascais), in Cascais, Portugal; Consorci Hospital General Universitari de València (further refered to as HValencia), in Valencia, Spain; Hospital Clínic i Provincial de Barcelona (further refered to as Hclinic) in Barcelona, Spain; Hospital Universitari Vall d'Hebron (further refered to as HVHebron), in Barcelona, Spain; Servizo Galego de Saúde (further refered to as SGalicia), in Galicia, Spain; Serviço de Saúde da Região Autónoma da Madeira (further refered to as SMadeira), in Madeira, Portugal; Grupo de Ativistas em Tratamentos (further refered to as GAT), in Lisbon, Portugal and Apoyo Positivo (further refered to as A+), in Madrid and Malaga, Spain.
HCascais: the intervention was implemented in the adult Emergency Department (ED) in September 2018. Criteria for HIV and HCV screening were: age 18 to 64 years; presenting to the ED; no record of previous serologies; need for phlebotomy for any reason.
HValencia: the intervention was implemented in 26 primary care sites of this Health department in València, in February 2019. Criteria for HIV, HBV, and HCV screening were: age 18 to 80 years; presenting to primary care; no record of previous serologies; need for phlebotomy for any reason.
HClinic: the intervention was implemented in the ED in January 2020. Criteria for HIV, HBV, and HCV screening were: age ≥16 years; presenting to the ED with genitourinary complaints or reporting recent high-risk exposures, such as chemsex, shared injecting materials, or unprotected penetrative intercourse.
HVHebron: the intervention was implemented in the adult ED in February 2020. Criteria for HCV screening were: age ≥18 years; presenting to the ED; no record of previous serologies; need for phlebotomy for any reason.
SGalicia: regional health service in Galicia, Spain, where the intervention was implemented in 54 primary care sites in the Pontevedra y O Salnés health area in March 2019. Criteria for HIV and HCV screening were: age 18 to 70 years; presenting to primary care; no record of previous serologies; need for phlebotomy for any reason.
SMadeira: regional health service in Madeira, Portugal, where the intervention was implemented in inpatient hospital wards in January 2020, and in the adult ED in July 2020. Criteria for HCV screening were: age 18 to 70 years; in inpatient or seen in the ED; no record of previous serologies; need for phlebotomy for any reason.
GAT: the intervention was implemented in three community-based voluntary counseling and testing (CBVCT) brick-and-mortar sites and 1 mobile unit in March 2019. Criterion for HIV screening was age ≥14, criteria for HBV screening were unvaccinated individual aged ≥14 from a high-prevalence country, and criteria for HCV screening were unvaccinated individual aged ≥14 with a history of exposure to the virus or other known risk factors.
A+: the intervention was implemented in a novel CBVCT site in Torremolinos in April 2019. Criterion for HIV screening was age ≥18, criteria for HBV screening were unvaccinated individual aged ≥18 from a high-prevalence country, and criteria for HCV screening were unvaccinated individual aged ≥18 with a history of exposure to the virus or other known risk factors. Material should be uploaded separately on submission. Please include any supplementary data, figures and/or tables.
Each participating HCO appointed:
1. A principal investigator in charge of strategic planning and scientific supervision.
2. A project manager, in charge of implementation and day-to-day management of the intervention.
3. One or more linkage to care navigators, in charge of patient management.
Participating HCOs then implemented the TEST model in 3 phases, with occasional guidance from peer experts from similar organizations.
Screening criteria and workflows were defined, and EHR modifications were used whenever possible to automate eligibility algorithms. Consent procedures were adjusted to ensure opt-out language was used, and refusal to participate in screening was noted in the patient's record. Written consent forms were avoided unless mandated by the local Ethics Committee. Laboratory order forms and patient profiles were updated and EHRs were changed to automatically populate laboratory order forms whenever possible. Biological specimen collection workflows were defined and integrated into standard patient flow. Dedicated testers and rapid tests were limited to CBOs and avoided in formal healthcare settings to facilitate integration and economies of scale. Laboratory testing procedures were updated to ensure reflex testing was used (i.e., positive first-line test results automatically triggered confirmatory testing on the same specimen without the need for physician or patient intervention). Patient notification procedures and linkage to care workflows were defined and assigned to specific people. Each site integrated the redesigned protocols into its policies, trained its staff in the new protocols, and kept an implementation log of monitoring and evaluation indicators that was regularly reviewed to ensure adherence to each TEST pillar. Positive feedback loops were cultivated by sharing key intervention milestones with personnel. Patient education materials and signposting were designed and visibly affixed in public areas.
A detailed description of all implementation activities is included in Supplementary material.
A time-series analysis was used to measure the effect of the TEST model over various periods before and after the intervention. Each HCO reported the number of tests performed (HCV RNA tests or/and HIV Ab or HBV Ag) before the intervention and again during and after the intervention. Data was collected in a shared monitoring database provided by laboratory or information technology departments and compiled after being reported by each HCO. Outcomes were analyzed by determining changes in testing volume, as follows:
• Baseline phase: 12-month period prior to the start of the intervention.
• Increase phase: After the introduction of the intervention.
• Disruption phase: During the first wave of the COVID-19 pandemic.
• Sustain phase: After the first wave of the pandemic.
Table 1 shows the specific timeline of each participating center.

Table 1. Summary of characteristics of participating HCOs.
To test whether these changes were likely to be related to implementing the intervention, principal investigators and project managers from participating organizations were asked to participate in structured, open-ended feedback interviews administered by an outside team after the sustain phase. To measure their opinion of the intervention and its effect on transition outcomes, principal investigators and project managers were asked to specify the degree of implementation of each of the 4 pillars of the TEST model and to describe any iterations over PDSA cycles (i.e., Plan, Do, Study, Act). The interviews served to corroborate the statement that the intervention resulted in improved outcomes by examining whether HCOs implemented the intervention framework as intended.
Common qualitative techniques were used to ensure that the principal investigator and project manager interviews were analyzed systematically, including consistent use of the interview guide, audiotaping, and transcription of the interview data.
The primary outcome measure was the change in BBV testing rates over time after the intervention (during the increase phase, the disruption phase, and the sustain phase) compared with baseline testing rates (12-month period prior to the start of the intervention) in each HCO. Other variables were also analyzed, including number of patients diagnosed and time from a positive test result to confirmation. Longitudinal data analysis in terms of ANOVA was also carried out to examine the possibility of a significant relation between the changes in the number of tests performed, the type of HCOs and the different study periods.
For the analysis of longitudinal data, a mixed ANOVA model was used. The number of tests (dependent variable) in this model is determined by the type of HCO [hospital, primary care center, or community-based voluntary counseling and testing (CBVCT)] and the time period during which the parameters were evaluated (baseline, rise, disruption, or sustain). A possible interaction between the kind of HCO and the time period was considered, and each unique center was entered as a random factor in the model. P-values with α = 0.05 were considered to be significant. All analyses were performed in R Core Team (2021) (https://www.R-project.org/) version 4.1.2.
Offering BBV screening is considered standard clinical practice in both Spain and Portugal. Local ethics committees were asked to give their opinion when enhanced screening practices required modifying consent procedures from written opt-in consent to oral opt-out consent.
External data management agencies were provided with exclusive monthly aggregate reports on screening production indicators. No patients identifying characteristics were shared outside each HCO.
Participant HCOs made up a diverse group of organizations, and their implementation of the pillars of the TEST varied accordingly. Table 2 shows a summary of the various levels of TEST implementation as well as testing rate values for each participating institution. T, Testing was successfully integrated into the clinical workflows of all organizations. E, Electronic health record modifications were not implemented in 4 of the 8 participating organizations: A+ is a small CBVCT that did not use an EHR system at the start of the intervention; HValencia opted to include implementation of the SLTC program in their management agreement incentives instead; HValencia and HClinic launched their programs 2 months before the start of the SARS-CoV-2 pandemic, and it was therefore impossible to continue with plans to implement EHR modifications. S, Systemic policy changes were achieved in all organizations, and were approved by all management bodies. T, Training was implemented from the start in all organizations, but repeat training was offered unevenly across HCOs, with decentralized centers facing greater logistic challenges in this regard.
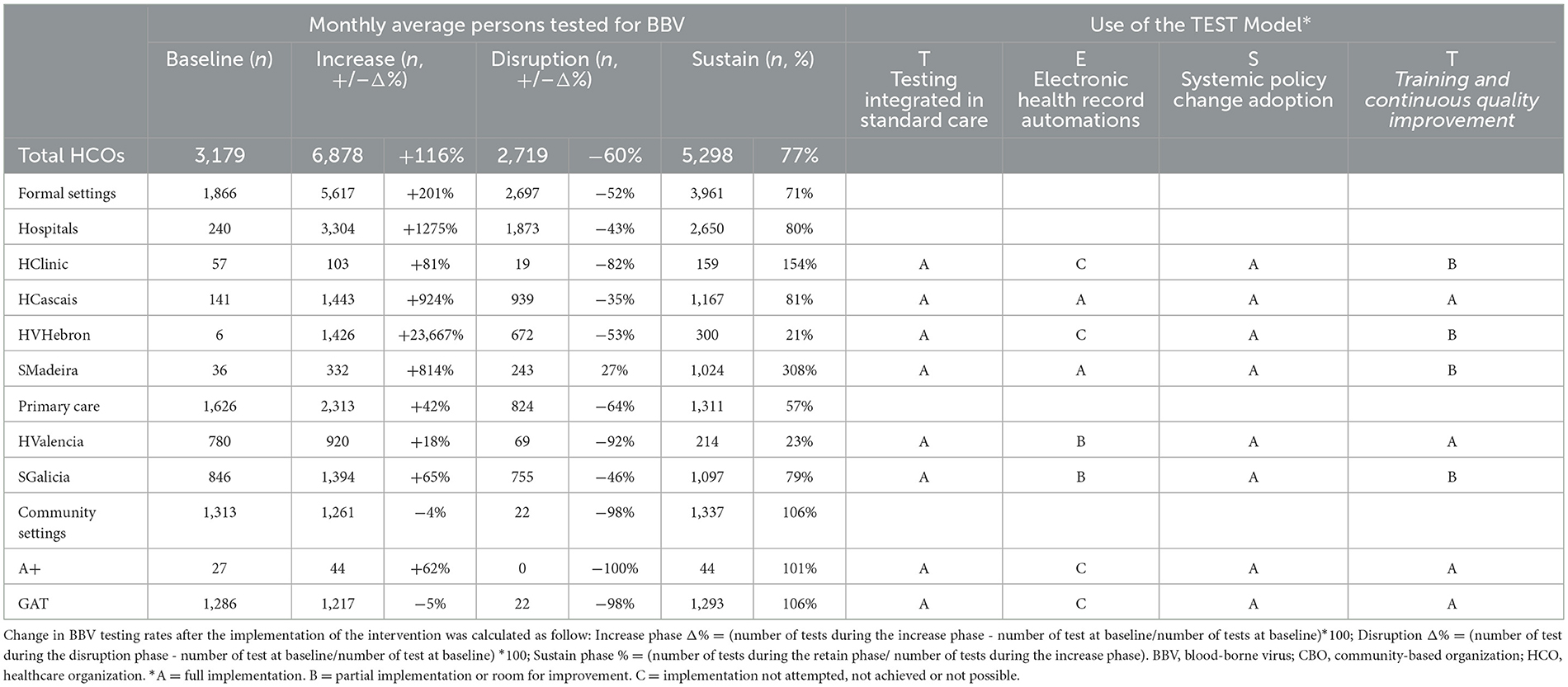
Table 2. BBV testing volume variation and adherence to the TEST model in participant organizations.
HCOs were successful in scaling up testing, with positive variation from baseline in all but 1 organization (GAT), and a global increase of 116% (ranging from −5% to +23,667%) in testing volume in the “increase” phase, as summarized in Table 1. Prevalence of HIV and HBV was higher in CBOs than in formal healthcare settings (1.2% vs. 0.8% for HIV Ab+; 0.6% vs. 0.5% for HBsAg+). Formal healthcare settings recorded the largest increases in testing volume (201%); of these, primary care recorded a more modest increase (42%), while hospital-based models of care recorded a global 14-fold (1,275%) increase in testing. HValencia was unsuccessful in implementing the screening in its ED due to the imposition of written opt-in consent forms by its local Ethics Committee, which proved too burdensome for the fast-paced environment of a large ED.
The first period of COVID-19 pandemic-related restrictions on freedom of movement (variously described as stay-at-home orders, shutdowns, or lockdowns) lasted from 15 March to 25 April 2020 in Spain, and from 19 March to 4 May 2020 in Portugal. All organizations observed an immediate combined 60% decrease in testing volume in the “disruption” phase. CBVCTs were the most affected sites, with a global 98% decrease in testing volume as lockdowns forced them to halt all activities. Formal healthcare settings observed a global 52% decrease in testing volume with heterogeneous effects depending on specific settings and the degree of implementation of the TEST model. HCOs that implemented SLTC protocols targeting patients seeking secondary care observed the smallest reduction in testing volume, at 43%. In contrast, those targeting patients in a primary care setting observed a larger reduction of 64%. The HCOs were most successful in implementing the “E” pillar of the TEST model — meaning using their EHR systems to automate patient eligibility assessment and laboratory orders— observed the smallest reduction in testing volume, at 31% (HCascais, SMadeira). In comparison, HCOs that did not use their EHR systems for this purpose observed a larger reduction of 78% (HVHebron, HClinic, A+).
As COVID-19 lockdowns were lifted, organizations recovered 77% of their average monthly testing in the “sustain” phase. As shown in Figure 1, CBVCTs showed the fastest, fullest recovery of testing volume post reopening, recovering 106% of their average monthly testing within 2 months. Although they were more vulnerable to the effects of restrictive pandemic control measures, they also showed the highest resilience of all organizations analyzed, further strengthening the case for investing in community-based organizations involved in BBV prevention. Formal healthcare settings, globally, had recovered 71% of their average monthly testing within 4 months. HCOs showed the strongest recovery in the “E” pillar of the TEST model, with a global 123% recovery of average monthly testing vs. 46% recovery in those not using EHR automations.
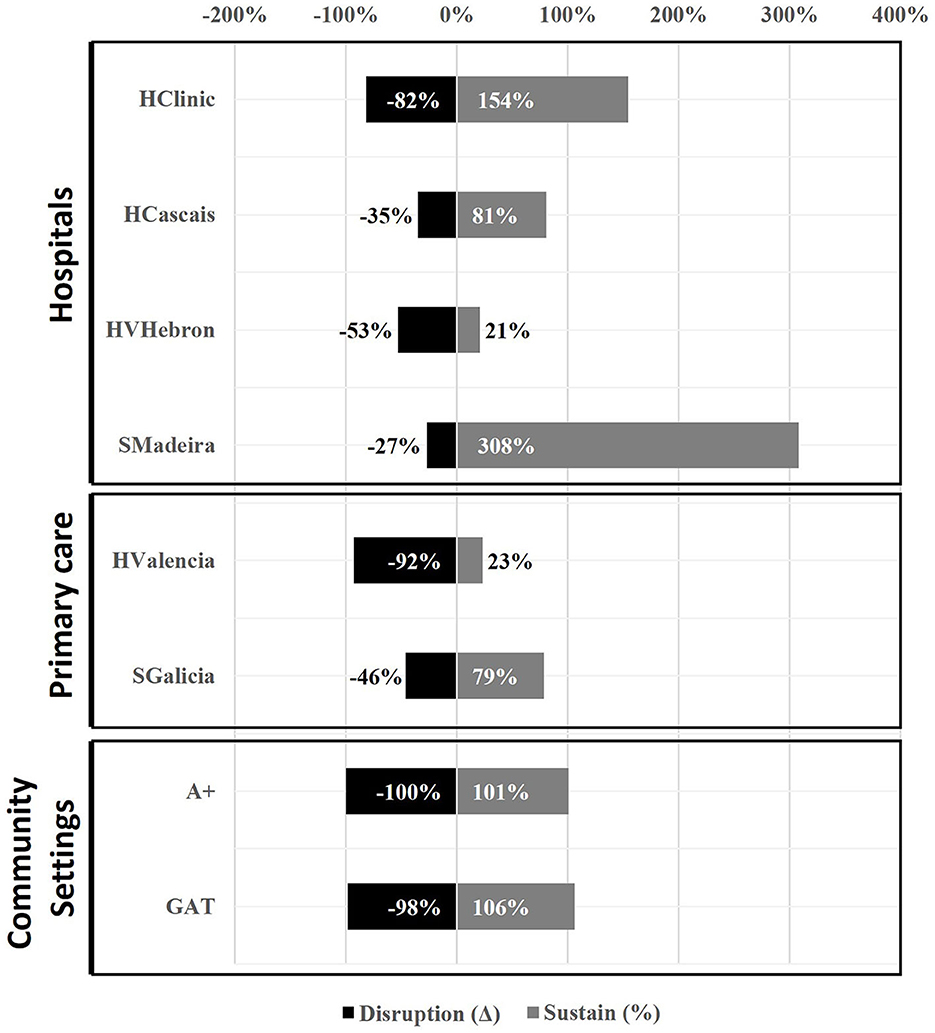
Figure 1. Blood borne viruses testing volume variation at participant organizations during the “disruption” phase and proportion of recovery in the “sustain” phase.
Although HVHebron initially showed one of the most remarkable increases in testing, it only recovered 21% of its average monthly testing volume after the lockdowns – the lowest of all HCOs. Following feedback from frontline ED staff and implementation of PDSA cycles, HVHebron has since changed its protocol and reduced the extent of human intervention in their enhanced SLTC program, thereby implementing the tenets of the “E” pillar of the TEST model. As of December 2021, HVHebron had managed to increase its testing output to 56% of its average monthly testing from before lockdowns.
The ANOVA test showed differences between the time periods evaluated, although they were not statistically significant (p = 0.059) (Table 3). There were no statistical differences between types of HCO (p = 0.774) when adjusting for time trends, neither in the interaction between different time trends and types of HCO (p = 0.296).
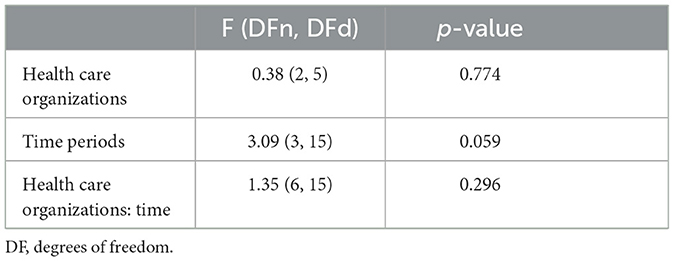
Table 3. Summary of the ANOVA test.
In addition to testing scale-up, other aspects were considered when assessing the merits of this intervention. The implementation of enhanced screening protocols allowed HCOs to diagnose a total of 1,860 patients over the study period (i.e., 1,139 HIV Ab+, 285 HBsAg+, 436 HCV RNA+, Table 4), of which 1179 were diagnosed during the “increase” phase, 79 during the “disruption” phase and 607 during the sustain phase. It is unlikely that these 79 patients (i.e., 58 HIV Ab+, 3 HBsAg+, 18 HCV RNA+) would have been diagnosed during this lockdown period were it not for the enhanced SLTC protocols, considering the lockdowns and travel restrictions. HCOs also diagnosed 4 acute HIV infections (AHI) over the study period. Since patients presenting with AHI have the highest likelihood of transmission to others, this is a significant contribution to individual and public health. HValencia recorded remarkable improvements in diagnosing late HIV presentation, from 52% to 33%, and diagnosed 94% and 69% of HBV and HCV patients, respectively, before the onset of severe liver disease. HCascais recorded an even more remarkable decrease in late HIV presentation, from 78% to 40% of patients diagnosed in the ED.
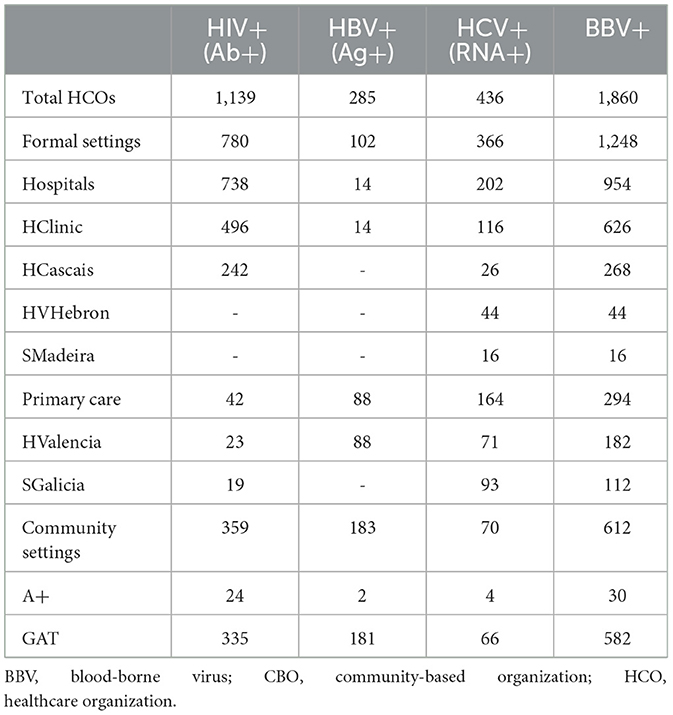
Table 4. Blood borne viruses diagnoses.
Testing volumes increased by 116% after the launch of the TEST model for enhanced SLTC, with formal healthcare settings recording larger increases than CBOs. While 1 participating CBO (A+) recorded a 62% increase in testing in the increase phase, some other (GAT) experienced a 5% decrease in testing due to staff budget control measures that reduced patient consultation hours over that period. Although our primary outcome measure of success was changes in testing volume, other variables were also meaningfully impacted. Specifically, the number of BBVs diagnoses were also enhanced (1860 diagnoses over the study period) and time from a positive test result to confirmation was reduced from weeks to hours following implementation of point of care RNA reflex testing in GAT. Although this significantly improves SLTC practices, it was not reflected in an increase in testing.
The effect of the implementation of the screening intervention and the impact of the COVID-19 pandemic differed according to the type of HCO analyzed. In CBVCTs, BBV testing was practically brought to a standstill during lockdowns. However, once they opened after the worst phase of the pandemic, tests numbers rapidly increased to pre-lockdown rates. One of the reasons for the fast recovery in CBVCTs was the high demand for pre-exposure prophylaxis (PrEP) after reopening, showing that levels of sexual activity did not vary during lockdowns. In addition, the 2 participating CBVCTs quickly adapted to the epidemiologic situation by implementing measures to increase their testing capacity, such as increasing the number of patient examination rooms and opening tents next to mobile units. These strategies, together with an increase in social media activity, led to a rapid recovery in testing rates. In contrast, formal settings in which the intervention was implemented in the ED (HCascais, HClinic), lockdowns did not drastically reduce testing compared to pre-pandemic rates, particularly if automation had been implemented, as EDs remained open. Furthermore, individuals seeking care for COVID-19 might have been tested for HIV, since the same social determinants of health increase the risk of infection in both diseases (30). In addition, individuals with symptomatic but untreated HIV might also have been at increased risk of symptoms requiring emergency care. Indeed, during the pandemic, patients with HIV have been shown to be more likely to seek emergency care than primary care or telehealth services (31).
Similar results have been reported in other countries. For instance, in an urban ED of a US hospital with a universal HIV screening program also including automated EMR, the volume of testing performed during the pre-pandemic period and pandemic period was not significantly different, in agreement with what we found in the formal settings in which testing intervention was implemented in the ED (32). On the other hand, a European survey on 71 CBVCTs services from 28 countries checking on the impact of COVID-19 pandemic on BBVs testing demonstrated a very major decrease (>50%) in the volume of testing for all the infections in this setting, in agreement with the results of our study (33). However, it is important to point out that while BBV screening should be broadly encouraged, it should also be tailored to the various situations. The opportunistic opt-out screening approach used in this study helps minimize any factors that might discourage participation, ensuring that individuals have the freedom to decline this or any other routine clinical investigations, thereby respecting their right to make informed choices about their healthcare (29).
However, in some cases, particularly in locations where disease prevalence is low, targeted screening to high-risk population may be more effective and cost-efficient. In those cases, it is important to establish appropriate default risk criteria to guide decision-making. Key considerations for defining default risk criteria include gather and analyse accurate and up-to-date prevalence data specific to the region or setting in question, consider the local epidemiological factors, including the incidence and distribution of BBVs, conduct a comprehensive risk assessment, refer to relevant national and international guidelines and regulations among others.
Although the COVID-19 pandemic reduced the number of in-person visits, it drove the development of other health care services, including telehealth, which are often used to educate patients and increase awareness of the importance of preventive care. However, despite efforts to provide alternatives to in-person care, COVID-19 and the resulting disruption of health systems may increase new infections and mortality rates for years to come.
Interestingly, some institutions reported that the profile of patients accessing testing during the pandemic differed with respect to the pre-pandemic period. Both SGalicia and SMadeira observed an increase in the proportion of non-native patients accessing care. Due to travel and work restrictions during the pandemic, immigrants might have remained in those communities longer than planned, forcing them to seek health care in their host countries. A considerable proportion of patients seen in HVHebron during lockdowns were also vulnerable immigrants. According to this hospital in Barcelona, patients with psychiatric and psychological disorders were also more frequently seen. This may correlate with a higher prevalence of psychiatric disease among people living with HIV or HCV (34, 35) for whom mental health care services may have been disrupted (36), while COVID-19 has exacerbated mental health conditions such as depression, social isolation, emotional distress, and substance abuse both in the general population and in people living with HIV (37, 38).
Our findings highlight the importance of using EHR systems to automate screening. HCOs that used their EHR systems to automate patient eligibility assessment and laboratory orders (fully implementing the tenets of the “E” pillar of the TEST model, level A in Table 1) had the smallest reduction in testing volume compared with organizations not using their systems for this purpose (partial or no implementation of the “E” pillar, levels B and C in Table 1) with 31% vs. 78%, respectively. Integration of HIV, HBV, and HCV into the flow of other laboratory tests already performed by HCOs through automation of the EHR and other technologies enables some patients to receive their serological results before discharge, thus facilitating timely disclosure, counseling, and referral, and avoiding the need for a follow-up appointment to give them their positive result and refer them to outpatient care, which is frequently challenging. However, implementation of automations in some organizations is both technically difficult and time consuming.
Participation in the intervention resulted in a positive culture change among healthcare professionals and communities alike, and both groups stated, subjectively, that awareness of the importance of screening for BBVs has increased. Patient attitudes toward enhanced screening practices were determined by recording the rate of refusal to undergo screening, which the 2 HCOs that specifically recorded refusal rates among patients eligible for screening (HCascais and SMadeira) estimated at <10%. This shows that the intervention was successful in reducing the stigma associated with testing.
Our study has several limitations. We did not conduct a systematic audit of culture and practices, and thus our assessments may contain some inaccuracies. We were unable to adjust for unmeasured confounders and did not evaluate possible modifiers of the effect of factors such as HCO size, number of healthcare workers involved, and other environmental factors. Existing SLTC practices differed considerably among participating HCOs, as did eligibility criteria for screening (e.g., different age cut-off points for inclusion/exclusion in screening, or symptoms suggestive of infection, in 1 case). The exact duration, in months, of each phase of implementation (i.e., baseline, increase, disruption, sustain) also differed among HCOs, as they were included in the project on a rolling basis and lockdown restrictions varied according to geography. Those differences in the times or seasons where the intervention was implemented could potentially expose individuals to varying environmental factors or disease prevalence and impact the observed results. Also, the heterogeneity in baseline risk (ED patients may inherently present with higher baseline risks, whereas primary care or organization-based screenings may target populations with different risk profiles) can influence screening outcomes.
The data presented correspond to entries made by participants in a shared monitoring database provided by laboratory or information technology departments. The figures could not be externally verified due to information governance issues and are thus susceptible to error. Our study compared performance with historical baseline testing volume rates. The quality of these data was called into question in some HCOs, particularly regarding second-line confirmatory testing. In addition to confirming new infections, HIV and HCV RNA tests may also be requested to monitor known infections, and this may have given a skewed perception that baseline practices were higher than they really were when appropriate control measures were not put in place (e.g., coding tests according to patient profile or requesting department). These potential errors were eliminated by using first-line antibody and serology tests alone as our baseline, as these are not repeated for patients already in care.
The degree of implementation of the TEST model is likely highly context-dependent, and limits the extent to which our results can be extrapolated to other organizations. Some HCOs did not have the resources or autonomy to fully implement the intervention. Some formal healthcare organizations in Spain and Portugal may lack the quality improvement culture needed to consistently support an iterative process that requires changes to be made at various time points, other than merely at the start of the intervention. This was somewhat mitigated by comparing our results with other interventions implementing the TEST model in the US (23–27) and conceptually similar interventions in the UK, which reported a 78% increase in HIV testing (39).
In interpreting the effect of the TEST model, we may have overlooked some positive and negative outcomes, such as the possible halo effect caused by increased healthcare staff awareness of the importance of screening, which could have increased testing beyond the established protocol, as seen in primary care centers in the HValencia. On the other hand, because staffs were aware that patients would likely be enrolled in screening where EHR modifications had been made, they could have reduced screening for indicator conditions and situations associated with high BBV prevalence, as seen in the ED of HCascais. This could be corrected by staff re-training or by including indicator conditions as further triggers for screening.
Although participant organizations also monitored their healthcare navigation process and corresponding LTC rates to ensure patients attended a first post-diagnosis visit with a specialist, we did not analyse this information in this study due to data quality concerns. Some HCOs refer patients to other organizations for care, and these do not always provide timely or accurate feedback on the success of patient LTC. Other organizations refer patients to in-house departments but record LTC rates of 100% which, according to the literature, are likely to be inaccurate. Where data quality was consistent, average LTC rates increased at the start of the intervention, only to decrease with the introduction of lockdown. However, further research is needed to establish the impact of the intervention and of the pandemic on LTC, an integral part of any meaningful screening program.
Our study did not include factors relating to cost-effectiveness analysis (CEA) of this quality improvement intervention, which is crucial for policymaking at the regional or national scale. However, previous CEA have found that HIV screening in the population is cost-effective for antibody prevalence of ≥0.1% in the US (40), ≥0.2% in the UK (41), and ≥0.06% in Portugal (42). On the other hand, HBV screening in the general population is cost-effective for HBsAg prevalence of ≥0.3% in the US (43), and ≥0.25% in the UK (41). For HCV screening in the general population, it is cost-effective for antibody prevalence of ≥0.07% in the US, HCV RNA prevalence of ≥0.26% in the UK (41) ≥0.13% in Spain (44) and ≥0.16% in Italy (45). Since we estimate that the cost of consumables and human resources is lower in Spain and Portugal than in the UK and the US, and that the HIV, HBV, and HCV prevalence figures found in our study are equal to or higher than the afore-mentioned thresholds, we hypothesize that BBV screening in the study populations will also be cost-effective in Spain and Portugal. However, this needs to be confirmed in detailed CEA studies.
Implementation of the TEST model enabled HCOs to increase and sustain BBV screening, even during COVID-19 lockdowns. Considering the ECDC's call for countries to increase test coverage and uptake, and the worldwide disruptions in BBV screening following the start of the SARS-CoV-2 pandemic, our study shows that effective, resilient, evidence-based models can increase screening. Additional research is needed to develop equally resilient patient linkage to care models in challenging times, and to assess the cost-effectiveness of this strategy.
The raw data supporting the conclusions of this article will be made available by the authors upon reasonable request.
Gilead Sciences' FOCUS Program funding supported screening and linkage to a first healthcare appointment after diagnosis, regardless of subsequent patient management. The studies involving humans were approved by the Local Ethics Committees of the eight participating centers. The studies were conducted in accordance with the local legislation and institutional requirements. The Ethics Committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants' legal guardians/next of kin because Offering BBV screening is considered standard clinical practice in both Spain and Portugal. Local Ethics Committees were asked to give their opinion when enhanced screening practices required modifying consent procedures from written opt-in consent to oral opt-out consent.
IV-P: Conceptualization, Formal analysis, Methodology, Supervision, Validation, Writing—original draft, Writing—review & editing, Investigation. EO: Methodology, Supervision, Validation, Writing—review & editing, Conceptualization, Investigation. IC: Methodology, Supervision, Validation, Writing—review & editing, Conceptualization, Investigation. MB: Methodology, Supervision, Validation, Writing—review & editing, Conceptualization, Investigation. JT-V: Methodology, Supervision, Validation, Writing—review & editing, Conceptualization, Investigation. VM-P: Methodology, Supervision, Validation, Writing—review & editing, Conceptualization, Investigation. MR: Methodology, Supervision, Validation, Writing—review & editing, Conceptualization, Investigation, Project administration, Resources. JG: Methodology, Supervision, Validation, Writing—review & editing, Conceptualization, Investigation. CE-S: Project administration, Writing—review & editing, Data curation, Investigation. MG: Project administration, Writing—review & editing, Data curation, Investigation. TM: Project administration, Writing—review & editing, Data curation, Software. MM: Project administration, Writing—review & editing, Data curation. VG: Project administration, Writing—review & editing, Data curation. JL-A: Project administration, Validation, Writing—review & editing, Data curation, Investigation, Methodology, Software, Supervision. AB-D: Project administration, Writing—review & editing, Data curation. SP: Project administration, Writing—review & editing, Data curation, Software. SD: Project administration, Writing—review & editing, Data curation. EX: Project administration, Validation, Writing—review & editing, Data curation, Investigation. MV: Project administration, Writing—review & editing, Data curation, Resources, Supervision. GG: Project administration, Writing—review & editing, Data curation, Investigation, Supervision. MH: Project administration, Writing—review & editing, Data curation. DM: Conceptualization, Data curation, Formal analysis, Supervision, Validation, Writing—review & editing, Funding acquisition, Investigation, Methodology, Project administration, Resources, Writing—original draft. MG: Methodology, Supervision, Validation, Writing—review & editing, Conceptualization, Investigation.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. We acknowledge funding from Gilead Sciences' FOCUS program to support HIV and viral hepatitis screening and linkage to the first medical appointment after diagnosis. FOCUS funding does not support activities beyond the first medical appointment and is agnostic to how HCOs handle subsequent patient care and treatment.
All authors met the authorship criteria set forth by the International Committee for Medical Journal Editors and retained complete control of the manuscript content. Vanessa Marfil Vives of Medical Statistics Consulting, Spain provided editorial support in the form of medical writing, assembling tables, and creating high-resolution images based on the authors' detailed instructions, collating author comments, copyediting, fact-checking, and referencing. Sofia Campos of ICF International performed data monitoring and management.
DM owns stock in and is an employee of Gilead Sciences. Data collection and management were conducted independently, with additional oversight of independent data monitoring agencies.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1268888/full#supplementary-material
1. Unidad de Vigilancia del VIH ITS y hepatitis en España Sistema de información sobre nuevos diagnósticos de VIH registro nacional de casos de SIDA. Instituto de Salud Carlos III, Madrid (2023). Actualización del continuo de atención del VIH en España, 2021-2022. Available online at: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/VIH/informes%20de%20vigilancia%20VIH%20y%20sida%20anteriores/Informe%20VIH_SIDA_2022_CCAA.pdf
2. Direção-Geral da Saúde/Instituto Nacional de Saúde Doutor Ricardo Jorge,. InfeçãO VIH e SIDA em Portugal - 2022. In: Instituto Nacional de Saúde Doutor Ricardo Jorge (INSA) e a Direção-Geral da Saúde (DGS) Available online at: https://repositorio.insa.pt/bitstream/10400.18/8383/3/Relato%cc%81rio_VIH_Portugal_2022_Vjulho2023.pdf
3. Dirección General de Salud Pública. Unidad de Vigilancia de VIH ITS y hepatitis en España. Instituto de Salud Carlos III. Vigilancia Epidemiológica Del VIH y SIDA en Espanña 2021. Sistema de Información sobre nuevos diagnóSticos de VIH y Registro Nacional de casos de SIDA. Available online at: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/VIH/informes%20de%20vigilancia%20VIH%20y%20sida%20anteriores/Informe%20VIH_SIDA_2022_CCAA.pdf
4. Carvalhana SC, Leitao J, Alves AC, Bourbon M, Cortez-Pinto H. Hepatitis B and C prevalence in Portugal: disparity between the general population and high-risk groups. Eur J Gastroenterol Hepatol. (2016) 28:640–4. doi: 10.1097/MEG.0000000000000608
5. del Amo J. Avances En La Política De Cribado De La Hepatitis C En El Sns. Retos en la Salud Pública Para la Enfermedad Hepática. San Lorenzo de El Escorial: Universidad Complutense de Madrid (2020).
6. European Centre for Disease Prevention Control (ECDC). Hepatitis B Annual Epidemiological Report for 2021. Stockholm ECDC (2020). Available online at: https://www.ecdc.europa.eu/sites/default/files/documents/hepatitis-b-annual-epidemiological-report-2021-1.pdf
7. Mugavero MJ, Castellano C, Edelman D, Hicks C. Late diagnosis of HIV infection: the role of age and sex. Am J Med. (2007) 120:370–3. doi: 10.1016/j.amjmed.2006.05.050
9. European Centre for Disease Prevention Control (ECDC). Public Health Guidance on Hiv, Hepatitis B and C Testing in the EU/EEA - an Integrated Approach. Stockholm (2018). Available online at: https://www.ecdc.europa.eu/sites/default/files/documents/hiv-hep-guidance-brief-6-december.pdf
10. UNAIDS. 90-90-90, an Ambitious Treatment Target to Help End the AIDS Epidemic. Geneva (2014). Available online at: https://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf
11. World Health Organization (WHO). Combating Hepatitis B and C to Reach Elimination by 2030: Advocacy Brief (2016) Available at: https://iris.who.int/bitstream/handle/10665/206453/WHO_HIV_2016.04_eng.pdf?sequence=1
12. Ministerio de Sanidad Servicios Sociales e Igualdad. Guía de recomendaciones para el diagnóstico precoz del VIH en el ámbito sanitario (2014). Available online at: https://www.sanidad.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/docs/GuiaRecomendacionesDiagnosticoPrecozVIH.pdf
13. Dirección General de Salud Pública Calidad e Innovación. Guía de cribado de la Infección por el VHC (2020). Available online at: https://www.sanidad.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/docs/GUIA_DE_CRIBADO_DE_LA_INFECCION_POR_EL_VHC_2020.pdf
14. Direção-Geral da Saúde. Norma 058/2011, Diagnóstico e Rastreio Laboratorial da Infeção pelo Vírus da Imunodeficiéncia Humana (VIH) (2014). Available online at: https://normas.dgs.min-saude.pt/wp-content/uploads/2019/09/diagnostico-e-rastreio-laboratorial-da-infecao-pelo-virus-da-imunodeficiencia-humana-vih.pdf
15. Direção-Geral da Saúde. Norma 027/2017, Avaliação diagnóstica da Infeção por Vírus da Hepatite C. (2017). Available at: https://normas.dgs.min-saude.pt/wp-content/uploads/2019/09/avaliacao-diagnostica-da-infecao-por-virus-da-hepatite-c.pdf
16. Rocha M, Pujol F, Berges J, Chanos SG, Mattioli, S, García, D. et al. High contribution, low public funding: Southern European Checkpoints' role in HIV detection in 4 countries. HepHIV 2019 Bucharest Conference: Challenges of Timely and Integrated Testing and Care. Bucharest. (2019).
17. Rao A. HIV self-test during the time of COVID-19, India. Indian J Med Res. (2020) 152:164–7. doi: 10.4103/ijmr.IJMR_2521_20
18. Zuniga JM. Continuity of HIV care in the presence of Covid-19. AIDS Rev. (2020) 22:131–2. doi: 10.24875/AIDSRev.20000074
19. Kowalska JD, Skrzat-Klapaczynska A, Bursa D, Balayan T, Begovac J, Chkhartishvili N, et al. HIV care in times of the COVID-19 crisis - where are we now in central and eastern europe? Int J Infect Dis. (2020) 96:311–4. doi: 10.1016/j.ijid.2020.05.013
20. Buti M, Dominguez-Hernandez R, Casado MA. Impact of the COVID-19 pandemic on HCV elimination in Spain. J Hepatol. (2020). doi: 10.1016/j.jhep.2020.12.018
21. Brown LB, Spinelli MA, Gandhi M. The interplay between HIV and COVID-19: summary of the data and responses to date. Curr Opin HIV AIDS. (2021) 16:63–73. doi: 10.1097/COH.0000000000000659
22. Prabhu S, Poongulali S, Kumarasamy N. Impact of COVID-19 on people living with HIV: a review. J Virus Erad. (2020) 6:100019. doi: 10.1016/j.jve.2020.100019
23. Lin X, Dietz PM, Rodriguez V, Lester D, Hernandez P, Moreno-Walton L, et al. Routine HIV screening in two health-care settings–New York City and New Orleans, 2011-2013. MMWR Morb Mortal Wkly Rep. (2014) 63:537–41.
24. White DAE, Giordano TP, Pasalar S, Jacobson KR, Glick NR, Sha BE, et al. Acute HIV discovered during routine HIV screening with HIV antigen-antibody combination tests in 9 us emergency departments. Ann Emerg Med. (2018) 72:29–40. doi: 10.1016/j.annemergmed.2017.11.027
25. Crumby NS, Arrezola E, Brown EH, Brazzeal A, Sanchez TH. Experiences implementing a routine HIV screening program in two federally qualified health centers in the southern United States. Pub Health Rep. (2016) 131 Suppl 1:21–9. doi: 10.1177/00333549161310S104
26. Haukoos JS, Lyons MS, White DA, Hsieh YH, Rothman RE. Acute HIV infection and implications of fourth-generation HIV screening in emergency departments. Ann Emerg Med. (2014) 64:547–51. doi: 10.1016/j.annemergmed.2014.07.004
27. Anderson ES, Galbraith JW, Deering LJ, Pfeil SK, Todorovic T, Rodgers JB, et al. Continuum of care for hepatitis C virus among patients diagnosed in the emergency department setting. Clin Infect Dis. (2017) 64:1540–6. doi: 10.1093/cid/cix163
28. Sanchez TH, Sullivan PS, Rothman RE, Brown EH, Fitzpatrick LK, Wood AF, et al. A novel approach to realizing routine HIV screening and enhancing linkage to care in the United States: protocol of the focus program and early results. JMIR Res Protoc. (2014) 3:e39. doi: 10.2196/resprot.3378
30. Millett GA. New pathogen, same disparities: why COVID-19 and HIV remain prevalent in U.S. communities of colour and implications for ending the hiv. Epidemic J Int AIDS Soc. (2020) 23:e25639. doi: 10.1002/jia2.25639
31. Khazanchi R, Winkelman TNA, Pandita D, Jelinek R, Shearer RD, Bodurtha PJ. Patient characteristics and subsequent health care use by location of SARS-CoV-2 testing initiation in a safety-net health system. JAMA Netw Open. (2021) 4:e2112857. doi: 10.1001/jamanetworkopen.2021.12857
32. Stanford KA, Friedman EE, Schmitt J, Spiegel T, Ridgway JP, Moore M, et al. Routine screening for HIV in an urban emergency department during the COVID-19 pandemic. AIDS Behav. (2020) 24:2757–9. doi: 10.1007/s10461-020-02899-x
33. Fernandez-Lopez L, Simoes D, Casabona J, Euro TC-IACoP. Impact of the COVID-19 pandemic on community-based testing for HIV, viral hepatitis and sexually transmitted infections in the who European region, March to August 2020. Eur J Public Health (2023) 33:528–35. doi: 10.1093/eurpub/ckad010
34. Hoare J, Sevenoaks T, Mtukushe B, Williams T, Heany S, Phillips N. Global systematic review of common mental health disorders in adults living with HIV. Curr HIV/AIDS Rep. (2021) 18:569–80. doi: 10.1007/s11904-021-00583-w
35. Yeoh SW, Holmes ACN, Saling MM, Everall IP, Nicoll AJ. Depression, fatigue and neurocognitive deficits in chronic hepatitis C. Hepatol Int. (2018) 12:294–304. doi: 10.1007/s12072-018-9879-5
36. Del Amo J, Diaz A, Polo R. The impact of coronavirus disease 2019 on people with Hiv. Curr Opin Infect Dis. (2022) 35:9–14. doi: 10.1097/QCO.0000000000000799
37. Serafini G, Parmigiani B, Amerio A, Aguglia A, Sher L, Amore M. The psychological impact of COVID-19 on the mental health in the general population. QJM. (2020) 113:531–7. doi: 10.1093/qjmed/hcaa201
38. Kalichman SC, El-Krab R. Social and behavioral impacts of COVID-19 on people living with hiv: review of the first year of research. Curr HIV/AIDS Rep. (2021). doi: 10.1007/s11904-021-00593-8
39. Hsu D, Ruf M, Leong G, Douthwaite S. The London initiative for glandular fever HIV testing (light) initiative: integration of opt-out HIV tests in primary care glandular fever serology order-sets - simple, effective and sustainable increase in HIV testing in line with UK and European guidelines. HIV Med. (2020) 21:e21–e2. doi: 10.1111/hiv.12914
40. Branson BM, Handsfield HH, Lampe MA, Janssen RS, Taylor AW, Lyss SB, et al. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep. (2006) 55:1–17.
41. Williams J, Miners A, Harris R, Mandal S, Simmons R, Ireland G, et al. Cost-effectiveness of one-time birth cohort screening for hepatitis C as part of the national health service health check program in England. Value Health. (2019) 22:1248–56. doi: 10.1016/j.jval.2019.06.006
42. Yazdanpanah Y, Perelman J, DiLorenzo MA, Alves J, Barros H, Mateus C, et al. Routine HIV screening in portugal: clinical impact and cost-effectiveness. PLoS ONE. (2013) 8:e84173. doi: 10.1371/journal.pone.0084173
43. Nayagam S, Sicuri E, Lemoine M, Easterbrook P, Conteh L, Hallett TB, et al. Economic evaluations of HBV testing and treatment strategies and applicability to low and middle-income countries. BMC Infect Dis. (2017) 17:692. doi: 10.1186/s12879-017-2778-x
44. Crespo J, Cuadrado A, Perello C, Cabezas J, Llerena S, Llorca J, et al. Epidemiology of hepatitis C virus infection in a country with universal access to direct-acting antiviral agents: data for designing a cost-effective elimination policy in Spain. J Viral Hepat. (2020) 27:360–70. doi: 10.1111/jvh.13238
Keywords: blood borne viruses, screening, linkage to care (LTC), human immunodeficiency virus (HIV), HVB, HCV (hepatitis C), COVID-19
Citation: Vaz-Pinto I, Ortega E, Chivite I, Butí M, Turnes-Vázquez J, Magno-Pereira V, Rocha M, Garrido J, Esteves-Santos C, Guimaraes M, Mourão T, Martínez Roma M, Guilera V, Llaneras-Artigues J, Barreira-Díaz A, Pérez Cachafeiro S, Daponte Angueira S, Xavier E, Vicente M, Garrido G, Heredia MT, Medina D and García Deltoro M (2024) Increasing and sustaining blood-borne virus screening in Spain and Portugal throughout the COVID-19 pandemic: a multi-center quality improvement intervention. Front. Public Health 11:1268888. doi: 10.3389/fpubh.2023.1268888
Received: 31 July 2023; Accepted: 18 December 2023;
Published: 24 January 2024.
Edited by:
Reza Valadan, Mazandaran University of Medical Sciences, IranReviewed by:
Vasco Ricoca Peixoto, New University of Lisbon, PortugalCopyright © 2024 Vaz-Pinto, Ortega, Chivite, Butí, Turnes-Vázquez, Magno-Pereira, Rocha, Garrido, Esteves-Santos, Guimaraes, Mourão, Martínez Roma, Guilera, Llaneras-Artigues, Barreira-Díaz, Pérez Cachafeiro, Daponte Angueira, Xavier, Vicente, Garrido, Heredia, Medina and García Deltoro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Inês Vaz-Pinto, aW5lcy52YXoucGludG9AaG9zcGl0YWxkZWNhc2NhaXMucHQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.