
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 06 December 2023
Sec. Occupational Health and Safety
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1266864
This article is part of the Research Topic Mental Health in Healthcare Workers and its Associations with Psychosocial Work Conditions View all 32 articles
 Xianming Cai1,2,3
Xianming Cai1,2,3 Tianshuo Zhao2,3,4
Tianshuo Zhao2,3,4 Linyi Chen2,3,5
Linyi Chen2,3,5 Sihui Zhang2,3
Sihui Zhang2,3 Ailing Yu6Xihong Sun7Shengnan Gao8Yuanshan Zhang9
Ailing Yu6Xihong Sun7Shengnan Gao8Yuanshan Zhang9 Chao Wang2,4
Chao Wang2,4 Juan Du2,4
Juan Du2,4 Yaqiong Liu2,4
Yaqiong Liu2,4 Qing-Bin Lu2,3,4
Qing-Bin Lu2,3,4 Fuqiang Cui2,3,4*
Fuqiang Cui2,3,4*Objective: This study evaluated job burnout among primary healthcare workers (PHCWs) in China during the COVID-19 pandemic, explored its influencing factors, and examined PHCWs' preferences for reducing job burnout.
Method: We conducted a multicenter cross-sectional study in Heilongjiang, Sichuan, Anhui, Gansu, and Shandong Provinces. An electronic questionnaire survey was conducted through convenience sampling in communities from May to July 2022. We collected sociodemographic characteristics, job burnout level, job satisfaction, and preferred ways to reduce job burnout among PHCWs.
Results: The job burnout rate among PHCWs in China was 59.87% (937/1565). Scores for each dimension of job burnout were lower among PHCWs who had a better work environment (emotional exhaustion OR: 0.60; depersonalization OR: 0.73; personal accomplishment OR: 0.76) and higher professional pride (emotional exhaustion OR: 0.63; depersonalization OR: 0.70; personal accomplishment OR: 0.44). PHCWs with higher work intensity (emotional exhaustion OR: 2.37; depersonalization OR: 1.34; personal accomplishment OR: 1.19) had higher scores in all job burnout dimensions. Improving work environments and raising salaries were the preferred ways for PHCWs to reduce job burnout.
Conclusion: Strategies should be developed to improve job satisfaction among PHCWs, enhance their professional identity, and alleviate burnout to ensure the effective operation of the healthcare system, especially during periods of overwork.
Job burnout is an important issue in the field of occupational health. A response to prolonged exposure to workplace stress, burnout is a syndrome manifested by emotional exhaustion, depersonalization, and a diminished sense of personal accomplishment at work (1). Job burnout has three main characteristics: (1) a feeling of energy expenditure or exhaustion, (2) increased perceptual distance from work or negative work-related emotions or feelings of cynicism, and (3) lowered professional performance. Burnout can occur in various industries and can be costly, resulting in employee tardiness, absenteeism, turnover, decreased performance, or even negative employee health outcomes (2–5).
Studies in Europe and the US have shown that long work hours are a major cause of burnout (6, 7). The phenomenon of long work hours is commonly found among healthcare workers worldwide, and the situation is particularly critical in China (1). The long, high-intensity work hours characteristic of healthcare work cause these workers to be highly prone to burnout. Job satisfaction is defined as the extent that the health workers are positive, negative or affective toward their work (8). The 2011 China Primary Care Workforce Survey showed that low job satisfaction and high occupational burnout were widespread (9). It was confirmed that lower job satisfaction can significantly contribute to job burnout of healthcare workers (10, 11). Studies suggest that healthcare worker burnout has both direct and indirect negative effects on healthcare institutions, healthcare workers themselves, and patients, including errors in diagnosis and treatment (12, 13), lowered professionalism and efficiency in healthcare services (14), and risks to the health and safety of physicians (15, 16). Burnout can even affect the orderly functioning of the whole healthcare system (14). Compared with the West, Asia has limited research on healthcare worker burnout, although its overall level is quite high. Cross-sectional studies in Malaysia (17), Yemen (18), and Hong Kong (19) found that more than 30% of healthcare workers had a high degree of job burnout. The Maslach Burnout Inventory (MBI) is the most widely used scale for measuring job burnout, includes subscales purported to measure each of these three dimensions. Many researchers have found the MBI had the greatest predictive validity (20).
China has a large population (21) and 2.2 physicians per 1,000 people (22), which is below the World Health Organization's recommendation. As a result, Chinese healthcare workers generally work long hours and have heavy workloads. High levels of burnout are prevalent among China's healthcare workers. One systematic review estimated that the job burnout rate in the medical field in China was 66.5–76.9% (23). A national cross-sectional survey of physicians in Chinese tertiary hospitals found that 38.4% of respondents met the criteria for burnout (24).
Since 2019, the COVID-19 pandemic has brought new challenges to healthcare workers. Primary healthcare workers (PHCWs) in China have made great contributions and borne high work stress under the country's evolving pandemic-prevention policies. It is important, then, to assess the level of burnout among PHCWs in China during the COVID-19 pandemic, analyze the factors affecting burnout, and explore PHCWs' preferences for reducing job burnout to promote healthy career development. To this end, we conducted a cross-sectional study to assess the prevalence of burnout among PHCWs during the COVID-19 pandemic and explore the factors affecting burnout.
We used a cross-sectional survey method and selected five provinces (Heilongjiang, Sichuan, Anhui, Gansu, and Shandong) as survey sites to recruit subjects from May to July 2022. Using nonrandom convenience sampling, we recruited subjects from the community who met the survey criteria. The selected study subjects filled out an anonymous questionnaire via an online platform (Survey Star, Changsha Ran Xing Science and Technology, Shanghai, China). The key variables in the questionnaire were all required and assigned logical values. Data were screened according to the requirements of the study, finally the questionnaire information of 1,561 cases were selected, and then the database was locked.
The inclusion criteria for survey respondents included the following: they needed to be PHCWs who had online access so they could complete the survey. Participation was voluntary.
Sample size calculation was based on the cross-sectional survey design. The overall burnout indicator for healthcare work obtained from the data was approximately p = 0.3, α = 0.05, and d = 0.1 × p = 0.03. The sample size for a purely random sample was derived from the formula for cross-sectional survey sample size. Considering the sample size expansion (1.5–2.0 times) problem for nonrandom sampling, the minimum sample size is expanded to Nsrs = 897 × 1.5 = 1,346:
The questionnaire was divided into four parts:
(1) Basic sociodemographic characteristics, such as gender, technical title, work unit, years of work, and education level.
(2) Maslach Burnout Inventory (MBI): The MBI contains three dimensions: emotional exhaustion, depersonalization, and lack of personal accomplishment. The scale was designed by Maslach and Jackson (25) and was adapted and refined for China by ChaoPing Li of Renmin University of China.
(3) Job satisfaction, divided into three evaluation aspects: work environment, salary, and work intensity.
(4) Preferences for reducing job burnout: Five improvement methods are given: (1) awarding honorary certificates or titles, (2) reducing work intensity, (3) improving work environment, (4) providing opportunities for further education, and (5) increasing salaries. The survey of preference for improving job burnout adopts the method of option ranking. PHCWs were first asked to select the three options that they personally thought would be most effective in improving burnout, and then the three options were ranked from most important to least important.
Burnout was measured using the MBI scale, quantified using the Likert-type scale, and evaluated according to the SS′ scoring principle: SS′ = 0.4 × mean score for emotional exhaustion + 0.3 × mean score for depersonalization + 0.3 × (6 – mean score for personal accomplishment) (26, 27). Based on the scores, the subjects were divided into three categories: (1) no job burnout (0 ≤ SS′ < 1.50), (2) mild job burnout (1.50 ≤ SS′ < 3.50), and (3) severe job burnout (3.50 ≤ SS′ < 6).
In this study, mild and severe job burnout are regarded as the levels of job burnout that are in need of improvement; that is, the detection rate of job burnout is positive:
The questionnaire was analyzed using R 4.1.2 (R Development Core Team) and IBM SPSS AMOS 26.0.0 (IBM Corporation, Armonk, NY, USA). Differences were statistically significant at p < 0.05.
We used the chi-square test to analyze the correlation between the job burnout level of healthcare workers and demographic factors. Stepwise logistic regression was used to analyze the factors affecting job burnout. We established a structural equation model (SEM) based on theoretical assumptions and the factors affecting burnout to explore the path coefficients of potential variables influencing burnout. The generalized least-squares (GLS) method was used to estimate the path coefficients. We computed the fit of the model to the data using the following: chi-squared/degree of freedom (CMIN/df), root-mean-square error of approximation (RMSEA), goodness-of-fit index (GFI), adjusted goodness-of-fit index (AGFI), and comparative fit index (CFI). Furthermore, multigroup SEM was used to explore similarities and differences in the model according to age, gender, years of work, and whether engaged in new COVID-19-related work.
We used Thurstone's pairwise comparison method to analyze the ranked items of burnout improvement methods. In this method, option combination information is converted into pairwise comparison information, and the value of column j for row i is divided into three cases: Rα, Rβ, and Rγ. The formula for calculating the probability table pij and the scale value Si is
We collected 1,561 valid questionnaires. Among the investigated PHCWs, the average age was 37.50 ± 10.30 years, 1,139 (72.97%) were female, and 45.16% (705/1,561) worked in rural areas. Most worked in village clinics (45.16%) and community healthcare centers (41.13%). Table 1 shows the personal and professional characteristics of the respondents.
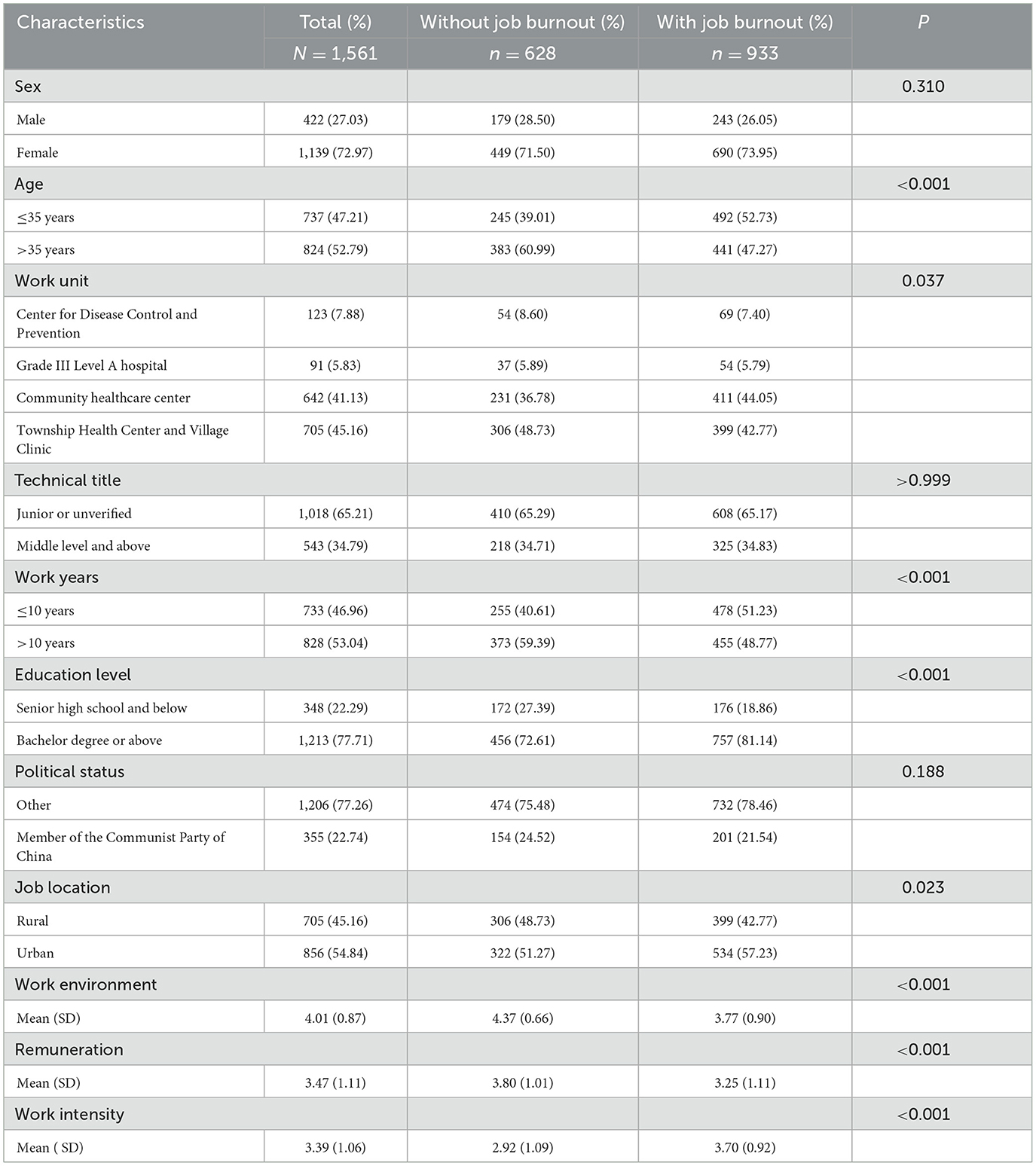
Table 1. Social demographic and burnout level of PHCWs.
The overall Cronbach's α coefficient of the Chinese version of the MBI scale in this study was 0.859. The internal Cronbach's α coefficients of the dimensions of emotional exhaustion, depersonalization, and personal accomplishment were 0.926, 0.914, and 0.843, respectively. The split-half reliabilities of emotional exhaustion, depersonalization, and personal accomplishment were 0.869, 0.712, and 0.878, respectively.
The χ2 value of Bartlett's sphericity test was 20,333.90, p < 0.001. The Kaiser–Meyer–Olkin measure of sampling adequacy was 0.922. Three factors with the characteristic root λ > 1 were extracted by exploratory factor analysis, and the cumulative variance contribution rate was 73.01%. Factors 1, 2, and 3 explained the three dimensions of personal accomplishment, depersonalization, and emotional exhaustion in the MBI scale, respectively (Supplementary Table S1).
The scores for the emotional exhaustion, depersonalization, and personal accomplishment dimensions of the PHCWs were 2.89 ± 1.38, 2.20 ± 1.34, and 3.74 ± 1.42 (see Supplementary Table S2).
The category scores measured by the MBI subscale were taken as the norm (28) and compared with our results. The mean scores for emotional exhaustion and depersonalization among Chinese PHCWs were higher than the general population norm and medical personnel norm; meanwhile, the mean scores for the personal accomplishment dimension were lower. All differences were statistically significant. This indicates that there is a high level of burnout among PHCWs in China (Supplementary Table S2).
The survey revealed that the burnout rate of PHCWs in China was 59.77% (933/1,561), among which 857 (54.90%) had mild burnout and 76 (4.87%) had severe burnout. Univariate statistical analysis revealed significant differences between burnout and non-burnout PHCWs for the following variables: age, work unit, years of work, education level, and work location (p < 0.05).
We established a logistic regression model using the stepwise regression method. Sociodemographic factors, work environment, work treatment, work intensity, and professional pride were included as independent variables in the initial logistic regression. Taking the no-job-burnout group as the control group, we conducted regression analysis with emotional exhaustion, personality disintegration, and personal accomplishment burnout (mild job burnout + severe job burnout) as dependent variables. Figure 1 shows the results.
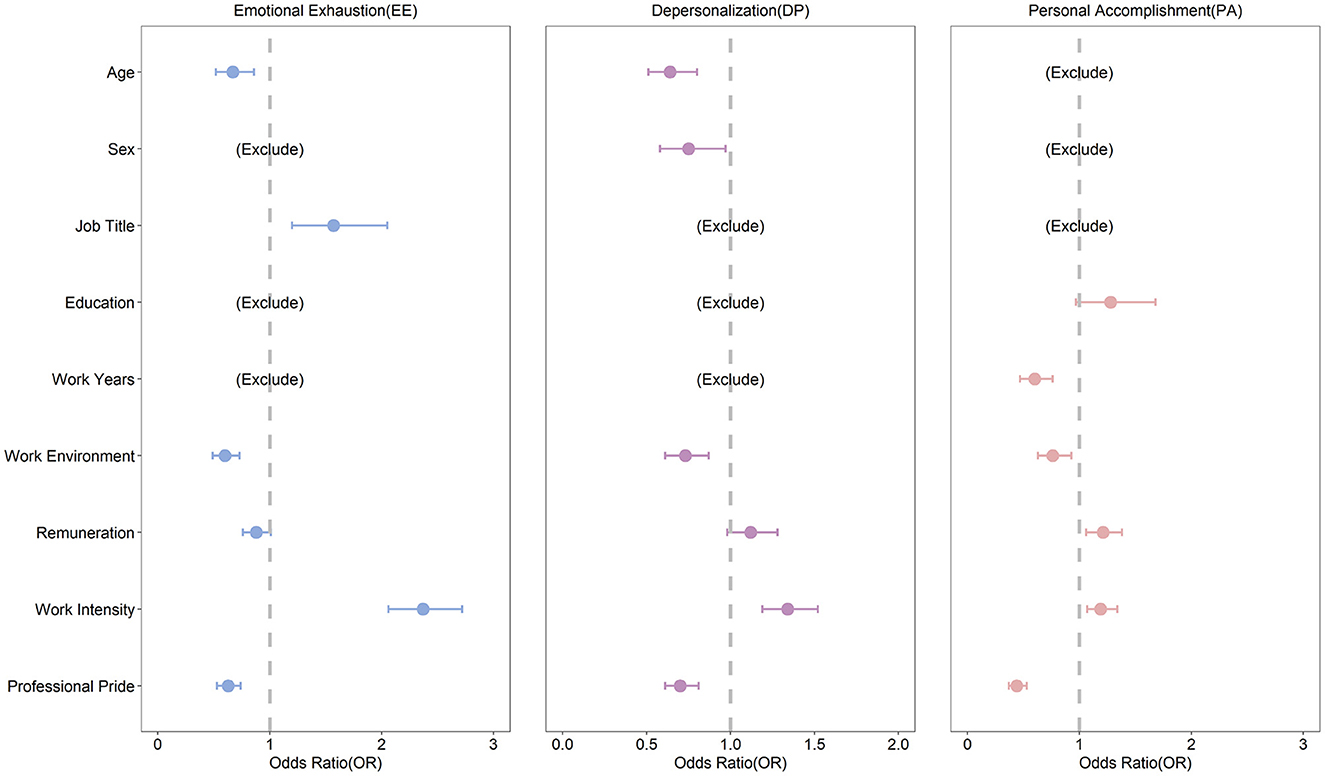
Figure 1. Forest plot of logistic analysis of burnout influencing factors.
For the emotional exhaustion dimension, the results showed that PHCWs aged > 35 years had lower scores for emotional exhaustion (OR: 0.67; 95% CI: 0.52–0.86). Better work environment (OR: 0.60; 95% CI: 0.49–0.73) and higher professional pride (OR: 0.63; 95% CI: 0.53–0.74) were associated with lower scores for emotional exhaustion. Meanwhile, PHCWs with high work intensity (OR: 2.37; 95% CI: 2.06–2.72) and higher technical titles (OR: 1.57; 95% CI: 1.20–2.05) had higher scores for emotional exhaustion.
For the depersonalization dimension, PHCWs aged > 35 years had lower depersonalization scores compared with those aged ≤ 35 years (OR: 0.64; 95% CI: 0.51–0.80). Females had lower depersonalization scores compared with males (OR: 0.75; 95% CI: 0.58–0.97). Similar to the emotional exhaustion dimension, better work environment (OR: 0.73; 95% CI: 0.61–0.87) and higher professional pride (OR: 0.70; 95% CI: 0.61–0.81) were associated with lower scores for depersonalization while high work intensity (OR: 1.34; 95% CI: 1.19–1.52) was associated with higher scores.
For the personal accomplishment dimension, over 10 years of work experience (OR: 0.60; 95% CI: 0.47–0.76), better work environment (OR: 0.76; 95% CI: 0.63–0.93), and lower professional pride (OR: 0.44; 95% CI: 0.37–0.53) were significantly associated with lower scores for personal accomplishment. Higher remuneration (OR: 1.21; 95% CI: 1.06–1.38) and higher work intensity (OR: 1.19; 95% CI: 1.07–1.34) were significantly associated with higher scores for personal accomplishment.
Based on this study's theoretical hypothesis and the previous analysis of the factors affecting job burnout, SEM was constructed as shown in Figure 2. There were three observed variables of social status: education, technical title, and workplace; three observed variables of job satisfaction: work environment, salary, and work intensity; and three observed variables of burnout: emotional exhaustion, personality disintegration, and personal fulfillment.
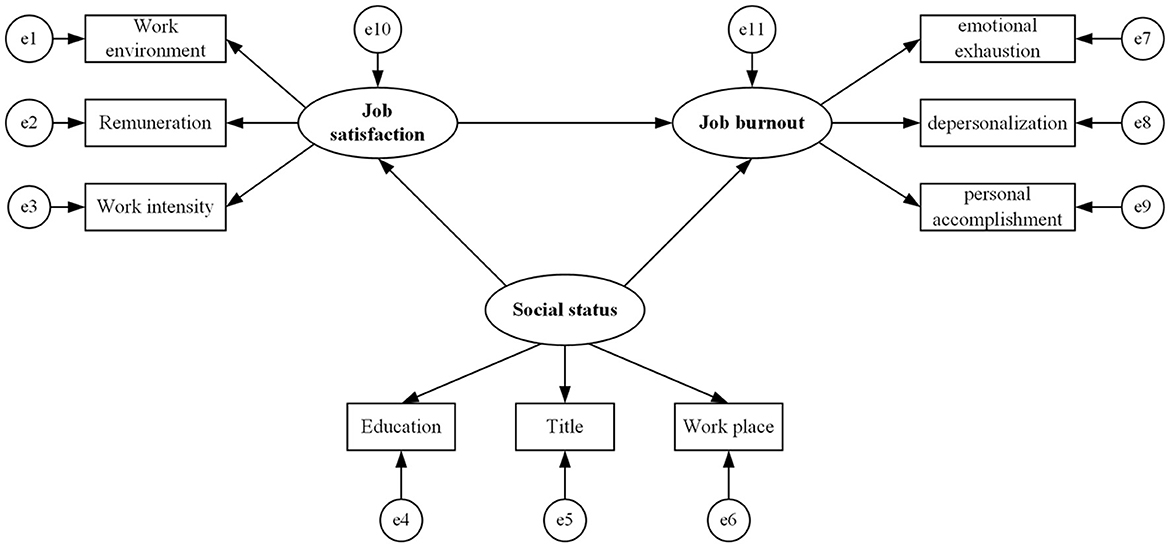
Figure 2. Structural equation model framework of job burnout.
The observed variable data were substituted into the SEM, and the model was fitted using the maximum likelihood method. The main fitting indexes of the model roughly reached the criteria for fitness, indicating acceptable model fit (Supplementary Table S3).
In the SEM, the standardized direct effect of job satisfaction on burnout was −0.352, that of social status on job satisfaction was −0.260, and that of social status on burnout was 0.165. All standardized direct effects were statistically significant. The regression coefficients of all observed variables of job satisfaction and social status reached statistical significance, indicating that each observed variable of the measurement model could explain the latent variables well.
We further used multigroup invariance modeling to explore the similarities and differences in the SEM between different groups to improve the empirical validity of the factors affecting burnout. We selected the sociodemographic variables of age, gender, years of work, and whether engaged in new COVID-19-related work for multigroup analysis.
PHCWs were divided into a younger group (≤35 years) and elder group (>35 years), a male and female group, a COVID-19-related work group and others, and a short work experience group (≤10 years) and long work experience group (>10 years). When the absolute value of the critical ratio of the path coefficient difference between different groups is >1.96, the corresponding path coefficient difference between groups is significant; that is, p < 0.05. Multigroup analysis showed that the influence of job satisfaction on job burnout was more significant among females (−3.079 vs. −1.940). The effect of social status on job burnout was more significant for the COVID-19-related work group (−0.221 vs. −0.029). There was no significant difference in the path coefficients among other models (Figure 3).
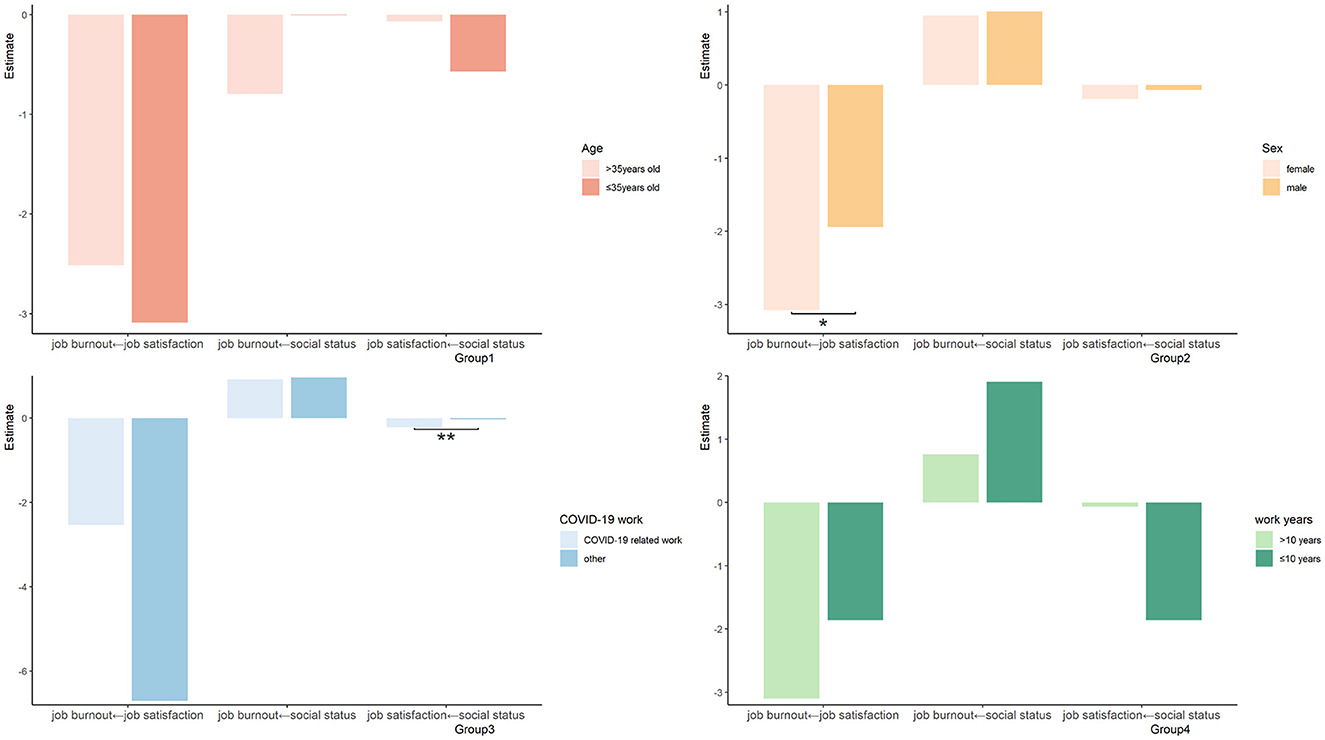
Figure 3. Multigroup invariance modeling of job burnout in different groups. *p < 0.05, **p < 0.01.
The option ranking method was used for the preferred ways to reduce job burnout. We presented five ways to reduce job burnout: (1) awarding an honorary certificate, (2) reducing work intensity, (3) improving the work environment, (4) providing opportunities for further study, and (5) Increasing wages.
Increasing wages (88.68%) and improving the work environment (83.09%) were found to be most effective. Analyzing the combination of options, most healthcare workers (34.98%) reduced their work intensity, improved their work environment, and increased their salaries. According to the ranking analysis of the importance of the options, the most effective healthcare workers (64.95%) can improve the work environment (Figure 4).
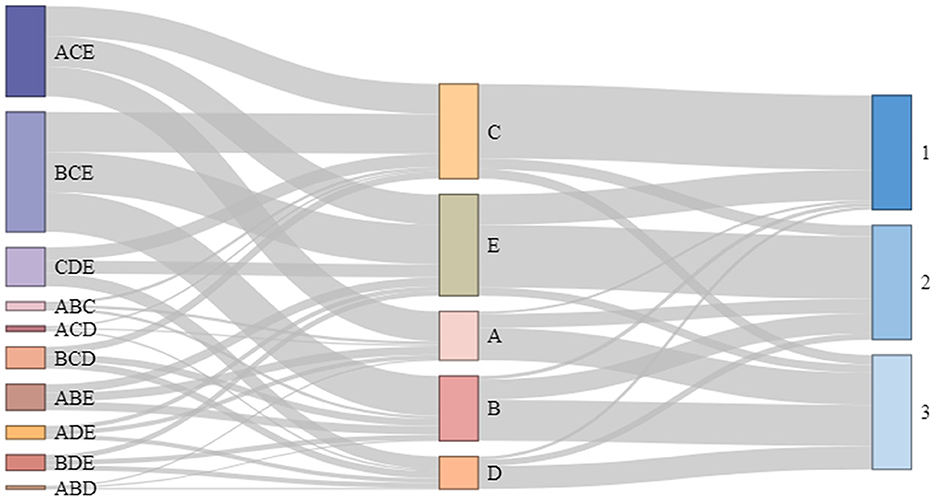
Figure 4. Sankey diagram of preference for improving job burnout. (A) Awarding an honorary certificate, (B) Improving work intensity, (C) Improving work environment, (D) Providing opportunities for further study, and (E) Increasing wages and allowances.
Based on the Thurston method, the scale values of the five options (1, 2, 3, 4, and 5) were ranked on a psychological valence chart. The results showed that the most-preferred ways for PHCWs to reduce job burnout were improving the work environment (0.913) and increasing salaries (0.810). Meanwhile, the scale values of awarding honorary certificates or titles (−0.342), reducing work intensity (−0.594), and providing opportunities for further study (−0.787) were all negative (Supplementary Figure S1).
The MBI scale has been widely used to measure job burnout. During COVID-19, this scale was used in Italy, the US, Belgium, India, Singapore, and other countries to measure the job burnout of frontline healthcare workers, and its reliability and validity were verified (29–32).
We used a modified Chinese version of the MBI burnout scale to conduct a presurvey and test scale reliability and validity at 10 sites in Heilongjiang, Sichuan, Gansu, Anhui, and Shandong Provinces. The Cronbach's α coefficients for emotional exhaustion, depersonalization, and personal accomplishment were >0.7, demonstrating that the scale had good reliability, internal consistency, and external consistency.
The overall reported job burnout rate among PHCWs was about 60%; mild burnout accounted for 55%, and severe burnout accounted for 5%. Galanis summarized 16 studies where the MBI was used to measure nurses' job burnout and found that the emotional exhaustion rate was 34%, the personality disintegration rate was 12%, and the low personal achievement rate was 15% (33). Compared with previous findings, the job burnout rate among PHCWs in China was found to be significantly higher (34, 35), suggesting that this issue warrants attention in China.
The results suggested that job burnout among PHCWs is characterized by high emotional exhaustion, high personality disintegration, and low personal accomplishment, among which the score for personal accomplishment was significantly below the norm. This is similar to the findings of Hu et al. (36) and Parandeh et al. (37). It can be attributed to the fact that PHCWs in China were mostly engaged in repetitive tasks with high work pressure and long work hours during the pandemic (38) and may have encountered unsupportive or uncooperative patients (39).
PHCWs played an important role in the struggle to contain COVID-19 (40). From 2020 to 2022, China's approach to the pandemic shifted from “zero clearing” to “dynamic clearing” (41, 42). PHCWs took on the tedious work of COVID-19 patient treatment, nucleic acid testing, epidemiological investigation, vaccination, isolation and prevention, and decontamination (43, 44), which involved long work hours and high work pressure.
The factors affecting burnout were diverse and changed over time, and could be both subjective and objective. Our findings showed that burnout level was associated with the age, years of work, education level, and work location of healthcare workers. Among them, age ≥ 35 years, better work environments, and more professional pride inhibited emotional exhaustion while more intense work exacerbated it. Gambaro et al.'s study on job burnout of healthcare workers also showed a negative correlation between age and job burnout. Similar to our findings, work experience has been shown to supply healthcare workers with the knowledge and emotion regulation skills they need to mitigate burnout (45). During the COVID-19 pandemic, healthcare staff with higher titles often had to assume more responsibilities, thus leading to emotional exhaustion (8, 46).
The depersonalization dimension was similar to that of emotional exhaustion. Therefore, PHCWs who are younger, have higher technical titles, and have higher work intensity should be the focus of interventions for burnout. In addition, females were less likely to show symptoms of depersonalization (i.e., holding negative or inappropriate attitudes toward their work objects) (47). Previous studies have also shown that female healthcare workers have more empathy for patients, better understand patients, and devote more time to them (48–50).
In the personal accomplishment dimension, healthcare workers with more than 10 years of work experience had lower levels of personal fulfillment. Studies have shown that longer years of work are usually a contributing factor to burnout (51, 52). Different from previous studies, we found that those with high work intensity showed a higher level of personal accomplishment (36). This reflects the sense of social responsibility and dedication shown by Chinese healthcare workers during the pandemic (38).
Our results highlight the important role of job satisfaction in reducing healthcare workers' job burnout. SEM showed that improving job satisfaction could reduce job burnout. Our findings partly confirm Goulet's and Singh theory of career commitment—that is, job satisfaction has a negative effect on job burnout (53). Therefore, as an important factor affecting PHCWs' professional development, job satisfaction should be an important intervention strategy in occupational health (54). Social status also affects the job satisfaction of healthcare workers, thus affecting job burnout. Thus, more attention should be paid to groups with higher social status (38).
Among the ways to reduce the job burnout among PHCWs, improving the work environment and increasing wages are the most important. During the COVID-19 pandemic, healthcare workers often worked in isolation wards and temporary nucleic acid test sites, and the work environments were relatively harsh, which could easily lead to burnout (38). Healthcare workers expressed the most dissatisfaction with the remuneration dimension. PHCWs in China have low salaries but bear higher workloads, greater risks of infection, and heavier physical and mental pressure (8, 55, 56). Incentive policies should be implemented to improve healthcare workers' job satisfaction and alleviate burnout by increasing their income.
This study used a cross-sectional survey that only reflected burnout levels at the time of the survey. Preexisting psychopathological conditions should be taken into consideration. It would be beneficial to confirm causality with longitudinal data in future studies. Second, we used the revised MBI scale to measure job burnout. Although the scale has good reliability and validity, it might be slightly different from the norm, which reduces comparability to some extent. Finally, we used multicenter convenience sampling. Although the survey area was selected in consideration of economic and geographic location and balanced urban/rural distribution, it did not strictly follow random sampling for the whole country, and the sample had large gender differences. Our research was based on the respondents and did not collect the characteristics of non-respondents. Therefore, the conclusions only represent the respondents, which might lead to non-response bias and underestimate or overestimate the level of job burnout. Thus, caution should be exercised in extrapolating from the conclusions.
We found that PHCWs in China had high levels of job burnout during the COVID-19 pandemic. Job burnout among PHCWs was related to their age, years of work, education level, and workplace and was influenced by job satisfaction and professional identity. At present, PHCWs in China have average salaries but high work intensity. Improving their work environments and salaries could reduce their job burnout. Healthcare managers can refer to healthcare workers' preferred ways to reduce job burnout and provide support to maintain their work enthusiasm and thus the stability of the whole healthcare system.
We evaluated the level of job burnout among PHCWs in China during COVID-19, analyzed its influencing factors, and summarized the preferred ways to reduce job burnout. However, this study is a cross-sectional study with a risk of non-response bias. Further evaluation is needed to inform future practice.
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
This study was approved by the Ethics Committee of Peking University Health Science Center, China (approval number: IRB00001052-21132) and the signal-free informed consent application was approved.
XC: Data curation, Formal analysis, Investigation, Methodology, Software, Visualization, Writing – original draft. TZ: Data curation, Formal analysis, Investigation, Methodology, Software, Visualization, Writing – original draft, Writing – review & editing. LC: Investigation, Methodology, Validation, Writing – review & editing. SZ: Methodology, Writing – review & editing, Formal analysis. AY: Investigation, Supervision, Writing – review & editing. XS: Investigation, Supervision, Writing – review & editing. SG: Investigation, Supervision, Writing – review & editing. YZ: Investigation, Supervision, Writing – review & editing. CW: Investigation, Supervision, Writing – review & editing. JD: Investigation, Project administration, Supervision, Validation, Writing – review & editing. YL: Investigation, Project administration, Supervision, Validation, Writing – review & editing. Q-BL: Investigation, Project administration, Supervision, Validation, Writing – review & editing. FC: Data curation, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the National Key Research and Development Program of China (2021YFC2301604) and National Science and Technology Project on Development Assistance for Technology, Developing China-ASEAN Public Health Research and Development Collaborating Center (No. KY202101004). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1266864/full#supplementary-material
1. Thompson SL, Salmon JW. Strikes by physicians: a historical perspective toward an ethical evaluation. Int J Health Serv. (2006) 36:331–54. doi: 10.2190/B5CX-UX69-45LY-2D6D
2. Robinson SE, Roth SL, Keim J, Levenson M, Flentje JR, Bashor K. Nurse burnout: work related and demographic factors as culprits. Res Nurs Health. (1991) 14:223–8. doi: 10.1002/nur.4770140309
3. Parker PA, Kulik JA. Burnout, self- and supervisor-rated job performance, and absenteeism among nurses. J Behav Med. (1995) 18:581–99. doi: 10.1007/BF01857897
4. Lee RT, Ashforth BE, A. meta-analytic examination of the correlates of the three dimensions of job burnout. J Appl Psychol. (1996) 81:123–33. doi: 10.1037/0021-9010.81.2.123
5. Vahey DC, Aiken LH, Sloane DM, Clarke SP, Vargas D. Nurse burnout and patient satisfaction. Med Care. (2004) 42:Ii57–66. doi: 10.1097/01.mlr.0000109126.50398.5a
6. Barck-Holst P, Nilsonne Å, Åkerstedt T, Hellgren C. Coping with stressful situations in social work before and after reduced working hours, a mixed-methods study. Eur J Soc Work. (2021) 24:94–108. doi: 10.1080/13691457.2019.1656171
7. Khodadadi A, Ravari A, Sayadi A, khodadadi H, Jafarinaveh H. Occupational burnout assessment among nurses working in Iranian hospital of Ali-ebn Abitaleb, Rafsanjan- Iran. J Occup Health Epidemiol. (2012) 1:103–10. doi: 10.18869/acadpub.johe.1.2.103
8. Zhang LF, You LM, Liu K, Zheng J, Fang J-b, Lu M, et al. The association of Chinese hospital work environment with nurse burnout, job satisfaction, and intention to leave. Nurs Outlook. (2014) 62:128–37. doi: 10.1016/j.outlook.2013.10.010
9. Li X, Lu J, Hu S, Cheng KK, Maeseneer J, Meng Q, et al. The primary health-care system in China. Lancet. (2017) 390:2584–94. doi: 10.1016/S0140-6736(17)33109-4
10. Wang H, Jin Y, Wang D, Zhao S, Sang X, Yuan B. Job satisfaction, burnout, and turnover intention among primary care providers in rural China: results from structural equation modeling. BMC Fam Pract. (2020) 21:12. doi: 10.1186/s12875-020-1083-8
11. Scanlan JN, Still M. Job satisfaction, burnout and turnover intention in occupational therapists working in mental health. Aust Occup Ther J. (2013) 60:310–8. doi: 10.1111/1440-1630.12067
12. West CP, Tan AD, Habermann TM, Sloan JA, Shanafelt TD. Association of resident fatigue and distress with perceived medical errors. Jama. (2009) 302:1294–300. doi: 10.1001/jama.2009.1389
13. Shanafelt TD, Balch CM, Bechamps G, Russell T, Dyrbye L, Satele D, et al. Burnout and medical errors among American surgeons. Ann Surg. (2010) 251:995–1000. doi: 10.1097/SLA.0b013e3181bfdab3
14. Dyrbye LN, Shanafelt TD. Physician burnout: a potential threat to successful health care reform. JAMA. (2011) 305:2009–10. doi: 10.1001/jama.2011.652
15. Shanafelt TD, Balch CM, Dyrbye L, Bechamps G, Russell T, Satele D, et al. Special report: suicidal ideation among American surgeons. Arch Surg. (2011) 146:54–62. doi: 10.1001/archsurg.2010.292
16. West CP, Tan AD, Shanafelt TD. Association of resident fatigue and distress with occupational blood and body fluid exposures and motor vehicle incidents. Mayo Clin Proc. (2012) 87:1138–44. doi: 10.1016/j.mayocp.2012.07.021
17. Al-Dubai SAR, Ganasegeran K, Perianayagam W, Rampal KG. Emotional burnout, perceived sources of job stress, professional fulfillment, and engagement among medical residents in Malaysia. Sci World J. (2013) 2013:137620. doi: 10.1155/2013/137620
18. Al-Dubai SA, Rampal KG. Prevalence and associated factors of burnout among doctors in Yemen. J Occup Health. (2010) 52:58–65. doi: 10.1539/joh.O8030
19. Siu C, Yuen SK, Cheung A. Burnout among public doctors in Hong Kong: cross-sectional survey. Hong Kong Med J. (2012) 18:186–92.
20. Edwards D, Burnard P, Coyle D, Fothergill A, Hannigan B, A. stepwise multivariate analysis of factors that contribute to stress for mental health nurses working in the community. J Adv Nurs. (2001) 36:805–13. doi: 10.1046/j.1365-2648.2001.02035.x
21. Bank TW. Population of China [EB/OL]. (2021). Available online at: https://data.worldbank.org/country/china (accessed May 7, 2023).
22. Bank TW. World Development Indicators of China [EB/OL]. (2021). Available online at: https://databank.worldbank.org/reports.aspx?source=2&country=CHN (accessed May 7, 2023).
23. Lo D, Wu F, Chan M, Chu R, Li D. A systematic review of burnout among doctors in China: a cultural perspective. Asia Pac Fam Med. (2018) 17:3. doi: 10.1186/s12930-018-0040-3
24. Yao H, Wang P, Tang Y-L, Liu Y, Liu T, Liu H, et al. Burnout and job satisfaction of psychiatrists in China: a nationwide survey. BMC Psychiatry. (2021) 21:593. doi: 10.1186/s12888-021-03568-6
25. Maslach C, Jackson SE. The measurement of experienced burnout. J Organ Behav. (1981) 2:99–113. doi: 10.1002/job.4030020205
26. Ahola K, Gould R, Virtanen M, Honkonen T, Aromaa A, Lönnqvist J. Occupational burnout as a predictor of disability pension: a population-based cohort study. Occup Environ Med. (2009) 66:284–90; discussion 2–3. doi: 10.1136/oem.2008.038935
27. Kalimo R, Pahkin K, Mutanen P, Topipinen-Tanner S. Staying well or burning out at work: work characteristics and personal resources as long-term predictors. Workand Stress. (2003) 17:109–22. doi: 10.1080/0267837031000149919
28. Maslach CJSE, Leiter MP. Maslach burnout inventory manual. Palo Alto, VA: Consulting Psychologists Press (1996).
29. Lasalvia A, Amaddeo F, Porru S, Carta A, Tardivo S, Bovo C, et al. Levels of burn-out among healthcare workers during the COVID-19 pandemic and their associated factors: a cross-sectional study in a tertiary hospital of a highly burdened area of north-east Italy. BMJ Open. (2021) 11:e045127. doi: 10.1136/bmjopen-2020-045127
30. Lasater KB, Aiken LH, Sloane DM, French R, Martin B, Reneau K, et al. Chronic hospital nurse understaffing meets COVID-19: an observational study. BMJ Qual Saf. (2021) 30:639–47. doi: 10.1136/bmjqs-2020-011512
31. Bruyneel A, Smith P, Tack J, Pirson M. Prevalence of burnout risk and factors associated with burnout risk among ICU nurses during the COVID-19 outbreak in French speaking Belgium. Intens Crit Care Nurs. (2021) 65:103059. doi: 10.1016/j.iccn.2021.103059
32. Jose S, Dhandapani M, Cyriac MC. Burnout and resilience among frontline nurses during COVID-19 pandemic: a cross-sectional study in the emergency department of a tertiary care center, North India. Indian J Crit Care Med. (2020) 24:1081–8. doi: 10.5005/jp-journals-10071-23667
33. Galanis P, Vraka I, Fragkou D, Bilali A, Kaitelidou D. Nurses' burnout and associated risk factors during the COVID-19 pandemic: a systematic review and meta-analysis. J Adv Nurs. (2021) 77:3286–302. doi: 10.1111/jan.14839
34. Wang Z, Xie Z, Dai J, Zhang L, Huang Y, Chen B. Physician burnout and its associated factors: a cross-sectional study in Shanghai. J Occup Health. (2014) 56:73–83. doi: 10.1539/joh.13-0108-OA
35. Low ZX, Yeo KA, Sharma VK, Leung GK, McIntyre RS, Guerrero A, et al. Prevalence of burnout in medical and surgical residents: a meta-analysis. Int J Environ Res Public Health. (2019) 16:1479. doi: 10.3390/ijerph16091479
36. Hu D, Kong Y, Li W, Han Q, Zhang X, Zhu LX, et al. Frontline nurses' burnout, anxiety, depression, and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: a large-scale cross-sectional study. EClinicalMedicine. (2020) 24:100424. doi: 10.1016/j.eclinm.2020.100424
37. Parandeh A, Ashtari S, Rahimi-Bashar F, et al. Prevalence of burnout among health care workers during coronavirus disease (COVID-19) pandemic: a systematic review and meta-analysis. Prof Psychol Res Pract. (2022) 53:564–73. doi: 10.1037/pro0000483
38. Wan Z, Lian M, Ma H, Cai Z, Xianyu Y. Factors associated with burnout among Chinese nurses during COVID-19 epidemic: a cross-sectional study. BMC Nurs. (2022) 21:51. doi: 10.1186/s12912-022-00831-3
39. Sun H, Zhao Y. Analysis and consideration on the current situation of resource allocation of licensedregistered nurses in China(in Chinese). Chinese Hospitals. (2019) 23:42–5. doi: 10.19660j.issn.1671-0592.2019.06.14
40. Haldane V, De Foo C, Abdalla SM, Jung AS, Tan M, Wu S, et al. Health systems resilience in managing the COVID-19 pandemic: lessons from 28 countries. Nat Med. (2021) 27:964–80. doi: 10.1038/s41591-021-01381-y
41. Liu J, Liu M, Liang W. The dynamic COVID-zero strategy in China. China CDC Wkly. (2022) 4:74–5. doi: 10.46234/ccdcw2022.015
42. Li Z, Chen Q, Feng L, Rodewald L, Xia Y, Yu H, et al. Active case finding with case management: the key to tackling the COVID-19 pandemic. Lancet. (2020) 396:63–70. doi: 10.1016/S0140-6736(20)31278-2
43. Ministry of Commerce Peoples's Republic of China. The Joint Prevention and Control Mechanism of the State Council Press Conference Text 2020.05.16 [EB/OL]. (2020). Available online at: http://www.nhc.gov.cn/xcs/fkdt/202005/e78dfc196504497586f324f0d9a5bc36.shtml (accessed March 30, 2023).
44. Li Q, Liu W, Wang J-Y, Wang X-G, Hao B, Hu Y-B, et al. Prevalence and risk factors of post-traumatic stress disorder symptoms among Chinese health care workers following the COVID-19 pandemic. Heliyon. (2023) 9:e14415. doi: 10.1016/j.heliyon.2023.e14415
45. Gambaro E, Gramaglia C, Marangon D, Azzolina D, Probo M, Rudoni M, et al. The mediating role of gender, age, COVID-19 symptoms and changing of mansion on the mental health of healthcare workers operating in italy during the first wave of the COVID-19 pandemic. Int J Environ Res Public Health. (2021) 18:13083. doi: 10.3390/ijerph182413083
46. Xie J, Li J, Wang S, Li L, Wang K, Duan Y, et al. Job burnout and its influencing factors among newly graduated nurses: a cross-sectional study. J Clin Nurs. (2021) 30:508–17. doi: 10.1111/jocn.15567
47. Finstad GL, Giorgi G, Lulli LG, Pandolfi C, Foti G, León-Perez JM, et al. Resilience, coping strategies and posttraumatic growth in the workplace following COVID-19: a narrative review on the positive aspects of trauma. Int J Environ Res Public Health. (2021) 18:9453. doi: 10.3390/ijerph18189453
48. Fukui S, Wu W, Salyers MP. Impact of supervisory support on turnover intention: the mediating role of burnout and job satisfaction in a longitudinal study. Adm Policy Ment Health. (2019) 46:488–97. doi: 10.1007/s10488-019-00927-0
49. Cho E, Jeon S. The role of empathy and psychological need satisfaction in pharmacy students' burnout and well-being. BMC Med Educ. (2019) 19:43. doi: 10.1186/s12909-019-1477-2
50. Barnett MD, Martin KJ, Garza CJ. Satisfaction with work-family balance mediates the relationship between workplace social support and depression among hospice nurses. J Nurs Scholarsh. (2019) 51:187–94. doi: 10.1111/jnu.12451
51. Pradas-Hernández L, Ariza T, Gómez-Urquiza JL, Albendín-García L, De la Fuente EI, Cañadas-De la Fuente GA. Prevalence of burnout in paediatric nurses: a systematic review and meta-analysis. PLoS ONE. (2018) 13:e0195039. doi: 10.1371/journal.pone.0195039
52. Shiao JS, Koh D, Lo LH, Lim MK, Guo YL. Factors predicting nurses' consideration of leaving their job during the SARS outbreak. Nurs Ethics. (2007) 14:5–17. doi: 10.1177/0969733007071350
53. Goulet LR, Singh P. Career commitment: a reexamination and an extension. J Vocat Behav. (2002) 61:73–91. doi: 10.1006/jvbe.2001.1844
54. Chen H, Liu F, Pang L, Liu F, Fang T, Wen Y, et al. Are you tired of working amid the pandemic? The role of professional identity and job satisfaction against job burnout. Int J Environ Res Public Health. (2020) 17:9188. doi: 10.3390/ijerph17249188
55. Shi X, Xiong D, Zhang X, Han M, Liu L, Wang J. Analysis of factors influencing the job satisfaction of medical staff in tertiary public hospitals, China: A cross-sectional study. Front Psychol. (2023) 14:1048146. doi: 10.3389/fpsyg.2023.1048146
Keywords: job burnout, COVID-19, primary healthcare workers, occupational health, MBI scale
Citation: Cai X, Zhao T, Chen L, Zhang S, Yu A, Sun X, Gao S, Zhang Y, Wang C, Du J, Liu Y, Lu Q-B and Cui F (2023) Job burnout among primary healthcare workers during COVID-19 pandemic: cross-sectional study in China. Front. Public Health 11:1266864. doi: 10.3389/fpubh.2023.1266864
Received: 25 July 2023; Accepted: 13 November 2023;
Published: 06 December 2023.
Edited by:
Juan Gómez-Salgado, University of Huelva, SpainReviewed by:
Sok King Ong, Universiti Brunei Darussalam, BruneiCopyright © 2023 Cai, Zhao, Chen, Zhang, Yu, Sun, Gao, Zhang, Wang, Du, Liu, Lu and Cui. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fuqiang Cui, Y3VpZnVxQGJqbXUuZWR1LmNu
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.