
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 16 October 2023
Sec. Children and Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1259109
 MoezAlIslam E. Faris1,2*
MoezAlIslam E. Faris1,2* Fakir Al Gharaibeh3
Fakir Al Gharaibeh3 M. Rezaul Islam3Dana Abdelrahim2Eman Rashid Saif4Eman Ali Turki4Mahra Khalfan Al-Kitbi4Salma Abu-Qiyas1
M. Rezaul Islam3Dana Abdelrahim2Eman Rashid Saif4Eman Ali Turki4Mahra Khalfan Al-Kitbi4Salma Abu-Qiyas1 Falak Zeb2
Falak Zeb2 Hayder Hasan1,2
Hayder Hasan1,2 Mona S. Hashim1,2Tareq M. Osaili1,2,5
Mona S. Hashim1,2Tareq M. Osaili1,2,5 Hadia Radwan1,2
Hadia Radwan1,2 Leila Cheikh Ismail1,2
Leila Cheikh Ismail1,2 Farah Naja1,2Fatima Zohra Bettayeb3
Farah Naja1,2Fatima Zohra Bettayeb3 Reyad Shaker Obaid1,2
Reyad Shaker Obaid1,2Background: Consumption of caffeinated energy drinks (CED) has escalated during the last few years, especially among schoolchildren, with evident adverse health sequelae in this critical age group.
Objective: This study examined the prevalence of CED consumption and its associations with sleep, physical and mental health, and dietary and lifestyle habits among schoolchildren in the United Arab Emirates (UAE).
Method: A structured self-administered online questionnaire was developed and disseminated among schoolchildren aged 14–18 years, selected from schools of the seven emirates of the UAE.
Results: More than 4,500 (N= 4,648) responses received. A relatively low prevalence of CED consumption (20%) was found among schoolchildren in the UAE. However, those who reported CED consumption were more likely to report unhealthy dietary (skipping breakfast, frequent snacking, and eating fast foods, low fruit, and vegetable intake) and lifestyle behaviors (long screen time, poor sleep health), in addition to poor self-reported mental and physical health than non-users. CED consumption was significantly and variably associated with multiple sociodemographic factors such as students’ nationality, parental companionship, sex, school type, education level (children’s and parents’), daily allowance, academic performance, screen time, sleep quality parameters, self-reported physical and mental health, and parents’ employment. Sources of knowledge about CED were social media (55%), friends/schoolmates (52%), and family members (52%). Students believed that CED constitute sugar (87%), caffeine (69%), artificial flavors (67%) sweeteners (54%), and stimulating components (43%). The majority (70%) of students reported that CED consumption increases the risks for heart disease, diabetes, high blood sugar (65%), addiction (64%), high blood pressure (59%), and obesity (57%).
Conclusion: These results offer important insights for health professionals, child health specialists, policymakers, and parents in the UAE regarding adolescents’ attitudes, knowledge and behaviors toward CED consumption.
Caffeinated energy drinks (CED) are beverages that contain caffeine and are marketed as enhancing concentration, reducing fatigue, and increasing energy (1). Consumption of CED is alarmingly escalating throughout the globe, with major concern directed toward its increased consumption among schoolchildren and adolescents, which may impose adverse health consequences on this critical age group (2, 3). In the Gulf Corporation Council (GCC) countries, including UAE, consumption of CED is exponentially increasing among children and adolescents (4).
Excessive caffeine intake via products such as CED, coffee, tea, soda, and chocolate bars can impose negative effects on children, including anxiety and poor sleep (5). These adverse effects are ascribed to the inclusion of caffeine, guarana, and taurine in the CED, with supposed performance-enhancing effects; making CED not recommended food for children and adolescents (6, 7). Most recently, Puupponen et al. (8) found that regular intake of CED was linked to inadequate sleep, poor self-rated health, and various health issues. Common reasons for consuming CED include taste/flavor, feeling alert, and getting energy (9). However, many children and adolescents remain unaware of the ingredients of CED, including caffeine, and their health implications (10).
In the United States, consumption rates among schoolchildren were varied and based on age, sex, and ethnicity (11), with a consistent and strong direct relationship between CED consumption and risk-taking behaviors such as alcohol consumption. Such positive associations between CED consumption and alcohol intake, alongside cannabis use, snus use, problematic social media use, short sleep skipping breakfast, drunkenness, and inadequate tooth brushing; were all reported among Finnish schoolchildren (8). Further, the consumption of CED by schoolchildren is also concerning because of its associations with increased risks for aggressive behaviors: truancy, fighting, and bullying (12, 13). Lastly, the high levels of sugar and acid in CED make them erosive beverages that lead to tooth decay and enamel erosion, which can result in long-term dental health problems (14).
The prevalence of CED consumption by school children and adolescents has been a topic of interest during the last decade, with variable prevalence reported in different parts of the world. The prevalence ranged variably from 24.4% in Finland (15), 28.0–31.3% in Hungary (16, 17), about 12–33% in Ontario/Canada (18), 35% in New Zealand (19), 42.3% in the Pacific region (20), 41.4–75.5% in Italy (6, 21, 22), 51.2% in Australia (23), 61.7% in Germany (24), 62% in Atlantic/Canada (25), 63% in Congo (26), and about 66% in the United States (27). In the GCC, the prevalence of CED consumption by schoolchildren reached 45–60% among middle and secondary schoolchildren (28, 29). In the UAE, only one study in Al Ain City/UAE revealed a prevalence of 27% among schoolchildren (30). Considering the large number of schoolchildren in the UAE distributed over the seven emirates, it is crucial to have an accurate estimate of the prevalence of CED consumption among UAE schoolchildren and to examine the relationship with the different health aspects and dietary and lifestyle behaviors.
Due to the improved economic and purchasing power of the schoolchildren and adolescents in the UAE, many types of CED are becoming widely available and affordable, with noticeable and obvious consumption of CED by young schoolchildren seen in different community settings (despite the legal prohibition of selling CED for those who are younger than 16 years old). The parental knowledge and practices, with their educational levels and sociodemographic backgrounds, toward CED are of pivotal significance in exploring the practice of CED consumption among schoolchildren in the UAE. Due to the lack of large-scale national assessment for CED consumption in the UAE, it becomes crucial to examine the prevalence of CED consumption among schoolchildren and young adolescents, to find out its relationship with nutritional status, sleep quality, physical and mental health, and dietary and lifestyle behaviors, and to explore the relationship with parental knowledge and practices toward CED in the UAE.
The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement was followed in the planning, implementation, and reporting of the present work (31).
This study used a cross-sectional design to assess CED consumption among a convenience sample of Schoolchildren across the UAE. Data collection started in November 2021 and concluded in March 2022. Data were collected using an online self-administered questionnaire disseminated via Google Forms. The questionnaire was prepared for students in Grades 8–12 (corresponding to ages 14–18 years). These grades were chosen to ensure that participating students had reached puberty (which is commonly considered age 10–14 years in girls and 12–16 years in boys).
We used a non-probability convenience sampling technique. The questionnaire was disseminated to all schools in the seven Emirates via the administrative departments of education/Ministry of Education. The administrative departments directed the link of the electronic questionnaire to the administration of each school, who then disseminated the link to teachers and class masters during their online teaching. Using a 95% confidence level, 1% margin of error (alpha error), and response rate of 50% from a given population of approximately 130,000 secondary school students, we estimated that the minimum viable sample size for sufficiently powered analyzes was 894 students. The endpoint used to power the analysis assumed that ≥15% of students would consume CED daily (28).
The self-administered online questionnaire was prepared in both the Arabic and English languages and comprised structured, closed-ended questions. There were no open-ended or continuing questions, meaning the questionnaire was simple and quick to answer; it was estimated that the questionnaire would take around 10–15 min to complete based on a pilot test. The questionnaire covered six domains: first, sociodemographic (sex, nationality, Emirate, school type, grade, average grade, daily allowance, parental companionship, parental education, and occupational status) and anthropometric information (self-reported body weight and height); second, CED consumption (parental use of CED, frequency and amount of CED intake, source of information, health effects, reasons of consumption, and ingredients of CED); third, questions on diet (frequency of eating breakfast, fruits, vegetable, fast food, and energy-dense snack), and lifestyle (smoking, physical activity, smart device use) behaviors; fourth, self-reported physical health and frequency of reporting headache, stomach aches; fifth, self-reported mental health and frequency of reporting angry, nervous, anxious, or arguing, feeling lonely; and sixth, sleep quality parameters (night sleep duration, experiencing difficulty falling asleep).
The frequency of CED consumption was categorized as daily, three or more times/week, and less than three times/week. We then tested the associations between the frequency of CED consumption and sociodemographic factors, physical exercise habits, sleep habits, mental and physical health (self-reported), dietary habits, and parents’ education and employment status.
We evaluated the relationships between CED consumption (outcomes, dependent variables) and students’ health and well-being parameters (exposures, independent variables). Students’ nutritional status (as the prevalence of overweight and obesity), dietary behaviors servings of fruits and vegetables per day, eating/skipping breakfast, snacking on energy-dense snacks (such as cookies, ice cream, candies, crackers, chocolate bars, potato chips, soda), and eating fast foods (that energy-dense, easily prepared processed foods in the Westernized restaurants such as burgers, pizza, chicken or chips), lifestyle behaviors (physical activity level, smart device use, and smoking), and psychological characteristics were assessed as the main exposures. Sex, age (and corresponding school grade), nationality, place of residence (i.e., with whom the student lived), educational level, grade point average (GPA), and school type were the main moderators examined.
Categorical variables were described using frequencies and percentages. Descriptive data, including mean, standard deviation, minimum, and maximum, were evaluated for weight-related variables (weight, height, and body mass index [BMI]). BMI was estimated based on students’ self-reported weight and height and then described as defined by the World Health Organization (WHO) growth chart z-scores for ages 5–19 years. These charts divide children (by z-scores) into five categories: less than −3 (severely thin), between −3 and − 2 (thin), between −2 and + 1 (normal), between +1 and + 2 (overweight), and more than +2 (obese). The growth chart cut-off points were applied to the whole population using Anthroplus Survey software. Parents’ and students’ CED consumption were described using frequencies and percentages. Students’ dietary habits, sleep habits, exercise habits, and physical and mental health (self-reported) were also described using frequencies and percentages. Smart device use was categorized as never, not every day, <2 h/day, >2 h/day. Sleep hours were grouped into two categories: ≤7 h, and ≥ 8 h. GPA was categorized as <80% or ≥ 80%. Physical activity was categorized as adequate (very good, good, and adequate) or inadequate (poor and very poor). Crosstabs and Pearson’s chi-square tests were used to evaluate the associations between the frequency of CED consumption (never, less than three times/week, three or more times/week, daily) and students’ sociodemographic data, sleep and physical activity data, self-reported physical and mental health, and parents’ data. The sub-sample of students who consumed CED was used for multiple-answer questions relating to these drinks (sorted by choice), and the frequencies and percentages for these items were obtained separately (100% did not cover the whole sample). Graphical illustrations were provided for sociodemographic, BMI, and multiple-answer data. All data were encoded and analyzed using IBM SPSS version 26.0. All significance levels were set at p < 0.05.
Official permission to conduct this study was obtained from the Ministry of Education and ethical approval was obtained from the University of Sharjah Research Ethics Committee on September 24, 2021 (REC-21-06-18-01). This committee also approved the research protocol, informed consent, and research tools. Students were required to submit the online self-report questionnaire assessing their CED consumption, dietary and physical activity habits, and self-reported physical and mental health. Students completed the questionnaire in their regular class sections. Student and parent/guardian consent was necessary for participation in the study using an electronic consent form. Participation was voluntary; no monetary or non-monetary incentives were given and participants were informed that they could withdraw from this study at any time.
Our analysis included 4,648 students comprised of 3,021 males (65%) and 1,627 females (35%). More than half (54%) were non-Arab, followed by Emirati citizens (22.2%). The majority were from Sharjah (about 72%), followed by Ajman (13%) and Dubai (10%). The vast majority of participants were from private schools (88%). Nearly grades 8–10 contributed the same proportion of participants (22–23%), followed by grades 12 (18%) and 11 (14%). Around 40% of students had a GPA of ≥90%, followed by those who had 80–89% (32%). About 94% of students lived with their parents. The majority (73.2%) of students received a low daily allowance of <25 dirhams (about 7$) and 14.5% received 25–50 dirhams (6.75–13.5 $; Table 1). The majority of fathers (75%) and mothers (69%) had college- or university-level education. Most (91%) fathers were employed but only 34% of mothers were employed (Table 1). One-fifth (20%) of the students and 14% of parents consumed CED; only 2% of the student consumers used to drink CED daily (Table 2). In terms of dietary habits, more than two-thirds (about 68%) of students reported having breakfast every day, less than half (43%) had two or more servings of vegetables/day, and one-third (33%) had two or more servings of fruits/day. Almost 75% of students consumed one serving or less of fast food per week. Less than two-thirds (Around 65%) of students reported consuming energy-dense snacks twice or less/day. Almost all (98%) students were non-smokers. About half of the students were of normal weight, 23.8% were overweight, and 18.2% were obese (Table 2).
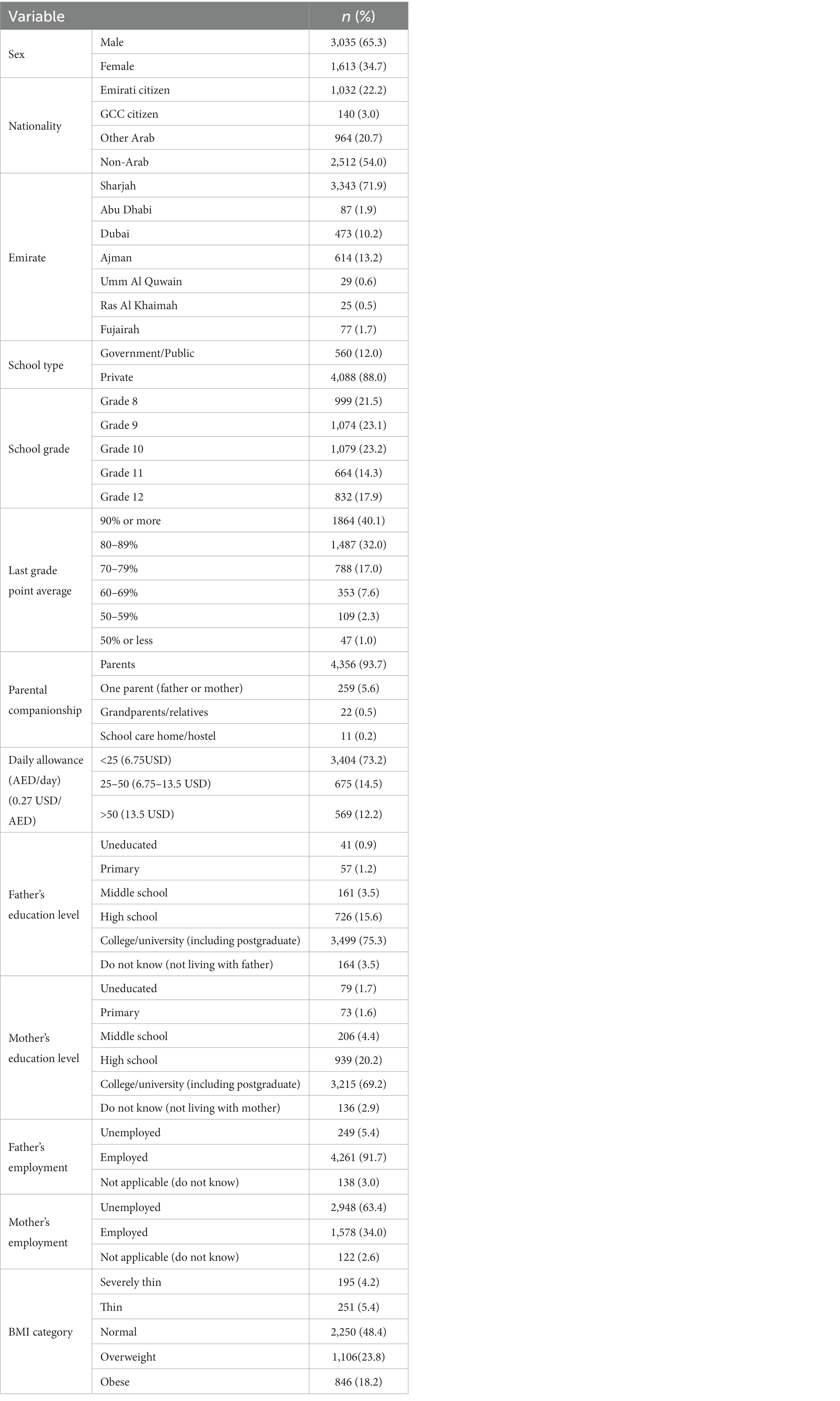
Table 1. Students’ sociodemographic and parental characteristics (N = 4,648).
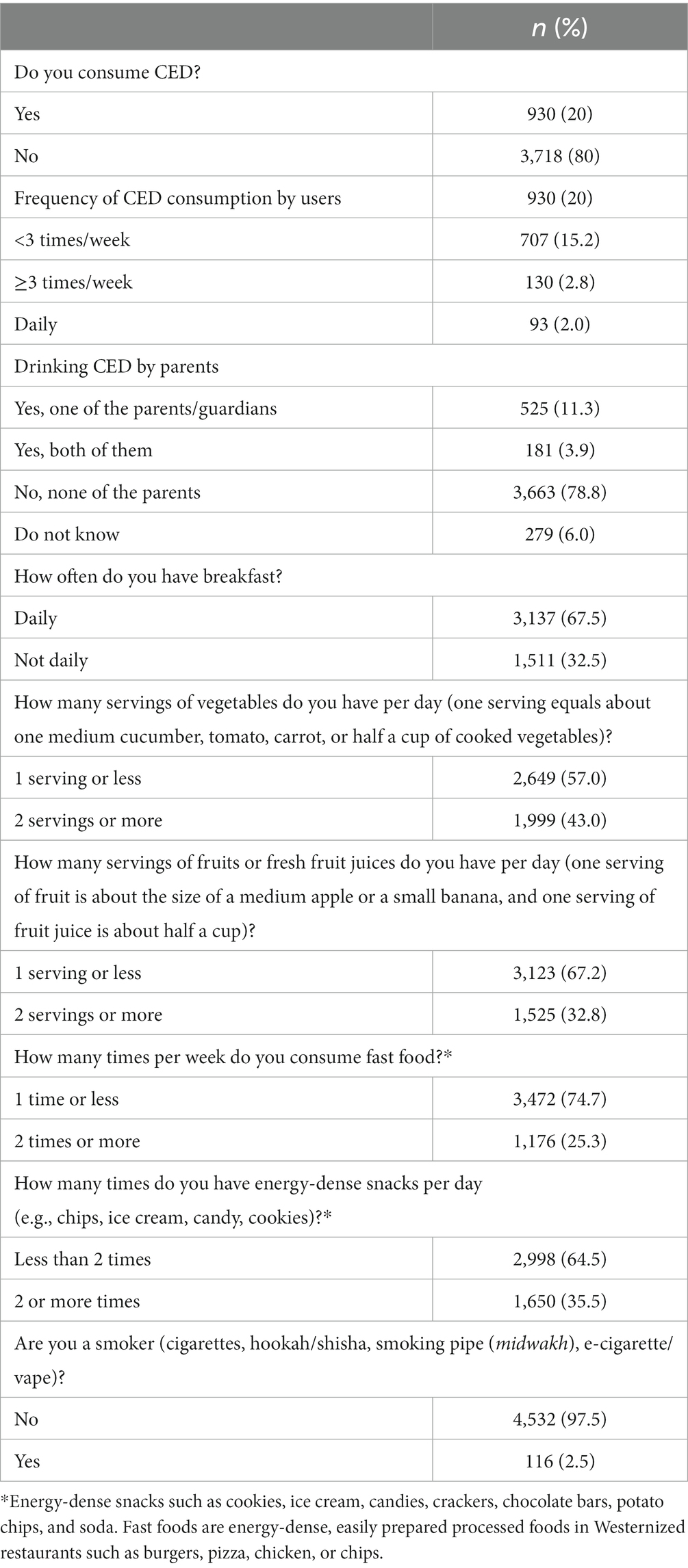
Table 2. Students’ CED consumption, and self-reported dietary and lifestyle habits (N = 4,648).
Reasons for consuming CED were their taste (18%), feeling energetic (11%), improving the ability to study (6%), and staying awake longer (6%) (Figure 1). Sources of information about CED among participants who consumed CED were social networking sites (around 55%), friends and schoolmates/peers (53%), and family members (51%) (Figure 2). Students reported some misconceptions about the ingredients of CED, although most (87%) believed that they contained sugar. More than two-thirds were aware of the CED content of caffeine (68%) and artificial flavoring (67%), fewer reported that CED may contain synthetic or artificial sweeteners (54%), carbon dioxide, and other gasses (45%), stimulating components or hormones (43%) and citric acid (41%) (Figure 3). Evaluation of students’ awareness about the long-term negative effects of the consumption of CED on their health showed commonly mentioned issues were heart disease and irregular heartbeat (70%), diabetes and high blood sugar (65%), addiction (64%), high blood pressure (59.5%), obesity (57%), and high blood lipids (40%) (Figure 4).
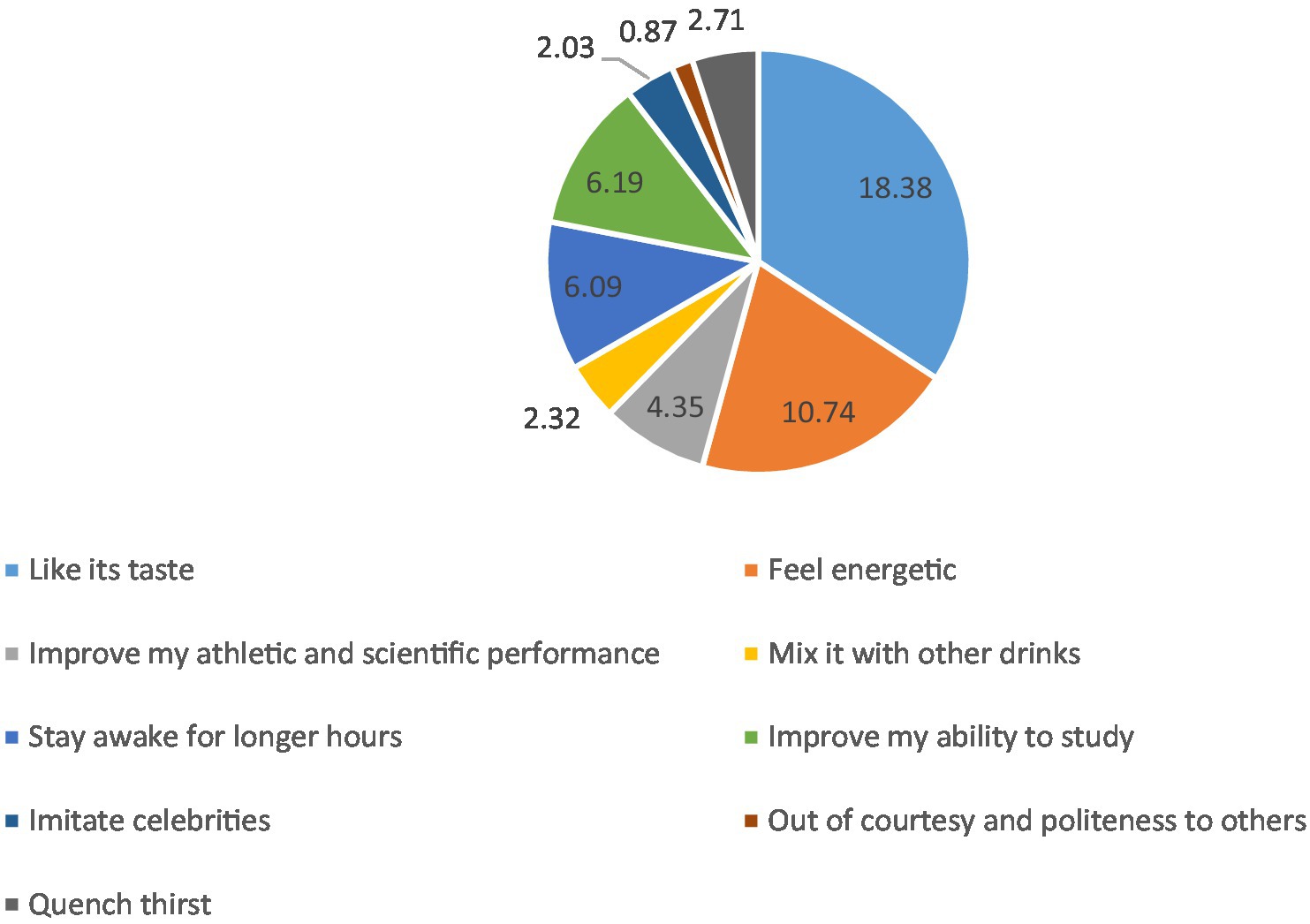
Figure 1. Reasons for consuming CED by schoolchildren (%) (N = 1,034; multiple answers).
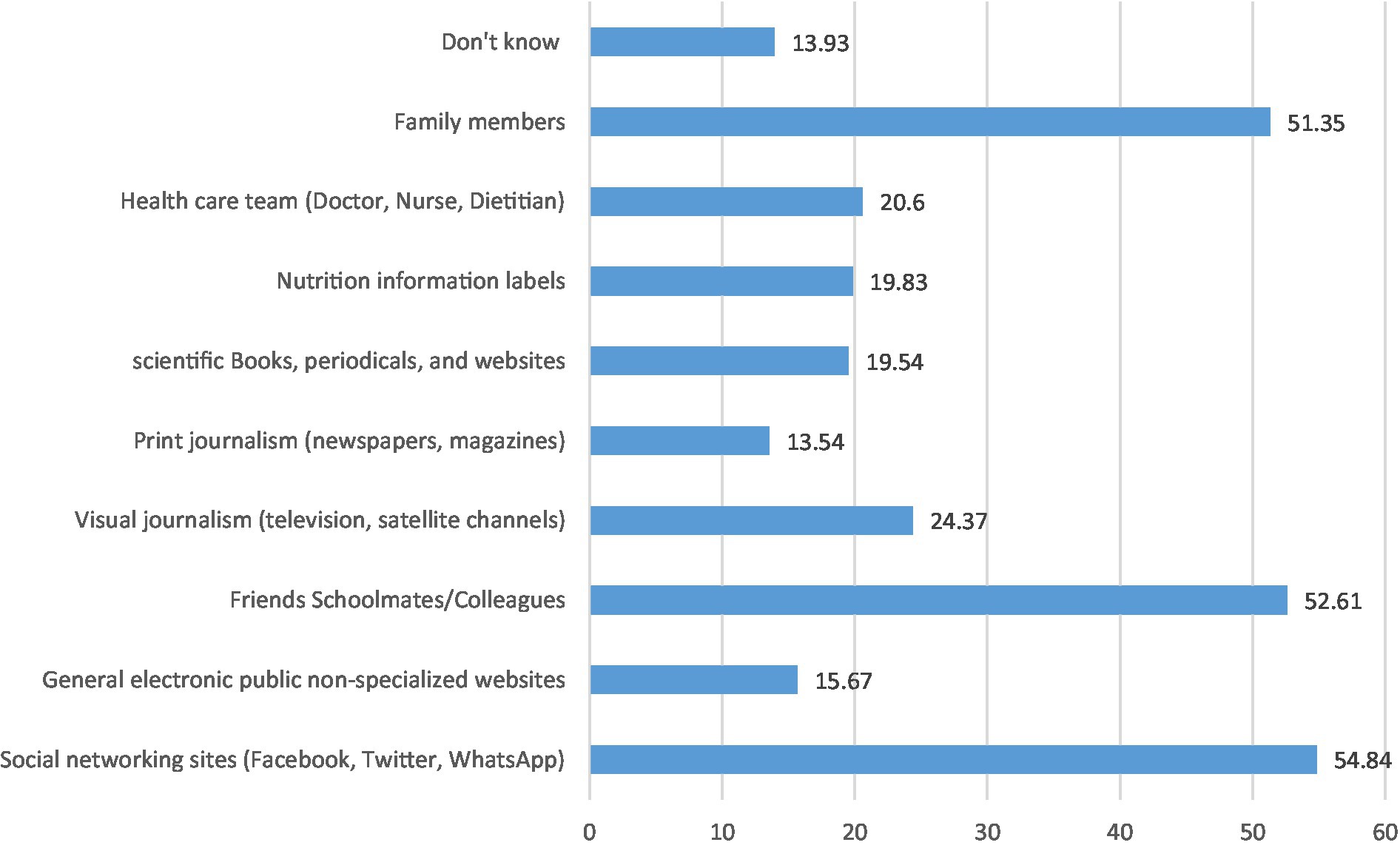
Figure 2. Sources of information about CED as per the perspectives of CED consumers (N = 1,034; multiple answers).
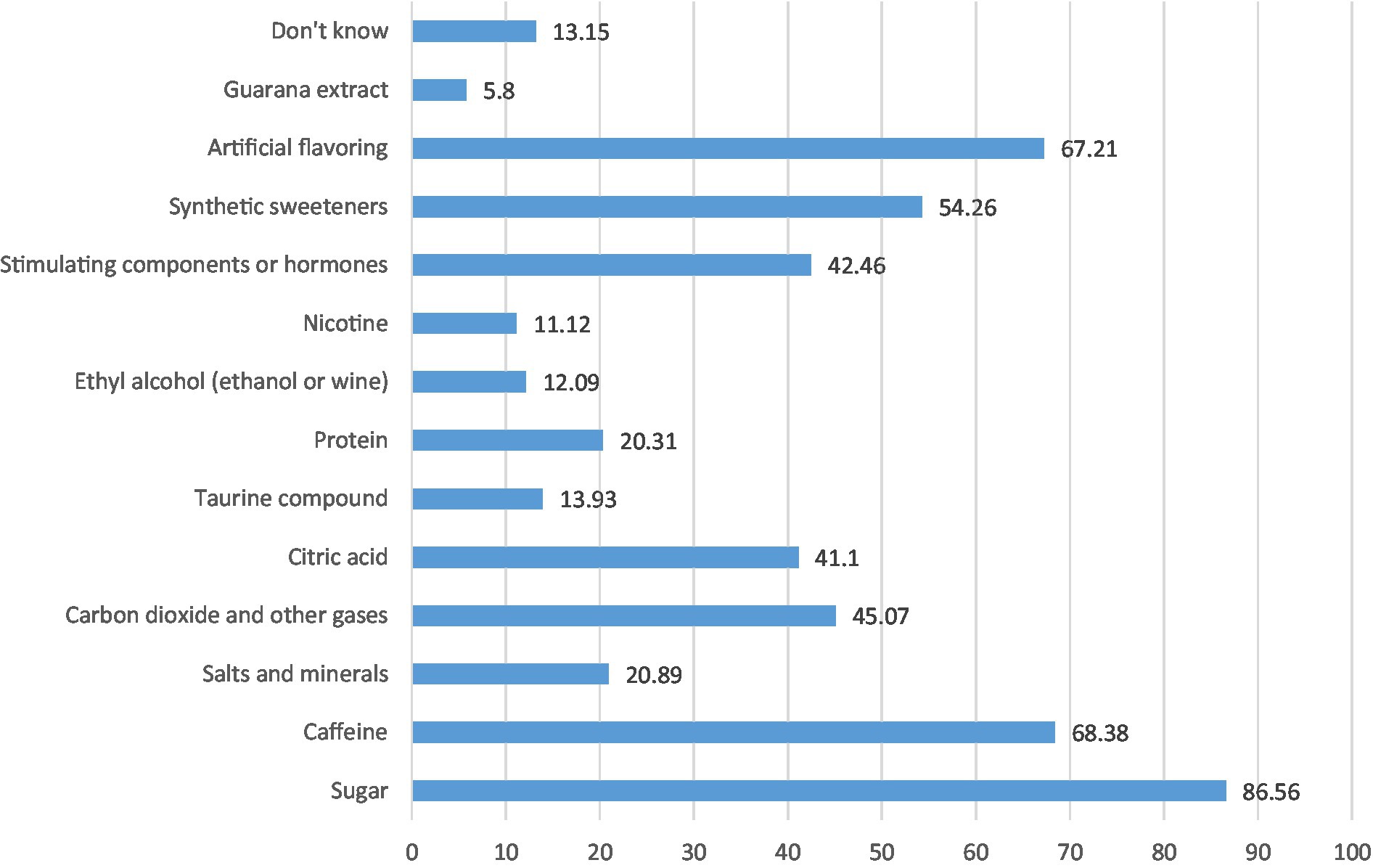
Figure 3. Ingredients of CED as reported by the CED consumers (N = 1,034; multiple answers) (%). *The ingredients listed reflect the perspectives of CED consumers and do not imply that they are present in CED.
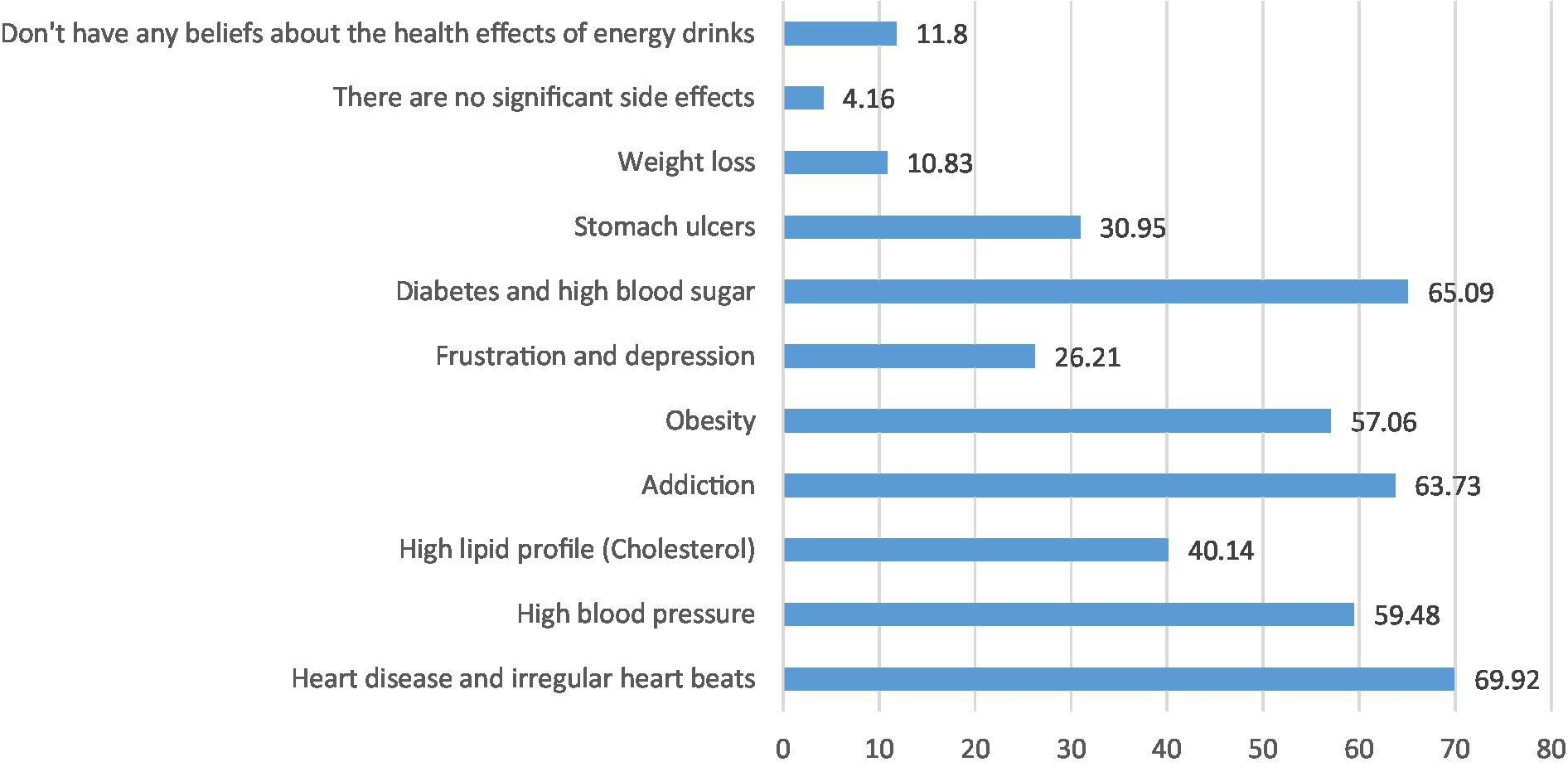
Figure 4. Opinions of CED consumers (%) about the long-term negative health effects associated with CED (N = 1,034; multiple answers). *Changes listed reflect the perspectives of CED consumers and do not imply that they are scientifically proven effects.
About two-thirds of the participating schoolchildren used smart devices <2 h per day (67%), exercised less than three times/week (62%), suffered from frequent headaches (64%), and suffered from frequent stomach aches (74%). About two-thirds (65%) of students described their physical activity as good-very good, about 56% described their mental health as good-very good, only 16% reported ≥8 h of sleep per night, and about 35% had difficulty falling asleep. About half-to-half reported the presence-absence of being frequently angry, nervous, anxious, or arguing (Table 3).
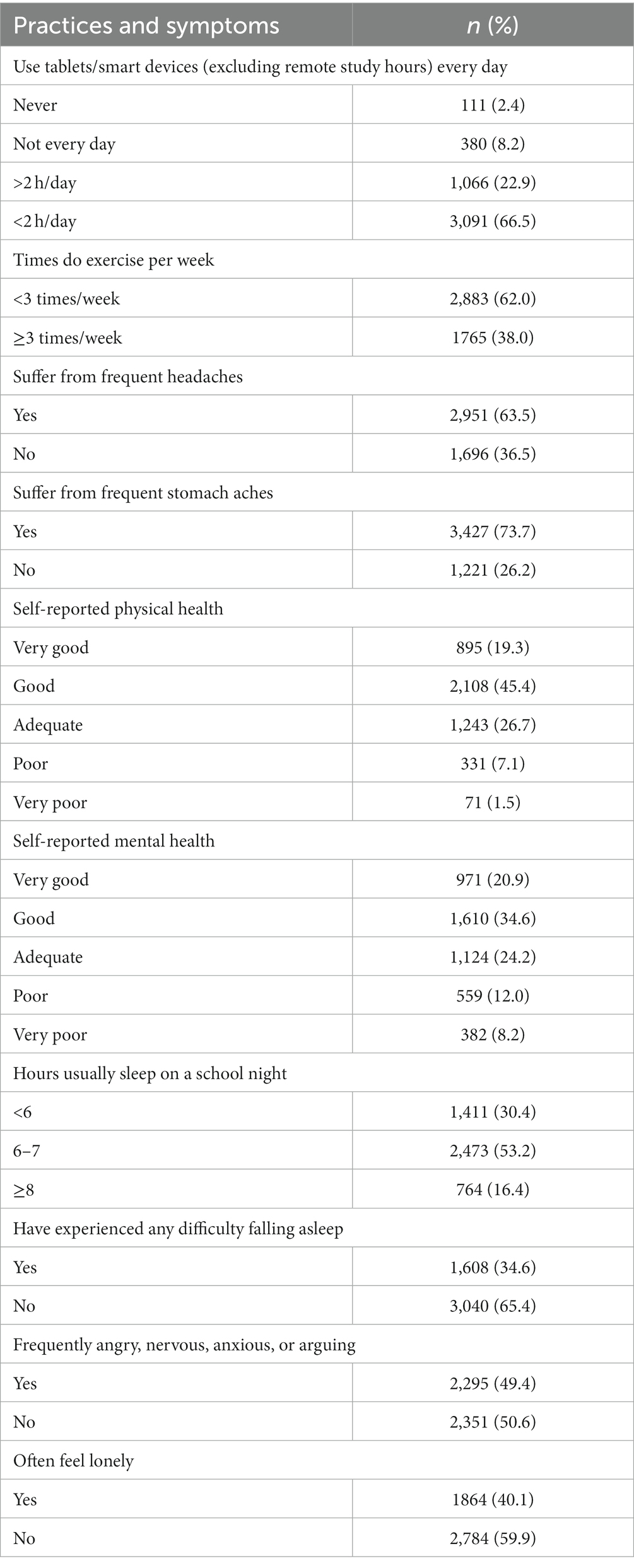
Table 3. Daily behaviors and self-reported physical and mental conditions of the study participants (N = 4,648).
The relationship between sociodemographic variables and CED consumption is presented in Table 4. Females reported a significantly lower intake of CED (p = 0.001) than males. There was a significant difference in CED consumption by nationality (p = 0.001), with non-Arab students reporting significantly lower consumption than all other nationalities (p = 0.001). There was a significant association between CED consumption and school grade (p = 0.001), with consumption significantly higher in higher grades (i.e., Grade 12 vs. Grades 8 and 9; p = 0.001).
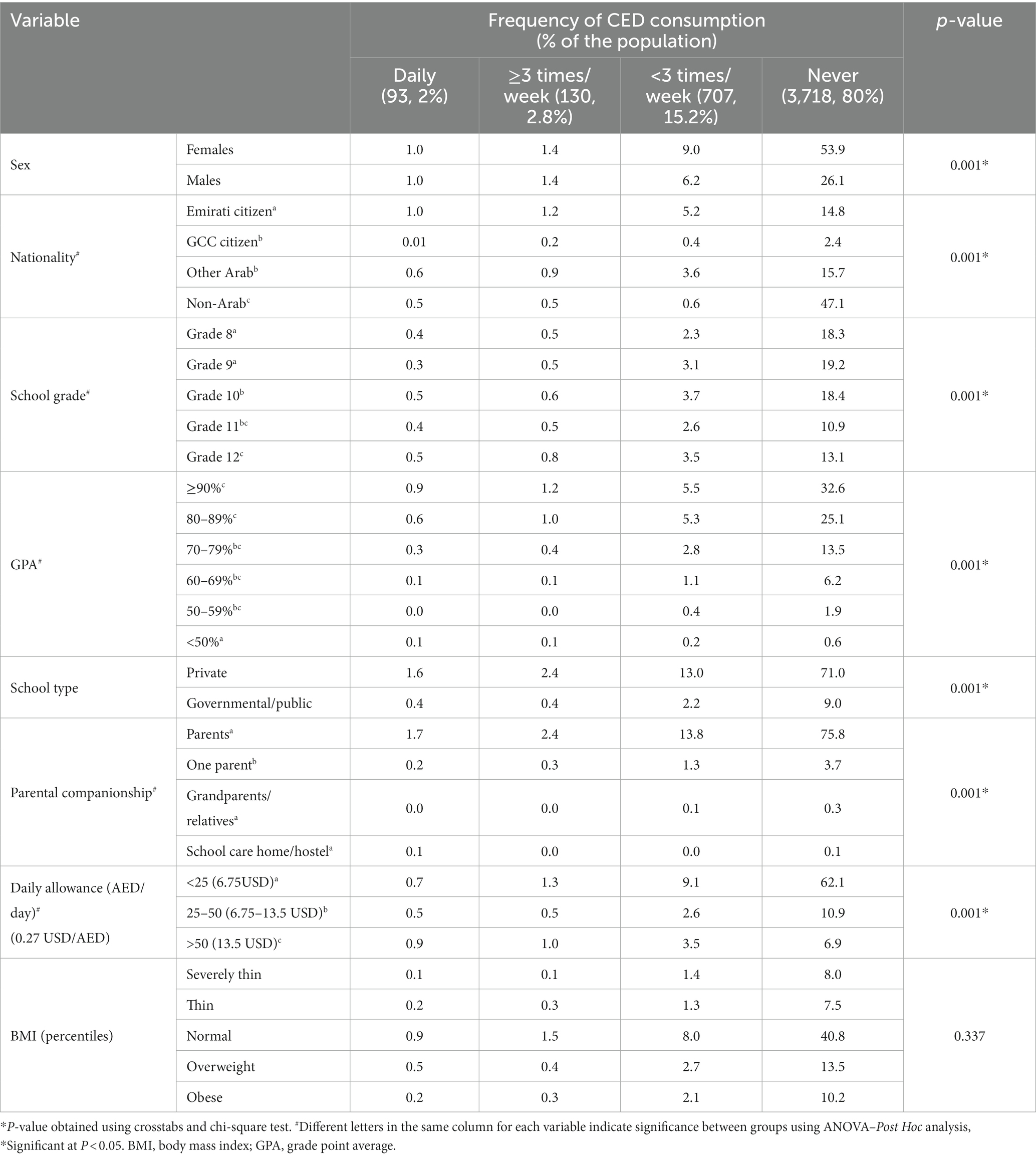
Table 4. Association between CED consumption and students’ sociodemographic characteristics (N = 4,648).
As shown in Table 4, Students with a GPA of ≤50% reported significantly higher consumption of CED compared with those with higher GPA levels (p = 0.001). Schoolchildren in governmental/public schools students reported significantly higher consumption of CED compared with their counterparts in private schools (p = 0.001). Students who lived with both parents had significantly (p = 0.001) lower consumption of CED compared with all types of companionship. Those who had a low daily allowance (≤ 25 Emirati dirhams AED, about 7 $ or less) had the lowest CED consumption, while students with a high daily allowance (>50 AED, about 14 $ or more) had the highest consumption of CED (p = 0.001; Table 5).
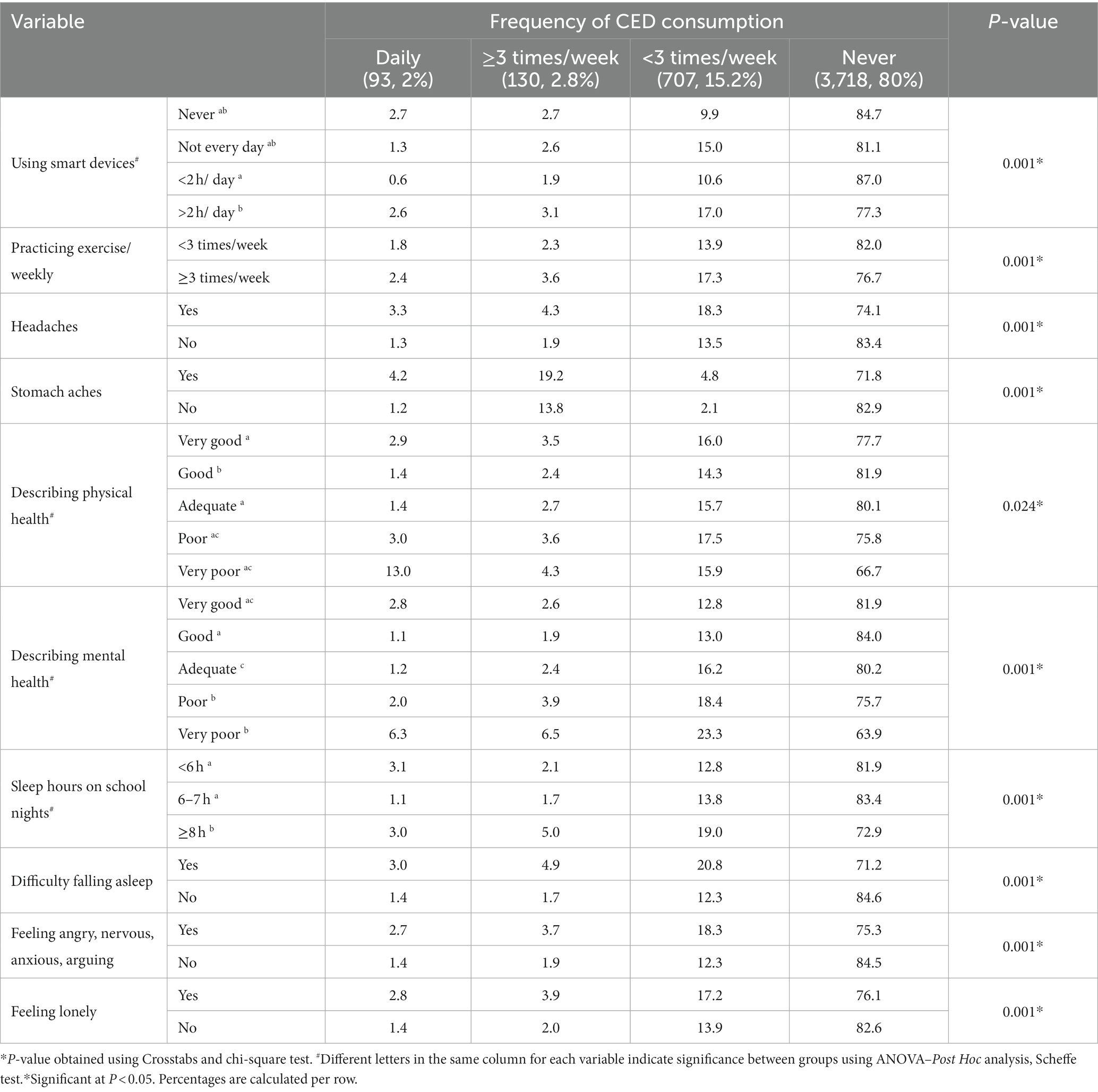
Table 5. Association between CED consumption and physical exercise, sleep, and physical and mental health (%).
A significant positive association was found between CED consumption and students’ use of smart devices (p = 0.001). Among those who never consumed CED, significantly more students had lower time duration for using smart devices (<2 h/day vs. >2 h/day, 87% vs. 77%; p = 0.001). Students who exercised more than three times/week had significantly higher CED consumption than those who exercised three or fewer times/week (p = 0.001). Students who reported headaches consumed significantly more CED than those without headaches (p = 0.001). The same trend was reported for stomach aches, students who consumed significantly more CED witnessed more stomach aches than those who did not consume CED (p = 0.001). Furthermore, those who reported “good physical health” had significantly less CED consumption than the other groups (p = 0.024). The same trend was reported or self-reported mental health, those who reported “good-very good mental health” had significantly less CED consumption than the other groups with higher CED consumption (p = 0.001).
Unexpectedly, there was a direct and significant association between CED consumption rate and the number of sleep hours per night on school days (p = 0.001). Students who slept <6 h/night and 6–7 h/night reported significantly lower CED consumption than those who slept ≥8 h/night (p < 0.05). Nonetheless, those who reported less CED consumption had reported significantly less difficulty falling asleep (p = 0.001). Moreover, those who reported feeling angry, nervous, anxious, or arguing reported significantly (p = 0.001) more CED consumption than those who did not. Along the same line, students who reported feeling lonely had significantly (p = 0.001) more CED consumption than those who did not feel lonely.
Students with uneducated fathers reported significantly more CED consumption than those children with all other levels of fathers’ education (p = 0.001). Similarly, students with mothers who had college/university education consumed significantly (p = 0.001) fewer CED than those with mothers who reported less educational level (Table 6). Students with employed fathers reported significantly (p = 0.001) fewer CED consumption than those with unemployed fathers. On the contrary, students with employed mothers reported significantly (p = 0.001) more CED consumption than those with unemployed mothers. Students who used to eat breakfast daily reported significantly (p = 0.001) fewer CED consumption than those who did not use to eat this meal. Students who consumed one serving or less of vegetables/day were significantly (p = 0.001) more likely to consume CED than those who consumed two or more servings of vegetables/day. However, no such association was found for fruit consumption. Students who used to frequently consume fast foods (energy-dense, easily prepared processed foods in Westernized restaurants) reported significantly (p = 0.001) more CED consumption than those who reported less frequent fast-food consumption. Moreover, students who used to frequently consume energy-dense snacks reported significantly (p = 0.001) more CED consumption than those with less frequent snacking. Though very small in number, smokers reported significantly (p = 0.001) more CED consumption than their non-smoker counterparts (Table 6).
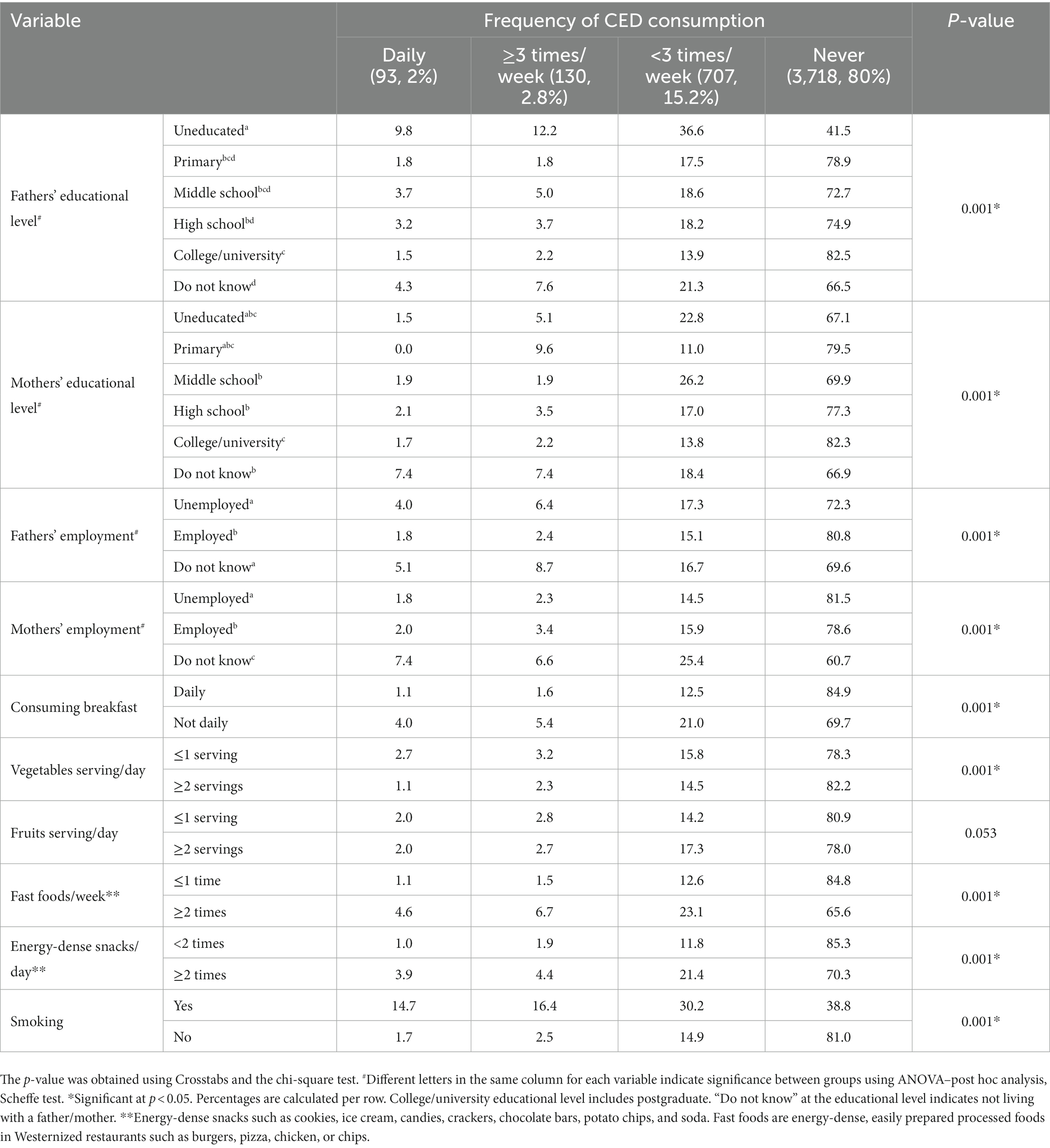
Table 6. Association between CED consumption and parental factors.
This survey-based research explored for the first time, at the national scale, the prevalence of CED consumption and their associations with sociodemographic, nutritional, dietary, lifestyle, and sleep characteristics of the schoolchildren in the UAE. We found that 20% of students consumed CED. Students learned about CED from different unreliable sources, such as social media, friends, schoolmates, and family members, and the majority were aware that consumption of CED was associated with adverse health consequences. We found significant associations between students’ CED consumption and various sociodemographic and health indicators, including nationality, place of residence, sex, type of school, daily allowance, GPA, physical and mental health, lifestyle and dietary habits, use of smart devices, sleep characteristics, and timing, perceived mental and physical health, and parental education level and employment status.
Our findings on the prevalence of CED consumption among schoolchildren are generally consistent with previous findings from the UAE (27%) (30) and close to one study from Australia (24%) (32). However, the reported prevalence is much lower than what was found in other parts of the globe, where the prevalence ranged from 28.0–66% (6, 16–27). Considering the similar economic and socioeconomic backgrounds in the GCC countries, the prevalence of CED consumption in the UAE is much lower than the reported high prevalence in Saudi Arabia (45–60%) among middle and secondary schoolchildren (28, 29). This relatively lower prevalence of CED consumption among school children in the UAE could be explained by the legal restriction on selling CED to children under 16 years old, which is announced and declared in supermarkets and large groceries and has been banned in school canteens (33, 34). Further, the increased awareness of parents and families about the adverse consequences of CED on children’s health may explain this notion (35).
The reported association between the male sex and CED consumption has been examined by several studies (25, 36, 37). Consistent with studies on school and college students, male students were much more likely to report CED consumption than females (11, 32, 37–40). This clear tendency by males could be explained by the masculinity ideology that characterizes young adolescent males (41). Such ideology states that male adolescents tend to have more stereotypically masculine beliefs driven by the male sex hormones (42), making them more likely to believe that CED work better, which, in turn, leads to drinking more of these formulated drinks (43).
The reported obvious differences between Arab and non-Arabs concerning the consumption of CED could be ascribed to the differences in the health education, knowledge, and family effect on children’s food selection and decisions, which are found to be largely affected by the ethnicity and racial background (44, 45). The reported higher CED consumption by higher grades is consistent with previous studies (18, 46) and could be explained by the role of sex hormones and an increased feeling of power and dependence associated with the increased age of students, especially male students (47).
The role of caffeine derived from CED in stimulating the central nervous system and increasing alertness leads cognitive function to the assumption that frequent CED consumption is expected to promote academic achievement presented in higher cumulative grade point average (GPA) (48). This proposed effect has been investigated by Champlin et al. (49) among college students. Consistent with our results on schoolchildren, Champlin and colleagues found that drinking CED was associated with a lower GPA even after controlling for potential confounding variables. Further in Pakistan, no relationship was found between the GPA and CED consumption among university students (50).
Daily allowance, which reflects the purchasing power and socioeconomic level of the school children, has a clear direct relationship with CED consumption. This was evident in our results and also corroborated by relevant research on university students in Beirut, Lebanon (51) and among adolescents in Australia (32) where the economic levels of the students positively determined the extent and type of CED consumption. However, this finding contradicts what was reported in Norway, where a larger proportion of high CED consumers was associated with adolescents with lower socioeconomic status (52). Albeit students in private schools reported higher purchasing power to afford the CED, they reported a lower prevalence of CED consumption than their counterparts in the public schools, a matter that could be interpreted by the level of knowledge and awareness about health sequelae of CED, rather than the economic pr purchasing power that determines the tendency to purchase and consume CED.
Family relationship presented in parental companionship is an integral component for healthy children’s growth and development and ensuring their mental and social well-being (53). This is clearly reflected in our results, where the schoolchildren with parental companionship exhibited a significantly lower prevalence of CED consumption than other groups of companionship.
The direct relationship between CED consumption with smart device use and screen time is consistent with and mirrors the results of several previous studies in different countries (30, 37, 52, 54, 55). In the United States, a large-scale national study on 32,418 schoolchildren from 252 to 263 schools (grades 8–10) revealed that each hour per day talking on a cellphone was associated with an increased risk of exceeding WHO caffeine intakes by 18% (OR = 1.15–1.21; p < 0.001), and only video game use was weakly linked to caffeine intake, with the latter comes mostly from CED (56). This notion was further confirmed by Larson et al. on 2,793 American adolescents in grades 6–12 (54).
The relationship between physical activity and CED consumption has been repeatedly examined among adolescents and adults with contradicting results reached (8, 30, 37, 52, 54, 55, 57). Consistent with our results, Puupponen et al. (8) found no association between frequent CED consumption and low physical activity and confirmed that frequent CED consumers showed a relatively higher likelihood of reporting high physical activity than non-consumers. Our and Puupponen’s findings disagree with the reported negative relationship between CED consumption and PA levels among Norwegian adolescents. The tendency of physically active students to consume CED comes from the fact that CED are purported and advertised to increase mental concentration as well as physical performance and help in achieving goals and winning competitions (58).
Headaches and stomach aches are known as common side effects of the excessive intake of caffeine (59, 60). Hence, the coexistence of more reported headaches and stomach aches among those with more frequent consumption of CED is expected, and comes in line with the existing literature linking CED with such adverse symptoms (61, 62). Reporting headaches and stomach aches are confirmed by relevant and recent reports among Icelandic adolescents who were exposed to excessive caffeine (62). Such unpleasant effects could be explained by the fact that excessive caffeine intake induces a pro-nociceptive state of cortical hyperexcitability (59), which in turn triggers such symptoms.
The poor self-reported physical and mental health among CED users reveals a plausible association between worsened physical and mental health with the consumption of CED among schoolchildren. Such a finding is consistent with what Halldorsson and colleagues found in their study on Icelandic adolescents (62). Further, they reported emotional and behavioral problems among adolescents who were exposed to CED (63). This is consistent with the several negative health indicators reported by Puupponen and colleagues (8). In the latter, even infrequent CED consumption was associated with adverse health indicators, while frequent CED consumers were more likely to report skipping breakfast, inadequate tooth brushing, current problematic social media use, smoking, snus, and cannabis use, feelings of insufficient sleep and reporting short sleep, low self-rated health, and multiple health complaints (8). All the aforementioned negative health indicators are consistent with the self-reported poor physical and mental health found among the CED consumers in the current work.
Though unexpected results indicate a positive relationship between CED consumption and sleep duration (i.e., sleep night hours), the difficulty in falling asleep is indicative of the adverse effect of CED on sleep quality. Sleep quality includes, but is not limited to, sleep hours and other six components as indicated in the Pittsburgh Sleep Quality Index (PSQI) (64). Having prolonged time to falling asleep could be explained by both the stimulatory effect of caffeine (the main ingredient of CED) and the plausible excessive exposure to blue light from the prolonged use of smart devices, especially if used at night, by the CED consumers. Both caffeine and the blue light radiated from smart devices’ screens have stimulatory effects on the CNS and may be involved in delaying sleep onset. According to the Sleep Foundation, the use of smart devices that emit artificial blue light in the evening and at night disrupts the natural sleep–wake cycle by preventing the brain from producing melatonin prior to bedtime (65). Our current finding on self-reported sleep duration contradicts several research works that indicated that CED consumption was associated with reduced sleep duration and sleep quality as well (5, 30, 32, 40, 54, 57, 62, 66, 67). Such discrepancy could be ascribed to the lack of utilization of validated subjective sleep quality questionnaires such as PSQI in the current work. Interestingly, the lack of sleep and skipped breakfast were the affectors that mediate emotional and behavioral problems that characterize CED consumers among 8,405 adolescents from 11 to 15 years old (63).
The reported association between unhealthy dietary behaviors such as breakfast skipping and a lower intake of fruits and vegetables with CED consumption mirrors the findings of other relevant reports (15, 54, 68). However, Nuss et al. (32) did not find such a negative relationship between fruit and vegetable consumption. Regarding frequent snacking and consumption of energy-dense fast foods, the observed association between CED consumption and these dietary patterns is also consistent with previous works (30, 32, 54, 69).
The obvious and noticeable coexistence of unhealthy dietary behavior with other unhealthy and risky lifestyle behaviors such as smoking and long screen time, could be explained by the low health awareness that characterizes those children and their families, a matter that needs further investigation to find out the clustering of these behaviors in the same group of participants.
Although the proportion of smoking school students was very low, CED consumption was predominant among those smoking children. This relationship between smoking and CED consumption is repeatedly documented in several reports (6, 8, 9, 46, 54) and could be ascribed to the clustering of unhealthy behaviors alongside with lack of awareness about the unhealthy dietary and lifestyle behaviors and their adverse health sequelae. As for schoolchildren and adolescents, these behaviors and the lack of knowledge and awareness are mostly a reflection of the family’s educational and awareness levels and the effect of peers (45, 70). In their extensive systematic review, Marinoni et al. (70) found that schoolchildren and adolescents with low parental monitoring, with lower grades, or those exposed to bad influences from peers are more likely to consume CED. They concluded that the consumption of CED by schoolchildren and adolescents lies in the potential interplay between influences by family members and peers, personality traits, and school performance.
In the current work, the increased reporting of poor self-reported mental health signs such as feeling angry, nervous, anxious, and lonely along with emotional and behavioral problems are evident for adolescents with CED consumption as reported in previous works (13, 17–19, 63, 68).
The overall adverse health effects of CED are exacerbated by the industry’s aggressive marketing directed to adolescents, and the absence of activated regulatory and parental supervision. To combat this growing public health concern, policymakers should consider creating a discrete regulatory category for CED, establishing an evidence-based upper limit on caffeine, insisting on the application of restricted CED sales for schoolchildren and adolescents, and enforcing regulating existing CED marketing strategies, particularly among schoolchildren and adolescents (12).
This was the first study to evaluate the prevalence of CED consumption among school students and examine its associations with various dietary and lifestyle- and health-related factors in the UAE. This study was conducted on a large scale, and participants were relatively evenly distributed across different school grades (Grades 8–12, corresponding to 14–18 years old). Therefore, our findings offer good evidence of the need to address issues around the consumption of CED among schoolchildren in the UAE. Moreover, our database serves as a valuable resource to further examine these parameters in the context of diverse sociodemographic variables, given the rich presence of different ethnicities in the UAE. However, the observational nature of this study means we cannot infer causality. Further, relying on self-reported CED consumption and other outcomes, the study can be susceptible to both social desirability bias and recall bias (52). Moreover, the associations between CED consumption and self-reported physical and mental health variables may be affected by the fact that caffeine, the principal active component of CED, is present in different foods and drinks along with other nutrients that may influence physical and mental health. In addition, only students who were in school on the day of the survey responded to the questionnaire. Therefore, adolescents who were absent or had pulled out were excluded from the study, which may affected the findings. Further, the BMI was calculated based on self-reported weight and height. The absence of comprehensive assessment tools, such as PSQI, and other validated measures for mental health and eating behaviors, lessens the robustness of the current findings and necessitates additional research to enhance their power. Lastly, the limited and unrepresentative sample size for the UAE schoolchildren makes the generalizability of the current results unattainable.
Our findings have broad policy implications for improving the provision of health services and health behaviors among UAE schoolchildren and adolescents. Our findings could also serve as a useful guideline for implementing government initiatives to improve school physical and mental health and nutrition, reduce childhood obesity, and prevent children from smoking. Given the potential health risks associated with CED, the UAE government has implemented policies to regulate CED consumption. For example, CED are only sold to customers over the age of 16 years, warning labels must be displayed on the packages of these drinks, and there is a tax on CED to discourage consumption. Overall, the UAE’s CED-related policies are intended to protect the health of young people by limiting their access to these potentially harmful products. Although the effectiveness of these policies is still being evaluated, they represent an important step toward promoting the health and well-being of UAE children and adolescents. Several interventions may be useful, such as specific rules about consuming caffeine and soft drinks in schools, the exclusion of vending machines selling soft drinks from school premises, providing safe drinking water, school-based health campaigns, the imposition of high taxes on caffeine and CED, and limiting their promotion and advertising in social media. In addition, the UAE launched a Family Protection Policy, which seeks to strengthen social ties in UAE families and communities (71). It is also important to develop innovative child/adolescent-friendly initiatives and secure their participation by including their views when considering overall protection and their best interests (72).
There is a relatively low prevalence of CED consumption among schoolchildren and adolescents in the UAE. Still, those who consumed CED have reported unhealthy dietary (skipping breakfast, frequent snacking and eating fast foods, low fruit, and vegetable intake) and lifestyle behaviors (long screen time, poor sleep quality component), accompanied by poor self-reported mental and physical health. Variable sociodemographic variables, such as nationality, parental companionship, school type, sex, education level, daily allowance, and parents’ employment and educational levels interplay with CED consumption among schoolchildren in the UAE.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by ethical approval was obtained from the University of Sharjah Research Ethics Committee on September 24, 2021 (REC-21-06-18-01). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
MF: Conceptualization, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. FA: Writing – review & editing, Supervision. MI: Writing – original draft. DA: Formal analysis. ES: Investigation, Writing – review & editing. ET: Investigation, Writing – review & editing. MA-K: Investigation, Writing – review & editing. SA-Q: Investigation, Writing – review & editing. FZ: Writing – review & editing. HH: Writing – review & editing. MH: Writing – review & editing. TO: Writing – review & editing. HR: Writing – review & editing. LC: Writing – review & editing. FN: Writing – review & editing. FB: Writing – review & editing. RO: Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Khouja, C , Kneale, D , Brunton, G , Raine, G , Stansfield, C , Sowden, A, et al. Consumption and effects of caffeinated energy drinks in young people: an overview of systematic reviews and secondary analysis of UK data to inform policy. BMJ Open. (2022) 12:e047746. doi: 10.1136/bmjopen-2020-047746
2. Li, P , Haas, NA , Dalla-Pozza, R , Jakob, A , Oberhoffer, FS , and Mandilaras, G . Energy drinks and adverse health events in children and adolescents: a literature review. Nutrients. (2023) 15:2537. doi: 10.3390/nu15112537
3. Oddy, WH , and O’Sullivan, TA . Energy drinks for children and adolescents. BMJ. (2009) 339:b5268. doi: 10.1136/bmj.b5268
4. Alhyas, L , El Kashef, A , and AlGhaferi, H . Energy drinks in the Gulf cooperation council states: a review. JRSM Open. (2016) 7:2054270415593717. doi: 10.1177/2054270415593717
5. Watson, EJ , Banks, S , Coates, AM , and Kohler, MJ . The relationship between caffeine, sleep, and behavior in children. J Clin Sleep Med. (2017) 13:533–43. doi: 10.5664/jcsm.6536
6. Gallimberti, L , Buja, A , Chindamo, S , Vinelli, A , Lazzarin, G , Terraneo, A, et al. Energy drink consumption in children and early adolescents. Eur J Pediatr. (2013) 172:1335–40. doi: 10.1007/s00431-013-2036-1
7. Glade, MJ . Caffeine–not just a stimulant. Nutrition. (2010) 26:932–8. doi: 10.1016/j.nut.2010.08.004
8. Puupponen, M , Tynjälä, J , Välimaa, R , and Paakkari, L . Associations between adolescents’ energy drink consumption frequency and several negative health indicators. BMC Public Health. (2023) 23:258. doi: 10.1186/s12889-023-15055-6
9. Visram, S , Cheetham, M , Riby, DM , Crossley, SJ , and Lake, AA . Consumption of energy drinks by children and young people: a rapid review examining evidence of physical effects and consumer attitudes. BMJ Open. (2016) 6:e010380. doi: 10.1136/bmjopen-2015-010380
10. Cadoni, C , and Peana, AT . Energy drinks at adolescence: awareness or unawareness? Front Behav Neurosci. (2023) 17:1080963. doi: 10.3389/fnbeh.2023.1080963
11. Arria, AM , Bugbee, BA , Caldeira, KM , and Vincent, KB . Evidence and knowledge gaps for the association between energy drink use and high-risk behaviors among adolescents and young adults. Nutr Rev. (2014) 72:87–97. doi: 10.1111/nure.12129
12. Al-Shaar, L , Vercammen, K , Lu, C , Richardson, S , Tamez, M , and Mattei, J . Health effects and public health concerns of energy drink consumption in the United States: a Mini-review. Front Public Health. (2017) 5:225. doi: 10.3389/fpubh.2017.00225
13. Holubcikova, J , Kolarcik, P , Madarasova Geckova, A , Reijneveld, SA , and van Dijk, JP . Regular energy drink consumption is associated with the risk of health and behavioural problems in adolescents. Eur J Pediatr. (2017) 176:599–605. doi: 10.1007/s00431-017-2881-4
14. Gambon, DL , Brand, HS , Boutkabout, C , Levie, D , and Veerman, ECI . Patterns in consumption of potentially erosive beverages among adolescent school children in the Netherlands. Int Dent J. (2011) 61:247–51. doi: 10.1111/j.1875-595X.2011.00067.x
15. Puupponen, M , Tynjälä, J , Tolvanen, A , Välimaa, R , and Paakkari, L . Energy drink consumption among Finnish adolescents: prevalence, associated background factors, individual resources, and family factors. Int J Public Health. (2021) 66:620268. doi: 10.3389/ijph.2021.620268
16. Girán, J , Girán, KA , Ormándlaky, D , Pozsgai, É , Kiss, I , and Kollányi, Z . Determinants of pupils' energy drink consumption – findings from a Hungarian primary school. Heliyon. (2023) 9:e15954. doi: 10.1016/j.heliyon.2023.e15954
17. Tóth, Á , Soós, R , Szovák, E , Najbauer N, M , Tényi, D , Csábí, G, et al. Energy drink consumption, depression, and Salutogenic sense of coherence among adolescents and young adults. Int J Environ Res Public Health. (2020) 17:1290. doi: 10.3390/ijerph17041290
18. Masengo, L , Sampasa-Kanyinga, H , Chaput, J-P , Hamilton, HA , and Colman, I . Energy drink consumption, psychological distress, and suicidality among middle and high school students. J Affect Disord. (2020) 268:102–8. doi: 10.1016/j.jad.2020.03.004
19. Utter, J , Denny, S , Teevale, T , and Sheridan, J . Energy drink consumption among New Zealand adolescents: associations with mental health, health risk behaviours and body size. J Paediatr Child Health. (2018) 54:279–83. doi: 10.1111/jpc.13708
20. Frayon, S , Wattelez, G , Cherrier, S , Cavaloc, Y , Lerrant, Y , and Galy, O . Energy drink consumption in a pluri-ethnic population of adolescents in the Pacific. PLoS One. (2019) 14:e0214420. doi: 10.1371/journal.pone.0214420
21. Scalese, M , Cerrai, S , Biagioni, S , Benedetti, E , Bastiani, L , Potente, R, et al. Trends in energy drink and combined alcohol and energy drinks consumption among Italian high school students, 2008–2019. Drug Alcohol Depend. (2021) 228:109061. doi: 10.1016/j.drugalcdep.2021.109061
22. Scalese, M , Denoth, F , Siciliano, V , Bastiani, L , Cotichini, R , Cutilli, A, et al. Energy drink and alcohol mixed energy drink use among high school adolescents: association with risk taking behavior, social characteristics. Addict Behav. (2017) 72:93–9. doi: 10.1016/j.addbeh.2017.03.016
23. Trapp, G , Hurworth, M , Christian, H , Bromberg, M , Howard, J , McStay, C, et al. Prevalence and pattern of energy drink intake among Australian adolescents. J Hum Nutr Diet. (2021) 34:300–4. doi: 10.1111/jhn.12789
24. Galimov, A , Hanewinkel, R , Hansen, J , Unger, JB , Sussman, S , and Morgenstern, M . Energy drink consumption among German adolescents: prevalence, correlates, and predictors of initiation. Appetite. (2019) 139:172–9. doi: 10.1016/j.appet.2019.04.016
25. Azagba, S , Langille, D , and Asbridge, M . An emerging adolescent health risk: caffeinated energy drink consumption patterns among high school students. Prev Med. (2014) 62:54–9. doi: 10.1016/j.ypmed.2014.01.019
26. Carsi Kuhangana, T , Muta Musambo, T , Pyana Kitenge, J , Kayembe-Kitenge, T , Kazadi Ngoy, A , Musa Obadia, P, et al. Energy drink consumption among adolescents attending schools in Lubumbashi, Democratic Republic of Congo. Int J Environ Res Public Health. (2021) 18:7617. doi: 10.3390/ijerph18147617
27. Miller, KE , Dermen, KH , and Lucke, JF . Caffeinated energy drink use by US adolescents aged 13–17: a national profile. Psychol Addict Behav. (2018) 32:647–59. doi: 10.1037/adb0000389
28. Faris, MA , Epuru, S , Al-Shimmari, S , and Al-Shimmari, E . Alarming high levels of energy drinks consumption among school children in hail, northern of Saudi Arabia. Int J Child Health Nutr. (2015) 4:1–13. doi: 10.6000/1929-4247.2015.04.01.1
29. Musaiger, A , and Zagzoog, N . Knowledge, attitudes and practices toward energy drinks among adolescents in Saudi Arabia. Glob J Health Sci. (2013) 6:42–6. doi: 10.5539/gjhs.v6n2p42
30. Almulla, AA , and Faris, MAE . Energy drinks consumption is associated with reduced sleep duration and increased energy-dense fast foods consumption among school students: a Cross-sectional study. Asia Pac J Public Health. (2020) 32:266–73. doi: 10.1177/1010539520931351
31. Von Elm, E , Altman, DG , Egger, M , Pocock, SJ , Gøtzsche, PC , and Vandenbroucke, JP . The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. (2007) 370:1453–7. doi: 10.1016/S0140-6736(07)61602-X
32. Nuss, T , Morley, B , Scully, M , and Wakefield, M . Energy drink consumption among Australian adolescents associated with a cluster of unhealthy dietary behaviours and short sleep duration. Nutr J. (2021) 20:64. doi: 10.1186/s12937-021-00719-z
33. UAE . Supermarkets take action on energy drink sales. (n.d.). Available at: https://www.thenationalnews.com/uae/uae-supermarkets-take-action-on-energy-drink-sales-1.698238.
34. Dubai Schools Ban Energy Drinks . Why such beverages are harmful for children. (n.d.). Available at: https://www.khaleejtimes.com/uae/dubai-school-bans-energy-drinks-why-such-beverages-are-harmful-for-children.
35. The National . Doctors and parents back Dubai school's prime energy drink warning. (n.d.). Available at: https://www.thenationalnews.com/uae/2023/05/28/doctors-and-parents-back-dubai-schools-prime-energy-drink-warning/.
36. Dillon, P , Kelpin, S , Kendler, K , Thacker, L , Dick, D , and Svikis, D . Gender differences in any-source caffeine and energy drink use and associated adverse health behaviors. J Caffeine Adenosine Res. (2019) 9:12–9. doi: 10.1089/caff.2018.0008
37. Lebacq, T , Desnouck, V , Dujeu, M , Holmberg, E , Pedroni, C , and Castetbon, K . Determinants of energy drink consumption in adolescents: identification of sex-specific patterns. Public Health. (2020) 185:182–8. doi: 10.1016/j.puhe.2020.05.040
38. Emond, JA , Gilbert-Diamond, D , Tanski, SE , and Sargent, JD . Energy drink consumption and the risk of alcohol use disorder among a National Sample of adolescents and young adults. J Pediatr. (2014) 165:1194–200. doi: 10.1016/j.jpeds.2014.08.050
39. Evren, C , and Evren, B . Energy-drink consumption and its relationship with substance use and sensation seeking among 10th grade students in Istanbul. Asian J Psychiatr. (2015) 15:44–50. doi: 10.1016/j.ajp.2015.05.001
40. Bryant Ludden, A , and Wolfson, AR . Understanding adolescent caffeine use: connecting use patterns with expectancies, reasons, and sleep. Health Educ Behav. (2009) 37:330–42. doi: 10.1177/1090198109341783
41. Chu, JY , Porche, MV , and Tolman, DL . The adolescent masculinity ideology in relationships scale: development and validation of a new measure for boys. Men Masculinities. (2005) 8:93–115. doi: 10.1177/1097184X03257453
42. Pletzer, B , Petasis, O , Ortner, TM , and Cahill, L . Interactive effects of culture and sex hormones on the sex role self-concept. Front Neurosci. (2015) 9:240. doi: 10.3389/fnins.2015.00240
43. Levant, RF , Parent, MC , McCurdy, ER , and Bradstreet, TC . Moderated mediation of the relationships between masculinity ideology, outcome expectations, and energy drink use. Health Psychol. (2015) 34:1100–6. doi: 10.1037/hea0000214
44. Rawlins, E , Baker, G , Maynard, M , and Harding, S . Perceptions of healthy eating and physical activity in an ethnically diverse sample of young children and their parents: the DEAL prevention of obesity study. J Hum Nutr Diet. (2013) 26:132–44. doi: 10.1111/j.1365-277X.2012.01280.x
45. Liu, KSN , Chen, JY , Ng, MYC , Yeung, MHY , Bedford, LE , and Lam, CLK . How does the family influence adolescent eating habits in terms of knowledge, attitudes and practices? A global systematic review of qualitative studies. Nutrients. (2021) 13:13. doi: 10.3390/nu13113717
46. Sampasa-Kanyinga, H , Masengo, L , Hamilton, HA , and Chaput, J-P . Energy drink consumption and substance use among middle and high school students. Int J Environ Res Public Health. (2020) 17:3110. doi: 10.3390/ijerph17093110
47. Berenbaum, SA , and Beltz, AM . How early hormones shape gender development. Curr Opin Behav Sci. (2016) 7:53–60. doi: 10.1016/j.cobeha.2015.11.011
48. McLellan, TM , Caldwell, JA , and Lieberman, HR . A review of caffeine’s effects on cognitive, physical and occupational performance. Neurosci Biobehav Rev. (2016) 71:294–312. doi: 10.1016/j.neubiorev.2016.09.001
49. Champlin, SE , Pasch, KE , and Perry, CL . Is the consumption of energy drinks associated with academic achievement among college students? J Prim Prev. (2016) 37:345–59. doi: 10.1007/s10935-016-0437-4
50. Khan, MS , Nisar, N , Arsalan, S , Naqvi, A , and Nawab, F . Caffeine consumption and academic performance among medical students of Dow University of health science (DUHS), Karachi, Pakistan. Ann Abbasi Shaheed Hosp Karachi Med Dent Coll. (2017) 22:179–84. doi: 10.58397/ashkmdc.v22i3.126
51. Ghozayel, M , Ghaddar, A , Farhat, G , Nasreddine, L , Kara, J , and Jomaa, L . Energy drinks consumption and perceptions among university students in Beirut, Lebanon: a mixed methods approach. PLoS One. (2020) 15:e0232199. doi: 10.1371/journal.pone.0232199
52. Kaldenbach, S , Strand, TA , Solvik, BS , and Holten-Andersen, M . Social determinants and changes in energy drink consumption among adolescents in Norway, 2017–2019: a cross-sectional study. BMJ Open. (2021) 11:e049284. doi: 10.1136/bmjopen-2021-049284
53. Thomas, PA , Liu, H , and Umberson, D . Family relationships and well-being. Innov Aging. (2017) 1:igx025. doi: 10.1093/geroni/igx025
54. Larson, N , DeWolfe, J , Story, M , and Neumark-Sztainer, D . Adolescent consumption of sports and energy drinks: linkages to higher physical activity, unhealthy beverage patterns, cigarette smoking, and screen media use. J Nutr Educ Behav. (2014) 46:181–7. doi: 10.1016/j.jneb.2014.02.008
55. Degirmenci, N , Fossum, IN , Strand, TA , Vaktskjold, A , and Holten-Andersen, MN . Consumption of energy drinks among adolescents in Norway: a cross-sectional study. BMC Public Health. (2018) 18:1391. doi: 10.1186/s12889-018-6236-5
56. Bradbury, KM , Turel, O , and Morrison, KM . Electronic device use and beverage related sugar and caffeine intake in US adolescents. PLoS One. (2019) 14:e0223912. doi: 10.1371/journal.pone.0223912
57. Sampasa-Kanyinga, H , Hamilton, HA , and Chaput, J-P . Sleep duration and consumption of sugar-sweetened beverages and energy drinks among adolescents. Nutrition. (2018) 48:77–81. doi: 10.1016/j.nut.2017.11.013
58. Galemore, CA . Sports drinks and energy drinks for children and adolescents–are they appropriate?: a summary of the clinical report. NASN Sch Nurse. (2011) 26:320–1. doi: 10.1177/1942602X11417310
59. Espinosa Jovel, CA , and Sobrino Mejía, FE . Caffeine and headache: specific remarks. Neurología. (2017) 32:394–8. doi: 10.1016/j.nrleng.2014.12.022
60. Garg, A , Rodriguez, A , Lewis, JT , Bansal, R , and Brahmbhatt, B . Energy drinks: a reversible risk factor for atrophic gastritis and gastric intestinal metaplasia. Cureus. (2020) 12:e12298. doi: 10.7759/cureus.12298
61. Alsunni, AA . Energy drink consumption: beneficial and adverse health effects. Int J Health Sci. (2015) 9:459–65. doi: 10.12816/0031237
62. Halldorsson, TI , Kristjansson, AL , Thorisdottir, I , Oddsdóttir, C , Sveinbjörnsson, J , Benediktsson, R, et al. H G: caffeine exposure from beverages and its association with self-reported sleep duration and quality in a large sample of Icelandic adolescents. Food Chem Toxicol. (2021) 157:112549. doi: 10.1016/j.fct.2021.112549
63. Veselska, ZD , Husarova, D , and Kosticova, M . Energy drinks consumption associated with emotional and Behavioural problems via lack of sleep and skipped breakfast among adolescents. Int J Environ Res Public Health. (2021) 18:6055. doi: 10.3390/ijerph18116055
64. Buysse, DJ , Reynolds, CF 3rd, Monk, TH , Berman, SR , and Kupfer, DJ . The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. (1989) 28:193–213. doi: 10.1016/0165-1781(89)90047-4
65. How blue light affects kids’ sleep? . (n.d.). Available at: https://www.sleepfoundation.org/children-and-sleep/how-blue-light-affects-kids-sleep#:~:text=View%20Source%20and%20duration.,than%20we%20should%20at%20bedtime.
66. Faris, MAE , Jahrami, H , Al-Hilali, MM , Chehyber, NJ , Ali, SO , Shahda, SD, et al. Energy drink consumption is associated with reduced sleep quality among college students: a cross-sectional study. Nutr Diet. (2017) 74:268–74. doi: 10.1111/1747-0080.12289
67. Lohsoonthorn, V , Khidir, H , Casillas, G , Lertmaharit, S , Tadesse, MG , Pensuksan, WC, et al. Sleep quality and sleep patterns in relation to consumption of energy drinks, caffeinated beverages, and other stimulants among Thai college students. Sleep Breath. (2013) 17:1017–28. doi: 10.1007/s11325-012-0792-1
68. Richards, G , and Smith, AP . Breakfast and energy drink consumption in secondary school children: breakfast omission, in isolation or in combination with frequent energy drink use, is associated with stress, anxiety, and depression Cross-Sectionally, but not at 6-month follow-up. Front Psychol. (2016) 7:106. doi: 10.3389/fpsyg.2016.00106
69. Alafif, N , Al-Rashed, A , Altowairqi, K , and Muharraq, A . Prevalence of energy drink consumption and association with dietary habits among governmental university students in Riyadh. Saudi J Biol Sci. (2021) 28:4511–5. doi: 10.1016/j.sjbs.2021.04.050
70. Marinoni, M , Parpinel, M , Gasparini, A , Ferraroni, M , and Edefonti, V . Psychological and socio-educational correlates of energy drink consumption in children and adolescents: a systematic review. Eur J Pediatr. (2022) 181:889–901. doi: 10.1007/s00431-021-04321-7
71. Al Gharaibeh, F , Mahmud, A , and Islam, MR . Community initiatives against Covid-19 in the United Arab Emirates. Community Dev J. (2022) 57:404–10. doi: 10.1093/cdj/bsab045
Keywords: adolescents, schoolchildren, energy drinks, caffeine, health behaviors, diet, health practice, lifestyle behaviors
Citation: Faris ME, Al Gharaibeh F, Islam MR, Abdelrahim D, Saif ER, Turki EA, Al-Kitbi MK, Abu-Qiyas S, Zeb F, Hasan H, Hashim MS, Osaili TM, Radwan H, Cheikh Ismail L, Naja F, Bettayeb FZ and Obaid RS (2023) Caffeinated energy drink consumption among Emirati adolescents is associated with a cluster of poor physical and mental health, and unhealthy dietary and lifestyle behaviors: a cross-sectional study. Front. Public Health. 11:1259109. doi: 10.3389/fpubh.2023.1259109
Edited by:
Saidur Mashreky, Centre for Injury Prevention and Research, BangladeshReviewed by:
Alessandro Porrovecchio, Université du Littoral Côte d’Opale, FranceCopyright © 2023 Faris, Al Gharaibeh, Islam, Abdelrahim, Saif, Turki, Al-Kitbi, Abu-Qiyas, Zeb, Hasan, Hashim, Osaili, Radwan, Cheikh Ismail, Naja, Bettayeb and Obaid. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: MoezAlIslam E. Faris, bWZhcmlzQHNoYXJqYWguYWMuYWU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.