
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 05 October 2023
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1257754
This article is part of the Research TopicEmerging Global Population Health Risks: From Epidemiological PerspectivesView all 14 articles
 Mariana Alejandra Rivero1*
Mariana Alejandra Rivero1* Lorena Paola Arce2,3
Lorena Paola Arce2,3 Silvina Elena Gutiérrez1Adela Tisnés4
Silvina Elena Gutiérrez1Adela Tisnés4 Juan Antonio Passucci1Julia Analia Silva1Ayelén Barón Prato4Florencia Sánchez1Julia Matias Brancher3
Juan Antonio Passucci1Julia Analia Silva1Ayelén Barón Prato4Florencia Sánchez1Julia Matias Brancher3 Silvia Marcela Estein1María Guadalupe Vizoso-Pinto2,3*
Silvia Marcela Estein1María Guadalupe Vizoso-Pinto2,3*Background: Hepatitis E virus (HEV) infection is a common cause of acute clinical hepatitis worldwide and is emerging as a disease in Argentina. It is primarily transmitted through contaminated water and food, following the fecal-oral route. Furthermore, is a zoonotic disease with swine as the primary reservoir. Prevalence of HEV infection in humans in several regions of Argentina remains unknown.
Objectives: (i) Determine the seroprevalence of HEV among the human population in Tandil, Buenos Aires, Argentina; (ii) Evaluate its association with demographic, socioeconomic and other risk exposures variables, and (iii) Describe and analyze spatial patterns related to HEV infection.
Methods: From August 2020 to July 2021, serum samples were collected from 969 individuals aged 1–80 years. Seroprevalence and 95% Confidence Interval was determined. To assess the factors associated with the presence of anti-HEV antibodies, associations between the variables and seropositivity were evaluated through bivariate and multivariate analysis. Spatial scanning for clusters of positivity was carried out. Factors associated with these clusters were also assessed.
Results: Anti-HEV antibodies were detected in 4.64% (IC 95% 3.27–6.02) of samples. Dark urine was associated with seropositivity (p = 0.02). Seropositivity was linked with the presence of natural water courses near their households (p = 0.02); the age (p = 0.04); and previous travel to Europe (p = 0.04). A spatial cluster of low rates of HEV seropositivity was detected, with greater distance of the households to water courses associated to the cluster, and male sex inversely associated to it.
Discussion and conclusion: This study is the first study to investigate the prevalence of HEV in the population from Tandil, Buenos Aires, Argentina. Considering HEV infection in the differential diagnosis in individuals presenting acute hepatitis is highlighted. The incorporation of HEV testing into blood screening policies should be mandatory. Factors related to the infection and spatial patterns of high and low risk were determined, and should be considered when implementing specific preventive measures.
Hepatitis E virus (HEV) infection is a worldwide emerging disease and a public health concern. It is also the first cause of acute viral hepatitis in the world with a disease burden of 20 million HEV infections worldwide, 3.3 million symptomatic cases and 56,000 deaths every year (1, 2). As new HEV subtypes have been identified from animal, human, and environmental isolates, new potential animal reservoirs have emerged, and evidence on the zoonotic transmission of the virus from animal hosts and the environment was provided (3). HEV genotypes 1 and 2 are restricted to humans and the infection is caused by accidental fecal contamination of drinking water. HEV genotypes 3, 4 and 7 are primarily zoonotic; interspecies transmission occurs through direct contact with infected animals and consumption of undercooked HEV-contaminated food. Parenteral transmission via transfusion of blood products has also been described (1, 2, 4, 5).
The progression of acute hepatitis E is often mild with spontaneous resolution being the normal. Interestingly, over 60% of infections display no symptoms at all. When symptoms are present, they often resemble those observed in acute hepatitis A, with approximately 65% of symptomatic cases exhibiting jaundice. Typical symptoms include asthenia, diarrhea, nausea, and/or vomiting, abdominal pain, fever, arthralgia, dark urine and light (clay/ash-colored) stool are common. Pruritus and/or upper right quadrant pain may also be present. Extrahepatic manifestations such as hematological, neurological, and renal disorders have also been described. In some cases, it can result in severe acute hepatitis. HEV infection in immunocompromised patients can cause chronic hepatitis leading to cirrhosis, and fulminant hepatitis. Pregnant women are more susceptible to fulminant hepatitis and obstetric complications, mainly during the third quarter of pregnancy. The mortality rate for adults in an epidemic area is 0.2–4.0%. However, in patients with chronic liver disease and pregnant women, the mortality rates can be significantly higher, reaching up to 70 and 25%, respectively (1, 2, 6, 7).
There is poor awareness of the disease among physicians. Thus, routine check for the disease is rarely conducted in the hospitals in most parts of the world. Thereby leading to misdiagnosis and underdiagnosis of the disease (5).
Seroprevalence rates of HEV among blood donors vary across continents. In Europe, some countries have reported relatively high seroprevalence. Bulgaria conducted a study with a prevalence of 25.9%, while Croatia and Serbia reported rates of 21.5 and 15.0%, respectively. France has shown a broad seroprevalence ranging from 3.2% to as high as 52.0% among different blood donor populations. Denmark, England, Greece, Italy, Spain, Germany, and Switzerland have reported seroprevalence rates of 20.6, 16.0, 9.43, 8.7, 7.3, 6.8, and 4.9%, respectively, with a significant number of infections acquired locally. Moving to South Africa, Thailand, and India in the African and Asian continents, seroprevalences have been notably higher, with values of 42.8, 29.7, and 17.7%, respectively. In contrast, in Japan seroprevalence reported is very low (3.4%) (5, 6).
The seroprevalence of HEV within different population groups and regions of the Americas can range from 0 to 40.6%, as reported by Fernandez Villalobos et al. (2). The USA and Canada had seroprevalences of 18.3 and 5.9% (5, 6). In South America, studies conducted among blood donors have shown current prevalence rates ranging from 1.8 to 9.8%, indicating moderate circulation of HEV in the region. However, there is limited research on the overall epidemiology of HEV in South America, and the burden of the disease remains largely unknown. First serological studies in the continent were conducted during the 1990s and early 2000s, revealing prevalence rates ranging from 0.1 to 8% among both rural and urban populations. In 2011, studies conducted in Bolivia, Brazil, and Colombia reported varying seroprevalences of HEV (8–12).
In a previous study performed in a non-endemic area from Argentina, the seroprevalence was very low (1.80%) (13). In other studies, in the northwest region of the country, the HEV seroprevalences were 5.6% (95% CI: 2.3–11.2%) for an indigenous population, 9.23% for blood donors in Tucumán Province (Argentina) and 9% in Salta province (14–16). In the central region, Córdoba city (Argentina), the overall IgG anti-HEV prevalence obtained in blood donors (n = 547) was 3.47% (17). Di Lello et al. (18) conducted a study in blood donors (n = 391) of five Argentinian regions and found that HEV seropositivity varied from 5.1 to 20.0%.
There is a lack of systematically retrieved evidence on the seroprevalence and risk factors of HEV in Argentina in general and in Tandil (Buenos Aires province) in particular, which is a medium-sized city located in the central region of Argentina, where farming is one of the main economic activities. Therefore, and in order to provide evidence for targeted prevention strategies we carried out this study from a random sample that allowed an inference to be made to the entire population and was also carried out under the One Health approach (4). To address this research gap and provide valuable insights for targeted prevention strategies, this study aimed to achieve the following objectives: (i) Determine the seroprevalence of HEV among the human population in Tandil, Buenos Aires, Argentina. (ii) Evaluate the association between HEV seroprevalence and various demographic, socioeconomic, and other risk exposure variables. (iii) Describe and analyze the spatial patterns associated with HEV infection.
The study area comprises the South-eastern region of Buenos Aires province (Argentina), in which it is located the Tandilia mountain system. This region is characterized by agricultural and livestock production and sustains the biggest industrial concentration of the country and the most important urban settlements. Climatic regime along the study area is subhumid to humid mesothermal, with little or no water deficiency during summer months (December, January, and February). Over the course of the year, the absolute maximum temperatures range 37–39°C, and the absolute minimum range −6 to −7°C (19). The present study was carried out specifically in Tandil city, the head town of the Tandil district (coordinates 37°19′00″S; 59°08′00″W; area 52,34 km2). This is a community located approximately 360 km from Buenos Aires capital city, with a total population of 150,162 inhabitants (20). In Figure 1, the map displays the location of the city on a chain of valleys that descend from the Tandilia mountain system, to the South and West, a transition to the mountain foothills, located to the North and Northeast, with smoother and the plain area, slopes to the north of the urban area. The most important basin is that of the Langueyú System, which crosses the entire urban area of the city. The Langueyú stream originates from the merging of Del Fuerte and White surface courses, which were enclosed in tubes during the 70’s and 80’s. The study area encompasses both urban and peri-urban regions, with the latter being near agricultural and livestock activities. The process of urban expansion has occurred along two axes of expansion: one of them to the Northwest, and another to the North Center East and South East. The first axis is notable for its susceptibility to flooding during precipitation events, and it is located nearby the Langueyú stream (21) (Figure 1). Tandil city possesses a water supply network coverage of approximately 90%, but only a 60% coverage of sewage network. The sewage network is only for effluents, because the rest of the urban drainage is channeled through a stormwater drainage network. Although the sewage network and sewage treatment plants are adequate, their operation is altered by clandestine connections of household stormwater drains to the sewage network. Furthermore, the stormwater drainage network, which includes piped streams, is affected by clandestine connections of industrial and sewage effluents (19).
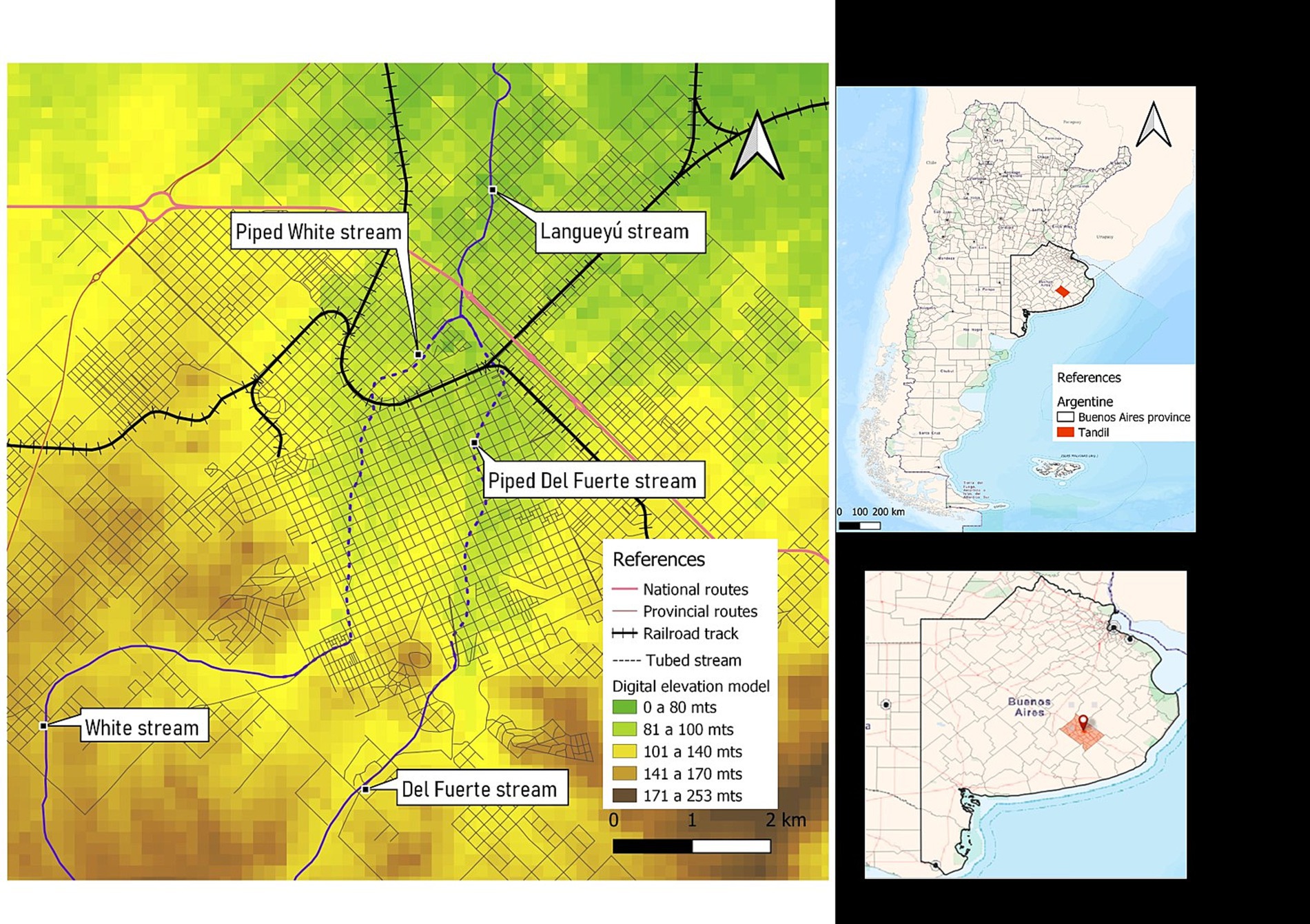
Figure 1. Map showing the location of the city of Tandil, in the province of Buenos Aires, Argentina. Digital elevation model and water courses.
Between August 2020 and July 2021, serum samples were collected from 969 individuals aged 1–80 years (median 44) by a random spatial sampling method. To assemble the sample of people to be analyzed, an anonymous list of all the people included in the digital medical records of the Tandil Public Health Integrated System was created. This list accounted for about 95% of the city’s total population and formed the sampling frame. A spatial random sampling without replacement was applied, considering the unequal distribution of the population according to age. The calculated minimum sample size was 783 assuming a seroprevalence of 9% with an absolute error of 2% and a confidence level of 95%. Immunocompromised individuals were excluded by asking about the history of immunosuppressive diseases or medications. Anti-HEV IgG was detected by a validated indirect in-house ELISA as described in Arce et al. (14) [sensitivity (93.33%), specificity (99.4%), and agreement (κ index = 0.94)], and seroprevalence within a 95% Confidence Interval (CI) was determined.
To assess the factors associated with the presence of anti-HEV antibodies, those individuals who agreed to be surveyed were interviewed by a trained interviewer using a semi-structured questionnaire designed ad hoc to obtain individual information on clinical and epidemiological data (Appendix 1). Information from these questionnaires included: socio-demographic, and housing characteristics, behaviors, education, occupation, animal and environmental exposure and clinical data. Data about knowledge of HEV infection and prevention measures were also collected. All the households of participants were geo-referenced using Global Positioning Systems (GPS).
Data analysis included descriptive statistics of means (with standard deviation) and medians (with first and third quartiles), depending on the distribution of the data, while categorical variables were expressed as percentages (%). The association between outcome (positivity) and the variables under analysis were assessed in two-way contingency table analyses using Pearson’s Chi-Squared Test or Fisher’s exact test if the expected value of one or more cells was less than 5. For quantitative variables two-sided Student’s t Test or Wilcoxon’s rank sum test were used. The null hypothesis stated that there were no differences between groups. Factors having significant p < 0.20 were selected and included in a multivariate logistic regression model. The maximum likelihood with a convergence criterion of 0.01 for a maximum of 10 interactions was used as the estimation method. The significance level was p < 0.05. The strength of association between each co-variable and seroprevalence was calculated and expressed as an estimated value by the adjusted OR and their respective 95% CI. To identify possible confusion factors, association between variables was assessed by χ2-test. In addition, interaction among variables was also evaluated in the logistic regression model. All statistical analyses were performed using InfoStat software (v2018).
The cartography was carried out by georeferencing the households of the volunteers included in the sampling; they were located on the map based on their geographical coordinates x and y. In turn, a digital elevation model of Tandil city was added, prepared from a 900 m2 satellite image from the SRTM (Shuttle Radar Topography Mission) mission. The resulting map was completed with information corresponding to the area reached by the running water and sewerage networks, each represented by a polygon over the city, making it possible to see what part of the population does not have these services.
Potential spatial clusters were investigated in the study area with space scan statistics using SaTScan software, v10.0.2. A Bernoulli model for high rates and low rates was performed for detecting spatial patterns (22). Also, factors associated with the clusters of high and low rates of positivity were assessed through bivariate and multivariate analyses with InfoStat software (v2018).
Then, the distances of each address of the people included in the sampling, in relation to the nearest watercourse, were calculated using ArcGIS software v10.2. The thematic cartography was completed with two maps. The first shows the areas according to flood risk and the second shows the location of the four wastewater treatment plants in Tandil (23).
The study complied with the revised Declaration of Helsinki for biomedical research involving human subjects, and was approved by the Ethics Committee of the National Institute of Epidemiology “Dr. Juan H. Jara,” Mar del Plata, Argentina (Code: RIVERO -02/2020) and the Teaching and Research Committee of the Integrated Public Health System of Tandil. Prior to enrolment, the researchers read an information sheet describing the study, answered any questions, and asked for written consent to participate. The participants received no compensation for their participation and were free to withdraw from the study at any time. Anonymity was guaranteed using an identification code.
None of the participants withdrawed from the study. Overall, 45/969 serum samples (4.64%) tested were positive for anti-HEV IgG (CI 95% 3.27–6.02).
Although 5 out of 40 (13%) seropositive cases had a previous diagnosis of hepatitis, the differences were not significant compared to seronegatives (8/108, 7%) (Fisher p = 0.51). None of the seropositive cases was previously diagnosed as an HEV infection.
Table 1 shows the signs and symptoms of subjects at p < 0.2 in the bivariate analysis as well as the relation with the seropositivity to HEV infection.

Table 1. Clinical characteristics of participants from Tandil, Buenos Aires Province, Argentina.
After the logistic regression analysis, the clinical manifestation associated with seropositivity to HEV was a history of dark urine OR 4.63 (CI 95% 1.23–17.39), p = 0.02.
Tables 2, 3 show the socio-demographic characteristics at p < 0.2 in the bivariate analysis as well as the relation with the seropositivity to HEV infection.
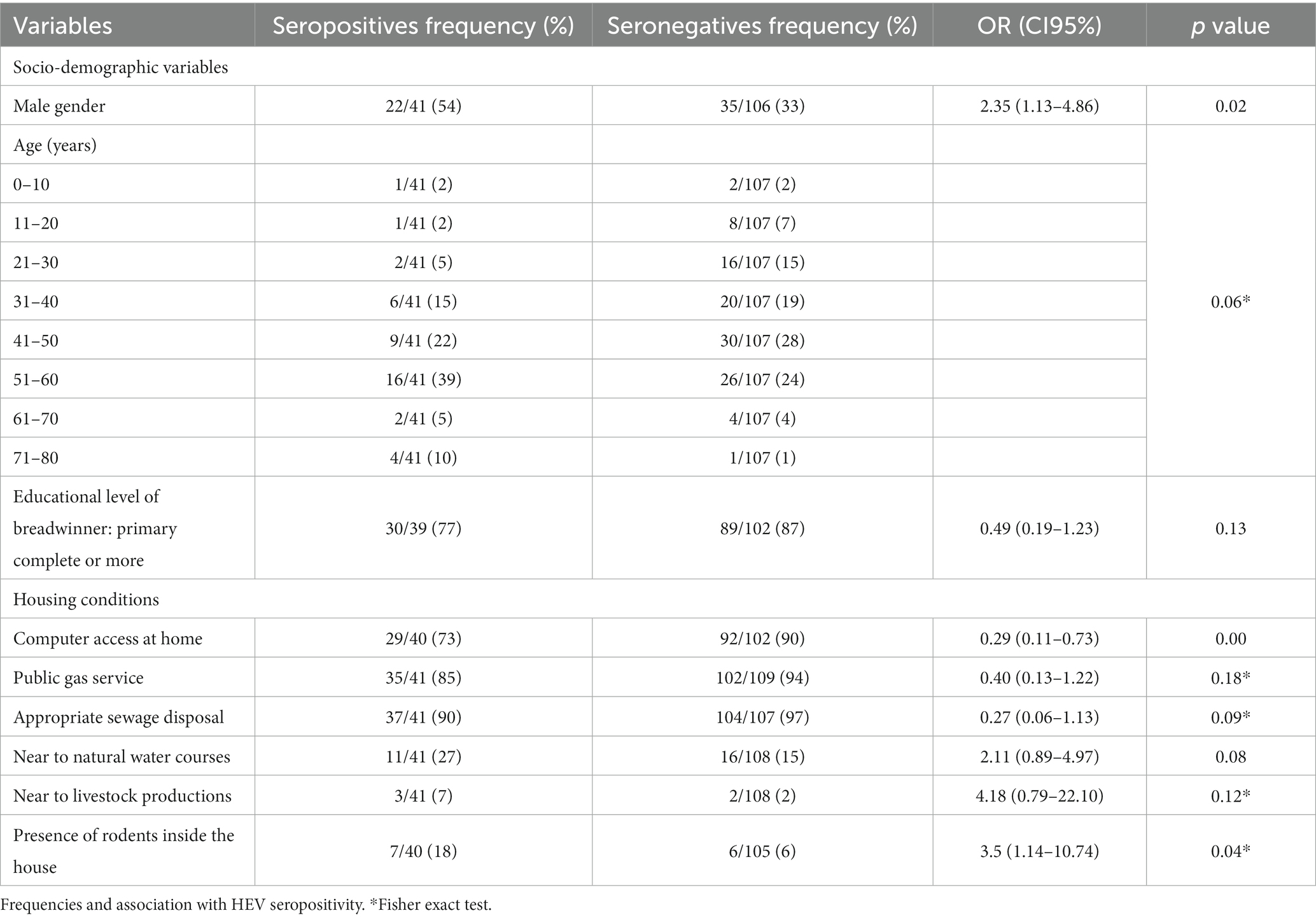
Table 2. Socio-demographic characteristics of participants from Tandil, Buenos Aires Province, Argentina.
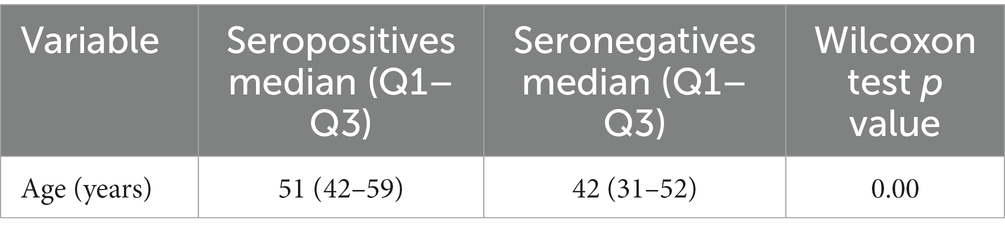
Table 3. Quantitative socio-demographic characteristics variables of respondents from Tandil, Buenos Aires Province, Argentina and association with HEV seropositivity.
In Tables 4, 5, occupations and other exposure activities of respondents at p < 0.2 in the bivariate analysis as well as the relation with the seropositivity to HEV infection are shown.
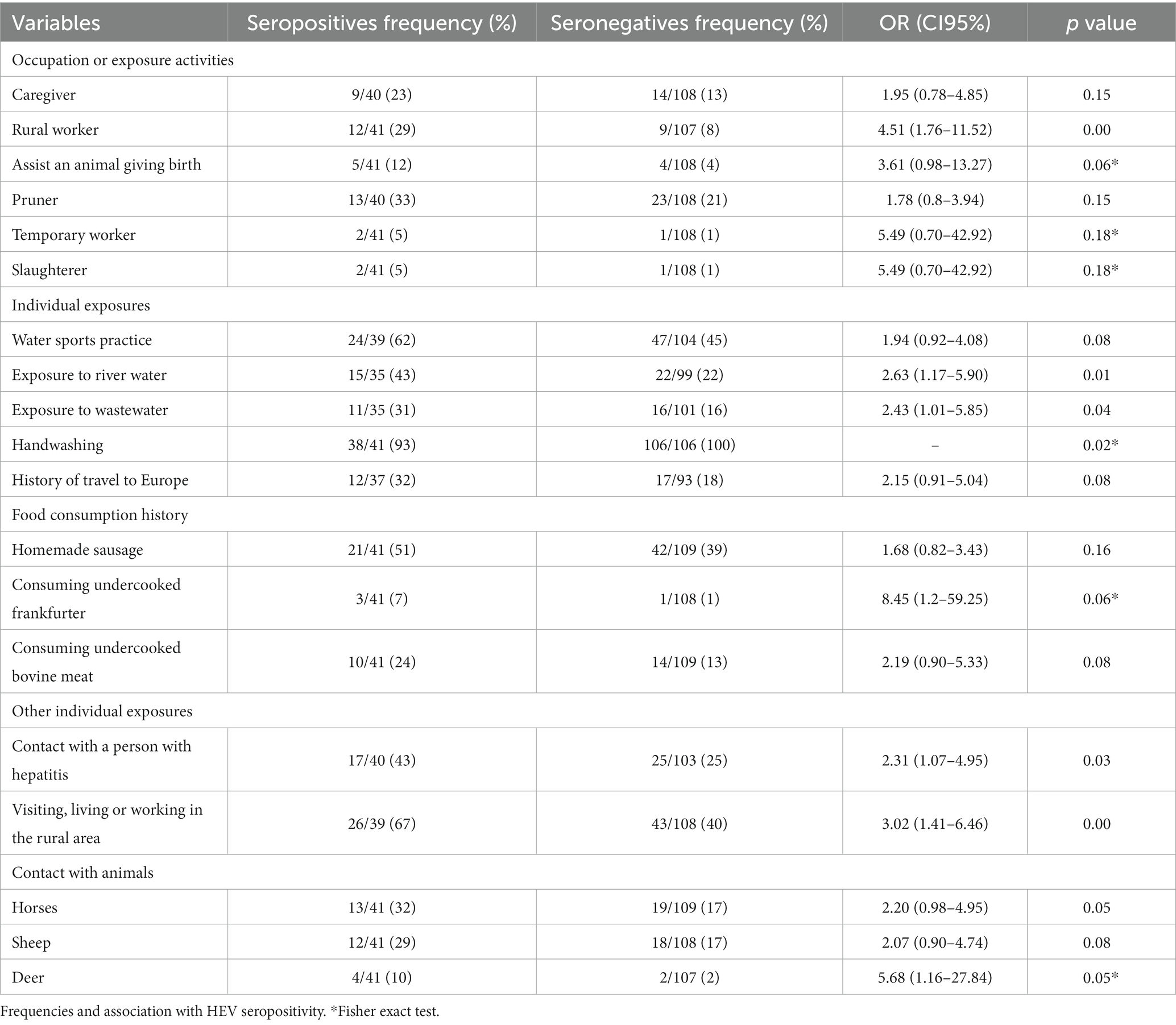
Table 4. Occupations and other exposure activities of participants from Tandil, Buenos Aires Province, Argentina.
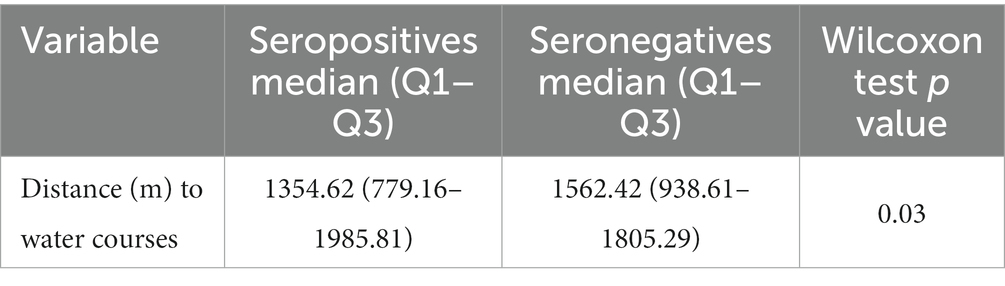
Table 5. Quantitative occupations and other exposure activities of respondents from Tandil, Buenos Aires Province, Argentina and association with HEV seropositivity.
After the logistic regression analysis, the significant predictors that best explained seropositivity to HEV were the presence of natural water courses near the households (OR: 3.24, 95% CI: 1.16–9.07, p = 0.02); the age as a quantitative variable (OR: 1.03, 95% CI: 1.00–1.06, p 0.04); and a history of previous travel to Europe (OR: 2.66, 95% CI: 1.01–7.01, p = 0.04) (Table 6).

Table 6. HEV seropositivity predictors in individuals from Tandil, Buenos Aires Province, Argentina as determined by multivariate logistic regression model.
The spatial distribution of the seropositive and seronegative cases is shown in Figure 2.
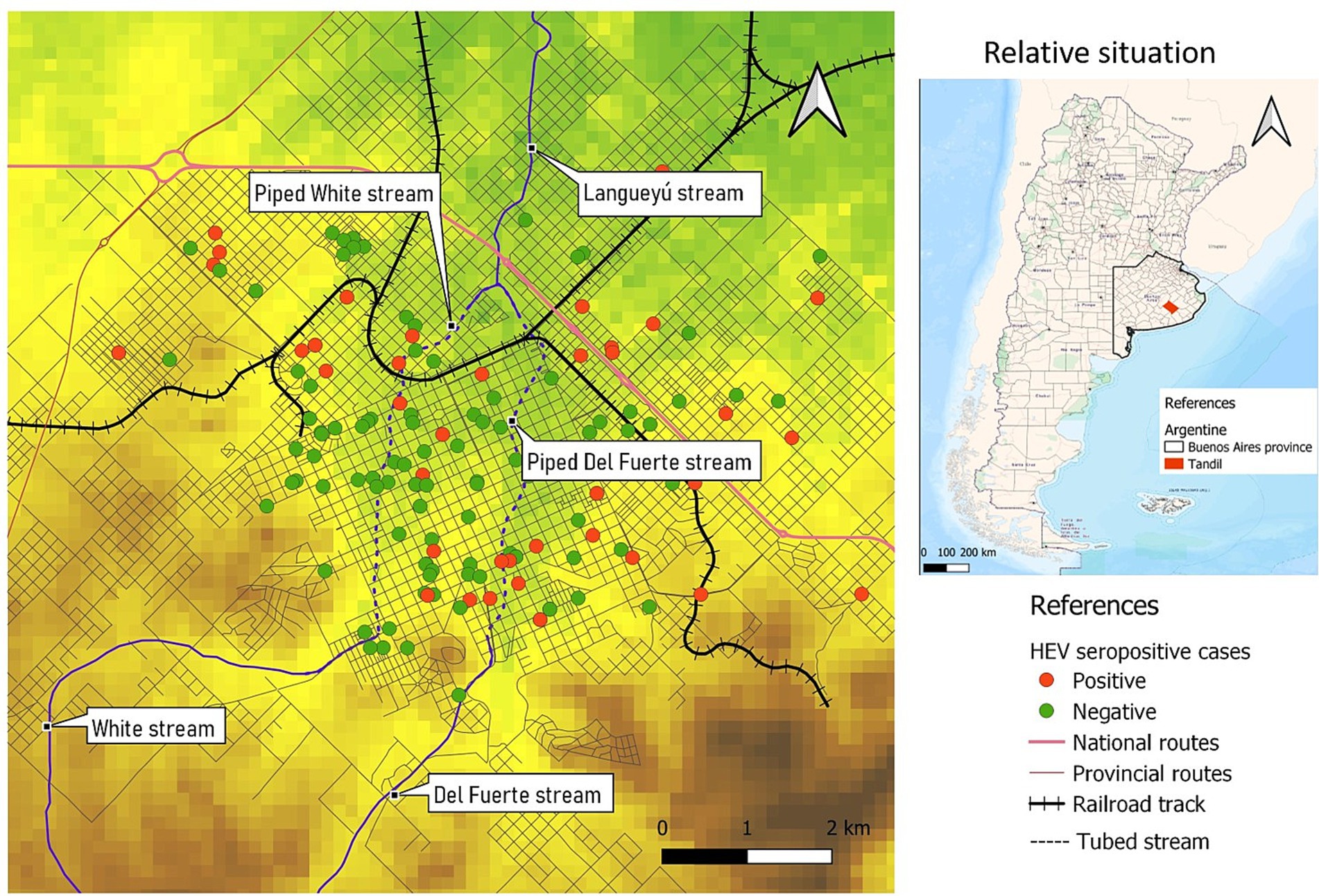
Figure 2. Spatial distribution of HEV seropositive cases and controls, Tandil, Buenos Aires Province, Argentina.
A spatial cluster of high rates of HEV seropositive cases was detected (coordinates of centroid: 37.308172S, 59.115827W; radius: 0.60 km). The entire population within the cluster, consisting of 5 individuals, exhibited seropositivity with a prevalence rate of 100% (p = 0.08). Additionally, a spatial cluster characterized by a low rate of HEV seropositivity cases was identified. The centroid of this second cluster was located at coordinates 37.323207S, 59.154066W, with a radius of 1.16 km. Within this cluster, a population of 25 individuals was observed, and none of them tested positive for HEV (0% seropositivity, p = 0.01) (Figure 3).
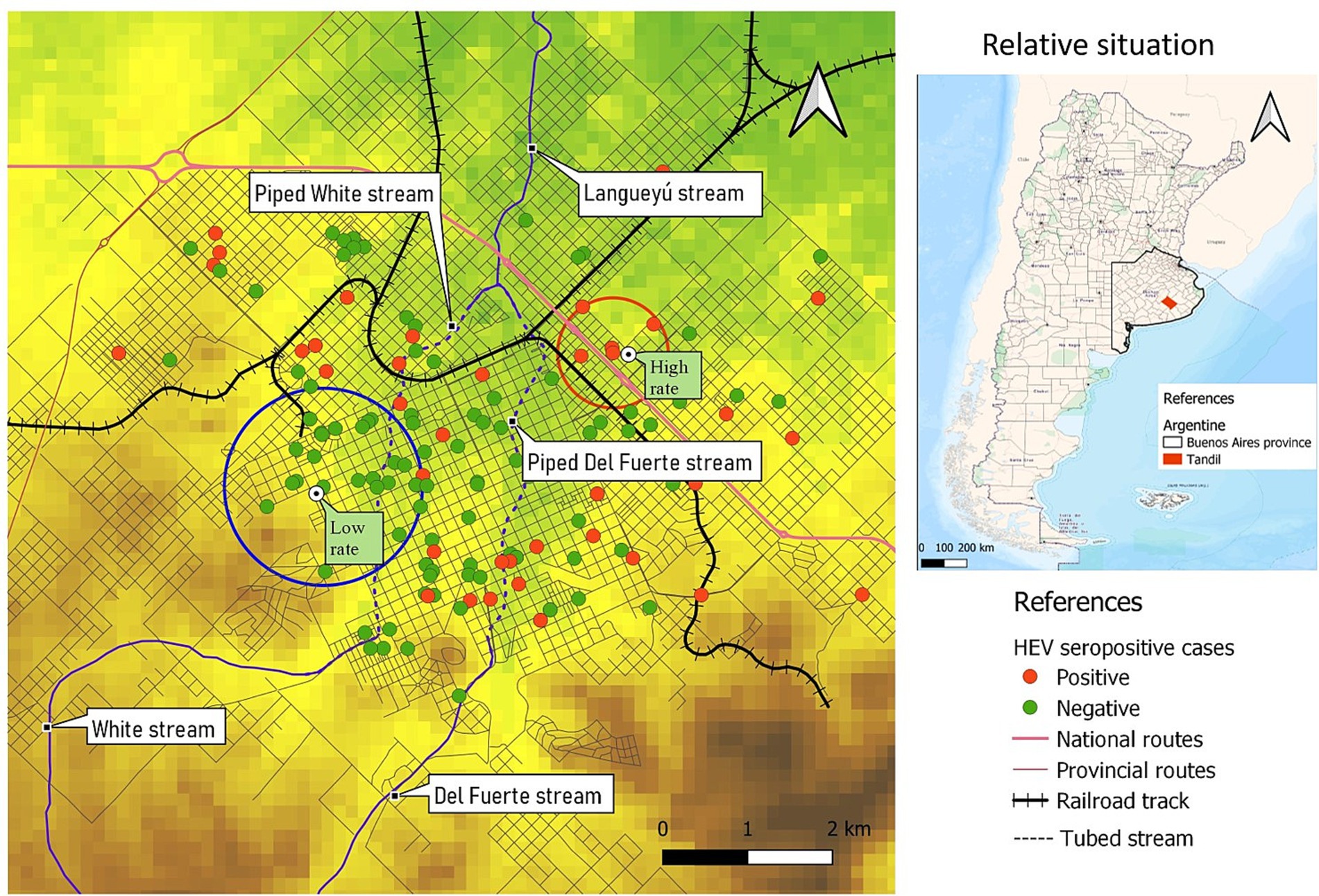
Figure 3. Spatial clusters of higher and lower risk of HEV.
Most of the individuals have access to appropriate sewage disposal and to safe drinking water at home (Figure 4). Significant differences in the proximity to water courses can be observed between individuals residing within the high-rate spatial cluster and those within the low-rate spatial cluster. Specifically, individuals living within the high-rate cluster tend to be in closer proximity to water courses compared to individuals residing within the low-rate cluster.
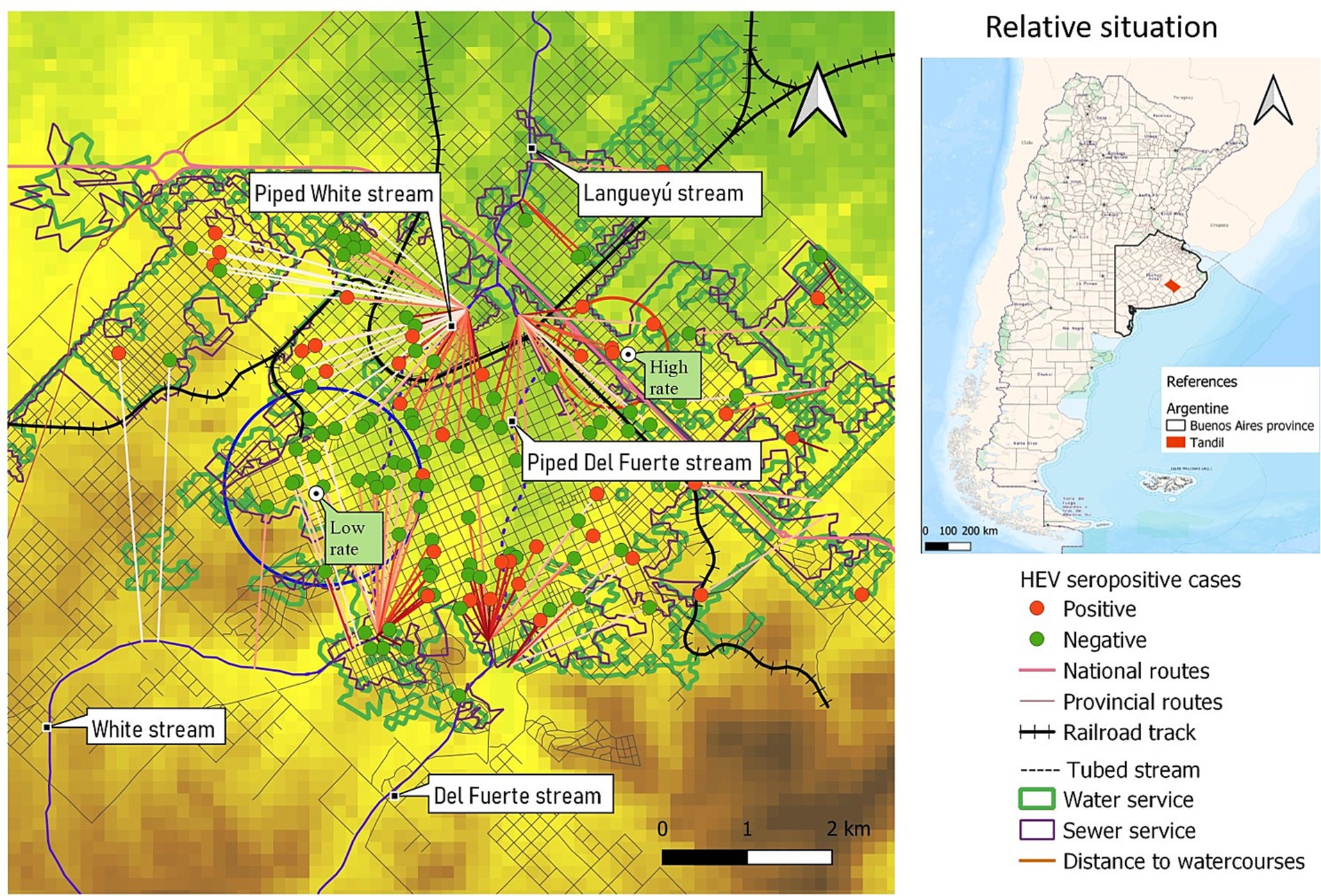
Figure 4. Distance to the nearest watercourses. Area covered by water and sewage services.
The high-risk spatial area is not only associated with increased risk but also coincides with regions prone to flooding during precipitation events. Additionally, it is situated in close proximity to the Langueyú stream (Figures 1, 4, 5). Furthermore, near the high-risk spatial cluster, there is a wastewater treatment plant (WTP) situated. Conversely, the occurrence of flooding events in the low-risk region is uncommon, as depicted in Figure 5.
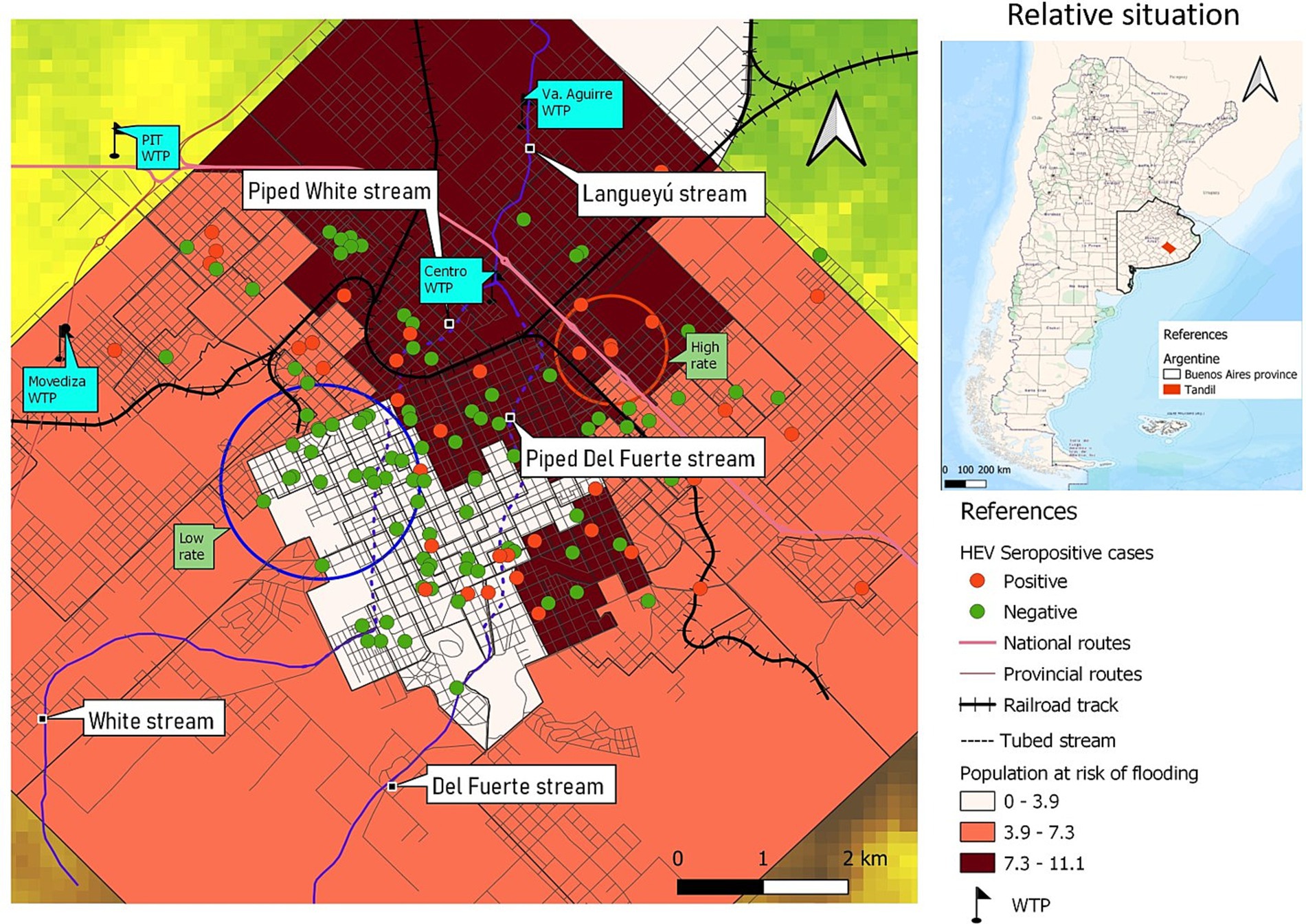
Figure 5. Population at risk of flooding and location of water treatment plants (WTP) in Tandil city.
In the evaluation of factors associated with residing within the high-rate spatial cluster, several variables showed significance (p < 0.2) in the bivariate analysis. These variables, as presented in Table 7, include male sex, engagement in rural work, and the proximity of water courses to residential areas.

Table 7. Variables at p < 0.2 related with being inside the high-risk spatial cluster of HEV seropositivity.
After the logistic regression analysis, the significant predictor that best explained being inside the high-risk spatial cluster of seropositivity to HEV was the presence of natural water courses near the households (OR: 7.50, 95% CI: 1.19–47.32, p = 0.03).
When assessing for factors associated with living inside the low-rate spatial cluster, variables at p < 0.2 in the bivariate analysis were: Male sex, rural work, distance to water courses and previous travel to Europe. All of them were inversely related to the low-risk cluster (Tables 8, 9).

Table 8. Variables at p < 0.2 related with being inside the low-risk spatial cluster of HEV seropositivity.

Table 9. Quantitative variable related with being inside the low-rate spatial cluster of HEV seropositivity.
After the logistic regression analysis, the significant predictors that best explained being inside the low-risk spatial cluster of seropositivity to HEV were the distance of natural water courses (OR 1.08; 95% CI 1.02–1.16; p = 0.01) and the male sex (OR 0.17; 95% CI 0.05–0.60; p = 0.00). Previous travel to Europe and rural activities was not incorporated into logistics because there were no individuals in the cluster with this characteristic.
Overall, 4.65 (95% CI 3.27–6.02) of the sera were positive. Although comparisons between studies are difficult due to differences in the demographics of the population studied and in the HEV antibody detection assays used, the results are similar to the levels reported in the Americas, that varies from 0 to 40.6%, as reported by Fernandez Villalobos et al. (2). And it is also close to the 5.6% seroprevalence seen in an indigenous population in northern Argentina, slightly higher to that reported in Córdoba (3.47%) and in Salta (9%), but lower to the seroprevalence observed in Tucumán (9.23%), all cities from Argentina (14–17).
In contrast to the aforementioned countries and regions where higher seroprevalence rates were reported (South Africa: 42.8%, Thailand: 29.7%, Bulgaria: 25.9%, Croatia: 21.5%, India: 17.7%, Serbia: 15%, southwest France: 16.6%, southwest England: 15.8%, Denmark in 2008: 20.6%, and the USA in 2002: 18.3%), the seroprevalence rate observed in Tandil is significantly lower (5, 6, 24). In the previously mentioned studies, seroprevalences correspond to sera from blood donors and not from the general population, differing from this study in the age of the individuals included.
None of the 41 seropositive cases had a previous diagnosis of HEV infection. Lack of knowledge among physicians and an absence of standardized diagnostic tests may result in increased morbidity and mortality from HEV infection (25).
Previous history of dark urine remained statistically significant after the logistic regression analysis. This sign was described before, related with the icteric phase of clinical presentation of acute hepatitis that may be prolonged for weeks or months in some cases. It should be considered for differential diagnosis, since hepatitis E seropositive cases presented this sign 4.63 times more often than seronegatives (7).
Despite not showing association in the logistic regression analysis, it is noteworthy that seropositive cases exhibited limited access to computers at home (p < 0.05). This variable, serving as an indirect indicator of socioeconomic status, indicates that the prevalence of HEV was higher among individuals from low income households. The reduced access to computers in poorer homes suggests a correlation between lower socioeconomic status and higher prevalence of HEV as it was reported in other regions of Latin America (26).
In the univariate analysis, male sex was found to be statistically associated with HEV infection and living inside the low-risk spatial cluster was inversely related with male sex; this result coincides with previous reports (27, 28). The higher incidence of the disease among males has been attributed to an increased presence of behavioral risk factors compared to females. Furthermore, men often engage in various environmentally related tasks that are traditionally considered “men’s jobs.” These tasks include activities such as irrigation farming using contaminated river water, and disposal of human and animal waste, swine veterinarians, pig slaughterers, meat inspectors, and sewage - workers.
Similar to other studies (2, 26, 30), we found that an increasing age is associated with HEV seroprevalence, mainly due to cumulative exposure but it may also be related to different lifestyles of the older adult.
Presence of natural water courses near the households was the exposure variable most related with a previous history of HEV infection. HEV cases were found to reside near water courses 3.24 times more often compared to seronegative cases. Additionally, the bivariate analysis revealed a significant association between exposure to river water and wastewater.
A spatial region with a high rate of cases was determined, in a peri-urban area that is close to agricultural areas and livestock. Moreover, people living inside the high-risk spatial cluster were 7.5 times closer to water courses than people living outside this area. Besides, the high-risk spatial cluster not only coincides with an area that is susceptible to flooding during precipitation events but is also situated in close proximity to the Langueyú stream. Also, a sewage treatment plant was located near the high-risk spatial cluster. It is noteworthy that the operation of the plant is altered by clandestine connections of home storm drains to the sewerage network. Furthermore, the stormwater drainage network, which includes piped streams, is affected by clandestine connections of industrial and sewage effluents (18). On the opposite, in the low-risk spatial cluster flooding events are unusual and people live more distant to water courses.
Contaminated water exposure is believed to have a significant impact on the transmission of various HEV subtypes, particularly in cases where direct zoonotic exposure is not involved. Several studies have highlighted the potential risk of environmental contamination in watersheds (such as rivers and dams) and the water distribution network due to the discharge of untreated urban wastewater or wastewater from pig slaughterhouses. This contamination can lead to waterborne infections among the exposed population. The notably high frequency of HEV RNA in urban sewage samples from Spain, the US, France and Israel clearly highlights the environmental presence of HEV (3, 31). This fact is underlined by the detection of HEV RNA in various water sources, especially during outbreaks of hepatitis E. Subclinical and sporadic infection in humans turns them into HEV reservoirs, being able to contaminate the environment through their feces (5). In turn, animals such as pigs or wild animals can act as reservoirs and can also directly impact the soil or surface waters, for example, by bathers or by defecation (32).
Today, most urban areas in the developing world still lack sufficient sewage treatment infrastructure. This deficiency not only results in significant ecological degradation of their waters but also poses substantial risks to human health. In unsewered urban areas, overflow from septic tanks and drainage from cesspools may enter surface waters via groundwater, and this pollution will largely act separately from the effects of urban stormwater runoff. Better knowledge on the source of HEV contamination, occurrence, persistance in water, and removal by water treatment is needed to unravel this transmission path (18, 32).
While HEV has the capability to infect various species such as bats, ferrets, rabbits, and chickens, the main reservoirs responsible for transmitting the virus to humans are swine, deer, and wild boar. Among these species, swine are widely regarded as the primary reservoir of HEV infection (25). There is a need to compile evidence on the zoonotic dissemination of the virus in animal hosts and the environment. In this work, the bivariate analysis revealed that seropositive cases presented rodents inside their houses with more frequency than seronegatives, although this was not statistically significant after logistic regression analysis. Besides, being a rural worker as well as visiting, living, or working in the rural area were related with the infection in the bivariate. Moreover, living inside the low-risk spatial cluster was inversely related to rural work. These exposures are also associated with contact with domestic animals.
Additionally, contact with deer was particularly identified as a risk factor in the bivariate analysis. This result coincides with (33) reports, who provided evidence of zoonotic transmission of HEV infection from deer to humans. Also, the presence of HEV RNA or antibodies has been described in deer, swine, cows, goats, and rodents, but no data is available for the area where this study was performed (34).
Prevention can be achieved through the provision of good basic hygiene. Handwashing was found to be a protective factor in the bivariate analysis. Moreover, in this study, previous contact with a case of hepatitis was associated with seropositivity in the bivariate analysis.
Previous travel to Europe was also related with seropositivity cases. Moreover, people living inside the low-risk spatial cluster were inversely associated with being in Europe. According to data published by European Centre for Disease Prevention and Control, the number of confirmed HEV cases in the European Union (EU) has been increasing each year from 514 in 2005 to 5,617 cases in 2015, representing a 10-fold increase. The most common way to become infected with HEV in the EU is through the consumption of raw or undercooked pork meat and liver (ECDC Report, 2017) (35). Furthermore, evidence suggests that HEV is an under-recognized pathogen in high-income countries. The actual number of human infections due to HEV in Europe is still unclear, given the widespread variations in clinical awareness, and testing surveillance practices, and a general lack of published information across the majority of EU/EEA Member States (35).
Consumption of undercooked HEV-contaminated food, such as meat, milk (cow, goat, sheep, and donkey) and molluscs, have been related to the infection; in this study, seropositive individuals had consumed more frequently homemade sausage, undercooked frankfurter and undercooked bovine meat than seronegative, although the differences were not statistically significant (36).
HEV seroprevalence estimated among the general population of Tandil city was 4.34%. Different factors related to the infection and a spatial pattern of high and low risk were determined, showing HEV multiple means of transmission. It is necessary to promote specific preventive actions (proper personal hygiene, handwashing after contact with animals, correct cook of animal products, provision for adequate clean drinking water, good environmental sanitation, proper disposal for animal and human feces) and specific diagnosis of HEV in the region under study, considering the populations with the highest risk of infection (people living near water courses and in floodable regions, adult men, rural worker, people traveling to Europe, etc.). Additionally, it is necessary to consider HEV in the differential diagnosis in individuals presenting acute hepatitis, particularly in populations susceptible to developing severe diseases, such as pregnant women, patients with chronic liver disease and immunocompromised patients. Considering it is an endemic disease in the region, it would be necessary to include HEV in the blood screening policy at donation centers to avoid transmission through blood transfusion, particularly to those who present a higher risk of experiencing more severe consequences.
These considerations could also be applied in other regions with similar socioeconomic characteristics.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by National Institute of Epidemiology “Dr. Juan H. Jara,” Mar del Plata, Argentina. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
MR: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing. LA: Investigation, Resources, Validation, Writing – review & editing. SG: Conceptualization, Investigation, Resources, Writing – review & editing. AT: Data curation, Funding acquisition, Methodology, Resources, Visualization, Writing – review & editing. JP: Data curation, Visualization, Writing – review & editing. JS: –. AB: Investigation, Writing – review & editing. FS: Investigation, Writing – review & editing. JM: Investigation, Writing – review & editing. SE: Conceptualization, Investigation, Writing – review & editing. MV-P: Funding acquisition, Project administration, Resources, Supervision, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by grant N°03-PIO-85H from Secretaría de Ciencia, Arte y Tecnología (UNCPBA), and PICT 2017-4652 and PICT2019-3382 from ANPCYT, Argentina.
We wish to thank to the Sistema Integrado de Salud Pública de Tandil for the assistance in the collection of serum samples. FS was holder of a fellowship from Secretaría de Ciencia, Arte y Tecnología (UNCPBA) (Subsidios de Ingreso a la Investigación (INI) 2021/2022).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1257754/full#supplementary-material
1. Blasco-Perrin, H, Abravanel, F, Blasco-Baque, V, and Peron, JM. Hepatitis E, the neglected one. Liver Int. (2016) 36:130–4. doi: 10.1111/liv.13014
2. Fernandez Villalobos, NV, Kessel, B, Rodiah, I, Ott, JJ, Lange, B, and Krause, G. Seroprevalence of hepatitis E virus infection in the Americas: estimates from a systematic review and meta-analysis. PLoS One. (2022) 17:e0269253. doi: 10.1371/journal.pone.0269253
3. Clemente-Casares, P, Pina, S, Buti, M, Jardi, R, MartIn, M, Bofill-Mas, S, et al. Hepatitis E virus epidemiology in industrialized countries. Emerg Infect Dis. (2003) 9:448–54. doi: 10.3201/eid0904.020351
4. de Oliveira, JM, Dos Santos, DRL, and Pinto, MA. Hepatitis E virus research in Brazil: looking back and forwards. Viruses. (2023) 15. doi: 10.3390/v15020548
5. Raji, YE, Toung, OP, Taib, NM, and Sekawi, ZB. Hepatitis E virus: an emerging enigmatic and underestimated pathogen. Saudi J Biol Sci. (2022) 29:499–512. doi: 10.1016/j.sjbs.2021.09.003
6. Kaufmann, A, Kenfak-Foguena, A, Andre, C, Canellini, G, Burgisser, P, Moradpour, D, et al. Hepatitis E virus seroprevalence among blood donors in Southwest Switzerland. PLoS One. (2011) 6:e21150. doi: 10.1371/journal.pone.0021150
7. Krain, LJ, Nelson, KE, and Labrique, AB. Host immune status and response to hepatitis E virus infection. Clin Microbiol Rev. (2014) 27:139–65. doi: 10.1128/CMR.00062-13
8. Di Cola, G, Fantilli, AC, Pisano, MB, and Re, VE. Foodborne transmission of hepatitis a and hepatitis E viruses: a literature review. Int J Food Microbiol. (2021) 338:108986. doi: 10.1016/j.ijfoodmicro.2020.108986
9. Dos Santos, DRL, Duraes-Carvalho, R, Gardinali, NR, Machado, LC, de Paula, VS, da Luz Wallau, G, et al. Uncovering neglected subtypes and zoonotic transmission of hepatitis E virus (HEV) in Brazil. Virol J. (2023) 20:83. doi: 10.1186/s12985-023-02047-6
10. Pisano, MB, Martinez-Wassaf, MG, Mirazo, S, Fantilli, A, Arbiza, J, Debes, JD, et al. Hepatitis E virus in South America: the current scenario. Liver Int. (2018) 38:1536–46. doi: 10.1111/liv.13881
11. Pisano, MB, Winter, M, Raimondo, N, Martinez-Wassaf, MG, Abate, SD, and Re, VE. New pieces in the transmission cycle of the hepatitis E virus in South America: first viral detection in wild boars from Argentina. Trans R Soc Trop Med Hyg. (2019) 113:497–9. doi: 10.1093/trstmh/trz034
12. Tissera, G, Lardizabal, MC, Torres, SB, Fantilli, AC, Martinez Wassaf, MG, Venezuela, F, et al. Hepatitis E virus infection in pregnant women, Argentina. BMC Infect Dis. (2020) 20:368. doi: 10.1186/s12879-020-05087-3
13. Rey, JA, Findor, JA, Daruich, JR, Velazco, CC, Igartua, EB, Schmee, E, et al. Prevalence of IgG anti-HEV in Buenos Aires, a nonendemic area for hepatitis E. J Travel Med. (1997) 4:100–1. doi: 10.1111/j.1708-8305.1997.tb00788.x
14. Arce, LP, Muller, MF, Martinez, A, Baiker, A, Marranzino, G, Agote, F, et al. A novel in-house enzyme-linked immunosorbent assay for genotype 3 hepatitis E virus reveals high seroprevalence in blood donors in northern Argentina. Front Microbiol. (2019) 10:2481. doi: 10.3389/fmicb.2019.02481
15. Pisano, MB, Lugo, BC, Poma, R, Cristobal, HA, Raskovsky, V, Martinez Wassaf, MG, et al. Environmental hepatitis E virus detection supported by serological evidence in the northwest of Argentina. Trans R Soc Trop Med Hyg. (2018) 112:181–7. doi: 10.1093/trstmh/try048
16. Remondegui, C, Ceballos, S, Arce, LP, Pintado, E, Vidaurre, R, Nitschko, H, et al. Serologic evidence of the circulation of the hepatitis E virus and the prevalence of antibodies against hepatitis a in an indigenous population in northern Argentina. Rev Argent Microbiol. (2021) 53:314–24. doi: 10.1016/j.ram.2020.10.006
17. Pisano, MB, Blanco, S, Di Cola, G, Fantilli, AC, Martinez Wassaf, MG, Carrizo, LH, et al. Hepatitis E virus in blood donors from Argentina: a possible source of viral infection? Travel Med Infect Dis. (2022) 48:102355. doi: 10.1016/j.tmaid.2022.102355
18. Di Lello, FA, Blejer, J, Alter, A, Bartoli, S, Vargas, F, Ruiz, R, et al. Seroprevalence of hepatitis E virus in Argentinean blood donors. Eur J Gastroenterol Hepatol. (2021) 33:1322–6. doi: 10.1097/MEG.0000000000001853
19. Cortelezzi, A, Barranquero, RS, Marinelli, CB, Fernandez San Juan, MR, and Cepeda, RE. Environmental diagnosis of an urban basin from a social-ecological perspective. Sci Total Environ. (2019) 678:267–77. doi: 10.1016/j.scitotenv.2019.04.334
20. INDEC, I. N. d. E. y. C. Censo nacional de población, hogares y viviendas 2022: resultados provisionales. Ciudad Autónoma de Buenos Aires: Instituto Nacional de Estadística y Censos (2023).
21. La Macchia, M. L. (2015). Modelización y análisis espacial del drenaje urbano de la ciudad de Tandil mediante TIG’s [Trabajos completos]. In II Jornadas Nacionales de Ambiente 2014: libro de trabajos completos (1a ed. ed., pp. 493-502). Tandil: Facultad de Ciencias Humanas. Universidad Nacional del Centro de la Provincia de Buenos Aires. Campus Universitario - Paraje Arroyo Seco s/n – 7000 Tandil Available at: http://www.iijornadasnacionalesdeambiente.com/.
22. Pfeiffer, DU, and Stevens, KB. Spatial and temporal epidemiological analysis in the big data era. Prev Vet Med. (2015) 122:213–20. doi: 10.1016/j.prevetmed.2015.05.012
23. Avalo, Estefanía, Paz, Laura, Cochero, Joaquín, Simonetti, Maximo, Suarez, Jimena, and Cortelezzi, Agustina. (2022). Caracterización de los vuelcos de plantas de tratamiento de aguas residuales ¿Dentro de los valores máximos legislados? Proceedings of the 11 Congreso de Ecología y Manejo de Ecosistemas Acuáticos Pampeanos Bahía Blanca, Buenos Aires, Argentina. (2022).
24. Buti, M, Dominguez, A, Plans, P, Jardi, R, Schaper, M, Espunes, J, et al. Community-based seroepidemiological survey of hepatitis E virus infection in Catalonia, Spain. Clin Vaccine Immunol. (2006) 13:1328–32. doi: 10.1128/CVI.00255-06
25. De Keukeleire, S, and Reynders, M. Hepatitis E: an underdiagnosed, emerging infection in nonendemic regions. J Clin Transl Hepatol. (2015) 3:288–91. doi: 10.14218/JCTH.2015.00039
26. Martinez Wassaf, MG, Pisano, MB, Barril, PA, Elbarcha, OC, Pinto, MA, Mendes de Oliveira, J, et al. First detection of hepatitis E virus in Central Argentina: environmental and serological survey. J Clin Virol. (2014) 61:334–9. doi: 10.1016/j.jcv.2014.08.016
27. Kuniholm, MH, Purcell, RH, McQuillan, GM, Engle, RE, Wasley, A, and Nelson, KE. Epidemiology of hepatitis E virus in the United States: results from the third national health and nutrition examination survey, 1988-1994. J Infect Dis. (2009) 200:48–56. doi: 10.1086/599319
28. Lewis, HC, Wichmann, O, and Duizer, E. Transmission routes and risk factors for autochthonous hepatitis E virus infection in Europe: a systematic review. Epidemiol Infect. (2010) 138:145–66. doi: 10.1017/S0950268809990847
29. Junaid, SA, Agina, SE, and Abubakar, KA. Epidemiology and associated risk factors of hepatitis e virus infection in plateau state, Nigeria. Virology. (2014) 5:15–26. doi: 10.4137/VRT.S15422
30. Christensen, PB, Engle, RE, Hjort, C, Homburg, KM, Vach, W, Georgsen, J, et al. Time trend of the prevalence of hepatitis E antibodies among farmers and blood donors: a potential zoonosis in Denmark. Clin Infect Dis. (2008) 47:1026–31. doi: 10.1086/591970
31. Ram, D, Manor, Y, Gozlan, Y, Schwartz, E, Ben-Ari, Z, Mendelson, E, et al. Hepatitis E virus genotype 3 in sewage and genotype 1 in acute hepatitis cases, Israel. Am J Trop Med Hyg. (2016) 95:216–20. doi: 10.4269/ajtmh.15-0925
32. Takuissu, GR, Kenmoe, S, Ndip, L, Ebogo-Belobo, JT, Kengne-Nde, C, Mbaga, DS, et al. Hepatitis E virus in water environments: a systematic review and meta-analysis. Lancet. (2003) 362:371–3. doi: 10.1016/S0140-6736(03)14025-1
33. Tei, S, Kitajima, N, Takahashi, K, and Mishiro, S. Zoonotic transmission of hepatitis E virus from deer to human beings. Food Environ Virol. (2022) 14:223–35. doi: 10.1007/s12560-022-09530-3
34. Reuter, G, Boros, A, and Pankovics, P. Review of hepatitis E virus in rats: evident risk of species orthohepevirus C to human zoonotic infection and disease. Viruses. (2020) 12:1148. doi: 10.3390/v12101148
35. European Centre for Disease Prevention and Control. Hepatitis E in the EU/EEA, 2005–2015. Stockholm: ECDC (2017).
Keywords: hepatitis E virus (HEV), seroprevalence, risk factors, spatial analyses, water exposure
Citation: Rivero MA, Arce LP, Gutiérrez SE, Tisnés A, Passucci JA, Silva JA, Barón Prato A, Sánchez F, Matias Brancher J, Estein SM and Vizoso-Pinto MG (2023) Exploring hepatitis E virus seroprevalence and associated risk factors among the human population in Tandil, Buenos Aires, Argentina. Front. Public Health. 11:1257754. doi: 10.3389/fpubh.2023.1257754
Edited by:
Russell Kabir, Anglia Ruskin University, United KingdomReviewed by:
Lisandru Capai, Université de Corse Pascal Paoli, FranceCopyright © 2023 Rivero, Arce, Gutiérrez, Tisnés, Passucci, Silva, Barón Prato, Sánchez, Matias Brancher, Estein and Vizoso-Pinto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mariana Alejandra Rivero, bXJpdmVyb0B2ZXQudW5pY2VuLmVkdS5hcg==; María Guadalupe Vizoso-Pinto, bWd2aXpvc29AZm0udW50LmVkdS5hcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.