 Stefania Paduano1*
Stefania Paduano1* Maria Chiara Facchini1Lucia Borsari2
Maria Chiara Facchini1Lucia Borsari2 Alessandra D’Alterio1Laura Iacuzio2Antonella Greco2Elisabetta Fioretti2Giacomo Creola2Zaynalabedin Kahfian2Stefano Zona3Annalisa Bargellini1
Alessandra D’Alterio1Laura Iacuzio2Antonella Greco2Elisabetta Fioretti2Giacomo Creola2Zaynalabedin Kahfian2Stefano Zona3Annalisa Bargellini1 Tommaso Filippini1,4
Tommaso Filippini1,4- 1Department of Biomedical, Metabolic and Neural Sciences – Section of Public Health, University of Modena and Reggio Emilia, Modena, Italy
- 2Department of Public Health – Public Hygiene Service, Local Health Authority of Modena, Modena, Italy
- 3Infection Control Strategic Group, Local Health Authority of Modena, Modena, Italy
- 4School of Public Health, University of California, Berkeley, Berkeley, CA, United States
Introduction: In Italy, over 4.8 million individuals aged 0–19 years have been infected with SARS-CoV-2. This study aims to evaluate the spread of SARS-CoV-2 within schools in Modena province and the influence of anti-SARS-CoV-2 vaccination coverage.
Methods: We performed a survey in the period 1 September-15 December 2021, involving student population aged 0–19 years and related teachers screened for SARS-CoV-2 infection using nasopharyngeal swab after the detection of an index case within their class. During the study period, vaccination against SARS-CoV-2 was actively offered to all subjects aged ≥12 years.
Results: A total of 13,934 subjects were tested, 12,534 students and 1,400 teachers (594 classes). We identified a total of 594 and 779 index and secondary cases, respectively. We found that 9.8% of students and 10.6% of teachers were positive for SARS-CoV-2. Overall at the test time, 32.5% were vaccinated with at least one dose of anti-SARS-CoV-2 vaccine. Among secondary cases, 7.8% were vaccinated compared to 34.9% among negative tested subjects. A higher secondary attack rate was for non-vaccinated subjects rather than vaccinated ones (8.1% vs. 1.4%). Higher secondary attack rates were reported for subjects attending infant and primary school (5.9 and 9.6%, respectively). Lower secondary attack rates were for those who attended middle school (4.9%) and especially high school (1.7%).
Conclusion: Our results highlight the differential spread of the infection within various educational settings and that the vaccination, available in the study period for the population aged ≥12, have mitigated SARS-CoV-2 spread in high and middle schools.
1. Introduction
In Italy, over 4.8 million individuals aged 0–19 years have been infected by SARS-CoV-2 virus, representing about 19% of all reported cases since the beginning of the pandemic (1, 2). Schools closures, home confinement, and social distancing measures have disrupted the children daily routines and adolescents and limited their access to social activities, which can have negative effects on their mental health and well-being, with a significant decrease in quality of life (3–5). COVID-19 has strictly related to children and adolescents’ development due to confinement measures (6).
Worldwide, one of the main preventive strategy against the COVID-19 pandemic was schools closure, even if, in the early stages of the pandemic, the role of children in the transmission of the virus was unknown (7). In Italy, most of the children did not present symptoms and for this reason they were quarantined at home without any molecular or antigenic tests (8). Additionally, physical distancing and specifically distance learning in school setting have been implemented in several countries, including Italy; as a consequence, no increased risk of infection was reported among workers of the education sector (9, 10).
Keeping school as a safe and accessible environment is of utmost importance and goes beyond the primary objective of the educational needs as it affects the social and mental development of children (6), and it is the primary means to reduce inequality (11). The role of school in SARS-CoV-2 spread and the effectiveness of its closure in the control of the epidemic has been long debated. Several studies showed that the prevalence of positive cases in schools is lower than in the general population when appropriate mitigation measures are implemented, as well as the number and size of clusters in educational settings are generally smaller (12–16).
The health behavioral policies adopted before the availability of the vaccination and still in use helped in mitigating the risk of viral spread in schools; particularly, contact tracing turned out to be useful to promptly isolate infected students and staff (17). Regular testing could be also a key strategy to control the epidemic in school settings characterized by lower vaccination coverage compared to the general adult population or after the waning of vaccine protection, minimizing lost days (18). A modeling study in simulated elementary and middle schools found that screening tests eased in-person schooling with limited transmission risk, and test-to-stay policies were associated with increased school attendance and only little incremental transmission. Epidemiological surveillance has been identified as a useful, low-cost option for the detection of outbreaks and identification of school environments that could benefit from increased mitigation (19).
A widespread increase in vaccination coverage for the pediatric population has been strongly recommended (20, 21). Initially, the European Medicines Agency (EMA) recommended the administration of the vaccine to children aged 12 years and above. Subsequently, this recommendation was extended to encompass children below 12 years (22). After that, on 7 December 2021, the Italian Ministry of Health extended the use of the vaccine to children aged 5–11 years (23). In Emilia Romagna Region, since 16 December 2021 vaccination against SARS-CoV-2 has been also available for subjects aged 5–11 years (24).
The acceptance of vaccination against SARS-CoV-2 among parents has a significant role: the safety of vaccination is considered the most important factor affecting vaccine hesitancy during childhood (25). Therefore, advocating the safety and efficacy of vaccines through trusted and institutional sources might help the development of a sense of confidence and security among parents and the general public (26, 27). Researchers underlined that virus circulation among students, educators, staff, and their family members is high when a highly infectious variant predominates in unvaccinated students. Nevertheless, the implementation of mitigation measures or use of vaccinations in students can substantially reduce these modeled risks (28). Especially, vaccination remains the most effective and sustainable strategy for risk reduction, thus efforts should focus on the increase of coverage and use of booster doses among eligible students and school staff (29).
Since children infected with SARS-CoV-2 are mostly without symptoms or with mild non-specific symptoms, outbreaks are difficult to record in educational settings (30, 31). Therefore, this study aims to assess the spread of SARS-CoV-2 within schools in Modena province and the influence of vaccination coverage in these settings.
2. Methods
This study was approved by the “Area Vasta Emilia Nord” Ethics Committee (approval no. AUO/0017667/20 of June 25, 2020).
2.1. Study population
We performed a survey in school settings of Modena province (Northern Italy) in the period from September 1 to December 15, 2021. We considered all students and teachers who were screened for SARS-CoV-2 infection through nasopharyngeal swab after the detection of an index case within their classroom, and the related onset of secondary cases.
According to ministerial and regional policies (32), teachers and students were tested if they attended the same class with a confirmed positive case in the 48 h prior test or symptoms onset (school contact). Differently from the general definition of close contact, the distance from the index case was not considered to define a school contact who has to be included in the screening. Screening tests were performed with molecular or antigenic tests, but in case of positive result with antigenic test, individuals needed molecular test to be considered a confirmed secondary case. Indication for quarantine varied from nursery, infant, primary and secondary (middle and high) schools, but the execution of at least one nasopharyngeal swab for SARS-CoV2 was mandatory for the re-admission to all the grades of school. Non-adherence to screening tests was very low (<5%). In the analysis, these few subjects were considered negative for SARS-CoV-2 screening. We considered as a school cluster the presence of 2 or more SARS-CoV-2 cases (students or teachers with a positive molecular SARS-CoV-2 test, regardless the occurrence of correlated symptoms) attending the same classroom within a period of 14 days. In the considered period, vaccination against SARS-CoV-2 was actively offered to all subjects aged at least 12 years, while for children under 12 years old, the use of vaccine was still not approved. All the data have been collected by the Public Health Department of Modena Local Health Authority (AUSL Modena) through an application with a specific designed format for contact tracing in the pandemic period.
2.2. Data analysis
For continuous variables, we reported mean, standard deviation (SD), and range (min-max). For categorical variables, we reported absolute (N) and relative (%) frequencies. We performed the analyses in the entire study population and in selected subgroups. In particular, we subdivided the sample of teachers/students into not-vaccinated and vaccinated for SARS-CoV-2. This latter group was further divided according to the type of educational setting. To evaluate the spread of infection, secondary attack rate was calculated. Secondary attack rate was defined as the number of secondary cases exposed to index cases divided by total number of tested subjects exposed to index cases. We also compared the daily incidence of new cases over time occurred in the study sample with those occurred in the overall population of Modena province. Moreover, we assessed the influence of vaccination coverage on the SARS-CoV-2 spread of within schools using a logistic regression model adjusted for relevant confounders, sex, age group, type of educational setting and school role (teachers/students) for calculating the odds ratio (OR) with 95% confidential intervals (95% CI). Data analysis was performed using statistical software Stata v17.0 (StataCorp, College Station, TX, USA, 2021).
3. Results
From September 1 to December 15, 2021, 594 classes were followed by the Public Health Dept. of AUSL Modena due to the identification of an index case, with 13,934 subjects tested for SARS-CoV-2. Specifically, we included 1,400 teachers and 12,534 students within different educational settings, from nursery school up to high school. The identified clusters were 265 with a range of 2–22 total cases within the class (from 1 to 21 secondary cases). Through swab testing in the study population, 1,373 (9.9%) were identified as confirmed cases (10.6% of teachers and 9.8% of students), of whom 594 were classified as index cases and 779 as secondary cases. Among index cases, 101 (17.0%) were teachers and 493 (83.0%) were students; among secondary cases, 47 (6.0%) and 732 (94.0%), respectively.
We collected data on vaccination status. Within the study population, information on the vaccination coverage was missing for only 24 (0.2%) subjects, respectively 14 teachers and 10 students, and none of them was a confirmed case. These data are summarized in Table 1, along with socio-demographic characteristics.
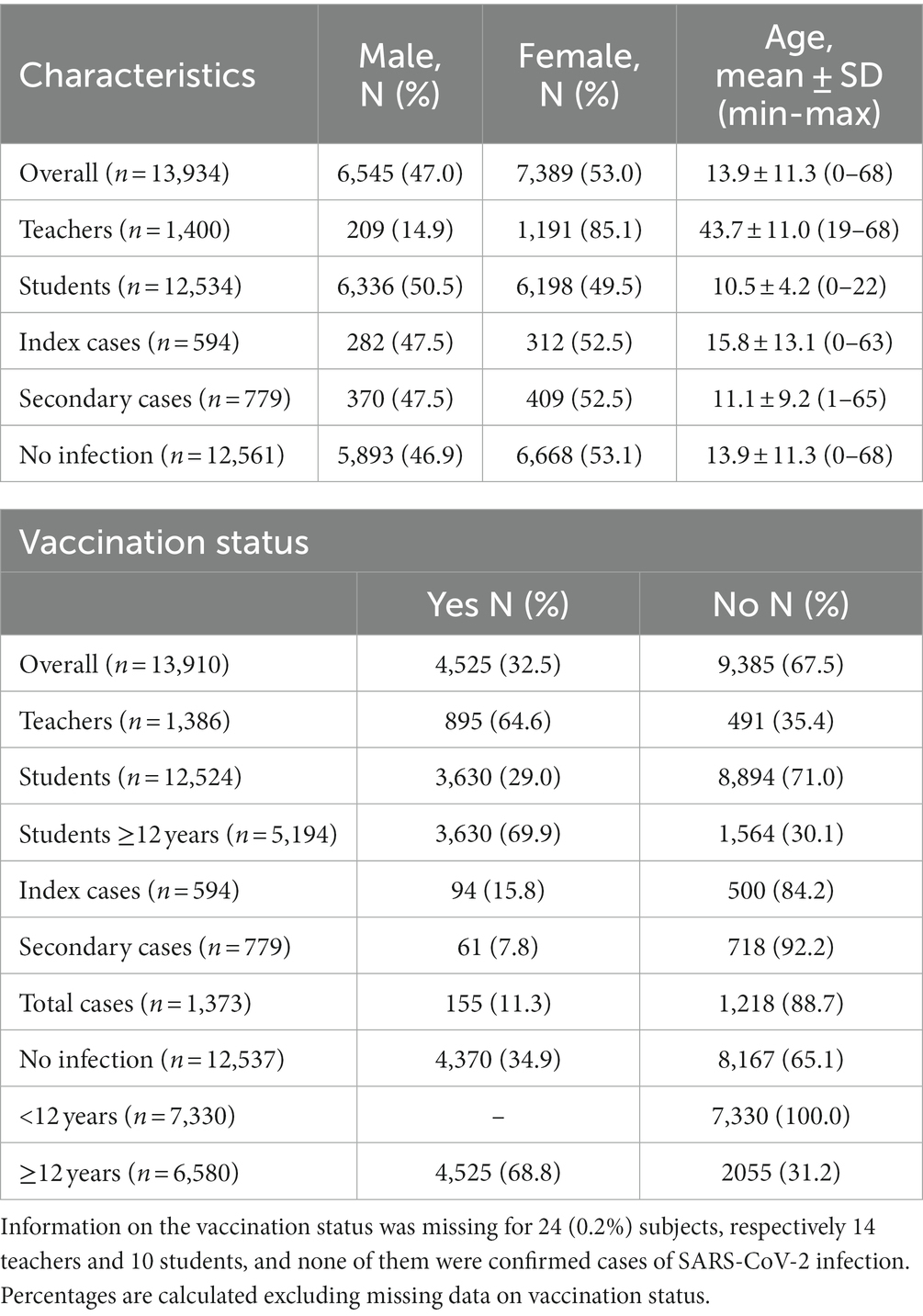
Table 1. Socio-demographic characteristics and vaccination status of the total population (n = 13,934) and divided into different subgroups.
Among all included subjects, 4,525 (32.5%) resulted to be vaccinated with at least one dose at the moment of exposure to virus. A higher percentage of vaccinated individuals (68.5%) could be observed considering only the population aged ≥12 years, for which the vaccination was regularly offered.
Out of 1,373 confirmed cases, only 155 (11.3%) were vaccinated, and the proportion decreased among secondary cases (7.8%), which are possibly related to school attendance.
In Tables 2, 3, we reported both secondary and index cases rate and secondary attack rate within the study population, divided into different subgroups based upon vaccination status or educational setting.
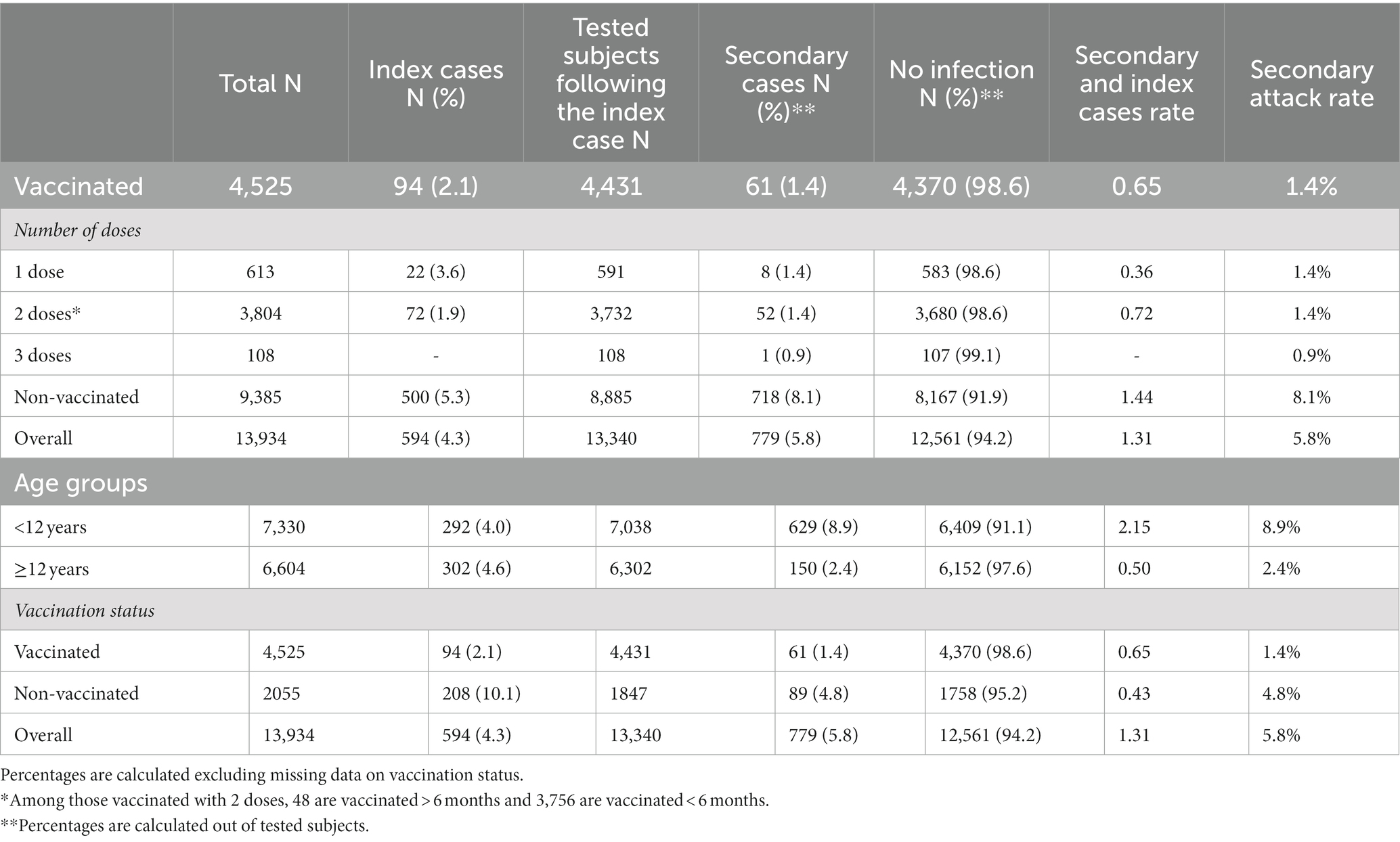
Table 2. Secondary/index cases rate and secondary attack rate within the study population, divided into different subgroups based on vaccination status.
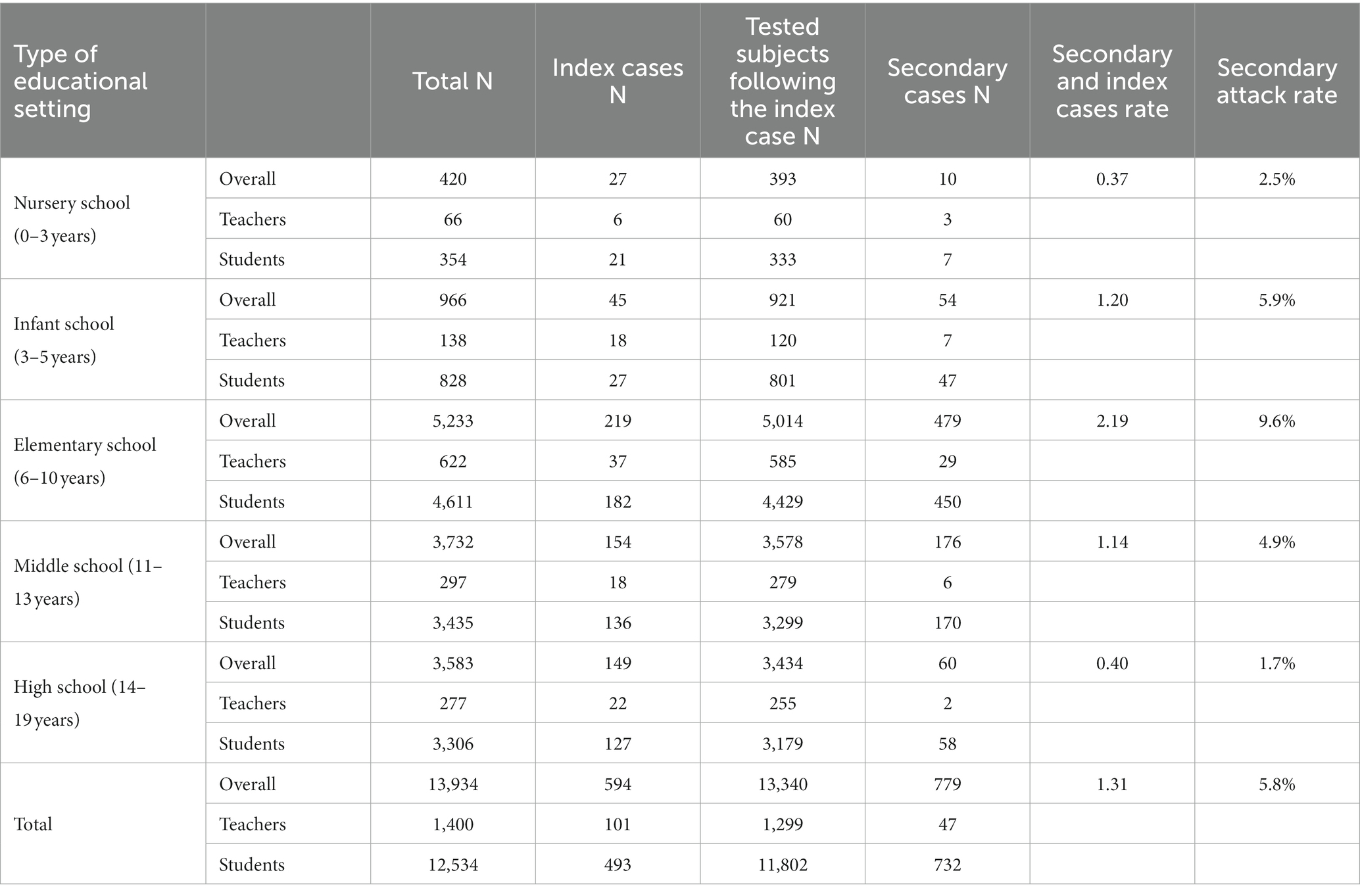
Table 3. Secondary/index cases rate and secondary attack rate within study population, divided into different subgroups based on educational setting.
Overall, the secondary attack rate for non-vaccinated subjects was higher than for vaccinated subjects (8.1% vs. 1.4%). A similar trend was also observed among people aged ≥12 years, who represented the target population for vaccination.
A logistic regression model was implemented to evaluate the vaccination coverage influence on the SARS-CoV-2 spread within schools. The results showed that being vaccinated was highly protective for risk of secondary infection within class following an index case (OR [95% CI]: 0.28 [0.20–0.40]). The analysis stratified by school role confirmed the protective effect of vaccination for students (OR [95% CI]: 0.41 [0.28–0.61]) and for teachers (OR [95% CI]: 0.09 [0.05–0.20]).
Higher secondary attack rates have been reported for subjects attending infant and elementary school (5.9 and 9.6%, respectively), compared to other types of educational settings. Indeed, lower secondary attack rates have been calculated for those who attend middle school and especially high school (4.9 and 1.7%, respectively). A low secondary attack rate (2.5%) was also seen for nursery school.
We also included data regarding the presence of symptoms in confirmed cases identified within our study population. As shown in Table 4, 662 (48.2%) confirmed subjects reported one or more symptoms, whereas 711 (51.8%) claimed to be asymptomatic. Among index cases, 391 (65.8%) subjects were symptomatic and 203 (34.2%) without symptoms. The proportion was inverted among secondary cases, 271 (34.8%) and 508 (65.2%), respectively.
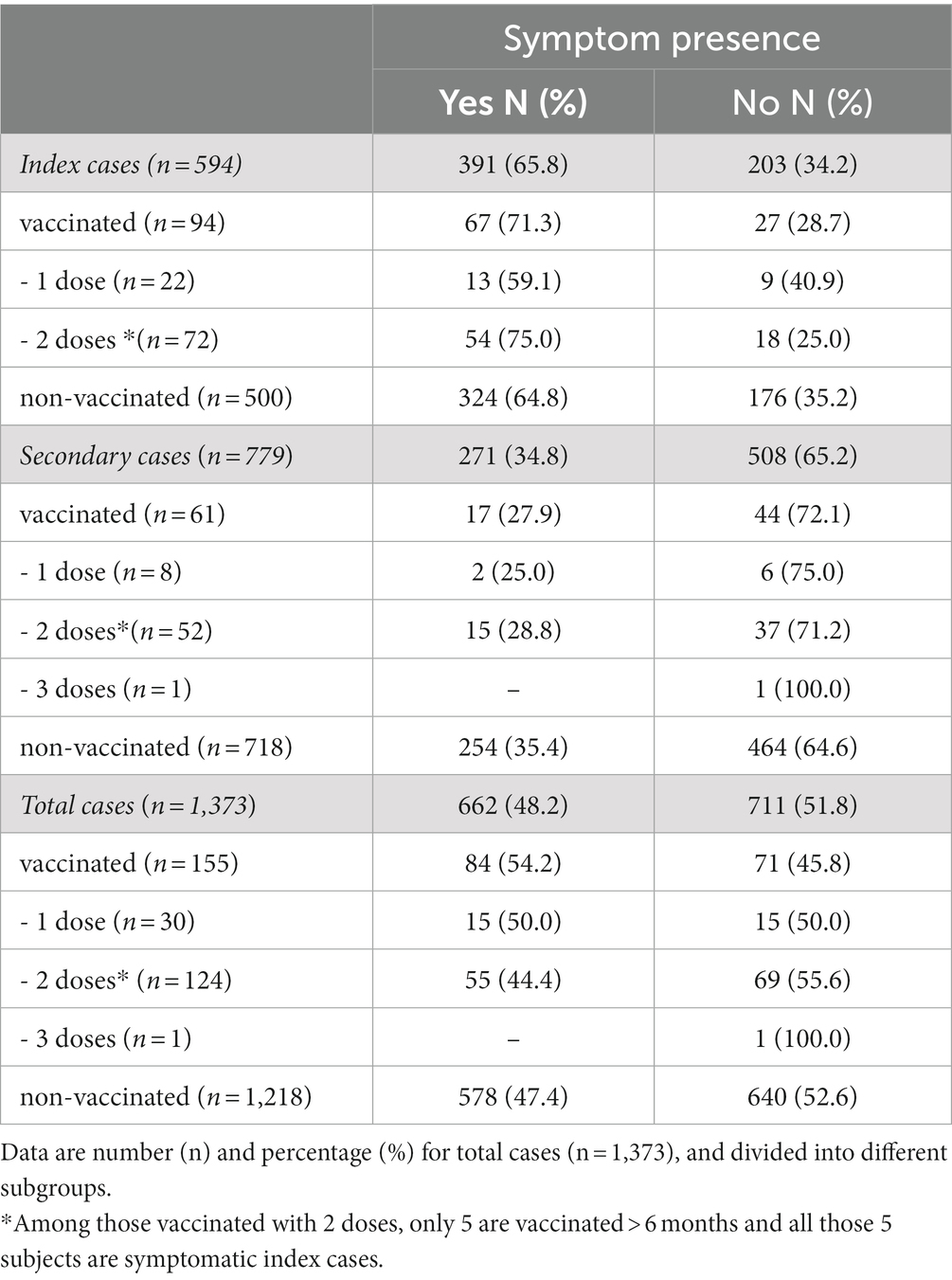
Table 4. Presence of symptoms in confirmed cases identified within study population between September 1 and December 15.
Figure 1 shows the total of daily cases and index cases at school, and confirmed cases in the entire population of the province of Modena. The trends nearly overlapped during our study period.
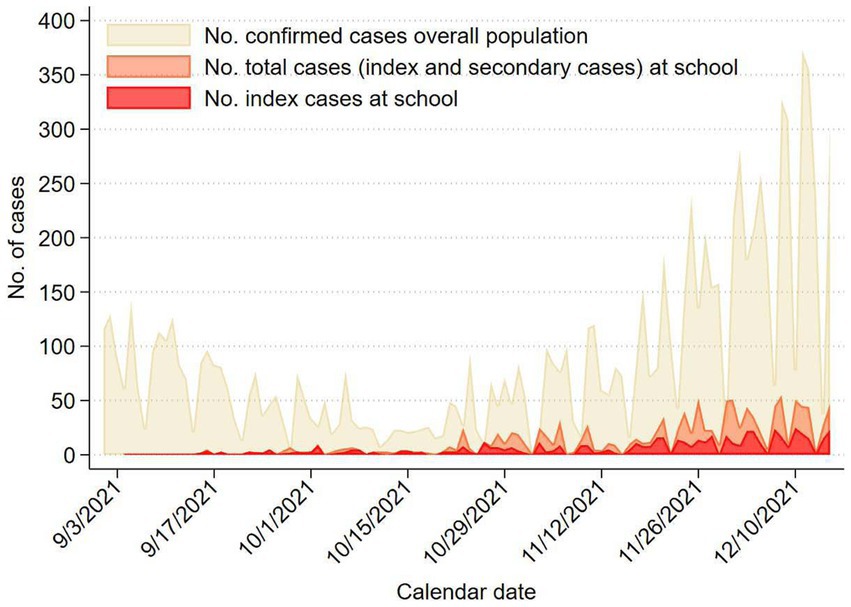
Figure 1. The daily number of confirmed cases in the overall population of Modena province, the number of total cases and of index cases in the scholastic population of Modena province from September 1 to December 15, 2021.
4. Discussion
This study aims to evaluate the spread of SARS-CoV-2 within schools of various types and grades in Modena province, from September to December 2021, further to rate the influence of vaccination in this environment.
The secondary attack rate was found higher in non-vaccinated subjects compared with value in vaccinated subjects (8.1% vs. 1.4%). Furthermore, the lowest secondary attack rate has been found for those who attended high school (1.7%).
Our results underline the effective protection of vaccination against SARS-CoV-2 as 88.7% of overall cases were not vaccinated. Particularly, the percentage of non-vaccinated subjects is 92.2% among secondary cases, which are those infections possibly related with school attendance. Therefore, vaccination shows a relevant impact in preventing transmission of SARS-CoV-2 within educational settings suggesting the collective beneficial effect of extensive vaccination in school population to reduce the outbreaks probability and the size (18). As a matter of that, comparison of secondary attack rates shows higher values for non-vaccinated subjects than vaccinated ones (8.1% vs. 1.4%). These data confirm that non-vaccinated subjects have a higher risk of contracting SARS-CoV-2 infection (33–35). As further demonstration for vaccination efficacy, lower secondary attack rate is reported for subjects with three doses of vaccine compared to those with only one dose (0.9% vs. 1.3%), suggesting that high levels of protection might be re-established through booster doses (36).
Based on different type of educational settings, lowest secondary attack rates were depicted for subjects attending middle school and especially high school (4.9 and 1.7%, respectively) compared to other settings. This difference may be explained by the observation that during the study period vaccination anti-SARS-CoV-2 was approved for people aged ≥12 years only. Our results show that having at least one vaccine dose is protective against transmission of virus, as reported by ECDC (20). In literature, widespread vaccine coverage is confirmed to be very important, especially among adolescents. Indeed, if the vaccine were not available to high school students, they would be expected to be at a higher risk of contracting the infection than primary school students, due to age-specific epidemiological characteristics and contact types (7).
It is interesting that a low secondary attack rate (2.5%) has been found also in nursery school. Possible explanations may be the different measures of isolation and quarantine adopted in that educational settings (32), the only one in which, during the study period, quarantine was disposed for all children of the same classroom, as a consequence of only one confirmed case. Moreover, analyzing transmission of respiratory disease in schoolchildren of different ages, in Japan Matsuda et al. have found a higher percentage of primary schools students with influenza than nursery or kindergarten children (23.4% vs 18.9%) over 5 influenza seasons (37).
It is also important to notice that many mitigation measures and health behavioral policies were adopted during our study period, according to ministerial and regional specific protocols (32): wearing a face mask was always mandatory, except for children aged <6 years and subjects with specific pathologies; periodic room ventilation and social distancing rules had to be guaranteed; the use of outdoor spaces was encouraged wherever possible.
Data regarding the symptoms presence in confirmed cases show a higher percentage of symptomatic individuals among index cases in comparison to secondary cases (65.8% vs. 34.8%). We can explain this difference due to the reason to perform swab testing within these two subgroups. Index cases were usually diagnosed with a positive swab test after the onset of symptoms. Instead, secondary cases underwent swab testing for screening protocol, as established by the Dept. of Public Health regardless of the symptoms presence (32).
According to our results, a comparison between scholastic cases and total cases in the overall population shows similar overlapping trends. This finding suggests that the SARS-CoV-2 transmission within schools was quite similar to the general virus circulation in Modena province over the same period; therefore, school contacts do not seem to have played a relevant role in the spread of the pandemic neither they have represented a higher risk factor for virus transmission, in line with the literature (12). Similarly, other studies revealed low rates of infection in school contacts, and SARS-CoV-2 circulation in schools was found to be much limited compared to the general population (17, 38).
A limitation of our investigations is that we did not have detailed data on symptoms but detailed information was not collected. However, considering the still limited evidence available on this topic, our findings expand the knowledge regarding the SARS-CoV-2 spread within schools and the impact of vaccination coverage in these settings. Some strengths should also be outlined. The epidemiological surveillance carried out by the Local Health Authorities were mandatory during the study period, thus occurrence of selection bias can be ruled out. Furthermore, the epidemiological investigation on the entire involved classes allowed a more in-depth study of transmission in different type of educational settings.
5. Conclusion
Vaccination against SARS-CoV-2 in children aged 12 years and older showed effectiveness in preventing virus transmission in school settings after the detection of an index case within their classroom. Indeed, a higher secondary attack rate was found among non-vaccinated subjects compared with vaccinated subjects. Furthermore, the lowest secondary attack rate has been found for those who attended high school. In conclusion, our findings highlight the importance of widespread anti-SARS-CoV-2 vaccination to reduce virus circulation also in school settings.
Data availability statement
The datasets presented in this article are not readily available due to privacy and legal restrictions. Requests to access the datasets should be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by “Area Vasta Emilia Nord” Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants and participants’ legal guardians/next of kin.
Author contributions
SP, LB, and TF: conceptualization. SP and TF: methodology and funding acquisition. SP, MF, AD’A, and TF: formal analysis. SP, LB, AB, and TF: investigation. LI, AG, EF, GC, ZK, and SZ: resources and recruitment. SP, MF, LB, AD’A, LI, ZK, and SZ: data curation. SP, MF, and TF: writing—original draft preparation. SP, MF, LB, AD’A, LI, AG, EF, GC, ZK, SZ, AB, and TF: writing—review and editing. SP, TF, and AB: project administration. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by grant “UNIMORE FAR (Fondo di Ateneo per la Ricerca) Dipartimentale 2023”.
Acknowledgments
The authors would like to express their gratitude to all the subjects for participating in this study. The content of this manuscript has been presented only in part at the 17th World Congress on Public Health, (Galante et al. The spread of SARS-CoV-2 and vaccination coverage: Results of health surveillance in schools of Modena province, Italy. Population Medicine. 2023;5 (Supplement):A426. doi:10.18332/popmed/164184).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Vinceti, M, Filippini, T, Rothman, KJ, Di Federico, S, and Orsini, N. SARS-CoV-2 infection incidence during the first and second COVID-19 waves in Italy. Environ Res. (2021) 197:111097. doi: 10.1016/j.envres.2021.111097
2. Istituto Superiore di Sanità. Task force COVID-19 del Dipartimento Malattie Infettive e Servizio di Informatica, Istituto Superiore di Sanità. Epidemia COVID-19. Aggiornamento nazionale: 18 gennaio 2023 (2023).
3. Nobari, H, Fashi, M, Eskandari, A, Villafaina, S, Murillo-Garcia, A, and Perez-Gomez, J. Effect of COVID-19 on health-related quality of life in adolescents and children: a systematic review. Int J Environ Res Public Health. (2021) 18:4563. doi: 10.3390/ijerph18094563
4. Ahn, SN. The potential impact of COVID-19 on health-related quality of life in children and adolescents: a systematic review. Int J Environ Res Public Health. (2022) 19:14740. doi: 10.3390/ijerph192214740
5. Saulle, R, De Sario, M, Bena, A, Capra, P, Culasso, M, Davoli, M, et al. School closures and mental health, wellbeing and health behaviours among children and adolescents during the second COVID-19 wave: a systematic review of the literature. Epidemiol Prev. (2022) 46:333–52. doi: 10.19191/EP22.5-6.A542.089
6. Ferrari, E, Palandri, L, Lucaccioni, L, Talucci, G, Passini, E, Trevisani, V, et al. The kids are alright (?). Infants' development and COVID-19 pandemic: a cross-sectional study. Int J Public Health. (2022) 67:1604804. doi: 10.3389/ijph.2022.1604804
7. Goldstein, E, Lipsitch, M, and Cevik, M. On the effect of age on the transmission of SARS-CoV-2 in households, schools, and the community. J Infect Dis. (2021) 223:362–9. doi: 10.1093/infdis/jiaa691
8. Paduano, S, Facchini, MC, Greco, A, Borsari, L, Mingrone, VM, Tancredi, S, et al. Characteristics and risk factors of isolated and quarantined children and adolescents during the first wave of SARS-CoV-2 pandemic: a cross-sectional study in Modena, northern Italy. Acta Biomed. (2021) 92:e2021449. doi: 10.23750/abm.v92iS6.12225
9. Paduano, S, Galante, P, Berselli, N, Ugolotti, L, Modenese, A, Poggi, A, et al. Seroprevalence survey of anti-SARS-CoV-2 antibodies in a population of Emilia-Romagna region, northern Italy. Int J Environ Res Public Health. (2022) 19:7882. doi: 10.3390/ijerph19137882
10. Paduano, S, Marchesi, I, Frezza, G, Turchi, S, and Bargellini, A. COVID-19 in school settings: webinar aimed at both teachers and educators. Ann Ig. (2021) 33:527–32. doi: 10.7416/ai.2021.2437
11. Ford, T, John, A, and Gunnell, D. Mental health of children and young people during pandemic. BMJ. (2021) 372:n614. doi: 10.1136/bmj.n614
12. Gandini, S, Rainisio, M, Iannuzzo, ML, Bellerba, F, Cecconi, F, and Scorrano, L. A cross-sectional and prospective cohort study of the role of schools in the SARS-CoV-2 second wave in Italy. Lancet Reg Health Eur. (2021) 5:100092. doi: 10.1016/j.lanepe.2021.100092
13. Macartney, K, Quinn, HE, Pillsbury, AJ, Koirala, A, Deng, L, Winkler, N, et al. Transmission of SARS-CoV-2 in Australian educational settings: a prospective cohort study. Lancet Child Adolesc Health. (2020) 4:807–16. doi: 10.1016/S2352-4642(20)30251-0
14. Otte Im Kampe, E, Lehfeld, AS, Buda, S, Buchholz, U, and Haas, W. Surveillance of COVID-19 school outbreaks, Germany, March to August 2020. Euro Surveill. (2020) 25:2001645. doi: 10.2807/1560-7917.ES.2020.25.38.2001645
15. Ismail, SA, Saliba, V, Lopez Bernal, J, Ramsay, ME, and Ladhani, SN. SARS-CoV-2 infection and transmission in educational settings: a prospective, cross-sectional analysis of infection clusters and outbreaks in England. Lancet Infect Dis. (2021) 21:344–53. doi: 10.1016/S1473-3099(20)30882-3
16. Djuric, O, Larosa, E, Cassinadri, M, Cilloni, S, Bisaccia, E, Pepe, D, et al. Surveillance, contact tracing and characteristics of SARS-CoV-2 transmission in educational settings in northern Italy, September 2020 to April 2021. PLoS One. (2022) 17:e0275667. doi: 10.1371/journal.pone.0275667
17. Caini, S, Martinoli, C, La Vecchia, C, Raimondi, S, Bellerba, F, D'Ecclesiis, O, et al. SARS-CoV-2 circulation in the school setting: a systematic review and Meta-analysis. Int J Environ Res Public Health. (2022) 19:5384. doi: 10.3390/ijerph19095384
18. Colosi, E, Bassignana, G, Contreras, DA, Poirier, C, Boelle, PY, Cauchemez, S, et al. Screening and vaccination against COVID-19 to minimise school closure: a modelling study. Lancet Infect Dis. (2022) 22:977–89. doi: 10.1016/S1473-3099(22)00138-4
19. Bilinski, A, Ciaranello, A, Fitzpatrick, MC, Giardina, J, Shah, M, Salomon, JA, et al. Estimated transmission outcomes and costs of SARS-CoV-2 diagnostic testing, screening, and surveillance strategies among a simulated population of primary school students. JAMA Pediatr. (2022) 176:679–89. doi: 10.1001/jamapediatrics.2022.1326
20. European Centre for Disease Prevention and Control. COVID-19 vaccine effectiveness in adolescents aged 12–17 years and interim public health considerations for administration of a booster dose. Stockholm: ECDC (2022) 8 February 2022.
21. Esposito, S, Giordano, R, Paini, G, Puntoni, M, Principi, N, and Caminiti, C. Can we get out of the COVID pandemic without adequate vaccination coverage in the pediatric population? Ital J Pediatr. (2022) 48:150. doi: 10.1186/s13052-022-01339-x
22. European Medicines Agency. EMA/653900/2021 - Comirnaty COVID-19 vaccine: EMA recommends approval for children aged 5 to 11. (2021). Available at: https://www.ema.europa.eu/en/news/comirnaty-covid-19-vaccine-ema-recommends-approval-children-aged-5-11.
23. Ministero della Salute. Estensione di indicazione di utilizzo del vaccino Comirnaty (BioNTech/Pfizer) per la fascia di età 5–11 anni. (2021).
24. Presidenza del Consiglio dei Ministri. Estensione della campagna vaccinale anti SARS-CoV-2/COVID-19 alla fascia pediatrica di età 5–11 anni. (2021).
25. Stojanovic, J, Boucher, VG, Gagne, M, Gupta, S, Joyal-Desmarais, K, Paduano, S, et al. Global trends and correlates of COVID-19 vaccination hesitancy: findings from the iCARE study. Vaccines (Basel). (2021) 9:661. doi: 10.3390/vaccines9060661
26. Khan, YH, Rasheed, M, Mallhi, TH, Salman, M, Alzarea, AI, Alanazi, AS, et al. Barriers and facilitators of childhood COVID-19 vaccination among parents: a systematic review. Front Pediatr. (2022) 10:950406. doi: 10.3389/fped.2022.950406
27. Vallis, M, Bacon, S, Corace, K, Joyal-Desmarais, K, Sheinfeld Gorin, S, Paduano, S, et al. Ending the pandemic: how behavioural science can help optimize global COVID-19 vaccine uptake. Vaccines (Basel). (2021) 10:7. doi: 10.3390/vaccines10010007
28. Giardina, J, Bilinski, A, Fitzpatrick, MC, Kendall, EA, Linas, BP, Salomon, J, et al. Model-estimated association between simulated US elementary school-related SARS-CoV-2 transmission, mitigation interventions, and vaccine coverage across local incidence levels. JAMA Netw Open. (2022) 5:e2147827. doi: 10.1001/jamanetworkopen.2021.47827
29. Head, JR, Andrejko, KL, and Remais, JV. Model-based assessment of SARS-CoV-2 Delta variant transmission dynamics within partially vaccinated K-12 school populations. Lancet Reg Health Am. (2022) 5:100133. doi: 10.1016/j.lana.2021.100133
30. Badal, S, Thapa Bajgain, K, Badal, S, Thapa, R, Bajgain, BB, and Santana, MJ. Prevalence, clinical characteristics, and outcomes of pediatric COVID-19: a systematic review and meta-analysis. J Clin Virol. (2021) 135:104715. doi: 10.1016/j.jcv.2020.104715
31. Qi, K, Zeng, W, Ye, M, Zheng, L, Song, C, Hu, S, et al. Clinical, laboratory, and imaging features of pediatric COVID-19: a systematic review and meta-analysis. Medicine (Baltimore). (2021) 100:e25230. doi: 10.1097/MD.0000000000025230
32. Direzione Generale Cura della Persona Salute e Welfare Regione Emilia Romagna. Indicazioni operative per la riapertura dei servizi educativi per l’infanzia e delle scuole. Protocollo regionale per la gestione del caso Covid-19 confermato in ambito scolastico, 2021/2022. (2021).
33. Fournier, PE, Houhamdi, L, Colson, P, Cortaredona, S, Delorme, L, Cassagne, C, et al. SARS-CoV-2 vaccination and protection against clinical disease: a retrospective study, Bouches-du-Rhone District, southern France, 2021. Front Microbiol. (2021) 12:796807. doi: 10.3389/fmicb.2021.796807
34. Haas, EJ, Angulo, FJ, McLaughlin, JM, Anis, E, Singer, SR, Khan, F, et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: an observational study using national surveillance data. Lancet. (2021) 397:1819–29. doi: 10.1016/S0140-6736(21)00947-8
35. Liu, Q, Qin, C, Liu, M, and Liu, J. Effectiveness and safety of SARS-CoV-2 vaccine in real-world studies: a systematic review and meta-analysis. Infect Dis Poverty. (2021) 10:132. doi: 10.1186/s40249-021-00915-3
36. Tartof, SY, Slezak, JM, Fischer, H, Hong, V, Ackerson, BK, Ranasinghe, ON, et al. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: a retrospective cohort study. Lancet. (2021) 398:1407–16. doi: 10.1016/S0140-6736(21)02183-8
37. Matsuda, A, Asayama, K, Obara, T, Yagi, N, and Ohkubo, T. Epidemiological survey to establish thresholds for influenza among children in satellite cities of Tokyo, Japan, 2014-2018. Western Pac Surveill Response J. (2022) 13:9–17. doi: 10.5365/wpsar.2022.13.3.911
38. Young, BC, Eyre, DW, Kendrick, S, White, C, Smith, S, Beveridge, G, et al. Daily testing for contacts of individuals with SARS-CoV-2 infection and attendance and SARS-CoV-2 transmission in English secondary schools and colleges: an open-label, cluster-randomised trial. Lancet. (2021) 398:1217–29. doi: 10.1016/S0140-6736(21)01908-5
Keywords: SARS-CoV-2, vaccination, schools, infection spread, health surveillance
Citation: Paduano S, Facchini MC, Borsari L, D’Alterio A, Iacuzio L, Greco A, Fioretti E, Creola G, Kahfian Z, Zona S, Bargellini A and Filippini T (2023) Health surveillance for SARS-CoV-2: infection spread and vaccination coverage in the schools of Modena province, Italy. Front. Public Health. 11:1240315. doi: 10.3389/fpubh.2023.1240315
Edited by:
Severino Jefferson Ribeiro da Silva, University of Toronto, CanadaReviewed by:
Ralitsa Raycheva, Plovdiv Medical University, BulgariaDusan Radivoje Mitic, University of Belgrade, Serbia
Copyright © 2023 Paduano, Facchini, Borsari, D’Alterio, Iacuzio, Greco, Fioretti, Creola, Kahfian, Zona, Bargellini and Filippini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stefania Paduano, c3RlZmFuaWEucGFkdWFub0B1bmltb3JlLml0