
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 06 October 2023
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1236527
This article is part of the Research Topic On the Cusp of the Silent Wave of the Long COVID Pandemic: Why, what and how should we tackle this emerging syndrome in the clinic and population? View all 12 articles
 Ignacio Pérez Catalán1*†
Ignacio Pérez Catalán1*† Celia Roig Martí1*†Sergio Fabra Juana1Elena Domínguez Bajo1Germán Herrero Rodríguez1Ana Segura Fábrega1María Varea Villanueva1Sofía Folgado Escudero1María José Esteve Gimeno1Daniela Palomo de la Sota2Alejandro Cardenal Álvarez3María Lidón Mateu Campos4Jorge Usó Blasco1‡
Celia Roig Martí1*†Sergio Fabra Juana1Elena Domínguez Bajo1Germán Herrero Rodríguez1Ana Segura Fábrega1María Varea Villanueva1Sofía Folgado Escudero1María José Esteve Gimeno1Daniela Palomo de la Sota2Alejandro Cardenal Álvarez3María Lidón Mateu Campos4Jorge Usó Blasco1‡ José Manuel Ramos Rincón5,6‡
José Manuel Ramos Rincón5,6‡Introduction: The long-term effects of SARS-CoV-2 are unclear, as are the factors influencing the evolution. Objective: to assess health-related quality of life 1 year after a hospital admission due to COVID-19 and to identify factors that may influence it.
Materials and methods: Retrospective observational study in a tertiary hospital from March 2021 to February 2022. Inclusion criteria: ≥18 years old and admitted for SARS-CoV-2 infection. Exclusion criteria: death, not located, refusal to participate, cognitive impairment, and language barrier. Variables: demographic data, medical history, clinical and analytical outcomes during hospital admission, treatment received, and vaccination against SARS-CoV-2 following admission. Participants were interviewed by phone 1 year after admission, using the SF-36 quality of life questionnaire.
Results: There were 486 included patients. The domains yielding the lowest scores were general health (median 65%, interquartile range [IQR] 45–80), vitality (median 65%, IQR 45–80), and mental health (median 73.5%, IQR 60–100). Multivariable analysis showed that female sex and fibromyalgia/fatigue had a negative influence on all domains. Obesity was associated with worse outcomes in physical functioning, physical role, bodily pain, and vitality. Other factors associated with worse scores were an older age in physical functioning and high age-adjusted Charslon comorbidity in physical functioning and general health. Age was associated with better results in emotional role and High C-reactive protein at admission on vitality.
Conclusion: One year after admission for COVID-19, quality of life remains affected, especially the domains of general health, vitality, and mental health. Factors associated with worse outcomes are female sex, fibromyalgia/chronic fatigue, and obesity.
To date, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has caused 676,609,955 confirmed cases and at least 6,881,955 deaths worldwide (1). The pathophysiology and clinical forms of the disease during its acute phase are already well known (2), but its long-term evolution is more uncertain, and the factors determining it, even more so. Long COVID, defined by the World Health Organization (WHO) in October 2021 as the presence of symptoms 3 months after SARS-CoV-2 infection, with a minimum duration of 2 months, which cannot be explained by an alternative diagnosis (3), now represents a significant challenge for health systems given its high prevalence, its great impact on quality of life, and the dearth of knowledge regarding its etiopathogenesis, predisposing factors, and even treatment. In addition, long COVID, also known as post-COVID condition or post-acute sequelae of COVID-19, can affect any organ system, including the central and peripheral nervous system and the cardiovascular, respiratory, or digestive systems, among others (4–7).
A recent meta-analysis in 1.2 million patients who had had a symptomatic SARS-CoV-2 infection showed that around 6.2% of them had symptoms associated with long COVID 3 months after infection (8). The mean duration of these symptoms was 9 months in those who required hospital admission and 4 months in those who did not (8). Although fatigue syndromes after infection have been previously described with other microorganisms, such as Epstein–Barr virus and cytomegalovirus, their pathogenesis is still unknown, and treatment is only symptomatic (9). However, as is the case after these infections, the long COVID syndrome may be very similar and even difficult to differentiate from myalgia encephalomyelitis/chronic fatigue syndrome (ME/CFS).
Thus, this study aims to assess health-related quality of life 1 year after a hospital admission due to SARS-CoV-2 infection and to identify factors that may influence it.
This retrospective observational study was performed in the city of Castellón (Spain), in a tertiary hospital with a catchment population of 283,000 inhabitants, from March 2021 to February 2022. Eligible patients were adults (≥ 18 years) admitted to the infectious diseases unit due to SARS-CoV-2 infection from March 2020 to February 2022, confirmed by real-time polymerase chain reaction (RT-PCR) or antigen test. Exclusion criteria were: died during the first admission or during follow-up (n = 137), could not be located at the time of the interview (n = 139), refused to participate (n = 9), presented prior to infection notable cognitive impairment at the time of the interview (n = 46), or had a language barrier (n = 3; Figure 1).
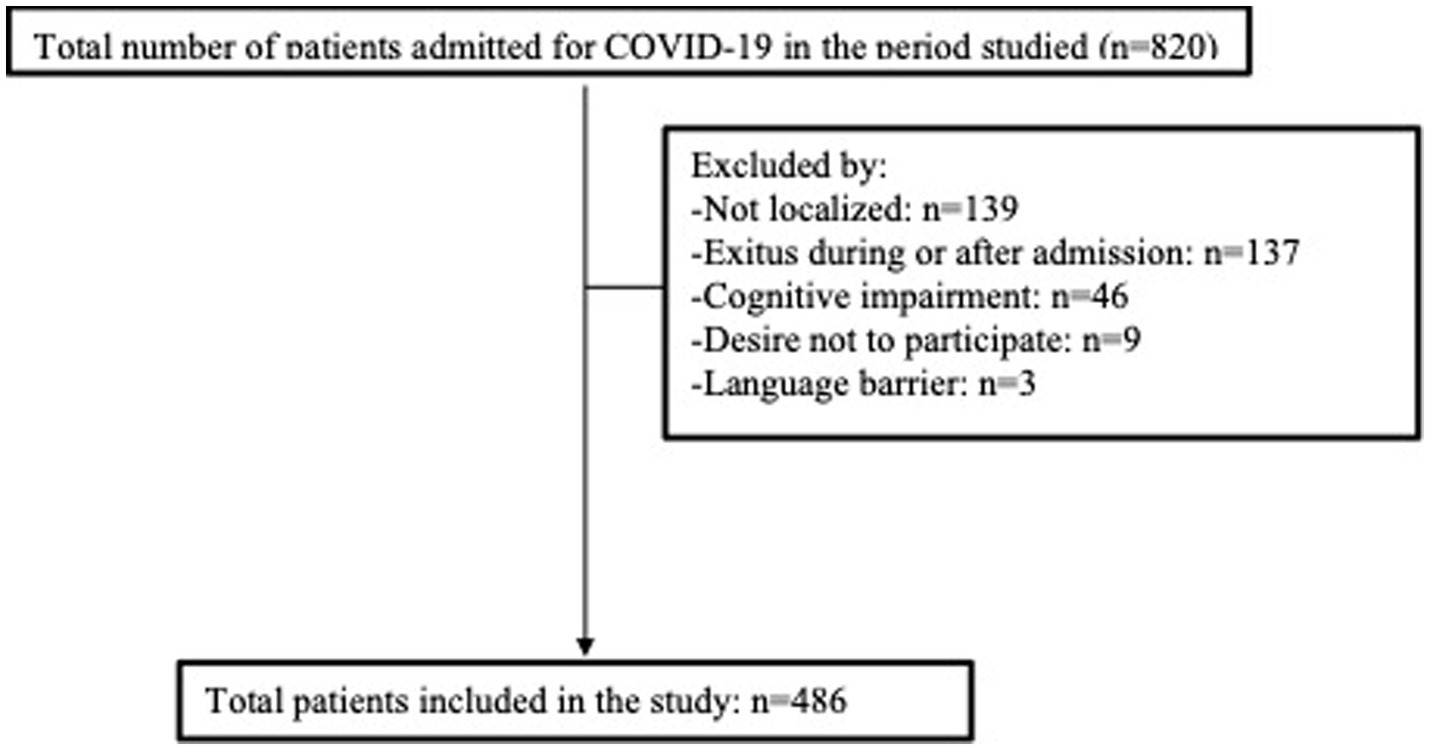
Figure 1. Flowchart.
Participants’ electronic medical records (EMRs) were reviewed using Orion Clinic software (Council for Universal Health Care and Public Health, Valencian Community, Spain). Data collected included demographic variables (age, sex), medical history [comorbidities including obesity, defined as body mass index ≥30 kg/m2, and age-adjusted Charlson comorbidity index (with higher scores indicating more comorbidity)], clinical outcomes [length of hospital stay, evolution to acute respiratory distress syndrome (ARDS), need for admission to the intensive care unit (ICU), type of respiratory support required, need for FiO2 (fraction of inspired oxygen), and Pa/FiO2 ratio on admission and extreme values during the hospital stay], laboratory test results [lymphocyte values, C-reactive protein (CRP), ferritin, and IL-6 and D-dimer at admission and extremes during the hospital stay], treatment (systemic corticosteroid therapy during admission and total days of corticosteroid therapy), vaccination against SARS-CoV-2 following the hospital admission (yes/no).
Following recruitment and provision of informed consent, the 36-item Short Form Survey (SF-36) on health-related quality of life questionnaire was administered by telephone by the investigators (all internal medicine specialists) 1 year after hospital discharge. The SF-36 evaluates eight domains, including physical functioning, physical role limitations, bodily pain, general health perceptions, energy/vitality, social functioning, emotional role limitations, and mental health (10). For each domain, a percentage value is generated, with higher scores indicating better quality of life in that domain.
Outcome variables were the score in the eight domains of the SF-36.
Statistical analysis was performed using SPSS software (version 23, IBM). First, a descriptive study was performed: quantitative variables were described as means (standard deviation, SD) or medians (interquartile range, IQR), depending on the normality of their distribution, and qualitative variables were described as absolute or relative frequencies. To test the association between the outcomes and the quantitative explanatory variables, the Pearson or Spearman correlation tests were performed, as appropriate. To compare the scores in each domain of the SF-36 test between the two groups of qualitative variables, the Mann–Whitney U test was used. The Bonferroni test was used to correct for multiple comparisons, so that taking into account a p = 0.05 and the fact that 42 variables were studied in the univariate study, only p < 0.0012 were considered statistically significant. Subsequently, a multivariable analysis was performed using multiple linear regression. The model included the variables that had shown a significant association with the outcome in the univariable analysis, plus sex and age.
A total of 486 patients were included (Figure 1). Their mean age was 61 years (SD 14), and 194 were women (39.9%). The review of the medical history showed that 111 (22.8%) were smokers or ex-smokers, 205 (44.2%) hypertensive, and 153 (31.5%) obese. The median age-adjusted Charlson comorbidity index was 2 (IQR 1–3). Median length of hospital stay was 10 days (IQR 6–15), and 100 patients (20.6%) required ICU admission, with a median stay in the unit of 6 days (IQR 4–10). ARDS was diagnosed in 193 patients (39.7%), and 93 (19.1%) required non-invasive—and 17 (3.5%) invasive—mechanical ventilation. Systemic corticosteroid therapy was administered to 432 (88.9%) patients during admission, with a median duration of 36 days (IQR 19–49). Of the total sample, 398 participants (81.9%) subsequently completed the vaccination regimen recommended at that time against SARS-CoV-2. Table 1 presents the results for FiO2, the Pa/FiO2 ratio, laboratory variables, and other descriptive indicators.
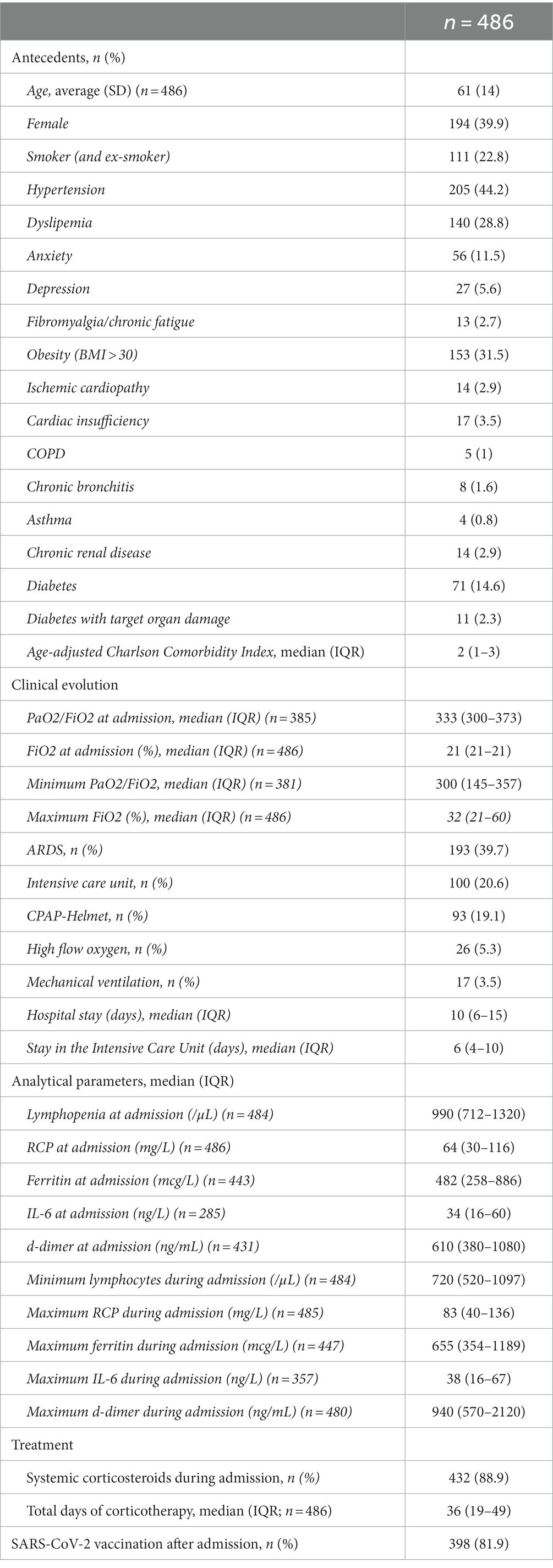
Table 1. Descriptive analysis.
According to each domain of the SF-36, median scores were as follows: physical functioning, 95% (IQR 70–100); physical role limitations, 100% (IQR 75–100); bodily pain, 90% (IQR 66.9–100); general health, 65% (IQR 45–80); vitality, 65% (IQR 45–80); social functioning, 100% (IQR 87.5–100); emotional role limitations, 100% (IQR 100–100); and mental health, 73.5% (IQR 60–100).
The influence of each of the variables studied on the results of each of the eight domains of the SF-36 test was analyzed. In the univariable study, female sex, obesity, and a history of fibromyalgia/chronic fatigue were significantly associated with poorer quality of life in all domains of the SF-36. A history of anxiety and depression also showed a negative influence in most domains. In contrast, the greater inflammatory response, represented especially by high levels of ferritin at and during admission, was significantly associated with better scores in some domains. Systemic treatment with corticosteroids during admission showed some protective effect in terms of body pain, regardless of the duration of treatment, although after correction by the Bonferroni test it did not show statistical significance and also showed no relationship with the rest of the domains. The rest of the results are presented in Tables 2, 3.
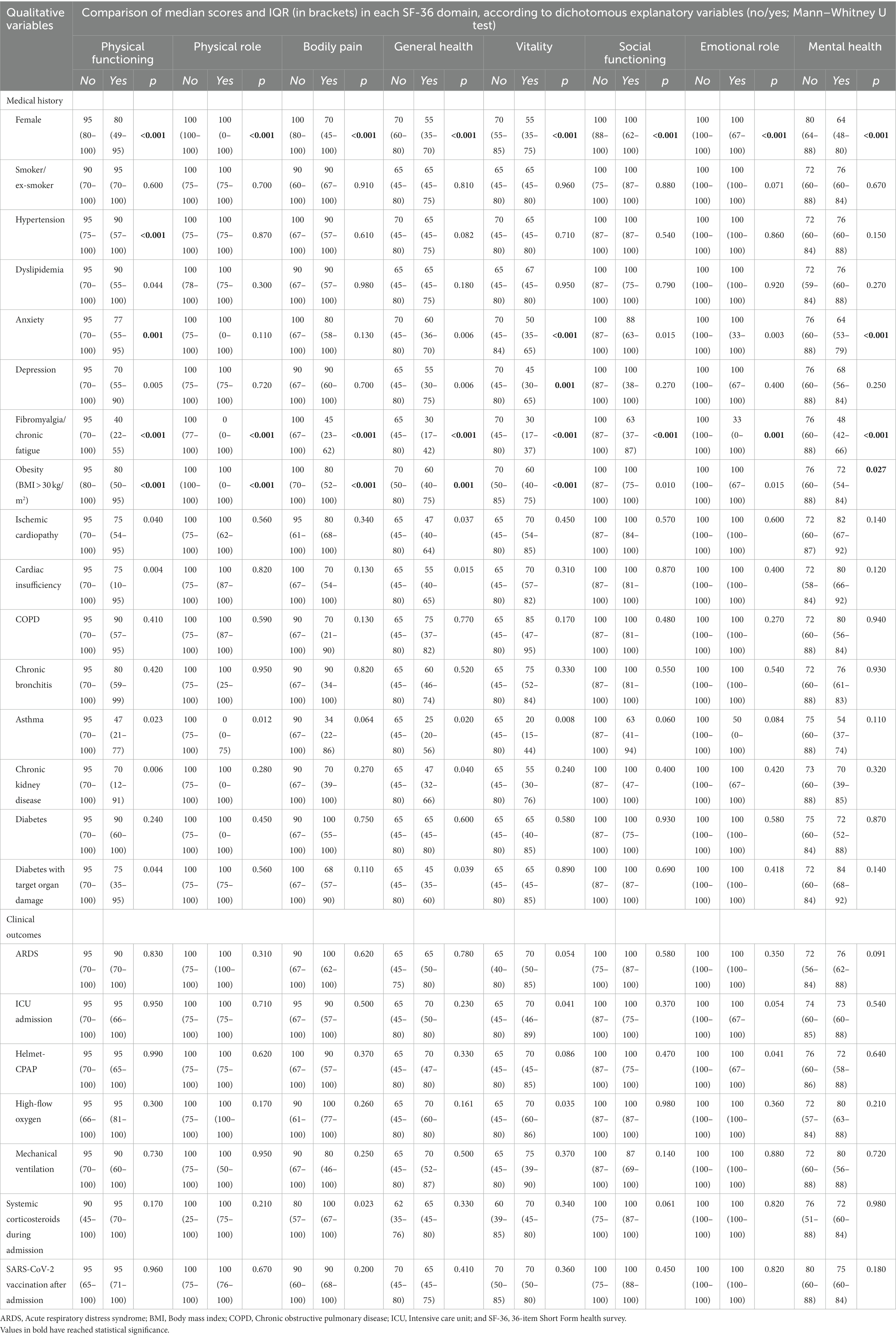
Table 2. Association between qualitative variables and median scores for each SF-36 domain 1 year after hospital admission for COVID-19.
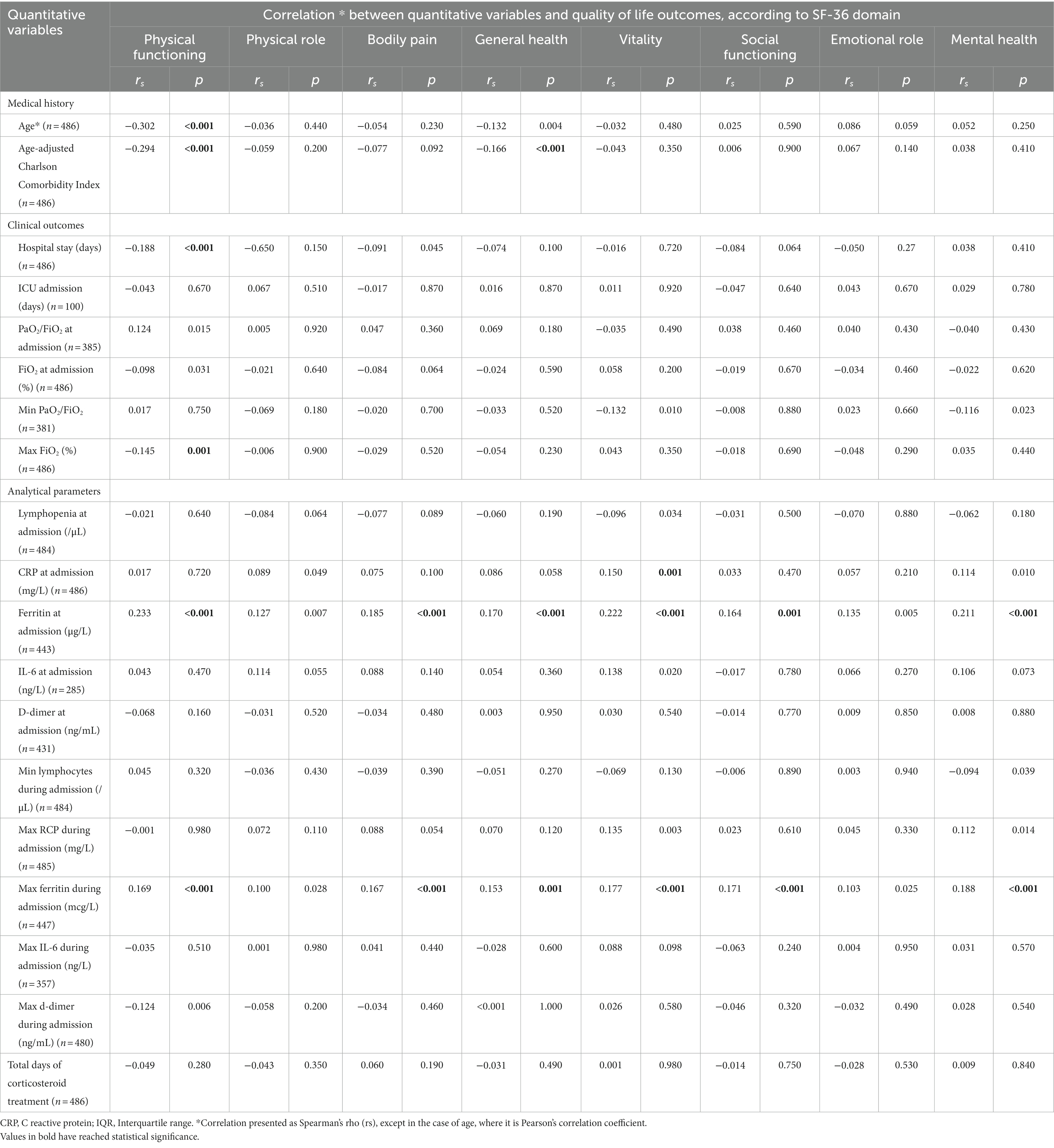
Table 3. Association between quantitative variables and quality of life outcomes, according to the different domains of the SF-36 test 1 year after hospital admission.
The multivariable model included all variables showing a statistically significant association in the univariable study and was adjusted for sex and age (Table 4). Both female sex and history of fibromyalgia/chronic fatigue continued to show a significant and negative association with all domains of the SF-36 test. Obesity had a smaller influence and was related to worse outcomes in physical functioning (p = 0.002), physical role (p < 0.001), bodily pain (p = 0.040) and vitality (p = 0.009). Other factors associated with worse scores on a particular domain of the SF-36 were: an older age in physical functioning (p = 0.047) and high age-adjusted Charslon comorbidity index in physical functioning (p = 0.013) and general health (p = 0.027). In contrast, older age was associated with better results in emotional role (p = 0.041) and a higher RCP value at admission showed better results in vitality (p = 0.031). No other statistically significant associations were observed.
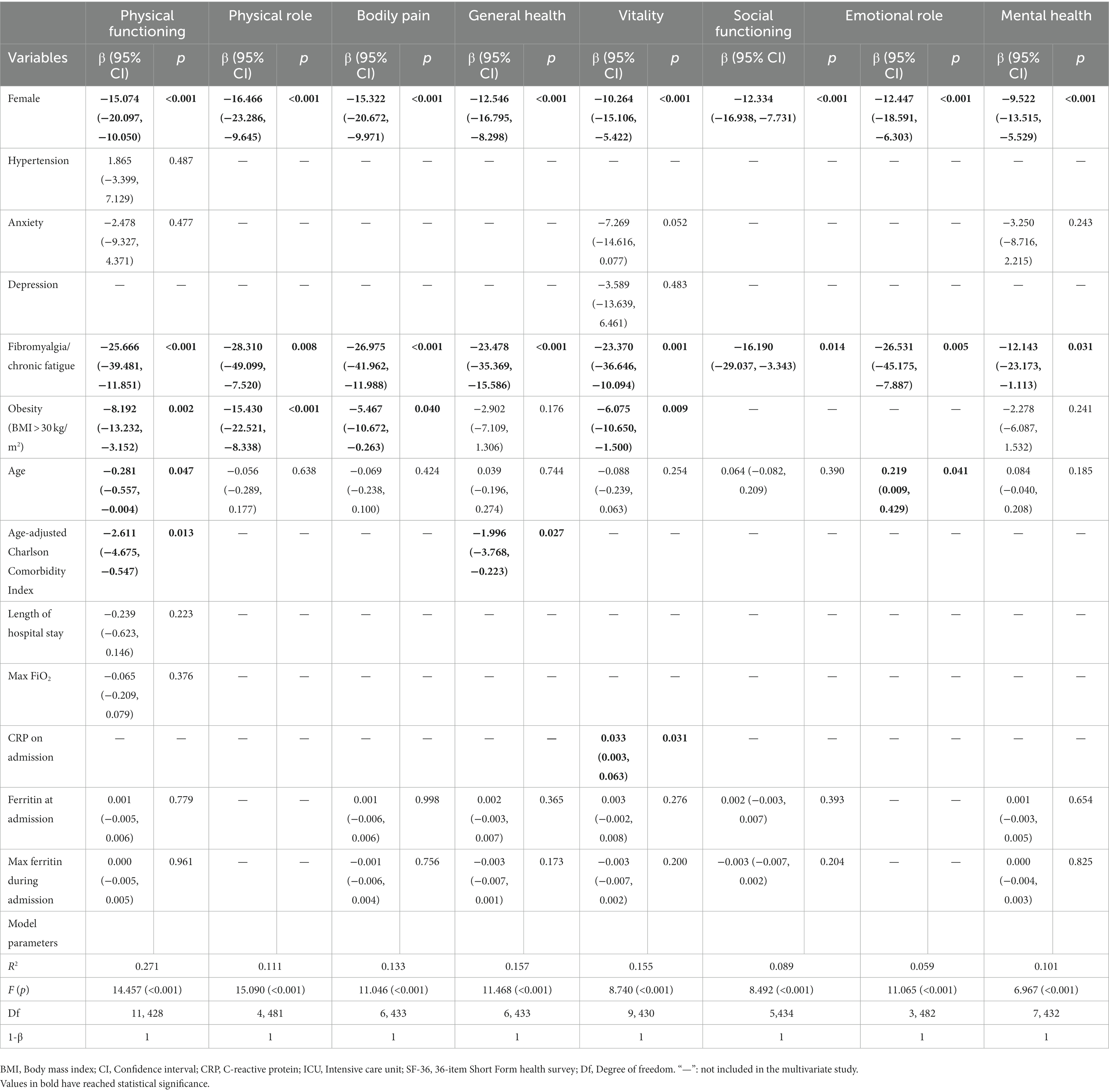
Table 4. Results of the multivariable linear regression analysis of the association between explanatory variables and quality of life domains on the SF-36.
Our cohort of patients is made up of adults in their 60s, mainly men, without particularly high comorbidity. None of them were vaccinated against SARS-CoV-2 at the time of their admission; slightly less than half presented ARDS, and practically all of them were treated with corticosteroids. The worst quality of life outcomes were obtained in the domains of general health, vitality, and mental state, with similar results to those observed by Koullias et al. (11), who administered a simpler version of the SF-36 at 6 months after admission for coronavirus disease 2019 (COVID-19). Our results are also consistent with theirs in terms of the acceptable scores obtained in the domains referring to physical issues. Those authors also observed significantly worse results in patients who had required hospital admission compared to those who had not and to the control group. The analysis of an Italian cohort also found, on this occasion using the EQ-5D-5L quality of life survey by phone call, that at 2 years after the index admission for COVID-19, the score was worse in the mental health domain, but scores were good in the other domains, including those related to physical aspects (12). Another study in our country, Spain, used the SF-36 to assess telematically quality of life in patients admitted to the hospital for COVID-19 during the first wave (as we did), at 3 and 12 months after the onset of infection (13). They compared the results with the reference population values in Spain in 1998, observing a statistically significant decrease in the score in all domains at 3 months (especially for physical role and emotional role), and in all domains except mental health at 12 months (14). Muñoz-Corona et al. (15) also described a much more evident deterioration in the domain of physical role in patients who required hospital admission, although in this case results were probably influenced by the fact that the SF-36 test was carried out 90 days after discharge, much sooner than in the other studies mentioned, including ours.
There was evidence, based on our results and the data already published in this regard, that COVID-19, and in our case hospital admission for this disease, produces a long-term deterioration in quality of life. Moreover, understanding the predisposing factors of this deterioration is very important, since it could enable preventive interventions and help identify the most susceptible groups of patients for more intense medical follow-up. In this sense, we observed that quality of life in practically all domains, is especially compromised for a very specific patient profile: female and with a history of fibromyalgia/chronic fatigue and to a lesser extent obesity. In contrast, the severity of the disease (represented by the degree of respiratory failure, the FiO2 required, the type of respiratory support, and the need for ICU admission) did not appear to have an impact on subsequent quality of life. In addition, in the univariable analysis, a greater inflammatory response showed a protective effect on quality of life 1 year after hospital admission, especially elevated ferritin levels on admission and the maximum levels during the hospital stay. However, this effect did not reach statistical significance in multivariable analysis. After an extensive literature review, we found no data on how elevation of acute phase reactants during acute infection influences long-term clinical course. However, it is likely that potential contributors to Long COVID include multiple organ injury due to excessive inflammation or clotting/coagulation issues in the acute phase (16). In addition, Qu et al. (17) observed that the C-reactive protein value after hospital discharge was not associated with changes in long-term physical or mental status. These results raise the hypothesis that the long COVID would be more influenced by a certain patient profile than by the severity of the acute infection.
Different studies have tried to identify what factors influence long-term quality of life outcomes in COVID-19. Female sex is the most frequently described determinant, in keeping with our findings (11, 12, 17–22). Likewise, obesity has been described as another relevant factor (21). Other long-term determinants mentioned in the literature are advanced age, chronic diseases like diabetes, heart failure, and chronic kidney disease, hospital stay, and the need for ICU admission (17, 20–22). In our sample, only age and age-adjusted Charlson comorbidity index were also associated with worse outcomes, although in the multivariate analysis both only maintained their negative effect on physical functioning and the age-adjusted Charslon comorbidity index also in general health.
Strengths of this study include its analysis of the impact of psychological and psychiatric comorbidities, not just physical ones, on long-term quality of life after admission for COVID-19. We also report laboratory results during the acute phase of infection. We also analyzed the use of corticosteroids, since there are data that suggest a protective effect on the persistence of symptoms after infection, probably due to its anti-inflammatory effect with consequent reduction of organ and tissue damage (23). In practically all of the studies cited, these variables are not analyzed, so our data are of special interest.
On the other hand, the study also presents several limitations, such as its retrospective nature or lack of estimation of size calculation/power calculation. The absence of a control group is also a limitation, as well as the lack of reference or expected values of the SF-36 test for a population similar to ours. In addition, we also do not have the score on the SF-36 test prior to infection. Finally, as included patients were infected in the early stages of the pandemic, the protective effect that vaccination against SARS-Cov-2 could have had prior to infection could not be assessed, although a recent systematic review and meta-analysis provides strong support in that line (24). The same occurs with antiviral drugs against SARS-CoV-2, as these were not contemplated in our center’s therapeutic protocol during the period when participants were admitted. At that time, the therapeutic protocol for COVID-19 pneumonia in our hospital only contemplated systemic corticotherapy, thromboprophylaxis with low molecular weight heparins and the consideration of empirical antibiotherapy if there was suspicion of bacterial coinfection. Recent data indicate that the use of nirmatrelvir/ritonavir in acute infection would significantly decrease the subsequent incidence of long COVID (25).
Patients who required admission for COVID-19 in 2020 and early 2021 continued to show a diminished quality of life 1 year after hospital discharge, especially in the domains of general health, vitality, and mental health. The main factors that may influence this would be female sex, a history of fibromyalgia/chronic fatigue, and, to a lesser extent, obesity. More data are needed to evaluate the role of the inflammatory response and specifically serum ferritin in it.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving humans were approved by Ethics and Drug Research Committee of the Castellón General University Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because informed consent was given verbally.
IP and CR: conception and design of the study, writing of the manuscript, bibliographic search, data collection, and analysis and interpretation of data. SeF, ED, GH, AS, MV, SoF, ME, DP, and AC: data collection and bibliographic search. MM, JU, and JR: conception and design of the study and writing of the manuscript. All authors contributed to the article and approved the submitted version.
We are grateful to the professionals in the Internal Medicine Service and the Infectious Diseases Unit at the University General Hospital of Castellón for their invaluable cooperation during the performance of the study, without which it would not have been possible. We also express our thanks to Meggan Harris for her assistance in editing and to Eva María Navarrete Muñoz for her assistance in the review of the statistics.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
IQR, Interquartile range; WHO, World Health Organization; ME/CFS, Encephalomyelitis/chronic fatigue syndrome; RT-PCR, Real-time polymerase chain reaction; EMRs, Electronic medical records; ARDS, Acute respiratory distress syndrome; ICU, Intensive unit care; RCP, C-Reactive protein; SF-36, 36-Item Short Form Survey; SD, Standard deviation; BMI, Body mass index; COPD, Chronic obstructive pulmonary disease; CI, Confidence interval; COVID-19, Coronavirus disease 2019.
1. Coronavirus Resource Center (2023). Available at: https://coronavirus.jhu.edu/map.html (Accessed May 22, 2023).
2. Gandhi, RT, Lynch, JB, and Del Rio, C. Mild or moderate Covid-19. N Engl J Med. (2020) 383:1757–66. doi: 10.1056/NEJMcp2009249
3. World Health Organization (2021). A clinical case definition of post COVID-19 condition by a Delphi consensus. Available at: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (Accessed November 24, 2022).
4. Logue, JK, Franko, NM, McCulloch, DJ, McDonald, D, Magedson, A, Wolf, CR, et al. Sequelae in adults at 6 months after COVID-19 infection. JAMA Netw Open. (2021) 4:e210830. doi: 10.1001/jamanetworkopen.2021.0830
5. Sigfrid, L, Drake, TM, Pauley, E, Jesudason, EC, Olliaro, P, Lim, WS, et al. Long Covid in adults discharged from UK hospitals after Covid-19: a prospective, multicentre cohort study using the ISARIC WHO clinical characterisation protocol. Lancet Reg Health Eur. (2021) 8:100186. doi: 10.1016/j.lanepe.2021.100186
6. Huang, C, Huang, L, Wang, Y, Li, X, Ren, L, Gu, X, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. (2021) 397:220–32. doi: 10.1016/S0140-6736(20)32656-8
7. Huang, L, Li, X, Gu, X, Zhang, H, Ren, LL, Guo, L, et al. Health outcomes in people 2 years after surviving hospitalisation with COVID-19: a longitudinal cohort study. Lancet Respir Med. (2022) 10:863–76. doi: 10.1016/S2213-2600(22)00126-6
8. Global Burden of Disease Long COVID Collaborators Wulf Hanson, S, Abbafati, C, Aerts, JG, al-Aly, Z, Ashbaugh, C, et al. Estimated global proportions of individuals with persistent fatigue, cognitive, and respiratory symptom clusters following symptomatic COVID-19 in 2020 and 2021. JAMA. (2022) 328:1604–15. doi: 10.1001/jama.2022.18931
9. Hickie, I, Davenport, T, Wakefield, D, Vollmer-Conna, U, Cameron, B, Vernon, SD, et al. Dubbo infection outcomes study group. Post-infective and chronic fatigue syndromes precipitated by viral and non-viral pathogens: prospective cohort study. BMJ. (2006) 333:575. doi: 10.1136/bmj.38933.585764.AE
10. Ware, JE Jr, and Sherbourne, CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. (1992) 30:473–83. doi: 10.1097/00005650-199206000-00002
11. Koullias, E, Fragkiadakis, G, Papavdi, M, Manousopoulou, G, Karamani, T, Avgoustou, H, et al. Long-term effect on health-related quality of life in patients with COVID-19 requiring hospitalization compared to non-hospitalized COVID-19 patients and healthy controls. Cureus. (2022) 14:e31342. doi: 10.7759/cureus.31342
12. d’Ettorre, G, Vassalini, P, Coppolelli, V, Gentilini Cacciola, E, Sanitinelli, L, Maddaloni, L, et al. Health-related quality of life in survivors of severe COVID-19 infection. Pharmacol Rep. (2022) 74:1286–95. doi: 10.1007/s43440-022-00433-5
13. Rodríguez-Galán, I, Albaladejo-Blázquez, N, Ruiz-Robledillo, N, Pascual-Lledó, JF, Ferrer-Cascales, R, and Gil-Carbonell, J. Impact of COVID-19 on health-related quality of life: a longitudinal study in a Spanish clinical sample. Int J Environ Res Public Health. (2022) 19:10421. doi: 10.3390/ijerph191610421
14. Alonso, J, Regidor, E, Barrio, G, Prieto, L, Rodríguez, C, de la Fuente, L, et al. Valores poblacionales de referencia de la versión española del Cuestionario de Salud SF-36 [population reference values of the Spanish version of the health questionnaire SF-36]. Med Clin (Barc). (1998) 111:410–6.
15. Muñoz-Corona, C, Gutiérrez-Canales, LG, Ortiz-Ledesma, C, Martínez-Navarro, LJ, Macías, AE, Scavo-Montes, DA, et al. Quality of life and persistence of COVID-19 symptoms 90 days after hospital discharge. J Int Med Res. (2022) 50:3000605221110492. doi: 10.1177/03000605221110492
16. Proal, AD, and Van Elzakker, MB. Long COVID or post-acute sequelae of COVID-19 (PASC): an overview of biological factors that may contribute to persistent symptoms. Front Microbiol. (2021) 12:698169. doi: 10.3389/fmicb.2021.698169
17. Qu, G, Zhen, Q, Wang, W, Fan, S, Wu, Q, Zhang, C, et al. Health-related quality of life of COVID-19 patients after discharge: a multicenter follow-up study. J Clin Nurs. (2021) 30:1742–50. doi: 10.1111/jocn.15733
18. Zhang, L, Lei, J, Zhang, J, Yin, L, Chen, Y, Xi, Y, et al. Undiagnosed long COVID-19 in China among non-vaccinated individuals: identifying persistent symptoms and impacts on Patients’ health-related quality of life. J Epidemiol Glob Health. (2022) 12:560–71. doi: 10.1007/s44197-022-00079-9
19. Anastasio, F, Barbuto, S, Scarnecchia, E, Cosma, P, Fugagnoli, A, Rossi, G, et al. Medium-term impact of COVID-19 on pulmonary function, functional capacity and quality of life. Eur Respir J. (2021) 58:2004015. doi: 10.1183/13993003.04015-2020
20. Arab-Zozani, M, Hashemi, F, Safari, H, Yousefi, M, and Ameri, H. Health-related quality of life and its associated factors in COVID-19 patients. Osong Public Health Res Perspect. (2020) 11:296–302. doi: 10.24171/j.phrp.2020.11.5.05
21. Chen, KY, Li, T, Gong, FH, Zhang, JS, and Li, XK. Predictors of health-related quality of life and influencing factors for COVID-19 patients, a follow-up at one month. Front Psychol. (2020) 11:668. doi: 10.3389/fpsyt.2020.00668
22. Todt, BC, Szlejf, C, Duim, E, Linhares, AOM, Kogiso, D, Varela, G, et al. Clinical outcomes and quality of life of COVID-19 survivors: a follow-up of 3 months post hospital discharge. Respir Med. (2021) 184:106453. doi: 10.1016/j.rmed.2021.106453
23. Catalán, IP, Martí, CR, Sota, DP, Álvarez, AC, Gimeno, MJE, Juana, SF, et al. Corticosteroids for COVID-19 symptoms and quality of life at 1 year from admission. J Med Virol. (2022) 94:205–10. doi: 10.1002/jmv.27296
24. Gao, P, Liu, J, and Liu, M. Effect of COVID-19 vaccines on reducing the risk of long COVID in the real world: a systematic review and Meta-analysis. Int J Environ Res Public Health. (2022) 19:12422. doi: 10.3390/ijerph191912422
Keywords: COVID-19, long COVID, post-acute COVID-19 syndrome, quality of life, SARS-COV-2
Citation: Pérez Catalán I, Roig Martí C, Fabra Juana S, Domínguez Bajo E, Herrero Rodríguez G, Segura Fábrega A, Varea Villanueva M, Folgado Escudero S, Esteve Gimeno MJ, Palomo de la Sota D, Cardenal Álvarez A, Mateu Campos ML, Usó Blasco J and Ramos Rincón JM (2023) One-year quality of life among post-hospitalization COVID-19 patients. Front. Public Health. 11:1236527. doi: 10.3389/fpubh.2023.1236527
Edited by:
Nuno Sepulveda, Warsaw University of Technology, PolandReviewed by:
Sławomir Kujawski, Ludwik Rydygier Collegium Medicum in Bydgoszcz Nicolaus Copernicus University in Toruń, PolandCopyright © 2023 Pérez Catalán, Roig Martí, Fabra Juana, Domínguez Bajo, Herrero Rodríguez, Segura Fábrega, Varea Villanueva, Folgado Escudero, Esteve Gimeno, Palomo de la Sota, Cardenal Álvarez, Mateu Campos, Usó Blasco and Ramos Rincón. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Celia Roig Martí, Y2VsaWEucm9pZy5tYXJ0aUBnbWFpbC5jb20=; Ignacio Pérez Catalán, bmFjaG9jczEzQGdtYWlsLmNvbQ==
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.