 Huanting Liu
Huanting Liu Qihui Gan2†
Qihui Gan2† Yuxi Liu
Yuxi Liu Chonghua Wan
Chonghua Wan- 1Key Laboratory for Quality of Life and Psychological Assessment and Intervention, Research Center for Quality of Life and Applied Psychology, School of Humanities and Management, Guangdong Medical University, Dongguan, China
- 2Institute of Health Law and Policy, Guangdong Medical University, Dongguan, China
Introduction: The study explored the relationship between subjective well-being and the quality of life among older adults. It highlights the importance of understanding how these factors are interconnected in the context of an aging population.
Methods: Descriptive statistics were used to analyze the scores of general demographic characteristics, subjective wellbeing and quality of life. Simple correlation analysis and canonical correlation analysis were employed to analyze the relationship between subjective wellbeing and quality of life among older adults.
Results: Data from 892 older adults were collected. Canonical correlation analysis revealed four pairs of canonical variables, with the first four pairs of canonical correlation coefficients all being statistically significant (0.695, 0.179, 0.147, 0.121) (p < 0.05), and the first pair of canonical variables explaining 93.03% of the information content. From the canonical loading coefficients, Vitality and mental health contributed the most to the quality of life (U1) canonical variable. The canonical variable V1, which corresponded to subjective wellbeing, was reflected by a combination of positive affect, negative affect, positive experience and negative experience. X1 (physical functioning), X2 (role-physical), X3 (bodily pain), X4 (general health), X5 (vitality), X6 (social functioning), X7 (role-emotional) and X8 (mental health) were positively correlated with Y1 (positive affect) and Y3 (positive experience), negatively correlated with Y2 (negative affect) and Y4 (negative experience). Cross-loadings revealed that physical functioning, bodily pain, general health, vitality, social functioning and mental health were the main factors reflecting the subjective wellbeing of older adults.
Discussion: As quality of life among older adults was highly correlated with subjective wellbeing, appropriate measures should be taken to account for individual characteristics of older adults, and various factors should be integrated to improve their subjective wellbeing.
1. Introduction
Population aging is a common social phenomenon throughout the contemporary world, including in China, whose population is gradually aging. According to the National Bureau of Statistics of China, by 2020, 13.5% of China’s total population was aged 65 or older. Due to their age, older adults face problems such as declining physiological functions, which in turn lead to a diminished sense of wellbeing. This is problematic, as wellbeing – especially among older adults – is vital for improving quality of life, promoting mental health and coping with the needs of an aging population (1).
The term subjective wellbeing includes affective states, the self- evaluations of quality of life and individual events and circumstances, including residence type (2). Subjective wellbeing was often used to assess overall quality of life (3, 4). Studies have shown that physical health status, mental health problems and subjective wellbeing among older adults were negatively correlated (5). Subjective wellbeing was influenced not only by health but also by lifestyle factors unrelated to health (6). It was also been found that the level of subjective wellbeing was influenced by other factors, such as personality (7), culture (8), interpersonal interaction (9), marital status (10), and economic factors (11). In recent years, there has been a growing recognition of the importance of subjective wellbeing and its various determinants, particularly among the older adult population. As societies continue to age, the wellbeing of older individuals becomes a significant area of concern, demanding a shift in focus toward their holistic experiences. Recent studies have focused on factors affecting subjective wellbeing among older adults, mainly demographic differences (12), rural residency (13), physical exercise (14), social support (15), and environmental conditions (16). There is a growing body of research demonstrating the relationship between social capital and wellbeing, with social capital positively affecting subjective wellbeing. Zhang (17) showed that social capital is a favorable predictor of wellbeing. Furthermore, the connections, trust, and support derived from social relationships, were closely intertwined with the wellbeing of older adults (18). As social dynamics evolve over time, older adults can experience changes in their social networks, potentially affecting their health and wellbeing (19, 20). Liu et al. (21) found that the neighborhood environment had a significant impact on older adults’ subjective wellbeing. Participation in social activities (22) and volunteering (23) also had a positive impact on wellbeing. Recognizing the significance of social capital sheds light on the ways in which communities and institutions can foster an environment that nurtures positive interactions and meaningful relationships among older individuals.
These factors were fundamentally related to quality of life (24). The WHO defined quality of life (25) as the experience of individuals from different cultures and value systems concerning their life goals, expectations, standards, and state of life in relation to the things they cared about. This concept encompasses physical health, mental health, independence, social relationships, personal beliefs and interactions with the surrounding environment. It has been demonstrated that quality of life among older adults is both positively and negatively associated with the construction of subjective wellbeing (26). In one investigation, quality of life was measured by the SF-36 Quality of Life Self-Measurement Scale, revealing a positive correlation between wellbeing and quality of life (27). Similarly, in a study of quality of life among adults with paraplegia, it was concluded that quality of life was significantly associated with subjective wellbeing (28).
Many studies have explored factors that influence subjective wellbeing, especially among older adults, such as physical health, mental health, living environment and social phenomena. Meanwhile, studies of overall quality of life have been conducted primarily on patients, such as cancer patients (29), particularly breast cancer patients (30), and adult paraplegics (28), but less so on older adults. Thus, the present study investigated subjective wellbeing and quality of life among older adults, particularly the correlation between them. More specifically, the study explored the influence of quality of life on subjective wellbeing among older adults and thereby provides a reference base for future research aimed at enhancing subjective wellbeing among older adults.
2. Methods
2.1. Design
This study used a cross-sectional questionnaire to examine the relationship between subjective wellbeing and the quality of life of older adults in the community in Dongguan City. Participants were required to undergo a face-to-face interview with an investigator lasting 20–25 min, during which the trained investigator and participants conversed in the local language. All participants were informed of the study’s purpose beforehand and were assured that their information and responses would remain confidential and anonymous. Participants also signed a written informed consent form.
2.2. Subjects
The research was conducted among older adult residents of Dongguan City from December 2018 to February 2019. In this study, ‘older adult’ was defined as individuals no younger than 60 years old and living in the community. An eligible list of older adults for the study was provided by the community committee. A multistage cluster sampling survey technique was used, and 892 older adults were invited to take part in the study (98.4% response rate). In the first stage, four districts were purposively selected out of 33 districts. In the second stage, 22 clusters were randomly selected from 26 communities with a probability proportional to older adults’ density. In the third stage, older adults were selected randomly within each cluster.
2.3. Measures
Subjective wellbeing was assessed using the Memorial University of Newfoundland Well-Being Scale (MUNSH) (31), which was widely used in geriatric research to measure the quality of life and health status of older adults. The scale consists of 24 items across four dimensions: five items in positive affect (PA), five items in negative affect (NA), seven items in positive experience (PE), and seven items in negative experience (NE). The scoring method was as follows: 2 points for ‘yes,’ 1 point for ‘do not know,’ and 0 points for ‘no,’ resulting in a total score range of −24 to 24. The scale was employed to assess the subjective wellbeing of Chinese older adults (32, 33). The Cronbach’s α coefficients of the four sub-dimensions of the MUNSH scale in the present study were 0.717, 0.739, 0.693, and 0.713, respectively, with a KMO coefficient of 0.907, indicating good reliability.
Quality of life was measured using the SF-36 Quality of Life Self-Measurement Scale (34), which consists of eight dimensions: 10 items for physical functioning (PF), four items for role-physical (RP), two items for bodily pain (BP), five items for general health (GH), four items for vitality (VT), two items for social functioning (SF), three items for role-emotional (RE), five items for mental health (MH), and one item to evaluate health status in the past year. The total number of entries was 36. Additionally, physical functioning, role-physical, bodily pain and general health were categorized as components of physical health (PCS), while role-physical, social functioning, mental health and vitality were categorized as components of mental health (MCS) – with higher scores indicating better quality of life. The Chinese version of the SF-36 is a valid and reliable tool for assessing health-related quality of life (HRQOL) within the Chinese population (35).
An original general demographic questionnaire was developed to collect data about the participants’ demographic characteristics, health status and social circumstances.
2.4. Statistical analysis
The data were organized using SPSS 26.0 software, after which a simple correlation analysis and canonical correlation analysis were performed.
Canonical correlation analysis (36) is a multivariate statistical method used to examine the correlation between two sets of variables. It involves extracting two representative integrated random variables from two groups of variables through dimensionality reduction, and these two variables are referred to as a pair of canonical variables. The correlation observed between the canonical variables is used to reflect the correlation between the original two groups of variables. The first set of variables was denoted as , while the second set was denoted as . Canonical correlation analysis extracted canonical components U from the first set of variables X via principal component analysis (U was a linear combination of ). The canonical components V were then extracted from the second set of variables Y (V was a linear combination of ) while maximizing the correlation between U and V. This U–V correlation reflected the correlation between the two sets of variables X and Y (37, 38). Canonical loadings analysis generated correlations between the original and canonical variables. Empirically, variables with an absolute value of 0.3 or greater in the canonical loadings were considered to meaningfully explain the canonical variables of interest (39). In this study, we selected important loadings using a cutoff value of 0.35.
Canonical redundancy (40) reflects the ability of each canonical variable to explain all variables in the variable group and can be divided into first and second canonical redundancy depending on the direction of action. First canonical redundancy indicates the percentage of canonical variables explained by their own variable group, whereas second canonical redundancy indicates the percentage of canonical variables explained by another variable group, numerically equal to the product of the first canonical redundancy and the square of the canonical correlation coefficient. The square of the canonical correlation coefficient indicates the percentage of common variation between the two groups of canonical variables.
The scores on the four dimensions – positive affect, negative affect, positive experience and negative experience (Y1 ~ Y4) – of the MUNSH were utilized as canonical variables U, while the eight dimensions – physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health (X1 ~ X8) – of the SF-36 scale were employed as canonical variables V. Canonical correlation analysis was performed between the U variables and the V variables, and a significance level of α = 0.05 was applied.
2.5. Ethical considerations
Ethical approval was received from the Institutional Ethics Committee of Guangdong Medical University, China (REC: PJ2018037) before the research was conducted. Privacy and data confidentiality were ensured. All participants were fully informed that their participation was entirely voluntary and that they could unconditionally withdraw from the study at any time. A small gift was given to each participant as a token of gratitude for their participation.
3. Results
3.1. Descriptive material
A total of 892 older adults, aged between 60 to 99 years old, with an average age of 68.592 ± 7.063, participated in the survey. Among the participants, 353 were male and 539 were female, with the majority being married (79.596%). The participants’ education level were distributed as follows: 602 had elementary school education or lower, 174 had middle school education, 96 had high school education, and 20 had college education or higher, as shown in Table 1.
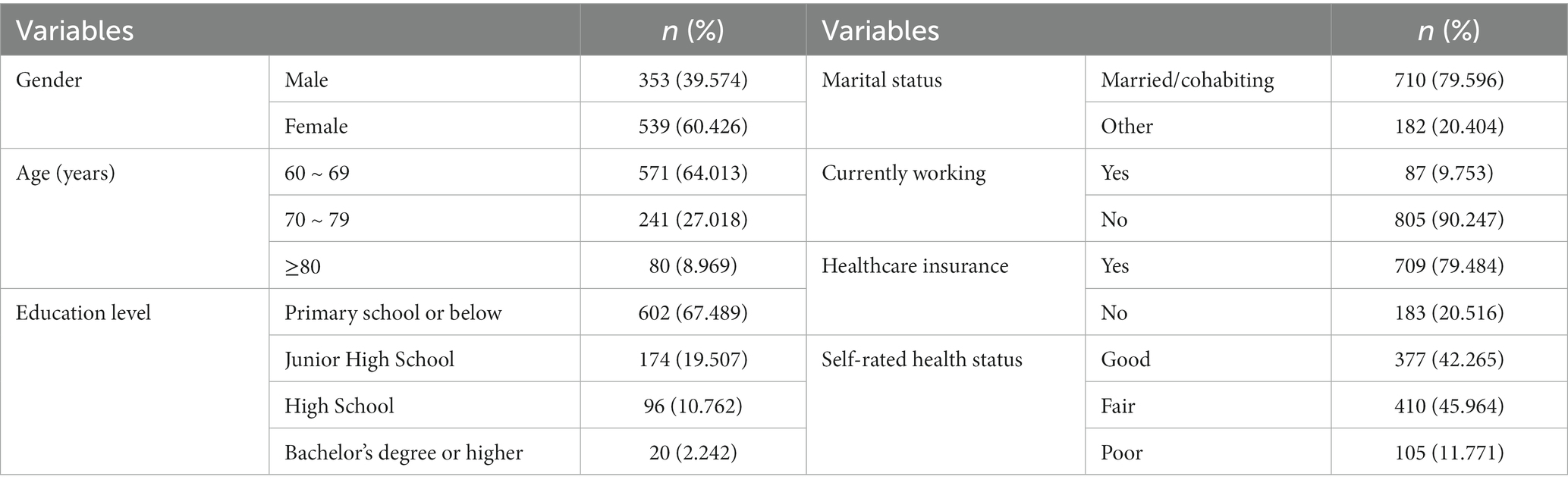
Table 1. Results of the analysis of the socio-demographic characteristics of the sample, n = 892.
3.2. Subjective wellbeing and quality of life scores of older adults
The total score of subjective wellbeing among older adults participants was 13.820 ± 8.975, with the following sub-scores: positive affect (7.418 ± 2.600), negative affect (1.776 ± 2.504), positive experience (10.264 ± 3.333) and negative experience (2.087 ± 2.783). The quality of life scores of the participants were as follows: physical functioning (82.786 ± 18.982), role-physical (71.553 ± 40.324), bodily pain (80.410 ± 19.653), general health (64.209 ± 19.845), vitality (75.471 ± 16.313), social functioning (83.981 ± 18.05), role-emotional (74.439 ± 37.264), and mental health (76.054 ± 15.303) (Table 2).
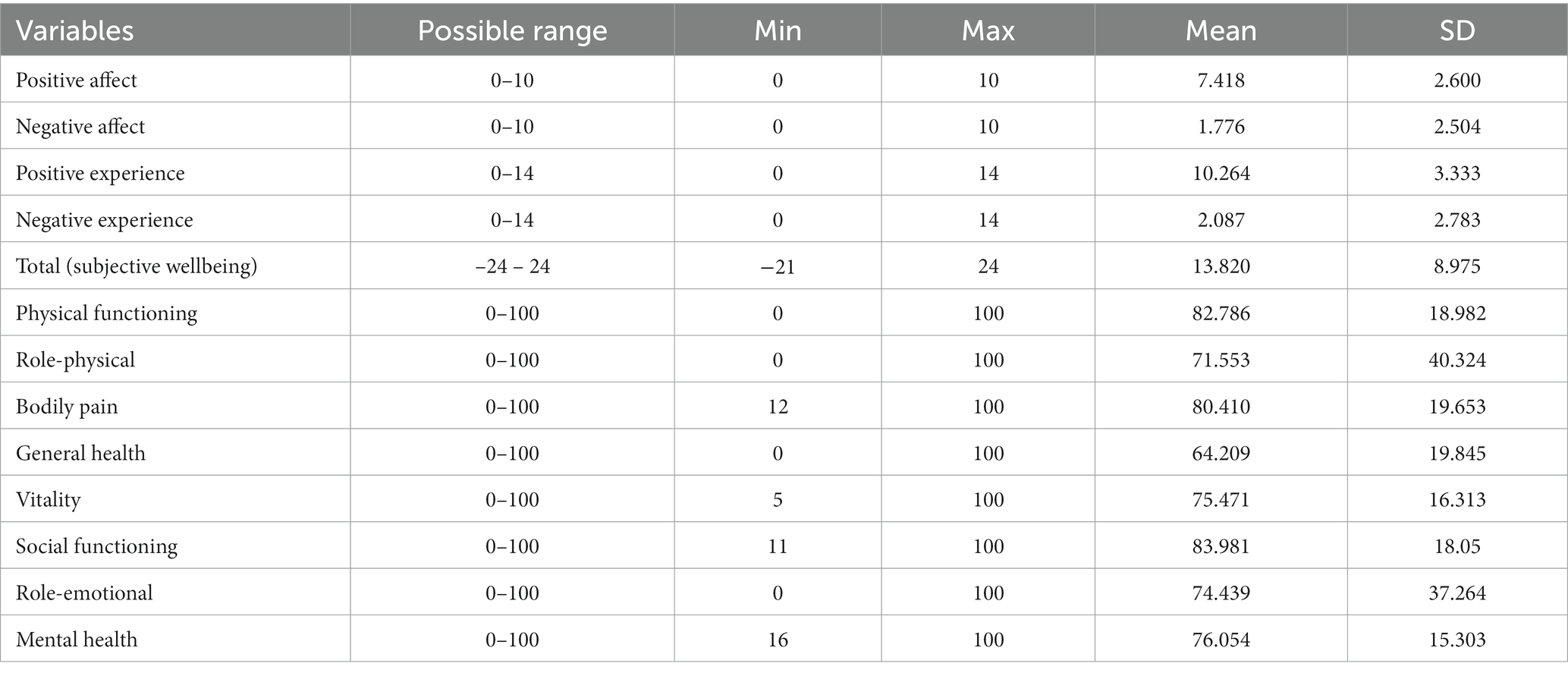
Table 2. Scores of subjective wellbeing and quality of life dimensions among older adults, n = 892.
3.3. Simple correlation analysis
Pearson’s simple correlation analysis was performed on the dimensions of both quality of life and subjective wellbeing. The results showed that the positive affect, positive experience and total subjective wellbeing scores were significantly and positively correlated with each of the quality of life dimensions, whereas negative affect and negative experience were significantly and negatively correlated with each of the quality of life dimensions (Table 3).
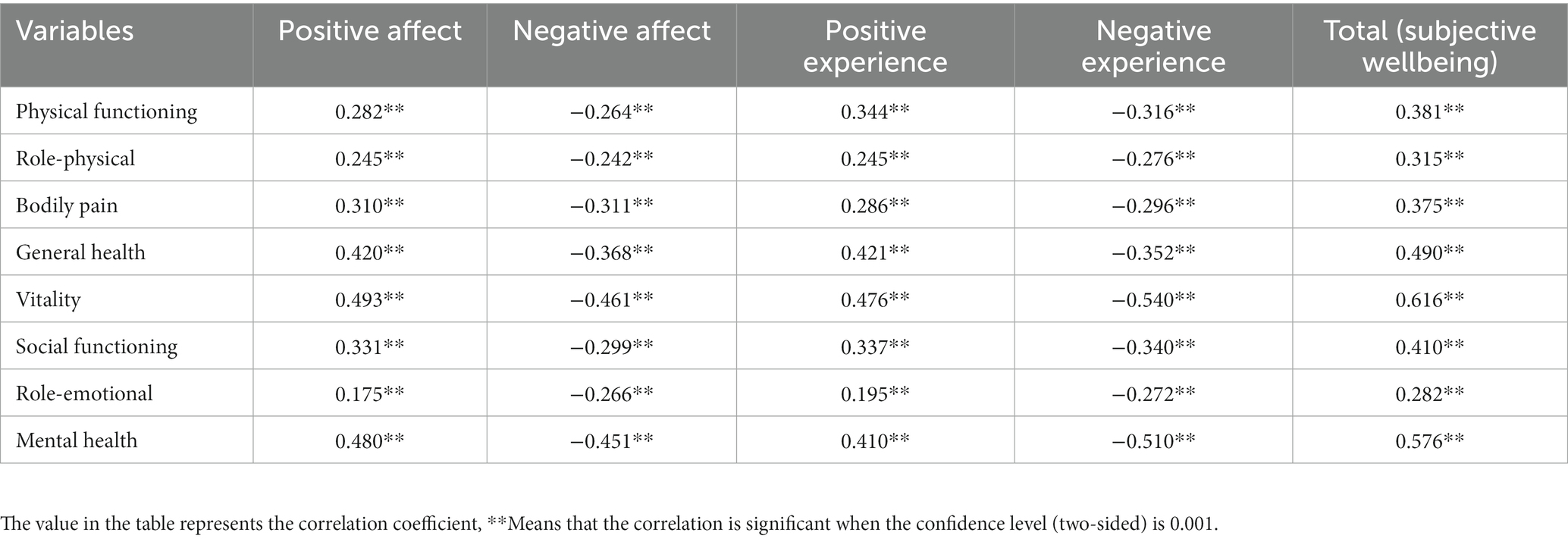
Table 3. Simple correlation analysis of subjective wellbeing scores and quality of life scores of older adults, n = 892.
3.4. Canonical correlation analysis
3.4.1. Canonical correlations and the tests
The canonical correlation analysis extracted a total of four pairs of canonical variables, all of which had statistically significant correlation coefficients (0.695, 0.179, 0.147, 0.121) (p < 0.05). Given the high cumulative contribution of the first pair of canonical variables, which accounted for 93.030%, further interpretation was provided for this pair, as shown in Table 4.

Table 4. Canonical correlation coefficients between wellbeing and QOL in older adults.
3.4.2. Standardized canonical coefficients for canonical variables
The magnitude of the absolute value of the standardized coefficients in the canonical correlation analysis represents the magnitude of the weights. As indicated by the standardized first canonical correlation coefficients (Table 5), for the first canonical variate (U1), the standardized canonical coefficients of physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health, as the variables of quality of life, were − 0.128, −0.010, −0.022, −0.222, −0.442, −0.007, 0.031, and −0.447, respectively. The coefficients of vitality (−0.442) and mental health (−0.447) contributed the most to quality of life. For the first canonical variate (V1), positive affect, negative affect, positive experience and negative experience were the variables of subjective wellbeing, and the standardized canonical coefficients were −0.338, 0.225, −0.292, and 0.388, respectively. The standardized canonical coefficients were approximately equal in absolute magnitude, indicating that the first canonical variate (V1) was reflected by a combination of positive affect (−0.338), negative affect (0.225), positive experience (−0.292) and negative experience (0.388). The two formulas presented below were derived from the canonical correlation analysis.
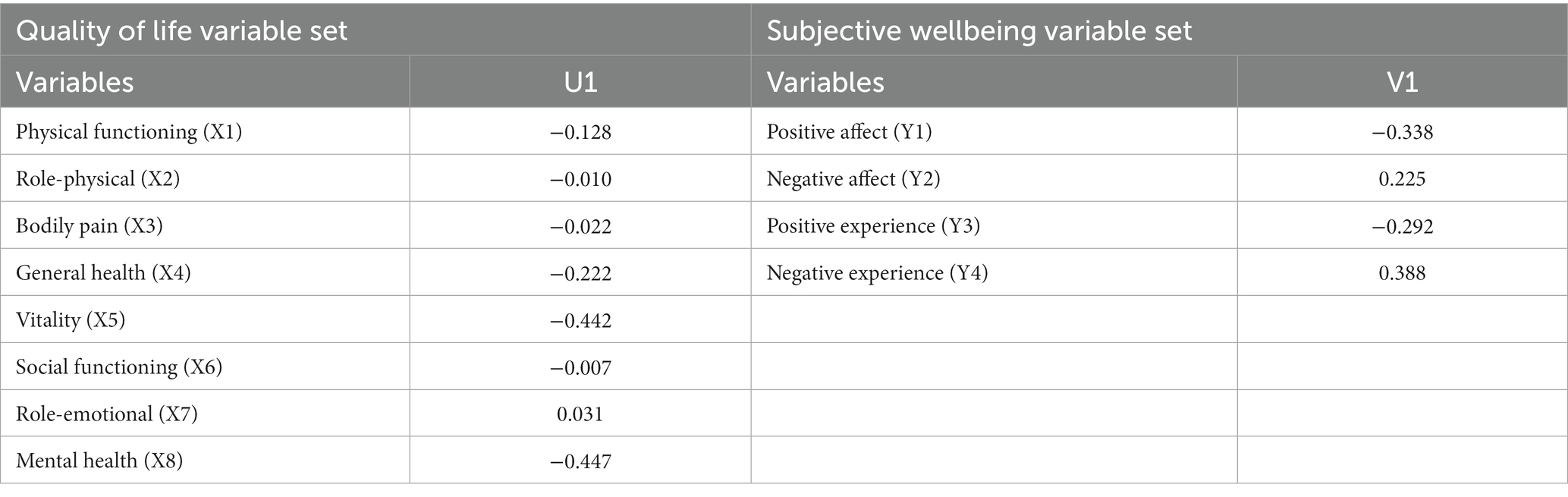
Table 5. Coefficients of standardized canonical variables for quality of life and subjective wellbeing of older adults, n = 892.
These equations are as follows:
3.4.3. Canonical loadings and cross loadings
Due to the large correlation between the dimensions of quality of life and those of subjective wellbeing as well as the possibility of covariance, explaining the problem solely through canonical weights would have been insufficient. In order to better reflect the relationship between the original and canonical variables, their correlation required further analysis by canonical loadings and cross-loadings (36).
As shown by the first set of canonical loading coefficients (Table 6), according to the canonical loading results, for the first pair of canonical variables of quality of life (U1), the most effective factor was vitality (−0.891), followed by mental health (−0.837), general health (−0.696), social functioning (−0.589), physical functioning (−0.543), bodily pain (−0.537), role-physical (−0.455) and role-emotional (−0.405). On the other hand, it showed that the first pair of canonical variables of quality of life (U1) was negatively correlated with the eight dimensions of quality of life. Similarly, for the first pair of canonical variables of subjective wellbeing (V1), the most effective factor was negative experience (0.848), followed by positive affect (−0.817), negative affect (0.755) and positive experience (−0.722). On the other hand, it demonstrated that the first pair of canonical variables of subjective wellbeing (V1) was negatively related to positive affect and positive experience, and positively related to negative affect and negative experience. Combining the canonical correlation coefficients revealed that the dimensions of quality of life were positively correlated with positive affect and positive experience of subjective wellbeing, and negatively correlated with negative affect and negative experience of subjective wellbeing.

Table 6. The loadings and cross loadings of the variables for the first canonical function in canonical correlation analysis, n = 892.
According to the cross-loadings, physical functioning, bodily pain, general health, vitality, social functioning and mental health were strongly correlated with subjective wellbeing (absolute value of cross-loadings was greater than 0.35), with cross-loadings of –0.378, −0.373, −0.484, −0.619, −0.409, and −0.581, respectively. Physical functioning, bodily pain, general health, vitality, social functioning and mental health were found to be the main factors reflecting subjective wellbeing among older adults.
3.4.4. Redundancy analysis
As can be seen from Table 7, the first canonical redundancy of the quality of life variable was 0.638, whereas the second was 0.308, indicating that the cumulative percentage of quality of life differences explained by their own canonical variables was 63.8%, while the cumulative percentage of subjective wellbeing differences explained by paired canonical variables was 30.8%. Similarly, the cumulative percentage of subjective wellbeing explained by its own canonical variables was 41.0%, whereas the cumulative percentage of quality of life explained by paired canonical variables was 19.8%. This demonstrates that quality of life and subjective wellbeing can be explained not only by their own canonical variables but also by each other’s canonical variables. The square of the canonical correlation coefficient was 0.483, indicating that the first canonical variable explained a certain proportion of the shared variance, further verifying the reliability of the analytical results.

Table 7. Explanatory ability of canonical variables.
4. Discussion
With the growing interest in improving the subjective wellbeing of older adults, it was important to understand the relationship between subjective wellbeing and quality of life. From the simple correlation analysis, it was clear that the quality of life of older adults was positively correlated with the total score of subjective wellbeing – importantly, the higher the quality of life of an older adult, the higher their subjective wellbeing, which was consistent with the findings of Bachmann et al. (41). This was attributable to the fact that older adults who had a high quality of life were more often in good health, while older adults with good subjective wellbeing also tended to have a healthy psyche and positive emotions (42). On the other hand, older adults with a good quality of life were less prone to negative emotions and had a higher level of life satisfaction (32, 33), thus leading to a higher level of subjective wellbeing.
Canonical correlation analysis showed that the dimensions of quality of life in older adults were positively correlated with positive affect and positive experience, and negatively correlated with negative affect and negative experience. Higher levels of physical function, role-physical, bodily pain and general health, reflecting somatic health in older adults, were associated with higher levels of the positive affect and positive experience, and lower levels of the negative affect and negative experience. This finding suggests that somatic health may have an effect on subjective wellbeing (37, 38). Physical health directly affected older adults’ experience of normal life. The healthier older adults were, the more energetic they felt, the more they interacted with others, the less lonely and miserable they felt, and the higher their subjective wellbeing. When older adults’ physical health was optimal, they had a greater likelihood of experiencing joy in life, which in turn enhanced their positive emotions and positive experiences of subjective wellbeing while minimizing their negative emotions and negative experiences to a corresponding degree (43). Conversely, poorer physical health due to chronic illness, painful experiences and/or economic stress all increased psychological stress in older adults, leading to anxiety and depression, which in turn directly affected their subjective wellbeing (44).
Similarly, the higher the vitality, social functioning, emotional functioning and mental health, all of which reflected the mental health of older adults, the higher the positive affect and positive experience, and the lower the negative affect and negative experience. Older adults might also have been more likely to experience loneliness due to a potential lack of family and friends (45). Negative affect was exacerbated among older adults who experienced prolonged feelings of sadness or depression. This, in turn, affected their perception estimation of life satisfaction and subjective wellbeing.
Canonical redundancy analysis was used to reflect the degree of variance explained by each typical variable with respect to the original set of variables as a whole. From the above results, it was clear that the subjective wellbeing of older adults could not be fully reflected in terms of quality of life, as it was also influenced by other factors. Therefore, when examining the subjective wellbeing of older adults, various factors needed to be comprehensively considered.
A correlation was observed between the quality of life and subjective wellbeing of older adults. Consequently, it is important to take appropriate measures that consider the individual characteristics of older adults to address their physical and psychological challenges. This approach can help older adults gain a more accurate perception of their quality of life and assess their subjective wellbeing. Moreover, it can mitigate the adverse effects of physical and psychological issues on their quality of life and emotional state, thereby enhancing not only their quality of life but also their subjective wellbeing. Due to the natural process of aging, degenerative changes in cognitive functions among older adults are inevitable and ultimately affect their physical and psychological health. Consequently, older adults are more susceptible to experiencing negative emotions and mental health problems. Therefore, it becomes crucial for family members, friends, and the community at large to closely monitor the psychological wellbeing of older adults. This vigilance can help identify negative factors at an early stage and facilitate constructive communication with older adults to address these factors before they escalate. Older adults should strive to maintain a positive and optimistic attitude, embracing every day with a positive mindset, and pursuing ‘happiness in old age.’
This study was limited by the available manpower and materials, and it was therefore not possible to conduct more extensive surveys in other areas of Dongguan City. In addition, subjective wellbeing among older adults is affected not only by quality of life but also by leisure and recreation, social environment, etc. Therefore, more substantial research is needed on the factors affecting subjective wellbeing among older adults. It is expected that, in the future, more in-depth research will be performed with more rigorous measures in the interest of improving the subjective wellbeing of older adults and helping them to age gracefully.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of Guangdong Medical University, China (REC: PJ2018037). Written informed consent was obtained from all subjects involved in the study.
Author contributions
HL, QG, and YL participated in study design, data collection, data analysis, and manuscript writing. QG, JT, and XS contributed to study design and made comments on the manuscript. CW assisted in writing the materials, collecting the data, and commenting on the manuscript. CW and YL was responsible for the overall content as the guarantor. All authors contributed to the article and approved the submitted version.
Funding
This research was funded by the Universities’ Young Innovative Talents Project of Guangdong Province (ID: 2021KQNCX024), Basic and Applied Basic Research Funding of Guangdong Province (ID: 2021A1515110436), Discipline Construction Project of Guangdong Medical University (ID: 4SG23032G), Guangdong Province Philosophy and Social Science Planning Project (ID: GD22YGL21), PHD Researcher Foundation of Guangdong Medical University (ID: GDMUB2021011), and Dongguan Science and Technology of Social Development Program (20211800905102).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ed, D, and Micaela, YC. Happy people live longer: subjective well-being contributes to health and longevity. Appl Psychol Health Well Being. (2011) 3:1–43. doi: 10.1111/j.1758-0854.2010.01045.x
2. Andrew, S, Angus, D, and Arthur, AS. Subjective wellbeing, health, and ageing. Lancet. (2015) 385:640–8. doi: 10.1016/S0140-6736(13)61489-0
3. Cummins, RA, Lau, AL, and Stokes, M. HRQOL and subjective well-being: noncomplementary forms of outcome measurement. Expert Rev Pharmacoecon Outcomes Res. (2004) 4:413–20. doi: 10.1586/14737167.4.4.413
4. Migliorini, C, Callaway, L, and New, P. Preliminary investigation into subjective well-being, mental health, resilience, and spinal cord injury. J Spinal Cord Med. (2013) 36:660–5. doi: 10.1179/2045772313Y.0000000100
5. Wang, SY, and Kim, G. The relationship between physical-mental comorbidity and subjective well-being among older adults. Clin Gerontol. (2020) 43:455–64. doi: 10.1080/07317115.2019.1580810
6. Lampropoulou, A. Personality, school, and family: what is their role in adolescents’ subjective well-being. J Adolesc. (2018) 67:12–21. doi: 10.1016/j.adolescence.2018.05.013
7. Abdullahi, AM, Orji, R, Rabiu, AM, and Kawu, AA. Personality and subjective well-being: towards personalized persuasive interventions for health and well-being. Inform. (2020) 12:e1. doi: 10.5210/ojphi.v12i1.10335
8. Yamaguchi, A, and Kim, MS. Effects of self-construal and its relationship with subjective well-being across cultures. J Health Psychol. (2015) 20:13–26. doi: 10.1177/1359105313496448
9. Nikitin, J, and Freund, AM. Does focusing on others enhance subjective well-being? The role of age, motivation, and relationship closeness. Psychol Aging. (2021) 36:69–82. doi: 10.1037/pag0000489
10. Becker, C, Kirchmaier, I, and Trautmann, ST. Marriage, parenthood and social network: subjective well-being and mental health in old age. PLoS One. (2019) 14:e218704. doi: 10.1371/journal.pone.0218704
11. Zhou, Y, Zhou, L, Fu, C, Wang, Y, Liu, Q, Wu, H, et al. Socio-economic factors related with the subjective well-being of the rural elderly people living independently in China. Int J Equity Health. (2015) 14:5. doi: 10.1186/s12939-015-0136-4
12. Lee, DM, Vanhoutte, B, Nazroo, J, and Pendleton, N. Sexual health and positive subjective well-being in partnered older men and women. J Gerontol B Psychol Sci Soc Sci. (2016) 71:698–710. doi: 10.1093/geronb/gbw018
13. Liang, Y, Niu, X, and Lu, P. The aging population in China: subjective well-being of empty nesters in rural eastern China. J Health Psychol. (2020) 25:361–72. doi: 10.1177/1359105317717599
14. An, HY, Chen, W, Wang, CW, Yang, HF, Huang, WT, Fan, S-Y, et al. The relationships between physical activity and life satisfaction and happiness among young, middle-aged, and older adults. Int J Environ Res Public Health. (2020) 17:4817. doi: 10.3390/ijerph17134817
15. Liu, C, Luo, D, Zhou, Y, Zhang, G, Feng, X, Wang, Z, et al. Optimism and subjective well-being in nursing home older adults: the mediating roles of gratitude and social support. Geriatr Nurs. (2022) 47:232–8. doi: 10.1016/j.gerinurse.2022.07.020
16. Ram, B, Limb, ES, Shankar, A, Nightingale, CM, Rudnicka, AR, Cummins, S, et al. Evaluating the effect of change in the built environment on mental health and subjective well-being: a natural experiment. J Epidemiol Community Health. (2020) 74:631–8. doi: 10.1136/jech-2019-213591
17. Zhang, W. Social capital, income and subjective well-being: evidence in rural China. Heliyon. (2022) 8:e8705. doi: 10.1016/j.heliyon.2021.e08705
18. Pinquart, M, and Sorensen, S. Influences of socioeconomic status, social network, and competence on subjective well-being in later life: a meta-analysis. Psychol Aging. (2000) 15:187–224. doi: 10.1037/0882-7974.15.2.187
19. Melendez-Moral, JC, Tomas-Miguel, JM, and Navarro-Pardo, E. Analyses of the social networks for the elderly through the Manheim interview. Salud Publica Mex. (2007) 49:408–14. doi: 10.1590/s0036-36342007000600007
20. Rook, KS. Social networks in later life: weighing positive and negative effects on health and well-being. Curr Dir Psychol Sci. (2015) 24:45–51. doi: 10.1177/0963721414551364
21. Liu, Y, Liu, H, Chen, Q, Xiao, J, and Wan, C. The Association of Perceived Neighbourhood Environment and Subjective Wellbeing in migrant older adults: A cross-sectional study using canonical correlation analysis. Int J Environ Res Public Health. (2023) 20:4021. doi: 10.3390/ijerph20054021
22. Helliwell, JF, and Putnam, RD. The social context of well-being. Philos Trans R Soc Lond Ser B Biol Sci. (2004) 359:1435–46. doi: 10.1098/rstb.2004.1522
23. Pavlova, MK, and Silbereisen, RK. Participation in voluntary organizations and volunteer work as a compensation for the absence of work or partnership? Evidence from two German samples of younger and older adults. J Gerontol B Psychol Sci Soc Sci. (2012) 67:514–24. doi: 10.1093/geronb/gbs051
24. LópezRuiz, V, HueteAlcocer, N, AlfaroNavarro, J, and NevadoPeña, D. The relationship between happiness and quality of life: a model for Spanish society. PLoS One. (2021) 16:e259528. doi: 10.1371/journal.pone.0259528
25. WHOQOL Group, W. Study protocol for the World Health Organization project to develop a quality of life assessment instrument (WHOQOL). Qual Life Res. (1993) 2:153–9. doi: 10.1007/BF00435734
26. Pilger, C, Santos, R, Lentsck, MH, Marques, S, and Kusumota, L. Spiritual well-being and quality of life of older adults in hemodialysis. Rev Bras Enferm. (2017) 70:689–96. doi: 10.1590/0034-7167-2017-0006
27. Ali, J, Marhemat, F, Sara, J, and Hamid, H. The relationship between spiritual well-being and quality of life among elderly people. Nurs Pract. (2015) 29:128–35. doi: 10.1097/HNP.0000000000000081
28. Finocchiaro, DN, Roth, PA, and Connelly, CD. Spiritual well-being as predictor of quality of life for adults with paraplegia. Rehabil Nurs. (2014) 39:285–93. doi: 10.1002/rnj.161
29. Yilmaz, M, and Cengiz, HO. The relationship between spiritual well-being and quality of life in cancer survivors. Palliat Support Care. (2020) 18:55–62. doi: 10.1017/S1478951519000464
30. Garduno-Ortega, O, Morales-Cruz, J, Hunter-Hernandez, M, Gany, F, and Costas-Muniz, R. Spiritual well-being, depression, and quality of life among Latina breast Cancer survivors. J Relig Health. (2021) 60:1895–907. doi: 10.1007/s10943-020-01147-9
31. Kozma, A, and Stones, MJ. The measurement of happiness: development of the Memorial University of Newfoundland scale of happiness (MUNSH). J Gerontol. (1980) 35:906–12. doi: 10.1093/geronj/35.6.906
32. Zhang, L, Wei, X, Ma, X, and Ren, Z. Physical health and quality of life among older people in the context of Chinese culture. Int J Environ Res Public Health. (2021) 18:6798. doi: 10.3390/ijerph18136798
33. Zhang, Q, Yang, Y, and Zhang, GL. Influence of life meaning on subjective well-being of older people: serial multiple mediation of exercise identification and amount of exercise. Front Public Health. (2021) 9:515484. doi: 10.3389/fpubh.2021.515484
34. Yang, Z, Li, W, Tu, X, Tang, W, Messing, S, Duan, L, et al. Validation and psychometric properties of Chinese version of SF-36 in patients with hypertension, coronary heart diseases, chronic gastritis and peptic ulcer. Int J Clin Pract. (2012) 66:991–8. doi: 10.1111/j.1742-1241.2012.02962.x
35. Wang, R, Wu, C, Zhao, Y, Yan, X, Ma, X, Wu, MH, et al. Health related quality of life measured by SF-36: a population-based study in Shanghai, China. BMC Public Health. (2008) 8:292. doi: 10.1186/1471-2458-8-292
36. Kabir, A, Merrill, RD, Shamim, AA, Klemn, RD, Labrique, AB, Christian, P, et al. Canonical correlation analysis of infant’s size at birth and maternal factors: a study in rural Northwest Bangladesh. PLoS One. (2014) 9:e94243. doi: 10.1371/journal.pone.0094243
37. Wang, D, Gao, H, Xu, X, Han, D, Yi, K, Hou, G, et al. Analysis of influence of physical health factors on subjective wellbeing of middle-aged and elderly women in China. BMC Public Health. (2022) 22:1127. doi: 10.1186/s12889-022-12655-6
38. Wang, W, Atingabili, S, Mensah, IA, Jiang, H, Zhang, H, Omari-Sasu, AY, et al. Teamwork quality and health workers burnout nexus: a new insight from canonical correlation analysis. Hum Resour Health. (2022) 20:52. doi: 10.1186/s12960-022-00734-z
39. Zarrel, VL, and Richard, MD. Some precautions in using canonical analysis. J Mark Res. (1975) 12:468–475. doi: 10.1177/002224377501200411
40. Arnold, LW. Redundancy analysis an alternative for canonical correlation analysis. Psychometrika. (1977) 42:207–219. doi: 10.1007/BF02294050
41. Bachmann, AS, Zaunbauer, AC, Tolke, AM, Siniatchkin, M, Kluck, C, Wiltfang, J, et al. Well-being and quality of life among oral cancer patients - psychological vulnerability and coping responses upon entering initial treatment. J Craniomaxillofac Surg. (2018) 46:1637–44. doi: 10.1016/j.jcms.2018.05.042
42. Diener, E. Subjective well-being. Psychol Bull. (1984) 95:542–75. doi: 10.1037/0033-2909.95.3.542
43. Elliot, D. Defining the relationship between health and well-being in bioethics. New Bioeth. (2016) 22:4–17. doi: 10.1080/20502877.2016.1155267
44. Conder, JA, Mirfin-Veitch, BF, and Gates, S. Risk and resilience factors in the mental health and well-being of women with intellectual disability. J Appl Res Intellect Disabil. (2015) 28:572–83. doi: 10.1111/jar.12153
Keywords: happiness, subjective wellbeing, quality of life, older adult, canonical correlation
Citation: Liu H, Gan Q, Tan J, Sun X, Liu Y and Wan C (2023) The association between quality of life and subjective wellbeing among older adults based on canonical correlation analysis. Front. Public Health. 11:1235276. doi: 10.3389/fpubh.2023.1235276
Edited by:
Claudio Alberto Davila-Cervantes, Facultad Latinoamericana de Ciencias Sociales, MexicoReviewed by:
Angela M. Goins, University of Houston–Downtown, United StatesRaman Mishra, Korea University, Republic of Korea
Copyright © 2023 Liu, Gan, Tan, Sun, Liu and Wan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuxi Liu, eXV4aWxpdTEyM0AxMjYuY29t; Chonghua Wan, d2FuY2hoQGhvdG1haWwuY29t
†These authors have contributed equally to this work and share first authorship