 George Gourzoulidis
George Gourzoulidis Myrto Barmpouni2
Myrto Barmpouni2 Jeffrey Vietri
Jeffrey Vietri
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 29 September 2023
Sec. Health Economics
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1229524
Objective: Higher valency pneumococcal conjugate vaccines (PCVs) are expected to improve protection against pneumococcal disease through coverage of additional serotypes. The aim of the present study was to evaluate the cost-effectiveness of 20-valent pneumococcal conjugate vaccine (PCV20) compared to 15-valent pneumococcal conjugate vaccine (PCV15) alone or followed by 23-valent polysaccharide vaccine (PPV23) for adults in Greece.
Methods: A published Markov model was adapted to simulate lifetime risk of clinical and economic outcomes from the public payer’s perspective. The model population was stratified based on age and risk profile (i.e., low, moderate, or high-risk of developing pneumococcal disease). Epidemiologic parameters, serotype coverage and vaccines’ effectiveness were based on published literature, while direct medical costs (prices €, 2022) were obtained from official sources. Main model outcomes were projected number of invasive pneumococcal disease (IPD) and all-cause non-bacteremic pneumonia (NBP) cases and attributable deaths, costs and quality-adjusted life-years (QALY) for each vaccination strategy. Sensitivity analyses were performed to ascertain the robustness of model results.
Results: Over the modeled time horizon, vaccination with PCV20 compared to PCV15 alone or PCV15 followed by PPV23 prevents an additional 747 and 646 cases of IPD, 10,334 and 10,342 cases of NBP and 468 and 455 deaths respectively, resulting in incremental gain of 1,594 and 1,536 QALYs and cost savings of €11,183 and €48,858, respectively. PSA revealed that the probability of PCV20 being cost-effective at the predetermined threshold of €34,000 per QALY gained was 100% compared to either PCV15 alone or the combination of PCV15 followed by PPV23.
Conclusion: PCV20 is estimated to improve public health by averting additional pneumococcal disease cases and deaths relative to PCV15 alone or followed by PPV23, and therefore translates to cost-savings for the public payer. Overall results showed that vaccination with PCV20 was estimated to be a dominant vaccination strategy (improved health outcomes with reduced costs) over PCV15 alone or followed by PPV23 for prevention of pneumococcal disease in adults in Greece.
Streptococcus pneumoniae can produce a range of infections collectively termed pneumococcal disease (1). Pneumococcal disease is a significant cause of morbidity and mortality globally, especially in patients with comorbidities and advanced age (2). Moreover, pneumococcal disease can be classified as either invasive pneumococcal disease (IPD) or non-invasive pneumococcal disease (3). More specifically, IPDs include infections such as bacteremia/sepsis, meningitis, or bacteremic pneumonia and non-invasive pneumococcal diseases include infections such as non-bacteremic pneumonia, otitis media, or sinusitis.
Non-bacteremic (non-invasive) pneumococcal pneumonia is much more common in adults than IPD, making up approximately 75% of cases of pneumococcal pneumonia (4, 5). Moreover, World Health Organization (WHO) reports that in most countries, pneumococcal surveillance systems are based on invasive disease infections (6), and therefore the burden of pneumococcal disease is most likely underestimated. In 2018, 42 confirmed cases of IPD were reported in Greece and the crude notification rate was 0.4 cases per 100,000 population (7). It has to be noted however that IPD is not under mandatory surveillance in Greece, with the exception of meningitis, therefore this number is probably an underestimate of the actual IPD cases (8).
The implementation of vaccination aimed to reduce the burden of the disease. In Greece, up to the end of 2022 there were 2 types of pneumococcal vaccines available for adults, the 13-valent pneumococcal conjugate vaccine (PCV13), which includes 13 serotypes, and the 23-valent pneumococcal polysaccharide vaccine (PPV23), which includes 23 serotypes. PCV13 was introduced in the adult National Immunization Program (NIP) for all persons ≥50 years of age as of December 2011. Prior to December 2011, Greece lacked a formalized adult NIP, but PPV23, which has been available on the market since 1999, was suggested in individuals deemed to have a higher susceptibility to pneumococcal disease by their attending physicians, although with low vaccination rates. In January 2015, the Greek NIP underwent revision, recommending the administration of PCV13 followed by PPV23 to individuals aged ≥65 years and those aged 19–64 years who are deemed to have an elevated risk of pneumococcal disease (8).
The recent approval of two new pneumococcal conjugate vaccines, 20-valent pneumococcal conjugate vaccine (PCV20) (9) and 15-valent pneumococcal conjugate vaccine (PCV15) (10), for use in Europe and the USA has resulted in an update of immunization program recommendations in European countries (11–14) and the USA (15, 16) in 2022. In addition to the PCV13 serotypes, PCV15 contains 2 additional serotypes (22F and 33F), while PCV20 contains 7 additional serotypes (8, 10A, 11A, 12F, 15B, 22F and 33F), that are among the most prevalent serotypes causing pneumococcal disease in adults. The suggested utilization of these newer conjugate vaccines was based on immunogenicity and safety studies (17–22).
The Greek NIP was recently modified considering the higher valency PCVs. According to the latest update, as provided by the Greek Ministry of Health on 07 February 2023, all pneumococcal vaccine-naïve persons ≥65 years of age and persons 18–64 years of age at increased risk for pneumococcal disease are suggested to receive 1 dose of PCV20. There are also specific recommendations for vaccination with PCV20 in adults with prior pneumococcal vaccination who are considered as not having completed their pneumococcal vaccination series (23).
Understanding the economic implications of updates in preventive and therapeutic public healthcare protocols is crucial for aiding healthcare decision-makers in the prudent utilization of limited healthcare resources, particularly in countries where pricing and reimbursement determinations rely on scientific proof through health technology assessment. In this light, the aim of the current study was to evaluate the cost-effectiveness of PCV20 compared to PCV15 alone or followed by PPV23 for adults in Greece.
A published deterministic model (24) with a Markov-type process was used to depict the lifetime risk of IPD and all-cause non-bacteremic pneumonia (NBP) and associated costs in adults aged 18–64 years with underlying conditions and all adults aged 65 years and older in Greece. Upon entering the model, the population is categorized based on age and risk profile, which includes low, moderate, or high risk. Persons may transition to a higher risk group, but not to a lower risk group, during the modeling lifetime horizon (82 years) (Figure 1).
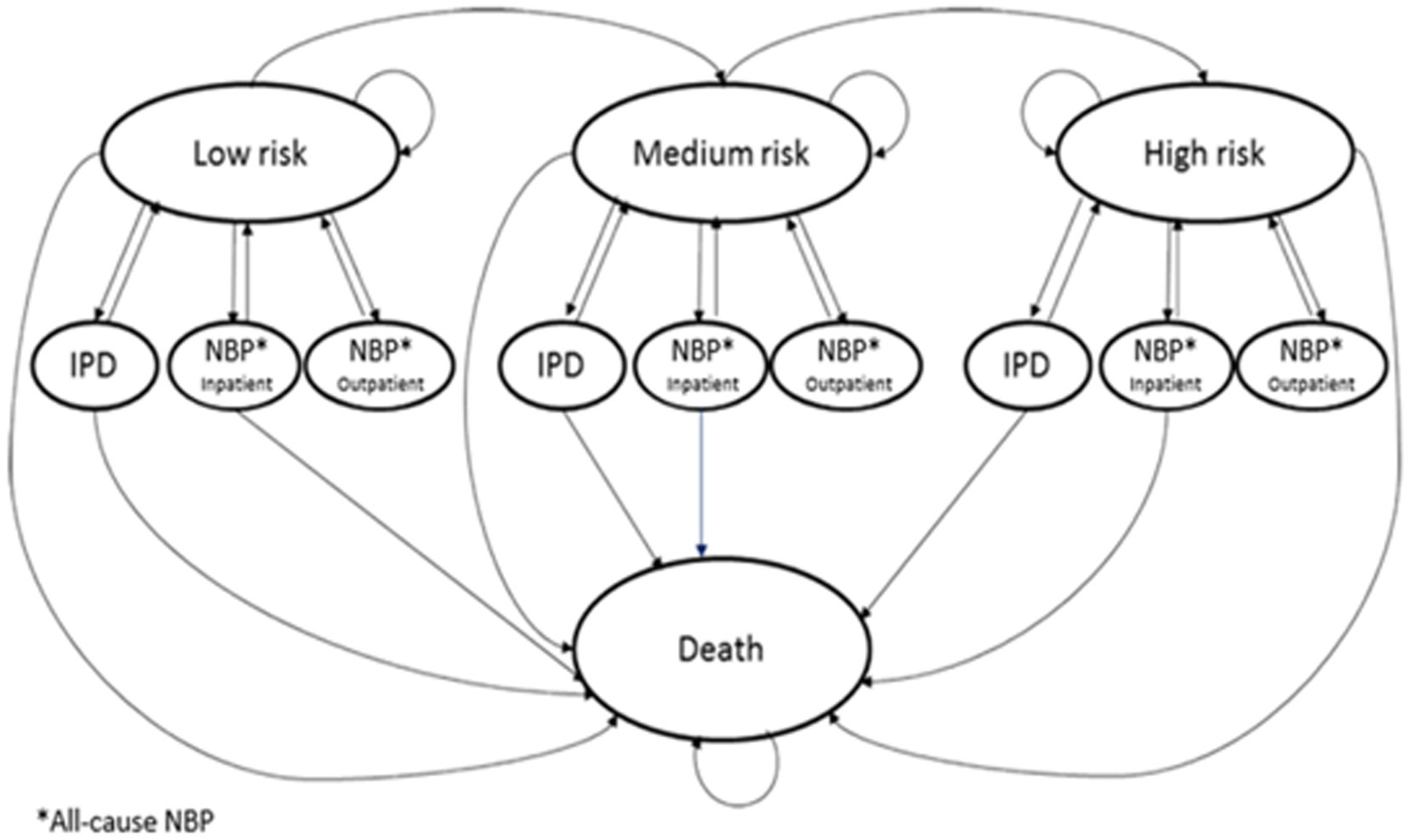
Figure 1. Model structure.
Annually, the projected clinical outcomes and economic costs for the model population are determined, taking into account various factors such as age, risk profile, disease/fatality rates, vaccination status, as well as the costs associated with vaccinations and medical care. The incidence of IPD is inclusive of both bacteremia and meningitis, while the occurrence of non-NBP is categorized by the care setting (inpatient or outpatient) for all causes. Individuals who have received the vaccine may experience a reduced risk of future IPD and all-cause NBP. The extent of risk reduction associated with vaccination depends on factors such as clinical presentation, types of vaccines used, the proportion of preventable diseases, as well as age and risk profile. Risk of death from IPD, all-cause NBP, and other causes is contingent upon age and individual risk profile. Expected medical treatment costs for IPD and all-cause NBP are generated based on event rates and unit costs in relation to care setting. The cost related to vaccination are accounted for in the year when the vaccine is administered. For each vaccination strategy, clinical outcomes and economic costs projected, including IPD and all-cause NBP cases and attributable deaths, life-years (LYs), quality-adjusted LYs (QALYs), and costs of vaccination and medical care treatment. The analysis was conducted from the perspective of a Greek public payer (EOPYY), and future model outcomes were discounted annually at a rate of 3.5%.as often used in such studies (25–27).
The model population size assessed in the cost-effectiveness model was Greek adults eligible for pneumococcal vaccination, divided in 5 age-groups (18–49 years, 50–64 years, 65–74 years, 75–84 years, 85–99 years) extracted from National Statistical Authority (28). The distributions of persons in each age group were allocated into low-, moderate and high-risk subgroup according to the existence of chronic and underlying comorbidities, based on local clinical experts’ opinion (Table 1). Meanwhile, the persons in the model population were assumed to receive either PCV20 alone, PCV15 alone or PCV15 followed by PPV23 during the modeling horizon.
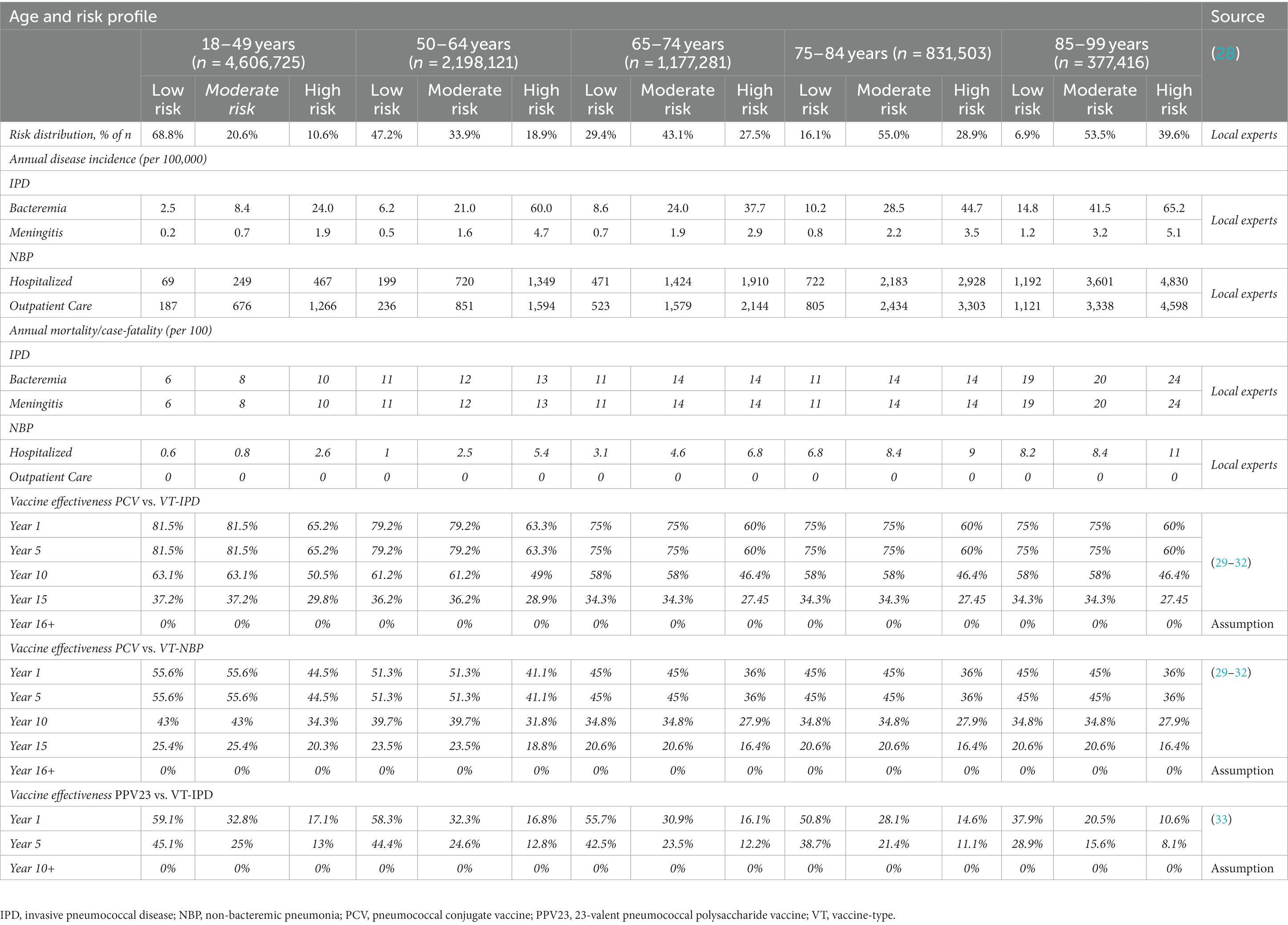
Table 1. Health inputs considered in the model.
The model inputs considered epidemiology, utilities, vaccine serotype coverage, vaccine effectiveness and uptake, and direct medical costs. These data which are presented in detail in the following sections were obtained from published studies and official Greek sources. The literature review and data collection were performed up to March 2023. A schematic of the model inputs and the outcomes considered is presented in Figure 2.
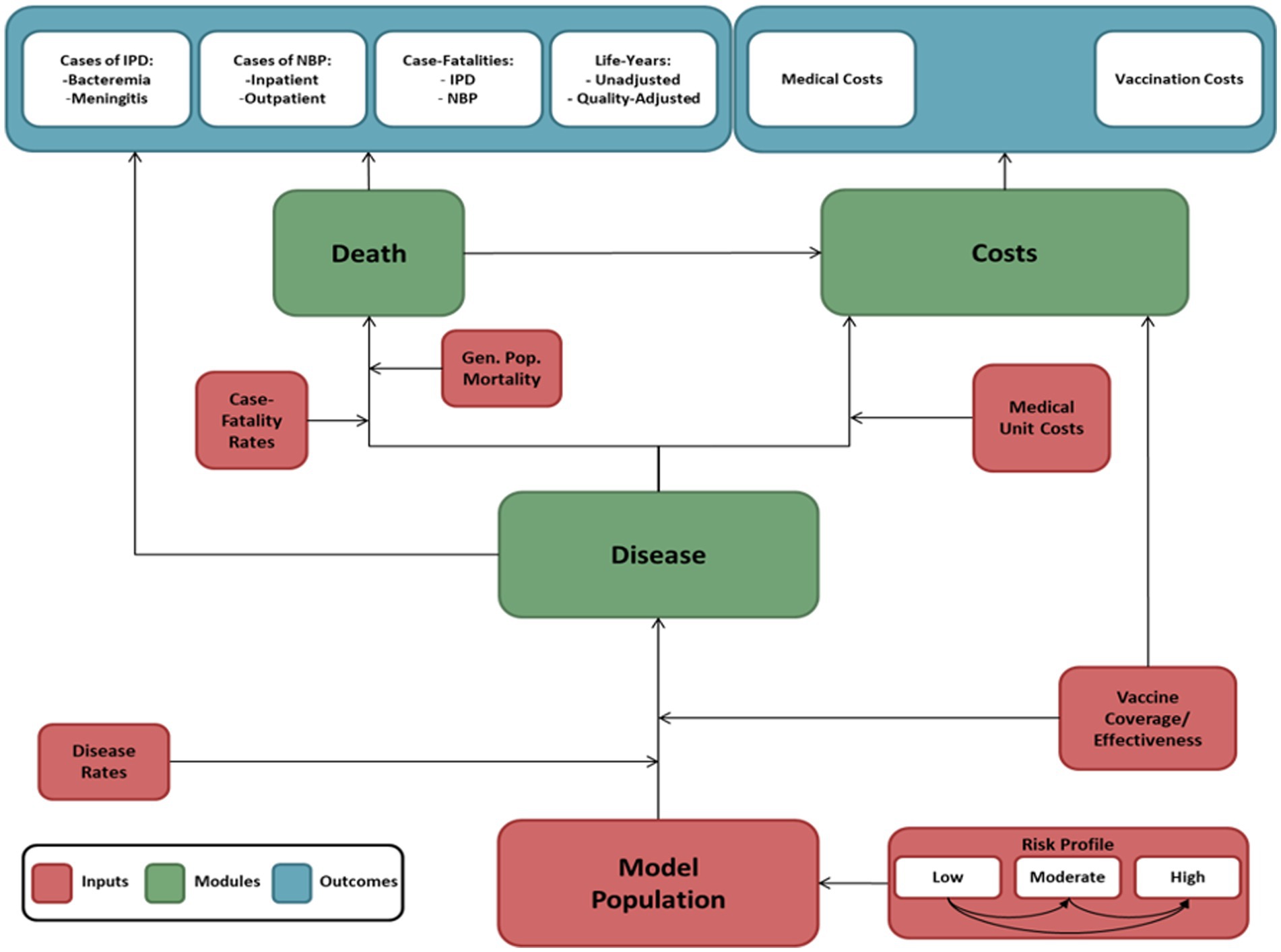
Figure 2. A schematic of the model inputs and the outcomes.
The disease incidence considered in the model was divided into bacteremia, meningitis and all-cause NBP (inpatient or outpatient care setting) incidence. Annual incidence of bacteremia, meningitis, and all-cause NBP were estimated by age and risk profile and were based on local clinical experts’ opinion (Table 1).
Mortality data were also divided into bacteremia, meningitis and all-cause NBP (inpatient or outpatient care setting) fatality and estimated by age and risk profile (Table 1). The mortality data of bacteremia, meningitis and all-cause NBP were derived from published studies and validated by local clinical experts, while the general population mortality was obtained from WHO National Life Tables for Greece (latest available).
The vaccine effectiveness (VE) of PCVs against VT-IPD and VT-NBP, for low−/moderate-risk persons aged 50–64 years, was derived using age-specific relative changes in VE against VT-IPD and VT-NBP (vs. age 65 years) from Mangen et al. (29). For individuals aged 18–49 years, the VE was assumed to be the same as that for individuals aged 50 years (29). For low−/moderate-risk individuals aged ≥65 years, VE obtained from randomized controlled trial data from the Community-Acquired Pneumonia Immunization Trial in Adults (CAPiTA) (29). For high-risk individuals VE was assumed to be equal to 80% of corresponding values for low−/moderate-risk persons (Table 1). This assumption was supported by findings from literature (30, 31) and a recent published cost-effectiveness study of PCV20 in the UK (24). Initial VE of PCVs was assumed to persist for 5 years, consistent with the CAPiTA trial (29, 32) and to annually wane thereafter, 5% during years 6–10 and 10% between years 11 and 15. After year 16, it was assumed that there was no efficacy through the end of the model horizon. These assumptions were also used in similar published cost-effectiveness studies (24, 34) (Table 1).
The VE of PPV23 against VT-IPD for low-, moderate-, and high-risk persons was derived for all ages by fitting a logarithmic curve to values for persons aged 65–74, 75–84, and 85–99 years, and then estimating the age-specific values across the three risk groups using relative risks from Djennad et al. and the population sizes (33) (Table 1). Based on published studies, it was assumed that the VE of PPV23 against VT-NBP was zero (35, 36) and consistent with base-case assumptions employed in several of economic evaluation studies (24, 34, 37–39). As for the vaccine waning for PPV23, it was obtained from Djennad et al. (33), with a linear decline to 76.2% of initial vaccine efficacy by year 5, followed by a linear decline to no efficacy by year 10. This assumption was also used in similar published cost-effectiveness studies (24, 34) (Table 1).
Age and risk profile specific vaccine uptake was considered in the analysis, and was assumed to be higher for persons aged 65 years and older compared to persons aged <64 years, based on local clinical experts. Vaccine uptake was assumed to be the same for all vaccination strategies. Moreover, vaccine serotype coverage was also included in the model, however in absence of detailed local data, the proportion of IPD and NBP against which the vaccines provide protection were derived from published data (40) and validated by local clinical experts (41). The assumption was made that the coverage against serotypes would be consistent across all age groups.
Age- and risk-specific health-state utility values for the general population were derived from published study (42). Moreover, the annual disutility associated with hospitalized disease (i.e., bacteremia, meningitis, and all-cause NBP) was −0.13 and based on a study by Mangen et al. (43). Annual disutility of NBP requiring outpatient care only (−0.004) was based on data from a study by Melegaro et al. (44). Regardless of age and risk profile, it was assumed that all disutilities were equal (Table 2).
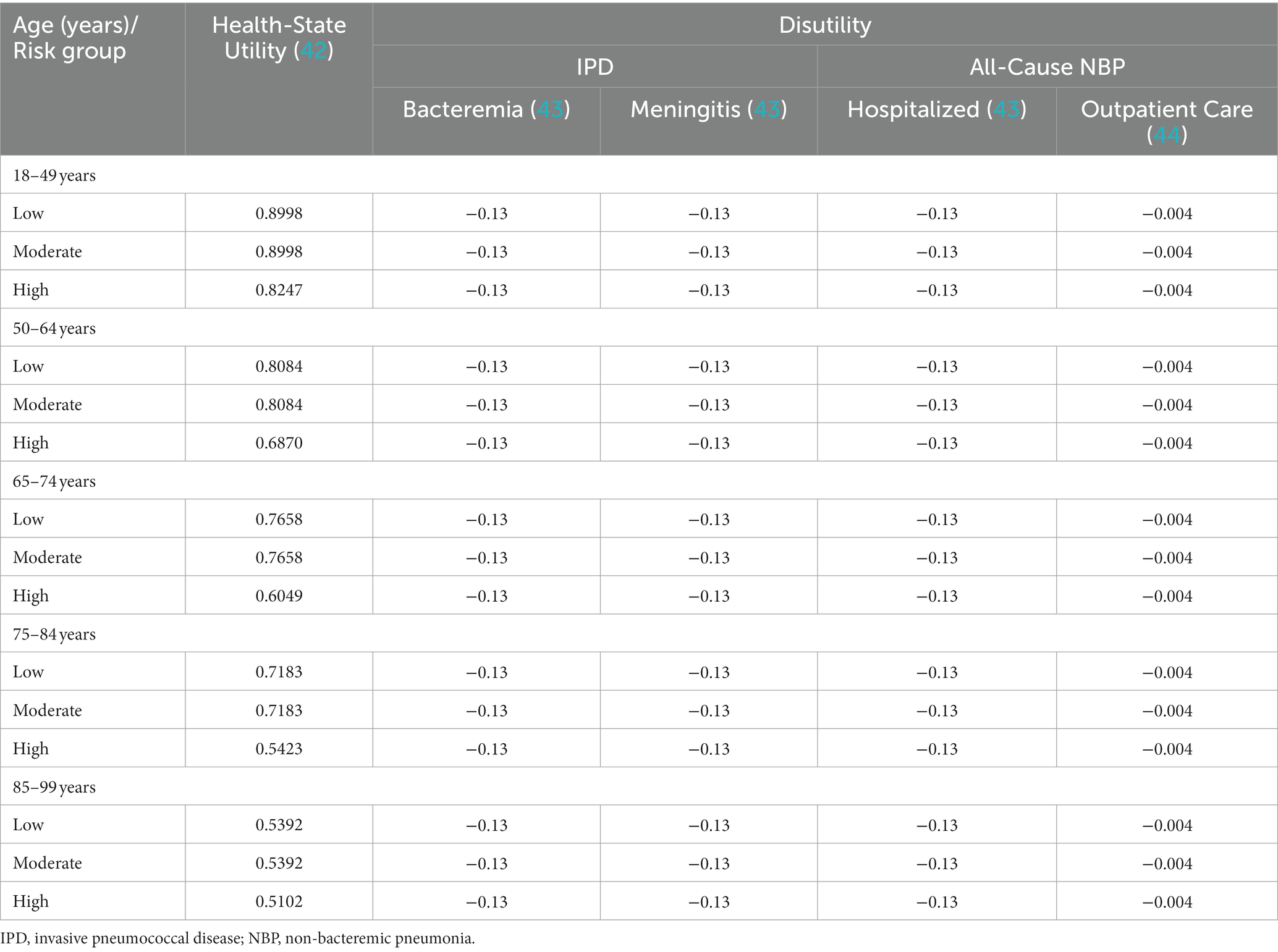
Table 2. Health-state utility and disutility inputs considered in the model.
The analysis was conducted from a public payer perspective and as such only health care costs reimbursed by the public payer were considered. In particular, the cost inputs considered in the model included vaccination costs and medical treatment costs for IPD and all-cause NBP. All unit costs correspond to the year of the analysis (2022, €).
In Greece, vaccines are fully reimbursed from the public payer, as per current legislation. The vaccine unit costs were sourced from the latest available price bulletin issued by the Greek Ministry of Health as well as the official list of the reimbursed medicines (Table 3) (45).
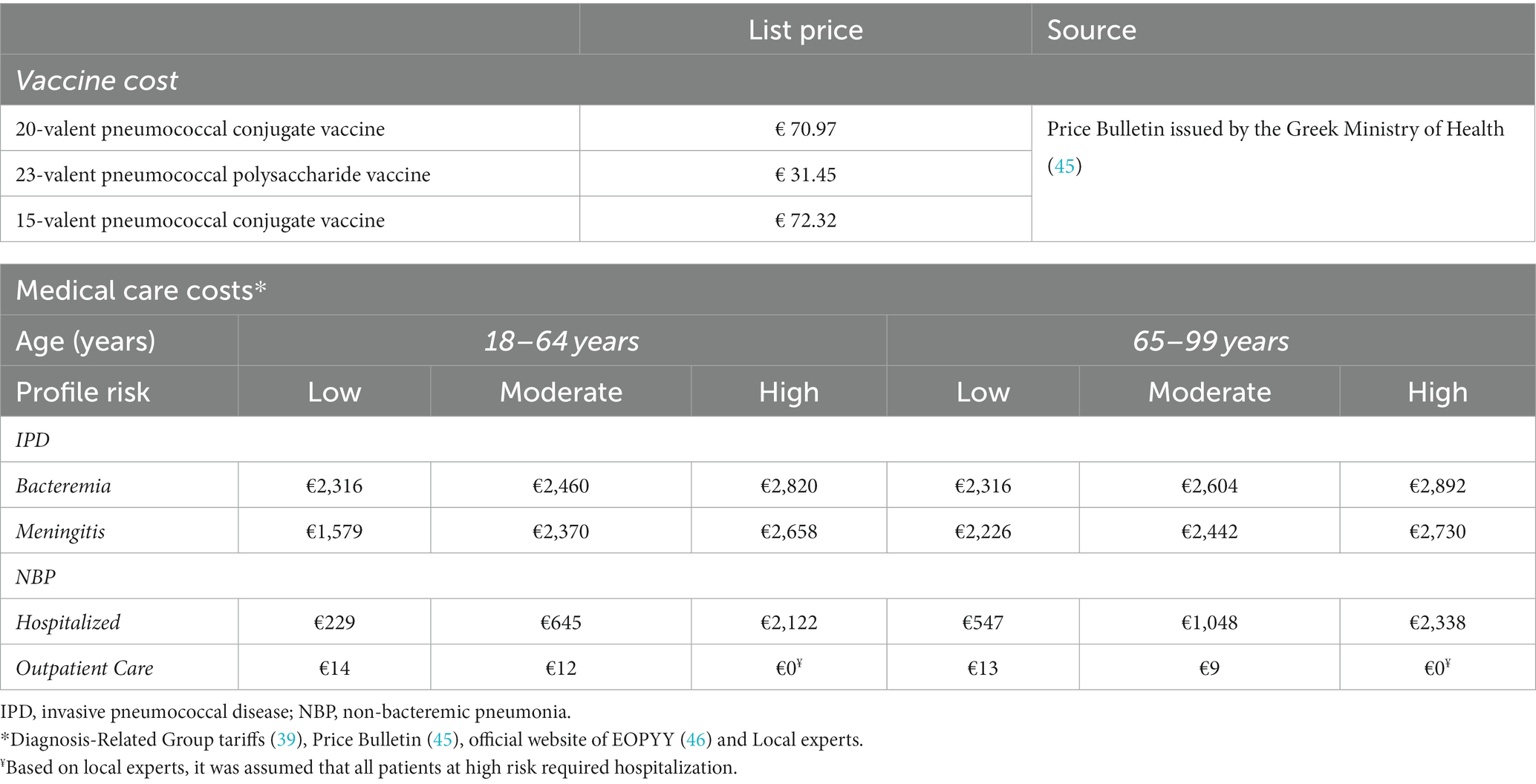
Table 3. Cost inputs considered in the model.
As for the management cost of bacteremia, meningitis and all-cause non-bacteremic pneumonia, this was derived after investigating the setting on which it is treated. More specifically, all patients with bacteremia and meningitis were considered as requiring hospitalization. For the case of pneumonia, local experts provided the proportion of patients deemed in need of hospitalization. Moreover, costs for treating and managing events in the inpatient setting were obtained from the corresponding Diagnosis-Related Group (DRGs) tariffs issued by the Greek Ministry of Health (47). Combining the resources utilized, the costs associated with outpatient management of pneumonia were estimated as provided by local experts, with the corresponding unit costs obtained from the drug price bulletin issued by the Greek Ministry of Health (45), Government gazette and the official website of public payer (EOPYY) (46) (Table 3).
Using the aforementioned method and data, the calculation was performed to determine the clinical outcomes and economic costs for each vaccination strategy. The main model outcomes included IPD and all-cause NBP cases and attributable deaths, LYs and QALYs gained, and lifetime costs. An incremental cost-effectiveness analysis was performed to identify the most cost-effective strategy. Despite the fact that, there is no official willingness-to-pay (WTP) threshold for Greece for a health intervention to be considered cost-effective, a WTP threshold of €34,000 per QALY/LY was used in the current analysis based on the recommendation that a health intervention should be considered cost-effective if the ICER is between one to three times the GDP per capita of that country (48–51). This formula for WTP threshold has been widely used in cost-effectiveness studies within global health (48–51). The Greek GDP per capita was taken from the International Monetary Fund (IMF), which estimated it at €17,000 using current prices (52) at the time of the analysis.
A one-way sensitivity analysis (OWSA) was undertaken to test the robustness of the results to individual inputs, holding all else constant. The parameters considered in OWSA were disease incidences, mortality, utility, disutility, VE, medical cost, and vaccine price. OWSA’s model results were recorded after changing each input to its upper and lower bound value in turn. The upper and lower bound values for each parameter were taken as percent of base case (−25% for lower bound and + 25% for upper bound).
Moreover, probabilistic sensitivity analysis (PSA), which assesses the stochastic parametric uncertainty, was used. This is a technique that provides an estimation of the joint uncertainty of costs and effectiveness, based on a simulation where assigning probabilistic distributions to key input parameters, recursively re-sampling new values for each parameter from their respective distribution, and subsequently estimating the costs and effectiveness of each intervention based on the new values is undertaken. A normal distribution was applied for disease incidences and mortality. A beta distribution was used for estimates of utility and disutility, while a triangular distribution was applied for VE. The PSA used simulation modeling to run 1,000 analyses, in order to be able to construct cost-effectiveness acceptability curves (CEAC), which indicate the likelihood of the incremental cost per QALY to fall below specified thresholds.
In addition, scenario analyses were conducted to assess the cost-effectiveness of vaccination of specific age/risk subgroups. More specifically, different age and risk profile groups such as (i) individuals aged 65 years and older at moderate or high risk, (ii) individuals aged 65 years and older at high risk, (iii) individuals aged 18–64 years at high risk and (iv) individuals aged 65 years and older were considered.
According to the base case analysis PCV20 resulted in fewer IPD and NBP cases and deaths compared to either PCV15 alone or PCV15 followed by PPV23. More specifically, over the modeled time horizon, vaccination with PCV20 compared to PCV15 alone or PCV15 followed by PPV23 prevents an additional 747 and 646 cases of IPD, 10,334 and 10,342 cases of NBP and 468 and 455 deaths respectively, resulting in incremental gain of 1,594 and 1,536 QALYs, respectively, (Table 4).
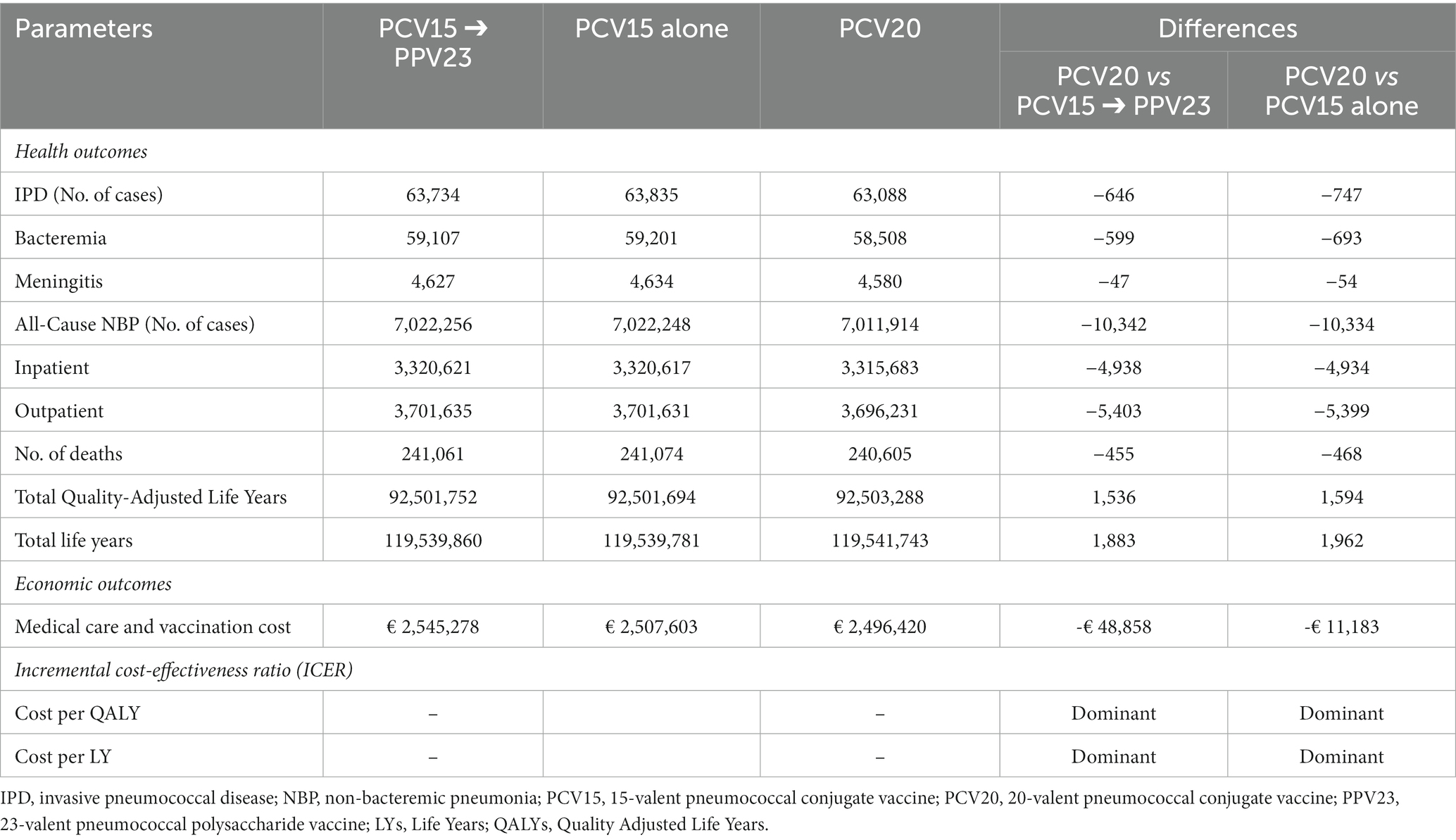
Table 4. Base case model results.
The lower number of pneumococcal disease cases with PCV20 compared to PCV15 alone or PCV15 followed by PPV23 translated to a reduction of medical costs of €11,183 and €48,858 respectively, over the model life-time horizon (Table 4).
The incremental analysis showed that, PCV20 compared to PCV15 alone or PCV15 followed by PPV23 resulted in both a QALY gain and a cost reduction. Hence, based on these findings, vaccination with PCV20 was estimated to be a dominant strategy (improved health outcomes with reduced costs) compared with PCV15 alone or PCV15 followed by PPV23 (Table 4).
The OWSA demonstrated the resilience of the findings to variations in the base case parameters of the model. It is important to mention that in all sensitivity analyses, vaccination with PCV20 was associated with lower costs and more QALYs gained as compared to PCV15 alone or PCV15 followed by PPV23, hence, PCV20 remained a dominant vaccination strategy. Moreover, the PSA confirmed the base case results. In particular, the analyses showed that at the predefined WTP of €34,000 per QALY/LY gained, vaccination with PCV20 had 100% probability of being a cost-effective option compared with PCV15 alone or PCV15 followed by PPV23.
Scenario analyses according to specific age- and risk- groups were also conducted. In all scenario analyses, PCV20 remains a cost-effective option compared with PCV15 alone or PCV15 followed by PPV23 (Supplementary file, Table 1).
Following recent approval of PCVs with expanded serotype coverage, the present study was undertaken from a public payer perspective to compare the health and economic outcomes of PCV20 with those of PCV15 vaccination strategies for adults in Greece. PCV20 was estimated to be a dominant vaccination strategy (improved health outcomes with reduced costs) over PCV15 alone or PCV15 followed by PPV23 for prevention of pneumococcal disease in adults in Greece.
The results of sensitivity analyses revealed that the base-case findings were not significantly affected by changes in input parameters and assumptions. In particular, PSA estimated that vaccination with PCV20 had a 100% probability of being a cost-effective vaccination option compared to PCV15 alone or followed by PPV23, respectively, under the WTP threshold of €34,000 per QALY gained. Furthermore, the OWSA revealed that in all sensitivity analyses, vaccination with PCV20 was associated with lower costs and more QALYs gained as compared to PCV15 alone or PCV15 followed by PPV23.
At the time of writing, a limited number of economic studies have been conducted to assess the cost-effectiveness of PCV20 compared to PCV15 or PCV15 followed by PPV23 were found in the international literature, however all of them are aligned with our results (53–55). More specifically, a cost-effectiveness study (54) conducted in Argentina from a payer’s perspective revealed that PCV20 compared to PCV15 followed by PPV23 averted more cases of IPD, all-cause NBP and deaths with a higher number of LYs and QALYs at a lower cost, hence, PCV20 was estimated to be a dominant vaccination strategy. Moreover, a recent study (53) conducted in Italy showed that PCV20 was a cost-effective vaccination strategy versus PCV15 alone (assuming a price that is equivalent to that of PCV13) in adults’ population. Additionally, a study performed in USA showed that PCV20 use are substantially more economically reasonable in the older adult population than PCV15 followed by PPSV23 (55).
The cost-effectiveness results stem from the inclusion of additional serotypes in PCV20 compared to PCV15 (8, 10A, 11A, 12F, and 15B) and PCV13 (8, 10A, 11A, 12F, 15B, 22F, and 33F), which are major causes of pneumococcal disease in the adult population. Despite the lack of a comprehensive national surveillance system for pneumococcal disease in Greece, that precluded the use of local morbidity and epidemiological data in our cost-effectiveness model, there are some recently published data underlining the clinical value of PCV20 in Greece (8, 41). According to the National Meningitis Reference Laboratory data for the period 2010–2020, in adults aged ≥65 years, PCV13, PCV15 and PCV20 were estimated to potentially cover 41.1, 42.5 and 54.8% of pneumococcal meningitis cases, respectively (8). In addition, in the interim analysis of an ongoing prospective study of adults ≥19 years old hospitalized with clinical and radiographically-confirmed community-acquired pneumonia (CAP) in the Ioannina and Kavala regions of Greece (EGNATIA study), PCV13, PCV15 and PCV20 were estimated to potentially cover 7.3, 8.1 and 9.8% of hospitalized all-cause CAP in adults aged ≥19 years, respectively (41).
Moreover, Greece, like many other countries, has an aging population. Older adults are particularly vulnerable to pneumococcal infections, as immunosenescence renders them more susceptible to disease and severe complications. According to a new demographic study, by 2,100 the proportion of the population aged 65 years and older is projected to increase, reaching one third of the overall Greek population (56). Therefore, it is of utmost importance to protect this high-risk population with appropriate and effective vaccines offering broad serotype coverage.
Furthermore, the additional serotypes of PCV20 compared to PCV13 are important in the epidemiology of pneumococcal disease not only in adults, but also in the pediatric population. In Greece, according to the National Meningitis Reference Laboratory pneumococcal meningitis data for the period 2010–2020, PCV13 serotypes represented 27.3%, PCV15 serotypes also represented 27.3%, and PCV20 serotypes represented 47.7% of pneumococcal meningitis cases in children aged <5 years (8). Moreover, another study which was conducted in Greece from November 2015–December 2020 in children aged ≤14 years with IPD and non-invasive pneumococcal disease (mainly otitis media) reported that PCV13 serotypes were responsible for 42.9% of pneumococcal disease (38.8% for IPD, 44.7% for non-invasive pneumococcal disease). PCV15 and PCV20 were estimated to potentially cover 46.3% (42.9% of IPD, 47.7% of non-invasive pneumococcal disease) and 64.9% (66.3% of IPD, 64.3% of non-invasive pneumococcal disease) of pneumococcal disease in children aged ≤14 years (57), respectively. Finally, in a cross-sectional study using molecular methods, data on oropharyngeal pneumococcal colonization over time was collected from 1,212 Greek children throughout the country during the period January–August 2017. Serotypes/serogroups 15A/B/C/F, 11A/D/E, 10A/B, 22A/F, 33F, 12A/B/F/44/46, 8, were all among the identified serotypes/serogroups in pneumococcal carriage (58).
Lastly, while cost-effectiveness analysis is a useful tool for evaluating the costs and benefits of health interventions, it typically does not capture all the value elements that vaccines offer. More specifically, vaccination can also have wider societal benefits, such as reducing the burden on healthcare systems, improving productivity by reducing absenteeism from work and school, helping combat antimicrobial resistance and preventing outbreaks that can have significant economic impacts (59, 60). These benefits are not always easy to quantify and may not be captured by a cost-effectiveness analysis, and that is true of the current analysis. In addition, the COVID-19 pandemic has highlighted the importance of vaccination in reducing the transmission of the virus, protecting populations from severe illness and death and supporting the society’s return to normality (59, 60). In this context, the value of vaccination may extend beyond the traditional cost-effectiveness analysis framework and a more comprehensive approach is needed to fully capture the societal and economic benefits of vaccination and to ensure that the health policy decisions makers are aligned with the broader goals of public health.
In terms of our study limitations, in the current analysis, it was postulated that the utility and disutility data acquired from the published studies (42–44) were relevant to the healthcare environment in Greece, nonetheless, considering the lack of available data at the local level and the limitations in terms of quality and validity of the relevant studies, this decision was deemed suitable. Moreover, whenever necessary, local experts were consulted and their input, including any pertinent local data, was taken into account to ensure the validation of the model’s inputs. However, a set of sensitivity analyses demonstrated the robustness of the model outcomes, as the key findings remained consistent across a broad spectrum of parameter values. Furthermore, the present model analysis did not include potential adverse events (AE) associated with PCV20, PCV15 and PPV23 vaccination, since most AE are of mild or moderate severity and serious AE are rare, hence the impact on model base case results would be negligible. The same approach has been used also in recent model publications in UK and Denmark (24, 34). However, in the absence of differential safety data, incorporating AEs would favor single-dose strategies. Additionally, the present analysis was undertaken from the viewpoint of the public payer perspective, focusing solely on direct costs. While adopting a societal perspective could prove valuable, the current analysis did not incorporate indirect costs, such as patient time, caregiver expenses, and productivity losses, which would reflect the missed opportunities for society as a whole. Moreover, it should be noted that the results have to be considered for the management of pneumococcal disease in the strict Greek setting and on the basis of the present time, disease costs, vaccine prices, epidemiology data and the NIP. Therefore, the results of current study may not be generalizable to other populations with different disease burdens and healthcare systems.
PCV20 is estimated to improve public health by averting additional pneumococcal disease cases and deaths relative to PCV15 alone or PCV15 followed by PPV23, and translates to cost-savings for the public payer. Overall results showed that vaccination with PCV20 was estimated to be a dominant vaccination strategy (improved health outcomes with reduced costs) over PCV15 alone or PCV15 followed by PPV23 for prevention of pneumococcal disease in adults.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
This study was an economic evaluation analysis which based on previously publicly available data and does not involve any new studies of human or animal subjects performed by any of the authors.
GG and CT conducted the analyses, collected the data, and interpreted the results. GG, MB, and VK wrote the manuscript. GG, MB, VK, JV, and CT contributed to results interpretation and manuscript writing. All authors reviewed and approved the final manuscript.
The study was supported by Pfizer, Hellas SA. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this manuscript or the decision to submit it for publication.
MB and VK were employed by Pfizer Hellas. JV was employed by Pfizer Inc.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1229524/full#supplementary-material
1. Thornton, JA, Durick-Eder, K, and Tuomanen, EI. Pneumococcal pathogenesis: “innate invasion” yet organ-specific damage. J Mol Med (Berl). (2010) 88:103–7. doi: 10.1007/s00109-009-0578-5
2. Maraki, S, Mavromanolaki, VE, Stafylaki, D, Hamilos, G, and Samonis, G. The evolving epidemiology of serotype distribution and antimicrobial resistance of Streptococcus pneumoniae strains isolated from adults in Crete, Greece, 2009-2016. Infect Chemother. (2018) 50:328–9. doi: 10.3947/ic.2018.50.4.328
3. Ludwig, E, Bonanni, P, Rohde, G, Sayiner, A, and Torres, A. The remaining challenges of pneumococcal disease in adults. Euro Res Rev Off J Euro Res Soc. (2012) 21:57–65. doi: 10.1183/09059180.00008911
4. Said, MA, Johnson, HL, Nonyane, BA, Deloria-Knoll, M, O’Brien, KL, AGEDD Adult Pneumococcal Burden Study Team, et al. Estimating the burden of pneumococcal pneumonia among adults: a systematic review and meta-analysis of diagnostic techniques. PLoS One. (2013) 8:e60273. doi: 10.1371/journal.pone.0060273
5. Huang, SS, Johnson, KM, Ray, GT, Wroe, P, Lieu, TA, Moore, MR, et al. Healthcare utilization and cost of pneumococcal disease in the United States. Vaccine. (2011) 29:3398–12. doi: 10.1016/j.vaccine.2011.02.088
7. ECDC. Annual epidemiological report for 2018. European Centre for Disease Prevention and Control, (2020). Available at: https://www.ecdc.europa.eu/en/publications-data/monitoring/all-annual-epidemiological-reports
8. Xirogianni, A, Marmaras, N, Georgakopoulou, T, Papandreou, A, Simantirakis, S, Magaziotou, I, et al. Pneumococcal meningitis in Greece: a retrospective serotype surveillance study in the post-PCV13 era (2010-2020). Vaccine. (2022) 40:5079–87. doi: 10.1016/j.vaccine.2022.07.015
9. European Medicines Agency (EMA). Summary of product characteristics Apexxnar. (2022). Available at: https://www.ema.europa.eu/en/documents/product-information/apexxnar-epar-product-information_en.pdf. (accessed January 10, 2023).
10. European Medicines Agency(EMA). Summary of product characteristics Vaxneuvance. (2022). Avaialble at: https://www.ema.europa.eu/en/documents/product-information/vaxneuvance-epar-product-information_en.pdf. (accessed January 10, 2023).
11. Federal Public Service Health Food Chain Safety and Environment. Vaccination against pneumococcal disease for adults. (2022). Available at: https://www.health.belgium.be/en/report-9674-vaccination-against-pneumococcal-disease-adults. (accessed May 23, 2023).
12. Public Health Agency of Sweden. Vaccination programmes and recommendations. (2022). Available at: https://www.folkhalsomyndigheten.se/the-public-health-agency-of-sweden/communicable-disease-control/vaccinations/vaccination-programmes/ (accessed May 23, 2023).
13. Norwegian Institute of Public Health. Pneumococcal vaccine for risk groups. (2022). Available at: https://www.fhi.no/en/id/vaccines/voksenvaksinasjon/pneumococcal-vaccine-for-risk-groups/ (accessed May 23, 2023).
14. Danish Health Authority. Vaccines for certain groups of people. (2022). Available at: https://www.sst.dk/da/viden/Forebyggelse/Vaccination/Vaccination-af-voksne/Tilskud-til-vacciner. (accessed May 23, 2023).
15. Kobayashi, M, Farrar, JL, Gierke, R, Britton, A, Childs, L, Leidner, AJ, et al. Use of 15-valent pneumococcal conjugate vaccine and 20-valent pneumococcal conjugate vaccine among U.S. adults: updated recommendations of the advisory committee on immunization practices - United States, 2022. MMWR Morb Mortal Wkly Rep. (2022) 71:109–7. doi: 10.15585/mmwr.mm7104a1
16. Musher, DM, Anderson, R, and Feldman, C. The remarkable history of pneumococcal vaccination: an ongoing challenge. Pneumonia (Nathan Qld). (2022) 14:5. doi: 10.1186/s41479-022-00097-y
17. Song, JY, Chang, CJ, Andrews, C, Diez-Domingo, J, Oh, MD, Dagan, R, et al. Safety, tolerability, and immunogenicity of V114, a 15-valent pneumococcal conjugate vaccine, followed by sequential PPSV23 vaccination in healthy adults aged ≥50 years: a randomized phase III trial (PNEU-PATH). Vaccine. (2021) 39:6422–36. doi: 10.1016/j.vaccine.2021.08.038
18. Platt, HL, Cardona, JF, Haranaka, M, Schwartz, HI, Narejos Perez, S, Dowell, A, et al. A phase 3 trial of safety, tolerability, and immunogenicity of V114, 15-valent pneumococcal conjugate vaccine, compared with 13-valent pneumococcal conjugate vaccine in adults 50 years of age and older. Vaccine. (2022) 40:162–2. doi: 10.1016/j.vaccine.2021.08.049
19. Hurley, D, Griffin, C, Young, M, Scott, DA, Pride, MW, Scully, IL, et al. Safety, tolerability, and immunogenicity of a 20-valent pneumococcal conjugate vaccine (PCV20) in adults 60 to 64 years of age. Clin Infect Dis. (2021) 73:e1489–97. doi: 10.1093/cid/ciaa1045
20. Essink, B, Sabharwal, C, Cannon, K, Frenck, R, Lal, H, Xu, X, et al. Pivotal phase 3 randomized clinical trial of the safety, tolerability, and immunogenicity of 20-valent pneumococcal conjugate vaccine in adults aged ≥18 years. Clin Infect Dis. (2022) 75:390–8. doi: 10.1093/cid/ciab990
21. Klein, NP, Peyrani, P, Yacisin, K, Caldwell, N, Xu, X, Scully, IL, et al. A phase 3, randomized, double-blind study to evaluate the immunogenicity and safety of 3 lots of 20-valent pneumococcal conjugate vaccine in pneumococcal vaccine-naive adults 18 through 49 years of age. Vaccine. (2021) 39:5428–35. doi: 10.1016/j.vaccine.2021.07.004
22. Cannon, K, Elder, C, Young, M, Scott, DA, Scully, IL, Baugher, G, et al. A trial to evaluate the safety and immunogenicity of a 20-valent pneumococcal conjugate vaccine in populations of adults ≥65 years of age with different prior pneumococcal vaccination. Vaccine. (2021) 39:7494–02. doi: 10.1016/j.vaccine.2021.10.032
23. Greek Ministry of Health. National Immunization Program (NIP) for adults. (2023). Available at: www.moh.gov.gr/articles/health/dieythynsh-dhmosias-ygieinhs/emboliasmoi/ethniko-programma-emboliasmwn-epe-enhlikwn/11251-ethniko-programma-emboliasmwn-enhlikwn-2023. (accessed March 23, 2023).
24. Mendes, D, Averin, A, Atwood, M, Sato, R, Vyse, A, Campling, J, et al. Cost-effectiveness of using a 20-valent pneumococcal conjugate vaccine to directly protect adults in England at elevated risk of pneumococcal disease. Expert Rev Pharmacoecon Outcomes Res. (2022) 22:1285–95. doi: 10.1080/14737167.2022.2134120
25. Gourzoulidis, G, Tzanetakos, C, Ioannidis, I, Tsimihodimos, V, Diogo, V, Karpouzos, G, et al. Cost-effectiveness of Empagliflozin compared with Dapagliflozin for the treatment of patients with type 2 diabetes mellitus and established cardiovascular disease in Greece. Clin Drug Investig. (2021) 41:371–11. doi: 10.1007/s40261-021-01013-w
26. Gourzoulidis, G, Koulentaki, M, Koumarianou, A, Samadas, E, Androulakis, N, Xynogalos, S, et al. Cost-effectiveness of trifluridine/tipiracil as a third-line treatment of metastatic gastric cancer, including adenocarcinoma of the gastrohesophageal junction, among patients previously treated in Greece. Expert Rev Pharmacoecon Outcomes Res. (2022) 22:259–9. doi: 10.1080/14737167.2021.1921576
27. Paulden, M, and O’Mahony, J. The 2013 revision to Nice 2019;s discounting guidelines: differential discounting has gone but unjustified selective application remains. Value Health. (2013) 16:A616. doi: 10.1016/j.jval.2013.08.1785
28. Hellenic Statistical Authority (EL. STAT.). Estimated population. (2021). Available at: https://www.statistics.gr/en/home/. (accessed March 10, 2023).
29. Mangen, M-JJ, Rozenbaum, MH, Huijts, SM, van Werkhoven, CH, Postma, DF, Atwood, M, et al. Cost-effectiveness of adult pneumococcal conjugate vaccination in the Netherlands. Eur Respir J. (2015) 46:1407–16. doi: 10.1183/13993003.00325-2015
30. Klugman, KP, Madhi, SA, Huebner, RE, Kohberger, R, Mbelle, N, Pierce, N, et al. A trial of a 9-valent pneumococcal conjugate vaccine in children with and those without HIV infection. N Engl J Med. (2003) 349:1341–8. doi: 10.1056/NEJMoa035060
31. French, N, Gordon, SB, Mwalukomo, T, White, SA, Mwafulirwa, G, Longwe, H, et al. A trial of a 7-valent pneumococcal conjugate vaccine in HIV-infected adults. N Engl J Med. (2010) 362:812–2. doi: 10.1056/NEJMoa0903029
32. Patterson, S, Webber, C, Patton, M, Drews, W, Huijts, SM, Bolkenbaas, M, et al. A post hoc assessment of duration of protection in CAPiTA (community acquired pneumonia immunization trial in adults). Trials Vaccinol. (2016) 5:92–6. doi: 10.1016/j.trivac.2016.04.004
33. Djennad, A, Ramsay, ME, Pebody, R, Fry, NK, Sheppard, C, Ladhani, SN, et al. Effectiveness of 23-valent polysaccharide pneumococcal vaccine and changes in invasive pneumococcal disease incidence from 2000 to 2017 in those aged 65 and over in England and Wales. EClin Med. (2018) 6:42–50. doi: 10.1016/j.eclinm.2018.12.007
34. Olsen, J, Schnack, H, Skovdal, M, Vietri, J, Mikkelsen, MB, and Poulsen, PB. Cost-effectiveness of 20-valent pneumococcal conjugate vaccine in Denmark compared with PPV23. J Med Econ. (2022) 25:1240–54. doi: 10.1080/13696998.2022.2152235
35. Tin Tin Htar, M, Stuurman, AL, Ferreira, G, Alicino, C, Bollaerts, K, Paganino, C, et al. Effectiveness of pneumococcal vaccines in preventing pneumonia in adults, a systematic review and meta-analyses of observational studies. PLoS One. (2017) 12:e0177985. doi: 10.1371/journal.pone.0177985
36. Chandler, T, Furmanek, S, Carrico, R, Balcom, D, Arnold, F, and Ramirez, J. 23-valent pneumococcal polysaccharide vaccination does not prevent community-acquired pneumonia hospitalizations due to vaccine-type Streptococcus pneumoniae. Microorganisms. (2022) 10:10. doi: 10.3390/microorganisms10030560
37. Heo, JY, Seo, YB, Choi, WS, Lee, J, Noh, JY, Jeong, HW, et al. Cost-effectiveness of pneumococcal vaccination strategies for the elderly in Korea. PLoS One. (2017) 12:e0177342. doi: 10.1371/journal.pone.0177342
38. Smith, KJ, Wateska, AR, Nowalk, MP, Raymund, M, Lee, BY, and Zimmerman, RK. Modeling of cost effectiveness of pneumococcal conjugate vaccination strategies in U.S. older adults. Am J Prev Med. (2013) 44:373–81. doi: 10.1016/j.amepre.2012.11.035
39. Stoecker, C, Kim, L, Gierke, R, and Pilishvili, T. Incremental cost-effectiveness of 13-valent pneumococcal conjugate vaccine for adults age 50 years and older in the United States. J Gen Intern Med. (2016) 31:901–8. doi: 10.1007/s11606-016-3651-0
40. Centers for Disease Control and Prevention. Active bacterial Core surveillance (ABCs) report emerging infections program network Streptococcus pneumoniae. Atlanta: Centers for Disease Control and Prevention (2018).
41. Liapikou, A, Konstantinidis, A, Kossyvaki, V, Skiadas, J, Menegas, D, Méndez, C, et al. Pneumococcal serotypes in adults hospitalized with community-acquired pneumonia in Greece using urinary antigen detection tests: the EGNATIA study, November 2017–April 2019. Hum Vaccin Immunother. (2022) 18:2079923. doi: 10.1080/21645515.2022.2079923
42. Sisk, JE, Whang, W, Butler, JC, Sneller, VP, and Whitney, CG. Cost-effectiveness of vaccination against invasive pneumococcal disease among people 50 through 64 years of age: role of comorbid conditions and race. Ann Intern Med. (2003) 138:960–8. doi: 10.7326/0003-4819-138-12-200306170-00007
43. Mangen, M-JJ, Huijts, SM, Bonten, MJM, and de Wit, GA. The impact of community-acquired pneumonia on the health-related quality-of-life in elderly. BMC Infect Dis. (2017) 17:208. doi: 10.1186/s12879-017-2302-3
44. Melegaro, A, and Edmunds, WJ. Cost-effectiveness analysis of pneumococcal conjugate vaccination in England and Wales. Vaccine. (2004) 22:4203–14. doi: 10.1016/j.vaccine.2004.05.003
45. Greek Ministry of Health. Drug Price bulletin. (2022). Available at: https://www.moh.gov.gr/ (accessed March 1, 2023).
46. National Organisation for Healthcare Services Provision. Official web site of EOPYY. (2022). Available at: https://www.eopyy.gov.gr/ (accessed April 3, 2023).
47. Greek Ministry of Health. Diagnosis-related group (DRG). (2011). Available at: https://www.moh.gov.gr/ (accessed May 7, 2023).
48. Woods, B, Revill, P, Sculpher, M, and Claxton, K. Country-level cost-effectiveness thresholds: initial estimates and the need for further research. J Int Soc Pharmacoecon Outcom Res. (2016) 19:929–5. doi: 10.1016/j.jval.2016.02.017
49. Thokala, P, Ochalek, J, Leech, AA, and Tong, T. Cost-effectiveness thresholds: the past, the present and the future. PharmacoEconomics. (2018) 36:509–2. doi: 10.1007/s40273-017-0606-1
50. Cameron, D, and Ubels, J. On what basis are medical cost-effectiveness thresholds set? Clashing opinions and an absence of data: a systematic review. Glob Health Action. (2018) 11:1447828. doi: 10.1080/16549716.2018.1447828
51. Tzanetakos, C, and Gourzoulidis, G. Does a standard cost-effectiveness threshold exist? The case of Greece. Value Health Region Issues. (2023) 36:18–26. doi: 10.1016/j.vhri.2023.02.006
52. International Monetary Fund. World economic outlook database. (2022). Available at: https://www.imf.org/external/pubs/ft/weo/2019/02/weodata/index.aspx (accessed January 3, 2023).
53. Polistena, B, Icardi, G, Orsi, A, Spandonaro, F, di Virgilio, R, and d’Angela, D. Cost-effectiveness of vaccination with the 20-valent pneumococcal conjugate vaccine in the Italian adult population. Vaccine. (2022) 10:10. doi: 10.3390/vaccines10122032
54. Mac Mullen, M, Carballo, C, and Seyahian, E. EE390 cost-effectiveness of the 20-valent pneumococcal conjugate vaccine vs 15-valent pneumococcal conjugate vaccine for adults in Argentina. Value Health. (2022) 25:S132. doi: 10.1016/j.jval.2022.09.636
55. Smith, KJ, Wateska, AR, Nowalk, MP, Lin, CJ, Harrison, LH, Schaffner, W, et al. Cost-effectiveness of newly recommended pneumococcal vaccination strategies in older underserved minority adults in the USA. Infect Dis Ther. (2022) 11:1683–93. doi: 10.1007/s40121-022-00669-x
56. Lamnisos, D, Giannakou, K, MMJHRP, J, Giannakou, K, and Jakovljevic, M. Demographic forecasting of population aging in Greece and Cyprus: one big challenge for the Mediterranean health and social system long-term sustainability. Health Res Policy Syst. (2021) 19:1–8. doi: 10.1186/s12961-020-00666-x
57. Koutouzis, E, Daikos, G, and Dellis, C. Serotype distribution of Streptococcus pneumoniae causing invasive and non-invasive disease in children ≤ 14 years of age in Greece in the last 5 years (2015-2020). (2017). Conference E-poster PD180/, 2022 #1236 ESPID
58. Syrogiannopoulos, GA, Grivea, IN, Moriondo, M, Nieddu, F, Michoula, AN, Calabrese, MR, et al. Molecular surveillance of pneumococcal carriage following completion of immunization with the 13-valent pneumococcal conjugate vaccine administered in a 3 + 1 schedule. Sci Rep. (2021) 11:24534. doi: 10.1038/s41598-021-03720-y
59. Beck, E, Biundo, E, Devlin, N, Doherty, TM, Garcia-Ruiz, AJ, Postma, M, et al. Capturing the value of vaccination within health technology assessment and health economics: literature review and novel conceptual framework. Vaccine. (2022) 40:4008–16. doi: 10.1016/j.vaccine.2022.04.050
Keywords: PCV20, PCV15, pneumococcal disease, Greece, pneumococcal conjugate vaccines
Citation: Gourzoulidis G, Barmpouni M, Kossyvaki V, Vietri J and Tzanetakos C (2023) Health and economic outcomes of 20-valent pneumococcal conjugate vaccine compared to 15-valent pneumococcal conjugate vaccine strategies for adults in Greece. Front. Public Health. 11:1229524. doi: 10.3389/fpubh.2023.1229524
Edited by:
Minghui Li, University of Tennessee Health Science Center (UTHSC), United StatesReviewed by:
Feroze A. Ganaie, University of Alabama at Birmingham, United StatesCopyright © 2023 Gourzoulidis, Barmpouni, Kossyvaki, Vietri and Tzanetakos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: George Gourzoulidis, Z291cnpvdWxpZGlzLmdAZ21haWwuY29t; Zy5nb3Vyem91bGlkaXNAaHRlLmdy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.