 Marília Silva Paulo1,2*
Marília Silva Paulo1,2* Mariana Peyroteo1,3,4
Mariana Peyroteo1,3,4 Mélanie R. Maia3,4
Mélanie R. Maia3,4 Cara Pries5Claudia Habl5
Cara Pries5Claudia Habl5 Luís Velez Lapão1,3,4,6
Luís Velez Lapão1,3,4,6- 1CHRC, NOVA Medical School, Faculdade de Ciências Médicas, NMS, FCM, Universidade Nova de Lisboa, Lisbon, Portugal
- 2Institute of Public Health, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates
- 3UNIDEMI, Department of Mechanical and Industrial Engineering, NOVA School of Science and Technology, Universidade NOVA de Lisboa, Caparica, Portugal
- 4LASI, Laboratório Associado de Sistemas Inteligentes, Guimarães, Portugal
- 5Gesundheit Österreich GmbH (Austrian National Public Health Institute), Vienna, Austria
- 6WHO Collaborating Center for Health Workforce Policy and Planning, Instituto de Higiene e Medicina Tropical, Universidade NOVA de Lisboa, Lisbon, Portugal
Introduction: The emergence of the COVID-19 pandemic in early 2020 led countries to implement a set of public health and social measures (PHSMs) attempting to contain the spread of the SARS-CoV-2 virus. This study aims to review the existing literature regarding key results of the PHSMs that were implemented, and to identify the PHSMs considered to have most impacted the epidemiological curve of COVID-19 over the last years during different stages of the pandemic.
Methods: The PHSM under study were selected from the Oxford COVID-19 Government Response Tracker (OxCGRT), supplemented by topics presented during the Rapid Exchange Forum (REF) meetings in the scope of the Population Health Information Research Infrastructure (PHIRI) project (H2020). The evidence- based review was conducted using Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines to identify which reviews have already been published about each PHSMs and their results. In addition, two modified Delphi panel surveys were conducted among subject matter experts from 30 European countries to uphold the results found.
Results: There were 3,212 studies retrieved from PubMed, 162 full texts assessed for eligibility and 35 included in this PHSMs summary. The measures with clearest evidence on their positive impact from the evidence-based review include social distancing, hygiene measures, mask measures and testing policies. From the modified Delphi panel, the PHSMs considered most significant in the four periods analyzed were case isolation at home, face coverings, testing policy, and social distancing, respectively.
Discussion: The evidence found has significant implications for both researchers and policymakers. The study of PHSMs’ impact on COVID-19 illustrates lessons learned for future pan- and epidemics, serving as a contribution to the health systems resilience discussion. These lessons, drawn from both the available scientific evidence and the perspectives of relevant subject matter experts, should also be considered in educational and preparedness programs and activities in the public health space.
1. Introduction
Since the emergence of the COVID-19 pandemic in early 2020, countries all over the world have selected and implemented several Public Health and Social Measures (PHSMs) in the process of trying to contain the spread of the SARS-CoV-2 virus. These clusters of PHSMs have significantly impacted the population and their application has been questioned in the political, social, and economic dimension.
In the present paper, instead of non-pharmaceutical interventions (NPIs), the concept of PHSMs is used as suggested by the World Health Organization (WHO), due to its clear and inclusive characteristics that describe public health and social interventions as “measures or actions by individuals, institutions, communities, local and national governments and international bodies to slow or stop the spread of an infectious disease, such as COVID-19” (1).
Many health-related policy measures that were applied to different degrees across the world, in combination or individually, can be considered PHSMs. These are usually a set of public health and social tools that have proved effective in limiting the spread and reducing the incidence and prevalence of infections during previous epi- or pandemic outbreaks, such as influenza A H1N1 (2).
During the early stages of the SARS-CoV-2 pandemic in March–May 2020, health systems preparedness, resilience, and capacity response in terms of allocating healthcare workers to combat shortages were considered foremost priorities and received a considerable amount of political attention (3). Still, after 3 years, these issues appear not to have found reflection in mid- to long-term policies, making it imperative to question the actual preparedness of health systems for future crisis events. Several stakeholders have developed interactive maps, dashboards, and catalogs summarizing PHSMs applied per country over time (4, 5). International agencies and universities, specifically the European Center for Disease Control (ECDC) and the University of Oxford, have created interactive maps displaying the epidemiological evolution of the pandemic and the PHSMs applied by countries with the aim of informing the public. Specific platforms were also built to communicate the changeable status of specific PHSMs. As an example, Re-Open EU was launched to provide up-to-date information on applicable travel and health measures in the European Union (EU) and the Schengen Associated countries (6).
At the same time, collaborative European projects conducted by Member State institutions and supported by EU programs, have arisen to address the need for a distributed research infrastructure on population health information as well as the need for rapid ad-hoc exchanges of information on health research and policy between countries during the pandemic. The Population Health Information Research Infrastructure (PHIRI) project maintains a continuously updated database of currently applicable PHSMs pertaining to COVID-19 in the participating countries, as well as of relevant research infrastructures, national health information sources, and training resources via the public Health Information Portal (7). PHIRI also conducts bi-weekly Rapid Exchange Forum (REF) gatherings between national project members and expert stakeholders from supra-national institutions to discuss specific urgent topics (8). Questions and topics discussed during each REF meeting are based on countries’ public health institutions’ requests, reflecting their most pressing needs for ad-hoc Pan-European information exchange on national population health developments, policies and research. To date, the REF meetings have addressed such questions particularly in the scope of COVID-19 and its impact on different dimensions of population health and health systems.
Strengthening and improving the resilience of health services requires proper and focused policymaking. Therefore, it is essential to understand how health-related policies and measures helped to contain the spread of the SARS-CoV-2 virus and which combinations of measures may have had the highest positive impact.
This paper aims to review the existing literature regarding the key effects of selected PHSMs, substantiate the findings through surveys with subject matter experts, and identify the PHSMs considered to have most impacted the epidemiological curve of COVID-19 over the last years during four different periods of the pandemic.
2. Methods
To continuously map COVID-19 health-related policies, indicators and impact measures considered to influence the pandemic’s epidemiological curve were identified. Analysis of those indicators selected on the basis of relevant scientific literature and countries’ requests via the PHIRI REF mechanism, were organized by PHSMs (indicator) in an evidence-based review.
2.1. Selection of indicators
Most of the indicators were selected from the Oxford COVID-19 Government Response Tracker (OxCGRT) which was developed by the Blavatnik School of Government, University of Oxford. The OxCGRT collected publicly available information on 24 indicators of government response to the pandemic, three of which were retired before the end of the Tracker’s active collection and publication period. The indicators included containment and closure policies such as school closures and restrictions in movement, economic policies, health system policies such as the COVID-19 testing regime, emergency investments into healthcare, and vaccination policies, among others. The OxCGRT collected and published real-time updates on different policy responses from 1st January 2020 to 31st December 2022, covering more than 180 countries, coded into multiple indicators (9, 10). For this study, 13 indicators were selected from among the OxCGRT indicators, particularly its categories C (containment and closure policies) and H (health systems policies) (11). Two of the selected indicators were modified based on topics presented in and priorities identified during the REF meetings in the scope of the PHIRI project (i.e., closure of kindergartens was added to the school closures indicator; aspects of several indicators within the OxCGRT category V, vaccination policies, were collated under one indicator). Furthermore, six indicators not individually tracked in scope of the OxCGRT were added to the selected indicators through the REF meeting mechanism (i.e., Closure of non-essential shops, gastronomy and cultural venues; Access restriction to shops, gastronomy and cultural venues; Social distancing; General hygiene measures; Voluntary quarantine by contact persons; Case isolation at home), arriving in total at 19 indicators, respectively PHSMs, under study. The 19 PHSMs under study were grouped into five clusters: access measures; distancing measures; movement restrictions; test, trace, vaccinate; communication measures (please see Table 1).
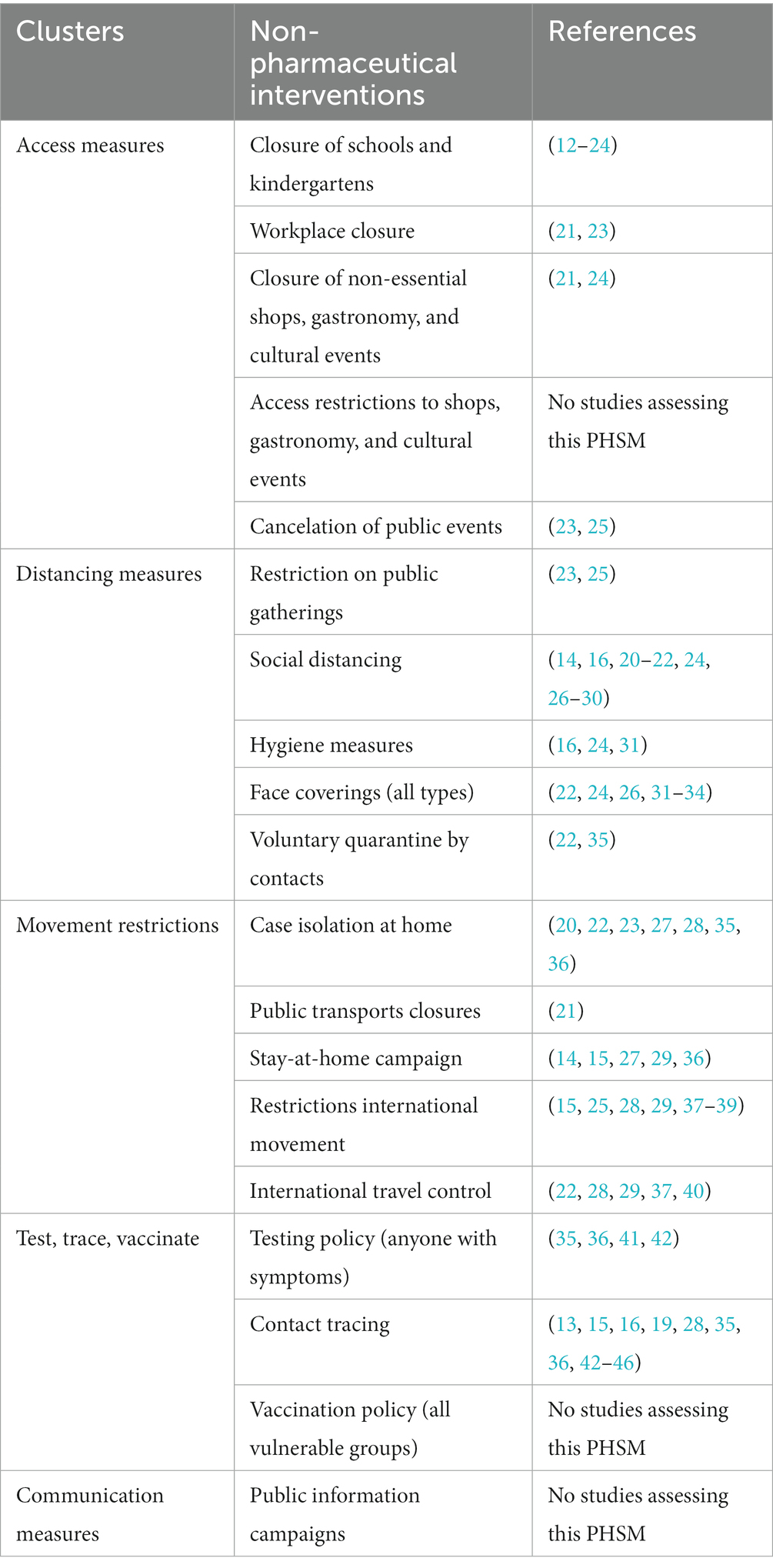
Table 1. Reviews reporting on the selected public health and social measures found.
2.2. Review of evidence research – reviews
This review of reviews aims to provide a summary of different reviews on PHSMs to answer our research question “Which PHSMs can be considered to have most impacted the epidemiological curve of COVID-19 from 2020 to 2022?.” This type of review was introduced in healthcare due to the high number of health interventions and clinical studies that exist, and the Cochrane group has described it as an Overview of Reviews (47). Review of reviews have a similar structure to systematic reviews but include reviews rather than primary studies. Therefore, we have used the PRISMA statement guidelines to report the review (48).
2.2.1. Eligibility criteria
Studies had to meet the following criteria: any type of review presenting structured methods and evidence of the impact of the selected PHSMs on reducing the epidemiologic curve of COVID-19. Exclusion criteria were a focus on the impact of PHSMs on topics outside of general population health (e.g., mental health) and on diseases other than COVID-19.
2.2.2. Information sources and search string
We developed a search string on PubMed MEDLINE using a combination of terms relating to the pandemic, the development of this search string focusing on the exposure (COVID-19) was very comprehensive: “covid 19”[Title/Abstract] OR “covid 19”[Title/Abstract] OR “covid 2019”[Title/Abstract] OR “COVID19”[Title/Abstract] OR “COVI-19”[Title/Abstract] OR “covid 2019”[Title/Abstract] OR “2019 ncov”[Title/Abstract] OR “2019 ncov”[Title/Abstract] OR “coronavirus disease 19”[Title/Abstract] OR “coronavirus disease 19”[Title/Abstract] OR “coronavirus disease 2019”[Title/Abstract] OR “coronavirus disease 2019”[Title/Abstract] OR “2019 novel Coronavirus”[Title/Abstract] OR “COVID19”[Title/Abstract] OR “coronavirus disease 2019”[Title/Abstract] OR “2019-coronavirus”[Title/Abstract] OR “coronavirus-2019”[Title/Abstract] OR “2019-coronavirus”[Title/Abstract] OR “coronavirus-2019”[All Fields] OR “SARS Coronavirus 2”[Title/Abstract] OR “sars cov 2”[Title/Abstract] OR “sars cov 2”[Title/Abstract] OR “CoV-2”[Title/Abstract] OR “COVID-2”[All Fields] OR “Wuhan coronavirus”[Title/Abstract] OR “covid 19”[MeSH Terms:noexp]. Then it was combined with all the indicators selected using the Title/Abstract term in the query box. No filters apart from limiting the search to the type of study eligible and to studies published in the English language were applied.
2.2.3. Selection process
All the citations retrieved from PubMed were uploaded into Covidence – Better systematic review management (49), which automatically removes duplicates and is ready to provide a PRISMA flowchart. A thorough screening of titles and abstracts followed by full-text screening was performed by four reviewers. Each methodological step was conducted by two independent researchers on Covidence to ensure their eligibility to be used to produce a narrative of the key results per PHMS.
2.2.4. Data items
Data was extracted using a prepared and specific sheet focusing on the type of scientific paper, the PHSMs reported, the type of review (type of study), the period where the study was conducted, the type of studies included by study design, and the number of studies included, the key results and recommendations if any. The data extraction items were tested in an excel sheet by two reviewers and then inserted into Covidence to allow double extraction. Each reviewer was blinded during the data extraction stage and a final data sheet was created highlighting any conflicts between the two extractors. The conflicts were all solved by the same author to ensure consistency. This last data extraction sheet was downloaded, and results were summarized by cluster of PHSM.
2.2.5. Study risk of bias assessment
Risk of bias in the studies included was assessed by a tool developed by Whiting and colleagues to assess the risk of bias in systematic reviews – ROBIS (50). This tool focuses on assessing four domains, comprising the adequate objectives and eligible criteria, the search and databases used, the study characteristics provided, and the synthesis of results, plus, an overall risk domain.
2.3. Modified Delphi technique
The modified Delphi technique sought to elucidate the most significant PHSMs applied in European countries during different periods of the pandemic in 2020-2021 by studying the perception of relevant subject matter experts from the PHIRI project network. The Delphi techniques are still evolving, but they can be defined as a complex method to structure group communication processes to reach a consensus, based on collected experts’ judgments (51).
2.3.1. First and second-round surveys
A two-round survey was designed and distributed to subject matter experts from all 30 countries participating in the PHIRI project. In the scope of the survey, subject matter experts were defined as members of the PHIRI project consortium and network who have been actively engaged in COVID-19 responses throughout the pandemic in the scope of research, design of policy, or advice to policymakers. This includes experts from side of national authorities such as Ministries of Health, national public health institutes, or other relevant government agencies and research institutions. In the first stage of the survey, the subject matter experts were asked to select, by way of multiple-choice questions from a list of initially 19 included measures, the three PHSMs which they considered had most impacted the epidemiological curve of COVID-19 during each period of the pandemic (March–May 2020, September 2020–February 2021, March–May 2021 and October–December 2021). After receiving the responses from the first round, analysis was performed. All the PHSMs that were selected among the most impactful measures by the majority of respondents of the first survey were taken forward for inclusion in the second round. The second survey was created from the resulting list of PHSMs per surveyed period, and again distributed to all members of the PHIRI project network. In this second survey, subject matter experts from each PHIRI member country were asked to rank the remaining PHSMs in order of their relative importance to decreasing or controlling the epidemiological curve of COVID-19 in each period of the pandemic, to arrive at a ranking of PHSMs deemed most impactful overall in each period by participants of the Delphi Panel.
3. Results
3.1. Evidence-based review
The search performed identified 3,212 citations. After duplicate removal, 3,050 were considered ineligible at the titles and abstract screening stage, 162 were screened for full-text and 35 were included (Figure 1).
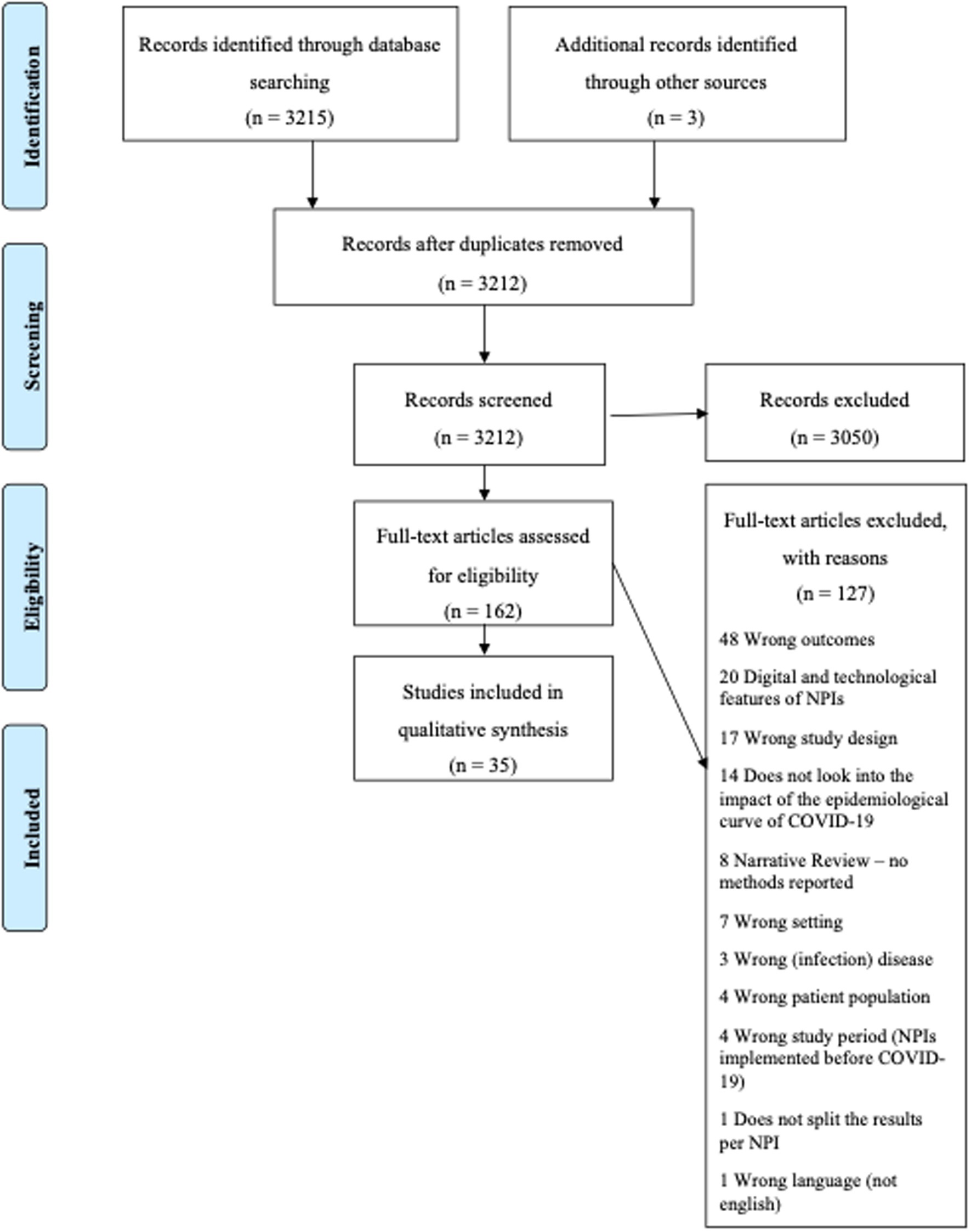
Figure 1. PRISMA-flow chart.
Of the 35 studies included, 16 were systematic reviews, 7 were systematic reviews and meta-analyses, 8 were rapid reviews, three were scoping reviews, and one was an evidence-based review. The number of papers included in these studies varied from 9 to 90 and all reviews addressed multiple countries. Most of the studies, 17 reviews, examined more than one PHSM in the same paper. The most studied PHSM was social distancing (Table 2).
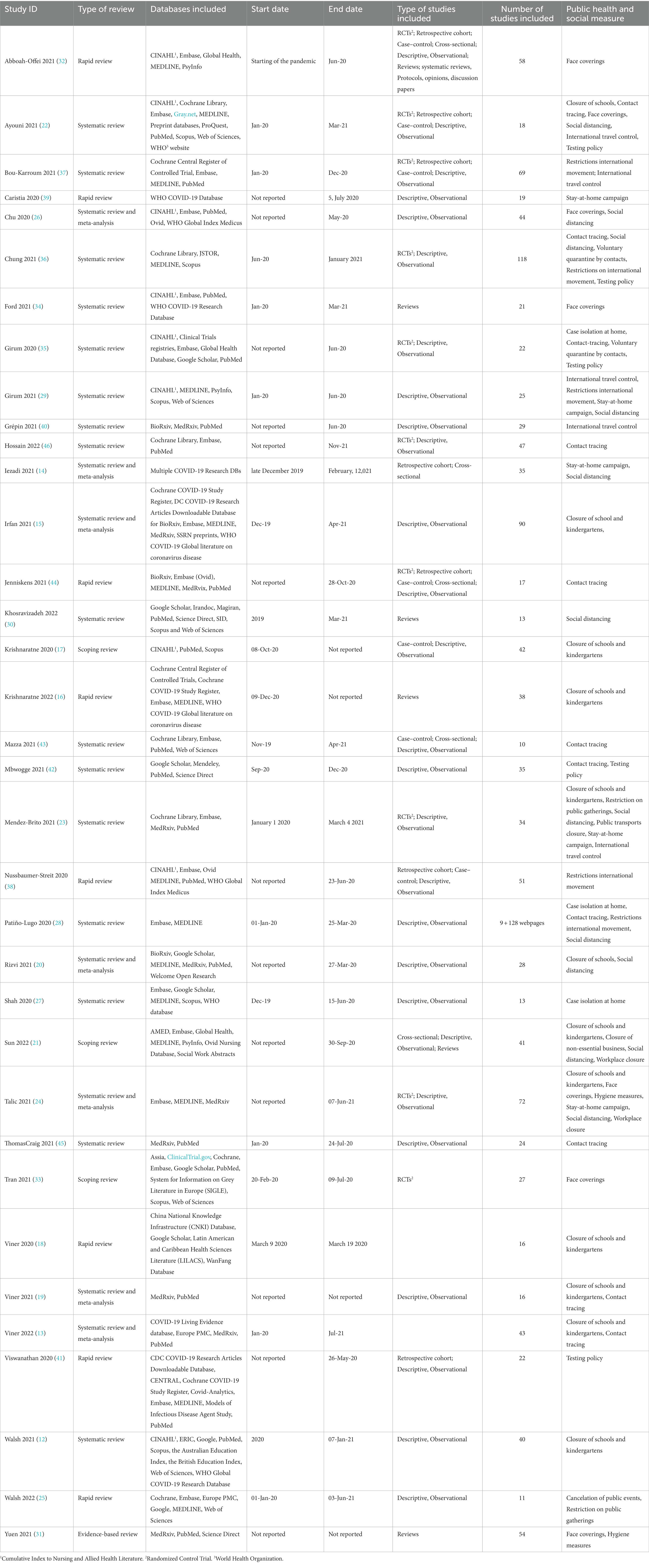
Table 2. Table of characteristics of the studies included.
Of the studies included, 23 (64%) had performed risk of bias assessment and another 23 (64%) had performed quality of evidence assessment of the studies included in their analysis (either quantitative or qualitative). From the risk of bias assessment performed, we assessed 33 studies as overall low risk of bias and two studies as unclear risk. The domains that contained more concerns were related to the search and the selection of databases (“Did the search include all appropriate range of databases for published and unpublished studies? Were methods additional to database search used to identify relevant reports?”) and to the sufficient studies characteristics available (“Were sufficient study characteristics available for both review authors and readers to be able to interpret the results?”). Please see the Supplementary material for a detailed risk of bias assessment.
The results are organized by PHSM, providing a summary of evidence on each measure. Table 1 shows an overview of the studies included for each PHSM.
3.1.1. Access measures
Thirteen studies assessed the impact of school and kindergarten closure on the transmission and incidence of SARS-CoV-2 (12–24). Six studies recommend the implementation of this PHSM with caution (12, 16, 20, 22–24) and four showed inconclusive results because it must be considered that the studies evaluated a set of combined measures (e.g., social distancing) and not this measure alone (13, 17, 19, 21). Nevertheless, eight studies showed evidence of positive impact on the epidemiological curve when the measure was implemented in periods of low incidence of SARS-CoV-2. One study assessed the impact of workplace closures, whereby it was possible to conclude that implementing this measure had a moderate impact on reducing transmission (21). As for the closure of non-essential shops, gastronomy and cultural events, two studies reported a significant reduction (between 12 and 29%) in SARS-CoV-2 transmission associated with this measure (21, 24). In the studies reviewed, there was no assessment of the impact of canceling public events on reducing the epidemiological curve of COVID-19.
3.1.2. Distancing measures
The most frequently implemented measures during public gatherings were providing hand disinfectant, wearing face masks, ensuring adequate ventilation, symptoms screening (i.e., temperature, symptom, travel, or close contact screening) and contact tracing. One study presented evidence that implementing a range of PHSMs can reduce the risk of SARS-CoV-2 transmission at mass gatherings (25); however, this risk is unlikely to be eliminated. All studies adopted a layered mitigation approach involving multiple public health measures; therefore, the effectiveness of any single measure under the umbrella of restrictions on public gatherings could not be determined. Some studies considered physical distancing, quarantine and contact tracing as part of the results analysis of social distancing (24, 26). For hygiene measures, the interventions studied fell into three broad categories: the main use of hand sanitizers, the use of soap, and those that provided education on hygiene practices only (24, 31). Further recommendations to be applied in specific contexts such as using gloves, gowns, and eye protection, saline nasal washing and gargling were also identified. From the included studies, we can infer that the implementation of hygiene measures had an impact on reducing the incidence of COVID-19. In addition, one study evaluated surface disinfection with chlorine or ethanol-based disinfectant, concluding its effectiveness in reducing SARS-CoV-2 transmission (24). There was consensus among 10 studies that using face covering reduces the risk of transmission, incidence, mortality, and hospitalization for COVID-19 (22, 24, 26, 31–34). The impact of not using a mask, using a face mask, surgical or medical masks, and N95 masks were analyzed. The latter may be associated with a greater risk reduction compared to surgical or similar masks according to included studies, particularly when mandatory use of N95 masks is implemented (26, 33). Five included studies demonstrated that voluntary quarantine by contacts effectively suppressed transmission of COVID-19 in conjunction with contact tracing. However, one study reports that particular consideration needs to be given to providing appropriate measures for vulnerable populations, as quarantine and screening may not be sufficient to address their needs (27).
3.1.3. Movement restrictions
As with voluntary quarantine of close contacts, case isolation at home was shown to be effective in suppressing transmission of COVID-19 (20, 22, 23, 27, 28, 35, 36). However, the effectiveness of this measure has been questioned with increasing evidence of natural immunity and disease resistance.
The two studies that analyzed the impact of the public transport closure did not show any significant difference in the progression of the epidemiological curve associated with this measure (21, 23). This may have been due to other measures already implemented during the studied time periods (resulting in low public transport congestion and face masks worn on public transport). One of the studies included an analysis of 12 papers, of which only one found an association between public transport closures and the reproduction number, growth rate, or case-related outcomes of COVID-19 (23).
The stay-at-home campaign focused on two complementary measures: lockdown and quarantine. Regarding the impacts of lockdown, all the studies that evaluated stay-at-home or isolation measures reported reductions in transmission, incidence, hospital and ICU admissions, and deaths from SARS-CoV-2. One of the studies reported that a combination of four measures, including restrictions on mass gatherings, school closures, workplace closures, and lockdowns in 32 countries, was associated with decreased incidence of COVID-19 (21). A similar decreasing incidence was observed when public transport closures were added. Quarantine was reviewed in two studies, which concluded that its implementation reports a decrease in the incidence of COVID-19.
The effectiveness of travelers’ quarantine and the need for arrival or exit screening were examined as measures to restrict international movement. Included studies show that the effectiveness of traveler quarantine depends on compliance and increases when traveler quarantine is implemented as a mandatory measure. Four studies demonstrate quarantine’s impact, especially for travelers from countries with a high prevalence of SARS-CoV-2 and detecting new cases that were initially negative (22, 36–38). In addition, it was found that reopening borders without travelers’ quarantine measures rapidly increased the number of new cases of COVID-19 (37). Studies also showed that screening travelers allowed for a delay in the next epidemic peak and a reduction in the number of cases compared to earlier peaks. However, in two separate countries lifting travel restrictions did not increase the number of cases when accompanied by other measures of physical distancing and quarantine of travelers. Complementarity of measures, such as quarantine and screening, showed a high impact in reducing the number of cases, mainly when screening was performed before day 14 of quarantine.
The included studies on international travel control measures, such as travel restrictions and border closure measures, showed mixed results in the association between border closure and reduction of critical cases or overall mortality from COVID-19 (22, 28, 29, 37, 40). On one hand, reducing transmission between countries appears to be more effective through border closures than screening for symptoms at airports, and is particularly useful in the early phase of an outbreak before the widespread distribution of the disease (36). On the other hand, border restrictions in combination with other measures (quarantine, isolation, social distancing, closure of schools and workplaces, working from home, and restrictions on internal movement) show that together these measures were effective in reducing the number of cases of COVID-19, but could not isolate the impact of international travel control measures. Additionally, one study presented inconclusive results in analyzing domestic and international travel restrictions (38).
3.1.4. Test, trace, and vaccinate
Specific to testing policies, most of the studies reviewed conclude that testing policies (along with case isolation, social distancing, and face masks) can effectively control a new outbreak of COVID-19. However, a study assessing the accuracy of screening strategies showed inconclusive results on the usefulness of combined screening, repeated symptom assessment, and rapid laboratory tests (41).
As for contact tracing, the nine studies included in this analysis showed the usefulness and benefits that digital tools – Contact Tracking Apps (CTA) with text warning systems – could have in managing an outbreak. Despite promising results on contact tracing policies, two studies highlight that for the results to be effective, these apps need to provide faster feedback on a positive test result and notify close contacts (42, 43). Two other studies mention the need for a high app usage rate (44, 45). Another study mentions that CTA must be combined with other interventions (such as social distancing and random testing) to reduce the epidemiological curve of SARS-CoV-2.
Combining both measures is essential, as one study found that each new case requires an average of 36 individuals to be analyzed, and laboratory testing (within 2 h) can increase the efficiency of this process (35). Vaccination policy in terms of the polices and strategies to vaccinate all or certain groups of the population was not addressed in any eligible studies included in this review.
3.1.5. Communication measures
Another PHSM that we investigated were public information campaigns, but there were no available studies describing the impact of public health campaigns on the epidemiological curve of COVID-19.
3.2. Modified Delphi technique
The first round of the survey received responses from subject matter experts from Belgium, Bosnia Herzegovina, Croatia, Estonia, Hungary, Italy, Norway, Portugal, Romania, Slovakia, Slovenia and Spain. For the period of March to May 2020, the PHSM considered most impactful among those implemented during this period were Stay-at-home campaigns with a relative majority of 45% survey participants choosing this measure in their responses. For the period of September 2020 to February 2021, the PHSMs deemed most impactful by respondents were “face coverings (of all types)” and “case isolation at home” each chosen by 45% of participants, respectively. For the period of March to May 2021 the PHSM deemed impactful by the highest number of respondents was “vaccination policy” chosen by 68% of participants. Finally, for the period of October to December 2021, the PHSM considered most important overall was again “vaccination policy,” chosen by 68% of participants. Results are presented in Figure 2.
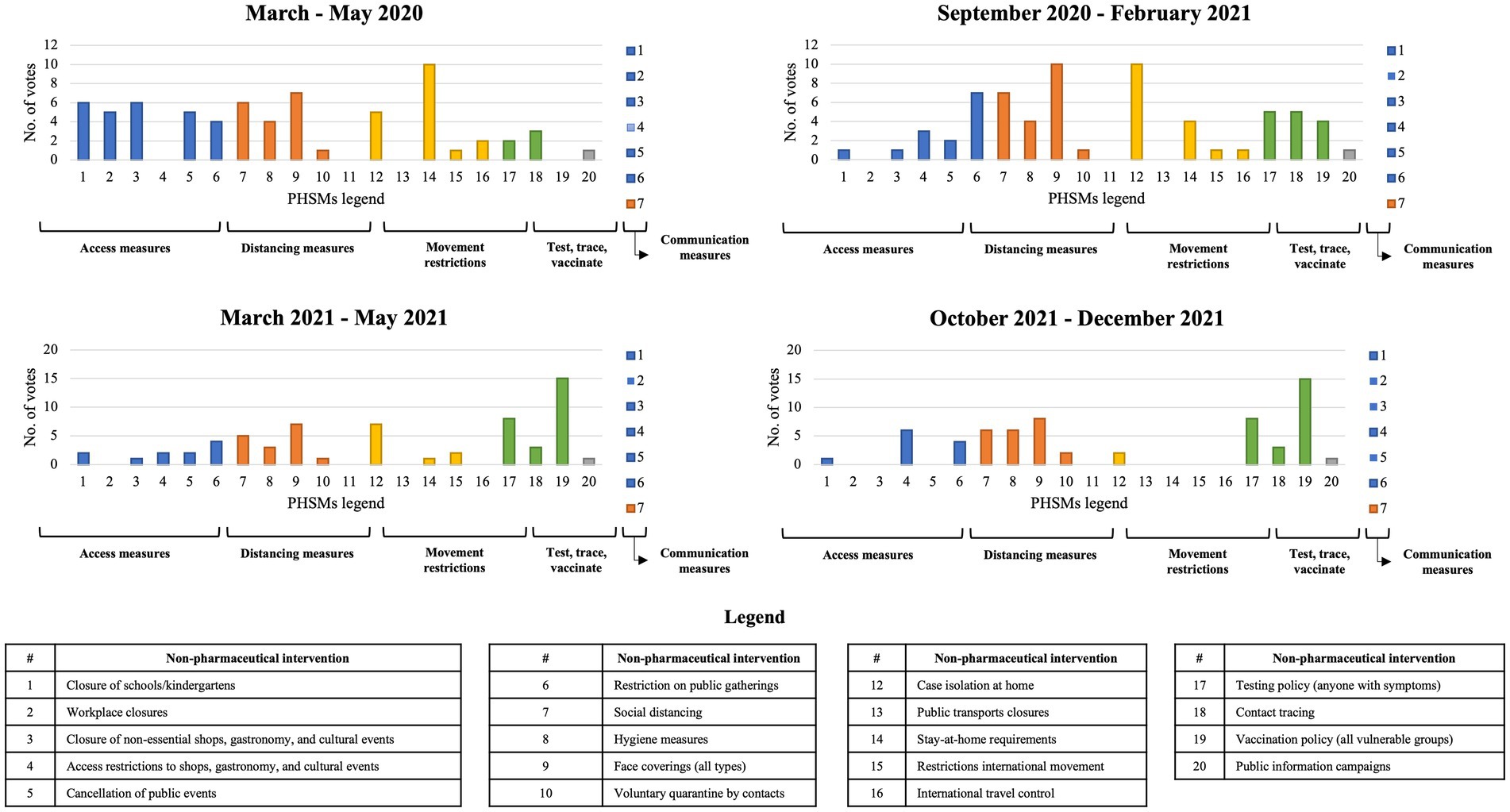
Figure 2. Results from the first Delphi technique round.
The second round of the survey received responses from subject matter experts from Albania, Austria, Belgium, Croatia, France, Italy, Norway, Portugal, Slovakia, Spain, and Sweden Public Health Experts. For the period of March to May 2020, the PHSM considered most impactful was “case isolation at home” as chosen by 50% of participants. For the period of September 2020 to February 2021, respondents considered “face coverings (of all types)” as the most relevant measure with 29% of participants choosing this option. For the period of March to May 2021, the PHSM considered most impactful was “testing policy” chosen by 21% of participants, followed by a tie between social distancing and vaccination policy. Finally, for the period of October to December 2021, the PHSM considered most impactful was “social distancing” chosen by 36% of participants, followed by vaccination policy (29%). Results are presented in Figure 3.
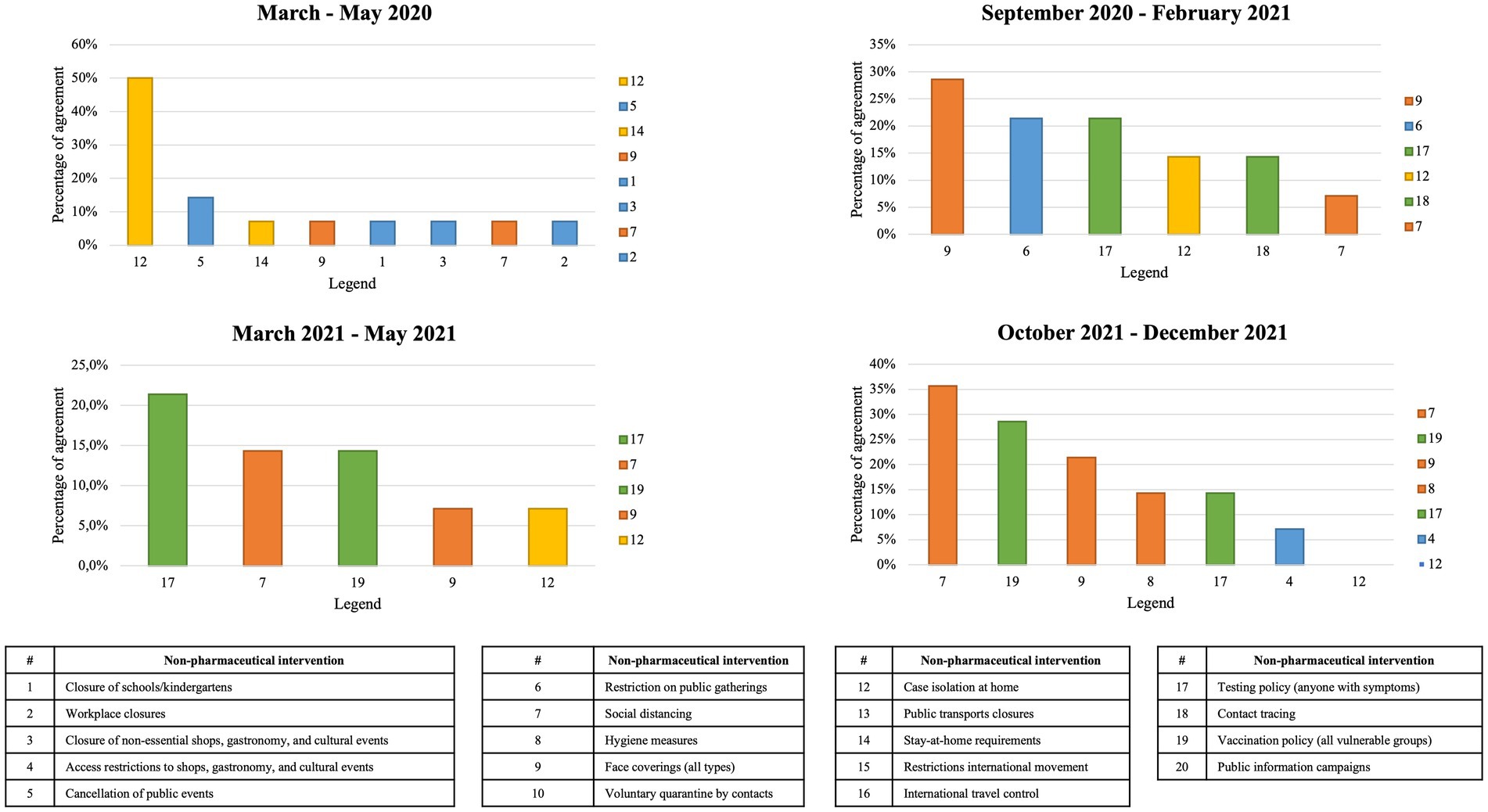
Figure 3. Results from the second modified Delphi technique round.
4. Discussion
4.1. Key findings
PHSM are key interventions at the disposal of policymakers in the public health space to address an epi- or pandemic, to limit spread of infectious disease, and to mitigate its impact. From this review, and in the context of COVID-19, one could consider that there are three sets of PHSMs, distinguished by different levels of evidence currently available regarding their impact: one set of PHSMs where there is clear evidence, one set with just moderate evidence, and another with to date still little evidence on their impact.
PHSMs with clear evidence of positive impact from the literature review are closure of non-essential shops, gastronomy and cultural events, hygiene measures, face coverings, voluntary quarantine by contacts, case isolation at home, stay-at-home campaign, restrict internal movement, and testing policies.
PHSMs with a moderate level of evidence, often to be implemented as a combined intervention are workplace closure, restrictions on public gatherings, social distancing, international travel control measures and contact tracing.
PHSMs with little evidence available to date, eventually requiring more studies are closure of schools and kindergartens, cancelation of public events, public transport closure, vaccination policy strategies, and public information campaigns.
Overall, combined interventions have shown to be effective and have a high impact in reducing the transmissibility of the disease, the collapse of health care services, and mortality (28).
Another interesting result lies in the comparison of evidence from the rapid review with the perceptions reported by subject matter experts via the modified Delphi panel technique. During the initial period (from March to May 2020), the PHSM identified as most impactful by subject matter experts was “case isolation at home,” which fits well with the evidence presented in the review and illustrates a strong focus during this period of the pandemic on measures that restricted people from their usual movements and activities.
In the next period (from September 2020 to February 2021), the PHSM identified as most impactful by the experts were “face coverings (of all types),” again aligning with the evidence drawn from the rapid review and representing a shift in focus during this period of the pandemic toward measures that would allow people to leave their homes and be somewhat active while still engaging in preventative measures.
In the following period (from March to May 2021), the PHSM considered most impactful by experts was “testing policy,” followed by a tie between social distancing and vaccination policy, representing a stage of the pandemic where societies were forced to adopt – and continuously adapt – different parallel clusters of measures to keep functioning. It was also the period when COVID-19 vaccination first became available to the population.
In the last surveyed period (from October to December 2021), the PHSM identified as most impactful by experts was “social distancing,” followed by vaccination policy. With most populations already vaccinated at this stage, this result seems to point toward a focus on avoiding infections among vaccinated people, as well as a continued prioritization of raising immunization rates in populations with still low rates of vaccination. Interestingly, the fact that we do not have vaccination policy studies focusing on priorities of the population to be vaccinated, just vulnerable groups vs. all, including children or not, reflected on the need of further studies as the vaccination policies rather just on the vaccines efficacy itself.
The review also identified a set of PHSMs that still require more study to determine their impact during the SARS-CoV-2 pandemic and potential utility in subsequent outbreaks. For instance, the use of contact tracing apps could represent an important tool in the future if their present limitations are addressed, and no eligible studies were identified in scope of this paper which examined the impact of communication measures, such as public information campaigns, pointing to the need for further research. Information technologies are still to make a difference; therefore it represents an area where researchers and policymakers should pay more attention and eventually invest more.
4.2. Lessons learned and future implications
The study of PHSMs’ impact on COVID-19 provides significant lessons learned for the expected next pandemic. These lessons should be integrated into both education- and preparedness programs in the public health space, as well as informing the policy decision process in acute phases of a comparable health crisis.
Besides PHIRI, several other European projects and activities have been initiated to address the impact of the COVID-19 pandemic and provide evidence-based support for future decision-making regarding the implementation of effective PHSMs across the region. A closer future collaboration between some of these projects and entities, as well as between the projects and national policymakers across Europe, could both stimulate wider scientific discussion and build additional resilience to fight future health crises armed with learnings from the previous pandemic. Notable European projects and programs in this domain include HERA (European Health Emergency Preparedness and Response Authority), VACCELERATE (Vaccine Infrastructures and Communication for Europe), COVID-19 Social Sciences Research Tracker, RECOVER-E (Rapid European COVID-19 Emergency Research response), CoVaRR-Net (COVID-19 Vaccine-induced Immunity, Variants, and Re-infections Network), and EPIPose (Epidemic Intelligence to Minimize COVID-19 Impacts on European Society, Public Health and the Economy).
When considering the policymakers perspectives, it is clear how the evidence during the COVID-19 pandemic was used – not only taking into consideration its absolute scientific validity but also the social context, whereby the evolution of PHSMs’ relevance follows the pandemic stages and shows a shifting focus on different dimensions of PHSMs over time, alongside new epidemiological developments as well as an evolving societal understanding of and amenability to different measures. Considering the available scientific evidence on PHSMs’ impact, as well as the subjective perspectives of subject matter experts who advise health policy, has allowed the present study to form a nuanced understanding of different measures’ significance over time and to highlight the complex overlapping dimensions of decision-making during a pandemic, which can be taken into account both by national policymakers and the experts engaged in counseling policy during future health crises. For this reason, analyses such as the one conducted in the scope of this paper can form a vital building block in informing health policy processes going forward.
4.3. Strengths and limitations
During the COVID-19 pandemic, thousands of scientific papers were published at a very fast pace, particularly in 2020 and 2021, making it difficult to assess and identify the key results to aid decision-making. The choice of performing a review of reviews, therefore, presents as a strength to summarize which PHSMs have most impacted the COVID-19 pandemic in Europe according to available evidence. The second strength to highlight is the use of the PHIRI REF network to engage subject matter experts in the modified Delphi panel, as they represent relevant expertise from many different European Member States and associated countries.
A limitation regarding the rapid review lies in some of the characteristics of available studies that were considered for inclusion. A good proportion of the excluded studies focused exclusively on the impact of PHSMs on outcomes related to anxiety, depression, loneliness and other aspects of mental health, thereby failing to meet the eligibility criteria as defined in the Methods chapter. Many studies conducted at the beginning of the pandemic were solely based on modeling approaches, i.e., intended to support only short-term decision-making. Among observational and modeling studies, we have extracted data only from observational studies. Another limitation of the review lies in the often mutually confounding nature of the PHSMs under study and is reflected in the fact that the available literature often examined a combination of measures from multiple clusters as defined in this paper. However, this circumstance simultaneously presents a strength: While it limits the ability of this study to rank individual PHSMs by the size of their impact on reducing the epidemiological curve of COVID-19 in absolute terms, it allows for observations on the complex interplay of available measures and their effects during different periods of the pandemic that hold meaningful lessons for researchers and policy makers in context of future outbreaks.
In terms of limitations affecting the methodology of the modified Delphi panel survey technique, the subject matter experts’ opinions and views do not represent official data from their countries but personal perception, and this can be seen as a limitation due to the resulting subjectivity. However, in addressing this limitation, we maintain that policy decisions, especially during a fast-moving crisis, are often based on the perception of relevant subject matter experts and the policymakers they advise. Studying the subjective perception of relevant experts in the field, therefore, provides a significant complement and substantiation – another piece of the evidence puzzle – to the results of the literature review.
5. Conclusion
The review identified one set of PHSMs with clear evidence of their positive impact – including closure of non-essential shops, gastronomy and cultural events, hygiene measures, face coverings, voluntary quarantine by contacts, case isolation at home, Stay-at-home campaign, restrict internal movement and testing policies – and another set of PHSMs with moderate available evidence, including workplace closure, restrictions on public gatherings, social distancing, international travel control measures, and contact tracing. Furthermore, evidence from the published literature appears to be largely congruent with the studied perceptions of national subject matter experts from European countries who were actively engaged in research, policy and policy advice during the pandemic. This knowledge is very important for public health decision-makers to be better prepared for the next pandemic.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
MSP, LL, and CP conceptualized the manuscript. MSP designed the search string. MSP, LL, MM, and MP have screened and extracted data. MSP and CP designed the modified Delphi surveys. MSP and MP wrote the draft of the manuscript. All authors revised the manuscript and approved its final version.
Funding
This project has received funding from the European Union’s Horizon 2020 research and innovation program under grant agreement No. 101018317. The present publication was also funded by Fundação Ciência e Tecnologia, IP national support through CHRC (UIDP/04923/2020).
Acknowledgments
All authors would like to acknowledge the EU, H2020 project PHIRI. MSP, MM, MP, and LL would like to acknowledge the student Willie Bernardi for its help in extracting data for the study. MM and LL would like to acknowledge Fundação para a Ciência e a Tecnologia (FCT – MCTES) for its financial support via the project UIDB/00667/2020 and UIDP/00667/2020 (UNIDEMI).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1226922/full#supplementary-material
References
1. World Health Organization . (2023). Public Health and Social Measures. Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/phsm (Accessed May 17, 2023)
2. Cowling, BJ, Ali, ST, Ng, TWY, Tsang, TK, Li, JCM, Fong, MW, et al. Impact assessment of non-pharmaceutical interventions against coronavirus disease 2019 and influenza in Hong Kong: an observational study. Lancet Public Health. (2020) 5:e279–88. doi: 10.1016/S2468-2667(20)30090-6
3. Aristodemou, K, Buchhass, L, and Claringbould, D. The COVID-19 crisis in the EU: the resilience of healthcare systems, government responses and their socio-economic effects. Eurasian Econ Rev. (2021) 11:251–81. doi: 10.1007/s40822-020-00162-1
4. Ivanković, D, Barbazza, E, Bos, V, Fernandes, ÓB, Gilmore, KJ, Jansen, T, et al. Features constituting actionable COVID-19 dashboards: descriptive assessment and expert appraisal of 158 public web-based COVID-19 dashboards. J Med Internet Res. (2021) 23:e25682. doi: 10.2196/25682
5. Khodaveisi, T, Dehdarirad, H, Bouraghi, H, Mohammadpour, A, Sajadi, F, and Hosseiniravandi, M. Characteristics and specifications of dashboards developed for the COVID-19 pandemic: a scoping review. J Public Health. (2023):1–22. doi: 10.1007/S10389-023-01838-Z/FIGURES/3
6. European Union . (2020). Re-open EU. Available at: https://reopen.europa.eu/en (Accessed July 11, 2022)
7. European Health Information Portal . (2021). Health Information Portal | European Health Information Portal. Available at: https://www.healthinformationportal.eu/health-information-portal (Accessed August 10, 2022)
8. Population Health Information Research Infrastructure . (2021). The PHIRI project | phiri.eu. Available at: https://www.phiri.eu/ (Accessed August 10, 2022)
9. Hale, Thomas, Angrist, Noam, Cameron-Blake, Emily, Hallas, Laura, Kira, Beatriz, Majumdar, Saptarshi, et al. (2020). Coronavirus government response tracker | Blavatnik School of Government. Oxford COVID-19 government response tracker. Available at: https://www.bsg.ox.ac.uk/research/research-projects/coronavirus-government-response-tracker (Accessed January 11, 2021)
10. University of Oxford . (2021). World’s first COVID-19 government response tracker launched today | Blavatnik School of Government. Available at: https://www.bsg.ox.ac.uk/research/research-projects/covid-19-government-response-tracker (Accessed October 4, 2021)
11. GitHub . (2023). OxCGRT/covid-policy-tracker…GitHub. Available at: https://github.com/OxCGRT/covid-policy-tracker/blob/master/documentation/codebook.md (Accessed May 17, 2023)
12. Walsh, S, Chowdhury, A, Braithwaite, V, Russell, S, Birch, JM, Ward, JL, et al. Do school closures and school reopenings affect community transmission of COVID-19? A systematic review of observational studies. BMJ Open. (2021) 11:e053371. doi: 10.1136/BMJOPEN-2021-053371
13. Viner, R, Waddington, C, Mytton, O, Booy, R, Cruz, J, Ward, J, et al. Transmission of SARS-CoV-2 by children and young people in households and schools: a meta-analysis of population-based and contact-tracing studies. J Infect. (2022) 84:361–82. doi: 10.1016/J.JINF.2021.12.026
14. Iezadi, S, Gholipour, K, Azami-Aghdash, S, Ghiasi, A, Rezapour, A, Pourasghari, H, et al. Effectiveness of non-pharmaceutical public health interventions against COVID-19: a systematic review and meta-analysis. PLoS One. (2021) 16:e0260371. doi: 10.1371/JOURNAL.PONE.0260371
15. Irfan, O, Li, J, Tang, K, Wang, Z, and Bhutta, ZA. Risk of infection and transmission of SARS-CoV-2 among children and adolescents in households, communities and educational settings: a systematic review and meta-analysis. J Glob Health. (2021) 11:1–15. doi: 10.7189/JOGH.11.05013
16. Krishnaratne, S, Littlecott, H, Sell, K, Burns, J, Rabe, JE, Stratil, JM, et al. Measures implemented in the school setting to contain the COVID-19 pandemic. Cochrane Database Syst Rev. (2022) 1:CD015029. doi: 10.1002/14651858.CD015029
17. Krishnaratne, S, Pfadenhauer, LM, Coenen, M, Geffert, K, Jung-Sievers, C, Klinger, C, et al. Measures implemented in the school setting to contain the COVID-19 pandemic: a rapid scoping review. Cochrane Database Syst Rev. (2020) 12:CD013812. doi: 10.1002/14651858.CD013812
18. Viner, RM, Russell, SJ, Croker, H, Packer, J, Ward, J, Stansfield, C, et al. School closure and management practices during coronavirus outbreaks including COVID-19: a rapid systematic review. Lancet Child Adolesc Health. (2020) 4:397–404. doi: 10.1016/S2352-4642(20)30095-X
19. Viner, RM, Mytton, OT, Bonell, C, Melendez-Torres, GJ, Ward, J, Hudson, L, et al. Susceptibility to SARS-CoV-2 infection among children and adolescents compared with adults: a systematic review and meta-analysis. JAMA Pediatr. (2021) 175:143–56. doi: 10.1001/JAMAPEDIATRICS.2020.4573
20. Rizvi, RF, Craig, KJT, Hekmat, R, Reyes, F, South, B, Rosario, B, et al. Effectiveness of non-pharmaceutical interventions related to social distancing on respiratory viral infectious disease outcomes: a rapid evidence-based review and meta-analysis. SAGE Open Med. (2021) 9:205031212110229. doi: 10.1177/20503121211022973
21. Sun, KS, Lau, TSM, Yeoh, EK, Chung, VCH, Leung, YS, Yam, CHK, et al. Effectiveness of different types and levels of social distancing measures: a scoping review of global evidence from earlier stage of COVID-19 pandemic. BMJ Open. (2022) 12:e053938. doi: 10.1136/BMJOPEN-2021-053938
22. Ayouni, I, Maatoug, J, Dhouib, W, Zammit, N, Ben, FS, Ghammam, R, et al. Effective public health measures to mitigate the spread of COVID-19: a systematic review. BMC Public Health. (2021) 21:1015. doi: 10.1186/S12889-021-11111-1
23. Mendez-Brito, A, El Bcheraoui, C, and Pozo-Martin, F. Systematic review of empirical studies comparing the effectiveness of non-pharmaceutical interventions against COVID-19. J Infect. (2021) 83:281–93. doi: 10.1016/J.JINF.2021.06.018
24. Talic, S, Shah, S, Wild, H, Gasevic, D, Maharaj, A, Ademi, Z, et al. Effectiveness of public health measures in reducing the incidence of COVID-19, SARS-CoV-2 transmission, and COVID-19 mortality: systematic review and meta-analysis. BMJ. (2021) 375:e068302. doi: 10.1136/BMJ-2021-068302
25. Walsh, KA, Tyner, B, Broderick, N, Harrington, P, O’Neill, M, Fawsitt, CG, et al. Effectiveness of public health measures to prevent the transmission of SARS-CoV-2 at mass gatherings: a rapid review. Rev Med Virol. (2022) 32:2285. doi: 10.1002/RMV.2285
26. Chu, DK, Akl, EA, Duda, S, Solo, K, Yaacoub, S, Schünemann, HJ, et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet. (2020) 395:1973–87. doi: 10.1016/S0140-6736(20)31142-9
27. Shah, K, Saxena, D, and Mavalankar, D. Secondary attack rate of COVID-19 in household contacts: a systematic review. QJM. (2020) 113:841–50. doi: 10.1093/QJMED/HCAA232
28. Patiño-Lugo, DF, Vélez, M, Salazar, PV, Vera-Giraldo, CY, Vélez, V, Marín, IC, et al. Non-pharmaceutical interventions for containment, mitigation and suppression of COVID-19 infection. Colomb Med. (2020) 51:1–25. doi: 10.25100/CM.V51I2.4266
29. Girum, T, Lentiro, K, Geremew, M, Migora, B, Shewamare, S, and Shimbre, MS. Optimal strategies for COVID-19 prevention from global evidence achieved through social distancing, stay at home, travel restriction and lockdown: a systematic review. Arch Public Health. (2021) 79:1–18. doi: 10.1186/S13690-021-00663-8/TABLES/3
30. Khosravizadeh, O, Ahadinezhad, B, Maleki, A, Najafpour, Z, and Golmohammadi, R. Social distance capacity to control the COVID-19 pandemic: a systematic review on time series analysis. Int J Risk Saf Med. (2022) 33:5–22. doi: 10.3233/JRS-210037
31. Yuen, E, Fried, J, Salvador, C, Gudis, DA, Schlosser, RJ, Nguyen, SA, et al. Nonpharmacological interventions to reduce respiratory viral transmission: an evidence-based review with recommendations. Rhinology. (2021) 59:114–32. doi: 10.4193/RHIN20.563
32. Abboah-Offei, M, Salifu, Y, Adewale, B, Bayuo, J, Ofosu-Poku, R, and Opare-Lokko, EBA. A rapid review of the use of face mask in preventing the spread of COVID-19. Int J Nurs Stud Adv. (2021) 3:100013. doi: 10.1016/J.IJNSA.2020.100013
33. Tran, TQ, Mostafa, EM, Tawfik, GM, Soliman, M, Mahabir, S, Mahabir, R, et al. Efficacy of face masks against respiratory infectious diseases: a systematic review and network analysis of randomized-controlled trials. J Breath Res. (2021) 15:ac1ea5. doi: 10.1088/1752-7163/AC1EA5
34. Ford, N, Holmer, HK, Chou, R, Villeneuve, PJ, Baller, A, van Kerkhove, M, et al. Mask use in community settings in the context of COVID-19: a systematic review of ecological data. EClinicalMedicine. (2021) 38:101024. doi: 10.1016/j.eclinm.2021.101024
35. Girum, T, Lentiro, K, Geremew, M, Migora, B, and Shewamare, S. Global strategies and effectiveness for COVID-19 prevention through contact tracing, screening, quarantine, and isolation: a systematic review. Trop Med Health. (2020) 48:91. doi: 10.1186/S41182-020-00285-W
36. Chung, SC, Marlow, S, Tobias, N, Alogna, A, Alogna, I, You, SL, et al. Lessons from countries implementing find, test, trace, isolation and support policies in the rapid response of the COVID-19 pandemic: a systematic review. BMJ Open. (2021) 11:e047832. doi: 10.1136/BMJOPEN-2020-047832
37. Bou-Karroum, L, Khabsa, J, Jabbour, M, Hilal, N, Haidar, Z, Abi Khalil, P, et al. Public health effects of travel-related policies on the COVID-19 pandemic: a mixed-methods systematic review. J Infect. (2021) 83:413–23. doi: 10.1016/J.JINF.2021.07.017
38. Nussbaumer-Streit, B, Mayr, V, Dobrescu, AI, Chapman, A, Persad, E, Klerings, I, et al. Quarantine alone or in combination with other public health measures to control COVID-19: a rapid review. Cochrane Database Syst Rev. (2020) 2020:CD013574. doi: 10.1002/14651858.CD013574
39. Caristia, S, Ferranti, M, Skrami, E, Raffetti, E, Pierannunzio, D, Palladino, R, et al. Effect of national and local lockdowns on the control of COVID-19 pandemic: a rapid review. Epidemiol Prev. (2020) 44:60–8. doi: 10.19191/EP20.5-6.S2.104
40. Grépin, KA, Ho, TL, Liu, Z, Marion, S, Piper, J, Worsnop, CZ, et al. Evidence of the effectiveness of travel-related measures during the early phase of the COVID-19 pandemic: a rapid systematic review. BMJ Glob Health. (2021) 6:e004537. doi: 10.1136/BMJGH-2020-004537
41. Viswanathan, M, Kahwati, L, Jahn, B, Giger, K, Dobrescu, AI, Hill, C, et al. Universal screening for SARS-CoV-2 infection: a rapid review. Cochrane Database Syst Rev. (2020) 2020:CD013718. doi: 10.1002/14651858.CD013718
42. Mbwogge, M . Mass testing with contact tracing compared to test and trace for the effective suppression of COVID-19 in the United Kingdom: systematic review. JMIRx Med. (2021) 2:e27254. doi: 10.2196/27254
43. Mazza, C, Girardi, D, Gentile, L, Gaeta, M, Signorelli, C, and Odone, A. Public health effectiveness of digital contact tracing in the COVID-19 pandemic: a systematic review of available data. Acta Biomed. (2021) 92:e2021439. doi: 10.23750/ABM.V92IS6.12237
44. Jenniskens, K, Bootsma, MCJ, Damen, JAAG, Oerbekke, MS, Vernooij, RWM, Spijker, R, et al. Effectiveness of contact tracing apps for SARS-CoV-2: a rapid systematic review. BMJ Open. (2021) 11:e050519. doi: 10.1136/BMJOPEN-2021-050519
45. Craig, KJT, Rizvi, R, Willis, VC, Kassler, WJ, and Jackson, GP. Effectiveness of contact tracing for viral disease mitigation and suppression: evidence-based review. JMIR Public Health Surveill. (2021) 7:e32468. doi: 10.2196/32468
46. Hossain, AD, Jarolimova, J, Elnaiem, A, Huang, CX, Richterman, A, and Ivers, LC. Effectiveness of contact tracing in the control of infectious diseases: a systematic review. Lancet Public Health. (2022) 7:e259–73. doi: 10.1016/S2468-2667(22)00001-9
47. Becker, LA, and Oxman, AD. Overviews of reviews In: Cochrane Handbook for Systematic Reviews of Interventions: Cochrane Book Series. eds. Julian PT Higgins and Sally Green Hoboken, NJ: Wiley (2008). 607–31.
48. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
49. Babineau, J . Product review: Covidence (systematic review software). J Canad Health Lib Assoc. (2014) 35:68. doi: 10.5596/c14-016
50. Whiting, P, Savović, J, Higgins, JPT, Caldwell, DM, Reeves, BC, Shea, B, et al. ROBIS: a new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol. (2016) 69:225–34. doi: 10.1016/j.jclinepi.2015.06.005
Keywords: COVID-19, health policy, public health and social measures, non-pharmaceutical interventions, modified Delphi expert consensus process
Citation: Paulo MS, Peyroteo M, Maia MR, Pries C, Habl C and Lapão LV (2023) Impacts of public health and social measures on COVID-19 in Europe: a review and modified Delphi technique. Front. Public Health. 11:1226922. doi: 10.3389/fpubh.2023.1226922
Edited by:
Morteza Arab-Zozani, Birjand University of Medical Sciences, IranReviewed by:
Margaret Haworth-Brockman, University of Manitoba, CanadaSi Ying Tan, National University of Singapore, Singapore
Copyright © 2023 Paulo, Peyroteo, Maia, Pries, Habl and Lapão. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marília Silva Paulo, bWFyaWxpYS5wYXVsb0BubXMudW5sLnB0