
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 12 October 2023
Sec. Public Health Education and Promotion
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1226420
This article is part of the Research Topic Health Promotion in Schools, Universities, Workplaces, and Communities View all 44 articles
 Nayara Tamayo-Fonseca1
Nayara Tamayo-Fonseca1 Pamela Pereyra-Zamora1*
Pamela Pereyra-Zamora1* Carmen Barona2,3,4Rosa Mas2,3Mª Ángeles Irles2
Carmen Barona2,3,4Rosa Mas2,3Mª Ángeles Irles2 Andreu Nolasco1
Andreu Nolasco1Background: Health literacy (HL) is the set of social and cognitive skills that determine person’s level of motivation and the ability to access, understand and use information to promote and maintain good health. The aim of this study is to assess the level of health literacy, and to analyze its relationship with sociodemographic variables, state of health, and use of health services in the population aged 15 and over in the Valencian Community (Spain).
Methods: Cross-sectional study based on a sample of 5,485 subjects participating in the Health Survey of the Valencia Community. The HLS-EU-Q16 was used. As outcome variables we considered HL categorized into 2 levels: Inadequate or Problematic HL and Sufficient HL and the standardized literacy index. Prevalence rates and HL means were estimated and OR were calculated to analyze the association between variables.
Results: A total of 12.8% of the subjects surveyed presented an inadequate or problematic degree of HL. This percentage was higher in people >85 years (63.1%), with a low level of education (46.5%), in retired people (27.4%) or in other work situations (25.0%), in foreigners (18.1%), in low-income people (16.2%), with a perception of poor health status (26.9%), chronic disease (18.5%) or with activity limitations (56.4% severe, 19.7% not severe). Significant differences were found. With the exception of chronic disease, all the variables analyzed were associated with HL. Low HL was associated with a lower consumption of medicines, a greater use of health services, general medical consultations, poorer knowledge of new health technologies and fewer preventive health visits.
Conclusion: The percentage of inadequate or problematic HL was globally not very high, but certain population subgroups notably presented a high degree of inadequate or problematic HL. Raising the HL level of such groups should be regarded as a priority. HL was shown to be associated with the service use and new health technology use. Enhancing the population’s HL should lead to the following: a greater probability of adopting preventive practices; improving the use of the health system; and boosting people’s abilities to manage and to improve their own health.
Health literacy (HL) is the set of social and cognitive skills that determine a person’s degree of motivation and ability to access, understand and use information to promote and maintain good health (1).
In recent years, there has been an increasing amount of research on health literacy. Recent studies have described the essential role of HL as it is one of the major predictors of the population’s health status. HL is also recognized as a key factor in the reduction of health inequalities (2–14).
Several institutions have been recommending the performance of standardized and regular measurements of the general population’s HL in order to broaden the evidence and to implement public health policies allowing people to promote and maintain their own good health (10, 14, 15).
Several instruments can be used to assess HL (7, 16–18). They are based on different definitions, conceptual frameworks and they evaluate distinct dimensions, skills, and domains. Europe has been developing instruments to measure HL since 2009 and they have been designed by the European Consortium on Health Literacy (HLS-EU Consortium) – which is part of the European Commission’s European Public Health Programme –, and since 2018, by the HLS19 Consortium of the WHO Action Network on Measuring Population and Organizational Health Literacy (M-POHL), which is integrated in the European Health Information Initiative (EHII WHO-Europe) (19, 20).
The first European Health Literacy Survey (HLS-EU) was conducted within the HLS-EU Consortium project, which was based on a comprehensive and general HL conceptual framework and definition. The project generated a range of HL measurement instruments for the general population, among which a questionnaire with 47 items (HLS-EU-Q47) that fall into 4 information management dimensions (find information, understand it, evaluate it and apply it) linked to each of the 3 health domains (care, prevention and health promotion). A short form of the HLS-EU-Q47 was also developed called the HLS-EU-Q16 questionnaire, with 16 items (20). In Spain, the latter has proven to be a swift, adequate, and valid instrument to measure the population’s level of HL (21).
In Spain, few studies have analyzed the HL of the general population (22, 23). The results of the first European Health Literacy Survey conducted between 2009 and 2012 showed that results varied significantly among different countries. In Spain, at least half of the respondents presented limited health literacy (with inadequate or problematic levels), but the average HL level was slightly higher than the average of the other European countries that took part in the survey (9, 20).
Various socioeconomic determinants affecting HL have generally been described. Education has shown to be a significant predictor of HL, together with age, employment and social status, income/financial deprivation, etc. (11, 20, 24, 25).
Previous studies have shown a range of negative effects on healthy lifestyles, self-perceived health, and activity limitations among people with limited HL (20, 25). Thus, patients with chronic diseases also present greater complications and vulnerability in their disease management (10).
Among older people, HL has been associated with poorer overall health, higher mortality rates, later diagnoses and increased premature mortality in the case of certain cancers (10, 17, 26–28).
Regarding service use, low HL has been associated with a higher number of hospitalizations and emergencies, a lesser use of preventive services, and a worse ability to take medication appropriately and to correctly interpret health labels and messages (3, 12, 20, 25).
Considering all the above, we hypothesized that sociodemographic environment and health status were related to population HL and that the latter could in turn be a determinant of health service use. Based on this assumption, the objectives of the present study were as follow: (a), to estimate the prevalence of inadequate or problematic health literacy and to analyze the relationship between this prevalence and the variables socioeconomic environment and health status; and (b), to analyze the association between HL and service use variables in the general population aged 15 and over in the Valencian Community.
Cross-sectional descriptive study based on a sample of 5,485 subjects, representative of the non-institutionalized population aged 15 or over, participating in the Health Interview Survey of the Valencian Community 2016 (HISVC-2016).
The HISVC-2016 data collection was carried out between May and December 2016, on a sample of 5,280 dwellings, identified from the Population Information System of the Regional Ministry of Universal Health and Public Health. The total sample size was 7,888 subjects in 2016, of which 5,485 were adults and 2,403 under 15 years of age residing in the Valencian Community, an autonomous community with almost five million inhabitants in 2016. The sample subjects were selected using a complex sampling design that assigned each subject a weighting according to their representativeness. The weights were included in the HISVC-2016 databases provided by the Health Plan Service of the Conselleria de Sanitat of the Generalitat Valenciana (the Health Ministry of the Valencian Government). The information was collected by means of a personal interview at the respondent’s home, assisted by tablets and other mobile devices. The questionnaire was completed by the interviewer, with the answers provided by the selected adult. Details on the survey methodology (sample design, sample size, sampling procedure, consent, ethics, etc.) have been previously published (29).
An informed consent was required from every participant in the HISVC-2016 by the Valencian Health Authorities. According to national regulations, data from National or Regional Health Surveys are public in Spain and the Valencian Health Authorities are responsible for and guarantee confidentiality and anonymity, making the approval of an ethics committee unnecessary (30). The researchers only had access to public data that had been rendered anonymous, and so this research poses no ethical issues.
To estimate HL, we used the HLS-EU-Q16 Questionnaire (31) that evaluates HL comprehensively and rapidly. It presents a suitable level of understanding and satisfactory psychometric properties (21). In this sense, reliability was high, with an intraclass correlation coefficient de 0.923 and a kappa of 0.814. The factorial analysis suggested a unifactorial structure with 79.1% of variability explained by the common factor, with high factorial loads. Consistency was also high, with Cronbach’s alpha values of 0.982. For the collection of the information on the Health Literacy module, answer support cards were used with information on the answers of the HLS-EU-Q16 questionnaire (1-very easy, 2-easy, 3-difficult, 4- very difficult), which were also included in the computer support itself.
The “literacy level” variable was constructed based on the 16 items in the questionnaire. We only used the data of the 5,148 subjects who validly answered at least 14 items, transforming each item into a dichotomous response: very difficult and difficult = 0; easy and very easy = 1. Each subject’s final score corresponded to the sum of the scores (0 or 1) of the 16 items. A score between 0 and 8 points was considered to represent an ‘inadequate level’, between 9 and 12 points, a ‘problematic level’, and between 13 and 16 points, a ‘sufficient level’. For the association analyses and the multivariate regression models, the variable was dichotomized into ‘Inadequate or problematic literacy’ (a score between 0 and 12) and ‘Sufficient literacy’ (a score between 13 and 16) (32). The standardized literacy index (SLI) calculated as (Mean-1)*(16/3) was calculated, with Mean = arithmetic mean of the scores (from 1 to 4) of the items answered. This index varied between 0 (lowest literacy) and 16 (highest literacy). The SLI behavior was characterized using established cut-off points and according to the sociodemographic characteristics of the health status of the population aged 15+ years.
The following sociodemographic variables were analyzed: sex (man, woman), age (15–24; 25–39; 40–64; 65–84; 85 and over), maximum level of studies attained (no studies, primary, secondary, university), employment status (working, unemployed, retired, studying, other situation), country of birth (Spain, other), income (<600, 600–1,200, 1,200–1,800, 1,800–2,700, >2,700 euros of monthly net income). The health status variables considered were: Self-perceived health (very good, good, fair, bad, very bad. For the analysis, it was classified as very good or good corresponded to ‘Good’; and fair, bad or very bad corresponded to ‘Bad’), chronic disease (yes/no) and activity limitations in the last 6 months, measured by the Global Activity Limitation Indicator – GALI (severely limited, limited but not severely, not at all limited). The following variables relating to service use were studied: medicine consumption (consumption over the last 2 weeks: yes/no); or use of health services (use of any service in the last 12 months: yes/no); consulted a general practitioner (any consultation over the last 4 weeks: yes/no); consulted a specialist (any consultation in the last 4 weeks: yes/no); need for care not met (no care received in the last 12 months: yes/no); knowledge and use of new health technologies (do you know of any health technology service: yes/no, and have you used one: yes/no); periodic preventive health check-ups (occupational, dentist, eye doctor: never or more than 3 years ago/less than 3 years ago); and preventive gynecological check-ups, mammography or cytology, only in women (never or more than 3 years ago/less than 3 years ago).
The percentages of inadequate or problematic literacy were calculated first, together with the SLI means, both globally and according to studied variable categories with 95% confidence intervals (CI95%). The Chi-square test was performed to analyze the relationship between inadequate or problematic literacy and demographic, socioeconomic and health status variables. Student’s t-test and ANOVA were performed to analyze differences in mean SLI values according to demographic, socioeconomic and health status categories. Bivariate and multivariate logistic regression models were adjusted to estimate the crude and adjusted odds ratios (ORs) of association between the dichotomous variable ‘Inadequate or problematic literacy /Sufficient literacy’ and the rest of the variables.
To analyze the association between HL and service use variables, we calculated the percentages of the variable categories according to each HL category (inadequate or problematic literacy/sufficient HL) and for the total, with 95% confidence intervals (CI95%).
Bivariate and multivariate logistic regression models were adjusted in order to estimate the crude and adjusted odds ratios (and 95% confidence intervals) of association between service use and the rest of variables.
In all estimates and models, the weights of the individuals in the sample were used according to the complex sample design. We employed IBM SPSS® software to perform all the calculations and a 0.05 significance level of reference.
Table 1 shows the percentages of inadequate or problematic literacy as well as the average health literacy index values according to different categories of the sociodemographic and health status explanatory variables. We found that in the Valencian Community, 12.8% of the surveyed subjects in the general population presented inadequate or problematic HL levels (12.5% of women and 13.0% of men). Certain population groups presented higher degrees of inadequate or problematic HL: people aged 85 years or over (63.1%); with a low level of education (46.5%); retired people (27.4%); people in other employment situations (25.0%); foreigners (18.1%); and low-income people (16.2%). They presented significant differences in all variables. In the same way, HL was worse among those who perceived their health status as poor (26.9%), had a chronic disease (18.5%), or activity limitations (56.4% severe, 19.7% not severe), again presenting significant differences (p < 0.05) in all variables.
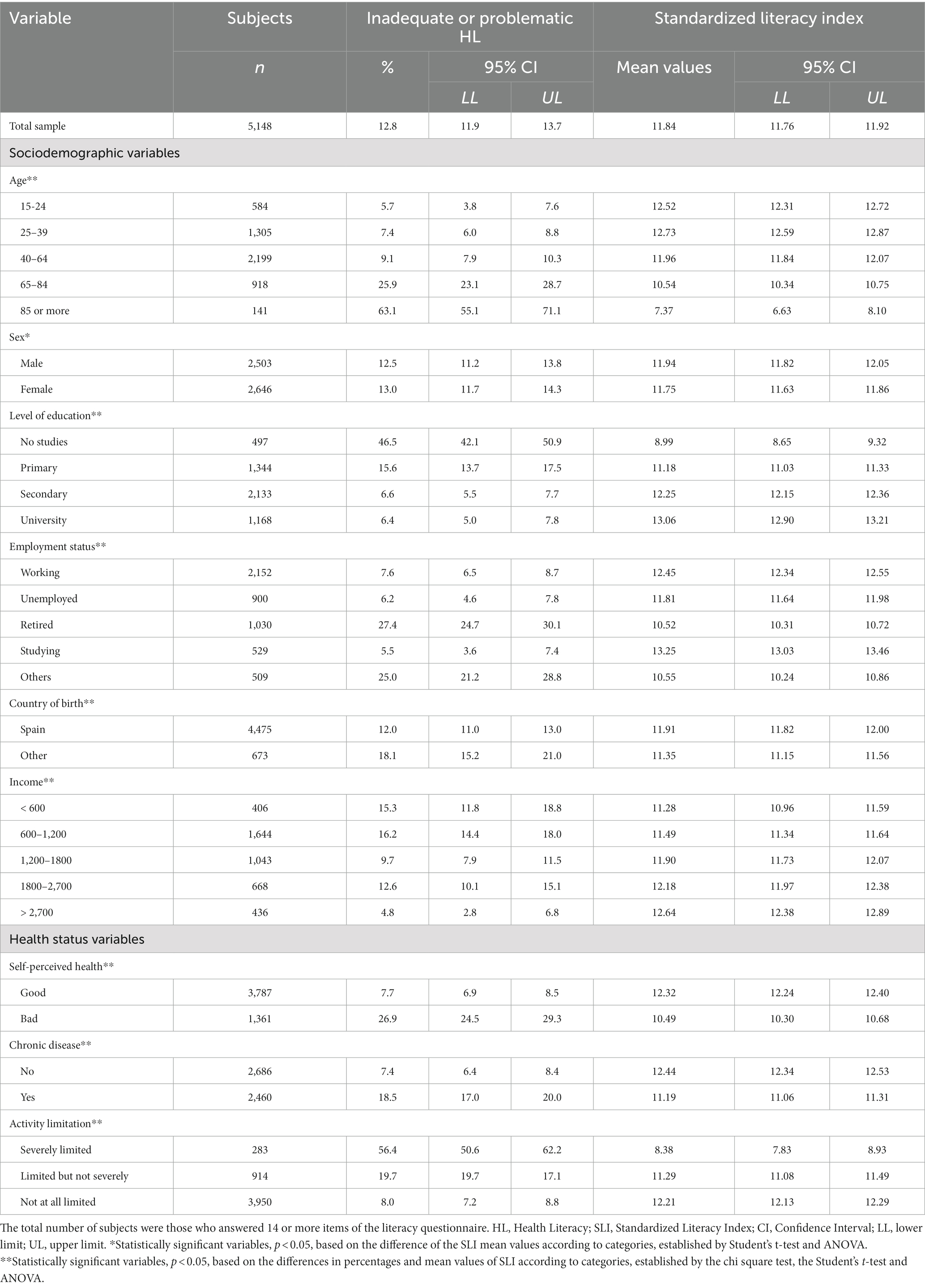
Table 1. Percentages of inadequate or problematic HL and mean values of the standardized literacy index (95% CI), according to categories of the explanatory sociodemographic and health status variables.
When adjusting a multivariate model, with HL (inadequate or problematic literacy vs. sufficient literacy) as a response variable and socioeconomic and health status variables as explanatory variables (Table 2), all presented a significant association except chronic disease.
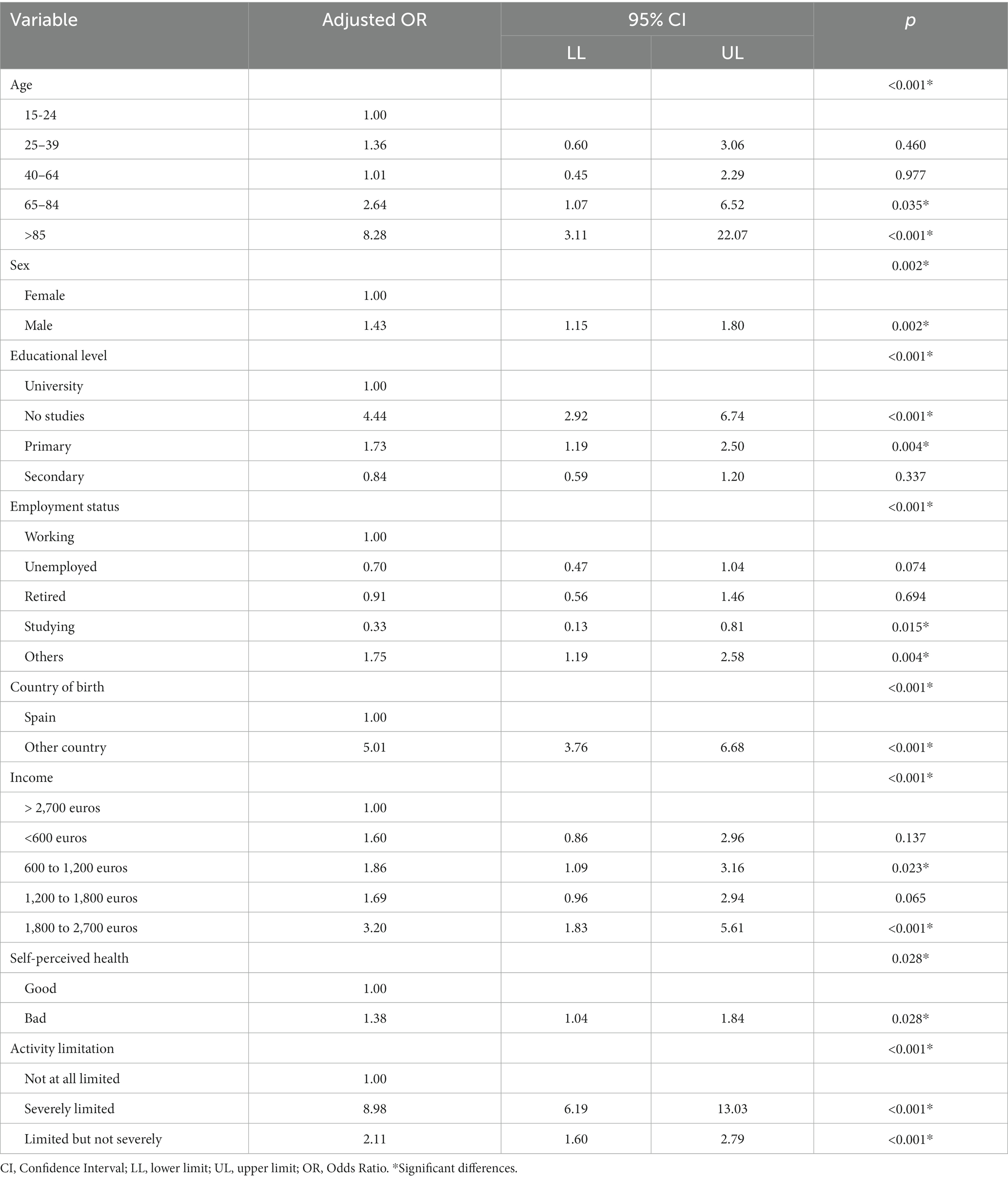
Table 2. Adjusted odds ratio and 95% CI association between health literacy (inadequate or problematic vs. sufficient literacy category) and other demographic, socioeconomic, and health variables.
An older man (65–84 years), with no higher education, retired, born outside Spain, with an income between 600 and 1,200 euros a month, with poor self-perceived health and functional limitation, would be highly likely of presenting inadequate or problematic literacy – with an estimated probability per model of 0.84762. On the other hand, a working and university-educated young woman (aged 25–39 years) born in Spain, earning over 2,700 euros a month, with good self-perceived health and no functional limitation would have a low probability of presenting inadequate or problematic literacy – with an estimated probability per model of 0.01794.
Regarding the variables related to medicine consumption, service use and preventive practices, subjects with inadequate or problematic HL presented: lower medicine consumption (10.0% vs. 32.1%); a greater use of health services in the last 12 months (95.1% vs. 84.8%); a higher percentage of general practitioner visits (39.5% vs. 20.8%) and specialist visits (18.0% vs. 12.2%), lower levels of knowledge (44.5% vs. 73.9%) and use (24.7% vs. 44.7%) of new health technologies and less preventive occupational, dentist and eye doctor check-ups (21.5% vs. 7.9%) as well as less gynecological visits (48.1% vs. 18.6%) with significant percentage differences (p < 0.05) – see Table 3.
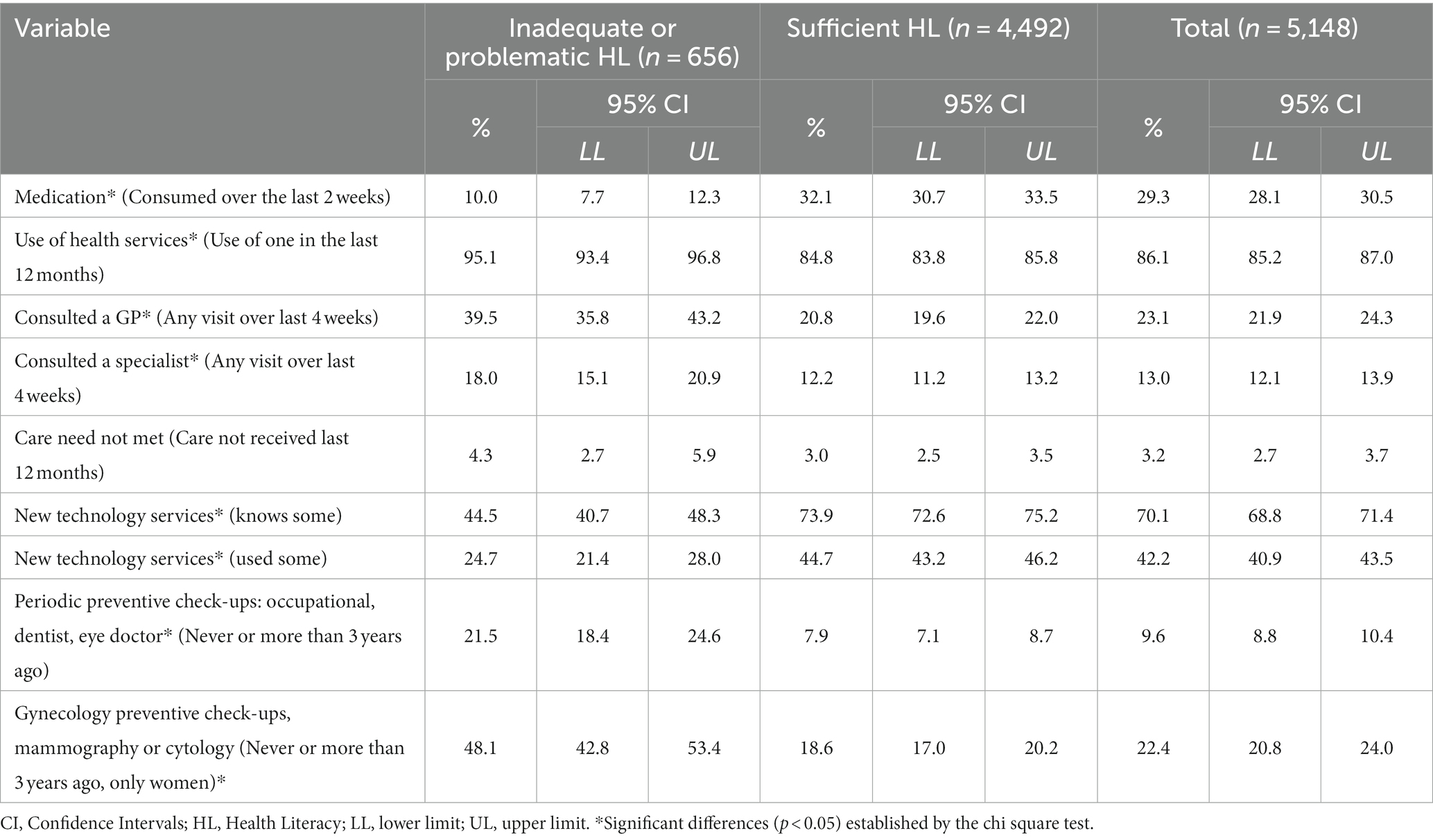
Table 3. Percentages and confidence intervals (95%) according to HL categories (inadequate or problematic HL, sufficient) of various results regarding medicine consumption, knowledge of new technologies, and use of health and preventive services.
Table 4 summarizes the association of the variables relating to services use (as outcome variables), including the use of preventive and general health services, medicine consumption, and knowledge and management of new technologies with HL variable (as explanatory variable). The results both of the simple analysis and adjusting for sociodemographic variables and health status revealed that people with inadequate or problematic HL were: 1.66 times more likely to use health services; 1.43 times more likely to consult a general practitioner; 1.41 and 2.08 times more likely of not having preventive health check-ups (including occupational, dentist, eye doctor visits as well as gynecological, mammography or cytology check-ups in the case of women). However, it was observed that inadequate HL could explain a lower probability of taking medication (OR 0.43) and poorer knowledge of new health technologies (OR 0.53).
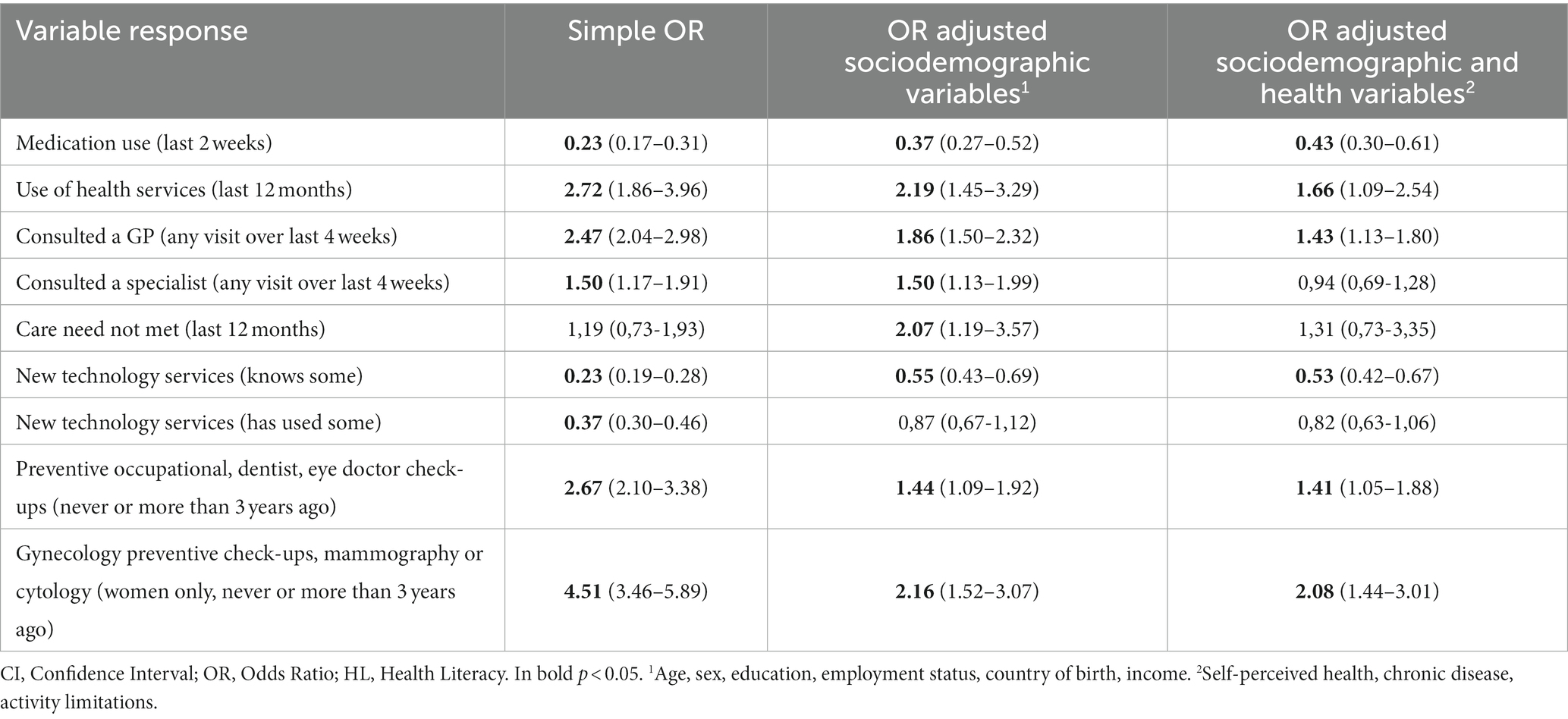
Table 4. Simple and adjusted odds ratio of several variables of use of preventive and health services, knowledge and management of new technologies with HL (inadequate or problematic), adjusting for sociodemographic variables and health status.
The Supplementary material presents the complete final model of the association between HL and different variables of use of preventive and health services, knowledge and management of new technologies, adjusted to socio-demographic variables and health status for the total population.
The present study centered on the adult population of the Valencian Community (Spain) and described HL according to categories of socioeconomic variables, health status, and use of health services. The results showed a significant association between HL and variables relating to service use and the use of new health technologies.
Although the global percentage of inadequate or problematic health literacy did not seem to be high (12.8%), some population subgroups presented values above 60% (for example, those aged above 85 years). Generally, the percentages of people with inadequate or problematic HL levels were lower than the percentages reported in other studies – i.e., between 28 and 66% of people with problematic HL levels (9, 28, 33–36).
In Europe, described levels of limited HL were higher – based on the HLS-EU Q47 (the long version of the questionnaire) –, the European average reaching 47.6% (8, 18). The country with the lowest reported levels of limited HL is the Netherlands, with 28.7% – still well above the levels found for the Valencian Community. The results in this work for Spain showed the highest percentages (together with Bulgaria) of populations with limited HL, accounting for around 58.3% (20) However, a study conducted in another Spanish region described values similar to ours, including a 15.4% rate of limited HL (10.3% inadequate literacy and 5.1% problematic literacy), which was also measured using the HLS-EU Q16 questionnaire (23).
HL level differences between countries have been explained both by contextual circumstances and individual traits (13, 20). In other words, HL depends on individual abilities and context-specific demands and expectations, determined by variables such as health culture, health care system complexity, the history of media education, information campaigns, as well as the contents of national and regional health policies. In this sense, in Spain’s case of a public and universal health system, this lower reported percentage of limited HL in the general population of the Valencian Community could perhaps be due to the population sample characteristics. Such features may include, for example: a population with high educational levels and young people; the type of information collected (the questionnaire was not self-administered so functional literacy was not assessed); a social desirability bias due to the interviewer’s presence; highly diligent interviewers who explained each questionnaire item; the participation of people with extensive health system knowledge and experience of health institutions; people who perceive low complexity in the access and use of health services in the region; a positive perception of personal competencies or skills; and populations that have participated in health education programs, among others. In this way, it would be important to assess the impact of intervention policies on self-care improvement promoted within the Valencian Community’s health strategy framework, such as attention to chronicity or active aging.
Regarding the HLS-EU-Q16 instrument, it should be noted that despite its extensive use (11, 28, 36–38), a recently published study questioned the representativeness of the underlying conceptual model used to measure HL (13). Another population study conducted in Spain (in the Mediterranean region of Catalonia, close to the Valencian Community) indicated that the substantial differences found may indicate a limitation specific to each country, which could be affecting the accuracy of the short HLS-EU-Q16 questionnaire (23). It would thus be necessary to further explore these result differences, as well as other variables associated with HL in the Valencian Community. The concepts underlying the measurements of an instrument based on a subjective, self-reported evaluation should also be examined (39). Moreover, an assessment of functional skills relating to health literacy could also be included, in addition to the self-declared/reported ability collected by the HLS-EU Q16 questionnaire.
Overall, the literature has shown that limited literacy follows a social gradient and may further accentuate existing inequalities (4–6, 10, 25, 36). Our results support the literature, which shows a significant relationship between HL and older age, low educational levels, low perceived social status, lower income, and migratory status, among others (3, 5, 6, 10). Moreover, most studies have found an association between limited HL and health status, mostly relating to self-perceived poor health, having a chronic disease and activity limitations (3, 10, 12, 20, 25). A study showed that in the Spanish population, age, level of education, and self-perceived health were the three main predictors of HL (measured with the HLS-Q47) (22). The study carried out in the Catalan population found that the factors educational level, socioeconomic status and physical limitations contributed the most to insufficient HL (measured using the HLS-EU-Q16) (23).
Regarding medicine consumption, subjects with insufficient HL presented lower levels of medication consumption. In this sense, evidence was found that a low HL level was related to worse skills in the appropriate taking of medication, worse performance in the use of dosing instruments, a lesser probability of identifying prescribed medications or a misinterpretation of labeling (3). It therefore showed that low literacy also leads to more negative experiences and errors in treatments and medication use. On the other hand, the evidence regarding adherence to medication treatments and procedures is not entirely clear (12, 40, 41).
With respect to service use, our results showed that subjects with inadequate or problematic HL made a greater use of health services, general practitioner consultations and specialist consultations. This trend has been reported in other studies (3, 12, 20, 25). For example, results of the latest study conducted in several European countries (HLS19) have shown that the higher the HL, the lower the use of emergency services, the fewer the contacts with GPs/family doctors, medical or surgical specialists, as well as short inpatient hospital services, and day patient hospital services (25).
However, when analyzing preventive practices, the results showed fewer preventive screenings among people with low HL. In this sense, the evidence shows less participation in health promotion programs and preventive programs, e.g., mammography screening and influenza immunizations (3, 5, 12, 42, 43). Concerning the use of Pap tests or colorectal cancer screening, the initial evidence was not entirely clear, although the latest studies point to the aforementioned association (3, 12, 43).
Our results showed poorer knowledge and use of new health technologies. Regarding the use of ICTs (information and communication technologies), some studies point to barriers relating to the use of websites, telephone interactions, and completion of health forms, etc. –which complicates the requirements to ensure successful decision-making by the low-HL (10, 44) In this sense, a series of recommendations have been proposed to promote better access and use of health information and therefore to improve HL (10, 44). In Spain, a study validated the eHealth questionnaire, which is a scale on the aptitude to use eHealth (45), that is, to measure digital literacy in health, which can be considered to specifically assess this dimension.
HL is an indicator of a population’s degree of competence to responsibly manage their own health. Greater HL levels could translate into a greater competence (44), and thus increase the probability of carrying out preventive practices, improving the use of the health system. The HL could, therefore, be a predictor variable of the use of services and the use of new health technologies.
In summary, the HL could act as a mediator of health outcomes and service use and new technologies. HL would thus behave similarly to the “self-perceived health” indicator. The latter is widely studied and recognized as a predictor of various health outcomes and service use (46, 47) However, unlike this indicator, the HL would behave as a potentially modifiable mediator, thanks to health education policies, health programs, or citizen empowerment, aimed at improving health equity and reducing or eliminating inequalities.
The present work was a cross-sectional study, which makes it difficult to draw causal conclusions. On the other hand, a standardized instrument (HLS-EUQ16) that has shown to present adequate comprehension and good psychometric properties was used. This validated instrument has proven to be a simple and reliable way to collect population HL information. The present study was based on a large, representative sample of the population of a Spanish region. These data (collected for the first time in the Valencian Community’s population), can be used as a starting point for follow-up studies and analyses of the important role of HL. Indeed, inequalities have increased significantly following the measures adopted to face the crisis and pandemic. In this study, we only used the category classification suggested in other studies (inadequate/problematic and sufficient). The full potential of continuous scoring and other literacy scale categories is worth exploring in the future.
Health literacy levels of the population of the Valencian Community (Spain) were measured. Percentages of inadequate or problematic HL differed according to the population group. The Valencian Community’s population presents an inadequate or problematic level of health literacy which is slightly below the European and Spanish average. A specific population profile with an inadequate or problematic HL level was identified. This profile should be regarded as a target group for HL improvement measures, including the implementation of specific policies and programs. The ultimate objective would thus be to reduce health disparities and to help to improve their health status.
HL was significantly associated with variables relating to service use and the use of new health technologies, both in the simple analysis and when adjusting for various demographic, socioeconomic environment and health status variables. Improving HL could improve the levels of use both of health services and of new health technologies.
The data analyzed in this study is subject to the following licenses/restrictions: The data of the Health Interview Survey of the Valencian Community 2016 analyzed for this study can be obtained from the Office of Health Plan (Conselleria de Sanitat of the Valencian Autonomous Government) on demand and by personal registration: https://www.sp.san.gva.es/suscripciones/inicioSuscripciones.jsp?menuRaizPortal=SANMS&Opcion=SANPS9I&MenuSup=SANMS&perfil=inst. Requests to access these datasets should be directed to https://www.sp.san.gva.es/suscripciones/inicioSuscripciones.jsp?menuRaizPortal=SANMS&Opcion=SANPS9I&MenuSup=SANMS&perfil=inst.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
AN and NT-F designed the protocol, led the project, and wrote the first draft. CB, RM, and MaI collected the necessary data. AN and PP-Z performed the statistical analysis. All authors providing critical comments, read, and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1226420/full#supplementary-material
HL, Health literacy; SLI, Standardized literacy index; HISVC, Health interview survey of the Valencian community; HLS-EU-Q16, European health literacy survey questionnaire; GALI, Global activity limitation indicator.
1. World Health Organization. Health promotion glossary. Geneva: World Health Organization (1998). 36 p.
2. Altin, SV, Finke, I, Kautz-Freimuth, S, and Stock, S. The evolution of health literacy assessment tools: a systematic review. BMC Public Health. (2014) 14:1207. doi: 10.1186/1471-2458-14-1207
3. Berkman, N, Sheridan, S, Donahue, K, Halpern, D, and Crotty, K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. (2011) 155:97–107. doi: 10.7326/0003-4819-155-2-201107190-00005
4. Nutbeam, D, and Lloyd, JE. Understanding and responding to health literacy as a social determinant of health. Annu Rev Public Health. (2020) 42:159–73. doi: 10.1146/annurev-publhealth-090419-102529
5. Stormacq, C, Van Den Broucke, S, and Wosinski, J. Does health literacy mediate the relationship between socioeconomic status and health disparities? Integrative review. Health Promot Int. (2019) 34:E1–E17. doi: 10.1093/heapro/day062
6. Mantwill, S, Monestel-Umaña, S, and Schulz, PJ. The relationship between health literacy and health disparities: a systematic review. PLoS One. (2015) 10:e0145455. doi: 10.1371/journal.pone.0145455
7. Haun, JN, Valerio, MA, Mccormack, LA, Sørensen, K, and Paasche-Orlow, MK. Health literacy measurement: an inventory and descriptive summary of 51 instruments. J Health Commun. (2014) 19:302–33. doi: 10.1080/10810730.2014.936571
8. Kondilis, BK, Kiriaze, IJ, Athanasoulia, AP, and Falagas, ME. Mapping health literacy research in the European Union: a bibliometric analysis. PLoS One. (2008) 3:e2519. doi: 10.1371/journal.pone.0002519
9. Sorensen, K, Pelikan, JM, Rothlin, F, Ganahl, K, Slonska, Z, Doyle, G, et al. Health literacy in Europe: comparative results of the European health literacy survey (HLS-EU). Eur J Pub Health. (2015) 25:1053–8. doi: 10.1093/eurpub/ckv043
10. Kickbusch, I, Pelikan, J, Apfel, F, and Tsouros, A. Health literacy: The solid facts. Copenhaguen: WHO Regional Office for Europe (2013). 86 p.
11. Pelikan, JM, StraBmayr, C, and Ganahl, K. Health literacy measurement in general and other populations: further initiatives and lessons learned in Europe (and beyond) In: RA Logan and ER Siegel, editors. Health literacy in clinical practice and public health. Amsterdam: IOS Press (2020). 170–91.
12. Dewalt, DA, Berkman, ND, Sheridan, S, Lohr, KN, and Pignone, MP. Literacy and health outcomes a systematic review of the literature. J Gen Intern Med. (2004) 19:1228–39. doi: 10.1111/j.1525-1497.2004.40153.x
13. Pelikan, JM, Link, T, Straßmayr, C, Waldherr, K, Alfers, T, Bøggild, H, et al. Measuring comprehensive, general health literacy in the general adult population: the development and validation of the HLS19-Q12 instrument in seventeen countries. Int J Environ Res Public Health. (2022) 19:1–31. doi: 10.3390/ijerph192114129
14. Organization for Economic Cooperation and Development (OECD). Health Literacy for people-centred care. Paris: OECD (2018).
15. World Health Organization. (2021). The Geneva charter for well-being. 10th Global Conference on Health Promotion. Available at: https://www.who.int/publications/m/item/the-geneva-charter-for-well-being-(unedited)
16. Sorensen, K, Van den Broucke, S, Fullam, J, Doyle, G, Pelikan, J, Slonska, Z, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. (2012) 12:80. doi: 10.1186/1471-2458-12-80
17. Mårtensson, L, and Hensing, G. Health literacy, a heterogeneous phenomenon: a literature review. Scand J Caring Sci. (2012) 26:151–60. doi: 10.1111/j.1471-6712.2011.00900.x
18. McCormack, L, Haun, J, Sørensen, K, and Valerio, M. Recommendations for advancing health literacy measurement. J Health Commun. (2013) 18:9–14. doi: 10.1080/10810730.2013.829892
19. Dietscher, C, Pelikan, J, Bobek, J, and Nowak, P. The action network on measuring population and organizational health literacy (M-POHL): a network under the umbrella of the WHO European health information initiative (EHII). Public Heal Panor. (2019) 5:65–71. Available at: https://iris.who.int/handle/10665/325113
20. HLS-EU Consortium. Comparative report on health literacy in eight EU member states In: J Pelikan, F Rothlin, and K Ganahl, editors. The European health literacy survey HLS-EU. Maastricht: Maastricht University (2012). 95.
21. Nolasco, A, Barona, C, Tamayo-Fonseca, N, Irles, MÁ, Más, R, Tuells, J, et al. Health literacy: psychometric behaviour of the HLS-EU-Q16 questionnaire. [Alfabetización en salud: propiedades psicométricas del cuestionario HLS-EU-Q16]. Gac Sanit. (2020) 34:399–402. doi: 10.1016/j.gaceta.2018.08.006
22. Luna Ruiz-Cabello, A. La alfabetización en salud de la población española: Variables relacionadas según los resultados del proyecto europeo de alfabetización en salud. Murcia: Universidad de Murcia (2015). 1–131.
23. Garcia-Codina, O, Juvinyà-canal, D, Amil-bujan, P, Bertran-noguer, C, González-mestre, MA, Masachs-fatjo, E, et al. Determinants of health literacy in the general population: results of the Catalan health survey. BMC Public Health. (2019) 19:1–12. doi: 10.1186/s12889-019-7381-1
24. Van Der Heide, I, Uiters, E, Sørensen, K, Röthlin, F, Pelikan, J, Rademakers, J, et al. Health literacy in Europe: the development and validation of health literacy prediction models. Eur J Pub Health. (2016) 26:906–11. doi: 10.1093/eurpub/ckw078
25. The HLS19 Consortium of the WHO Action Network M-POHL. International report on the methodology, results, and recommendations of the European health literacy population survey 2019–2021 (HLS19) of M-POHL Vienna:Austrian National Public Health Institute. (2021). Available at: https://m-pohl.net/Int_Report_methdology_results_recommendations
26. Sudore, RL, Yaffe, K, Satterfield, S, Harris, TB, Mehta, KM, Simonsick, EM, et al. Limited literacy and mortality in the elderly: the health, aging, and body composition study. J Gen Intern Med. (2006) 21:806–12. doi: 10.1111/j.1525-1497.2006.00539.x
27. Doyle, G, Caferkey, K, and Fullam, J. The European health literacy survey: Results from Ireland. Dublin: HLS-EU Consortium (2012). 94 p.
28. Wångdahl, J, Lytsy, P, Mårtensson, L, and Westerling, R. Health literacy among refugees in Sweden – a cross-sectional study. BMC Public Health. (2014) 14:1030. doi: 10.1186/1471-2458-14-1030
29. Generalitat Valenciana. (2018). Conselleria de Sanitat Universal i Salut Pública. Encuesta de Salud 2016 de la Comunitat Valenciana. Metodología. Valencia. Spain. Available at: https://www.sp.san.gva.es/DgspPortal/docs/ES_Metodologia2018.pdf
30. Conselleria de Sanitat Universal i Salut Pública. (2022). Generalitat Valenciana. Dirección General de Salud Pública y Adicciones. Polìticas de salud/Encuestas de Salud. Available at: https://www.sp.san.gva.es/sscc/opciones4.jsp?CodPunto=3785&Opcion=SANMS502&MenuSup=SANMS50&Nivel=2 (Accessed June 19, 2018)
31. HLS-EU Consortium. (2012). HLS-EU-Q measurement of health literacy in Europe: HLS-EU-Q47; HLS-EU-Q16; and HLS-EU-Q86. Available at: http://webcache.googleusercontent.com/search?q=cache:zPMAULoeWZcJ:www.forumitesss.com/wp-content/uploads/2015/02/HLS-EU-Q-tools-and-introduction-2.pdf+&cd=1&hl=es& (Accessed April 4, 2018)
32. Röthlin, F, Pelikan, J, and Ganahl, K. (2013). Die Gesundheitskompetenz von 15-jährigen Jugendlichen in Österreich. Wien: Abschlussbericht der österreichischen Gesundheitskompetenz Jugendstudie im Auftrag des Hauptverbands der österreichischen Sozialversicherungsträger (HVSV) 93. Available at: www.lbihpr.lbg.ac.at (Accessed October 10, 2022)
33. Berens, E-M, Vogt, D, Messer, M, Hurrelmann, K, and Schaeffer, D. Health literacy among different age groups in Germany: results of a cross-sectional survey. BMC Public Health. (2016) 16:1151. doi: 10.1186/s12889-016-3810-6
34. Nakayama, K, Osaka, W, Togari, T, Ishikawa, H, Yonekura, Y, Sekido, A, et al. Comprehensive health literacy in Japan is lower than in Europe: a validated Japanese-language assessment of health literacy. BMC Public Health. (2015) 15:505–12. doi: 10.1186/s12889-015-1835-x
35. Nurjanah, N, Rachmani, E, and Manglapy, YM. “Assessing health literacy on student using online HLS-EU-16,” in Proceedings of the 2nd International Seminar on Public Health and Education. Conference paper, Book 2. Indonesia:Semarang. (2015).
36. Svendsen, MT, Bak, CK, Sørensen, K, Pelikan, J, Riddersholm, SJ, Skals, RK, et al. Associations of health literacy with socioeconomic position, health risk behavior, and health status: a large national population-based survey among Danish adults. BMC Public Health. (2020) 20:1–12. doi: 10.1186/s12889-020-08498-8
37. Rouquette, A, Nadot, T, Labitrie, P, Van den Broucke, S, Mancini, J, Rigal, L, et al. Validity and measurement invariance across sex, age, and education level of the French short versions of the European health literacy survey questionnaire. PLoS One. (2018) 13:e0208091–15. doi: 10.1371/journal.pone.0208091
38. Levin-Zamir, D, Baron-Epel, OB, Cohen, V, and Elhayany, A. The Association of Health Literacy with health behavior, socioeconomic indicators, and self-assessed health from a National Adult Survey in Israel. J Health Commun. (2016) 21:61–8. doi: 10.1080/10810730.2016.1207115
39. Gerich, J, and Moosbrugger, R. Subjective estimation of health literacy—what is measured by the HLS-EU scale and how is it linked to empowerment? Health Commun. (2018) 33:254–63. doi: 10.1080/10410236.2016.1255846
40. Hyvert, S, Yailian, AL, Haesebaert, J, Vignot, E, Chapurlat, R, Dussart, C, et al. Association between health literacy and medication adherence in chronic diseases: a recent systematic review. Int J Clin Pharm. (2022) 45:38–51. doi: 10.1007/s11096-022-01470-z
41. Schönfeld, MS, Pfisterer-Heise, S, and Bergelt, C. Self-reported health literacy and medication adherence in older adults: a systematic review. BMJ Open. (2021) 11:1–13. doi: 10.1136/bmjopen-2021-056307
42. Komenaka, I, Nodora, J, Hsu, C-H, Martinez, M, Gandhi, G, Bouton, M, et al. Association of Health Literacy with Adherence to screening mammography guidelines. Obstet Gynecol. (2015) 125:852–9. doi: 10.1097/AOG.0000000000000708
43. Baccolini, V, Isonne, C, Salerno, C, Giffi, M, Migliara, G, Mazzalai, E, et al. The association between adherence to cancer screening programs and health literacy: a systematic review and meta-analysis. Prev Med (Baltim). (2022) 155:106927. doi: 10.1016/j.ypmed.2021.106927
44. Singh, H, Kolschen, J, Samkange-Zeeb, F, Brand, T, Zeeb, H, and Schüz, B. Modifiable predictors of health literacy in working-age adults – a rapid review and meta-analysis. BMC Public Health. (2022) 22:1450–13. doi: 10.1186/s12889-022-13851-0
45. Paramio Pérez, G, Almagro, BJ, Hernando Gómez, Á, and Aguaded Gómez, JI. Validación de la escala eHealth literacy (eHEALS) en población universitaria española [validation of the eHealth literacy scale (eHEALS) in Spanish university students]. Rev Esp Salud Publica. (2015) 89:329–38. doi: 10.4321/S1135-57272015000300010
46. Tamayo-Fonseca, N, Nolasco, A, Quesada, JA, Pereyra-Zamora, P, Melchor, I, Moncho, J, et al. Self-rated health and hospital services use in the Spanish National Health System: a longitudinal study. BMC Health Serv Res. (2015) 15:492. doi: 10.1186/s12913-015-1158-8
Keywords: health literacy, HLS-EU-Q16, use of health services, health inequalities, Spain, health promotion, socioeconomic determinants, new health technologies
Citation: Tamayo-Fonseca N, Pereyra-Zamora P, Barona C, Mas R, Irles M& and Nolasco A (2023) Health literacy: association with socioeconomic determinants and the use of health services in Spain. Front. Public Health. 11:1226420. doi: 10.3389/fpubh.2023.1226420
Edited by:
Teresa Vilaça, University of Minho, PortugalReviewed by:
Xin Wee Chen, Universiti Teknologi MARA, MalaysiaCopyright © 2023 Tamayo-Fonseca, Pereyra-Zamora, Barona, Mas, Irles and Nolasco. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pamela Pereyra-Zamora, cGFtZWxhLnBlcmV5cmFAdWEuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.