
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health, 14 September 2023
Sec. Occupational Health and Safety
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1224332
This article is part of the Research TopicMental Health in Healthcare Workers and its Associations with Psychosocial Work ConditionsView all 32 articles
 Juan Jesús García-Iglesias1,2
Juan Jesús García-Iglesias1,2 Juan Gómez-Salgado1,3*
Juan Gómez-Salgado1,3* Joao Apostolo2
Joao Apostolo2 Rogério Rodrigues2
Rogério Rodrigues2 Emília Isabel Costa2,4
Emília Isabel Costa2,4 Carlos Ruiz-Frutos1,3Santiago Martínez-Isasi5,6Daniel Fernández-García7
Carlos Ruiz-Frutos1,3Santiago Martínez-Isasi5,6Daniel Fernández-García7 Ángel Vilches-Arenas8,9
Ángel Vilches-Arenas8,9Background: A large number of workers attend work despite being ill. Attending work during sickness can have a number of consequences for the worker (e.g., worsening of physical and mental condition), for co-workers, and for the company, and for service users.
Objectives: The aim of this study was to assess the factors influencing presenteeism and mental health of workers during the COVID-19 pandemic.
Methods: A systematic review following the PRISMA format was conducted in the PubMed, Scopus, Web of Science (WoS), Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycInfo, and ScienceDirect electronic databases in January 2023, using the following key words: Presenteeism, Mental Health, and COVID-19. The eligibility criteria applied were original articles published in English, Spanish, French, German, and Portuguese, workers during the COVID-19 pandemic (data collection date: January 01, 2020 – January 01, 2023), and articles assessing at least one measure of presenteeism and mental health status. Methodological quality was assessed using the critical appraisal tools of the Joanna Briggs Institute. The followed protocol is listed in the International Prospective Register of Systematic Reviews (PROSPERO) with code CRD42023391409.
Results: A total of 25 studies were included in this review recruiting a total of 164,274 participants. A number of factors influencing mental health and sickness presenteeism were identified: (1) mental health-related factors (burnout [in 4 studies], stress [in 9 studies], depression [in 1 study], fear of COVID-19 [in 1 study], no well-being [in 2 studies], etc.); (2) individual factors (health status [in 1 study], being young [in 1 study], workers who experienced interrupted medical care [in 2 studies], having a chronic disease [in 1 study], etc.); (3) factors related to the situation caused by COVID-19 (confinement, symptoms, loss of contract, risk of bankruptcy, etc. [in 1 study each one]); and (4) factors derived from working conditions (organisational support [in 1 study], patient care [in 1 study], work functioning or task performance impairment [in 4 studies], work fatigue [in 2 studies], safety climate [in 1 study], workload [in 1 study], etc.).
Conclusion: Identifying the key determinants of presenteeism and understanding the phenomena and origins of sickness presenteeism will help to create a safe working environment and optimal organisational systems to protect vulnerable workers in a pandemic context.
Systematic review registration: The unique identifier is CRD42023391409.
Work attendance during illness can be an occupational health and public health problem, as it is directly related to productivity and the worker’s perception of ineffectiveness (1). Sickness presenteeism is a type of behaviour displayed by some workers who, despite being ill and having physical and/or psychological conditions, decide to go to work or continue with their workday (2). On the other hand, presenteeism means that workers attend work physically and comply with their working hours, but do not really work or contribute anything beyond their presence (3). It is estimated that around 1 in 3 European workers engage in sickness presenteeism (3) and the cost that presenteeism incurs in the workplace is higher than the cost of treatment for these physical and mental illnesses, or even absenteeism (failing to work due to sickness) and sick leaves (4).
This decision is usually made autonomously by the worker and may depend on personal characteristics, the economic situation and type of work, the individual’s values and concerns about leaving their job unattended, among other things (5). In fact, both job demands and resources may be elements that influence a worker’s decision to work despite being sick, according to the Job Demands-Resources Model (6, 7). In this line, authors such as Pohling et al. (8) focused on occupational environmental factors and work climate as the theoretical basis for explaining presenteeism according to the Person-Environment (mis)fit theory. When a misfit between work and the person occurs as a result of these factors, workers experience stress and subsequent psychological burnout as a result. This misfit, together with the need to save resources, leads to workers continuing to work despite this situation (9).
Attending work during sickness can have a number of consequences for the worker (e.g., worsening physical and mental condition), for co-workers, and for the company and service users (10), hence the importance of its study and evaluation. Nevertheless, before the pandemic, some authors had already found possible links between certain mental health-related problems (such as depression) and a change in productivity caused by sickness presenteeism (11–13).
According to the Cambridge dictionary (14), a worker is someone who works in a particular job or in a particular way or someone who works for a company or organisation but does not have a powerful position. Self-employed workers or workers in small businesses may have replacement difficulties in the event of absence from work and are often compelled to work despite being ill (15). A study in Portugal determined that self-employed workers were 85% less likely to take sick leave than employees (14). This can be justified by the need to continue working despite being sick because of the economic difficulties in general, and the pandemic in particular, in order to find solutions to keep their businesses going (16). Another occupational group with high levels of sickness presenteeism is healthcare workers (5). In this case, work attendance during illness can undermine the quality of care provided, increase the likelihood of incidents that may compromise patient safety and clinical practise (17), and even lead to infecting patients and/or co-workers (18). Specific factors justifying these high levels of presenteeism or sickness presenteeism among health workers may include feelings of professionalism and loyalty (19), personal circumstances, and working conditions (stressful work, high complexity, long working hours, low staffing levels, etc.) (18, 20), situations that worsened considerably during the COVID-19 pandemic.
The COVID-19 pandemic has led many organisations to change the way they work and, consequently, the working conditions of their workers. In addition to the pandemic’s impact on people’s mental health (21), the economic situation and job insecurity also worsened (some people worked despite being ill in order not to lose their jobs), some workers switched to teleworking (teleworking from home despite being ill and performing work duties outside of their working hours), chronic programmes were temporarily suspended, and people’s health and consumption habits began to change, with the subsequent consequences at the physical, mental, and social levels (22). Despite recommendations for social distancing and isolation in the case of COVID-19-like symptomatology, many workers were forced to work in order not to lose their jobs or see their income reduced, especially workers with a lower level of education and lower socio-economic status (23), with the consequent impact this may have on their mental health. This study is necessary so as to know the factors that influence presenteeism and to assess which professions suffer the most from sickness-related presenteeism so that organisations and/or companies can take measures based on scientific evidence.
Therefore, the aim of this study was to assess the factors associated with mental health and working conditions that affect presenteeism of workers during the COVID-19 pandemic.
A systematic review of association (aetiology and risk) (24) was conducted following the PRISMA statement guidelines (Preferred Reporting Items for Systematic reviews and Meta-Analyses) (25, 26). The followed protocol is listed in the International Prospective Register of Systematic Reviews (PROSPERO) with code CRD42023391409. This topic was not covered recently by a Review in IJPH or in another journal.
The search was carried out in the Pubmed, Scopus, Web of Science (WoS), Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycInfo, and ScienceDirect electronic databases based on the keywords that the research question yielded following the PEO strategy (27). The research question was What are the factors related to mental health and working conditions that affect presenteeism of workers during the COVID-19 pandemic? (Table 1).
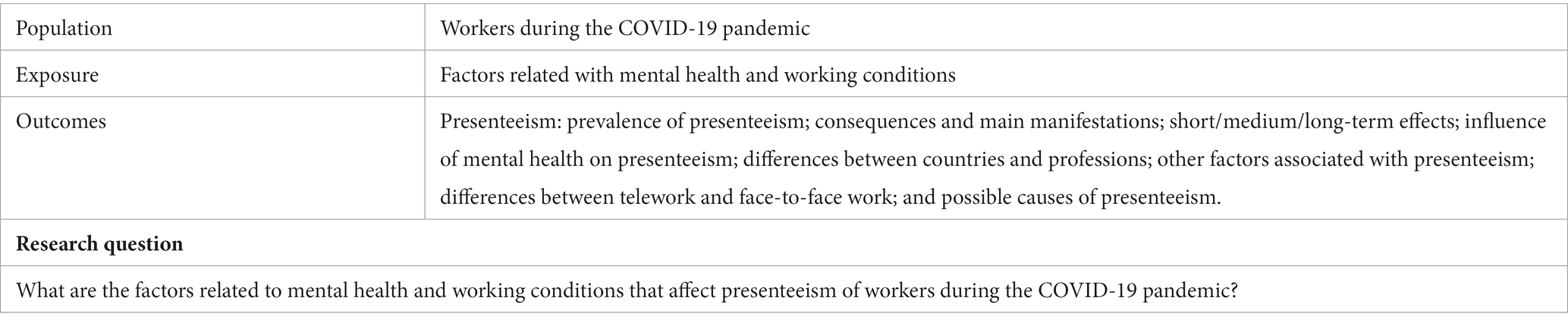
Table 1. PEO format: keywords.
Following these keywords, the Medical Subject Headings (MeSH) thesaurus was consulted, yielding the descriptors Presenteeism, Mental Health, and COVID-19. In order to improve the collection of published studies in line with the subject of the study, synonymous terms were used to complete the search strategy based on the MeSH descriptors (Table 2), which were joined using the Boolean operators and and or.
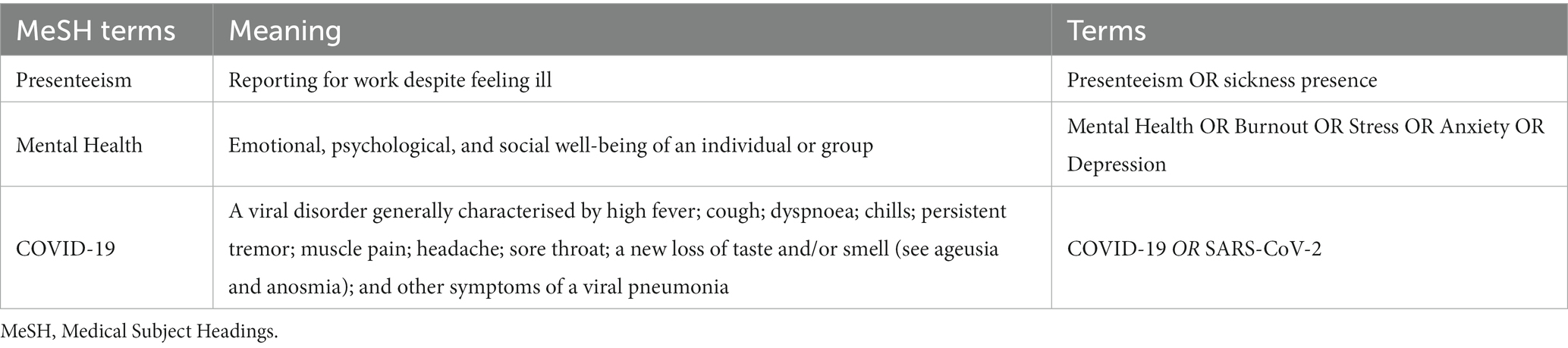
Table 2. Terms and definitions used in the search.
In this case, the terms Presenteeism, sickness presence, Mental Health, Burnout, Stress, Anxiety, Depression, COVID-19, and SARS-CoV-2 were used. Table 3 shows the search strategy used, carried out on January 17, 2023, for each of the aforementioned databases during the search process.
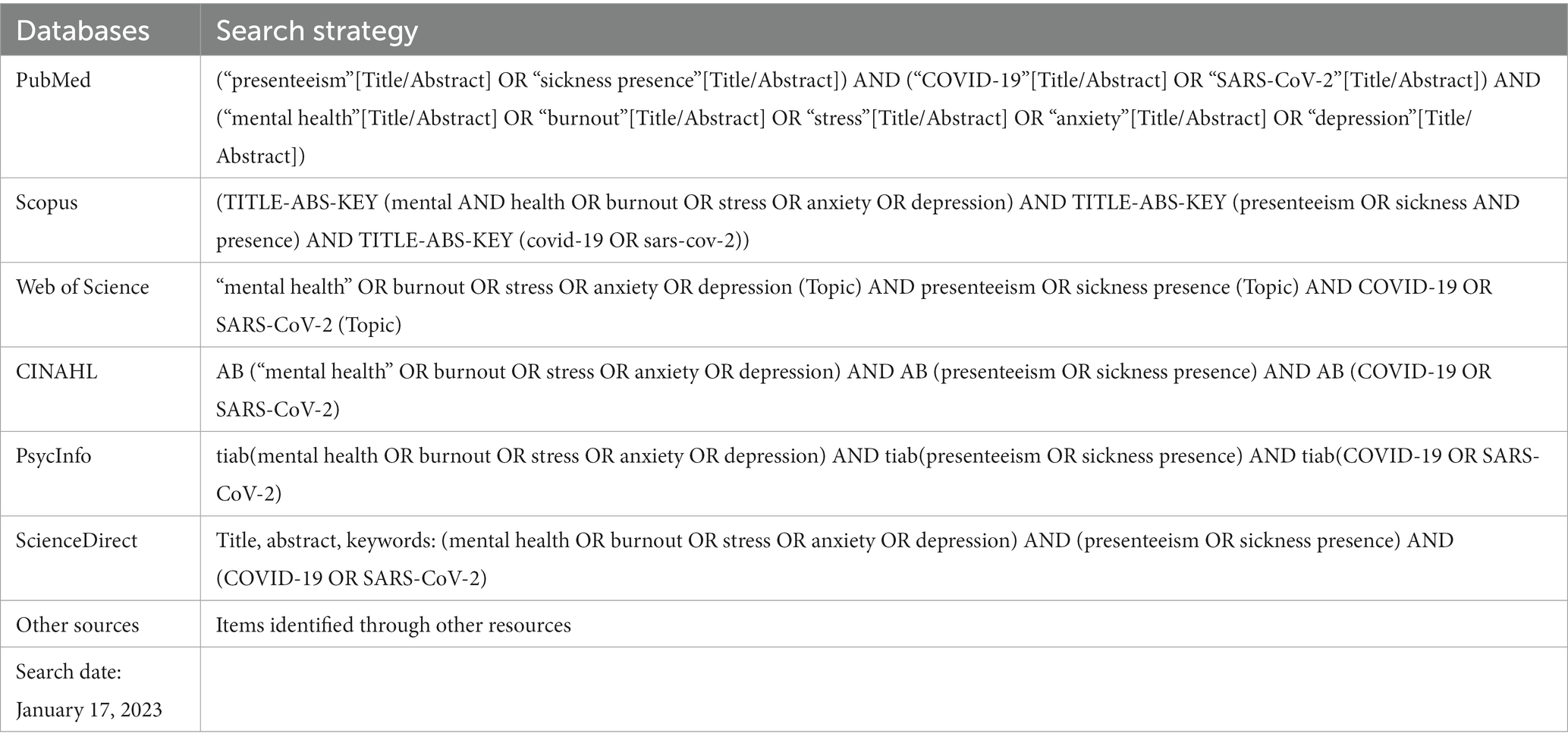
Table 3. Search strategy used in each database.
The following criteria were used for the selection of articles:
• Original articles published in English, Spanish, French, German, and Portuguese.
• Type: original articles, short communications, and case reports.
• Population: workers during the COVID-19 pandemic (someone who works in a particular job or in a particular way or someone who works for a company or organisation).
• Data collection date: January 01, 2020 – January 01, 2023.
• Articles assessing any of the following values and/or effects and those that include at least one measure of presenteeism and mental health status (presenteeism, mental health, and factors associated): prevalence of presenteeism or sickness presenteeism, consequences and main manifestations, short/medium/long-term effects; influence of mental health on sickness presenteeism, and possible causes of sickness presenteeism; and other factors that reduce or increase presenteeism or sickness presenteeism; differences between countries and professions; differences between telework and face-to-face work.
• Studies of low scientific-technical quality after applying the quality assessment tool.
• Population: students.
• Date of data collection: if out of the inclusion period or if the date of data collection was missing.
• Articles that did not answer the research question and were not related to the objective of the review. Studies that did not assess presenteeism or sickness presenteeism as well as mental health were excluded.
• Type: opinion articles, editorials, and letters to the editor.
Based on the aforementioned consensual search strategy, two investigators independently performed the searches, eliminated duplicate studies, and selected articles for inclusion after reading the abstract and title according to the previously established criteria. Subsequently, the same two authors reviewed the full text of potentially eligible studies and the decision to include or exclude them in the review was made by consensus. Discrepancies were resolved by a third author. For the data collection after reading the full text of the articles, specific information on the studies was extracted, such as authors’ names and year of publication; context in which the study was conducted; objective of the study; type of study; sample, methodology, and instruments used for data collection; main findings; and quality of the study after applying the critical appraisal tools.
Two reviewers independently determined the methodological quality of the selected studies using the critical appraisal tools of the Joanna Briggs Institute (JBI) at the University of Adelaide. These tools allowed assessing the methodological quality of a study and determining the extent to which a study has excluded or minimised the risk of bias in its design, conduct, and/or analysis. The versions for analytical cross-sectional studies (8-items) (28), for qualitative research (10 items) (29), for cohort studies (11 items), and for Randomised Controlled Trials (13 items) (30) were used, setting the cut-off point at 6 to be accepted for inclusion in this review for the first two, 8 for the third, and 10 for the fourth (Supplementary material). The basic parameters of the included articles conform to the applied inclusion criteria (especially study design, year of publication, and country origin).
The initial search strategies identified a total of 88 references, which were then screened according to the topic of this review. A total of 25 studies were finally selected (Figure 1), recruiting a total of 164,274 participants. 22 of which were analytical cross-sectional studies, 1 qualitative research, 1 cohort study, and 1 randomised controlled trial.
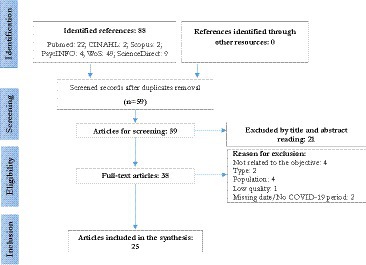
Figure 1. Search results (PRISMA – Flowchart).
Four studies had been conducted in Japan (31–34) and 4 in United Kingdom (35–38), 3 in United States (39–41), 2 in China (42, 43), Germany (44, 45), and the Republic of Korea (46, 47), and 1 in Sweden (16), Wales (48), Canada (22), Turkey (49), Lithuania (50), Portugal (51), Australia and New Zealand (52), and Belgium and the Netherlands (53). In 14 of the 25 selected articles, collection took place in 2020; 6 of the 25 were collected in 2021; and the remaining 5 were collected over months in both 2020 and 2021. No studies were found with data collected in 2022 or later. Regarding participants, in 10 studies the sample consisted of health professionals, in 2 studies the sample was collected in the educational environment, and another 2 samples included self-employed workers. The remaining studies (11 out of 25) included workers from other occupational fields or general workers. Working from home or remote working was assessed in 3 of the 25 studies.
It was found that between 70.6% (43) and 26% (38) of the subjects in the included studies showed sickness presenteeism. In addition, a number of factors may have also favoured presenteeism or sickness presenteeism, such as mental health-related factors [burnout (34, 45, 49, 51), stress (33–35, 38, 42, 44, 45, 47, 49), depression (46), fear of COVID-19 (49), no well-being (16, 40), cyberbullying (51), sleep disturbance (34), concern about having enough food (41), social isolation (38), and no resilience (38)]; individual factors [poor marital relationship (31), health status (42), being young (38), attention-deficit/hyperactivity disorder symptoms (32), workers who experienced interrupted medical care (33, 40), low physical activity (38, 50), sedentary behaviours (52), having children (41), having health insurance (41), and having a chronic illness (38)]; factors related to the situation caused by COVID-19 [confinement (45), having symptoms of respiratory infectious disease (48), not volunteering to work on the frontline (47), impact on business operations, loss of contract, and risk of bankruptcy (16)]; and factors arising from working conditions [perceived organisational support (49), direct patient care (39), work functioning or task performance impairment (31, 42, 43, 53), work fatigue (34, 43), safety climate (22), workload (22), having no one to replace them (48), geographical distribution (48), transition from in-person to online modes of working (34, 35), salary of less than $35,000 (41), increase in working hours, work–family conflict (16)].
The included studies were assessed with the JBI critical appraisal tool, where analytical cross-sectional studies, qualitative research, and randomised controlled trials obtained medium-high scores.
Table 4 shows the characteristics of each of the 25 studies included in this review.

Table 4. Characteristics of the studies included in the systematic review.
The aim of this study was to assess the factors influencing presenteeism or sickness presenteeism and mental health of workers during the COVID-19 pandemic. In this sense, a series of factors related to mental health that may affect presenteeism have been found, as well as a number of factors specific to the individual, factors inherent to the situation caused by the COVID-19 pandemic, and factors derived from working conditions, among others.
Stress is one of the main contributing factors to working despite being ill which, in turn, may be one of the reasons why workers continue to work despite being ill (33–35, 38, 42, 44, 45, 47, 49), and in many cases workload, pressure from colleagues, and organisational culture play a part in this relationship (54). Stress was already related to sickness presenteeism prior to the COVID-19 pandemic, so it appears that COVID-19 is not the only factor that may influence sickness presenteeism as expected (55).
There are some high-pressure work environments, such as that of the study by Jia et al. (42), carried out on a sample of 4,261 medical staff, in which it was observed that in high-pressure environments, health problems are more likely to appear and medical staff are more likely to ignore their own health problems, thus increasing sickness presenteeism. In addition to the field of healthcare, it has been observed that the shift from face-to-face work to teleworking has led to workers being forced to be constantly online and on email, thereby generating constant stress, as they worry about losing their jobs (35). For many workers, they had to stay online at all times to prove their worth at work or to convince their employers that they were not avoiding their duties while working from home (56).
Continuous stressful situations can lead to sickness presenteeism due to burnout, as observed in the studies by Basar et al. (49), Ferreira et al. (51), Haehnle et al. (45), and Shimura et al. (34), and to symptoms of depression as seen in the study by Lee et al. (46), in which an association between SP and depression was found to be higher among blue-collar and less educated workers. In the case of the latter, the depressive symptoms of workers who were not able to obtain paid sick leave were 2.18 times higher than those who had the option to do so, hence symptoms of stress, depression, or anxiety were likely to appear. These excessive work demands may lead to presenteeism, while burnout may be a consequence resulting from this situation (9). In this regard, there are a number of factors that could buffer these demands, such as well-being (16, 40) or work engagement (55).
On the other hand, there was only one study that determined a relationship between nurses’ fear of contracting COVID-19 and stress-related presenteeism (49), which can lead to reduced performance, productivity, and efficiency in organisations (57). Other factors such as cyberbullying (51), sleep disturbance (34), concern about having enough food (41), social isolation (38), and no resilience (38) were also related to sickness presenteeism.
It was observed that having a chronic illness could be correlated with sickness presenteeism despite having a decompensated disease. In fact, at the onset of the disease, workers continue to work despite manifesting symptoms until they are forced to take sick leave due to exacerbation of the symptoms or prolonged duration of the disease (38). To avoid this problem, continued regular treatment is recommended in order to manage the disease and maintain health (56), as was the case among workers who experienced interrupted medical care (33, 40).
On the other hand, self-perception of one’s own health status determines whether workers assess their illness as sufficiently serious, moderate or mild for them to continue working or not (42). It is known that when working in high-pressure environments, health problems are more likely to occur and therefore, health is compromised (58). In this case, during the COVID-19 pandemic, fever was identified as one of the main symptoms used by workers to be absent from work as it may be related to COVID-19 (48). However, previously, this type of symptom was not a usual reason for taking sick leave and some workers, despite having fever, continued to work. In fact, feeling unable to take sick leave can negatively affect health and vice versa (59).
Other factors such as poor marital relationship (31), being young (38), attention-deficit/hyperactivity disorder symptoms (32), low physical activity (38, 50) and sedentary behaviours (52), having children (41), and having health insurance (41) may be related to sickness presenteeism.
In a study conducted in New South Wales between March and June 2021 on a sample of 122 veterinarians, it was determined that one of the factors associated with sickness presenteeism among those suffering from influenza-like illness during the COVID-19 pandemic was that they attended work despite having symptoms of respiratory infectious disease (48). The same could happen with COVID-19 signs and symptoms; people with mild symptoms may continue attending work despite the possible risk of virus transmission (57). This could again be explained by the sample’s high level of work engagement, the shortage of staff, and the company’s specific sick leave policies (36). According to Okawara et al. (33), workers do not attach the same importance to some signs and symptoms as to others. Those symptoms related to mental health, pain, burnout, or sleep were more susceptible to higher sickness presenteeism, whereas others such as signs and symptoms related to skin or hair problems, etc. showed moderate levels of sickness presenteeism and workers did see the need to take sick leave due to this type of symptomatology. This dichotomy will depend on the individual and whether they consider the symptoms to be sufficiently adverse or severe (60). In this regard, consideration should be given to what is meant by ‘unable to work due to illness’, i.e., is it a total inability to work, or is it an inability to perform functions at an expected level? (48).
Other factors contributing to presenteeism or sickness presenteeism during the COVID-19 pandemic (16) may be its impact on business operations, loss of contract and risk of bankruptcy, not volunteering to work on the front line (47), or confinement itself (45), which may in turn be indicators of poor socio-economic and working conditions (54).
Direct patient care (39) and workload (22) may be factors associated with presenteeism, which is particularly observed in services with a shortage of staff and with workers under high time pressure (5). Related to the above, perceived organisational support (49) and safety climate (22) may be contributing factors to sickness presenteeism. In some organisations, it is not easy for workers to choose to stay at home when they are sick, which may lead to frustration, resentment towards the company, depressive symptoms, and lower work engagement (61).
Only one of the studies (45) analysed the relationship between shift work and sickness presenteeism. As in other studies conducted prior to the COVID-19 pandemic (62), health workers who were on shifts attended work while sick more often than health workers who were not on shifts, and perhaps this may be influenced by their own biorhythms. Work-related fatigue may also be related to sickness presenteeism (34, 43), so long working hours need to be managed (62), communication and monitoring systems within the company should be improved, and a replacement plan should be in place to prevent workers from not taking sick leave on the grounds that there is no one to cover them (48).
Regarding the transition from in-person to online modes of working (34, 35), improving the work environment for workers while working from home is important to reduce the negative health outcomes associated with this type of activity, reduce absenteeism, and increase productivity.
Other variables related to working conditions may be work functioning or task performance impairment (31, 42, 43, 53), salary of less than $35,000 (41), increased working hours, work–family conflict (16), and geographical distribution (48).
It is estimated that the mean value of lost production per person per week, including absenteeism and presenteeism, can be in a range between €161 and €82 (53).
Contrary to many studies, there was one study in which the authors found no significant relationship between sickness presenteeism and age, sex, education of the self-employed, and size of the company (16). This could be explained by the characteristics of the sample, being young and highly engaged workers.
Finally, in a meta-analysis that assessed the status and factors influencing presenteeism among clinical nurses before the pandemic (63), it was observed that presenteeism scores were higher in publications prior to 2020, but in this case, they did find statistically significant differences in terms of age, sex, marital status, experience, region, and service groups that could be explained by the change in working conditions that a pandemic such as the COVID-19 one has brought about. In this line, and as has been detected, sickness presenteeism has been found to be a risk factor for future sickness absenteeism and may lead to decreased self-perceived health as observed in a systematic review conducted prior to the COVID-19 pandemic (64).
There are a number of limitations to this study. Although certain factors favouring or reducing the likelihood of sickness presenteeism have been detailed, it is possible that many of these factors are a consequence of sickness presenteeism or may even interact with it, and it might not be possible to discern cause from consequence. On the other hand, the samples were highly heterogeneous, and the time of collection and the instruments used also differed, making it difficult to compare the samples, which is why no meta-analysis was proposed. Most of the finally selected studies were cross-sectional and used hetero-administered instruments via online surveys, with the limitations that this method entails. Finally, each country has its own rules on sick leave entitlement, which may result in a person needing to continue to work despite being ill.
A number of factors have been identified that influence mental health and sickness presenteeism, such as factors directly related to mental health (burnout, stress, depression, fear of COVID-19, no well-being, cyberbullying, sleep disturbance, concern about having enough food, social isolation, and no resilience); individual factors (poor marital relationship, health status, being young, attention-deficit/hyperactivity disorder symptoms, workers who experienced interrupted medical care, low physical activity and sedentary behaviours, having children, having health insurance, and having a chronic illness); factors related to the situation caused by the COVID-19 pandemic (confinement, having symptoms of respiratory infectious disease, not volunteering to work on the front line, impact on business operations, loss of contract, and risk of bankruptcy); and factors arising from working conditions (perceived organisational support, direct patient care, work functioning impairment or task performance, work fatigue, safety climate, workload, having no one to cover them, geographical distribution, transition from in-person to online modes of working, salary of less than $35,000, increased working hours, and work–family conflict).
Identifying the key drivers of presenteeism or sickness presenteeism and understanding the underlying phenomena and origins will help to create a safe working environment and optimal organisational systems to protect vulnerable workers from medical and occupational adversity, especially in a pandemic context where changes, challenges, and consequences have had a considerable impact.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
JJG-I, JG-S, JA, RR, EC, CR-F, SM-I, DF-G, and ÁV-A: conceptualization, data curation, formal analysis, investigation, methodology, resources, software, supervision, validation, visualization, writing – original draft, and writing – review and editing. JJG-I, JG-S, JA, RR, EC, and ÁV-A: project administration. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1224332/full#supplementary-material
1. Koopman, C, Pelletier, KR, Murray, JF, Sharda, CE, Berger, ML, Turpin, RS, et al. Stanford presenteeism scale: health status and employee productivity. J Occup Environ Med. (2002) 44:14–20. doi: 10.1097/00043764-200201000-00004
2. Demerouti, E, Le Blanc, PM, Bakker, AB, Schaufeli, WB, and Hox, J. Present but sick: a three-wave study on job demands, presenteeism and burnout. Career Dev Int. (2009) 14:50–68. doi: 10.1108/13620430910933574
3. Johns, G. Presenteeism in the workplace: a review and research agenda. J Organ Behav. (2010) 31:519–42. doi: 10.1002/job.630
4. d’Errico, A, Ardito, C, and Leombruni, R. Work organization, exposure to workplace hazards and sickness presenteeism in the European employed population. Am J Ind Med. (2016) 59:57–72. doi: 10.1002/ajim.22522
5. Loeppke, R, Taitel, M, Haufle, V, Parry, T, Kessler, RC, and Jinnett, K. Health and productivity as a business strategy: a multiemployer study. J Occup Environ Med. (2009) 51:411–28. doi: 10.1097/JOM.0b013e3181a39180
6. Aronsson, G, and Gustafsson, K. Sickness presenteeism: prevalence, attendance-pressure factors, and an outline of a model for research. J Occup Environ Med. (2005) 47:958–66. doi: 10.1097/01.jom.0000177219.75677.17
7. McGregor, A, Magee, CA, Caputi, P, and Iverson, D. A job demands-resources approach to presenteeism. Career Dev Int. (2016) 21:402–18. doi: 10.1108/CDI-01-2016-0002
8. Nordenmark, M, Vinberg, S, and Strandh, M. Job control and demands, work-life balance and wellbeing among self-employed men and women in Europe. Vulnerable Groups Inclusion. (2012) 3:18896. doi: 10.3402/vgi.v3i0.18896
9. Pohling, R, Buruck, G, Jungbauer, KL, and Leiter, MP. Work-related factors of presenteeism: the mediating role of mental and physical health. J Occup Health Psychol. (2016) 21:220–34. doi: 10.1037/a0039670
10. Miraglia, M, and Johns, G. Going to work ill: a meta-analysis of the correlates of presenteeism and a dual-path model. J Occup Health Psychol. (2016) 21:261–83. doi: 10.1037/ocp0000015
11. Webster, RK, Liu, R, Karimullina, K, Hall, I, Amlôt, R, and Rubin, GJ. A systematic review of infectious illness presenteeism: prevalence, reasons and risk factors. BMC Public Health. (2019) 19:799. doi: 10.1186/s12889-019-7138-x
12. Toyoshima, K, Inoue, T, Shimura, A, Masuya, J, Ichiki, M, Fujimura, Y, et al. Associations between the depressive symptoms, subjective cognitive function, and presenteeism of Japanese adult workers: a cross-sectional survey study. Biopsychosoc Med. (2020) 14:1–7. doi: 10.1186/s13030-020-00183-x
13. Johnston, DA, Harvey, SB, Glozier, N, Calvo, RA, Christensen, H, and Deady, M. The relationship between depression symptoms, absenteeism and presenteeism. J Affect Disord. (2019) 256:536–40. doi: 10.1016/j.jad.2019.06.041
14. Cambridge University Press. WORKER | English Meaning - Cambridge Dictionary. Cambridge: Cambridge University Press (2023).
15. Conway, PM, Hogh, A, Rugulies, R, and Hansen, ÅM. Is sickness presenteeism a risk factor for depression? A Danish 2-year follow-up study. J Occup Environ Med. (2014) 56:595–603. doi: 10.1097/JOM.0000000000000177
16. Nordenmark, M, Hagqvist, E, and Vinberg, S. Sickness presenteeism among the self-employed and employed in northwestern Europe—the importance of time demands. Saf Health Work. (2019) 10:224–8. doi: 10.1016/j.shaw.2019.01.003
17. Goncalves, J, and Martins, PS. The effect of self-employment on health: evidence from longitudinal social security data. SSRN Electron J. (2021) 57:1527–43. doi: 10.2139/ssrn.3117309
18. Vinberg, S, Landstad, BJ, Tjulin, A, and Nordenmark, M. Sickness presenteeism among the Swedish self-employed during the Covid-19 pandemic. Front Psychol. (2021) 12:12. doi: 10.3389/fpsyg.2021.723036
19. Brborović, H, Daka, Q, Dakaj, K, and Brborović, O. Antecedents and associations of sickness presenteeism and sickness absenteeism in nurses: a systematic review. Int J Nurs Pract. (2017) 23:12598. doi: 10.1111/ijn.12598
20. Garrow, V. Presenteeism: a review of current thinking. Brighton: Institute for Employment Studies (2016):1–84.
21. Rainbow, JG, and Steege, LM. Presenteeism in nursing: an evolutionary concept analysis. Nurs Outlook. (2017) 65:615–23. doi: 10.1016/j.outlook.2017.03.005
22. Elstad, JI, and Vabø, M. Job stress, sickness absence and sickness presenteeism in Nordic elderly care. Scand J Public Health. (2008) 36:467–74. doi: 10.1177/1403494808089557
23. Ruiz-Frutos, C, Ortega-Moreno, M, Dias, A, Bernardes, JM, García-Iglesias, JJ, and Gómez-Salgado, J. Information on COVID-19 and psychological distress in a sample of non-health workers during the pandemic period. Int J Environ Res Public Health. (2020) 17:1–18. doi: 10.3390/ijerph17196982
24. Mansour, S, Azeem, MF, Dollard, M, and Potter, R. How psychosocial safety climate helped alleviate work intensification effects on presenteeism during the COVID-19 crisis? A moderated mediation model. Int J Environ Res Public Health. (2022) 19:13673. doi: 10.3390/ijerph192013673
25. Jaspal, R, and Breakwell, GM. Socio-economic inequalities in social network, loneliness and mental health during the COVID-19 pandemic. Int J Soc Psychiatry. (2020) 68:155–65. doi: 10.1177/0020764020976694
26. Moola, S, Munn, Z, Sears, K, Sfetcu, R, Currie, M, Lisy, K, et al. Conducting systematic reviews of association (etiology): the Joanna Briggs Institute’s approach. Int J Evid Based Healthc. (2015) 13:163–9. doi: 10.1097/XEB.0000000000000064
27. Moher, D, Liberati, A, and Tetzlaff, JADPG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. (2009) 151:264–9. doi: 10.7326/0003-4819-151-4-200908180-00135
28. Page, MJ, McKenzie, JE, Bossuyt, P, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The prisma 2020 statement: an updated guideline for reporting systematic reviews. Med. Fluminensis. (2020) 57:444–65. doi: 10.1136/bmj.n71
29. Munn, Z, Stern, C, Aromataris, E, Lockwood, C, and Jordan, Z. What kind of systematic review should i conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med Res Methodol. (2018) 18:5. doi: 10.1186/s12874-017-0468-4
30. Moola, S, Munn, Z, Tufanaru, C, Aromataris, E, Sears, K, Sfetcu, R, et al. In: EMZ Aromataris, editor. JBI Manual for Evidence Synthesis. Adelaide: JBI (2020)
31. Lockwood, C, Munn, Z, and Porritt, K. Qualitative research synthesis: methodological guidance for systematic reviewers utilizing meta-aggregation. Int J Evid Based Healthc. (2015) 13:179–87. doi: 10.1097/XEB.0000000000000062
32. Tufanaru, C, Munn, Z, Aromataris, E, and Campbell, JHL. Chapter 3: systematic reviews of effectiveness In: Z Munn and E Aromataris, editors. JBI Manual for Evidence Synthesis. JBI Manual for Evidence Synthesis. Adelaida: The Joanna Briggs Institute (2020).
33. Fujino, Y, Okawara, M, Hino, A, Muramatsu, K, Nagata, T, Tateishi, S, et al. A prospective cohort study of presenteeism and increased risk of divorce among Japanese workers. J Occup Environ Med. (2022) 64:E695–9. doi: 10.1097/JOM.0000000000002670
34. Nakai, T, Tsuji, T, Tsuda, H, Sotodate, T, Namba, Y, Uenishi, T, et al. Working conditions, work productivity, quality of life, and depressive symptoms in undiagnosed adults with and without attention-deficit/hyperactivity disorder (ADHD) symptoms during the COVID-19 pandemic. Neuropsychiatr Dis Treat. (2022) 18:1561–72. doi: 10.2147/NDT.S358085
35. Okawara, M, Ishimaru, T, Tateishi, S, Hino, A, Tsuji, M, Ogami, A, et al. Treatment interruption is a risk factor for sickness presenteeism: a large-scale cross-sectional study during the COVID-19 pandemic. J Occup Health. (2022) 64:e12313. doi: 10.1002/1348-9585.12313
36. Shimura, A, Yokoi, K, Ishibashi, Y, Akatsuka, Y, and Inoue, T. Remote work decreases psychological and physical stress responses, but full-remote work increases presenteeism. Front Psychol. (2021) 12:730969. doi: 10.3389/fpsyg.2021.730969
37. Adisa, TA, Ogbonnaya, C, and Adekoya, OD. Remote working and employee engagement: a qualitative study of British workers during the pandemic. Inf Technol People. (2021) 36:1835–1850. doi: 10.1108/ITP-12-2020-0850
38. Blake, H, Yildirim, M, Wood, B, Knowles, S, Mancini, H, Coyne, E, et al. Covid-well: evaluation of the implementation of supported wellbeing centres for hospital employees during the COVID-19 pandemic. Int J Environ Res Public Health. (2020) 17:1–22. doi: 10.3390/ijerph17249401
39. Gnanapragasam, SN, Tinch-Taylor, R, Scott, HR, Hegarty, S, Souliou, E, Bhundia, R, et al. Multicentre, England-wide randomised controlled trial of the “foundations” smartphone application in improving mental health and well-being in a healthcare worker population. Br J Psychiatry. (2022) 2:1–9. doi: 10.1192/bjp.2022.103
40. Van Der Feltz-Cornelis, CM, Varley, D, Allgar, VL, and de Beurs, E. Workplace stress, presenteeism, absenteeism, and resilience amongst university staff and students in the COVID-19 lockdown. Front Psych. (2020) 11:588803. doi: 10.3389/fpsyt.2020.588803
41. Cheslack-Postava, K, Bresnahan, M, Ryan, M, Musa, GJ, Amsel, L, DiMaggio, C, et al. Occupational conditions associated with negative mental health outcomes in New York state health professionals during the COVID-19 pandemic. J Occup Environ Med. (2022) 64:E417–23. doi: 10.1097/JOM.0000000000002566
42. Sagui-Henson, SJ, Prescott, MR, Corcoran, JB, Pillai, S, Mattila, L, Mathur, S, et al. Effectiveness of evidence-based Telecoaching delivered through an employer-sponsored mental health benefits platform. Telemed e-Health. (2022) 28:486–94. doi: 10.1089/tmj.2020.0555
43. Tilchin, C, Dayton, L, and Latkin, CA. Socioeconomic factors associated with an intention to work while sick from COVID-19. J Occup Environ Med. (2021) 63:363–8. doi: 10.1097/JOM.0000000000002147
44. Jia, H, Shang, P, Gao, S, Cao, P, Yu, J, and Yu, X. Work stress, health status and presenteeism in relation to task performance among Chinese medical staff during COVID-19 pandemic. Front Public Health. (2022) 10:10. doi: 10.3389/fpubh.2022.836113
45. Li, Y, Guo, B, Wang, Y, Lv, X, Li, R, Guan, X, et al. Serial-multiple mediation of job burnout and fatigue in the relationship between sickness presenteeism and productivity loss in nurses: a Multicenter cross-sectional study. Front Public Heal. (2022) 9:9. doi: 10.3389/fpubh.2021.812737
46. Schulze, S, Merz, S, Thier, A, Tallarek, M, König, F, Uhlenbrock, G, et al. Psychosocial burden in nurses working in nursing homes during the Covid-19 pandemic: a cross-sectional study with quantitative and qualitative data. BMC Health Serv Res. (2022) 22:949. doi: 10.1186/s12913-022-08333-3
47. Haehnle, S, Fegert, JMJM, Koenig, E, Hoffmann, U, Hähnle, S, Fegert, JMJM, et al. Burnout symptoms among child and adolescent psychiatric/psychotherapy professionals during the 2020/2021 winter lockdown of the Covid-19 pandemic. Z Kinder Jugendpsychiatr Psychother. (2022) 50:300–11. doi: 10.1024/1422-4917/a000876
48. Lee, K-SS, Lee, D-WW, Park, JY, Kim, H-YY, Yun, J-YY, Hong, Y-CC, et al. Association between sickness presenteeism and depressive symptoms in Korean workers during the COVID-19 pandemic: a cross-sectional study. J Affect Disord. (2022) 319:344–51. doi: 10.1016/j.jad.2022.09.029
49. Han, S, Choi, S, Cho, SH, Lee, J, and Yun, JY. Associations between the working experiences at frontline of COVID-19 pandemic and mental health of Korean public health doctors. BMC Psychiatry. (2021) 21:298. doi: 10.1186/s12888-021-03291-2
50. Pasfield, K, Gottlieb, T, Tartari, E, Ward, MP, and Quain, A. Sickness presenteeism associated with influenza-like illness in veterinarians working in New South Wales: results of a state-wide survey. Aust Vet J. (2022) 100:243–53. doi: 10.1111/avj.13153
51. Basar, U, Dogan, A, and Ertugrul, B. Antecedents of nurse burnout during a pandemic: managerial way out. J Health Manag. (2022) 2022:1–10. doi: 10.1177/09720634221121364
52. Žilinskas, E, Puteikis, K, Mameniškienė, R, Zilinskas, E, Puteikis, K, and Mameniskiene, R. Quality of sleep and work productivity among white-collar workers during the COVID-19 pandemic. Medicina. (2022) 58:883. doi: 10.3390/medicina58070883
53. Ferreira, P d C, Barros, A, Pereira, N, Marques Pinto, A, and Veiga Simão, AM. How presenteeism shaped teacher burnout in cyberbullying among students during the COVID-19 pandemic. Front Psychol. (2021) 12:745252. doi: 10.3389/fpsyg.2021.745252
54. Hunter, JR, Meiring, RM, Cripps, A, Suppiah, HT, Vicendese, D, Kingsley, MI, et al. Relationships between physical activity, work ability, absenteeism and presenteeism in Australian and New Zealand adults during COVID-19. Int J Environ Res Public Health. (2021) 18:12563. doi: 10.3390/ijerph182312563
55. van Ballegooijen, H, Goossens, L, Bruin, RH, Michels, RR, and Krol, M. Concerns, quality of life, access to care and productivity of the general population during the first 8 weeks of the coronavirus lockdown in Belgium and the Netherlands. BMC Health Serv Res. (2021) 21:227. doi: 10.1186/s12913-021-06240-7
56. Daniels, S, Wei, H, Han, Y, Catt, H, Denning, DW, Hall, I, et al. Risk factors associated with respiratory infectious disease-related presenteeism: a rapid review. BMC Public Health. (2021) 21:1955–12. doi: 10.1186/s12889-021-12008-9
57. De Oliveira, TCDS, Muzeka, ALP, Batista, E, Dos Santos, GNFE, Da, RLFI, Legey, ÂLC, et al. Worker health impacts from working from home during the COVID-19 pandemic. Work J Prev Assess Rehabil. (2022) 72:9–17. doi: 10.3233/WOR-210553
58. Hansen, CD, and Andersen, JH. Going ill to work--what personal circumstances, attitudes and work-related factors are associated with sickness presenteeism? Soc Sci Med. (2008) 67:956–64. doi: 10.1016/j.socscimed.2008.05.022
59. Kim, J, Kim, YK, Leem, SH, and Won, JU. Association between job-related stress and experience of presenteeism among Korean workers stratified on the presence of depression. Ann. Occup Environ Med. (2019) 31:e26. doi: 10.35371/aoem.2019.31.e26
60. Prasad, KDV, and Vaidya, R. Occupational stress and its impact on work-life balance and psychological well-being of remote working women employees in information technology enabled sector during Covid-19 pandemic: an empirical study in Hyderabad metro. Rev Int Geogr Educ Online. (2021) 11:619–30.
61. Brunner, B, Igic, I, Keller, AC, and Wieser, S. Who gains the most from improving working conditions? Health-related absenteeism and presenteeism due to stress at work. Eur J Health Econ. (2019) 20:1165–80. doi: 10.1007/s10198-019-01084-9
62. Chudasama, YV, Gillies, CL, Zaccardi, F, Coles, B, Davies, MJ, Seidu, S, et al. Impact of COVID-19 on routine care for chronic diseases: a global survey of views from healthcare professionals. Diabetes Metab Syndr. (2020) 14:965–7. doi: 10.1016/j.dsx.2020.06.042
63. Ni, WY, Wang, JL, Yun, J, Xie, WQ, Ma, C, and Su, SH. The status and influencing factors of presenteeism among clinical nurses: a systematic review. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. (2023) 41:286–93. doi: 10.3760/cma.j.cn121094-20220617-00326
Keywords: COVID-19, mental health, occupational health, presenteeism, workers
Citation: García-Iglesias JJ, Gómez-Salgado J, Apostolo J, Rodrigues R, Costa EI, Ruiz-Frutos C, Martínez-Isasi S, Fernández-García D and Vilches-Arenas & (2023) Presenteeism and mental health of workers during the COVID-19 pandemic: a systematic review. Front. Public Health. 11:1224332. doi: 10.3389/fpubh.2023.1224332
Edited by:
Yoshihisa Fujino, University of Occupational and Environmental Health Japan, JapanReviewed by:
Vasiliki Eirini Chatzea, Hellenic Mediterranean University, GreeceCopyright © 2023 García-Iglesias, Gómez-Salgado, Apostolo, Rodrigues, Costa, Ruiz-Frutos, Martínez-Isasi, Fernández-García and Vilches-Arenas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan Gómez-Salgado, c2FsZ2Fkb0B1aHUuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.