 Guillermo Baudelio Gómez-Morales1
Guillermo Baudelio Gómez-Morales1 Brenda Sofía Rosas-Torres2
Brenda Sofía Rosas-Torres2 Williams Jesús Hernández-Jiménez1
Williams Jesús Hernández-Jiménez1 Estefanía Mattenberger-Cantú2
Estefanía Mattenberger-Cantú2 Javier Vargas-Villarreal2
Javier Vargas-Villarreal2 Horacio Almanza-Reyes3*
Horacio Almanza-Reyes3* Francisco González-Salazar1,2*
Francisco González-Salazar1,2*- 1Northeast Biomedical Research Center, Institute of Mexican Social Security, Monterrey, Mexico
- 2Basic Science Department, University of Monterrey, Garza García, Mexico
- 3Faculty of Medicine and Psychology of the Autonomous, University of Baja California, Tijuana, Mexico
Introduction: Hispanic immigrants are a fast-growing population in the United States of America (USA) that disproportionately suffer from chronic diseases. Despite the increasing prevalence of obesity in Latin-American countries, only a few studies have examined the onset of chronic diseases in Mexican and Central American migrants in Mexico.
Objective: The objective of this study is to determine the prevalence of obesity, diabetes, and hypertension in Central American immigrants who are in the process of traveling through northeastern Mexico to the United States.
Methods: An observational, descriptive, cross-sectional study was conducted among migrants, mostly Central Americans. Migrants who agreed to participate in the study were interviewed face-to-face by researchers to obtain their sociodemographic data. To obtain the prevalence, many health indicators related to obesity, diabetes, and hypertension, including weight, height, fasting glucose, and blood pressure, were measured.
Results: In total, 520 migrants were interviewed; sociodemographic data indicated that most participants were men (76%), from Honduras (72.6%), single (61.2%), and have elementary level of education (48.6%). The somatometric evaluation revealed that 28.9% were diagnosed as overweight, 10.7% with obesity, and 3.3% with malnutrition. Of less prevalence, 8.8% were detected with hypertension and 4.6% had fasting hyperglycemia. The mean participant age was 29.11 ± 10.00 years. For each participant, the average weight was 66.72 ± 13.09 kg; the average height was 1.64 ± 0.08 m; the average body mass index (BMI) was 24.59 ± 4.32; the mean systolic and diastolic pressures were 116.26 ± 15.13 and 74 ± 9.65, respectively; and the average glycemia was 100.97 ± 21.99. El Salvador showed the highest proportion of people with diabetes (14.7%). Women who participated in this study had a higher proportion of obesity (23.4%, p = 0.02) and overweight (36.2%) than men (8.4 and 29.2%, respectively). People from Mexico, Nicaragua, and Honduras reported a high prevalence of overweight participants (63.6, 47.4, and 30.7%, respectively), while people from El Salvador and Nicaragua had a high prevalence of obese participants (23.5 and 21.1%, respectively).
Conclusion: We found significant differences in the rates of obesity, diabetes, and hypertension between groups of Central American migrants and their place of origin, age, educational level, and gender. Our findings highlight the importance of exploring differences within groups of Central American migrants traveling through northeastern Mexico to the United States, which may explain several health indicators.
1 Introduction
Obesity is a worldwide epidemic caused by an increase in the consumption of foods with poor nutritional value, rich in sugars with high fructose content, and with saturated trans fats. This, accompanied by a lack of exercise, causes the accumulation of fat in tissues (1). The United States and Mexico have high rates of obesity (2). However, Central American countries are not exempt from suffering from eating disorders due to bad eating habits that cause an imbalance between energy intake and expenditure (3–6). Obesity is often accompanied by significant comorbidities such as diabetes and hypertension (7, 8). It is important to identify these disorders early because when diabetes and hypertension become complicated, they can be extremely disabling and may lead to significant economic losses in the health sector due to long-term treatments. In Mexico, the prevalence of diabetes has reached 14% of the adult population and is one of the leading causes of mortality, representing 14% of all deaths in 1 year (9). Hispanic immigrants are a fast-growing population in the United States. According to data from the United States census (10), the Latin population reached a total of 62.5 million people in 2021, which shows a 19% increase from the 50.5 million of Latinos in 2010. Therefore, there is a high prevalence of general obesity among Latin immigrants (11).
Immigrants are characterized by being young people who regularly travel alone and who would ideally be healthy and without any chronic-degenerative diseases (12). However, with increasing frequency, immigration populations are shifting to include caravans or groups where entire families travel to the United States (13). There are reports indicating that Latino, Mexican, and Central American migrants change their eating habits and suffer from obesity while living in the United States for years (14). To date, the presence of obesity, diabetes, and hypertension has not been characterized in the population of Central American migrants while transiting through the Mexican territory. Most of the studies are of Central American migrants in the United States (15). Thus, the main objective of this research was to determine the prevalence of obesity, diabetes, and hypertension in Central American immigrants in the process of traveling through northeastern Mexico to the United States. Comparing the prevalence of these conditions in the country of transit (northeastern Mexico) with those reported in the countries of destinations (United States) and ejection (Central American countries) will guide in decision-making of public policies and programs to achieve significant effectiveness and efficiency in the administration of resources to prevent diabetes, obesity, and hypertension across all the regions.
2 Materials and methods
An observational, descriptive, cross-sectional study was carried out in a migrant shelter called Casa Nicolás. This shelter is located in Guadalupe Nuevo Leon, a metropolitan zone of Monterrey Mexico, and hosts approximately 1,500 migrants per year. Guadalupe city is a town with a population of 643,143 habitants. This investigation was carried out from January 2019 to March 2021. During this period, the majority of the people hosted in this shelter were Central Americans, mainly from Honduras, Guatemala, Nicaragua, and El Salvador.
2.1 Sample and sample size
Considering a population of 1,500 migrants in 1 year, a sample size was calculated using Fisterra’s online sample size calculator. With a confidence level of 95%, we looked for a sample size sufficient to detect a proportion of diabetes of 4% with an accuracy of 2%. In this way, the calculated sample size was 369 migrants, with an adjustment to 434 individuals consisting of up to 15% of the individuals who did not want to perform all the tests. The sampling was non-probabilistic by quota. The data were collected in the shelter every week during the year 2019 until March 2021 to complete the desired sample size.
2.2 Selection criteria
Migrants over the age of 13 years who spent the night in the shelter were asked for their signed written consent to participate in the study. People over 18 years of age signed a consent, while those under 18 years of age were asked for their signed assent along with parental consent. Migrants older than 13 years of any gender, nationality, or religion who gave consent to participate were included in this study. Migrants who stated that they had left their country of origin for more than 6 months or who commented that they had lived in Monterrey, Mexico for a longer time were excluded. This is because after spending an average of 6 months living in Guadalupe, Nuevo León, they adapt to the food and customs that are very different from those of their country of origin. People whose surveys were illegible were removed from the study.
2.3 Procedures
The people who agreed to participate were interviewed early in the morning to collect their sociodemographic data. After completing the interview, the following procedures shown in Sections 3.4–3.8 were performed.
2.4 Weight and height
With the least amount of clothing possible, on an empty stomach, patients were weighed on a Nuevo León S.A. DE C.V., brand pedestal scale. The scale model was P-220, and the material was iron, with measurements of 26.8 cm × 36.8 cm, with a capacity of 220 kg. The manufacturing place is Monterrey, Mexico. Weight was recorded in kilograms with a precision of one decimal.
2.5 Height
On a pedestal scale, with their back facing the wall, height was measured using the stadiometer of the scale brand Nuevo León S.A. DE C.V. Height was recorded in meters.
2.6 Glucose
Fasting blood glucose was determined using a Johnson and Johnson brand glucometer, model OneTouch Ultra TM 2. After following a hand hygiene routine and cleaning with a 70% isopropyl alcohol swab, a finger was punctured with a lancet and pressed in the same manner to extract a drop of blood. This drop of blood was placed on a Johnson and Johnson glucose test strip, model OneTouch Ultra. The reading from the device was manually transcribed with a pencil or pen onto the data collection sheet designed for this purpose. When fasting glucose value was greater than 126 mg/Dl, the patient was considered to have diabetes mellitus (DM), whereas the patient was considered without DM when the reading was 125 mg/dL or less.
2.7 Blood pressure
Blood pressure was taken in all individuals who accepted the procedure. The conditions for measuring blood pressure were as follows: migrants had to be seated and at rest (participants were asked to make inhalations and exhalations repeatedly to be completely relaxed) for at least 15 min before taking the blood pressure sample using a Microlife model BP3UG1-2E automatic blood pressure measuring cuff. The cuff was placed on the patient’s left arm, two finger widths above the elbow crease, and adjusted so that it was not too tight or too loose on the arm. The cuff was properly aligned with the brachial artery, and the start button of the device was pressed to begin measurement. The systolic and diastolic blood pressure readings were recorded. Data were manually collected with a pen on the corresponding data collection sheet. For the registry, individuals were considered to have arterial hypertension (HBP) when the systolic pressure was greater than or equal to 140 mmHg and the diastolic pressure was greater than or equal to 90 mmHg. Individuals were considered to be without HBP when the systolic pressure value was less than 140 mmHg and the diastolic pressure was less than 90 mmHg.
2.8 Somatometric diagnosis
To carry out the somatometric diagnosis of the individuals, the formula of weight in kg/ = body mass index (BMI) was used. The result of this formula was compared with internationally valid somatometric diagnostic tables by the World Health Organization (WHO) (16). The BMI figures less than 18.5 m2SC indicate underweight, as shown in Table 1 as malnutrition. The figures between 18.5 m2SC and 24.9 m2SC indicate normal weight. The figures between 25 m2SC and 29.9 m2SC indicate overweight, and the values greater than or equal to 30 m2SC indicate obesity.
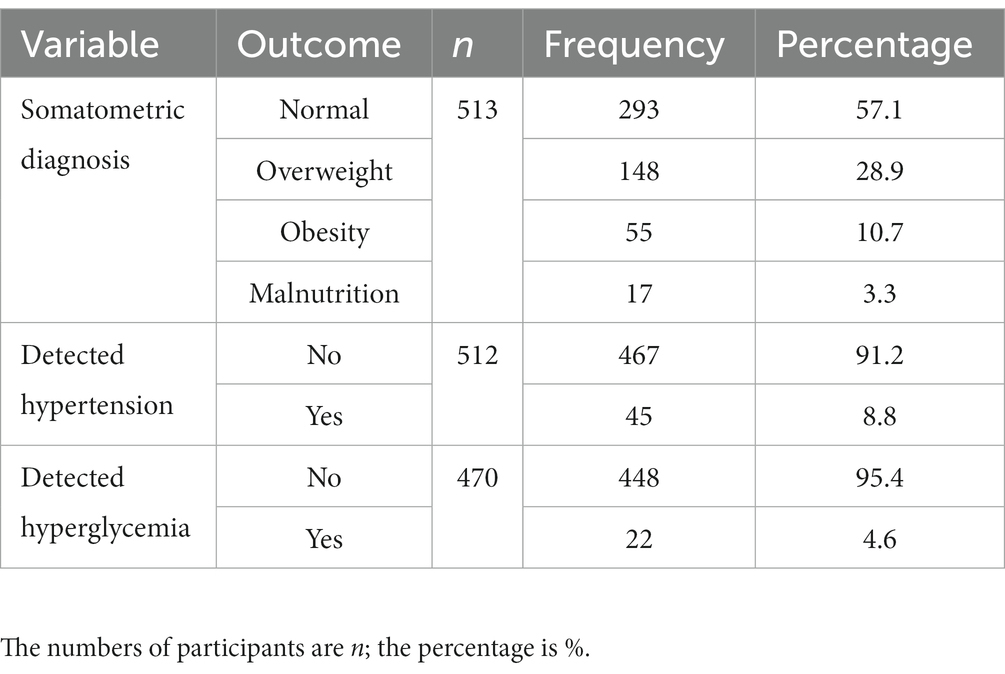
Table 1. Somatometric diagnosis, diabetes, and hypertension.
2.9 Statistical analysis
The data of the people previously stored in a Microsoft Excel® database were analyzed with the help of the IBM® SPSS® Statistics V25 program. All quantitative data were used to calculate means and standard deviations, while qualitative data were used to calculate proportions. The proportion of obesity, overweight, diabetes, and hypertension was calculated by dividing the number of people with the characteristic over the total number of individuals evaluated with this procedure. Finally, the associations between the presence of obesity, overweight, diabetes, and hypertension were calculated, contrasting with the proportions of the rest of the independent variables, for which the chi-square statistic was used. Differences between proportions were considered statistically significant when value of ps were less than ≤0.05.
2.10 Ethical considerations
To carry out this research, the protocol was first registered in the ethics and research committee of the University of Monterrey, and it was registered with the number 042016-CIE. Authorization was then requested from the shelter authorities in which they agreed to the weekly survey of the migrants since their population changes every 3 days due to the shelter’s stay regulations. All adult participants signed an informed consent, while the minors signed an assent document and their parents signed the informed consent. During the course of this project, international laws for conducting research studies with humans were respected, including the Helsinki Code and the general health law of the United Mexican States. Patient data were kept confidential at all times.
3 Results
3.1 Sociodemographic characteristics of the study
For the present study, there were a total of 520 participants (Table 2). According to sociodemographic data, the majority of participants (76%) were men, and they mainly came from Honduras (72.6%). Most of the participants were single (61.2%) and had elementary level of education (48.6%). Most of the immigrants (66.1%) traveled alone, 31.2% traveled with family, and ony 2.8% traveled with friends. The mean age of the migrants traveling from El Salvador was 27.8 ± 7.38 years, while the mean age of migrants traveling from Nicaragua was 39.0 ± 12.15 years, from Guatemala was 31.2 ± 9.86 years, and from Mexico was 30.0 ± 11.51 years.
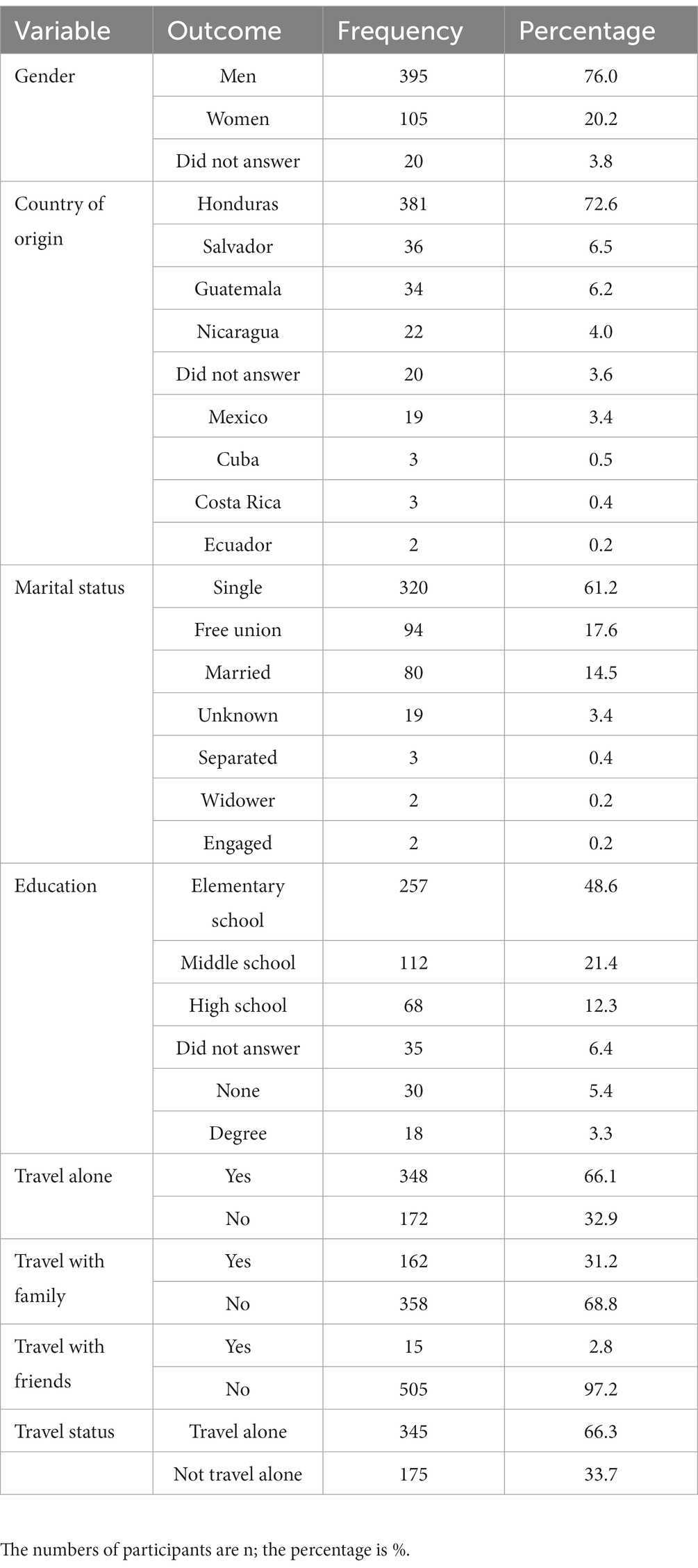
Table 2. Sociodemographic characteristics.
3.2 Comorbidities in the study
Regarding previous comorbidities diagnosed, it was found that, among the people interviewed, 3.2% referred to have a previous diagnosis of diabetes and 4.5% of hypertension; however, only 0.7% of the people were suffering from psychiatric/mental illness. Additionally, 88.1% consumed alcoholic beverages, whereas 29.8% mentioned smoking (Table 3).
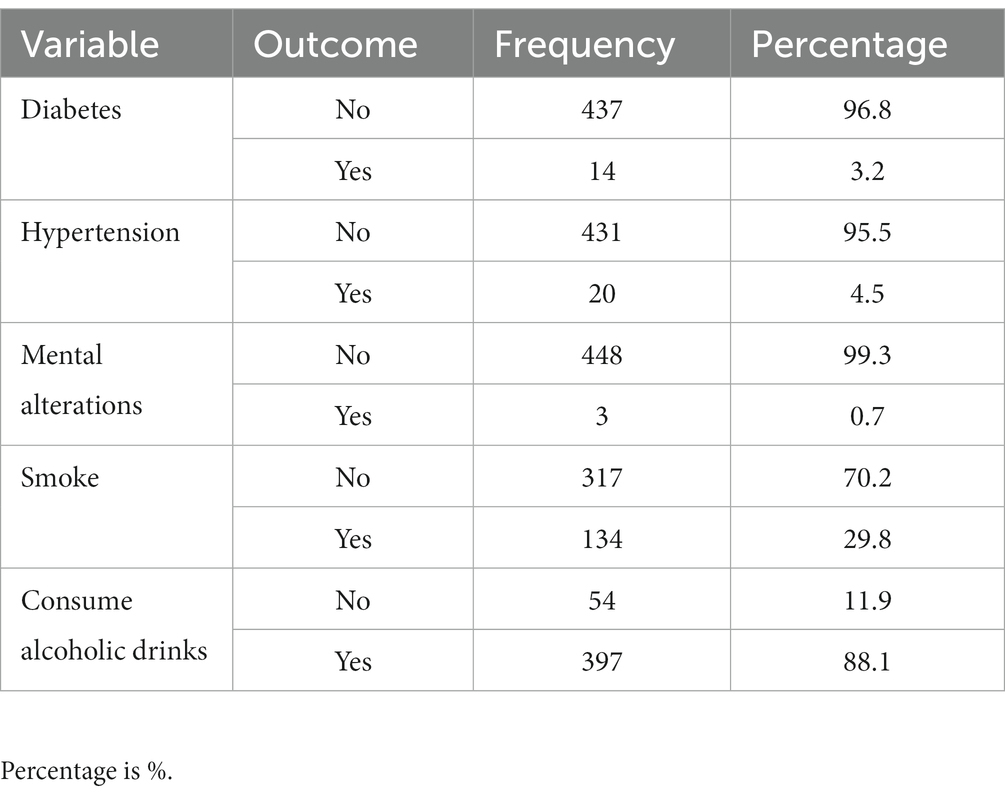
Table 3. Comorbidities according to survey results.
3.3 Somatometric diagnosis, diabetes, and hypertension of the study
Regarding the somatometric diagnosis (reported in Table 1), 28.9% were diagnosed as overweight, 10.7% with obesity, and 3.3% with malnutrition; this adds up to 42.9% of people who have somatometric issues. In addition, only 8.8% of people were detected with hypertension, while 4.6% had fasting hyperglycemia. As shown in Table 4, for each participant, the average age was 29.11 ± 10.00 years; the average weight and height were 66.72 ± 13.09 kg and 1.64 ± 0.08 m, respectively; the average BMI was 24.59 ± 4.32 kg/m2; the mean systolic and diastolic pressures were 116.26 ± 15.13 mmHg and 74 ± 9.65 mmHg, respectively; and the average glycemia was 100.97 ± 21.99 mg/dL. Table 5 shows the cross-tabulation of sociodemographic characteristics and diabetes. In terms of gender, it was found that men had hyperglycemia more often than women, but it was not statistically significant. Additionally, people with a married status and those who traveled alone had a higher proportion of diabetes, and those with the highest proportion of diabetes had a higher level of education, but none of these differences were statistically significant. However, it was found to be statistically significant (p = 0.02) that El Salvador had the highest proportion of people with diabetes (14.7%) compared to migrants in other countries such as Guatemala or Mexico where no cases of diabetes were reported.
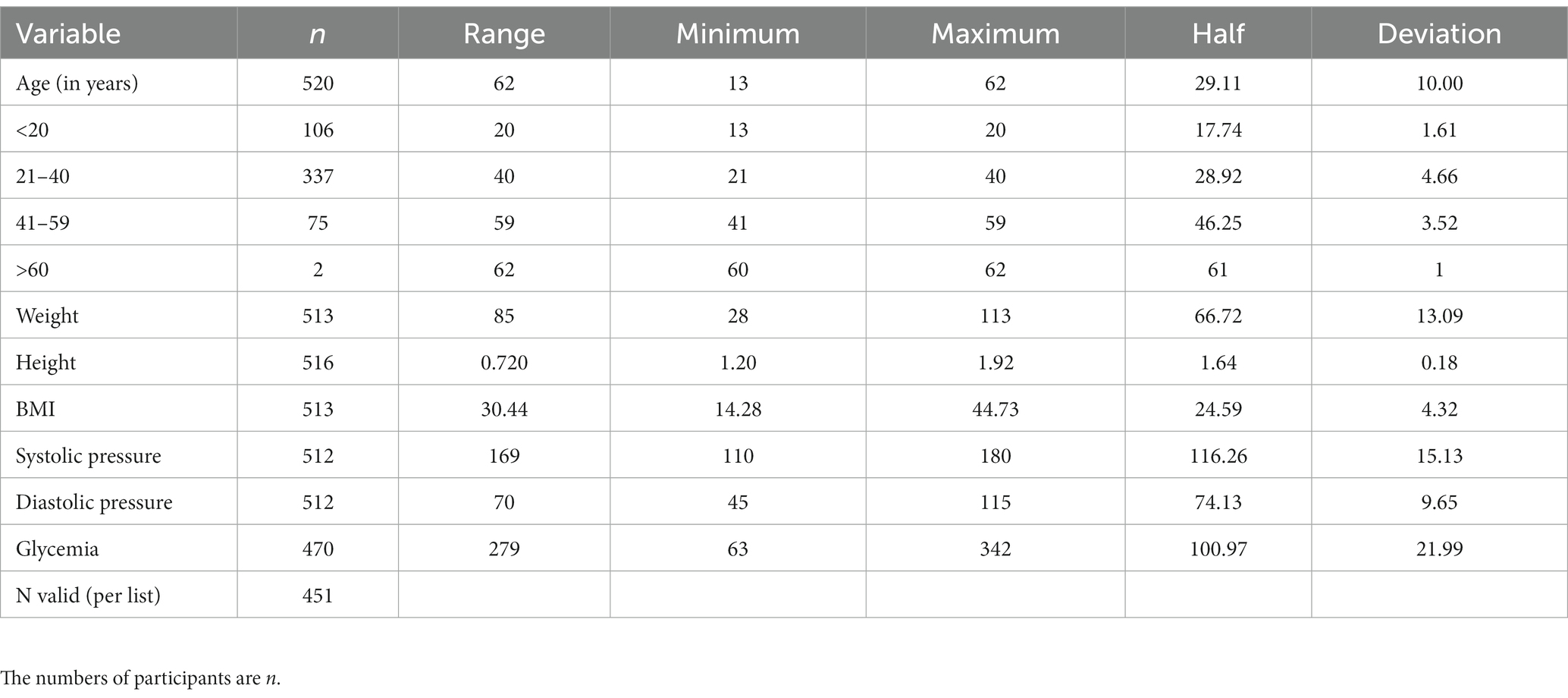
Table 4. Relationship between anthropometric characteristics, hypertension, and diabetes.
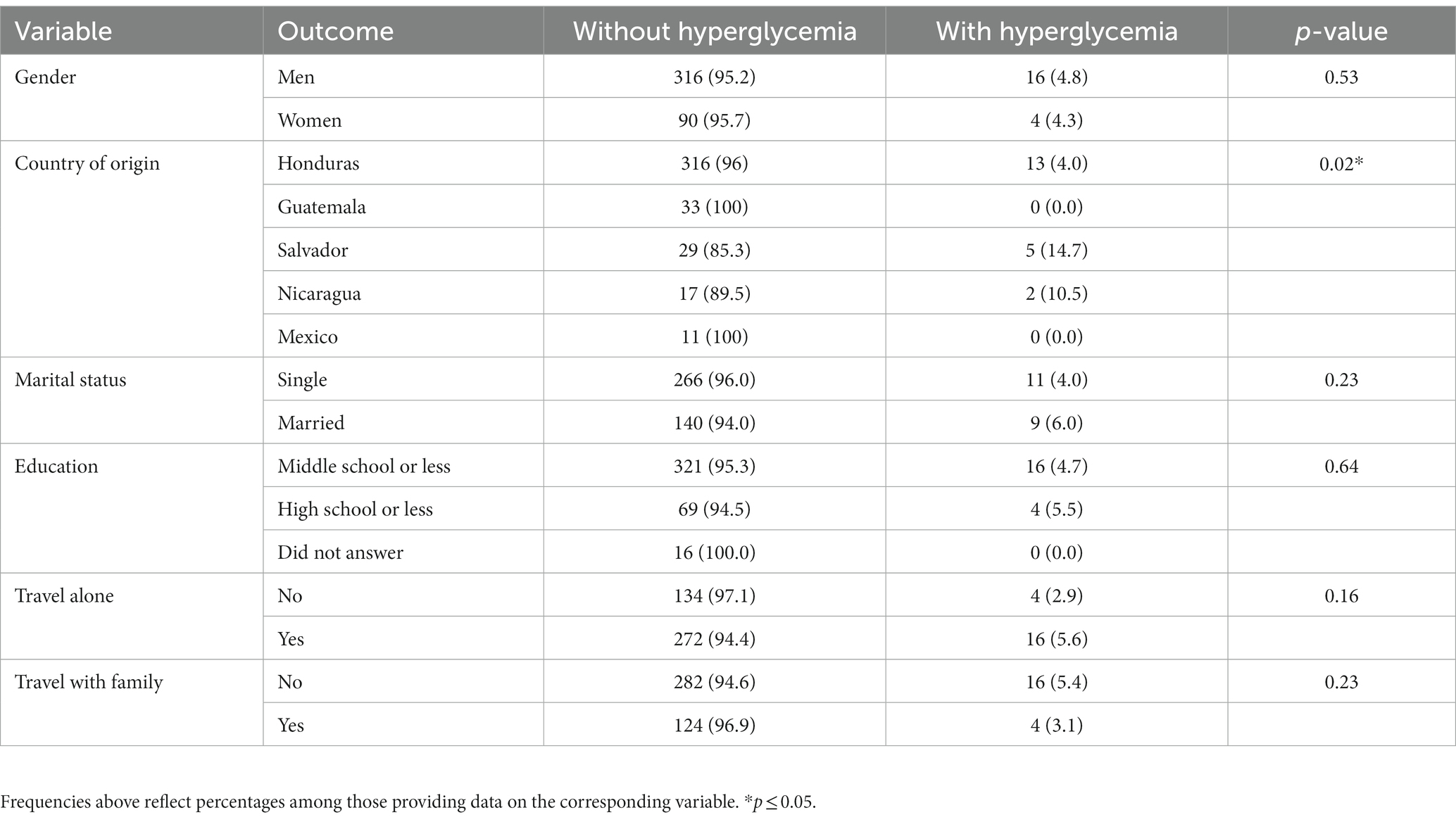
Table 5. Crossed table diabetes with sociodemographic characteristics.
3.4 Relationship of diabetes and different comorbidities in the study
The cross-tabulation of some comorbidities of the participants and the presence or absence of diabetes is shown in Table 6. Regarding the presence of hypertension, it is important to note that there was a higher proportion (23.1) of people with hypertension and diabetes, with a statistical significance of 0.005. Furthermore, it is clear that hypertension is the variable that gives a differentiated diagnosis of diabetes. As shown in Table 6, hypertension is the only statistically representative comorbidity in our population compared to smoking, alcohol consumption, and somatometric diagnosis relationship. Participants with a BMI indicating malnutrition, obesity, and overweight have a higher proportion of diabetes (in that order) compared to those with a normal BMI, but these differences were not statistically significant.
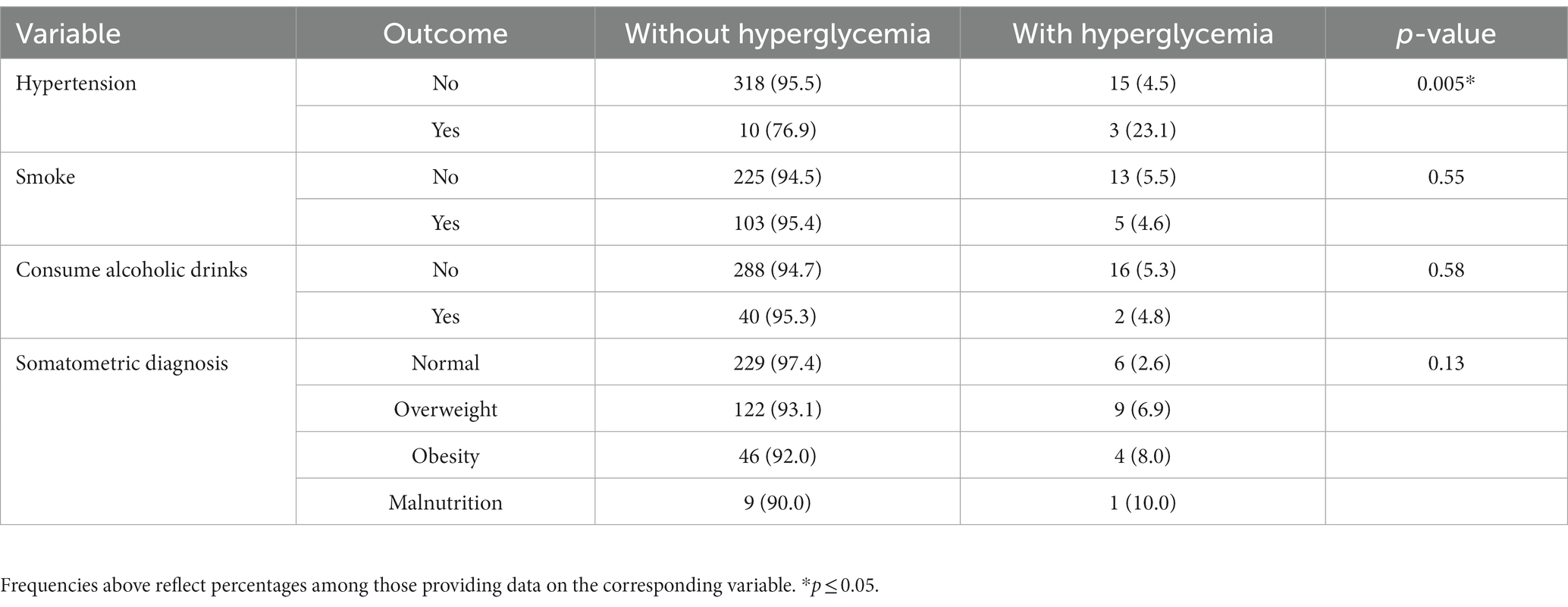
Table 6. Relationship of diabetes and different comorbidities.
3.5 Somatometric diagnosis with sociodemographic characteristics of the study
Table 7 shows that, in the group including participants with malnutrition, obesity, and overweight, women have a higher proportion of obesity (23.4%) and overweight (36.2%) than men (8.4 and 29.2%, respectively), with statistically significant differences. People from Mexico, Nicaragua, and Honduras were more overweight (63.6, 47.4, and 30.7%, respectively), and people from El Salvador and Nicaragua were more obese (23.5 and 21.1%, respectively). Married people were more overweight and obese than those who were single (34.2 and 20.1%, respectively). People who travel with family were more overweight and obese than those who travel alone (34.4 and 22.7%, respectively). Finally, Table 8 indicates that overweight, obesity, and hypertension were much more common in people who presented with diabetes during the fasting blood glucose test. Additionally, people who smoke or drink alcoholic beverages were more likely to be obese.
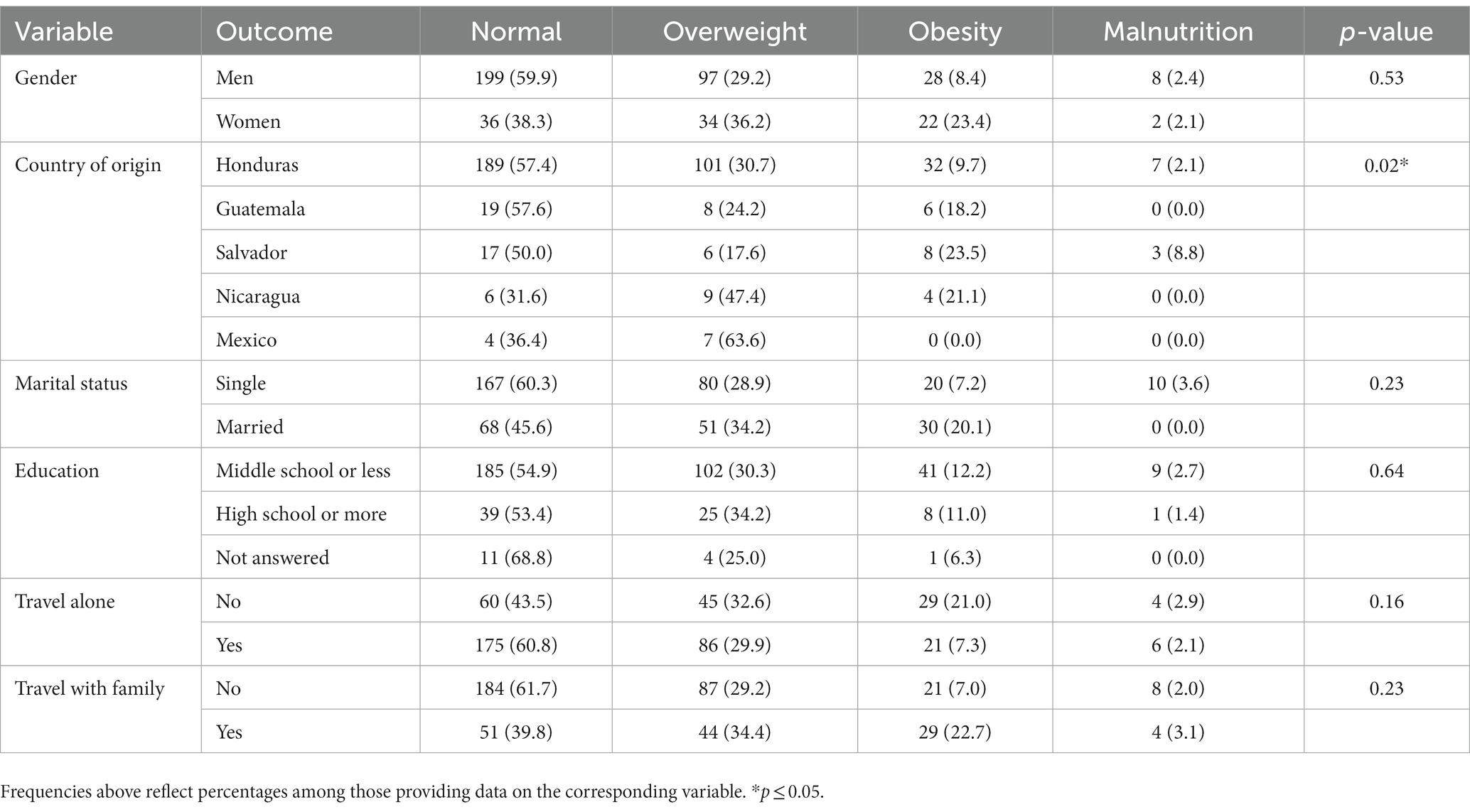
Table 7. Crossed-table somatometric diagnosis with sociodemographic characteristics.
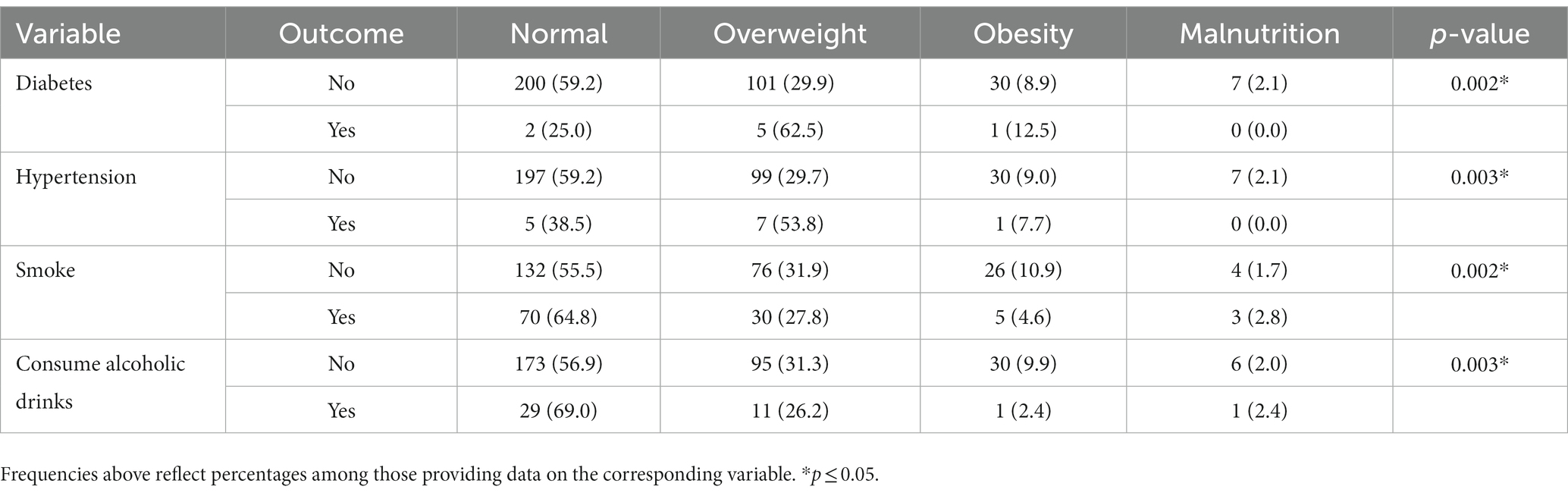
Table 8. Comorbidities with somatometric diagnosis.
4 Discussion
This study shows statistically significant differences in the prevalence of obesity, diabetes, and hypertension according to the country of origin for Mexican and Central American migrants from a migrant shelter in Guadalupe, Nuevo Leon. The estimated cost of diabetes mellitus in 2000 was $ 65 billion in Latin America and the Caribbean (17). This burden was attributed to lost productivity due to mortality and disability, as well as direct medical costs caused by the treatment of diabetes and its long-term complications (17). Diabetes, cardiovascular diseases, and obesity represented economic losses in the United States for more than 2.8 billion dollars annually, which represents 7% of the total health expenditure. In Mexico, health expenses for diabetes and its complications were more than $1.2 billion in 2023 (18). No studies examining the costs of diabetes or other chronic diseases have been published in Honduras. However, there is only one study from the Coordination of Chronic Noncommunicable Diseases of the Ministry of Health where the estimated cost of diabetes mellitus in 2015 was 1.29% from the gross domestic product (GDP), which was expected to increase to 2.59% in 2020 (19). Barcelo et al. (20) conducted a study to determine the direct costs (healthcare expenses such as insulin, oral hypoglycemic agents, tests, consultations, hospitalizations, emergency visits, and complications treatment) and indirect costs (lost resources due to premature mortality and temporary and permanent disabilities) related to diabetes in 29 countries from Latin America and the Caribbean in 2015 (20). The healthcare costs of diabetes in 2015 were annually estimated to be $1,039 billion in Honduras, $1,471 billion in Guatemala, $628 million in Nicaragua, $2,545 billion in Cuba, $814 million in Costa Rica, and $2,537 billion in Ecuador (20). The financial consequences of the increase of diabetes in countries considered as expellers represent one of the main challenges to health systems, indicating a need to implement public policies and programs to achieve greater effectiveness and efficiency in controlling, diagnosing, and treating diabetes in migrants from countries in transit and in receptor countries.
For this reason, the evidence of the prevalence of obesity, diabetes, and hypertension in the countries of origin in comparison with the country of transit present could explain the differences. However, according to data from previously reported publications, the prevalence of diabetes in the countries of origin does not align with the differences that this investigation found. For example, according to the STEP survey carried out in Guatemala in 2015 (21), it was reported that 5.7% of the population reported having DM in the age range of 18–44 years, contrary to what our results report, which has a prevalence of 0%. In Mexico, data from the 2018 national health survey reported a prevalence of 1.8% in the age group of 20–39 years (22), whereas data from our survey showed that migrants from Mexico reported a prevalence of 0%. These differences in the percentage of diabetes in the group of migrants from Guatemala and Mexico may be due to two factors. First, there was a small number of participants from both countries (34 participants from Guatemala and 19 from Mexico), the majority fit into a relatively young group (age between 18 and 44 years), and none were diabetic. Second, various investigations show that immigrants have a significantly lower daily intake of sugary drinks, processed red meats, and sodium. They also have a higher intake of vegetables, fruits, and whole grains compared to people born in the United States (23, 24). These findings support the idea that immigrants have more favorable health behaviors that are associated with a lower risk of chronic diseases (23, 24). Interestingly, the data from El Salvador obtained in our study indicated a prevalence of diabetes of 14.7% in people with an average age of 31 years. These data contrast with the results of the National Survey of Chronic Noncommunicable Diseases in the Adult Population of El Salvador, which reported a 3.2% prevalence of diabetes mellitus in the age group of 20–40 years (25). These findings in the migrant group from El Salvador could be attributed to genetic and behavioral differences, which make different ethnic subgroups more susceptible to diabetes rather than hypertension (26). Previous studies indicate that immigrants have differences in lifestyle and diet that may affect their risk of developing chronic diseases such as hypertension (27, 28). It is well known that more recent immigrants have lower blood pressure than those who live in the United States for longer periods of time (29, 30). Data from our study found that people traveling from Nicaragua with an average age of 39 years had a 10.5% prevalence of diabetes. These data contrast greatly with the results obtained in the Survey of Diabetes, Hypertension and Risk Factors for Chronic Diseases in Nicaragua, which indicated a prevalence of 2.0% in participants within the age range of 20–39 years (31). Additionally, a study conducted by the National Autonomous University of Nicaragua found that, in the north, center, and Pacific of Nicaragua, there was a 4.6% prevalence of diabetes mellitus in people between 30 and 39 years of age (32). Finally, from the data of 326 people from Honduras with an average age of 28 years, it was found that the prevalence of diabetes was 4.0%. This finding is very similar to the data reported by Bermúdez-Madriz et al. (33) in the review article about the health system in Honduras, reporting a 6.2% prevalence (group <19 years in urban areas) of DM (33).
In a recently published meta-analysis from (11), 52 studies with 436,654 immigrant Latinos in the United States reported a pooled prevalence for arterial hypertension of 28% (95% confidence intervals (CIs): 23–33%), type 2 diabetes mellitus of 17% (95% CIs: 14–20%), general obesity of 37% (95% CIs: 33–40%), and abdominal obesity of 54% (95% CIs: 48–59%) (11). The obtained results from our participants were as follows: The prevalence of arterial hypertension was 8.8%, type 2 diabetes mellitus was 4.6%, and general obesity was 10.7%. In previous studies, high rates of factors associated with obesity have been observed, with more than 45% of new immigrants in the United States being reported as overweight or obese. These factors vary according to the place of origin, the duration of residence in the United States and regions of current residence, and sociodemographic characteristics (15). Among the six immigrant groups studied, the group considered from Latin America and the Caribbean had higher prevalence rates of overweight and obesity than the Asian/Pacific/Oceanic and Sub-Saharan African groups. The prevalence of combined overweight and obesity was higher in men (54%) than in women (38%). Men had a higher prevalence of overweight and women had a slightly higher prevalence of obesity among immigrants from Latin America and the Caribbean, which indicates notable heterogeneity in the prevalence of overweight and obesity within and between hometown groups by age, poverty level, years of residence in the United States, and regions of current residence (15).
Regarding the previously diagnosed comorbidities, it was found that, among the people interviewed, 3.2% reported having a previous diagnosis of diabetes. Undiagnosed diabetes is an indicator of a lack of diabetes awareness. A literature review conducted by (34) reported that the prevalence of undiagnosed diabetes was higher in Honduras (range 29.9–50%), Nicaragua (43.3%), and Costa Rica (10.3–28.4%). These reported values are much higher than those determined in our study (34). This discrepancy may be because the majority of Honduran migrants have good diabetes awareness. Irazola et al. (35) described that awareness increased slightly with educational level. However, most studies do not report associations between undiagnosed diabetes and age, sex, educational level, socioeconomic status, or geographic location (34, 35). In our study, we found that migrants who had a higher prevalence of diabetes had a higher educational level; however, none of those correlations were statistically significant. In our population, 8.2% of people were detected with hypertension and 4% with diabetes. An interesting finding was that 23.1% of patients with diabetes were hypertensive, while only 4.5% of people without diabetes were hypertensive. This comorbidity has already been reported in previous studies such as the one from Petrie et al. (36), where 85% of people with diabetes also had hypertension. A review published in 2014 (37) showed that more than 50% of patients with diabetes also have hypertension. Thus, the results found in our study are consistent with what was previously reported in the literature, though the proportion is much lower. This can be explained by the sample consisting of a young population that involves a few years of evolution with diabetes and perhaps hypertension could be developed as a common comorbidity in patients with diabetes. It should be noted that Central American immigrants are a heterogeneous racial and ethnic group representing multiple countries of origin with different levels of education, socioeconomics, and cultural traditions, and these variables vary across different regions of Central America. These factors influence the prevalence of obesity, diabetes, and hypertension that has not been studied in previous research on Central American immigrants traveling through northeastern Mexico to the United States.
4.1 Study limitations
The first limitation of the study is that our data were gathered from a cross-sectional study of immigrants, and, therefore, the associations found are not proof of causality. Second, there is a high heterogeneity for all the results since the immigrant populations differ in many aspects, such as the country of origin (migrants from eight countries were reported), migratory status, educational levels, socioeconomic aspects, and whether they traveled accompanied or alone. These differences could explain the various inconsistencies found between the different populations of migrants. Third, we cannot definitively state whether our results are primarily due to a selection of Central American migrants bound for the United States or a selection of Central American migrants returning to Mexico. Fourth, analyses of the study’s descriptive statistics results may not be representative of all immigrants from these ethnic groups, and there may be selection bias as a result of recruitment through migrant shelter. Fifth, participation in this study was largely limited to migrants from Honduras, at 72.6% of the study population. Sixth, the measurements for blood glucose and blood pressure were only taken once in each participant, which is a limitation for monitoring their diabetes and hypertension.
4.2 Study strengths
Like many other studies regarding the health of immigrants, our study contains important advantages. First, the representative sample size of Central American immigrants over a 26-month period (January 2019 to March 2021) used the same sampling and data collection methodologies among its participants. Another strength of this study was its participatory approach based on the migrant community, which was guided by a multidisciplinary steering committee, comprised of academic researchers, physicians, and representatives of the migrant community, and this facilitated the appropriate study protocol and interpretations of the findings. The third strength was the use of health indicators to determine obesity, diabetes, and hypertension in the Central American migrant population. These indicators allowed us to rule out the possibility that the differences in health examinations between individuals from different Central American countries can be homogenized to have identical values in the abovementioned different countries. Fourth, our research design used data from a United States-Mexico border state, which allowed us to rule out the possibility of replicating this study in Mexican border cities with a high confluence of Central American migration.
4.3 Future research
First, more large-scale, multicenter studies are needed in different United States–Mexico border cities that use the same metrics to assess obesity, diabetes, and hypertension as well as facilitate the development of new interventions targeted at Central American immigrants. Second, it would be important to implement diabetes education among the Central American immigrant populations on the northern border of Mexico. Third, and most importantly, gender- and age-specific interventions must be targeted at specific immigrant groups, who are at a higher risk of developing diabetes earlier in the life course. Fourth, future research should investigate many other important socioeconomic and sociocultural factors that affect the prevalence and management of obesity, diabetes, and hypertension.
5 Conclusion
This study determined that diabetes does not have a homogeneous distribution in migrant populations. A notable heterogeneity was found in the prevalence of obesity, diabetes, and hypertension among the groups of Central American migrants and their place of origin, age, educational level, and gender. It should be noted that the participation in this study is largely limited to migrants from Honduras, with 72.6% of the study population. Nevertheless, with this population, it could be determined that diabetes is more common in Salvador and Nicaragua and less frequent in Honduras, Guatemala, and Mexico. The presence of increased diabetes in Salvador and Nicaragua cannot be explained by differences in the prevalence of diabetes in the countries of origin. There are no factors associated with the presence of diabetes in the population of Central American and Mexican migrants since neither age, gender, marital status, nor education were associated with a higher prevalence of diabetes. Finally, the presence of arterial hypertension as a comorbidity occurred in a lower proportion than previously reported. Obesity is most common in migrant women than men. Nicaragua and Mexico have a higher proportion of overweight participants, whereas El Salvador and Mexico have a higher proportion of obesity participants. According to the reviewed literature, this is the first study that evaluates the association between obesity, diabetes, and hypertension in a representative sample of the Central American immigrant population traveling through northeastern Mexico to the United States.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving humans were approved by the Ethics and Research Committee of the University of Monterrey, with the number 042016-CIE. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin. Written informed consent was obtained from the individual(s), and minor(s)’ legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
Author contributions
GG-M, BR-T, and WH-J were involved in the study design, analysis, and data collection. EM-C, JV-V, HA-R, and FG-S wrote the original manuscript, prepared the analysis, and interpreted the data. BR-T, HA-R, and FG-S helped with the analysis and gave essential comments on multiple versions. All authors approved the final version of the manuscript.
Funding
The authors received the support of the University of Monterrey to make the payment of the article processing charge of this article.
Acknowledgments
The authors thank the staff of the migrant shelter Casanicolás and the University of Monterrey for making the payment of open access rights of the article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mahmoud, AM. An overview of epigenetics in obesity: the role of lifestyle and therapeutic interventions. Int J Mol Sci. (2022) 23:1341. doi: 10.3390/ijms23031341
2. Flórez, KR, Dubowitz, T, Saito, N, Borges, G, and Breslau, J. Mexico–United States migration and the prevalence of obesity: a transnational perspective. Arch Intern Med. (2012) 172:1760. doi: 10.1001/2013.jamainternmed.77
3. Pérez, W, Melgar, P, Garcés, A, De Marquez, AD, Merino, G, and Siu, C. Overweight and obesity of school-age children in El Salvador according to two international systems: a population-based multilevel and spatial analysis. BMC Public Health. (2020) 20:687. doi: 10.1186/s12889-020-08747-w
4. Laux, TS, Bert, PJ, González, M, Unruh, M, Aragon, A, and Lacourt, CT. Prevalence of obesity, tobacco use, and alcohol consumption by socioeconomic status among six communities in Nicaragua. (2012). 32:217–225.
5. Gregory, CO, Ramirez-Zea, M, Martorell, R, and Stein, AD. Activities contributing to energy expenditure among Guatemalan adults. Int. J. Behav. Nutr. Phys. Activ. Activ. (2007). doi: 10.1186/1479
6. Jiwani, SS, Carrillo-Larco, RM, Hernández-Vásquez, A, Barrientos-Gutiérrez, T, Basto-Abreu, A, Gutierrez, L, et al. The shift of obesity burden by socioeconomic status between 1998 and 2017 in Latin America and the Caribbean: a cross-sectional series study. Lancet Glob Health. (2019) 7:e1644–54. doi: 10.1016/S2214-109X(19)30421-8
7. Grundy, SM. Obesity, metabolic syndrome, and cardiovascular disease. J Clin Endocrinol Metab. (2004) 89:2595–00. doi: 10.1210/jc.2004-0372
8. Schmidt, C, Reitzle, L, Paprott, R, Bätzing, J, and Holstiege, J. Diabetes mellitus and comorbidities - a cross-sectional study with control group based on nationwide ambulatory claims data. J. Health Monitor. (2021) 6:19–35. doi: 10.25646/8327
9. Barquera, S, Campos-Nonato, I, Aguilar-Salinas, C, Lopez-Ridaura, R, Arredondo, A, and Rivera-Dommarco, J. Diabetes in Mexico: cost and management of diabetes and its complications and challenges for health policy. Glob Health. (2013) 9:1–9. doi: 10.1186/1744-8603-9-3
10. US Census Bureau. USA Census Bureau: Explore Data. Available at: https://data.census.gov/mdat/#/ (2023).
11. Paixão, TM, Teixeira, LR, de Andrade, CAF, Sepulvida, D, Martinez-Silveira, M, Nunes, C, et al. Systematic review and Meta-analysis of metabolic syndrome and its components in Latino immigrants to the USA. Int J Environ Res Public Health. (2023) 20:1307. doi: 10.3390/ijerph20021307
12. Medina-Macías, O, Stoesslé, P, Perales-Rendón, LE, Moreno-Cuevas, JE, and González-Salazar, F. Latent tuberculosis in migrants travelling through the northeast regions of Mexico. J Clin Tuberc Other Mycobact Dis. (2020) 21:100194. doi: 10.1016/j.jctube.2020.100194
13. Wurtz, HM. A movement in motion: collective mobility and embodied practice in the central American migrant caravan. Mobilities. (2020) 15:930–44. doi: 10.1080/17450101.2020.1806511
14. Cokkinides, VE, Bandi, P, Siegel, RL, and Jemal, A. Cancer-related risk factors and preventive measures in US Hispanics/Latinos. CA Cancer J Clin. (2012) 62:353–63. doi: 10.3322/caac.21155
15. Choi, JY. Prevalence of overweight and obesity among US immigrants: results of the 2003 new immigrant survey. J Immigr Minor Health. (2012) 14:1112–8. doi: 10.1007/s10903-011-9560-8
16. World Health Organization. A healthy lifestyle - WHO recommendations. A healthy lifestyle - WHO recommendations (2010). Available at: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations (accessed October 23, 2023).
17. Barceló, A, Aedo, C, Rajpathak, S, and Robles, S. The cost of diabetes in Latin America and the Caribbean. (2003). Available at: www.who.int/bulletin/
18. Gonzalez, D, Aracena, B, Montañez, J, Serván, E, and Rivera, G. Cuentas en diabetes mellitus, enfermedades cardiovasculares y obesidad. 2006th ed (2006).
19. Duarte, RM. El Impacto Económico De La Diabetes Mellitus Como Problema De Salud Pública En Honduras. Rev Med Hondur. (2017):85.
20. Barcelo, A, Arredondo, A, Gordillo-Tobar, A, Segovia, J, and Qiang, A. The cost of diabetes in Latin America and the Caribbean in 2015: evidence for decision and policy makers. J Glob Health. (2017) 7:020410. doi: 10.7189/jogh.07.020410
21. Brathwaiteo, O. National Survey on the Prevalence of Noncommunicable diseases and their risk factor in the population of 18 years of age or older. Domain I: Urban Metropolitan Department of Guatemala. December 2015. Available at: https://epidemiologia.mspas.gob.gt/index.php (2022).
22. Shamah-Levy, T. National Health and nutrition survey 2018–19: National Results. Cuernavaca, Mexico: National Institute of Public Health (2020).
23. Brown, AGM, Houser, RF, Mattei, J, Mozaffarian, D, Lichtenstein, AH, and Folta, SC. Hypertension among US-born and foreign-born non-Hispanic blacks: National Health and nutrition examination survey 2003-2014 data. J Hypertens. (2017) 35:2380–7. doi: 10.1097/HJH.0000000000001489
24. Dawson, AZ, Walker, RJ, Gregory, C, and Egede, LE. Relationship between social determinants of health and systolic blood pressure in United States immigrants. Int J Cardiol Hypertens. (2019) 2:100011. doi: 10.1016/j.ijchy.2019.100011
25. Ministry of Health of El Salvador. Prevalence of chronic kidney disease, arterial hypertension, diabetes mellitus and risk factors in the adult population of El Salvador. National Survey of chronic noncommunicable diseases in the adult population of El Salvador. (2015)
26. Rodriguez, F, Hicks, LS, and Lápez, L. Association of acculturation and country of origin with self-reported hypertension and diabetes in a heterogeneous Hispanic population. BMC Public Health. (2012) 12:1–8. doi: 10.1186/1471-2458-12-768
27. Lesser, IA, Gasevic, D, and Lear, SA. The association between acculturation and dietary patterns of south Asian immigrants. PLoS One. (2014) 9:e88495. doi: 10.1371/journal.pone.0088495
28. Holmboe-Ottesen, G, and Wandel, M. Changes in dietary habits after migration and consequences for health: a focus on south Asians in Europe. Food Nutr Res. (2012) 56:18891. doi: 10.3402/fnr.v56i0.18891
29. Koya, DL, and Egede, LE. Association between length of residence and cardiovascular disease risk factors among an ethnically diverse group of United States immigrants. J Gen Intern Med. (2007) 22:841–6. doi: 10.1007/s11606-007-0163-y
30. Rosenthal, T, Grossman, E, Knecht, A, and Uri, G. Blood pressure in Ethiopian immigrants in Israel: comparison with resident Israelis. J Hypertens. (1989) 7:S53–5. doi: 10.1097/00004872-198902001-00016
31. Iniciativa Centromericana de diabetes (CAMDI). Encuesta de diabetes, hipertensión y factores de riesgo de enfermedades crónicas. Managua, Nicaragua: Iniciativa Centromericana de diabetes (CAMDI) (2010).
32. Aráuz, I, Delgado, Y, and Delgado, E. Prevalencia de Diabetes Mellitus y factores de riesgo en mayores de 20 años de las cabeceras departamentales de Nicaragua. Revista Cientíca de la UNAN-León (2014). Available at: http://ageconsearch.umn.edu
33. Luis Bermúdez-Madriz, J, del Rocío Sáenz, M, Muiser, J, and Acosta, M, Sistema de salud de Honduras
34. Avilés-Santa, ML, Monroig-Rivera, A, Soto-Soto, A, and Lindberg, NM. Current state of diabetes mellitus prevalence, awareness, treatment, and control in Latin America: challenges and innovative solutions to improve health outcomes across the continent. Curr Diab Rep. (2020) 20:62. doi: 10.1007/s11892-020-01341-9
35. Irazola, V, Rubinstein, A, Bazzano, L, Calandrelli, M, Chung-Shiuan, C, Elorriaga, N, et al. Prevalence, awareness, treatment and control of diabetes and impaired fasting glucose in the southern cone of Latin America. PLoS One. (2017) 12:e0183953. doi: 10.1371/journal.pone.0183953
36. Petrie, JR, Guzik, TJ, and Touyz, RM. Diabetes, hypertension, and cardiovascular disease: clinical insights and vascular mechanisms. Can J Cardiol. (2018) 34:575–84. doi: 10.1016/j.cjca.2017.12.005
Keywords: Central American immigrant, obesity, diabetes, hypertension, Central American immigrants in Mexico
Citation: Gómez-Morales GB, Rosas-Torres BS, Hernández-Jiménez WJ, Mattenberger-Cantú E, Vargas-Villarreal J, Almanza-Reyes H and González-Salazar F (2024) Prevalence of obesity, diabetes and hypertension in immigrant populations in northeastern Mexico. Front. Public Health. 11:1220753. doi: 10.3389/fpubh.2023.1220753
Edited by:
Åke Sjöholm, Gävle Hospital, SwedenReviewed by:
Akshyaya Pradhan, King George Medical University, IndiaPalmira Immordino, University of Palermo, Italy
Copyright © 2024 Gómez-Morales, Rosas-Torres, Hernández-Jiménez, Mattenberger-Cantú, Vargas-Villarreal, Almanza-Reyes and González-Salazar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Horacio Almanza-Reyes, YWxtYW56YXJleWVzQGhvdG1haWwuY29t; Francisco González-Salazar, ZnJhbmNpc2NvLmdvbnphbGV6QHVkZW0uZWR1