 M. Murat Oktay1,2
M. Murat Oktay1,2 Mustafa Boğan
Mustafa Boğan Hasan Bayram
Hasan Bayram- 1Emergency Department, School of Medicine, Gaziantep Islam Science and Technology University, Gaziantep, Türkiye
- 2Department of Emergency Medicine, School of Medicine, Gaziantep University, Gaziantep, Türkiye
- 3Emergency Department, School of Medicine, Istanbul Medeniyet University, Istanbul, Türkiye
- 4Emergency Department, School of Medicine, Düzce University, Düzce, Türkiye
- 5Biostatistics Department, School of Medicine, Gaziantep University, Gaziantep, Türkiye
- 6Emergency Department, Şehitkamil State Hospital, Gaziantep, Türkiye
- 7Department of Pulmonary Medicine, School of Medicine, Koç University, Istanbul, Türkiye
- 8Department of Pulmonary Medicine, School of Medicine, Gaziantep University, Gaziantep, Türkiye
Objective: It is known that the inhalation of air pollutants adversely affects human health. These air pollutants originated from natural sources such as desert storms or human activities including traffic, power generating, domestic heating, etc. This study aimed to investigate the impacts of desert dust storms, particulate matter ≤10 μm (PM10) and daily maximum temperature (MT) on mortality and emergency department (ED) visits due to stroke in the city of Gaziantep, Southeast Turkey.
Method: The data on mortality and ED visits due to stroke were retrospectively recruited from January 1, 2009, to March 31, 2014, in Gaziantep City Centre.
Results: PM10 levels did not affect ED visits or mortality due to stroke; however, MT increased both ED visits [adjusted odds ratio (OR) = 1.002, 95% confidence interval (CI) = 1.001–1.003] and mortality (OR = 1.006, 95% CI = 0.997–1.014) due to stroke in women. The presence of desert storms increased ED visits due to stroke in the total population (OR = 1.219, 95% CI = 1.199–1.240), and all subgroups. It was observed that desert dust storms did not have an increasing effect on mortality.
Conclusion: Our findings suggest that MT and desert dust storms can induce morbidity and mortality due to stroke.
Introduction
Stroke is a neurological condition that is seen because of the disruption in cerebral perfusion due to thromboembolic events, the majority of which are associated with ischemia. It causes significant mortality and morbidity. The most important cause of secondary injuries at the cellular level in stroke patients is the depletion of oxygen and glucose due to interrupted blood flow (1–3).
It is known that the inhalation of pollutants dispersed in the atmosphere adversely affects human health (4–10). High level of car traffic, increased combustion of fossil fuels for industrial activities, transport, and domestic heating lead to elevated levels of air pollutants including particulate matter (PM) levels in the atmosphere (4). Air pollution causes human health problems such as respiratory, cardiovascular, cerebrovascular, and obstetric diseases (4, 5, 7–11). Basic biological mechanisms that explain the effects of air pollutants on vascular structures are still controversial (3). The severity of the effects of this condition on human health varies depending on the type of pollutant, its concentration in the atmosphere, and the duration of its stay in the atmosphere.
Climate change is a global health concern, and the Intergovernmental Panel on Climate Change (IPCC) reported globally averaged greenhouse gas concentrations, along with land and ocean surface temperatures, have strikingly increased across the past decades (12). These increased temperatures have led to global warming resulting in increased risk for extreme meteorological and environmental events including extreme temperatures and desert dust storms (8, 12, 13). Epidemiological studies suggest an association between increased temperatures, and desert dust storms and morbidity and mortality (6, 10, 12, 14). People with pre-existing chronic diseases are at greater risk for increased adverse health outcomes (8), with vulnerable populations and people in low-middle income countries at a high level of susceptibility (10, 15).
Gaziantep is located in Southeast Turkey, close to the Syrian border. It is one of the most heavily polluted cities in Turkey (16), with the city under increased risk of desert dust storms, as is also experienced in other Southeastern Anatolian provinces in Turkey (17). The annual mean concentration of inhalable PM with a diameter ≤ 10 μm (PM10) in all Turkish city centres in 2000 was 49 μg/m3, and even higher in Gaziantep (55 μg/m3) (16). The PM with a diameter ≤ 2.5 μm (PM2.5) annual exposure for Gaziantep is reported as 66 μg/m3, which is 6.6 × 10 μg/m3 WHO guideline (18). The city of Gaziantep is at risk of desert dust storms like the other South-eastern Anatolian provinces in Turkey (17). Gaziantep and these provinces in the Southeast Turkey are under the effects of dust storms originating from deserts located in the Middle East’s Syrian Desert and Africa’s Saharan Desert (13, 17, 19). Studies reported that the frequency of desert dust storms has increased in the Middle East (20).
Recently, we have investigated effects of desert dust storms, PM10 and maximum temperature on morbidity and mortality due to cardiovascular and pulmonary diseases, and we found that desert dust storms, PM10 levels and maximum temperature were associated with increased mortality and ER visits due to acute coronary syndrome, asthma, COPD, lower respiratory tract infections and pulmonary emboli (5, 8). The current study aimed to investigate the impact of desert dust storms, PM10 levels and maximum temperature on mortality and emergency department (ED) visits due to stroke in the city of Gaziantep, Southeast Turkey.
Methods
The study was conducted retrospectively in Gaziantep after obtaining the approval of the ethics committee (23.06.2014/228). The study was carried out in accordance with the Declaration of Helsinki.
Health data
Health data were collected from three hospitals in Gaziantep city. The city-affiliated mortality rates were collected from the Ministry of Health. Data collected in 1916 days, from January 1, 2009, to March 31, 2014, were evaluated in this study. Collected data were analysed within the total population and in four separate subgroups. Subgroups were based on gender and age groups of individuals above and below 65 (≥65 & <65) years of age. Patients over 16 years of age admitted to the ED with a diagnosis and cause of death associated directly with a stroke were included in the study. Patients who could be diagnosed with stroke by clinical examination and radiological imaging modalities (magnetic resonance imaging, MRI or computed tomography, CT) were included in the study. Haemorrhagic strokes were excluded.
Climate and particulate matter pollution data
The highest, the lowest, and average temperature values, as well as humidity, air pressure, and wind velocity data for the relevant dates (01, 2009 to March 31, 2014), were obtained from the General Directorate of Meteorology. Information daily on PM10 values in Gaziantep was obtained from the Air Quality Laboratory of the Ministry of Environment and Urbanization. Information regarding daily desert dust storms within the dates of the study period was obtained from the website owned and operated by the NASA.1 Daily aerosol optical depth (AOD) over land and ocean mean values were obtained for the coordinates of Gaziantep City. AOD values indicate how much direct sunlight is prevented from reaching the ground by these aerosol particles. An increased AOD value indicates more dust and haze in the atmosphere (21, 22). As reported by the National Oceanic and Atmospheric Administration, an AOD of 0.01 corresponds to an extremely clean atmosphere, and a value of 0.4 corresponds to a very hazy condition. In the present study, we used an AOD value >0.5 as an indicator of a desert dust storm day (5, 7, 8). Additionally, the presence of desert dust storm days was also confirmed by the records of Gaziantep Airport, Gaziantep, Turkey.
Statistical analysis
Normal distribution of the data was tested using the Shapiro–Wilk test. The Student’s T-Test and Mann–Whitney U Test were used in the comparison of two independent groups of variables with normal or without normal distribution, respectively. Generalized Adaptive Additive Poisson Regression models (23, 24) were utilized to analyse the impact of the daily effect of PM10 levels, and the lag effect in the subsequent 3 days (lag0 = day zero; lag1 = day one; lag2 = day two, lag3 = day three of high PM10 levels, respectively), daily maximum temperature (MT0 = day zero (0) of maximum temperature levels), and presence of dust storm (DS0 = day zero (0) of dust storms) on ED visits and mortality due to stroke. Log link family was used for the smoothing function and penalized smoothing splines were used to adjust for seasonal patterns and long-term trends in disease morbidity adding time as a smoothing variable. All univariate statistical analyses were performed by SPSS for Windows (version 24.0) and generalized additive Poisson regression models were applied by mgcv package in R (version 3.4.1) for generalized additive modelling (GAM). The GAM command in mgcv was applied to solve the smoothing parameter estimation problem by using the generalized cross-validation (GCV) criterion. The best degree of freedom was automatically selected by GCV based on the Un-Biased Risk Estimator (UBRE) criterion. Adjusted odds ratios (ORs) and 95% confidence interval (CI) estimates were calculated to show the direction of the effects.
Results
It was found that 89 dust storms occurred during the time of the study. Mean, minimum, and maximum temperature values were significantly higher (p = 0.001) on dusty days in comparison to dust-free days, and this comparison is provided in Table 1. Contrarily, mean air pressure (mbar) values were higher on dust-free days as compared to dusty days (p = 0.001). There was no significant difference between PM10 levels and relative humidity in dusty days, as compared to dust free days. PM10 levels (Figure 1A) and maximum temperatures (Figure 1B) for Gaziantep are provided in Figure 1.

Table 1. Descriptive statistics for pollutants and meteorological variables.
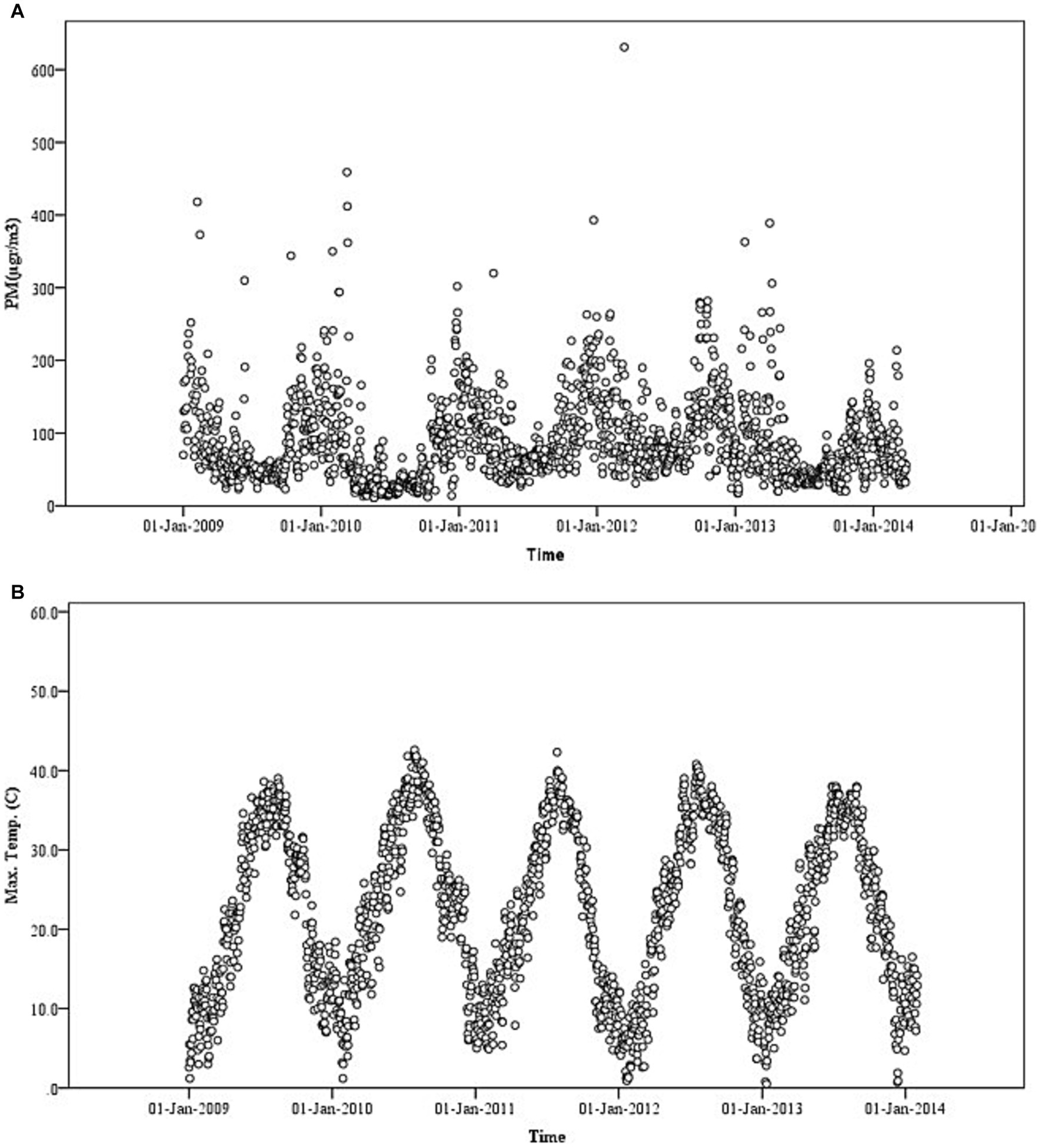
Figure 1. Daily mean of (A) particulate matter ≤10 μm (PM10) levels and (B) mean temperature (°C) in Gaziantep City Centre from September 01, 2009 to January 31, 2014 (5).
Approximately 10,000,000 ED visits were reviewed, and stroke was detected in 65,429 patients (6.54%). Of these patients, females and males were 36,056 (55.10%) and 29,373 (44.9%), respectively. The mean age of the ED visited patients was 61.36 years (females = 61.33 years and males = 61.39 years). Of the patients included in the study, 33,205 (51.79%) were below 65 years. Of stroke patients, 64,113 (98%) were discharged, and 1,316 (2%) patients died after ED visit (females = 729, 55.39% and males = 587, 44.61%). The mean age of the patients, who died was 73.45 years (females = 75.24 years and males = 71.66 years). Among patients died, 257 (19.52%) were below 65 years.
PM10 levels and residual effects (lag0-3) did not have an effect on the mortality due to stroke. However, we observed that maximum temperature increased mortality (OR = 1.007, 95% CI = 1.001–1.013), while leading to a slight decrease in the number of ED visits in the total population (OR = 0.999, 95% CI = 0.998–1.000). Maximum temperature was associated with increased mortality due to stroke in total population (OR = 1.007, 95% CI = 1.001–1.013). Similarly, there was an association between maximum temperature and both mortality (OR = 1.006, 95% CI = 0.997–1.014) and ED visits (OR = 1.002, 95% CI = 1.001–1.003) due to stroke in women. Although desert dust storms did not increase mortality, they were associated with an increase in ED visits due to stroke in the total population (OR = 1.219, 95% CI = 1.199–1.240) and subgroups of women (OR = 1.158, 95% CI = 1.131–1.186) and men (OR = 1.296, 95% CI = 1.264–1.328). The results presenting the association between PM10, maximum temperature and desert dust storms and ED visits and mortality due to stroke are shown in Table 2 and Figure 2.
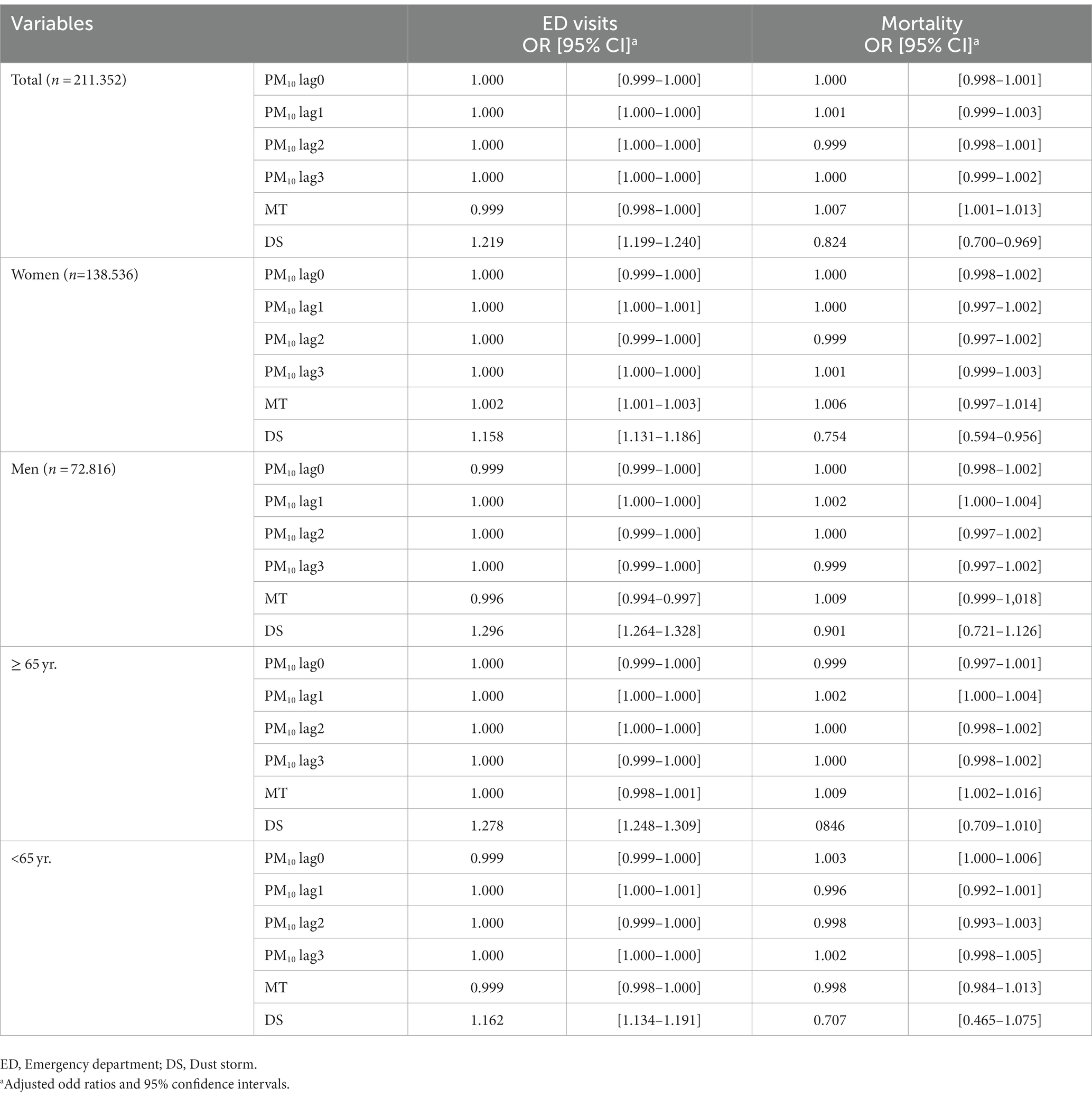
Table 2. Results of generalized additive Poisson models for predicting number of emergency department visits and mortality due to stroke.
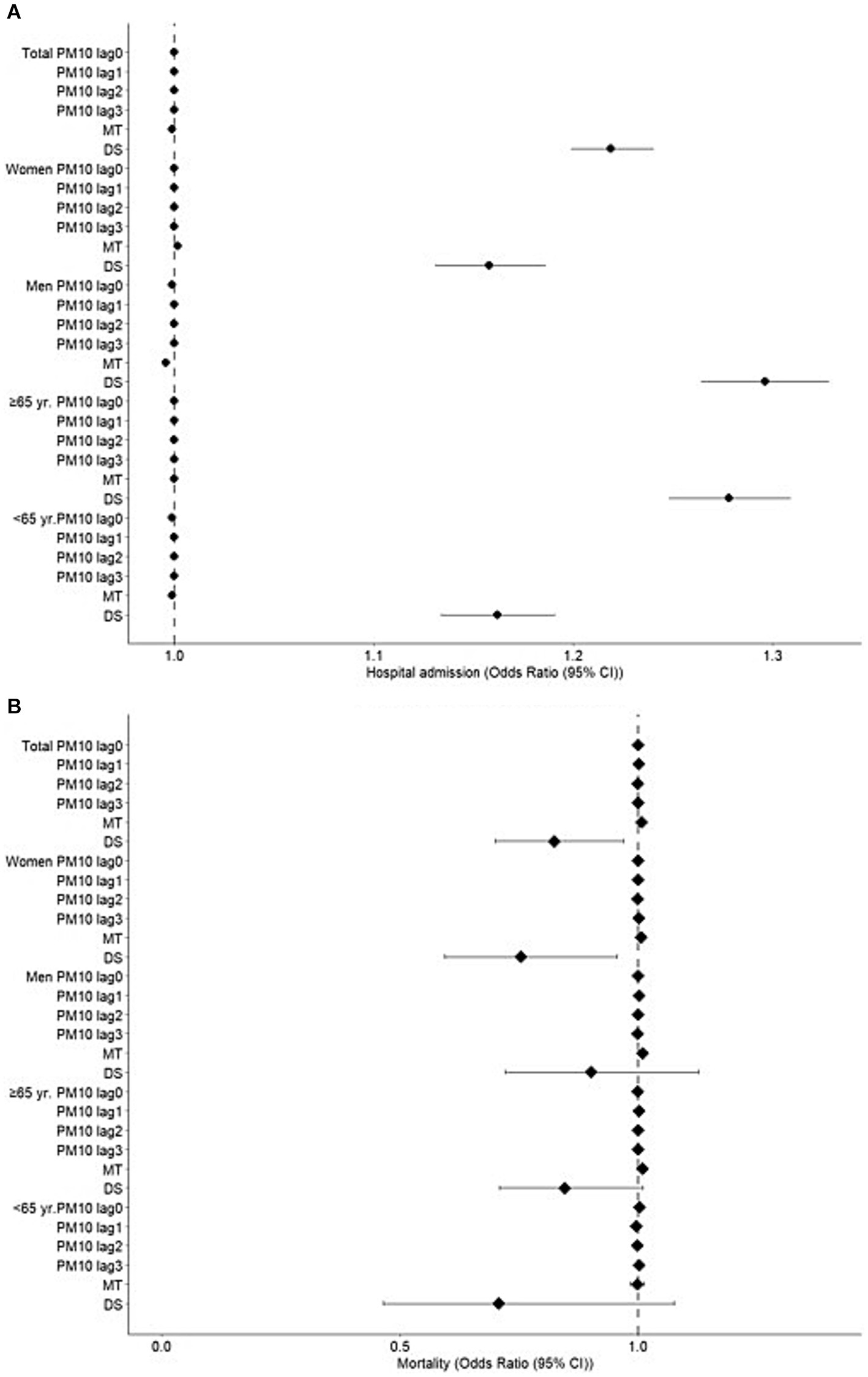
Figure 2. Effects of particulate matter ≤10 μM (PM10, at a lag time of 0–3 days), maximum temperatures (MT) and desert dust storms (DS) on stroke. Results of generalized additive Poisson models for predicting number of emergency department (ED) visits and deaths due to stroke.
Discussion
In the present study, we investigated the effects of PM10 pollution, desert dust storms, and daily temperatures on mortality and morbidity due to stroke, in Southeast Turkey. Although PM10 levels did not associate with ED visits or mortality due to stroke, desert dust storms were positively associated with ED visits. Similarly, maximum temperature had a positive association with stroke mortality in the study population, and ED visits in women. Furthermore, maximum temperature was associated with increased mortality in only patients ≥65 years old. These findings suggest that desert dust storms and higher daily temperatures can increase the risk for mortality and ED visits due to stroke.
Nearly 3 million people die each year due to ischemic heart disease or ischemic stroke associated with air pollution rather than conventional risk factors such as obesity, diabetes, and smoking, wherein air pollution also increases the symptoms of sensitive individuals who have a chronic disease (5, 25). The relationship between desert dust storms, which is a natural source of air pollution, and stroke-related ED visits and stroke-related mortality has been demonstrated in various studies (26–28). The fact that dust storms, which were shown to increase the prevalence of ischemic stroke, not only contain PM originating from soil and other earth sources but also contain microorganisms such as bacteria and fungi, acidic gases, plant pollen, and various minerals suggesting that such health effects should not only be associated with the core PM levels (29–32).
Studies investigating the impact of desert dust storms on cerebral mortality and morbidity have reported positive associations. In a study investigating the association between dust storms and county-level non-accidental mortality in the United States from 1993 to 2005, Crook et al., found that total non-accidental mortality increased by 7.4% in the whole country (26). Mallone et al., reported a significant relationship between dust storms and cerebrovascular mortality in Italy (27). In their study on Asian desert dust storms, Yorifuji and Kashima investigated the Asian dust and suspended particulate matter and mortality due to stroke, and they found a positive relationship between dust storms and ischemic and haemorrhagic stroke in 47 cities in Japan (28). According to this study, a 10 μg/m3 increase of dust particles were positively associated with mortality due to intracerebral haemorrhage and ischemic stroke. However, our findings did not show a positive association between dust storms and stroke mortality. In contrast, there was an inverse relation between dust storms and mortality. Although we do not have a clear explanation for this discrepancy, we still think that this may be related to the recording of the last cause of death in the data obtained from the cemetery’s institution.
Studies also suggest an association between desert dust and morbidity due to stroke. In their research studying the association between Asian dust storms and ischemic stroke, Kamouchi et al., did not find a significant association with the incidence of ischemic stroke; however, Asian dust was significantly associated with the incidence of atherothrombotic brain infarction (33). Similarly, Yang et al., reported an increase in the number of visits due to stroke during dust storm days, whereas there was no significant relationship in the subsequent 3 days following the storm (34). However, they found that the risk of haemorrhagic stroke was higher than that of ischemic stroke (34). In a study of more than 800,000 were hospitalized because of stroke, Kang et al., found an increase in the number of stroke cases on the 1st and 2nd days following the Asian dust storms (35). In a recent study from Iran, dust storms were related with an increase in the risk of stroke (36). In agreement with these studies, we demonstrated an association between desert dust storms and increases in the number of ED visits due to ischemic stroke.
The majority of studies on PM levels and cerebral diseases suggested a positive relations (37–45); however, some failed to show such a relationship (46). In a study conducted on 7,594 patients, it was found that a 10 μg/m3 increase in PM10 levels was associated with increased cerebrovascular mortality (42). Similarly, Yan et al., showed that short-term exposure to PM10 led to an increase in stroke-related mortality, which peaked at lag1 (47). In a meta-analysis by Scheers et al., the authors found a significant association between exposure to PM10 and PM2.5 and increased hazard ratio for overall stroke events and stroke mortality, respectively (2).
Similarly, studies of particulate pollution reported positive associations with increases in cerebrovascular morbidity. In a study by Xiang et al., it was shown that each 10 μg/mm3 increase in PM10 levels resulted in a 1% increase in the number of daily admissions due to stroke (39). Alimohammadi et al., also found a correlation between the increases in PM levels and the number of patients presented to emergency room because of stroke (40). The prevalence of ischemic stroke was observed to increase on lag0-2 days following PM10 elevation (41). In a study of 63,997 stroke cases, PM10 exposure was shown to have a nonlinear but delayed relationship with stroke (43). Women and individuals over the age of 65 years were more affected by PM10 exposure (43). Chen et al., showed that PM10 exposure was cumulatively effective in increasing stroke-related hospitalizations by 4.1% at lag0 and lag1 days (44). Zhang et al., showed that every 10 μg/m3 increments in PM10 level increased stroke-related ED admissions (45). In that study, 65,429 patients were admitted and of those, 1,316 patients died. More recently, in single-pollutant model, each 10 μg/m3 increase in exposure to PM10 was associated with increase in OR for hospital admissions due to recurrent ischemic cerebrovascular events (48). Similarly, levels of PM10 were significantly associated with acute cerebrovascular events in a study collecting data of 2,534 days in a large metropolitan area (49). In contrast to these reports, we could not detect an association between PM10 levels and mortality or ED visits due to stroke. In subgroup analysis, there was no association in women or older adult, either.
Evidence suggests an impact of changes in ambient temperature on cerebrovascular diseases, and both low (50) and higher (51) temperatures reported to induce cerebrovascular mortality. It was also found that although PM10 had an increasing effect on stroke events in cold seasons, this became non-significant in warm seasons suggesting that temperatures may modify adverse health effects of air pollutants (39). Interestingly, increased average daily temperatures reduced the risk of stroke in male population in a recent study from Iran. The authors speculated that high average temperatures could be protective on the risk of Sadeghimoghaddam et al. (36). Although it was shown that meteorological changes (temperature, humidity, and pressure) could influence haemorrhagic stroke, these changes did not have any effect on ischemic stroke (6). In our study population, increased maximum temperatures were associated with mortality due to stroke in the general population, as well as in patients above 65 years. And although we could not find a relation between maximum temperature and visit due to stroke in the general population, we observed an association between maximum temperature and increased ED stroke visits in females, while this was decreased in males. We think that the increase in air temperature as well as clinical conditions such as tachycardia, increased systemic arterial pressure, hyperthermia, and fluid and electrolyte imbalance displacement contributed to the mortality.
Limitations of the study
The most significant limitation was the fact that this was a retrospective study.
Conclusion
Our findings have demonstrated that PM10 pollution, desert dust storms and meteorological variables such as ambient temperature can adversely affect cerebrovascular mortality and morbidity in Southeast Turkey. Health authorities, national and local authorities should develop mitigation strategies and take preventive measures against global climate change and environmental problems such as air pollution.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the participants was not required to participate in this study in accordance with the national legislation and the institutional requirement. Approval details from ethics committee: (23.06.2014/228).
Author contributions
MO, BA, and HB participated in designing the study. MB, HG, and MO provided the meteorological and hospital data. SK performed statistical modeling and tabulation of results and wrote the first draft of the paper. MB, BA, and HB helped in writing the final manuscript and discussion of the results. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
1. Saini, V, Guada, L, and Yavagal, DR. Global epidemiology of stroke and access to acute ischemic stroke interventions. Neurology. (2021) 97:S6–S16. doi: 10.1212/WNL.0000000000012781
2. Scheers, H, Jacobs, L, Casas, L, Nemery, B, and Nawrot, TS. Long-term exposure to particulate matter air pollution is a risk factor for stroke: meta-analytical evidence. Stroke. (2015) 46:3058–66. doi: 10.1161/STROKEAHA.115.009913
3. Lee, KK, Miller, MR, and Shah, ASV. Air pollution and stroke. J Stroke. (2018) 20:2–11. doi: 10.5853/jos.2017.02894
4. Tecer, LH. A factor analysis study: air pollution, meteorology, and hospital admissions for respiratory diseases. Toxicol Environ Chem. (2009) 91:1399–411. doi: 10.1080/02772240902732316
5. Al, B, Bogan, M, Zengin, S, Sabak, M, Kul, S, Oktay, MM, et al. Effects of dust storms and climatological factors on mortality and morbidity of cardiovascular diseases admitted to ED. Emerg Med Int. (2018) 2018:3758506–7. doi: 10.1155/2018/3758506
6. Çevik, Y, Doğan, NÖ, Daş, M, Ahmedali, A, Kul, S, and Bayram, H. The association between weather conditions and stroke admissions in Turkey. Int J Biometeorol. (2015) 59:899–905. doi: 10.1007/s00484-014-0890-9
7. Bogan, M, Al, B, Kul, S, Zengin, S, Oktay, M, Sabak, M, et al. The effects of desert dust storms, air pollution, and temperature on morbidity due to spontaneous abortions and toxemia of pregnancy: 5-year analysis. Int J Biometeorol. (2021) 65:1733–9. doi: 10.1007/s00484-021-02127-8
8. Boğan, M, Kul, S, Al, B, Oktay, M, Akpinar Elçi, M, Pinkerton, KE, et al. Effect of desert dust storms and meteorological factors on respiratory diseases. Allergy. (2022) 77:2243–6. doi: 10.1111/all.15298
9. Bayram, H, Bauer, AK, Abdalati, W, Carlsten, C, Pinkerton, KE, Thurston, GD, et al. Environment, global climate change, and cardiopulmonary health. Am J Respir Crit Care Med. (2017) 195:718–24. doi: 10.1164/rccm.201604-0687PP
10. Bayram, H, Rice, MB, Abdalati, W, Akpinar Elci, M, Mirsaeidi, M, Annesi-Maesano, I, et al. Impact of global climate change on pulmonary health: susceptible and vulnerable populations. Ann Am Thorac Soc. (2023) 20:1088–95. doi: 10.1513/AnnalsATS.202212-996CME
11. Hu, LW, Lawrence, WR, Liu, Y, Yang, BY, Zeng, XW, Chen, W, et al. Ambient air pollution and morbidity in Chinese. Adv Exp Med Biol. (2017) 1017:123–51. doi: 10.1007/978-981-10-5657-4_6
12. IPCC. Summary for policymakers In: Core Writing Team, H Lee and J Romero, editors. Climate change 2023: synthesis report. Contribution of working groups I, II and III to the sixth assessment report of the intergovernmental panel on climate change. Geneva, Switzerland: IPCC (2023). 1–34.
13. Bayram, H., and Öztürk, A. B. (2021). Global climate change, desertification, and its consequences in Turkey and the Middle East. In: K.E. Pinkerton and W.N. Rom (eds.), Climate change and global public health, 445–458 Berlin: Springer.
14. Semenza, JC, Rubin, CH, Falter, KH, Selanikio, JD, Flanders, WD, Howe, HL, et al. Heat-related deaths during the July 1995 heat wave in Chicago. N Engl J Med. (1996) 335:84–90. doi: 10.1056/NEJM199607113350203
15. Pinkerton, K, Rom, W, Carlsten, C, JJK, J, Bayram, H, Sigsgaard, T, et al. Climate change and global public health. Turk Toraks Derg. (2013) 14:115–22. doi: 10.5152/ttd.2013.54
16. Köne, AÇ, and Büke, T. A comparison for Turkish provinces’ performance of urban air pollution. Renew Sust Energ Rev. (2012) 16:1300–10. doi: 10.1016/j.rser.2011.10.006
17. Baltaci, H. Spatial and temporal variation of the extreme Saharan dust event over Turkey in March 2016. Atmosphere. (2017) 8:41. doi: 10.3390/atmos8020041
18. WHO-Breathlife (2023). The air pollution in Gaziantep, Turkey. Available at: https://breathelife2030.org/city_data/gaziantep/ (Accessed August 18, 2023).
19. Perfumo, A, and Marchant, R. Global transport of thermophilic bacteria in atmospheric dust. Environ Microbiol Rep. (2010) 2:333–9. doi: 10.1111/j.1758-2229.2010.00143.x
20. Ganor, E, Osetinsky, I, Stupp, A, and Alpert, P. Increasing trend of African dust, over 49 years, in the eastern Mediterranean. J Geophys Res Atmos. (2010) 115:D07201. doi: 10.1029/2009JD012500
21. NOAA Research. (2020). NOAA earth system research laboratory global monitoring division. Available at: https://www.esrl.noaa.gov/gmd/grad/surfrad/aod/ (Accessed March 3, 2020).
22. Wilcox, EM, Lau, KM, and Kim, KM. A northward shift of the North Atlantic Ocean intertropical convergence zone in response to summertime Saharan dust outbreaks. Geophys Res Lett. (2010) 37:L04804. doi: 10.1029/2009GL041774
23. Aldrin, M, and Haff, IH. Generalised additive modelling of air pollution, traffic volume and meteorology. Atmos Environ. (2005) 39:2145–55. doi: 10.1016/j.atmosenv.2004.12.020
24. Ravindra, K, Rattan, P, Mor, S, and Aggarwal, AN. Generalized additive models: building evidence of air pollution, climate change and human health. Environ Int. (2019) 132:104987. doi: 10.1016/j.envint.2019.104987
25. Orru, H, Idavain, J, Pindus, M, Orru, K, Kesanurm, K, Lang, A, et al. Residents' self-reported health effects and annoyance in relation to air pollution exposure in an industrial area in eastern-Estonia. Int J Environ Res Public Health. (2018) 15:252. doi: 10.3390/ijerph15020252
26. Crooks, JL, Cascio, WE, Percy, MS, Reyes, J, Neas, LM, and Hilborn, ED. The association between dust storms and daily non-accidental mortality in the United States, 1993-2005. Environ Health Perspect. (2016) 124:1735–43. doi: 10.1289/EHP216
27. Mallone, S, Stafoggia, M, Faustini, A, Gobbi, GP, Marconi, A, and Forastiere, F. Saharan dust and associations between particulate matter and daily mortality in Rome, Ialy. Environ Health Perspect. (2011) 119:1409–14. doi: 10.1289/ehp.1003026
28. Yorifuji, T, and Kashima, S. Associations of particulate matter with stroke mortality: a multicity study in Japan. J Occup Environ Med. (2013) 55:768–71. doi: 10.1097/JOM.0b013e3182973092
29. Tarnoki, AD, Turker, A, Tarnoki, DL, Iyisoy, MS, Szilagyi, BK, Duong, H, et al. Relationship between weather conditions and admissions for ischemic stroke and subarachnoid hemorrhage. Croat Med J. (2017) 58:56–62. doi: 10.3325/cmj.2017.58.56
30. Karanasiou, A, Moreno, N, Moreno, T, Viana, M, de Leeuw, F, and Querol, X. Health effects from Sahara dust episodes in Europe: literature review and research gaps. Environ Int. (2012) 47:107–14. doi: 10.1016/j.envint.2012.06.012
31. Yatkın, S, and Bayram, A. The air borne particulate matter pollution in İzmir. DEÜ Mühendislik Fakültesi, Fen ve Mühendislik Dergisi. (2007) 9:1527.
32. Yang, CY, Cheng, MH, and Chen, CC. Effects of Asian dust storm events on hospital admissions for congestive heart failure in Taipei, Taiwan. J Toxicol Environ Health Part A. (2009) 72:324–8. doi: 10.1080/15287390802529880
33. Kamouchi, M, Ueda, K, Ago, T, Nitta, H, and Kitazono, T, Fukuoka Stroke Registry Investigators. Relationship between Asian dust and ischemic stroke: a time-stratified case-crossover study. Stroke. (2012) 43:3085–7. doi: 10.1161/STROKEAHA.112.672501
34. Yang, CY, Chen, YS, Chiu, HF, and Goggins, WB. Effects of Asian dust storm events on daily stroke admissions in Taipei, Taiwan. Environ Res. (2005) 99:79–84. doi: 10.1016/j.envres.2004.12.009
35. Kang, JH, Liu, TC, Keller, J, and Lin, HC. Asian dust storm events are associated with an acute increase in stroke hospitalisation. J Epidemiol Community Health. (2013) 67:125–31. doi: 10.1136/jech-2011-200794
36. Sadeghimoghaddam, A, Khankeh, H, Norozi, M, Fateh, S, and Farrokhi, M. Effects of dust events and meteorological elements on stroke morbidity in northern Khuzestan, Iran. J Educ Health Promot. (2021) 10:406. doi: 10.4103/jehp.jehp_1686_20
37. Guan, T, Xue, T, Liu, Y, Zheng, Y, Fan, S, He, K, et al. Differential susceptibility in ambient particle-related risk of first-ever stroke: findings from a National Case-Crossover Study. Am J Epidemiol. (2018) 187:1001–9. doi: 10.1093/aje/kwy007
38. Guo, P, Wang, Y, Feng, W, Wu, J, Fu, C, Deng, H, et al. Ambient air pollution and risk for ischemic stroke: a short-term exposure assessment in South China. Int J Environ Res Public Health. (2017) 14:1091. doi: 10.3390/ijerph14091091
39. Xiang, H, Mertz, KJ, Arena, VC, Brink, LL, Xu, X, Bi, Y, et al. Estimation of short-term effects of air pollution on stroke hospital admissions in Wuhan, China. PloS One. (2013) 8:e61168. doi: 10.1371/journal.pone.0061168
40. Alimohammadi, H, Fakhri, S, Derakhshanfar, H, Hosseini-Zijoud, SM, Safari, S, and Hatamabadi, HR. The effects of air pollution on ischemic stroke admission rate. Chonnam Med J. (2016) 52:53–8. doi: 10.4068/cmj.2016.52.1.53
41. Zhong, H, Shu, Z, Zhou, Y, Lu, Y, Yi, B, Tang, X, et al. Seasonal effect on association between atmospheric pollutants and hospital emergency room visit for stroke. J Stroke Cerebrovasc Dis. (2018) 27:169–76. doi: 10.1016/j.jstrokecerebrovasdis.2017.08.014
42. Wichmann, J, and Voyi, K. Ambient air pollution exposure and respiratory, cardiovascular and cerebrovascular mortality in Cape Town, South Africa: 2001–2006. Int J Environ Res Public Health. (2012) 9:3978–4016. doi: 10.3390/ijerph9113978
43. Wang, Z, Peng, J, Liu, P, Duan, Y, Huang, S, Wen, Y, et al. Association between short-term exposure to air pollution and ischemic stroke onset: a time-stratified case-crossover analysis using a distributed lag nonlinear model in Shenzhen, China. Environ Health Glob Access Sci Source. (2020) 19:1. doi: 10.1186/s12940-019-0557-4
44. Chen, L, Zhang, Y, Zhang, W, Chen, G, Lu, P, Guo, Y, et al. Short-term effect of PM1 on hospital admission for ischemic stroke: a multi-city case-crossover study in China. Environ Pollut. (2020) 260:113776. doi: 10.1016/j.envpol.2019.113776
45. Zhang, Y, Ma, Y, Feng, F, Cheng, B, Wang, H, Shen, J, et al. Association between PM10 and specific circulatory system diseases in China. Sci Rep. (2021) 11:12129. doi: 10.1038/s41598-021-91637-x
46. Vivanco-Hidalgo, RM, Wellenius, GA, Basagaña, X, Cirach, M, González, AG, Ceballos, P, et al. Short-term exposure to traffic-related air pollution and ischemic stroke onset in Barcelona, Spain. Environ Res. (2018) 162:160–5. doi: 10.1016/j.envres.2017.12.024
47. Yan, Y, Chen, X, Guo, Y, Wu, C, Zhao, Y, Yang, N, et al. Ambient air pollution and cerebrovascular disease mortality: an ecological time-series study based on 7-year death records in Central China. Environ Sci Pollut Res Int. (2021) 28:27299–307. doi: 10.1007/s11356-021-12474-z
48. Xu, R, Tian, Q, Lu, W, Yang, Z, Ye, Y, Li, Y, et al. Association of short-term exposure to air pollution with recurrent ischemic cerebrovascular events in older adults. Int J Hyg Environ Health. (2022) 240:113925. doi: 10.1016/j.ijheh.2022.113925
49. Versaci, F, Anticoli, S, Pezzella, FR, Mangiardi, M, Di Giosa, A, Marchegiani, G, et al. Impact of weather and pollution on the rate of cerebrovascular events in a large metropolitan area. Panminerva Med. (2022) 64:17–23. doi: 10.23736/S0031-0808.21.04525-0
50. McDonagh, R, and Harbison, J. Autumn weather and winter increase in cerebrovascular disease mortality. Ir Med J. (2016) 109:479.
Keywords: desert dust storms, maximum temperature, stroke, emergency department visits, mortality
Citation: Oktay MM, Al B, Boğan M, Kul S, Gümüşboğa H and Bayram H (2023) Impact of desert dust storms, PM10 levels and daily temperature on mortality and emergency department visits due to stroke. Front. Public Health. 11:1218942. doi: 10.3389/fpubh.2023.1218942
Edited by:
Paolo Lauriola, International Society Doctors for the Environment (ISDE), ItalyReviewed by:
Domenico Vito, Polytechnic University of Milan, ItalyCopyright © 2023 Oktay, Al, Boğan, Kul, Gümüşboğa and Bayram. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mustafa Boğan, bXVzdGFmYWJvZ2FuQGhvdG1haWwuY29t