 Nisreen Alwan
Nisreen Alwan Shatha Almazrouei1
Shatha Almazrouei1 Wissam Ghach
Wissam Ghach- 1College of Health Sciences, Abu Dhabi University, Abu Dhabi, United Arab Emirates
- 2Faculty of Communication, Arts and Sciences, Canadian University Dubai, Dubai, United Arab Emirates
Introduction: Disinfection is one of the most effective hygienic practices that would limit the spread of the Coronavirus Disease (COVID-19) through deactivating the coronavirus on contaminated skin, supplies, and surfaces. However, the type and concentration of disinfectants should be carefully selected to avoid damaging surfaces and to limit the side effects of these chemicals on household members and users. The aim of this study is to assess the public levels of awareness and performance concerning the safe use of household cleaning products and disinfectants during the spread of COVID-19 in the Emirate of Abu Dhabi.
Methods: The cross-sectional study was conducted between October and December 2021 among 750 residents of Abu Dhabi, Al Dhafrah, and Al-Ain regions. A google survey was distributed electronically for the online recruitment of the general population. Mann-Whitney and Kruskal-Wallis tests were used to determine whether significant differences exist in the levels of awareness and performance with regard to gender, region, education level, and diagnosis with COVID-19. Spearman correlation was used to test if any correlation existed between levels of awareness and performance. Kruskal-Wallis test was also used to check if significant differences exist in the mean score of performance with respect to irritation-to-poisoning symptoms.
Results: The study population recorded a lower mean score of awareness (5.37 out of 12) than performance (11.75 out of 16). The majority of the study population claimed a minimum of one irritation-to-poisoning symptom during the handling of household cleaners and disinfectants. Significant differences exist in the awareness and performance mean scores among various educational levels (P < 0.001). The level of awareness was statistically significant with regard to infection with SARS-CoV-2 (P < 0.05). Also, the level of performance was significantly different between males and females (P < 0.001). Kruskal-Wallis test showed that the mean score of performance is statistically significant with all the studied irritation-to poisoning symptoms (P < 0.05).
Conclusions: Awareness campaigns and training programs are recommended to address the safe use of household cleaning products and disinfectants in the United Arab Emirates (UAE).
1. Introduction
The Coronavirus Disease 2019 (COVID-19), caused by the novel coronavirus SARS-CoV-2, was responsible for causing the cataclysmic pandemic globally (1). This has brought the world to a standstill creating a universal huge impact. As a result, more than 500 million infected cases and six million deaths were reported throughout the world (2). SARS-CoV-2 is transmitted mainly through human-to-human and surfaces-to-human close interactions especially when the surfaces are exposed to coughing, sneezing, and aerosols from COVID patients (3). To limit the spread of SARS-CoV-2, WHO has recommended social distancing and regular practices of hygiene on the personal and household levels (4).
Disinfection is one of the hygienic practices that provide an effective way to limit the spread of COVID-19 through deactivating the coronavirus on contaminated skin, supplies, and surfaces (4). Cleaning with soapy water using mechanical processes such as brushing or scrubbing removes dirt, debris, and organic elements, but may not kill microorganisms (5). Therefore, a chemical disinfectant is required after cleaning with soap and water to kill any remaining microorganism. Ethanol, isopropanol, hydrogen peroxide, sodium hypochlorite, other chlorine-containing disinfectants, benzalkonium chloride, or quaternary ammonium compounds are all examples of chemical disinfectants (6). However, the type and concentration of disinfectants should be carefully selected to avoid damaging surfaces and to limit the side effects of these chemicals on household members and users. For example, alcohol-based hand sanitizers may cause dermal and digestive irritation to death when ingested or dermally absorbed by accident (7). Household cleaners (e.g., sodium hypochlorite) may lead to acute lung diseases and cancer when mixed with acid or amine products, respectively (8). Thus, users shall be well-educated about these chemicals for safe utilization with no unintended health risks.
Since the beginning of the pandemic, several medical centers around the world have reported accidental poisoning cases related to the misuse of disinfectants (9–11). Responding to their anxiety about being infected with SARS-CoV-2, people increased their hygiene practices (e.g., sanitizer use) and thereby increased the risk of exposure to chemical disinfectants when misused (8, 9, 12). Between 2019 and 2020, Dammam Poison Control Center in Saudi Arabia revealed that the public exposure increased from 9.8 to 20.4% and from 0.4 to 3.4% for surface disinfectants and hand sanitizers, respectively (9). Additionally, CDC recorded in its Morbidity and Mortality Weekly Report (April 2020) a sharp increase in the chemical exposures (COVID cleaners and disinfectants) in the United States of America (USA) (13). Among the reported cases, an adult woman claimed difficulty breathing, coughing, and wheezing following her smelling of a mixture of 10% bleach solution, vinegar, and hot water (13). Also, a pre-school aged child claimed dizziness, vomiting, and poor responsiveness after ingesting an unknown amount of an ethanol-based hand sanitizer (13). The investigation among the population revealed limited knowledge and consequently high-risk practices regarding the safe handling of household cleaning-disinfection products during the spread of COVID-19 in the United States (14). According to the literature, public awareness, practices, and sources of information were the interrelated variables that affected the safe use of chemical disinfectants among the populations (14–16).
In the UAE, it had been observed that people are experiencing vast growth in their awareness because of the huge number of campaigns and activities related to the coronavirus pandemic on the internet and social media platforms (1, 17). A study conducted by Baniyas et al. (1) depicted that the majority of medical students gained awareness about the pandemic from social media (high risk of inaccurate information) and a very less fraction of around 5% got information from health practitioners. Two studies had investigated COVID-related knowledge and practices (e.g., precautions and personal hygiene) among different populations in the UAE (1, 17). However, no studies assessed the public community's awareness and performance regarding the use of cleaners and disinfectants at the household level where chemicals (e.g., sodium hypochlorite) could be fatal when misused.
This study evaluates the public awareness and performance of using disinfectants and household cleaners in the UAE specifically in the Emirate of Abu Dhabi. The outcome is expected to enrich the governmental authorities, healthcare professionals, and public health researchers with new evidence on the public awareness of the safe use of household chemicals and their potential implications on the public health of the communities in UAE as part of the UN sustainability goal of well-being (SDG 3).
2. Methods
This cross-sectional study was conducted between October and December 2021 to evaluate the public community's awareness and performance regarding the use of household cleaning products and disinfectants in the Emirate of Abu Dhabi. An online Google survey was distributed throughout email and social media platforms.
2.1. Population
The total number of respondents was 750 persons residing in Abu Dhabi, Al Dhafrah, and Al-Ain regions. The study population was stratified into groups based on gender, age, educational level, and prior infection with SARS-CoV-2. Individuals below 18 years old were excluded from the study.
2.2. Study tool
The questionnaire was adapted from the Morbidity and Mortality Weekly Report (2020)—Centers for Disease Control and Prevention (14) and validated by experts and academicians in the field. The structure of the study tool was divided into 6 sections: (1) Sociodemographic data; (2) Participants' experience with SARS-CoV-2; (3) Sources of information about preventive measures of COVID-19; (4) 9 awareness-related items with 4-point Likert scale (strongly disagree to strongly agree); (5) 9 performance-related items with Yes/No and Always-Sometimes-Never scales; and (6) 8 symptom-related items with Always-Sometimes-Never scale. Each awareness/performance item was graded on a score of 0 for an incorrect response and 1 for a correct response. For the awareness variable, a score of ≤ 3 was considered weak, between 4 and 6 was considered average, and 7 or above was considered good awareness. Likewise, for the variable performance, scores of 6 or below were considered weak, scores between 7 and 11 inclusive were considered average, and scores 12 and above were considered good performance.
2.3. Study analysis
The data were analyzed using the Statistical Package for the Social Sciences, version 22 (SPSS, International Business Machine Corp. IBM, Chicago, IL, USA). Percent frequency was obtained from SPSS and organized in tables to reflect the sociodemographic profile of the participants and their level of awareness and performance. The scores of awareness and performance were evaluated by descriptive analyses. Mann-Whitney test was used to determine if significant mean differences exist with regard to gender and diagnosis with COVID-19. Kruskal-Wallis test was used to check for mean differences with regard to region and education level. No comparison was made for age as the distribution was not very representative for each interval. Prior to that, normality and homogeneity of variances were tested using Kolmogorov-Smirnov and Levene's tests respectively for all variables rendering violations in these two assumptions with P < 0.05. Spearman correlation test was used to determine the correlation between awareness and performance of participants regarding the safe use of disinfectants-cleaners. Kruskal-Wallis test was used to investigate whether significant differences exist in awareness and performance with respect to irritation-to-poisoning symptoms. All data analysis was carried out at a significance level of <0.05.
2.4. Ethical considerations
The study protocol was approved by the Institutional Review Board (IRB) at the University (CoHS-21-10-32). The questionnaire included a consent form introducing the respondents to the study's purpose, benefits, confidentiality, and the absence of potential risks. In addition to that, it reinforces that participation in this study is voluntary and that the submission of the questionnaire indicates the individual's consent to participate in the study.
3. Results
3.1. Sociodemographic profile of the study population
A total of 750 participants completed the online questionnaire through email and social media outlets (Facebook, LinkedIn, and Instagram). The profile of the sample population is presented in Table 1. The Emirate of Abu Dhabi was almost equally represented by the sample population. The sex ratio (M:F) of the sample population was 1:1.12, where 683 participants (91.1 %) were between the ages of 18 and 39 years with a mean age of 27.6 (±SD = 8.39). In terms of educational level, around 70 % of the participants were well-educated (bachelor's level or higher). Looking at the medical status of the sample population, more than half of the participants (54.3 %) claimed that they have not been infected with SARS-CoV-2.
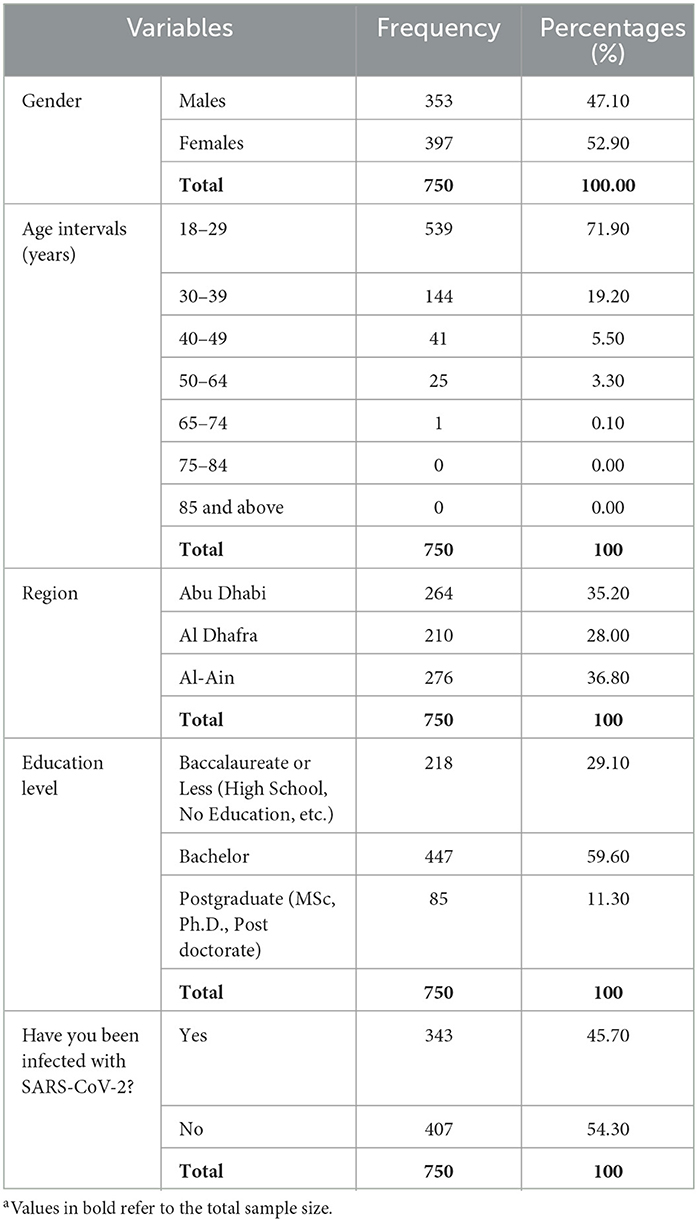
Table 1. Sociodemographic profile of the study populationa.
3.2. Sources of information about preventive measures of COVID-19
Focusing on the sources of information on the preventive measures of COVID-19 (Figure 1), 65.3 % of the responses indicated that the participants obtained information from healthcare professionals, governmental agencies, international agencies, and organizations (Ministry of Health and Prevention; National Emergency Crisis and Disasters Management Authority; Centers for Disease Control and Prevention; World Health Organization; and Healthcare Professionals such as Medical Doctors, Nurses, and Public Health Specialists). On the other hand, 34.7 % of the participants' responses preferred other resources such as social media platforms, internet search engines, and personal experience.
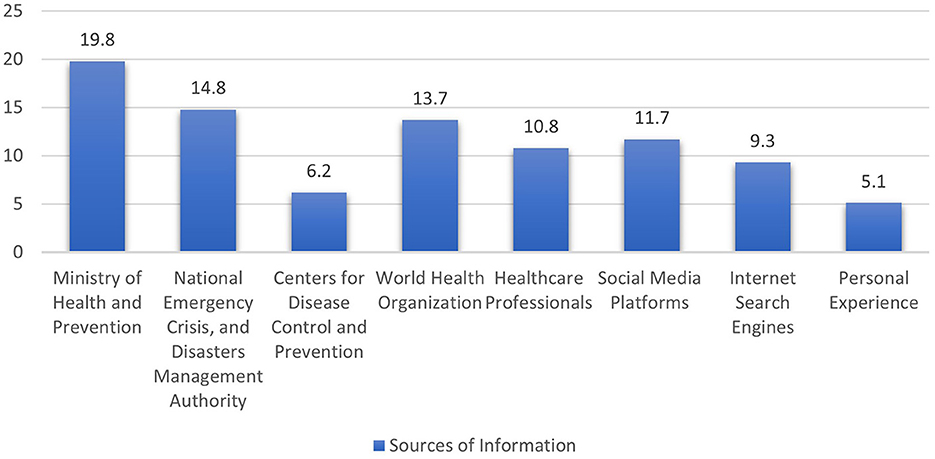
Figure 1. Percentage frequency of the participants' reliance on local and international sources of COVID-19 information.
3.3. Community's levels of awareness and performance
A total of nine questions were utilized to assess the community's awareness regarding the safe use of household cleaning products and disinfectants as represented in Table 2. The mean score was 5.37 out of 12 (±SD of 2.66) where only 25 % of the sample population (188 out of 750 participants) showed weak awareness of storage, personal protective equipment (PPE), and application protocols of the cleaning-disinfecting products. At the awareness level, more than 50 % of the study population did not recognize the CDC and WHO recommendations for non-mixing chlorine solution with any other substances (e.g., acid, ammonia), and keeping chlorine solution at ambient temperature (4, 18).
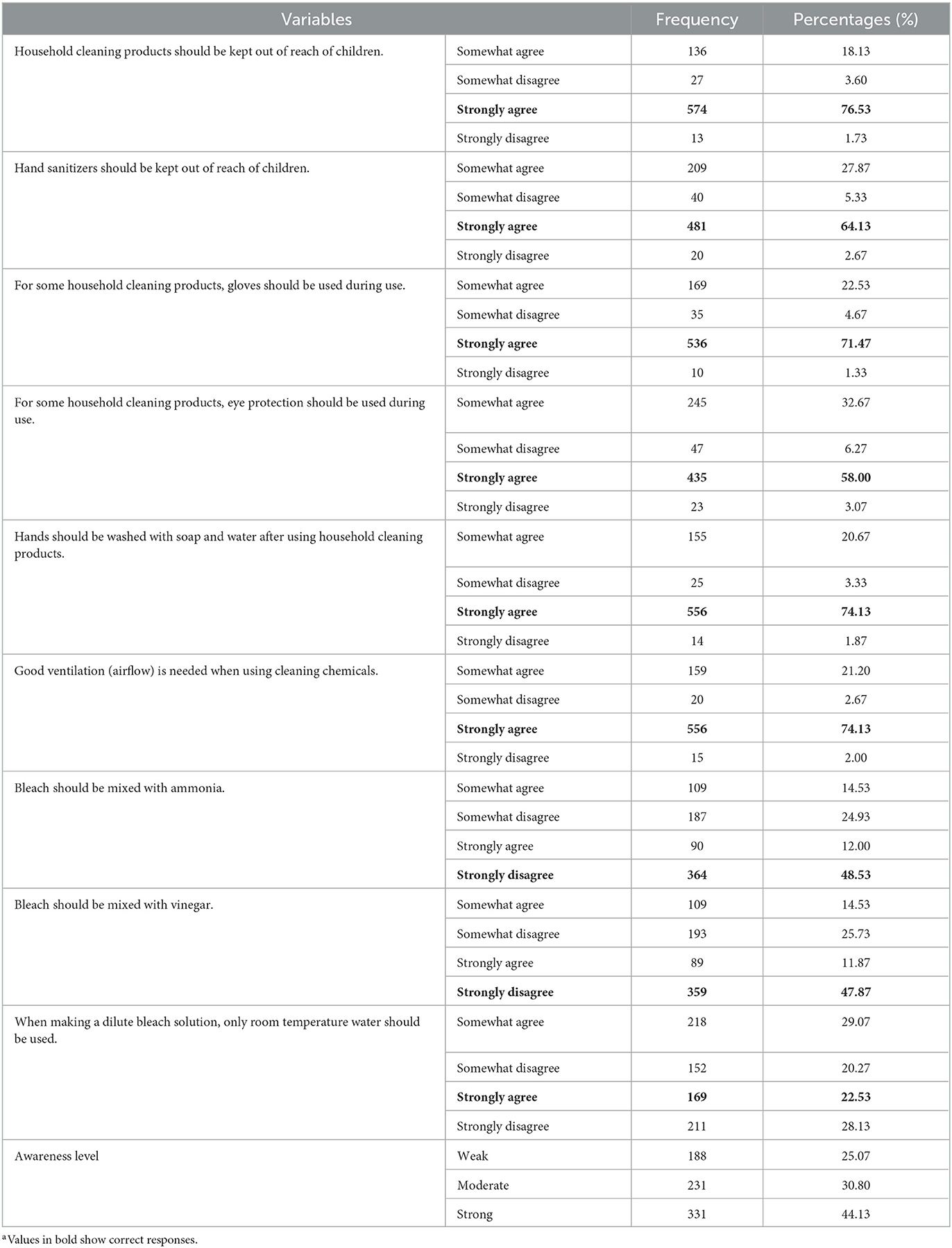
Table 2. Community's level of awareness regarding the use of household cleaning products and disinfectantsa.
A total of nine questions were utilized to assess the community's performance regarding the safe use of household cleaning products and disinfectants (Table 3). The mean score was 11.75 out of 16 (±SD = 3.16) where only 9 % of the sample population (67 out of 750 participants) showed weak performance during the use of cleaning products and disinfectants in household settings. At the performance level, more than 50 % of the study population recorded low adherence to the WHO and CDC guidelines for never inhaling the vapor of household cleaners during the hygiene process; washing vegetables, fruits, and skin with household cleaners (4, 19, 20).

Table 3. Community's level of performance regarding the use of household cleaning products and disinfectantsa.
The Spearman correlation test showed that the community awareness and performance were weakly correlated (rho = 0.251, p < 0.001).
3.4. Association of awareness and performance with the participants' sociodemographics
The mean scores of awareness and performance levels per sociodemographic variable and the total mean score of awareness and performance are shown in Table 4. Results of the Mann-Whitney test showed no significant differences in the awareness level between males and females (P = 0.303 > 0.05, Table 4) although females have a higher mean awareness score than males. As per the P-value of the Kruskal-Wallis test, no significant differences existed in the awareness level among the three regions in the Emirate of Abu Dhabi (Table 4) with the highest mean score in Al-Ain followed by Al Dhafra then Abu Dhabi, respectively. Significant differences exist in the level of awareness among different levels of education (P < 0.001) with the highest mean score in participants holding post graduate degrees followed by those holding a bachelor's degree and less with those with baccalaureate or less (Table 4). According to the Mann-Whitney test, significant differences exist in the awareness level between those diagnosed with COVID-19 and those who were not (P = 0.024 <0.05, Table 4).

Table 4. Awareness and performance level mean scores classified as per socio-demographic variables.
On the other hand, results of the Mann-Whitney test showed significant differences in the performance level between males and females (P < 0.001, Table 4) with males having a higher mean performance score than females. As per the P-value of the Kruskal-Wallis test, no significant differences existed in the performance level among the three regions in the Emirate of Abu Dhabi (P = 0.491 > 0.05, Table 4) with the highest mean score in Abu Dhabi followed by Al Dhafra then Al–Ain, respectively. Significant differences exist in the level of performance among different levels of education (P < 0.001) with the highest mean score in participants holding a bachelor's degree followed by those holding post graduate degrees and less with those with baccalaureate or less (Table 4). According to the Mann-Whitney test, no significant differences exist in the performance level between those diagnosed with COVID-19 and those who were not (P = 0.918 > 0.05, Table 4).
3.5. Symptoms encountered during the use of household chemicals
To study the relationship between community performance and non-safe exposure to household cleaning products and disinfectants, the occurrence of irritation-to-poisoning symptoms had been investigated as shown in Figure 2. Participants who claimed no irritation-to-poisoning symptoms ranged between 33.7 % (Skin irritation) and 49.6 % (Upset stomach). However, the rest of the sample population had claimed a minimum of one irritation-to-poisoning symptom when they used household cleaners and disinfectants during COVID-19. The claimed symptoms among the sample population were comparable with the highest occurrence of skin irritation (Sometimes-to-always: 66.3 %) and the lowest occurrence of upset stomach (Sometimes-to-always: 50.4 %).
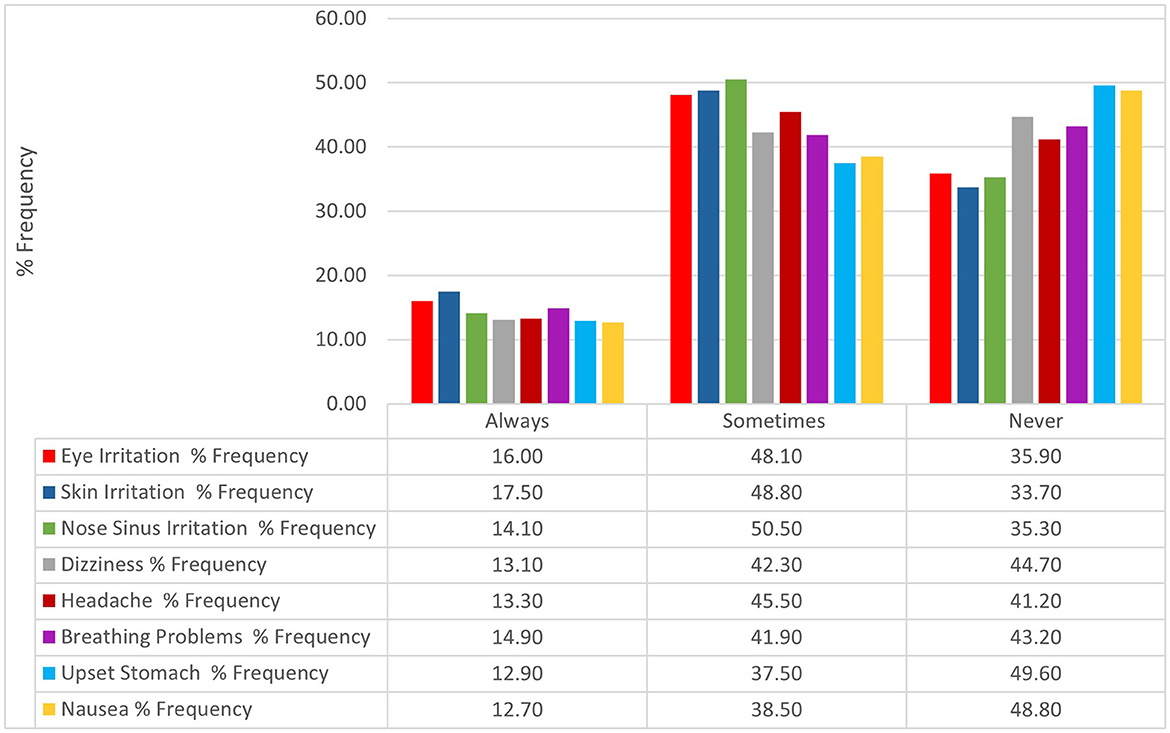
Figure 2. Percentage frequency of symptoms encountered by the study population.
The Kruskal-Wallis test was applied to investigate significant differences in the awareness and performance level mean score among the irritation-to-poisoning symptoms. The test revealed statistical significance between the awareness and performance levels and all the studied symptoms (P < 0.05): Eye irritation (A & P levels: P < 0.001); Skin irritation (A & P levels: P < 0.001); Nose-sinus irritation (A level: P = 0.001; P level: P < 0.001); Dizziness (A & P levels: P < 0.001); Headache (A & P levels: P < 0.001); Breathing problems (A & P levels: P < 0.001); Upset stomach (A & P levels: P < 0.001); and Nausea (A & P levels: P < 0.001) (Table 5).
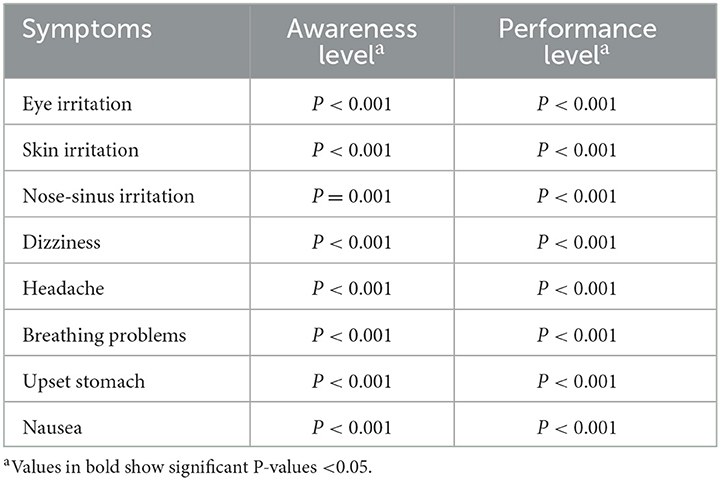
Table 5. Statistical results of awareness and performance levels as per symptoms.
4. Discussion
This study is the first study that assessed public awareness and performance regarding the safe use of household cleaning products and disinfectants during the spread of the pandemic in the UAE. For the first time, it sheds light on the quality of the prevention measures to stop the spread of the SARS-CoV-2 virus within households in the Emirate of Abu Dhabi. An anticipated output is to provide healthcare professionals and public health scientists with new evidence on the public awareness and performance of household cleaning products and disinfectants in the Emirate of Abu Dhabi. The outcome and implications of this study are not limited to the pandemic era and may provide a database to estimate the extent of the safe use of household cleaners during day-to-day application after the pandemic. Public health initiatives may use these findings to design effective awareness campaigns using pictorial instructions, animation videos, real life-based storytelling, and technical training programs to highlight misconceptions and mishandling of cleaning products and disinfectants at the household level. Additionally, the study findings could stress on the research communities to overcome the gap of absence/limited surveys of chemical awareness through the development and validation of new tools in multiple languages for developed and developing countries, and to integrate the knowledge of chemical safety in the educational curricula at the academic institutions. In comparison with similar studies, this study population showed a higher level of awareness (moderate-to-strong) regarding the safe process of disinfection (14–16, 21). In consistent to other studies (15, 21), the awareness level was somehow low concerning the safe use of some cleaning products and disinfectants such as the acceptance of child's exposure to sanitizers which may increase the risk of children poisoning by ingesting the residue of alcohol when putting their hands in their mouths or eating food directly post disinfection with sanitizers (9, 22). Additionally, the elevation of hygiene processes along with the low awareness regarding the preparation of cleaning products may increase the risk of hazardous releases such as chloroform and chloramine, or chlorine gas when bleach is mixed with ammonia or vinegar, respectively (8, 23). Also, diluting a chlorine solution at a high temperature is not recommended where a loss of disinfection power is expected by the decomposition of hypochlorite (the active ingredient of bleach) (24).
Compared to the other Middle Eastern studies (15, 16), the study population showed a higher level of performance (moderate-to-strong) than awareness. This finding could be explained by the focus of awareness campaigns on the practical awareness of disinfectants rather than the basic and scientific knowledge (16). Similar to other published studies (14, 25), the incidence of some inappropriate practices (e.g., washing vegetables and fruits with a chlorine solution, disinfecting bare skin with chemical detergents, inhaling the smell of household cleaners, and less frequently drinking or gargling with household products) were reported in this study.
The Spearman correlation test showed a weak correlation between community awareness and performance. This finding could be explained by a presence of an third factor (attitude) who have higher influence on the participants' adherence to the safe processes than awareness variable (26). However, the attitude variable which was not investigated to prove this hypothesis.
Another important variable was the occurrence of irritation-to-poisoning symptoms among half of the study population during their use of household cleaning products and disinfectants. Specifically, headache, respiratory and dermal irritations were the main reported symptoms in comparison to the Egyptian study where multiple respiratory and dermal symptoms of chemical toxicity were commonly detected (15). The recorded symptoms were completely associated (P <0.05) with the participants' awareness and performance to confirm that the study population and their family members were somehow vulnerable to food poisoning and respiratory problems according to the low awareness and misuse of cleaning products at homes (15).
Notable variables were gender and education level, and prior infection with SARS-CoV-2 regarding the levels of awareness and performance. The gender-based finding was inconsistent with the literature where females recorded a higher awareness but lower performance scores than males (16, 27–29). The dominant role of mothers, homemakers, or cleaning staff would explain why females had a higher level of awareness concerning hygiene processes and products (30). Well-educated participants (Bachelor and higher levels) recorded higher scores of awareness and performance than less/non-educated participants. As mentioned in the literature, the higher the education level, the higher the awareness and performance levels concerning preventive measures and disinfectant use (16, 29, 31). In addition, education may play an important role in choosing reliable sources of information and avoiding any online sources with misinformation and no scientific support (32). Participants who previously experienced COVID-19 recorded a higher mean score of awareness than the participants who had never been diagnosed with COVID-19. This is in congruence with a study conducted by Aldhahri and Alghamdi (33) regarding awareness about COVID symptoms.
Several limitations are noted in this study. Findings were based on subjective analysis which may not be associated with clinical investigations. Self-responding bias is expected to affect the study finding too. The electronic data collection may weaken the randomness of the sampling especially that the lack of familiarity with the electronic devices and/or social media platforms is expected among the public community. As a result, the age distribution of the sample population was affected by the electronic procedure of data collection where most of the participants were young participants (aged 18–39) who are expected to have more accessibility to the social media platforms.
The awareness and performance levels concerning the use of household cleaning products and disinfectants were moderate-to-strong among the majority of the study population. However, public awareness was lower than their performance level along with the incidence of irritation-to-poisoning symptoms among the majority of the study population, indicating the necessity of more training programs (theoretical and practical awareness) in governmental webpages, academic institutions, private companies, and the entertainment public places of Abu Dhabi. It was also found that the regional districts of Abu Dhabi showed almost similar levels of performance and awareness. Associated variables such as gender, educational level, and prior infection with SARS-CoV-2 contributed positively to either awareness, performance, or both levels among the study population. Community-based interventions and future studies are recommended to address the above-mentioned variables in addition to the levels of awareness and performance in using cleaning products and disinfectants at the household levels in the UAE.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Institutional Review Board (IRB) at Abu Dhabi University (CoHS-21-10-32). The patients/participants provided their written informed consent to participate in this study.
Author contributions
Conceptualization, formal analysis, supervision, and writing—review and editing: WG and NA. Methodology, data curation, writing—original draft preparation, and project administration: SA, MA, JA, FA, WG, and NA. All authors contributed to the article and approved the submitted version.
Funding
This research study was hosted and resourced by the Abu Dhabi University, and the Canadian University Dubai.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
UAE, United Arab Emirates; COVID-19, Coronavirus Disease 2019; USA, United States of American; WHO, World Health Organization; CDC, Centers for Disease Control and Prevention; US, United States; SPSS, Statistical Package for the Social Sciences; PPE, Personal Protective Equipment.
References
1. Baniyas N, Sheek-Hussein M, Al Kaabi N, Al Shamsi M, Al Neyadi M, Al Khoori R, et al. COVID-19 knowledge, attitudes, and practices of United Arab Emirates medical and health sciences students: a cross sectional study. PLoS ONE. (2021) 16:e0246226. doi: 10.1371/journal.pone.0246226
2. World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. (2022). Available online at: https://covid19.who.int/ (accessed August 26, 2022).
3. Desai AN, Patel P. Stopping the Spread of COVID-19. JAMA. (2020) 323:1516–1516. doi: 10.1001/jama.2020.4269
4. World Health Organization. Cleaning and Disinfection of Environmental Surfaces in the Context of COVID-19. Geneva: World Health Organization (2022).
5. World Health Organization. Essential Environmental Health Standards in Health Care. (2008). Available online at: https://www.who.int/publications/i/item/9789241547239 (accessed June 13, 2022).
6. Samara F, Badran R, Dalibalta S. Are disinfectants for the prevention and control of COVID-19 safe? Health Secur. (2020) 18:496–8. doi: 10.1089/hs.2020.0104
7. Mahmood A, Eqan M, Pervez S, Alghamdi HA, Tabinda AB, Yasar A, et al. COVID-19 and frequent use of hand sanitizers; human health and environmental hazards by exposure pathways. Sci Total Environ. (2020) 742:140561. doi: 10.1016/j.scitotenv.2020.140561
8. Rai NK, Ashok A, Akondi BR. Consequences of chemical impact of disinfectants: safe preventive measures against COVID-19. Crit Rev Toxicol. (2020) 50:513–20. doi: 10.1080/10408444.2020.1790499
9. Mahmoud NF, Al-Mazroua MK, Afify MM. Toxicology practice during COVID-19 pandemic: experience of the dammam poison control Center-Eastern Province, Saudi Arabia. Int J Toxicol. (2021) 40:388–94. doi: 10.1177/10915818211017128
10. Rosenman KD, Reilly MJ, Wang L. Calls to a state poison center concerning cleaners and disinfectants from the onset of the COVID-19 pandemic through April 2020. Public Health Rep. (2021) 136:27–31. doi: 10.1177/0033354920962437
11. Mousavi-Roknabadi RS, Arzhangzadeh M, Safaei-Firouzabadi H, Mousavi-Roknabadi RS, Sharifi M, Fathi N, et al. Methanol poisoning during COVID-19 pandemic; a systematic scoping review. Am J Emerg Med. (2022) 52:69–84. doi: 10.1016/j.ajem.2021.11.026
12. Saddik B, Hussein A, Albanna A, Elbarazi I, Al-Shujairi A, Temsah M-H, et al. The psychological impact of the COVID-19 pandemic on adults and children in the United Arab Emirates: a nationwide cross-sectional study. BMC Psychiatry. (2021) 21:1–18. doi: 10.1186/s12888-021-03213-2
13. Chang A, Schnall AH, Law R, Bronstein AC, Marraffa JM, Spiller HA, et al. Cleaning and disinfectant chemical exposures and temporal associations with COVID-19 — national poison data system, United States, January 1, 2020– March 31, 2020. MMWR Morb Mortal Wkly Rep. (2020) 69:496–8. doi: 10.15585/mmwr.mm6916e1
14. Gharpure R, Hunter CM, Schnall AH, Barrett CE, Kirby AE, Kunz J. Knowledge and practices regarding safe household cleaning and disinfection for COVID-19 prevention — United States, May 2020. MMWR Morb Mortal Wkly Rep. (2020) 69:705–9. doi: 10.15585/mmwr.mm6923e2
15. Ahmad MA, Ghaleb SS, Ali IAER, Khalil DM, Hafeez NGA, A. survey study on disinfectants use among egyptians for corona virus protection “knowledge, practice and toxicity”. Int J Med Toxicol Leg Med. (2021) 24:324–30. doi: 10.5958/0974-4614.2021.00102.9
16. Safari Z, Fouladi-Fard R, Vahidmoghadam R, Hosseini MR, Mohammadbeigi A, Omidi Oskouei A, et al. Awareness and performance towards proper use of disinfectants to prevent COVID-19: the case of Iran. Int J Environ Res Public Health. (2021) 18:2099. doi: 10.3390/ijerph18042099
17. Lutfi L, AlMansour A, AlMarzouqi A, Hassan SH, Salman Z, Hamad H, et al. Knowledge, attitude, and practice toward COVID-19 among UAE residents: an online cross-sectional survey. Dubai Med J. (2021) 4:107–14. doi: 10.1159/000516805
18. Centers for Disease Control Prevention. Cleaning, Disinfection, and Hand Hygiene in Schools – a Toolkit for School Administrators. (2021). Available online at: https://www.cdc.gov/coronavirus/2019-ncov/community/schools-childcare/clean-disinfect-hygiene.html (accessed August 26, 2022).
19. Centers for Disease Control Prevention. Show Me the Science – When & How to Use Hand Sanitizer in Community Settings. Handwashing in Communities: Clean Hands Save Lives. (2020). Available online at: https://www.cdc.gov/handwashing/show-me-the-science-hand-sanitizer.html (accessed July6, 2022).
20. Centers for Disease Control Prevention. Fruit and Vegetable Safety. (2022). Available online at: https://www.cdc.gov/foodsafety/communication/steps-healthy-fruits-veggies.html#:~:text=Washing (accessed July 6, 2022).
21. Gharpure R, Miller GF, Hunter CM, Schnall AH, Kunz J, Garcia-Williams AG. Safe use and storage of cleaners, disinfectants, and hand sanitizers: knowledge, attitudes, and practices among US adults during the COVID-19 pandemic, May 2020. Am J Trop Med Hyg. (2021) 104:496. doi: 10.4269/ajtmh.20-1119
22. Tambling RR, Tomkunas AJ, Russell BS, Horton AL, Hutchison M. Thematic analysis of parent–child conversations about covid-19:“playing it safe.” J Child Fam Stud. (2021) 30:325–37. doi: 10.1007/s10826-020-01889-w
23. Kollert S, Döring F, Gergs U, Wischmeyer E. Chloroform is a potent activator of cardiac and neuronal Kir3 channels. Naunyn Schmiedebergs Arch Pharmacol. (2020) 393:573–80. doi: 10.1007/s00210-019-01751-x
24. Su Y, Morrison D, Ogle R. Chemical kinetics of calcium hypochlorite decomposition in aqueous solutions. J Chem Heal Saf. (2009) 16:21–5. doi: 10.1016/j.jchas.2008.07.002
25. Chaurasia V, Gupta A, Patel R, Chauhan S, Adichwal NK, Kamble S. Self-care, household cleaning and disinfection during COVID-19 pandemic: a study from Metropolitan Cities of India. Ann Data Sci. (2022) 9:1085–101. doi: 10.1007/s40745-022-00377-w
26. Al-Hanawi MK, Angawi K, Alshareef N, Qattan AMN, Helmy HZ, Abudawood Y, et al. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: a cross-sectional study. Front public Heal. (2020) 8:217. doi: 10.3389/fpubh.2020.00217
27. Taghrir MH, Borazjani R, Shiraly R. COVID-19 and Iranian medical students; a survey on their related-knowledge, preventive behaviors and risk perception. Arch Iran Med. (2020) 23:249–54. doi: 10.34172/aim.2020.06
28. Minhas S, Chaudhry RM, Sajjad A, Manzoor I, Masood A, Kashif M. Corona pandemic: awareness of health care providers in Pakistan. AIMS Public Heal. (2020) 7:548. doi: 10.3934/publichealth.2020044
29. Rintu KA, Prattay KMR, Sikdar KYK, Rahman T, Sarkar MR, Hossain T, et al. Cross-sectional study to evaluate people's knowledge, attitude and practice towards using disinfectants and sanitizers during COVID-19 pandemic in Bangladesh. Dhaka Univ J Pharm Sci. (2022) 21:117–26. doi: 10.3329/dujps.v21i2.63113
30. Kovacs DC, Small MJ, Davidson CI, Fischhoff B. Behavioral factors affecting exposure potential for household cleaning products. J Expo Anal Environ Epidemiol. (1997) 7:505–20.
31. Shouli MM, Elsayied HAE, Bsharat RM, Shouli KM. The extent of adherence to the precautionary measures among University students in palestine during COVID-19 pandemic. Am J Nurs. (2021) 10:270–8. doi: 10.11648/j.ajns.20211006.15
32. Cuan-Baltazar JY, Muñoz-Perez MJ, Robledo-Vega C, Pérez-Zepeda MF, Soto-Vega E. Misinformation of COVID-19 on the internet: infodemiology study. JMIR public Heal Surveill. (2020) 6:e18444. doi: 10.2196/18444
Keywords: COVID-19, awareness, performance, disinfectants, household cleaners, United Arab Emirates (UAE)
Citation: Alwan N, Almazrouei S, Almazrouei M, Aldhaheri J, Alismaili F and Ghach W (2023) Evaluation of public awareness and performance toward the safe use of household disinfectants-cleaners to prevent COVID-19 in the Emirate of Abu Dhabi. Front. Public Health 11:1214240. doi: 10.3389/fpubh.2023.1214240
Received: 03 May 2023; Accepted: 12 June 2023;
Published: 28 June 2023.
Edited by:
Maha M. Farid, Helwan University, EgyptReviewed by:
Marwa Abdelrahim, Assiut University, EgyptHebat Allah Ahmed Amin, Helwan University, Egypt
Copyright © 2023 Alwan, Almazrouei, Almazrouei, Aldhaheri, Alismaili and Ghach. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nisreen Alwan, bmlzcmVlbi5hbHdhbkBhZHUuYWMuYWU=; Wissam Ghach, d2lzc2FtLmdoYWNoQGN1ZC5hYy5hZQ==