
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 27 September 2023
Sec. Public Health Education and Promotion
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1212396
 Syed Muhammad Zeeshan Haider Hamdani1,2*†
Syed Muhammad Zeeshan Haider Hamdani1,2*† Jie Zhuang1*†
Jie Zhuang1*† Syed Ghufran Hadier2,3†
Syed Ghufran Hadier2,3† Haris Khurram4†
Haris Khurram4† Syed Danish Haider Hamdani2,5†Shaista Shireen Danish2Syeda Urooj Fatima2,6†
Syed Danish Haider Hamdani2,5†Shaista Shireen Danish2Syeda Urooj Fatima2,6† Wang Tian1
Wang Tian1Background: The decline in adolescent physical fitness is a significant global public health concern, and Pakistan is no exception. The country’s absence of a health-related physical fitness (HRPF) evaluation system has compounded this issue. To bridge this gap, this study aims to develop a scientifically-based HRPF evaluation system for the adolescent population that meets international standards. The evaluation system identifies at-risk children and improves adolescent health outcomes, including obesity, cardiovascular and musculoskeletal disorders, chronic diseases, and psychological illnesses, through crucial physical fitness evaluation. This study specifically aims to establish an HRPF evaluation system for school adolescents aged 12–16 in Pakistan.
Methods: A cross-sectional study was conducted among 2,970 school adolescents aged 12–16 years in the South Punjab, Pakistan. The study used a stratified sampling technique to select participants. The HRPF evaluation system included four components: cardiorespiratory endurance, core muscular endurance, muscular strength, and body composition. Data were collected through standardized tests and anthropometric measurements.
Results: The study’s results indicated that the HRPF evaluation scoring system was feasible and valid for evaluating the HRPF of school adolescents in the South Punjab region of Pakistan. The results of the evaluation system categorized participants into five groups based on their performance: excellent (6.2%), good (24.9%), medium (50.7%), poor (17%), and very poor (1.2%).
Conclusion: The study establishes an HRPF evaluation system for Pakistani school adolescents. This system lays the foundation for implementing effective strategies to improve their physical health. The findings offer valuable insights to policymakers, health professionals, and educators, enabling them to promote fitness and devise impactful interventions for enhancing HRPF in this population.
The rapid development of the economy, urbanization, and changes in modern life have contributed to the emergence of various diseases (1). One such disease is obesity, which is increasingly prevalent among adolescents worldwide (2). Additionally, global variations in human growth at different ages are essential to identifying the factors that contribute to this trend, including genetics, diet, physical activity (PA) levels, physical fitness (PF), and socioeconomic variables (3). The decline of adolescent PF has emerged as another global concern threatening human health (4). PF is a crucial indicator of an individual’s overall health. It is associated with a reduced risk of chronic diseases, such as cardiovascular disease, type 2 diabetes, and certain types of cancer (5). In the late 19th century, many nations began recognizing health-related physical fitness (HRPF) research as a critical indicator of an individual’s overall health and well-being (6. p4). Consequently, assessing PF and its relationship to health became a top priority for promoting the health of children and adolescents (7). As a result of the pressing health issues faced by adolescent populations, many countries placed great importance on HRPF research as a means of solving these problems (8).
Health-related physical fitness reference standards provide a way to measure and track changes in fitness levels over time and identify individuals at risk of health problems related to low PF (9). HRPF reference standards are essential for identifying and managing the impact of health problems related to physical inactivity and sedentary behavior (SB) among adolescents (10). Growth and PF reference standards identify at-risk individuals and can also be used to monitor the effectiveness of interventions to address these children and adolescents’ health issues, such as obesity (11, 12). Furthermore, reference standards of different anthropometric measures provide a benchmark for measuring changes in height, weight, and body mass index (BMI) over time, allowing for the identification of individuals at risk of health problems related to under or over-nutrition (13). HRPF reference standards are vital for research and clinical practice as they provide a standardized basis for diagnosing and managing growth disorders, such as short stature or delayed puberty. The reference standards also allow researchers to compare PF levels across different populations and identify existing disparities over time (14).
Researchers and policymakers are working to guide school-aged adolescents toward engaging in fitness activities based on scientifically-informed practices to promote overall health. This information can help in the development of effective health promotion and disease prevention programs, target high-risk populations, and monitor changes in health status over time (15). The measurement and evaluation of PF in adolescents have become a significant area of focus in sports science research as they provide valuable information about the current state of PF and health among adolescent populations (16). Adolescents are a critical population to monitor regarding PF and health, as this is a time of rapid physical and emotional development that can have a lasting impact on overall health and well-being (17, 18). PF evaluation systems for adolescents typically measure several vital components of physical fitness, including cardiovascular endurance, muscular strength and endurance, and body composition (19).
Over the years, numerous countries have conducted extensive theoretical and experimental research on HRPF among adolescents; these researchers have identified specific characteristics and trends in the field, including unique aspects of HRPF in adolescents that must be considered when developing appropriate measurement and evaluation tools (20). Despite these differences, there is a shared trend toward increasing scientific rigor and precision in the measure of HRPF in order to better guide and promote health among school-aged children. This trend underscores the importance of adopting a standardized and evidence-based approach to assessing HRPF, which can lead to more effective interventions and better health outcomes.
The need for HRPF evaluation systems is contingent upon various factors across different regions of the world, including regional variations in disease prevalence, cultural and socioeconomic influences, and access to healthcare (21). PF evaluation systems for adolescents serve various essential public health purposes in different regions. One important use of these systems is to monitor and identify disparities in health by comparing PF levels across other regions and demographic groups around the globe. By detecting disparities in health, PF evaluation systems can provide a basis for developing targeted public health interventions (22).
Moreover, PF evaluation systems are essential for developing health promotion programs; the information obtained from these systems can be used to design and evaluate programs to improve PF and reduce the risk of chronic diseases (23). The global burden of chronic diseases, including heart disease, diabetes, and obesity, is increasing, making it necessary to use PF evaluation systems to address this trend (24). These systems can play a vital role in assessing PF to reduce the global burden of chronic diseases by providing insight into risk factors and guiding the development of effective public health interventions.
The global prevalence of obesity, SB, physical inactivity, and low level of HRPF among adolescents, particularly in developing countries like Pakistan, is a complex health problem (25, 26). However, limited previous research has been found to focus on these health issues, with few studies examining PF, PA, and SB among adolescents in Pakistan (25, 27, 28). Furthermore, previous studies were limited by factors such as sample size, age differences, socioeconomic disparities, and other potential confounding variables that may affect the results (28, 29). Therefore, it is urgent to strengthen the research on the evaluation and measurement of the health-related physical fitness of adolescents in Pakistan.
Thus, the objective of this study is to establish a health-related physical fitness evaluation system of key health-related physical fitness indicators, including hand-grip strength (HG), modified pull-up (MPU), plank endurance (PE), and 20-m shuttle run (VO2max), among school adolescents aged 12–16 in the South Punjab region of Pakistan. This evaluation system will employ globally recognized assessment indices for anthropometric characteristics, obesity, and internal physiological mechanisms such as muscular strength, cardiovascular fitness, endurance, and cardiorespiratory fitness. By doing so, this study aims to address the gaps in the literature and provide a scientific and logical based comprehensive evaluation of the HRPF of adolescents in the South Punjab region.
The present cross-sectional study aimed to establish an evaluation system of health-related physical fitness indicators among adolescents in South Punjab, Pakistan. This study was conducted as part of the Young teen’s Assessment Active Lifestyle Involvement—PAKistan Study (YAALI-Pak) (28), which seeks to understand the lifestyle habits and associated health outcomes of Pakistani adolescents.
A panel of nine experts in sports science and physical education in Pakistan was invited to provide an opinion on the development process of the adolescent HRPF evaluation system for the South Punjab region. The panel offered consensus-based opinions on the inclusion of indicators and weightage for each measure, tailoring the evaluation system to the unique characteristics and needs of the region. The experts expressed satisfaction with the adherence to the protocols established by the WHO and CDC for conducting measurement methods and physiological tests (6, 14, 30). The HRPF evaluation system meets the highest standards for measuring and monitoring adolescent physical fitness in the region.
The researchers employed a stratified random sampling method to obtain a representative sample. The South Punjab region was used as the stratum and further divided into three sub-strata: Multan, Bahawalpur, and D.G. Khan. The majority of the populations of these stratums are a good representation of the Southern Punjab population. So, these areas/regions contain the representative population of South Punjab. From 360 higher schools in the region, 20 higher schools were randomly selected from each stratum using an equal allocation method, making up 16.67% (60 higher schools) of the total schools in the region. A general sample of 50 students from each school was taken/selected. The total sample size was 3,000, as shown in Table 1. Finally, 2,970 respondents were included in the study after removing non-responsive or incomplete respondents, which was about 1%.
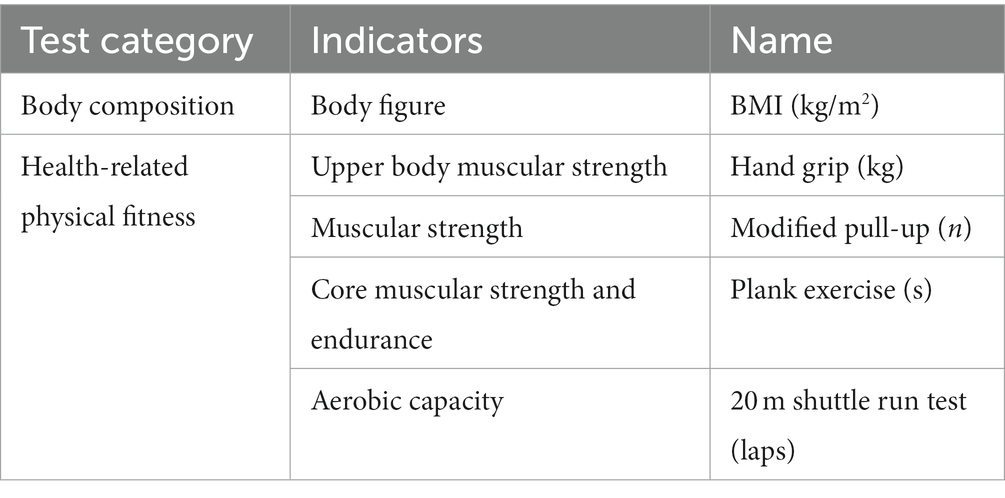
Table 1. List of indicators included in the health-related physical fitness evaluation system.
Moreover, the sample size power of the test was greater than 80%, and sample size calculators and formulas provide sample size at a 5% level of significance with a 95% precision level lower than this sample size (28, 31). The current study was conducted in south Punjab, including three divisions: Multan, Bahawalpur, and D. G. Khan. A total of 60 schools, with 20 schools from each division, participated in the study. The sample size included 3,000 participants aged between 12 and 16 years, with 50 students randomly selected from each school. The findings of this study can be generalized to the population of school-going adolescents aged 12–16 years in the South Punjab region. After removing 30 non-responsive participants, a total of 2,970 school adolescents (49.73% boys and 50.26% girls) were included in the final analysis. The majority of the populations of these stratums are a good representation of the Southern Punjab population. Only physically and mentally healthy adolescents with no prior injury record or intention to receive monetary compensation were included in the study. Workshops were conducted to inform relevant parties, including the school management, parents, test and measurement staff, and students, about the study project and testing procedures.
The Shanghai University of Sport’s School of Exercise and Health, along with its Ethics Advisory Committee, approved the research design and methodology in September 2018 the study approval number (1716516032). To uphold ethical standards, the study obtained written and verbal consent from relevant authorities, including educational authorities, school management, and parents, prior to conducting sampling and testing procedures. Data collection took place in 2019 after receiving approval from the education authorities. These precautions ensured the protection of participants and adherence to institutional regulations. The study adheres to all ethical standards and complies with the Declaration of Helsinki.
From the perspective of the development of the health-related physical fitness evaluation system, all national and international groups working on developing or implementing their evaluation system strive for consensus on how to interpret the concept of building and which evaluation indicators should be used for field-based tests. This study chose HRPF indicators like muscular strength, muscular endurance, and cardiorespiratory fitness among adolescents in Pakistan based on consultation with subject-matter experts and a thorough review of the aforementioned global trends in health-related physical fitness research. In order to create a scientific and systematized system for detecting HRPF, it is necessary to choose a specific number of indicators that can more truly reflect the fitness development characteristics of adolescents. This will allow each indicator to reflect a particular physical characteristic of a given age accurately. The following indicators were used in the current study to achieve the objectives mentioned above: body composition (BMI), muscle strength (Hand-grip/Modified pull-up), cardiopulmonary fitness (20-m shuttle run), and muscle endurance (Plank; Table 1).
The study followed a rigorous protocol for HRPF indicators, modeled according to the National Adolescents Fitness Survey (NYFS-2012) by the Centers for Disease Control and Prevention in the United States (32). To ensure the accuracy and consistency of the results, the subjects were given ample time to warm up before the physical fitness tests were conducted. Additionally, the students were advised to perform cool-down exercises after the tests to minimize the risk of any potential injuries. Detailed measurement procedures can be found in previous studies (28, 32).
Data were collected during the 2019 academic year across schools in the South Punjab Region, Pakistan. School visit schedules were formulated around school timetables. Two days prior to each visit, the test team communicated with school personnel to communicate test requirements (33). On the day of the visit, the researcher randomly chose students for data recording. Only these selected students constituted the study sample. The class teacher assured their presence for subsequent visits (34).
The testing procedure spanned 3 consecutive days at each school during regular hours:
Anthropometric data were gathered, including height, weight, and specific body measurements (32). A plank exercise was also conducted for core muscular endurance (33). Later, participants filled out the International Physical Activity Questionnaire (short form).
Physical fitness tests measuring strength, like handgrip strength and modified pull-ups were conducted (34).
Tests assessing aerobic capacity, such as the Shuttle Run Test (20 m), performed (28).
To ensure engaged participation, the research team interspersed fun activities amidst the tests (34).
Before each physical test, participants underwent a 10-min standard warm-up consisting of light aerobic exercises and dynamic stretches to prepare their bodies. Post-test, a 5-min cool-down of slow walking and static stretches was advised to minimize injury risks (32).
The individuals’ anthropometric characteristics were measured per the procedures outlined in the literature. The measurements were taken while the individuals were barefoot and wearing lightweight clothing to prevent inaccurate readings. Height was measured using a height-measuring scale, and weight was measured using a portable digital weight machine. Body mass index (BMI) was then calculated using height and weight values (32).
Health-related physical fitness indicators are important because they provide a measurement of an individual’s physical health and ability to perform physical tasks. To assess these indicators (cardiovascular endurance, cardiorespiratory fitness, muscular strength, and endurance), one should choose a specific test for each consistent and effective indicator in a particular research environment. As part of the YAALI-PAK study, detailed information regarding measurement tools and test procedures has already been published (28).
The Plank exercise is an isometric test to evaluate the muscles’ endurance in the body’s core region (33). Test Method: To perform the Plank test, the participant assumes a prone position with their elbows bent, shoulders and elbows perpendicular to the ground, and feet on the ground. They lift their body off the ground, keeping their trunk straight and tightening their abdominal and pelvic floor muscles. The tester times the duration of the hold with a stopwatch, and the test ends if the participant deviates from the standard position. The recorded time in seconds is then reported to the recorder.
Grip strength is a commonly used measure of upper limb muscle strength and reflects an adolescent’s level of upper limb development (34). The GRIPX Digital Hand Dynamometer Grip Strength Measurement is a standard device used to measure hand-grip strength in this study. Before testing, the handle distance is adjusted to the palm size using the handle adjustment knob. During testing, the subject stands with feet naturally separated, shoulders adducted, and arms neutrally rotated, with arms naturally opened 30 degrees’ parallel to the body interface but not touching it. The subject is instructed to squeeze the handle for 3–5 s, and the numeric result is displayed on the device’s LCD screen and recorded by the recorder.
The Modified Pull-Up (MPU) test is a hanging strength assessment used to measure muscular strength in the body, particularly in the back muscles. The test involves using a modified horizontal bar and a gymnastics mat. The bar is adjusted to an appropriate height and positioned on a flat surface, and a nylon strap hangs 8 in down from the center of the bar. During the test, the participant hooks the bar with an overhand grip of both hands, palms facing away from the body, and keeps their body straight with arms at a 90-degree angle to the trunk. The participant then bends their arms to make their chin touch or exceed the crossbar and straightens their arms to recover. The number of correctly completed pull-ups is recorded, and the test ends when the participant pauses for two or more seconds, cannot maintain the correct position, or requests to stop. Scores are based on the number of correctly completed pull-ups.
The Shuttle Run Test 20 m assessed the participants’ aerobic capacity by measuring the time to run back and forth across a marked 20 m track while keeping up with the beeps at increasing speeds. The test began at a speed of 8.0 km/h and increased by 0.5 km/h each minute. Participants were required to cross the finish line before the beep sounded, and failure to do so twice resulted in disqualification. The recorder recorded the completed laps as the final result.
The chosen methods and tests ensure a holistic assessment of adolescent health and fitness (28). They were selected for their precision, reliability, and alignment with established standards in adolescent health research (32).
The present study comprehensively analyzed the adolescent population’s anthropometric and health-related physical fitness indicators. Descriptive analysis and inferential statistics were calculated, such as percentages, frequencies, mean, and standard deviation. To obtain normative reference values and LMS curves using the Lambda (λ), Mu (μ), and Sigma (σ) methods (35). The LMS method was applied using R statistical software version 3.0.2 to generate LMS curves for age-specific and gender-specific indicators. The normative reference values obtained through the LMS method were used to draw indexes for individual health-related physical fitness indicators. The back substitution test approach was applied to ensure the standard’s cross-validation and applicability. The study used a consensus-based approach to establish indicators and their weightage for a comprehensive evaluation system of health-related physical fitness in adolescents aged 12–16. The experts’ input led to criteria for both genders, resulting in practical and relevant evaluation. Incorporating scientific principles and methods in this study enhances its credibility and applicability.
Table 2 shows the population’s age and gender-specific demographic descriptive analysis. The current study testified a total of 2,970 participants aged 12–16 years’ school adolescents. Boys and girls were distributed equally as 1,477 (49.7%) and 1,493 (50.3%). Further, around 20% of the population was distributed from each age group with each gender.
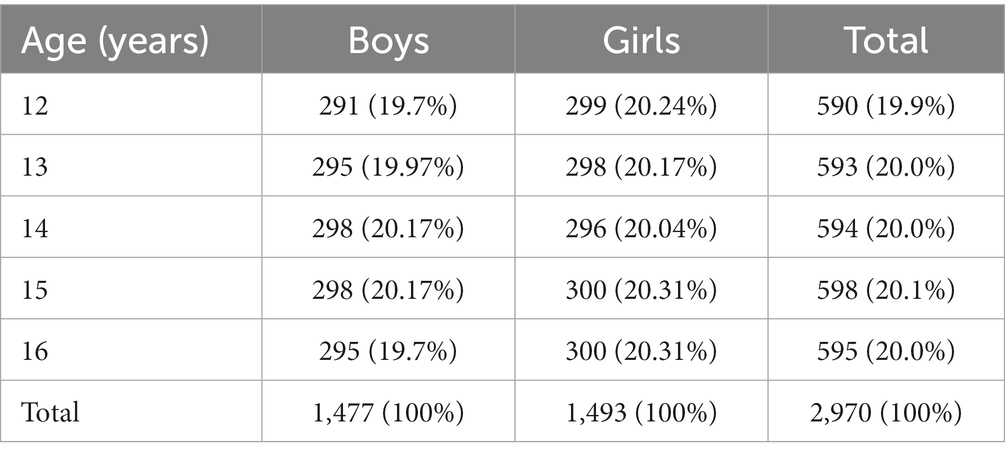
Table 2. Age and gender-specific frequency analysis N (%).
After numerous adjustments and verifications, the current study used the LMS method to develop reference values and percentile curves for adolescents of different ages. The obtained reference values and percentile curves for both boys and girls are presented in Table 3 and Figure 1. The median (P50th) centiles for body mass index (BMI) in boys and girls aged 12–16 years ranged from 16.59 to 17.48 and 15.71 to 16.81, respectively. The median (P50th) BMI for boys increased by 0.89, while for girls, it increased by 1.1. After analyzing the trend and variation of BMI in boys and girls showed a negligible change over the course of 1 year (approximately). Overall, male participants had higher BMI percentile values compared to female participants.
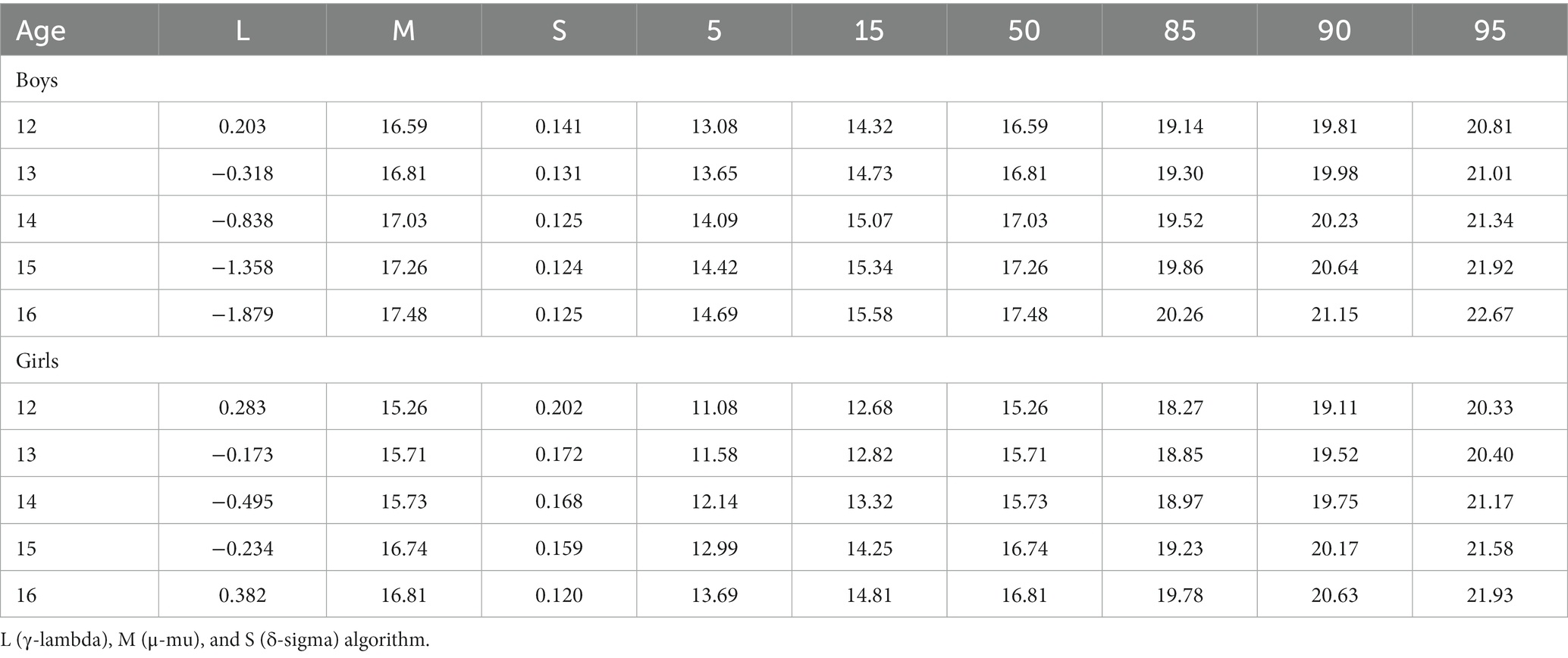
Table 3. Age and gender-specific BMI percentile generated by the LMS method.

Figure 1. BMI (kg/m2) smoothed percentile curves for South Punjab (A) Boys and (B) Girls.
Additionally, the study employed the LMS method to establish reference values and percentile curves for hand-grip strength in adolescents of both genders. After several adjustments and verifications, the study obtained the hand-grip strength values for boys and girls of different ages, presented in Table 4 and Figure 2. The Smoothed LMS curves (for the 3rd, 10th, 35th, 50th, 65th, and 90th centiles) for the hand-grip strength of boys and girls are also shown in Figure 2, while the corresponding numerical data are provided in Table 4. The results indicate that boys have better hand-grip strength test scores than girls across all age groups, as evidenced by the centiles. The 50th centile value for hand-grip strength for boys and girls ranges from 22.53 to 35.47 and 13.12 to 20.18 kg, respectively.
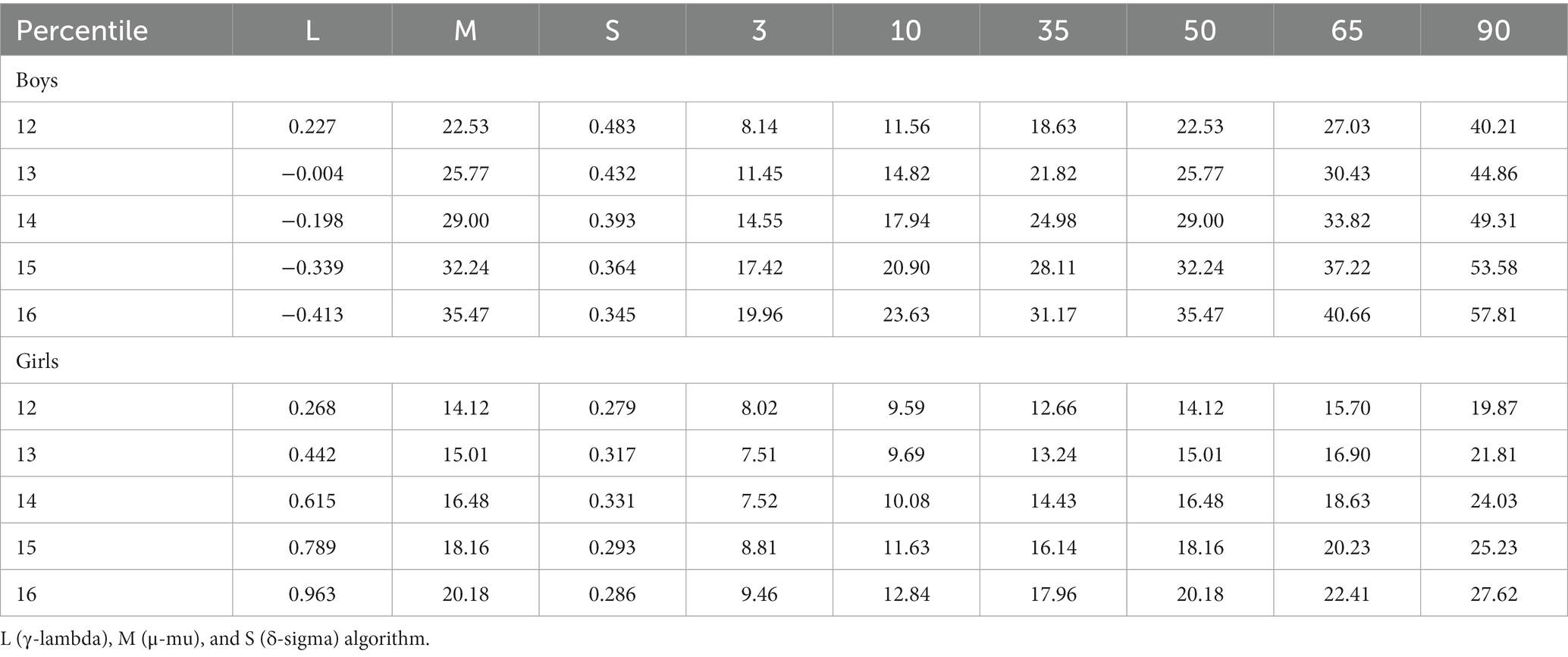
Table 4. Hand grip indicators men and women P 50th measured value.
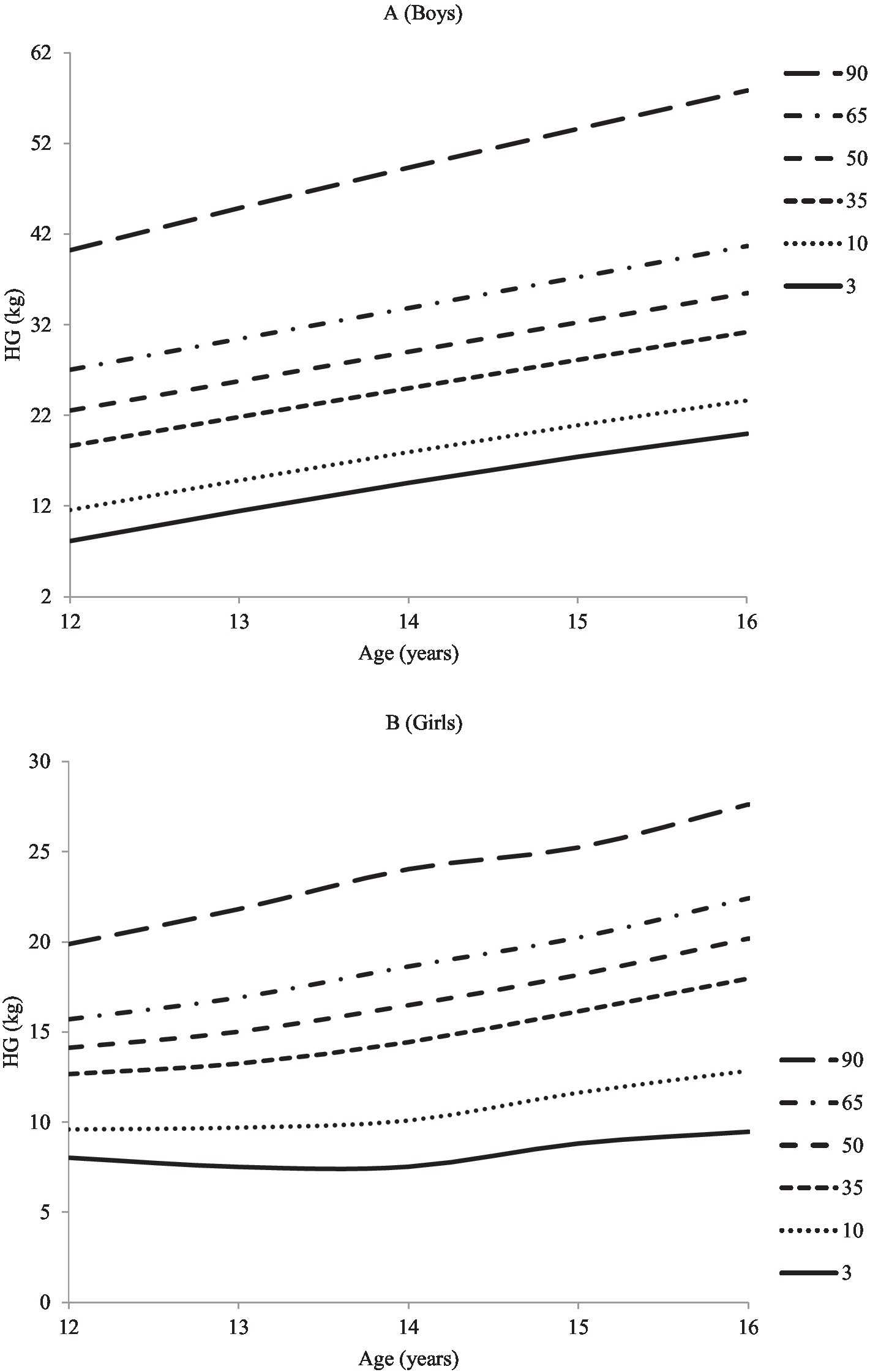
Figure 2. Hand grip strength (kg) percentile curve for the adolescents (A) Boys and (B) Girls.
Additionally, an average annual increase of approximately 3–5 kg was observed in boys and girls. The study also found that muscle strength increases with age in both boys and girls, with a marked increase between the ages of 14 and 15. Overall, the results presented in Table 4 indicate that boys have a higher hand-grip strength percentile than girls.
The back substitution test is a crucial step in evaluating the cross-validation of an evaluation system. This study involves randomly extracting a small data set from a larger one to assess the consistency between the fitted and actual values. In our study, we used the LMS method to establish reference norms for HRPF indicators and identify the absolute mean error rate by comparing the p50 values of the large (actual value) and small (fitted values). The back substitution process assessed the degree of coincidence between data sets generated using a random sampling method to test the cross-validation of the standard. By conducting the back substitution test, we ensured that a lower error rate indicated higher accuracy for our evaluation system. In this study, we employed back substitution and evaluated one index from the body shape and health-related physical fitness indicator. This back-substitution approach ensured the standard was based on valid scientific principles, increasing its credibility and applicability.
Table 5 presents an example of the back substitution test used to determine body composition indicators. This process involves adopting the 50th percentile of the BMI fitted value and comparing it to the actual value in the data. The results show that the absolute difference between the actual and fitted values of each age group is generally within the allowable mean absolute error rate of the measurement. This finding indicates that the actual and fitted values of absolute mean error is within an acceptable range across the 12 to the 16-year-old age group for both genders.
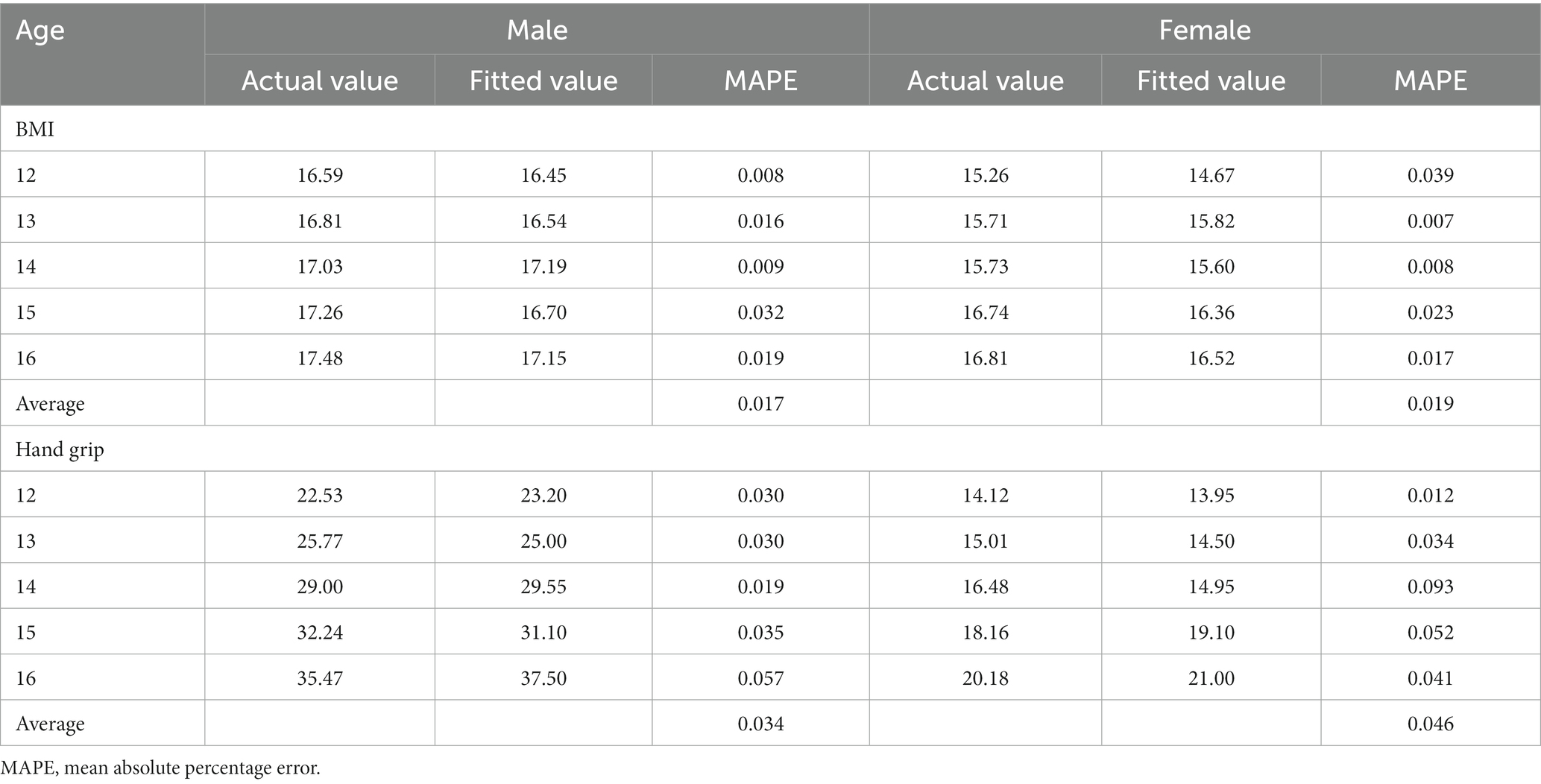
Table 5. Back substitution test of BMI, Hand grip age, and gender-specific comparison of P 50th measured value with the fitted value (kg).
The current study aimed to evaluate the health-related physical fitness of adolescents by establishing a normative standard using the LMS method and cross-validating the standard through a back substitution test to provide individual indicator indexes for our HRPF evaluation system.
In this study, the percentile method was adopted to formulate and constitute the rating standard for the evaluation system. This method was chosen due to the normal distribution of the samples for the two categories of indicators: anthropometric characteristics (BMI) and HRPF indicators. This approach allows for the appropriate interpretation and comparison of the results within the context of a normal distribution.
This study describes the index cut-off points for the five-level scoring system used in the current evaluation system. The evaluation of individual indicators utilizes a five-point scale, with scores ranging from 1 to 5. A score of 1 indicates poor performance, while a score of 5 indicates excellent performance. This five-grade classification method is utilized to determine an indicator’s relative position within the context of the entire age and gender group of the evaluated individuals. A higher score indicates better performance on a particular indicator. The scores for each indicator for both male and female ages specifically serve as the evaluation standard for that specific indicator.
After establishing LMS normative reference standard, the five-point index scoring standards are interpreted as follows: Index of anthropometric characteristics BMI categories “1 lean, obese: [≤P5, ≥ P95], 3 over-weight: [P85, P95), 5 normal weight: [P5, P85).” 1 represents a poor performance within P3–P10, 2 represents a below-average performance within P10–P35, 3 represents an average performance with in P35–P65, 4 represents a good performance within P65–P90, and 5 represents an excellent performance more than ≥P90. “1 Very Poor: [P3, P10], 2 Poor: [P10, P35), 3 Medium: [P35, P65), 4 Good: [P65, P90), 5 Excellent: ≥ P90.” This study has set a minimum limit line for individual score categories of HRPF indicators. If the test value is lower than the third percentile, no score will be given to encourage people to truly exercise their abilities in the test. No minimum line is set for the body shape test. Considering the characteristics of HRPF indicators in actual use.
The growth and development of adolescents are key indicators of their overall health status during this critical developmental period. One of the most visible manifestations of adolescent growth and development is the change in BMI concerning age. The results of the age and gender-specific BMI measurements are presented in Table 6. This information allows for the assessment of the adolescent’s growth and development status, as well as the identification of any potential health concerns.
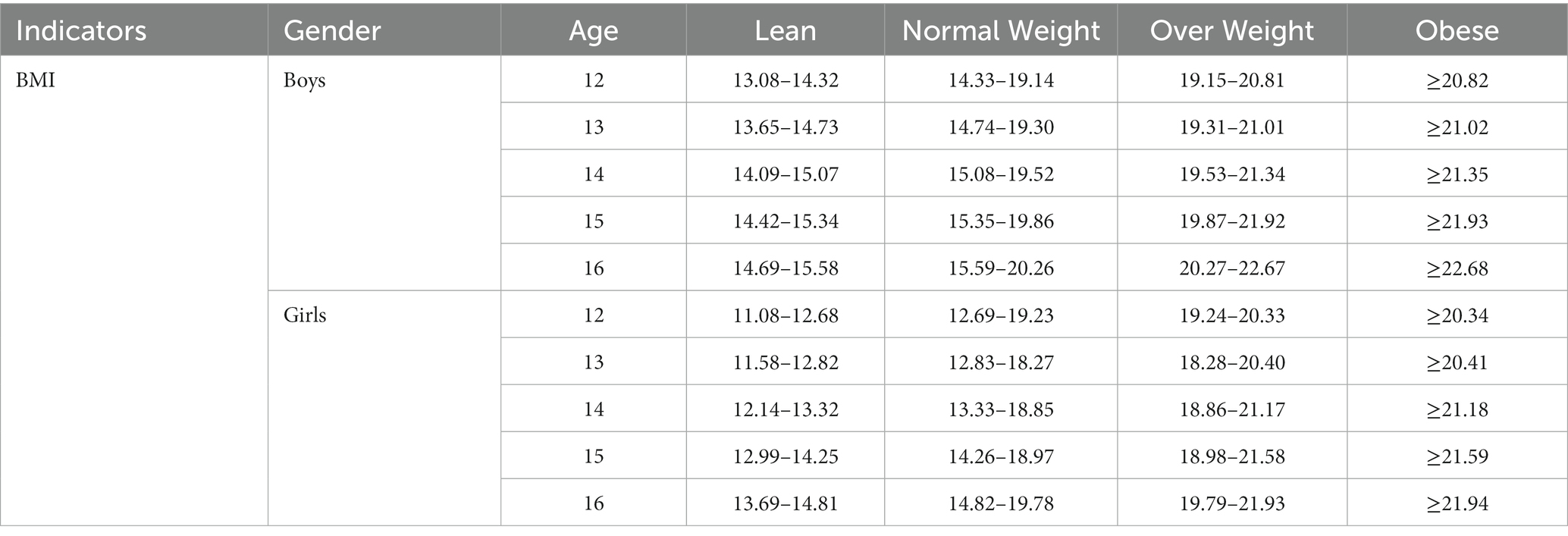
Table 6. Index for BMI age and gender-specific according to the single indicator evaluation standard.
The current study has selected the hand grip strength and the modified pull-up test to evaluate adolescents’ muscular strength effectively. These primary indicators have been chosen for their relevance and accuracy in assessing muscular strength. The results of these evaluations are presented in Table 7, providing a comprehensive understanding of the age and gender-specific range Scores for hand grip and modified pull-up test for the adolescents of south Punjab region Pakistan.
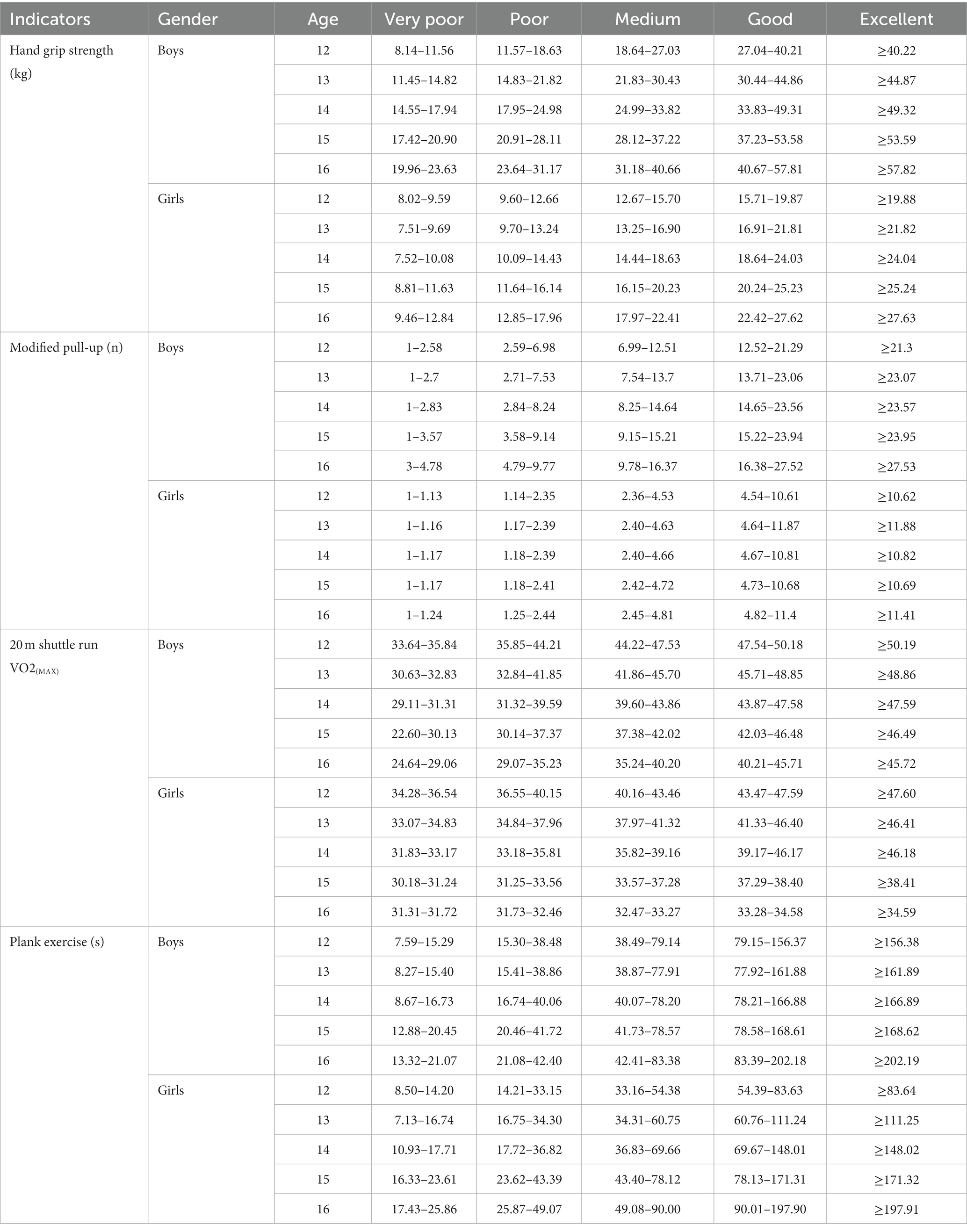
Table 7. Indexes for HRPF indicators age and gender-specific according to the single indicator evaluation standard.
The results of these evaluations, specifically those related to the 20 m shuttle run test, are presented in Table 7. This study provides extensive evidence to understand the adolescent’s cardiorespiratory fitness/aerobic capacity and allows for the identification of any potential areas of concern. The Plank exercise test was utilized to assess the level of muscular endurance in study participants. The findings of these assessments are outlined in Table 7, which presents a comprehensive analysis of the range of scores specific to age and gender, offering a deeper insight into the results of the Plank test. Table 7 describes indexes for HRPF indicators age and gender-specific according to single indicator evaluation standard range/scores for the 20 m shuttle run, hand grip, modified pull up, and plank for adolescents. As per the criteria, the single index system scoring classification method evaluation presents the hand grip, modified pull-up, plank exercise, and 20-m shuttle run test’s indexes (scores/cut-off) values for cardiovascular endurance/cardiorespiratory fitness, muscular strength, and muscular endurance.
A comprehensive indicator system for assessing the growth and development of adolescents has been established (Figure 3) taking into account the nature of growth and development among the adolescent population of south Punjab’s region Pakistan, as well as the desirability, quantification, and representativeness of the indicators. Expert opinion was utilized to evaluate each indicator’s rationality and validity. The evaluation grade is divided into five categories: very reasonable, reasonable, basically reasonable, unreasonable, and very unreasonable, with scores of 1–5, respectively. Table 8 presents the statistical results of the expert evaluation. This approach ensures the selection of appropriate and relevant indicators for the assessment of adolescent growth and development. It allows for the identification of any potential areas of improvement in the indicator system.
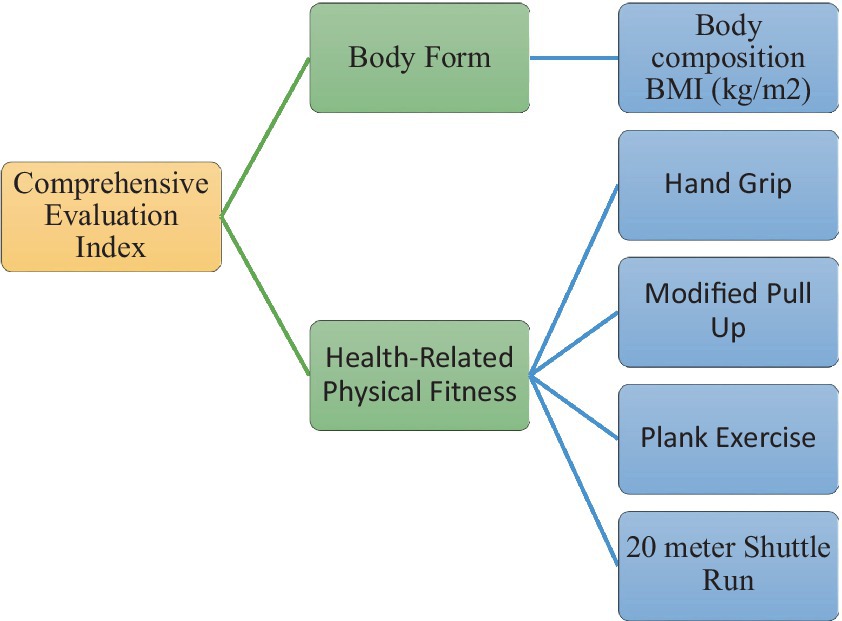
Figure 3. Comprehensive evaluation index system for school adolescents.
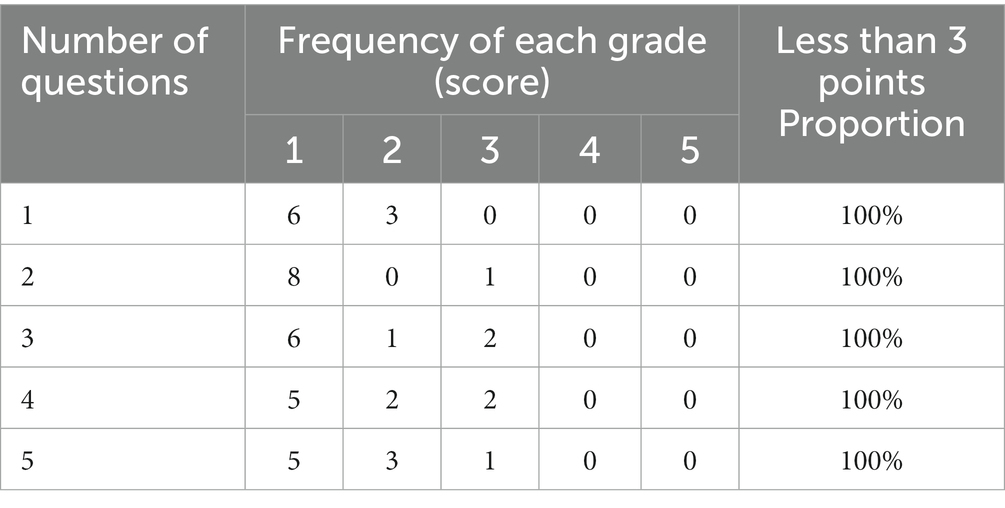
Table 8. Inclusion statistics of rationality of each index in the HRPF evaluation system.
In the process of further analysis method can be used to assess the relative importance of indicators by forming A judgment matrix (Cij) based on the five scales of relative importance. The matrix Cij represents the relative importance of indicator Ci compared to indicator Cj for a specific level. By using a judgment matrix to measure the importance of indicators, it is possible to conduct a systematic and comprehensive analysis to determine the relative importance of each indicator for the specific level. This approach allows for the identification of key indicators that have the greatest impact on the level and guides decision-making on which indicators to prioritize in the evaluation process.
The calculation process of indicator weight is as follows: build a judgment matrix Cij. Tables 9, 10 show from the evaluation results that the experts’ recognition of the health-related physical fitness indicator of adolescents reflected by their anthropometric characteristics (BMI) and HRPF has reached 100%, indicating that it is reasonable to choose BMI and HRPF indicators (HG, MPU, and PE and 20 m shuttle run test) as the first level indicators of the evaluation system of south Punjab region’s adolescents. Our results 100% of the experts believe it is reasonable to choose the body composition to reflect the body shape/anthropometric characteristics and HRPF indicators to reflect the overall health and fitness. The reasonableness of four secondary indicators of HRPF, including hand grip, modified pull-up, plank and 20 m shuttle run test, is relatively recognized, and the proportion of basically satisfied in each question (100%) is highly reasonable. At the same time, the experts have a good command of the hand grip, modified pull-up, plank, and 20 m shuttle run test.
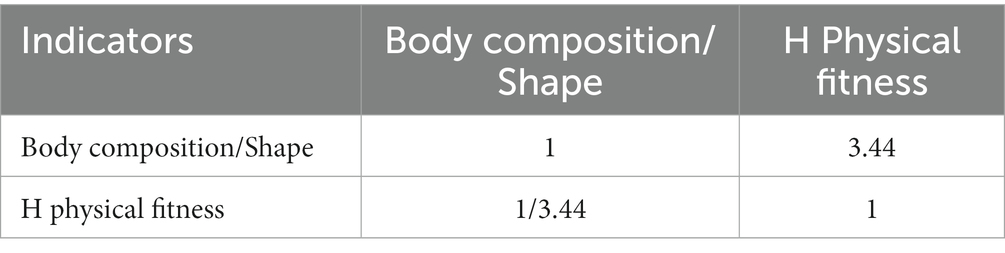
Table 9. Comprehensive evaluation index judgment.
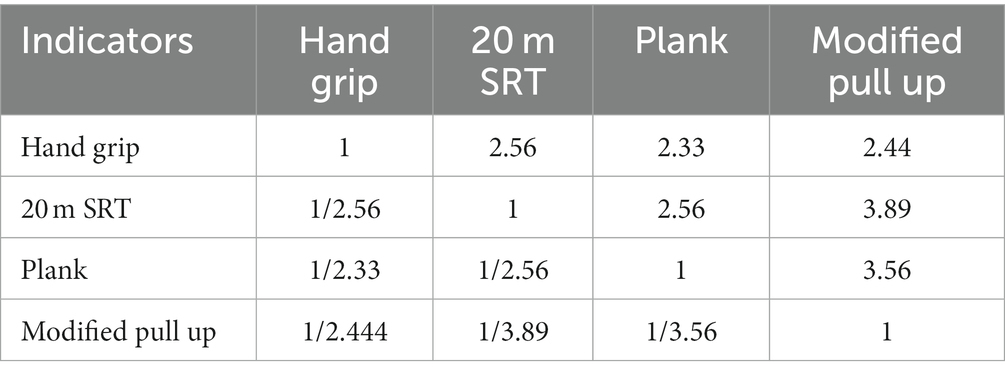
Table 10. Judgment matrix of health-related physical fitness indicators index.
According to the relative importance of each indicator, and the size of its impact on HRPF and role, determine their respective weight in the comprehensive evaluation system. Table 10 shows the Judgment Matrix of the HRPF index. The weight of each index is calculated according to the importance judgment matrix.
Table 11 shows the judgment matrix of comprehensive evaluation indicators and physical fitness indicators, respectively. According to the expert’s judgment Value of Index Importance statistic opinion analysis, all the indicators of health-related physical fitness and BMI were given weight in the evaluation system. Wherein, Equations (1) and (2) are weight calculation equations, and equations (3, 4) are weight logic error tests. The consistency test indexes are all less than 0.1, so it can be considered that the above matrices have good consistency.
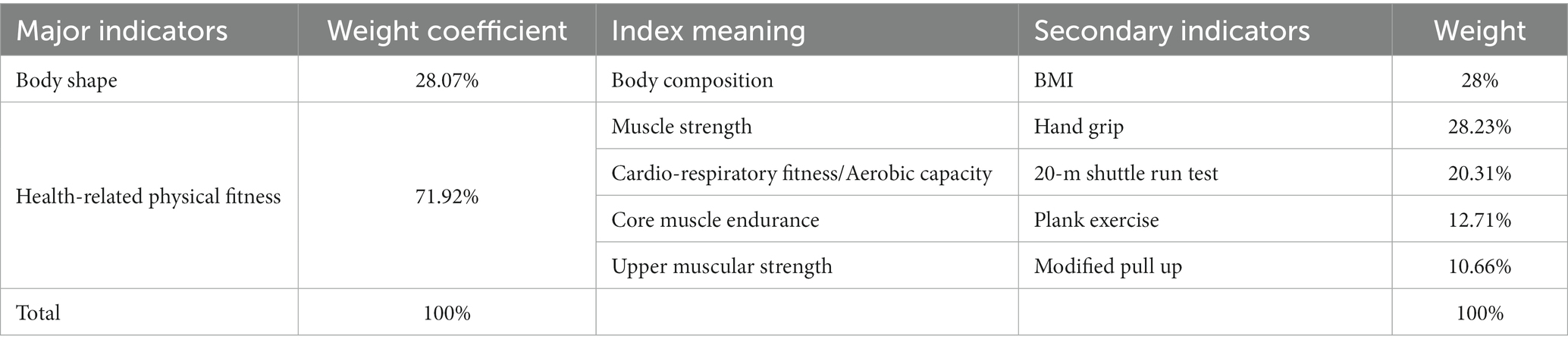
Table 11. Weight of each evaluation index in the evaluation index system.
The formula is as follows:
The researcher made adjustments based on expert questionnaire suggestions, and the final weight of each indicator is shown in Table 11. According to the expert’s judgment Value of Index Importance statistic opinion analysis, all the indicators of health-related physical fitness and BMI were given weight by using above mention equation in the evaluation system as hand grip 28.23%, modified pull up 10.66%, plank 12.71%, 20 m shuttle run test 20.31%, and BMI 28.07% (Table 11). We compared the importance and unimportance of the indicators at the same level in the comprehensive evaluation system of adolescents according to their importance in the system and score.
The scoring standards for all indicators of adolescents in all age groups serve as the foundation for comprehensive evaluation. The final evaluation is determined by calculating the total score of all indicators based on the weights assigned to each indicator. This approach allows for a comprehensive assessment of the overall health status of adolescents by taking into account the various indicators that reflect different aspects of adolescent growth and development. The weighting system ensures that the most important indicators have the greatest impact on the final evaluation.
Example: The evaluation system was applied to a sample of 12-year-old male students, Wang. The results showed that the system effectively categorized their HRPF level based on their performance in the different physical fitness tests. Specifically, using the equation (1 × 0.2807 + 3 × 0.2031 + 2 × 0.2823 + 3 × 0.1066 + 4 × 0.1231), we calculated the total score for each participant, and the results were compared with Table 12 to determine their HRPF category. For instance, student Wang scored 2.247, indicating poor HRPF and placing him in the second category of the evaluation system. These findings demonstrate the potential of the proposed comprehensive evaluation system for monitoring and improving individual HRPF.
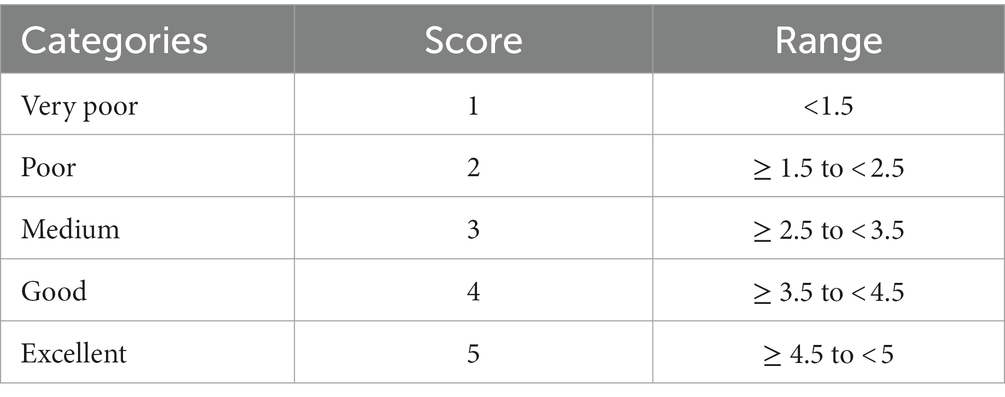
Table 12. Comprehensive rating criteria age and gender-specific score.
The evaluation process is divided into five grades: excellent grade, good grade, medium grade, poor grade, and very poor grade. The final evaluation grade is determined by calculating the total score of all indicators, considering the weight assigned to each indicator. Any indicator with no score will not be considered in the comprehensive evaluation. This approach ensures that only complete and accurate data is used in the evaluation process and eliminates any potential bias that may be introduced by missing data (Table 12). Comprehensive Rating Criteria score very poor, poor, medium, good, and excellent.
This study provides a health-related physical fitness evaluation system for adolescents in the South Punjab region of Pakistan. This evaluation system is categorized into five levels: very poor, pass, medium, good, and excellent. The HRPF evaluation system was used to assess the physical fitness level of the participants, where 17% of adolescents were categorized as poor, while 1.2% had a very poor HRPF level. About 50.7% of the adolescents had a medium HRPF level, and 24.9% were evaluated as good, whereas only 6.2% of the participants were classified as excellent.
The evaluation system generates age and gender-specific HRPF individual indexes, offering detailed research evidence to initiate effective strategies for improving the health of adolescents. These indexes provide an overview of adolescents’ HRPF levels, which can aid in developing appropriate intervention strategies for enhancing their physical fitness.
It is the first time any information has been published on the evaluation system for adolescents’ health-related physical fitness in the south Punjab region of Pakistan. To the best of our knowledge, this is the first article to precisely examine HRPF indicator assessment with these indicators and tools in Pakistan. Although our study evaluated the physical fitness of adolescents in school settings, which may not be as accurate as laboratory tests with an epidemiological approach, assessments conducted in more experimental settings could provide a more realistic representation of real-world performance. Physical fitness, which is commonly understood as the basic ability of the human body to perform physical activity, is a reflection of the functions of various organ systems in relation to muscle work. Childhood and adolescence are crucial periods for the development of muscle strength, speed, and endurance. As such, the physical fitness evaluation during this time typically focuses on these key aspects to assess overall fitness and identify any areas of weakness or deficiency that may require further attention or intervention.
Muscular strength is a crucial component of HRPF that is often overlooked. Adolescents, in particular, must pay attention to their muscular strength levels to ensure healthy growth and development (20). Muscular strength plays a vital role in maintaining overall physical fitness and improving quality of life. Adolescents with adequate muscle strength are better able to perform daily activities and maintain good health. According to research, muscular strength positively correlates with physical performance and endurance (36). Strong muscles enable adolescents to engage in physical activities that require physical effort, such as playing sports, carrying heavy bags, and running long distances (37). In addition, adequate muscular strength helps to improve bone density and prevent the onset of chronic diseases such as osteoporosis (38). Studies show that physical activity, including resistance training, positively impacts bone mineral density (39). Adolescents who engage in regular physical activity that includes resistance training have an increased chance of maintaining strong bones throughout their lives.
Furthermore, muscular strength also plays a vital role in preventing obesity and reducing the risk of metabolic disorders such as diabetes (40). Adequate muscle mass and strength increase the body’s metabolic rate, which leads to the burning of more calories at rest. As a result, adolescents who have adequate muscle strength are less likely to become overweight or obese. The result of this study enables the identification of any potential areas of concern regarding their muscular strength, aiding in the development of targeted interventions to improve their overall health and well-being.
Assessing cardiorespiratory fitness/aerobic capacity is crucial to evaluating adolescents’ physical development and strength (41, 42). In selecting indicators for assessing cardiorespiratory fitness/aerobic capacity in adolescents, it is important to consider the overall development of the human body system and the ability to assess cardiorespiratory fitness/aerobic capacity during both rest and exercise. To this end, maximum oxygen uptake has been chosen as the primary indicator for effectively evaluating adolescents’ cardiorespiratory fitness/aerobic capacity. Cardiovascular fitness measures the body’s ability to use oxygen during physical activity. It is considered an important aspect of overall physical fitness, particularly among adolescents. Adolescence is a crucial development period during which physical, cognitive, and emotional changes occur. Adequate cardiorespiratory fitness is important for adolescents to be able to participate in physical activities, sports, and other forms of physical exertion without experiencing fatigue or shortness of breath. It also helps to improve their overall health and well-being. Adequate cardiovascular fitness is associated with a lower risk of cardiovascular diseases like hypertension, stroke, and heart disease (43, 44). Adolescents with ample cardiovascular fitness have a better physical function, including improved endurance and energy levels, allowing them to participate in physical activities and sports easily (45). Additionally, better cardiovascular fitness tends to have better mental health and academic performance, including a lower risk of depression and anxiety and improved concentration and cognitive function, respectively (46, 47).
Muscular endurance is one of the important components of health-related physical fitness, which refers to the ability of muscles to exert force repeatedly or sustain a contraction for an extended period (48). It plays a crucial role in maintaining good health and overall fitness, particularly among adolescents at a stage of growth and development. The plank test is one of the commonly used measures of muscular endurance that can be used to assess and monitor the fitness level of adolescents (33, 49, 50). The plank test is a simple and effective method of assessing the muscular endurance of the core muscles, including the rectus abdominis, transverse abdominis, and erector spinae muscles (51, 52). The plank test has several benefits in assessing muscular endurance among adolescents. It is a quick and easy test that does not require special equipment or expensive technology, making it accessible to individuals of all fitness levels (51, 52). It is a safe and non-invasive method of assessing fitness, as it does not involve strenuous or potentially harmful exercises. The plank exercise test is an objective and reliable measure of muscular endurance that quantifies how much time an individual can hold the plank position. It can help identify individuals at risk of developing musculoskeletal problems due to poor core stability, such as lower back pain or postural abnormalities (53, 54). It can motivate adolescents to improve their fitness level and overall health by setting achievable goals for increasing their plank time (27, 55). Lastly, the plank test can help to promote good posture and balance, which are important for preventing falls and maintaining proper body alignment (56). The period of adolescence presents an opportune time for the development of muscular endurance due to the heightened excitability of the cerebral cortex and the adaptability of neural processes. Table 8 shows the health-related physical fitness evaluation system individual indexes age-specific and gender-specific for adolescents in the South Punjab region of Pakistan. This evaluation system is categorized into five levels: very poor, pass, medium, good, and excellent. The results of the HRPF evaluation system was used to assess the physical fitness level of the participants, where 17% of adolescents were categorized as poor, while 1.2% had a very poor HRPF level. About 50.7% of the adolescents had a medium HRPF level, and 24.9% were evaluated as good, whereas only 6.2% of the participants were classified as excellent. This data provide an overview of the HRPF level of adolescents in the region and can be useful for developing appropriate intervention strategies to improve the physical fitness of this population.
Additionally, adolescents in this age range may lack knowledge and coordination when participating in HRPF assessments. It is also worth noting that the flexibility component of HRPF was not included in this study, following the United States committee on fitness measurement and health outcomes in the adolescent recommendation, which concluded that the relationship between flexibility and health was unclear due to the lack of scientific literature (57). Therefore, flexibility was not considered in the current study.
Although our study evaluated the physical fitness of adolescents in school settings, which may not be as accurate as laboratory tests with an epidemiological approach, assessments conducted in more experimental settings could provide a more realistic representation of real-world performance.
This study successfully developed a foremost systematic health-related physical fitness evaluation system to assess the health of adolescents in the South Punjab region of Pakistan. The study filled a research gap by providing an evaluation system for HRPF in Pakistan. This study also established the index of two primary indicators, BMI and four HRPF indicators. The weight coefficients were determined by the opinion of the experts for both the primary and secondary level indicators, resulting in a comprehensive evaluation standard. This system provides precise age and gender-specific HRPF assessments, identifying potential areas of concern. With the application of this evidence, effective interventions can be designed to address these health issues. Therefore, this study contributes significantly to the academic literature and is a valuable tool for public health professionals in promoting the health and well-being of adolescents in Pakistan.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by The Ethics Advisory Committee of the School of Exercise and Health at the Shanghai University of Sport. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
SMZHH and JZ contributed to conception and design of the study. SMZHH, SGH, SDHH, SD, and SF organized the database. SMZHH and HK performed the statistical analysis. SMZHH wrote the first draft of the manuscript. All authors contributed to the article and approved the submitted version.
The researcher acknowledged the administrative and technical support of the Education Department and the volunteers involved during data collection. Researchers also acknowledge that students participated in the study for academic purposes.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Miranda, JJ, Barrientos-Gutiérrez, T, Corvalan, C, Hyder, AA, Lazo-Porras, M, Oni, T, et al. Understanding the rise of cardiometabolic diseases in low-and middle-income countries. Nat Med. (2019) 25:1667–79. doi: 10.1038/s41591-019-0644-7
2. Swinburn, BA, Kraak, VI, Allender, S, Atkins, VJ, Baker, PI, Bogard, JR, et al. The global Syndemic of obesity, undernutrition, and climate change: the lancet commission report. Lancet. (2019) 393:791–846. doi: 10.1016/S0140-6736(18)32822-8
3. El Shafie, AM, El-Gendy, FM, Allahony, DM, Hegran, HH, Omar, ZA, Samir, MA, et al. Development of LMS and Z score growth references for Egyptian children from birth up to 5 years. Front Pediatr. (2021) 8:598499. doi: 10.3389/fped.2020.598499
4. Kohl, H III, Murray, T, and Salvo, D. Foundations of Physical Activity and Public Health. Champaign, IL: Human Kinetics Publishers (2019).
5. World Health Organization Global recommendations on physical activity for health. (2010). World Health Organization.
6. Medicine, ACOS. ACSM's Health-Related Physical Fitness Assessment Manual. Philadelphia, PA: Lippincott Williams & Wilkins (2013).
7. Shi, C, Chen, S, Wang, L, Yan, J, Liang, K, Hong, J, et al. Associations of sport participation, muscle-strengthening exercise and active commuting with self-reported physical fitness in school-aged children. Front Public Health. (2022) 10:873141. doi: 10.3389/fpubh.2022.873141
8. Fatusi, AO, and Hindin, MJ. Adolescents and youth in developing countries: health and development issues in context. J Adolesc. (2010) 33:499–508. doi: 10.1016/j.adolescence.2010.05.019
9. Hobold, E, Pires-Lopes, V, Gómez-Campos, R, de Arruda, M, Andruske, CL, Pacheco-Carrillo, J, et al. Reference standards to assess physical fitness of children and adolescents of Brazil: an approach to the students of the Lake Itaipú region—Brazil. PeerJ. (2017) 5:e4032. doi: 10.7717/peerj.4032
10. Cadenas-Sanchez, C, Intemann, T, Labayen, I, Peinado, AB, Vidal-Conti, J, Sanchis-Moysi, J, et al. Physical fitness reference standards for preschool children: the PREFIT project. J Sci Med Sport. (2019) 22:430–7. doi: 10.1016/j.jsams.2018.09.227
11. Hendrey, G, Holland, AE, Mentiplay, BF, Clark, RA, and Williams, G. Do trials of resistance training to improve mobility after stroke adhere to the American College of Sports Medicine guidelines? A systematic review. Arch Phys Med Rehabil. (2018) 99:584–597.e13. doi: 10.1016/j.apmr.2017.06.021
12. de Onis, M, Onyango, AW, Borghi, E, Siyam, A, Nishida, C, and Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. (2007) 85:660–7. doi: 10.2471/BLT.07.043497
13. Hardwick, SA, Deveson, IW, and Mercer, TR. Reference standards for next-generation sequencing. Nat Rev Genet. (2017) 18:473–84. doi: 10.1038/nrg.2017.44
14. World Health Organization WHO child growth standards: Length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and development. (2006). World Health Organization.
15. Fan, C. The physical health evaluation of adolescent students based on big data. Mob Inf Syst. (2021) 2021:2356869. doi: 10.1155/2021/2356869
16. Lang, JJ, Zhang, K, Agostinis-Sobrinho, C, Andersen, LB, Basterfield, L, Berglind, D, et al. Top 10 international priorities for physical fitness research and surveillance among children and adolescents: a twin-panel Delphi study. Sports Med. (2023) 53:549–64. doi: 10.1007/s40279-022-01752-6
17. Kumar, B, Robinson, R, and Till, S. Physical activity and health in adolescence. Clin Med. (2015) 15:267–72. doi: 10.7861/clinmedicine.15-3-267
18. Hoyt, LT, Chase-Lansdale, PL, McDade, TW, and Adam, EK. Positive youth, healthy adults: does positive well-being in adolescence predict better perceived health and fewer risky health behaviors in young adulthood? J Adolesc Health. (2012) 50:66–73. doi: 10.1016/j.jadohealth.2011.05.002
19. Kabiri, LS, Messineo, A, Gattu, N, Ray, BD, and Iammarino, NK. Health-related physical fitness and activity in homeschool: a systematic review with implications for return to public school. J Sch Health. (2021) 91:948–58. doi: 10.1111/josh.13080
20. Fühner, T, Kliegl, R, Arntz, F, Kriemler, S, and Granacher, U. An update on secular trends in physical fitness of children and adolescents from 1972 to 2015: a systematic review. Sports Med. (2021) 51:303–20. doi: 10.1007/s40279-020-01373-x
21. Keating, XD, Stephenson, R, Liu, X, and Colburn, J. Cross-cultural comparison of youth fitness testing in China and the US: an ecological systems model approach. ICHPER-SD J Res. (2019) 10:20–7.
22. Kriemler, S, Meyer, U, Martin, E, van Sluijs, EMF, Andersen, LB, and Martin, BW. Effect of school-based interventions on physical activity and fitness in children and adolescents: a review of reviews and systematic update. Br J Sports Med. (2011) 45:923–30. doi: 10.1136/bjsports-2011-090186
23. Flynn, MAT, McNeil, DA, Maloff, B, Mutasingwa, D, Wu, M, Ford, C, et al. Reducing obesity and related chronic disease risk in children and youth: a synthesis of evidence with ‘best practice’ recommendations. Obes Rev. (2006) 7:7–66. doi: 10.1111/j.1467-789X.2006.00242.x
24. Bauer, UE, Briss, PA, Goodman, RA, and Bowman, BA. Prevention of chronic disease in the 21st century: elimination of the leading preventable causes of premature death and disability in the USA. Lancet. (2014) 384:45–52. doi: 10.1016/S0140-6736(14)60648-6
25. Laar, RA, Shi, S, Ashraf, MA, Khan, MN, Bibi, J, and Liu, Y. Impact of physical activity on challenging obesity in Pakistan: a knowledge, attitude, and practice (KAP) study. Int J Environ Res Public Health. (2020) 17:7802. doi: 10.3390/ijerph17217802
26. Ullah, I, Islam, MS, Ali, S, Jamil, H, Tahir, MJ, Arsh, A, et al. Insufficient physical activity and sedentary behaviors among medical students during the COVID-19 lockdown: findings from a cross-sectional study in Pakistan. Int J Environ Res Public Health. (2021) 18:10257. doi: 10.3390/ijerph181910257
27. Liu, Y, Hadier, SG, Liu, L, Hamdani, SMZH, Hamdani, SD, Danish, SS, et al. Assessment of the relationship between body weight status and physical Literacy in 8 to 12 year old Pakistani school children: the PAK-IPPL cross-sectional study. Child Aust. (2023) 10:363. doi: 10.3390/children10020363
28. Hamdani, SMZH, Jie, Z, Hadier, SG, Tian, W, Hamdani, SDH, Danish, SS, et al. Relationship between moderate-to-vigorous physical activity with health-related physical fitness indicators among Pakistani school adolescents: Yaali-Pak study. ScientificWorldJournal. (2022) 2022:6402028. doi: 10.1155/2022/6402028
29. Imtiaz, A, ulHaq, Z, Afaq, S, Khan, MN, and Gillani, B. Prevalence and patterns of physical activity among school aged adolescents in Pakistan: a systematic review and meta-analysis. Int J Adolesc Youth. (2020) 25:1036–57. doi: 10.1080/02673843.2020.1831559
30. Fakhouri, T.H.I. (2014). Physical activity in US youth aged 12–15 years, 2012. US Department of Health and Human Services, centers for disease control.
31. Suresh, K, and Chandrashekara, S. Sample size estimation and power analysis for clinical research studies. J Hum Reprod Sci. (2012) 5:7–13. doi: 10.4103/0974-1208.97779
32. CDC. Anthropometry procedures manual. United States: CDC. (2017). Available at: https://wwwn.cdc.gov/nchs/data/nhanes/2017-2018/manuals/2017_Anthropometry_Procedures_Manual.pdf (Accessed December 14, 2021).
33. Hamdani, SMZH, Zhuang, J, Hadier, G, Tian, W, Hamdani, SDH, Shireen, S, et al. Normative reference standard for CORE muscular endurance of adolescent 12-16 years from South Punjab Pakistan: a cross-sectional study. Pak J Physiol. (2022) 18:3–8.
34. Hamdani, SMZH, Zhuang, J, Tian, W, and Hadier, SG. Normative reference standard for handgrip strength among adolescent students in South Punjab Pakistan: a cross-sectional study. J Bus Soc Rev Emerg Econ. (2021) 7:997–1009. doi: 10.26710/jbsee.v7i4.2064
35. Cole, TJ. The LMS method for constructing normalized growth standards. Eur J Clin Nutr. (1990) 44:45–60.
36. Moran, J, Sandercock, G, Ramirez-Campillo, R, Clark, CCT, Fernandes, JFT, and Drury, B. A Meta-analysis of resistance training in female youth: its effect on muscular strength, and shortcomings in the literature. Sports Med. (2018) 48:1661–71. doi: 10.1007/s40279-018-0914-4
37. Britton, U, Issartel, J, Symonds, J, and Belton, S. What keeps them physically active? Predicting physical activity, motor competence, health-related fitness, and perceived competence in Irish adolescents after the transition from primary to second-level school. Int J Environ Res Public Health. (2020) 17:2874. doi: 10.3390/ijerph17082874
38. Alvarez-Pitti, J, Casajús-Mallén, JA, Leis-Trabazo, R, Lucía, A, López de Lara, D, Moreno-Aznar, LA, et al. Exercise as medicine in chronic diseases during childhood and adolescence. Anal Pediatr. (2020) 92:173.e1–8. doi: 10.1016/j.anpedi.2020.01.010
39. Zago, M, Capodaglio, P, Ferrario, C, Tarabini, M, and Galli, M. Whole-body vibration training in obese subjects: a systematic review. PLoS One. (2018) 13:e0202866. doi: 10.1371/journal.pone.0202866
40. Carbone, S, del Buono, MG, Ozemek, C, and Lavie, CJ. Obesity, risk of diabetes and role of physical activity, exercise training and cardiorespiratory fitness. Prog Cardiovasc Dis. (2019) 62:327–33. doi: 10.1016/j.pcad.2019.08.004
41. Ruiz, JR, Castro-Pinero, J, Espana-Romero, V, Artero, EG, Ortega, FB, Cuenca, MM, et al. Field-based fitness assessment in young people: the ALPHA health-related fitness test battery for children and adolescents. Br J Sports Med. (2011) 45:518–24. doi: 10.1136/bjsm.2010.075341
42. Ortega, FB, Ruiz, JR, Castillo, MJ, and Sjöström, M. Physical fitness in childhood and adolescence: a powerful marker of health. Int J Obes. (2008) 32:1–11. doi: 10.1038/sj.ijo.0803774
43. Lee, I-M, Shiroma, EJ, Lobelo, F, Puska, P, Blair, SN, Katzmarzyk, PT, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. (2012) 380:219–29. doi: 10.1016/S0140-6736(12)61031-9
44. Warburton, DER, Nicol, CW, and Bredin, SSD. Health benefits of physical activity: the evidence. CMAJ. (2006) 174:801–9. doi: 10.1503/cmaj.051351
45. Landry, BW, and Driscoll, SW. Physical activity in children and adolescents. PM&R. (2012) 4:826–32. doi: 10.1016/j.pmrj.2012.09.585
46. Biddle, SJH, and Asare, M. Physical activity and mental health in children and adolescents: a review of reviews. Br J Sports Med. (2011) 45:886–95. doi: 10.1136/bjsports-2011-090185
47. Donnelly, JE, and Lambourne, K. Classroom-based physical activity, cognition, and academic achievement. Prev Med. (2011) 52:S36–42. doi: 10.1016/j.ypmed.2011.01.021
48. Hussain, A, and Khandekar, G. Comparative study of health related physical fitness among physical education students and non-physical education students belongs to South Kashmir. Int J Yogic Hum Mov Sports Sci. (2019) 4:776–8.
49. Imai, A, and Kaneoka, K. The relationship between trunk endurance plank tests and athletic performance tests in adolescent soccer players. Int J Sports Phys Therap. (2016) 11:718–24.
50. Fraser, BJ, Rollo, S, Sampson, M, Magnussen, CG, Lang, JJ, Tremblay, MS, et al. Health-related criterion-referenced cut-points for musculoskeletal fitness among youth: a systematic review. Sports Med. (2021) 51:2629–46. doi: 10.1007/s40279-021-01524-8
51. Tong, TK, Wu, S, and Nie, J. Sport-specific endurance plank test for evaluation of global core muscle function. Phys Ther Sport. (2014) 15:58–63. doi: 10.1016/j.ptsp.2013.03.003
52. Lee, J, Jeong, K, Lee, H, Shin, J, Choi, J, Kang, S, et al. Comparison of three different surface plank exercises on core muscle activity. Phys Therap Rehab Sci. (2016) 5:29–33. doi: 10.14474/ptrs.2016.5.1.29
53. Sadler, SG, Spink, MJ, Ho, A, de Jonge, XJ, and Chuter, VH. Restriction in lateral bending range of motion, lumbar lordosis, and hamstring flexibility predicts the development of low back pain: a systematic review of prospective cohort studies. BMC Musculoskelet Disord. (2017) 18:179. doi: 10.1186/s12891-017-1534-0
54. Standaert, CJ, Herring, SA, and Pratt, TW. Rehabilitation of the athlete with low back pain. Curr Sports Med Rep. (2004) 3:35–40. doi: 10.1249/00149619-200402000-00007
55. Ha, AS, Lonsdale, C, Lubans, DR, and Ng, JYY. Increasing students’ physical activity during school physical education: rationale and protocol for the SELF-FIT cluster randomized controlled trial. BMC Public Health. (2017) 18:11. doi: 10.1186/s12889-017-4553-8
56. Tompsett, C, Burkett, B, and McKean, MR. Development of physical LITERACY and movement competency: a literature review. J Fitness Res. (2014) 3:53–7.
Keywords: physiological testing, cardiorespiratory fitness, muscle strength, public health, evaluation system, protocol and measurement method
Citation: Hamdani SMZH, Zhuang J, Hadier SG, Khurram H, Hamdani SDH, Danish SS, Fatima SU and Tian W (2023) Establishment of health related physical fitness evaluation system for school adolescents aged 12–16 in Pakistan: a cross-sectional study. Front. Public Health. 11:1212396. doi: 10.3389/fpubh.2023.1212396
Edited by:
Lotte Vallentin-Holbech, Aarhus University, DenmarkReviewed by:
Dartagnan Pinto Guedes, North University of Paraná, BrazilCopyright © 2023 Hamdani, Zhuang, Hadier, Khurram, Hamdani, Danish, Fatima and Tian. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Syed Muhammad Zeeshan Haider Hamdani, c3llZGhhbWRhbmlwaGRAZ21haWwuY29t; emVlc2hhbmhhbWRhbmlAYnp1LmVkdS5waw==; Jie Zhuang, emh1YW5namllQHN1cy5lZHUuY24=
†ORCID: Syed Muhammad Zeeshan Haider Hamdani, https://orcid.org/0000-0001-7632-0869
Jie Zhuang, https://orcid.org/0000-0002-2442-7418
Syed Ghufran Hadier, https://orcid.org/0000-0001-5164-5886
Haris Khurram, https://orcid.org/0000-0003-1814-4742
Syed Danish Haider Hamdani, https://orcid.org/0009-0002-3320-4678
Syeda Urooj Fatima, https://orcid.org/0000-0003-2009-4326
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.