 Thi-Phuong-Lan Nguyen1*
Thi-Phuong-Lan Nguyen1* M. Rifqi Rokhman2,3
M. Rifqi Rokhman2,3 Imre Stiensma4
Imre Stiensma4 Rachmadianti Sukma Hanifa4
Rachmadianti Sukma Hanifa4 The Due Ong5
The Due Ong5 Maarten J. Postma4,6,7
Maarten J. Postma4,6,7 Jurjen van der Schans4,8,9
Jurjen van der Schans4,8,9- 1Faculty of Public Health, Thai Nguyen University of Medicine and Pharmacy, Thái Nguyên, Vietnam
- 2Unit of Global Health, Department of Health Sciences, University Medical Center Groningen, Groningen, Netherlands
- 3Faculty of Pharmacy, Universitas Gadjah Mada, Groningen, Indonesia
- 4Unit of Global Health, Department of Health Sciences, University of Groningen, University Medical Center Groningen, Groningen, Netherlands
- 5Department of Health Financing and Health Technology Assessment, Health Strategy and Policy Institute, Hanoi, Vietnam
- 6Centre of Excellence in Higher Education for Pharmaceutical Care Innovation, Universitas Padjadjaran, Bandung, Indonesia
- 7Department of Economics, Econometrics, and Finance, University of Groningen, Groningen, Netherlands
- 8Department of Economics, Econometrics and Finance, Faculty of Economics and Business, University of Groningen, Groningen, Netherlands
- 9Faculty of Management Sciences, Open University, Heerlen, Netherlands
Background: Cost-effectiveness analyses (CEAs) on prevention of non-communicable diseases (NCDs) are necessary to guide decision makers to allocate scarce healthcare resource, especially in Southeast Asia (SEA), where many low- and middle-income countries (LMICs) are in the process of scaling-up preventive interventions. This scoping review aims to summarize the cost-effectiveness evidence of primary, secondary, or tertiary prevention of type 2 diabetes mellitus (T2DM) and cardiovascular diseases (CVDs) as well as of major NCDs risk factors in SEA.
Methods: A scoping review was done following the PRISMA checklist for Scoping Reviews. Systematic searches were performed on Cochrane Library, EconLit, PubMed, and Web of Science to identify CEAs which focused on primary, secondary, or tertiary prevention of T2DM, CVDs and major NCDs risk factors with the focus on primary health-care facilities and clinics and conducted in SEA LMICs. Risks of bias of included studies was assessed using the Consensus of Health Economic Criteria list.
Results: This study included 42 CEAs. The interventions ranged from screening and targeting specific groups for T2DM and CVDs to smoking cessation programs, discouragement of smoking or unhealthy diet through taxation, or health education. Most CEAs were model-based and compared to a do-nothing scenario. In CEAs related to tobacco use prevention, the cost-effectiveness of tax increase was confirmed in all related CEAs. Unhealthy diet prevention, mass media campaigns, salt-reduction strategies, and tax increases on sugar-sweetened beverages were shown to be cost-effective in several settings. CVD prevention and treatment of hypertension were found to be the most cost-effective interventions. Regarding T2DM prevention, all assessed screening strategies were cost-effective or even cost-saving, and a few strategies to prevent T2DM complications were found to be cost-effective in certain settings.
Conclusion: This review shows that the cost-effectiveness of preventive strategies in SEA against T2DM, CVDs, and their major NCDs risk factors are heterogenous in both methodology as well as outcome. This review combined with the WHO “best buys” could guide LMICs in SEA in possible interventions to be considered for implementation and upscaling. However, updated and country-specific information is needed to further assess the prioritization of the different healthcare interventions.
Systematic review registration: https://osf.io, identifier: 10.17605/OSF.IO/NPEHT.
1. Introduction
Non-communicable diseases (NCDs) such as type 2 diabetes mellitus (T2DM), cardiovascular diseases (CVDs), cancer, and chronic respiratory diseases are the leading causes of death worldwide and therefore constitute an important global health problem (1). Through the past century, the burden of NCDs was concentrated in developed countries, but in recent years, their incidence, burden, and mortality in low- and middle-income countries (LMICs) have escalated (2–5). Globally, NCDs are responsible for more than 40 million lives lost per year in LMICs, accounting for roughly three quarters of global mortality (6). The United Nations (UN) has responded to this situation by prioritizing the reduction of the burden of NCDs as part of the Sustainable Development Goals (7).
In Southeast Asia (SEA), NCDs such as CVDs or T2DM are emerging as a major and growing burden for the public health sector and the economy. CVDs were the leading cause of death in SEA in 2019 (8). Their crude mortality rate in SEA countries, such as Vietnam, Indonesia or Myanmar, was about 300 per 100, 000 populations in 2019 (8). According to the International Diabetes Federation, there are ~90 million Southeast Asians with diabetes (2). From 2019 to 2045, the number of people with diabetes is expected to increase by over 70% in SEA, compared to only 51% globally (9). Consequently, the economic costs of CVDs, diabetes mellitus and associated complications in SEA will increase correspondingly (10).
Diabetes and CVDs are preventable through controlling modifiable behavioral risk factors (for example by managing tobacco use, physical inactivity, unhealthy diet and alcohol consumption), managing metabolic risk factors (such as hypertension, hyperlipidemia) (11) or early treatment. Therefore, in several SEA countries, national policies or regional programs for the primary (prevention of disease occurrence), secondary (early detection of disease), and tertiary (prevention of disease complications) prevention of NCDs are emerging. However, adequate evidence concerning the cost-effectiveness of the regional interventions is absent, since only a very limited number of rigorous evaluations have been done.
In order to tackle the rising costs of NCDs in SEA, the challenge for decision-makers in healthcare is to implement effective interventions at the lowest possible cost and to find the most cost-effective intervention(s) to combat specific diseases. Cost-effectiveness analysis (CEA) is a helpful tool to prioritize health interventions that will yield the greatest benefits under restricted budgets. This information is essential for SEA countries as most of them are in the process of scaling-up interventions in the course of the “Global strategy for the prevention and control of non-communicable diseases,” which was adopted by the World Health Assembly in 2000 (12).
Therefore, this study aims to review the cost-effectiveness of interventions aimed at primary, secondary and tertiary prevention in LMICs in SEA, that focus on T2DM and CVDs by providing screening and prevention of the main risk factors through targeting people at risk for specific diseases, or who already have those diseases.
2. Methods
We provide a review of CEAs of implemented interventions that ranged from prevention and behavior change to screening, diagnostic and care and medical treatment. Interventions had to focus on T2DM and CVDs and the risk factors associated with those diseases, including behavioral risk factors (smoking, alcohol consumption, physical inactivity, and unhealthy diets) and metabolic risk factors (hypertension, hyperlipidemia). The Preferred Reporting Items for Systematic reviews and Meta-Analyses for Scoping Review (PRISMA-ScR) statement was followed for this review (13).
The selection of studies followed the PICO: population: any population within the SEA and must be a low- and middle-income country; Intervention: interventions on type 2 diabetes, cardiovascular diseases and the risk factors associated with those diseases, including behavioral risk factors and metabolic risk factors; Comparator: no limitation on comparator; and Outcome: incremental cost-effectiveness ratio (ICER) or reported both costs and effects. The protocol of this scoping review was registered on the Open Science Framework with the document number 10.17605/OSF.IO/NPEHT.
2.1. Search strategy
The search was conducted using the databases Cochrane Library, EconLit, PubMed, and Web of Science, for articles published between 01/01/2000 and 30/01/2023. The following search terms were used in combination and modified according to the requirements of the specific database: (T2DM, CVDs and major risk factors) AND (South-East Asia) AND [(community) or (primary healthcare)] and [(intervention) or (evaluation)] AND [(effectiveness) or (cost-effectiveness)]. A detailed example of the complete search terms is presented in Supplementary Document 1.
The titles and abstracts were screened independently by three researchers (TPL Nguyen, JvdS, MRR) to decide on the relevance of each study, and assessed according to predefined inclusion and exclusion criteria (see below). Discrepancies on the inclusion of articles were resolved through discussion followed by mutual consensus between the three researchers to reach a final decision. Next, relevant studies were retrieved in full text and reviewed by the same three researchers. All references of the included articles were scanned for the identification of further articles.
2.2. In- and exclusion criteria
We included CEA which focused on primary, secondary, or tertiary prevention of diabetes and CVDs and major risk factors; interventions implemented at primary health-care facilities and clinics as well as at various sites within communities, schools, work sites, and individual homes in a LMIC in SEA. In terms of design, CEA had to be done either in trial-based or model-based design. We excluded CEAs conducted in Singapore, since Singapore is a high-income country in SEA (14). The classification of countries by income is based on the system provided by the UN, which categorizes countries into different income groups based on their Gross National Income per capita. Given the native and learned languages of the research team, studies written in a language that was not English, Burmese, Indonesian or Vietnamese, and studies which were not written as a full original research article in a peer-reviewed journal were also excluded.
2.3. Data extraction
Data extraction of each included article was done independently by two researchers, using a custom-made data extraction form in Excel. Discrepancies between the two researchers on the data extraction were resolved through discussion followed by mutual consensus between researchers to reach a final decision. If no consensus was reached, a third author was consulted. The following variables were extracted: disease indication/risk factor, type of intervention, country, design, method, intervention, comparator, population, time horizon, discount rate, currency (reference year), incremental quality-adjusted life years (QALYs)/ life years gained/disability-adjusted life years (DALYs) averted, cost of intervention, cost of the comparator, average cost-effectiveness ratio (ACER), and incremental cost-effectiveness ratio (ICER). If necessary, data were calculated based on the available information provided in the article.
2.4. Risk of bias
We assessed the risk of bias by rating each of the included studies using the Consensus of Health Economic Criteria (CHEC)-list (15). The evaluation was conducted by two independent researchers and any disagreement was resolved by the researchers together.
3. Results
In our scoping review, we included 42 CEAs comparing one or more interventions (Figure 1), consisting of individual interventions, community-based interventions, and/or population-based interventions. The interventions ranged from screening and targeting specific groups of the population for CVD (16–30) and T2DM (high-risk) individuals (16, 31–41) to smoking cessation programs (42–47); or discouragement of smoking or an unhealthy diet through taxation (38, 39, 42, 46, 48–51); or health education (16, 20, 46, 49–52) (Figure 2). We found no CEA that focused on the harmful use of alcohol or physical inactivity.
Figure 1. Study selection process.
Figure 2. Classification of interventions.
Almost all studies were based on a cost-effectiveness decision modeling analysis in which a combination of input parameter sources or extrapolation was used to compare the cost-effectiveness of the different interventions. The remaining studies only estimated costs and effects of interventions based on one study (34, 41). Furthermore, the evaluated studies were conducted in single countries (Thailand, Malaysia, Vietnam, Philippines, Indonesia, Myanmar and Cambodia), except the study by Webb conducted in 183 nations which included 3 countries in LMICs in SEA (52).
Table 1 provides an overview of the characteristics and design of each selected study. Most of the studies compared the interventions with a do-nothing scenario, i.e., the cost and health benefits in the absence of the proposed intervention. Furthermore, the minimum of a 10-year implementation horizon was considered in the majority of the studies selected, except for a few studies: Priyadi et al. (34) conducted an observational study over 4 years, Aziz et al. (25) conducted an RCT over 6 months, Satyana et al. (44) modeled participants aged 15–54 years and followed them until 55 years old (44), Hnit et al. (41) only measured one time screening (41), and Nguyen-Thi et al. (40) conducted a modeling study over 5 years (40). In almost all studies, future costs and health benefits were discounted according to the suggested 3% rate, except in the study of Cheng and Estrada (48), which discounted at 7% and in the study of Satyana et al. (44), which discounted at 5%. Four studies did not mention the discount rate at all (25, 32, 39, 54), while the studies by Hnit et al. (41) and Priyadi et al. (34) did not apply discounting. The model-based studies covered interventions in Indonesia, Vietnam, Thailand, the Philippines, Cambodia, Myanmar, and Malaysia.
Table 1. Design of costs and effects; cost-effectiveness studies focused on screening, prevention, and/or treatment of diabetes, CVDs or related risk factors.
3.1. Cost-effectiveness of interventions on main modifiable behavior risk factors for NCDs
3.1.1. Tobacco use
Studied interventions focused on the prevention of tobacco use by means of increasing the price of tobacco products or tax, making tobacco packaging less appealing, banning the marketing of tobacco products, creating a smoke-free environment, eliminating exposure to second-hand tobacco smoke, smoking cessation programs, and mass media campaigns on the harm of tobacco (Table 2).
Table 2. Results of costs and effects; cost-effectiveness studies focused on the prevention of tobacco use.
All reviewed studies addressing these interventions confirmed that a tax increase on tobacco products would be cost-effective in the SEA population (46, 48, 50, 53). Higashi et al. (53) concluded that graphic warning labels on cigarette packs would be the most cost-effective option, followed by a tax increase on tobacco products and mass media campaigns to educate about tobacco harm. Furthermore, Nguyen et al. (46) identified that offering smoking cessation services, banning advertising, promotion and sponsoring, and creating smoke-free environments are cost-effective. Ha and Chisholm (20) also concluded that media campaigns against smoking would be very cost-effective in the Vietnamese population (20).
Seven studies assessed the economic and health impact of smoking cessation programs in the SEA setting (42–47, 50). Three of them considered brief advice by a physician and counseling in hospital to be cost-effective (42, 45, 47). However, the study in Vietnam (42) found no cost-effectiveness of physician brief advice compared with pharmaceutical aids, while another study in the Thailand context found the combination of counseling and pharmaceuticals to be cost-effective (45). In the study of Thavorn and Chaiyakunapruk (47) in Thailand, a structured community pharmacist-based smoking cessation program was cost-saving and health gaining compared to usual care.
Moreover, two studies analyzed an intervention that was not considered in the WHO “best buys,” concerning a smoking ban enforced either in public or at work (50, 53). In Indonesia, the smoking ban was dominant compared to the current situation (50). Studies by Tan et al. (43) in Malaysia and Satyana et al. (44) concluded that optimization of smoking cessation programs among those of working age was potentially cost saving in the long term. Yet, these studies did not introduce specific interventions, but based the analysis on assumptions comparing smokers and never-smokers (43, 44). Although smoking cessation was also proven to be cost-effective in the Vietnamese population, the effect was less cost-effective compared to graphic packaging warning labels and taxation of tobacco products (53).
3.1.2. Unhealthy diet
The reduction of sodium/salt intake was recognized as one of the important interventions to control blood pressure and manage CVD events. These salt intake reductions are established by setting a target salt level in foods, providing lower sodium options, communication and media campaigns focused on reducing salt intake or raising awareness through labeling, and setting up a national policy that combines government-industry agreements, government monitoring and public education (20, 49, 51, 52). The reduction of cholesterol levels by medication (20), and reduction of sugar consumption through taxation on sugar-sweetened beverages (38, 39) were also reported to reduce the burden of CVDs (Table 3).
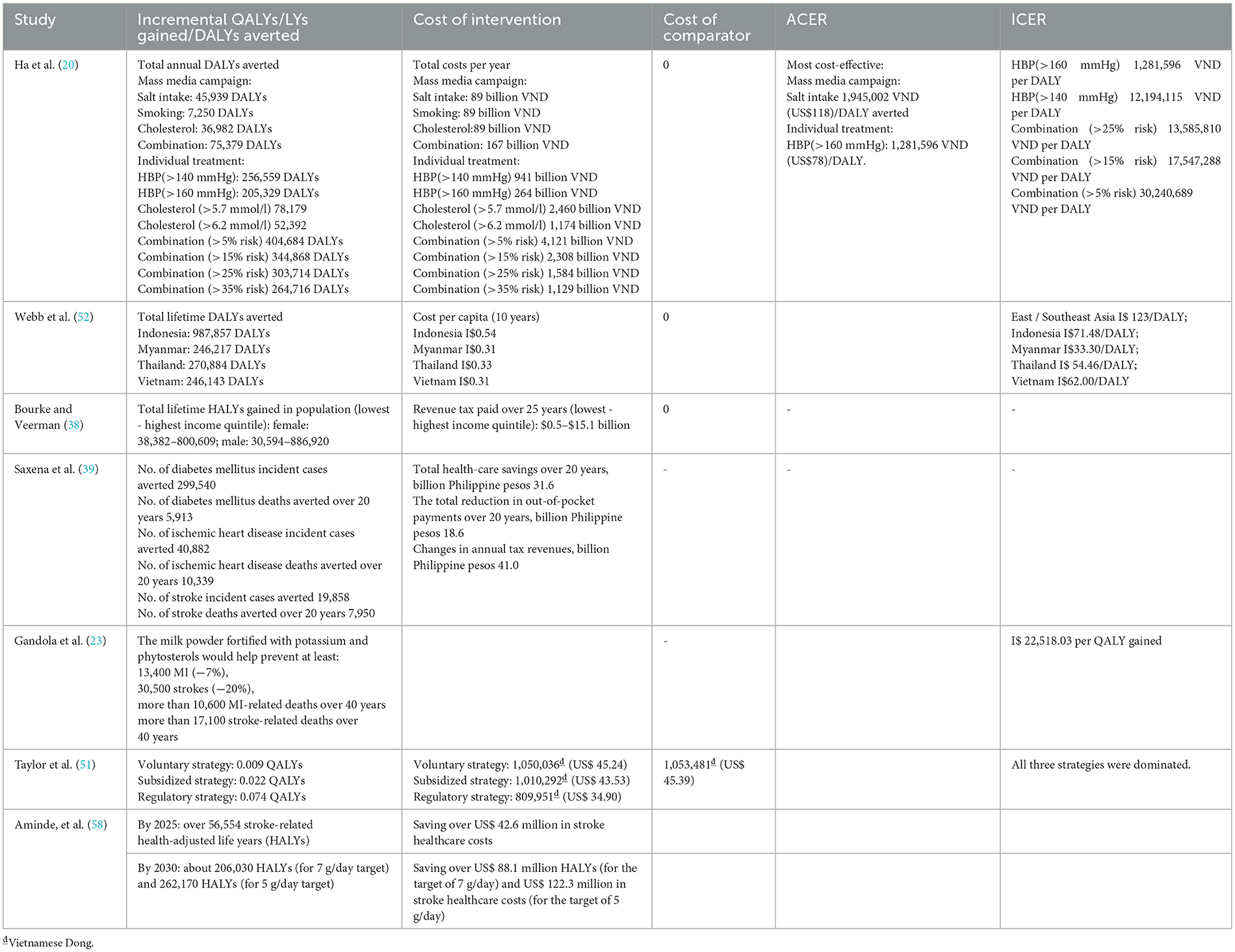
Table 3. Results of costs and effects; cost-effectiveness studies focused on prevention of unhealthy diet.
Four studies in our review assessed the cost-effectiveness of reducing salt intake through a mass media campaign in Vietnam (20, 49, 51) or in a combination of SEA countries (52). Ha and Chisholm (20) looked at the introduction of a mass media campaign to reduce salt intake compared to a broad context of health care interventions. The study compared different health education interventions through mass media in a Vietnamese setting, i.e., (1) to reduce salt intake; (2) to reduce smoking; (3) to reduce cholesterol concentrations and (4) a combination of these three strategies. A mass media campaign focused on the reduction of salt intake turned out to be the most cost-effective option with a cost-effectiveness ratio of US$ 118/DALY averted. Webb et al. (52) focused on an intervention that combined targeted industry agreements and public education to decrease population sodium intake. Overall, the study concluded that introducing this ‘soft regulation' intervention would be considered highly cost-effective worldwide, since 99.6% of the countries under study identified a cost-effective ratio of <1 times the gross domestic product (GDP) per capita. The ICER of the combined region of South and SEA was 123 I$/DALY. Taylor et al. (51) compared salt substitution strategies using potassium chloride to reduce sodium intake vs. no substitution. They found that all three strategies, e.g., voluntary strategy (no involvement or coordination from government in the market and food industry, no coordinated mass media campaign), subsidized strategy (a communication and media campaign to drive uptake), and regulatory strategy (no media campaign as compliance was assured through regulation) were cost-effective (51).
Bourke and Veerman (38) and Saxena et al. (39) assessed the cost-effectiveness of a tax increase on sugar-sweetened beverages in Indonesia and the Philippines. According to both studies, the tax increase on sugared drinks would be cost-effective in preventing NCDs such as T2DM, ischemic heart disease, stroke, and obesity. The interventions focused on increasing tax compared to no taxation, in which all tax payments came from the client's pocket, instead of the producer's pocket. In both countries, health effects and reduction of out-of-pocket payments for health care services through increasing tax were greater for higher-income quintiles compared to the lower-income quintiles. Nevertheless, assessing the impact of the taxation from a societal perspective instead of a health care perspective or governmental perspective could change the cost-effectiveness of this intervention by including the higher spending of the consumers.
3.2. Cost-effectiveness of interventions on CVD
3.2.1. Primary/secondary prevention (e.g., screening and treatment for risk factors)
Within our review, seven studies assessed the prevention of CVD and related risk factors in Vietnam (18, 20), Thailand (56), Indonesia (16, 19) and Malaysia (23, 54).
Interventions focused on individuals in the study by Ha and Chisholm (20) were divided into two categories: treatments based on elevated levels of cholesterol and systolic blood pressure, and treatments based on the 10-year risk (5, 15, 25, and 35% individual risk) of a CVD event. High cholesterol treatment (>5.7 mmol/l and >6.2 mmol/l) was based on treatment with statins, elevated systolic blood pressure (>140 mmHg or >160 mmHg) was treated with a combination of a β-blocker and a diuretic, and individual risk treatment was based on a combination regime of aspirin, diuretics, β-blockers, and statins. The authors concluded that the individual treatment of systolic blood pressure >160 mmHg would be the most cost-effective intervention (US$78 per DALY), even comparing with population-based mass media strategies. However, with a limited budget for investing in such health care interventions, mass media education on salt intake and a combination of targeting salt intake, cholesterol and tobacco should be considered as the first step in the prevention of CVDs. Treatment for elevated levels of systolic blood pressure or at-risk individuals for CVD could also be considered as cost-effective interventions in this country (20). In Thailand, the authors estimated the cost-effectiveness of a self-management program (joining educational session to get information about metabolic syndrome, metabolic control, and self-management skills) vs. the control group (receiving general advice or ordinary care, such as weight control and exercise) among patients with metabolic syndrome. The intervention was found to be cost-effective and recommended to be applied in health care settings, which can reduce the burden of the metabolic syndrome (56). For Malaysia, the consumption of a milk powder product fortified with potassium (+1050.28 mg/day) and phytosterols (+1200 mg/day) was shown to be cost-effective to lower systolic blood pressure and low-density lipoprotein cholesterol, among 35- to 75-year-olds; the ICER was equal to I$ 22, 518.03 per QALY gained (23).
To detect risk factors and undiagnosed CVDs, four studies considered screening as an intervention in Vietnam (18), Malaysia (54), and Indonesia (16, 19). Selvarajah et al. (54) only considered the cost per high CVD risk detected, without the additional treatment. They concluded that a targeted gender- and age-specific screening compared to a universal screening strategy could contribute to effective allocation of already scarce resources. In Vietnam, the strategy of community screening for undiagnosed and untreated hypertension combined with an increase in concurrent treatment to prevent CVD was evaluated. Compared to a no-screening scenario, screening (selected based on age, sex, or screening interval) in general was considered cost-effective in the prevention and early detection of CVD (18). Similarly, Selvarajah et al. (54) found a significant impact of age, sex, and screening interval; a more beneficial cost-effectiveness ratio resulted when considering an increase in treatment uptake (scenario of uptake of treatment, adherence to treatment, and relative risk reductions for those adhering to treatment). A combination of screening and treatment strategies was assessed in the study by Rattanavipapong et al. (16) in the context of the Package of Essential non-communicable disease (PEN) interventions. A no-screening scenario for hypertension and diabetes was compared to the current PEN interventions, with only a once-in-a-lifetime screening, and two adjusted PEN policy options in which screening of high-risk individuals takes place at either the community level or at the primary healthcare level. As expected, implementation of all interventions dominated (fewer costs, higher health benefits) compared to the no-screening scenario, but the PEN strategy is still considered the most cost-effective option. Additionally, targeting specific high-risk individuals within the PEN strategy could improve the cost-effectiveness of this scenario. Another study in Indonesia, by Angell et al. (19), which assessed from a health system perspective, considered a mobile technology-enabled primary care intervention for CVD risk management (health staff assesses CVD risk using mobile technologies and provides a decision support application on a tablet device, including classification of risk level, consultations if needed, reminding patients to attend follow-up visits, adherence to medicine). It showed that the intervention is cost-effective in comparison with the usual care and it was therefore recommended for application in practice (19).
3.2.2. Tertiary prevention
This section covers reports on drug therapy and counseling for individuals who have had heart failure with reduced ejection fraction, atrial fibrillation, myocardial infarction, stroke and post-stroke (17, 21, 22, 24–26, 28–30, 57) (Supplementary Table S1).
All studies considered stroke prevention (21, 22, 24–26, 29), except one which evaluated treatment for heart failure patients with reduced ejection fraction (17, 28, 30, 57). The majority of these studies showed that the interventions were cost-effective (22, 24–26, 29). For example, Rivaroxaban was found to be cost-effective compared to Warfarin and Aspirin for Stroke Prevention Atrial Fibrillation (SPAF) in the Indonesian setting (22). In the study of Rattanachotphanit et al. (24) on patients with non-valvular atrial fibrillation and a high risk of thrombosis, direct-acting oral anticoagulant treatment was found to be cost-effective from both payer and societal perspectives for stroke prevention. One study in Malaysia used the shared care approach and evaluated the integrated care pathway for post stroke patients. It was implemented to guide primary care teams for incorporating further rehabilitation, and regular screening for post-stroke complications among patients residing at home. This intervention was very cost-effective in comparison with usual care (25). The study of Ng et al. (26) aimed to evaluate the cost-effectiveness of non-vitamin K antagonist oral anticoagulants (NOACs) and warfarin care bundles in patients with atrial fibrillation in Thailand; it showed that patient self-management of warfarin was a highly cost-effective intervention, while a novel oral anticoagulant was unlikely to be cost-effective with regard to stroke prevention (26). Among studies on stroke prevention, only the study on NOAC intervention in patients with atrial fibrillation was not found to be cost-effective (21). The study by Krittayaphong et al. (17), which investigated an add-on dapagliflozin treatment for heart failure patients with reduced ejection fraction, showed that it was a cost-effective treatment. In the study by Rattanavipapong et al. (29), both therapy with Alteplase combined with Endovascular vs. Alteplase and therapy of Endovascular vs. supportive care for acute ischemic stroke showed to be cost-effective interventions in Thailand.
Four studies are related to Acute Coronary Disease or heart failure (17, 28, 30, 57). All of them were found to be cost-effective interventions, except one scenario in the study of Mendoza et al. (28). That study in the Philippines suggested that the intervention is only likely to be cost-effective when add-on dapagliflozin treatment is compared with the standard therapy among heart failure with reduced ejection fraction. Krittayaphong and Permsuwan (17) evaluated treatment for heart failure patients with reduced ejection fraction and showed that add-on dapagliflozin treatment was cost-effective compared with standard therapy. At Thobari et al. (30) found that Ticagrelor was vastly more cost-effective compared to clopidogrel in treatment for acute coronary disease to prevent cardiovascular events in the Indonesian setting. Krittayaphong and Permsuwan (57) reported that treating patients with acute decompensated heart failure with Sacubitril-valsartan was cost- effective when compared to enalapril.
3.3. Cost-effectiveness of interventions on T2DM
3.3.1. Primary/secondary prevention of T2DM (screening and treating for risk factors)
From the studies included in this review, two studies focused on screening for T2DM in Indonesia (16) and in Vietnam (36), and one focused on the strategy of lifestyle interventions to prevent the development of T2DM in Thailand (56) (Supplementary Table S2).
As mentioned in Section 3.2.1, the PEN strategy was considered dominant (more effects and cost saving) in the screening for T2DM and hypertension (16). The second screening study considered the scenario of screening at community health stations vs. district health centers for different age groups (36). All scenarios were deemed cost-effective interventions, except screening among the group of people younger than 35 years at both community health stations and district health stations (36). The study on lifestyle modification was based on a self-management program (focused on retention of healthy behaviors using the self-management skills the participants were taught) (56). The self-management program was considered to be cost saving, most likely due to the longer time horizon of the analysis (56).
3.3.2. Tertiary prevention of T2DM
Within the diabetic population, preventive foot care, diabetic retinopathy screening, and effective glycemic control are considered in this section. Nine studies addressed the cost-effectiveness of glycemic control in T2DM, mainly assessing the different formulations of insulin (27, 31–35, 40, 55). There was one study on screening for diabetic peripheral neuropathy (41) and one on cost-effectiveness evaluation of bariatric surgery for morbidly obese patients with diabetes (37).
Switching to biphasic insulin from other glycemic control interventions (32) and starting it in insulin naïve patients (27) was found to be cost-effective in Indonesia. Introduction of long-acting insulin in insulin-naïve individuals resulted in a cost-effective scenario in Indonesia (31). However, in the context of Thailand, treatment with long-acting insulin was not considered cost-effective when compared to treatment with neutral protamine Hagedorn insulin (55). Furthermore, treatment with insulin detemir was not a cost-effective strategy, compared to insulin glargine treatment in Thailand (33). It is noted that all of these studies applied the IMS CORE Diabetes Model for their analysis.
The observational study of Priyadi et al. (34) in Indonesia showed that the cost-effectiveness values of T2DM treatment with complications of kidney and peripheral vascular disease varied between health care provider and payer perspectives. Reducing 1 mg/dL blood glucose in T2DM treatment without kidney complication would require lower cost than in T2DM treatment with complication of Peripheral Vascular Disease (PVD). From the perspective of the payer, ICER of complications of kidney disease was IDR 215.723 per 1 mg/dL blood glucose reduction, while that of complications of peripheral vascular disease was IDR 234.591 per 1 mg/dL blood glucose reduction. From the perspective of the healthcare provider, ICER of complications of kidney disease was IDR 166.289 per 1 mg/dL blood glucose reduction and that of complications of PVD was IDR 681.853 per 1 mg/dL blood glucose reduction.
A study in Vietnam showed that gliclazide-based intensive glucose control was cost-effective compared with standard glucose control, from a healthcare payer perspective (40). The ICER for a 5-year scenario was $1, 764 per LY and $1, 878 per QALY. A study in Cambodia that focused on estimating the burden of T2DM, in term of costs and impacts, demonstrated that coverage for medications would be cost-effective, with $27 per DALY averted (35).
A cross-sectional study comparing screening strategies, diabetic foot screen proforma vs. biothesiometry, found ICER equal to $41.79 per diabetic peripheral neuropathy case detected, among diabetic patients in Myanmar (41). Another study in Thailand performed a cost-effectiveness evaluation of bariatric surgery compared to standard treatment for T2DM control in morbidly obese T2DM patients. The ICER was 26, 907.76 THB/QALY, making it a cost-effective intervention (37).
3.4. Risk of bias
The quality of the studies reviewed was assessed using the CHEC-list, which identified several key sources of bias (Supplementary Document 2). Limited generalizability was a major concern, with only 22.2% of studies reporting on how their results could be implemented in other settings. Furthermore, only 35.6% of studies employed a societal perspective as recommended by the WHO CHOICE guidelines for cost-effectiveness analysis. Ethical and distributional issues were also frequently overlooked, with only 37.8% of studies explicitly addressing these concerns. Outcomes valuation and the choice of time horizon were additional sources of bias, with only 42.4 and 57.8% of studies, respectively performing model validity and extrapolation of the result into a life-time horizon. These biases highlight the need for caution when interpreting the results by carefully considering the characteristics of the population, the interventions under study, and the assumptions being made on the model.
4. Discussion
This review covers the cost-effectiveness of a range of interventions implemented in LMICs in SEA, including Indonesia, Vietnam, Thailand, the Philippines, Cambodia, Myanmar, and Malaysia. The interventions varied from screening and targeting specific groups for T2DM and CVDs to smoking cessation programs, discouragement of smoking or unhealthy diet through taxation, and health education. In CEAs related to tobacco use prevention, the cost-effectiveness of tax increase was confirmed in all related studies. Unhealthy diet prevention, mass media campaign, salt substitution strategy, and tax increase on sugar-sweetened beverages were also shown to be cost-effective in several settings. In addition, for CVD prevention, treatment of hypertension was found to be the most cost-effective intervention. Regarding T2DM prevention, all assessed screening strategies were cost-effective or even cost-saving, and a few strategies to prevent T2DM complications were found to be cost-effective in certain settings.
The WHO presented an updated list in 2017 of “best buys” interventions to inform policymakers on cost-effectiveness; the list includes recommended interventions focused on the prevention and control of NCDs (59). The interventions focus on both the main risk factors for NCDs (tobacco, harmful use of alcohol, unhealthy diet and physical inactivity) and the four disease areas (CVD, T2DM, cancer and chronic respiratory disease). The interventions presented were selected based on proven effectiveness and a clear link to the global NCD targets. All selected interventions were tested against the WHO average cost-effectiveness threshold of ≤ I$ 100/DALY averted in low and lower middle-income countries. Interventions above the I$ 100/DALY averted threshold, or with cost-effectiveness data not available, were labeled as such (59). Country specific or additional data is needed for these two intervention categories. In this literature review, we have provided an overview of the cost-effectiveness studies performed in SEA to compare interventions aimed at preventing or treating T2DM and/or hypertension and related CVDs. Comparing these studies to the WHO “best buys” interventions will help to prioritize interventions or combinations of interventions for upscaling in the SEA region.
Overall, the evidence on cost-effectiveness of prevention and treatment targeted at T2DM, hypertension, and CVD is scarce in SEA. This point was also mentioned in a similar review in LMICs over the world (58); for the prevention of harmful use of alcohol and physical inactivity, it is even absent. The WHO “best buys” and the literature presented in this review give an indication of interventions that are cost-effective in comparison with the absence of implementation. In general, the WHO “best buys” and the local literature were in line with the cost-effectiveness of the interventions reviewed herein. However, considering the limited health budgets in most SEA countries, funding for interventions must be allocated wisely to ensure maximum impact on health outcomes. Therefore, the budget impact of each intervention needs to be considered to establish a sustainable introduction of the specific interventions. Furthermore, prioritization of possible effective interventions requires country-specific information to assess the incremental cost-effectiveness and added value within the current health care systems and compared to any interventions already in place. Scientific evaluations of the cost-effectiveness of multiple preventive interventions and treatment strategies for T2DM and CVD, combined with country-specific data, could give first insights into these priorities. Studies such as those by Ha and Chisholm (20) and Ortegón et al. (60) help to balance the provision of healthcare with the highest value.
The countries included in this review are diverse with regard to economics, culture, implementation capacity, and health systems. No evidence was found for scaling up these interventions from one country to another country in this region. To scale up and transfer interventions to other countries, it is advised to consider other factors such as health impact, acceptability, sustainability, scalability, multisectoral actions, training needs, and suitability of existing facilities, besides the evidence on cost-effectiveness (59). Furthermore, it is important to put the intervention in the health care context of a country, considering potential obstacles to implementation such as different motivation, less adherence to treatment, different availability, and quality of service.
We reviewed the cost-effectiveness of NCD prevention and treatment programs that focused on T2DM, CVD and their risk factors conducted in LMICs in SEA. This review provides initial evidence that can support the efforts of scaling up interventions in this region.
When focusing on tobacco consumption in a community or primary healthcare setting, it is important to consider that patient-focused interventions like counseling are cost-effective. However, in combination with discouragement of tobacco use (e.g., taxation, warning on package) or increased awareness of the harm of tobacco products, they could even be more cost-effective. This finding was in line with results from a previous study of a review of primary and secondary prevention interventions for cardiovascular disease in all LMICs in the world (58, 61). Furthermore, when focusing on unhealthy diets in a community or primary healthcare setting, the reduction of salt intake, even when compared to tobacco use, is considered to be highly cost-effective. A systematic review of economic evaluations of population-based sodium reduction interventions in all settings (62) or in South Asian countries (61) also showed similar results. This suggests that salt reduction should be a primary target when considering changing unhealthy diets. Unfortunately, no specific community based or primary healthcare-based interventions were evaluated with respect to cost-effectiveness in a SEA setting.
When focusing on the primary or secondary prevention of CVD in a community or primary healthcare setting, individual drug treatment should be one of the priorities, even more in comparison to population-based interventions like mass media campaigns focused on, for example, salt intake. Screening, preferably in the community, can be a cost-effective addition in identifying at risk or undiagnosed CVD patients. This finding was also mentioned in recent reviews of primary or secondary prevention interventions for CVD, T2DM in LMICs (58, 63). However, with limited resources available, investing in mass media education in prevention of CVD should be considered first, because of the lower costs. Furthermore, when focusing on the primary or secondary prevention of T2DM in a community or primary healthcare setting, lifestyle interventions and/or drug treatment should be considered.
An approach of combined interventions (treatment and prevention) and the WHO “best buys” recommendations suggest that combining community-based intervention with primary health care will help to reduce costs and provide synergistic effects to interventions (20) and provide an example of such an intervention of mass media education and treatment for hypertension or lowering cholesterol. Another example is the combination of targeted industry agreements and public education in the reduction of sodium intake (52). Multiple SEA countries, like Vietnam, Indonesia, and Myanmar, stayed well below the WHO threshold of 100 I$/DALY averted with an ICER ranging from 30 to 70 I$/DALY averted; therefore, the combined approach may be recommended for other countries in the region. However, further cost-effectiveness evidence of these combined interventions is needed in a local context to decide on the added value per country.
Concerning the intervention design, no evidence was available on the cost-effectiveness of interventions aimed at the underlying health system to improve NCD management, such as interventions that synergize community-based intervention and health facility intervention vs. usual care or that improve the capacity of the health service. Also, evidence on the cost-effectiveness of interventions that treated hypertension integrated with T2DM is not yet available. From the methodological perspective, several studies conducted CEA by comparing an intervention with a no intervention-scenario, while the WHO CEA guideline advice is to compare the intervention with the current best alternative intervention(s) in place. Therefore, future studies may consider using this as a comparator instead.
ICER and thresholds used varied across the studies. This observation is similar to that in a previous review on lung cancer; it is well-known that the cost-effectiveness of interventions can vary in the local environment of one country to another (64). According to WHO “best buys,” except for tertiary prevention among the T2DM population, a cut-off threshold of I$100 per DALY averted in LMICs should be applied to deem an intervention cost-effective. Papers included in this review applied either a cut-off point in terms of GDP per capita per DALY averted or a specific threshold of 160, 000 BAHT/QALY or 120, 000 BAHT/QALY in Thailand (~10, 000–14, 000 I$ or ½ × GDP per capita per DALY averted). Noticeably, some of them did not quantify their outcome as QALY or DALY and did not introduce a threshold in their study (34, 38, 39, 41, 43, 49, 54). In general, CEAs in SEA show cost-effectiveness and recommend applying these interventions in practice. Exceptions are the studies in Thailand by Permsuwan et al. (55) and Permsuwan et al. (33) that switched insulin from one to another type and the study on stroke prevention by Dilokthornsakul et al. (21). However, specific information is needed per country to assess the ICER and added value in the current health care, comparing to the interventions already in place, or to prioritize between different prevention options.
A strength of this review is the identification of the WHO “best buys” as a guideline of possible interventions to be considered for implementation and upscaling in LMICs in SEA. In addition, several interventions are suggested for inclusion in WHO's list, such as screening and managing CVD and DM2, providing pharmacological therapies for reducing tobacco use, or healthy lifestyle to prevent CVD (Box 1).
Box 1. Recommendations of cost-effectiveness interventions to beat NCD in LMICs in SEA.
Reducing tobacco use.
• Discouragement of tobacco use through taxation, warning on package.
• Counseling, brief advice to smokers.
• Health education to increase awareness of the harm of tobacco products.
Reducing unhealthy diet.
• Reducing salt intake through a government “soft regulation” strategycombines targeted industry agreements, government monitoring, and public education.
• Reducing salt intake through behaviors change communication andmass media campaigns.
• Reducing sugar consumption through effective taxation onsugar-sweetened beverages.
Prevention and management of CVD.
• Screening and managing CVDs.
• Individual drug treatment.
• Mass media campaign.
Manage diabetes.
• Individual drug treatment.
• Lifestyle intervention.
A limitation of this study is that updated and country specific information is scarce. Before scaling up any of the interventions, however, further assessment of the prioritization of the different healthcare interventions is needed. Only one study in Vietnam focused on the prioritization between different prevention options (20). In this review, we found a lack of overall prioritization of interventions, while there are many options for interventions to reduce the NCD burden in the region. In the context of budget scarcity, further evidence should be provided to set priorities and to guide local policymakers. Out of the 42 studies included, 37 were designed as modeling studies. These model-based evaluations require many input parameters for their study's purpose, however, most of them lack local context data and must depend on assumptions. These models could be updated when local data of each country becomes available.
Future studies may consider other interventions which reduce harmful alcohol intake, physical inactivity, or investigate synergies between health facility interventions and community interventions. Moreover, they could consider implementation factors in a specific context, such as acceptability, feasibility, and relevance to current policies of a country.
5. Conclusion
This review shows that the cost-effectiveness of preventive strategies in SEA against type 2 diabetes mellitus, cardiovascular diseases (CVDs), and their major NCDs risk factors are heterogenous in both methodology as well as outcome. This review combined with the WHO “best buys” list and could be a guideline of possible interventions to be considered for implementation and upscaling in LMICs in SEA. However, updated and country-specific information is needed to further assess the prioritization of the different healthcare interventions. In addition, several interventions which have not yet been included in the “best buys” list could be proposed to WHO for potential inclusion.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
T-P-LN contributed to conception, design of the study, and wrote the first draft of manuscript. MRR and JvdS organized the database. All authors performed data analysis and interpretation, wrote sections of the manuscript, contributed to manuscript revision, read, and approved the submitted versions.
Funding
Scaling-Up NCD Interventions in South-East Asia (SUNI-SEA) is a research consortium project delivered through a collaboration of nine consortium members. This project has received funding from the European Union's Horizon 2020 research and innovation program grant agreement no. 825026, under the umbrella of the Global Alliance for Chronic Diseases (project SU 2).
Acknowledgments
We would like to thank members of publication committee of the SUNI-SEA those gave us valuable comments. We also appreciate Pamela Wright for reviewing the English in this paper.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1206213/full#supplementary-material
References
1. World Health Organization. Non-Communicable Diseases: Progress Monitor 2020. Geneva: World Health Organization (2020).
2. International Diabetes Federation. IDF diabetes atlas tenth edition 2021: Global diabetes data report 2000-2045. (2021). Available online at: https://diabetesatlas.org/data/en/world/ (accessed November 30, 2021).
3. Allen L, Cobiac L, Townsend N. Quantifying the global distribution of premature mortality from non-communicable diseases. J. Pub. Health. (2017) 39:698–703. doi: 10.1093/pubmed/fdx008
4. Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392:1736–88. doi: 10.1016/S0140-6736(18)32203-7
5. Allen LN, Wigley S, Holmer H. Implementation of non-communicable disease policies from 2015 to 2020: a geopolitical analysis of 194 countries. Lancet Glob Health. (2021) 9:e1528–38. doi: 10.1016/S2214-109X(21)00359-4
6. World Health Organization. Noncommunicable Diseases. (2021). Available online at: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed October 7, 2021).
7. United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development (2015) 1–35 p.
8. Zhao D. Epidemiological features of cardiovascular disease in Asia. JACC. (2021) 1:1–13. doi: 10.1016/j.jacasi.2021.04.007
9. International Diabetes Federation. IDF Diabetes Atlas, 9th Edn. Brussels: International Diabetes Federation (2019), p. 1–168.
10. Walker IF, Garbe F, Wright J, Newell I, Athiraman N, Khan N, et al. The economic costs of cardiovascular disease, diabetes mellitus, and associated complications in South Asia: a systematic review. Value Health Reg Issues. (2018) 15:12–26. doi: 10.1016/j.vhri.2017.05.003
11. World Health Organization. Global Atlas on Cardiovascular Disease Prevention and Control. Geneva: World Health Organization (2011).
12. World Health Organization. Global Strategy for the Prevention and Control of Noncommunicable Diseases. Geneva: World Health Organization (2011), p. 6.
13. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
14. United Nations. World Economic Situation and prospects 2022. New York, NY. (2022). Available online at: https://desapublications.un.org/file/728/download (accessed March 17, 2021).
15. Evers S, Goossens M, De Vet H, Van Tulder M, Ament A. Criteria list for assessment of methodological quality of economic evaluations: consensus on health economic criteria. Int J Technol Assess Health Care. (2005) 21:240–5. doi: 10.1017/S0266462305050324
16. Rattanavipapong W, Luz ACG, Kumluang S, Kusumawardani N, Teerawattananon Y, Indriani D, et al. One step back, two steps forward: an economic evaluation of the PEN program in Indonesia. Health Syst Reform. (2016) 2:84–98. doi: 10.1080/23288604.2015.1124168
17. Krittayaphong R, Permsuwan U. Cost-utility analysis of add-on dapagliflozin treatment in heart failure with reduced ejection fraction. Int J Cardiol. (2021) 322:183–90. doi: 10.1016/j.ijcard.2020.08.017
18. Nguyen TPL, Wright EP, Nguyen TT, Schuiling-Veninga CCM, Bijlsma MJ, Nguyen TBY, et al. Cost-effectiveness analysis of screening for and managing identified hypertension for cardiovascular disease prevention in Vietnam. PLoS ONE. (2016) 11:1–17. doi: 10.1371/journal.pone.0155699
19. Angell B, Lung T, Praveen D, Maharani A, Sujarwoto S, Palagyi A, et al. Cost-effectiveness of a mobile technology-enabled primary care intervention for cardiovascular disease risk management in rural Indonesia. Health Policy Plan. (2021) 36:435–43. doi: 10.1093/heapol/czab025
20. Ha DA, Chisholm D. Cost-effectiveness analysis of interventions to prevent cardiovascular disease in Vietnam. Health Policy Plan. (2011) 26:210–22. doi: 10.1093/heapol/czq045
21. Dilokthornsakul P, Nathisuwan S, Krittayaphong R, Chutinet A, Permsuwan U. Cost-effectiveness analysis of non-vitamin K antagonist oral anticoagulants versus warfarin in Thai patients with non-valvular atrial fibrillation. Heart Lung Circ. (2020) 29:390–400. doi: 10.1016/j.hlc.2019.02.187
22. Dwiprahasto I, Kristin E, Endarti D, Pinzon RT, Yasmina A, Thobari JA, et al. Cost effectiveness analysis of rivaroxaban compared to warfarin and aspirin for stroke prevention atrial fibrillation (SPAF) in the Indonesian healthcare setting. Ind J Pharm. (2019) 30:74–84. doi: 10.14499/indonesianjpharm30iss1pp74
23. Gandola AE, Dainelli L, Zimmermann D, Dahlui M, Detzel P. Milk powder fortified with potassium and phytosterols to decrease the risk of cardiovascular events among the adult population in Malaysia: a cost-effectiveness analysis. Nutrients. (2019) 11:6. doi: 10.3390/nu11061235
24. Rattanachotphanit T, Limwattananon C, Waleekhachonloet O, Limwattananon P, Sawanyawisuth K. Cost-effectiveness analysis of direct-acting oral anticoagulants for stroke prevention in Thai patients with non-valvular atrial fibrillation and a high risk of bleeding. Pharmacoeconomics. (2019) 37:279–89. doi: 10.1007/s40273-018-0741-3
25. Abdul Aziz AF, Mohd Nordin NA, Muhd Nur A, Sulong S, Aljunid SM. The integrated care pathway for managing post stroke patients (iCaPPS©) in public primary care health centres in Malaysia: impact on quality adjusted life years (QALYs) and cost effectiveness analysis. BMC Geriatr. (2020) 20:1–10. doi: 10.1186/s12877-020-1453-z
26. Ng SS, Nathisuwan S, Phrommintikul A, Chaiyakunapruk N. Cost-effectiveness of warfarin care bundles and novel oral anticoagulants for stroke prevention in patients with atrial fibrillation in Thailand. Thromb Res. (2020) 185:63–71. doi: 10.1016/j.thromres.2019.11.012
27. Shafie AA, Gupta V, Baabbad R, Hammerby E, Home P. An analysis of the short- and long-term cost-effectiveness of starting biphasic insulin aspart 30 in insulin-naïve people with poorly controlled type 2 diabetes. Diabetes Res Clin Pract. (2014) 106:319–27. doi: 10.1016/j.diabres.2014.08.024
28. Mendoza VL, Tumanan-Mendoza BA, Punzalan FER. Cost-utility analysis of add-on dapagliflozin in heart failure with reduced ejection fraction in the Philippines. ESC Heart Fail. (2021) 8:5132–41. doi: 10.1002/ehf2.13583
29. Rattanavipapong W, Worakijthamrongchai T, Soboon B, Luankongsomchit V, Kongmuangpuk M, Isaranuwatchai W, et al. Economic evaluation of endovascular treatment for acute ischaemic stroke in Thailand. BMJ Open. (2022) 12:1–7. doi: 10.1136/bmjopen-2022-064403
30. Thobari J, Krisdinarti L, Nugroho D, Haposan J, Firdaus I, Suryandani RR, et al. Cost-effectiveness of Ticagrelor for acute coronary disease to prevent cardiovascular events in three hospitals in Indonesia. Open Access Maced J Med Sci. (2022) 10:1211–7. doi: 10.3889/oamjms.2022.9671
31. Home P, Baik SH, Gálvez GG, Malek R, Nikolajsen A. An analysis of the cost-effectiveness of starting insulin detemir in insulin-naïve people with type 2 diabetes. J Med Econ. (2015) 18:230–40. doi: 10.3111/13696998.2014.985788
32. Gupta V, Baabbad R, Hammerby E, Nikolajsen A, Shafie AA. An analysis of the cost-effectiveness of switching from biphasic human insulin 30, insulin glargine, or neutral protamine Hagedorn to biphasic insulin as part 30 in people with type 2 diabetes. J Med Econ. (2015) 18:263–72. doi: 10.3111/13696998.2014.991791
33. Permsuwan U, Thavorn K, Dilokthornsakul P, Saokaew S, Chaiyakunapruk N. Cost-effectiveness of insulin detemir versus insulin glargine for Thai type 2 diabetes from a payer's perspective. J Med Econ. (2017) 20:991–9. doi: 10.1080/13696998.2017.1347792
34. Priyadi A, Permana H, Muhtadi A, Sumiwi SA, Sinuraya RK, Suwantika AA. Cost-effectiveness analysis of type 2 diabetes mellitus (T2DM) treatment in patients with complications of kidney and peripheral vascular diseases in Indonesia. Healthcare. (2021) 9:1–9. doi: 10.3390/healthcare9020211
35. Feldhaus I, Nagpal S, Verguet S. Alleviating the burden of diabetes with health equity funds: economic evaluation of the health and financial risk protection benefits in Cambodia. PLoS ONE. (2021) 16:628. doi: 10.1371/journal.pone.0259628
36. Toi PL, Wu O, Thavorncharoensap M, Srinonprasert V, Anothaisintawee T, Thakkinstian A, et al. Economic evaluation of population-based type 2 diabetes mellitus screening at different healthcare settings in Vietnam. PLoS ONE. (2021) 16:1–18. doi: 10.1371/journal.pone.0261231
37. Viratanapanu I, Romyen C, Chaivanijchaya K, Sornphiphatphong S, Kattipatanapong W, Techagumpuch A, et al. Cost-effectiveness evaluation of bariatric surgery for morbidly obese with diabetes patients in Thailand. J Obes. (2019) 2019:1–14. doi: 10.1155/2019/5383478
38. Bourke EJ, Veerman JL. The potential impact of taxing sugar drinks on health inequality in Indonesia. BMJ Glob Health. (2018) 3:1–8. doi: 10.1136/bmjgh-2018-000923
39. Saxena A, Koon AD, Lagrada-Rombaua L, Angeles-Agdeppa I, Johns B, Capanzana M. Modelling the impact of a tax on sweetened beverages in the Philippines: an extended cost–effectiveness analysis. Bull World Health Organ. (2019) 97:97–107. doi: 10.2471/BLT.18.219980
40. Nguyen-Thi HY, Nguyen NTQ, Le NDT, Beillat M, Ethgen O. Cost-effectiveness of gliclazide-based Intensive glucose control vs. standard glucose control in type 2 diabetes mellitus: an economic analysis of the ADVANCE trial in Vietnam. Front Public Health. (2020) 8:1–9. doi: 10.3389/fpubh.2020.562023
41. Hnit MW, Han TM, Nicodemus L. Accuracy and cost-effectiveness of the diabetic foot screen proforma in detection of diabetic peripheral neuropathy in Myanmar. J ASEAN Fed Endocr Soc. (2022) 37:31–7. doi: 10.15605/jafes.037.01.06
42. Higashi H, Barendregt JJ. Cost-effectiveness of tobacco control policies in Vietnam: The case of personal smoking cessation support. Addiction. (2011) 107:658–70. doi: 10.1111/j.1360-0443.2011.03632.x
43. Tan QY, Zomer E, Owen AJ, Chin KL, Liew D. Impact of tobacco use on health and work productivity in Malaysia. Tob Control. (2020) 29:111–7. doi: 10.1136/tobaccocontrol-2018-054677
44. Satyana RPU, Uli RE, Magliano D, Zomer E, Liew D, Ademi Z. Assessing the impact of smoking on the health and productivity of the working-age Indonesian population using modelling. BMJ Open. (2020) 10:1–12. doi: 10.1136/bmjopen-2020-041832
45. Tosanguan J, Chaiyakunapruk N. Cost-effectiveness analysis of clinical smoking cessation interventions in Thailand. Addiction. (2016) 111:340–50. doi: 10.1111/add.13166
46. Nguyen DT, Luong KN, Phan HT, Tran AT, Dao ST, Poudel AN, et al. Cost-effectiveness of population-based tobacco control interventions on the health burden of cardiovascular diseases in Vietnam. Asia Pac J Public Health. (2021) 33:854–60. doi: 10.1177/1010539521999873
47. Thavorn K, Chaiyakunapruk N. A cost-effectiveness analysis of a community pharmacist-based smoking cessation programme in Thailand. Tob Control. (2008) 17:177–82. doi: 10.1136/tc.2007.022368
48. Cheng KJG, Estrada MAG. Cost-effectiveness analysis of the 2019 cigarette excise tax reform in the Philippines. Prev Med. (2021) 145:106431. doi: 10.1016/j.ypmed.2021.106431
49. Aminde LN, Phung HN, Phung D, Cobiac LJ, Veerman JL. Dietary salt reduction, prevalence of hypertension and avoidable burden of stroke in Vietnam: modelling the health and economic impacts. Front Pub Health. (2021) 9: 682975. doi: 10.3389/fpubh.2021.682975
50. Matheos CC, Liew D, Zomer E, Ademi Z. Cost-effectiveness analysis of tobacco control strategies in Indonesia. Value Health Reg Issues. (2023) 33:65–75. doi: 10.1016/j.vhri.2022.08.013
51. Taylor C, Hoek AC, Deltetto I, Peacock A, Ha DTP, Sieburg M, et al. The cost-effectiveness of government actions to reduce sodium intake through salt substitutes in Vietnam. Arch Pub Health. (2021) 79:1–13. doi: 10.1186/s13690-021-00540-4
52. Webb M, Fahimi S, Singh GM, Khatibzadeh S, Micha R, Powles J, et al. Cost effectiveness of a government supported policy strategy to decrease sodium intake: global analysis across 183 nations. BMJ. (2017) 24:356. doi: 10.1136/bmj.i6699
53. Higashi H, Truong KD, Barendregt JJ, Nguyen PK, Vuong ML, Nguyen TT, et al. Cost-effectiveness of tobacco control policies in Vietnam. Appl Health Econ Health Policy. (2011) 9:183–96. doi: 10.2165/11539640-000000000-00000
54. Selvarajah S, Haniff J, Kaur G, Guat Hiong T, Bujang A, Chee Cheong K, et al. Identification of effective screening strategies for cardiovascular disease prevention in a developing country: using cardiovascular risk-estimation and risk-reduction tools for policy recommendations. BMC Cardiovasc Disord. (2013) 13:1–10. doi: 10.1186/1471-2261-13-10
55. Permsuwan U, Chaiyakunapruk N, Dilokthornsakul P, Thavorn K, Saokaew S. Long-term cost-effectiveness of insulin glargine versus neutral protamine hagedorn insulin for type 2 diabetes in Thailand. Appl Health Econ Health Policy. (2016) 14:281–92. doi: 10.1007/s40258-016-0228-3
56. Sakulsupsiri A, Sakthong P, Winit-Watjana W. Cost-effectiveness analysis of the self-management program for Thai patients with metabolic syndrome. Value Health Reg Issues. (2016) 9:28–35. doi: 10.1016/j.vhri.2015.10.004
57. Krittayaphong R, Permsuwan U. Cost-utility analysis of sacubitril-valsartan compared with enalapril treatment in patients with acute decompensated heart failure in Thailand. Clin Drug Investig. (2021) 41:907–15. doi: 10.1007/s40261-021-01079-6
58. Aminde LN, Takah NF, Zapata-Diomedi B, Veerman JL. Primary and secondary prevention interventions for cardiovascular disease in low-income and middle-income countries: a systematic review of economic evaluations. Cost Effectiv Res Alloc. (2018) 16:1–34. doi: 10.1186/s12962-018-0108-9
59. World Health Organization. “Best Buys” and Other Recommended Interventions for the Prevention and Control of Noncommunicable Diseases. Geneva: World Health Organization. (2017).
60. Ortegón M, Lim S, Chisholm D, Mendis S. Cost effectiveness of strategies to combat cardiovascular disease, diabetes, and tobacco use in sub-Saharan Africa and South East Asia: Mathematical modelling study. BMJ. (2012) 344:1–15. doi: 10.1136/bmj.e607
61. Singh K, Chandrasekaran AM, Bhaumik S, Chattopadhyay K, Gamage AU, De Silva P, et al. Cost-effectiveness of interventions to control cardiovascular diseases and diabetes mellitus in South Asia: a systematic review. BMJ Open. (2018) 8:e017809. doi: 10.1136/bmjopen-2017-017809
62. Hope SF, Webster J, Trieu K, Pillay A, Ieremia M, Bell C, et al. A systematic review of economic evaluations of population-based sodium reduction interventions. PLoS ONE. (2017) 17:3600. doi: 10.1371/journal.pone.0173600
63. Sharma M, John R, Afrin S, Zhang X, Wang T, Tian M, et al. Cost-effectiveness of population screening programs for cardiovascular diseases and diabetes in low- and middle-income countries: a systematic review. Fron Pub Health. (2022)10:820750. doi: 10.3389/fpubh.2022.820750
Keywords: cost-effectiveness, non-communicable disease, prevention, risk factor, Southeast Asia, scoping review
Citation: Nguyen T-P-L, Rokhman MR, Stiensma I, Hanifa RS, Ong TD, Postma MJ and van der Schans J (2023) Cost-effectiveness of non-communicable disease prevention in Southeast Asia: a scoping review. Front. Public Health 11:1206213. doi: 10.3389/fpubh.2023.1206213
Received: 15 April 2023; Accepted: 25 September 2023;
Published: 09 November 2023.
Edited by:
Anoop Kumar, Delhi Pharmaceutical Sciences and Research University, IndiaReviewed by:
Guvenc Kockaya, Analysis and Consultancy Plc., TürkiyeKrzysztof Kaczmarek, Medical University of Silesia, Poland
Copyright © 2023 Nguyen, Rokhman, Stiensma, Hanifa, Ong, Postma and van der Schans. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Thi-Phuong-Lan Nguyen, bmd1eWVudGhpcGh1b25nbGFuQHRubWMuZWR1LnZu; bnRwbGFuNzVAZ21haWwuY29t